European Journal of Radiology 81 (2012) 2794–2800 Contents lists available at SciVerse ScienceDirect European Journal of Radiology journa l h o me pa ge: www.elsevier.com/locate/ejrad Three-dimensional volume rendering digital subtraction angiography in comparison with two-dimensional digital subtraction angiography and rotational angiography for detecting aneurysms and their morphological properties in patients with subarachnoid hemorrhage Fahrettin Kucukay a,∗ , R. Sarper Okten a , Ayhan Tekiner b , Mustafa Dagli a , Cevdet Gocek b , Mehmet Akif Bayar b , Turhan Cumhur a a Turkiye Yuksek Ihtisas Hospital, Department of Radiology, Ankara, Turkey b Ankara Education and Teaching Hospital, Department of Neurosurgery, Ankara, Turkey a r t i c l e i n f o Article history: Received 8 September 2011 Accepted 14 October 2011 Keywords: Intracranial aneurysm Rupture Cerebral angiography Digital subtraction angiography Three-dimensional imaging a b s t r a c t Objective: Subarachnoid hemorrhage (SAH), which can cause mortality and severe morbidity, is a serious condition whose underlying cause must be determined. We aimed to compare 2D digital subtrac- tion angiography (2DDSA), rotational angiography (RA) and 3D volume rendering digital subtraction angiography (3DVRDSA) for detecting aneurysms and their morphological properties in patients with subarachnoid hemorrhage. Materials and methods: After an initial diagnosis of SAH with computed tomography, 122 patients (52 males and 70 females with a mean age of 47.77 ± 12.81 ranging between 20 and 83 years) underwent 2DDSA imaging, RA and 3DVRDSA imaging for detection of aneurysms. The location of the aneurysm, the best working angles, the dome/neck ratios, the largest diameter of the aneurysm, the shape of the aneurysm, the presence of spasms or pseudostenoses, and the relationship to the neighboring arteries were recorded. Results: 2DDSA missed 15.6% of the aneurysms that had a mean size of 2.79 ± 0.74 mm. RA was superior to 2DDSA for detecting aneurysm neck, and 3DVRDSA was superior to RA for detecting aneurysm neck. 3DVRDSA conclusively depicted the shape of the aneurysms in all patients. 3DVRDSA imaging was supe- rior to 2DDSA and RA in the detection of the aneurysm relationship to neighboring arteries. The sensitivity and specificity of 3DVRDSA imaging for the detection of vasospasms were 100 and 84%, respectively. Conclusions: 3DVRDSA imaging is superior to 2DDSA and RA for detecting intracranial aneurysms and their morphological properties, especially those of small, ruptured aneurysms. However, 2DDSA should not be neglected in cases of vasospasm. © 2011 Elsevier Ireland Ltd. All rights reserved. 1. Introduction Subarachnoid hemorrhage (SAH) is an emergent condition with case-fatality rates that vary between 8.3% and 66.7% in different studies [1]. The risk of sudden death before reaching a hospital is 12.4% [2]. In patients with subarachnoid hemorrhages, the under- lying cause remains to be determined. Aneurysms are the cause of subarachnoid hemorrhage in 85% of cases [3]. For this reason, a ∗ Corresponding author at: Turkiye Yuksek Ihtisas Hospital, Department of Radi- ology, Kizilay sokak No. 4, 06100 Sihhiye, Ankara, Turkey. Tel.: +90 3123061619; fax: +90 3123124120. E-mail address: [email protected] (F. Kucukay). detailed examination with diagnostic imaging modalities to detect intracranial aneurysms is necessary. Two-dimensional digital subtraction angiography (2DDSA) is accepted as the gold standard imaging technique for the diag- nosis of intracranial aneurysms [4–10]. However, detecting small aneurysms that can also rupture and restrictions in identifying the morphological properties of aneurysms (location, neck, shape, and the relationship to the neighboring artery) are limitations of 2DDSA. Rotational angiography (RA) and three-dimensional digital subtraction imaging (3DDSA) are advantageous not only because they detect small aneurysms and identify morphologi- cal properties of intracranial aneurysms but also because they reduce the radiation dose, reduce the contrast volume that needs to be injected, and have a shorter procedure time [4–12]. There are a number of reports related to this topic, but few have 0720-048X/$ – see front matter © 2011 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ejrad.2011.10.006

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Tcrp
FMa
b
a
ARA
KIRCDT
1
cs1lo
of
0d
European Journal of Radiology 81 (2012) 2794– 2800
Contents lists available at SciVerse ScienceDirect
European Journal of Radiology
journa l h o me pa ge: www.elsev ier .com/ locate /e j rad
hree-dimensional volume rendering digital subtraction angiography inomparison with two-dimensional digital subtraction angiography andotational angiography for detecting aneurysms and their morphologicalroperties in patients with subarachnoid hemorrhage
ahrettin Kucukaya,∗, R. Sarper Oktena, Ayhan Tekinerb, Mustafa Dagli a, Cevdet Gocekb,ehmet Akif Bayarb, Turhan Cumhura
Turkiye Yuksek Ihtisas Hospital, Department of Radiology, Ankara, TurkeyAnkara Education and Teaching Hospital, Department of Neurosurgery, Ankara, Turkey
r t i c l e i n f o
rticle history:eceived 8 September 2011ccepted 14 October 2011
eywords:ntracranial aneurysmuptureerebral angiographyigital subtraction angiographyhree-dimensional imaging
a b s t r a c t
Objective: Subarachnoid hemorrhage (SAH), which can cause mortality and severe morbidity, is a seriouscondition whose underlying cause must be determined. We aimed to compare 2D digital subtrac-tion angiography (2DDSA), rotational angiography (RA) and 3D volume rendering digital subtractionangiography (3DVRDSA) for detecting aneurysms and their morphological properties in patients withsubarachnoid hemorrhage.Materials and methods: After an initial diagnosis of SAH with computed tomography, 122 patients (52males and 70 females with a mean age of 47.77 ± 12.81 ranging between 20 and 83 years) underwent2DDSA imaging, RA and 3DVRDSA imaging for detection of aneurysms. The location of the aneurysm,the best working angles, the dome/neck ratios, the largest diameter of the aneurysm, the shape of theaneurysm, the presence of spasms or pseudostenoses, and the relationship to the neighboring arterieswere recorded.Results: 2DDSA missed 15.6% of the aneurysms that had a mean size of 2.79 ± 0.74 mm. RA was superiorto 2DDSA for detecting aneurysm neck, and 3DVRDSA was superior to RA for detecting aneurysm neck.
