Nuovi anticoagulanti orali nella fibrillazione atriale: impariamo ad usarli Raffaele De Caterina Tigullio Cardiologia 2016 Santa Margherita Ligure, 7-8 aprile 2016 Centro Congressi Grand Hotel Miramare Sessione Plenaria 4 Terapia antitrombotica 7 aprile 2016 - ore 16:00-17:40 Sala Portofino Università “G. d’Annunzio” – Chieti e Fondazione “G. Monasterio” – Pisa, Italia 7 aprile 2016, 16:00-16:20, 20 min. + 5 min. disc.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Nuovi anticoagulanti orali nella fibrillazione atriale: impariamo ad usarli
Raffaele De Caterina
Tigullio Cardiologia 2016 Santa Margherita Ligure, 7-8 aprile 2016
Centro Congressi Grand Hotel Miramare
Sessione Plenaria 4Terapia antitrombotica7 aprile 2016 - ore 16:00-17:40
Sala Portofino
Università “G. d’Annunzio” – Chieti eFondazione “G. Monasterio” – Pisa, Italia
7 aprile 2016, 16:00-16:20, 20 min. + 5 min. disc.

Prof. Raffaele De CaterinaConflitti d’interesse
§ Co-author ESC Guidelines on Atrial Fibrillation 2010-2012
§ Steering Committee member, National Coordinator forItaly, and Co-author of APPRAISE-2, ARISTOTLE,AVERROES, ENGAGE-AF, Re-DUAL PCI
§ Fees, honoraria and research funding from Sanofi-Aventis, Boehringer Ingelheim, Bayer, BMS/Pfizer,Daiichi-Sankyo, Novartis, Merck

3 argomenti principali
}Pazienti con alterata funzione renale
}La fibrillazione atriale «valvolare»
}Pazienti a basso rischio tromboembolico
3 argomenti principali
}Pazienti con alterata funzione renale
}La fibrillazione atriale «valvolare»
}Pazienti a basso rischio tromboembolico
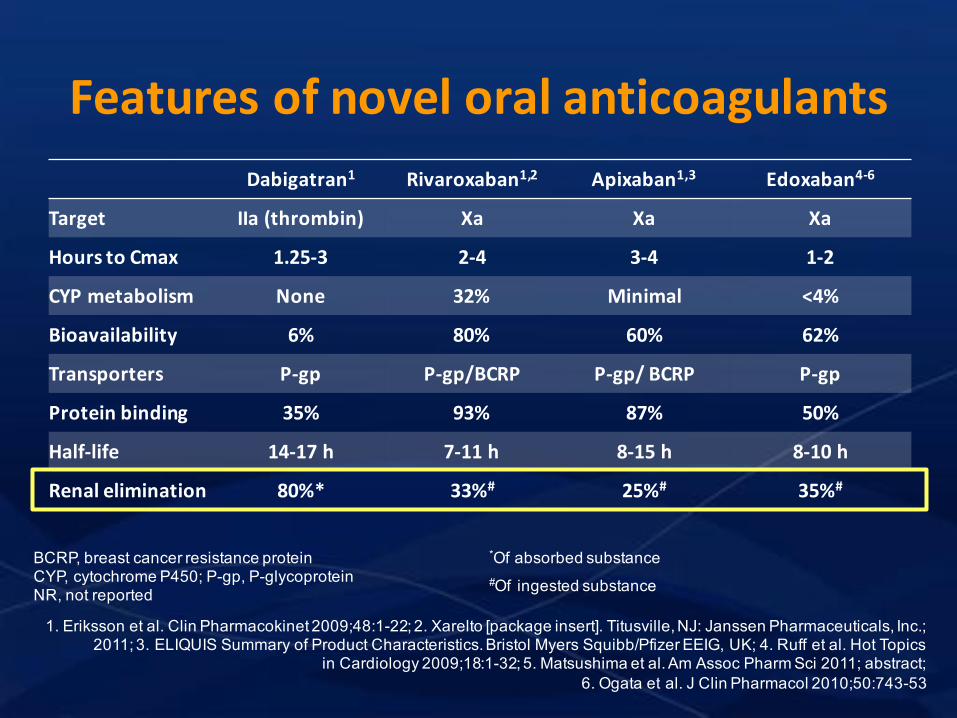
FeaturesofnoveloralanticoagulantsDabigatran1 Rivaroxaban1,2 Apixaban1,3 Edoxaban4-6
Target IIa(thrombin) Xa Xa Xa
HourstoCmax 1.25-3 2-4 3-4 1-2
CYPmetabolism None 32% Minimal <4%
Bioavailability 6% 80% 60% 62%
Transporters P-gp P-gp/BCRP P-gp/BCRP P-gp
Proteinbinding 35% 93% 87% 50%
Half-life 14-17h 7-11h 8-15h 8-10h
Renalelimination 80%* 33%# 25%# 35%#
1. Eriksson et al. Clin Pharmacokinet 2009;48:1-22; 2. Xarelto [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc.; 2011; 3. ELIQUIS Summary of Product Characteristics. Bristol Myers Squibb/Pfizer EEIG, UK; 4. Ruff et al. Hot Topics
in Cardiology 2009;18:1-32; 5. Matsushima et al. Am Assoc Pharm Sci 2011; abstract; 6. Ogata et al. J Clin Pharmacol 2010;50:743-53
BCRP, breast cancer resistance protein CYP, cytochrome P450; P-gp, P-glycoproteinNR, not reported
*Of absorbed substance#Of ingested substance

