EFFECTS OF AN IN-CENTER RESISTANCE TRAINING PROGRAM ON FUNCTIONAL MEASURES, STRENGTH, AND QUALITY OF LIFE IN END STAGE RENAL DISEASE ______________________ A Thesis Presented to The Faculty of Springfield College ______________________ In Partial Fulfillment Of the Requirements for the Degree Master of Science ______________________ By Jennifer McKinnon December, 2014

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

EFFECTS OF AN IN-CENTER RESISTANCE TRAINING PROGRAM ON
FUNCTIONAL MEASURES, STRENGTH, AND QUALITY OF LIFE IN
END STAGE RENAL DISEASE
______________________
A Thesis
Presented to The
Faculty of Springfield College
______________________
In Partial Fulfillment
Of the Requirements for the Degree
Master of Science
______________________
By
Jennifer McKinnon
December, 2014

i
Dedication
I am dedicating my thesis to my mother, Cathy, who has
always been a positive role model in my life. My mother
has been a lifelong example of hard work and perseverance.
In the face of adversity and many challenges along the way,
she has always pushed through and did what she had to do to
make things work. She has taught me the importance of hard
work, honesty and integrity, being humble in every
situation, and never giving up. My mother has not lived
the easiest of lives, yet she is constantly pushing
forward, kindly and hopefully, yet never backing down from
her beliefs all the while. She is a strong, beautiful
person inside and out and I can only hope to be the kind of
person she is one day. Thank you, mom, for providing a
wonderful example for me and others in your life, and
instilling in me many of the same virtues and passions that
you have continued to demonstrate.

ii
Acknowledgments
First, I would like to thank Pioneer Valley Dialysis
and the Western Massachusetts Kidney Center for allowing
this study to be done in their facilities. I would also
like to thank all of the patients who volunteered to take
part in the study, despite not always having a great deal
of energy to expend. Next, I would like to thank Dr.
Headley for guiding me in my graduate school experience and
being a great teacher. I would like to thank Dr. Matthews
for all of your help and statistical knowledge. Dr. Dodge,
thank you for your help and allowing the use of the manual
muscle test apparatus for the data collection. A large
thank you to Michael Bruneau for donating so much of your
time, effort, and knowledge throughout the entire research
process. It was incredibly helpful to have your assistance
and support whenever it was needed.
Lastly, I would like to thank Dan Soule for his
endless support throughout the entire graduate school
process. Without your multi-dimensional help the last few
years, I would not be where I am today.
December 2014 J. R. M.

iii
Table of Contents
Page
Dedication . . . . . . . . . . . . . . . . . . . . . . i
Acknowledgments . . . . . . . . . . . . . . . . . . . ii
List of Tables . . . . . . . . . . . . . . . . . . . . v
List of Figures . . . . . . . . . . . . . . . . . . . vii
Abstract . . . . . . . . . . . . . . . . . . . . . . . 2
Introduction . . . . . . . . . . . . . . . . . . . . . 3
Method . . . . . . . . . . . . . . . . . . . . . . . . 7
Subjects . . . . . . . . . . . . . . . . . . . . . 8
Measuring Instruments . . . . . . . . . . . . . . 8
Procedures . . . . . . . . . . . . . . . . . . . . 12
Statistical Analyses . . . . . . . . . . . . . . . 14
Results . . . . . . . . . . . . . . . . . . . . . 14
Discussion . . . . . . . . . . . . . . . . . . . . 18
References . . . . . . . . . . . . . . . . . . . . . . 25
Appendix A. RESEARCH DESIGN . . . . . . . . . . . . . 35
Statement of the Problem . . . . . . . . . . . . 36
Definition of Terms . . . . . . . . . . . . . . 36
Delimitations . . . . . . . . . . . . . . . . . . 39
Limitations . . . . . . . . . . . . . . . . . . . 40
Hypotheses . . . . . . . . . . . . . . . . . . . 40
Appendix B. REVIEW OF LITERATURE . . . . . . . . . . . 41
Frailty . . . . . . . . . . . . . . . . . . . . . 44

iv
Dialysis and Aerobic Training . . . . . . . . . . 53
Muscle Evaluation . . . . . . . . . . . . . . . . 67
Combination Training . . . . . . . . . . . . . . 73
Resistance Training . . . . . . . . . . . . . . . 80
Summary . . . . . . . . . . . . . . . . . . . . . 96
Appendix C. INFORMED CONSENT FORM . . . . . . . . . . 98
Appendix D. MEDICAL HISTORY FORM . . . . . . . . . . . 101
Appendix E. DATA SHEET . . . . . . . . . . . . . . . 103
Appendix F. EXERCISE SHEET . . . . . . . . . . . . . 104
Appendix G. SF-36 . . . . . . . . . . . . . . . . . . 105
Appendix H. SHORT PHYSICAL PERFORMANCE BATTERY. . . . 110
Appendix I. INFORMATIONAL FLYER . . . . . . . . . . . 115
Appendix J. YMCA MEMBERSHIP FORM . . . . . . . . . . 117
Appendix K. STATISTICS TABLES. . . . . . . . . . . . . 118
BIBLIOGRAPHY . . . . . . . . . . . . . . . . . . . . . 138

v
List of Tables
Table Page
1. Descriptive Statistics for Subjects . . . . 29
2. Descriptive Statistics for Short Physical
Performance Battery (SPPB). . . . . . . . . 30
3. Descriptive Statistics for Manual Muscle
Test (MMT) in Pounds. . . . . . . . . . . . 31
K4. 2x2 Mixed Factorial ANOVA Comparing PCS
Scores from the SF-36 Between Baseline
and 8-Weeks . . . . . . . . . . . . . . . .118
K5. 2x2 Mixed Factorial ANOVA Comparing MCS
Scores from the SF-36 Between Baseline
and 8-Weeks . . . . . . . . . . . . . . . .119
K6. 2x3 Mixed Factorial ANOVA Comparing SPPB
Total Balance Scores Over Three Time
Periods for Treatment and Control Groups. .120
K7. 2x3 Mixed Factorial ANOVA Comparing SPBB
Gait Speed Test Scores Over Three Time
Periods for Treatment and Control Groups. .121
K8. 2x3 Mixed Factorial ANOVA Comparing SPPB
Chair Stand Scores Over Three Time Periods
for Treatment and Control Groups. . . . . .122
K9. 2x3 Mixed Factorial ANOVA Comparing SPPB
Total Scores Over Three Time Periods for
Treatment and Control Groups. . . . . . . .123
K10. 2x3 Mixed Factorial ANOVA Comparing Right
Biceps MMT Scores Over Three Time Periods
for Treatment and Control Groups. . . . . .124
K11. 2x3 Mixed Factorial ANOVA Comparing Left
Biceps MMT Scores Over Three Time Periods
for Treatment and Control Groups . . . . . 125
K12. 2x3 Mixed Factorial ANOVA Comparing Right
Shoulder MMT Scores Over Three Time Periods
for Treatment and Control Groups . . . . .126

vi
K13. 2x3 Mixed Factorial ANOVA Comparing Left
Shoulder MMT Scores Over Three Time Periods
for Treatment and Control Groups . . . . .127
K14. 2x3 Mixed Factorial ANOVA Comparing Right
Calf MMT Scores Over Three Time Periods for
Treatment and Control Groups . . . . . . .128
K15. 2x3 Mixed Factorial ANOVA Comparing Left
Calf MMT Scores Over Three Time Periods
for Treatment and Control Groups . . . . .129
K16. 2x3 Mixed Factorial ANOVA Comparing Right
Quadriceps MMT Scores Over Three Time Periods
for Treatment and Control Groups . . . . .130
K17. 2x3 Mixed Factorial ANOVA Comparing Left
Quadriceps MMT Scores Over Three Time Periods
for Treatment and Control Groups . . . . .131
K18. 2x3 Mixed Factorial ANOVA Comparing Right
Hamstrings MMT Scores Over Three Time Periods
for Treatment and Control Groups . . . . .132
K19. 2x3 Mixed Factorial ANOVA Comparing Left
Hamstrings MMT Scores Over Three Time Periods
for Treatment and Control Groups . . . . .133
K20. 2x3 Mixed Factorial ANOVA Comparing Right
Adductor MMT Scores Over Three Time Periods
for Treatment and Control Groups . . . . .134
K21. 2x3 Mixed Factorial ANOVA Comparing Left
Adductor MMT Scores Over Three Time Periods
for Treatment and Control Groups . . . . .135
K22. 2x3 Mixed Factorial ANOVA Comparing Right
Abductor MMT Scores Over Three Time Periods
for Treatment and Control Groups . . . . .136
K23. 2x3 Mixed Factorial ANOVA Comparing Left
Abductor MMT Scores Over Three Time Periods
for Treatment and Control Groups . . . . .137

vii
List of Figures
Figure Page
1. Schematic diagram illustrating study design
and testing session flow. . . . . . . . . . 34

1 Running head: END STAGE RENAL DISEASE
Effects of an In-center Resistance Training Program on
Functional Measures, Strength, and Quality Of Life in End
Stage Renal Disease
Jennifer McKinnon
Springfield College

2
END STAGE RENAL DISEASE
Abstract
The purpose of this study was to examine the effects of an
8-week resistance training program on quality of life,
strength, and functional ability of end-stage renal disease
(ESRD) patients on dialysis. A total of 10 dialysis
patients completed the study with 5 in the training group
and 5 in the control group. Resistance training was
performed in an intra-dialytic setting during the first
hour of dialysis using bands and ankle weights. Patients
exercised major muscle groups which included: biceps,
shoulders, quadriceps, hamstrings, calves, hip
adductors/abductors, and core. Measurements for QOL were
assessed by the SF-36 at baseline and 8-weeks.
Measurements for strength and functional ability were
assessed at baseline, 4-weeks, and 8-weeks, using an MMT
and the SPPB, respectively. 2x2 and 2x3 ANOVA’s with
repeated measures were computed (p = 0.05). Strength
measures improved for the treatment group in the MMT calf,
hamstring, and quadriceps muscles when compared to the
control group. SPPB results demonstrated improvements in
chair stand performance and total score. In conclusion,
resistance training programs are safe and effective for
ESRD patients and can result in strength and functional
improvements.

3
END STAGE RENAL DISEASE
Effects of an In-center Resistance Training Program on
Functional Measures, Strength, and Quality
Of Life in End Stage Renal Disease
The amount of patients with end-stage renal disease
(ESRD) who are treated with dialysis and transplantation in
the United States has risen by over 57% between 1995 and
2010 (Chen et al., 2010). As a result, healthcare
financial expenditure has increased and averages around $28
billion annually. Patients with ESRD are increasingly
sedentary and have low functional abilities compared with
healthy individuals of the same age (Headley et al., 2002).
These components often result in patients becoming quite
frail (Brown & Johansson, 2010). Frailty is characterized
by poor physical performance, weakness, exhaustion,
fatigue, low physical activity, and poor nutrition. In
turn, frailty is also associated with a higher risk of
hospitalization and death for dialysis patients in
particular (Chen et al., 2010). ESRD patients are also at
higher risk for cardiovascular disease and other serious
comorbidities due to their poor overall health state
(Howden, Fassett, Isbel, & Coombes, 2012). Despite various
medical advancements, patients continue to be limited
physically, which results in negative impact on health,
quality of life, activities of daily living, and morbidity
4
END STAGE RENAL DISEASE
and mortality outcomes (Painter, 2005). Thus, researchers
and healthcare providers continue to search for a safe and
effective program to improve these factors.
Strength training, or resistance training, is known to
increase physical performance and functional capacity,
improve muscular strength and function, decrease blood
pressure, and improve inflammation (Chen et al., 2010).
The effects of resistance training can also improve quality
of life, nutrition, and increase independence for dialysis
patients (Chen et al., 2010). The primary focus of care
for dialysis patients is on disease management as opposed
to prevention. Despite research that indicates vast
improvements in this patient population, exercise is still
a very under-utilized tool (Johansen, 2005).
Researchers have examined the effect of exercise on
dialysis patients focusing primarily on aerobic training
(Chen et al., 2010). Peak oxygen uptake (VO2peak) is often
used as the primary measure within these studies. Due to
the fact that VO2peak is a widely recognized physiological
measure pertaining to exercise capacity, it is considered
to be a valid measure of physical function and fitness
(Chen et al., 2010). While several researchers have
reported increases in VO2peak following aerobic training in
this patient population, the increases are somewhat modest

5
END STAGE RENAL DISEASE
and it has not yet been fully established as to how it
actually improves the lives of patients with ESRD (Howden
et al., 2012). Researchers have examined a combination of
resistance and aerobic training, yet the primary emphasis
still tends to remain on the aerobic training portion
(Segura-Orti, Kouidi, & Lison, 2009).
Although some researchers have studied a combination
of aerobic and resistance training, few have focused on
resistance training alone for this population. Muscle
strength is a vital determinant of physical function and
independence in older populations and those with chronic
disease. As previously stated, dialysis patients are weak
compared to healthy individuals. Weakness is a major
limitation to physical function and quality of life for
patients with ESRD. Muscle strength has been shown to be
an important predictor for gait speed and other factors
that impact upon activities of daily living (Segura-Orti et
al., 2009).
The majority of studies involving training ESRD
patients involve a protocol of exercise on non-dialysis
days. The theory behind exercise on non-dialysis days is
that patients are too tired and fatigued during dialysis to
participate in physical activity. Researchers, therefore,
have hypothesized that patients will be more energized and

6
END STAGE RENAL DISEASE
motivated to move on their days off of dialysis (Chen et
al., 2010). However, dialysis patients have been reported
to feel too weak and apprehensive to begin a program due to
complications with their fistula or musculoskeletal injury,
for instance (Chen et al., 2010). As a result, most of
these studies have had low compliance rates from dialysis
patients.
A study that addresses the previously mentioned
barriers is necessary in order to determine the range of
benefits for dialysis patients. Since most researchers
only include subjects who have no other comorbidities, more
current studies should involve frail subjects of an older
age group. According to the American College of Sports
Medicine, this detrained population has the most to gain
from an exercise program (Thompson, Gordon, & Pescatello,
2009). By performing the exercise program within the first
hour or two of dialysis, the compliance component would
also be addressed. The patients would be coming in for
dialysis regardless and would not have to do any extra
driving or take any extra time out of their daily
schedules. Resistance training was chosen for the current
study due to its known effects on musculoskeletal function
and its ability to be done in a primarily seated position.

7
END STAGE RENAL DISEASE
Few studies have examined older dialysis patients due
to their decreased functional ability and higher incidence
of comorbidities. Older and more deconditioned patients,
however, have the most to gain from training. The current
study was designed to examine the impact of an in-center
resistance training program on functional measures,
strength, and quality of life in end-stage renal disease
patients on dialysis. Due to evidence showing that
resistance training builds muscle, the researcher
hypothesized that a resistance training program would
improve functional ability and muscular strength, which in
turn, would also improve quality of life in the ESRD
patient population.
Method
The study was designed to determine the effects of a
resistance training program on dialysis patients over an
eight week period. Effects that were examined include
strength measures, the Short Physical Performance Battery
(SPPB) testing (Freire, Guerra, Alvarado, Guralnik, &
Zunzunegui, 2012) for functional capacity of activities of
daily living, frailty, and the SF-36 for quality of life.
Measurements were taken at baseline, a four-week period
halfway into the training period, and post-training at
eight weeks.

8
END STAGE RENAL DISEASE
Subjects
Patients from the XXXXXXX XXXXXX Dialysis Center and
the XXXXXXX XXXX Kidney Center in Western Massachusetts
were recruited for the current study. The subjects
included 10 (n = 5 in experimental group, n = 5 in usual
care group) patients who were asked to sign an Informed
Consent Form (Appendix C) prior to testing. A
comprehensive medical history was obtained prior to
admission into the study (Appendix D). Subjects whose
physicians did not approve their participation were not
allowed to do the study. Subjects who suffered from any
recent or current musculoskeletal injury and were not
physically able to perform the necessary exercises were
excluded from the study. In total, about 40 patients were
approached during recruitment. Of these, four patients
were not medically cleared for participation.
Measuring Instruments
In this study, the researcher measured strength using
dynamometry. Specifically, the Lafayette Manual Muscle
Testing (MMT) System was used (Model 01165, Lafayette,
Indiana), which is an ergonomic hand-held device for
objectively quantifying muscle strength. The accuracy for
this instrument is determined to be ± 1 % over full scale
or ± 0.2 lbs (Lafayette Instrument Company, 2009). The

9
END STAGE RENAL DISEASE
test is performed with the researcher applying force to the
limb of a patient or subject. The objective of the test is
for the researcher to overcome the patient’s resistance.
The MMT records the peak force and the time required to
achieve the outcome. This dynamometer is portable, easy
and efficient, and offers several different features and
functions. Some of the features include three molded
plastic stirrups with pads, automatic or manual storage of
data, a measurement range of 0-300 lbs, and an LCD display
with different menu options. In a study from Martin and
colleagues (2006), 20 participants (9 men and 11 women)
between the ages of 61 and 81 years were recruited in order
to test the hand-held dynamometer (HHD) against the gold
standard Biodex dynamometry when examining strength
measures. There was a correlation between the measures (r
= 0.91, p < 0.0001) and classification of individuals into
tertiles of muscle strength showed favorable agreement
between the two measurement methods (Kappa =0.69, p <
0.0001) (Martin et al., 2006).
Functional ability and activities of daily living were
measured by The Short Physical Performance Battery (SPPB)
(Brazier et al., 1992). The SPPB is a tool designed to
quantify physical performance and decline over time. The
test focuses primarily on lower extremity function and

10
END STAGE RENAL DISEASE
includes a 4-m walk to measure gait speed, one chair stand
(followed by 5 timed chair stands, if the first is
successfully completed), and balance stands with the feet
held in different positions for 10 s each. The test battery
is designed to be easily administered in a variety of
contexts or settings, can be administered after a short
course of training, and takes about 10 min to complete.
Each test within the battery is scored 0-4 with a maximum
score of 12. Scores are then summed to compute one final,
overall score. The test has been shown to be predictive of
risk of disability among community-dwelling older patients
(Brazier et al., 1992). In addition, use of the test has
predicted patient mortality, the need for admission to a
nursing home and reliance on health care among the general
older population, as well as continued decline in
activities of daily living (ADLs). Additionally, the SPPB
has been successful in predicting the development of
disability (inability to perform ADLs or decreased
mobility) among those individuals who had no disability at
the time of administering the test. Test-retest
reliability was evaluated using individuals over the age of
65 and has a reported Intra-class Correlation Coefficient
(ICC) of .90 with an inter-rater reliability ICC between
.73 and .82 with a 95% confidence interval. Independent
11
END STAGE RENAL DISEASE
samples t-tests were used to compare means and establish
validity, which was analyzed to be high (Freire et al.,
2012).
Quality of life (QOL) was measured using the SF-36
(Medical Outcomes Study, Rand Corporation), which is a
multi-purpose, short-form health survey with 36 questions.
The SF-36 yields an 8-scale profile of functional health
and well-being scores, as well as psychometrically-based
physical and mental health summary measures and a health
utility index. The eight scaled scores are the weighted
sums of the questions from each section and each scale is
directly transformed into a 0-100 scale on the assumption
that each question carries equal weight. It is a generic
measure, as opposed to one that targets a specific age,
disease, or treatment group. Accordingly, the SF-36 has
been useful in surveys of general and specific populations,
comparing the relative burden of diseases, and in
differentiating the health benefits produced by a wide
range of different treatments. Both internal consistency
and test-retest reliability have been shown to be high for
the SF-36 with coefficients greater than .75 and a 95%
confidence interval. Distribution of scores conformed to
expected values for validity demonstrating both internal
and external consistency (Brazier, et al., 1992).