3DVRDSA conclusively depicted the shape of the aneurysms in all patients. 3DVRDSA imaging was supe-rior to 2DDSA and RA in the detection of the aneurysm relationship to neighboring arteries. The sensitivityand specificity of 3DVRDSA imaging for the detection of vasospasms were 100 and 84%, respectively.Conclusions: 3DVRDSA imaging is superior to 2DDSA and RA for detecting intracranial aneurysms andtheir morphological properties, especially those of small, ruptured aneurysms. However, 2DDSA shouldnot be neglected in cases of vasospasm.© 2011 Elsevier Ireland Ltd. All rights reserved.
. Introduction
Subarachnoid hemorrhage (SAH) is an emergent condition withase-fatality rates that vary between 8.3% and 66.7% in differenttudies [1]. The risk of sudden death before reaching a hospital is2.4% [2]. In patients with subarachnoid hemorrhages, the under-
ying cause remains to be determined. Aneurysms are the causef subarachnoid hemorrhage in 85% of cases [3]. For this reason, a
∗ Corresponding author at: Turkiye Yuksek Ihtisas Hospital, Department of Radi-logy, Kizilay sokak No. 4, 06100 Sihhiye, Ankara, Turkey. Tel.: +90 3123061619;ax: +90 3123124120.
E-mail address: [email protected] (F. Kucukay).
720-048X/$ – see front matter © 2011 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.ejrad.2011.10.006
detailed examination with diagnostic imaging modalities to detectintracranial aneurysms is necessary.
Two-dimensional digital subtraction angiography (2DDSA) isaccepted as the gold standard imaging technique for the diag-nosis of intracranial aneurysms [4–10]. However, detecting smallaneurysms that can also rupture and restrictions in identifyingthe morphological properties of aneurysms (location, neck, shape,and the relationship to the neighboring artery) are limitationsof 2DDSA. Rotational angiography (RA) and three-dimensionaldigital subtraction imaging (3DDSA) are advantageous not onlybecause they detect small aneurysms and identify morphologi-
cal properties of intracranial aneurysms but also because theyreduce the radiation dose, reduce the contrast volume that needsto be injected, and have a shorter procedure time [4–12]. Thereare a number of reports related to this topic, but few have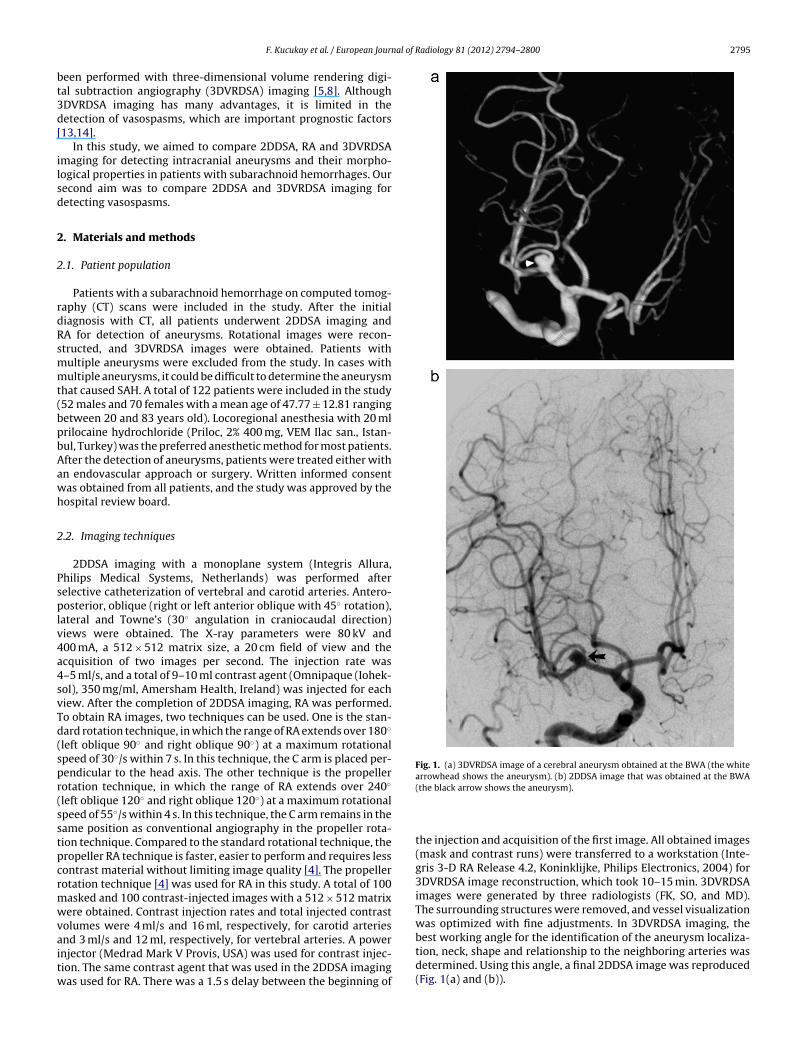
nal of Radiology 81 (2012) 2794– 2800 2795
bt3d[
ilsd
2
2
rdRsmmt(bpbAawh
2
Psplv4a4svTd(spr(sstpcrmwvaitw
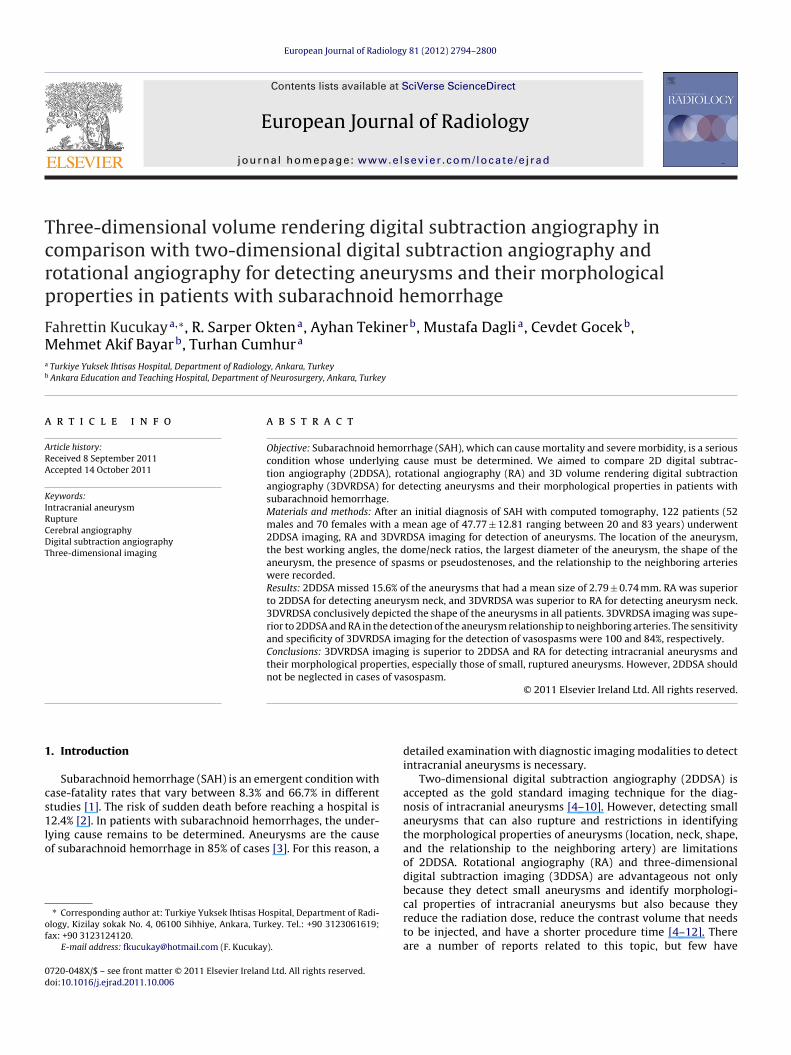
Fig. 1. (a) 3DVRDSA image of a cerebral aneurysm obtained at the BWA (the whitearrowhead shows the aneurysm). (b) 2DDSA image that was obtained at the BWA
F. Kucukay et al. / European Jour
een performed with three-dimensional volume rendering digi-al subtraction angiography (3DVRDSA) imaging [5,8]. AlthoughDVRDSA imaging has many advantages, it is limited in theetection of vasospasms, which are important prognostic factors13,14].
