l,,rriirlri. ,pr,l l",r,r,.rl. Ll'rl.,trr(rt\q l'as 1:' st'Ptl 2 :;-i|' Tlie WHO Antenatal Care Randomised Controlied Trial: rationale and study desigu '. Y. Al-N'lazrou'l' rrolii, U Farnt)tq' . Berendesr for the ir GrouP al Care Trial Research are listed at the end of the PaPer os'ario' Arscrrti'ln' sHosl)ilnl Cirlcro- Ot)slfiriao'.4r'ic[i'n'Arlns'Hni'rlttn'Ctrlrrt'KJtcrrXncttUltii'crstlv' KLorr Xrtt't;, ,',',-1,,,,'i, ';'r'1 \'rlr()rrr;/ /':iliilr;l' oi Cirii'l H.'rtliL 'trr'l ;;:ffi;::. l.;;;;;;;'rLr r\irr/D\rii' trir:ri'':'; tir' u-( ' SumErary' The \Norld Heal tiorls in develoPing countrles controlled trial to eva consisting oi tests' clini demonstrated to be outcomes These actilities four visits during the cours or the traditiolal Protra .{rr,i ; css /,r, corrcsPortrrcr tcc: Dr, } ose .l i' Tfu tJ,?li.Y \il,l;: |^"fiT:,^o tl"iHfil Procrnmne of Research' DeteloPm( lili,i';:"il'",ilsation' 12r I Geneva 27' s'^ itzerl'\nd' r 19qS BlrckNell S(iencc Ltd'

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
l,,rriirlri. ,pr,l l",r,r,.rl. Ll'rl.,trr(rt\q l'as 1:' st'Ptl 2 :;-i|'
Tlie WHO Antenatal Care Randomised Controlied
Trial: rationale and study desigu
'. Y. Al-N'lazrou'l'rrolii, U Farnt)tq'. Berendesr for the
ir GrouPal Care Trial Research
are listed at the end of the PaPer
os'ario' Arscrrti'ln' sHosl)ilnl Cirlcro-
Ot)slfiriao'.4r'ic[i'n'Arlns'Hni'rlttn'Ctrlrrt'KJtcrrXncttUltii'crstlv'KLorr Xrtt't;, ,',',-1,,,,'i, ';'r'1
\'rlr()rrr;/ /':iliilr;l' oi Cirii'l H.'rtliL 'trr'l
;;:ffi;::. l.;;;;;;;'rLr r\irr/D\rii' trir:ri'':'; tir' u-( '
SumErary' The \Norld Heal
tiorls in develoPing countrles
controlled trial to eva
consisting oi tests' clini
demonstrated to be
outcomes These actilitiesfour visits during the cours
or the traditiolal Protra
.{rr,i ; css /,r, corrcsPortrrcr tcc: Dr, } ose .l i' Tfu
tJ,?li.Y \il,l;: |^"fiT:,^o tl"iHfilProcrnmne of Research' DeteloPm(
lili,i';:"il'",ilsation' 12r I Geneva 27' s'^ itzerl'\nd'
r 19qS BlrckNell S(iencc Ltd'
28 l. Villar er al.
women Pres('lrting for A^uC nt these clinics over an average period of
lsmonths rtill hivc been recruiteJ '{s tvomen attcnding thc control
clinicsreceir'ethetcststandardtreirtment,.rsolrrentlyofferedinthcseclinics, in<iivir'lual iniormed consent is requested onlv from lvomen
attending the inten'ention clinics Authorities of the corresPonding health
districts ind all participating clinics have Provided written institutional
in(ormed consent before randomisation'
The Primary outcome oI the trial in relation to ndternol conditions is
the ratetf a morbidity indicator index' defined as the Pr6ence o( at least
one of the follorving conditions for which ANC is relevant: (a) Pre-
".t"*pd" o, eclamplia during pregnancy or.within 24 h of detivery; G)
DostDartum anaem; {traemoglobin < 90 g/L); or (c) severe urinary tEct
In-f-".'tionl pu"lon"plrritis' deiined as 'ln ePisode . requiring antibiohc
treatment and/or hosPitalisarion The primaw /ctnl outcome is the rate
of lorv birthr{eight (< l50O t) AdYerse matemal and fetal outcomes are
exPected for = 10L of th" tinttol group- Several matemal and perinatal
secondary outcomes are also consiJered' A comPrehensive cost-effective
ness anaivsis and viomen's and Provident' satisfaction evaluation are
performed concrrrrer,ttlv \(ith the;ial Health{are programmes should
Le riSorouslv evaluated bv randomised . controlled trials' rvhich are
feasit'leindcveloPingcountriesandihouldbecontiuctedbciorein:ro(iu(:iq netv iie'ltnl'l:t5 1!r heillih i'ntcr\ enti('ns'
Introduction
Antenatal care (Ai.\IC) Programmes, as currently Practised' originate from models
.lcveloped in the earlv dccades oi
Kinedom. TIre core of thcse earlv
,rne"u.-rluared, although, as medical k
tests for screening for disease and Prim
;;;;;".added"toroutineANC,"'*lY, j[t"":l":;1,:",:"1'H;^i:?:;:Y';:d only a ferv attemPts have been made
aLrl visits.2{ain a substantlll numlrer of visits for the
mothers-to-be (as manv as 16) r'itlr Iittle or no distinction betwcen high- arrtl lorv-
,trt r,r'o*"n. Rec!'ntl\', cost-bcncfit asPects of antenatal cnrc lrave been acldresst'd
in r"uornl countries, and attemPts are heing made to redtlce costs for ciients and
ifr" n"nfrn-.nt"."rvices.r To a large t'rtt'rrt' developing countries lrave adoPted' rt
i".-,r, in ,ft*ty, tlre antcnatal Programnrt:t ol the de!€loPed countrics with t)nly
-ilt "alr"ti*". Horvcver, tirc cirt'oftcn consists of irregularlv spaceci risits
"r'ith
iong ttuiiing time atrd p:oor iectllrack to tlrc lvomcrr' and thcre is little cttrnnruni-
cattn betwien tlrc ANC clinics nnd the oL'stetric dePartments lncl nraternitv units
' leqs ilh.!'r!cil 5.i(n(c Lt.l t',r,llrrlri' n !' t !t!'ti i:t' tti'l':v l:' )uFPl : 17-:$
l.]lr, l.VlJO rl,ric,trlirli rart RC7: rrlli(),lIli('rl,l.1 sltlriy dcri.qtr 29
Tl',. '. aliclitr' (rf tlr('c()rltcnt and thr rati
i i:,its nttds to trt' cvaluated This \Las earl
stated, 'llv sontc ctlritrus chancc, ANC lras c
r:rost scrcenirlg Protcdures hate tx'cn sub
'ihc cntotivc ntnrosphcrc slrould bc rcmove\l
;,:;;i ;..n ';r: ""ll
int '-"tigatc<i
t'r' randomiscd coutr()llcJ trials' i More reccntll"
tir( US t'trblr. l{caltlt Scn'ice l*p"it t'anet (nr thc C()ntcnt tri l'rcrr'rtal Care troted
i:1 its rcvle\\' that the literaturc on Frcnatal carc ictifitics rr'as olicn Iimited and
tiral manv studies \\'erc tonOuti"i rt'ithout nraximal scicntific ri8('ur'r Sirnilar
annafuaiont ,.'g1g lrritcd at bv a EuroPcan Panel"
The necd for randonrised controlled triils on procedures and examinations
i*f ri"a i. ."**tly Practised ANC has been identified; as u'ell as the evaluation
of the content, nunrber and timing of prenatal care visits for lvomen with differing
."in"i".i .,*'"1 risks Such tria'is can establish nrininral levels of care for r^ omen
ar l()\\' risk ti'\rou,:ll comP.trilr'; less frequent or less ilrtense Prenatal care with
si.rn.iard care."- "'"'s,i.."nroi..randomisedconrro,ecr,,'*,$;:);r#;',::i:iJi,:,r#'i1
Division of ReProductive Health
rtith research insttutions in develoPint
rogranlme of ANC rthich emPhasise
oscrtial elenrenls oi cart thal hale t'een d
:ra,;r cfi(ctiIe than a i;aillit'l"ai '\\'estc
,r:rd fetai morhiditr" The relative cos" ol
and 1\omen's satisfaction lfith the nert- -
The trial includes random allocation of ANC clinics (clusters) to either a
traditional programme ol care (i e tlre "V\'estern' model as currently in place) or a
rationally designed Protramme foorsing on the esseniial elements of proven
efficac'. The purpose of the Present ptpJ' it to discuss the rationale' design and
methoiological features of the trial'
Hypotheses that a ne$' model of ANC which includes
lvn to be effective in imProvint maternal'
ore efficient than the traditional Packate
nd perinatal end Points among sintleton
oresnancies and is not more exPensl\'e' End points are listed in detail in Table 1'
ih""fo[o.ting secondary hypotheses s ill also be exPlored:
oThereisadifferentialeffectoftheinterventiondePendintontlrecharacteristicsof the ANC clinics i e clinic size and prenatal care protider (obstetrician-
Svnaecologist, general practitioner' midwife)'
rlgg8Bllckr^,cllscienceLtd.Pa.dinlrird'r'iPtrrrr'rt'rlEpidcrrriolqy'12'Suppl2'27-5S

30 l. Viltar er al'
frUt" f. O'tto
^ i:[ :1 i:rffi r"'l''stv<il*1:ir inder'
B. secondarv outcomes $ed diseas- durhB pregnancy.
tlDut EeaEnmt dudnt P€8nanc'vj
for matemal comPlications
"ll1'J'o, a,,"'t"nne 8ro\rth retardationb
il,il "i "'i"t"
oaiierY ( < 3i neeks)
il;;i G;;;*'s lnd Prelieli'erv nrprure or membranes
< 35 \(eeks
35-36 treeks
*.i,-" "i.Jitn' 'rtldicited Frelerm deli*erv
< l5 rrc'eks
fr6h stilbi h)
from hosPital
a Proc6s outcomdn"1" oi "n,"nu,"l ,vith Pregnanc.v comPlications'
Rate of elective an
DaYs of hosPital
D. Economic outcomE
Cost-effe(tivenss
Satisfaction outcomes
Rate of rvomen satishe'l lr'ith the two ANC models
li"i*rr,i"* *trtit"ion/dissatisf 'lctioniollolving conditions
delivelv;.Proteinuriadtlivelv; Proteinuria(1) pre'eclampsia * "cliTi]:l"-::';". i],-i;;r" on qualitative ex minarion 19
p:lli:it]Sl^1[:l]8"":'-""1* jil :i ji "::':x:u:;','x$:.T[',:dl
jtl'ffi:*'j$$**.*:x,1":il*jilfl"ti::;-li,:r.*'J;1":'"'-i,,1;H}i:'JT"','ll1:*f,:'lUlnll' :.*":fliilf;:I";;":J#;;ii;- n"''ibroti.'' siven to treat
lrf if to.otl.. uno"'iu;nl'gtiffi':l*':tJ::J,'il1)period not availoble' use the hcst'obstctric estinrrte; bclorv
q::**gol^ffi*lHt'*llll'u.*'io" ror 'ctnl
distiL\s or ccPhaloPelvic disProPortron'
10th
, l!)o$ Blnt{scll Slrcrl(c Ll('l Pn'rii'lr'' nx'l I'('i'xrl'tl [l'i'L',"ir""til' 12' guPPl :' ]i-ii'

Tltt' WHO itttctntal cnre RCT: ralionnl( n tl slrrdrT dtsl'grr 31
r Tht're is; ciiffcrentiai eifNt of thc intervention anronc nrultiple pregnancies'
It is not e\Pccted that thc study ra'ill have adequate Po\^'er io test these h{o
secondarv hvFrotheses in other than an exPloraton manner'
6ric1 IrislonT of lirc plnrrrrirrg llnsc ot' the trinl
This initiativc oricinated <iuring'1991 out o[ the interest of thc UNDP/UNFPA/
trials u'hich the Programme is uniqueh'
The logistics an.l thc cost of such a massir'
an international effort' ovember 1991 1r'ith a grouP of obstetri-
conomists to set the frameu'ork for the
randomised controlled trial evaluating a
+L - h.^r ^.nr \\' a s preDa rec. a,*t " t"a,"":Jl'::l ::li'fl :;
tt":'*Hil':i;
lljl-"jl.:."^i.-.,,-:;;,;1.t""=. and an initiati'e for raising the tunds (or the: .\,FLa)""'! ' '- --
r;,air.',as Lr uncrrec Reuc'"' Loi th:iff iffi:J::lXi',n;t1,T I[i:l;
agencies have Priorty cotmtries and
needs of the shrdy Protocol' e 8 a con
with most of these initial issue
d and met for the
and the tYPe and
Thaiiand on 1 MaY
after four and a half vears of PreParation'
four countries ra'ere recruitin8 women into
a l99S Blackwell S.icncc Ltd Pn"lhlri( n'rd P 'riintlt
Efid'niolog! 71 SuPPl 2' 27-58

32 /. Villar et al'
bv : 200 staff, working in the clinics
aid religiously tlifferent' share the
effective intewentions for health care'
ad been recruited and data collection
the PreParatory Period could
We think that the tedious and
ral investigators' meetings' have been
n of the trial' We never would have
t of a Pragmatic trial' and the sense of
The i'alue of meetings and site visits
mes regarded as a 'luxu1y' rather than
ised triais.rr
action among some highly motiYated
'we cannot i'ait so long to have the
should be made to avoid the seduction
h intervention before it has been proved
countries where resources are Scarce'
Is are vaiuable because cf ihe Potential
effective metlical Praciices \\'e also h'rd
ation of conducting pilot str'rdies' n'hich
ence on PostPoning or eliminating a
.t: As it is said, 'once the Senie escaPes
d usually impossible to put him (or her)
e rvith Ar\C.
