1 S3-Leitlinie Therapie der Psoriasis vulgaris - Leitlinienreport AWMF-Register-Nr.: 013 - 001, 2021 ICD-10 Code: L40.0 Schlagworte: Psoriasis, Psoriasis vulgaris, Systemtherapie Psoriasis, Topische Therapie Psoriasis Zitation der Leitlinie: Nast A et al. Deutsche S3-Leitlinie zur Therapie der Psoriasis vulgaris, adaptiert von EuroGuiDerm. (2021) Zitation des Leitlinienreports: Dressler C, Nast A. Guideline development report: Update of the German S3 guideline for the treatment of psoriasis vulgaris. (2021) Leitlinienkoordination: Prof. Dr. Alexander Nast

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
S3-Leitlinie
Therapie der Psoriasis vulgaris - Leitlinienreport
AWMF-Register-Nr.: 013 - 001, 2021
ICD-10 Code: L40.0
Schlagworte: Psoriasis, Psoriasis vulgaris, Systemtherapie Psoriasis, Topische Therapie Psoriasis
Zitation der Leitlinie: Nast A et al. Deutsche S3-Leitlinie zur Therapie der Psoriasis vulgaris, adaptiert von EuroGuiDerm. (2021)
Zitation des Leitlinienreports: Dressler C, Nast A. Guideline development report: Update of the German S3 guideline for the treatment of psoriasis vulgaris. (2021)
Leitlinienkoordination: Prof. Dr. Alexander Nast

2
Guideline development report: Update of the German S3 guideline for the treatment of psoriasis vulgaris
Authors:
Dr. Corinna Dressler, MSc1
Prof. Dr. med. Alexander Nast1
Institution: 1 Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin, Humboldt-
Universität zu Berlin, and Berlin Institute of Health; Department of Dermatology, Venereology und
Allergy, Division of Evidence-Based Medicine (dEBM)
Corresponding author:
Dr. Corinna Dressler, MSc
Division of Evidence-Based Medicine,
Department of Dermatology, Venereology and Allergy
Charité – Universitätsmedizin Berlin
Charitéplatz 1
10117 Berlin
Germany
Tel.: + 49 30 450 518 373
Fax: + 49 30 450 7518 977
Keywords: Psoriasis [MeSH], Guideline [MeSH], Evidence-Based Medicine [MeSH], methods report, Review [MeSH]

3
Contents Guideline Development Group .......................................................................................................... 4
Introduction ........................................................................................................................................ 5
Nomination of experts........................................................................................................................ 5
Management of Conflict of Interests ................................................................................................. 6
Funding ................................................................................................................................................ 7
The guideline development process: selecting the focus ................................................................. 7
National adaption process of the EuroGuiDerm guideline ............................................................... 7
External consultation and approval of German guideline ................................................................ 9
Dissemination, implementation and evaluation of the German guideline ...................................... 9
Updating the guideline ..................................................................................................................... 10
Research priorities (in line with EuroGuiDerm) ............................................................................... 12
Cost and economic considerations .................................................................................................. 12
Population and health questions covered by the guideline ........................................................... 13
Selecting and specifying guideline questions .................................................................................. 14
Search methods and results, evidence selection & critical appraisal of evidence ......................... 14
Developing background texts ........................................................................................................... 16
Developing recommendations and the consensus process ............................................................ 17
References ........................................................................................................................................ 20
Appendix A: Declarations of Interest ............................................................................................... 21

4
Guideline Development Group
Title Surname First Name Role and Affiliation Nominating organization
Expert panel
Dr. med. Altenburg Andreas Dermatologist; Dermatologie, Venerologie und Allergologie, Immunologisches Zentrum, Städtisches Klinikum Dessau DDG
Prof. Dr. med. Augustin Matthias Pharmacoeconomics, dermatologist; Universitätsklinikum Hamburg-Eppendorf, Institut für Versorgungsforschung in der Dermatologie und bei Pflegeberufen
DDG
Prof. Dr. med. Boehncke Wolf-Henning Dermatologist; Service de Dermatologie et Vénéréologie, Hôpitaux Universitaires de Genève DDG
Prof. Dr. med. Härle Peter Rheumatologist, Katholisches Klinikum Mainz, Zentrum für Rheumatologische Akutdiagnostik, Klinik für Rheumatologie, Klinische Immunologie und Physikalische Therapie
DGRh
Prof. Dr. med. Mrowietz Ulrich Dermatologist; ; Psoriasis-Zentrum, Klinik für Dermatologie, Venerologie, Allergologie, Universitätsklinikum Schleswig-Holstein, Campus Kiel
DDG
Prof. Dr. med. Ockenfels Hans-Michael Dermatologist; ,Haut- und Allergieklinik, Klinikum Hanau BVDD
Dr. med. Philipp Sandra Office-based dermatologist, Brandenburg DDG
Prof. Dr. med. Reich Kristian Dermatologist; Dermatologikum Hamburg DDG
PD Dr. med. Rosenbach Thomas Office-based dermatologist, Osnabrück BVDD
Dr. med. Schlaeger Martin Office-based dermatologist, Oldenburg BVDD
Prof. Dr. med. Schmid-Ott Gerhard Psychiatrist, Berolina Klinik, Löhne DGPPR
Dr. med. Sebastian Michael Office-based dermatologist, Mahlow BVDD
Dr. med. von Kiedrowski Ralph Office-based dermatologist, Selters BVDD
PD Dr. med. Weberschock Tobias
Dermatologist; Klinik für Dermatologie, Venerologie und Allergologie, Universitätsklinikum Frankfurt, Frankfurt/Main und Arbeitsgruppe EbM Frankfurt, Institut für Allgemeinmedizin, Goethe-Universität Frankfurt, Frankfurt/Main
DDG
Patient representatives
Klaus Joachim Deutscher Psoriasis Bund e.V. DPB
Koza Joachim Deutscher Psoriasis Bund e.V. DPB
Methodologists and coordinating research team
Dr. Dressler Corinna dEBM n/a
Prof. Dr. med. Nast Alexander dEBM n/a
Notes: BVDD = Berufsverband der Deutschen Dermatologen (Professional Association of German Dermatologists); DDG = Deutsche Dermatologische Gesellschaft (German Society of Dermatology); dEBM = Division of Evidence-Based Medicine; DGPPR = Deutsche Gesellschaft für klinische Psychotherapie und Psychosomatische Rehabilitation (German Association for Clinical Psychotherapy and Psychosomatics); DGRh = Deutsche Gesellschaft für Rheumatologie (German Society of Rheumatology); DPB = Deutscher Psoriasis Bund (German Psoriasis Alliance)

