This Back in Focus resource was developed and funded by AbbVie.. Date of preparation: June 2015; AXHUR150807p The Impact of Back Pain

This Back in Focus resource was developed and funded by AbbVie.. Date of preparation: June 2015; AXHUR150807p The Impact of Back Pain.
Dec 29, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

This Back in Focus resource was developed and funded by AbbVie.. Date of preparation: June 2015; AXHUR150807p
The Impact of Back Pain

• Who gets back pain?
• How many patients consult you each day for back pain?
• How many patients keep coming back to see you because of back pain?
• How does back pain affect the people you treat?
• When is back pain ‘just back pain’?
– When could it mean something more?
A few thoughts…
• 60-80% of adults report lower back pain at some point in their life1
• Approximately 6–9% of UK adults consult their GP about lower back pain each year2,3
Back pain: burden of disease
1. Waddel et al. Occup Med. 2001; 51:124–135. 2. Dunn and Croft. Spine, 2005; 16:1887–1892. 3. Cremin and Finn. Ir Med J 2002; 95141–95142.
Prevalence of inflammatory back pain
1. Hamilton et al. Clin Exp Rheumatol 2012; 30;4 p621.
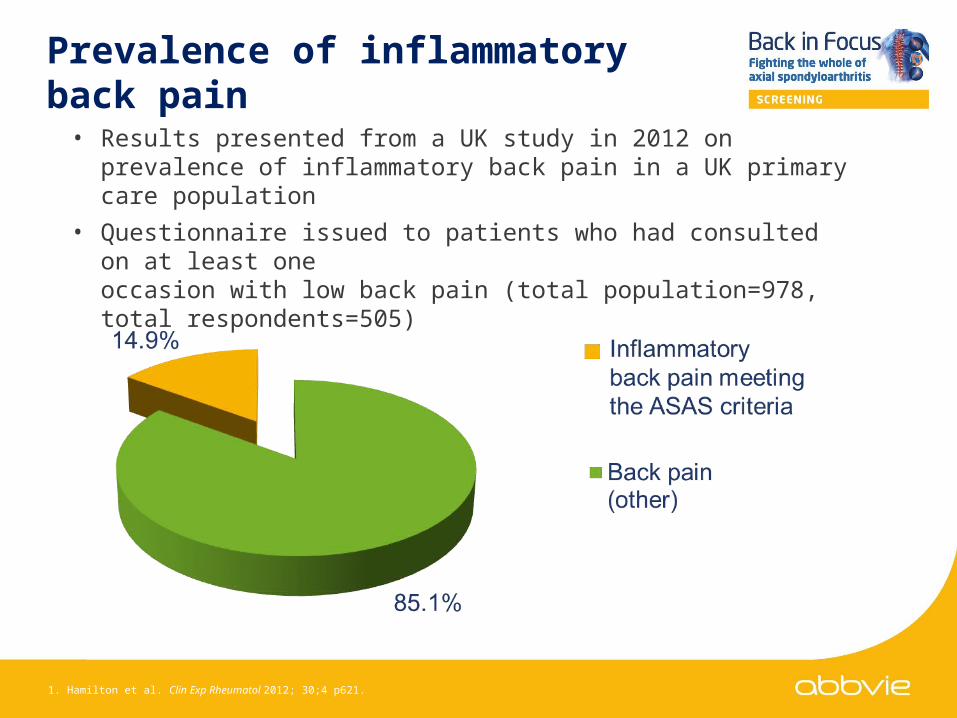
• Results presented from a UK study in 2012 on prevalence of inflammatory back pain in a UK primary care population
• Questionnaire issued to patients who had consulted on at least one occasion with low back pain (total population=978, total respondents=505)

The economic burden of back pain
1. de Souza and Frank, Disability and rehabilitation 2011;33:310–318. 2. Maniadakis and Gray. Pain 2000; 84:95–103. 3. van Tulder et al. Eur Spine J 2006; 15 (Suppl. 2):S169–S191.
£0 £2,000 £4,000 £6,000 £8,000 £10,000 £12,000 £14,000
Back pain
Coronary heart disease
Rheumatoid arthritis
Lower respiratory tract infections
Alzheimer's disease
Stroke
Diabetes
Arthritis
Multiple sclerosis
Deep vein thrombosis & pulmonary embolism
Depression
Insulin dependent diabetes
Critical limb ischaemia
Epilepsy
Benign prostatic hyperplasia
Multiple sclerosis
Migraine
Indirect costsDirect costs
Cost in 1998 ~ £1632 million
75-85% workers’
absenteeism
• Over half of chronic back pain patients may suffer with insomnia1
• Back pain also has psychosocial effects– Emotional stresses– Relationship breakdowns– Severe emotional distress to partners– Limitations in fulfilling their family role2
The impact of back on patients’ lives
1. Tang et al. J Sleep Res. 2007;16:85–95. 2. de Souza and Frank. Disability and rehabilitation 2011;33:310–318.

