THYROID COMPLICATING PREGNANCY

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

THYROID COMPLICATING PREGNANCY
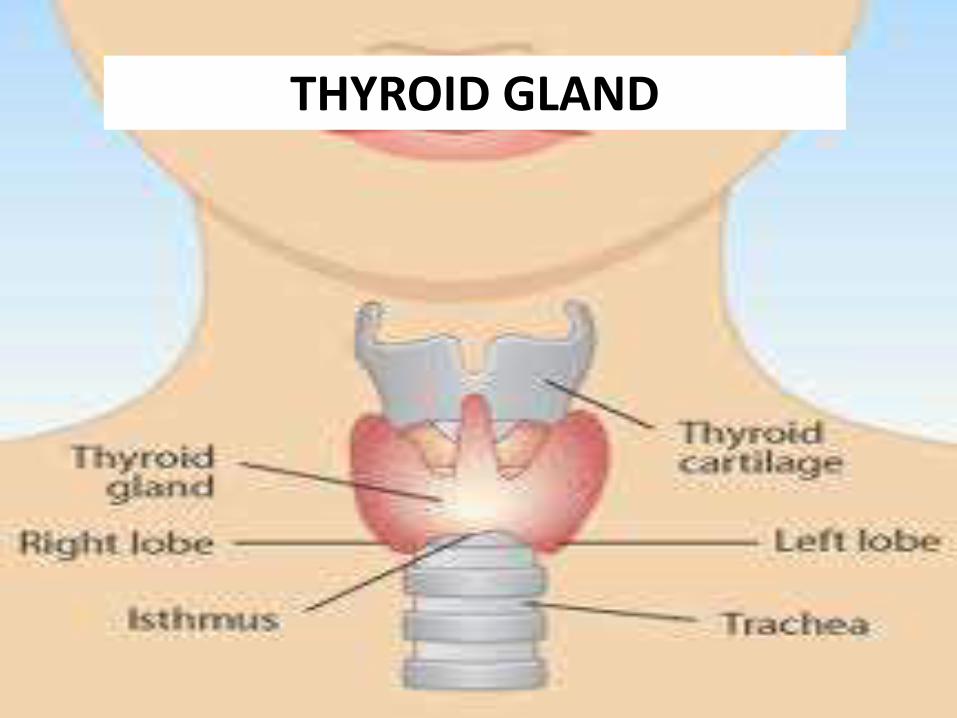
THYROID GLAND
MATERNAL THYROID PHYSIOLOGY
During pregnancy, maternal thyroid function is modulated by three factors
• An increase in HCG concentrations that stimulate the thyroid glands,
• Significant increases in urinary iodide excretion, resulting in a fall in plasma iodine concentrations,
• An increase in thyroxine-binding globulin (TBG) during the first trimester, resulting in increased binding of thyroxine

THYROID IN PREGNANCY
• Thyroid hormone concentrations in blood are increased in pregnancy, partly due to the high levels of oestrogen and due to the weak thyroid stimulating effects of human chorionic gonadotropin(hCG) that acts like TSH.
• Thyroxine (T4) levels rise from about 6–12 weeks, and peak by mid-gestation; reverse changes are seen with TSH

AUTOIMMUNE THYROID DISEASE There are mainly two types of thyroid antibodies: Those that are
directed towards cytoplasmic antigen(thyroid peroxidise(TPOAb) and thyroglobulin (TgAb) antibodies) and those directed to the TSH receptor(TSHRAb).
The thyroid autoimmunity,with normal thyroid function ,has been associated with increased miscarriage rate which may be due to:
Subtle maternal thyroid dysfunction An underlying autoimmune imbalance reflected by the presence of
thyroid antibodies which result in rejection of the fetus. Thyroid antibodies which crosses the placenta and directly affecting
the developing fetal thyroid gland ,increase early loss Increased maternal age of women with thyroid autoimmunity

Definition: It is defined by excessive thyroid hormone production due to an overactive gland.
Incidence: Hyperthyroidism occurs in about 2 per 1000 pregnancies
Types: Based on biochemical test
Subclinical:- suppressed TSH ,normal T4 and T3
Overt:- suppressed TSH and elevated T4 and /or T3
Causes :
• Intrinsic thyroid disease :• Autoimmunehyperthyroidism(Grave’sdisease) due to thyroidstimulating antibody• Nodular thyroid disease –single or multiple –nodule >3cm• Sub – acute thyroiditis –generalised thyroid tenderness• Excessive ,exogenous thyroidhormone• Factitious
• Therapeutic• Gestational thyrotoxicosis:• Hyperemesis gravidarum• Placenta mediated• Hydatidiform mole• Multiple gestation• hydrops• Trophoblastic diseases

Restlessness Fatigue Weakness Weight loss Diarrhoea Heat intolerance Nervousness Tachycardia/palpitations Increased frequency of bowel habits Skin/hair/nail changes Skin is soft and moist
Onycholysis (separation of distal nail from its bed)
Hair becomes soft,fine and may thin
Eye signs
Lid lag
Lid retraction and stare
Specific to grave’s disease:
Grave’s orbitopathy
Chemosis
Proptosis
Dysconjugate gaze
Pretibial myxedema
Thyroid bruit
Clubbing

On examination, patient may exhibit
Tachycardia
Tremor
Goitre
Muscle weakness
Lid retraction or lag
TSH decreased and T4 elevates
Patients with grave’s disease may have antibodies to thyroid peroxidise or TSH receptor.

