Informatie Bethesda I 23.11% 54.25% 16.04% 3.77% 1.42% 1.42% 12.50% 57.70% 19.60% 4.20% 1.80% 4.20% 0.00% 10.00% 20.00% 30.00% 40.00% 50.00% 60.00% 70.00% Bethesda 1 Bethesda 2 Bethesda 3 Bethesda 4 Bethesda 5 Bethesda 6 Normal referrals Thyroid Pathway CONCLUSION Thyroid Pathway: a quick and comprehensive diagnostic pathway for patients with thyroid nodules or symptomatically enlarged thyroid gland Carlijn de Betue, Erik von Meyenfeldt, Jeanette Bakker, Elske Massolt, Francien van Nederveen. Albert Schweitzer Hospital, Dordrecht, the Netherlands. Department of surgery (CB, EM), radiology (JB), endocrinology (EM), pathology (FN) contact: [email protected] The International Forum on Quality and Safety in Healthcare – Amsterdam 2 – 4 May 2018 • With the “Thyroid Pathway” referral lines are clearer; with on-site cytological representability determination, non-diagnostic Bethesda 1 FNA-results can be decreased by ± 50%. • The “Thyroid Pathway” prevents repeat visits and diagnostic tests, leading to a decreased overall burden to patients and a quicker diagnosis and plan. BACKGROUND • GP’s refer patients with palpable thyroid nodule and/or symptomatically enlarged thyroid gland to our endocrine team (endocrinologists, radiologists, nuclear medicine specialists, pathologists, endocrine surgeons) for work-up and treatment for (suspected) thyroid cancer. • In the past it was unclear how and when to refer, leading to delays in diagnosis, repeat visits and inefficient use of resources for the hospital. • We redesigned the diagnostic process for this patient group, and named it the “Thyroid pathway” RESULTS 1 • Referral lines were clearer to GP’s and fellow hospital physicians, limiting the number of referrals to the “wrong” specialist or without the proper work- up, limiting repeat visits and diagnostic tests. • A year after implementation (2016) the number of non-diagnostic FNA’s (Bethesda 1) were 12.5% (of n=168) in patients within the Thyroid Pathway as compared to 23.1% (of n=212) for patients subjected to FNA without on-site cytological technician. This is a decrease of 46% non- diagnostic FNA’s, which require repeat FNA. METHODS Thyroid Pathway: Within 1 radiology department visit and 1 endocrinologist visit the patient receives a diagnostic/treatment plan. FNA = fine needle aspiration. TP = thyroid pathway. GP = general practitioner RESULTS 2 DISCUSSION - Problems encountered involve misplanning of patients (missing Pathway patients, wrong patients on Pathway- slots ); improved training of the planning personnel might improve this. - Involved healthcare providers need to be aware of the Thyroid Pathway and the associated benefits for improved referrals Fig 1. Classification of fine needle aspiration (FNA) samples in 2016, according to Bethesda system for reporting Thyroid Cytology Bethesda 1 is non-diagnostic and requires repeat FNA. Bethesda 2-6 classifies the cytology by the grade of suspicion of thyroid cancer (see pictures on the right). This figure shows the number per Bethesda classification within “Normal referrals” (blue) and patients within the “Thyroid Pathway”. In the Thyroid Pathway there were fewer non-diagnostic FNA’s. Good FNA quality Patient Refer to Thyroid Pathway (TP) GP TP time slot: Ultrasound + FNA Radiologist Assesment FNA quality Cytology technician Meeting: Results + plan Multidisplinary team First clinic visit: Discuss results + plan Endocrinologist Poor FNA quality: repeat FNA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Informatie
BethesdaI
23.11%
54.25%
16.04%
3.77% 1.42% 1.42%
12.50%
57.70%
19.60%
4.20% 1.80%
4.20%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
Bethesda1 Bethesda2 Bethesda3 Bethesda4 Bethesda5 Bethesda6
Normalreferrals ThyroidPathway
CONCLUSION
Thyroid Pathway: a quick and comprehensive diagnostic pathway for patients with thyroid nodules or symptomatically enlarged thyroid glandCarlijn de Betue, Erik von Meyenfeldt, Jeanette Bakker, Elske Massolt, Francien van Nederveen.Albert Schweitzer Hospital, Dordrecht, the Netherlands. Department of surgery (CB, EM), radiology (JB), endocrinology (EM), pathology (FN) contact: [email protected]
The International Forum on Quality and Safety in Healthcare – Amsterdam 2 – 4 May 2018
• With the “Thyroid Pathway” referral lines are clearer; with on-site cytological representability determination, non-diagnostic Bethesda 1 FNA-results can be decreased by ± 50%.
• The “Thyroid Pathway” prevents repeat visits and diagnostic tests, leading to a decreased overall burden to patients and a quicker diagnosis and plan.
BACKGROUND• GP’s refer patients with palpable thyroid nodule
and/or symptomatically enlarged thyroid gland to our endocrine team (endocrinologists, radiologists, nuclear medicine specialists, pathologists, endocrine surgeons) for work-up and treatment for (suspected) thyroid cancer.
• In the past it was unclear how and when to refer, leading to delays in diagnosis, repeat visits and inefficient use of resources for the hospital.
• We redesigned the diagnostic process for this patient group, and named it the “Thyroid pathway”
RESULTS 1• Referral lines were clearer to GP’s and fellow
hospital physicians, limiting the number of referrals to the “wrong” specialist or without the proper work-up, limiting repeat visits and diagnostic tests.
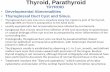
• A year after implementation (2016) the number of non-diagnostic FNA’s (Bethesda 1) were 12.5% (of n=168) in patients within the Thyroid Pathway as compared to 23.1% (of n=212) for patients subjected to FNA without on-site cytological technician. This is a decrease of 46% non-diagnostic FNA’s, which require repeat FNA.
METHODSThyroid Pathway:
Within 1 radiology department visit and 1 endocrinologist visit the patient receives a diagnostic/treatment plan. FNA = fine needle aspiration. TP = thyroid pathway. GP = general practitioner
RESULTS 2
DISCUSSION- Problems encountered involve misplanning of patients (missing Pathway patients, wrong patients on Pathway-
slots ); improved training of the planning personnel might improve this.- Involved healthcare providers need to be aware of the Thyroid Pathway and the associated benefits for
improved referrals
Fig 1. Classification of fine needle aspiration (FNA) samples in 2016, according to Bethesda system for reporting Thyroid CytologyBethesda 1 is non-diagnostic and requires repeat FNA. Bethesda 2-6 classifies the cytology by the grade of suspicion of thyroid cancer (see pictures on the right).This figure shows the number per Bethesda classification within “Normal referrals” (blue) and patients within the “Thyroid Pathway”.In the Thyroid Pathway there were fewer non-diagnostic FNA’s.
GoodFNAquality
Patient Refer to ThyroidPathway (TP)
GP
TPtimeslot:Ultrasound+FNA
Radiologist
Assesment FNAquality
Cytologytechnician
Meeting:Results +plan
Multidisplinaryteam
Firstclinic visit:Discuss results +plan
Endocrinologist
PoorFNAquality:
repeatFNA
Related Documents