Thyroid Emergencies And The Acute Take Dr Sutapa Ray. Consultant Endocrinologist. Harrogate And District Foundation Trust.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Thyroid Emergencies And The Acute Take
Dr Sutapa Ray.
Consultant Endocrinologist.
Harrogate And District Foundation Trust.
Lesson Plan : Case based discussions
Acute illness.
Thyroid storm
Drugs – Amiodarone
Pregnancy
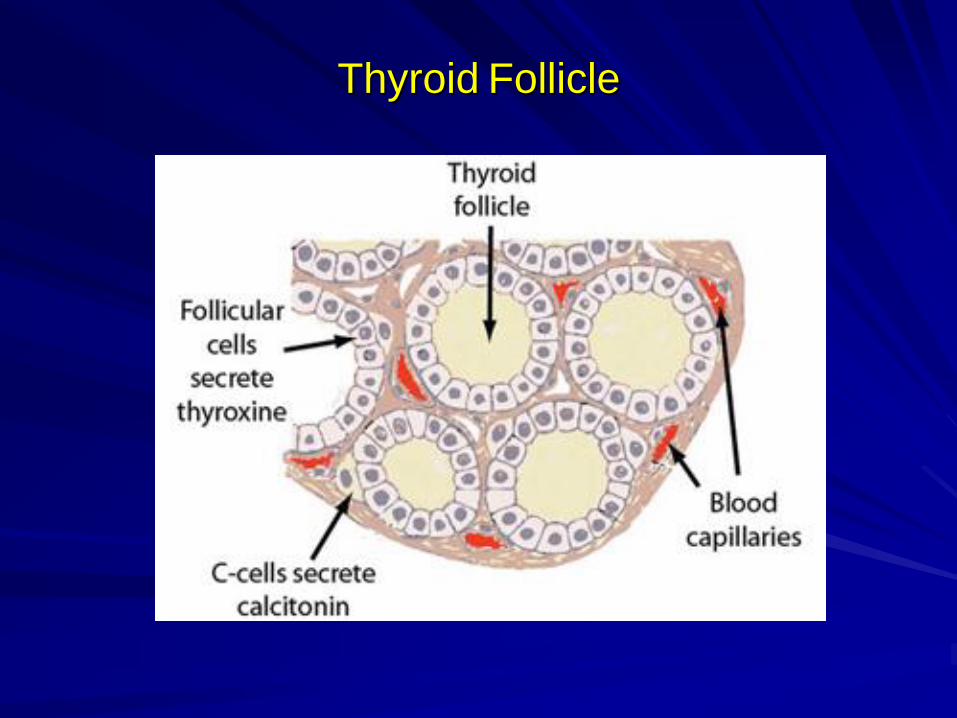
Thyroid Follicle
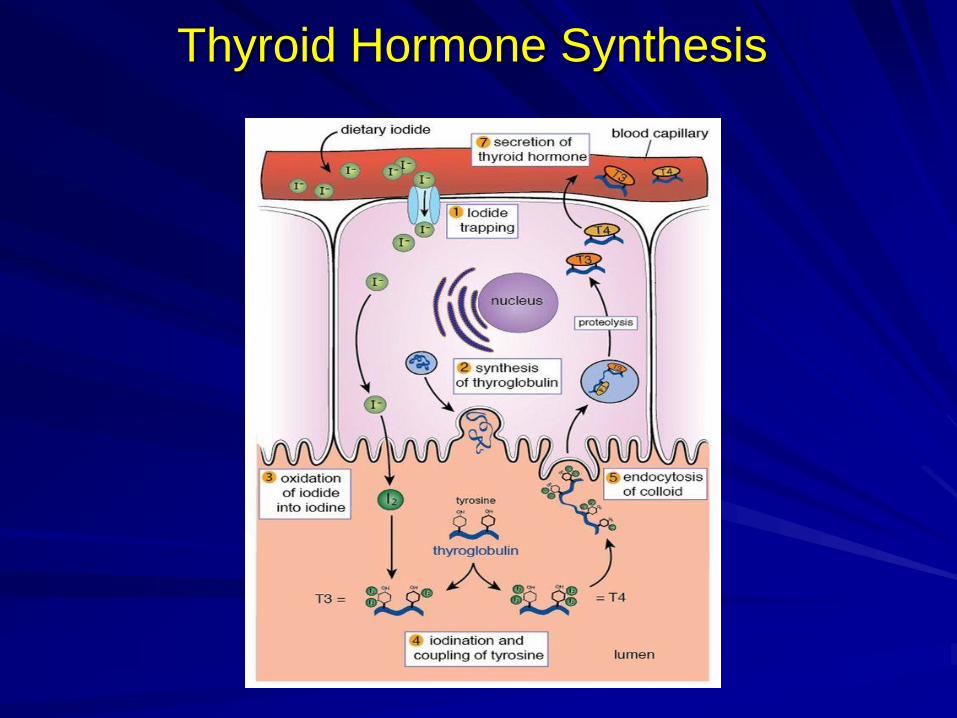
Thyroid Hormone Synthesis
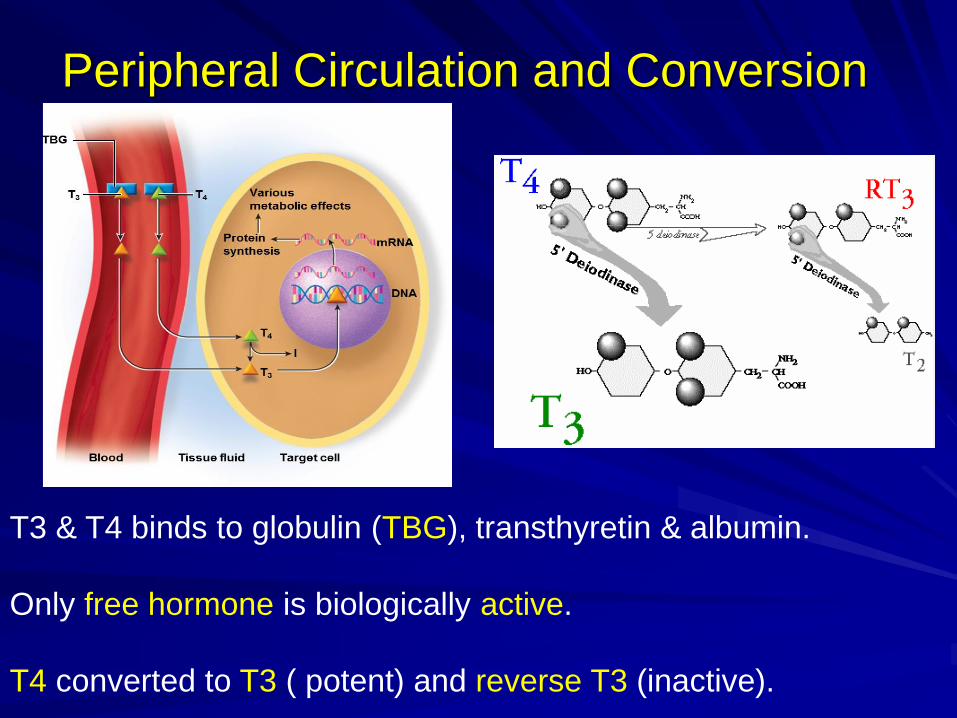
Peripheral Circulation and Conversion
T3 & T4 binds to globulin (TBG), transthyretin & albumin.
