THYROID GLAND By : Iman Qasem Kteo

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
THYROID GLAND
By : Iman Qasem Kteo

THE THYROID GLAND
The thyroid gland is a butterfly-shaped organ located in the Lower neck, anterior to the trachea.
***It consists of Two lateral lobes connected by an isthmus. 5
cm long and 3 cm wide and weighs about 30 g .
***The blood Flow to the thyroid is very high approximately
five times the blood flow to the Liver .
***This reflects the high metabolic activity of the thyroid
Gland

Functions
*** Stimulates & maintains metabolic processes
* Produces thyroid hormones T3-triiodothyronine and T4-thyroxine
* These hormones regulate metabolism & affect the growth and
function of other systems in the body
*** Secretes calcitonin to lower serum calcium levels
*** Parathyroid gland secretes PTH to raise serum calcium levels

HYPOTHYROIDISM - TESTS

•SERUM THYROID-STIMULATING HORMONE
the best way to initially test thyroid function is to measure the TSH level in a
blood sample.
**A high TSH level indicates that the thyroid gland is failing (primary
hypothyroidism) .
**the TSH level is low, usually indicates that the person has an overactive
thyroid that is producing too much thyroid hormone (hyperthyroidism


T4 TESTS
T4 circulates in the blood in two forms:
1 )T4 bound to proteins that prevent the T4 from entering the various tissues
that need thyroid hormone.
2 )free t4, which does enter the various target tissues to exert its effects .
T3 TESTS
Patients who are hyperthyroid will have an elevated T3 level. In some
individuals with a low TSH, only the T3 is elevated and the FT4 is
normal. T3 testing rarely is helpful in the hypothyroid patient, since it is
the last test to become abnormal .

Normal Value
T.S.H : 0.4 to 4.5 mU/L (milliunites per litre)
T3 : (1.15 to 3.10 nmol/L).
T4 : (58.5 to 150 nmol/L).

•THYROID ANTIBODIES
In many patients with hypothyroidism or hyperthyroidism, lymphocytes make
antibodies against their thyroid that either stimulate or damage the gland.. also
in diagnose the thyroid problems .
**positive anti-thyroid peroxidase and/or anti-thyroglobulin antibodies in a
patient with hypothyroidism make a diagnosis of hashimoto’s thyroiditis .
**+ev antibodies in a hyperthyroid patient,
the most likely diagnosis is autoimmune
thyroid disease

•RADIOACTIVE IODINE UPTAKE
The patient is Administered a tracer dose of iodine 123 (123I) or
another Radionuclide, With a scintillation counter, detects the
Gamma rays released from the breakdown of 123I in the thyroid .
**Patients with hyperthyroidism
exhibit a high uptake Of the 123I
** Patients with hypothyroidism
exhibit a very low uptake.

•THYROID SCAN, RADIOSCAN, OR SCINTISCAN
**determining the location, size, Shape, and anatomic
function of the thyroid gland
**Identifying Areas of increased function (“hot” areas) or
decreased function (“Cold” areas) can assist in diagnosis .
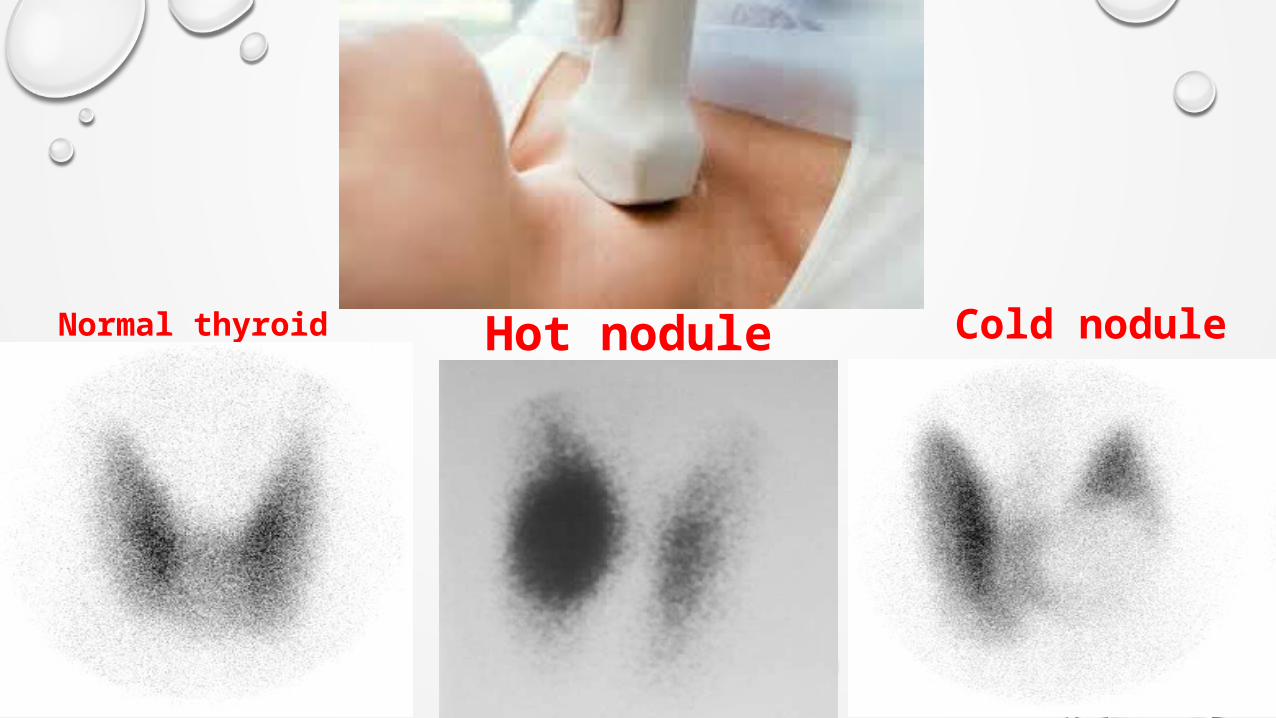
Normal thyroid Hot nodule Cold nodule