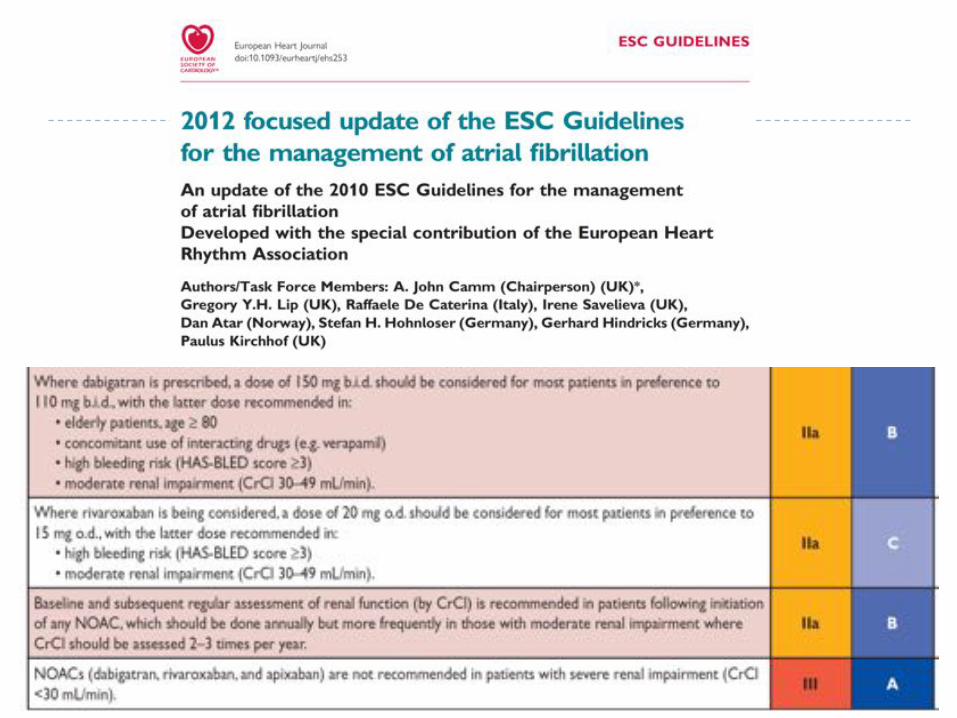
Rationale for caution with regard to NOACs} All NOACs have some degree of renal excretion and
therefore accumulation in cases of impaired renal function
} This is in contrast with VKAs, which are all removed through the liver
} Therefore: caution of use in case of renal insufficiency
} But:} How to estimate renal function} What threshold level to use for «caution»} What specific threshold and dose adjustment to use for
the different NOACs
How to estimate renal function} Creatinine clearance (CrCl) as an approximation of the
glomerular filtration rate (GFR)} Problems with measurement of CrCl (U x V/P) due to the
need of 24h urine collection and day-to-day variability} Therefore estimated CrCl (eCrCl) have become the