• Chronic back pain is defined as pain which occurs for >3 months1
• Identifying back pain as acute or chronic is one of the key processes in determining the source of the pain:
– Acute back pain
• Usually mechanical, often acute in onset, arising from structural changes that may be in the spinal joints, vertebrae or soft tissues
– Chronic back pain
• Can be either mechanical or inflammatory, resulting in chronic back pain lasting >3 months1
Back pain: acute vs. chronic
1. Sieper et al. Ann Rheum Dis 2009; 68:784–788.
It is important to distinguish inflammatory from mechanical back pain as early as possible as the underlying causes are usually
different as is subsequent management and treatment

Comparison of inflammatory and mechanical back pain
1. Sieper, J et al. Ann Rheum Dis 2009; 68:784-788 2.Chien, JJ and Bajwa, ZH. Current pain and headache reports 2008; 12:406-411
IBP
Age at onset <40 years
Insidious onset; less likely to be acute
Pain improves with exercise
Pain does not improve with rest
Pain at night that may wake patient during second half of the night
Morning stiffness >30 minutes
MBP
Age at onset; any age
Variable onset; may be acute
Pain may worsen with movement
Pain often improves with rest

• How long has the patient had back pain?1
• How old was the patient when the back pain started?1
• Is there a family history of AS?2
• Does the pain improve with the use of NSAIDs?1,3
• Has the patient experienced any leg pain, numbness or tingling?• Does the patient have a history of other musculoskeletal problems?4
• Has the patient experienced anterior uveitis (iritis), psoriasis, IBD or peripheral arthritis?3
• What is the usual pattern over a 24 hour period?1 • Has the patient experienced alternating buttock pain?1,5
Important questions to ask a patient with chronic back pain
1. Sieper et al. Ann Rheum Dis. 2009; 68:784–788. 2. Evnouchidou, J Immunol, 2011; 186:1909–13. 3. Braun et al. Ann Rheum Dis, 2011; 70:896–904. 4. Mander, M et al. Ann Rheum Dis 1987; 46:197–202. 5. Rudwaleit et al. Arthritis Rheum 2006; 54:569–578

1
1
1
1
ASAS criteria for identifying inflammatory back pain
Adapted from Sieper et al. Ann Rheum Dis. 2009; 68:784–788.
Inflammatory back pain requiring further investigation is usually indicated if the answer is ‘yes’ to 4 or more of these parameters

Non-radiographic disease
(X-ray –ve)
Radiographic disease
X-ray +vesacroiliitis
Radiographic disease X-ray +ve
sacroiliitis and/or spinal changes
Time (years)
Estimatedproportion of affected individuals
Axial SpA (ASAS criteria)
Ankylosing Spondylitis (mNYC)
MRI -ve
MRI +vesacroiliitis
Patients with chronic back pain ≥3 months and aged <45 years
Axial SpA spectrum of disease
Isdale A, et al. Rheumatology (Oxford). 2013 Dec;52(12):2103-5.
The figure depicts the spectrum of disease in patients with axSpA. The severity of disease progresses with time in a proportion of patients and the sizes of the boxes are estimates of the proportion of patients in each tertile. The first tertile represents early non-radiographic disease, the second and third tertiles represent radiographic disease (AS) with the most severe end of the spectrum including spinal involvement (syndesmophyte formation, fusion or posterior element involvement).