Methods
Trinl organlsation
ata coordinating units are located at IVHO in
nd safety monitoring committee was
of the kial; it reviews periodically
is informed monthly of thc (ollowing
an,.i fetal deaths bv trial arm' as rvell as
r' lq98 ilhc}tlvell S(icrr'J Ll't I'krl"'lrit r',rJ ,'r'irr'r"rl E''r'l''rnrulo'iy r2' SuPPI 2' 27-i8
I
I
Thc WHO anttnntal utrc RCT: rntitunb nnd sltlhT ricsigrr 33
rc:iuitmcnt rat!5 and Percelltage of hig,h-risk u olr1elr in tlre itrtcrvention arm \rllo
.i() not rcccivc thc baiic neu ANC modcl Tlre ..l'rta coordinatinil urlit produccs
the5.-,reports 1-. r,r'gll .rs rePorts to monitor thc qu'rlitv o[ data collected' such as
f"r."^,Jg. oi nrissing .'all',es fo' the main t'tttct'nrc variattlcs and numbcr of
antenataivisits by triai arm. lt also c<)nducts intcriN arlal1'ses oi primart' orttcomes
at specified numbcrs oi \^'omcn that c()mPlc'te'l lhc stuJv'll Tlrc frrst of sr'rch
in,rilrn nnniur"a rr.as conducted rr'hen 'l200tl 6lrttrPleletl wo cn's 1g66161s rr'erP
ar':ilable in Ccneva.
Trial doanrtcntntiofi and thc collnllorali'oe fftit'Ltlk
.{ detailed protocol u'as prepared in English and Spanish' supported by tw3
smaller documents written in a cookbooi style (also in English and spanish).
These trr'o smaller documents are the Mow'il "f Opcrotiorrs and the Marrrrnl o/
Clirirni .artieilio rshich are used at the clinics ancl local slu'iv offices for the dar'
ro-daY imPlementation oi the trial'
An ANC checklist and all data collec
into Spanish and Arabic. A bimonthlv s
cenrally produced. lt highlighs study
commonlY asked questions, uPdates
shares information about studv sites a- ttointuir,ing the coliaboration and the unif(rmritv of a multicenEe' multi
:ui:urai, ranoinrised controlled trial is in itself a nrajcr chellenge The trial
coordinatins unit in Geneva *.,"Tl;ff il:iilliil:il:':l'ij[ iffi"f :i
tioni u'ith queries related to data monitorint'
ths in Geneva, and site visits eYery 3months to
l,ocally, periodic n'orkshops for the inten'ention
Broup's staff are conducted to revielr' the protocol including.a periodic clinical
check-list evaluation and summary form assessment This eJfort has created a
i"aing of "n
international team a"i contributed to high morale among trial staff'
Selection of study sites: criterir and statistical considerltiotls
The clinics in eaclr study site have been selected because they serve similar
p"pJ,i"* with regard io socio-demographic factors' and have study-relevant
mortality and morbidity rates of the same o'der of magnitude' An ANC
;r%t;;*" following traditional standards delivered through the public sector
rvas already available to Pregnant rr'omen Each clinic orcluster u'as exPected to
^o"ug" ia*Iy between 450-and 500 nert ANC rvomen during the study Period'
Hor.,""r,"r, ". tire number of clusters has a greater impact on statistical power than
the sizes of the clusters, smaller antenatalllinics, Potentially supplying as fevv as
f 199E Btackh'ell Socnce Ltd Pdcdiatti" nn'l R titt'llol EPide'niotosy 12' SuPPl 2' 27-58
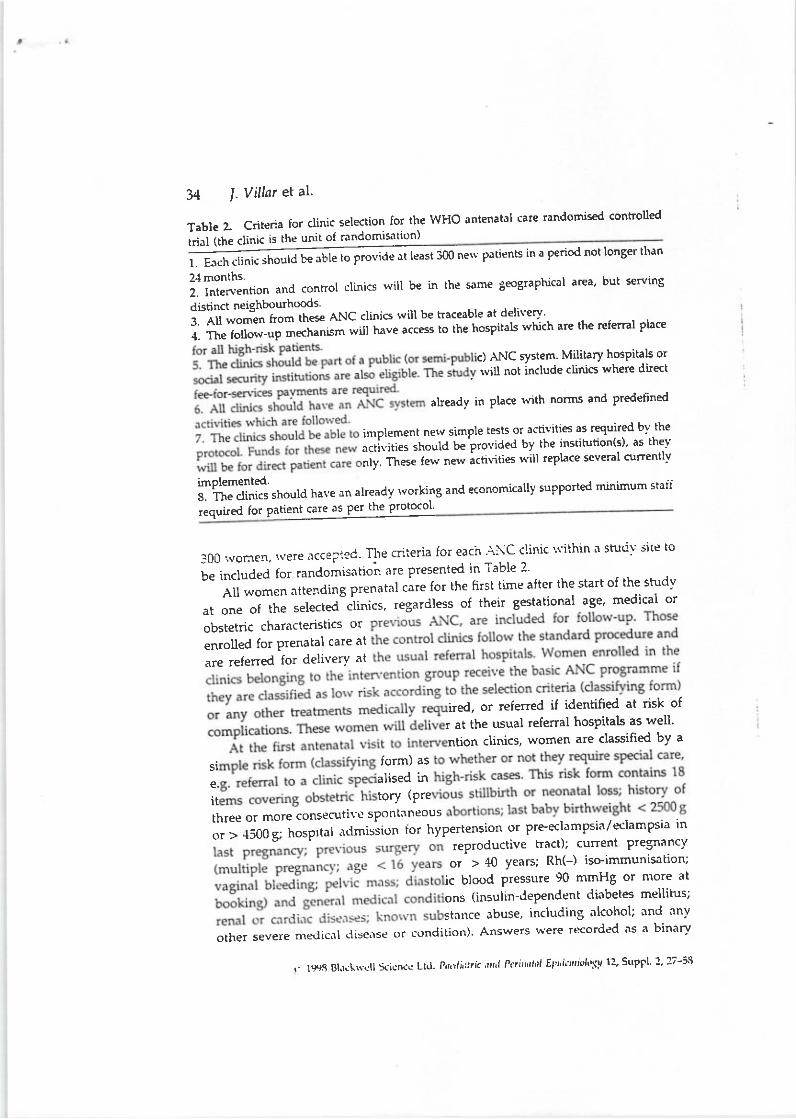
24months.il i'iii^-.""" and control clinics will be in the same SeograPhical area' but serving
.ti.iin.t neishbourhcrds.;1;;;;1;;;* thes€ ANc clinics rvill be traceable at deliverv
.
i. ff"';u;;;;;echanism rvill have access ro the hospitals which are the referral place
c) ANC system Military hosPitals or
, lvill not include cliniG where direcl
alreadv in place rvith norms and predefined
imPlenent nelv simPle tests or activiti€s as required b'"--the
activities should be Provided by the instihrtion(s)' as the]/
ntv' Tftest ferv nerv ictivities r't'ill rePlace several curentlv
34 l. V illar et al'
Table Z Criteria for clinic selection for the WHO antenatal care randomised controlled
Jrr'i i. ai." is the unii of randomis"rtion)
@nelv patients in a period not longer tlran
imolemented.il'"riJJ,.ti tn.rd ha'e an alreadv rvorking and economically supported minimum stall
,"qJJ rot p"ti""l.--!-B"t th" Ptot-ol'
300 rvorren,'.vere acce;ied- TIre criieria for each l'\C clinic "rithin
a studv sitc to
i" l.,.ira"a for randomisation' are presented in Table 2 . ,
All women attending prenatal care for the first time after the start of the shrdv
",;;;.; the s"lected-cii.ics, regardless of their gestational age, medical or
obstetric characteristics or
enroled for Prenatal care at
are referred for deliverv at
ired, or referred iJ identified at risk of
r at the usual refenal hospitals as well'
ntion clinics, women are classified by a
si form) as
e. alised in
it tory (Pre
three or more conseotivc sPontaneous
;;, ;i; ;, hospr tal ar'tmission ror hvPertension ;J"tff '; i:1:f Hg::'";
or > 40 years; Rh(-) iso-immunisation;
ic blood Pressure 90 mmHg or more at
ons (insulin-dependent diabetes mellitus;
stitrrce abuse, including alcohol; and anv
orher severe medicnl disense or condition) Answers were recorded as a binary
ilgesB!.r!\w,rllSLicn(!Ltd.P'I,tli'rrri'n,I'iP"i'nrrrriEt'r'ii"'i('[rsvl:'SuPFI2'27-i3

Thc WHO i,tttL.l,ttttttl carl IiCT; rntiL)nnlc fitt(l slrrd.rT dtsiqrr 35
variahle (vcs/no). \f omell lrith a Positivc re'sPolls( t() any oi thc questions rr'erc not
cc.rnsicicrc'd elig,iblc for thc Irasic conr;x.rnctrt of thL'nc\\' Progranrmc but renrainc{ ill
thc interventi<in grouP r('ceivilrg the carc ctrrrcsltolrdilrg tr'r thc dctecled contlition or
risk fackrr. lt should tc n('tBl that the risk classificaticrn form is an intL'8ral Pnrt of
the interventiorr ('Nerv B.rsic Progranrmc' and 'S1--cial Care') and should not t't'
corrsidercd as an cntrv critcri(nl ti' tllc triil. Figltre 1 provitlcs a fl()$'chart showing
thc path that rr'orrtcn follorr' in the th o aInrs oi tht' trial \{omerr u'ho did trot agree
tc, particip.rtc in thc trial rtcre asked to Protidc the inforrnation needed to conrPlete
the 'classifyine' f<.rmr for'oascline dcsoiptive PurPos(s onl)''
all ,.'onrcn ettending, the studv clinics regardless o[ thc care received and the
number of Yisits rvere included in the assessm€nt of trial outcomes (intention-to-
treat). Again, the trial comPares two systems of care; the basic Programme is a
compon;t of the care offered to the inten'ention group \{omen B'ill be followed
untii discharge lrom the hosPitals Post partum, including those rvho refuse to
p.rrticipate in- or <tiscontintre the ne\\' Prograrnnrc becausc of.either medical or
personal situations. Hortever, given tlre equivalcuce naiure of the trial' subjects
ivho reruse to ParticiPate to anv extent at all in the inten'ention will not be
regarded as belonging to the inten'ention grouP for the primary analysis'
siondary analvses-r.-iu include all enrolled subiects to the extent that their follor.r-
up data are ar ailable. Women u'ho refuse to initiate or continue the neu' ANC
progr"^nl" are offered the 'traditional' ANC at the same clinic or referred to an
altei,rati.e clinic i, ii is locoted nearbr-and does not represeni an! in'onterrience
io; tlrt t\ on1en. Tire prop<xtion oi r" omcn reiusinq tire llel\' ProEirammc (droP-
outs), or \r-ho discontinue the trial Protocol after randomisation (transfer rate) are
regarded as a Process outcome.
Trial desigtt
The study currently under way is a multicentre randomised trial of two different
models oi ANC. The nerv model of care u'ill be compared rT'ith the existint form of
I ..$ r-l
Figure 1. S
Controlledrandomisntiprovide thepurposes only.
( l99E Blacknell Sde ^<e
Ltd P,ralioln.a,1 Pc,tnlol Elid?mioloSv 72, SuPPl 2' 27-58

36 /. Vill,rr et al.
ntly ireclurvill
are r;ndomised (cluster randomisation)
each of four sites and rvithin clinic
ite were the number of Pretnant women
e year Previous to the study' the tyPe of
ministrative health svstem to rvhich they
each of three studv sites and 17 in the
fourth site.
