Thymus Transplantation for Infants with complete Di George Syndrome Graham Davies – Consultant Immunologist Evey Howley Immunology CNS – Thymus Transplant

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Thymus Transplantation for Infants with complete Di George
Syndrome
Graham Davies – Consultant Immunologist
Evey Howley Immunology CNS – Thymus Transplant

What is complete Di George syndrome and other associated Immuno-deficient conditions
Why is a Thymus important for effective immunity?
Thymus Transplant pathway at GOSH
Outcome and Mortality post Transplant
Meet our families
Future for Thymus Transplant
Summary

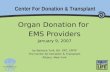
Stem cells
Pre T cells
“educated” in
thymus emerge
into blood as
naïve T cells
B
Blood
Bone marrow
T
NK
Thymus Stem cells in the
bone marrow make
all the cells in the
blood
Pre T

Di George Syndrome is a genetic primary immune deficiency (approx 1 in 4000). In most cases Di George Syndrome results from chromosomal 22q.11 deletion
Heart defects Endocrine problems such as hypocalcaemia,
hypoparathyroidism and hypothyroidism Low set and smaller ears Slanted small eyes, hooded eyelids Small jaw, mouth Small head Cleft lip/palate Absent or non- functioning thymus gland = Complete Di
George syndrome
What is Di George syndrome?

Charge Syndrome =
C – Coloboma of the eye which causes visual impairment- a hole in one of the structures of the eye
H – Heart defects of differing severities
A – Atresia of the choanae – narrowing or blocking of the passage that go from the nose to the throat
R - Poor growth or development
G – Genital and/or urinary abnormalities
E – Ear abnormalities causing hearing impairment
PAX-1 genetic mutation
Thymic aplasia resulting in Hypoparathyroidism, Omenn's syndrome, SCID
Fetal toxin exposure – Poorly controlled Diabetes in 1st Trimester
Other conditions associated with Di George phenotype

Rare inherited disease caused by autosomal recessive loss-of-function mutations in FOXN1 gene
A mutation in this gene has been associated with T-cell immunodeficiency, resulting from Athymia Congenital alopecia universalis
Nail dystrophy
This gene encodes a transcription factor essential for the development of the thymus
What is FOXN-1?

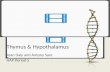
Courtesy of Louise Markert - unpublished
0
200
400
600
800
1000
1200
1400
CD3
CD4
naïve CD4
Survival of 31 untreated patients w ith Complete
DiGeorge
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.5 1 1.5 2
Years

Why is a thymus gland important?

A T-cell or T-lymphocyte is a type of WBC
Essential for the immune system function
Scans for abnormal cells/infections
Recognise what is self and what is foreign
Two types:
CytotoxicT cells (CD8 +) scan and destroy
Helper T cells (CD4 +) cells activate an immune response
What is the Function of a T cell ?

Louise Markert Clin Immunol. 2010 135:236
Thymus Transplantation

Thymus Transplant at GOSH
Inclusion
Complete athymia
Features of DGS including at least one of:
22q.11 deletion
Hypoparathyroidism
Heart defect
CHARGE
Exclusion
Previous HSCT - update
Heart surgery planned within 3 months
Ventilator dependent
Severe muscle wasting
HIV infection
CMV infection - update
First transplant at GOSH took place May 2009.

Infants are referred to GOSH, athymia confirmed
Identify Thymus, via screening Cardiac surgery lists
Donors are matched by blood group (ABO) only - no tissue matching at this time
Initial screened by age (<1year) and pre-existing diagnosis – 22q.11 deletion, Trisomy 21, Immunodeficiency
Consent for Thymus donation and viral screening of baby and mother
A 2nd Thymus is often collected within days in case of failed screening 1st
Thymus Transplant at GOSH

Selecting Donor thymuses
Age <12 months
ABO compatible
Not MHC matched
No chromosomal defect (trisomy, 22q etc)
No known infection
No previous cardiac surgery
109 thymuses cultured for 37 Tx

Thymus in the Laboratory

2
2
2
1
2 1
4
2
2
1
1
1
10
1
1
1 1
Wider Multidisciplinary Team!

Ciclosporin A
ATG 2mg/kg x3 doses D -3 -2 -1
Methylprednisolone
Prednisolone
Immunoglobulin continue
+/- anti-biotics
+/- anti-fungals
+/- anti-virals
Pre Conditioning & Prophylaxis options

Around a 3inch incision is
made into both thighs, down to
the muscle
Approx. 15 slices per thigh
The surgeon creates a small hole for each slice within the
infants muscle
The thigh muscle creates an effective replica home environment
Procedure

Wound care post transplant - observe PEWS, fluid balances (Ca), documentation Pain relief Continue isolation Continue IVIG and other prescribed treatments Regular blood tests - Lymphocyte Sub Sets to monitor T
Cell function, viral loads, thyroid stimulation Respond to symptoms as they occur – CTLs, GVHD Continue support & education with parents Repatriate 3 months Biopsy
Post Transplant