•FINE-NEEDLE ASPIRATION BIOPSY
Use of a small-gauge needle to sample the thyroid tissue for
Biopsy is a safe and accurate method of detecting malignancy..
Results are reported as
( 1 )negative (benign), (2) Positive (malignant) ,
(3 )indeterminate (suspicious), and (4) inadequate
(nondiagnostic).

FINE-NEEDLE ASPIRATION BIOPSY

•SERUM THYROGLOBULIN
Thyroglobulin (tg) can be measured reliably in the serum
By radioimmunoassay. Clinically, it is used to detect
persistence Or recurrence of thyroid carcinoma.

HYPERTHYROIDISM
◊ Hyperthyroidism is the second most prevalent endocrine Disorder, after
diabetes mellitus .
◊ Graves’ disease, the most Common type of hyperthyroidism, results
from an excessive Output of thyroid hormones
◊ It affects women eight times more frequently Than men

◊ The disorder may Appear after an
emotional shock,
stress ,
infection ,
◊ but The exact significance of these relationships is not understood.
◊ Other common causes of hyperthyroidism include Thyroiditis and
excessive ingestion of thyroid hormone

Signs and Symptoms – Exophthalmos – Weight loss despite excellent appetite – hypermetabolic state– Insomnia– Fatigue– Palpitations– Heat intolerance– Sweating– Diarrhea– Deterioration in handwriting– Menstrual irregularities– Muscle weakness/– Nervousness– Tachycardia– Goiter– Elevated plasma levels of thyroxin and/or triiodothyronine

Exophthalmos
Exophthalmos is a disease affecting the eyes. it is a
condition of altered thyroid metabolism that causes protein depositions
within the extra ocular muscles and causes the eyeballs to
protrude, forcing the eyelids open. This disease is more
common
in middle aged women and people who smoke.

CausesExophthalmos is most often caused by thyroid problems,
particularly Grave’s Disease. Less often, it can be caused by something in the eye socket such as:
Cancerous tumor Mucocoele (mucus-filled cyst) Blood clots Eye injury Sinus infection Bacterial infection

Symptoms include One or both eyes bulging out of the socket (more
commonly both eyes) Dry, red, & itchy eyes Puffy or swollen eyes Irritation Photophobia (sensitivity to light) Limited eye movement Blurred/double visionSymptoms will continue to worsen if not treated and can
lead to blindness.

THYROID STORM

THYROID STORM
Thyroid storm (thyrotoxic crisis) is a form of severe
hyperthyroidism, Usually of abrupt onset. Untreated, it is
almost always Fatal, but with proper treatment the mortality
rate is reduced Substantially. The patient with thyroid storm or
crisis is critically Ill and requires astute observation and
supportive Nursing care during.