Only free hormone is biologically active.
T4 converted to T3 ( potent) and reverse T3 (inactive).
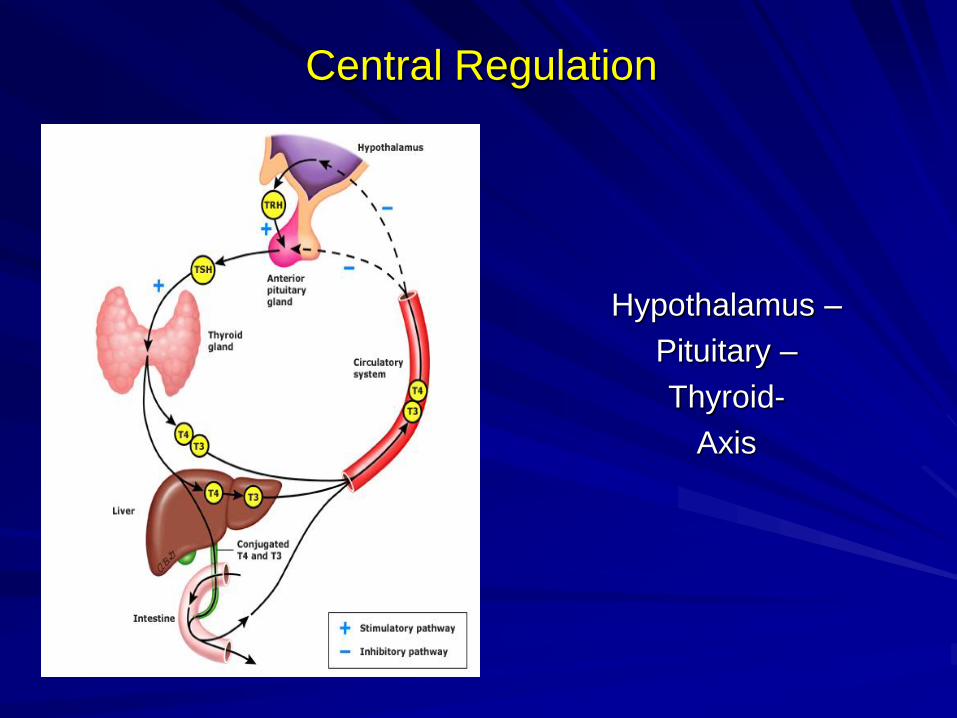
Central Regulation
Hypothalamus –
Pituitary –
Thyroid-
Axis
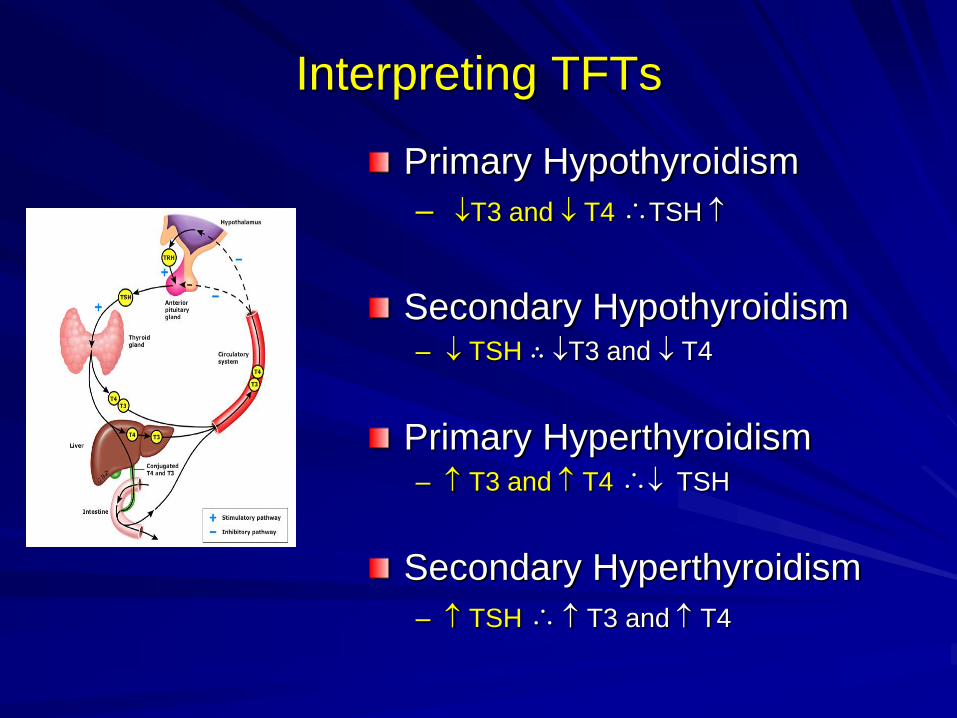
Interpreting TFTs
Primary Hypothyroidism
– T3 and T4 ∴TSH
Secondary Hypothyroidism – TSH ∴ T3 and T4
Primary Hyperthyroidism – T3 and T4 ∴ TSH
Secondary Hyperthyroidism
– TSH ∴ T3 and T4
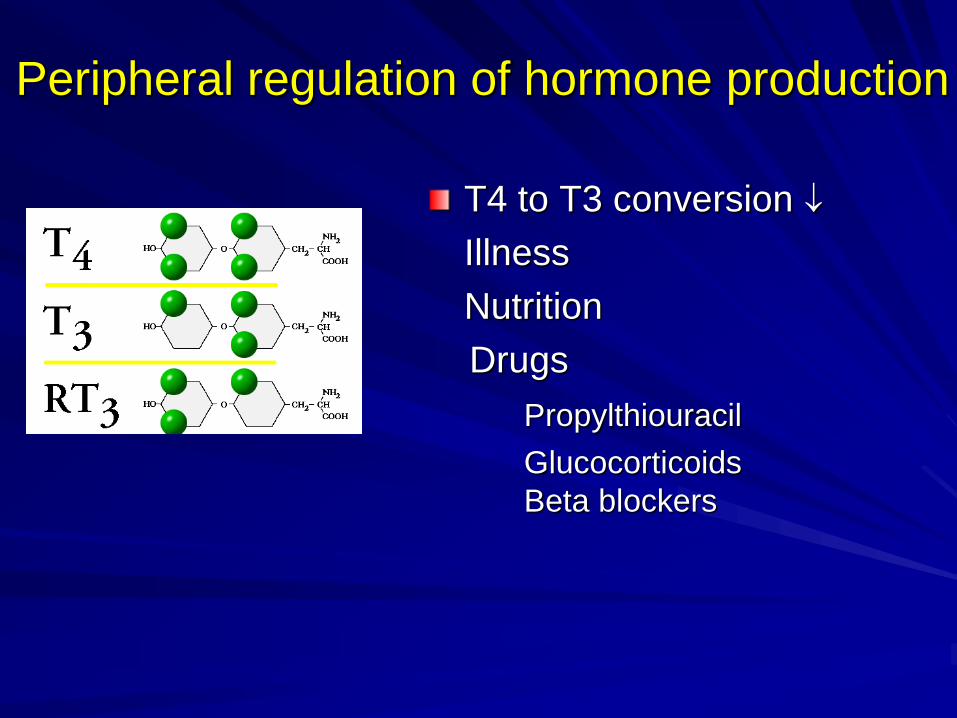
Peripheral regulation of hormone production
T4 to T3 conversion
