Headache ISSN 0017-8748 C 2007 the Authors doi: 10.1111/j.1526-4610.2007.00695.x Journal compilation C 2007 American Headache Society Published by Blackwell Publishing Correspondence and Clinical Notes Clinical Notes MRA Captures Vasospasm in Fatal Migrainous Infarction Nina Marshall, MBBS; William A. Maclaurin, FRANZCR; George Koulouris, FRANZCR A 57-year-old woman presented with an escalation of her headaches which ultimately progressed to multi- ple strokes and death. MRI/MRA demonstrated diffuse vasospasm and other causes of stroke were excluded on premortem investigation and postmortem examination. Reversible MRI abnormalities, vasospasm on angiogram and fatal migrainous infarction have been previously reported; however, no previous case with this combination of clinical, imaging, and postmortem findings has been documented. Key words: migraine, stroke, magnetic resonance imaging Abbreviations: MRI magnetic resonance imaging, MRA magnetic resonance angiogram, CT computed tomogra- phy, ECG electrocardiogram, pANCA perinuclear pattern antineutrophil cytoplasmic antibody, cANCA pytoplasmic pattern antineutrophil cytoplasmic antibody, C3 complement 3, C4 comple- ment 4, ANA antinuclear antibodies, ENA extractable nuclear antigen, APTT activated partial thromboplastin time, PET positron emission tomography, SPECT single photon emission com- puted tomography (Headache 2007;47:280-302) CASE REPORT A 57-year-old woman with a history of migraine since childhood presented with severe escalating headaches, non- responsive to her usual medication. There was no history of cerebrovascular or thromboembolic disease, diabetes or mis- carriage. Her migraines were characterized by visual aura, severe headache, nausea, vomiting, and occasional right- sided numbness. In the 2 weeks prior to her admission there had been progression in the frequency of her headaches. These headaches were typical of her migrainous episodes but were remarkable in their severity such that she twice presented to From the Department of Radiology, Alfred Hospital, Prahran, Australia. Address all correspondence to Dr. Nina Marshall, Department of Radiology, Alfred Hospital, Commercial Road, Prahran, Vic. 3181, Australia. Accepted for publication September 5, 2006. the emergency department. On both occasions a brain CT revealed no abnormality and lumbar puncture was negative for hemorrhage and meningitis. She had previously used var- ious medications and it had been several years since a formal neurological review. A concomitant consultation diagnosed chronic daily headache with analgesic rebound headache and underlying episodic migraine. Her medication was rational- ized to overcome the rebound element. Her intermittent use of paracetamol and oral opioids was altered to paracetamol and rapid onset nonsteroidals. After initial improvement the patient represented with recurrent severe migraine. Due to the severity of her symptoms a lignocaine infusion was com- menced for analgesia. Over the next 24 hours there was fur- ther decline with confusion, blurred vision, and ongoing vi- sual aura. The infusion was ceased at this point. Importantly there was no instability in blood pressure or heart rate dur- ing the infusion and regular ECGs were normal. Over the next 5 days there was further gradual clinical deterioration with a persisting delirium, right arm weakness, and finally near total visual loss. 280

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Headache ISSN 0017-8748C© 2007 the Authors doi: 10.1111/j.1526-4610.2007.00695.xJournal compilation C© 2007 American Headache Society Published by Blackwell Publishing
Correspondence and Clinical Notes
Clinical Notes
MRA Captures Vasospasm in Fatal Migrainous Infarction
Nina Marshall, MBBS; William A. Maclaurin, FRANZCR; George Koulouris, FRANZCR
A 57-year-old woman presented with an escalation of her headaches which ultimately progressed to multi-ple strokes and death. MRI/MRA demonstrated diffuse vasospasm and other causes of stroke were excluded onpremortem investigation and postmortem examination. Reversible MRI abnormalities, vasospasm on angiogramand fatal migrainous infarction have been previously reported; however, no previous case with this combination ofclinical, imaging, and postmortem findings has been documented.
Key words: migraine, stroke, magnetic resonance imaging
Abbreviations: MRI magnetic resonance imaging, MRA magnetic resonance angiogram, CT computed tomogra-phy, ECG electrocardiogram, pANCA perinuclear pattern antineutrophil cytoplasmic antibody,cANCA pytoplasmic pattern antineutrophil cytoplasmic antibody, C3 complement 3, C4 comple-ment 4, ANA antinuclear antibodies, ENA extractable nuclear antigen, APTT activated partialthromboplastin time, PET positron emission tomography, SPECT single photon emission com-puted tomography
(Headache 2007;47:280-302)
CASE REPORTA 57-year-old woman with a history of migraine since
childhood presented with severe escalating headaches, non-responsive to her usual medication. There was no history ofcerebrovascular or thromboembolic disease, diabetes or mis-carriage. Her migraines were characterized by visual aura,severe headache, nausea, vomiting, and occasional right-sided numbness.
In the 2 weeks prior to her admission there hadbeen progression in the frequency of her headaches. Theseheadaches were typical of her migrainous episodes but wereremarkable in their severity such that she twice presented to
From the Department of Radiology, Alfred Hospital, Prahran,Australia.
Address all correspondence to Dr. Nina Marshall, Departmentof Radiology, Alfred Hospital, Commercial Road, Prahran, Vic.3181, Australia.
Accepted for publication September 5, 2006.
the emergency department. On both occasions a brain CTrevealed no abnormality and lumbar puncture was negativefor hemorrhage and meningitis. She had previously used var-ious medications and it had been several years since a formalneurological review. A concomitant consultation diagnosedchronic daily headache with analgesic rebound headache andunderlying episodic migraine. Her medication was rational-ized to overcome the rebound element. Her intermittent useof paracetamol and oral opioids was altered to paracetamoland rapid onset nonsteroidals. After initial improvement thepatient represented with recurrent severe migraine. Due tothe severity of her symptoms a lignocaine infusion was com-menced for analgesia. Over the next 24 hours there was fur-ther decline with confusion, blurred vision, and ongoing vi-sual aura. The infusion was ceased at this point. Importantlythere was no instability in blood pressure or heart rate dur-ing the infusion and regular ECGs were normal. Over thenext 5 days there was further gradual clinical deteriorationwith a persisting delirium, right arm weakness, and finallynear total visual loss.
280
Headache 281
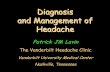
Urgent brain CT and MRI (4 days postcessation of lig-nocaine infusion) imaging revealed several acute infarcts.There were 2 occipital infarcts, 2 insular cortical infracts,and several deep white matter infarcts with a preponder-ance in the posterior vascular territories (Fig. 1). The MRangiogram demonstrated multiple region areas of severe nar-rowing involving the anterior and posterior circulation (Fig.2). A repeat lumbar puncture was normal and there were nolaboratory findings to indicate vasculitis (normal pANCA,cANCA, C3, C4, ANA, ENA, rheumatoid factor).
Despite anticoagulation (APTT maintained at 50-60)and methylprednisolone (1 g intravenous daily for 3 days) thepatient steadily deteriorated to become comatose. Repeatbrain CT at 3 days following the MR imaging demonstratedextension of the parieto-occipital infarcts and the patientdied 2 days later.
Postmortem revealed minor age-related athero-sclerotic change in normal caliber cerebral arteries. Therewere no findings to support a thromboembolic cause forstroke. There were bilateral nonhemodynamically signif-icant carotid stenoses (50% at carotid bifurcation on theright, 40% on the left) and no intracardiac thrombus. Therewas no atherosclerosis of the basilar or vertebral arteries.There was no microscopic evidence of vasculitis. The
Fig 1.—(A and B) MR imaging diffusion-weighted axial sequences demonstrate areas of high signal indicating acute cerebralinfarction involving the left frontal and bilateral occipital lobes, insular cortices, and multifocal deep white matter involvement. (C)MR angiography of the posterior circulation (anteroposterior view) demonstrates alternating areas of stenosis, resulting in a typicalbeaded appearance.
intracranial arteries demonstrated patchy partial ischemicnecrosis within the vascular media. Lesions of this naturehave been previously reported to occur in vasospasm.1 Inthe absence of other causes of stroke, migraine-induced va-sospasm and subsequent cerebral infarction was postulatedas the cause of death.
COMMENTSThis patient suffered an unusual illness commencing
with severe migraine with aura which deteriorated into mul-titerritory cerebral infarction. The initial strokes were oc-cipital (appropriate to the visual aura) and other causes ofstroke were excluded by both pre- and postmortem findings.We believe these strokes thus satisfy the established criteriafor stroke due to migraine.2
Migraine has been implicated as an independent riskfactor in stroke with the incidence of active migraine (bothwith and without aura) in stroke patients reported as highas 3.7%.3 Ischemic cerebral infarctions occurring during mi-graine have been reported most frequently in the middlecerebral artery territory4 though anterior, posterior circu-lation, and bilateral infarcts have also been reported.5,6 Theassociation is better established among women using the oral

282 February 2007
Fig 2.—(A) Anteroposterior and (B) lateral MR angiogram images of the right anterior cerebral circulation reveal the characteristicfindings of vasospasm as evidenced by multiple short-segment stenoses (arrowheads). Small caliber anterior (curved arrow) andmiddle cerebral arteries (solid arrow) are depicted.
contraceptive pill (not applicable in this case).3,4 A 2004 pa-per by Kruit et al reviewed MRI findings in migraine patientswith controls matched for cardiac and cerebrovascular riskfactors. In this study, both patients and controls were asymp-tomatic for stroke. There was no overall difference reportedin the prevalence of either infarction or subclinical whitematter lesions between those with migraine and controls,with the exception of posterior circulation events in migrainewith aura, such as seen in this instance.4
A potential confounder in this case was the concurrentlignocaine infusion which may have cerebral and cardiovas-cular toxicity. Cardiovascular depression due to arrhythmiamay result in watershed infarct and cerebral toxicity cancause seizures and respiratory arrest. These effects have beenreported in larger dose intrathecal administration. Previousreviews monitoring lignocaine infusion at this dose for thispurpose have reported no significant cerebral or cardiovas-cular sequelae.7
Several imaging modalities have documented abnormalcerebral perfusion in migraine. Woods et al documented areversible reduction in cerebral blood flow of 40% during aspontaneous migraine attack on PET scanning.8 Seto et alrecorded a case of significant regional decrease in blood flowon a technicium-99m single photon emission CT (SPECT)after normal MR brain and cerebral angiography studies.9
Reversible T2 signal change in patients with concurrent basi-lar migraine at the time of imaging have been captured onMRI reflecting abnormal cerebral hemodynamics and pos-sibly early changes of ischemia during migraine attacks.10
While the majority of angiographic studies in migrainepatients both during migraine and between attacks havebeen normal,11 angiographically documented arterial nar-rowing during migraine attack is not uncommon.12 Arterialnarrowing is not synonymous with vasospasm and there areseveral potential mimics. Cerebral angiography can of itselfcause transient vasospasm. Arterial narrowing due to dissec-tion can occur and there is an increased incidence of carotiddissection in migraine patients.13 Use of medications likeergotamine may cause vascular spasm and subsequent cere-bral infarction or brain hemorrhage.4 Sanin reported a caseof angiographically proven reversible vasospasm with sub-sequent infarction in a migraineur with similar anterior andposterior territory involvement. That patient had, however,been treated with intravenous dihydroergotamine precedingthe infarction.14
Intraluminal clot has also been demonstrated angio-graphically in migranous infarction in the absence of ei-ther an established embolic source or vasospasm support-ing thrombosis due to hypoperfusion as a mechanism forstroke.5 There are multiple case reports of angiographically