DescriPtion of the stutlv siles
Khon Kaen Province' Thailand
kok) is the:entre oi ihe north-:astern Dnrt
their babies at the health-care facility
ANC scheme follows the traclitional
Table 3. Allocittion of clinics across sites
Numbcr of rindolnised units
per stIatumrCountry
ThailnndArgentirlnCuba
Khrrl K.lcn ProvtnceRosarioHavlna
2 largt', 5 meditlnr, { small
I hrge, 15 srn.rll'12 smallJ nrediunr, S small
Itrtttahnc'/v P:rtients n veir' tvPe oi clitric
t(hi.h th,.v lrr.h)ns.(iree-st.rnding/ hosPitnl nssociirtcJ) 'lnd hciltlr-c'rre j)-stem to rrhich thcy b('lt)n8'
t l(E)S Dt.r(L\(rll l.icniu I t.l i''r'r'li,''ri x"l l'r''nxtl't' ir'rhnrir'l'\v l2'SttPfl l'::-5St)
TIrr' tt'fjO n tL'ttniil cnrc I(CT: r'tliontlt nd sirrrfil dcsigrr 37
irar.r:r.rtoc;it rnel scr.rlosr tlsts ftrr s"'plrilis (trstr'rllr' \'Dlll-) arc routinel\'
ix'ril1611{. Tr.,rl tlrrsts.,i l.o"',,,',, ttrxrlid .tt.c l]i\'cn l(! Frcgnilll rt<rmcn tluritlg'tirc antcrrat.rl },.'ri<rl. UncontPiicattC dqlivcrics rrc attcndt'd and cttnductcd by
,',u.s.., t.ll.r.1". courr,licatci dclivcrics art' lrranagctl t'v mcdical officcrs or
,.li"rr",l n. apProPrinll. Facilitic's for Cacsar"atr sNti(nr arc availablc in all tlrrcc
6ft-hed aurl .ii :tr-tC crr::rrnunit) h()sililals nrrd itr sort'tc trf tlrr:1Ghcd hospitals'
\urscs ir(!t't't tirc c(n'l1l:rullitY hosFit'lli all(i ulitlrr'i\es ftrrnr thc lrcalth cclltres nle
.cht,dtllt,.i [l,r a lrtl;lrc r.rsit it' Pt.:i},;rrtur)] \\.()t,11(.It itr tircir rtsl.rcctive areas for
riving lrcalth t'.luc;,tiott alld rrall.lsclllcllt oi thr-';rostpartunr 1:crioC
Rosario, Argentina
Rosario, the second largest city in the countrt" is located = 300km from Buenos
Aircs. lt has a krtal pp;'ut61i(11 of ovcr one million inh'lbitants Health care
i:riludin,: ,\\C i: pr,'r:irlecl t'\' .r nri\ oi i'iilate' Irttlllr' hc'alih ald social st'curitv
.c:'.i[cs. .\iut(\sl all dcli\.cries irl lhr- '-'rrt'.riic s\':t('l.l'l (rccr'r: ir: iirc ]rosr''itals'
intcnatal clinics includcd in the stud! arc thtrsc'.lttached to trt't' hosltitals as rvell
o, fr""-r,nnd,ng clinics. all belonginc to the pul'lic svstem'. ldcall\" tlre traditional
'\!cstern' svstelll is recornnrended, rr'ith a t:lininrutl of file antenatal tisits Per
rtc,nran. \'lost of the fu\C is provided bv olrstctric/Evnaecologv specialists'
ll:i ani. Culr.r
!la!an.r is the caFital of Cuba' The tiial i' irlrPlcrrcntei in threc municipalities of
ti\c citY, Centro Habana, Habana Vieia antl Habana del Este Poh'clinics located.in
ii"*;t"". provide ANC to all Pregnant rsometr resident ill these nruniciPalities
and all deliveries are referred io iertiary care hospitals nr 'NC is Provided by
ceneral Dractitioners or obstetric sPecialists' complemetrted b1' a conrprehensive
i-t". i t"Ja, medical and nutriiional services The amount and content of care
i; .qrl."i* i" afre best Ar.NC in deseloPed countries' tr'hich.has contributed to the
Iort levels of negative Pregnancv outcomes in this PoPulation'
Jeddah, Saudi Arabia
Jeddah is ihe second lartst city in the Kingdom oI Saudi Arabia and is the maior
r;;;". The populatio'n of the city is estimated to be 15. million u'ith 17800
a"ti.1"ri", p"i y"r.. Health care is provided by the Ministry of Health'
*"t'"^r*tlf aiencies such as tlte Lniversitl' hosPital' military hosPitals and
itro t 1' tt " priuui" sector. Tlre Mirristr of Healih renders its sen ices through eight
f.".pt;"f, oitd o n"uuo,k of 37 Prirnan'Health Care Centres (PHCC) distributed
throughout the city. Obstetric sun ic"s a'e available in t\vo Seneral hosPitals and
trr:o #temiry hospitals' ANC sen'ices arc available in all the PHCCs as u'ell as in
( lgqs Blackwcll Scicn.c Lld Pnr''lintri" nnd P{'rittitnt F'Pi'lct"idofv 72' SuPPl 2' 17-5E
38 J. Villnr et al
t rvomen follows to a larte extent
and frequencv of sisits' AII care is
s. A lbrmal scoring s)'stem is used to
nsultant clinics located in cither larger
deliveries takes Place in hosPitals'
Interuefltiol1
The rrial inr,olves a diject comParison of trvo programnres.of ANC. one is the
;ffi;; ;.\r; ;;rently offered'in the selected sitesihich follorvs the 'traditional'
model. A detailed rlescriPtion of baseline A'\C was obtained before the
,r.0"r,tr",t...*eotheristhenelv.Plosram6grvhichincludesscientificallv
"."i""i"I, .ii*tt'e-oriented activities
r5'16
ActiYities included in the new Protramme. fall within three general areas:
(") ;;;;;; ".io"' r"' Iteattlt condltilns likelv to increase the risk of speciiic
oiu"rr" ora-.onr"t of pregnancy; (b) th'
tl\ese outcomes beneficiallv; (c)
pro'clents, especiallv e:llergen':es'
As rtith anv other sireening
conform to the common critena for scr er' screening ior
nerv medical risks in ANC is a continu of the screening
I nunrerical risk-
clinics, is not inclucled because of its lo'v
ck of evidence of the effectiveness of such
d controlled trialsrq Therapeutic inten'en-
ff:i,$:ff: lvere serected irom
It is inevitable in a multinational trial such as this that the actual
trial is'Pragmatic' irl its orientation rather than 'explan'rtory"a) Horvcver' in order
to standardise the interyention' all stutlv sites use a.Mnrrrr'rl rrf Clirricrrl Actii'itics
an,l a clirrical activities'checkiisf (Fig.i) that translateLl irrto local languagc is
atltletl ttr all medic'rl '"to'J' in the iitenention clinics' arr.l completed at each
ANC visit.Neverthcless, tr trutnber of elot-unrented deviations from the formal protocol
have occttrre.l in tlle studY sites ln Th'liland' ihe uterirrt' hciSht chart Nirs not
implemented, althouqh the actual measuremcnts lvere taken 'rnd recordetl in the
, l\r"S Bl.r.hvcll I icrl.( LtJ lir'1"'rl'r' r'r'i 'I"li"'ri'rl
l':t'i'l'1rrx'/r"(v 12' SuPfi :' :;-is

Tlrc WHO nnlollj.lal cnrc RCT: rfilittnnlc n ii sllrrltT dt'sigr:
I}ASI(',lNTENATAI, C^RE CII ECKI,IST
( llE - t: f l lL 1t-tl t lflLt C-tkflf.l, Ol'f lt l ltRL tlliolil tTt t l'rll t.t l)Lb l( ,rE\tt i,/r ./,s! ra1d,"!,,.a{r{ /r' n'. o/ r^d
39
( hnk trrdd tio _SuJl Suhj!(r rio_ -:--
$dn Bp@ibt. lu ant@tot .nc non
Figure 2. Basic anteratal care checklist included in all medical records of women attending
an]enatal care clinics randomised to the inten'ention artn of the trial Care providers
complete this form at each visit following standard procedures lt is exPe(ted that this
me(hanism lacilitates the inPlementation of dle intervention and reduces Protocol deviations'
C 1998 Blickrrcll Scie ^ce
Ltd. Pa.,lialtic nttd Pcirnh Elidcntiology 72, Suppl 2,27-58
FtlL$ \'tsrl ,,.,d/ro,tr',.t!trrrt.o tatfih.ti"td r.*ddttn iJ Fllintn'n tur" lI fite t i!" Ltur tt\tt ttr,anrt,tlal. ut4 .t ull *t^ itit tP t'
'h ntu'
l,ATt:llt :nd inl rlh
a i,\v^,,r r.,r 'nd,:t'* cllirln ln lltr h:rk F.?rrnm
(nnr.ll\ E\d.Jnd Ilh rqrr
()t.r&, ($hun.l rr:6trf,rtio utrrin. h.ilhr
(r ^ .rs lr$ E oorEn d stl *dtl rb )
R.Di3 nrnil'i16l. &t d'6.f trnD|nnis 5TB ' ud6<ir
t.:. rd rruinoL dilrrr'
ic ro[r..d$!r 6.nuri6irlt mrjaid for co.r::Gn.iq hd l'.. fd dcrB*6
I
SICOID VISIT rrd SUDSEQL:EIT YTSITS Gc'tato nlu$ a?ri 'ol\t<Lt:l,^TE: 16 ll il
al'n(. cilnEr6lq atii!
rr.\ri r.tctiN.i.r: ?!:iiJncr ctr:.. h.th fdrl hr&r n':
f r n. lrtr td Drd.m rd. tu[l'fu!.om t [l tt' 6 'drErlr. fol'..cdllDDl.i.nuton
R..mDddrnoi tor.hcr!cn.'6
THIRD vlSITr lld DATEI
ir'!nurrorod (!..6d.io(,
R..6hh.nd.tm! fr l-rdDn rcntrarnion
FOITRTH VISIT: .dd DATE: ,
D.t..tion of btrc.ch pwnEno. & r.f.ml lor.r!.m.lr'Rd
CohDld. ANC !.r(r<omn.nd i' b. broughl tohotpn,
40 l. Villar et al.
medical records, and all women had a haemoglobin test at the fust visit which was
not recommended in the protocol ln Saudi Arabia, all Rh(-) tvomen were not
eligible tbr tlre basic comPonent of ANC, and the recommended routine vaBinal
"ti*ir,o,ion rvas not culturally acceptable ln Argentina' many phvsicians in the
inten'ention clinics requestcd one ultrasound assessment' even if there rvas no
medical indic^tion, ,.'hich was not recommended in the trial; if the woman had
,roi a"Ur"r"d by rveek 41 o[ g€station, the next visit was conducted at the ANC
clinic rather than in the hospital as required in the Proto€ol; physicians in one unit
randomised to the intervention ErouP imPlemented a glucose tolerance screening
test, although this was not included in the Protocol'A final
-explanation is needed in resPect of the imPlementation of the trial
in Cuba. Because of the universal availability of family doctors' it is possible
that, although rvomen had a reduced number of visits at the clinic' they rvould
;."piu."'tt""r" visits by Soing to the family doctor's of6ce' lve have instructed
these doctors to refer iU pregnant women to the A'NC clinic' but there is still the
possibilir,v of rvomen demanding care that cannot be refused Fortunately' there is
a routine data-collection system in B'hich family doctors have to record anv formal
ANC visit and such a visit is also registered in the \roman's 'd\C card All visits
recorded on this cJrd nie nbstracted iI the time of ,.1eliven bv the inl'estigators.
Tlrerefore'iftherearee\trauisitsrof.rmilv(ioctors,ihe\,rr.illbeincludedinthenumber of visits made to clinics other than the original antenatal clinic'
Moskitrg ol in te roen t ion
Considerable efforts are made to mask treatment status for deliverv and neonatal
care providers. The staff responsible ior data collection after birth at the hospiial
le,el are unarvare o[ the treatment status oi r\,omen ilr the Study' In Argentina, all
deliveries occurring in the ParticiPating hospitals' even those from other clinics in
the city, are reco.-ded, miking it very difficult for hospital clerk to identif'v
intervJntion status. The study site in Thailand is an excePtion' as delivery occurs
atthesameinstihrtionsrvherewomenattend(orANC.Therefore,itispossiblethatstaffinthedelivervroomkntrrvthetleatmentstatusandPerhaPsactdifferently based on their belief ol the effect of ANC' The Primary outcomes are
little influenced by intraParh'rnr care, horvever, and it is exPected tlut this effect
willbeminimal.lVervillncvertheless.rtt('mPttoevaluatethiseffect,ifpresent,using trvo mechanistns:
(a) lnfornration on intraPartunr events Partiall)r unrelated to ANC' such as
emergency Caesarean section atttl iorceps tlelivery, rvill be collected'
Comparisons rvill be made bet\\'eelr the two treatment grouPs'
(b) Trenis in Pcrinatal outcomcs u'ill be lrbsewed at all ParticiPating hosPitals ior
their total PoPulation.
, lqrs Bl.rllw(ll ici(!\.r Lr(|. nr,1i,,r,n .rnJ t'ri LP"l "i'l+tt 12, Srrpfl 1 11-55
Tlrc h/HO a luntai crrll l(C'l'; t'tllt.rttnlr i i siraiy ricsi;]rr {1
Ollcoltc,rt(?srr,('s
Antcn.ltal carc is a conrplcx sqt of aciiYitics (t'.rsicallv a nrttliiplt,tsic scrtltritrg
proccdurc) aiDl('d at rcducing nratcrnal antl fclrl rrrorbielitr' 'rttd m(trtalitv b\'
iccrcasing, tlrc likclihotxl that a Prcgnant rltltrtatr uill crpcrience scrit'tts
ctxrplicatio.s rlurinS prcsnanc* or childl'irth, and lr\: irllPr()\'irlg t1c mntcrtral
and fetal outcontcs oi \ronlcl'l \\'ith colrplicntioll:. lt is clear tlrlt' iI orrli n]ilte:'nal
dcath and Prc-latrour fet.rl death are consi.le'teti (outc()nlcs th;rt A\C shorrltl
ideallv prei'cnt), the sanrple sizc rc<1uirt'cl r'rtltl..l ['t' crtrenrc]r' largc arr..1
unrealistic; thus, surroSatc measulrls and a molL''itlitv itrclcx ate used to trtcasure'
intcr!ention eifect.