Illness
Nutrition
Drugs
Propylthiouracil
Glucocorticoids
Beta blockers
David
72 yr male.
– Smoker, COPD, IHD.
– Admitted with pneumonia and dehydration
– Noted tachycardia
– TSH < 0.05 miu/ l ( 0.05 – 4.5 miu/l)
David : Management ?
TSH :- < 0.05 mIu/l (0.05- 4.5 mIu/l) Supressed
T3 :- 1.6 pmol/l ( 2.3 – 5.6 pmol/l) Low
T4 :- 12.2 pmol/l (10- 20 pmol/l) Low normal
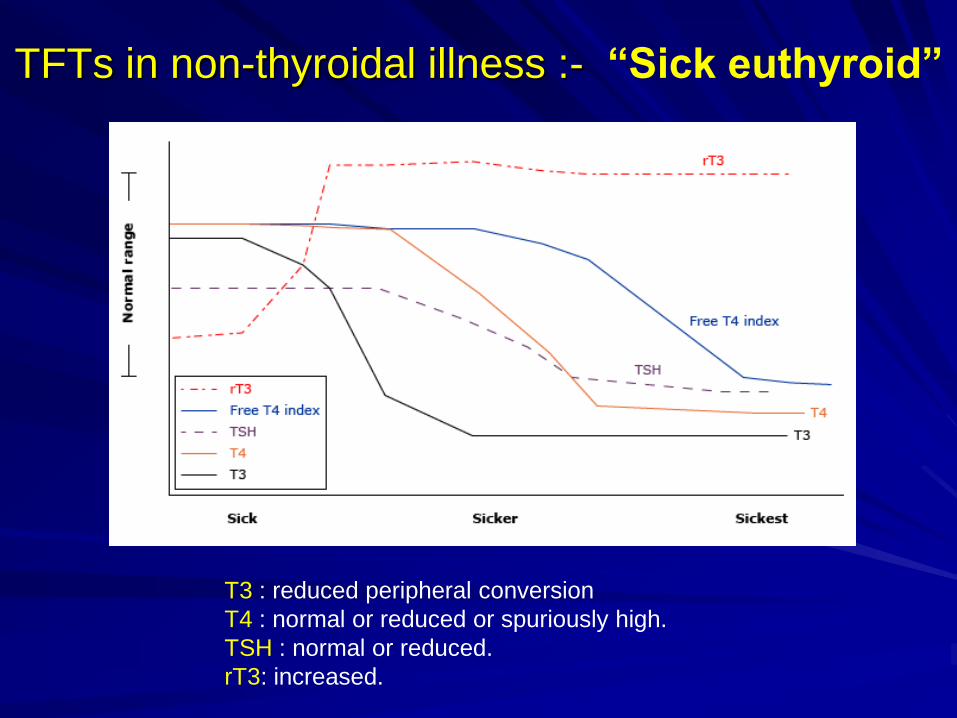
TFTs in non-thyroidal illness :- “Sick euthyroid”
T3 : reduced peripheral conversion
T4 : normal or reduced or spuriously high.