0%
10%
20%
30%
40%
< 1month
1-3months
3-6months
6-12months
1-3years
3-5years
5-10years
10years or
more
Perc
en
tag
e o
f p
ati
en
ts
n=791
Interval between symptom onset and first consultation with GP in patients with AS
Adapted from Hamilton L. et al. Rheumatology 2011;50:1991–1998.
Months Years
Time
+
Although ~60% of patients
consult their GP within 1 year of symptom onset,
~40% wait between 1 and
10+ years

Interval between symptom onset and diagnosis of AS
0%
10%
20%
30%
40%
Pe
rce
nta
ge
of
pa
tie
nts
n=778
<1 1-3 3-6 6-12 1-3 3-5 5-7 7-10 10 +
Months Years
Time
Nearly 40% of patients experience
a delay over >5 years between
symptom onset and diagnosis of AS
Over 20% experience a delay
of 10+ years
Mean delay is 8.57 years
Adapted from Hamilton L, et al. Rheumatology 2011;50:1991–1998

Red flag symptoms of more serious conditions1–3
Source of back pain History Observation/examination
Abdominal aortic aneurysm
• Sudden onset of intermittent/ continuous abdominal pain radiating to the back
• History of cardiovascular disease• Previous collapse
• Pulsating abdominal mass• Low or high blood pressure• Tachycardia (rapid heart beat)
Tumours • Age ≥50 years• History of cancer• Back pain at night and at rest; may
have neurological deficits (if tumour destruction is extensive and causes neurological compression)
• Neurological deficits• Swollen lymph nodes• Systemic symptoms, including
fever/chills and malaise• Unexplained weight loss
Renal disease • Recent UTI• History of kidney stones• History of polycystic kidney
• Associated with history of frequent kidney infections
• UTI: back tenderness, fever/chills, urinary urgency/burning
• Kidney stones: nausea/vomiting, pain radiating to the groin, blood in the urine, possible fever
• Polycystic kidney: back and abdominal tenderness, blood in the urine, increased abdomen size
1. Adapted from BMJ Best Practice. Assessment of back pain. Accessed June 2015. Last updated September 2014. 2. Bangle SD et al. Cleveland Clinic Journal of Medicine. 2009;76:393–399. 3. Differentiating back pain from kidney pain. Available at http://www.integrative-healthcare.org/mt/archives/2006/02/differentiating.html. Accessed June 2015. Last updated February 2006.
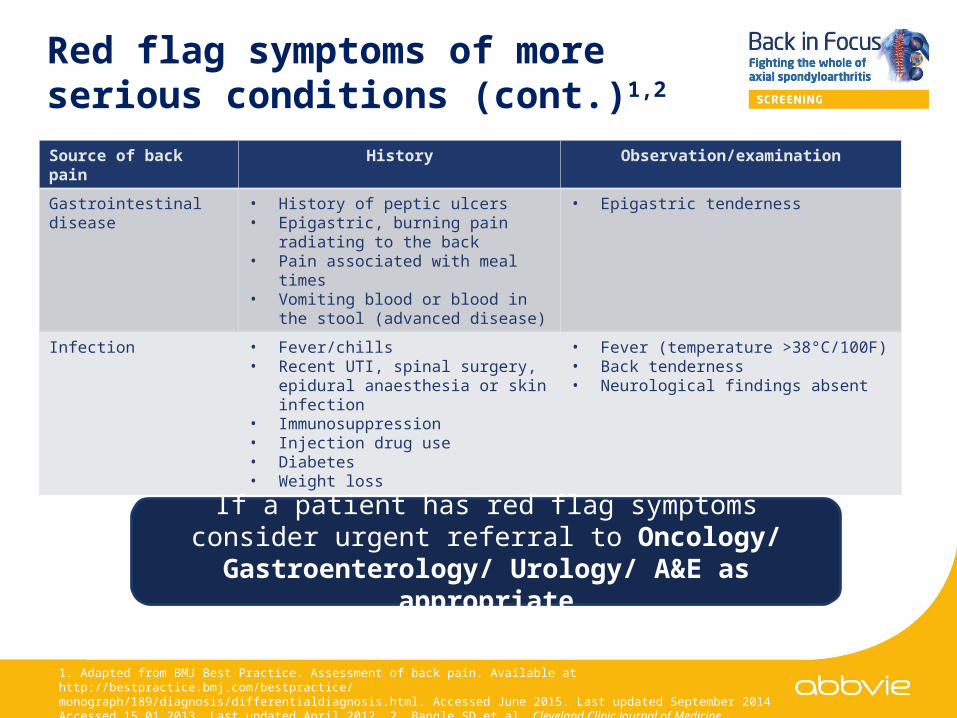
Red flag symptoms of more serious conditions (cont.)1,2
Source of back pain History Observation/examination
Gastrointestinal disease • History of peptic ulcers• Epigastric, burning pain radiating to