Headache 283
demonstrated arterial narrowing in migraine patients wherepotential mimics have been excluded.1,12 These cases differfrom ours in that they demonstrated transient and com-pletely spontaneously reversible episodes of vasoconstric-tion.
In our case, failure to obtain a follow-up with formalcerebral angiogram or repeat MRA means the durationand pattern of vasospasm (persistent or intermittent) is un-known.
Various mechanisms have been postulated for migraine-associated stroke including altered perfusion pressures andactivation of the clotting and endothelin systems leading to atriad of vasoconstriction, thrombosis, and resultant ischemia.Increased platelet aggregability has been documented in pa-tients with migraine.4 It remains unclear whether the patho-genesis in migraine and thus migrainous infarction is medi-ated primarily by a neurological or a vascular event. Cutrerand Black discussed the 2 main theories in a recent review ofmigraine imaging. The vasogenic theory ascribes migraine tocerebral dysregulation with the aura resulting from vasocon-striction and the subsequent headache to vasodilation. Theneurogenic theory describes migraine as a disorder wherevascular changes occur as a response to neurological dys-function. In this case the abnormally functioning neuronshave a decreased metabolic demand which leads to a reduc-tion in blood flow.15
Certainly there has often been no clear relationship be-tween the distribution of documented vasospasm and neu-rological sequelae. A case series by Solomon et al of 13 mi-graineurs with angiographically demonstrable lesions dur-ing their attacks reported variable correlation between thedocumented areas of spasm and symptoms, thus suggest-ing that vascular spasm may be an epiphenomena in mig-raine.12
The Kruit study documented an increased lesion loadwhich paralleled the frequency of migraine attacks.4 Thisleads to speculation of the possibility of cumulative braininsult and progressive damage. It is not clear why extensivevasospasm occurred at this time in this patient or why theclinical course progressed so rapidly to cause ultimately fatalinfarction. There have been only 2 previously reported casesof fatal migrainous infarction.12,16
While the pathophysiology of migraine and stroke inmigraine remains elusive, this case is noteworthy due tothe lethal outcome and remarkable for the previously un-reported widespread areas of vasospasm as depicted by MRangiography.
Conflict of Interest: None
REFERENCES
1. Cole A, Aube M. Migraine with vasospasm and de-layed intracerebral haemorrhage. Arch Neurol. 1990;47:53-56.
2. Headache Classification Subcommittee of the Interna-tional Headache Society. The international classification ofheadache disorders: 2nd ed. Cephalagia. 2004;24(suppl 1):9-160.
3. Milhaund D, Bogousslavsky J, van Melle G, LiotP. Ischaemic stroke and active migraine. Neurology.2001;57:1805-1811.
4. Kruit MC, van Buchem MA, Hofman PAM, et al. Mi-graine as a risk factor for subclinical brain lesions. JAMA.2004;291:427-434.
5. Demirkaya S, Odabasi Z, Gokcil Z, Ozdag F, KutukcuY, Vural O. Migranous stroke causing bilateral anteriorcerebral artery territory infarction. Headache. 1999;39:513-516.
6. Moen M, Levine SR, Newman DS, Dull-Baird A, BorwnGG, Welch KMA. Bilateral posterior cerebral arterystrokes in a young migraine sufferer. Stroke. 1988;19:525-528.
7. Williams DR, Stark RJ. Intravenous lignocaine (lidocaine)infusion for the treatment of chronic daily headache withsubstantial medication overuse. Cephalalgia. 2003;23:963-971.
8. Woods RP, Iacoboni M, Mazziotta JC. Bilateral spread-ing cerebral hypoperfusion during spontaneous mi-graine headache. New Engl J Med. 1994;331:1689-1692.
9. Seto H, Shimizu M, Futatsuya R, et al. Basilar artery mi-graine: Reversible ischaemia demonstrated by Tc-99m HM-PAO brain spect. Clin Nucl Med. 1994;19:215-218.
10. Maytal J, Libman RB, Lustrin ES. Basilar artery migraineand reversible imaging abnormalities. Am J Neuroradiol.1998;19:1116-1119.
11. Lieberman AN, Jonas S, Hass WK, et al. Bilateral cervi-cal carotid and intracranial vasospasm causing cerebral is-chaemia in a migrainous patient: A case of “diplegic mi-graine.” Headache. 1984;24:245-248.
12. Solomon S, Lipton RB, Harris PY. Arterial stenosis inmigraine: Spasm or arteriopathy? Headache. 1990;30:52-61.
13. Olesen J, Friberg L, Olsen TS, et al. Timing and topographyof cerebral blood flow, aura, and headache during migraineattacks. Ann Neurol. 1990;28:791-798.
14. Sanin LC, Mathew NT. Severe diffuse intracranial va-sospasm as a cause of extensive migrainous cerebral infarc-tion. Cephalalgia. 1993;13:289-292.
15. Cutrer FM, Black DF. Imaging findings of migraine.Headache. 2006;46:1095-1107.
16. Selby G, Fryer JA. Fatal migraine. Clin Exp Neurol.1984;20:85-92.

284 February 2007
Reversible Cerebral Vasoconstriction in Spontaneous Intracranial HypotensionWouter I. Schievink, MD; M. Marcel Maya, MD; William Chow, MD;
Charles Louy, MD
Myelography showed an opening pressure of 0 cm H2O and multiple thoracic meningeal diverticula in a 52-year-old woman suffering from orthostatic headaches of instantaneous onset. MR-angiography showed severe segmentalarterial stenosis of the anterior and posterior circulation, which resolved over a 4-day period following an epiduralblood patch. Spontaneous intracranial hypotension should be considered in the differential diagnosis of reversiblecerebral vasoconstriction.
Key words: headache, intracranial hypotension, vasospasm, subarachnoid hemorrhage
Abbreviations: CSF, cerebrospinal fluid, CT computed tomography, MR magnetic resonance, MRI magnetic res-onance imaging, TCD transcranial Doppler
INTRODUCTIONSpontaneous intracranial hypotension is an important
cause of new daily persistent headaches in young and middle-aged adults.1 The cause of spontaneous intracranial hypoten-sion is a spontaneous spinal cerebrospinal (CSF) leak oftenassociated with a generalized connective-tissue disorder.1
The cranial magnetic resonance imaging (MRI) changesof spontaneous intracranial hypotension have been well-described and include subdural fluid collections, enhance-ment of the pachymeninges, engorgement of venous struc-tures, pituitary hyperemia, and sagging of the brain. Becausespontaneous intracranial hypotension may mimic subarach-noid hemorrhage and other neurovascular disorders, angiog-raphy is frequently performed in this patient population.2
Engorgement of venous structures has been confirmed in pa-tients with spontaneous intracranial hypotension,3-5 but ar-terial abnormalities are rarely reported. We report a unique
From the Maxine Dunitz Neurosurgical Institute, Cedars-SinaiMedical Center, Los Angeles, CA (Dr. Schievink); ImagingMedical Group, Cedars-Sinai Medical Center, Los Angeles, CA(Dr. Maya); Department of Neurology, Cedars-Sinai MedicalCenter, Los Angeles, CA (Dr. Chow); Department of Anes-thesiology, Cedars-Sinai Medical Center, Los Angeles, CA (Dr.Louy).
Address all correspondence to Dr. Wouter I. Schievink, MD,The Maxine Dunitz Neurosurgical Institute, Cedars-Sinai Med-ical Center, 8631 West Third Street, Suite 800E, Los Angeles,CA 90048.
Accepted for publication August 4, 2006.
patient with spontaneous intracranial hypotension who de-veloped severe, but transient, segmental cerebral arterialstenosis.
CASE REPORTThis 52-year-old woman suffered the acute onset of se-
vere posterior head and neck pain during yoga stretchingexercises. The headaches were noted to be exquisitely posi-tional in that they were completely relieved by lying downand occurred within minutes of assuming the upright po-sition. There was associated nausea, vomiting, and ringingin the ears. Neurologic examination and MRI of the brainwith and without gadolinium were normal. The patient wasdiagnosed with migraine headaches and treated with al-bital/acetaminophen/caffeine tablets, but her headaches per-sisted. The patient sought another opinion and was evaluated13 days after the onset of headache.
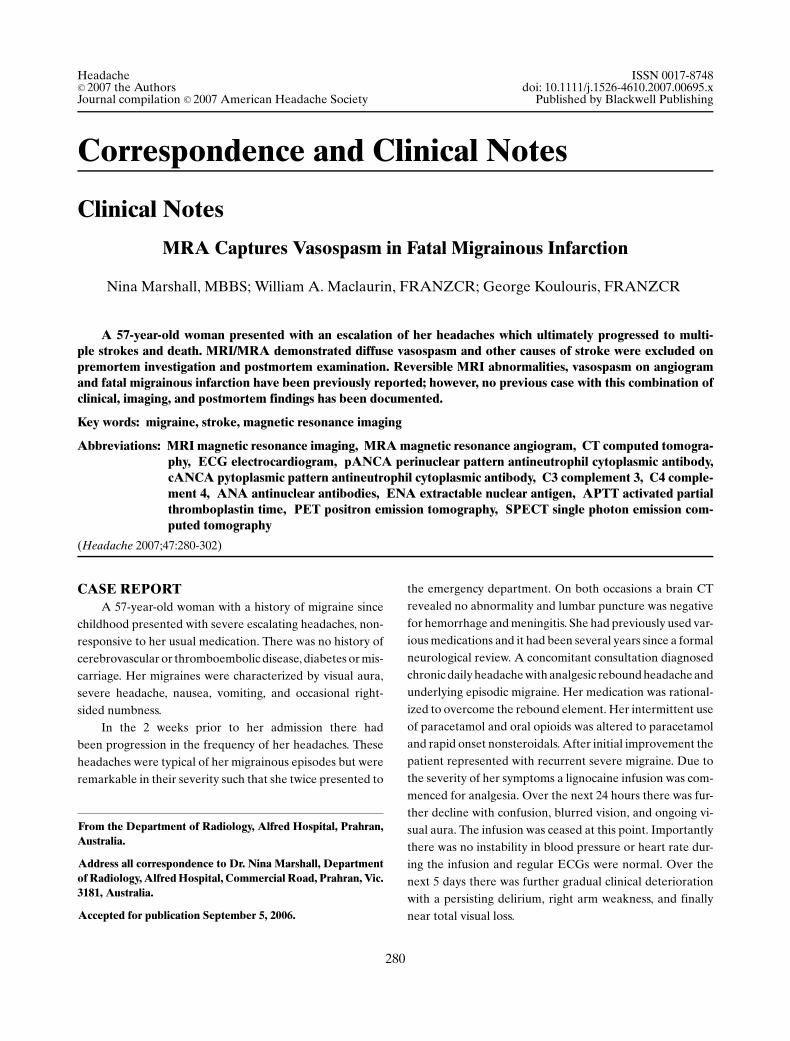
The patient presented in the prone position on the ex-amination table. There was no history of migraine or expo-sure to diet pills, stimulants, or illicit drugs. General medi-cal and neurologic examinations were normal. Blood pres-sure was 122/69 mmHg. The patient was admitted to thehospital for intravenous hydration and further evaluation.Opening pressure at the time of myelography was 0 cm H2Oand only 2 cm3 of CSF could be obtained with aspiration.Examination of CSF was normal. Post-myelography com-puted tomography (CT) scanning showed meningeal diver-ticula arising from the right T8 and left T12 nerve roots (Fig.1). The next day, the patient noted visual blurring and anMRI/MR-angiogram was obtained. MRI was normal but
Headache 285
Fig 1.—Axial CT-myelograms showing meningeal diverticula arising from the right T8 (A) and left T12 (B) nerve roots.
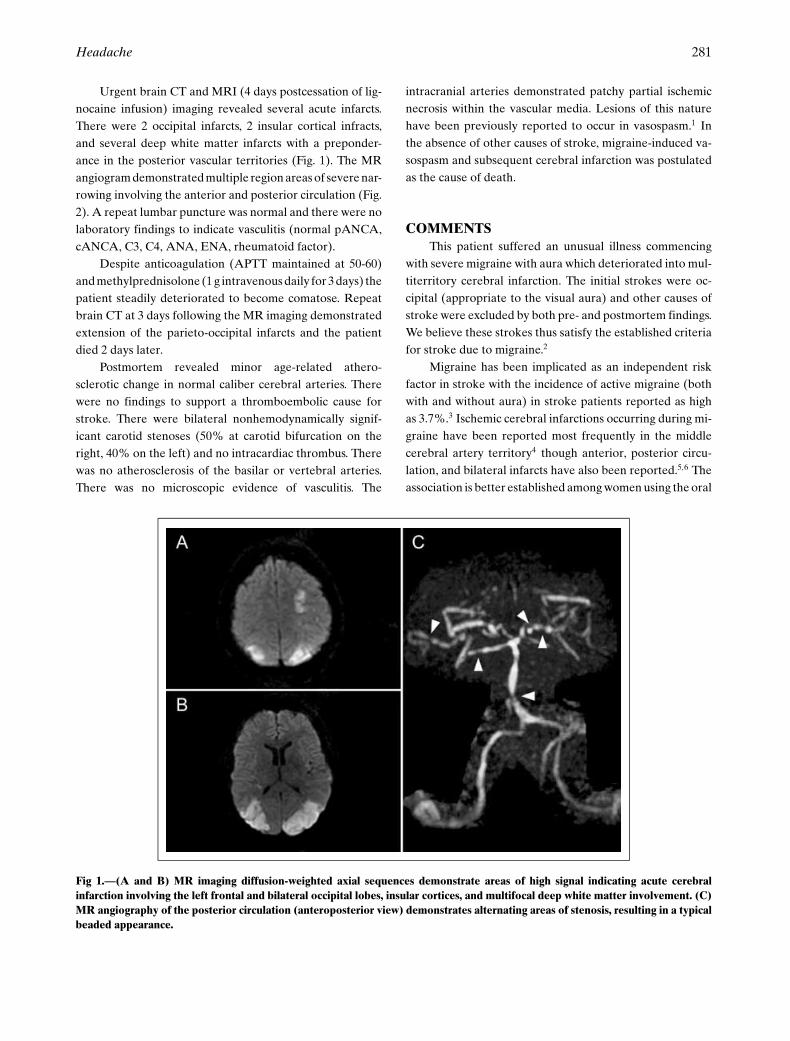
MR-angiography showed severe segmental stenosis of in-tracranial carotid, anterior cerebral, and middle cerebral ar-teries as well as the basilar artery (Fig. 2). Nimodipine wasstarted and the patient was placed in the intensive care unit.Transcranial Doppler (TCD) examination showed markedelevation of blood velocities bilaterally (Table 1). An epidu-ral blood patch was placed at the T12-L1 level and the pa-tient noted immediate improvement of her headaches. CT-angiography confirmed the cerebral arterial stenoses. Serial
Fig 2.—MR-angiograms of the right carotid (A), left carotid (B), and posterior (C) circulations showing severe arterial stenosis andresolution of stenoses 4 days later (D–F).
MR-angiography and TCD evaluations revealed resolutionof the arterial stenosis over the subsequent 4 days (Fig. 2 andTable). Her orthostatic headache recurred gradually and anepidural blood patch was repeated with good, but again onlytransient, relief of her headaches. Percutaneous placementof tissue sealant (Tisseel) was performed at the T7-T8 andT11-T12 levels without any benefit.
Left T11-12 and right T7-T8 partial hemilaminec-tomies were performed. A meningeal diverticulum that was