12
END STAGE RENAL DISEASE
Procedures
The subjects (N = 10) were patients from Western
Massachusetts who receive dialysis three times per week for
about 4 hrs each session. Each subject was given detailed
instructions on the exercise protocol prior to testing. An
initial pilot session was used to determine a subject-
specific workload that would elicit a rate of perceived
exertion (RPE) of either 3 or 4 (moderate to somewhat hard)
on a graduated Borg scale of 1 to 10 (Borg, 1970).
Patients performed resistance exercise which encompassed
the major muscle groups. Exercises included: bicep curls,
lateral shoulder raises, anterior shoulder raises, seated
row, triceps extension, bent leg raises, leg extension,
calf raises, hip adduction squeeze, hip abduction, and sit-
to-stands. Postural exercises which included chin tucks
and scapular retractions in addition to core and breathing
exercises where the core is engaged were also part of the
exercise routine. Exercises were performed using ankle
weights, resistance bands, and dumbbells. Exercise
progression was gradual and modifications were sometimes
necessary due to the type of diseased population involved.
Once the RPE was reduced to a 2 for a patient, weight was
increased. Patients were instructed to perform each
exercise once for 8-12 repetitions. Certain exercises

13
END STAGE RENAL DISEASE
(bicep curls, anterior and lateral shoulder raises, row,
and triceps extension) were performed in the waiting room
prior to dialysis due to the motion required. The arm with
the fistula was also worked prior to dialysis in the
waiting room since it cannot be used during. Training was
performed at the beginning of each dialysis session to
ensure minimal fatigue.
A usual care control group (n = 5) was used to assess
differences in effects of training. The control group
proceeded with their typical dialysis care. No resistance
training was performed by this group. The subjects in this
group were given the same testing as the experimental
group.
Testing was performed at baseline, four weeks after
the start of training, and post training after eight weeks.
The testing was performed during the mid-week dialysis
session in order to allow for the most normal bodily fluid
distribution. Differences in strength were assessed using
manual muscle testing at each testing interval. SPPB
testing was used to determine changes in ability for ADL’s
during each testing interval as well. Scores from the SF-
36 were obtained at baseline and post training only to
assess any changes in QOL from the time between the start
of the program and the end of training.

14
END STAGE RENAL DISEASE
Statistical Analyses
Functional ability and strength were measured three
times (pre, mid, & post) and QOL was measured twice (pre &
post). A 2 x 3 mixed factorial ANOVA was computed for
strength and functional ability. This was based on time
(pre, 4 weeks, & 8 weeks) and group (strength, or
experimental, & control). A 2 x 2 mixed factorial ANOVA
was computed for QOL based on SF-36 scores. The alpha
level was set at 0.05 and all statistical analyses were
performed using IBM-SPSS (version 21.0).
Results
The results will be reported in different sections of
the document based on the type of testing. They will be
described in the following subsections; Descriptive
Characteristics of Subjects, SF-36, SPPB, and MMT.
Descriptive Characteristics of Subjects
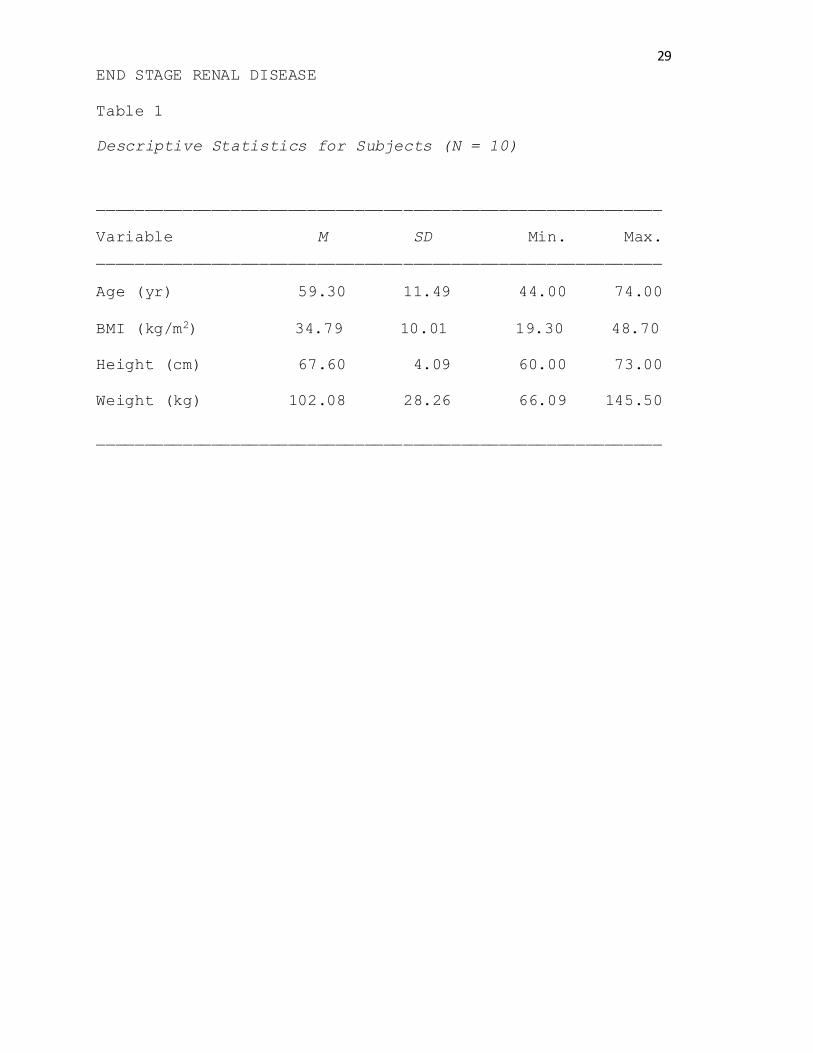
A total of 10 subjects (6 male, 4 female) completed
the study. Subjects ranged in age from 44 to 74 years of
age with a mean age of 59.3 ± 11.5 years. The majority of
subjects were in the overweight to obese category based on
BMI (M = 34.78 kg/m2 ± 10.01 kg/m2). The average height and
weight for the 10 subjects was 67.6 cm ± 4.09 cm and 102.1
kg ± 28.2 kg, respectively. As for ethnicity, 50% of
subjects were Caucasian, 30% were Hispanic, and 20% were

15
END STAGE RENAL DISEASE
African American (Table 1). ANOVA summary tables can be
found in Appendix K.
The QOL variable assessed by the SF-36 health
questionnaire was analyzed with a 2 X 2 mixed factorial
ANOVA. The SPPB and MMT results were analyzed using a 2 X
3 mixed factorial ANOVA. Mauchly’s test of sphericity was
used to test for the basic assumption of homogeneity of
variance when more than two time points were analyzed. If
significant differences existed, the Greenhouse-Geisser
statistic was used to adjust for the degrees of freedom.
Simple effects tests were conducted as post hoc tests for
significant interactions. Results of these analyses are
described below in the following sections; SF-36, SPPB, and
MMT.
SF-36
Results from the SF-36 health and QOL questionnaire
were divided between the physical component score (PCS) and
the mental component score (MCS). Mean PCS baseline scores
were 26.90 ± 7.01 and 32.78 ± 6.96 for treatment and
control groups, respectively. The 8-week mean PCS scores
were 28.88 ± 11.35 and 33.24 ± 2.88 for the treatment and
control groups, respectively. The baseline MCS scores were
55.22 ± 13.68 for the treatment group and 45.02 ± 11.55 for
the control group. The 8-week MCS scores for the treatment

16
END STAGE RENAL DISEASE
group were 58.94 ± 6.61 and 43.86 ± 13.92 for the control
group. No significant interactions or main effects were
found for the MCS or the PCS.
SPPB
No significant interactions existed for total balance,
gait speed, chair stand, and total score. No significant
main effects for time or group existed for total balance
and gait speed. For group, significant differences existed
for the chair stand score and total score. Significant
time effects were found for chair stand and total score.
Significant differences existed between baseline and 8-week
testing as well as 4-week testing and 8-week testing (p =
.03) for the chair stand. The total SPPB score demonstrated
a significant time interaction between baseline and 8-weeks
(p = .05).
MMT
Significant interactions existed for calf (right and
left), quadriceps (right and left), and hamstrings (right
and left). Simple effects tests were conducted to
determine where the significant differences existed. Both
the right and left calf force increased in the treatment
group from baseline to 8-week testing (p = .00 and p = .03,
respectively) while the left calf force also improved from
4-weeks to 8-weeks (p = .01). Both the right and left

17
END STAGE RENAL DISEASE
quadriceps demonstrated significant time effects for the
treatment group between baseline and 8-weeks (p = .00 and p
= .00, respectively). Additionally, significant time
effects existed for the treatment group for the left
quadriceps for baseline to 4-week testing and 4-week to 8-
week testing (p = .00 and p = .01, respectively). There
were significant time effects for the right and left
hamstring force measurements from baseline to 8-weeks (p =
.01 and p = .03, respectively). A significant time effect
also existed for the treatment group from baseline to 4-
weeks for the right hamstring (p = .02). In addition, a
significant time effect existed from 4-weeks to 8-weeks for
the control group (p = .01).
Significant differences were found between groups for
the right calf and the left quadriceps MMT measurements.
The control group demonstrated higher left calf strength
values than the treatment group at baseline (p = .04; A =
20.00, B = 40.86) and for the right quadriceps (p = .02; A
= 28.02, B = 36.74). However, there were no significant
changes over time for the control group. No significant (p
> .05) differences were found for biceps, shoulders, hip
adductors, or hip abductors based on treatment condition.

18
END STAGE RENAL DISEASE
Discussion
The purpose of the research was to determine whether 8
weeks of resistance training would improve strength,
activities of daily living, and quality of life in ESRD
patients on dialysis. The researcher hypothesized that the
strength training protocol would increase strength
measures, increase ability and ease for activities of daily
living, and improve quality of life following 8 weeks (3
times per week) of training the major muscle groups.
Overall, the treatment group demonstrated improvements in
repeated chair stands and total scores for activities of
daily living. Significant treatment group improvements
were also evident in strength scores for hamstrings,
quadriceps, and calves, as demonstrated by the MMT
measurements.
No differences were observed in QOL based on the SF-36
questionnaire following the 8-week training program.
Resistance training is known to increase muscle mass and
strength which can result in increased independence for
frail populations which, in turn, may result in
improvements in quality of life. Dialysis patients often
display lower than average (when compared to healthy
populations) PCS and MCS scores on the SF-36 health-related
quality of life questionnaire. Segura-Orti et al. (2008)

19
END STAGE RENAL DISEASE
found similar results after administering the questionnaire
to 27 dialysis patients who were randomized to either a 24-
week resistance program compared with low intensity aerobic
program. The PCS and MCS sections of the SF-36 at baseline
were found to be lower than the general population. The
intra-dialytic training program did not statistically
affect the SF-36 scores (Segura-Orti et al., 2008). Slight
improvements in the scores were demonstrated, however,
which should be of some value. An increase of 5 points on
the PCS has been associated with a 10% increased survival
(DeOreo, 1997). The minimal clinically important
difference (MCID) is defined as the minimal difference in
scores of an outcome measure that is perceived by patients
as beneficial or harmful (Keurentjes et al., 2012). The
MCID value for the SF-36 is different depending on the
patient population but ranges from 3-5 score units for ESRD
patients (Pagels, Soderkvist, Medin, Hylander, & Heiwe,
2012). In the current study, the treatment group
demonstrated differences for both PCS and MCS score domains
between baseline and 8-week testing. The scores were
indicative of meeting the MCID value (PCS baseline = 26.90
± 7.01 and 8 week = 28.88 ± 11.35; MCS baseline =
55.22±13.68 and 8-week = 58.94 ± 6.61).

20
END STAGE RENAL DISEASE
The SPPB has been used to determine the functional
ability especially for very frail populations. The test
battery includes balance, gait, and lower body strength,
all scored together for a total overall score. After the
8-week resistance training protocol, the lower body
strength (tested by repeated chair stands) and the total
overall scores were improved for the training group and no
differences observed in the control group. This is in
accordance with the MMT results which demonstrated
significant improvements for lower body muscle groups
(calves, quadriceps, and hamstrings) and will be discussed
in detail later. Segura-Orti et al. (2008) found that
resistance training during hemodialysis resulted in
improvements in METs and physical performance testing (sit-
to-stand-to-sit tests and 6-min walk tests) after 24 weeks
of training. Although no differences were observed in
change over time between the two groups, a significant
change was observed in intragroup analysis for the training
group. After 8-weeks of training, the researcher
demonstrated differences for the repeated chair stands
(between baseline and 8-weeks and between 4-week and 8-week
testing) and total scores (between 4-week testing and 8-
week testing). Physical limitation has been shown by low
SPPB scores, which has been shown to predict disability

21
END STAGE RENAL DISEASE
when scores are less than 7 (Chen et al., 2010). In
addition, a change in SPPB scores of one point has been
found to be clinically meaningful for functional capacity
(Chen et al., 2010). Findings for the current study
demonstrated treatment group scores at baseline increasing
from an average of 4.40 ± 2.97 to 6.40 ± 2.61 (p = .03)
after completion of the 8-week training program. These
findings indicate improvements for this population in only
8 weeks which could be beneficial for functional ability in
a very frail population.
Dynamometry is one of the most common ways to assess
muscle strength and the MMT is a portable, easy, and
accurate form of measurement. While no differences were
evident in bicep or shoulder strength in the current study,
lower body strength improved after 8 weeks of training in
the treatment group. A low intensity intra-dialytic
strength training study exhibited significant improvements
from baseline in knee extensor strength with twice weekly
sessions for 48 sessions total (Chen et al., 2010). Lower
body exercises were performed using ankle weights with two
sets of eight repetitions for each exercise. Headley et
al. (2002) also demonstrated increased strength and
functional capacity after 12 weeks of resistance training
in patients with ESRD; however, the training protocol was
22
END STAGE RENAL DISEASE
performed outside of the dialysis center on non-dialysis
days. Results from the current study demonstrate that
significant strength differences are possible after only
eight weeks of training, with some effects seen in only
four weeks. For instance, a significant interaction was
observed between baseline testing and 8-week testing and 4-
week testing and 8-week testing in the left calf for the
treatment group. Also, left hamstring results demonstrated
an interaction between 4-week testing and 8-week testing
for the treatment group.
A limitation of the current study was the potential
variability between MMT measurements since this was reliant
on the tester strength overcoming the patient strength. To
address this issue, the same tester was used for each
patient throughout the three testing periods in order to
minimize error. Another limitation was that the SPPB is
more commonly used for very old and frail populations.
Since there was a range of fitness levels between the
patients, this may have not been the most appropriate test
to use for functional ability. Finally, the study may have
also been limited by the small sample size.
Currently, a randomized control study (Bennett,
Breugelmans, Chan, Calo, & Ockerby, 2012) is underway in
Australia to examine the impact of an exercise physiologist

23
END STAGE RENAL DISEASE
coordinated resistance exercise program on the physical
function of dialysis patients. A total of 180 participants
will be recruited from 15 hemodialysis clinics and will
consist of three groups in which patients will be allocated
to either 12, 24, or 36 weeks of the exercise intervention
(Bennett et al., 2013). The intervention will consist of
six lower body resistance exercises using resistance bands
and tubes and will be done in a seated position during the
first hour of dialysis treatment. The primary outcomes are
physical function, quality of life, cost-utility analysis,
falls risk, medication use, blood pressure, and morbidity.
Results of the study are expected to determine whether it
is effective to employ the use of an accredited exercise
physiologist supervised resistance training program for
dialysis patients, as well as the cost-utility of exercise
physiologists in dialysis centers (Bennett et al., 2013).
Studies like Bennett et al. (2013) and the current study
could show the benefits and efficacy of utilizing exercise
physiologists in dialysis centers, something that has not
been tested in this patient population.
In conclusion, an 8-week, intra-dialytic resistance
training program demonstrated strength improvements in
hamstring, quadriceps, and calf muscle groups.
Additionally, the current resistance training program also

24
END STAGE RENAL DISEASE
showed significant improvements in functional ability for
repeated chair stands and total scores for the SPPB. In
order to demonstrate improvements in quality of life
measures and other strength measures, future studies may
want to explore longer training periods, a larger sample
size, and possibly utilize a program with some combination
of resistance and aerobic exercise. No injuries were
reported during this study, also demonstrating that a
properly supervised, progressive resistance training
protocol is safe for dialysis patients.

25
END STAGE RENAL DISEASE
References
American College of Sports Medicine. Thompson, W. R.,
Gordon, N. F., Pescatello, L. S. (2009). ACSM’s
Guidelines for Exercise Testing and Prescription.
Philadelphia: Lippincott Williams & Wilkins.
Bennett, P. N., Breugelmans, L., Chan, D., Calo, M., &
Ockerby, C. (2013). A Combined Strength and Balance
Exercise Program to Decrease Falls Risk in Dialysis
Patients: A Feasibility Study. Journal Of Exercise
Physiology Online, 15(4), 26-39.
Borg, G. (1970). Institute of Applied Psychology: Self
Appraisal of Physical Performance Capacity. Reports
from the institute of applied psychology, The
University of Sweden, 32(e-book).
Brazier, J., Harper, R., Jones, N., O'Cathain, A., Thomas,
K., Usherwood, T., & Westlake, L. (1992). Validating
the SF-36 health survey questionnaire: New outcome
measure for primary care. British Medical Journal
(Clinical Research Ed.), 305(6846), 160-164.
Brown, E., & Johansson, L. (2010). Old age and frailty in
the dialysis population. Journal of Nephrology, 23(5),
502-507.
Chen, J., Godfrey, S., Ng, T., Moorthi, R., Liangos, O.,

26
END STAGE RENAL DISEASE
Ruthazer, R., & ... Castaneda-Sceppa, C. (2010).
Effect of intra-dialytic, low-intensity strength
training on functional capacity in adult haemodialysis
patients: A randomized pilot trial. Nephrology,
Dialysis, Transplantation: Official Publication of The
European Dialysis and Transplant Association -
European Renal Association, 25(6), 1936-1943.
doi:10.1093/ndt/gfp739
DeOreo, P. B. (1997). Hemodialysis patient-assessed
functional health status predicts continued survival,
hospitalization, and dialysis-attendance compliance.
American Journal Of Kidney Diseases: The Official
Journal Of The National Kidney Foundation, 30(2), 204-
212.
Freire, A., Guerra, R., Alvarado, B., Guralnik, J., &
Zunzunegui, M. (2012). Validity and reliability of the
short physical performance battery in two diverse
older adult populations in Quebec and Brazil. Journal
of Aging and Health, 24(5), 863-878.
doi:10.1177/0898264312438551
Headley, S., Germain, M., Mailloux, P., Mulhern, J.,
Ashworth, B., Burris, J., & ... Jones, M. (2002).
Resistance training improves strength and functional
measures in patients with end-stage renal disease.