5
Introduction This report describes the methods and processes used to develop the 2020 update of the German
evidence- and consensus-based (S3) guideline for the treatment of psoriasis vulgaris (Deutsche S3-
Leitlinie zur Therapie der Psoriasis vulgaris – Update 2020, AWMF Registry No. 013/001).
The copyright lies with the German Dermatological Society (DDG) except for pages 13 – 20 for which
the copyright lies with the European Dermatology Forum (EDF). This report is licensed under CC BY NC.
The update of this guideline has been published in the Journal of the German Society of Dermatology
(Journal der Deutschen Dermatologischen Gesellschaft). When citing the guideline, please use one or
more of the references below depending on the language version and parts of the guideline you are
referring to:
• German version:
o Nast A et al. Deutsche S3-Leitlinie zur Therapie der Psoriasis vulgaris, adaptiert von
EuroGuiDerm – Teil 1: Therapieempfehlungen und Monitoring. 2021. J Dtsch Dermatol
Ges (in print)
o Nast A et al. Deutsche S3-Leitlinie zur Therapie der Psoriasis vulgaris, adaptiert von
EuroGuiDerm – Teil 2: Therapiemonitoring, besondere klinische Situationen und
Vorliegen von Komorbidität. 2021. J Dtsch Dermatol Ges (in print)
• English version:
o Nast A et al. German S3-Guideline on the treatment of Psoriasis vulgaris, adapted from
EuroGuiDerm – Part 1: Treatment goals and treatment recommendations. 2021. J
Dtsch Dermatol Ges (in print)
o Nast A et al. German S3-Guideline on the treatment of Psoriasis vulgaris, adapted from
EuroGuiDerm – Part 2: Part 2: Treatment monitoring and specific clinical or comorbid
situations. 2021. J Dtsch Dermatol Ges (in print)
Nomination of experts
Experts were nominated by German scientific medical societies (dermatology, psychiatry and
psychosomatic medicine, rheumatology). A nominated rheumatologist reviewed the chapter on
psoriatic arthritis. A list of the experts is given above (each person had one vote).
To be eligible for nomination and participation, an individual had to fulfil at least one of the following
criteria:
- Extensive clinical experience in the treatment of psoriasis
6
- Relevant publications in the field of psoriasis
- Relevant experience in evidence-based medicine
Additionally, patient representatives were recruited by the German Psoriasis Patient Association
(Deutscher Psoriasis Bund). Patient representatives had one vote each.
Management of Conflict of Interests
All members of the guideline development group completed and returned conflict of interest forms
before the first meeting (kick-off meeting) in February 2019. The forms were developed by the AWMF
specifically for use in the development of clinical practice guidelines (version 2018) [1].
Conflicts of interests were classified as minimal, moderate or severe, as recommended by the AWMF
in its algorithm for managing conflicts of interest [1]. The head of the dEBM (Alexander Nast, AN), who
chaired the group throughout the guideline development process, also completed a conflict of interest
form. His declaration was evaluated externally by the president of the German Society of Dermatology.
These and the conflict of interest declarations of the group members can be found in Appendix A.
The overview of conflicts of interest was presented by the chair and then discussed with the entire
group. The group agreed unanimously to follow the AWMF requirements that:
(a) the group be facilitated during its meetings by a member without relevant conflicts of interest;
(b) experts abstain from voting on recommendations in which they have conflicts of interest that
have been rated as moderate; and
(c) experts with severe conflicts of interest not be permitted to take part in the group.
Definition of COI classification:
• None: no direct personal honoraria, no research grants (or minor research funding e.g. <
10.000) from companies that may have a relevant benefit from the guideline’s
recommendations
• Minimal: less than moderate
• Moderate: personal honoraria (e.g. total >4,000€/year) or research grants >50,000€, from
companies that may have a relevant benefit from the guideline’s recommendations
• Severe: Employment by or significant share of personal income from companies that may have
a relevant benefit from the guideline’s recommendations
Particular relevance for assessment: time period “kick-off-event” till final consensus conference
of guideline, as well as period one year before project initiation.

7
Voting abstentions during the consensus conference were recorded in the conference protocols. These
are available upon request.
Funding
The adaptation process of the guideline was funded exclusively through the guideline-funding program
of the Germany Dermatological Society (DDG). The members of the guideline development group
received no payments for their work. The guideline development group worked independently and the
DDG had no influence on the focus or content of the guideline.
The guideline development process: selecting the focus
The group held an initial kick-off meeting online to decide the strategy for updating the previous
version of the guideline. Key questions and relevant outcomes were also discussed, see below.
Additionally, the definitions of „disease severity“ and „treatment goals“ were discussed with the aim
of updating the text.
Selection of key questions and relevant outcomes
a) UV treatment (2011): No major changes/no new evidence, a critical literature review was not
deemed necessary
b) Topical treatment (2011): No major changes/no new evidence, a critical literature review was not
deemed necessary
c) Systemic treatment: Add new chapter for each newly approved drug; amend existing chapters if
necessary
In the past, the German evidence- and consensus-based (S3) guideline for the treatment of psoriasis
vulgaris had been developed in close cooperation with the European Psoriasis Guideline and other
national guidelines (e.g. Dutch Psoriasis Guideline). Therefore, an adaptation of the EuroGuiDerm
guideline for the systemic treatment psoriasis vulgaris would save time and resources.
For the 2020 update, an even tighter pan-European cooperation was initiated under the name of
EuroGuiDerm guideline development. The 2020 Update of the European/EuroGuiDerm Psoriasis
Guideline was developed by the “EuroGuiDerm – Centre for Guidelines Development”. EuroGuiDerm
brings together multiple national societies to develop a European Guideline to serve as a draft for
national adaptation. A multi national Methods Board newly developed a Methods Manual. For more
information, please see https://www.edf.one/de/home/Guidelines/EDF-EuroGuiDerm.html.
National adaption process of the EuroGuiDerm guideline
The national societies planning to adapt the European psoriasis guideline were involved in several
working steps on the European level:

8
i) Input into scoping processes and hence, the focus of the EuroGuiDerm psoriasis guideline, approval
of key questions and methods
ii) Participation in the external review/ approval of the EuroGuiDerm psoriasis guideline
iii) In addition, a national consensus process was initiated to reconfirm or adapt the recommendations
on the national level.
i) Input during the scoping process of the EuroGuiDerm guideline
A scoping document was developed by EuroGuiDerm and presented to the German expert group for their input.
The aim of the scoping process is to identify:
• Areas with the greatest potential for improvement of skin health and reducing skin health inequalities in Europe
• Possible obstacles to putting future dermatological guideline and consensus statement recommendations into practice in Europe
• Uncertainty or disagreement on best practice • Potential to improve outcomes or make better use of resources • Identify areas that change rapidly
The German psoriasis guideline development group approved the scoping document, the further
suggested procedure, the outline and methods as well as the selected key questions and selected
outcomes of the EuroGuiDerm psoriasis guideline.
ii) Participation in the external review AND approval of the EuroGuiDerm guideline
The consultation draft of the EuroGuiDerm guideline was presented to the German guideline
development group in a modified online Delphi voting process. We used an online survey tool (Lime
Survey) to present the draft chapter by chapter. Each person was asked to read the chapter and then
vote on a) the text and b) on the recommendations individually. Each person was asked to either agree
(and therefore approve) or disagree with the text/recommendations. In case someone disagreed, it
was mandatory to submit alternative suggestions. The results were collected and fed back to the
EuroGuiDerm guideline development group. Approval rates were calculated.
iii) The national consensus process
In addition to the modified Delphi process described above, three online consensus conferences took
place. During the three consensus conferences, all chapters of the EuroGuiDerm psoriasis guideline
were discussed:
a) Comments submitted by the German group during the external review phase were presented to all
members, any changes to the EuroGuiDerm guideline resulting from these comments were presented;
the supporting evidence was reviewed again, where applicable. The group discussed these changes.

9
b) In general, the group discussed all comments submitted during the German online pre-voting,
chapter by chapter, recommendation by recommendation. The group decided whether the
text/recommendations can be accepted within the German health care setting or if there is a need for
change.
According to the steps for a nominal group technique, all comments from the online pre-voting were
noted, discussed in rounds one by one, which was followed by pre-voting, final discussion, and final
consensus voting.
The discussion was moderated by Prof. Dr. Alexander Nast (AWMF Guideline Adviser). All nominated
experts and the patient representatives were entitled to vote. Abstentions due to COI were noted. A
strong consensus was the primary goal, which was defined a prior as>95% agreement. If that could not
be achieved after extended discussion, consensus (≥75% agreement) was accepted.
The wording of recommendations was translated, as explained in TABLE 6.
External consultation and approval of German guideline
The final version of the adapted guideline was sent to the German Dermatological Society (DDG) and
the German professional association of Dermatologist (Berufsverband der Deutschen Dermatologen;
BVDD) for final approval. It was also reviewed by the other involved stakeholders (see above including
the patient organisation) and by the reviewers of the Journal of the German Dermatological Society.
All comments received were collected and reviewed. Minor changes concerning spelling or grammar
were incorporated by the dEBM. Substantial comments were compiled in an overview document.
Subsequently, all comments were submitted to the members of the German guideline development
group and by discussion. Decisions were documented. All reviewers received feedback to their
comments. An anonymised version of all comments, feedback and actions taken are available upon
request. Final approval for the guideline was given on 19.02.2021 by the members of the German
guideline group. The representatives of the involved scientific societies approved the guideline
(procura).
Dissemination, implementation, and evaluation of the German guideline
The success of a guideline depends on whether it is accepted and used in clinical practice. To this end,
the present guideline will be produced in a short and long version available on the dEBM psoriasis
website and the AWMF homepage, as well as in print and online in the JDDG. It will also continue to
be publicized and discussed in seminars and other events of the BVDD and DDG. Furthermore, all of
the experts involved in the development of the guideline were encouraged to give talks and present
the results and recommendations of the guideline at conferences.

10
Early introduction of students and residents to medical guideline has been recognized as an important
tool of guideline implementation.
A dissemination plan has been developed in the with the DDG/BVDD internal SOP, see below.
Measuring the impact of a guideline is difficult given that treatment decisions are made on a case-by-
case basis and take many individual factors into account. There is therefore no practical, universally
applicable test to determine whether optimal treatment decisions have been made in everyday clinical
practice. It is, however, possible to explore whether changes in certain aspects of practice, such as
prescribing behaviour, have taken place over time and are associated with the publication of a
guideline. An analysis of such changes and of doctors’ awareness of the psoriasis S3 guideline is
planned as part of the dEBM’s continuing guideline development work.
Updating the guideline
Clinical practice guidelines should ideally be updated at regular intervals to account for changes in
technologies and evidence, as well as policy and infrastructure. While conventional treatments for
psoriasis vulgaris are unlikely to change substantially in the near future, advances in systemic
treatments using biologics will probably require a partial or full update within several years.
Since this guideline is based on the Living EuroGuiDerm guideline, the German guideline development
group will closely follow the developments on the European level, the update of the Cochrane Review,
which the EuroGuiDerm guideline used, and decide when chapters need to be updated. The guideline
will be re-evaluated for its content, usability, and timeliness yearly.

11
TABLE 1: DISSEMINATION PLAN
Audience Responsible person
Communication and implementation tools to be used Time at which they are to be developed, piloted or to take place
Is dEBM support needed, and if yes what kind of support?
Dermatologist & researchers, societies, pharmaceutical companies
dEBM Team Full guideline & methods report, decision grid I +II & flow chart:
• AWMF website
After final approval by DDG/BVDD to manage submission
Dermatologist & researchers, societies, pharmaceutical companies
ANast Implementation slides After final approval by DDG/BVDD to manage communication with the press (Martin Dittmann)
Dermatologist & researchers
ANast Journal publication (JDDG) After external review to coordinate, format and submit; assist with the translation (Matthew Gaskins)
Dermatologist & researchers, societies, pharmaceutical companies
DDG/BVDD guideline office
Communication and dissemination in line with the SOP When new and every 3 months Martin Dittmann
Dermatologist & researchers, societies,
CDressler& Martin Dittmann
Website presenting material including updates After external review Martin Dittmann

Research priorities (in line with EuroGuiDerm)
• -Which are the predictors for treatment success or the occurrence of adverse events?
• -What is the role of therapeutic drug monitoring?
• -When should a treatment be stopped in case of clearance?
• -Which treatments can be combined safely and lead to improved efficacy?
• What is the most suitable treatment option in given comorbid situations?
Cost and economic considerations
Cost and economic considerations were discussed (Wirtschaftlichkeitsgebot).