In this study, we aimed to compare 2DDSA, RA and 3DVRDSAmaging for detecting intracranial aneurysms and their morpho-ogical properties in patients with subarachnoid hemorrhages. Ourecond aim was to compare 2DDSA and 3DVRDSA imaging foretecting vasospasms.
. Materials and methods
.1. Patient population
Patients with a subarachnoid hemorrhage on computed tomog-aphy (CT) scans were included in the study. After the initialiagnosis with CT, all patients underwent 2DDSA imaging andA for detection of aneurysms. Rotational images were recon-tructed, and 3DVRDSA images were obtained. Patients withultiple aneurysms were excluded from the study. In cases withultiple aneurysms, it could be difficult to determine the aneurysm
hat caused SAH. A total of 122 patients were included in the study52 males and 70 females with a mean age of 47.77 ± 12.81 rangingetween 20 and 83 years old). Locoregional anesthesia with 20 mlrilocaine hydrochloride (Priloc, 2% 400 mg, VEM Ilac san., Istan-ul, Turkey) was the preferred anesthetic method for most patients.fter the detection of aneurysms, patients were treated either withn endovascular approach or surgery. Written informed consentas obtained from all patients, and the study was approved by theospital review board.
.2. Imaging techniques
2DDSA imaging with a monoplane system (Integris Allura,hilips Medical Systems, Netherlands) was performed afterelective catheterization of vertebral and carotid arteries. Antero-osterior, oblique (right or left anterior oblique with 45◦ rotation),
ateral and Towne’s (30◦ angulation in craniocaudal direction)iews were obtained. The X-ray parameters were 80 kV and00 mA, a 512 × 512 matrix size, a 20 cm field of view and thecquisition of two images per second. The injection rate was–5 ml/s, and a total of 9–10 ml contrast agent (Omnipaque (Iohek-ol), 350 mg/ml, Amersham Health, Ireland) was injected for eachiew. After the completion of 2DDSA imaging, RA was performed.o obtain RA images, two techniques can be used. One is the stan-ard rotation technique, in which the range of RA extends over 180◦
left oblique 90◦ and right oblique 90◦) at a maximum rotationalpeed of 30◦/s within 7 s. In this technique, the C arm is placed per-endicular to the head axis. The other technique is the propellerotation technique, in which the range of RA extends over 240◦
left oblique 120◦ and right oblique 120◦) at a maximum rotationalpeed of 55◦/s within 4 s. In this technique, the C arm remains in theame position as conventional angiography in the propeller rota-ion technique. Compared to the standard rotational technique, theropeller RA technique is faster, easier to perform and requires lessontrast material without limiting image quality [4]. The propellerotation technique [4] was used for RA in this study. A total of 100asked and 100 contrast-injected images with a 512 × 512 matrixere obtained. Contrast injection rates and total injected contrast
olumes were 4 ml/s and 16 ml, respectively, for carotid arteries
nd 3 ml/s and 12 ml, respectively, for vertebral arteries. A powernjector (Medrad Mark V Provis, USA) was used for contrast injec-ion. The same contrast agent that was used in the 2DDSA imagingas used for RA. There was a 1.5 s delay between the beginning of(the black arrow shows the aneurysm).
the injection and acquisition of the first image. All obtained images(mask and contrast runs) were transferred to a workstation (Inte-gris 3-D RA Release 4.2, Koninklijke, Philips Electronics, 2004) for3DVRDSA image reconstruction, which took 10–15 min. 3DVRDSAimages were generated by three radiologists (FK, SO, and MD).The surrounding structures were removed, and vessel visualizationwas optimized with fine adjustments. In 3DVRDSA imaging, thebest working angle for the identification of the aneurysm localiza-tion, neck, shape and relationship to the neighboring arteries was
determined. Using this angle, a final 2DDSA image was reproduced(Fig. 1(a) and (b)).
2796 F. Kucukay et al. / European Journal of
Table 1Categorical variables used for comparison.