27
END STAGE RENAL DISEASE
American Journal of Kidney Diseases: The Official
Journal of The National Kidney Foundation, 40(2), 355-
364.
Howden, E., Fassett, R., Isbel, N., & Coombes, J. (2012).
Exercise training in chronic kidney disease patients.
Sports Medicine (Auckland, N.Z.), 42(6), 473-488.
doi:10.2165/11630800-000000000-00000
Johansen, K. (2005). Exercise and chronic kidney disease:
Current recommendations. Sports Medicine (Auckland,
N.Z.), 35(6), 485-499.
Keurentjes, J. C., Van Tol, F. R., Fiocco, M., Schoones, J.
W., & Nelissen, R. G. (2012). Minimal clinically
important differences in health-related quality of
life after total hip or knee replacement: A systematic
review. Bone and Joint Research, 1(5), 71-77.
Lafayette Instrument Company. (2009). Lafayette manual
muscle testing system. Retrieved from:
http://www.lafayetteevaluation.com/product_detail.asp?
itemid=26
Martin, H. J., Yule, V. V., Syddall, H. E., Dennison, E.
M., Cooper, C. C., & Sayer, A. (2006). Is hand-held
dynamometry useful for the measurement of quadriceps
strength in older people? A comparison with the gold
28
END STAGE RENAL DISEASE
standard biodex dynamometry. Gerontology, 52(3), 154-
159. doi:10.1159/000091824
Pagels, A. A., Soderkvist, B. K., Medin, C., Hylander, B.,
& Heiwe, S. (2012). Health-related quality of life in
different stages of chronic kidney disease and at
initiation of dialysis treatment. Health and Quality
Of Life Outcomes, 1071.
Painter, P. (2005). Physical functioning in end-stage renal
disease patients: Update 2005. Hemodialysis
International. International Symposium on Home
Hemodialysis, 9(3), 218-235.
Segura-Ortí, E., Kouidi, E., & Lisón, J. (2009). Effect of
resistance exercise during hemodialysis on physical
function and quality of life: Randomized controlled
trial. Clinical Nephrology, 71(5), 527-537.
Thompson, W., Gordon, N., & Pescatello, L. (2009). A
preview of ACSM’s guidelines for exercise testing and
prescription, eighth edition. ACSM’s Health and
Fitness Journal, 13(4), 23-26.
29
END STAGE RENAL DISEASE
Table 1
Descriptive Statistics for Subjects (N = 10)
___________________________________________________________
Variable M SD Min. Max.
___________________________________________________________
Age (yr) 59.30 11.49 44.00 74.00
BMI (kg/m2) 34.79 10.01 19.30 48.70
Height (cm) 67.60 4.09 60.00 73.00
Weight (kg) 102.08 28.26 66.09 145.50
___________________________________________________________

30
END STAGE RENAL DISEASE
Table 2
Descriptive Statistics for Short Physical Performance
Battery (SPPB)
___________________________________________________________
Variable Baseline 4 Week 8 Week
___________________________________________________________
Balance T 2.00±1.58 2.60±0.89 3.20±1.10
C 3.40±0.89 3.60±0.55 3.40±0.89
Gait Speed T 1.50±0.58 1.25±0.50 1.25±0.50
C 1.00±0.00 1.00±0.00 1.20±0.45
Chair Stands T 1.00±1.00 1.20±1.30 2.00±1.87
C 1.60±0.89 2.00±1.22 2.20±1.48
Total T 4.40±2.97 5.00±2.55 6.40±2.61
C 6.40±0.89 6.60±1.67 6.80±2.49
___________________________________________________________
T = Treatment Group, C = Control Group. Values represented
in M ± SD, p < .05.
Each score was based on time in seconds

31
END STAGE RENAL DISEASE
Table 3
Descriptive Statistics for Manual Muscle Test (MMT) in
Pounds (N = 10)
___________________________________________________________
Variable Group Baseline 4 Week 8 Week
___________________________________________________________
Biceps
Right T 32.44±5.98 35.84±8.16 46.96±9.63
C 27.88±5.98 32.14±8.16 30.28±9.63
Left T 29.66±6.91 27.54±6.54 38.00±6.90
C 31.32±6.91 32.14±6.54 30.94±6.90
Shoulder
Right T 31.86±8.36 31.28±6.75 32.50±6.39
C 32.80±8.36 29.80±6.75 29.40±6.39
Left T 30.14±7.02 31.60±6.96 31.62±4.62
C 28.68±7.02 23.38±6.96 25.70±4.62
Calf
Right T 20.00±5.98 25.66±5.05 33.36±5.69a
C 40.86±5.98* 32.94±5.05 36.82±5.69
Left T 19.84±7.81 23.24±2.73c 25.20±4.97a
C 37.24±7.81 28.56±2.73 30.58±4.97
Quadriceps
Right T 28.02±2.12 32.94±5.42 40.72±4.82a
C 36.74±2.12 38.40±5.42 35.18±4.82

32
END STAGE RENAL DISEASE
Left T 23.22±5.94b 28.74±4.67c 41.82±4.78a
C 34.30±5.94* 33.40±4.67 30.22±4.78
Hamstrings
Right T 21.56±4.67 35.36±5.52c 34.80±3.44a
C 27.84±4.67 26.54±5.52 26/80±3.44
Left T 23.18±4.60 32.36±6.52 33.06±5.48a
C 31.91±20.18 25.42±14.24c 31.86±15.65
Adductors
Right T 23.40±6.54 26.26±6.21 29.20±4.70
C 29.14±15.75 23.78±12.53 23.46±6.45
Left T 23.42±7.80 23.84±7.46 29.04±3.29
C 25.50±21.17 19.36±8.63 20.94±8.22
Abductors
Right T 27.78±8.00 32.50±9.48 36.80±12.32
C 34.20±19.74 32.32±17.74 31.16±7.23
Left T 29.18±12.92 36.64±11.82 38.62±6.83
C 29.40±8.50 31.18±20.15 27.80±8.30
___________________________________________________________
* Control significantly greater than treatment
a – 8-week significantly greater than baseline
b – 4-week significantly greater than baseline
c – 8-week significantly greater than 4-week

33
END STAGE RENAL DISEASE
Figure Caption
Figure 1. Schematic diagram illustrating study design and
testing session flow.

34
END STAGE RENAL DISEASE
35
END STAGE RENAL DISEASE
Appendix A
RESEARCH DESIGN
Patients with end stage renal disease (ESRD) are
increasingly sedentary and have low functional abilities
compared with healthy individuals of the same age (Headley
et al., 2002). Many dialysis patients, especially older
patients, can be classified as frail (Chen et al., 2010).
Frailty is characterized by poor physical performance,
weakness, exhaustion and fatigue, low physical activity,
and poor nutrition. Frailty, in turn, is also associated
with a higher risk of hospitalization and death for
dialysis patients in particular (Chen et al., 2010).
Despite various medical advancements, patients continue to
be limited physically, which then results in a negative
impact on health, quality of life, activities of daily
living, and morbidity and mortality outcomes (Painter,
2005).
Strength training, or resistance training, is known to
increase physical performance and functional capacity,
improve muscular strength and function, decrease blood
pressure, and improve markers of inflammation (Chen et al.,
2010). Resistance training can also improve quality of
life, nutrition, and independence for dialysis patients
(Chen et al., 2010). The primary focus of care for

36
END STAGE RENAL DISEASE
dialysis patients is on disease management as opposed to
prevention. Despite the research that indicates vast
improvements in this patient population, exercise is still
a very under-utilized tool (Johansen, 2005).
Statement of the Problem
The current study was designed to measure the changes
in strength, functional ability, and quality of life in
ESRD patients on dialysis following an in-center resistance
training program. The researcher measured strength,
functional ability, and quality of life over an eight week
in-center training session.
Definition of Terms
Several terms were utilized in this study, which include:
Activities of Daily Living
Activities of daily living (ADL’s) include any basic
self-care tasks that one must do on a daily basis. These
include tasks such as eating, dressing, bathing, using a
restroom, and rising from a seated position, among others
(Segura-Ortí, Kouidi, & Lisón, 2009).
Dialysis
Dialysis is the process of separating smaller solute
molecules from larger ones in a solution by means of
diffusion through a selectively permeable membrane, used to

37
END STAGE RENAL DISEASE
filter the blood of metabolic wastes, urea, and excessive
ions (Craig & King, 2006).
End Stage Renal Disease
The fifth stage of chronic kidney disease (CKD), end
stage renal disease is the loss of kidney function, usually
requiring dialysis (Johansen, 2005).
Fistula
The National Kidney Foundation (NKF) defines a fistula
as a dialysis access port that is made by joining an artery
to a vein under the skin in order to make a bigger blood
vessel (Smart & Titus, 2011).
Frailty
Brown and Johansson (2010) defined frailty as a
syndrome involving the decline of multiple systems, where
physiological instability leaves the individual at risk for
loss of, or further deterioration in, function when exposed
to perceived minor stressors, such as cold weather. It
encompasses 3 of the following 5 features: weight loss
(unintentional weight loss of at least 5% of the previous
year’s body weight), weakness (determined by grip
strength), slow walking speed, low physical activity and
self-reported exhaustion.

38
END STAGE RENAL DISEASE
Functional Ability
Painter (2005) defined physical functioning and
functional ability as a multi-factorial approach
encompassing many individual factors that comprise an
individuals’ ability to perform activities of daily living
independently.
Quality of Life
The term quality of life (QOL) is a multi-dimensional
approach that references the general well-being of
individuals. The term is used in a wide range of contexts,
including the fields of development and healthcare (Felce &
Perry, 1995).
Resistance Training
Resistance training is defined as a method of exercise
designed to enhance musculoskeletal strength, power, and
local muscular endurance. Resistance training encompasses
a wide range of training modalities including, weight
machines, free weights, medicine balls, elastic cords or
bands, and body weight. Resistance training will be
operationally defined as the strength enhancing modality of
performing exercises using free weights for the upper body
and ankle weights for the lower body (Bulckaen et al.,
2011).

39
END STAGE RENAL DISEASE
Strength
Strength is a measurement of external force production
by a human subject in a specific exercise, such as knee
extension or hand grip, and may be performed either
statically or dynamically, the latter in either concentric
or eccentric mode, at a specified angular velocity (Chen et
al., 2010). Dynamometry will be operationally defined as
the isometric measurement of muscle strength using manual
muscle testing (MMT) with a hand-held device (Martin et
al., 2006).
Delimitations
The current study was delimited by the following factors.
1. Only subjects who were medically cleared and signed
a consent form were included in the study.
2. Only subjects who were diagnosed with chronic
kidney disease and were currently on dialysis were included
in the study.
3. Subjects involved in this study were from the
Western Massachusetts area.
4. Only subjects with no significant musculoskeletal
injury or limitation which restricted the ability to
perform the required exercises were included in this study.

40
END STAGE RENAL DISEASE
Limitations
Certain limitations should be taken into consideration when
interpreting the results of this research.
1. No attempt was made to control for any other pre-
existing conditions or comorbidities so as not to leave out
a patient population that had the most potential for
benefit derivation.
2. The results of the investigation were limited to
the accuracy of the instrument used during testing.
3. The effort from the subjects could not be
controlled during training and testing sessions.
Hypotheses
The following hypotheses were tested within the context of
this research investigation:
1. No significant mean difference in mean strength,
functional scores, and quality of life scores would exist
between baseline and post-training.
2. No significant mean difference in mean strength,
functional scores, and quality of life scores would exist
between the training group and the control group.
3. No significant group by time interaction would
exist for strength, functional scores, or quality of life
scores in the ESRD subjects.

41
END STAGE RENAL DISEASE
Appendix B
REVIEW OF LITERATURE
The number of patients with end-stage renal disease,
(ESRD) treated with dialysis and transplantation in the
United States, has risen by over 57% over the last fifteen
years (Chen et al., 2010). This has resulted in increased
healthcare financial expenditure that averages around $28
billion annually (Chen et al., 2010). Patients with ESRD
are increasingly sedentary and have low functional
abilities compared with healthy individuals of the same age
(Headley et al., 2002). Frailty is characterized by poor
physical performance, weakness, exhaustion and fatigue, low
physical activity, and poor nutrition. This, in turn, is
also associated with a higher risk of hospitalization and
death for dialysis patients in particular (Chen et al.,
2010). ESRD patients are also at higher risk for
cardiovascular disease and other serious comorbidities due
to their poor overall health state (Howden, Fassett, Isbel,
& Coombes, 2012). Despite various medical advancements,
patients continue to be limited physically, which then
results in negative impacts on health, quality of life,
activities of daily living, and morbidity and mortality
outcomes (Painter, 2005).

42
END STAGE RENAL DISEASE
Strength training, or resistance training, is known to
increase physical performance and functional capacity,
improve muscular strength and function, decrease blood
pressure, and improve inflammation (Chen et al., 2010).
The effects of resistance training can also increase
quality of life, nutrition, and independence for dialysis
patients (Chen et al., 2010). The primary focus of care
for dialysis patients is on disease management as opposed
to prevention. Despite the research that indicates vast
improvements in this patient population, exercise is still
a very under-utilized tool (Johansen, 2005).
Most of the studies that have looked at the effect of
exercise on dialysis patients have focused on aerobic
training. VO2peak is often used as the primary measure
within these studies. Due to the fact that VO2peak is a
widely recognized physiological measure pertaining to
exercise capacity, it is considered to be a valid measure
of physical function and fitness. While several studies
have reported increases in VO2peak following aerobic training
in this patient population, the increases are somewhat
modest and it has not yet been fully established as to how
it actually improves the lives of patients with ESRD
(Johansen, 2005). Other studies have done a combination of

43
END STAGE RENAL DISEASE
resistance and aerobic training, yet the primary emphasis
still tends to remain on the aerobic training portion.
Fewer studies have focused on resistance training
alone for this population. Muscle strength is a vital
determinant of physical function and independence in older
populations and those with chronic disease. As previously
stated, dialysis patients are weak compared to healthy
individuals. Weakness is a major limitation to physical
function and quality of life for patients with ESRD.
Muscle strength has been shown to be an important predictor
for gait speed and other factors of activities of daily
living (Johansen, 2005).
The majority of studies involving training ESRD
patients involve a protocol of exercise on non-dialysis
days. The theory behind this is that dialysis patients are
too tired and fatigued during dialysis to partake in
physical activity. Therefore, it is often thought that
they will be more energized and motivated to move on their
days off of dialysis. However, dialysis patients have been
reported to feel too weak and nervous to begin a program
due to complications with their fistula or musculoskeletal
injury, for instance (Johansen, 2005). Therefore, these
studies have had low compliance rates from the patients to
even begin a program.

44
END STAGE RENAL DISEASE
Upon review of the literature on this topic, studies
which look at aerobic training on non-dialysis days seems
to be the most common type. Other studies have looked at a
combination of aerobic and resistance training. Even fewer
have looked at such variables as resistance training or
intra-dialytic training. The following studies discuss some
form of exercise training for dialysis patients and the
outcome variables that follow as a result.
Frailty
Since dialysis management has been changing over time
as a result of the age changes in the dialysis population,
there are many overlapping problems with gerontology and
nephrology care (Brown & Johansson, 2010). Frailty is
common in dialysis patients at any age, but especially so
for older dialysis patients. It is now considered to be a
more sensitive marker of morbidity and mortality than
chronological age alone (Brown & Johansson, 2010).
Integration of the geriatric concept of frailty into
dialysis care has major potential to improve identification
of high risk patients. Johansen, Chertow, Jin, and Kutner
(2007) used data from the U.S. Renal Data System (USRDS) to
determine the prevalence and predictors of frailty among
dialysis patients and to discover the degree to which
frailty was linked with death and hospitalizations.

