Thrombocytopenia Thrombocytopenia Dr S W Bokhari Dr S W Bokhari Consultant Haematologist Consultant Haematologist University Hospital Coventry and University Hospital Coventry and Warwickshire Warwickshire

Thrombocytopenia Dr S W Bokhari Consultant Haematologist
Jan 01, 2016
Thrombocytopenia Dr S W Bokhari Consultant Haematologist University Hospital Coventry and Warwickshire. Thrombocytopenia. You are the Surgical HO asked to clerk patient on ward pre-operatively prior to hernia repair. - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ThrombocytopeniaThrombocytopenia
Dr S W BokhariDr S W Bokhari
Consultant HaematologistConsultant Haematologist
University Hospital Coventry and University Hospital Coventry and WarwickshireWarwickshire

ThrombocytopeniaThrombocytopenia
You are the Surgical HO asked to clerk patient on You are the Surgical HO asked to clerk patient on ward pre-operatively prior to hernia repair.ward pre-operatively prior to hernia repair.
You notice from results on CRRS that his platelet You notice from results on CRRS that his platelet count one week earlier was 25. No previous results.count one week earlier was 25. No previous results.
How do you approach this problem?How do you approach this problem?

Repeat FBCRepeat FBC
Hb 13g/dL WCC 8 Neuts 2.5 Plts 28 MCV 102Hb 13g/dL WCC 8 Neuts 2.5 Plts 28 MCV 102
Ask for blood film to be reviewedAsk for blood film to be reviewed
Film commentFilm comment – confirmed thrombocytopenia, – confirmed thrombocytopenia, normalnormal
platelet morphology; mild macrocytosis; no other platelet morphology; mild macrocytosis; no other abnormalabnormal
featuresfeatures
Inform surgeons/theatres etcInform surgeons/theatres etc
Peripheral blood filmPeripheral blood film
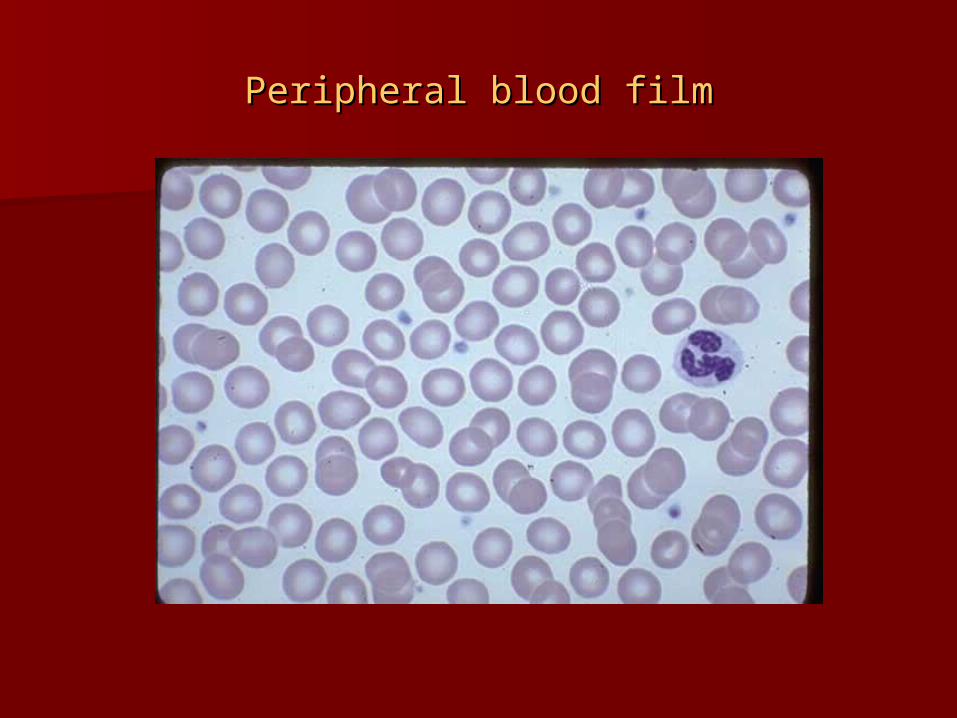
Platelet clumpingPlatelet clumping