Age Years oldGender Male or femaleAneurysm localization Group 1 to group 12Best working angle Type 1 to Type 8Dome/neck ratio Narrow necked, wide neckedThe longest diameter of the
aneurysm<3 mm, 3–10 mm, >10 mm
The shape of the aneurysm Lobulated or roundPresence of spasm Yes or noRelationship to the
neighboring arteryYes or no
Visibility of aneurysm details2DDSA
Neck 1 = conclusive, 2 = ambiguous, 3 = insufficientLocation 1 = conclusive, 2 = ambiguous, 3 = insufficientShape 1 = conclusive, 2 = ambiguous, 3 = insufficientRelationship to the
neighboring artery1 = conclusive, 2 = ambiguous, 3 = insufficient
RANeck 1 = conclusive, 2 = ambiguous, 3 = insufficientLocation 1 = conclusive, 2 = ambiguous, 3 = insufficientShape 1 = conclusive, 2 = ambiguous, 3 = insufficientRelationship to the
neighboring artery1 = conclusive, 2 = ambiguous, 3 = insufficient
3DVRDSANeck 1 = conclusive, 2 = ambiguous, 3 = insufficientLocation 1 = conclusive, 2 = ambiguous, 3 = insufficientShape 1 = conclusive, 2 = ambiguous, 3 = insufficientRelationship to the
neighboring artery1 = conclusive, 2 = ambiguous, 3 = insufficient
23
2
tidot2fptt(
taiwitp
a1wa
3(
Ga
R
A total of 75.8% (25 of 33) of the aneurysms that had the largest
DDSA = 2D digital subtraction angiography; RA = rotational angiography;DVRDSA = 3D volume rendering digital subtraction angiography.
.3. Image interpretation
All images were evaluated by three radiologists (FK, SO, and MD)o reach a consensus. Consensus was achieved while reading themages. The location of the aneurysms, the best working angles, theome/neck ratios, the largest diameter of the aneurysms, the shapef the aneurysms, the presence of a spasm or of pseudostenoses, andhe relationship to the neighboring arteries were recorded from theDDSA, RA and 3DVRDSA images. The 2DDSA images were analyzedrom anteroposterior, −45◦ or +45◦ oblique, ipsilateral and Towne’srojections. There were no differences in measuring or calculatinghe size and ratios between the 2DDSA, RA and 3DVRDSA imagingechniques. Aneurysm locations were categorized into 12 groupsTable 1).
The best working angle is defined as the angle that the neck ofhe aneurysm, relationship to the neighboring arteries and arteriesrising from the aneurismal sac are best seen. The best work-ng angles were categorized into 8 types. Craniocaudal projections
ere unable to give angulations more than −45◦ to 45◦ in 2DDSAmaging in 4% of the aneurysms (5 of 122). Therefore, reanalysis ofhe best working angles within the limits of monoplane angiogra-hy system were performed.
Dome/neck ratios were calculated. Based on this ratio, theneurysms that had a dome/neck ratio equal to or greater than
were classified as narrow-necked aneurysms, and if this ratioas below 1, then the aneurysms were classified as wide-necked
neurysms.The longest diameter of the aneurysms was classified into
groups: group 1 (≤3 mm), group 2 (3–10 mm) and group 3>10 mm).
The shape of the aneurysms was categorized into 2 groups.roup 1 included lobulated aneurysms and group 2 included round
neurysms.The presence of spasm was evaluated from the 2DDSA andA images. The presence of pseudospasm or pseudostenosis was
Radiology 81 (2012) 2794– 2800
evaluated from the 3DVRDSA images. The capability of 3DVRDSAto detect spasms was also analyzed.
The visibilities of the aneurysm location, neck, shape and rela-tionship to the neighboring artery were classified into 3 categories(1 = conclusive, 2 = ambiguous, 3 = insufficient).
2.4. Statistical analysis
Two-tailed �2 tests and Fischer’s exact tests were used for com-parisons between categorical variables in 2DDSA, RA and 3DVRDSAimages. SPSS version 11.5 (SPSS Inc., 2002) was used for data analy-ses. p < 0.05 was considered statistically significant. The sensitivityand specificity of 3DVRDSA imaging for the detection of vasospasmswere also calculated.
3. Results
None of the procedures were associated with morbidity ormortality, and the procedure was well tolerated by all patients.In all patients with subarachnoid hemorrhages, aneurysms weredetected with a combination of 2DDSA, RA and 3DVRDSA imag-ing. The results of categorical variable analysis are summarized inTable 2. A total of 52 of 122 aneurysms (42.6%) were seen in malepatients, and 70 of 122 aneurysms (57.4%) were seen in femalepatients.
A total of 35 of 122 aneurysms (28.7%) were located in the M1segment. This segment was the most frequently observed locationin our series.
Most of the best working angles (BWAs) were located in Type 2,and the Type 6. BWA was not predictable based on aneurysm loca-tion, dome/neck ratio, shape of the aneurysm and longest diameterof the aneurysm. A total of 74 of the 122 aneurysms (60.7%) werenarrow necked, and 48 of the 122 (39.3%) aneurysms were widenecked.
The longest diameter of the aneurysms was ≤3 mm in 33 of the122 aneurysms (27%), 3–10 mm in 79 of 122 aneurysms (64.8%) and>10 mm in 10 of 122 aneurysms (8.2%). The mean longest diam-eter was 5.76 ± 3.69 mm, and they ranged between 1.53 mm and22.72 mm.
The shape of the aneurysms was lobulated in 81 of 122aneurysms (66.4%) and round in 41 of 122 (33.6%).
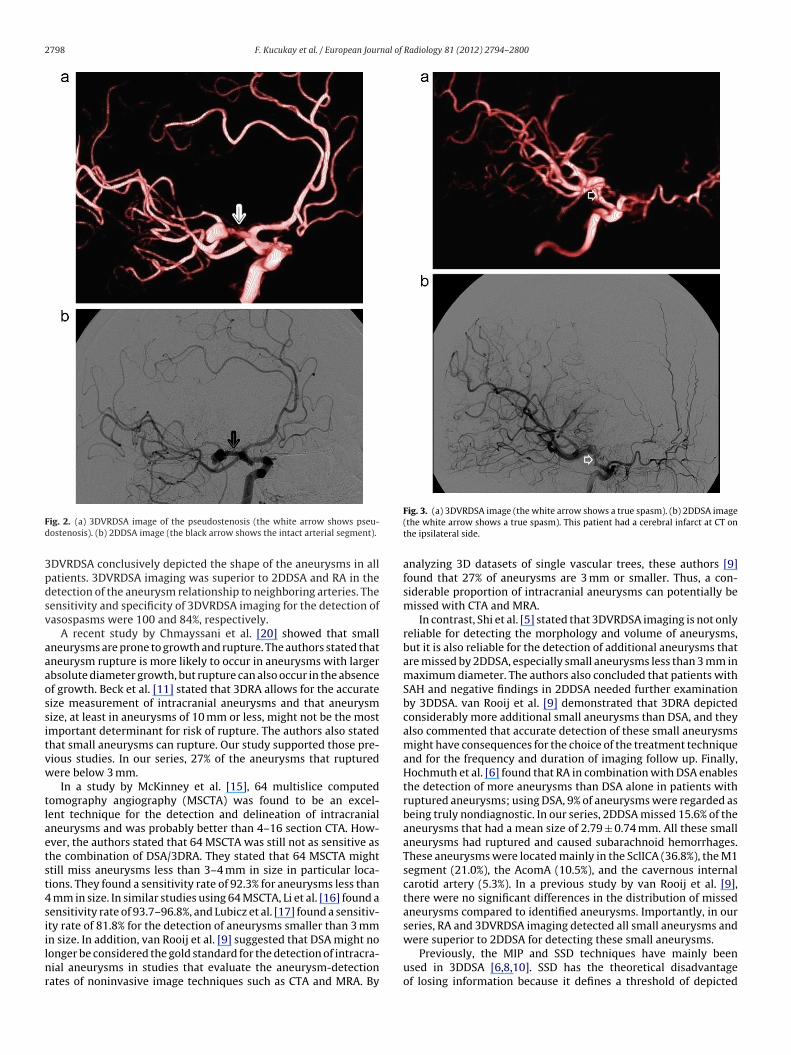
Spasms related to aneurysms were observed in 12 of 122aneurysms (9.8%) in 2DDSA images. However, in the 3DVRDSAimages, we observed that 30 of 122 (24.6%) aneurysms had relatedspasms (true plus pseudospasms) (Figs. 2(a), (b) and 3(a), (b)). Thesensitivity and specificity of 3DVRDSA imaging for the detection ofvasospasms were 100 and 84%, respectively.