45
END STAGE RENAL DISEASE
Primary outcome variables included time to death, time to
first all-cause hospitalization or death, or time to first
non-vascular access-related hospitalization or death up to
one year after study enrollment (Johansen et al., 2007).
A total of 2,275 patients were included in an analytic
cohort who completed the patient questionnaire from the
Dialysis Morbidity and Mortality Study (DMMS). This was a
prospective study of 3,931 dialysis patients (approximately
equally distributed between hemodialysis and peritoneal
dialysis) who started therapy in 1996 or early 1997.
Questionnaires were distributed by dialysis unit personnel
and included demographic information, comorbid conditions,
quality of life (SF-36), nutritional status, pre-ESRD care,
and laboratory data. For frailty, a score of < 75 on the
PF scale of the SF-36 was used for a marker of weakness and
slowness while a score of <55 on the vitality scale of the
SF-36 was used to define poor endurance or exhaustion
(Johansen et al., 2007). About two thirds of the subject
population met the criteria for being frail (Johansen et
al., 2007). Age was found to be related to frailty, yet a
significant number of patients from younger age groups were
also found to be frail (including 44% of patients under 40
years of age and more than half of patients between the
ages of 40 and 50) and women were more likely to be frail

46
END STAGE RENAL DISEASE
than men in all age groups (Johansen et al., 2007). In
addition, frailty was more common in patients with comorbid
conditions and patients on hemodialysis were more likely to
be frail than patients on peritoneal dialysis (Johansen et
al., 2007).
Following univariate analysis, the frail patients were
over three times as likely to die within one year, than
those who were not classified as frail. The frail patients
were also more likely to be hospitalized for any reason or
die when compared with those who were not considered to be
frail (Johansen et al., 2007). The results were not
significantly different when limited to patients who were
over the age of 65 years (Johansen et al., 2007). The
study showed that a very high proportion of ESRD patients
met the definition of frailty and that frailty was found to
be predictive of poor outcomes among this patient
population. However, there were some limitations from this
study which included no longitudinal evaluation, no blood
samples were obtained to explore links, and the particular
patient cohort was slightly younger and healthier than the
general ESRD population.
Lo, Chiu, and Sarbjit (2008) designed a prospective
cohort study to examine the links between elderly dialysis
patients and changes in functional status associated with

47
END STAGE RENAL DISEASE
hospitalization. Since so many older dialysis patients
experience high levels of mortality and morbidity, frailty
and functional limitations commonly coincide with this
patient population. Acute hospitalization is a determinant
of functional disability in the general population and is
predictive of mortality and/or the need for long-term care
(Lo et al., 2008). Due to high rates of disability and
functional impairment in dialysis patients, the researchers
composed a pilot study to examine functional limitations at
the time of hospital admission and one week following
discharge in dialysis patients who were admitted to a
single acute care setting in a three month period.
All patients (n = 30) were 65 years of age or older
and completed both baseline and post-discharge assessments.
Baseline data was collected and included age, sex, cause of
end-stage renal disease, reason for admission, and living
circumstances prior to admission. Patients were assessed
within 24 hours of being admitted to the hospital and again
one week after discharge. Testing included the 4-item
Basic Activity of Daily Living (BADL) measure, the Lawton-
Brody Scale of Instrumental Activities of Daily Living
(IADL), the timed up-and-go (TUG) physical performance test
and grip strength, and cognitive function testing using the
Trails A & B tests and the clock test. Data were

48
END STAGE RENAL DISEASE
summarized as mean +/- SD or median and quartiles when
appropriate and all analyses were performed using SPSS,
version 11.0 with 95% confidence intervals (Lo et al.,
2008).
The mean age of subjects who completed the testing was
73.8 +/- 5.9 years with the most common cause for renal
disease being diabetes (Lo et al., 2008). The main reason
for hospitalization varied and ranged from fluid overload
to stroke and diabetes complications. The median length of
time for the hospital stay was four days with a range from
1-29 days (Lo et al., 2008).
At the time of admission, 8 of the 30 subjects
reported being independent with BADLs which included
bathing, dressing, and walking, etc. while no patient
reported complete independence with IADLs which included
such things as driving, meal preparation and housework, and
finances. Both BADL and IADL scores were lower at
discharge in comparison with admission (BADL, 13.9 +/- 2.8
and 13.1 +/- 2.3, P = 0.001; IADL, 13.3 +/- 2.5 and 12.2
+/- 2.5, P = 0.0001) (Lo et al., 2008). A total of 22 out
of 30 patients reported a decline in either BADL or IADL
scores between hospital admission and one week after
discharge. Additionally, one week following discharge,
only three out of the eight patients who initially reported

49
END STAGE RENAL DISEASE
independence with BADLs reported still being independent
(Lo et al., 2008). Patients exhibited a significant
decline in lower limb and upper limb muscle strength when
tested using the TUG and hand grip tests. The patients
reported increased difficulty with basic personal care and
experienced an average slowing in gait of 20% +/- 10.9% (Lo
et al., 2008). Cognitive function testing also showed
trends toward deterioration, but did not reach statistical
significance (Lo et al., 2008).
The results of this study postulate declines in
physical and mental function in the dialysis patients being
observed. The researchers summarized that elderly dialysis
patients are especially prone to functional decline, as is
even more evident at the time of hospitalization. The
biggest limitation of this study was the assessment of
function at the time of admission, as opposed to prior to
admission, because it may result in an underestimation of
the impact that hospitalization has on functional abilities
and independence. The researchers concluded that more
research should be performed and development of a
preventative and rehabilitative intervention for the
dialysis population is essential.
Falls are a major problem in older people, especially
older dialysis patients, and are a predictor of future

50
END STAGE RENAL DISEASE
hospitalization, functional decline, and other health
risks. Cook et al. (2006) used a prospective cohort study
to determine the incidence of falls and proportion of
dialysis patients who fall during a one year period.
Patients over the age of 65 years and undergoing chronic
hemodialysis were used to document the resultant morbidity
and mortality of this patient population and to identify
fall risk factors for this group. A fall was defined by
researchers as an event that resulted in a patients’ coming
to rest inadvertently on the ground or other lower level.
In contrast, an injurious fall was defined as those that
caused minor (cuts or bruises) or major (fractures or
hospitalizations) injuries (Cook et al., 2006).
All consenting patients (n = 168) participated in a
full clinical evaluation. This evaluation included:
Assessment of depressive symptoms using the Mental Health
Inventory, a cognitive assessment using the Folstein Mini-
Mental Status Examination and clock drawing task,
assessment of falls which included recalling events from
the previous 12 months, fear of falling, and falls
efficacy, a vision assessment, hearing assessment, foot
abnormality assessment, and an assessment of orthostatic
blood pressure and heart rate. In addition, each patient
was also asked to perform the timed up-and-go (TUG) test in

51
END STAGE RENAL DISEASE
order to evaluate functional mobility. The patients were
then visited by a research nurse every two weeks in order
to determine whether or not the patients had fallen.
Data were analyzed using descriptive statistics in the
form of mean +/- standard deviation. A total of 151 (93%)
dialysis patients attempted the TUG test. Of these, 75
patients were able to perform the test appropriately and 58
(77%) of those patients achieved a score that was
considered to be low risk for falls (< 15 s). Out of the
last 76 patients that could not complete the test, 43
required a cane, 12 required a walker, and 21 required
additional assistance with walking (Cook et al., 2006).
The patients were followed for a median of about 468 days
during which a total of 305 falls occurred among 76
patients over a period of 190.5 person years with a fall
incidence rate of 1.60 falls per person year and an average
of 2.78 falls per person. Out of the 76 patients who
experienced a fall, 45 (57%) had multiple falls of two or
more with a range of 2 to 48 (Cook et al., 2006).
Walking (indoors; n = 91, outdoors; n = 41) was found
to be the most common activity at the time of falls for
patients. Additionally, there was a high prevalence of
falls when patients stood from a seated position (n = 72)
and when rising from a supine position (n = 28). Falls

52
END STAGE RENAL DISEASE
were found to occur with similar frequency on both dialysis
and non-dialysis days but on dialysis days, falls were more
common after dialysis (73%) than before (27%) dialysis
(Cook et al., 2006). Most of the injuries from falls were
minor (136, or 81%, of 305) while 12 of the falls (7%)
resulted in patients loss of consciousness from head
injuries and eight of the falls (4%) resulted in fractures.
A total of 26 (16%) patients were hospitalized from the
fall and six patients (4%) died within seven days of their
fall as a direct result of injuries sustained from the fall
(Cook et al., 2006). As for factors that are predictive of
falls, male gender, history of falls, a low average pre-
dialysis systolic blood pressure, and higher comorbidity
were found to be statistically significant fall risk
factors. Age was found to increase the odds for
experiencing more falls yet was not statistically
significant. Vision, number of medications, and cognitive
impairment were not considered to be predictive of falls
(Cook, et al., 2006).
This study showed that dialysis patients are generally
more frail and susceptible to falls. Recognition and
implementation of fall prevention programs for this patient
population could help to improve quality of life and
minimize morbidity and mortality rates in dialysis

53
END STAGE RENAL DISEASE
patients. This study, however, was limited by certain
factors which include the fact that patients were recruited
from a single in-center dialysis setting which decreased
the generalizability of the results. Also, bi-weekly
patient interviews were used to assess falls which may
result in patient bias and recall issues.
Dialysis and Aerobic Training
Malagoni et al. (2008) examined the acute and long-
term effects of an exercise program performed at home for
dialysis patients. The researchers decided to look at the
effects of a walking program on physical capacity, post-
dialysis fatigue, and health-related quality of life. A
six month at-home walking program was chosen as the
exercise modality. A total of 31 dialysis patients (19 men
and 12 women) with ESRD were obtained for the study and
distributed into one of two groups which included an
exercise group (n = 17) and a control group (n = 14).
Participants had undergone hemodialysis three times per
week for a minimum of one year before taking part in the
study.
Outcome measures were analyzed at baseline and at the
end of the six month walking rehabilitation program.
Participants were tested on physical capacity using the 6-
minute walk test (6MWT) and on quality of life and post-

54
END STAGE RENAL DISEASE
dialysis fatigue using the Medical Outcomes Study Short
Form Health Survey (SF-36). Maximal speed for the exercise
group was assessed using an incremental treadmill test
which began at 1.5 km/hour with progressive increments of
0.1 km/hour every 10 minutes until the patient could no
longer maintain that speed (Malagoni et al., 2008).
Sessions were performed twice daily for 10 minutes each at
a speed level to 50% of the individual patients’ maximal
speed on non-dialysis days. The intensity and duration of
the exercise sessions were progressively increased and/or
modified while the duration was kept constant. Daily
training records and any listed symptoms were obtained on
each follow-up visit. The control group was not prescribed
any exercise and no additional testing was performed past
baseline for this group.
T-tests and regression analyses were performed during
data analysis and a p value less than 0.05 was considered
statistically significant. A total of 20 patients (13 from
the exercise group and 7 from the control group) actually
completed the study. The exercise group averaged 45 +/- 36
hours of training time with an average walking speed of 2.4
+/- 0.5 km/hour (Malagoni et al., 2008). The 6MWT distance
significantly increased in the exercise group following
training and remained the same for the control group at the

55
END STAGE RENAL DISEASE
end of the study. Significant improvements were observed
in the physical role, bodily pain, and mental health scores
of health related quality of life for the exercise group.
Physical functioning and mental health scores were
correlated with changes in the 6MWT distance. Decreases
were seen in post-dialysis fatigue scores as well as in
recovery time. For the control group, overall decreases
were seen in all of the subscales, especially general
health, and post-dialysis fatigue scores and recovery time
remained unchanged (Malagoni et al., 2008).
Surviving patients were re-evaluated approximately 19
months later. Patients from the exercise group reported a
continued active lifestyle with only four patients
reporting a reduction in physical activity due to physical
condition. The patients from the control group reported no
increase in their daily activity levels.
In summary, the researchers found that a low intensity
walking program prescribed at the hospital and performed at
home significantly increased physical capacity of dialysis
patients (Malagoni et al., 2008). Performance, post-
dialysis fatigue, and health related quality of life was
improved in the exercise group compared to the control
group. The intensity of the walking program allowed for
patients with low functional capabilities, who are normally

56
END STAGE RENAL DISEASE
excluded from training studies, to take part in the study
and improve their health. As with any study, there were
some limitations which included the small sample size and
the fact that the groups were not randomized.
A study by Storer, Casaburi, Sawelson, and Kopple,
(2005) chose to examine the effects of endurance training
on muscle strength and physical function. The researchers
sought to test three different hypotheses. The first of
which included the effect of aerobic training having the
ability to counteract the results of anemia in dialysis
patients. Second, the researchers wanted to determine the
effects of endurance training in dialysis patients on
improvements in cardiopulmonary fitness, physical
performance, and muscle strength, power, and fatigability.
Lastly, the researchers examined endurance training and the
rapidity of the increases in the tolerated amount of work
during training (Storer et al., 2005).
A total of 12 participants (7 males, 5 females) who
were undergoing maintenance hemodialysis participated in
the exercise study. Two comparison groups were also
involved in the study, a group of 12 non-exercising
dialysis patients, and a group of 12 healthy, sedentary
volunteers. All were matched for age, gender,
race/ethnicity, and completed baseline studies of

57
END STAGE RENAL DISEASE
cardiopulmonary fitness and muscle function. The exercise
group also completed physical performance tests and took
part in a 10 week (3 times per week) exercise program on a
cycle ergometer during hemodialysis. VO2peak was assessed
using an electrically braked cycle ergometer while the
subjects’ blood pressure and heart rhythm were monitored.
Muscle strength and fatigability were assessed using the
seated leg-press exercise machine. Measures of physical
performance included stair climbing, the timed up-and-go
test, and a timed distance course. For the exercise
training group, exercise was performed during the first 90
minutes of the dialysis session while heart rate, blood
pressure, and RPE were monitored every 10 minutes.
Interval training was used in order to increase the
patients’ exercise tolerance until they could perform 20
minutes at their specific work rate. At that point,
duration was then increased up to 40 minutes and work load
was increased from there.
Both VO2peak (22%, P < 0.001) and peak work rate
significantly increased in the exercise group following
training (Storer et al., 2005). These variables were both
lower than values of normal, healthy controls even after
training, however. Neither of these variables changed in
the non-exercise groups over the course of the study.

58
END STAGE RENAL DISEASE
Maximal voluntary muscle strength and fatigability improved
significantly following training yet no significant changes
were seen in leg power. Stair climb performance (14% -
22%, P = 0.031), time to walk the walking course (19%, P =
0.003), and time to complete the timed-up-and-go test (12%,
P = 0.012) all improved significantly from baseline (Storer
et al., 2005).
Storer et al. (2005) determined that hemodialysis
patients can improve their exercise capacity. It was also
seen that work rate exercise improvements could be evident
after just eight to ten weeks of exercise training.
However, for more significant strength gains, it was
suggested that a future study focus more on resistance
training (Storer et al., 2005). A limitation of this study
included the young, fairly healthy subject population that
could not be generalized to the overall dialysis
population. The small sample size was another limitation
of this study.
Bulckaen et al. (2011) used a prospective, controlled,
non-randomized intervention study to examine the effects of
exercise training on physical performance of dialysis
patients. Since hemodialysis patients are generally quite
similar in regard to physical abilities and comorbidities,
the researchers stressed the importance of finding a safe

59
END STAGE RENAL DISEASE
and effective implementation of exercise for this patient
population (Bulckaen et al., 2011). Therefore, the goal of
the study was to evaluate the effects of two different six
month training programs that were adapted to physical
ability on physical performance of hemodialysis patients.
Following a 12 month run-in control period, the
patients took part in two different exercise training
schedules for a six month time period. Testing and
evaluations were performed at baseline, at the end of the
control period, after three months of training, and again
after six months of training. A total of 18 patients (mean
age 62 +/- 15 years) who were on hemodialysis three times
per week completed the study protocol. Body weight and
blood samples were obtained from each patient and
evaluation tests included the 6-minute walk test and the
constant treadmill test (speed of 3 km/h, 10% grade). The
patients were also given a pedometer in order to assess any
extra or spontaneous physical activity. The patients took
part in low levels of coordination exercise during their
thrice weekly dialysis periods, as well as additional
training outside of the dialysis center based on their own
willingness. Nine patients (7 men, 2 women) took part in
an advised walking group which followed a specific home
design walking program monitored by a pedometer. The other
60
END STAGE RENAL DISEASE
nine patients (6 men, 3 women) took part in a home design
program as well as a supervised walking group that occurred
two times per week in a gym on a treadmill and an arm
ergometer. The participants were instructed to walk until
they were limited by fatigue or dyspnea and were
recommended to progressively increase their activity
levels.
Upon completion of the exercise training program, both
groups exhibited significant and progressive improvement in
endurance performance on the treadmill test when compared
with baseline measures. However, the amount of meters
walked was significantly greater in the supervised walking
group than the advised walking group (Bulckaen et al.,
2011). Results of the 6MWT showed significant improvements
in the supervised walking group only, yet daily number of
steps only improved with the advised walking group by the
end of the training period (Bulckaen et al., 2011). The
researchers concluded that training programs may be
elicited for use of safely increasing physical performance
in dialysis patients. It was recommended that training
programs be continued for at least six months and that
home-based measures may be taken as an easy approach while
supervised programs can give additional benefits in certain
patients (Bulckaen et al., 2011). This study had certain

61
END STAGE RENAL DISEASE
limitations however, which included the fact that the
groups were not randomly assigned. The groups were based
on willingness and ability, which could skew the results to
a select few healthy and motivated dialysis patients.
Another limitation included the small sample size and the
single-center design.
Petersen, Murray, McMahon, Kent, and McKenna (2009)
examined endurance training to determine the effects on
extra-renal potassium regulation and exercise performance
in dialysis patients. Potassium regulation was chosen
because dialysis patients often suffer from anemia which
impairs potassium regulation during exercise and affects
exercise performance (Petersen et al., 2009). Six dialysis
patients and six matched control patients were analyzed and
completed the study. Several tests were given at baseline,
pre-train, and post-train periods. These tests included an
aerobic power (VO2) test, a quadriceps strength test, a
quadriceps fatigue test, and blood sampling and processing.
The exercise training was performed on a stationary cycle
ergometer for 30 minutes during the first hour of the
patients’ dialysis treatment with a five minute warm-up and
a five minute cool-down. This was done three times per
week for a total of six weeks. The training intensity
began at a work rate equal to 50% of the patients’ pre-

62
END STAGE RENAL DISEASE
train VO2peak and was then increased by 10% each week after
that.
Despite the treatment and administration of Epoetin
for anemia, the dialysis patients showed impairment in
extra-renal potassium regulation during exercise (Petersen
et al., 2009). Training was not found to significantly
improve acute potassium regulation in the dialysis
patients. The dialysis patients also had lower VO2peak
values and knee extensor peak torque when compared to the
control subjects, as can be expected. There were no
changes in these variables following training, however, the
researchers found that time to fatigue and total work
performed were both increased after training. No muscle
strength changes were seen following training and dialysis
patients demonstrated higher knee extensor fatigue than
controls.
The findings suggested that the dialysis patients had
poor exercise performance due to impaired extra-renal
potassium regulation. However, exercise performance
improved despite no changes in potassium regulation. This
study had several limitations which included the small
sample size and the fact that the subjects were relatively
healthy and cannot necessarily be generalized to the
dialysis population. Also, the study did not have a non-

63
END STAGE RENAL DISEASE
training dialysis group with which to make comparisons.
Therefore, any exercise improvements potentially could have
been due to a familiarization effect.
Wilund et al. (2010) used intra-dialytic exercise
training to examine the effects on oxidative stress and
epicardial fat. Excessive oxidative stress that is often
accompanied by uremia is thought to play a role in chronic
inflammation of chronic kidney disease patients. This, in
turn, plays a significant role in atherosclerosis
development (Wilund et al., 2010). The purpose of the
study was to evaluate how effective aerobic exercise
training is on the risk factors of dialysis patients that
may lead to the extreme cardiovascular disease risk for
this population.
A total of 17 patients (9 females and 8 males) on
maintenance hemodialysis and between the ages of 30 and 70
years were recruited for the study. The subjects were
randomly assigned to either an intradialytic exercise
training group or a usual care control group. Patients in
the exercise group cycled three times per week during
dialysis on a cycle ergometer placed in front of the
dialysis chairs. Training began at an individualized time
and pace then progressed based on patient ability until
they were able to cycle continuously for a 45 minute period

64
END STAGE RENAL DISEASE
at an RPE between 12 and 14 (0-20 scale). The control
group was not given any access to the cycle ergometers
during dialysis.
Baseline testing was performed in addition to testing
after the four month intervention period on non-dialysis
days. Physical performance was measured according to the
distance walked during an incremental shuttle walk test
(ISWT) over a 10 m course while paced by a series of beeps.
Blood chemistry was analyzed from blood samples obtained
from patients in a non-fasted state. Blood pressure and
cardiac function via echocardiography were also assessed
for this study.
Statistical analyses revealed that the groups did not
differ significantly at baseline (Wilund et al., 2010).
Serum lipid peroxidation was found to be reduced by 38% (p
< 0.05) following training in the exercise group and no
differences were seen for the control group. The distance
walked on the ISWT increased significantly in the exercise
group by 15% (P = 0.03) and remained unchanged in the
control group (Wilund et al., 2010). No significant
effects were seen with the exercise group and relative
heart wall thickness, or left atrial volume thickness.
However, epicardial fat thickness was significantly reduced
following training (-9.8%, P = 0.03) and remained the same

65
END STAGE RENAL DISEASE
for the control group (Wilund et al., 2010). Also, the
change in ISWT performance was found to be inversely
correlated to the change in epicardial fat (r = -0.66, P =
0.01) (Wilund et al., 2010).
Wilund et al. (2010) concluded that four months of an
intradialytic exercise program improved physical
performance and reduced serum oxidative stress and
epicardial fat levels in dialysis patients. The data
suggested that exercise training may help to reduce CVD
risk (Wilund et al., 2010). However, the study was limited
by a relatively small sample size. This also meant that
the researchers could not control for many factors that
could have potentially impacted the study, such as
medications, diabetes, etc.
Some studies researched the effects of endurance
training on muscle atrophy. Kouidi et al. (1998) examined
the low exercise capacity of dialysis patients and the
structural and functional alterations in skeletal muscle
that affect this issue. Excess nitrogenous waste products
in the urine of ESRD patients cause uremic myopathy which
results in abnormal function and structure of the muscle
fibers (Kouidi et al. 1998). For that reason, the study
was designed in order to evaluate the muscle fiber profile
of the lower limbs of dialysis patients.