As far as poteniial fctal outcomes are collcernc|.l, ollc aitcrnative is Perinatal
mortality, r.'hich can be considered as a Elobal indicator of fetal/nertborn health'
Ho*e.,er, perinatal death is also related to certailr aetiological factors such as
congenital malfonllations, intrapartu:n coDl|li''ltiorrs ()r tvPc of neotratat care
upon rthich ANC has linritt'd elfect Furthe'rrrrtrre A\C h'rs littic eff('ct orr
pcrinatal nrort.rlitY among norrr,ai biriirrlcigirt iniants For lr\allrPlc, in the'C)xl<rrci
region, UK, from l9&l to 1987, onh 61i of all irrtrapartum or }rostPartunl deaths
r.'!re term sintleton babies uithout congenital malfornrations or evidence of
severe infection. In this region, oi all perinatal deaths, onll' 47? of nertboms rr'ho
died rvere considered to have a complicated antenatal historv.:r Neonatal irte.sive
care units do remarkabh'rtell in 'rescuing frorn death' \'en' Preternr infants rl
Excludinq cotrgcnital maltomlatiolt alrtl introrrartuill dL'atll. it is tcn ulllil'eit that
.r-\C r{ili inllrrcnrc }rerirat.rl nrortalitr'\\'itlrout ci\rllsinS ths iatc oi'-'rclcml deii!en'
or intrauterine gror.ith retardation (1UGR). Bv reducing the inct.lctrce of IUGR:'an.i
Frcterm deliven', ANC can influence fetal, irrkaP.rrtutl and r]e(nlatal death
There are legitimate concerns arising from tlre use of lorl' birtlrh'eight as t'
primary outcome of a proiect such as the Present one, u-ithout differentiating
Letween preterm delivery and IUGR rthich require gestational age estimation'
Althougtr an accePtable ievel of reliability-can be obtained in the estimation of
Sestati;nal age in developing courtries,r{ rve believe that imPlementing a
io-rnon system of Eestational age or nervborn assessment ra'ithin a very large
trial in four countries is impractical.
Trials that are exPected to have modest imProvements or no imProvements in
relatively rare outcomes can use combined indices (e g matemal morbidity index)
or surrogate measures instead of the ideal outcomes' We have chosen as the
primary-outcome of the trial in relation to maternal conditions the rate of maternal
morbiiity indicator index. This is defined as the Preserlce of at least one of the
follou'ing severe conditions for u'hich ANC is likely to be relevant:
(a) pre-eclampsia or eclampsia during prcgnancv or u'ithin 2'l hours of deliverv;
proteinuria is defined as 2.0 g or more in 24 hours or 2+ or more otl qualitative
examination (diPstick);
i 1q98 Blackwellsciene Ltd- Jrnc,rialri. r,r.l Pl.riralnl Eli,lt),Li)lo.g, 12, SuPPI 2,27-iS
42 /. Villrr et al'
(b) postPartum inaemia ( in); and
i;j ;;";" urirary tract in defined 'rs anv episode of these
corr(litiolls requiring a t or hosPitalisation'
These comPonents are relatively independent from each other and I^'e exPect
that only a small percentage of one of these
]".aii"itt.'rtit ""'*eigtttei ittae variable' but
"].i.i,rt"t" three conlitions rvil as secondary
outconres. The primary outconre in relati be the rate of
i"* "U'tr,fl-"tgi,
t< i;oog), as a surrogate measure -for Perinatal mortality'
;::";;; ";;.""re variabl-es inclucle other matemal and Perinatal events such as
the rate of incomplete tetanus tmmunisation' t'reech Presentation at birth' the rate
of treated svphiiis or a PostPartum hospital stay for maternal complications of
1 rveek or more (Table 1).
Thc economic e-tnluntiotr
There is an ecouomic evalua[ion alongsicle this randomised controlled trial' A
U"*it..i a"=."p,iolr oi its nieii]o!1oh-t3i-\' is Fresented elservhcre in this Supple-
i,"*ii gr,"i],:. lhe .'coltonric eveiuation airiis to assess rvhetlrer the ntrr'
Drosranlme is more c'rsceilet:ive th
itoilan,',aing the service an.-1 ior healt
ivill estimate the unit cos[s oi care tha
particiPatilg in the clirlical trial Unit c
il;;;; "^:it type of care (collected in calculate the
,o,ot aoro oi tt"otth c']re given lo \rome the trial The
t care duringt'Pes o[
delir'Pregnan rvillcare. ln.ostr, ony consultation and PrescriPtio ' the
and lost income. All costs incurred unt Post
Assessmett of tonrcn's nntl proaiLlts' pcrcept'totts of rynlity ol care
of grcat inPortance and consielerable efforts are
lcd itescripttn of its nethodology is presented
.l" Lr sirort, tltis comPonent ains to comPare the
sr.rbiective perccptiotr of the tlualitv of
reasons bellintl it, il'l \\'olllcll altelrdi
control units. The sttt..1v 'rlso ain]s kt
nurses anrl othcr ililicd !-crsorrDcl) !''"runits lncl lhe r]ew .'lntclliltal Pac
, le')s ijl.r.l$.ll S.rcn.! l-I.i. I'.r,lftlrit 'tl"i l'lti'Iitrl [,,,'i(1'In'1"'ir/ 12' Strl'PI 2' lt-is
l}r' lVFl() l,ttlt'nttt.,lcnrr' RCT: tiliittil.' tl' 1sllr'iv r{r'str'l +i
considcrations, thc stlbieati\'(' dinrcnsiotl atrrrrtrs htrtlr rls('rs alld provi''ic:s is a
crucial slcnrcrrt ttr trc takr'D itrto account b('(()r('rc('oll'tnlcn(linS thc atlol'titrrr oI the
rrcrt ANC Pxckailc- This c()DrPollcnl rtill also lrroville uscftri inftrrrrr'rtitrtr alrr'rut
thc obstacli+ that m.1\' 1,n1'q t(r he ovcrconlc drrtille rcPlicati('tl antl s('rlint uF'
Results are particulariv rele'r'allt for a nlulticr'lrtrr' trial, cnrricd out ill crtrelnclv
differcnt coritcxts. The sttr.lv i5 organist'd into t\\'o st.lscs lrr thc first phase' 'ruethrro.:raplric aPPr()ach ftrllou'ttl techniclucs sttcir :rs itrcus SrttuPs alr.l irr-.lcpth
irrtcn iesis uith hc.rlth Pcrsolurl.'l atttl rvontcn, iu ortler tir 'lsscss thc iranre tll
culturallv rclaterl valucs in e[erv countn. Tll(' fill'lillgs \\'erc incQrPor'lted ilr thc
,eco,1d sta,r" (qual)titatiYc), aud rtill also L'e used kr itltcrPr('t tllc results of tlre
quantitatire cu'nPonents. The second plrase uses a standardised' close-ended
questio,r,raire to alt ANC Providers ParticiPating in the trial in every country' and
another questionnaire to a random sample of ra'omen attcnding the clinics'
Qualitatir"e data u'ill be anah'sed bv applving the'grounded theo4' approach'"
that e\ables an illductive illtcrPretation oi tllc illfortllatioll Quanlitative data rtillhe a:ralvsed using stalrdard statistical tcchrli(lues'
Basclinc surz,ev
A formal sun'ey describing ANC Practices uas inrplemented in all eligible clinics
immediatelv before randornisation to obtain a detailed description of clirric and
serr.ice clraracteristics Lrefore the interventiolls. lnfort:ratiolt is availatrle on thc'
clinicai uracticcs .rnd servicc. ()l tire clinics. Tlrere ar.' i\\'o c()l'r'lPo:lents oi this A\Csuncr':cliniclevclatrdPatienilevel.Atthecli:ricletcl,c't'teiornrr''asconrpleter'lfor each clinic particiPating in the study in each coutrtrl. bY the studv field director
and t5e clinic ftcal person. The s.,n,ev coordinators liaised with the clinic staff and
authorities to obtain the most uP-to-date description oi the clinic The visit was not
communicated to the clinic staff in advance and a 'tvpical day' of the clinic u'as
chosen to avoid selection bias of patients and procedures' The principal
investigator of each countrv prepared the agenda for tlle visits'
The-patient component of the survev rtas also conducted before randomisation
and after completing the 'clinic level' form. lt *'as carried out by the dinic focal
pe.son undei the iupen'ision of the shrdy field director and implemented
simultaneously in all ciinics at a given study site An index day n'as chosen by the
sh:dy field director to conduct the sun'ey. The clinic focal person used the dinic
Iogblok to determine the medical record numbers corresponding to the
co-nsecutive visits of women before the index day A minimum of 64 consecutive
records of pregnant women B'ere aimed at each clinic (cluster)' At the Patientlerel, 2913 meJical records u'ere revierr-ed. The desiSn and methodology of tltis
sun'ev is described elsctvhcre irr tl s Supplement ls
Tables 4 and 5 Present the characteristics of the 53 clinics randomised to tlre
inten,entionandcontrolgroups,usingdatafromtlreantenatalcarecontentsun,ey
r I99S Btnckh'ell Scicn ca Lld PnL\liol/i. nt l Prri'r''ill Et"i'd'r"i'lost' 12, Suppl l' 17-i9

44 l. Villtr et al'
Table ,1. Ch,rr.rcteristics oi the clinics randonrised irl the IVHO
,*"Ji "i ,ft1 nrtennt'ri inrc (-ontcrrt slrr\ t'v lt tl.r" t11n;': level"
Antenatal Care Trinl:
Cllaractcristicslnten'ention(27 clinics)
Control(26 clinics)
Number of clinics
Type and PlaceP blic hcnllh syslcl't
MuniciPal or Provinci'rllvlinistry of Health
LocatiotrU rbanRur,rl
Type of ANC clinicP.rrt oi a Poll'clinicP.rrt oi .r hosPital
Higlr-risk clinii ar'.rilablc in s'rnre btrildirrg
Separate antenatal consultati()n roon1
Lotv-risk r"omenHigh-risk rr'omen
Piitete .'irtssitrs r('r)n1
\-'i\\' [iiltiarts/'nlolrin (n1l.,'1:1 |
Openins tinle (hoursr' rr t'-k) t n"ean)
Resources availableFornral risk score classi[icatiotl
Nutritional assessment
Uterire heiEiht measurcment
Bloo.l !ttets.,te r'leasurcDlellts
Dentnl exalni11itionPreslr.rncy Lest
Ith (- ) antibodicsHaenroglobirFasting blood glucose test
Uterine height chart
illaternal rveight gain chart
V,rginaI sPectrlumH.rnLlJre'ltl DoPPIer
Fetal sietl'r()sc()Pe
Tetanus ttrxoir.l
Schcdulc visits ti)r r()ltlirt 'JrcColtinttitv oi clre
I{anrrL d('s rnllilrl,ld lo i1'1lt_r'isl tr'r'rttutt
Cardiok\coiir.rphOr.rl gluct-rse ltstGlucose iolcrancc teitrorrltlrrrr'd
1il2
21
6
:07
21
l472
20
6
19
7
23
72
l9
33.2
23.5
13