Of the 122 aneurysms, 32 (26.2%) had an artery associated withthe aneurysmal sac, and 90 of 122 aneurysms (73.8%) did not havean artery associated with the aneurysmal sac.
A total of 70.8% (34 of 48) of the wide-necked aneurysms wereobserved in female patients (p < 0.05), and 81.8% (27 of 33) of thewide-necked aneurysms were observed in the aneurysms wherethe longest diameter was less than 3 mm (p < 0.05). A total of 65.9%(27 of 41) of the aneurysms that had lobulated contours were wide-necked aneurysms (p < 0.05). Finally, the aneurysms that causedspasms were narrow necked in 80% (24 of 30) of cases (p < 0.05).
The aneurysms that had a relationship with the neighboringartery were narrow necked in 81.3% (26 of 32) of cases (p < 0.05),and those with a relationship with the neighboring artery werelobulated in 84.4% (27 of 32) of cases.
diameter below 3 mm were round.The visibility of aneurysm details is summarized in Table 3.
Conclusive visibility of the location of the aneurysm in the 2DDSA

F. Kucukay et al. / European Journal of Radiology 81 (2012) 2794– 2800 2797
Table 2Results of categorical variable analysis.
Age 47.77 ± 12.81 ranging between 20 and 83 years oldGender Male = 52 of 122 (42.6%), female = 70 of 122 (57.4%)Aneurysm localization Group 1 = 28.7% (35 of 122); group 2 = 27.9% (34 of 122); group 3 = 26.2% (32 of 122); group 4 = 5.7% (7 of 122); group
5 = 2.5% (3 of 122); group 6 = 2.5% (3 of 122); group 7 = 1.6% (2 of 122); group 8 = 1.6% (2 of 122); group 9 = 0.8% (1 of122); group 10 = 0.8% (1 of 122); group 11 = 0.8% (1 of 122); group 12 = 0.8% (1 of 122)
Best working angle Type 1 = 13.1% (16 of 122); Type 2 = 16.4% (20 of 122), Type 3 = 12.3% (15 of 122); Type 4 = 15.6% (19 of 122); Type5 = 15.6% (19 of 122); Type 6 = 16.4% (20 of 122), Type 7 = 4.1% (5 of 122); Type 8 = 6.6% (8 of 122)
Dome/neck ratio Narrow necked = 60.7% (74 of the 122); wide necked = 39.3% (48 of the 122)The longest diameter of aneurysm <3 mm = 27% (33 of the 122); 3–10 mm = 64.8% (79 of 122); >10 mm = 8.2% (10 of 122 aneurysm)The shape of the aneurysm Lobulated = 66.4% (81 of 122); round = 33.6% (41 of 122)Presence of spasm Yes = 9.8% (12 of 122); no = 91.2% (110 of 122)Relationship to the neighboring artery Yes = 26.2% (32 of 122); no = 73.8% (90 of 122)
io1c1Trloam((
wtaawTi5fiaavib(R
TV
2p
Visibility of aneurysm details Fully explained in Table 3
mages was 73% (89 of 122). Ambiguous and insufficient visibilitiesf the aneurysm locations on the 2DDSA images were 11.5% (14 of22) and 15.6% (19 of 122), respectively. RA and 3DVRDSA imagesonclusively detected all aneurysm locations (100%). A total of5.6% (19 of 122) of the aneurysms could not be detected by 2DDSA.he mean size of missed aneurysms by 2DDSA was 2.79 ± 0.74 mm,anging between 1.53 mm and 4.15 mm. These aneurysms wereocated in the SclICA (36.8%, 7 of 19), the M1 segment (21.0%, 4f 19), the AcomA (10.5%, 2 of 19), the cavernous internal carotidrtery (5.3%, 1 of 19), the basilar artery (5.3%, 1 of 19), the A1 seg-ent (5.3%, 1 of 19), the A2 segment (5.3% 1 of 19), the A3 segment
5.3%, 1 of 19), and the bifurcation of the internal carotid artery5.3%, 1 of 19).
Conclusive visibility of the aneurysm neck in the 2DDSA imagesas 35.2% (43 of 122). Ambiguous and insufficient visibilities of
he aneurysm neck in the 2DDSA images were 2.5% (3 of 122)nd 62.3% (76 of 122), respectively. Conclusive visibility of theneurysm neck in the RA images was 72.1% (88 of 122 aneurysms),hereas ambiguous visibility was 27.9% (34 of 122 aneurysms).
here was no insufficient visibility of the aneurysm neck in the RAmages. RA revealed conclusive visibility of the aneurysm neck in1.1% (45 of 88) of the aneurysms that had ambiguous and insuf-cient visibility in the 2DDSA images. Conclusive visibility of theneurysm neck in the 3DVRDSA images was 97.5% (119 of 122), andmbiguous visibility was 2.5% (3 of 122). There was no insufficientisibility of the aneurysm neck in the 3DVRDSA images. Regard-
ng the conclusive visibility of the aneurysm neck, the differenceetween RA and 3DVRDSA imaging was statistically significantp < 0.05). Additionally, the difference between 2DDSA imaging andA was significant (p < 0.05). The 2DDSA, RA and 3DVRDSA imagingable 3isibility of the aneurysm details in 2DDSA, RA and 3DVRDSA imaging.