66
END STAGE RENAL DISEASE
Seven patients (5 men and 2 women) with a mean age of
44 years were included in the study. Each patient was
diagnosed with ESRD and had been on maintenance dialysis
treatment for at least one year prior to the study (3 days
per week, 4 hours per session). No patient was known to
have a serious comorbidity and almost all of them had
complained of muscular weakness. Before starting the
program, each patient had a full medical examination as
well as a symptom limited treadmill exercise test using the
Bruce protocol. Blood pressure and electrocardiograms were
monitored continuously throughout and blood samples for
lactate concentration were collected. Peak oxygen
consumption was determined from the highest VO2 obtained
during the exercise test. Peak extension forces of the
lower limbs were measured using a dynamometer and muscle
biopsies were obtained from the vastus lateralis from the
left leg of each patient. The exercise training program
was comprised of 90 minute indoor sessions under
supervision. This was done three times per week for six
months and took place on non-dialysis days.
Exercise training was found to have a positive effect
on the recovery of atrophic muscle fibers in the dialysis
patients. Consequently, muscle strength and exercise
performance also increased following exercise training

67
END STAGE RENAL DISEASE
(Kouidi et al., 1998). Size and strength of muscle fibers
and capillaries increased following exercise training when
compared to baseline measures. After six months of
training, the average cross-sectional area of muscle
improved by 29% with the type I fiber area increased by 26%
and the type II by 24%. Training also had an effect on the
fiber type proportion and shifted the ratios of fiber types
to more normal values. The researchers discovered a 51%
increase in type II fiber proportion and a 42% decrease in
type I fiber proportion, making it a more even distribution
(Kouidi et al., 1998). A restoration of mitochondria was
also observed from the biopsies post training. Overall,
the results demonstrated that exercise training caused
substantial improvements in restoring atrophic muscles in
dialysis patients.
Muscle Evaluation
As previously stated, chronic kidney disease (CKD) is
associated with muscle wasting and limited functional
capacity. Since the reason(s) for this have not been fully
recognized, in 2006 McIntyre et al. decided to look into
skeletal muscle mass and function in a cross-sectional
study of CKD patients. A total of 134 patients (60 on
hemodialysis, 28 on peritoneal dialysis, and 46 CKD stage 4
patients) were included in the study. A cross-sectional

68
END STAGE RENAL DISEASE
area of muscle and fat were obtained from a biopsy of the
thigh from each patient. Functional assessments were
measured from the sit-to-stand 60 test and the sit-to-stand
5 test. These were done in order to determine the number
of sit-to-stands possible for the patients as well as the
time taken to perform the movement. The tests required the
patients to rise, with arms folded across the chest, from a
seated position out of a chair (about 46 cm) and returning
to the seated position. The time it took and the amount of
times completed were recorded. ANOVA was used for
comparisons between groups and univariate regression
analysis was used in order to assess the impact of
determinants on muscle mass. Linear regression analysis
was also performed to look at the relationship between
cross-sectional muscle area (CSA) and functional
performance (McIntyre et al., 2006).
Muscle mass was found to be about 9% lower in dialysis
patients than patients with stage 4 CKD. There were no
significant differences in muscle CSA between patients
receiving hemodialysis and peritoneal dialysis (McIntyre et
al., 2006). Muscle CSA showed a positive correlation with
the sit-to-stand 60 test and a negative correlation with
the sit-to-stand 5 test for overall physical function and
condition for all patients (p < 0.001). A significant

69
END STAGE RENAL DISEASE
reduction in muscle CSA was found to be associated with
substantial reductions in functional capacity as well. The
stage 4 CKD patients exhibited severe uremia, yet
experienced less muscle wasting when compared to the
dialyzed patients. The researchers suggested that a
physiological rather than an anatomical approach to CSA
might improve functional performance correlations (McIntyre
et al., 2006).
Sakkas et al. (2003) developed a study to characterize
the degree of abnormality found in a non-locomotor muscle
of renal failure patients. This was done in hopes of
eliminating any potential effect from disuse atrophy. The
researchers hypothesized that the morphometric and
histochemical make-up of the muscle in renal failure
patients would be abnormal when compared with age-matched
controls without renal failure.
The renal failure patient group was comprised of 22
dialysis patients (12 women and 10 men) and the control
group included 20 (10 women and 10 men) participants.
Blood samples were taken in order to measure creatinine,
albumin, hemoglobin, and parathyroid hormone. A rectus
abdominal muscle biopsy was taken from each subject.
The patients with renal failure showed significantly
higher serum creatinine concentrations (t = 11.8, P < 0.01)

70
END STAGE RENAL DISEASE
and lower albumin (t = -2.8, P < 0.01) and hemoglobin
concentrations (t = -9.4, P < 0.01) when compared with the
control group (Sakkas et al., 2003). Many patients tested
positive for malnourishment. Type IIa muscle fibers were
found to be 26% smaller in the renal failure group than the
control group. When compared with the control group,
muscle biopsies from the patient group showed three times
as many atrophied muscle fibers. The control group also
had greater capillary density per muscle fiber than the
patient group. The researchers concluded that uremia and
malnutrition are major factors in the role of muscle
atrophy in renal disease patients. It was suggested that
exercise training interventions for building muscle be used
to improve physical function and nutrition for renal
failure (Sakkas et al., 2003).
Looking further into skeletal muscle dysfunction, a
study by Lewis et al. (2012) evaluated the potential
morphometric and biochemical bases for muscle abnormalities
seen in dialysis patients. The researchers hypothesized
that limitations in muscle oxidative capacity and diffusion
reserves are at least partially responsible for the
reduction in muscle endurance capacity in this patient
population. In order to examine this, 60 dialysis patients
(37 males and 23 females) with an average time of 49 months

71
END STAGE RENAL DISEASE
on dialysis were included. The dialysis was performed on
these patients three times per week with each session
lasting approximately four hours. The study also included
21 normal control subjects (16 males and 5 females) who
were matched in sedentary lifestyle behavior, age, gender,
and race/ethnicity (Lewis et al., 2012).
In order to assess baseline muscle structure and any
changes that occur following training, biopsies were taken
from the right vastus lateralis muscle. Assessment of
muscle fiber classification and capillarity and fiber
proportions (into types I, IIA, and IIX) was completed from
the biopsies. Fiber oxidative capacity was evaluated by
measuring the activity of succinate dehydrogenase (SDH),
which is one of the main mitochondrial enzymes in the Krebs
cycle (Lewis et al., 2012).
The results showed a significantly reduced oxidative
capacity in addition to lower capillary density in the
muscle fibers of the dialysis patients when compared to
control subjects. The researchers concluded that the
impaired muscle strength and endurance in dialysis patients
can be explained, in part, by the lower oxygen delivery
ability and capillarity within the major muscle fiber
types. The impairment results in lower energy production
which pairs with the reduced substrate levels and oxygen

72
END STAGE RENAL DISEASE
delivery to reduce endurance and exercise tolerance (Lewis
et al., 2011).
Kemp et al. (2004) also examined muscle function in
hemodialysis patients, yet used a non-invasive, in vivo
technique to do so. The researchers used P-magnetic
resonance spectroscopy (P-MRS), magnetic resonance imaging
(MRI), and near-infrared spectroscopy (NIRS) to establish
relationships between expected mitochondrial metabolic
defects and muscle wasting in this patient population. The
study aims were to provide a definition of muscle metabolic
abnormalities, establish possible effects of reduced oxygen
supply, mitochondrial dysfunction, changes in contractile
efficiency, and to establish the effects of these factors
on muscle wasting (Kemp et al., 2004).
A total of 23 male hemodialysis patients (mean age of
50 years) were compared with 15 male control subjects (mean
age of 43 years). Muscle metabolism and oxygenation
kinetics were studied using MRI at rest followed by P-MRS
during an exercise-recovery protocol. Three to five
minutes of 0.5 Hz isometric plantarflexion was performed at
50% and 75% of maximum voluntary force (MVC) during muscle
evaluation and ended with a five minute recovery period.
The researchers defined the key measurement as the rate
constant of post-exercise NIRS recovery (equal to

73
END STAGE RENAL DISEASE
0.693/half-time) which is reflective of the extent to which
oxygen supply exceeds demand in recovering muscle (Kemp et
al., 2004).
Differences were analyzed using unpaired t-tests and
all results were shown as means +/- standard deviation.
When examining the CSA of the posterior calf muscles, the
CSA of the dialysis patients was found to be significantly
smaller than the control subjects. When compared with
controls, patients’ tolerable exercise duration was
reduced. Phosphocreatine depletion as a result of exercise
was not significantly different between groups, yet
recovery was slower in patients. This was suggestive of a
mitochondrial ATP synthesis functional defect (Kemp et al.,
2004). Muscle wasting was evident in the patients and was
determined to be due to the mitochondrial defect. This
study was limited, however, in the fact that only male
subjects were examined and by the small sample size.
Combination Training
The previous study showcased the structural changes
that occur in the musculature of dialysis patients,
indicating the importance for studies to evaluate the
impact of exercise training in this population. Kopple et
al. (2007) examined the role that exercise in general plays
on transcriptional muscle changes. Certain growth factors,

74
END STAGE RENAL DISEASE
specifically insulin-like growth factor (IGF) are thought
to stimulate or suppress protein synthesis or inhibit
protein degradation of muscle (Kopple et al., 2007). The
study was performed in order to examine the effects of
training on mRNA levels of the right vastus lateralis
muscle of dialysis patients.
A total of 51 dialysis patients completed baseline
testing, which included a muscle biopsy, and were then
randomized to one of four groups which included; endurance
training, strength training, endurance training and
strength training, and no training. This group was
compared against 20 normal control subjects. All
participants reported a sedentary lifestyle and no
comorbidities. The dialysis patients exercised for 21.5
+/- 0.7 weeks. Exercise training began with a 5-10 minute
warm-up and stretching period. Endurance training subjects
used a cycle ergometer and strength training subjects used
leg extension/leg curl and leg press/calf extension
combination machines. Resistance and/or repetitions, as
well as time spent exercising, were increased as tolerated.
Skeletal muscle IGF was significantly lower in the
dialysis patients than in the control subjects prior to
exercise training. These values rose significantly
following the training regimen for the exercise groups,

75
END STAGE RENAL DISEASE
bringing the mRNA levels closer to normal (Kopple et al.,
2007). This study was limited by several factors. First,
each group was made up of small patient numbers. Second,
there were an uneven number of patients per group which
could have resulted in treatment bias. Third, all of the
muscle analyses were performed only on the right vastus
lateralis muscle, which may not be a reflection of growth
factor responses of other muscles. However, the
researchers believed that the results provide evidence for
an anabolic response from exercise in sedentary dialysis
patients (Kopple et al., 2007).
(Orcy, Dias, Seus, Barcellos, and Bohlke (2012)
compared the effects of a combined aerobic and resistance
exercise program with a resistance program alone on
functional performance of dialysis patients. The
researchers used a randomized control trial to examine the
effects since adequate physical function is a major
component of independence and quality of life (Orcy et al.,
2012). Participants were assessed for functional
performance prior to the training and again 10 weeks later,
at the end of the training period. Following random
assignment to the intervention groups, subjects exercised
for 30 minutes, three times per week, within the first two
hours of dialysis. Aerobic exercise was performed on a

76
END STAGE RENAL DISEASE
mechanically braked cycle ergometer and resistance
exercises were performed with elastic bands, therapeutic
balls, dumbbells, and ankle weights (Orcy et al., 2012).
The outcome measure was the difference between the 6-
minute walk test (6-MWT) before the intervention period and
following 10 weeks of training. At baseline, the 6-MWT
results showed no significant differences between the
training groups (Orcy et al., 2012). The results from the
study showed no significant difference in the 6-MWT for the
resistance training group (-19.2 +/- 53.9 m). However,
there was a significant difference in distance covered on
the 6-MWT (39.7 +/- 61.4 m) for the combined training group
(Orcy et al., 2012). These results were limited by certain
factors. One such factor was the large refusal rate to
enter the study by potential participants, which made it
difficult to generalize the findings. Also, the evaluation
was based on a single test factor, which may not have
allowed for a true analysis of the various factors that
impact upon dialysis patients.
Segura-Orti et al. (2009) constructed a randomized
controlled trial to examine the effects of exercise during
hemodialysis on physical function and quality of life.
More specifically, the researchers looked at the effects of
intra-dialytic resistance training on patients’ exercise

77
END STAGE RENAL DISEASE
capacity, physical function, muscle strength, and health
related quality of life. A 24 week resistance training
program was implemented for this study.
A total of 27 patients from two different dialysis
clinics were recruited for the study. These patients were
required to be in a stable medical condition and had been
on dialysis for at least three months prior to starting the
study. Before beginning the program, all patients were
clinically examined and underwent a graded exercise test on
a non-dialysis day to evaluate exercise capacity.
Dynamometry was performed in order to evaluate muscle
strength of the lower limbs in addition to functional
testing. An RPE score was given for each test and each
patient was given a health related quality of life survey
to complete. Patients were then randomly assigned into a
progressive resistance exercise group (Group A) or a low
level aerobic exercise training program (Group B; as an
attention control group). Since the primary goal of the
study was to examine resistance training effects, the
number of patients in the resistance training group was
double that of the aerobic training group. Following the
six months of training, each measurement was repeated.
Primary outcome measures included the sit-to-stand-to-sit
test (STS 10 and STS 60), the 6-minute walk test (6MWT),

78
END STAGE RENAL DISEASE
and dynamometer measurements of the knee extensors.
Secondary outcomes included a treadmill graded exercise
test (Bruce protocol) and the Medical outcomes survey short
form (SF-36) (Segura-Orti et al., 2009).
Exercise training was performed during the first two
hours of hemodialysis three times per week over a period of
six months. Five minute warm-ups and cool downs were
performed by both groups and main exercise sessions
occurred for 25 minutes. Resistance training exercises
were composed of four progressive isotonic and isometric
resistance exercises that targeted the major muscle groups
of the lower extremities (Segura-Orti et al., 2009). The
exercises were progressed by increasing the resistance in
order for the patient to be able to perform 3 sets of 15
repetitions. The intensity of each exercise was set based
on an RPE level between 12 and 14 on a scale of 0 to 20.
The aerobic exercise for the second group was performed on
a stationary bicycle at a constant low workload (Segura-
Orti et al., 2009).
Between groups analysis was performed using a two-way
repeated measure ANOVA with mean and standard deviation
calculated for all variables. At baseline, Group A was
15.7% slower in STS 10 performance than Group B, yet this
was not statistically significant (Segura-Orti et al.,

79
END STAGE RENAL DISEASE
2009). Also, the Group A performance on the 6MWT was 13.7%
less than that of Group B. No other significant
differences were evident. Following training, Group A
decreased the time to perform STS 10 by 22.3% (p < 0.05)
while Group B only decreased the performance time by 6.4%
(Segura-Orti et al., 2009). With respect to the STS 60,
Group A increased their repetition amount by 17.7% (p <
0.05) while Group B’s increase was 2.2%. Group A also
increased their 6MWT distance by 11.2% (p < 0.05) and Group
B increased by 8.9% (Segura-Orti et al., 2009). After
completion of training, Group A showed a substantial MET
improvement of 15.8% (p < 0.05) and Group B showed a 6.3%
increase. Dynamometry showed a 5.9% increase in leg
strength for Group A and an 8.1% decrease for Group B
(Segura-Orti et al., 2009). No significant differences in
health related quality of life were evident in either
group.
The intra-dialytic training program seemed to have an
effect on acting against the muscular atrophy associated
with hemodialysis patients yet failed to show a significant
effect on quality of life. The researchers determined that
increasing the workload for this patient population is safe
and future studies may want to add to this in order to test
additional benefits. To summarize, intra-dialytic
80
END STAGE RENAL DISEASE
resistance training was shown to be feasible and effective
in this case and resulted in significant improvements in
physical functioning for dialysis patients (Segura-Orti et
al., 2009).
Resistance training
Certain studies examined the effects of resistance
training alone on dialysis patients. Kuge, Suzuki, and
Isoyama (2005) used handgrip exercise training to examine
whether or not there is an effect on forearm vasodilator
response to arterial occlusion and to determine if there is
a relationship between muscle contraction function and the
vasodilator response in hemodialysis patients. A six week
study was performed with eight patients (6 males and 2
females) who had been on dialysis for at least 30 months
and had no cardiovascular disease or physical training
contraindications. Additionally, seven healthy volunteers
(3 males and 4 females) free from renal disease were
included as an age-matched control group (Kuge et al.,
2005).
Measurements of muscle strength and endurance were
obtained using a handgrip dynamometer on the hand without
arterio-venous shunt for hemodialysis. Forearm strength
was determined by having the subject grip the dynamometer
as strongly as possible. Muscle endurance was then

81
END STAGE RENAL DISEASE
determined by the time period from muscle contraction
initiation to the time when strength declined to 60% of the
maximum value (Kuge et al., 2005). Tissue oxygenation and
hemodynamics were analyzed using near infrared-spectroscopy
(NIRS) which allowed for a non-invasive, continuous
measurement. Handgrip exercise training took place four
times per week for six weeks on non-dialysis days. During
the first week, 50 repetitive handgrip contractions were
performed at 60% of the patients’ maximal strength value
(measured previously). From there, contractions were
increased by 20 contractions a week, up to 150 contractions
and took 15 to 30 minutes to accomplish each set.
The maximum voluntary contraction for the patient
group (200 Newtons) was significantly lower than that of
the control subjects (378 Newtons). Following training,
the patient group value was increased to 226 Newtons (Kuge
et al., 2005). Muscle endurance for the patients (32
seconds) was also lower than the control subjects (48
seconds) at baseline, but improved to 43 seconds following
training (Kuge et al., 2005). Vasodilator responses in the
forearm (estimated from the changes in oxyhemoglobin and
oxygen saturation) were smaller in the dialysis patients in
comparison with the control group and did not change after
training.