Outcomes …

cDGS Patients transplanted -34 (35Tx)
Median age 8 mo (2-26)
32 Hypoparathyroid
16 Major cardiac defect
3 Hypothyroid
22 Atypical picture
9/12 CHARGE
CD3 120 -1250
No naïve T cells
Absent/subnormal PHA
1 Mat Engraftment
1TA GVHD
22Q.11 delCHARGE
TBX1 mut
Mat diabetesUnknown
DGS
ATG
Yes, 19No, 11
Withheld,4

Significant infections before TTx – 19 patients
Gastrointestinal Rotavirus 8 Norovirus 3 Sapovirus 2 C. difficile 2
Respiratory RSV 2 Parainfluenza 1 Corona virus 1 Boccavirus 1
Systemic CMV 1 Adenovirus 1 HHV6 1
Local mycobacterial BCG 3 NTM sternal abscess

Outcomes
1 lost graft
Septic shock
Developed B NHL
Re-transplanted after 1 year
8 deaths
7 early
3 patients long term poor reconstitution
1 on long term immunosuppression

Reconstitution

PTH
Chance Parathyroid Transplant ( 1 patient)
Davies et al 2019

Reconstitution of Parathyroid Function in one patient

Complications: Inflammatory Reconstitution syndrome (IRS)
Mycobacteria driven (3pts) 2 BCG, 1 NTM sternal abscess All 3 have low total T cell numbers but good % naïve and good
TRECs
Enteropathy driven by infections (6 pts) Rota/Noro/ Adeno/ C.diff
Skin disease HHV6 ( 1patient)
No identified driver skin +/or gut (3pts) Systemic IRS – fevers, high CRP, capillary leak

Summary Immune reconstitution from 6 months
Thymic emigrants with diverse repertoire, but usually not normal numbers
Possibly better reconstitution with some Class 2 MHC matching
Mortality 9/37 – infection commonest cause
Inflammatory disease Related to preceding infections especially GI tract & BCG
Unknown trigger
Not related to ATG usage or to MHC matching
Need better peri-reconstitution management
Autoimmunity Most commonly thyroid
Possibly lessened by some MHC 2 matching

Families met along the way …

Family Participation
Donor for
research
Donor for
transplant
Thymus Transplant Recipient


2 families, 1 transplant
Recipient – AO
Infection – CMV
Compassionate use
Ethics
Family understanding
Altruism
Isolation and separation
Uncertainty
Donor
New baby
Timing of the approach
Protecting their own priority
Right amount of contact

CMV and Outcome
CK14
CD1a

AO

As you know, after the transplantation my wife and daughter stayed in an isolated room in the
hospital. The isolated rooms in Turkey are not same as the ones in your hospital. My wife could not exit the hospital, while I was not able to see my daughter. My bad mood and workload also avoided me from writing you earlier.
At last, we left the hospital and moved home three months ago. The progress in AO is amazing for
us. AO is very happy, she smiles and makes different sounds all the day. Last week, she learned to throw a kiss. She smiles unless we try to feed her.
We still feed her with nasogastric tube. We cannot feed her from mouth. She does not accept anything other than food with rice flour. She hates the spoon. She pretend coughing or sleeping when we approach her with spoon, even the it is empty. She is completely an actress.
She uses her hands but do not step on the ground properly. Our physical therapy and rehabilitation doctor tells that AO was in bed for a long time, so this is normal and will get better with time. She showed us some exercises, we practice them and try to strengthen her legs and feet.
We are happy and full of hope for the future
AO at home

Meet our Family’s


Meet Our Family’s

Explore HLA matching – Frozen Thymus tissue bank
Explore autoimmune phenomena
Effect of newborn screening for SCID
Newly designed thymus transplant pathway information booklets for families
Deliver European Family day
Explore family experience for both donor and recipient
Future

Acknowledgements
Jeans for Genes Campaign
Mason Medical Research Trust
Austen Worth Matthew Buckland Alexandra Kreins Kimberley Gilmour Melissa Cheung Paul Kelly Irene Obiri-Yeboa Clare Marriot Neil Sebire Dyanne Rampling Joe Curry Stefano Giuliani Winnie Ip Stuart Adams Susanne Kricke Eleanor Watt Giovanna Lucchini Maaike Kusters Susan Ross Anna Furmanski Tessa Crompton Athina Soragia –Gzaki Ben Margetts Adrian Thrasher

Malgorzata Pac, Warsaw Jolanta Bernatoniene, Bristol Kim Neuling, Coventry Ronald Bremner, Birmingham Hans-Christian Erichsen, Oslo Marianne Iversen, Copenhagen Mike Browning, Leicester Tiia Voor,Tartu Mihaela Bataneant, Timisoara Ronan Leahy, Dublin Despina Moshous, Paris Manfred Honig, Florence Junghans,Ulm Tim Niehaus, Gregor Duckers, Krefeld Silvana Martino, Torino Leena Kainulainen, Turku Mervi Taskinen, Helsinki Fulvio Porta, Brescia David Pace, Malta Susanne Matthes, Anita Lawitschka, Vienna Andrew Gennery, Newcastle Olov Ekwall, Stockholm Anna Sediva, Prague Fiona Shackley, Sheffield Kamile Aydan, Ankara Gasper Markelj, Ljubyana Peter Ciznar, Bratislava Stephen Jolles, Cardiff.
CO-MANAGING CLINICIANS
All the parents and families
Related Documents