CLINICAL MANIFESTATIONS
Thyroid storm is characterized by:
•High fever
•Extreme tachycardia
•Exaggerated symptoms of hyperthyroidism
,gastrointestinal (Weight loss, diarrhea, abdominal pain) or cardiovascular (Edema, chest pain, dyspnea, palpitations)
•Altered neurologic or mental state, which frequently Appears as delirium psychosis, somnolence, or coma

THYROID CANCER
Cancer of the thyroid is much less prevalent than other Forms
of cancer. There are several types of Cancer of the thyroid
gland . External radiation of the head, neck, or chest in infancy
And childhood increases the risk of thyroid carcinoma .

SIGNS AND SYMPTOMS
• Common
– Asymptomatic
mass
– Cough
– Dyspnea
– Dysphagia
• Common
– Asymptomatic
mass
– Cough
– Dyspnea
– Dysphagia
• Rare
– Pain
– Stridor
– Vocal cord paralysis
– Rapid enlargement
• Rare
– Pain
– Stridor
– Vocal cord paralysis
– Rapid enlargement

CAUSES AND RISK FACTORS Genetics: Family History: Radiation Exposure:
Radiation therapy to Head or Neck. Exposure to Radioactive Iodine during childhood, or other radioactive
substances Chronic Iodine deficiency ↑ risk for Follicular carcinoma.
Gender: Female > Males.
Age: More common at young adults.
Race: White race > Black race.

TYPE OF THYROID CANCER
•Papillary adenocarcinoma• Incidence 50%
Most common and least aggressive
Asymptomatic nodule in a normal gland
Starts in childhood or early adult life, remains localized
Metastasizes along the lymphatics if untreated
More aggressive in the elderly
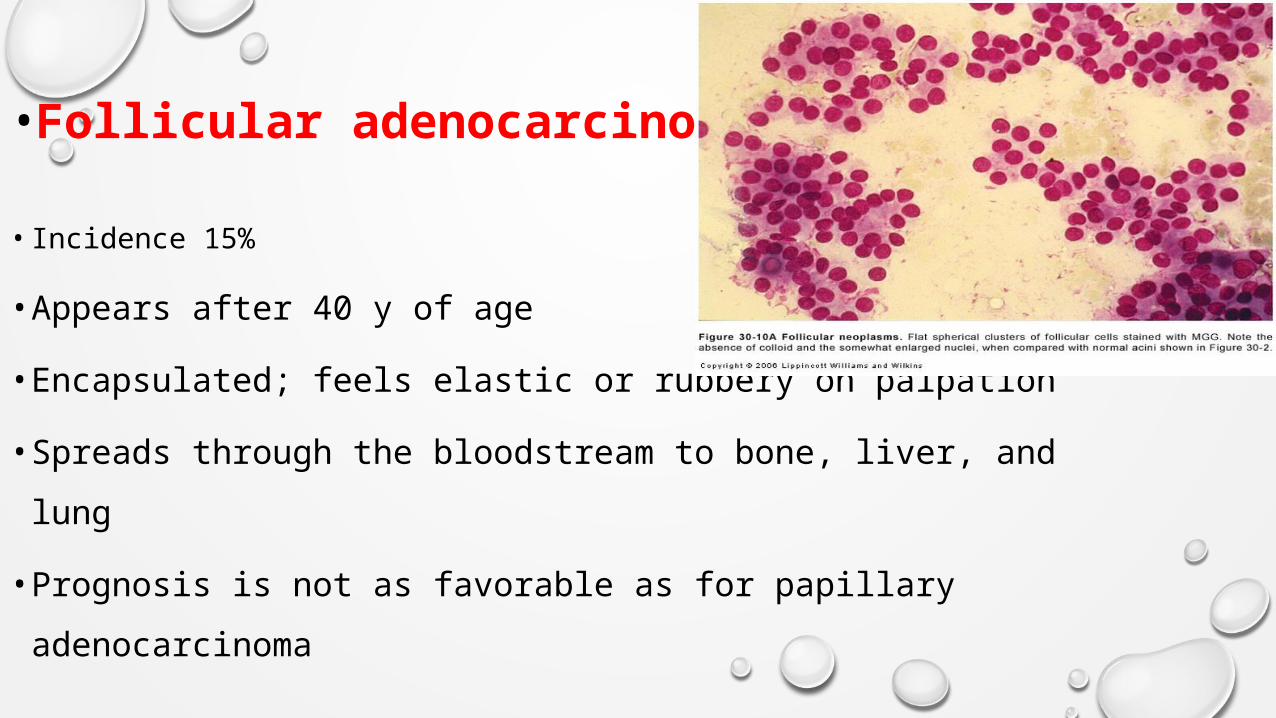
•Follicular adenocarcinoma
• Incidence 15%
• Appears after 40 y of age
• Encapsulated; feels elastic or rubbery on palpation
• Spreads through the bloodstream to bone, liver, and lung
• Prognosis is not as favorable as for papillary
adenocarcinoma

