THOMAS L. SPRAY, MD THOMAS L. SPRAY, MD Chief, Cardiothoracic Surgery Chief, Cardiothoracic Surgery Alice Langdon Warner Endowed Chair Alice Langdon Warner Endowed Chair The Children’s Hospital of Philadelphia The Children’s Hospital of Philadelphia Professor of Surgery Professor of Surgery The University of Pennsylvania The University of Pennsylvania THE BORDERLINE LEFT VENTRICLE: Where to draw the line The Cardiac Center at The Children’s Hospital of Philadelphia NO DISCLOSURES

THOMAS L. SPRAY, MD THOMAS L. SPRAY, MD Chief, Cardiothoracic Surgery Chief, Cardiothoracic Surgery Alice Langdon Warner Endowed Chair Alice Langdon Warner.
Dec 31, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

THOMAS L. SPRAY, MDTHOMAS L. SPRAY, MD
Chief, Cardiothoracic SurgeryChief, Cardiothoracic Surgery Alice Langdon Warner Endowed ChairAlice Langdon Warner Endowed Chair
The Children’s Hospital of PhiladelphiaThe Children’s Hospital of Philadelphia Professor of SurgeryProfessor of Surgery
The University of PennsylvaniaThe University of Pennsylvania
THE BORDERLINE LEFT VENTRICLE:
Where to draw the line
The Cardiac Center at The Children’s Hospital of Philadelphia NO DISCLOSURES
ANATOMY OF VENTRICULAR HYPOPLASIA
LV Hypoplasia:• Aortic Stenosis• AS/ Mitral Stenosis• Coarctation of Aorta• TAPVR• IAA/VSD• TGA• Unbalanced AVSD

CAN VENTRICULAR GROWTH BE STIMULATED AFTER BIRTH?
What Are The Signals For Ventricular Growth?
Positive: Flow (Volume, Shear Stress) Preload (Compliance) Negative: Afterload (Hypertrophy)

CAN YOU VARY PRELOAD TO LV?
• Adjustable ASD• Leave Vertical Vein Open In
TAPVR:• Left-to-Right Shunt Volume Re-
Presented To LV• ? Capacitance of Functional LA

LV “GROWTH” DEMONSTRATED WITH
REPAIR
Septal Shift, Volume Loading of LV, Volume Unloading of RV
Relief of Afterload on LV/RV

LIMITATIONS TO BVR IN LV HYPOPLASIA:
“Fixed” Structural Lesions
• Endomyocardial Fibroelastosis• MV Stenosis• Straddling AV Valves• Anatomically Abnormal AV
Valves• Residual Outflow Obstructive
Lesions
LV GROWTH IN CRITICAL AORTIC STENOSIS
• Criteria for BVR• Ross-Konno• Resection of EFE• Ross-Konno-MVR if MS• PHTN Late Complication