Visibility of 2DDSA
Aneurysm locationConclusive 73.0% (89 of 122)
Ambiguous 11.5% (14 of 122)
Insufficient 15.6% (19 of 122)
Aneurysm neckConclusive 35.2% (43 of 122)
Ambiguous 2.5% (3 of 122)
Insufficient 62.3% (76 of 122)
Aneurysm shapeConclusive 41.8% (51 of 122)
Ambiguous 33.6% (41 of 122)
Insufficient 24.6% (30 of 122)
Aneurysm relationship to the neighboring arteryConclusive 28.7% (35 of 122)
Ambiguous 2.5% (3 of 122)
Insufficient 68.9% (84 of 122)
DDSA = 2D digital subtraction angiography; RA = rotational angiography; 3DVRDSA = 3D
< 0.05 is statistically significant.
techniques conclusively determined visibility of aneurysm necks in35.2% (43 of 122), 72.1% (88 of 122) and 97.5% (119 of 122) of cases,respectively.
Conclusive visibility of aneurysm shape was 41.8% (51 of 122)in 2DDSA imaging. Ambiguous and insufficient visibilities of theaneurysm shape with 2DDSA imaging were 33.6% (41 of 122) and24.6% (30 of 122), respectively. Conclusive, ambiguous and insuffi-cient visibilities of the aneurysm shape on rotational angiographswere 98.4% (120 of 122), 1.6% (2 of 122) and 0% (0 of 122), respec-tively. 3DVRDSA imaging conclusively determined the aneurysmshape in 100% of cases (122 of 122 aneurysms).
Conclusive, ambiguous and insufficient visibilities of theaneurysm relationship to the neighboring artery in 2DDSA imagingwere 28.7% (35 of 122), 2.5% (3 of 122) and 68.9% (84 of 122), respec-tively, and these were 70.5% (86 of 122), 28.7% (35 of 122) and 0.8%(1 of 122), respectively, for RA and 96.7% (118 of 122), 3.3% (4 of122) and 0% (0 of 122), respectively, for 3DVRDSA. The differencesbetween 2DDSA imaging and RA (p < 0.05), RA and 3DVRDSA imag-ing (p < 0.05), and 2DDSA imaging and 3DVRDSA imaging (p < 0.05)were all statistically significant (Table 3).
Age, gender, presence of spasm and the BWA had no significantcorrelation with other categorical variables. There was no signifi-cant correlation between the remaining categorical variables.
4. Discussion
The results of this study demonstrated that 2DDSA missed 15.6%of the aneurysms that had a mean size of 2.79 ± 0.74 mm. RA wassuperior to 2DDSA in the detection of aneurysm necks. 3DVRDSAimaging was superior to RA in the detection of aneurysm necks.
RA 3DVRDSA imaging
100% 100%0% 0%0% 0%
72.1% (88 of 122) 97.5% (110 of 122)27.9% (34 of 122) 2.5% (3 of 122)
0% 0%
98.4% (110 of 122) 100%1.6% (2 of 122) 0%0% 0%
70.5% (86 of 122) 96.7% (118 of 122)28.7% (35 of 122) 3.3% (4 of 122)
0.8% (1 of 122) 0%
volume rendering digital subtraction angiography.
2798 F. Kucukay et al. / European Journal of Radiology 81 (2012) 2794– 2800
Fd
3pdsv
aaaossitvw
tlaetst4siilnr
ig. 2. (a) 3DVRDSA image of the pseudostenosis (the white arrow shows pseu-ostenosis). (b) 2DDSA image (the black arrow shows the intact arterial segment).
DVRDSA conclusively depicted the shape of the aneurysms in allatients. 3DVRDSA imaging was superior to 2DDSA and RA in theetection of the aneurysm relationship to neighboring arteries. Theensitivity and specificity of 3DVRDSA imaging for the detection ofasospasms were 100 and 84%, respectively.
A recent study by Chmayssani et al. [20] showed that smallneurysms are prone to growth and rupture. The authors stated thatneurysm rupture is more likely to occur in aneurysms with largerbsolute diameter growth, but rupture can also occur in the absencef growth. Beck et al. [11] stated that 3DRA allows for the accurateize measurement of intracranial aneurysms and that aneurysmize, at least in aneurysms of 10 mm or less, might not be the mostmportant determinant for risk of rupture. The authors also statedhat small aneurysms can rupture. Our study supported those pre-ious studies. In our series, 27% of the aneurysms that rupturedere below 3 mm.
In a study by McKinney et al. [15], 64 multislice computedomography angiography (MSCTA) was found to be an excel-ent technique for the detection and delineation of intracranialneurysms and was probably better than 4–16 section CTA. How-ver, the authors stated that 64 MSCTA was still not as sensitive ashe combination of DSA/3DRA. They stated that 64 MSCTA mighttill miss aneurysms less than 3–4 mm in size in particular loca-ions. They found a sensitivity rate of 92.3% for aneurysms less than
mm in size. In similar studies using 64 MSCTA, Li et al. [16] found aensitivity rate of 93.7–96.8%, and Lubicz et al. [17] found a sensitiv-ty rate of 81.8% for the detection of aneurysms smaller than 3 mm
n size. In addition, van Rooij et al. [9] suggested that DSA might noonger be considered the gold standard for the detection of intracra-ial aneurysms in studies that evaluate the aneurysm-detectionates of noninvasive image techniques such as CTA and MRA. ByFig. 3. (a) 3DVRDSA image (the white arrow shows a true spasm). (b) 2DDSA image(the white arrow shows a true spasm). This patient had a cerebral infarct at CT onthe ipsilateral side.
analyzing 3D datasets of single vascular trees, these authors [9]found that 27% of aneurysms are 3 mm or smaller. Thus, a con-siderable proportion of intracranial aneurysms can potentially bemissed with CTA and MRA.