TSH : normal or reduced.
rT3: increased.
TFTs in acute illness
DO NOT check unless strong suspicion. Pyrexia , tachycardia, altered mental ( not responding to therapy)
AND
History of thyroid disease / Recent exposure to iodine contrast medium.
– ( Exception acute tachy-arrhythmias.)
TSH alone inadequate.
? Protective to reduce catabolism.
Supplements of no benefit.
45 yr old
– Admitted with UTI and acute confusion
– Temp 40 °C, BP 110/60, AF 160.
– Graves’s. Due clinic next week.
TSH < 0.05 ( 0.01 – 4.5 mIu/ l)
T4 > 70 ( 10- 20) pmol ,
T3 > 35 (2.5-6.5) pmol.
– Carbimazole 20 mgs OD, concordant.
Thyroid
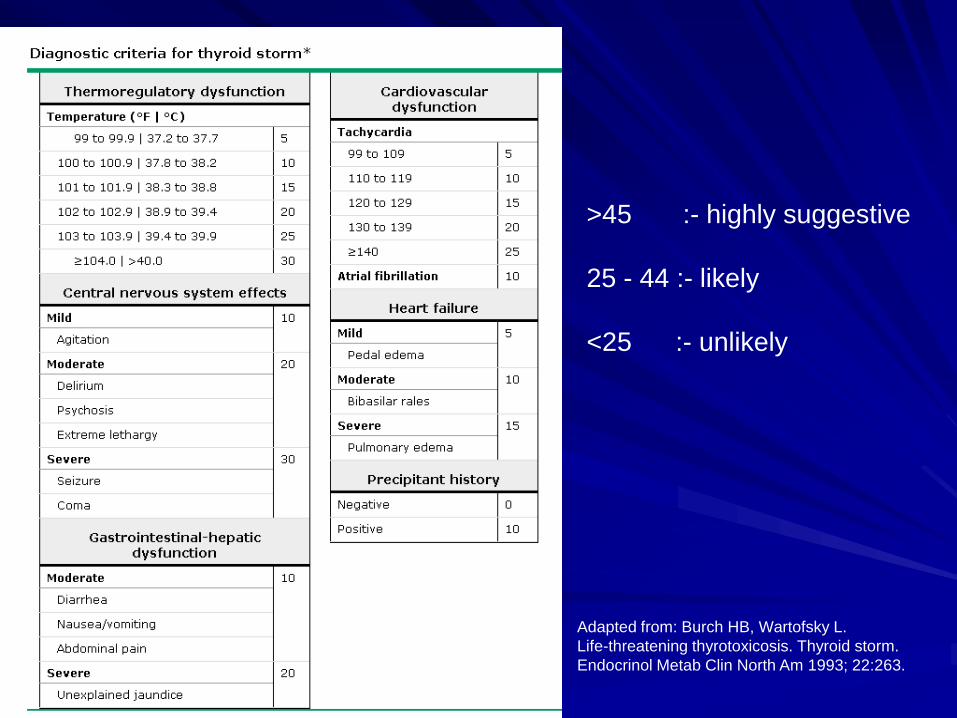
>45 :- highly suggestive
25 - 44 :- likely
<25 :- unlikely
Adapted from: Burch HB, Wartofsky L.
Life-threatening thyrotoxicosis. Thyroid storm.
Endocrinol Metab Clin North Am 1993; 22:263.
Treatment Strategy
Reduce hormone production and release
Lower conversion of T4 to T3
Block peripheral action
Remove circulating hormones
Treat precipitating factors
Symptomatic treatment
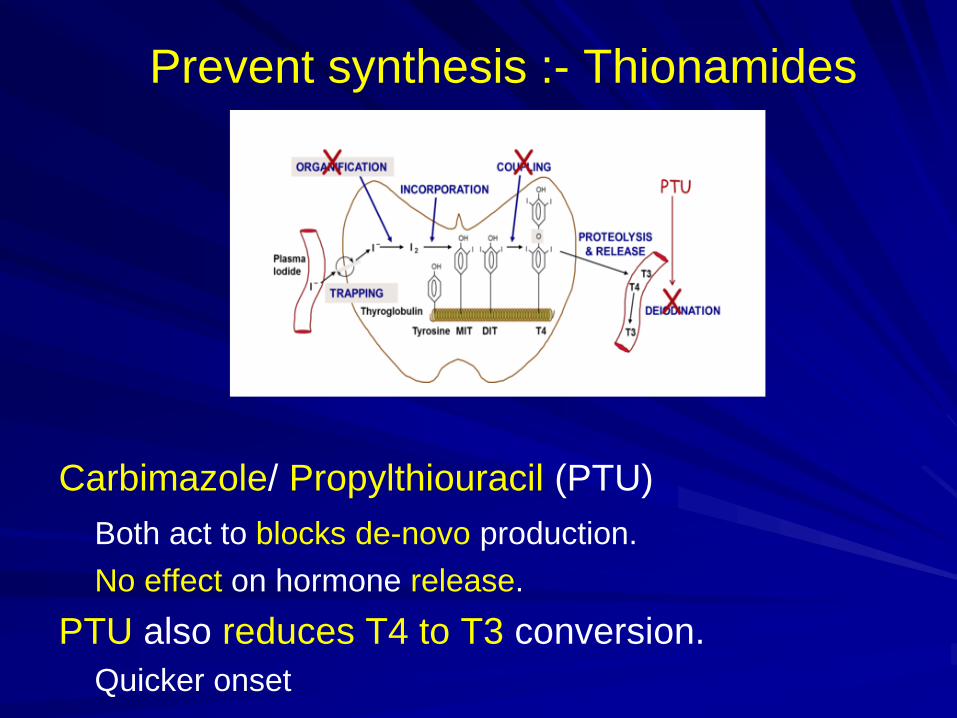
Prevent synthesis :- Thionamides
Carbimazole/ Propylthiouracil (PTU)
Both act to blocks de-novo production.