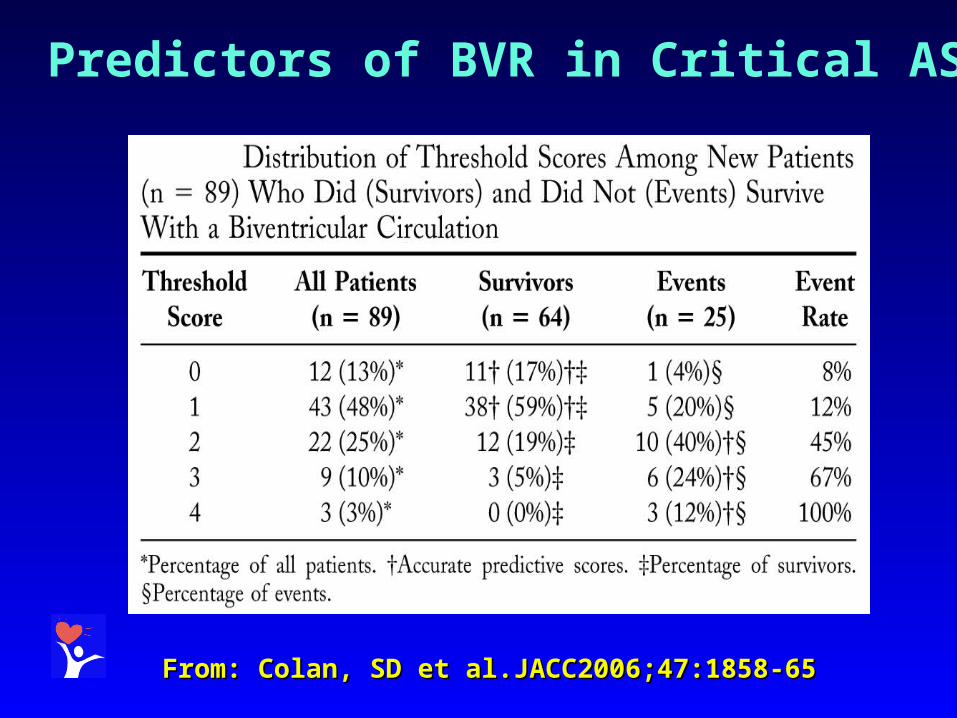
Predictors of BVR in Critical AS:New “Rhodes” Score
12.16 (BSA) + 0.59 (aortic valve annulus z-score) +5.73 (LAR) – 7.02
Discriminant cutoff of 0.46 accurately predicts 91% of survivors and 80% events (death)
From: Colan, SD et al.JACC2006;47:1858-65From: Colan, SD et al.JACC2006;47:1858-65
From: Colan, SD et al.JACC2006;47:1858-65From: Colan, SD et al.JACC2006;47:1858-65
Predictors of BVR in Critical AS
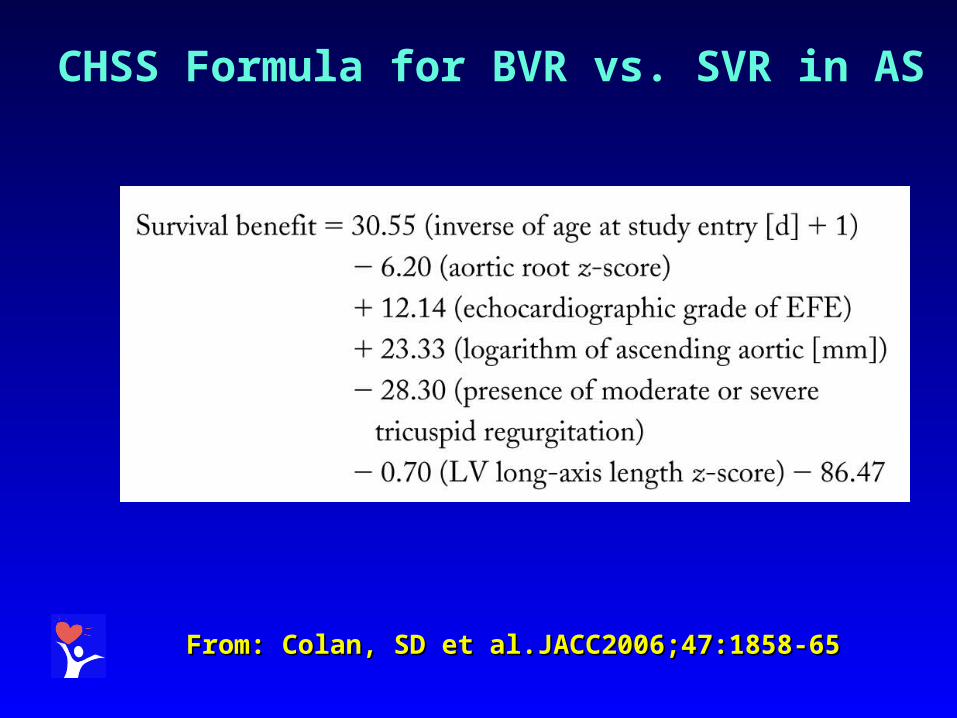
From: Colan, SD et al.JACC2006;47:1858-65From: Colan, SD et al.JACC2006;47:1858-65
CHSS Formula for BVR vs. SVR in AS

SURVIVAL BASED ON MANAGEMENT
From: Hickey, EJ, et al. JTCVS 2007;134:1429-37

LV GROWTH IN “HLH COMPLEX” / CoA
• Repair Coarctation• ? ASD Restriction/ Closure• ? PA Band If VSD• When is BVR Failing And
Requires Conversion To SVR?

From: Serraf, A et al. JACC 1999;33:827-34From: Serraf, A et al. JACC 1999;33:827-34
HLHC Survival and Reoperation-Free SurvivalHLHC Survival and Reoperation-Free Survival

LV GROWTH IN TAPVR
• Is The LV Ever Too Small?
• Should The Vertical Vein/ ASD Be Left Open?