standard, through formulas estimating it based on serum creatinine and on anthropometric variables} Cockroft-Gault} MDRD} CK-Epi} Mayo quadratic formula} Schwartz formula
} Cystatin C levels-based method
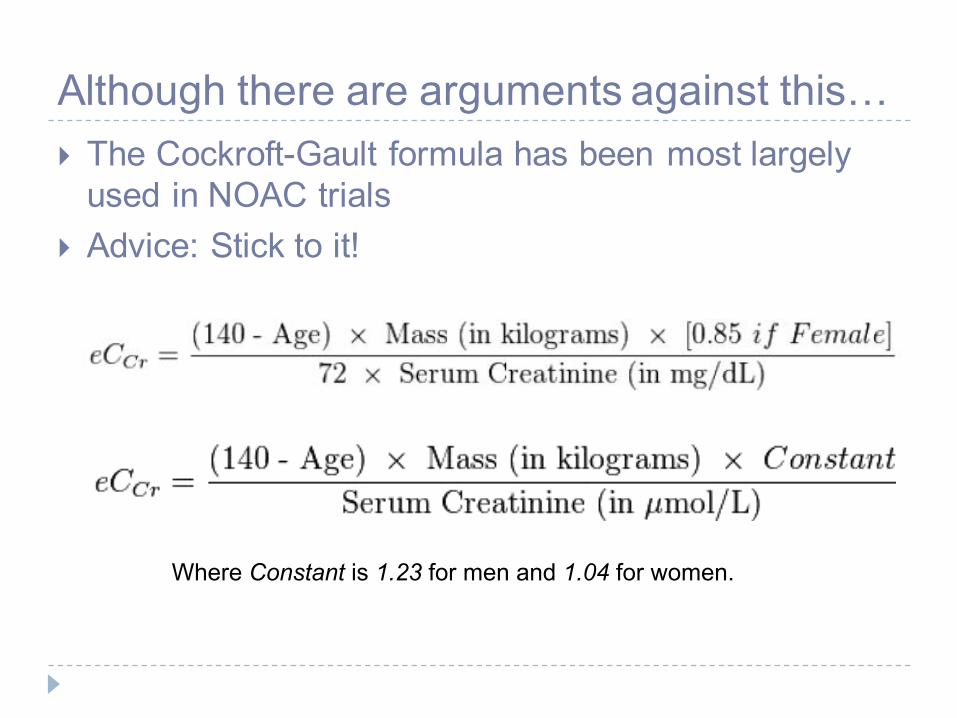
Although there are arguments against this…} The Cockroft-Gault formula has been most largely
used in NOAC trials} Advice: Stick to it!
Where Constant is 1.23 for men and 1.04 for women.
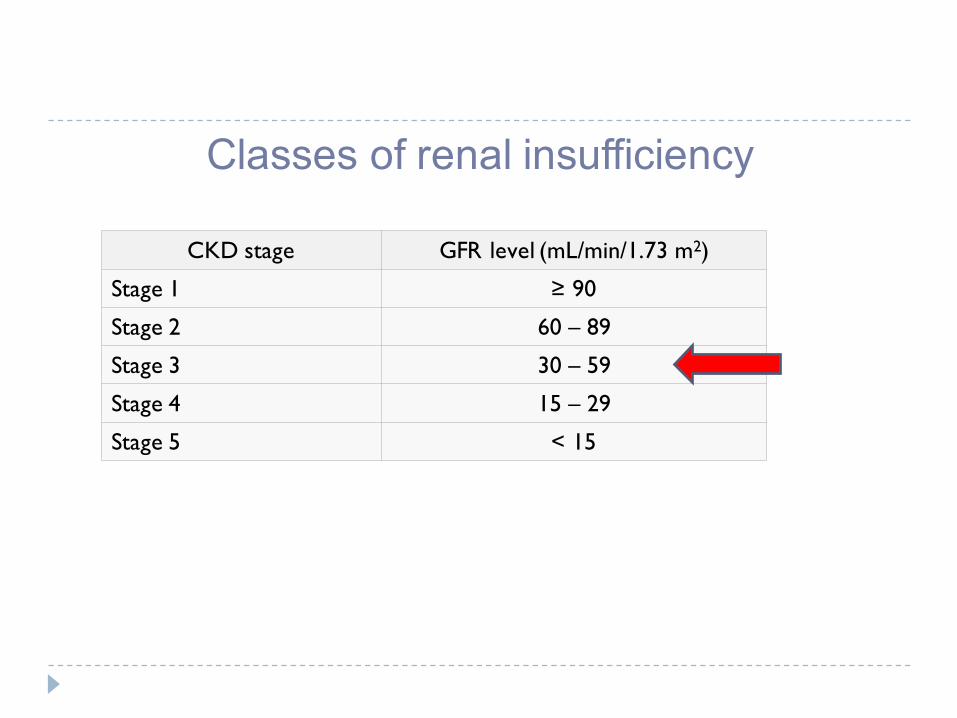
Classes of renal insufficiency
CKD stage GFR level (mL/min/1.73 m2)
Stage 1 ≥ 90
Stage 2 60 – 89
Stage 3 30 – 59
Stage 4 15 – 29
Stage 5 < 15
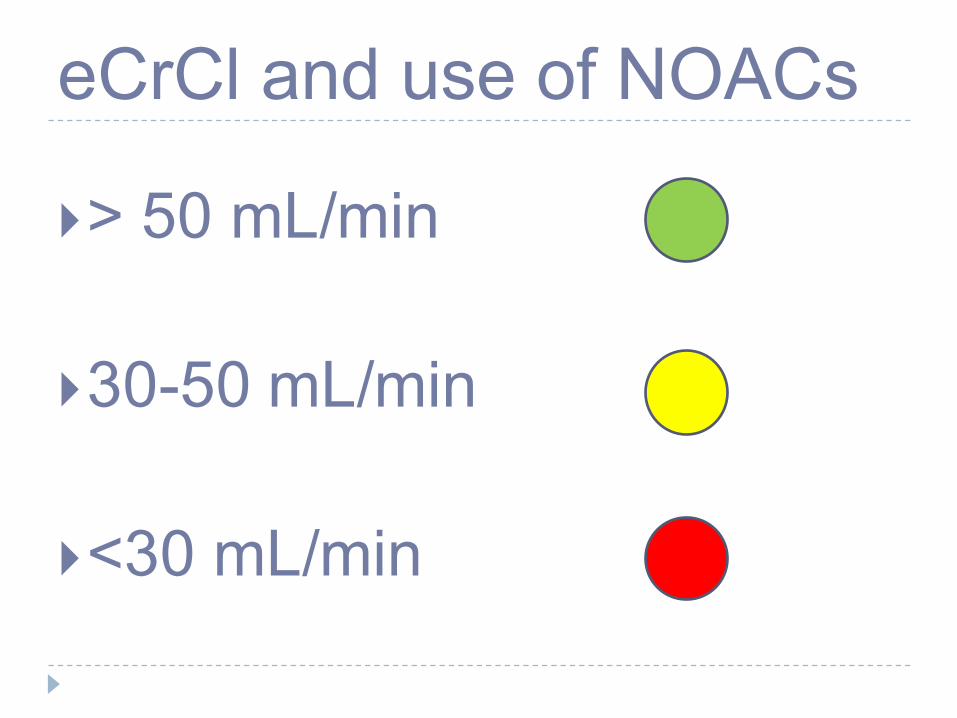
eCrCl and use of NOACs
}> 50 mL/min
}30-50 mL/min
}<30 mL/min