82
END STAGE RENAL DISEASE
Kuge et al. (2005) discovered that training improved
maximal muscle strength (125% of initial value) and
endurance (163% of initial) in the dialysis patients (Kuge
et al., 2005). However, the six week program did not
improve the decreased vasodilator response to arterial
occlusion in the patient group. The results showed that
exercise capacity was increased due to the handgrip
exercise training produced by skeletal muscle improvements
but not by changes in blood perfusion for muscle
oxygenation in this patient population (Kuge et al., 2005).
Johansen et al. (2006) studied the effects of
resistance exercise training and the administration of an
anabolic steroid on body composition and muscle function of
hemodialysis patients. Anabolic steroid use was chosen as
an intervention due to its use to alleviate anemia
associated with ESRD, it has few adverse effects, and it
has been shown to increase lean body mass and improve
physical performance (Johansen et al., 2006). The
researchers designed a 12 week study where patients were
randomly assigned into one of four groups including;
nandrolone decanoate (a synthetic testosterone derivative)
injections, weekly placebo injections, lower extremity
resistance exercise training during dialysis sessions (3
times per week) plus weekly placebo injections, and

83
END STAGE RENAL DISEASE
resistance exercise plus weekly nandrolone injections
(Johansen et al., 2006).
Nandrolone decanoate and an identical looking placebo
were injected weekly by the dialysis unit nursing staff,
who were blinded to the treatment assignments. The
resistance training of the lower extremities was performed
during dialysis three times per week with starting weights
determined according to a three-repetition maximum using
ankle weights. Knee extension, hip flexion and abduction,
ankle dorsiflexion and plantar flexion were performed at
each session (Johansen et al., 2006). Body composition was
assessed using dual energy x-ray absorptiometry (DEXA) and
muscle size was measured using magnetic resonance imaging
of the quadriceps muscle. Muscle strength was tested
during knee extension with a computerized dynamometer and
physical performance was assessed by having patients walk a
timed 20 foot distance, climbing stairs, and the sit-to-
stand 5 times test (Johansen et al., 2006). Patients were
given accelerometers for a one week period to measure
physical activity levels. The SF-36, Human Activity
Profile (HAP), and the Physical Functioning (PF)
questionnaires were given to the patients as a self-
reported measure of function. Baseline characteristics and
84
END STAGE RENAL DISEASE
any changes in outcome measures were compared using ANOVA
(Johansen et al., 2006).
A total of 68 patients completed the study with an age
range of 26 to 88 and an average age of 56 +/- 13 years.
Significant changes in body weight occurred in patients who
received the nandrolone decanoate (F = 20.64, P < 0.0001)
in that those patients gained weight yet decreased their
fat mass (Johansen et al., 2006). There was no significant
weight gain associated with exercise but was associated
with an increase in body fat mass for the exercise only
group. Quadriceps muscle cross-sectional area increased
significantly for patients who were assigned to the
exercise and nandrolone decanoate, yet decreased in
patients who were assigned to receive placebo injections
only (Johansen et al., 2006). Significant muscle strength
changes were seen in knee extension and hip flexion and
abduction for those who were assigned to resistance
exercise training. Neither nandrolone nor exercise was
associated with improvements in any of the physical
activity or performance measures. However, exercise was
found to be associated with improvements in self-reported
physical functioning on the SF-36 questionnaire (Johansen
et al., 2006).

85
END STAGE RENAL DISEASE
In summary, the researchers determined that both
nandrolone injections and resistance training during
dialysis have anabolic effects. However, the anabolic
effects of exercise were applied only to the trained
muscles while the anabolic effects of the nandrolone
injections were more systemic (Johansen et al., 2006).
This study was limited by certain factors, one of which
included the lack of dietary intake being monitored during
the study. Also, lean body mass, which was a primary
outcome measure within the study, is influenced by
hydration levels which are likely to change throughout the
12 week period. Further studies are necessary to determine
whether or not this type of intervention improves survival
rates for this patient population.
Similarly, a study by Cheema et al. (2007) used a
randomized, controlled trial of resistance training during
hemodialysis to examine the effects on progressive exercise
for anabolism in kidney disease, or PEAK study. The
purpose of the study was to determine whether a full body,
high intensity resistance training program during dialysis
could cause shifts in skeletal muscle quantity and quality
in patients. The researchers hypothesized that the
training regimen would increase skeletal muscle cross
sectional area (CSA) and decrease intra-muscular lipid

86
END STAGE RENAL DISEASE
infiltration in addition to other health-related changes
(Cheema et al., 2007). It was speculated that the other
health related changes that would be affected were
improvements in exercise capacity, psychological health
aspects, inflammatory markers, nutrition, and quality of
life.
A total of 49 patients were randomly assigned
(computer generated) into either a progressive resistance
training (PRT) and usual care group or a usual care control
group. Patients assigned to the PRT group performed
exercise in a seated or supine position from a standard
hemodialysis chair with the limb that contained the
arteriovenous graft or fistula having been exercised
immediately before each dialysis session (Cheema et al.,
2007). During PRT, two sets of eight repetitions of ten
exercises were performed for the major target muscle groups
of both upper and lower extremities. A rating of perceived
exertion between 15 and 17 (out of 0 – 20) was the goal.
Upper body exercises were performed using free weight
dumbbells and included; the shoulder press, side shoulder
raise, triceps extension, biceps curl, and external
shoulder rotation. Lower body exercises were performed
unilaterally with weighted ankle cuffs and included; the
seated knee extension, supine hip flexion, supine hip

87
END STAGE RENAL DISEASE
abduction, supine straight-legged raise, and seated
hamstring curls with resistance bands (Cheema et al.,
2010). The abdominal muscles were also targeted with leg
lifts, depending on patient ability. Patients within the
usual care group continued to receive their normal care as
well but were given no instructions to exercise or any
equipment access (Cheema et al., 2007).
Each outcome measure was obtained at baseline and
again following 12 weeks of training. Computerized
tomography of the non-dominant mid-thigh was done on a non-
dialysis day in order to evaluate thigh muscle CSA and
attenuation. The CT scans also analyzed areas of
subcutaneous and total fat for the thigh. Peak force of
the knee extensors, hip abductors, and triceps was measured
using an isometric digital dynamometer. The 6-minute walk
test was used to measure exercise capacity. A dietician
obtained all nutritional and anthropometric measures after
dialysis and the Mini-Nutritional Assessment was used to
evaluate nutritional status. Blood samples were collected
before dialysis, prior to the midweek session, and at least
48 hours after the previous exercise session to assess C-
reactive protein (CRP), albumin, creatinine, and blood
count. In addition, the Medical Outcomes Trust Short Form-
36, or SF-36, was used to measure health related quality of

88
END STAGE RENAL DISEASE
life along with the Geriatric Depression Scale. The
Physical Activity Scale for the Elderly was given to the
patients in order to evaluate activity levels apart from
the exercise program of the study. All data were expressed
as mean +/- standard deviation and all data was included
regardless of patient compliance (Cheema et al., 2007).
No statistically significant differences were found
between groups at baseline. Thigh muscle CSA did not show
any significant change between groups by the end of the 12
week period. However, muscle quality improved
significantly in the PRT group when compared with the
control group (Cheema et al., 2007). As for secondary
outcome measures, statistically significant increases were
seen in total strength, body weight, body mass index, and
mid-arm circumference and mid-thigh circumference in the
PRT group compared to the control group. There were
reductions evident in the inflammatory marker CRP following
12 weeks of training. The PRT group also showed
significant improvements in two out of the eight areas for
quality of life, which included physical function and
vitality. In contrast, both of these measures showed
decline for the control group (Cheema et al., 2007). No
other secondary outcomes showed clinically significant
changes over the course of the study. Compliance to the

89
END STAGE RENAL DISEASE
program was calculated at around 85.1% in the PRT subjects
who completed both assessments (Cheema et al., 2007).
This study had some limitations which included
obtaining patients from a single site, unblended assessment
of the secondary outcomes of physical performance measures,
and not giving the control group something else to do,
which is often not an ideal situation. However, the study
resulted in significant improvements in muscle quality,
strength, body weight, BMI, and physical function and
vitality measures. This training program did not seem to
result in increases of muscle CSA. However, the
researchers suggested that future studies may want to use a
similar program but also investigate muscle biopsies, since
they are more sensitive to change (Cheema et al., 2007).
Headley et al. (2002) designed a twelve week
resistance training program to test strength and functional
measures in ESRD patients. The researchers hypothesized
that moderate intensity training would improve muscle
strength in this patient population, which would then
increase the functional ability of the patients.
A total of ten dialysis patients completed the program
and were tested four times. The first two tests were
baseline tests, the third test occurred after six weeks of
training, and the fourth test followed 12 weeks of

90
END STAGE RENAL DISEASE
training. Subjects were tested based on anthropometric
measures, the 6-minute walk test, computerized dynamometry,
grip test, gait speed tests, and the sit-to-stand-to-sit
test. Following a six week control period, participants
performed supervised resistance training twice per week for
12 weeks and were given exercise bands and a video to
follow on their own at home once per week. Average
attendance for the supervised training sessions was 87.7%
(Headley et al., 2002).
The results showed no significant body mass changes
over the course of the study. However, body fat percentage
increased after six weeks of training (20.0 % +/- 5.5%, P <
0.05) and 12 weeks of training (19.6% +/- 4.8%, P < 0.05)
when compared with baseline testing. As for strength, peak
torque of leg extensors at 90 degrees was greater after the
12 week training period, yet did not change at 120 degrees
or 150 degrees. Grip strength scores did not differ
following training in either arm following 12 weeks of
training either (Headley et al., 2002). Distance covered
during the 6MWT increased significantly following training
when compared with baseline testing. Maximum walking speed
during the gait speed test also increased significantly
after the 12 week training program. The time to complete
the sit-to-stand-to-sit test 10 times showed a significant

91
END STAGE RENAL DISEASE
decrease after both the 6 and 12 test periods, despite the
fact that the time taken was still 36.8% slower when
compared to healthy individuals (Headley et al., 2002).
The training program resulted in a work volume
performance increase of 26% after the 12 weeks of training
in comparison with the first week. However, the
researchers conceded that an isotonic assessment would have
been more ideal for determining changes since the work
performed was isotonic itself. Also, the increased body
fat finding was difficult to explain, given the nature of
the strength improvements and the researchers suggested
that dietary intake should have been monitored during the
course of the study (Headley et al., 2002). Regardless,
the findings concluded that ESRD patients can indeed
benefit from a resistance training program and potentially
fight the wasting and deconditioning associated with the
disease.
Chen et al. (2010) developed a pilot study to
determine the safety and efficacy of a low intensity
progressive strength training in an intra-dialytic setting.
A randomized, controlled trial was used with patients over
30 years of age who were undergoing hemodialysis three
times per week and had no serious comorbidities. Physical
performance was the primary outcome measure with secondary

92
END STAGE RENAL DISEASE
measures including knee extensor strength, lean and fat
mass, quality of life, and disability levels. A total of
44 participants were randomized into either an exercise
group or an attention-control group (Chen et al., 2010).
Exercise training was performed twice weekly for a
total of 48 exercise sessions that took place during the
second hour of hemodialysis. The sessions were supervised
and began with a five minute warm-up and ended with a five
minute cool-down period. Using ankle weights, the
participants in the exercise group performed exercises that
included; seated knee extension with dorsi/plantar flexion,
seated leg curl, leg raises, and pelvic tilt. Sessions
included two sets of eight repetitions for each exercise
with a 1-2 minute rest between sets. Intensity of exercise
was determined using a 0-10 RPE scale with a target RPE of
6 (somewhat hard). Exercise progressed as participants’
were able to complete their sets with a lower RPE score.
Attention control participants did stretching exercises
with light resistance bands performed in a semi-recumbent
position (Chen et al., 2010).
Physical performance scores were measured according to
the Short Physical Performance Battery (SPPB) score, which
includes performance based measures of strength, endurance,
and balance. Knee extensor strength was measured using a

93
END STAGE RENAL DISEASE
Nicholas Manual Muscle Tester and body composition was
assessed using dual x-ray absorptiometry (DEXA). Quality
of life was assessed using a self-reported measure based on
the Medical Outcomes Survey Short Form (SF-36) and
disability was measured using 12 items from the Activities
of Daily Living (ADL) questionnaire. Comparisons between
the treatment and control groups were performed using
independent sample t-tests and Spearman’s rank coefficient
of correlation was used to assess associations between the
primary and secondary outcomes (Chen et al., 2010).
At baseline, 50% of participants scored low on the
SPPB and 77% reported difficulty with at least one ADL
(Chen et al., 2010). Following exercise training, SPPB
scores were significantly improved when compared with the
control group, yet balance and gait speed did not change in
either group. Knee extensor strength improved
significantly in the training group when compared with the
control group. Lean body mass increased significantly with
strength training and fat mass was reduced. When compared
with controls, the strength training group showed improved
self-reported physical activity, physical function, and ADL
disability scores (Chen et al., 2010). Overall, the
researchers determined that strength training resulted in
improvements in physical performance, nutritional status,

94
END STAGE RENAL DISEASE
and physical activity of dialysis patients. The use of an
attention control group allowed for a more ethical approach
to the research. In contrast, only a healthy subset of
patients was used in this study, not allowing for
generalizability.
Bennett, Breugelmans, Chan, Calo, and Ockerby (2012)
recognized the significant risk of falling for older people
receiving hemodialysis. For that reason, a feasibility
study was constructed to test a reduction in falls risk in
this patient population after a strength and balance
intervention. A total of 24 participants were recruited
for the study with 18 out of the 24 (75%) aged 60 years or
older. Only subjects who suffered from end-stage kidney
disease, were at least 18 years of age, and who had been
receiving hemodialysis for at least three months were
included (Bennett et al., 2012).
The falls risk was measured using the five item Short
Form Physiological Profile Assessment (PPA). The specific
measures used for the study included; edge contrast
sensitivity, hand reaction time using a computer mouse or a
button press system, knee joint proprioception using a
joint matching test, lower limb (quadriceps) strength test,
and postural sway while standing on foam (Bennett et al.,
2012). The PPA was done immediately before and after the

95
END STAGE RENAL DISEASE
eight week strength and balance exercise intervention. A
software program then calculated the overall falls risk
scores for each individual (standardized for age and
gender). Lower scores in proprioception, reaction time,
postural sway, and overall falls score indicated a lower
falls risk while higher scores in contrast sensitivity and
lower limb strength indicated lower falls risk (Bennett et
al., 2012).
The exercise intervention was made up of both
resistance and balance exercises. Strength exercises
included hip abduction, ankle plantar flexion and dorsi
flexion, straight leg raise, hip flexion, knee extension,
and knee flexion. Each was done in a seated position and
performed during dialysis. Exercises started out at a
resistance that participants were able to perform one set
of 10 repetitions for each and a moderate intensity (RPE of
15 to 17). Once participants were able to complete a set
of 20 repetitions of each exercise, the exercises were then
progressed. Participants were asked to stand and maintain
a position for 30 to 90 seconds for static balance. This
exercise was progressed by narrowing the support base,
decreasing hand support, challenging the support surface,
and/or closing their eyes. Dynamic balance was worked by
the participants walking on a 2.5 m line using heel/toe

96
END STAGE RENAL DISEASE
walking, backward walking, and lateral walking (Bennett et
al., 2012).
A significant decrease in overall falls risk was
evident between pre and post-tests (z = -3.11, P < 0.008)
(Bennett et al., 2012). Of note, 14 participants (58%)
were classified into a lower falls risk category on the
post- intervention PPA when compared with the pre-
intervention PPA. Falls risk remained the same for eight
participants (33%) and two patients performed worse and
were classified into a higher risk category. Reaction time
decreased (improved) and knee extension force improved
following training (Bennett et al., 2012).
Overall, a significant decrease in falls risk was
evident in dialysis patients following an eight week
strength and balance program. Identifying high risk
patients and starting a strength and balance program has
many potential benefits for this patient population. This
study was limited by the small number of participants and
no comparison control group. Additionally, the PPA
measurement tool requires specific equipment, software, and
training (Bennett et al., 2012).
In conclusion, exercise training has been shown to
result in significant changes and improvements overall in
dialysis patients. The irony of most dialysis programs is

97
END STAGE RENAL DISEASE
that they keep patients alive yet they do very little about
their declining physical function. It is important to
determine a safe and effective way of training to combat
the decline in function and quality of life. More
specifically, a program that strengthens patients in a
manner that promotes compliance and independence is
essential.