UNBALANCED AV CANAL
• 10% Of All Common Atrioventricular Canal• Right Dominant More Common Than Left
Dominant Forms• Right Dominant Associated With SubAS, CoA,
Arch Hypoplasia• High Morbidity And Mortality• Not Usually Associated With Down Syndrome • Few Published Reports
BACKGROUNDBACKGROUND

• RV Volume > LV Volume In “Balanced” AV RV Volume > LV Volume In “Balanced” AV CanalCanal
• Degree Of Unbalance Of AV Valves May Not Degree Of Unbalance Of AV Valves May Not Correlate With Ventricular VolumesCorrelate With Ventricular Volumes
• Position Of Ventricular Septum May Be DisplacedPosition Of Ventricular Septum May Be Displaced• Patch Closure Of VSD May Increase LV VolumePatch Closure Of VSD May Increase LV Volume• Abnormal Geometry Of LV Outflow Tract And Abnormal Geometry Of LV Outflow Tract And
Ventricle Alters Accuracy Of MeasurementsVentricle Alters Accuracy Of Measurements
UNBALANCED AV CANAL
ERRORS IN MEASUREMENT OF VENTRICULAR VOLUME IN AVC

UNBALANCED AV CANAL
• Considered To Be Higher Risk Lesion Than HLHS In Staged Reconstruction
• Atrioventricular Valve Regurgitation Is Common
• More Likely To Require Atrioventricular Valvuloplasty Or Replacement Than HLHS
SINGLE VENTRICLE REPAIRSINGLE VENTRICLE REPAIR

UNBALANCED AV CANAL
• Antegrade Flow In Ascending AortaAntegrade Flow In Ascending Aorta• No PDA Or Only Left-To-Right No PDA Or Only Left-To-Right
Ductal FlowDuctal Flow• Restrictive Or No VSDRestrictive Or No VSD• AVVI > 0.27, Inflow Into Both AVVI > 0.27, Inflow Into Both
Ventricles SymmetricVentricles Symmetric• ““Potential” LV Volume > 15 ml/mPotential” LV Volume > 15 ml/m22
• Unbalance To The Left VentricleUnbalance To The Left Ventricle
FACTORS FAVORING TWO VENTRICLE REPAIR

LV GROWTH IN UNBALANCED AVSD
• LV Inflow Primary Issue, Not LV Size
• Small MV, Especially With Small/Restrictive VSD or Restricted LV Inflow May Preclude Successful Repair Despite Reasonable LV Size (MR Through Cleft)

UNBALANCED AV CANAL
IMPORTANT ANATOMIC/PHYSIOLOGIC IMPORTANT ANATOMIC/PHYSIOLOGIC VARIABLESVARIABLES
• Direction Of Ascending Aortic Flow• Ductal Shunt Direction• Relative Atrioventricular Valve Size• Atrioventricular Valve Anatomy/Fxn• Subaortic Stenosis • Arch Hypoplasia/Coarctation• Size Of VSD And Direction Of Shunt• Size Of LV/RVSize Of LV/RV
The CHOP ApproachThe CHOP ApproachThe CHOP Approach
• Principle: If the inlet is sufficient the ventricle will be as well, so long as there is no other source of flow into the ventricle, i.e. VSD
• Derivative Principle: In the presence of a VSD, the LV cavity may appear seductively attractive for a 2V repair, but the inlet may be limiting!
• Principle: If the inlet is sufficient the ventricle will be as well, so long as there is no other source of flow into the ventricle, i.e. VSD
• Derivative Principle: In the presence of a VSD, the LV cavity may appear seductively attractive for a 2V repair, but the inlet may be limiting!
UNBALANCED AV CANAL