No effect on hormone release.
PTU also reduces T4 to T3 conversion.
Quicker onset
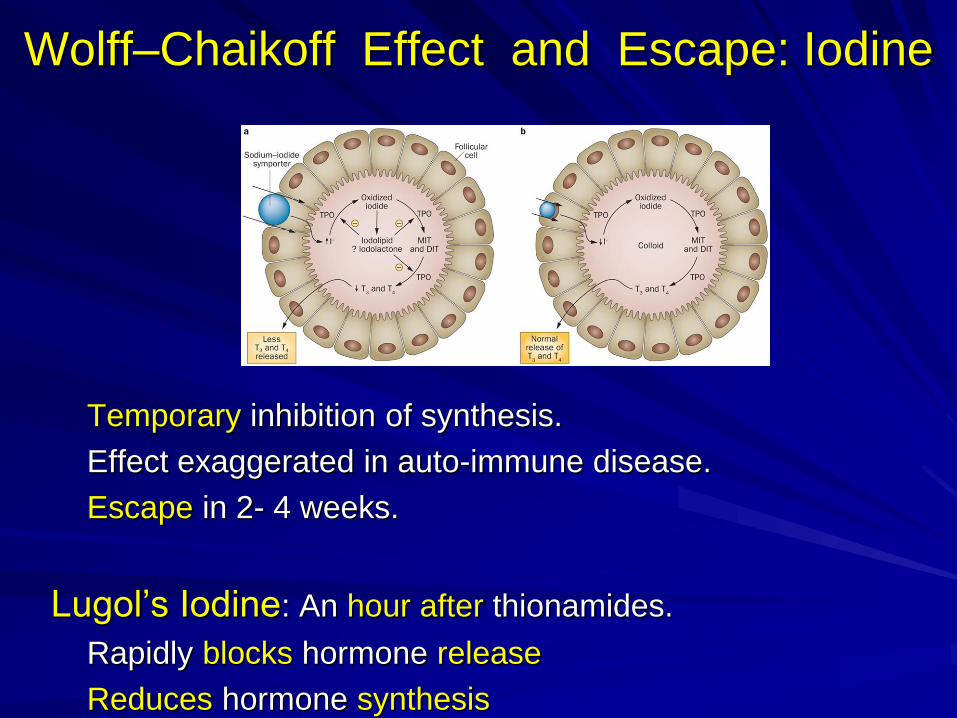
Wolff–Chaikoff Effect and Escape: Iodine
Temporary inhibition of synthesis.
Effect exaggerated in auto-immune disease.
Escape in 2- 4 weeks.
Lugol’s Iodine: An hour after thionamides.
Rapidly blocks hormone release
Reduces hormone synthesis
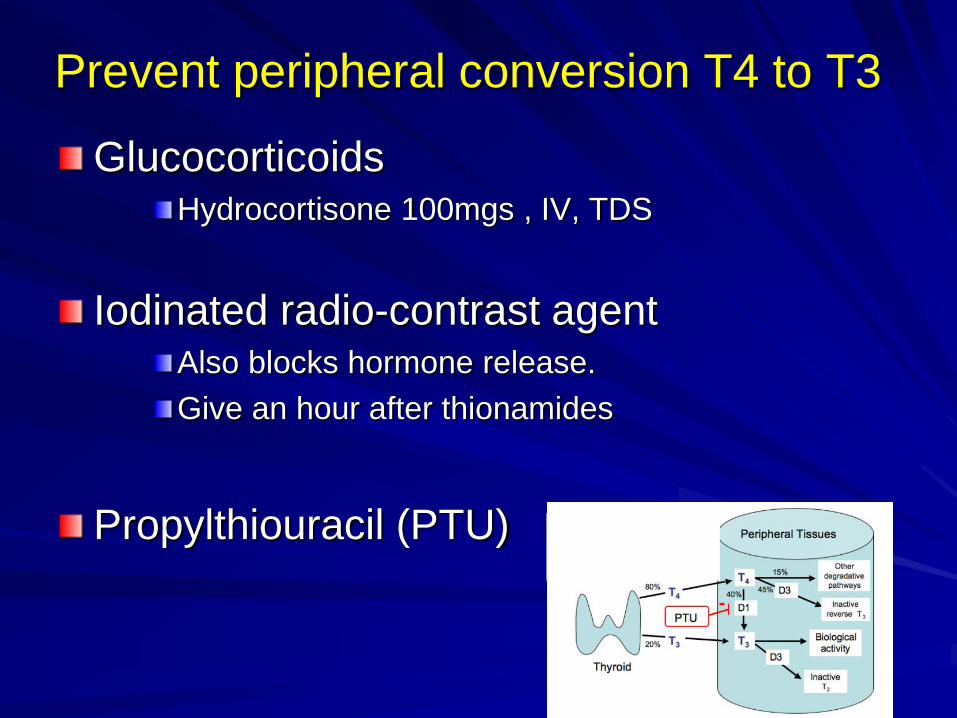
Prevent peripheral conversion T4 to T3
Glucocorticoids Hydrocortisone 100mgs , IV, TDS
Iodinated radio-contrast agent Also blocks hormone release.