i9
lt.9
12
2626
1619
24
2526
266
12
l619
26
l6i620
262{tt'
12T271t-
16
2i272726
59
27
22
27
27
27
21
t55l5
, I!',ti lll,rch"! tl S(icnct' Ll(l i'r,di'tl'x n'xl !"t!t't l li'f it ti"ln':y t:' S PFI 2' l7-5H
Tlrc I'VHO nt t'nnl.ll rnrc RCT; '1iii()"rllt'
rt'lrl sllrilt/ dcs+j'r .15
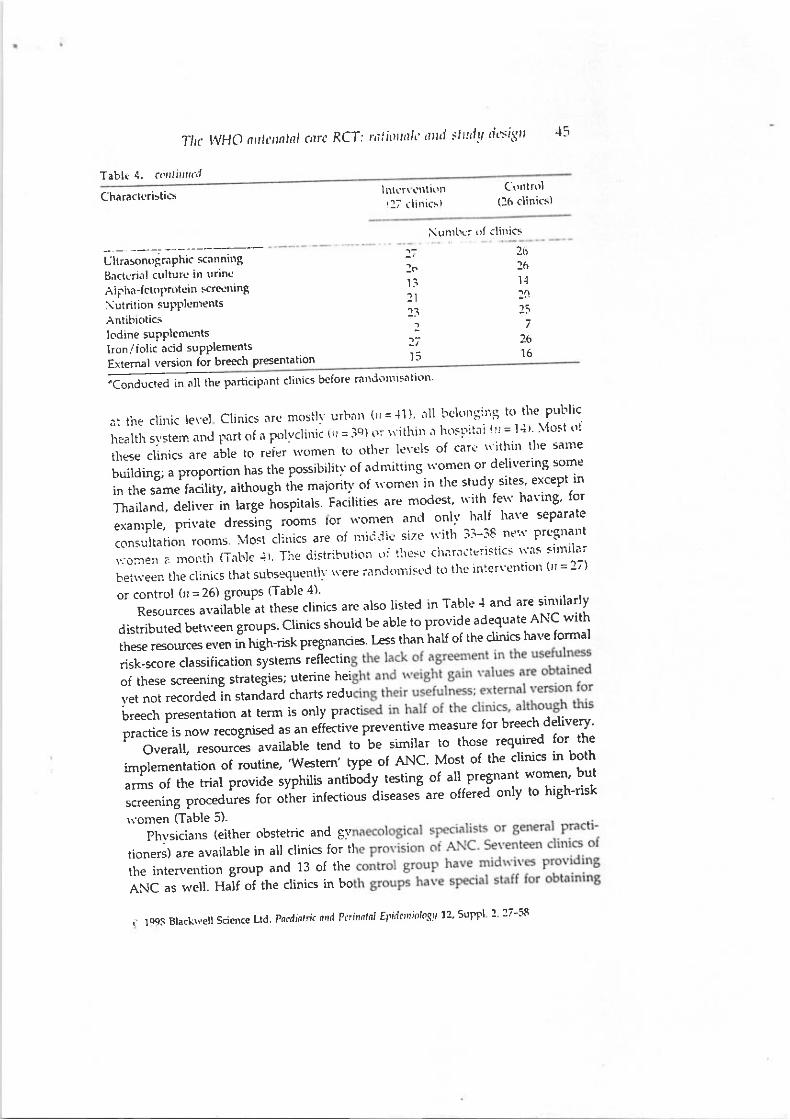
Tabl( 4. corllirlx.rl
Charnct{]ristics
Ultrason(,gr.1Phic sclnniDB
B.Ctcri<11 culturc irr trrine
Ailha-f ctoProtuin sctettring
\utrition su['Pl!'nrentsAntibrotic.Iodine suPPlcmcnts
lirl('r\ \'trti(rn1l; (litrics)
(i)ntrol(16 clinics)
!unrlrrr (,, (lilrics
lron,/f olic acid supPlements
Extemal version for breech Presentation
26
l614
:0li
7
26l6
t;lo1i2ll3l
?7r5
;A;;,*,"d ln-fl ,l* ParticiPnnt clinics before ralld(rllrsati(rn'
ai the clitric level Clinics nrc mosill urharr ('lr=-l'l)' ill bcl(rnqirlq k) the Pul'lic
f-r".i,it ti.,"* ""0 }rart of fl Polvclini; (ir = jq) (l \Lithirr '1
hosrliiai rri = l'lr' \'lost oi
iir"r..f**, or" "Ll",o,"it' tt't'rn"rr to other levels of cart rr'ithin tlre sarre
I"riir"S, a proPortion has tlre possibilitv of admittins \romen or delivering some
t^ ir," .,?t"J f"J try, although t'tte m"io'iq' of rr'onreu in the studi' sites' excePt in
Thailand, deliver in large hospitals Fatiliti"t o'" modcst' l\'ith ferr' having' for
exanrple, private clressing rooms lor women and onh' half l\are separate
.on.'.if,^rio^ rooms. \4ost clinics are of nric.i'liL'size rtith 3l-38 ne".. Prcsnarlt
\ro:ne11 a nrorrtlr (Tal'lc +t Ti1e distrihtrtior tr: tltc:'c cllilriiicrisiics \\'as silllilai
t,eirr'een lhe clinics that suhsequentll rr-ere;an''lott''istl to thc in:crtentiotr (rt = 27)
or control (rr = 26) ErouPs ffable 4)'
Resources available at these clinics are also Iisted in Table { and are sinrilarly
distributed behr-een groups Clinics should be able to provide adequate AI'\C with
these resources even in high-risk pregnancies t'ess tlmn half of the clinics have formal
risk-score classification systefis reflectin
of these screening strategies; uterine hei
vet not recorded in standard charts redu
Lreech presentation at term is only pract
practice is now recognised u' un "ff"ttit"
p'"r'entive measure for breech delivery'
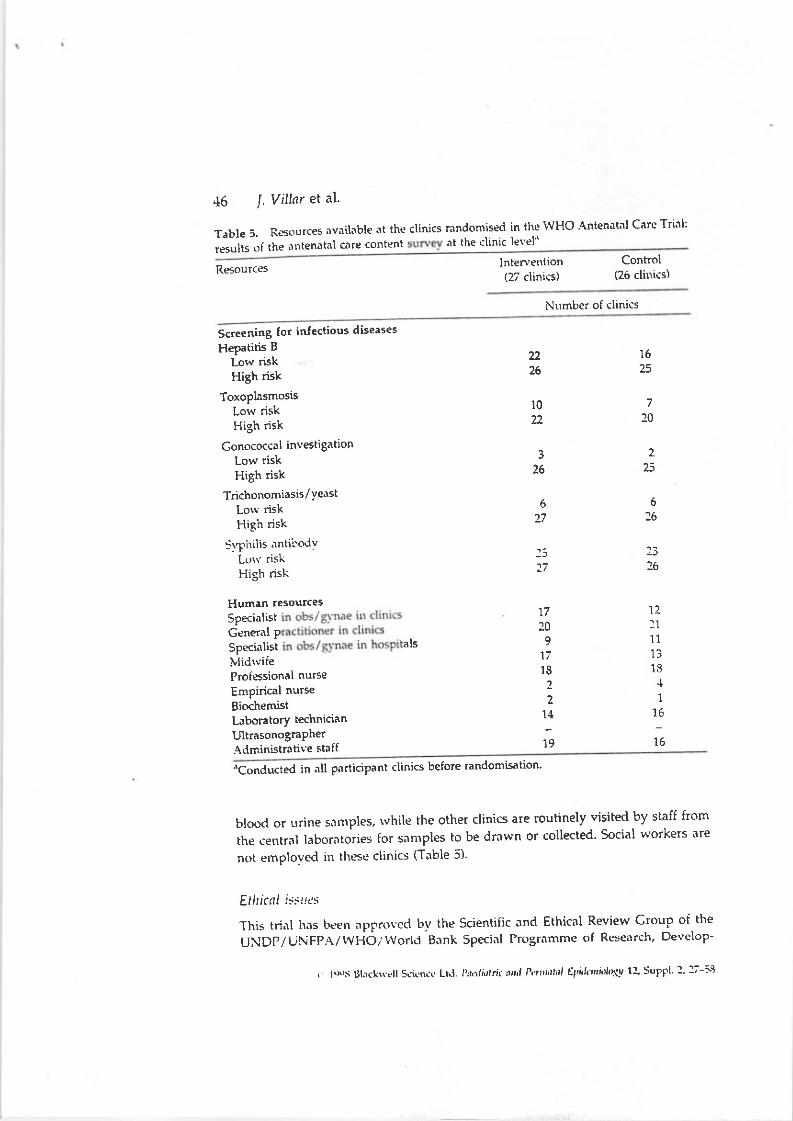
"'TJ;;;;;.f r""u"ur" tend to'be similar to those required for- the
imDlementation of routine, 'WLte*' type of ANC' Most of the clinics in both
:ff;i#;ipt",o"-typr'ii" antiuoay testing of all.pregnant women' but
screening procedures fo. otit"' int"ttio" ii'"ut"'- "'" offered only to high-risk
r,' onren (Table 5).
Phvsicians (€ither obstetric and Sv
tioners) are available in all clinics for tl
the inten'ention group and 13 of the
ANC as u'ell. Half of the clinics in bo
a lqgs Blackr.'cll Scic ^ce
Lld Pocdtoti( nt P'ri't'rlnl El'idcrriolosu 12' SuPFI 2' l7-Ss
45 I. Villar et al'
Table 5. Resources available '1t the clinics ranclomised in the i{HO 'Antenatal Care Trial:
results of the nntenatal c'1re content at the clinic level'
Resourceslnterverrtion(27 clinics)
Control(26 clinits)
Nr.rmber of clinics
Screening (or infecdous diseases
Hepatitis B
Low riskHigh risk
ToxoplasmosisLow riskHigh risk
Conococcal investiSationLow riskHigh risk
Trichonomiasis/YeastLorv riskHigh risk
Sv[.irilis antirodvLcrrr' riskHigh risk
Human resourcesSpecialistGener.rl PSpecialisi als
lvlidrviieProfessional nurse
Empirical nurse
Bi(rchemistLaboratory technician
UltrasonograPher.{dministrative staif
2226
l022
3
76
627
:377
17
209
'ti1S
2
214
19
16E
7
20
E
6
l6
26
12:111
1313l,l
16
15
bloocl or trrine sar:rples, rvhile the other clinics are routinely visited by staff from
the central laboratories for samples to be drawn or collected' Social workers are
not ernploved irr these clinics (Table 5)-
Etlricnl isslrcs
This trint has L.|ten appmved by the scientific and Ethical Review croup of the
UNDP/IJNFPA/wHO,/worlli Bank SPecinl Programme of Researclr' Develop-
''Conclucted in nll ParticiPant clinics before randomisation'
, le S Uhckrrrll SLicN( Ltl. t',& ririllr. ,,r,, Ptnt,it Eni.h",li,t$u 11 SuPlti :' l7-i3
Tnc l(,9O rl'li'rlnlnJ iarc RCT: r 'tiiotialt itttri sl'lrril/ iir'si:lri 'l;
Irrt, tluctitltr' the WHO Secrctarilt
i'i..tt nntt thc lnstitutional Rcvic\\'
ct'trtres a ntl co;rsponding health
their babies'(b) Most u'omen attendinS prenatal ca-'
do not receive' nor rtill theY in
continue Performint those tests
randomisation status'
g 1998 Blackr\'ell S'ien ce Ltd' Po.llirlti' o'1d Ptri'rnlnl EPnicnri('los? 12' SuPPt 2' 27-58
48 l. Villtr et al.
rvould receive the 'best stan(lard treatment'as currently offered in these clinics'
The collectetl tlata .rre usetl no differentlv from their routine use by clinical
departnrcnts or cotrntry health authorities for analysis of risk or outcome
inforrnation. .\n ex.rnrple of this strategv has recentlv been published for a trial
of s.r""ning for colorectal cancer in a healthy population in Denmark'3r
Furthermore, because of the cluster allocation, pre-randomisation informed
consent oi individual rvomen is not logisticallv feasible to obtain. The inlomred
conserlt in the intervention clinics is obtained Post-randomisation as it is the cl'inic
that is the unit of randomisation-
There has been a recent inten'ention trial in rvhich a written informed consent
is only obtained from the person legallv responsible for the unit of randomisation'
In tliat particular cluster randomisation trial, \'hich was of vitamin Asupplementation to children, consent lvas obtained lrom all of the 29 'village
de..elopnrettt committee' chairmen, and on-ly verbal consent was obtained from
the caietakers of ParticiPating children.32 In another trial that evaluated a
combination oi ANC and trr'o models of deliven, but rvith t'omen as the unit of
randomisation,'r informed consent \Yas sought onlv irom the exPerimental grouP'
The consent .lcsign rte are usins in this trial is related to the ProPosed design
bv Zelena)Jrrri hns r:a!':ttl\. l.recn ciiticallv re., ie,.. ed (t/lc silgla rotrrlotttis.'d rcttscttf
Jrsi,.:,rl i,r icre:cr:cg irr ir,tlir itiuai ;an icrnri:atlcrn in cJlrcer treatmenl iriais'1
Although titcse autllors ,.'iiscouragetl it ior cancer theraPeutic trials, rvlrere
individrrals are the urlit oi ranelomisation, r{e believe that most of the limitations
identifiecl bv then either tlo not apply or .rre unavoidable because of the
characteristics of communitv trials, especialiy rthere different EeograPhical units
are randonrised. Tllis concePt seems to be shared by experts in the field
(D. Altnr:rn, person.rl connrurrication to J. VilLrr; Oxford, UK, 1996)'
Discussion
This large, complex, randomised community trial has been implemented with the
assistan;e of collaborating cetrtres in developing countries and a selected group of
international scientists acting as .rdvisers. [t is the unanimous opinion of all
concerncd that this ri:lorous evaluation has been long overdue' The nerv A'r\C
p.rckage repre;ent:i,r maior dep rture irom the Present recommetrded form of
iare, ,vtrich is strorglv rootc(l ilr obstctric culture. We rvill not be able to determine
\r,hethcr anv Fotertial bencirt irom tht' intervention is rclated to the fre(lnencv, the
ovcrall content or.r specific nctivitY of the neh'PackaBe. If the results of the study
clerronstrate thit thc llc!\' tntxlel is sit:rilar or evcn better thalr the tradition.rl
mo.lel, this rantlonrise'tl controllctl ,..lesign would be basic tr.r the accePtance of the
proposL{ rrel\' programnlc. Nonetheless, there are disappointing rePorts that
rtxults oI ran.lrtnrisccl trials shouing clear beneficial elfects have not been
incorporited into prncticL'cvctr loltg liter the form.rl publication of the trials.3i':5
, Itrrs lilr.f\\(ll LLr('t!(. l-lJ j'r,1j,i,lrn-,,,,J l\'rintrl Ei,ti'ttti,'ln:u l2,Srtrfl- l.:;-13

Thc INHO ntluntnl cnrc .liCT; ..rtionnlL, nntl slntly tlcsign 49
Onc area of concern in a trial such as ours tllnl can seriousl], aficct its rEults isq hether or rrot clinicians are comolf in6 u,ith th('nor raodcl of ANC. Obviously,if the tu'o 6;roup; reccive more or lq;s tlre s,rnr(' tvpe of care the trial will be ofIimited valuc. This could r6ult from tlrc intcrtcntiul trouF being providcd u'ithcare additional to that recommcnded in trre tri,ll pr(')t(rcol because stalf see thestandard ANC nrore fatourabir'. Converselr', the stafi o[ thr'control group mayadopt the heu-' model ('therapeutic c()rrtamil,ttio!]') and reLiucc the number ofvisits. One trial on thc routine use of cpisiotorrrt h.rs incieed encountered thisproblem.sT The follorr,ing meclranisms arc in place in tlre prcsent trial to reduceand evaluate inten'ention compliance: exterEi\-e initial training with interventionprotocols; continuous monitorint of protocol conpliance by visits to the clinics atleast every fortnight by the study field director or local principal investigator; andhequent site visits to the study sites by trial coordinators. Compliance rvith theintervention was evalu.lted using the'ANC checklist' (Fig. 2) implemented in theinberlention eroup. This checkiist has comDl!'ted in a randorn sanrFlc oi Yisits bY
the clinician rsponsible tbr the visit, an e\ternal observer and bv using dataobtained from the medical records. Agreement anrong these three 'checklists'\r'as calculated.