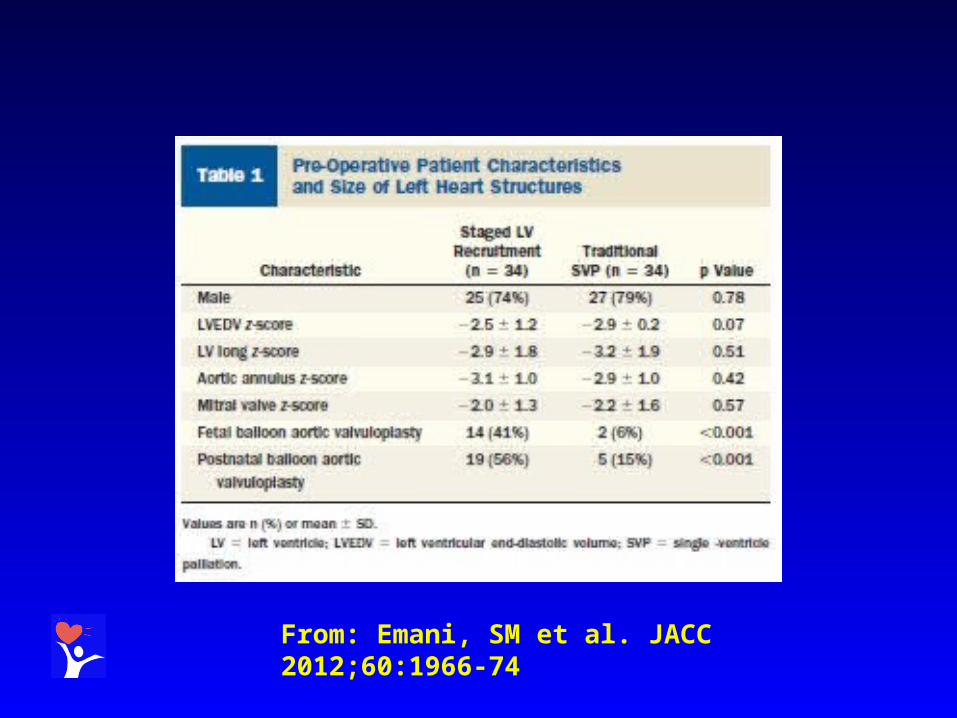
STAGED LV RECRUITMENT
From: Emani, SM, et al. JACC 2012;60:1966-74
ADVANTAGES OF LV “Rehabilitation”
• BVR eventually accomplished in 33% or more• LV size, function improves• Growth of left heart structures
DISADVANTAGES OF LV “Rehabilitation”
• AV still abnormal – AVR likely if previous intervention• MV still abnormal – MS/MR common, may eventually require MVR• LV diastolic function improved – long-term outcome unknown• Late exercise performance not known• PA pressures may not normalize• All risks of Norwood still present

LV POST “Rehabilitation”
From: Emani, SM et al. JACC 2012;60:1966-74

CHOP Selection Criteria For BVR (Survival 96%)
• MV Z-score >-3.7, Smallest MV dimension >5 mm
• No significant MS whether or not MV abnormal• Small PFO/ASD, modest gradient (<8 mm Hg.)• Mild LV hypoplasia (RV/LV 0.7-1.9)• Small or no VSD• No significant EFE• Mild-moderate arch gradient• Antegrade flow in arch

Endocardial Fibroelastosis (EFE)• Major risk factor for poor outcome• Hard to diagnose• 3 Types: Grade 1 – Pap M involvement only
Grade 2 – Pap M and some endocardial involvement
Grade 3 – Extensive endocardial involvement
• Should all grades be addressed?• ? Effect of residual EFE• ? Results of scarring after resection

WHEN IS SVR BETTER THAN BVR?
• After 1 Yr., SVR functional survival good for >20 yr.
• Functional results after BVR not well studied long-term
• Late decrease in compliance, elevated PVR and valve lesions may limit late options (Tx)
• Survival @ 20 yr. may be better with SVR, but ? @ 40 yr.
“GOOD” BVR CANDIDATES
• Anatomically normal but hypoplastic left-sided intracardiac structures with antegrade arch flow
• AV stenosis with normally-functioning MV• No or Grade 1 EFE• MV Z-score >-3• AAVI > .27 with inflow into LV (CAVC)

“POOR” BVR CANDIDATES
• LV hypoplasia plus unrestrictive VSD• Stenotic AV plus
abnormal/stenotic/hypoplastic MV• ? Grade 3 EFE with abnormal MV• ? Left-sided structures with Z-value <-4• AVVI >0.27 but with inflow directed into RV
(CAVC)

SUMMARY
• Decisions About Ventricular Suitability For BV Repair Remain Difficult
• Despite Improved Measurement Techniques, Absolute Limits of LV/RV Hypoplasia Preventing BVR Remain Unclear
• Primary Issue Is Asessment Of Adequacy Of Ventricular Inflow and EFE
• Much Early LV/RV “Growth” After BVR Is Septal Repostioning From VSD Closure Or Decrease In RV Volume Load And Increase In LV Preload