13
The following sections are taken from the methods report of the ‘EuroGuiDerm guideline for the systemic treatment of psoriasis vulgaris1’. They equally apply to the German setting
Population and health questions covered by the guideline The target population are adult patients with psoriasis vulgaris, moderate to severe severity, and adult patients with psoriasis arthritis, who have also been diagnosed with moderate to severe psoriasis vulgaris. This guideline applies to both, hospital and practice based (private and public) dermatologists. Leading health questions - all referring to adult individuals (male/female/indeterminate) with moderate or severe plaque type psoriasis – are :
- Which treatment option should be chosen with regard to patients’ needs, taking efficacy, safety/tolerability of the different treatment options and comorbidities into consideration?
- How should the selected treatment option best be managed and monitored? - How should frequent comorbid situations (e.g. concomitant arthritis) best be managed?
The relevant interventions discussed during the kick-off conference are listed in Table 2. This list was generated based on the update of the Cochrane review on systemic treatments for psoriasis vulgaris [2], which we collaborated with. The subcommittee decided to exclude those that are crossed out in Table 2 because they were not licensed for psoriasis vulgaris at that time. Relevant comparison are head-to-head studies of the below mentioned drugs or versus placebo. The outcomes chosen are: 90% improvement in the Psoriasis Area Severity Index (PASI 90) and severe adverse events (SAEs), and PASI 75 and adverse events (AEs)2. We worked in collaboration with the team updating the Cochrane review.
TABLE 2: SYSTEMIC INTERVENTIONS FOR PSORIASIS VULGARIS
Systemic conventional treatments
Small molecules
Anti-TNF alpha Anti-IL12/23
Anti-IL17 Anti-IL23
FAEs Apremilast Infliximab Ustekinumab Secukinumab Tildrakizumab
Acitretin Tofacitinib Etanercept Brodalumab Guselkumab
Ciclosporin BMS-986165 Adalimumab Ixekizumab Rizankizumab
Methotrexate Certolizumab Bimekizumab Mirikizumab
- treatments crossed out are included in the Cochrane Review but not in the guideline
Additionally, the below listed comorbidities and special situations are addressed by the guideline.
TABLE 3: OVERVIEW OF TOPICS & KEY QUESTION IN RELATION TO COMORBIDITIES AND SPECIAL PATIENT
POPULATIONS/ISSUES
TOPIC QUESTION(S)
Psoriatic arthritis - How should psoriasis patients with concomitant psoriatic arthritis be managed?
Inflammatory bowel disease - How should psoriasis patients with inflammatory bowel disease be managed?
1 Available at: https://www.edf.one/de/home/Guidelines/EuroGuiDerm-psoriasis-vulgaris.html CC BY NC Copyright @ EDF, 2 The Cochrane Review 2020 reported PASI75 and AE outcome data as secondary analysis, see sections:
PASI75 Analysis 3.1 – 3.10 (pages 469 – 505) and AE Analysis 6.1.- 6.10 (pages 528 – 536)

14
Cancer - How should psoriasis patients with a history of malignancies be managed?
Depression - How should psoriasis patients with a history of depression and/or suicidal ideation be managed?
Diabetes mellitus - How should psoriasis patients with diabetes mellitus be managed?
Heart disease - How should psoriasis patients with ischaemic heart disease and/or congestive heart failure be managed?
Kidney disease - How should psoriasis patients with kidney failure / renal impairment be managed?
Neurology - Which treatments are appropriate for psoriasis patients with neurological diseases?
Hepatitis - When and how should psoriasis patients be screened for viral hepatitis and how should patients who test positive be managed?
Tuberculosis screening - How to screen for tuberculosis before and during biologic treatment
Tuberculosis and treatment - How to manage psoriasis in patients with positive tuberculosis test results
Pregnancy - How should psoriasis patients with a wish for pregnancy in the near future or who are pregnant be managed?
Vaccinations - How should vaccinations in psoriasis patients on systemic treatment be managed?
Immunogenicity - What is the role of anti-drug antibodies in biologic treatments?
COVID 19 - Guidance for systemic therapy of psoriasis during Covid 19 pandemic
Selecting and specifying guideline questions
This guideline is an update of the European Psoriasis Guideline 2015 & 2017 [3, 4]. The subcommittee considered the range of topics addressed in the previous version(s) as well as new ones, and then choose the key questions to focus on accordingly during the kick-off meeting (see Table 3).
Search methods and results, evidence selection & critical appraisal of evidence
We were aware that the Cochrane Review “Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis” published in 2017 is a living review and an update was underway. Since Cochrane reviews represent the gold standard with regard to methodological rigor, a member of the EuroGuiDerm Team (CD) joined the Cochrane Team to support efficient work and save resources and to foster the production of one rigorously conducted, high quality systematic review and network-meta analysis. The methods used in the conduct of this review are transparently reported in the full review document : https://doi.org/10.1002/14651858.CD011535.pub3.
Additionally, we developed an evidence to decision framework outlining: PICO, setting, perspective, purpose of the guideline & research evidence on problems (based on the scoping process), benefits & harms of the interventions (evidence from above mentioned review), and also different disease definitions & treatment goals to foster national considerations/implementation options. We included a flow chart and a decision grid, which display the most important recommendations. The subcommittee reviewed this framework, comments were integrated, final version see Appendix 1 of the EuroGuiDerm methods report.