HistoryHistory
40 year old man40 year old man
Symptoms:Symptoms:
Bleeding history – severity and durationBleeding history – severity and duration
Recent illness – including infections esp. viralRecent illness – including infections esp. viral
Patient had noticed easy bruising for previous 2 Patient had noticed easy bruising for previous 2 months.months.
Fit and well with no recent illnessFit and well with no recent illness

Mucosal bleeding

Purpura

Past Medical HistoryPast Medical History
Infections – bacterial, viral, fungalInfections – bacterial, viral, fungal Autoimmune diseaseAutoimmune disease Liver diseaseLiver disease MalignancyMalignancy
Occasional backpainOccasional backpain
Road traffic accident 5 years ago following which heRoad traffic accident 5 years ago following which he
received blood transfusionreceived blood transfusion

Family HistoryFamily History
Congenital causes of thrombocytopeniaCongenital causes of thrombocytopenia Autoimmune diseaseAutoimmune disease
Mother – IDDMMother – IDDM
Sister recently diagnosed with SLESister recently diagnosed with SLE

Drug HistoryDrug History
Long list to consider!Long list to consider!
-immune-mediated-immune-mediated
-direct effect on BM or MK-direct effect on BM or MK
Alcohol intakeAlcohol intake
Takes diclofenac for backpainTakes diclofenac for backpain
30 units alcohol per week – spirits30 units alcohol per week – spirits
Smokes 15/daySmokes 15/day
Social HistorySocial History
Occupation - ? Exposure to toxic agentsOccupation - ? Exposure to toxic agents Dietary historyDietary history Recent travel abroad – infectionsRecent travel abroad – infections Risk factors for HIVRisk factors for HIV
Recently made redundant having previously worked Recently made redundant having previously worked inin
motor industrymotor industry
No recent travel abroadNo recent travel abroad
No risk factors for HIVNo risk factors for HIV
ExaminationExamination
Bleeding/bruisingBleeding/bruising AnaemiaAnaemia Clubbing/jaundice (other features of CLD)Clubbing/jaundice (other features of CLD) LymphadenopathyLymphadenopathy Signs of malignancySigns of malignancy HepatomegalyHepatomegaly SplenomegalySplenomegaly
Features associated with congenital causes esp. Features associated with congenital causes esp. FanconiFanconi
anaemiaanaemia

Bruising over arms and legsBruising over arms and legs
? Yellow sclera? Yellow sclera
Liver palpable 3cmLiver palpable 3cm
No other findingsNo other findings