286 February 2007
Table. Results of Transcranial Doppler Examination
Velocities (cm/s)∗Days after onsetof headache Right MCA Left MCA
14 195 20115 190 14016 160 11617 127 12118 103 5419 111 6820 81 8821 95 9122 91 73
∗Normal values, <100 cm/s.
spontaneously leaking CSF was encountered arising fromthe left T12 nerve root. This was repaired with a 5-mmYasargil aneurysm clip. A meningeal diverticulum also wasencountered arising from the right T8 nerve root. No sponta-neous CSF leak was encountered, but with a Valsalva maneu-ver of 30 mmHg a small amount of CSF could be observedseeping through small rents in the meningeal diverticulum.This was repaired with muscle pledgets secured around thenerve root with 4-0 nylon sutures and reinforced with tissuesealant (Tisseel).
The patient recovered well from surgery with completeresolution of her headaches. No recurrence has been notedduring one year of follow-up.
COMMENTWe describe a unique patient with spontaneous intracra-
nial hypotension who developed severe, but transient, seg-mental stenosis of large and medium-sized cerebral arter-ies. The frequency of reversible cerebral vasoconstriction inspontaneous intracranial hypotension remains to be estab-lished, but among 56 patients with spontaneous intracranialhypotension who underwent intracranial MR-angiographyat our institution, only the presently reported patient showedany arterial abnormalities (unpublished data). The timing ofthese MR-angiograms studies, however, was variable hav-ing been performed between 1 day and 30 years after theonset of symptoms. A total of 23 patients underwent MR-angiography within 2 weeks of the onset of symptoms, 9of whom had presented with a thunderclap headache. Theexact cause of the vasoconstriction in our patient is un-clear. The vasoconstriction remained asymptomatic, was first
noted 14 days after the onset of headache, and had re-solved by day 18. It is unlikely that the vasoconstrictionaccounted for the initial presentation with a thunderclapheadache, because the headache was exquisitely positionalfrom the onset. Chaves and colleagues6 have reported apatient with intracranial hypotension caused by an iatro-genic lumbar CSF leak, who suffered multiple cerebral in-farcts from reversible cerebral vasoconstriction. These au-thors hypothesized that the cerebral vasoconstriction wastriggered by the anatomical displacement of the brain andassociated structures that was caused by the loss of CSFvolume.6 Mechanical stimuli—along with chemical, neuro-genic, and electrical factors—can provoke cerebral arte-rial constriction. Reversible cerebral vasoconstriction alsohas been reported in the postpartum period, which maybe associated with dural puncture and CSF loss.6 It is un-likely that the lumbar puncture precipitated the vasocon-striction in our patient, because the opening pressure wasvery low to begin with and only 2 cm3 of CSF could beaspirated.
In the presently reported patient, it cannot be ex-cluded that the vasoconstriction was related to the myel-ogram, which was performed the day prior to the firstMR-angiogram showing vasoconstriction. Current second-generation, low-osmolar, nonionic myelogram contrastagents, such as the iohexol used in our patient, are notknown to be associated with cerebral vasoconstriction. Inthe past, however, “vasospasm” has been reported follow-ing myelography using Pantopaque.7 The patient with in-tracranial hypotension and reversible cerebral vasoconstric-tion reported by Chaves and colleagues did not undergomyelography6 (see also C. Chaves, personal communication,2005).
In addition to subarachnoid hemorrhage and thepostpartum period, reversible vasoconstriction of largeand medium-sized cerebral arteries may be associatedwith cocaine or methamphetamine use, ingestion of er-gotamine derivatives or sympathomimetics, administra-tion of intravenous immunoglobulins, reversible poste-rior leukoencephalopathy, and possibly, unruptured cere-bral aneurysms.8-10 None of these factors were presentin our patient. Reversible cerebral vasoconstriction asso-ciated with a thunderclap headache frequently is consid-ered “idiopathic.” Spontaneous intracranial hypotension al-ready is included in the differential diagnosis of thunder-clap headache9 and should also be considered in the dif-ferential diagnosis of reversible cerebral vasoconstriction.Recording the opening pressure is important in patients withcerebral vasoconstriction who undergo lumbar puncture.