98
END STAGE RENAL DISEASE
Appendix C
INFORMED CONSENT FORM
CONSENT TO PARTICIPATE VOLUNTARILY
IN A RESEARCH INVESTIGATION
Department of Exercise Science and Sport Studies
XXXXXXXXXXX COLLEGE
XXXXXXXXXXX, XX XXXXX
________________________ _________________
Responsible Faculty Member Investigator’s Name
_______________________ _________________
Subject’s Name Date
PROJECT TITLE: Effects of an In-center Resistance Training
Program on Functional Measures, Strength, and Quality
Of Life in End Stage Renal Disease
You are being asked to participate in a research
investigation as described in this form below. All such
investigational projects carried out within this department
are governed by the regulations of both the Federal
Government and XXXXXXXXXXX College. These regulations
require that the investigator(s) obtain from you a signed
agreement (consent) to participate in this project.
The investigator will explain to you in detail the
purpose of the project, the procedures and/or drugs to be
used, and the potential benefits and foreseeable risks of
participation. You may ask the investigator any questions
you may have to help you understand the project and you may
expect to receive satisfactory answers to questions. A
basic explanation of the project is written below.
If, after this discussion, you decide to agree to
participate in the project, please sign this form on the
line indicated below in the presence of a witness and the
investigator.
I. The purpose of this research project is to
examine the effect that exercise performed early
in dialysis has on functional performance
measures (i.e. activities of daily living),

99
END STAGE RENAL DISEASE
strength, and quality of life. Your participation
in this project may require completing three 45-
minute exercise bouts during three of your
dialysis procedures weekly. You will be randomly
assigned to either an exercise group or a usual
care control group. During the testing, medical
personnel will be in the facility and aware of
the testing. The exercise intensity used will
require you to perform resistance exercise at a
moderate to somewhat-hard intensity based on your
perception of the exercise. You were chosen for
the study because you are a hemodialysis patient
with arm access and your doctor agreed you could
tolerate exercise during dialysis. The
approximate number of subjects involved in this
process is 20. The study is expected to last for
eight weeks. The procedures to be used include
performing resistance training exercises of the
upper and lower extremities during your dialysis
treatments in the dialysis center.
II. Risks: Since you are a stable dialysis patient,
the risks from moderate exercise should be
minimal. Exercise studies during dialysis have
been carried out and found to be extremely safe.
However, exercise during dialysis does carry a
risk of triggering previously silent cardiac
disease and can result in shortness of breath and
muscle soreness. Testing will be carried out with
medical personnel present at the site and under
close supervision of the investigator. The person
performing all testing is AED certified. In
addition, should any unforeseen physical injury
occur, personnel trained in emergency care will
be present to provide assistance. XXXXXXXXXXX
College and the dialysis center do not have a
program for compensating patients for injury or
complications arising from research but medical
care will be made available as needed at usual
charges.
III. Benefits: Possible and desired benefits of
participating in this study are: If this study
does demonstrate that exercise can result in
significant improvements in functional measures,
strength, and quality of life, you might benefit
100
END STAGE RENAL DISEASE
from increased strength, greater levels of
independence, more ease of performance of
activities of daily living (such as, using
stairs, bathing, getting dressed, using the
restroom, etc.), and feel better overall. Upon
completion of the study, you will be given a 3
month, free membership at the YMCA in XXXXXXXXXXX
or XXXXXXXXX. You will also be informed of any
new findings that could affect your treatment.
Being a participant in this research project will
not affect any of the ordinary charges associated
with the treatment of your condition.
IV. The information obtained about you will be kept
in confidence, although you are free to release
it to your own physician. The information may be
used for statistical or scientific purposes
without identifying you as an individual.
Any significant new findings will be provided to you during
the course of the study.
You are free to withdraw from this project at any time
without penalty or loss of benefits to which you would
otherwise be entitled.
Should an unforeseen physical injury occur, appropriate
first aid will be provided, but no financial compensation
will be given. Further information can be obtained from the
Office of Academic Affairs of XXXXXXXXXXX College
concerning pertinent questions about the research and an
explanation of your rights as a research subject. The
Office of Academic Affairs serves as the official contact
office in the event of research related injury to you (XXX-
XXX-XXXX).
I CERTIFY THAT I HAVE READ AND FULLY UNDERSTAND THE ABOVE
PROJECT. MY QUESTIONS HAVE BEEN ANSWERED TO MY SATISFACTION
BY THE INVESTIGATOR. I WILLINGLY CONSENT TO PARTICIPATE.
______________________ ____________________________
Signature of Witness Signature of Subject or
Guardian
______________________ ____________________________
Date Signature of Investigator

101
END STAGE RENAL DISEASE
Appendix D
MEDICAL HISTORY FORM
Project Title: Effects of an In-center Resistance
Training Program on Functional
Measures, Strength, and Quality Of Life
in End Stage Renal Disease
Investigator: Jennifer McKinnon (XXX) XXX-XXXX
Patient name: . Date: _________
This form should be completed and signed by the
physician of the patient who enrolls in this research. By
completing this form, the physicians are not assuming any
responsibility for the administration of the testing
sessions.
Contraindications to Exercise Testing / Participation
Please check all that apply:
_____ Poorly controlled hypertension with systolic blood
Pressure consistently above 160 mmHg and diastolic
blood pressure consistently above 100 mmHg.
_____ Uncompensated congestive heart failure.
_____ Cardiac arrhythmia requiring the use of an anti-
arrhythmic agent.
_____ Persistent hyperkalemia (high potassium levels).
_____ Recent history of unstable angina.
_____ Significant valvular heart disease.
_____ Myocardial infarction within the past 6 months.
_____ Significant cerebral or peripheral arteriosclerosis.
_____ Bone disease with a risk of fracture during exercise.
_____ Any orthopedic or musculoskeletal limitation or
injury within the last three months.
_____ A recent significant change in the resting ECG
suggesting infarction or other acute cardiac event.
_____ Third degree AV heart block without pacemaker.
_____ Severe aortic stenosis.
_____ Suspected or known dissecting aneurysm.
_____ Active or suspected myocarditis or pericarditis.
_____ Thrombophlebitis or intra-cardiac thrombi.
_____ Recent systemic or pulmonary embolus.
_____ Acute infections.

102
END STAGE RENAL DISEASE
Report of Physician
Please check that which applies:
I know of no reason that the patient may not
participate.
I recommend that the patient not participate.
Physician’s Signature : _________________ _
Physician’s name in full : _________________ _
(Print)

103
END STAGE RENAL DISEASE
Appendix E
DATA SHEET
Patient ID: _______________ Date:_______________
Group: _______________
Age: _______________
Gender: _______________
Ethnicity: _______________
Height: _____.___ X 2.54 = _____.___ 100 = _____.___
in cm m
Weight: ______.___ 2.2 = _______.___BMI: _______.__ kg/m2 lbs kg
BMI Classification:_________________________
Manual Muscle Test: Right Left
Biceps _____Trial 1 _______Trial 2 _______Trial 1 _______Trial 2
Shoulder _____Trial 1 _______Trial 2 _______Trial 1 _______Trial 2
Calf _____Trial 1 _______Trial 2 _______Trial 1 _______Trial 2
Quadriceps______Trial 1 _______Trial 2 _______Trial 1 _______Trial 2
Hamstrings_______Trial 1 _______Trial 2 _______Trial 1 _______Trial 2
Adductors ______Trial 1 _______Trial 2 _______Trial 1 _______Trial 2
Abductors ______Trial 1 _______Trial 2 _______Trial 1 _______Trial 2
Manual Muscle Test Classification (Use average of 2
trials):________________________

104
END STAGE RENAL DISEASE
Appendix F
EXERCISE SHEET
Patient ID:
Date:
Exercise Sets
Repetitions
Band/Weight
RPE
Waiting
Room
Bicep Curls
Lateral Shoulder Raise
Anterior Shoulder Raise
Seated Row
Triceps Extension
Sit-To-Stands
Dialysis
Chair
Bent Leg Raise
Leg Extension
Calf Raise
Hip Adduction Squeeze
Hip Abduction
Chin Tuck
Scapular Retraction
Core
Notes/Comments:

105
END STAGE RENAL DISEASE
Appendix G
SF-36

106
END STAGE RENAL DISEASE

107
END STAGE RENAL DISEASE

108
END STAGE RENAL DISEASE

109
END STAGE RENAL DISEASE

110
END STAGE RENAL DISEASE
Appendix H
SPPB
Short Physical Performance Battery
1. Repeated Chair Stands
Instructions: Do you think it is safe for you to try and
stand up from a chair five times without using your arms?
Please stand up straight as quickly as you can five times,
without stopping in between. After standing up each time,
sit down and then stand up again. Keep your arms folded
across your chest. Please watch while I demonstrate. I’ll
be timing you with a stopwatch. Are you ready? Begin
Grading: Begin stop watch when subject begins to stand up.
Count aloud each time subject arises. Stop the stopwatch
when subject has straightened up completely for the fifth
time. Also stop if the subject uses arms, or after 1
minute, if subject has not completed rises, and if
concerned about the subject’s safety.. Record the number of
seconds and the presence of imbalance.. Then complete
ordinal scoring.
Time: _____sec (if five stands are completed)
Number of Stands Completed: 1 2 3 4 5
Chair Stand Ordinal Score: _____

111
END STAGE RENAL DISEASE
0 = unable
1 = > 16.7 sec
2 = 16.6-13.7 sec
3 = 13.6-11.2 sec
4 = < 11.1 sec
2. Balance Testing
Begin with a semitandem stand (heel of one foot placed by
the big toe of the other foot). Individuals unable to hold
this position should try the side-by-side position. Those
able to stand in the semitandem position should be tested
in the full tandem position. Once you have completed time
measures, complete ordinal scoring.
a. Semitandem Stand
Instructions: Now I want you to try to stand with the side
of the heel of one foot touching the big toe of the other
foot for about 10 seconds. You may put either foot in
front, whichever is more comfortable for you. Please watch
while I demonstrate.
Grading: Stand next to the participant to help him or her
into semitandem position. Allow participant to hold onto
your arms to get balance. Begin timing when participant has
the feet in

112
END STAGE RENAL DISEASE
position and lets go.
Circle one number
2. Held for 10 sec
1. Held for less than 10 sec; number of seconds held _____
0. Not attempted
b. Side-by-Side stand
Instructions: I want you to try to stand with your feet
together, side by side, for about 10 sec. Please watch
while I demonstrate. You may use your arms, bend your
knees, or move your body to maintain your balance, but try
not to move your feet. Try to hold this position until I
tell you to stop.
Grading: Stand next to the participant to help him or her
into the side-by-side position. Allow participant to hold
onto your arms to get balance. Begin timing when
participant has feet together and lets go.
Grading
2. Held of 10 sec
1. Held for less than 10 sec; number of seconds held_____
0. Not attempted
c. Tandem Stand

113
END STAGE RENAL DISEASE
Instructions: Now I want you to try to stand with the heel
of one foot in front of and touching the toes of the other
foot for 10 sec. You may put either foot in front,
whichever is more comfortable for you. Please watch while I
demonstrate.
Grading: Stand next to the participant to help him or her
into the side-by-side position. Allow participant to hold
onto your arms to get balance. Begin timing when
participant has feet together and lets go.
Grading
2. Held of 10 sec
1. Held for less than 10 sec; number of seconds held_____
0. Not attempted
Balance Ordinal Score: _____
0 = side by side 0-9 sec or unable
1 = side by side 10, <10 sec semitandem

114
END STAGE RENAL DISEASE
2 = semitandem 10 sec, tandem 0-2 sec
3 = semitandem 10 sec, tandem 3-9 sec
4 = tandem 10 sec
3. 8’ Walk (2.44 meters)
Instructions: This is our walking course. If you use a cane
or other walking aid when walking outside your home, please
use it for this test. I want you to walk at your usual pace
to the other end of this course (a distance of 8’). Walk
all the way past the other end of the tape before you stop.
I will walk with you. Are you ready?
Grading: Press the start button to start the stopwatch as
the participant begins walking. Measure the time take to
walk 8’. Then complete ordinal scoring.
Time: _____ sec
Gait Ordinal Score: _____
0 = could not do
1 = >5.7 sec (<0.43 m/sec)
2 = 4.1-6.5 sec (0.44-0.60 m/sec)
3 = 3.2-4.0 (0.61-0.77 m/sec)
4 = <3.1 sec (>0.78 m/sec)
Summary Ordinal Score: _____
Range: 0 (worst performance) to 12 (best performance).

115
END STAGE RENAL DISEASE
Appendix I
INFORMATIONAL FLYER
Resistance Training Study for Dialysis Patients
Who can participate? Patients with CKD on dialysis who are
at least 18 years of age and who are not currently enrolled
in a regular (3 days per week for at least 6 months)
exercise training program. Patients must be cleared to
participate by their physician.
What does it involve? Patients will either be randomly
assigned to a normal care group (no exercise) or an
exercise group in which resistance training will be
performed 3 times per week for 8 weeks during their
dialysis sessions. Some exercises requiring both arms will
be performed in the waiting room prior to dialysis and the
remaining exercises will be performed in the dialysis
chair.
What do you get? Free testing will be done for both groups
to analyze quality of life, functional ability for
activities of daily living, and strength plus 8 weeks of
free personal training for the exercise group. Each

116
END STAGE RENAL DISEASE
participant will receive a free 3 month membership at the
YMCA in XXXXXXXXXXX or XXXXXXXXX!
If interested contact Jen McKinnon at XXXXXXXXXXX College
XXX-XXX-XXXX, XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
117
END STAGE RENAL DISEASE
Appendix J
YMCA MEMBERSHIP FORM
TO: YMCA of Greater XXXXXXXXXXX Membership
FROM: S. A. E. Headley, PhD, FACSM, CSCS, RCEP
Professor, Exercise Science & Sport Studies
Program Director, Clinical Exercise Physiology
XXXXXXXXXXX College
DATE:
_____________________________________ was a participant in
the In Center Resistance
Training Program conducted through XXXXXXXXXXX College. As
a reward for completing all
phases of the study, the YMCA has partnered with the
College to allow this patient to have a 3-
month free membership.
This letter serves as verification
of_________________________’s_ completion of the program.
If you need further verification of this please contact
XXXXXXXX XXXXXX at XXX-XXX-XXXX
S. A. E. Headley, PhD, FACSM, CSCS, RCEP
Professor, Exercise Science & Sport Studies
Program Director, Clinical Exercise Physiology
XXXXXXXXXXX XXXXXXX
XXXXXXXXXXX XX, XXXXX

118
END STAGE RENAL DISEASE
Appendix K
STATISTICS TABLES
Table K4
2x2 Mixed Factorial ANOVA Comparing PCS Scores from the SF-
36 Between Baseline and 8-Weeks
___________________________________________________________
Source SS df MS F p η²
___________________________________________________________
Between Subjects
A(Group) 131.07 1 131.07 1.36 > .05 .15
Error between 771.13 8 96.39
Within Subjects
B(Time) 7.44 1 7.44 .35 > .05 .04
AB 2.88 1 2.88 .14 > .05 .02
Error within 167.50 8 20.94
___________________________________________________________

119
END STAGE RENAL DISEASE
Table K5
2x2 Mixed Factorial ANOVA Comparing MCS Scores from the SF-
36 Between Baseline and 8-Weeks
___________________________________________________________
Source SS df MS F p η²
___________________________________________________________
Between Subjects
A(Group) 798.85 1 798.85 3.81 < .05 .97
Error between 1675.52 8 209.44
Within Subjects
B(Time) 8.19 1 8.19 0.12 > .05 .02
AB 29.77 1 29.77 0.43 > .05 .05
Error within 555.60 8 69.45
___________________________________________________________

120
END STAGE RENAL DISEASE
Table K6
2x3 Mixed Factorial ANOVA Comparing SPPB Total Balance
Scores Over Three Time Periods for Treatment and Control
Groups
___________________________________________________________
Source SS df MS F p η²
___________________________________________________________
Between Subjects
A(Group) 5.63 1 5.63 2.11 > .05 .21
Error between 21.33 8 2.67
Within Subjects
B(Time) 1.87 2 .93 3.50 > .05 .30
AB 1.87 2 .93 3.50 > .05 .30
Error within 4.27 16 .27
___________________________________________________________
Mauchly’s Sphericity W = .984; p > .05

121
END STAGE RENAL DISEASE
Table K7
2x3 Mixed Factorial ANOVA Comparing SPBB Gait Speed Test
Scores Over Three Time Periods for Treatment and Control
Groups
___________________________________________________________
Source SS df MS F p η²
___________________________________________________________
Between Subjects
A(Group) .47 1 .47 1.46 > .05 .17
Error between 2.27 7 .32
Within Subjects
B(Time) .08 2 .04 .53 > .05 .07
AB .23 2 .11 1.53 > .05 .18
Error within 1.03 14 .07
___________________________________________________________
Mauchly’s Sphericity W = .749; p > .05

122
END STAGE RENAL DISEASE
Table K8
2x3 Mixed Factorial ANOVA Comparing SPPB Chair Stand Scores
Over Three Time Periods for Treatment and Control Groups
___________________________________________________________
Source SS df MS F p η²
___________________________________________________________
Between Subjects
A(Group) 2.13 1 2.13 0.45 > .05 .05
Error between 37.87 8 4.73
Within Subjects
B(Time) 3.27 2 1.63 5.30 < .05 .40
AB .47 2 .23 0.76 > .05 .09
Error within 4.93 16 .31
___________________________________________________________
Mauchly’s Sphericity W = .611; p > .05

123
END STAGE RENAL DISEASE
Table K9
2x3 Mixed Factorial ANOVA Comparing SPPB Total Scores Over
Three Time Periods for Treatment and Control Groups
___________________________________________________________
Source SS df MS F p η²
___________________________________________________________
Between Subjects
A(Group) 13.33 1 13.33 .94 > .05 .11
Error between 113.87 8 14.23
Within Subjects
B(Time) 7.47 2 3.73 4.35 < .05 .35
AB 3.47 2 1.73 2.02 > .05 .20
Error within 13.73 16 .86
___________________________________________________________
Mauchly’s Sphericity W = .834; p > .05

124
END STAGE RENAL DISEASE
Table K10
2x3 Mixed Factorial ANOVA Comparing Right Biceps MMT Scores
Over Three Time Periods for Treatment and Control Groups
___________________________________________________________
Source SS df MS F p η²
___________________________________________________________
Between Subjects
A(Group) 518.34 1 518.34 .62 > .05 .07
Error between 6703.77 8 837.97
Within Subjects
B(Time) 357.86 1 357.86 4.98 > .05 .38
AB 183.62 1 183.62 2.55 > .05 .24
Error within 575.46 8 71.93
___________________________________________________________
Mauchly’s Sphericity W = .962; p > .05

125
END STAGE RENAL DISEASE
Table K11
2x3 Mixed Factorial ANOVA Comparing Left Biceps MMT Scores
Over Three Time Periods for Treatment and Control Groups
___________________________________________________________
Source SS df MS F p η²
___________________________________________________________
Between Subjects
A(Group) .53 1 .53 .01 > .05 .00
Error between 3440.53 8 430.07
Within Subjects
B(Time) 125.67 2 62.83 .48 > .05 .06
AB 183.87 2 91.93 .71 > .05 .08
Error within 2085.00 16 130.31
___________________________________________________________
Mauchly’s Sphericity W = .849; p > .05

126
END STAGE RENAL DISEASE
Table K12
2x3 Mixed Factorial ANOVA Comparing Right Shoulder MMT
Scores Over Three Time Periods for Treatment and Control
Groups
___________________________________________________________
Source SS df MS F p η²
___________________________________________________________
Between Subjects
A(Group) 11.04 1 11.04 .02 > .05 .00
Error between 5923.22 8 740.40
Within Subjects
B(Time) 17.59 2 8.79 .43 > .05 .05
AB 20.67 2 10.33 .50 > .05 .06
Error within 328.90 16 20.56
___________________________________________________________
Mauchly’s Sphericity W = .576; p > .05

127
END STAGE RENAL DISEASE
Table K13
2x3 Mixed Factorial ANOVA Comparing Left Shoulder MMT
Scores Over Three Time Periods for Treatment and Control
Groups
___________________________________________________________
Source SS df MS F p η²
___________________________________________________________
Between Subjects
A(Group) 202.80 1 202.80 .38 > .05 .05
Error between 4267.96 8 533.50
Within Subjects
B(Time) 18.73 2 9.36 .30 > .05 .04
AB 59.07 2 29.53 .95 > .05 .11
Error within 498.02 16 31.13
___________________________________________________________
Mauchly’s Sphericity W = .797; p > .05

128
END STAGE RENAL DISEASE
Table K14
2x3 Mixed Factorial ANOVA Comparing Right Calf MMT Scores
Over Three Time Periods for Treatment and Control Groups
___________________________________________________________
Source SS df MS F p η²
___________________________________________________________
Between Subjects
A(Group) 832.13 1 832.13 2.17 < .05 .91
Error between 3075.35 8 384.42
Within Subjects
B(Time) 188.39 2 94.19 2.24 > .05 .22
AB 418.14 2 209.07 4.97 < .05 .38
Error within 672.46 16 42.03
___________________________________________________________
Mauchly’s Sphericity W = .775; p > .05

129
END STAGE RENAL DISEASE
Table K15
2x3 Mixed Factorial ANOVA Comparing Left Calf MMT Scores
Over Three Time Periods for Treatment and Control Groups
___________________________________________________________
Source SS df MS F p η²
___________________________________________________________
Between Subjects
A(Group) 273.01 1 273.01 79.15 < .05 .91
Error between 2569.59 8 321.20
Within Subjects
B(Time) 249.17 2 124.59 1.72 > .05 .18
AB 608.01 2 304.00 4.19 < .05 .34
Error within 1159.82 16 72.49
___________________________________________________________
Mauchly’s Sphericity W = .687; p > .05