Furthermore, u'e have informed care providers in the control clinics in detailthat they are part of a randomised controlled trial, and rve have explained itsnature and have encouraged them to adhere to their standard -ANC protocols andreferral practices. This is |en'important for a comrnr:nitY trial expectins to trul\,c()mpare t\l-o dj.iferent forms of care rather tilan a rigorous .{\C protocol(inien ention) r's. an ANC r\'ithoui a protocol.i' Clinics in both arms of the trialalso receivcd scheduled visits for monitoring patient recruitment and thecompleteness of medical records.
A trial rrith characteristics such as ours provides many opportunities forintroducing bias. We have rnade considerable efforts during the preparation of theprotocol and the implementation to follou, recommended guidelines forrandomised controlled trials in reproductive health3e and for the futue reportingof such trials.o An unpredictable allocation sequence was centrally prepardusing a computerZeneratd random sequence and kept at the cenEal unit untilthe time of treahnent implementation, thus eliminating the possibility oI allocationdeciphering which is more likely to occur in unmasked trials. Cl.inic staff were notaware of group stahrs (allocation concealment) until the time of initiation of thetraining workshops and patient recruitment, thus preventing selection bias, as
after this time there is no longer the possibility of refusing to accept anyparticipant into the sh:dy-
Ho$,evel, there are, in theory, at least t$,o instances in lr,hich clinic staff cansubvert the randomisation process. Firstl)', they can discourage high-risk patientsrthom they may know are considering attending an intervention clinic, iI theyperceive that these women will have poorer outcomes if enrolled in the new,
! l9S Blackr{ell Science Ltd. Pocdtattic nnl Ptnna|r',l.l E idcniology 72, Suppl. 2, 27-56

50 l. V illar et al'
simplified ANC model secondlv' individu'rl ed only in
i;'J;';';"*'"; clinics i. tire inten'enti ge of the
;;;;;.;;;;is#ent rherefore' clinicians c according
a" *i."iii"y b"",*ve will be the omen can rehtse to ParticiPate
i" in"'""* *.Oa "fcare
and re f,odcl in this or another clinic'
ln both instances the intervent be 'healthie/ than the control
group and Produce better Perinatal outcome- For the'first situation there "*,,1x,11"$:::;,:":ii::'fl::,HJ:::
,nd tit.,rtion, rve are going to analyse the
particiPates excludingthe shrdy.
Horvever, it is likely that rvomen rvho refuse to ParticiPatewill miss more data on
outcome variables than the total PoPulaiion and contribute less to the final
:nalvsis. Thev rvill, nesertlrcless' hai'e is detailed a baseline risk-tlescription as the
ffifi;;P,;ro,'ing fot totnpu'ison lvith those \^'omen s'ho agreed to be in
the ner* model meniation of the inten ention Ho\t'e'er'
ose protidine care tltrring iabottr anti
sPital d.lia clerks are masked to group
t bias. lt u'ould be possible"ls recentlv
masked, as this is a sub,ective Processias during analvsis is to
as r,;r'll as detailed and
the lar':est trial on this
. analvses rvill be conducted'
ibias and recoSnising that large trials are
ations,{3 it is possible that we will observe
n'ention al bias
is empiri ls Yield
larger estimates o[ treatment effect than double- 17V"\'aa
Randomised controlled trials evaluating drug and non-drug forms of medical
care are particularly important for tJeveloping countries' where resources allo-
cated to health are scarce and should be used for the imPlementation of cost-
efiecti,re forms of care This allorvs prioritis'rtion of lrealth-care services to optimise
the use of resources These trials als
against the transfer oI incffective
south. ConverselY, resttlts of ran
developing countries have inflrretrccrl P
iotn .i,,ingr, nrulticentred rantlomisctl controlletl trials rvould have lvoided the
rvidespreact use of perinatat technobgies of dubious "ffectiveness
!5 1''11
, logs ill.r(krscll Sdenc!' t-ld lh,',iirrlri' 'r,,rl PnDut f!&1'tlln'!tt l2' SrrFFl :':7-is
Tllc WHO nnt l!fll carc RCT: rntionnlc nnd strrr l dcslgrr 51
Tirerc is norr clear cvidcncr.'that h('alth L.'rioritl irltcrventiolls cnn b('evah'talt'dbt,developing countrt re;clrcltcrs ill the conte\t ol largc rancionriscd c()ntrolled
trials and rcstrlrs put'lished in learling iournals.:'{"-i" Dcspitc tlrese success stories,
conducting large-scalc, cutiins-ctl3e health serlicc rtscarch in developing
coL:ntrics is a lirrmitlable trsk. Donol agencics .lrc llot totltlll convincc.l t'i thc
lrcr..el ior thesc trials ftrr the r'\'alultioll of nrt'tiic.l] ilt tcr\'('n ti()l'ls. Partictrlarlv tht'
non-clrug forms oi cart' that s(--l.n 'lqgicalh' gotrd llris ilttitudt is Prescnt evell ifthe trials are relrtiveh' itrcxirensivc bl' industri.ilised coutltries' stand.rrcis ltr the
case of the current conrplex trial, several largc agcncies h.ld to be enroiled to
complete its total budget oi USS 2.5 million for 3 vears and includirrg more than
24 000 women in four countries. Furthermore, the cost of field 'a'ork, overheads
and researchers' salaries is often hard to explain to potential donors rthen thev use
the current logic of international research funding.5r lt is clear tirat the reu ard ofqroup menrbership, satisfling both iniellectuai curiositv atr..j comnlitnrent to
reDroductile Ireilith, nltlxrugit \-erv it)llx)rinnr to;rll rr; us. llis t(' he comnlemented
bv tangiblc rerrirrd s ior those in thc trenches oi primar\ data collection, ii rTell-
designed, relevant trialsi2 are to be successful.
Acknowledgements
Thrs is a collaboratitc eflort her\reen the I-\DP/U\-FP,\ /'\\'HO/'\\ orld Eank Special
Pro-qramme of Ileseerch, Drrteloinrcnt alld R$('.1r(h Tr.r: 1ilrc ilr liunr,li: IiciiloluciiL)11 nnd
tii,.. \\'!lC Divrsi(n o; Reorrro'.rcrir-c Hd,rith (Tu(hllical S'-ii't'(rrtl
.{,lditional support rias pror-ided tor the imPlemenlatron oi thc srudY bl-: i\lunicipal
Govemment, Citi of Rosario, Argentina; Ministry of Health, Cuba; National Institute of
Public Health, Mexico; The Poputation Council - Regional Of6ce for Latin America and the
Caribbean; Ministry of Health, Saudi Arabia; Swedish Agencv ior Research Cooperation-
sith Developing iountries 6[DA/5AREC); Ministrv of Public Health and Faorlt-v of
lvledicine, Khon Kaen Universiqv, Thailand; DePartment for International DeveloPment(DflD) of the United Kingdom; Mother Care - Iohn Snow lnc.; National Institute for Child
Health & Human Development (NICHD), National Institutes of Health (NIH), USA; the
l{orld BankFor the preparatory phase: University o[ western Ontario, DePartment of EPidemiology
& Biostatistics, Canadi; National lnstitute of Public Health, Noruay; United Nations
Development Programme; University of Uppsala, DePartment of Obstetrics & Gynaecol'
ogy, Sweden.' We would like to thank esPecially the r'romen and their babies who participated in this
trial and the many doctors, nurses and other staff of the clinics and hosPitals that made the
implementation of this Proiect Possible.Special thanks are given to Dr M. Koblinskv lor her personal interest and suPPort for
this project, to Dr O. Meirik for his permanent encouragement and suPPort, to Dr D Khan
Neeiorui. for het eiforts in editing the trial's Ne\{sletter and to \4rs Christine Crav for her
help in the preparation of the manuscriPt.
r 1996 Blaclscll Science Ltd Pnnlintri. n .l P{ nhl El'itt ,iolosy 72, SUFPI 1 27-53
52 l. V illar et al'
Manbers of the WHO Antctlatll Care Trial R*eorch Grortp
Trial coordinating unit
Data coordinating unit
tisticianms Analyst, Statistiial Assistant (until July 1997)
en (from JulY 1997)
Steering committee
Health economics SrouP
Miranda Mugford, Health Economist' UK
iri" ii*,..,"nt"rtit Economics Researcher' uK
ffi fox-tusnbY, Health Economist' UK
QualitY of care grouP
Ana Lans.er, Reproductive Health Specialist' ltlerico
c"i,*o "ui*"n.iu, Public Ht"rlth Spccirlist' Nlexico
\lariana Ro-mero, Public Health EPidemiolotist' Argentrna
Georgina Roias, PsYchologist' Cuba
iirt? f".n"iti,, Public llealth Nurse' Thlilnnd
iUuneera AIOsmi, Nurse' Sau'li ArabLr
r.lg96BlackwdllSdcnrcLrd,nr.lri,lr(fln/Ari,rdlxlEi'i.lc,,xd'rtiYflSuPFl:':7-iS
Tllc ltIHO at ctntal care RCT:;nlilrttilk' n'lrl stl/dy dfsiq'I
Data and s.rfetl' monitoring committee
Countn data coordinators
Eciuardo Bcrgcl, Argentina
Liana CamPodonico, ArgentmiEIva Diaz, CubaMohammed Gandeh, Saudi tuabia
Yaortaret Sirguakool' Thailand
Field coorditrators
.ilicia del Pino, ArBentinaIuan Vdzqucz, Cuba
iuaUi "*e"a
Helal' Srudi Arabia
Kamron Chaisiri, Tlniland
-D,r"i;.-ir)riir;.1 : rtsiil ltiiLrrts nti'1 si!i(
Centro Rosarino de Estudios Perinatales (CREP)' Rosario' Argentina
Countrv coordinators
los6 M. Beliziin and Guillermo Carroli
Clinic suPen'isors
Susana Difulvio; Madela Ferronato; Sil\ia Galliano
Clinic directors / Physicians
( l99B Blnckr{'ell Sciencc Ltd. Pndlrn,'i( nnJ Pnnnt//l EPidc'niotog! 72' SuPPl 2' 27-53
5l
i
I
I
54 l. Villor et al'
lleco; G.U. Paz; R.A. Gorina; G' Lombarte;
; S. Carbognani; E.F. Guzmac D' Crmta;
ini; S. Parfait; A. Cartizo; l Alcacer;
D. \'lovano; A. Treidel; !l Alesandrelli;
; I. Blanco
Trial focal Persons in clinics
M. Baneiro; S. Vera; I C6rdoba; A Martinez; N Sosa; E Rol6n; S Pirani; B' Moreto;
ii. i"tri.^l, n. ;g-l,izam6,t; N Band; G' Deft€s; N' Arin€; F' Burgueio; S' clemente; A'
Piekella; .q.. Mdrquez; S Aguilar
Chiel nridu'ife or ntrrse
S. Abarno; T.R Paz; R.A. Raitrome; C- '\meriso; \l Carr6; V' LrlPez; !l E Galiano; L'
Ba,lin; O. SamPieri; C Llompart; S' Seco
Hospital Gineo-Obst6trico 'America Arias" Havana' Cuba
Counrrv coordinators
L'baltlo Farnr.rt .rrrd Juan V'izqr'rez
Field coordinator
tuan Carlos Vdzquez
Clinic suPen'isors
Isabel Rivero; Guillermina Curra; Juan Quintero
Clinic coordinators
Alfrctlo Abeleltla: Elise.r r-le Annas; Jorge L. Grrcia YY, M.". De los Angclx Golpe; Luz
it.riJ* v-iG, fsrrcl C.rLrrer'r; Rot'citt' l''icz; Zeiln Riter6n; Dolores Mustelicr; Lisette
f .'it.-"n,ti"; llarhl Aquin(); CLr ra Hern'in.lcz B'tngo
Trial foc.rl Pcn;ons irr clinics
Nrrrma Trianr; Piblo Ven('re(r; Crrcit'lo Espirosa;SiN'ia Niela; D'rimi Mrso; Olga
i;l;'ig.i;il i'1"; i.ra P('rez !lt'm':incz: \l'ridi l. Roso; lllirn'r '\* artr Diaz; Raisa Calvo;
Anrarilvs lllartin
r loos Rl.r.h..ll Sl:rctrt:r Lrd. lir,lli'ririr r 'l .1'/i nh E/'i''')"ir'/"."iv 12' SuPFI :' l7-i8
Tfic l4/H() inlc tttttl cflrc IiCf; ,tllionnh' n'rl slrr'h7 rltsiqrr 55
I-losPital tocal t*rsonsk'rsuDcls.rclo;Odr)ri(('Sttrk)Donurrso;Rnf cl\';rrrcsas;Carlrrsl('rtric;BirtraraTrilkr;D.rvi.lc Casrgrandi; L()urJ$ Marcr(r
Ir{inistry of Health, Riyadh and National Cuard King Khalid Hospital'
Jeddah, Saudi Arabia
Countrv coordinators
) agob Al'\4azrou and Hassan Ba'arletl
Local investiSation team
\1<.hanrltrctl BllLlo; T.rrtfik Khol'r; Talal lkranr; Kh'rli'l '\['[r'.rs
Trial focal Persons in clildcs
Zainat, Emam; Kh.rdija \'larzoc; Antulmma Salicr; Omvm'r Salcm; Kalthoour i\'[ostafa;
Sh;k; B"t;;; Firida Akbar; Kha*ria ElAhm'rd1'; Buthai'rra lvl.shlrour; Glrava EI'Ta1'eb;
Sobiria El-Sod.rnr'; Sohta Al-Sheikh
Ciilti. (iirectors,''pitvsicians
S.1iliaBan..lD:.Amir.rHem:r.i:\uzira\{aIri1,ar;RiiatEI-Bilmarr'i;HctlcllHnssa|l;\^.,cdad;il; i* ;;Ja; Farida Sar'rrtak; Mol'nmtned Haicz; Anal Kamal: Sa(a Hatata;
Favka Ashkan
Faculty of Medicine, Khon Kaen University Provincial Health Office
"iJ i'""ftft Promotion Centre, Region Khon Kaen' Thailand
Countq' coordinators
Pisake Lumbiganon; r.'arong Winiyakul; Kamron Chaisiri; Chompilas Chongsomdui
Clinic suPervisors
PongsriSarrduisrriya;PannapaMadst}un;JitlaPratniwauPanavadeesutthiwong
HosPital directors/PhYsicians
Uthni Uklrotsnnakarn; I'ra1'<xrn Kortit: Suri)a RattanaParilr'\'a; Sus'annachai Watta)'in8-
charoenchai; Xarrcrrit nfte#ciitrpht'ng: Kaicm Phathiritlri6ul; ChomPot Woratharakul;
Cha\\'alit r.\iharargkul; Tuem SaYbuathors; \Vichai UssavaPhark; IIPoP StnPaoPradrsr;
\ViPat Saliddeechaikool
a lqgs lJlrckNcll Sci{rntto Ltd Pn('drnlrii n'rJ P''j'/ah' El)i'h,,r;",,lotu 13' SuPPl l :7-58
56 l. Villar el al.