the back• Pain associated with meal times• Vomiting blood or blood in the stool
(advanced disease)
• Epigastric tenderness
Infection • Fever/chills• Recent UTI, spinal surgery, epidural
anaesthesia or skin infection• Immunosuppression• Injection drug use• Diabetes• Weight loss
• Fever (temperature >38°C/100F)• Back tenderness• Neurological findings absent
1. Adapted from BMJ Best Practice. Assessment of back pain. Available at http://bestpractice.bmj.com/bestpractice/monograph/189/diagnosis/differentialdiagnosis.html. Accessed June 2015. Last updated September 2014 Accessed 15.01.2013. Last updated April 2012. 2. Bangle SD et al. Cleveland Clinic Journal of Medicine. 2009;76:393–399.
If a patient has red flag symptoms consider urgent referral to Oncology/ Gastroenterology/ Urology/ A&E
as appropriate
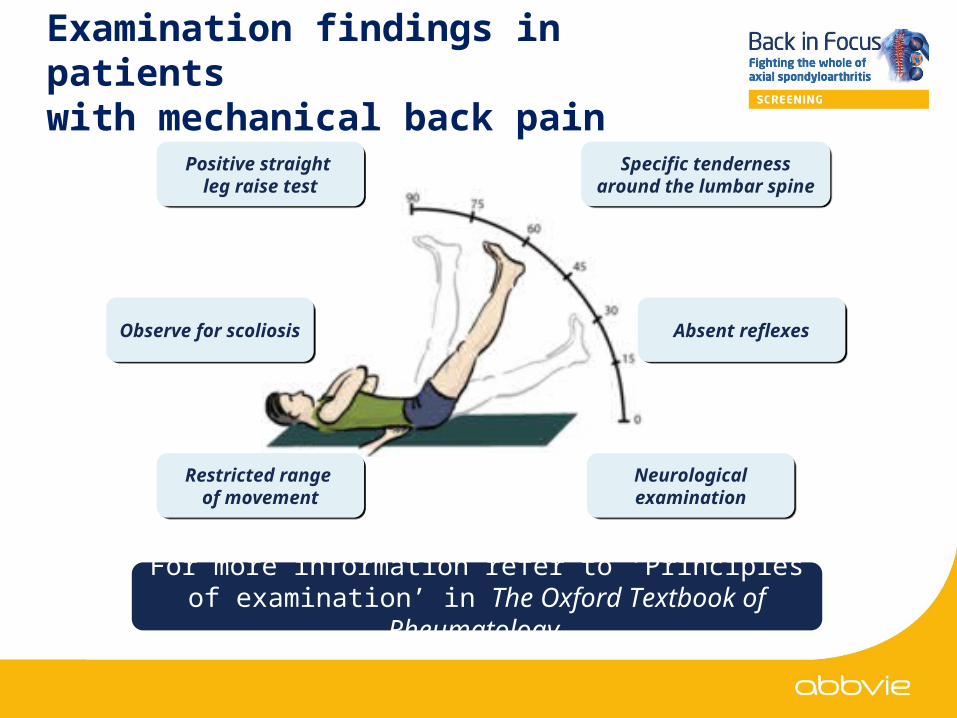
Examination findings in patients with mechanical back pain
Positive straight leg raise test
Positive straight leg raise test
Specific tenderness around the lumbar
spine
Specific tenderness around the lumbar
spine
Absent reflexesAbsent reflexesObserve for scoliosis
Observe for scoliosis
Restricted range
of movement
Restricted range
of movement
Neurological examinationNeurological examination
For more information refer to ‘Principles of examination’ in The Oxford Textbook of Rheumatology

Physical examination is often unremarkable in patients with
inflammatory back pain
Examination findings in patients with inflammatory back pain
Look for other inflammatory conditions such as psoriasis, uveitis, peripheral arthritis,
enthesitis
Neurological examination is essential
Tenderness over enthesitis sites
Observed postural changes
Reduction in the range of
movement in the lumbar spine
Loss of hip abduction
Pain or tenderness over the sacroiliac joint, lumbar spine and/or
thoracic spine

Inflammatory
back pain
Who to refer to
Mechanical
back pain
Based on Braun, J et al. Ann Rheum Dis 2011; 70:896–904.
If IBP is suspected refer to rheumatology
If IBP is suspected refer to rheumatology
If MBP is suspected refer to local musculoskeletal interface service
If MBP is suspected refer to local musculoskeletal interface service

• Back pain is a common reason for primary care consultations
• It is important to be able to distinguish between back pain of mechanical and inflammatory origin as the referral pathways and treatments differ
• ‘Red flags’ should be investigated immediately
Summary
Related Documents