Give an hour after thionamides
Propylthiouracil (PTU)
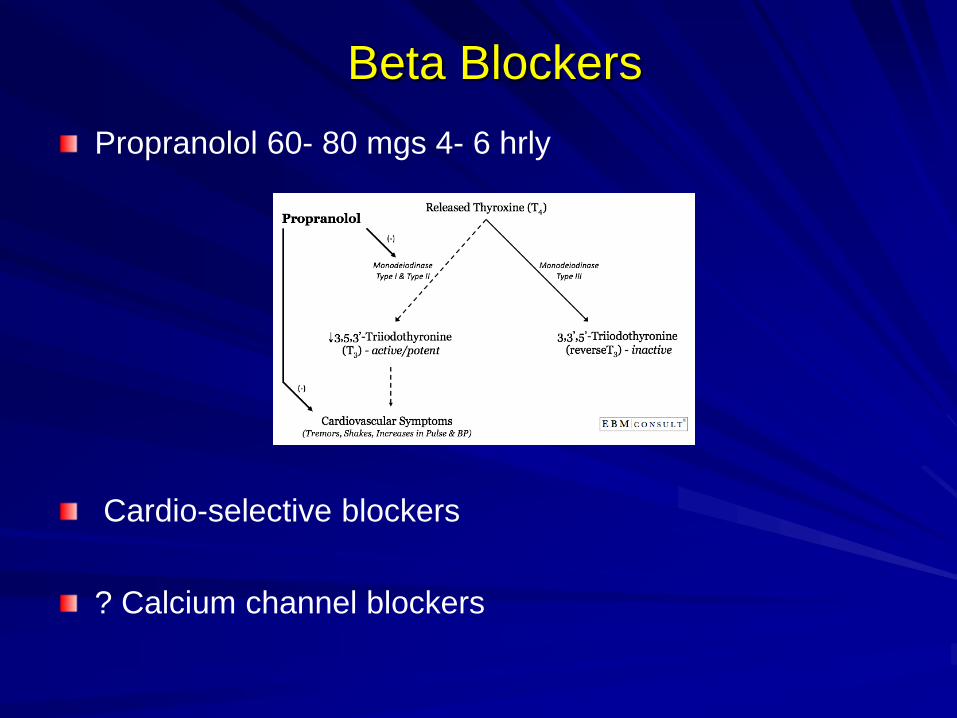
Beta Blockers
Propranolol 60- 80 mgs 4- 6 hrly
Cardio-selective blockers
? Calcium channel blockers
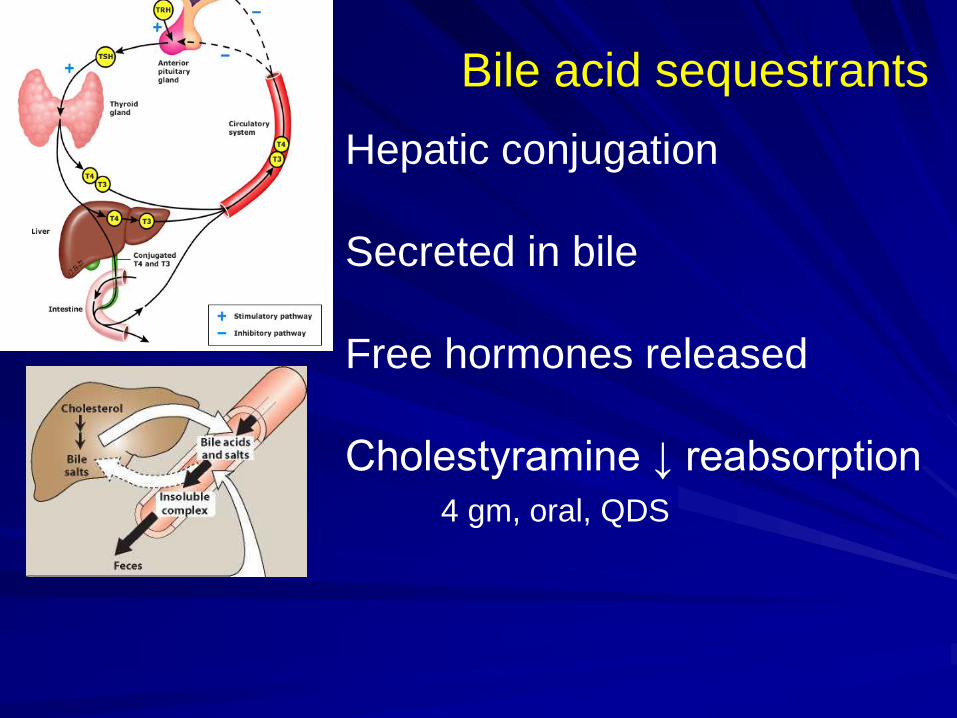
Bile acid sequestrants
Hepatic conjugation
Secreted in bile
Free hormones released
Cholestyramine ↓ reabsorption
4 gm, oral, QDS
Plasmapheresis :- If all else fails!
Removes
– cytokines, antibodies, T3 and T4
Effective within 2 - 3 sessions
Prepare for urgent surgery
Thyroid Storm
Life-threatening. Mainly CVS:- Heart failure, arrhythmia
Mortality 10-30%.
Hormone levels may not be profoundly raised.
Precipitating factors Surgery, trauma, infection, parturition, Iodine load.