Trial focal Persons in clinics
.\nchana Puchoksiri; Jirnwan KitlerdPomPatoi; Arunvanhupan; Sukalya SrialnaraU t{imon R'rtanlchoilt; Such'rda
i Changthom; Khannistha :llaheor; Suntosapom Ciuipromm'r
Chief midwife or nttrse
Iarunvanee Pulvasunti; Jintana Suvannatat; PrakaytiP boPrasert; Naveeya Chuaksuchinda;
i*.'r^,rn Xr.n "neejan;
PomthiP Kon8nSaea Khanittha Chansafiuan; Supawadee Asada-
,rio.rgtot; p"t.tt"t* Silee; noon$hiP fongsap; Boonlerd Chanchurnni; Supunya Sonhai
Administrative and secretarial suPPort
loyce Sta:ks (uP to Se PtemL'er '1996)
Christine Crav (trom Octobcr l996)
References
1 Rosen \1, \,erLrtz l. Hill , Ciring lor trur future: a returt bv the exPcrt Panel on the
con
" .ed-\'isit5
Prc- natil care
visits on oerin.ltal outcome among ltrtt'risk r{or
o -
ltfoof.i r, Wtfton .1, Clement S. bas 5, Smeton N A randomized controll€d trial comParhg
trro ,.h"drt., of ontenatal visits: the antenatal care Proj€dBritis'[ Medicnl lourtrdl1996;312:
546-553.l
- c.*n on" AL. Effeclrrcrrrss tl d Eftici.,tcu _ Rnndorrr R.fl.rtiorrs o,r Hr'rl,,r sr,r.'icds.The
,luftielt Pro*incial HosPiral Trust: Cambridqe Universit-v Pre;-" UK 1969' PP Jr-{'6'
o -"L-iia-irt
c, cnattingius 5. Tle scientiiic basis of nnlenatal cnre. Reporr fiom rr sr.te oi
the art conference. .{ctn Oisicrriri"''l Cv'tu'ritlolticrr Sconiimlico 1991;70: 105-'109'
z.- st".' p. Rituals in antenatal c.1re - do we need them? Brihs,, Medi.al ]ournal 1993; 307:
687-498.i firceffu f. Does Prenatal care imProve birth outcomes? A critical review ' Obslet'ics atd
cun,'coloe! 1995; 85: 468--179.g" fu.i""r t, Hall M, Horvie PlV' Reid !1, Barbour R, Florev CD, el nl Should obstetricians
see women with normal Pregnancils? A multicentre randomized conkolled trial of routine
"ii.ni*f .nr" 1'y generai Pr;ctitioners ar.l midrvives compared rvith shared care led by
obstetriciins. Briti;h tvladic'tl Jr'rrrrrnl l99tr; 312: 5il-559'iO- A"ff.","ig fS. Vcth(xloktqical l'robltrrrs and Possible entl['oints in thc elnlu'1tion oi
anten.rtal carJ h trnntionrl lol:'ntl ', T(,1'lr''\r/ 'lsstss'tt:ttl i Hcnhh Cott'1992; E (SuPPl l):
33-39.1l lteirert C. ivlulticctrtcr tri.ris .rnd irl[cl: luxurv or necessitv? Conlrollci Clitric'tl'frrnls
1990; 11: 39q-10'1.12 Sitvermln W, i\ltm.rn D. P,'itietrts' Prelt'reDces nnd randonrizcd trials' Ld,lrct 1996; l'17:
171-17.1.
13.{rrnillscP.lrricrinr.rrraiysisirrclirliiJllti.rls.-Sld'is'i'il'!M'''lititrtl99l;10:92i-937l-l Rotlrman K. Placebo r:r.rni.T. ijlrli-'/l |tl,:,lt,ttl lournnl 1996; 313: 3-4'
, !1x)S ljl.r(:{r(ll::nll\r LlJ. I'.,,1/;r'Irri,L,iI t\'t!'t nltfil ttiln:i! 1?, Strppl. I l;-i$

Tlrc ltHO nrtlcrntnl cnrc RCT: t'illittndlL' nnd strrdy dlslqrr 57
c .:ollttrlt ol routilre antcnata! cnrr: l'e or i'tllL'\'intc ad\'crsc nratcrnal outcomes
/b: l - 1.1,
telrt oi rouhlre anlcnntal care: ll Po\r'cr t('
i..-rnr"., .,'nl" spcrtal corrditiols and
It,hrt,rl tit l(rc)i;76: 'l5-25
tlcrt DL ,tss'rssin; thc effLtcti\'!'l1css oi a
tldrcatioll of irfarLs with lor{risk scorc for earlY PrenatalH.'dllh Orsrrrri:ntio'r 1991 ; 25:
durirrg pregnanc-v lr.;' Elfccti'c Cate-in
sr Cha"lmers-1, En'kin M, Keirse MINC'
365.pr"gr'r'tuti. aititudes in theraPeutic trials'
rhns,.n '\ C.rsr: conrrol studY ol intraPartum
r tr.L'rii-,rJ Jtrrrrtr'rl l99l; 306: 743-750'
ics 1995;9':l 277-271'ss oi inte^'entions to Prevent or treat
t C' Al-Oiinli lvi' ci nl' ConcePtual
and Providers' PercePiion oI the
olled Trial' Pneditlric atll.d Pctinotal
ttn.lc.l Theory ' Sfroleties lor Q aliloli-oc rleseatch'
anoli G, Farnot U, Lumbiganon P' ef al The practice
]ri,J il iiri"t"" p"rts ofihe world particiPating in
c"^i"riJ iiii. ra o*ic attd Pctittotol E1idmtiology
A randomized comParison of routhe vs selective iron
:';':,;;;;li";;)iutt cottcse olNutritior 1e1; 10: 3-10'
;l;fi#i ;ril;it'i"rs. rvJ Eigtand lournot olMedicine
Sondergaard O Randomized studY of
tood toi ['"cet 196;348:7467-7471' -
i"t"g"*"nt fo' l"tge cornmunity trials
C, HoPkins M' Kennedy J Simulated'
irial br ish lournql ol Obslettics otd
S, FaYers P' Machin D Randomised
nal oiCancl1995; 31A: 1934-7944'
i 1996 Black}rell Science Ltd I'ncrirnlrr' n"ri P 'tit,I]tdl
Epidcniol8 1z' Suppl 2' 27-55
58 l. Villnt et al.
Q[ the results of a trial on medical Practicc:o,rtroll.r'l Cli,ri.nl T rids 1996; 77l. 535'
actice. lrrcet 1993i 312; 8n-g/-g'man sPirit: The chatlenges of randomizedwnal 1995; 153: 753-786'6;34S:1172'
39 Vitlar l, controlled trials for the
evaluahon o ne 7996:2* 365-375'
40 Begg C, (l'l lmProvin8 the quality
of reportrng tement ,|,4rVtA 1996;276:
637-539.ai' S.i"f, KF. Subverting randomization in controllerl trials lA'vl'4 195; 274:1{5G1'158'
ii COar".fr" P. Blindini during data analvsis and writing of manuscriPts' Controllcd
Cliticnl Trials l 6:77:2' :t-293
ii i.n"r, ii. nnnao-;"a trials. human nahrre and reporrint liuidelines. l.Ancct 7996:
3{8:596_598+l- i.h.ll, KF, Chalnrers l, Ha)-es RJ, Altman DG Empirical evidence oi bias: dimensions
"i-"ii.J"r"gi."l quality assciated rvirh esrimarE of treatment eftect in controlled trials.
of clinical triaIaborntive Crthe coilaborirt
17 Arqentine Episiotonrv Tiiii C"iiacorat
control,.'d trial. Ii,rccl 199i; 3-12: 15:i-l51Sli"'\;iiir i, ri*", U, Barros F, i/ictora C, Lanser '\, Betizi'n J\I A ran'{onized trial oi
pty.f,"l*Of t"pp"rt during high risk preg rancies \ko Errglnrr'i /orirrrnl of Mrdicitrc 1992;
327:12(fi-1271ig S^i,f, A, Hatcher J, Nlackenzie I, Thompson S, Bal t' M'rcturria I' cl 'rl Randomize''i
i""-iiJ,.irr of heatmenr oi clrronic suppurative oritrs medll in Kenlran school clrildren.
Lrx,!?t 1996; 3'lS: 1123-1131
SO A"ti.;n;Vt, Villar l, Corrz.rlcz L Compodonico L' Bergel E Cllcium suPPlementatio!'r
io pr".=nt t vp"rt"*ive tlisorders oi pregnancv. -\-.:t, Errgl,rrrrl /orrra,rl ,r[,lIdicirre I991; 32-l:
1399-r {05-ii Vtacuettt F, StePhens R. Marketing clinical trials Larrcet 1996; 3'18: 111-l 12'
ii ii"aa" p.,'i, viitnt J, Carroli G Randomized clinical trials in Perin'ltoloty in Latin
America. Enrly Hrr.arott D&'cloPnlc l 1992;29: i2i-127 '
, l,r,)S lit.r(l\.(.ll c(rc'riL I...1. i'.r,,lir ,r.,r,trl I',,r,,r,r:,'l E-r.l,rii,i,\u rl, SuPPI l. l:-i5

Origirrul Arti<:lc"'
PATTERN AND FACTORS ASSOCIATED WITH GLYCEMICCONTROL OF SAUDI DIABETIC PATIENTS
Ahdul Rrhrrau r\l-Nuaiur. rrB. mcpc r.rcp. Solcmrn N,lirdad. lrssc. iusc. prrD:
Khalid Al-Rube ran. MIr FRcrci Yacob Al-Mazrou. rtu. phD. Frr('Cp:
Omcr Al-Attas. phD: Nasscr Al-Daghari. [,tsc
Background: Thc pattcrn and factors which can bc assciated with the glyccmic control of Saudi adult diabeticpaLients were exanrincd in this study.Patienls alld llelhods: Confirmcd diabetic patrenls lionl all regions of Sardi Arahia conslituted thc stud]popularion. Random blood glucosc <10 mnrol/L and >l0lnnrol/L Nas used to catcgonze patieuts into Sood andpoor SI),cemic control paticnts. respectivel).Results: Thcre werc 613 confirnrcd non-insulin dependent diabelic patients (NIDDM).50% \['ith Sood gl!'ccmicconlrol. Patienls with poor gllcemic conrrol *ere sig ificanrly older than patients with good glycemic control(51 5 rs. .17 \ears. Pd) 0001). The insulin-rreared diabetic populrtion amountcd to l3ft. comp.tled rvith J3%and -l-1% for oral agenl and dier. respeclivel) The rite ol insulin users among poor gllcenric conlrol diab€ticpopulation uas Istt. compared with 509r for oral xErenls. There \\as:r significant relalionship bet$'een
Sl\cefiic conuol and age. and lrealmenl nloduljties ol Dl\'l Subjects who had good glycemic control of DMrvere yoonger and tbllowing J dicl regimen. 'rhilc lhose \rho had poor glFenlic control werc older and on
insulin trcatment- Multivariale analysis cornprising.lI5 indiYiduals $as conducted to fin(l out thc faclors that
can potentially influence. or ma)' be associaled \\ilh. lhe control of DM.Conclusion: The association ol insulin therap) with po()r glycemic control is not a cluse+ffect relationship-
lnsulin therapy in our study populat,on is underutilizfd. given the high rate of poor glycemic conrrol and high
rare of relauve occurrence of complication amon€l th. Scudi diabetic population. There is a nced to addrcss thc
imponrnce ol maintaining go<xl glyccmic conlrol. and the relson for the low rate of insulin users. Closeperiodic monitoring of g)ycemrc control. urilizins laboralories and homc glucose moniloring deviccs. is
required. Eflbctive impletncntation of rhese D)easures. in addirron ro diabetes education. will have an irnpJct on
rhe turure outcome of the Srudi dirbetic populalion.Ann Soutli ltled l99E: l8(2 t.109'l 12.