•Medullary• Incidence 5%
Appears after 50 y of age
Occurs as part of multiple endocrine neoplasia (MEN)
Hormone-producing tumor causing endocrine dysfunction
symptoms
Metastasizes by lymphatics and bloodstream
Moderate survival rate

• ANAPLASTIC
• 5%
50% in patients older than 60 y
Hard, irregular mass that grows quickly and
spreads by direct invasion to adjacent tissues
May be painful and tender
Survival for patients with anaplastic cancer
is usually less than 6 months

THYROIDECTOMY

Thyroidectomy• Thyroidectomy, although rare, may be performed for patients
with:
• thyroid cancer
• hyperthyroidism
• pregnant women
• patients who do not want radiation therapy
• patients with large goiters who do not respond to anti-thyroid
drugs.

Thyroidectomy• Types
• The two types of thyroidectomy include:
1.Total thyroidectomy:
2.Subtotal thyroidectomy: up to five-sixths of the
gland is removed

Post-operative Thyroid hormone.
Replacement therapy.
Suppression of TSH release.

NURSING CARE PLANS
• Nursing priorities
1.Reverse/manage hyperthyroid state preoperatively.
2.Prevent complications.
3.Relieve pain.
4.Provide information about surgical procedure, prognosis, and
treatment needs.

NURSING DIAGNOSIS
• acute Pain, May be related to Surgical
interruption/manipulation of tissues/muscles
• Possibly evidenced by guarding behavior; restlessness
•Planning
• Report pain is relieved/controlled

Nursing Interventions
Assess verbal and nonverbal reports of pain Place in semi-Fowler’s position and support head and neck
with sandbags or small pillows. Maintain head and neck in neutral position and support
during position changes. Instruct patient to use hands to support neck during movement and to avoid hyperextension of neck.
Give cool liquids or soft foods, such as ice cream or popsicles. Encourage patient to use relaxation techniques: guided
imagery, soft music, progressive relaxation. Administer analgesics and/or analgesic throat sprays and
lozenges as necessary.

• 2. Ineffective airway clearance
• Nursing diagnosis
• Risk for ineffective airway clearance Risk factors may
include Tracheal obstruction; swelling, bleeding,
laryngeal spasms
•Planning
• Maintain patent airway, with aspiration prevented.

Nursing Interventions
Monitor respiratory rate, depth, and work of breathing.
Auscultate breath sounds
. Assess for dyspnea, and cyanosis. Note quality of voice.
Caution patient to avoid bending neck; support head with pillows
Assist with repositioning, deep breathing exercises, and/or coughing as indicated.
Suction mouth and trachea as indicated, noting color and characteristics of sputum
Investigate reports of difficulty swallowing.
Provide steam inhalation; humidify room air.

• Nursing diagnosis• Knowledge, deficient [learning need] regarding condition, prognosis,
treatment, self-care, and discharge needs, May be related to recall, misinterpretation ,Unfamiliarity with information resources
• Possibly evidenced by development of preventable complications
• Planning.
• Participate in treatment regimen.
• Initiate necessary lifestyle changes.

Nursing Interventions
Review surgical procedure and future expectations. Discuss need for well-balanced, nutritious diet Recommend avoidance of goitrogenic foods, e.G., Excessive
ingestion of seafood, soybeans, turnips. Identify foods high in calcium and vitamin d.
Review importance of rest and relaxation, avoiding stressful
situations and emotional outbursts.

Instruct in incisional care: cleansing, dressing application.
Recommend the use of loose-fitting scarves to cover scar,
avoiding the use of jewelry.
Apply cold cream after sutures have been removed.
Discuss possibility of change in voice.
Identify signs and symptoms requiring medical evaluation.

• Nursing diagnosis
• impaired verbal Communication, May be related to ,
• Vocal cord injury/laryngeal nerve damage ,Tissue edema; pain/discomfort
• Possibly evidenced by
• Impaired articulation, does not/cannot speak
•Planning• Establish method of communication in which needs can be
understood
•Nursing interventions
Assess speech periodically. Encourage voice rest.
Keep communication simple. Ask yes or no questions.
Provide alternative methods of communication as appropriate:
slate board, picture board.
Anticipate needs as possible. Visit patient frequently.
Maintain quiet environment

Thank You
By : Iman Qasem
Kteo
Related Documents