15
Furthermore, a number of special topics were supported by systematic searched or systematic literature reviews. A detailed description of the methods and procedures applied to review and evaluate the literature for each chapter on special patient populations/specific treatment circumstances are provided in the appendix. An overview is show in Table 4, all details are reported in the Appendices. TABLE 4: OVERVIEW OF SPECIFIC TOPICS & TYPE OF EVIDENCE REVIEW THE RECOMMENDATIONS ARE BASED ON
Topic Type of evidence review
Evidence review methods for part 1: general recommendation for adult patients with plaque type psoriasis:
Psoriasis vulgaris Sbidian E, Chaimani A, Afach S, Doney L, Dressler C, Hua C, Mazaud C, Phan C, Hughes C, Riddle D, Naldi L, Garcia-Doval I, Le Cleach L. Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis. Cochrane Database of Systematic Reviews 2020, Issue 1. Art. No.: CD011535. DOI: 10.1002/14651858.CD011535.pub3.
The methods are reported in the full review document : https://doi.org/10.1002/14651858.CD011535.pub3 (also available upon request [email protected] )
A protocol 'Systemic pharmacological treatments for chronic plaque psoriasis' (Sbidian 2015) was published for the first review. This review is an update of 'Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis' (Sbidian 2017).
Evidence review methods for part 2: specific recommendations for adult patients with plaque type psoriasis and comorbid conditions and/or specific issues:
Psoriasis Arthritis Update of a systematic review, Evidence to decision framework developed
Inflammatory Bowel Disease Narrative review by co-authors
Cancer Systematic search, a methodologist with medical background from the EuroGuiDerm Team conducted a topic specific but non-systematic screening
Depression Systematic search, a methodologist with medical background from the EuroGuiDerm Team conducted a topic specific but non-systematic screening
Diabetes mellitus Systematic review
Heart Disease Systematic search, a methodologist with medical background from the EuroGuiDerm Team conducted a topic specific but non-systematic screening
Kidney Disease Narrative review
Neurological diseases Narrative review
Viral hepatitis Systematic review
Tuberculosis Screening Systematic search, a methodologist with medical background from the EuroGuiDerm Team conducted a topic specific but non-systematic screening
Tuberculosis Treatment Systematic search, a methodologist with medical background from the EuroGuiDerm Team conducted a topic specific but non-systematic screening
Pregnancy Systematic search, a methodologist with medical background from the EuroGuiDerm Team conducted a topic specific but non-systematic screening
Vaccinations Narrative review by co-author
COVID19 Narrative review by co-authors
16
Immunogenicity Narrative review by author
Several chapters /author groups were supported by a methodologist who conducted systematic search. The non-systematic selection of published materials was not restricted by publication type. Guideline were included, also from other specialities. Additionally, we used the AGREE II instrument domain 8 to evaluate [5] the identified guidelines. The evaluations are included in the Appendix 12 of the EuroGuiDerm methods report. There were 13 guidelines referred to with regards to the “specific circumstances” chapters. Only two were not evidence based.
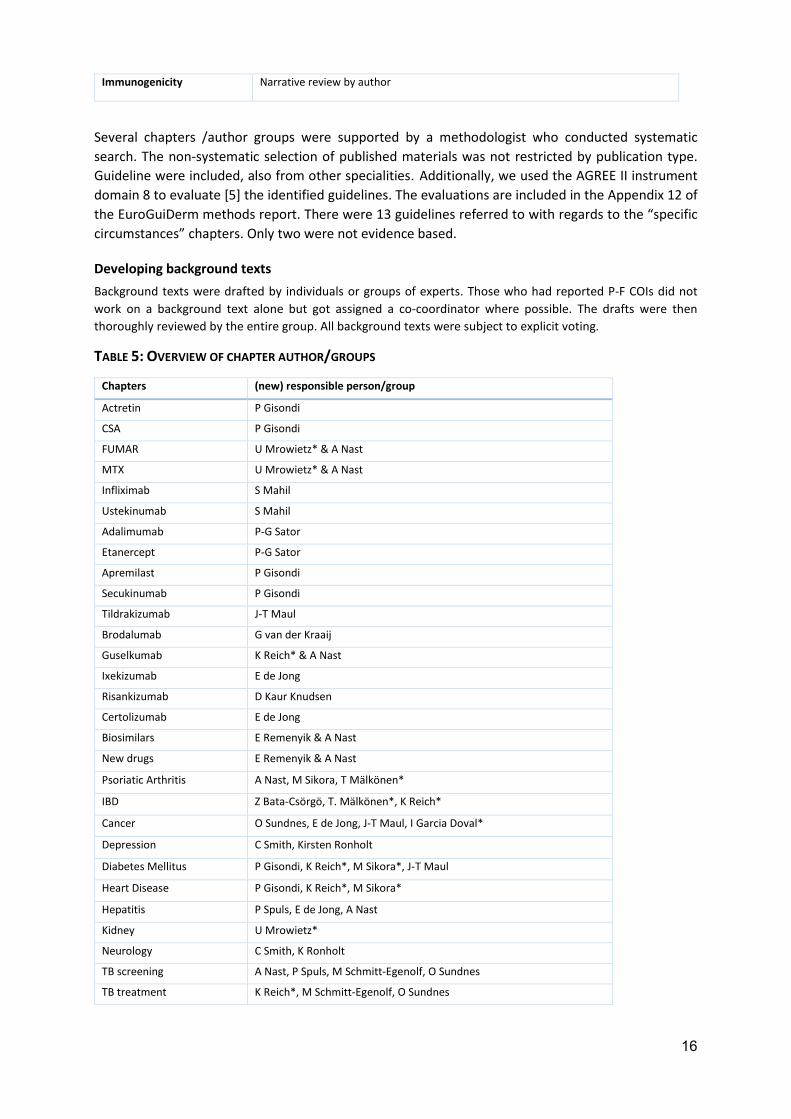
Developing background texts Background texts were drafted by individuals or groups of experts. Those who had reported P-F COIs did not work on a background text alone but got assigned a co-coordinator where possible. The drafts were then thoroughly reviewed by the entire group. All background texts were subject to explicit voting.
TABLE 5: OVERVIEW OF CHAPTER AUTHOR/GROUPS
Chapters (new) responsible person/group
Actretin P Gisondi
CSA P Gisondi
FUMAR U Mrowietz* & A Nast
MTX U Mrowietz* & A Nast
Infliximab S Mahil
Ustekinumab S Mahil
Adalimumab P-G Sator
Etanercept P-G Sator
Apremilast P Gisondi
Secukinumab P Gisondi
Tildrakizumab J-T Maul
Brodalumab G van der Kraaij
Guselkumab K Reich* & A Nast
Ixekizumab E de Jong
Risankizumab D Kaur Knudsen
Certolizumab E de Jong
Biosimilars E Remenyik & A Nast
New drugs E Remenyik & A Nast
Psoriatic Arthritis A Nast, M Sikora, T Mälkönen*
IBD Z Bata-Csörgö, T. Mälkönen*, K Reich*
Cancer O Sundnes, E de Jong, J-T Maul, I Garcia Doval*
Depression C Smith, Kirsten Ronholt
Diabetes Mellitus P Gisondi, K Reich*, M Sikora*, J-T Maul
Heart Disease P Gisondi, K Reich*, M Sikora*
Hepatitis P Spuls, E de Jong, A Nast
Kidney U Mrowietz*
Neurology C Smith, K Ronholt
TB screening A Nast, P Spuls, M Schmitt-Egenolf, O Sundnes
TB treatment K Reich*, M Schmitt-Egenolf, O Sundnes