Specific recommendations for the 4 NOACs in non-valvular AF in patients with renal insufficiency

3 argomenti principali
}Pazienti con alterata funzione renale
}La fibrillazione atriale «valvolare»
}Pazienti a basso rischio tromboembolico
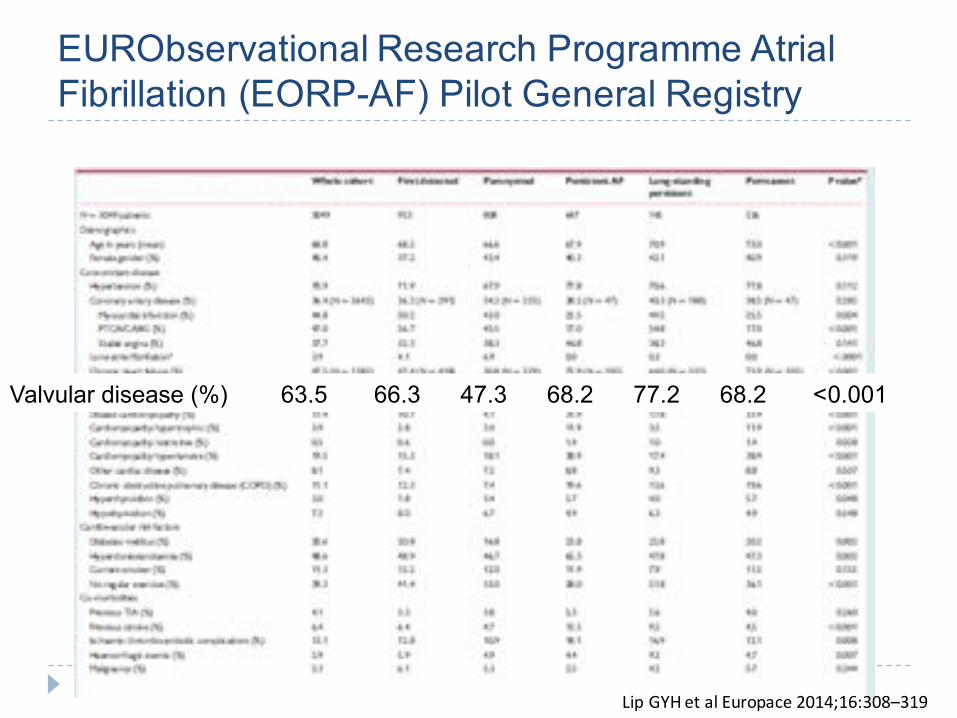
EURObservational Research Programme Atrial Fibrillation (EORP-AF) Pilot General Registry
LipGYHetalEuropace2014;16:308–319
Valvular disease (%) 63.5 66.3 47.3 68.2 77.2 68.2 <0.001

Valvular AF: Changing definitions in guidelines} By convention, the term nonvalvularAF is restricted to cases in
which the rhythm disturbance occurs in the absence of rheumatic mitral stenosis or a prosthetic heart valve.ACC/AHA/ESC 2001 Guidelines for the Management of Patients With Atrial Fibrillation
- FusterV et al
} By convention, the term “non-valvularAF” is restricted to cases in which the rhythm disturbance occurs in the absence of rheumatic mitral valve disease, a prosthetic heart valve, or mitral valve repair.’American College of Cardiology/American Heart Association/European Society of
Cardiology 2006 guidelines
} ValvularAF includes rheumatic valvular disease and prosthetic valves2012 focused update of the ESC Guidelines for the management of atrial fibrillation -
Camm J et al]

CONCLUSIONS
} Evidence of the lack of precise and unique definitions of the origin of AF
} Important heterogeneity and uncertainties in the answers given by physicians who usually treat patients with AF
} It is urgent to issue clear widely accepted definitions of the origin of AF, which should improve clinical practice and research.

DeCaterinaF&CammAJEurHeartJ2014;35:3328-35
We propose the term ‘mechanical and rheumatic mitral valvular AF’ (acronym: MARM AF) as an accurate description of a disease entity worthy of being kept separated from other forms of AF, but with possible internal differences between the two conditions here encompassed.

