© Schattauer 2013 Phlebologie 4/2013 1 Thrombosis of the small saphenous vein E. Mendoza Venenpraxis, Wunstorf Keywords Small saphenous vein, thrombosis, leg pain, duplex ultrasonography Summary Thromboses of the truncal veins are usually very painful. The short saphenous vein, which passes directly over the sural muscles, is par- ticularly painful when walking. These throm- boses can either occur spontaneously or be caused by cramped posture (squatting), im- mobilisation of the leg, or after calf injuries. Thrombosis of the superficial leg veins is par- ticularly dangerous because these usually communicate with the deep veins of the leg via a wide opening which permits the throm- bus to grow into the deep vein of the leg. The differential diagnosis must include a pos- sible complication of treatment of the short saphenous vein such as sclerotherapy or en- doluminal treatment (e.g. Venefit or LASER). Thromboses of superficial leg veins are clas- sically called phlebitis. Use of the term „thrombosis of the superficial vein of the leg“ has been suggested instead of phlebitis to prevent confusion with infectious events. Schlüsselwörter Vena saphena parva, Thrombose, Bein- schmerz, Duplexsonographie Zusammenfassung Thrombosen der Stammvenen sind meist sehr schmerzhaft. Besonders beim Laufen schmerzt die Thrombose der V. saphena par- va, die direkt auf der Wadenmuskulatur auf- liegend verläuft. Diese Thrombosen können spontan auftreten oder motiviert nach Zwangshaltungen (Hocke), Beinruhigstellung oder nach Wadenverletzungen. Von einer Thrombose in oberflächlichen Beinvenen geht eine besondere Gefährdung aus, da die- se meist über eine breite Mündung mit der tiefen Beinvene verbunden sind und hierüber ein Einwachsen des Thrombus in die tiefe Beinvene möglich ist. Differenzialdiagnostisch muss eine Folge nach Behandlung der V. saphena parva erwogen wer- den, wie die Sklerotherapie oder endolumina- len Behandlungen (z.B. Venefit oder LASER). Thrombosen oberflächlicher Beinvenen wur- den klassisch Phlebitis genannt. Um Ver- wechslungen mit infektiösen Vorgängen zu vermeiden, wurde die Verwendung des Be- griffs „Thrombose der oberflächlichen Bein- vene“ statt Phlebitis vorgeschlagen. Correspondence to Dr. Erika Mendoza Venenpraxis Wunstorf Speckenstr. 10, 31515 Wunstorf Thrombose der Vena saphena parva Phlebologie 2013;42: 219–222 DOI: 10.12687/phleb2153-4-2013 Received: June 15,2013 Accepted: June 17,2013 Young Phlebology Case Report A 50-year-old male was referred by his gen- eral practitioner to rule out a thrombosis. History The general history is unremarkable, he is taking no medication, and is otherwise healthy. Previous phlebological findings: Dis- crete reflux in left short saphenous vein, to date no treatment indicated, symptom- free, refilling time after muscle pump over 48 seconds, no skin changes. The acute history reveals: Patient had renovated the parquet flooring in his apart- ment at the weekend. Since Sunday even- ing he had had progressive pain in the calf that had become increasingly worse. He had been wearing compression since the evening before, which gave him some re- lief. Findings Calf relatively unremarkable on inspection, pronounced pain on pressure along the dorsal midline. Ultrasonography Complete occlusion of the small sa- phenous vein extending into the Giacomini vein, the deep veins of the leg are not af- fected (▶ Fig. 1, ▶ Fig. 2, ▶ Fig. 3) (2). Treatment The only medication that is licensed for treatment of superficial thromboses is Fon- daparinux at a dose of 2.5 mg for 6 weeks. However, the guideline recommends thera- peutic anticoagulation if the clot extends until next of the deep veins of the leg. Therefore, Fondaparinux was injected at a therapeutic dosage (7.5 mg for a patient weighing 85 mg) for the first 20 days until the first follow-up ultrasonography. He was also to wear class II compression (a knee sock) during the day and take 400 mg ibu- profen up to three times daily after meals as required. Follow-up after 3 weeks The patient was symptom-free on com- pression and therapeutic anticoagulation. Slight pain on pressure of the calf. Ultraso- nography showed the picture of thrombus to be unchanged. Prescribed treatment was to continue the compression and switch to Arixtra 2.5 mg for a further 3 weeks. Focus on duplex ultrasonography

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

© Schattauer 2013 Phlebologie 4/2013
1
Thrombosis of the small saphenous veinE. MendozaVenenpraxis, Wunstorf
KeywordsSmall saphenous vein, thrombosis, leg pain, duplex ultrasonography
SummaryThromboses of the truncal veins are usually very painful. The short saphenous vein, which passes directly over the sural muscles, is par-ticularly painful when walking. These throm-boses can either occur spontaneously or be caused by cramped posture (squatting), im-mobilisation of the leg, or after calf injuries. Thrombosis of the superficial leg veins is par-ticularly dangerous because these usually communicate with the deep veins of the leg via a wide opening which permits the throm-bus to grow into the deep vein of the leg.The differential diagnosis must include a pos-sible complication of treatment of the short saphenous vein such as sclerotherapy or en-doluminal treatment (e.g. Venefit or LASER).Thromboses of superficial leg veins are clas-sically called phlebitis. Use of the term „thrombosis of the superficial vein of the leg“ has been suggested instead of phlebitis to prevent confusion with infectious events.