Headache 287
Conflict of Interest: None
REFERENCES
1. Schievink WI. Spontaneous spinal cerebrospinal fluidleaks and intracranial hypotension. JAMA. 2006;295:2286-2296.
2. Schievink WI, Wijdicks EF, Meyer FB, et al. Spontaneousintracranial hypotension mimicking aneurysmal subarach-noid hemorrhage. Neurosurgery. 2001;48:513-516.
3. Koss SA, Ulmer JL, Hacein-Bey L. Angiographic featuresof spontaneous intracranial hypotension. AJNR Am J Neu-roradiol. 2003;24:704-706.
4. Roll JD, Larson TC 3rd, Soriano MM. Cerebral angio-graphic findings of spontaneous intracranial hypotension.AJNR Am J Neuroradiol. 2003;24:707-708.
5. Baryshnik DB, Farb RI. Changes in the appearance of ve-nous sinuses after treatment of disordered intracranial pres-sure. Neurology. 2004;62:1445-1446.
6. Chaves C, Freidberg SR, Lee G, et al. Cerebral vasospasmfollowing intracranial hypotension caused by cerebrospinalfluid leak from an incidental lumbar durotomy. J Neurosurg.2005;102:152-155.
7. Smith RA, Collier HF, Underwood FO. Cerebral vasospasmfollowing myelography. Surg Neurol. 1973;1:87-90.
8. Call GK, Fleming MC, Sealfon S, et al. Reversible cerebralsegmental vasoconstriction. Stroke. 1988;19:1159-1170.
9. Dodick DW. Thunderclap headache. J Neurol NeurosurgPsychiatry. 2002;72:6-11.
10. Singhal AB. Cerebral vasoconstriction syndromes. TopStroke Rehab. 2004;11:1-6.
Symptomatic Occipital Epilepsy Misdiagnosed as MigraineBindu Menon
Two young patients with symptomatic occipital lobe epilepsy due to discrete lesions of cysticercosis weremisdiagnosed and treated for 2 years as migraine with visual aura. The patients suffered from frequent visual seizuresoften followed by migraine-like headache. Seizures manifested with colored and mainly circular elementary visualhallucinations of up to 1 minute duration. Headache, often severe and of long duration, was frequently associatedwith nausea, photophobia, and phonophobia. Both patients became seizure-free with appropriate treatment of theunderlying disease and epileptic seizures.
Key words: migraine, epilepsy, occipital epilepsy
Episodic elementary visual hallucinations followed byheadache are common and with the same sequence in mi-graine with aura1 and visual occipital lobe seizures.2 How-ever, elementary visual hallucinations of visual seizures aremarkedly different in quality, location, and chronological de-velopment in comparison with the visual aura of migraine.3,4
Elementary visual hallucinations of occipital seizuresare brief for seconds to 3 minutes, develop fast within sec-onds and are predominantly colored and circular.3,4 Theyusually start in the periphery of a hemifield and often marchto other seizure symptoms or convulsions. Conversely, vi-sual aura of migraine consists mainly of achromatic zigzaglinear patterns, starts in the center of the visual field, it grad-ually progresses over >4 min usually lasting <30 min towardthe periphery of one hemifield and often leaves a scotoma.5
From the Department of Neurology, Sri Venkateswara Instituteof Medical Sciences, Tirupati 517507, India.
Address all correspondence to Bindu Menon, Department ofNeurology, Sri Venkateswara Institute of Medical Sciences,Tirupati 517507, India.
Accepted for publication August 1, 2006.
Postictal headache, often indistinguishable for migraine asdefined by the International Classification of Headache Dis-orders (ICHD-2),1 occurs in more than half of patients withvisual seizures.4
Misdiagnosis of visual occipital seizures as migraine ap-pears to be common with significant repercussion on man-agement issues.1,4
We report 2 patients with symptomatic occipitalepilepsy who were misdiagnosed as migraine with aurathough ictal clinical symptoms were typical of visual epilepticseizures despite severe postictal migraine like headache.
CASE REPORTSFirst Case.—A 14-year-old boy started having brief
attacks of elementary visual hallucinations followed byheadache at age of 11 years. These consisted of flashes oflight simulating a yellow bulb being turned on and off in-termittently in his right visual hemifield. They lasted for30 seconds to 1 minute and were strictly unilateral. Theseepisodes were often followed by left-sided headache associ-ated with nausea, vomiting, photophobia, and phonophobia.The headache started immediately after the end of the visual
288 February 2007
seizures, lasted for 1 to 2 hours and was minimally relievedwith analgesics and sleep. The visual seizures with or with-out headache were diurnal and mainly in the morning hourswith no apparent triggering factors.
There was no family history of migraine. His father hada single episode of afebrile convulsions in his childhood.
The diagnosis of migraine with visual aura was madeand he was treated with β-blockers and flunarazine with noimprovement. On the contrary, his attacks became more fre-quent and at the age of 13 years one of his habitual seizuresprogressed to a generalized tonic clonic convulsion.
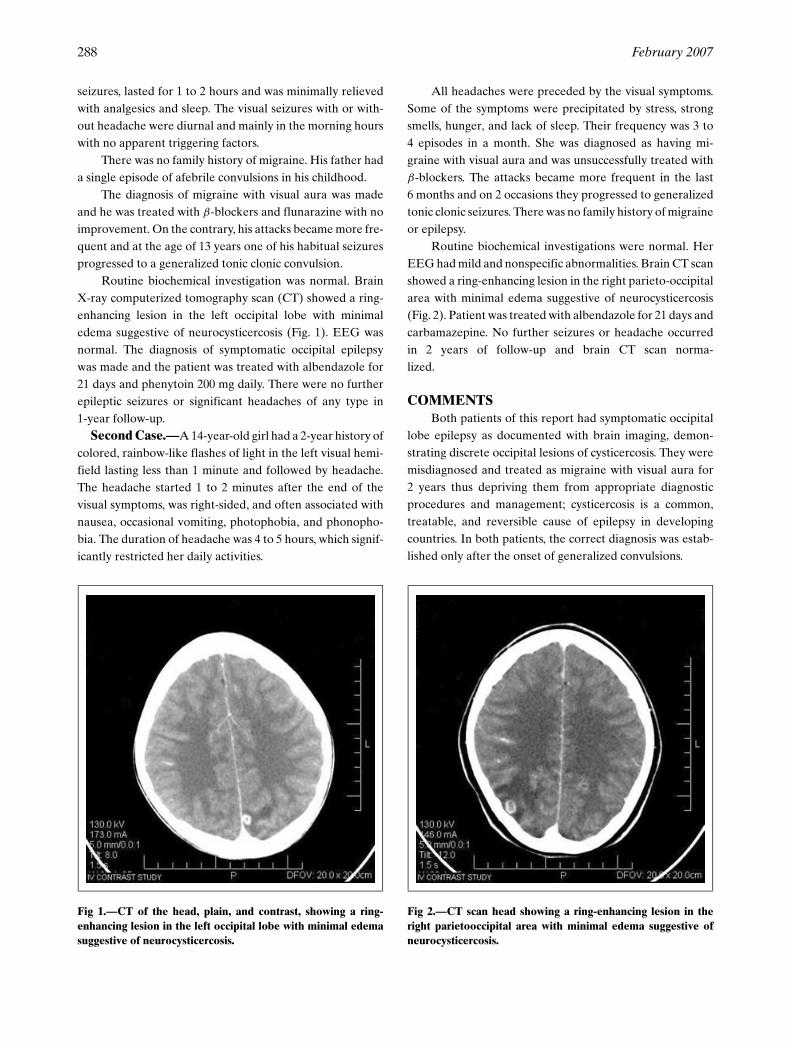
Routine biochemical investigation was normal. BrainX-ray computerized tomography scan (CT) showed a ring-enhancing lesion in the left occipital lobe with minimaledema suggestive of neurocysticercosis (Fig. 1). EEG wasnormal. The diagnosis of symptomatic occipital epilepsywas made and the patient was treated with albendazole for21 days and phenytoin 200 mg daily. There were no furtherepileptic seizures or significant headaches of any type in1-year follow-up.
Second Case.—A 14-year-old girl had a 2-year history ofcolored, rainbow-like flashes of light in the left visual hemi-field lasting less than 1 minute and followed by headache.The headache started 1 to 2 minutes after the end of thevisual symptoms, was right-sided, and often associated withnausea, occasional vomiting, photophobia, and phonopho-bia. The duration of headache was 4 to 5 hours, which signif-icantly restricted her daily activities.
Fig 1.—CT of the head, plain, and contrast, showing a ring-enhancing lesion in the left occipital lobe with minimal edemasuggestive of neurocysticercosis.
All headaches were preceded by the visual symptoms.Some of the symptoms were precipitated by stress, strongsmells, hunger, and lack of sleep. Their frequency was 3 to4 episodes in a month. She was diagnosed as having mi-graine with visual aura and was unsuccessfully treated withβ-blockers. The attacks became more frequent in the last6 months and on 2 occasions they progressed to generalizedtonic clonic seizures. There was no family history of migraineor epilepsy.
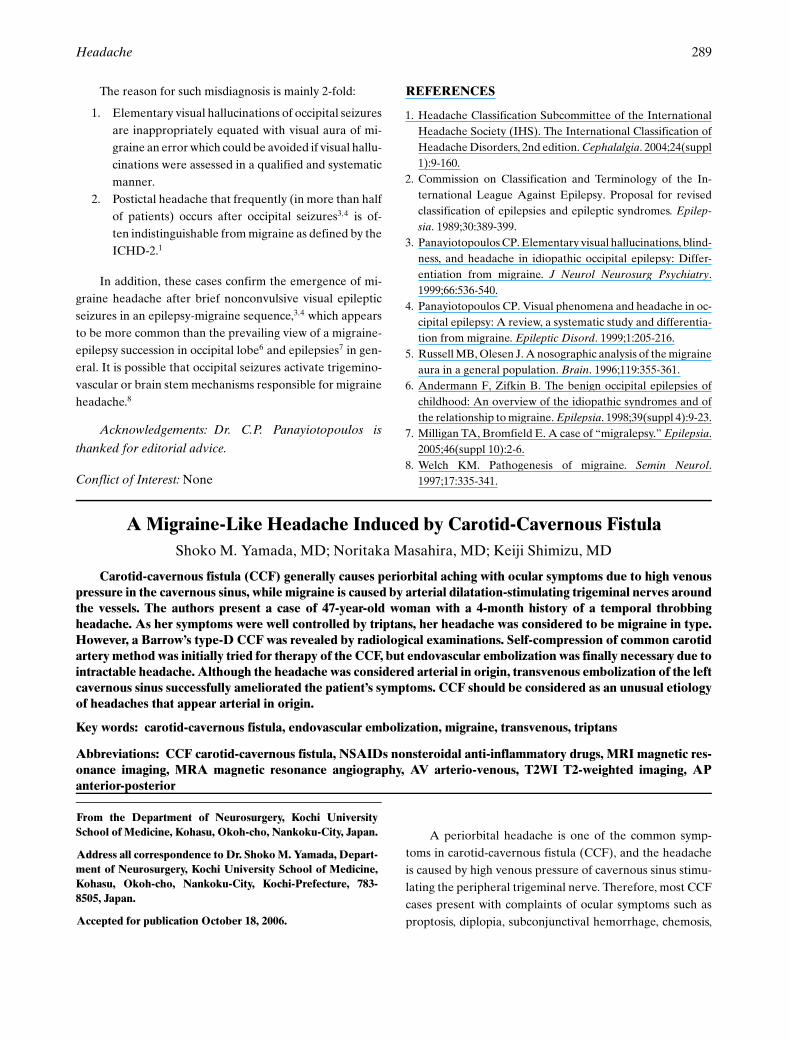
Routine biochemical investigations were normal. HerEEG had mild and nonspecific abnormalities. Brain CT scanshowed a ring-enhancing lesion in the right parieto-occipitalarea with minimal edema suggestive of neurocysticercosis(Fig. 2). Patient was treated with albendazole for 21 days andcarbamazepine. No further seizures or headache occurredin 2 years of follow-up and brain CT scan norma-lized.
COMMENTSBoth patients of this report had symptomatic occipital
lobe epilepsy as documented with brain imaging, demon-strating discrete occipital lesions of cysticercosis. They weremisdiagnosed and treated as migraine with visual aura for2 years thus depriving them from appropriate diagnosticprocedures and management; cysticercosis is a common,treatable, and reversible cause of epilepsy in developingcountries. In both patients, the correct diagnosis was estab-lished only after the onset of generalized convulsions.
Fig 2.—CT scan head showing a ring-enhancing lesion in theright parietooccipital area with minimal edema suggestive ofneurocysticercosis.
Headache 289
The reason for such misdiagnosis is mainly 2-fold:
1. Elementary visual hallucinations of occipital seizuresare inappropriately equated with visual aura of mi-graine an error which could be avoided if visual hallu-cinations were assessed in a qualified and systematicmanner.
2. Postictal headache that frequently (in more than halfof patients) occurs after occipital seizures3,4 is of-ten indistinguishable from migraine as defined by theICHD-2.1
In addition, these cases confirm the emergence of mi-graine headache after brief nonconvulsive visual epilepticseizures in an epilepsy-migraine sequence,3,4 which appearsto be more common than the prevailing view of a migraine-epilepsy succession in occipital lobe6 and epilepsies7 in gen-eral. It is possible that occipital seizures activate trigemino-vascular or brain stem mechanisms responsible for migraineheadache.8
Acknowledgements: Dr. C.P. Panayiotopoulos is
thanked for editorial advice.
Conflict of Interest: None
REFERENCES
1. Headache Classification Subcommittee of the InternationalHeadache Society (IHS). The International Classification ofHeadache Disorders, 2nd edition. Cephalalgia. 2004;24(suppl1):9-160.
2. Commission on Classification and Terminology of the In-ternational League Against Epilepsy. Proposal for revisedclassification of epilepsies and epileptic syndromes. Epilep-sia. 1989;30:389-399.
3. Panayiotopoulos CP. Elementary visual hallucinations, blind-ness, and headache in idiopathic occipital epilepsy: Differ-entiation from migraine. J Neurol Neurosurg Psychiatry.1999;66:536-540.
4. Panayiotopoulos CP. Visual phenomena and headache in oc-cipital epilepsy: A review, a systematic study and differentia-tion from migraine. Epileptic Disord. 1999;1:205-216.
5. Russell MB, Olesen J. A nosographic analysis of the migraineaura in a general population. Brain. 1996;119:355-361.
6. Andermann F, Zifkin B. The benign occipital epilepsies ofchildhood: An overview of the idiopathic syndromes and ofthe relationship to migraine. Epilepsia. 1998;39(suppl 4):9-23.
7. Milligan TA, Bromfield E. A case of “migralepsy.” Epilepsia.2005;46(suppl 10):2-6.
8. Welch KM. Pathogenesis of migraine. Semin Neurol.1997;17:335-341.
A Migraine-Like Headache Induced by Carotid-Cavernous FistulaShoko M. Yamada, MD; Noritaka Masahira, MD; Keiji Shimizu, MD
Carotid-cavernous fistula (CCF) generally causes periorbital aching with ocular symptoms due to high venouspressure in the cavernous sinus, while migraine is caused by arterial dilatation-stimulating trigeminal nerves aroundthe vessels. The authors present a case of 47-year-old woman with a 4-month history of a temporal throbbingheadache. As her symptoms were well controlled by triptans, her headache was considered to be migraine in type.However, a Barrow’s type-D CCF was revealed by radiological examinations. Self-compression of common carotidartery method was initially tried for therapy of the CCF, but endovascular embolization was finally necessary due tointractable headache. Although the headache was considered arterial in origin, transvenous embolization of the leftcavernous sinus successfully ameliorated the patient’s symptoms. CCF should be considered as an unusual etiologyof headaches that appear arterial in origin.
Key words: carotid-cavernous fistula, endovascular embolization, migraine, transvenous, triptans
Abbreviations: CCF carotid-cavernous fistula, NSAIDs nonsteroidal anti-inflammatory drugs, MRI magnetic res-onance imaging, MRA magnetic resonance angiography, AV arterio-venous, T2WI T2-weighted imaging, APanterior-posterior
From the Department of Neurosurgery, Kochi UniversitySchool of Medicine, Kohasu, Okoh-cho, Nankoku-City, Japan.
Address all correspondence to Dr. Shoko M. Yamada, Depart-ment of Neurosurgery, Kochi University School of Medicine,Kohasu, Okoh-cho, Nankoku-City, Kochi-Prefecture, 783-8505, Japan.
Accepted for publication October 18, 2006.
A periorbital headache is one of the common symp-toms in carotid-cavernous fistula (CCF), and the headacheis caused by high venous pressure of cavernous sinus stimu-lating the peripheral trigeminal nerve. Therefore, most CCFcases present with complaints of ocular symptoms such asproptosis, diplopia, subconjunctival hemorrhage, chemosis,

290 February 2007
or with a periocular bruit.1 Evans Schiffman reported oneCCF patient who presented initially only with a headache,and then developed visual disturbances.2 In contrast, mi-graine is a severe pulsating headache caused by dilatation ofarteries in the central nervous system stimulating the trigem-inal nerve.3 While it is conceivable that CCF could causemigraine or migraine-type symptoms, there has been no re-port of CCF patients whose presenting symptoms were onlymigraine.
CASE PRESENTATIONA 47-year-old woman with a 4-month history of a
migraine-like headache was referred to our hospital be-cause of worsening of the headache. The patient had nohistory of headaches or head trauma prior to the migraine-like headache. She was neurologically intact, complainingof a left temporal throbbing headache radiating to the leftoccipital area, which had been poorly controlled by non-steroidal anti-inflammatory drugs (NSAIDs), antidepres-sants, and minor tranquilizers. Only triptans ameliorated herheadache, but the effectiveness lasted for a few hours. Shewas aware of neither aura nor any associated symptoms be-fore the headache occurred. The headache occurred 3 to 4times a day without worsening with exertion. She felt nau-sea at the time of the headache and even vomited whenthe headache was aggravated. Magnetic resonance imag-ing (MRI) demonstrated a flow void sign in the left cav-ernous sinus (Fig. 1A) and magnetic resonance angiography(MRA) revealed an abnormal high intensity extravascularlesion in the cavernous portion of the left internal carotidartery (Fig. 1B), consistent with a CCF. A left Barrow’stype-D CCF was diagnosed by conventional angiography(Fig. 2A).4 The patient complained of only a headache, andophthalmologic examinations identified no abnormalities.Therefore, the patient was initially treated conservativelyby trying to control her headache with NSAIDs, triptans(sumatriptan, zomitriptan, rizatriptan), and carbamazepine(tegretol). We prescribed carbamazepine, considering thatthe CCF might stimulate the trigeminal nerve in the cav-ernous sinus and expecting that she did not take too manyNSAIDs for her headache. In addition to the medication,self-compression of common carotid artery and jugular veinwas tried for the patient.5 Triptans were somewhat effec-tive in controlling the patient’s symptoms, although she re-quired doses every 3 to 4 hours daily due to limited ef-ficacy. Because of the limitations of medical therapy andself-compression method, endovascular embolization wasperformed 2 weeks after the first angiography, using atransvenous approach to the left cavernous sinus. The sinus
was packed by coiling and angiographically arterio-venous(AV) shunting and the vascular networks extending from ex-ternal carotid artery completely disappeared (Fig. 2B). Thepatient was discharged from our hospital 3 weeks after theembolization necessitating no medication, and she has beenfree from the headache for more than 1 year.
COMMENTSA migraine-like headache is a very rare presentation of
CCF with patients complaining predominantly of headachesin the periorbital region. Our patient complained of a throb-bing headache in the left temporal region radiating to theleft occipital area, which was atypical for CCF patients. Inmigraine cases, headache symptoms localize to the tempo-ral region in 58.3% of the patients and to the occipital re-gion in 39.8% of affected individuals.6 Our case presentedwith a classic migraine picture, with headache extendingfrom the temporal to occipital regions. Furthermore, trip-tans, migraine-specific headache-relieving drugs, which actby preventing the release of inflammatory substances fromnerve endings and causing arterial vasoconstriction, were apartially effective therapy in this case, as would be expectedin a typical migraine.3 Thus, it is natural to consider that theheadache in our case was symptomatically migraine arisingfrom arterial dilatation.
Could a migraine-like headache alone be an active in-dication of endovascular surgery for CCF? It has been re-ported that indirect types of CCF tend to have a more be-nign course and can resolve spontaneously.7 In our case, thedirect fistula was angiographically very weak with insignifi-cant A-V shunting (Fig. 2A, black arrow head). Based on theevidence, we expected spontaneous resolution of our CCFutilizing self-compression of the common carotid artery andjugular vein, which was reported to be successful in 30%of dural CCF and 17% of direct CCF.5 This approach wasnot successful in this case. We finally performed endovascu-lar embolization with alleviation of all symptoms as medicaltherapy with triptans and NSAIDs was only partially effec-tive.
Which approach should be selected in cases such as this,transvenous or transarterial? Generally, treatment for CCFis via transvenous embolization,8,9 but the goal of treatmentin our case was to ameliorate the patient’s migraine-likeheadache rather than elimination of the fistula. The patient’spulsating headache was presumably caused by stretching ofdural arteries draining into the cavernous sinus, rather thanby high pressure of the cavernous sinus itself, because an-giography displayed normal intracranial venous flow with-out distension of the superior or inferior ophthalmic veins