Exclusion criteria regarding valvular disease in recent oral anticoagulation trialsRE-LY History of heart valve disorder (i.e. prosthetic valve or haemodynamically relevant valve disease)
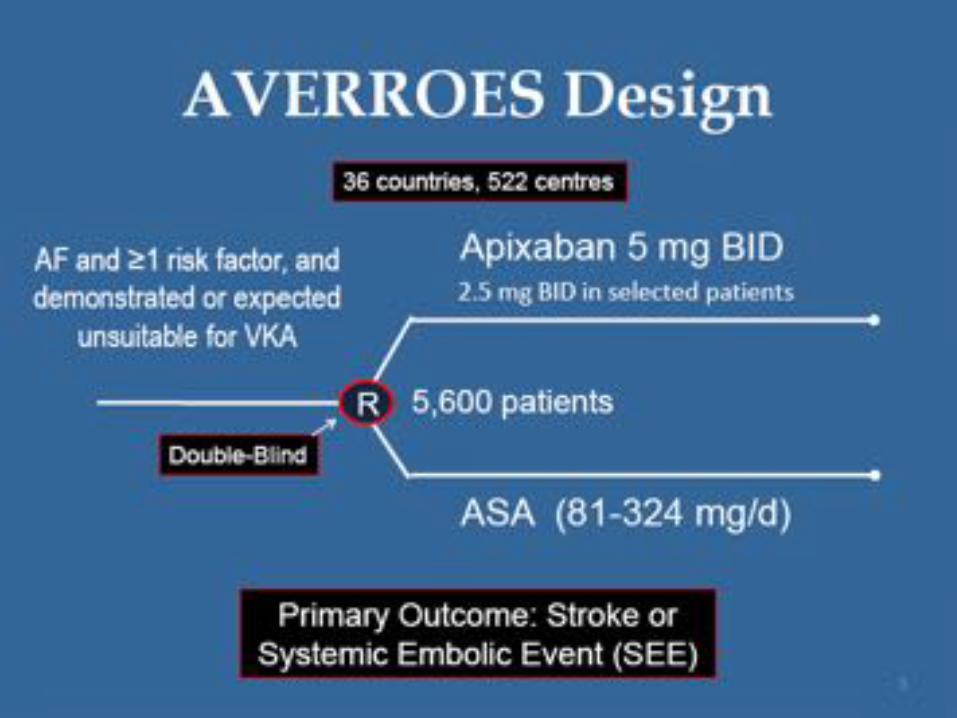
AVERROES Valvular disease requiring surgery. Prosthetic mechanical heart valve.
ROCKET AF Haemodynamically significant mitral valve stenosis. Prosthetic heart valve. Annuloplasty with or without prosthetic ring, commissurotomy, and/or valvuloplasty are permitted.
ARISTOTLE Moderate or severe mitral stenosis, conditions other than atrial fibrillation that required anticoagulation (e.g. a prosthetic heart valve)
ENGAGE-AF Moderate or severe mitral stenosis, unresected atrial myxoma, or a mechanical heart valve (subjects with bioprosthetic heart valves and/or valve repair could be included)
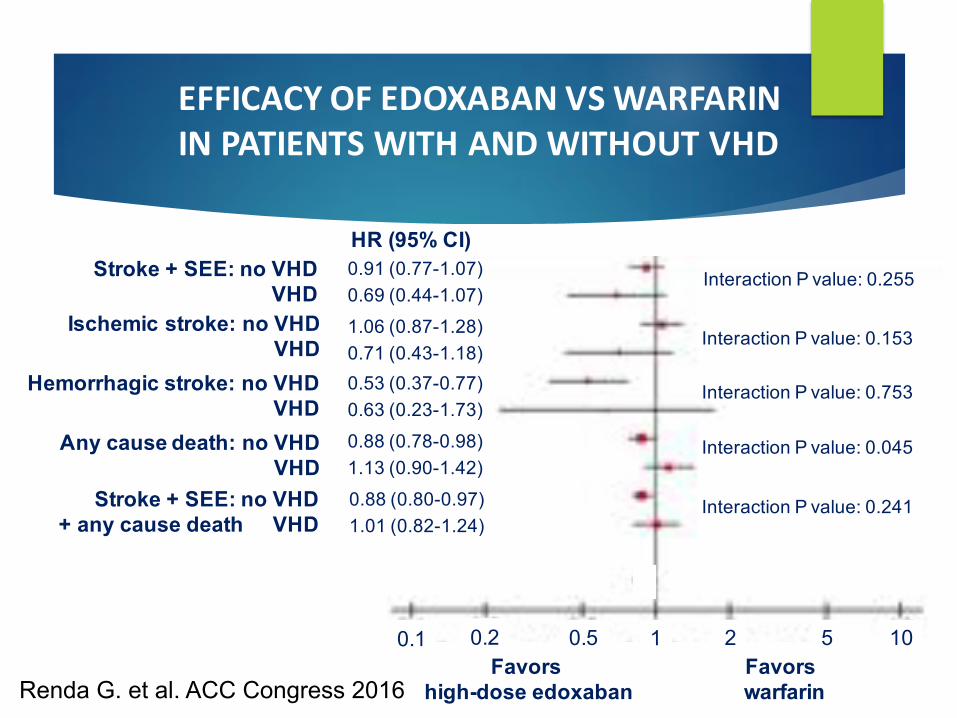
EFFICACYOFEDOXABANVSWARFARININPATIENTSWITHANDWITHOUTVHD
Stroke + SEE: no VHDVHD
Ischemic stroke: no VHDVHD
Hemorrhagic stroke: no VHDVHD
Any cause death: no VHDVHD
Stroke + SEE: no VHD+ any cause death VHD
Interaction P value: 0.255
Interaction P value: 0.153
Interaction P value: 0.753
Interaction P value: 0.045
Interaction P value: 0.241
Favors high-dose edoxaban
Favorswarfarin
HR (95% CI)
0.91 (0.77-1.07)0.69 (0.44-1.07)1.06 (0.87-1.28)0.71 (0.43-1.18)0.53 (0.37-0.77)0.63 (0.23-1.73)0.88 (0.78-0.98)1.13 (0.90-1.42)0.88 (0.80-0.97)1.01 (0.82-1.24)
105210.50.20.1
Renda G. et al. ACC Congress 2016

SAFETYOFEDOXABANVSWARFARININPATIENTSWITHANDWITHOUTVHD
Major bleeding: no VHDVHD
Intracranial bleeding: no VHDVHD
Major + clin. relevant: no VHDnon-major bleeding VHD
Any overt bleeding: no VHDVHD
Primary composite: no VHDoutcome VHD
Interaction P value: 0.573
Interaction P value: 0.675
Interaction P value: 0.469
Interaction P value: 0.274
Interaction P value: 0.414
Favors high-dose edoxaban
Favorswarfarin
HR (95% CI)0.82 (0.71-0.94)0.74 (0.53-1.02)0.48 (0.35-0.66)0.39 (0.15-0.98)0.85 (0.79-0.92)0.91 (0.76-1.09)0.86 (0.80-0.92)0.95 (0.80-1.12)0.88 (0.81-0.96)0.96 (0.8-1.15)
105210.50.20.1
Renda G. et al. ACC Congress 2016