InvestigationsInvestigations
FBCFBC
Pancytopenia or isolated thrombocytopeniaPancytopenia or isolated thrombocytopenia
MCVMCV
Blood filmBlood film
Confirm thrombocytopeniaConfirm thrombocytopenia
Platelet size and morphologyPlatelet size and morphology
Red cell fragmentsRed cell fragments
Red cell abnormalities e.g. target cellsRed cell abnormalities e.g. target cells
WBC featuresWBC features
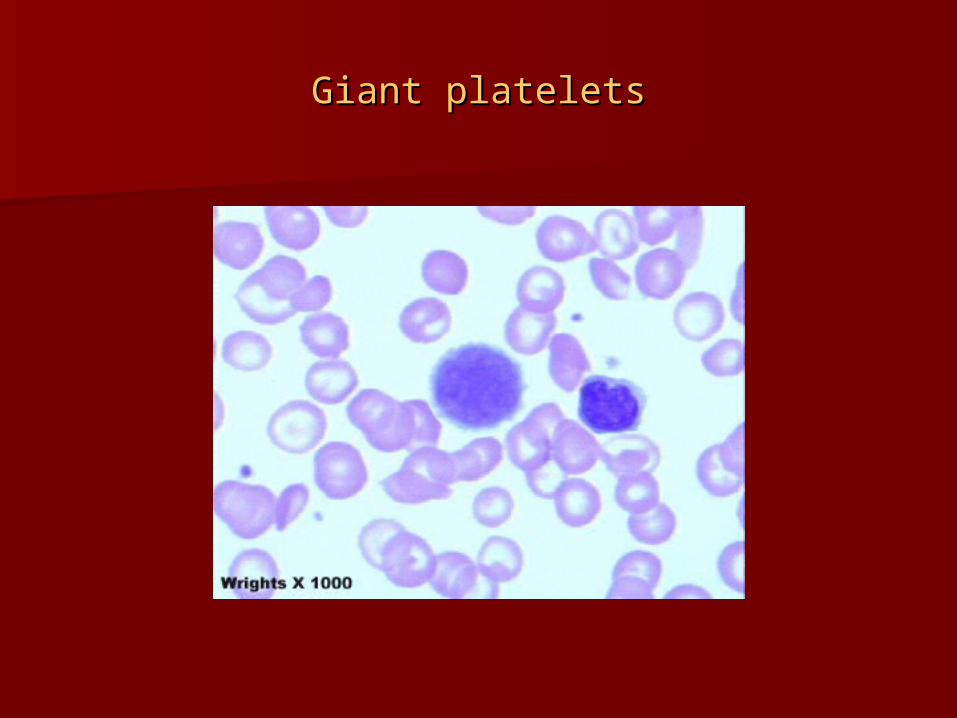
Giant plateletsGiant platelets

Red cell fragmentsRed cell fragments

Target cellsTarget cells

Hypersegmented neutrophilHypersegmented neutrophil

Hb 13g/dL WCC 5 Neuts 2.0 Plts 28 MCV 102Hb 13g/dL WCC 5 Neuts 2.0 Plts 28 MCV 102
Target cells and stomatocytesTarget cells and stomatocytes

Renal functionRenal function Liver functionLiver function
B12 and folateB12 and folate
Full clotting screenFull clotting screen
Normal renal functionNormal renal function
AST 160 Alk phos 170 ALT 130 Bili 60 AST 160 Alk phos 170 ALT 130 Bili 60 γγGT 100GT 100
B12 110 Folate 1.4B12 110 Folate 1.4
PT ratio 1.6 APTT ratio 1.4 Normal fibrinogen and TTPT ratio 1.6 APTT ratio 1.4 Normal fibrinogen and TT

Autoantibody screen + specific autoantibodies as Autoantibody screen + specific autoantibodies as indicatedindicated
Antiphospholipid antibodiesAntiphospholipid antibodies
Lupus anticoagulantLupus anticoagulant
Anticardiolipin antibodiesAnticardiolipin antibodies
Autoantibodies screen negativeAutoantibodies screen negative
Antiphospholipid antibodies positiveAntiphospholipid antibodies positive

Virology testingVirology testing
EBV, CMV, toxoplasmaEBV, CMV, toxoplasma
Hep B, CHep B, C
HIVHIV
Hepatitis C positiveHepatitis C positive
Presumed secondary to blood transfusionPresumed secondary to blood transfusion

Causes of thrombocytopeniaCauses of thrombocytopenia
Failure of productionFailure of production
Increased consumption/destructionIncreased consumption/destruction
Abnormal pooling - splenomegalyAbnormal pooling - splenomegaly

Failure of productionFailure of production
Congenital:Congenital:
Fanconi anaemia, TAR (thrombocytopenia with absentFanconi anaemia, TAR (thrombocytopenia with absent
radii), Wiskott-Aldrich syndrome, Bernard-Soulier radii), Wiskott-Aldrich syndrome, Bernard-Soulier synd.*,synd.*,
May-Hegglin anomaly*, Alport synd. variant*, Grey May-Hegglin anomaly*, Alport synd. variant*, Grey plateletplatelet
synd.*synd.*
Acquired:Acquired: – specific thrombocytopenia – specific thrombocytopenia
Infection esp. viral Infection esp. viral
Nutritional deficiency – B12/folateNutritional deficiency – B12/folate
Toxic effect of drugs (more often immune) or alcoholToxic effect of drugs (more often immune) or alcohol