Headache 291
Fig 1.—Preoperative magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA). (A) Axial (left) and coronal(right) views of T2-weighted imaging (T2WI) in MRI reveal a flow-void sign in the left cavernous sinus (white arrows). (B) MRAdemonstrates high intensity lesion (black arrows) at the cavernous portion of the left internal carotid artery.
(Fig. 2A). Considering the angiographical evidence, transve-nous embolization of the left cavernous sinus might inter-rupt the normal venous circulation of the left Sylvian veinpotentially causing right hemiparesis or aphasia; however,transarterial embolization of dural arteries is palliative andthe arteries recanalize with high frequency.10 In spite of thecomplexity of feeding arteries, dural fistulas simply drain intothe cavernous sinus with intervening vascular networks con-tained within the adjacent dura. The authors finally selectedtransvenous embolization of the cavernous sinus, which suc-cessfully obliterated the vascular networks from left externalcarotid artery (Fig. 2B) and alleviated all headache symp-toms.
Conflict of Interest: None
REFERENCES
1. Ghosh S, Larsen D, Day JD. Cavernous carotid fistulas. In:Winn RH, ed. Youmans Neurological Surgery, Fifth ed. NewYork: Saunders; 2003:2341-2352.
2. Evans RW, Schiffman JS. Headache as the only symptomof a spontaneous dural carotid-cavernous fistula. Headache.2005;45:1256-1259.
3. Smith TR, Sunshine A, Stark SR, Littlefield DE, SpruillSE, Alexander WJ. Sumatriptan and naproxen sodium forthe acute treatment of migraine. Headache. 2005;45:983-991.
4. Barrow DL, Spector RH, Braum IF, et al. Classification andtreatment of spontaneous carotid-cavernous fistulas. J Neu-rosurg. 1985;62:248-256.
5. Higashida RT, Hieshima GB, Halbach VV, Bentson JR,Goro K. Closure of carotid cavernous sinus fistulae by
292 February 2007
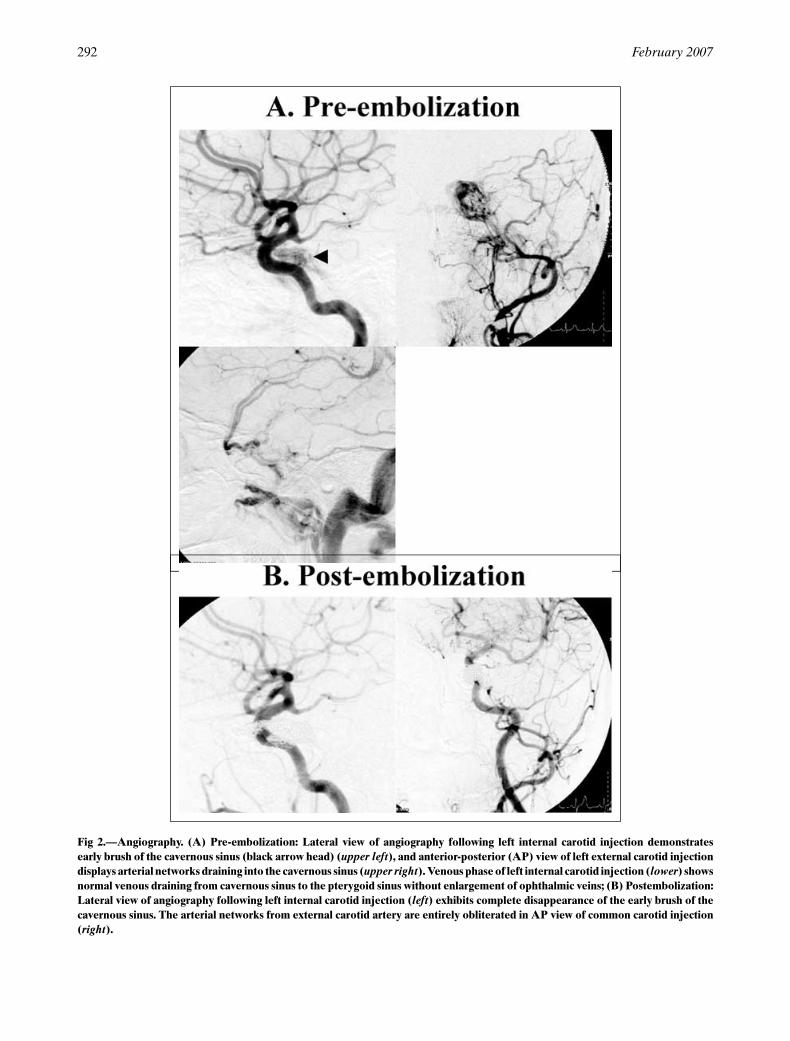
Fig 2.—Angiography. (A) Pre-embolization: Lateral view of angiography following left internal carotid injection demonstratesearly brush of the cavernous sinus (black arrow head) (upper left), and anterior-posterior (AP) view of left external carotid injectiondisplays arterial networks draining into the cavernous sinus (upper right). Venous phase of left internal carotid injection (lower) showsnormal venous draining from cavernous sinus to the pterygoid sinus without enlargement of ophthalmic veins; (B) Postembolization:Lateral view of angiography following left internal carotid injection (left) exhibits complete disappearance of the early brush of thecavernous sinus. The arterial networks from external carotid artery are entirely obliterated in AP view of common carotid injection(right).

Headache 293
external compression of the carotid artery and jugular vein.Acta Radiol (Suppl) (Stockholm). 1986;369:580-583.
6. Kelman L. Migraine pain location: A tertiary care study of1283 migraineurs. Headache. 2005;45:1038-1047.
7. Yamashita K, Taki W, Nishi S, et al. Transvenous emboliza-tion of dural caroticocavernous fistulae: Technical consider-ations. Neuroradiology. 1993;35:475-479.
8. Bellon RJ, Liu AY, Adler JR Jr, Norbash AM. Percutaneoustransfemoral embolization of an indirect carotid-cavernous
fistula with cortical venous access to the cavernous sinus. JNeurosurg. 1999;90:959-963.
9. Kirsht AF, Burson T. Combined pretemporal and endovas-cular approach to the cavernous sinus for the treatment ofcarotid-cavernous dural fistulae: Technical case report. Neu-rosurgery. 1999;44:415-418.
10. Halbach VV, Higashida RT, Hieshima GB, Hardin CW, Pri-bram H. Transvenous embolization of dural fistulas involv-ing the cavernous sinus. Am J Neuroradiol. 1989;10:377-383.
Thunderclap Headache Caused by Minimally InvasiveMedical Procedures: Description of 2 Cases
Flavio Devetag Chalaupka, MD; Giorgio Caneve, MD; Michela Mauri, MD; Giuseppe Zaiotti, MD
We report 2 very unusual cases of thunderclap headache complicating minimally invasive medical procedures.In the first case headache developed as the consequence of a pneumocephalus caused by an inadvertent intrathecalpuncture during oxygen-ozone therapy for lumbar disk herniation. The second case involved intracranial hypoten-sion, caused by the persistence of the needle, used for epidural anesthesia, and then penetrated in the subarachnoidspace.
Key words: headache, pneumocephalus, intracranial hypotension, CSF leak, epidural anesthesia, oxygen-ozonetherapy
Thunderclap headache is defined as a paroxysmal andexcruciatingly severe headache presenting with extremeabruptness.1 It exists as either a primary or a secondary con-dition. It can be associated with serious vascular intracra-nial disorders, particularly subarachnoid hemorrhage, col-loid cyst of the third ventricle, acute sinusitis, and intracra-nial hypotension.1 In all cases, an intracranial disease shouldalways be ruled out by appropriate investigations.
We describe 2 patients with severe headache of suddenonset secondary to minimally invasive medical procedures,like oxygen-ozone therapy for lumbar disk herniation andepidural anesthesia.
CASESA 27-year-old man with no significant history of
headache underwent oxygen-ozone therapy for lumbar diskherniation at the L4-L5 level. About 2 minutes after the end
From the Department of Neurology and Neurophysiology, S.Maria del Prato Hospital, Feltre, Italy.
Address all correspondence to Flavio Devetag, Department ofNeurology and Neurophysiology, “S. Maria del Prato” Hospi-tal,Via Bagnols sur Ceze 3 32032 Feltre (BL) – Italy.
Accepted for publication August 4, 2006.
of the injection, he developed severe nonpulsating pain ofabrupt onset in the left side of the face and in the occip-ital area. On the next day the headache was widespread,worsened by movement, coughing and straining and accom-panied by photophobia, nausea, and vomiting.
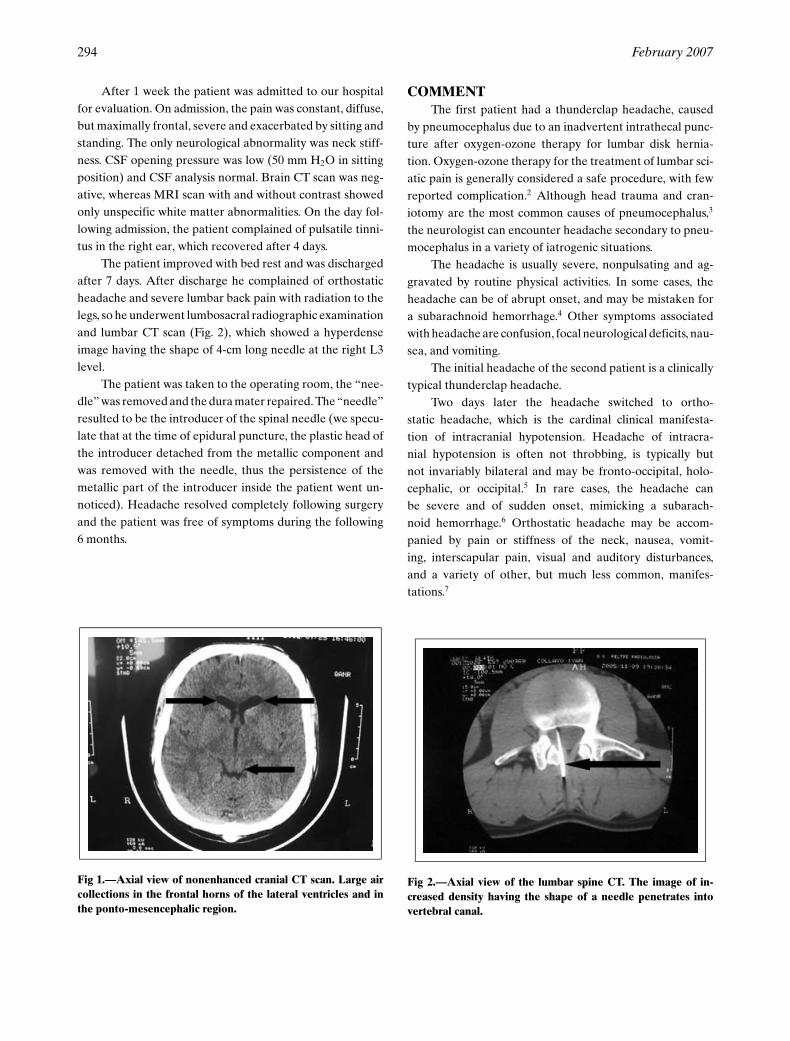
On admission, he complained of severe, diffuse, andconstant pain worsened by Valsalva-like maneuvers. Neckrigidity was the only reported neurological abnormality. Abrain CT scan revealed a large air collection in the frontalhorns of the lateral ventricles and a smaller one in the ponto-mesencephalic region (Fig. 1). He improved with bed restand was discharged from the hospital after 4 days. Therewere no further symptoms in the following 2 years.
A 36-year-old man with no significant past history ofheadache had enjoyed excellent health until February 2005when he had an epidural anesthetic, done at the L2-L3 level,for varicotomy of the right saphenous vein. After discharge,he was asymptomatic for 8 months even though he some-times complained of mild local low backache. In October2005, he developed a severe headache of sudden onset whilemountain climbing, reaching the maximal intensity after afew seconds. The headache was diffuse and associated withneck tension. Over several subsequent days the pain wasmaximally frontal, not pulsating and so severe as to disruptsleep.
294 February 2007
After 1 week the patient was admitted to our hospitalfor evaluation. On admission, the pain was constant, diffuse,but maximally frontal, severe and exacerbated by sitting andstanding. The only neurological abnormality was neck stiff-ness. CSF opening pressure was low (50 mm H2O in sittingposition) and CSF analysis normal. Brain CT scan was neg-ative, whereas MRI scan with and without contrast showedonly unspecific white matter abnormalities. On the day fol-lowing admission, the patient complained of pulsatile tinni-tus in the right ear, which recovered after 4 days.
The patient improved with bed rest and was dischargedafter 7 days. After discharge he complained of orthostaticheadache and severe lumbar back pain with radiation to thelegs, so he underwent lumbosacral radiographic examinationand lumbar CT scan (Fig. 2), which showed a hyperdenseimage having the shape of 4-cm long needle at the right L3level.
The patient was taken to the operating room, the “nee-dle” was removed and the dura mater repaired. The “needle”resulted to be the introducer of the spinal needle (we specu-late that at the time of epidural puncture, the plastic head ofthe introducer detached from the metallic component andwas removed with the needle, thus the persistence of themetallic part of the introducer inside the patient went un-noticed). Headache resolved completely following surgeryand the patient was free of symptoms during the following6 months.
Fig 1.—Axial view of nonenhanced cranial CT scan. Large aircollections in the frontal horns of the lateral ventricles and inthe ponto-mesencephalic region.
COMMENTThe first patient had a thunderclap headache, caused
by pneumocephalus due to an inadvertent intrathecal punc-ture after oxygen-ozone therapy for lumbar disk hernia-tion. Oxygen-ozone therapy for the treatment of lumbar sci-atic pain is generally considered a safe procedure, with fewreported complication.2 Although head trauma and cran-iotomy are the most common causes of pneumocephalus,3
the neurologist can encounter headache secondary to pneu-mocephalus in a variety of iatrogenic situations.
The headache is usually severe, nonpulsating and ag-gravated by routine physical activities. In some cases, theheadache can be of abrupt onset, and may be mistaken fora subarachnoid hemorrhage.4 Other symptoms associatedwith headache are confusion, focal neurological deficits, nau-sea, and vomiting.
The initial headache of the second patient is a clinicallytypical thunderclap headache.
Two days later the headache switched to ortho-static headache, which is the cardinal clinical manifesta-tion of intracranial hypotension. Headache of intracra-nial hypotension is often not throbbing, is typically butnot invariably bilateral and may be fronto-occipital, holo-cephalic, or occipital.5 In rare cases, the headache canbe severe and of sudden onset, mimicking a subarach-noid hemorrhage.6 Orthostatic headache may be accom-panied by pain or stiffness of the neck, nausea, vomit-ing, interscapular pain, visual and auditory disturbances,and a variety of other, but much less common, manifes-tations.7
Fig 2.—Axial view of the lumbar spine CT. The image of in-creased density having the shape of a needle penetrates intovertebral canal.