In contrast, Shi et al. [5] stated that 3DVRDSA imaging is not onlyreliable for detecting the morphology and volume of aneurysms,but it is also reliable for the detection of additional aneurysms thatare missed by 2DDSA, especially small aneurysms less than 3 mm inmaximum diameter. The authors also concluded that patients withSAH and negative findings in 2DDSA needed further examinationby 3DDSA. van Rooij et al. [9] demonstrated that 3DRA depictedconsiderably more additional small aneurysms than DSA, and theyalso commented that accurate detection of these small aneurysmsmight have consequences for the choice of the treatment techniqueand for the frequency and duration of imaging follow up. Finally,Hochmuth et al. [6] found that RA in combination with DSA enablesthe detection of more aneurysms than DSA alone in patients withruptured aneurysms; using DSA, 9% of aneurysms were regarded asbeing truly nondiagnostic. In our series, 2DDSA missed 15.6% of theaneurysms that had a mean size of 2.79 ± 0.74 mm. All these smallaneurysms had ruptured and caused subarachnoid hemorrhages.These aneurysms were located mainly in the SclICA (36.8%), the M1segment (21.0%), the AcomA (10.5%), and the cavernous internalcarotid artery (5.3%). In a previous study by van Rooij et al. [9],there were no significant differences in the distribution of missedaneurysms compared to identified aneurysms. Importantly, in ourseries, RA and 3DVRDSA imaging detected all small aneurysms and
were superior to 2DDSA for detecting these small aneurysms.Previously, the MIP and SSD techniques have mainly beenused in 3DDSA [6,8,10]. SSD has the theoretical disadvantageof losing information because it defines a threshold of depicted

nal of
HiiRntnsptttataTibuptva4
Srdopavlnwai(i2a
cppbcottar
itavsa[v2cewo
F. Kucukay et al. / European Jour
ounsfield units and because it defines only contiguous objects fornformation [6]. Sugahara et al. [8] showed that the MIP and SSDmages are significantly superior to those of standard 2DDSA andA for the detection of aneurysms. MIP and SSD images were sig-ificantly superior to both standard 2DDSA and rotational DSA forhe visualization of the aneurysm neck and the relationship witheighboring arteries. Additionally, SSD images were significantlyuperior to those of MIP, standard 2DDSA and RA for detecting theresence of lobulation [8]. Similarly, Anxionnat et al. [10] reportedhat 3D SSD and MIP images are superior to 2DDSA in depictinghe aneurysm neck and shape. 3DDSA was found to be valuable forhe evaluation of the potential for endovascular treatment, finding
working view, and performing accurate measurements. In addi-ion, Hochmuth et al. [6] commented that compared to DSA, 3DDSAllowed for a more realistic estimation of the therapeutic risk.hese authors also found [6] that delineation of the aneurysm neckmproved with RA in 71% of the cases, which is important becauseetter clarification of the anatomic situation helps to eliminatenexpected findings during the surgical procedure. For instance,recise visualization of the aneurysm neck makes the decisiono perform coil placement easier and the procedure safer. Parentessel demonstration and the relationship of the parent vessel todjacent vessels were found to be better using RA than 2DDSA in5% and 50% of the aneurysms, respectively [6].
The 3DVRDSA method has some advantages over the MIP andSD techniques. In 3DVRDSA, the entire DSA dataset can be incorpo-ated within the 3D image, whereas only a small fraction of data isisplayed on MIP and SSD images. The number, density and opacityf voxels can be adjusted separately to allow for a change in trans-arency of selected materials. The 3D appearance is maintainednd thereby allows for better analysis of the relationship amongascular structures [8]. Wan et al. [5] declared that due to its excel-ent ability to depict spatial relationships between aneurysms andeighboring arteries, 3DVRDSA imaging is useful for interventionhen determining therapeutic protocols and working projection
ngles. In our series, RA was superior to 2DDSA, and 3DVRDSAmaging was superior to RA in the detection of the aneurysm neckp < 0.05). Aneurysm shape was conclusively detected by 3DVRDSAn all patients. Finally, 3DVRDSA imaging was superior to bothDDSA and RA in detecting the relationship between the aneurysmnd neighboring arteries (p < 0.05).
One of the issues to consider is the radiation dose of 3DDSAompared to 2DDSA; 3DDSA may have a higher radiation dose com-ared to 2DDSA. However, in a study by Schueler et al. [12], theatient radiation dose for 3DRA was significantly lower than foriplanar DSA, by nearly 4 times in peak skin dose and 40% lower inumulative dose. Additionally, Abe et al. [7] stated that the numberf DSA exposures is decreased with 3DDSA, both when determininghe working projection and during the procedure. 3DDSA is essen-ial for optimal diagnosis and embolization of cerebral aneurysmsnd can reduce the number of exposures and the side effects ofadiation [7].
The development of cerebral ischemia due to vasospasm, whichs a major cause of morbidity and mortality, is a poor prognos-ic factor for patients with subarachnoid hemorrhages. There is
debate about whether the degree of angiographically visibleasospasms causes worsening of the patient’s status and clinicalymptoms. Crowley et al. stated that there is a strong associ-tion between angiographic vasospasms and cerebral infarction18]. Infarcts developed in 6 (3%) of 209 patients with no/mildasospasms, 12 (10%) of 118 with moderate vasospasms, and5 (46%) of 54 with severe vasospasms. Vergouwen et al. [19]
ommented that in their study, the majority of patients with mod-rate to severe angiographic vasospasms did not have neurologicalorsening of any cause or cerebral infarction. These authors alsobserved that cerebral infarction had a direct effect on outcome
Radiology 81 (2012) 2794– 2800 2799
independent of angiographic vasospasm. They suggested that othercoexisting factors might be involved in the pathogenesis of delayedcerebral ischemia, which should also be an important research tar-get to improve outcome after subarachnoid hemorrhage. In ourseries, 9.8% (12 of 122) of patients with ruptured aneurysms hadvasospasms. A total of 7 out of 12 (58.3%) vasospasms were severe,and cerebral infarction on the effected lobe was observed in 4 of 7(57.1%) cases with vasospasms. Our results were similar to one ofCrowley et al. [18]. Severe cerebral artery angiographic spasm didcause a cerebral infarct, which was different from the findings ofVergouwen et al. [19]. However, large clinical studies are requiredto support our findings. Pseudostenosis [13] is a stenosis that isseen in 3DDSA but is revealed not to be a real stenosis in 2DDSA.These authors [13] found that the incidence of a pseudostenosis in3DVRDSA images of intracranial arteries was relatively high: 34%of 3DDSA examinations. Yao et al. [14] revealed that 3DRA wasless useful than 2DDSA for the evaluation of vasospasms after sub-arachnoid hemorrhage. The sensitivity, specificity, and positive andnegative predictive values of 3DRA for detecting vasospasms were100, 76, 90, and 100%, respectively. In our study, pseudosteno-sis was observed in 3DVRDSA images in 14.8% (18 of 122) of theaneurysms, and the sensitivity and specificity of 3DVRDSA fordetecting vasospasms were 100 and 84%, respectively.