Clinical diagnosis of hyperthyroidism is always be confirmed by measuring free T4
and T4 levels along with TSH
Suggestive complaints include nervousness, heat intolerance, palpitations, thyromegaly or goitre, failure to gain weight or loss weight, exophthalmos.
Women with gestational thyrotoxicosis are rarely symptomatic,have minimal thyroid enlargement and are TSHRAb negative

Antithyroglobulin antimicrosomal antibodies and thyroid stimulating immunoglobulin should be measured
Radioactive iodine uptake and scans should not be done during pregnancy as it cross the placenta and damage the fetal thyroid gland permanently

The goal of management of thyrotoxicosis is primarily to normalize ,but not to suppress thyroid hormone levels and to secondarily treat bothersome adrenergic symptoms of hyperthyroidism
Treatment of hyperthyroidism in pregnancy focuses on stopping release of T4 and inhibiting conversion of T4 to T3

Treatment options for nonpregnant women include treatment for 12 – 24 months with antithyroid drugs, radioactive iodine to partially ablate the thyroid gland and near total thyroidectomy.
Use of antithyroid drugs (carbimazole, methimazole, propylthiouracil)

Thyroid function should be assessed every 4-6 weeks.
Subtotal thyroidectomy is an option for patients who are noncompliant or refractory to medications.Surgery is best undertaken in the second trimester.Radioiodine treatment is contraindicated in pregnancy.
Thyrotoxicosis or thyroid storm is treated with large dose of PTU,600mg loading dose ,followed by 200 – 300mg every 6 hrs should be administered
Pregnancy outcomes
Thio – amide drugs
Radio – ablative therapy

ANTENATAL MANAGEMENT:
The goal of the treatment during pregnancy is to maintain free T4 in the upper normal range with lowest dose of thio amides.
Treatment with beta blockers for the symptomatic relief of severe adrenergic symptoms until freeT4 levels are normalised
Women on thio –amide prior to pregnancy or newly diagnosed toxic nodules or Grave’s disease should be continued or started on thio amide during pregnancy.
The usual starting dose of PTU is 50 – 100 mg 3 times a day and methiomezole 5 – 20 mg twice daily.
Thyroid studies should be repeated every 4 weeks and the dosage should be based on T4 level and not on TSH level . Dosage should be reduced when the T4 level reaches the normal.
FETAL MONITORING:
Foetuses of women taking antithyroid drug during the third trimester or those with a persistent TSHRAbhave an increased risk for developing goiter.
Because of the placental transfer of thyroid stimulating immunoglobulins fetal grave’s disease may develop that results in nonimmune hydrops or fetal demise.
Documentation of fetal heart rate at each visit and USG every 2- 4 weeks in the third trimester
If any fetal abnormlity present routine fetal blood sampling for thyroid indices are recommended
Labor and delivery:
Treatment of symptomatic women with hyperthyroidism in labor include antithyroidmedication , beta – blockers if necessary and supportive care.
If thyrotoxicosis is suspected in laborappropriate management include –elective caesarean delivery may be suitable to avoid dystocia from an extremely large fetal goitre and for the management of fetal airway.
The ex utero intrapartum treatment(EXIT) was developed to to manage airway obstruction with large neck masses.

There may be relapse of Grave’s disease
usually within the first 3 months after
delivery
Antithyroid therapy needs to be
reintroduced.
Perform TSH and free T4 approximately 6
weeks post partum.
Methimazole cause thyroid dysfunction in
breast feeding infants .In low dose (10 – 20
mg/day) does not pose a major risk to
nursing infants.