Headache 295
In addition to clinical symptoms, the diagnosis of in-tracranial hypotension is made after well-established di-agnostic investigations. The cerebrospinal fluid openingpressure is typically low and brain MRI shows diffusemeningeal gadolinium enhancement, which is limited topachymeninges.
It can occur spontaneously or after medical and surgi-cal procedures and spine trauma.8 Intracranial hypotensionis usually a benign condition; however, potentially fatal com-plications are the formation of an acute intracranial subduralhematoma,8 subarachnoid hemorrhage,9 and spinal subduralhematoma.10
In our case, the development of intracranial hypoten-sion is due to the permanence of the introducer of the spinalneedle placed during epidural anesthesia. It remained in theback at the L2-L3 level for 8 months after the procedure andpenetrated the subarachnoid space.
Conflict of Interest: None.
REFERENCES
1. Headache Classification Subcommittee of the Interna-tional Headache Society. The international classification ofheadache disorders 2nd edition. Cephalalgia. 2004; Suppl 1.
2. Andreula CF, Simonetti L, de Santis F, Agati R, RicciR, Leonardi M. Minimally invasive oxygen-ozone therapyfor lumbar disk herniation. Am J Neuroradiol. 2003;24:996-1000.
3. Ruge JR, Cerullo LJ, McLone DG. Pneumocephalus in pa-tients with CSF shunts. J Neurosurg. 1985;63:532-536.
4. Becker WJ. Pneumocephalus as a cause for headache. CanJ Neurol Sci. 2002;29:278-281.
5. Pastor-Juan MR, Poyatos C, Soto-Sarrion C. Neumocefalotras anesthesia epidural. Rev Neurol. 2003;36:999-1000.
6. Schievink WI, Wijdicks EF, Meyer FB, Sonntag VK. Sponta-neous intracranial hypotension mimicking aneurysmal sub-arachnoid hemorrhage. Neurosurgery. 2001;48:513-516; dis-cussion 516-517.
7. Mokri B. Headaches caused by decreased intracranialpressure: Diagnosis and management. Curr Opin Neurol.2003;16:319-326.
8. Sciubba DM, Kretzer RM, Wang PP. Acute intracranial sub-dural hematoma following a lumbar CSF leak caused byspine surgery. Spine. 2005;30:730-732.
9. Wells JB, Sampson IH. Subarachnoid hemorrhage present-ing as post-dural puncture headache: A case report. Mt SinaiJ Med. 2002;69:109-110.
10. Guthikonda M, Schmidek HH, Wallmann LJ, Snyder TM.Spinal subdural hematoma: Case report and review of theliterature. Neurosurgery. 1979;5:614-616.
Perineural Invasion of Sinonasal Lymphoma: A RareCause of Trigeminal Neuropathy
Chih-Wei Liang, MD; Ying-Lin Chen, MD
Trigeminal neuropathy is characterized by sensory disturbance of the division of trigeminal nerve, and some-times is associated with pain. Trigeminal neuropathy secondary to perineural invasion of sinonasal lymphoma isextremely rare. Likewise, sinonasal lymphoma is infrequently demonstrated initially with cranial neuropathy. Thepresent case served to broaden the differential diagnosis of secondary trigeminal neuropathy and to alert cliniciansto cautiously assess perineural spread of occult neoplasm in sinonasal tract and larynx or pharynx for cases withevolving trigeminal neuropathy or even other cranial nerve neuropathy in which no definite cause is identified.
Key words: trigeminal neuropathy, sinonasal lymphoma, perineural invasion
Differential diagnosis of trigeminal neuropathy com-prises a variety of clinical etiologies. Idiopathic trigeminal
From the Departments of Otolaryngology-Head and NeckSurgery, Chang Gung Memorial Hospital and Chang GungUniversity, Taipei, Taiwan.
Address all correspondence to Dr. Ying-Lin Chen, No. 5,Fu-Hsing Street, Kuei-Shan, Tao-Yuan, Taiwan, Republic ofChina.
Accepted for publication July 31, 2006.
neuropathy, however, is often judged while no definite causeis found.
Unawareness of the neoplastic perineural invasion as apossible cause of trigeminal neuropathy may delay in diag-nosis of underlying malignant tumor. Inarguably, it is some-times difficult to detect such occult tumor because these ma-lignant tumors may locate in some area where visual inspec-tion is not easily carried out. Long lasting, evolving trigem-inal neuropathy should arouse clinician’s suspicion of ma-lignancy involvement. In addition to thorough neurological
296 February 2007
examinations, we advocate cautious head and neck investi-gation and use of MRI for unexplained trigeminal neuropa-thy, which may signify serious underlying disease. Herein, wepresent a patient with trigeminal neuropathy as the primaryclinical presentation of sinonasal lymphoma. Perineural in-vasion was illustrated radiographically to demonstrate thisrare mode of cancer spreading and to emphasize diligentevaluation of cancer involvement before diagnosis of idio-pathic trigeminal neuropathy is made.
CASE REPORTAn 83-year-old male patient sought evaluation from
a neurologist in May 2005 because of a consistent numb-ness, altered sensation, and intermittent pain over right facefor a couple of months. The patient has medical history ofessential hypertension, hepatitis B, liver nodules and cysts,and benign prostate hypertrophy. Detailed neurological ex-ams showed reduced perception to light touch and pin-prick, numbness sensation, and a dull ache in the distribu-tion of right mandibular division of the trigeminal nerve.Besides, the patient demonstrated anisocoria of pupils anddiplopia at right gaze. There was no other neurologicaldeficit. Brain MRI was performed on June 17, 2005 and dis-played a space occupying lesion at right posterior ethmoidsinus, right orbital apex at parasella region, and anterior as-pect of sphenoid sinus. The patient was then referred to our
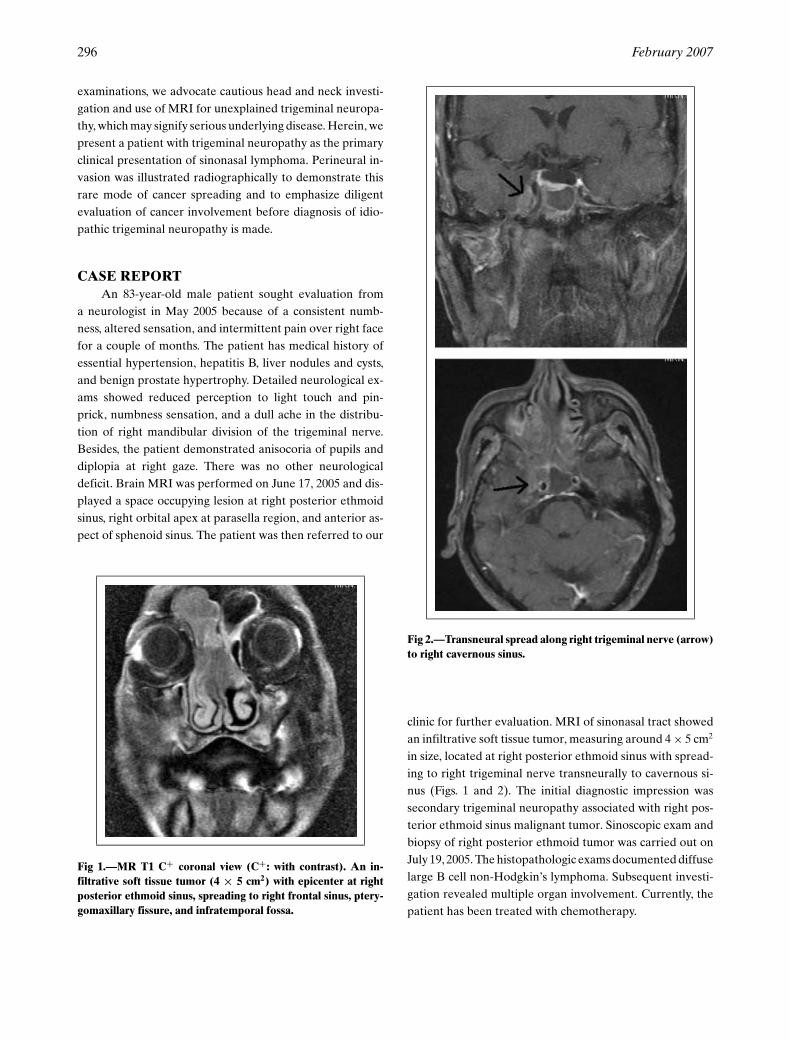
Fig 1.—MR T1 C+ coronal view (C+: with contrast). An in-filtrative soft tissue tumor (4 × 5 cm2) with epicenter at rightposterior ethmoid sinus, spreading to right frontal sinus, ptery-gomaxillary fissure, and infratemporal fossa.
Fig 2.—Transneural spread along right trigeminal nerve (arrow)to right cavernous sinus.
clinic for further evaluation. MRI of sinonasal tract showedan infiltrative soft tissue tumor, measuring around 4 × 5 cm2
in size, located at right posterior ethmoid sinus with spread-ing to right trigeminal nerve transneurally to cavernous si-nus (Figs. 1 and 2). The initial diagnostic impression wassecondary trigeminal neuropathy associated with right pos-terior ethmoid sinus malignant tumor. Sinoscopic exam andbiopsy of right posterior ethmoid tumor was carried out onJuly 19, 2005. The histopathologic exams documented diffuselarge B cell non-Hodgkin’s lymphoma. Subsequent investi-gation revealed multiple organ involvement. Currently, thepatient has been treated with chemotherapy.