EFFICACYOFNOACSVERSUSWARFARININPATIENTSWITHORWITHOUTVHD:
STROKE/SEE
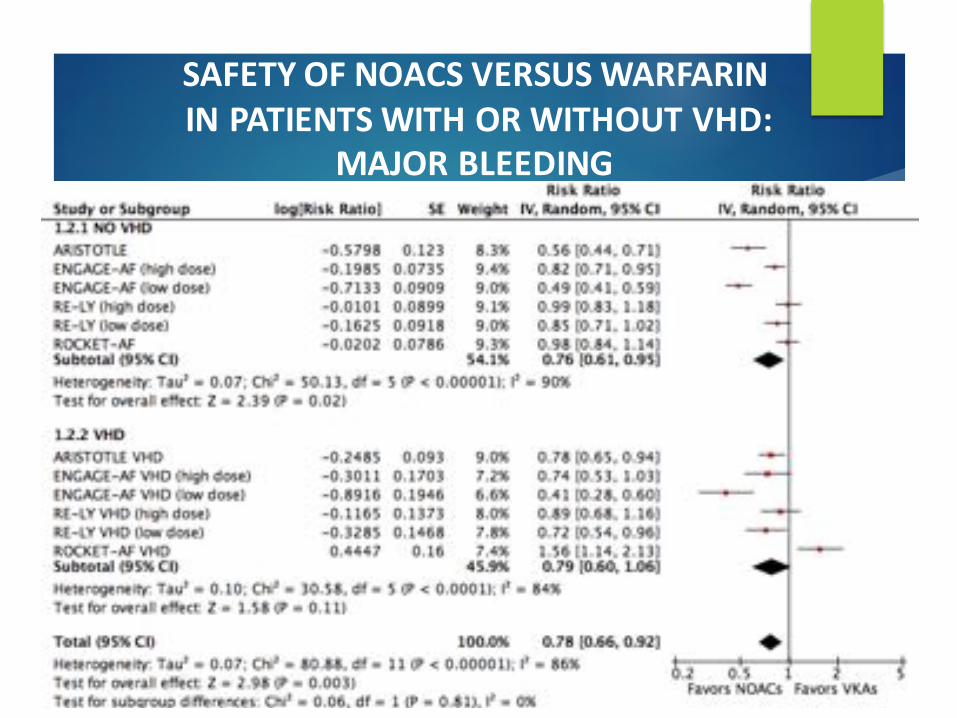
SAFETYOFNOACSVERSUSWARFARININPATIENTSWITHORWITHOUTVHD:
MAJORBLEEDING

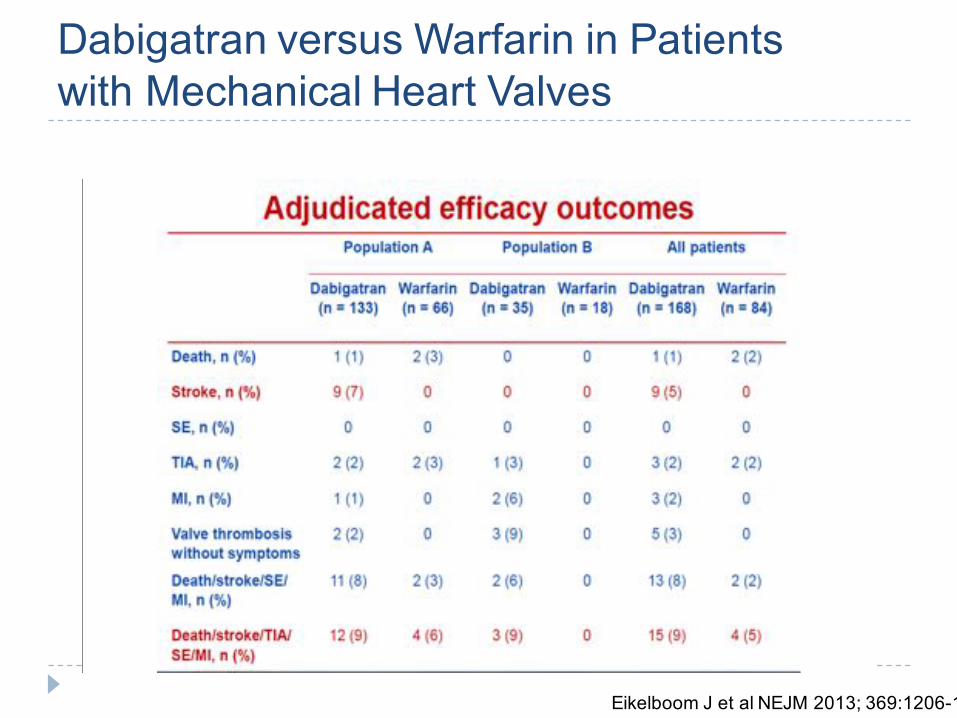
Dabigatran versus Warfarin in Patientswith Mechanical Heart Valves
Randomization 2:1 168 DE 84 warfarin
Eikelboom J et al NEJM 2013; 369:1206-14
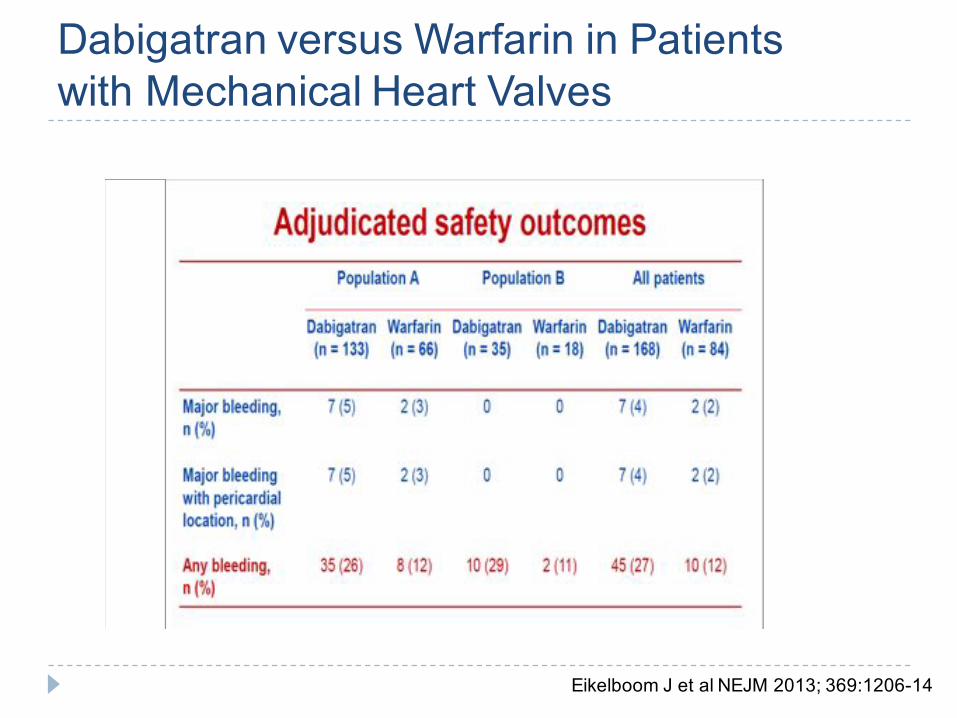
Dabigatran versus Warfarin in Patientswith Mechanical Heart Valves
Eikelboom J et al NEJM 2013; 369:1206-14
Dabigatran versus Warfarin in Patientswith Mechanical Heart Valves
Eikelboom J et al NEJM 2013; 369:1206-14