Failure of productionFailure of production
Acquired: Acquired: – as part of bone marrow failure– as part of bone marrow failure
Drugs including chemotherapyDrugs including chemotherapy
RadiotherapyRadiotherapy
Marrow infiltration – malignant/non-malignantMarrow infiltration – malignant/non-malignant
Aplastic anaemiaAplastic anaemia

Bone marrow aspirateBone marrow aspirate

Bone marrow trephineBone marrow trephine

Increased destruction of plateletsIncreased destruction of platelets
ImmuneImmune
Idiopathic: Idiopathic:
ITP (acute and chronic)ITP (acute and chronic)
Secondary:Secondary:
Autoimmune disease e.g. SLEAutoimmune disease e.g. SLE
Infections e.g. HIV, Hepatitis CInfections e.g. HIV, Hepatitis C
Drugs e.g. heparin (HIT), quinine, quinidine, Drugs e.g. heparin (HIT), quinine, quinidine, gold gold saltssalts
Lymphoproliferative disease e.g. CLLLymphoproliferative disease e.g. CLL
Neonatal alloimmune thrombocytopeniaNeonatal alloimmune thrombocytopenia
Post-transfusion purpuraPost-transfusion purpura

Increased destruction of plateletsIncreased destruction of platelets
Non-immuneNon-immune
Microangiopathic haemolytic anaemia (MAHA)Microangiopathic haemolytic anaemia (MAHA)
DICDIC
HUSHUS
TTP – idiopathic or 2TTP – idiopathic or 2º e.g. pregnancy, º e.g. pregnancy, infection, infection, metastatic carcinoma, drugs, BMT, AI metastatic carcinoma, drugs, BMT, AI diseasedisease
Pregnancy relatedPregnancy related
Gestational thrombocytopeniaGestational thrombocytopenia
PreeclampsiaPreeclampsia
HELLPHELLP

ManagementManagement
Few spontaneous bleeding problems if plts > 30Few spontaneous bleeding problems if plts > 30
Unless:Unless:
Abnormal platelet functionAbnormal platelet function
Associated coagulopathyAssociated coagulopathy
In general patients need treatment if In general patients need treatment if symptomatic or increased risk of bleeding e.g. symptomatic or increased risk of bleeding e.g. peri/post-operatively, trauma, obstetricperi/post-operatively, trauma, obstetric
In general would want platelets > 50 for minor op In general would want platelets > 50 for minor op and >80/100 for major op. and >80/100 for major op.
May need to transfuse plts if count higher but May need to transfuse plts if count higher but abnormal functionabnormal function

ManagementManagement
May need bone marrow to determine whether May need bone marrow to determine whether cause of thrombocytopenia is failure of cause of thrombocytopenia is failure of production or increased destructionproduction or increased destruction
Stop any possible implicated drugsStop any possible implicated drugs
In general if failure of production:In general if failure of production:
Platelet transfusionsPlatelet transfusions
Treat underlying cause e.g. B12/folate Treat underlying cause e.g. B12/folate replacementreplacement

ManagementManagement
In general if increased destruction:In general if increased destruction:
Avoid platelet transfusions as these are often Avoid platelet transfusions as these are often ineffective and can make clinical situation worse ineffective and can make clinical situation worse e.g. TTP, HITe.g. TTP, HIT
Exception - DICException - DIC
May be required if life-threatening bleeding e.g. ITPMay be required if life-threatening bleeding e.g. ITP
Treat underlying cause e.g. CLLTreat underlying cause e.g. CLL
ITP:ITP:
Immunosuppression – steroids, IVIG, other Immunosuppression – steroids, IVIG, other immunosuppressive agentsimmunosuppressive agents
SplenectomySplenectomy

ManagementManagement
TTP-HUS may require plasma exchange/FFPTTP-HUS may require plasma exchange/FFP
NAIT/PTP may require HPA1NAIT/PTP may require HPA1A A neg pltsneg plts
Related Documents