SUMMARY• Adjusting Preload To Stimulate Ventricular Growth May Be
Useful After Relief Of Obstruction Distally, but presumes adequate MV
• Overall Results With BVR In Patients With Borderline LV Not Much Different Than SV Reconstruction, Possibly With More Morbidity and Late Mortality
• Even When BVR Successful, Ventricles Can Have Abnormal Compliance
• AVSD Group Especially Difficult- MR May Limit Ability To Tolerate LV Loading
• Molecular Mechanisms Of LV Growth Remain To Be Clarified


From: Emani, SM et al. JACC 2012;60:1966-74

From: Emani, SM et al. JACC 2012;60:1966-74

From: Emani, SM et al. JACC 2012;60:1966-74

From: Emani, SM et al. JACC 2012;60:1966-74

From: Emani, SM et al. JACC 2012;60:1966-74

From: Emani, SM, et al. JTCVS 2009;138:1276-82

From: Emani, SM, et al. JTCVS 2009;138:1276-82


From: Cavigelli-Brunner, A., et al. Pediatr Cardiol 2012;33:506-12
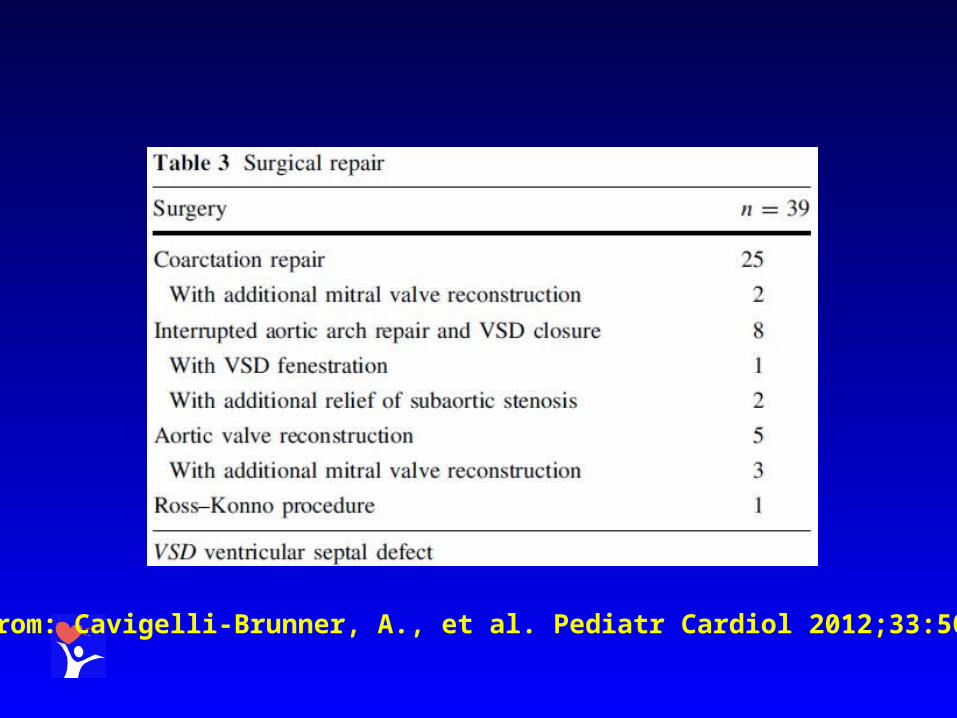
From: Cavigelli-Brunner, A., et al. Pediatr Cardiol 2012;33:506-12