Miscarriage
Pre-term delivery
Pre-eclampsia
CCF
Placental abruption
Thyroid storm
Infection
IUGR
Prematurity
Stillbirth
Hyperthyroidism
Hypothyroidism
Increased perinatal mortality and morbidity

HYPOTHYROIDISM
• Definition: It is defined as inadequate thyroid production despite pituitary gland stimulation(primary) or insufficient stimulation of the thyroid by the pituitary or hypothalamus. (central hypothyroidism)
• Incidence: 1-3 per 1000 pregnancy
• Types:• Subclinical:- elevated TSH and normal free T4
• Overt:- elevated TSH and low free T4

HYPOTHYROIDISM
Causes:
• Autoimmune distruction of thyroid gland(hashimoto’s thyroiditis) –most common
• Iodine deficiency – leading cause
• Radio ablation of the thyroid for Grave’s disease or thyroid nodule
• Thyroidectomy – partial or near complete for treatment of benign or malignant neoplasm,Grave’disease)
• Medications – Lithium,amioderone

HYPOTHYROIDISM
Signs and symptoms:• vague ,nonspecific signs and symptoms that are
insidious in onset• fatigue • constipation• cold intolerance• weight gain • carpel tunnel syndrome• hair loss• voice changes• reduced memory• muscle cramps• dry skin

Diagnosis during pregnancy is very
difficult
serum TSH is more sensitive than free T4 for
detecting hypothyroidism.If TSH is
abnormal , then elevation of free T4 is
recommended.
The range for serum TSH concentration in
nonpregnant individual is 0.45 – 4.5 mU/L
Strong family history
Known autoimmune disease
Presence of goitre
Previous therapeutic neck irradiation
Those taking medication known to cause
thyroid disturbance
TSH testing for hypothyroidism should
ideally be done prior to pregnancy

Management:
Discussion of
the importance of euthyroidism at the time of
conception
Risk of hypothyroidism to mother and off
spring
Anticipation of medication changes during
pregnancy
Management:
Preconceptional councelling:
The goal of treatment is bringing a euthyroid state at the time of conception
TSH should be considered as an indication of adequate replacement and women should delay pregnancy until TSH is normal
Do not take levothyroxine and multivitamins at the same time since iron and calcium may interfere with absorption of thyroxine
All women should have adequate iodine intake (200microgram/day)

Antenatal management:
By 16 week of gestation women need an
increase in thyroid hormone by 47 %.
This begins as early as 5th week of gestation
and those with previous history of
thyroidectomy
Patients can be told to take a double dose of
their levothyroxine on two days out of seven
A low normal TSH is the goal during
pregnancy (<2.5mU/ml)

Antenatal management:
Newly diagnosed women during pregnancy
should be initiated on 1.0 – 2.0 microgram/kg
/day or 100 microgram of levothyroxine daily
Thyroid stimulating hormone should be
measured in 6 weeks and levothyroxine dose
adjusted in 25 or 50 microgram
When normalized TSh should be checked
every 6 -8 weeks through out pregnancy

Labor and delivery:
Known hypothyroid women should be
euthyroid before delivery
Obstetric complications include increased risk
of still birth , pre term delivery , pre –
eclampsia,and placental abruption,increased
risk of breech and low birth weight

Post partum care:
After delivery levothyroxine therapy should be returned to the prepregnant dose and the TSH should be checked in 6 – 8 weeks
Breastfeeding is not contraindicated in women treated for hypothyroidism. Levothyroxine is excreated into breast milk but levels are too low to alter thyroid function in infants
Annual monitoring of serum TSH is recommended as changing weight and age may modify thyroid function.

POST PARTUM THYROIDITIS
Post partum thyroiditis is caused by a rebound in thyroid autoimmunity after delivery leading to lymphatic infiltration of the thyroid gland and transient changes in the thyroid function.

POST PARTUM THYROIDITIS-Clinical phases:
Phase 1:- The autoimmune destruction of the gland first results in release of stored thyroid hormone into the circulation. This hyperthyroid phase generally occurs between 1 and 4 months after delivery and is self limiting to 1 – 2 months. The onset is abrupt ,with symptoms of fatigue and palpitation . A small painless goitre may develop. If these symptoms become severe , it require treatment with Beta – blockers until resolution of hyperthyroid phase. Antithyroidmedications are not beneficial.

POST PARTUM THYROIDITIS-Clinical phases: Phase 2:
The loss of functioning thyrocytes from the immune destruction results in hypothyroid phase between 3 and 8 months postpartum. The hypothyroid phase usually last longer than hyperthyroid phase ( 4 – 6 months). This disorder is often unrecognised because women usually present with nonspecific symptoms including fatigue , weight gain , loss of concentration and depression. The hypothyroid phase should be treated in women who are symptomatic and in those planning a pregnancy near in future. It is usually recommended to treat women for approximately for 6 months and withdraw thyroid hormone , unless pregnancy is being attempted. A TSH should be rechecked in 5 – 6 weeks after withdrawal of thyroid hormone.

Nursing care:
Education of the pregnant women is necessary
to plan treatment.
Discuss with the women and her family members
about the outcome.
Assist the client to cope with the discomfort and
frustrations due to symptoms.
Nutritional councelling with a registered dietician
will help in selecting a well balanced diet.
Related Documents