Multi-pronged approach
Effect of Amiodarone on Thyroid Hormones
Amiodarone and the Thyroid Gland
Intrinsic effect
↓ T4 to T3 conversion
Blocks T3 receptor binding
Destructive thyroiditis
Effect due to iodine content
Failure of Wolff Chakoff effect
Jod Basedow effect
– ↑ hormone production as
increased substrate (iodine)
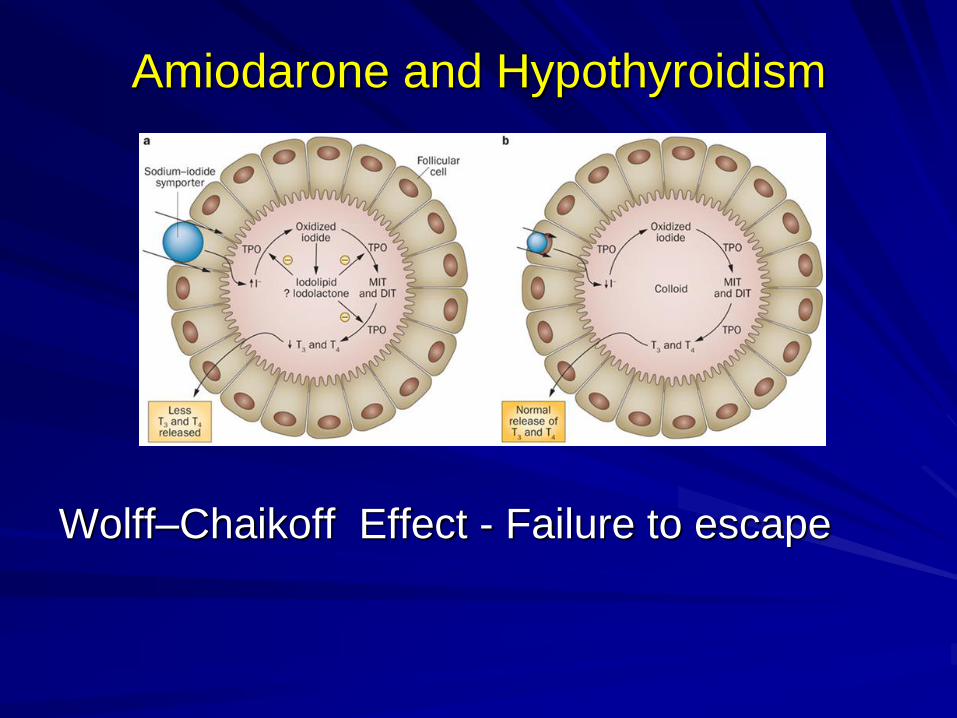
Amiodarone and Hypothyroidism
Wolff–Chaikoff Effect - Failure to escape

Amiodarone induced Hyperthyroidism
Type 1
Pre-existing thyroid disease
Excess iodine as substrate
Increased T4 and T4 synthesis
Thionamides
Type 2
Without known disease.
Direct toxicity
Excess release of T3 & T4
Glucocorticoids

Expected changes with Amiodarone?

Expected changes with Amiodarone
At 0– 3 mths
T4 rises by 20 to 40
T3 decreases by up to 30
TSH may exceed the upper
limit of normal.
Beyond 3 mths.
T4 remains slightly elevated
or in the upper normal range.
T3 concentrations remain in
the low normal range.
TSH normalises

Kiran
Primi, 6/40 gestation.
Vomiting. Dehydration. Recent weight loss.
Admitted to Obstetrics for IV fluids.
TSH < 0.01 miu/l ( 0.01 – 4.5)
T4 22. pmol/l ( 10- 20 )
T3 6.7 pmol/l (2.5 – 6.3)
Diagnosis? Medication ?
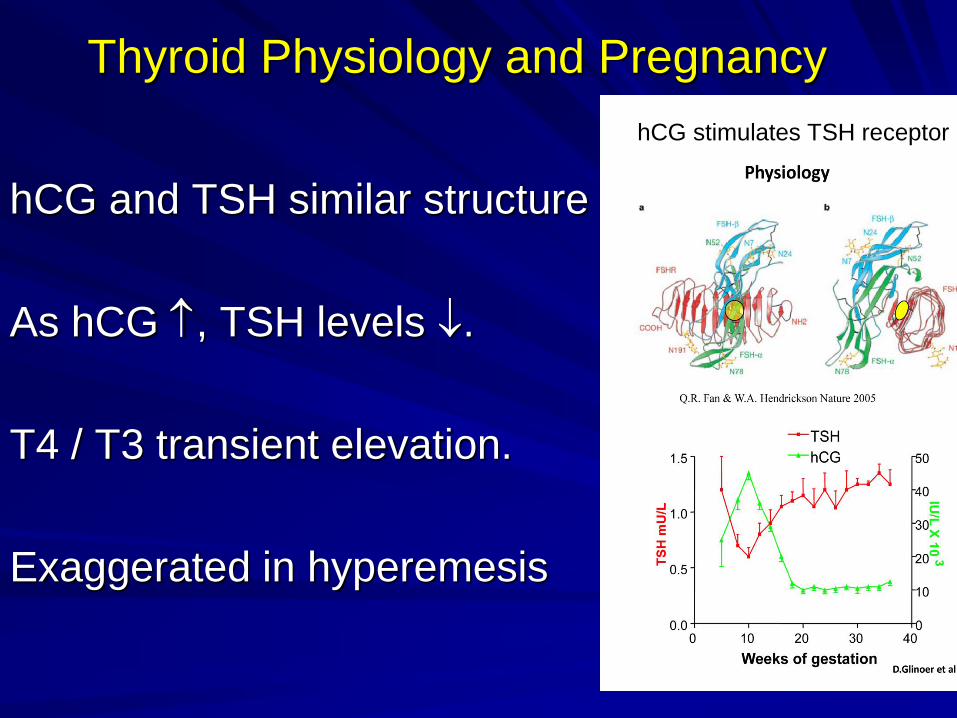
Thyroid Physiology and Pregnancy
hCG and TSH similar structure
As hCG , TSH levels .