SchlüsselwörterVena saphena parva, Thrombose, Bein-schmerz, Duplexsonographie
ZusammenfassungThrombosen der Stammvenen sind meist sehr schmerzhaft. Besonders beim Laufen schmerzt die Thrombose der V. saphena par-va, die direkt auf der Wadenmuskulatur auf-liegend verläuft. Diese Thrombosen können spontan auftreten oder motiviert nach Zwangshaltungen (Hocke), Beinruhigstellung oder nach Wadenverletzungen. Von einer Thrombose in oberflächlichen Beinvenen geht eine besondere Gefährdung aus, da die-se meist über eine breite Mündung mit der tiefen Beinvene verbunden sind und hierüber ein Einwachsen des Thrombus in die tiefe Beinvene möglich ist. Differenzialdiagnostisch muss eine Folge nach Behandlung der V. saphena parva erwogen wer-den, wie die Sklerotherapie oder endolumina-len Behandlungen (z.B. Venefit oder LASER). Thrombosen oberflächlicher Beinvenen wur-den klassisch Phlebitis genannt. Um Ver-wechslungen mit infektiösen Vorgängen zu vermeiden, wurde die Verwendung des Be-griffs „Thrombose der oberflächlichen Bein-vene“ statt Phlebitis vorgeschlagen.
Correspondence toDr. Erika Mendoza Venenpraxis Wunstorf Speckenstr. 10, 31515 Wunstorf
Thrombose der Vena saphena parvaPhlebologie 2013;42: 219–222DOI: 10.12687/phleb2153-4-2013Received: June 15,2013Accepted: June 17,2013
Youn
g Ph
lebo
logy
Case Report
A 50-year-old male was referred by his gen-eral practitioner to rule out a thrombosis.
History
The general history is unremarkable, he is taking no medication, and is otherwise healthy.
Previous phlebological findings: Dis-crete reflux in left short saphenous vein, to date no treatment indicated, symptom-free, refilling time after muscle pump over 48 seconds, no skin changes.
The acute history reveals: Patient had renovated the parquet flooring in his apart-ment at the weekend. Since Sunday even-ing he had had progressive pain in the calf
that had become increasingly worse. He had been wearing compression since the evening before, which gave him some re-lief.
Findings
Calf relatively unremarkable on inspection, pronounced pain on pressure along the dorsal midline.
Ultrasonography
Complete occlusion of the small sa-phenous vein extending into the Giacomini vein, the deep veins of the leg are not af-fected (▶ Fig. 1, ▶ Fig. 2, ▶ Fig. 3) (2).
Treatment
The only medication that is licensed for treatment of superficial thromboses is Fon-daparinux at a dose of 2.5 mg for 6 weeks. However, the guideline recommends thera-peutic anticoagulation if the clot extends until next of the deep veins of the leg. Therefore, Fondaparinux was injected at a therapeutic dosage (7.5 mg for a patient weighing 85 mg) for the first 20 days until the first follow-up ultrasonography. He was also to wear class II compression (a knee sock) during the day and take 400 mg ibu-profen up to three times daily after meals as required.
Follow-up after 3 weeks
The patient was symptom-free on com-pression and therapeutic anticoagulation. Slight pain on pressure of the calf. Ultraso-nography showed the picture of thrombus to be unchanged. Prescribed treatment was to continue the compression and switch to Arixtra 2.5 mg for a further 3 weeks.
Focus on duplex ultrasonography
Phlebologie 4/2013 © Schattauer 2013
2
Youn
g Ph
lebo
logy
E. Mendoza: Thrombosis of the small saphenous vein
CommentsThrombosis of the superficial veins is no longer called phlebitis (1) in order to avoid the misleading suffix „itis“ which suggests an infection. In fact, „venous inflam-mation“ has often been, and frequently continues to be, treated with antibiotics for further diagnostic investigations and treat-ment in phlebological practices.
The clinical picture after treatment of the short saphenous vein by sclerotherapy (▶ Fig. 4) (3) or endoluminal procedures (▶ Fig. 5) is similar to thrombosis of the short saphenous vein.