Dabigatran versus Warfarin in Patientswith Mechanical Heart Valves
Possible explanations for negative study results
Inadequate blood levels of dabigatran
Play of chance with relatively few events seen in the warfarin arm
Differences in the mechanism of action of dabigtran compared with warfarin
e.g., the inability of dabigatran to suppress activation of coagulation that occurs when blood is exposed to the artificial surface of prosthetic valves

} Best definition: «Mechanical valve And Rheumatic Mitral stenosis AF» (MARM-AF)
} Yet, these two settings—mechanical valve and rheumatic mitral stenosis—are quite different
}Can NOACs be used in mitral stenosis?

Giant left atrial thrombus in mitral stenosis

Why LA thrombosis in mitral stenosis may be different from mechanical valves
} No foreign surfaces} Preservation of the valvular endothelium
and presence of fibrotic tissue – no metal} Blood rheology changes and LA stasis
(giant left atrium), as in «non-valvular» AF, probably more relevant than contact activation of coagulation
} Contrary to (most) mechanical valves, standards with VKAs contemplate the same INR intensity as in «non-valvular» AF

A still huge epidemiological problem, but mostly affecting least-developed countries
3 argomenti principali
}Pazienti con alterata funzione renale
}La fibrillazione atriale «valvolare»
}Pazienti a basso rischio tromboembolico

Caso clinico
} A.P. è un signore di 45 anni, in buona forma fisica, non in sovrappeso, senza scompenso, diabete, senza evidenza di malattia vascolare
} Ma è iperteso, ben controllato con amlodipina + ramipril
} E’ stato sempre bene, tranne che per tre episodi di fibrillazione atriale parossistica, favoriti da pasti abbondanti, regrediti rapidamente
} Lo condanniamo subito alla iattura degli anticoagulanti?
Messaggio da portare a casa:
}Sì!!!

Due argomenti da discutere
}Fibrillazione atriale parossistica}Basso punteggio CHADS2VA2Sc

Due argomenti da discutere
}Fibrillazione atriale parossistica

This evidence has led to the current recommendations: treat AF according to patient’s risk profile, and NOT according to the presentation pattern of AF

Evidence-based Medicine
Not always what is logical is true…
But sometimes it is!