Headache 297
DISCUSSIONTrigeminal neuropathy was first designated by Spillane
and Wells in 1959 as a disorder characterized by transientor persistent sensory disturbance that usually involves thedistribution of one or more divisions of trigeminal nerve.1
Although it is uncommonly encountered, it will cause signif-icant orofacial symptoms—usually annoying numbness andsensory disturbance. A broad variety of local and systemicdisorders would result in trigeminal neuropathy. The mostcommon causes are nonneoplastic cerebral disorders andidiopathic origin.2 Trigeminal neuropathy associated withmalignant disease is typically resulting from tumor depo-sition around the trigeminal nerve either intracranially orextracranially.3 Clinical features that highly suggest malig-nancy involvement are neuropathy in more than one terri-tory of the trigeminal nerve and other accompanying neu-rologic features, such as dysfunction of branches of facialnerve.3,4
Perineural spread of head and neck cancer is uncom-monly encountered as the cause of cranial neuropathy.Trigeminal neuropathy with facial pain and paresthesia wasthe most common presenting feature and may lead to the di-agnosis of perineural invasion.4,5 Adenoid cystic carcinomaand squamous cell carcinoma in naso- and oropharynx, sali-vary glands, and paranasal cavities accounted for most ofsuch cases.5,6 An extensive medline search revealed no sim-ilar reports of secondary trigeminal neuropathy associatedwith perineural invasion of sinonasal lymphoma. Occult neo-plasm in pharynx or larynx may extend to invade trigemi-nal nerve and therefore thorough examination of these sitesfor unexplained, evolving trigeminal neuropathy is manda-tory.4,6 On the other hand, in patients who had a history ofprevious management of carcinoma, development of trigem-inal neuropathy or other cranial neuropathy may indicatetumor recurrence.4,5
Clinical presentations of sinonasal lymphoma may benonspecific complaints, such as nasal obstruction or fullnesssensation, and are very likely to be ignored by both pa-tients and clinicians. Interestingly, this patient did not com-plain of any nasal symptoms throughout the course, whichmay be attributed to varying level of individual toleranceto nasal obstruction and the indolent growing nature of thetumor. Notably, this lack of symptoms may preclude nasalneoplasm from initial differential diagnosis. Search for etiol-ogy of trigeminal neuropathy relies on establishing thoroughmedical and dental history, investigating any systemic dis-ease that could include trigeminal neuropathy as primary orsecondary clinical presentation, and image studies. Gadolin-
ium contrast-enhanced MRI (Gd-MRI) with fat suppressionis the choice of image tool to delineate mass lesion or vascu-lar deformities around the base of brain or along the courseof the trigeminal nerve. Characteristic presentations of neo-plastic perineural spread include foraminal enlargement ordestruction, fatty tissue obliteration, and nerve enlargementor enhancement.7 Moreover, perineural tumor growth ofmandibular or maxillary divisions of trigeminal nerve is bestvisualized by Gd-MRI in the coronal plane. We advocateotolaryngologists consultation and prompt use of MRI forall patients with long-standing trigeminal neuropathy thatno definite etiology is identifiable.
COMMENTSPatients with trigeminal neuropathy have infrequently
presented to otolaryngologists. However, neoplasms of headand neck may give rise to the secondary trigeminal neuropa-thy, especially with evolving paresthesia and pain in orofacialregion. Meticulous physical examinations of head and neckalong with image studies will prevent misdiagnosis of oc-cult neoplasm with perineural invasion and assure adequatetreatment of underlying disease in time.
Conflict of Interest: None
REFERENCES
1. Gibbin KP, Griffith IP. Idiopathic sensory trigeminal neu-ropathy. J Laryngol Otol. 1978;92:915-923.
2. Dumas M, Perusse R. Trigeminal sensory neuropathy: Astudy of 35 cases. Oral Surg Oral Med Oral Pathol Oral RadiolEndod. 1999;87:577-582.
3. Shotts RH, Porter SR, Kumar N, et al. Longstanding trigem-inal sensory neuropathy of nontraumatic cause. Oral SurgOral Med Oral Pathol Oral Radiol Endod. 1999;87:572-576.
4. Schifter M, Barret AP. Perineural spread of squamous cellcarcinoma involving trigeminal and facial nerves. Oral SurgOral Med Oral Pathol. 1993;75:587-590.
5. Boerman RH, Maassen EM, Joosten J, et al. Trigeminal neu-ropathy secondary to perineural invasion of head and neckcarcinomas. Neurology. 1999;53:213-216.
6. Ballantyne AJ, McCarten AB, Ibanez ML. The extension ofcancer of the head and neck through peripheral nerves. AmJ Surg. 1963;106:651-667.
7. Marsot-Dupuch K, De Givry SC, Ouayoun M. Wegenergranulomatosis involving the pterygopalatine fossa: An un-usual case of trigeminal neuropathy. Am J Neuroradiol.2002;23:312-315.

298 February 2007
Repeat Trigeminal Nerve Radiosurgery for Refractory Cluster HeadacheFails to Provide Long-Term Pain Relief
Shearwood McClelland III, MD; Gene H. Barnett, MD; Gennady Neyman, PhD;John H. Suh, MD
Objective/Background.—Medically refractory cluster headache (MRCH) is a debilitating condition that hasproven resistant to many modalities. Previous reports have indicated that radiosurgery for MRCH provides lit-tle long-term pain relief, with moderate/significant morbidity. However, there have been no reports of repeatedradiosurgery in this patient population. We present our findings from the first reports of repeat radiosurgery forMRCH.
Methods.—Two patients with MRCH underwent repeat gamma knife radiosurgery at our institution. Each fulfilledclinical criteria for treatment, including complete resistance to pharmacotherapy, pain primarily localized to the ophthalmicdivision of the trigeminal nerve, and psychological stability. Both patients previously received gamma knife radiosurgery(75 Gy) for MRCH with no morbidity, but no long-term improvement of pain relief (Patient 1 = 5 months, Patient 2 = 10months) after treatment. For repeat radiosurgery, each patient received 75 Gy to the 100% isodose line delivered to the rootentry zone of the trigeminal nerve, and was evaluated postretreatment. Pain relief was defined as: excellent (free of MRCHwith minimal/no medications), good (50% reduction of MRCH severity/frequency with medications), fair (25% reduction),or poor (less than 25% reduction).
Results.—Following repeat radiosurgery, long-term pain relief was poor in both patients. Neither patient sustained anyimmediate morbidity following radiosurgery. Patient 2 experienced right facial numbness 4 months postretreatment, whilePatient 1 experienced no morbidity.
Conclusion.—Repeat radiosurgery of the trigeminal nerve fails to provide long-term pain relief for MRCH. Given thereported failures of initial and repeat radiosurgery for MRCH, trigeminal nerve radiosurgery should not be offered forMRCH.
Key words: refractory cluster headache, repeat gamma knife radiosurgery, trigeminal nerve, pain relief
Medically refractory cluster headache (MRCH) is char-acterized by sudden onset of excruciating unilateral painoriginating around the temple, eye, or cheek primarily alongthe ophthalmic division of the trigeminal nerve.1 Occur-ring in approximately 20% of cluster headache patients,MRCH poses significant challenges to patients and treat-ing physicians alike.2 Multiple surgical modalities have been
From the Department of Neurosurgery, University of Min-nesota Medical School, Minneapolis, MN (Dr. McClelland);Brain Tumor Institute, Department of Neurosurgery, TheCleveland Clinic Foundation, Cleveland, OH (Dr. Barnett);and Brain Tumor Institute, Department of Radiation Oncol-ogy, The Cleveland Clinic Foundation, Cleveland, OH (Drs.Neyman and Suh).
Address all correspondence to Shearwood McClelland III, MD,Department of Neurosurgery, University of Minnesota Medi-cal School, 420 Delaware Street SE, Mayo Mail Code 96, Min-neapolis, MN 55455.
Accepted for publication August 23, 2006.
attempted, with the majority associated with significant mor-bidity and only modest clinical efficacy.3-11 Previous studieshave investigated the role of radiosurgery to treat MRCH,yielding poor to moderate long-term efficacy and significantmorbidity.12,13 However, there have been no reports of re-peat radiosurgery for MRCH. We report on 2 patients whopreviously underwent radiosurgery for MRCH without ef-ficacy who subsequently underwent repeat radiosurgery forMRCH.
CLINICAL MATERIALS AND METHODSPatient Histories.—Patient 1 was a 41-year-old man
with a 13-year medical history of right-sided MRCHfor which he had taken verapamil, tegretol, neurontin,amitriptyline, lithium, valproic acid, and methadone unsuc-cessfully. His headaches were retroorbital in location, asso-ciated with tearing and redness of his right eye, and typicallyoccurred 3 to 4 times per day, lasting 30 to 40 minutes induration. Patient 2 was a 33-year-old man with a 30-month

Headache 299
medical history of right-sided MRCH for which he had takenverapamil, desyrel, DHE-45, demerol, and capsaicin unsuc-cessfully. His headaches were frontotemporal and periorbitalin location, typically occurring 15 to 20 times per month, eachlasting 6 to 7 hours in duration, with a sufficient number ofepisodes lasting between 15 and 180 minutes to meet the In-ternational Classification of Headache Disorders criteria forchronic cluster headache.1,14
Because of the intractability of their headaches despiteprophylactic interventions, both patients chose to undergogamma knife radiosurgery fully aware of the experimentalnature of the procedure, as well as alternative treatmentsand side effects. Each patient’s right trigeminal nerve wastargeted with 75 Gy (collimator factor = 0.80, equivalent to82 Gy with contemporary collimator factor of 0.87) to the100% isodose line, using a model B gamma knife (ElektaAB, Stockholm). Although there was no morbidity follow-ing treatment, neither patient experienced long-term painrelief. After a discussion of all alternative treatments, riskof failure, and risk of side effects, each patient elected toundergo repeat radiosurgery of the trigeminal nerve.
Radiosurgical Retreatment.—Both patients were ad-mitted for outpatient radiosurgery to our Gamma KnifeCenter. Each patient arrived on the morning of the proce-dure, and a stereotactic frame was applied under local anes-thesia with intravenous sedation. The frame was oriented tomake the base ring of the frame parallel to the trigeminalnerve axis.15 Preoperative imaging systematically includedmagnetic resonance (MR) and computed tomography (CT)scans. Axial MR sequences (Siemens 1.5 Tesla) included T2high-resolution (0.5 mm) 3-dimensional acquisition and 3-dimensional T1 acquisition, as previously described.12 CTbone window served to check and (when necessary) correctfor potential MR distortion.13 A single 4-mm collimator wasused to target the cisternal segment of the nerve ipsilateralto symptom onset, defined as the portion between Meckel’scave and the pons. The anatomic target was the proximaltrigeminal nerve, previously described as the radiosurgicaltarget for essential trigeminal neuralgia and MRCH.12,13,15-17
Both patients received 75 Gy (collimator factor = 0.80) tothe 100% isodose line, using a model B gamma knife (ElektaAB), as previously reported for trigeminal neuralgia.16
Post-Treatment Course.—Outcomes were divided into4 pain relief categories, as previously described:12,13 excel-lent (free of MRCH with minimal/no medications), good(50% reduction of MRCH severity/frequency with medica-tions), fair (25% reduction of MRCH), and poor (less than25% reduction of MRCH). Although neither patient suf-fered any immediate morbidity, both patients experienced
poor long-term pain relief outcomes. Patient 1 experiencedno morbidity, but postretreatment also had no pain relief.Thirteen days after repeat radiosurgery, Patient 2 was hos-pitalized 10 days for continuing MRCH. One month postre-treatment, he experienced good pain relief which lasted 3additional months until the headaches recurred, this timeoccurring 2 to 3 times per day, along with complaints ofright facial numbness. Six months after retreatment, he un-derwent a stereotactic right trigeminal glycerol neurolysis.Unfortunately, the patient continued to have no pain reliefat 12 months postretreatment. Neither patient experiencedcorneal reflex pathology, complete analgesia along the firstdivision of the trigeminal nerve, or anesthesia dolorosa.
COMMENTSThe observation that invasive surgical approaches in-
volving the trigeminal nerve provided moderate degrees ofpain relief for MRCH patients4-6,11,18 led to the idea of usingradiosurgery as a treatment modality for this patient popu-lation, with the hope of avoiding the significant morbidity(corneal reflex damage, anesthesia dolorosa) directly pro-portional to the degree of pain relief reported with lesion-ing procedures such as percutaneous radiofrequency retro-gasserian rhizotomy (PRFR).6,8,19 Although an initial retro-spective report indicated that trigeminal nerve radiosurgerycould provide excellent pain relief for the majority of MRCHpatients,13 a subsequent prospective report involving morepatients and a longer degree of follow-up concluded that thechances of long-term excellent pain relief following wereminimal at best, and that the procedure carried a 50% riskof morbidity.12 Because of these adverse findings, the latterstudy recommended that radiosurgery for MRCH may notbe warranted.
The two patients in our report chose to undergo repeatradiosurgery during the 7-year span between the initial pos-itive report and the subsequent negative findings regardingtrigeminal nerve radiosurgery for MRCH. The findings ofpoor pain relief in both of our patients, combined with thoseof the aforementioned prospective study and our experiencewith long-term outcomes, appear to emphatically indicatethat radiosurgery of the trigeminal nerve is an inappropriatetreatment option for MRCH, even when repeated more dis-tally along the trigeminal nerve in the same patients.20 Thisfinding is in stark contrast to the literature on repeat radio-surgery for trigeminal neuralgia, which has demonstrated anoticeable benefit for many patients who initially failed toexperience pain relief following radiosurgery.21−23 Our find-ings, along with those from initial radiosurgery for MRCH