Spread of the clot into the deep veins of the leg, be it by spontaneous thrombosis or as a result of treatment as in Figures 4 and 5, must be sought and ruled out – in this case treatment according to the guidelines for treatment of deep vein thrombosis would be given.
Focus on duplex ultrasonography
Abbb.. 1::
Abbb.. 2
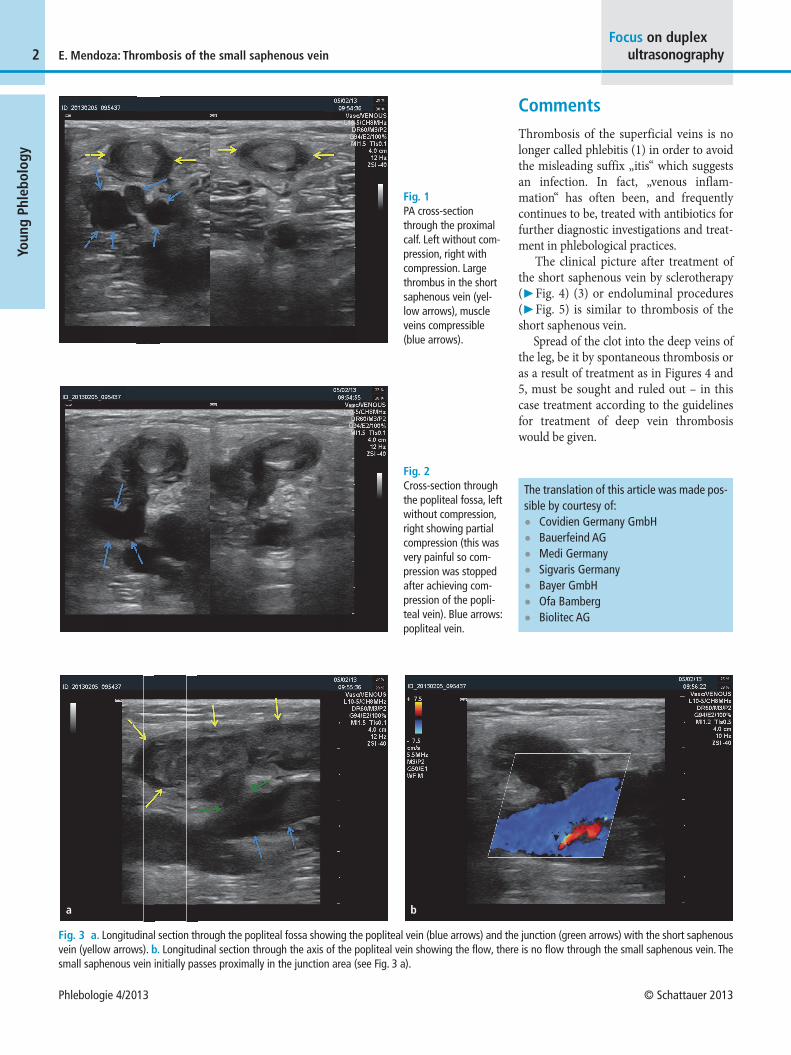
Fig. 1 PA cross-section through the proximal calf. Left without com-pression, right with compression. Large thrombus in the short saphenous vein (yel-low arrows), muscle veins compressible (blue arrows).
Fig. 2 Cross-section through the popliteal fossa, left without compression, right showing partial compression (this was very painful so com-pression was stopped after achieving com-pression of the popli-teal vein). Blue arrows: popliteal vein.
Fig. 3 a. Longitudinal section through the popliteal fossa showing the popliteal vein (blue arrows) and the junction (green arrows) with the short saphenous vein (yellow arrows). b. Longitudinal section through the axis of the popliteal vein showing the flow, there is no flow through the small saphenous vein. The small saphenous vein initially passes proximally in the junction area (see Fig. 3 a).