T4 / T3 transient elevation.
Exaggerated in hyperemesis
hCG stimulates TSH receptor
Lisa
Para 0, Gravida 2 , 9/ 40 gestation.
Recent UTI
TFTs done earlier TSH 6.5 miu/l ( 0.01 – 4.5)
T4 11.2pmol/l ( 10- 20 )
T3 3.8 pmol/l (2.5 – 6.3)
TPO antibodies elevated.
Diagnosis?
? Intervention – holiday for 3 weeks tomorrow
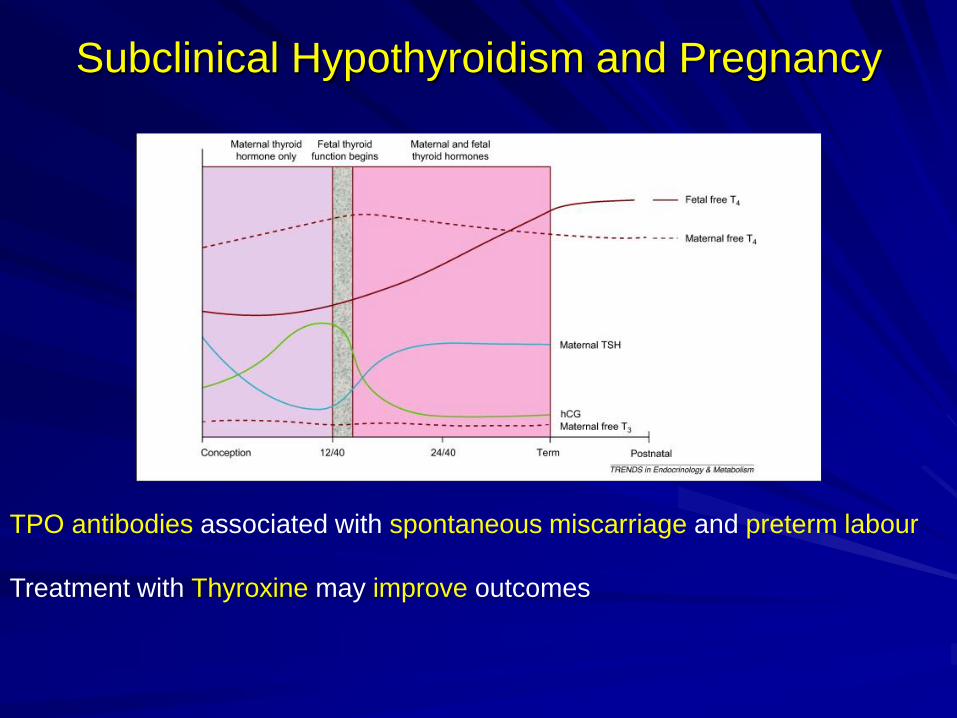
Subclinical Hypothyroidism and Pregnancy
TPO antibodies associated with spontaneous miscarriage and preterm labour
Treatment with Thyroxine may improve outcomes
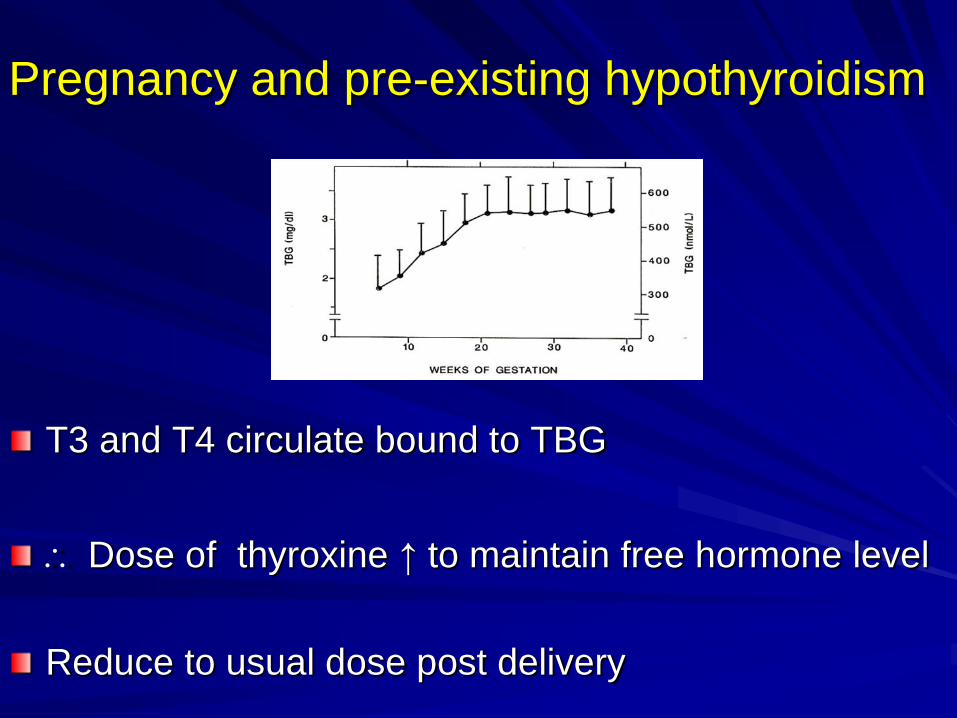
Pregnancy and pre-existing hypothyroidism
T3 and T4 circulate bound to TBG
Dose of thyroxine ↑ to maintain free hormone level
Reduce to usual dose post delivery

Summary
Acute illness.
Thyroid storm
Effect of Amiodarone
Pregnancy.

Related Documents