Due argomenti da discutere
}Fibrillazione atriale parossistica}Basso punteggio CHADS2VA2Sc
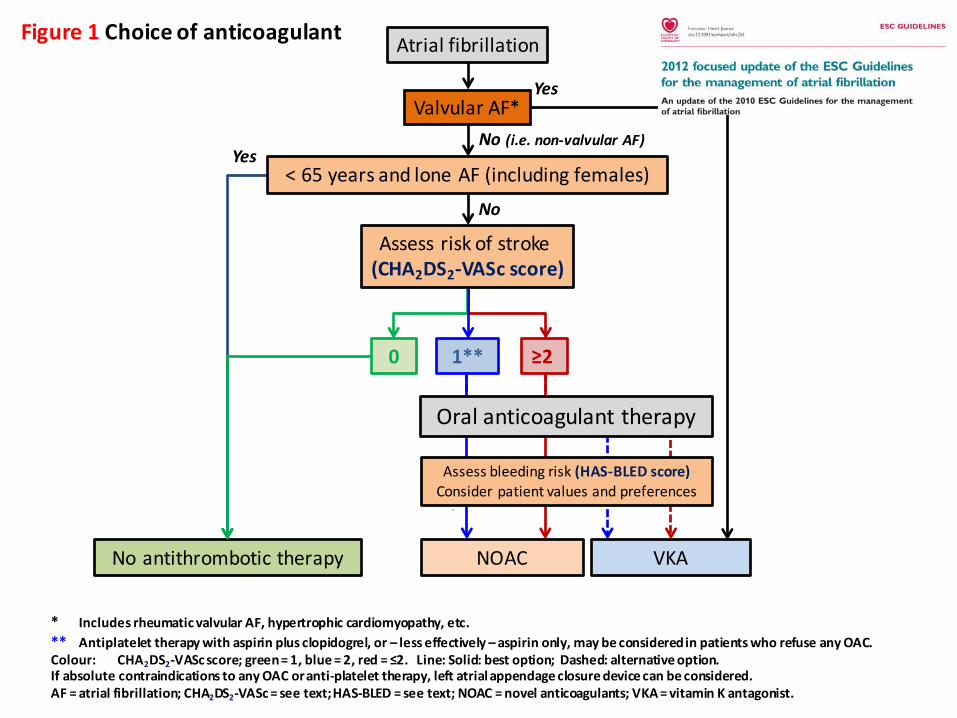
Atrialfibrillation
ValvularAF*
VKA
Yes
Noantithrombotictherapy
Yes
0
* IncludesrheumaticvalvularAF,hypertrophiccardiomyopathy,etc.** Antiplatelettherapywithaspirinplusclopidogrel,or– lesseffectively– aspirinonly,maybeconsideredinpatientswhorefuseanyOAC.Colour: CHA2DS2-VAScscore;green=1,blue=2,red=≤2.Line:Solid:bestoption;Dashed:alternativeoption.IfabsolutecontraindicationstoanyOACoranti-platelettherapy,leftatrialappendageclosuredevicecanbeconsidered.AF=atrialfibrillation;CHA2DS2-VASc=seetext;HAS-BLED=seetext;NOAC=novelanticoagulants;VKA=vitaminKantagonist.
1** ≥2
NOAC
Oralanticoagulanttherapy
Assessbleedingrisk(HAS-BLEDscore)Considerpatientvaluesandpreferences
No(i.e.non-valvularAF)
Assessriskofstroke(CHA2DS2-VAScscore)
No
<65yearsandloneAF(includingfemales)
Figure1 Choiceofanticoagulant

Is OAC Necessary in AF Patients with a CHA2DS2-VAScScore=1 (males) or 2 (females)? A nationwide cohort study
Chao, Liu … Lip, Chen. JACC 2015 ;65(7):635-42. Presented at ESC 2014
OAC should be consideredfor AF patients with 1additional stroke risk factor(ie. CHA2DS2-VASc score of1 (males) or 2 (females))
Ischaemic stroke rates in non-anticoagulated male andfemale patients with 1 additional stroke risk factor
AF females(CHA2DS2-VASc score=1)
AF males(CHA2DS2-VASc score=1)
AF males(CHA2DS2-VASc score=1)
AF females(CHA2DS2-VASc score=2)
Total PatientsCongestive heart failureHypertension
Age 65-74 yearsDiabetes mellitusVascular disease
Risk of ischemic stroke
Ann
ual r
ate o
f isc
hem
ic str
oke (
%)
0
1
2
3
4
5
2.75
2.372.18
3.50
2.96
1.96
2.55
2.22
1.91
3.34
2.88
2.250.23 0.30
0.500.33 0.26
0.39
Dabigatran 110mgDabigatran 150mgRivaroxaban 20/15 mgApixaban 5/2.5 mgEdoxaban 30 mgEdoxaban 60mg
Patients receiving NOACs in randomized trials*
Ann
ual r
ate o
f ICH
(%)
0
1
2
3

OAC, Aspirin, or No Therapy in Patients WithNonvalvular AF With 0 or 1 Stroke Risk Factor Based
on CHA2DS2-VASc scoreLip et al J Am Coll Cardiol 2015;65(14):1385-94
Low-risk patients have a truly low risk for stroke and bleeding.
With 1 additionalstroke risk factor,there was asignificantincrease in eventrates (particularlymortality) if non-anticoagulated.
Event Rates Per 100 PYs at 1 Year FU According to Treatment Strategy Initiated at Day 14 After Discharge With Incident AF

Net Clinical Benefit for Oral Anticoagulation,
Aspirin, or No Therapy in Nonvalvular AF Patients With One Additional Risk Factor of the CHA2DS2-
VASc Score (Beyond Sex)
Lip et al JACC 2015;66:488–90
Net clinical benefitNet clinical benefit analyses for 1 year offollow-up, for aspirin vs no treatment, warfarinvs no treatment, and for warfarin vs aspirin
No treatment
No treatment
Aspirin
Aspirin
Warfarin
Warfarin
–0.54 (-1.84 – 0.75)
+1.68(0.55-2.81)
+2.22(0.59-3.85)
‘….. This analysis supports a positiveadvantage for stroke prevention with OACs compared with no therapy or with aspirin among patients with AF who have a single stroke risk factor other than a sex factor (i.e., CHA2DS2-VASc score 1 in men or 2 in women)’

Is it worthwhile not to anticoagulate a patient in whom risk stratification is uncertain, in the era of NOACs?


Stroke Prevention in Atrial Fibrillation Proposed Anticoagulation Flow Chart
CHA2DS2-VASc= Congestive heart failure, Hypertension, Age ≥75 [doubled], Diabetes, Stroke [doubled]-Vascular disease, Age 65–74, Sex category [female]; NOACs = nonvitamin K antagonist oral anticoagulants
Modified from Lip GY, et al. International Journal of Cardiology 180 (2015) 246–254
Non-valvular AF
CHA2DS2-VASc Score
0 (male) or 1 (female)Ie, low risk
1 (male) ≥ 2
No antithrombotic therapy
NOACs(N)OACs

Grazie!
Related Documents