Abbb.. 3aa3b
a b
The translation of this article was made pos-sible by courtesy of: • Covidien Germany GmbH• Bauerfeind AG • Medi Germany• Sigvaris Germany• Bayer GmbH• Ofa Bamberg• Biolitec AG
© Schattauer 2013 Phlebologie 4/2013
3
Youn
g Ph
lebo
logy
E. Mendoza: Thrombosis of the small saphenous veinFocus on duplex
ultrasonographyAbbb.. 4aa) 4b)
4cc)a b
c
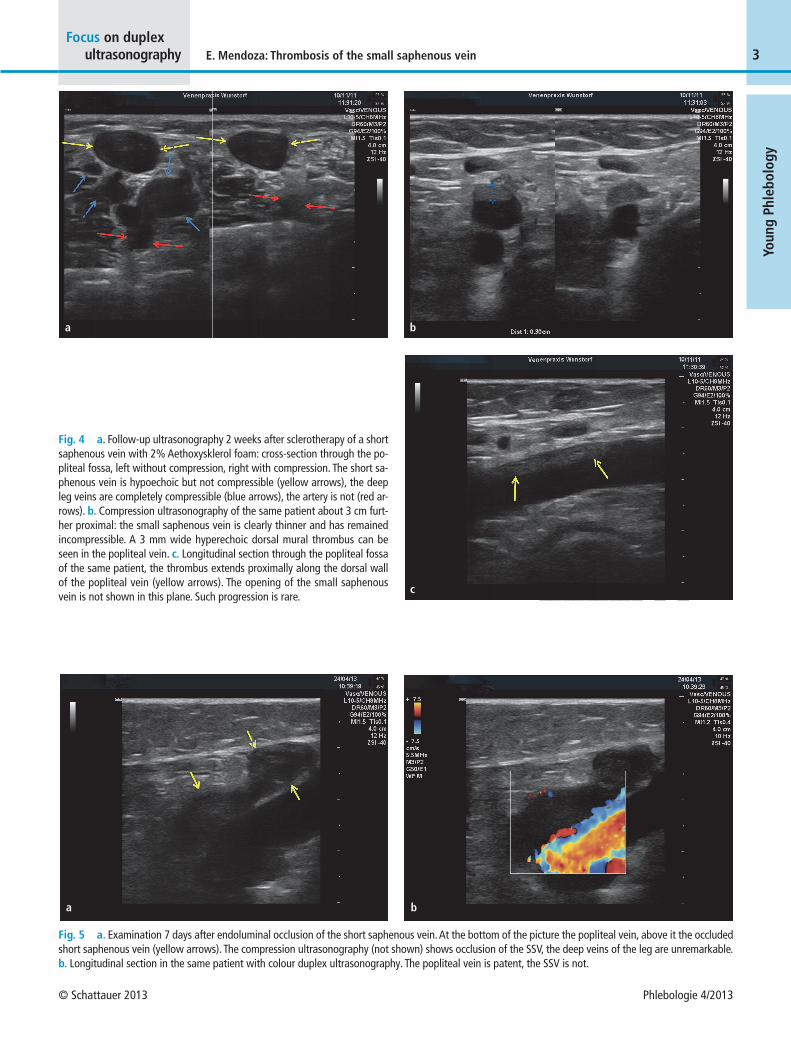
Fig. 4 a. Follow-up ultrasonography 2 weeks after sclerotherapy of a short saphenous vein with 2% Aethoxysklerol foam: cross-section through the po-pliteal fossa, left without compression, right with compression. The short sa-phenous vein is hypoechoic but not compressible (yellow arrows), the deep leg veins are completely compressible (blue arrows), the artery is not (red ar-rows). b. Compression ultrasonography of the same patient about 3 cm furt-her proximal: the small saphenous vein is clearly thinner and has remained incompressible. A 3 mm wide hyperechoic dorsal mural thrombus can be seen in the popliteal vein. c. Longitudinal section through the popliteal fossa of the same patient, the thrombus extends proximally along the dorsal wall of the popliteal vein (yellow arrows). The opening of the small saphenous vein is not shown in this plane. Such progression is rare.
Abbb.. 5aa 5b)
a b
Fig. 5 a. Examination 7 days after endoluminal occlusion of the short saphenous vein. At the bottom of the picture the popliteal vein, above it the occluded short saphenous vein (yellow arrows). The compression ultrasonography (not shown) shows occlusion of the SSV, the deep veins of the leg are unremarkable. b. Longitudinal section in the same patient with colour duplex ultrasonography. The popliteal vein is patent, the SSV is not.

Phlebologie 4/2013 © Schattauer 2013
4
Youn
g Ph
lebo
logy
E. Mendoza: Thrombosis of the small saphenous vein
References1. Kalodiki E, Strvrtinova V, Allegra C, Andreozzi
GM, Antignani PL, Avram R, Brkljacic B, Cada-riou F, Dzsinich C, Fareed J, Gaspar L, Geroulakos
G, Javien A, Kozak M, Lattimer CR, Minar E, Partsch H, Passariello F, Patel M, Pécsvárady Z, Poredos P, Rotocil K, Scuderi A, Sparovec M, Szos-tek M, Skorski M. Superficial vein thrombosis: a consensus statement. Int Angiol 2012; 31: 203–216.
2. Hartmann K. Duplexsonographie bei Thrombose. Phlebologie 2012, 41: 412–314.
3. Reich-Schupke S, Stücker M. Foam Sclerotherapy. Phlebologie 2013; 42: 31–36.
Focus on duplex ultrasonography
Related Documents