17
Pregnancy C Smith, S Mahil, E de Jong, J-T Maul
Vaccinations U Mrowietz, N Yawalkar
COVID-19 P Gisondi, M Sikora, U Mrowietz*
Immunogenicity K Reich*
* P-F COIs
Developing recommendations and the consensus process
Recommendations were drafted by the chapter co-authors. As detailed in Table 4 the general recommendations for the treatment of psoriasis vulgaris as well as the recommendations for hepatitis, diabetes mellitus and psoriasis arthritis are evidence and consensus-based recommendations. For each of these a systematic review had been conducted.
Co-authors submitted draft background texts and the drafted recommendations, at times multiple suggestion with different strength and/or wording, all of which were subject to (pre-)voting.
Three consensus conferences were scheduled. Prior to each one, an online survey tool (limesurvey) was used so that each member of the guideline development subcommittee was able to have time to read each draft including the suggested recommendations and vote3. Voters were able to agree or disagree with a) the text and b) the recommendation(s). In case of disagreement, it was mandatory to give a reason why and cite supporting literature. Subcommittee members were hence able to vote without others being present or seeing what others had chosen. This made it possible for members who may be less comfortable to engage in group discussions to participate.
The consensus conferences were online conference for which participants dialled in by telephone. We used a screen sharing tool to show the drafts that were discussed. The conferences took place on 27 November 2019, 3 December 2019, 4 February 2020.
Each chapter/topic was discussed separately. The EuroGuiDerm Team prepared the drafts showing the pre-voting results and any comments submitted during online voting. No names were displayed to foster an open discussion.
Alexander Nast facilitated all three consensus conferences. He presented results from the pre-voting alongside the background text and after discussion, the recommendation(s). After each section he opened up the floor for discussion. Benefits, harms, processes and procedures were extensively discussed. The nominal group techniques was chosen to facilitate the consensus process [6]. As suggested by the EuroGuiDerm Methods Manual, the (pre-)votes of those with personal financial COIs were not counted.
In accordance with the EuroGuiDerm Manual, we used phrasing suggested by the GRADE Working Group to standardize the wording of all recommendations [7]. This is reported as show in Table 6. The strength of the consensus is also reported. Recommendations and texts were discussed and voted upon until a majority of more than 50% agreed.
TABLE 6: WORDING OF RECOMMENDATIONS [8-11]
Strength Wording Symbols Implications
3 The drafts on depression, malignancy, guselkumab and certolizumab were circulated prior to the final consensus conference but no pre-voting took place due to a lack of time.

18
Strong recommendation for the use of an intervention
‘We recommend . . .’
„es wird empfohlen“/ „wir empfehlen“
↑↑ We believe that all or almost all informed people would make that choice. Clinicians will have to spend less time on the process of decision-making, and may devote that time to overcome barriers to implementation and adherence. In most clinical situations, the recommendation may be adopted as a policy.
Weak recommendation for the use of an intervention
‘We suggest . . .’
„es kann empfohlen werden”
↑ We believe that most informed people would make that choice, but a substantial number would not. Clinicians and health care providers will need to devote more time on the process of shared decision-making. Policy makers will have to involve many stakeholders and policy making requires substantial debate.
No recommendation with respect to an intervention
‘We cannot make a recommendation with respect to . . .’
„es kann keine Empfehlung für oder gegen … ausgesprochen werden”
0 At the moment, a recommendation in favour or against an intervention cannot be made due to certain reasons (e.g. no reliable evidence data available, conflicting outcomes, etc.)
Weak recommendation against the use of an intervention
‘We suggest against . . .’
„es kann nicht empfohlen werden”
↓ We believe that most informed people would make a choice against that intervention, but a substantial number would not.
Strong recommendation against the use of an intervention
‘We recommend against . . .’
„es wird nicht empfohlen ”
↓↓ We believe that all or almost all informed people would make a choice against that intervention. This recommendation can be adopted as a policy in most clinical situations.
TABLE 7: STRENGTH OF CONSENSUS
100 % consensus 100% agreement
Strong consensus Agreement of >95% participants

19
Consensus Agreement of >75-95% participants
Agreement of the majority Agreement of >50-75% participants
The final presentation of the recommendations looks as shown below. When the consensus strength identical for more than one recommendations, this was only displayed once in the left column of the recommendation block, where applicable.
We recommend to do tuberculosis screening according to local regulations.
↑↑
Strong consensus1
Expert consensus
1 due to personal-financial conflict of interest x abstentions
FIGURE 1 EXAMPLE OF HOW RECOMMENDATIONS ARE PRESENTED
Additionally, the management recommendations and lab controls were also voted on. The consensus strength is displayed in the upper right corner of the management recommendation field (light blue).
Dissemination and Implementation (EuroGuiDerm)
A decision grid I + II and a flow chart were developed to foster implementation. We included both in the external reviews. Feedback was collected and the comments we received were overall positive : “helpful”, ”clear”, ”useful”.
Furthermore, we developed a dissemination and implementation plan, see Table 1.
Barriers and facilitators to implementation/application
By implementation one refers to patient care following the recommendations presented in the guideline [12]. As described in the EuroGuiDerm Methods Manual (see EDF https://www.edf.one/de/home/Guidelines/EDF-EuroGuiDerm.html) guideline implementation is effected by a variety of factors, which are specific to location and setting. The main barrier to implementation may be the national/local definitions of disease and treatment goals as well as drug costs and drug availabilities. Main facilitators to implementation may be the decision grid and the flow chart we developed. Also, we included 11 national societies and experts from 14 countries to foster national/local adoption/adaption. The national societies were informed about the status of the guideline development and invited to form nation review committees early on to encourage adaption/adoption - this process is also clearly laid out in the EuroGuiDerm Manual (Chapter 10).
Quality standards/ monitoring indicators/ Evaluation Methods (EuroGuiDerm)
Monitoring and evaluation may consider: • Change in practice performance • Change in health outcomes • Change in end-user knowledge and understanding