From: Cavigelli-Brunner, A., et al. Pediatr Cardiol 2012;33:506-12

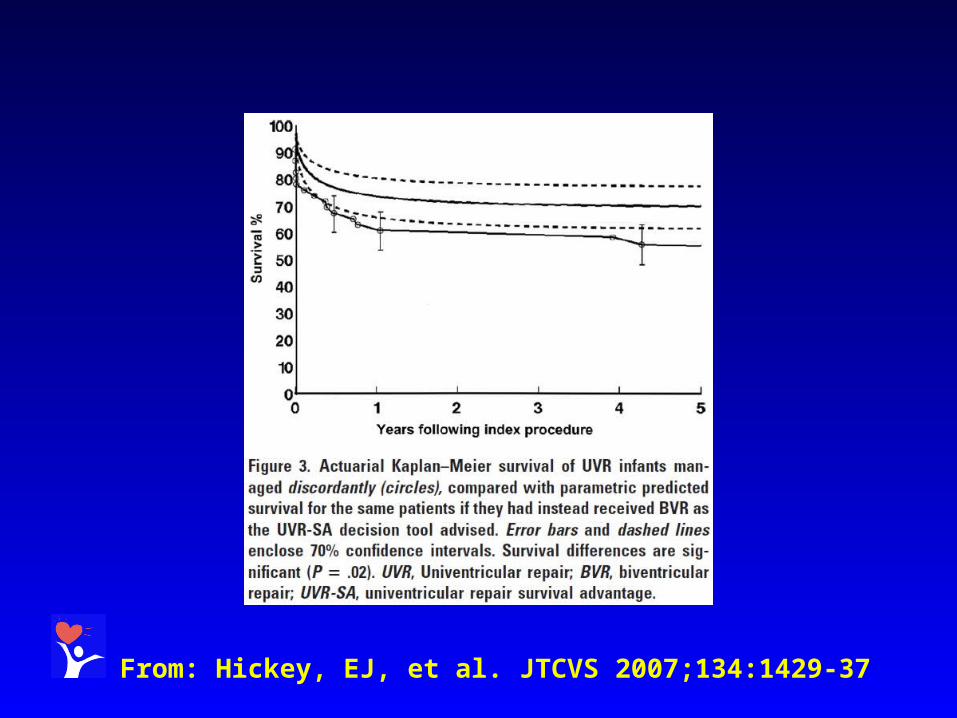
From: Hickey, EJ, et al. JTCVS 2007;134:1429-37

From: Hickey, EJ, et al. JTCVS 2007;134:1429-37
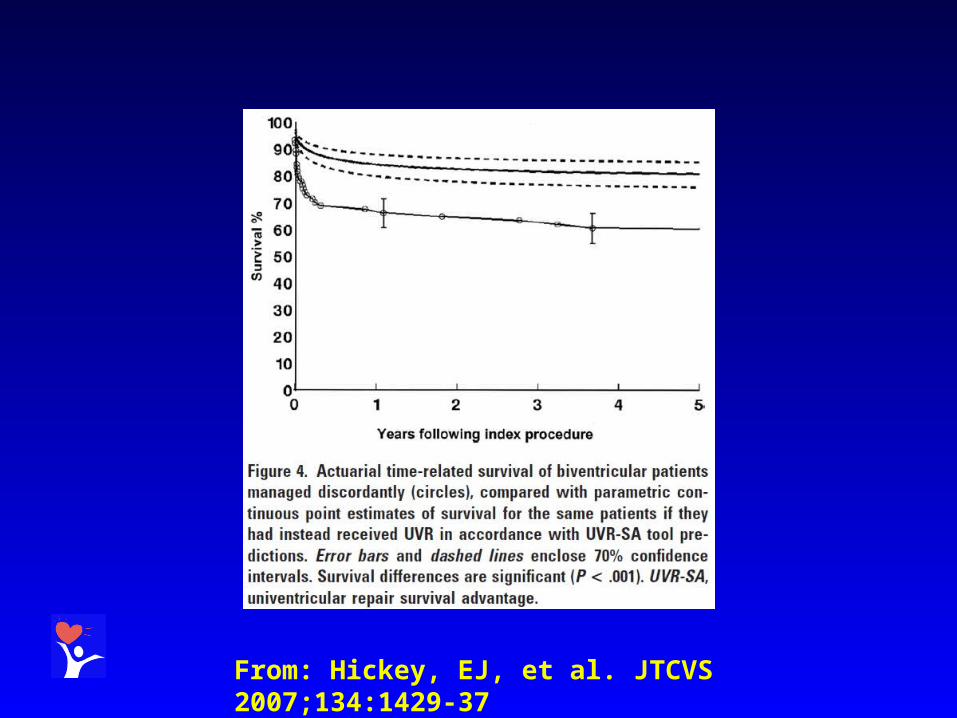
From: Hickey, EJ, et al. JTCVS 2007;134:1429-37

From: Hickey, EJ, et al. JTCVS 2007;134:1429-37

From: Hickey, EJ, et al. JTCVS 2007;134:1429-37

From: Hickey, EJ, et al. JTCVS 2007;134:1429-37

From: Hickey, EJ, et al. JTCVS 2007;134:1429-37


From: Avitabile, CM, et al. Ann Thorac Surg 2015;99:877-83

From: Avitabile, CM, et al. Ann Thorac Surg 2015;99:877-83


Related Documents