There are some limitations of this study. We did not compare3DVRDSA imaging with CT angiography or MR angiography fordetecting aneurysms and their morphological properties. In ourclinic, CTA and MRA are not the routine procedures used in thepreinterventional evaluation of ruptured aneurysms. For subarach-noid hemorrhages, our protocol includes routine 2DDSA imagingwith RA and 3DVRDSA imaging following CT imaging of the head.Our 2DDSA imaging was performed with a monoplane angiog-raphy system instead of a biplane system. Additionally, we didnot compare our results with unruptured aneurysms, especiallywith smaller ones. The existence of subarachnoid hemorrhage inall patients led us to search for an aneurysm in a detailed fash-ion. Finally, we did not analyze the effects of our findings onendovascular or surgical approaches, and we did not comparewhich therapeutic method could benefit from our findings. Futureclinical studies comparing 3DVRDSA with 128 or more-multisliceCTAs for detection of small aneurysms and identification of mor-phological properties of them may be interesting.
In conclusion, 3DVRDSA imaging is superior to 2DDSA and RA fordetecting the aneurysms and their morphological properties (loca-tion, neck, shape, relation with neighboring arteries), especiallysmall, ruptured aneurysms. However, 2DDSA should still be used incases with vasospasms, which are important poor prognostic fac-tors in patients with SAH, in which 3DVRDSA plays a limited role.The pseudostenosis phenomenon that is seen in 3DVRDSA imag-ing remains a technical problem to be solved in the diagnosis ofaneurysms in patients with SAH.
Conflict of interest
The authors state that there is no actual or potential conflict ofinterest in relation to this article.
References
[1] Nieuwkamp DJ, Setz LE, Algra A, Linn FH, de Rooij NK, Rinkel GJ. Changes incase fatality of aneurysmal subarachnoid haemorrhage over time, according toage, sex, and region: a meta-analysis. Lancet Neurol 2009;8:635–42.
[2] Huang J, van Gelder JM. The probability of sudden death from rupture ofintracranial aneurysms: a meta-analysis. Neurosurgery 2002;51:1101–5.
[3] van Gijn J, Kerr RS, Rinkel GJ. Subarachnoid haemorrhage. Lancet2007;369(January):306–18.
[4] Gauvrit JY, Leclerc X, Vermandel M, et al. 3D rotational angiography: use ofpropeller rotation for the evaluation of intracranial aneurysms. AJNR Am JNeuroradiol 2005;26:163–5.
2 nal of
[
[
[
[
[
[
[
[
[
[
800 F. Kucukay et al. / European Jour
[5] Shi WY, Li YD, Li MH, et al. 3D rotational angiography with volume ren-dering: the utility in the detection of intracranial aneurysms. Neurol India2010;58:908–13.
[6] Hochmuth A, Spetzger U, Schumacher M. Comparison of three-dimensionalrotational angiography with digital subtraction angiography in the assess-ment of ruptured cerebral aneurysms. AJNR Am J Neuroradiol 2002;23:1199–205.
[7] Abe T, Hirohata M, Tanaka N, et al. Clinical benefits of rotational 3D angiog-raphy in endovascular treatment of ruptured cerebral aneurysm. AJNR Am JNeuroradiol 2002;23:686–8.
[8] Sugahara T, Korogi Y, Nakashima K, Hamatake S, Honda S, Takahashi M.Comparison of 2D and 3D digital subtraction angiography in evaluation ofintracranial aneurysms. AJNR Am J Neuroradiol 2002;23:1545–52.
[9] van Rooij WJ, Sprengers ME, de Gast AN, Peluso JP, Sluzewski M. 3D rotationalangiography: the new gold standard in the detection of additional intracranialaneurysms. AJNR Am J Neuroradiol 2008;29:976–9.
10] Anxionnat R, Bracard S, Ducrocq X, et al. Intracranial aneurysms: clinical valueof 3D digital subtraction angiography in the therapeutic decision and endovas-cular treatment. Radiology 2001;218:799–808.
11] Beck J, Rohde S, Berkefeld J, Seifert V, Raabe A. Size and location of rupturedand unruptured intracranial aneurysms measured by 3-dimensional rotationalangiography. Surg Neurol 2006;65:18–25 [discussion 25–7].
12] Schueler BA, Kallmes DF, Cloft HJ. 3D cerebral angiography: radiation dosecomparison with digital subtraction angiography. AJNR Am J Neuroradiol2005;26:1898–901.
13] Hirai T, Korogi Y, Ono K, Yamura M, Uemura S, Yamashita Y. Pseudosteno-sis phenomenon at volume-rendered three-dimensional digital angiography
[
Radiology 81 (2012) 2794– 2800
of intracranial arteries: frequency, location, and effect on image evaluation.Radiology 2004;232:882–7.
14] Yao GE, Li Q, Jiang XJ, et al. Vasospasm after subarachnoid hemor-rhage: a 3D rotational angiography study. Acta Neurochir Suppl 2011;110:221–5.
15] McKinney AM, Palmer CS, Truwit CL, Karagulle A, Teksam M. Detection ofaneurysms by 64-section multidetector CT angiography in patients acutelysuspected of having an intracranial aneurysm and comparison with dig-ital subtraction and 3D rotational angiography. AJNR Am J Neuroradiol2008;29:594–602.
16] Li Q, Lv F, Li Y, Luo T, Li K, Xie P. Evaluation of 64-section CT angiography fordetection and treatment planning of intracranial aneurysms by using DSA andsurgical findings. Radiology 2009;252:808–15.
17] Lubicz B, Levivier M, Franc ois O, et al. Sixty-four-row multisection CT angiog-raphy for detection and evaluation of ruptured intracranial aneurysms:interobserver and intertechnique reproducibility. AJNR Am J Neuroradiol2007;28:1949–55.
18] Crowley RW, Medel R, Dumont AS, et al. Angiographic vasospasm is stronglycorrelated with cerebral infarction after subarachnoid hemorrhage. Stroke2011;42:919–23.
19] Vergouwen MD, Ilodigwe D, Macdonald RL. Cerebral infarction after subarach-noid hemorrhage contributes to poor outcome by vasospasm-dependent and
-independent effects. Stroke 2011;42:924–9.20] Chmayssani M, Rebeiz JG, Rebeiz TJ, Batjer HH, Bendok BR. Rela-tionship of growth to aneurysm rupture in asymptomatic aneurysms≤7 mm: a systematic analysis of the literature. Neurosurgery 2011,doi:10.1227/NEU.0b013e31820edbd3.
Related Documents