20
References 1 Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF) - Ständige Kommission Leitlinien. AWMF-Regelwerk „Leitlinien“. 1. Auflage 2012. http://wwwawmforg/leitlinien/awmf-regelwerkhtml. 2 Sbidian E, Chaimani A, Afach S, et al. Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis. Cochrane Database Syst Rev. 2020; 1: Cd011535. 3 Nast A, Gisondi P, Ormerod AD, et al. European S3-Guidelines on the systemic treatment of psoriasis vulgaris--Update 2015--Short version--EDF in cooperation with EADV and IPC. J Eur Acad Dermatol Venereol. 2015; 29: 2277-94. 4 Nast A, Spuls PI, van der Kraaij G, et al. European S3-Guideline on the systemic treatment of psoriasis vulgaris - Update Apremilast and Secukinumab - EDF in cooperation with EADV and IPC. Journal of the European Academy of Dermatology and Venereology: JEADV. 2017; 31: 1951-63. 5 AGREE Next Steps Consortium. The AGREE II Instrument. http://www.agreetrust.org. abgerufen am: 6 Commission GAotSMSA-SG. AWMF Guidance Manual and Rules for Guideline Development, 1st Edition 2012. English version. 2012. 7 Guyatt G, Oxman AD, Akl EA, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011; 64: 383-94. 8 Guyatt GH, Oxman AD, Schunemann HJ, et al. GRADE guidelines: a new series of articles in the Journal of Clinical Epidemiology. J Clin Epidemiol. 2011; 64: 380-2. 9 The GRADE Working Group. http://www.gradeworkinggroup.org/. abgerufen am: 10 Werner RN, Nikkels AF, Marinovic B, et al. European consensus-based (S2k) Guideline on the Management of Herpes Zoster - guided by the European Dermatology Forum (EDF) in cooperation with the European Academy of Dermatology and Venereology (EADV), Part 1: Diagnosis. J Eur Acad Dermatol Venereol. 2017; 31: 9-19. 11 Werner RN, Nikkels AF, Marinovic B, et al. European consensus-based (S2k) Guideline on the Management of Herpes Zoster - guided by the European Dermatology Forum (EDF) in cooperation with the European Academy of Dermatology and Venereology (EADV), Part 2: Treatment. J Eur Acad Dermatol Venereol. 2017; 31: 20-29. 12 Committee of Ministers of the Council of Europe. Developing a Metholology for Drawing up Guidelines on Best Medical Practices: Recommendation Rec(2001). 13. ed. Strasbourg: Cedex F.

Appendix A: Declarations of Interest
Im Folgenden sind die Interessenerklärungen als tabellarische Zusammenfassung dargestellt sowie die Ergebnisse der Interessenkonfliktbewertung und Maßnahmen, die nach Diskussion der Sachverhalte von der der LL-Gruppe beschlossen und im Rahmen der Konsensuskonferenz umgesetzt wurden.
Berater-/ Gutachter-
tätigkeit
Mitarbeit in einem Wissenschaftlichen
Beirat (advisory board)
Bezahlte Vortrags-/ oder Schulungstätig-
keit
Bezahlte Autoren-/ oder Coautoren-
schaft
Forschungsvorhaben/ Durchführung
klinischer Studien
Eigentümer-interessen
(Patent, Urheberrecht, Aktienbesitz)
Indirekte Interessen
Von CoI betroffene
Themen der Leitlinie,
Einstufung bzgl. der Relevanz, Konsequenz
Altenburg, Andreas nicht zutreffend nicht zutreffend nicht zutreffend nicht zutreffend nicht zutreffend nicht
zutreffend
Mitglied: PsoNet BVDD, Mitglied Deutsche Dermatologische Gesellschaft, Mitglied Deutsches Register Morbus Adamantiades-Behcet e.V., Schriftführer
Keine Relevanz
Keine Einschränkung
Augustin, Matthias
Abbvie, Almirall, Amgen, Biogen Idec, Boehringer Ingelheim, Celgene, Centocor, Eli Lilly, Hexal, Janssen, LEO Pharma, Novartis, Pfizer, Sandoz, Trevi
Abbvie, Almirall, Amgen, Biogen Idec, Boehringer Ingelheim, Celgene, Centocor, Eli Lilly, Hexal, Janssen, LEO Pharma, Novartis, Pfizer, Sandoz, Trevi
Abbvie, Almirall, Amgen, Biogen Idec, Boehringer Ingelheim, Celgene, Centocor, Eli Lilly, Hexal, Janssen, LEO Pharma, Novartis, Pfizer, Sandoz, Trevi
-
Abbvie, Almirall, Amgen, Biogen Idec, Boehringer Ingelheim, Celgene, Centocor, Eli Lilly, Hexal, Janssen, LEO Pharma, Novartis, Pfizer, Sandoz, Trevi
- Mitglied: DDG, BVDD, IPC, EADV
Moderate Relevanz
Enthaltung Systemtherapie
Boehnke, Wolf-Henning -
Abbvie, Almirall, Celgene, Leo, Lilly, Novartis, UCB
Abbvie, Celgene, Novartis, UCB - Pfizer -
Mitglied: -
Moderate Relevanz
Enthaltung Systemtherapie
Dittmann, Martin - - - - - - Mitglied: -
Keine Relevanz

22
Keine Einschränkung
Dressler, Corinna BfArM - - - - -
Mitglied: Deutsches Netzwerk für Evidenzbasierte Medizin (dNEBM) Cochrane Scientific Committee
Keine Relevanz
Keine Einschränkung
Härle, Peter - - Abbvie, UCB, MSD, Sharp&Dome, DGRh, DGIM, DGUM
- - - Mitglied: DGRh, DGIM, DGUM
Moderate Relevanz
Enthaltung Systemtherapie
Klaus, Joachim - - - - - - Mitglied: -
Keine Relevanz
Keine Einschränkung
Koza, Joachim - - - - - - Mitglied: Deutscher Psoriasis Bund e.V. - Vorsitzender
Keine Relevanz
Keine Einschränkung
Mrowietz, Ulrich Abbvie Almirall Celgene Eli Lilly Janssen-Cilag
Leo Pharma, Medac, Novartis, UCB
Mitglied: Berufsverband der Deutschen Dermatologen, Deutsche Dermatologische Gesellschaft, Gesellschaft für Dermopharmazie
Moderate Relevanz
Enthaltung Systemtherapie
Nast, Alexander IQWIG, BfArM, IQWIG - - - Novartis 2018 <10.000 -
Mitglied: DDG - Leitlinienbeauftragter EDF - Leitlinienbeauftragter EADV
Keine Relevanz
Keine Einschränkung