300 February 2007
with long-term follow-up and a study examining the long-term results of radiofrequency rhizotomy in the treatment ofMRCH lend support to the hypothesis that MRCH is cen-tral in origin, rather than peripheral.11,12,24 This reasoning hasbeen supported by the recent success of deep brain stimula-tion (DBS) of the posterior hypothalamus for MRCH, whichhas provided comparable long-term pain relief with minimalmorbidity compared with PRFR or alternative lesioning pro-cedures.11,25 Given the low likelihood of the trigeminal nervebeing involved in the origin of MRCH, the reasons for thefailure of repeat trigeminal nerve radiosurgery for MRCHbecome evident.
In conclusion, our experience with the first two reportedcases of repeat radiosurgery for MRCH revealed that re-peat trigeminal nerve radiosurgery does not provide long-term pain relief for patients with poor pain relief follow-ing initial radiosurgery. Given the reported failures of initialand repeat radiosurgery for MRCH, trigeminal nerve radio-surgery should not be offered as a modality for this patientpopulation.
Acknowledgments: We would like to thank Jane Rein
and Betty Jamison for invaluable assistance.
Conflict of Interest: None
REFERENCES
1. International Headache Society. International Classificationof Headache Disorders, 2nd ed., Headache ClassificationSubcomittee of the HIS. Cephalagia. 2004;24(suppl 1):1-160.
2. Leone M. Chronic cluster headache: New and emergingtreatment options. Curr Pain Headache Rep. 2004;8:347-352.
3. Franzini A, Ferroli P, Leone M, Broggi G. Stimulation ofthe posterior hypothalamus for treatment of chronic in-tractable cluster headaches: First reported series. Neuro-surgery. 2003;52:1095-1101.
4. Green MW. Long-term follow-up of chronic clusterheadache treated surgically with trigeminal tractotomy.Headache. 2003;43:479-481.
5. Matharu MS, Goadsby PJ. Persistence of attacks of clus-ter headache after trigeminal nerve root section. Brain.2002;125(Pt 5):976-984.
6. Mathew NT, Hurt W. Percutaneous radiofrequency trigem-inal gangliorhizolysis in intractable cluster headache.Headache. 1988;28:328-331.
7. Meyer JS, Binns PM, Ericsson AD, Vulpe M. Sphenopala-tine gangionectomy for cluster headache. Arch Otolaryngol.1970;92:475-484.
8. Rozen TD. Interventional treatment for cluster headache:A review of the options. Curr Pain Headache Rep. 2002;6:57-64.
9. Rowed DW. Chronic cluster headache managed by nervusintermedius section. Headache. 1990;30:401-406.
10. Solomon S, Apfelbaum RI. Surgical decompression of thefacial nerve in the treatment of chronic cluster headache.Arch Neurol. 1986;43:479-482.
11. Taha JM, Tew JM Jr. Long-term results of radiofrequencyrhizotomy in the treatment of cluster headache. Headache.1995;35:193-196.
12. Donnet A, Valade D, Regis J. Gamma knife treatment forrefractory cluster headache: Prospective open trial. J NeurolNeurosurg Psychiatry. 2005;76:218-221.
13. Ford RG, Ford KT, Swaid S, Young P, Jennelle R. Gammaknife treatment of refractory cluster headache. Headache.1998;38:3-9.
14. Olesen J. The international classification of headachedisorders, 2nd edition (ICHD-II). Rev Neurol (Paris).2005;161:689-691.
15. Regis J, Bartolomei F, Metellus P, et al. Radiosurgery fortrigeminal neuralgia and epilepsy. Neurosurg Clin N Am.1999;10:359-377.
16. Kondziolka D, Lunsford LD, Flickinger JC, et al. Stereo-tactic radiosurgery for trigeminal neuralgia: A multiinstitu-tional study using the gamma unit. J Neurosurg. 1996;84:940-945.
17. Regis J. High-dose trigeminal neuralgia radiosurgery asso-ciated with increased risk of trigeminal nerve dysfunction.Neurosurgery. 2002;50:1401-1403.
18. Kirkpatrick PJ, O’Brien MD, MacCabe JJ. Trigeminal nervesection for chronic migrainous neuralgia. Br J Neurosurg.1993;7:483-490.
19. O’Brien MD, MacCabe JJ. Trigeminal nerve section for un-remitting migrainous neuralgia. In: Rose FC, Zilkha KJ,eds. Progress in Migraine Research, Vol 1. London: Pitman;1981:185-187.
20. McClelland S III, Tendulkar RD, Barnett GH, Neyman G,Suh JH. Long-term results of radiosurgery for refractorycluster headache. Neurosurgery. 2006;59:1258-1263.
21. Hasegawa T, Kondziolka D, Spiro R, Flickinger JC,Lunsford LD. Repeat radiosurgery for refractory trigemi-nal neuralgia. Neurosurgery. 2002;50:494-502.
22. Pollock BE, Foote RL, Link MJ, Stafford SL, Brown PD,Schomberg PJ. Repeat radiosurgery for idiopathic trigem-inal neuralgia. Int J Radiat Oncol Biol Phys. 2005;61:192-195.
23. Zhang P, Brisman R, Choi J, Li X. Where to locate theisocenter? The treatment strategy for repeat trigeminal neu-ralgia radiosurgery. Int J Radiat Oncol Biol Phys. 2005;62:38-43.
24. Goadsby PJ, Bahra A, May A. Mechanisms of clusterheadache. Cephalalgia. 1999;19(suppl 23):19-23.
25. Leone M, Franzini A, Broggi G, Bussone G. Hypothala-mic deep brain stimulation for intractable chronic clusterheadache: A 3-year follow-up. Neurol Sci. 2003;24(suppl2):143-145.

Headache 301
Cysticercosis Headache: An Important Differential of ChildhoodHeadache Disorder in Endemic Countries
Devendra Mishra, MD
Neurocysticercosis is a common pediatric central nervous system (CNS) disease in endemic areas, presentingusually with seizures but has pleomorphic manifestations, including migraine-like secondary headache. We hereinreport a pediatric patient with tension-type headache as the sole presenting feature of single cysticercus granuloma.
Key words: neurocysticercosis, tension type headache, tapeworm headache
Abbreviations: NC neurocysticercosis, SCG single cysticercus granuloma, EITB enzyme-linked immunoelectro-transfer blot, ICT intracranial hypertension, CECT contrast-enhanced computed tomography
Neurocysticercosis (NC) is the most common parasiticdisease of the CNS worldwide. It is a frequent neurologicaldisorder in many countries of Latin America, Africa, andAsia, and in many industrialized nations with a high indexof immigration from these endemic areas.1 The disease haspleomorphic manifestations based on the site, size, and num-ber of cysts, and the host immune response.1 Headache as amanifestation of NC can be due to multiple causes viz., (i)raised intracranial tension2,3 (more commonly in those withmultiple lesions or with intraventricular lesions—“tapeworm
headache”), (ii) postictal or interictal,4,5 or (iii) an ictal mani-festation.4,5 Headache as the sole manifestation of NC, with-out evidence of raised ICT or associated seizures, has beenuncommonly reported in the literature, and most reportsare confined to migraine-like headaches.4 We herein reporta pediatric patient with tension-type headache as the solepresenting feature of single cysticercus granuloma (SCG),and discuss pertinent diagnostic and therapeutic issues.
CASE-REPORTA 7-year-old girl with normal development and no sig-
nificant past history presented with complaints of frequentepisodes of headache lasting hours to days, which had startedgradually around 3 to 4 months back. The headache was mod-erate in severity (Grade 6 on Visual Analog Scale), holocra-nial in location, tightening in quality, not worsening withroutine physical activity but causing some disability (Disabil-ity Grade 2, on a 0 to 4 disability scale). There was no aura,
From Department of Pediatrics, Chacha Nehru Bal Chikit-salaya (Maulana Azad Medical College).
Address all correspondence to Dr. Devendra Mishra, Depart-ment of Pediatrics, Chacha Nehru Bal Chikitsalaya (MaulanaAzad Medical College), Geeta Colony, Delhi 110031.
Accepted for publication November 14, 2006.
photo/phono-phobia, nausea, or vomiting. The headache oc-curred every 4 to 5 days and had been gradually increasingin severity.
On examination, the systemic examination was unre-markable, especially with respect to neurological deficit, ev-idence of raised intracranial pressure, hypertension, sinustenderness, and dental or ear problems. There was no pa-pilledema. A clinical diagnosis of “frequent episodic tensiontype headache” (International Headache Society category2.2.2) was considered.6 The patient was advised to maintaina headache diary and referred for an ophthalmologic consul-tation for refraction and orthoptic evaluation, and called forfollow-up after a week. However, before the follow-up ex-amination, the patient consulted another physician and un-derwent a cranial CT. The contrast-enhanced CT scan of thehead showed a ring-enhancing lesion in the right high pari-etal region with minimal perilesional oedema, suggestive ofneurocysticercosis.7 IgG-ELISA for cysticercosis, Montouxtest with 5 TU PPD, chest X-ray and hemogram were non-contributory. The patient was treated with dexamethasone(5 days), albendazole (28 days), and anticonvulsants. Therewas no recurrence of headache over a follow-up period of 8months and a repeat CECT head 6- 1
2 months later showeddisappearance of the lesion.
COMMENTSHeadache is a common disorder in the pediatric age
group with the prevalence reported to be as high as 37% to51% in 7-year-olds, and further increasing with increasingage.8 Secondary headache associated with neurocysticerco-sis has also been reported.5,9-12 However, most of these re-ports concern presence of headache in patients with neuro-cysticercosis lesions and having either seizures5 or evidenceof raised ICT.9,10 As raised ICT is the second most common

302 February 2007
presentation of NC in India,9,10 headache, without seizuresand/or raised ICT, as the sole presenting manifestation ofSCG has not been reported frequently.4 A community-basedstudy from an endemic-area found that one-third of the mi-graine sufferers undergoing CT examination had evidenceof NC, although no association was found with tension-typeheadache.11
The pathophysiology of the headache in our patient isunclear. As the CT scan showed edema surrounding the en-hancing cyst, the episode may have been due to sudden re-lease of cyst contents and subsequent host inflammatory re-sponse. The episodes could also have been an epileptic event.Although seizure-associated headache is a known entity,12
headache as the sole manifestation of epilepsy is, however,uncommon.4 Possibilities of a vascular origin or a subarach-noid hemorrhage have also previously been proposed butlack of a recurrence, and absence of evidence of SAH onCT, respectively, rules out these possibilities.
Given the high prevalence of NC in India4,10 and thepropensity of NC to remain asymptomatic,1 the possibil-ity of coincident existence of SCG is a distinct possibil-ity. However, there was no recurrence of headache af-ter the resolution of the granuloma thereby pointing tothe SCG as the cause of the headache. It has been pre-viously proposed that patients with headache and SCGdo not require any therapy other than analgesics (al-though 2 of the 15 patients reported received albenda-zole).4 Our patient was treated with cysticidals as per thedepartmental protocol for single ring-enhancing cysticercusgranuloma.
As per American Academy of Neurology recommen-dations, obtaining a neuroimaging study on a routine basisis not indicated in children with recurrent headaches and anormal neurological examination; and neuroimaging shouldbe considered in children in whom there are historical fea-tures to suggest the recent onset of severe headache, changein the type of headache, or if there are associated featuresthat suggest neurologic dysfunction.8 Based on the same andon the basis of published criteria (IHS), we made a clini-cal diagnosis and deferred the neuroimaging for the patient.However, the presence of the SCG on a fortuitous CT studyraises an important point regarding the need for neuroimag-ing in patients with headache in cysticercosis-endemic coun-tries. International League Against Epilepsy recommendsneuroimaging in all seizure patients from endemic countriesprior to labeling idiopathic epilepsy.13 Whether similar rec-ommendations for neuroimaging for patients with headachein cysticercosis-endemic countries are also required is an is-sue worth debating.
In conclusion, we present a child with recent-onset ten-sion type headache and suggest that NC may mimic any typeof primary headache disorder. We propose that in endemiccountries neuroimaging must be considered earlier duringthe evaluation of a pediatric patient with headache.
Conflict of Interest: None
REFERENCES1. Garcia HH, Del Bruto OH. Taenia solium cysticercosis. In-
fect Dis Clin North Amer. 2000;14:97-119.2. Thacker AK, Saxena R, Gupta AK, Sarakari NBS. Disap-
pearing CT lesion in a non-epileptic patient. J Assoc PhysIndia. 1993;41:467-468.
3. University of South Alabama Headache Center. Imagesfrom headache. Tapeworm headache. Headache. 2004;44:374.
4. Rajshekhar V. Severe episodic headache as the sole present-ing ictal event in patients with a solitary cysticercus granu-loma. Acta Neurol Scand. 2000;102:44-46.
5. Garg RK, Kar AM, Singh MK. Prednisolone-responsiveheadache in patients with solitary cysticercus granuloma andseizures. Headache. 2004;44:65-69.
6. Headache Classification Subcommittee of the Interna-tional Headache Society (IHS). International Classifica-tion of Headache Disorders, 2nd edition. Cephalalgia.2004;24(suppl 1):1-160.
7. Rajshekar V. Etiology and management of single CT lesionsin patients with seizures: Understanding a controversy. ActaNeurol Scand. 1991;84:465-470.
8. Lewis DW, Ashwal S, Dahl G, et al. Practice parame-ter: Evaluation of children and adolescents with recurrentheadaches. Report of the Quality Standards Subcommit-tee of the American Academy of Neurology and the Prac-tice Committee of the Child Neurology Society. Neurology.2002;59:490-498.
9. Singhi P, Ray M, Singhi S, Khandelwal N. Clinical spectrumof 500 children with neurocysticercosis and response to al-bendazole therapy. J Child Neurol. 2000;15:207-213.
10. Kalra V, Mittal R, Rana KS, Gupta A. Neurocysticerco-sis: Indian experience. In: Perat MV, ed. New Developmentsin Neurology. Bologna, Italy: Monduzzi Editore S.p.A.;1998:353-359.
11. Cruz ME, Cruz I, Preux PM, Schantz P, Dumas M. Headacheand cysticercosis in Ecuador, South America. Headache.1995;35:93-97.
12. Garg RK, Kar AM. Episodic headache in a non-epileptic patient having disappearing single (ring-enhancing) CT lesion. Neurol India. 1997;45:110-111.
13. Commission on Tropical Diseases of the InternationalLeague Against Epilepsy. Relationship between epilepsyand tropical diseases. Epilepsia. 1994;35:89-93.
Related Documents