130
END STAGE RENAL DISEASE
Table K16
2x3 Mixed Factorial ANOVA Comparing Right Quadriceps MMT
Scores Over Three Time Periods for Treatment and Control
Groups
___________________________________________________________
Source SS df MS F p η²
___________________________________________________________
Between Subjects
A(Group) 62.21 1 62.21 .28 < .05 .96
Error between 1766.36 8 220.80
Within Subjects
B(Time) 156.83 2 78.41 2.44 > .05 .23
AB 279.15 2 139.57 4.34 < .05 .35
Error within 514.27 16 34.12
___________________________________________________________
Mauchly’s Sphericity W = .922; p > .05

131
END STAGE RENAL DISEASE
Table K17
2x3 Mixed Factorial ANOVA Comparing Left Quadriceps MMT
Scores Over Three Time Periods for Treatment and Control
Groups
___________________________________________________________
Source SS df MS F p η²
___________________________________________________________
Between Subjects
A(Group) 14.28 1 14.28 .04 > .05 .01
Error between 2624.67 8 328.08
Within Subjects
B(Time) 275.15 2 137.58 6.02 < .05 .43
AB 683.32 2 341.66 14.94 < .05 .65
Error within 365.90 16 22.87
___________________________________________________________
Mauchly’s Sphericity W = .350; p > .05

132
END STAGE RENAL DISEASE
Table K18
2x3 Mixed Factorial ANOVA Comparing Right Hamstrings MMT
Scores Over Three Time Periods for Treatment and Control
Groups
___________________________________________________________
Source SS df MS F p η²
___________________________________________________________
Between Subjects
A(Group) 92.58 1 92.58 .37 > .05 .04
Error between 1996.15 8 249.52
Within Subjects
B(Time) 254.32 2 127.16 3.58 > .05 .31
AB 360.50 2 180.25 5.08 < .05 .39
Error within 568.12 16 35.51
___________________________________________________________
Mauchly’s Sphericity W = .613; p > .05

133
END STAGE RENAL DISEASE
Table K19
2x3 Mixed Factorial ANOVA Comparing Left Hamstrings MMT
Scores Over Three Time Periods for Treatment and Control
Groups
___________________________________________________________
Source SS df MS F p η²
___________________________________________________________
Between Subjects
A(Group) .30 1 .30 .00 > .05 .00
Error between 3270.32 8 408.79
Within Subjects
B(Time) 128.83 2 64.41 1.97 > .05 .20
AB 314.68 2 157.34 4.80 < .05 .38
Error within 524.40 16 32.78
___________________________________________________________
Mauchly’s Sphericity W = .454; p > .05
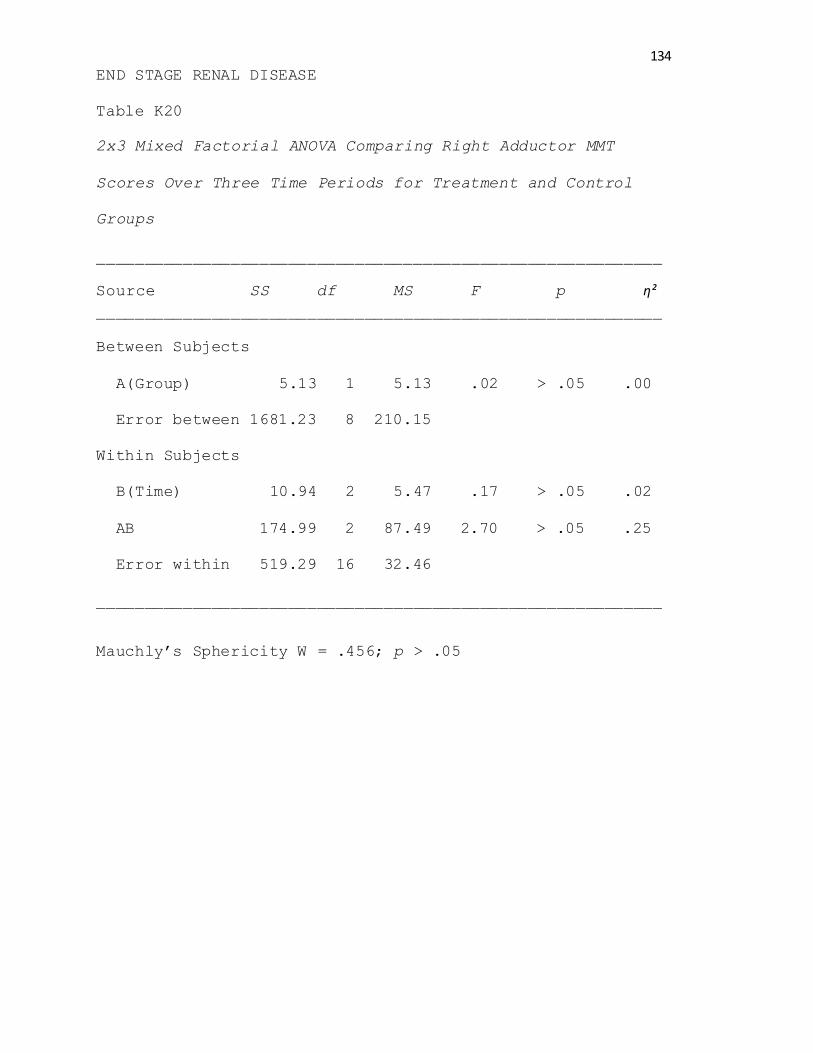
134
END STAGE RENAL DISEASE
Table K20
2x3 Mixed Factorial ANOVA Comparing Right Adductor MMT
Scores Over Three Time Periods for Treatment and Control
Groups
___________________________________________________________
Source SS df MS F p η²
___________________________________________________________
Between Subjects
A(Group) 5.13 1 5.13 .02 > .05 .00
Error between 1681.23 8 210.15
Within Subjects
B(Time) 10.94 2 5.47 .17 > .05 .02
AB 174.99 2 87.49 2.70 > .05 .25
Error within 519.29 16 32.46
___________________________________________________________
Mauchly’s Sphericity W = .456; p > .05

135
END STAGE RENAL DISEASE
Table K21
2x3 Mixed Factorial ANOVA Comparing Left Adductor MMT
Scores Over Three Time Periods for Treatment and Control
Groups
___________________________________________________________
Source SS df MS F p η²
___________________________________________________________
Between Subjects
A(Group) 91.88 1 91.88 .34 < .05 .89
Error between 2189.90 8 273.74
Within Subjects
B(Time) 66.51 2 33.25 .78 > .05 .09
AB 133.14 2 66.57 1.57 > .05 .16
Error within 679.64 16 42.48
___________________________________________________________
Mauchly’s Sphericity W = .581; p > .05

136
END STAGE RENAL DISEASE
Table K22
2x3 Mixed Factorial ANOVA Comparing Right Abductor MMT
Scores Over Three Time Periods for Treatment and Control
Groups
___________________________________________________________
Source SS df MS F p η²
___________________________________________________________
Between Subjects
A(Group) .30 1 .30 .00 > .05 .00
Error between 3456.60 8 432.08
Within Subjects
B(Time) 44.74 2 22.37 .45 > .05 .05
AB 182.35 2 91.17 1.84 > .05 .19
Error within 792.57 16 49.54
___________________________________________________________
Mauchly’s Sphericity W = .520; p > .05

137
END STAGE RENAL DISEASE
Table K23
2x3 Mixed Factorial ANOVA Comparing Left Abductor MMT
Scores Over Three Time Periods for Treatment and Control
Groups
___________________________________________________________
Source SS df MS F p η²
___________________________________________________________
Between Subjects
A(Group) 214.94 1 214.94 .59 > .05 .07
Error between 2930.73 8 366.34
Within Subjects
B(Time) 124.00 2 62.00 1.48 > .05 .16
AB 152.40 2 76.20 1.82 > .05 .19
Error within 671.61 16 41.98
___________________________________________________________
Mauchly’s Sphericity W = .462; p > .05

138
END STAGE RENAL DISEASE
BIBLIOGRAPHY
American College of Sports Medicine. Thompson, W. R.,
Gordon, N. F., Pescatello, L. S. (2009). ACSM’s
Guidelines for Exercise Testing and Prescription.
Philadelphia: Lippincott Williams & Wilkins.
Bennett, P. N., Breugelmans, L., Chan, D., Calo, M., &
Ockerby, C. (2012). A Combined Strength and Balance
Exercise Program to Decrease Falls Risk in Dialysis
Patients: A Feasibility Study. Journal Of Exercise
Physiology Online, 15(4), 26-39.
Brazier, J., Harper, R., Jones, N., O'Cathain, A., Thomas,
K., Usherwood, T., & Westlake, L. (1992). Validating
the SF-36 health survey questionnaire: New outcome
measure for primary care. British Medical Journal
(Clinical Research Ed.), 305(6846), 160-164.
Brown, E., & Johansson, L. (2010). Old age and frailty in
the dialysis population. Journal Of Nephrology, 23(5),
502-507.
Bulckaen, M., Capitanini, A., Lange, S., Caciula, A.,
Giuntoli, F., & Cupisti, A. (2011). Implementation of
exercise training programs in a hemodialysis unit:
effects on physical performance. Journal Of
Nephrology, 24(6), 790-797. doi:10.5301/JN.2011.6386

139
END STAGE RENAL DISEASE
Cheema, B., Abas, H., Smith, B., O’Sullivan, A., Chan, M.,
Patwardhan, A., & ... Fiatarone Singh, M., (2007).
Randomized controlled trial of intradialytic
resistance training to target muscle wasting in ESRD:
the Progressive Exercise for Anabolism in Kidney
Disease (PEAK) Study. American Journal Of Kidney
Diseases, 50 (4), 574-584.
Chen, J., Godfrey, S., Ng, T., Moorthi, R., Liangos, O.,
Ruthazer, R., & ... Castaneda-Sceppa, C. (2010).
Effect of intra-dialytic, low-intensity strength
training on functional capacity in adult haemodialysis
patients: A randomized pilot trial. Nephrology,
Dialysis, Transplantation: Official Publication Of The
European Dialysis And Transplant Association -
European Renal Association, 25(6), 1936-1943.
doi:10.1093/ndt/gfp739
Cook, W., Tomlinson, G., Donaldson, M., Markowitz, S.,
Naglie, G., Sobolev, B., & Jassal, S. (2006). Falls
and fall-related injuries in older dialysis patients.
Clinical Journal Of The American Society Of
Nephrology: CJASN, 1(6), 1197-1204.

140
END STAGE RENAL DISEASE
Craig, L. C. and King, T. P. (2006) Dialysis, in Methods of
Biochemical Analysis, Volume 10 (ed D. Glick), John
Wiley & Sons, Inc., Hoboken, NJ, USA.
doi: 10.1002/9780470110270.ch6
Felce, D., & Perry, J. (1995). Quality of life: Its
definition and measurement. Research in Developmental
Disabilities, 16(1), 51-74.
Freire, A., Guerra, R., Alvarado, B., Guralnik, J., &
Zunzunegui, M. (2012). Validity and reliability of the
short physical performance battery in two diverse
older adult populations in Quebec and Brazil. Journal
of Aging and Health, 24(5), 863-878.
doi:10.1177/0898264312438551
Headley, S., Germain, M., Mailloux, P., Mulhern, J.,
Ashworth, B., Burris, J., & ... Jones, M. (2002).
Resistance training improves strength and functional
measures in patients with end-stage renal disease.
American Journal of Kidney Diseases: The Official
Journal Of The National Kidney Foundation, 40(2), 355-
364.
Howden, E., Fassett, R., Isbel, N., & Coombes, J. (2012).
Exercise training in chronic kidney disease patients.
Sports Medicine (Auckland, N.Z.), 42(6), 473-488.
doi:10.2165/11630800-000000000-00000

141
END STAGE RENAL DISEASE
Johansen, K. (2005). Exercise and chronic kidney disease:
Current recommendations. Sports Medicine (Auckland,
N.Z.), 35(6), 485-499.
Johansen, K., Chertow, G., Jin, C., & Kutner, N. (2007).
Significance of frailty among dialysis patients.
Journal Of The American Society Of Nephrology: JASN,
18(11), 2960-2967.
Johansen, K., Painter, P., Sakkas, G., Gordon, P., Doyle,
J., & Shubert, T. (2006). Effects of resistance
exercise training and nandrolone decanoate on body
composition and muscle function among patients who
receive hemodialysis: A randomized, controlled trial.
Journal Of The American Society Of Nephrology: JASN,
17(8), 2307-2314.
Kemp, G., Crowe, A., Anijeet, H., Gong, Q., Bimson, W.,
Frostick, S., & ... Roberts, J. (2004). Abnormal
mitochondrial function and muscle wasting, but normal
contractile efficiency, in haemodialysed patients
studied non-invasively in vivo. Nephrology, Dialysis,
Transplantation: Official Publication Of The European
Dialysis And Transplant Association - European Renal
Association, 19(6), 1520-1527.

142
END STAGE RENAL DISEASE
Kopple, J., Wang, H., Casaburi, R., Fournier, M., Lewis,
M., Taylor, W., & Storer, T. (2007). Exercise in
maintenance hemodialysis patients induces
transcriptional changes in genes favoring anabolic
muscle. Journal Of The American Society Of Nephrology:
JASN, 18(11), 2975-2986.
Kouidi, E., Albani, M., Natsis, K., Megalopoulos, A.,
Gigis, P., Guiba-Tziampiri, O., & ... Deligiannis, A.
(1998). The effects of exercise training on muscle
atrophy in haemodialysis patients. Nephrology,
Dialysis, Transplantation: Official Publication Of The
European Dialysis And Transplant Association -
European Renal Association, 13(3), 685-699.
Kuge, N., Suzuki, T., & Isoyama, S. (2005). Does handgrip
exercise training increase forearm ischemic
vasodilator responses in patients receiving
hemodialysis? The Tohoku Journal of Experimental
Medicine, 207(4), 303-312.
Lafayette Instrument Company. (2009). Lafayette manual
muscle testing system. Retrieved from:
http://www.lafayetteevaluation.com/product_detail.asp?
itemid=26

143
END STAGE RENAL DISEASE
Lewis, M., Fournier, M., Wang, H., Storer, T., Casaburi,
R., Cohen, A., & Kopple, J. (2012). Metabolic and
morphometric profile of muscle fibers in chronic
hemodialysis patients. Journal of Applied Physiology
(Bethesda, Md.: 1985), 112(1), 72-78.
doi:10.1152/japplphysiol.00556.2011
Lo, D., Chiu, E., & Jassal, S. (2008). A prospective pilot
study to measure changes in functional status
associated with hospitalization in elderly dialysis-
dependent patients. American Journal of Kidney
Diseases: The Official Journal Of The National Kidney
Foundation, 52(5), 956-961.
doi:10.1053/j.ajkd.2008.04.010
Malagoni, A., Catizone, L., Mandini, S., Soffritti, S.,
Manfredini, R., Boari, B., & ... Manfredini, F.
(2008). Acute and long-term effects of an exercise
program for dialysis patients prescribed in hospital
and performed at home. Journal Of Nephrology, 21(6),
871-878.
Martin, H. J., Yule, V. V., Syddall, H. E., Dennison, E.
M., Cooper, C. C., & Sayer, A. (2006). Is Hand-Held
Dynamometry Useful for the Measurement of Quadriceps
Strength in Older People? A Comparison with the Gold

144
END STAGE RENAL DISEASE
Standard Biodex Dynamometry. Gerontology, 52(3), 154-
159. doi:10.1159/000091824
McIntyre, C., Selby, N., Sigrist, M., Pearce, L., Mercer,
T., & Naish, P. (2006). Patients receiving maintenance
dialysis have more severe functionally significant
skeletal muscle wasting than patients with dialysis-
independent chronic kidney disease. Nephrology,
Dialysis, Transplantation: Official Publication of The
European Dialysis And Transplant Association -
European Renal Association, 21(8), 2210-2216.
Orcy, R., Dias, P., Seus, T., Barcellos, F., & Bohlke, M.
(2012). Combined resistance and aerobic exercise is
better than resistance training alone to improve
functional performance of haemodialysis patients--
results of a randomized controlled trial.
Physiotherapy Research International: The Journal for
Researchers and Clinicians in Physical Therapy, 17(4),
235-243. doi:10.1002/pri.1526
Painter, P. (2005). Physical functioning in end-stage renal
disease patients: Update 2005. Hemodialysis
International. International Symposium on Home
Hemodialysis, 9(3), 218-235.

145
END STAGE RENAL DISEASE
Petersen, A., Leikis, M., McMahon, L., Kent, A., & McKenna,
M. (2009). Effects of endurance training on extrarenal
potassium regulation and exercise performance in
patients on haemodialysis. Nephrology, Dialysis,
Transplantation: Official Publication of the European
Dialysis And Transplant Association - European Renal
Association, 24(9), 2882-2888. doi:10.1093/ndt/gfp157
Sakkas, G., Ball, D., Mercer, T., Sargeant, A., Tolfrey,
K., & Naish, P. (2003). Atrophy of non-locomotor
muscle in patients with end-stage renal failure.
Nephrology, Dialysis, Transplantation: Official
Publication of the European Dialysis and Transplant
Association - European Renal Association, 18(10),
2074-2081.
Segura-Ortí, E., Kouidi, E., & Lisón, J. (2009). Effect of
resistance exercise during hemodialysis on physical
function and quality of life: Randomized controlled
trial. Clinical Nephrology, 71(5), 527-537.
Smart, N., Titus, T. Outcomes of Early versus Late
Nephrology Referral in Chronic Kidney Disease: A
Systematic Review. American Journal of Medicine.
November 2011; 124(11): 1073-1080. E2.

146
END STAGE RENAL DISEASE
Storer, T., Casaburi, R., Sawelson, S., & Kopple, J. (
2005). Endurance exercise training during
haemodialysis improves strength, power, fatigability
and physical performance in maintenance haemodialysis
patients. Nephrology, Dialysis, Transplantation:
Official Publication of the European Dialysis and
Transplant Association - European Renal Association,
20(7), 1429-1437.
Wilund, K., Tomayko, E., Wu, P., Ryong Chung, H.,
Vallurupalli, S., Lakshminarayanan, B., & Fernall, B.
(2010). Intradialytic exercise training reduces
oxidative stress and epicardial fat: a pilot study.
Nephrology, Dialysis, Transplantation, 25(8), 2695-
2701.
Related Documents
![Thesis Agrawal[1]](https://static.cupdf.com/doc/110x72/545abd35b1af9f39378b5eba/thesis-agrawal1.jpg)










![Thesis ROBOGUN[1]](https://static.cupdf.com/doc/110x72/577d2cb81a28ab4e1eacb48b/thesis-robogun1.jpg)