23
Ockenfels, Hans-Michael - - - - Novartis, Janssen,
Almirall - Mitglied: -
Keine Relevanz
Keine Einschränkung
Philipp, Sandra AbbVie, Biogen, Boehringer-Ingelheim, Celgene, Eli Lilly, Janssen, LEO Pharma, MSD, Novartis, Pfizer
Mitglied im wissenschaftlichen Beirat des deutschen Psoriasisbundes, 2.Vorsitzende des Psonet Berlin-Brandenburg
AbbVie, Almirall, Amgen, Biogen, BMS GmbH, Boehringer Ingelheim, Celgene, Eli Lilly, Hexal, Janssen, Leo Pharma, MSD, Mundipharma, Novartis, Pfizer, UCB Pharma
Co-Autorenvertrag mit Thieme
Co-Autorenschaften bei Manuskripten bzw. Poster Leo, Novartis, Abbvie, Janssen,
AbbvIe, Almirall, Biogen, Boehringer-Ingelheim, Celgene, Dermira, Eli Lilly, GSK, Janssen, Leo Pharma, Maruho, Merck, Novartis, Pfizer, UCB Pharma, VBL Therapeutics
nein
Mitglied: Mitglied in der DDG (Deutschen Dermatologischen Gesellschaft), der BDG (Berliner Dermatologischen Gesellschaft), der ADF ( Arbeitsgemeinschaft Dermatologische Forschung, Mitglied im Wissenschaftlichen Beirat des Psoriasisbundes, 2.Vorsitzende im Psonet Berlin-Brandenburg
Moderate Relevanz
Enthaltung Systemtherapie
Reich, Kristian
AbbVie, Affibody, Almirall, Amgen, Boehringer Ingelheim, Celgene, Forward Pharma, GlaxoSmithKline, Janssen-Cilag, Kyowa Kirin, LEO Pharma, Lilly, Medac, Merck Sharp & Dohme Corp., Novartis, Ocean Pharma, Pfizer, Sanofi UCB Pharma,
AbbVie, Affibody, Almirall, Amgen, Boehringer Ingelheim, Celgene, Forward Pharma, GlaxoSmithKline, Janssen-Cilag, Kyowa Kirin, LEO Pharma, Lilly, Medac, Merck Sharp & Dohme Corp., Novartis, Ocean Pharma, Pfizer, Sanofi UCB Pharma,
Abbvie, Almirall, Biogen-Idec, Bristol-Myers Squibb, Celgene, Janssen-Cilag, LEO Pharma, Lilly, Medac, Merck Sharp & Dohme Corp., Novartis, Sandoz, Sanofi, UCB Pharma, Valeant.
Div.
Abbvie, Affibody, Biogen-Idec, Boehringer Ingelheim Pharma, Bristol-Myers Squibb, Celgene, Covagen, Forward Pharma, Fresenius Medical Care, Galapagos, Janssen-Cilag, Kyowa Kirin, LEO Pharma, Lilly, Medac, Merck Sharp & Dohme Corp., Miltenyi, Novartis, Ocean Pharma, Pfizer, Sandoz, Sanofi, Sun Pharma, Takeda, UCB Pharma, Valeant
Keine Mitglied: Deutscher Psoriasis Bund, Wissenschaftlicher Beirat
Moderate Relevanz
Enthaltung Systemtherapie

24
Rosenbach, Thomas -
Leo, Lilly, Janssen, UCB, Celgene, Deutscher Psoriasis Bund
Novartis, Leo, Almirall, RG Gesellschaft für Information und Organisation, BIG, PsoNet regionale Netzwerke, Deutscher Psoriasis Bund, Janssen
- - -
Mitglied: Deutsche Dermatologische Gesellschaft, Berufsverband Deutscher Dermatologen, Deutscher Psoriasis Bund
Moderate Relevanz
Enthaltung Systemtherapie
Schlaeger, Martin
Gutachter der Schlichtungsstelle ÄKN Keine Keine
S3 Leitlinie Psoriasis, S2k Kinder Psoriasis 2014-2017
Keine Keine
Mitglied: Berufsverband der Deutschen Dermatologen seit 1982 Beauftragter für Leitlinien und Qualitätsmanagement
Keine Relevanz
Keine Einschränkung
Schmid-Ott, Gerhard Keine Keine Keine Leo Pharma, Neu-
Isenburg Keine Keine
Mitglied: Mitglied des wissenschaftlichen Beirats des Deutschen Psoriasis Bundes e.V.
Moderate Relevanz
Enthaltung Systemtherapie
Sebastian, Michael -
Abbvie, UCB, Janssen-Cilag, Celgene Novartis, Lilly, Almirall
- -
Abbvie, Böhringer Ingelheim, Celgene, Dr. Reddy, GSK, MSD, Mundipharma, Novartis, UCB Pharma, Janssen, Almirall, Leo Pharma, Galderma, Lilly, Regeneron, Incythe, Pfizer
- Mitglied: -
Moderate Relevanz
Enthaltung Systemtherapie
Weberschock, MSc (Epi), Tobias
Stiftung Warentest, BGU Krankenhaus, DGPI e.V., Medizinischer Dienst des Spitzenverbandes Bund der Krankenkassen e. V. (MDS), Universität Bremen - SOCIUM
-
Frankfurter Fortbildungsreihe, Evidenzbasierte Medizin, Landesärztekammer Bad Nauheim, Antibiotic Stewardship
- - -
Mitglied: DDG (Dermatologie), DNEbM (Evidenzbasierte Medizin, DGA (Andrologie), EAA (Andrologie), GMA
Keine Relevanz
Keine Einschränkung

25
von Kiedrowski, Ralph
AbbVie, Janssen-Cilag, LEO, Lilly, Medac, Novartis
AbbVie, ALK Scherax, Almirall Hermal, Biogen, Boehringer Ingelheim, Celgene, Hexal, Janssen-Cilag, LEO, Novartis, Pfizer
AbbVie, Almirall Hermal, Biogen, BMS, Celgene, Hexal, Janssen-Cilag, LEO, Lilly, Medac, MSD, Novartis, Pfizer, UCB
Biogen, Celgene, Janssen-Cilag, LEO, Lilly, Novartis
AbbVie, Almirall Hermal, Biogen, BMS, Celgene, Foamix, Janssen-Cilag, LEO, Lilly, Medac, Menlo, MSD, Novartis, Pfizer, Regeneron, Tigercut, UCB
Nein
Mitglied: Berufsverband der Deutschen Dermatologen (BVDD)/Vorstand Deutsche Dermatologische Gesellschaft (DDG)/Präsidium und Vorstand
Moderate Relevanz
Enthaltung Systemtherapie
Related Documents