Ke1 Words: Dirl)eres mellltus. gl)-cemic control.
Drrhetes urellitus (DM) is a diseasi rvith a high prevalence
rvorldrvide. and in rhe last feu, lears ils prevalence has
become nrore widespread in the third \r'orld or developingcounrries.r This is especially the case in the MiddleEastern courrtrics. uhich havc expericnccd an upward
surge in the prevllcrrce of DI\1 over rhc lasl l0 yelrs.- -fhis
is rhe likclv result of economical dcvelopment and changcs
rn lifestyle. especially in nutritionul habits.r The long-ternr
nicrorasculur and nracrovascular coutplications of.liltere:' are rcsponsrblc for sigrific nt morbidity and
rntrrtalirl' Diabctcs is thc leading catlsc of
I-r()n rhJ DcpJnnrtrr r)f N'lcdi.itrc (Drs Al'Nurnn \lrtd."l xnd Ai'R!ltr'rrnr. Kin! lih.rtid Linitcr\iry Horprtul. rhc DepJnn]e r ol ItrGrhernisr^(Dr\ .\l lrrrs rnd Al'Drlhuri) I'i'rS Sru{l U r\crvt\. !rrd Ihc D.Prrurl.rnlof Prc\.trr'\e Nlcdrcitr.lDr Al-iUr,'rou) Ilrnr\rn'ot Hc]lrh R,\rdh. Sruil,
\Jdr.ss rcp r rcqucsrs Jnd corrcsB)ndcn.. rr' DI ^l-Nuairrr:DcprnnEnr ol Medrcinc (MBC-.16). KrnS Fri$l st-..eirh\r llosprrrl I
Rc!('rrch C.nrrc. P.O. Br)\ -1151. Rivrdh I ll I l. SJrdr ArrbirAcccpred lbr publicrlirnr l5 No\cmbcr l19? Rc.ttvcd l0 APril l9{)7
blindness in adulrs. the nrost common cause of end-stagte
renal disease, accounting for 3Ola-40% of lhis population.is responsible for.10c,/c of all non-traumatic ampulations ofthe lower exlremities in adults. and is a major risk factorfor cardiac and cerebrovascular diseases."
Saudi Arabia has an estinatcd population of 13.2
million. 70% of rvhom are under 30 years of age.6 DM'rclated complications arc a fiequent (rcurrence among
Suudi diabctic patients. A review of 1000 consecutive
Saudi diabetic patrents in a gencral hospital showed an
incidence rate ol 329i for rctinoPathy. 26% lorlrl,pertension. il.l9. fol ischenrrc hcart disease. and 6.9'lilu ren l insufticiencl'.' Diaberes-related hospituladmissions arc liequenl and tcnd to occupy hospital beds
[or a longer time. as comprred to orl]er di:,cases.s
Eprdenriological studies hrve establishcd a relalionshiptrcrween hyperglyccmi nd the de!elopment ol lhe long-rcrnr complications of diabcres.'' rr The importancc of tightglycenric control with respect to dl]lay or In the prevcntion
,turtlr o! Suth tlt,li itt lil lN. ,\r 1. lt)t)lt I09
.\l--\l il'.'
of compir.ation. \\a\ nol cslirhlrshed unril lecentlr'. 'flrc
Diaherei Compii,-ation Contr<tl Tri:rl (DCCT) has provcrl
lhe imponan:. o: tight glyccmic cotttrol lirr thc prcvcntiulof conrrol complicalion antong insulin-tlcpel]dcnr Dl\'lpatienrs. - The conclusions ol Ihe I)CCT stu(l)' rcprobabil apolicable to the non'insulin dcpcndent dilhctcsrnellitu< r\lDD\Ir pitricnts as u'cll. Scvcral faclors uercrccognize6 a. plly'ing a tole in glyccmic control. iulons*'hiCh ar: duration ol- DIll. obesilr and hr pcncnsion.r-' r'
This oap3: is part ol a populution-b sctl
cpirlemio)ogical studl of chronic ntctabolic dtstrrdcr untonlSludi aciul: subje:ts liotn all rcgions ol Sludi Arabil. Itlrruses o: lhe pattern and factors afl'ectin! glvccntic
control oi non-insulin dependent diabetic patients.
Patients and Methods
The \ational Epidemiological Household Survey forChronic \'letabolic Diseases, which included DM, was
conducted among Saudi subjects over the age of l-5 years
in different regions of Saudi Arabia between 1990 and
1993. This \ras a nal.ional study wiih several objectives,
among them to measurc the Prevalence of Dlvl,
h ypercholesterolem ia and obcsity at national. regional and
rrrbal lerels Based on this, a sample srze of 37.000 u'as
calculated in order to sludy the pattern o[ glycemic controlof Saudi diabetic p3trents- A multistage slratified cluster
r3r':dom sampling technique was used for the selection ofthc studi population. The assigned population sample oIrhc srudS *as distribured between the different regions in
accordanc,: rlrth the regional population distribution as
provided h1 the National Population Council (NPC). There
u'as an initial adjustment for t1'pe of area (urban or rural),and populatron distribution in each region. as per the NPC.
Ciries and rillages ofeach region were ltsted and a random
sclcction of .r certain number of cities and villages
conducled in accordance u'ith the allocated share of each
region rn the national sample. The administrarive nraps oiIhc selccted ctttes and villales wcre revieq'ed lnd a
random selection of a number oi dlstricls in these cities
and villasc\ !\ as made
Primarl' care physicians \\'ho worl in these localitiesu,crc assenrbled and givert tlrientation lecturcs and
rvorkshops on difl-erent aspecls of the studi'. such as fillingout thc forms that include pcrsonal. dtmographic. social
irnd medical historl'. spccificalll dara rclaling to DM. such
il\ prcsent historl oi scll--reportins. Thc nlcdicll rccords ol
llrc\c plucntr '...crc rcYic\r,cd tt, conlirnr the diagnosii ol'
DIr4. Thc primari cirrc nh-vsiciilns uere itlso lrarucd ttn the
propcr mcthod rrl blrrxl hirrdlinS. ilnd nleusurcmcDt ol
hui:hl and rrcighl. lvhich is done al thc Prrnrarv Carc
Clinic (l'CCr. usurlly t\\,o or thrcc drvs alicr the prttcnl'sittrtrul "isltEvcn'third purirllel strect in anv of thcsc ltrulitics u'as
sclccred- und thctr cvcl\ third llouse u'lrs includccl in thissrud) All subjccti ovct thc agc ol l5 1'curs in tlre\c lrouses
rvcrc askcrl to plrticilirlc in lhis slu(l!- All thc intcr\ icu,e(l
sul'riccls rvcre rcqucstcd t() xttcrd llrc PCC lirr rvciglrt.Ircilht and bltxxl rncnsurcrncnts. Rantkrn blcxxl samplcswerc dnrwn in nn IIDTA tutrc. ccntrilirgcd. and lhc scrunrstored liozcn unlrl conrpletion ol lhc t rget s mplc. 1'hcsumplc's u'clc senl li()zcn to the Cenlrul Laktratory. KingSaud Univclsity. Riyildh. from all ()vcr thc countr\,.
Slmples u,ere stu-cd ll -10'C until assayctl. Upolrcuchirs thc targct nurrber of 100 subiccts pcr physiciiln incach district or city. or 50 subiccts pcr physiciun in caclrvillase-. rhc records wcrc scnt ro thc ccntrll oflicc inRiyadh lirr data entry. A computer program was dcsigncd.usin!: DBasc IV soliware package for data enlry. Alicr lhccomplctron of data entry. thcre was a final adjuslmcnt lorgender. age. region, urban or rural population distributron.in accordance with the NPC. using Statpack Gold soltwarcpackage, of a number of records fronr different regions and
age groups.Serum samplcs were used for glucose analysis on a
glucose analyzer (Beckman Paragon, Fullcrton. CA. USA)The method depends on the rate of oxygen consunrption b]the enzymc glucose oxidase. The instrument rvas calibratetlprior to glucosc determination. using qualitl controlsamples provided with thc solutions. The mcan valucsobuined on the controls were within thc values quoted h1
the manufacturer. The results were expressed by SI units(mmol/L). The intra- and inlerassay coefficicnts ol'variation were 1.'7 7o and, 2.69o, respectivclv.
A cutoff of random blo<d glucose (RBS) of l0 mmol/l-was uscd to categorize patients rnro goo<J (RBS<10
mmol/L) and poor glycemic control ([tBS>10 mmol/L).The WHO criteria for defilition of obesity (BMI>30) v.as
adopred.r6There are many variables which are belicved to
rnfluence the glycemic control of diabetic paticnr!i. Thesernclude age, gender. body mass indcx, region. plirce r;lresidencc (urbau or rural), duration oi DM. and treatmcnLmodalities of DM (dret, oral agents and insulin).
Vanous types ol-univariate analyses rvere emploled t(lassess the distribution o[ observations. to providc' an
understanding of thc relationships between variables. unC
lo selecl rhe variables surtable for inclusion in multivarrareanallses. Chi-squared test. Student's l-test, and Fisher'sexact lesl wcre performed to assess the significance of thcrelationships bet,a'cen variables. The 57c lcvel was set s
thc ler cl ol significancc.\{ultiple logistic analysis was uscd lo cxanriDe thc
assoc'iation bctrvccn the odds ol gll'cenric control and anrpretlictrrr.belielc'd to inlluence rt. ildjusling il lbr thc othcrpretlicrors incluclcd in rhc Sclrlcssemln nrodel. I98?.r;
Lolit tp) = 115,*, + b.\, + .... + bt\l
A back\v rd elirnination rv s crnploycd to sclcct lhc bcst,tiuing rrrtrlcl. Thc initi l nrodel inclucled all uain cflcctsThc cll'ccl with thc srn llcst Z-ralro u,as rsnrolcd urrd thcmtxl,.,l rclitted witll rhe renlaiDing cfl'ccts. Thc- unal!sis hld
It0 Aa at..,l \ t.tt ihln ,,.l;'/ /ri. M,:. /q'Jl
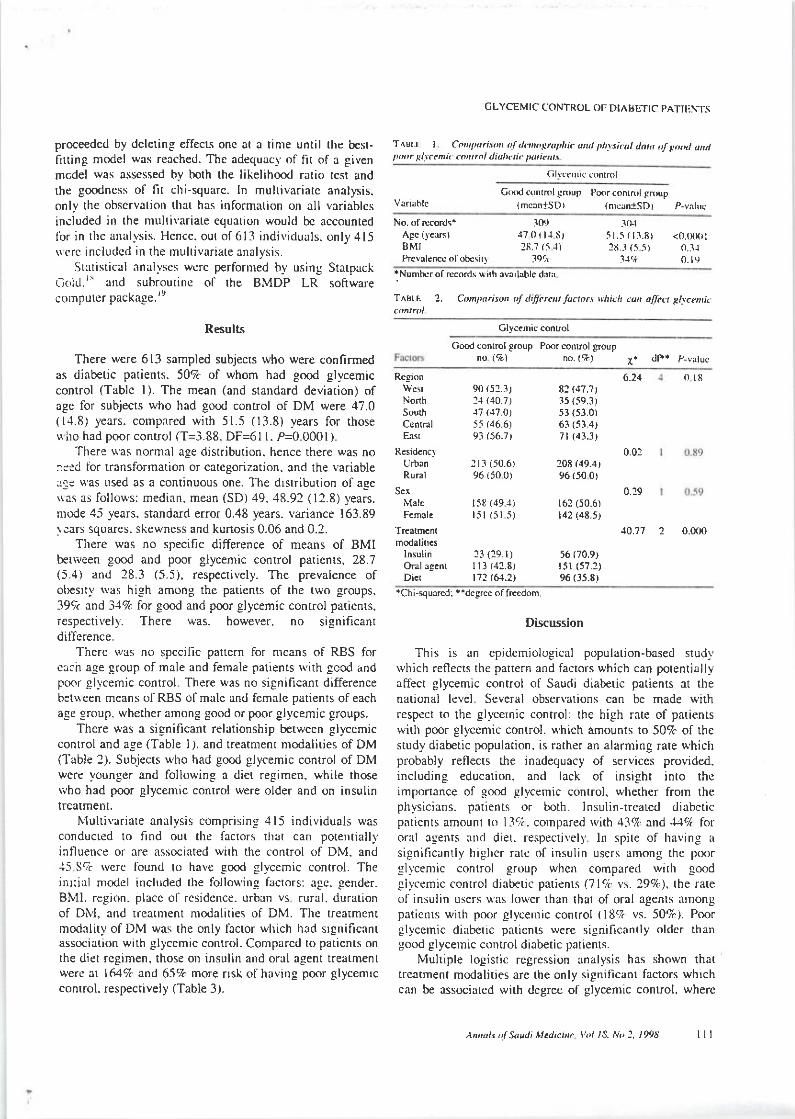
proceeded by deleting effects onc at a time until the b€sl-firtin8 model was reached. The adequacl'of fit of a givenmcdel was assessed by both the likelihood ralio resr andthe goodness o[ fit chi-squarc. ln multivariatc analysis.only the obscrvalion that has information on all variablcsincluded in the multivariate equation would bc accountedlbr in the analysis. Hcncc. out of6l3 individuals. only 415$crc includcd in the multivariate analysis.
Srarisrical analyscs were performed bv using StatpackC<,1d.'' and subroutine of the BMDP LR softwareconrputcr package.re
Results
There were 613 sampled subjecrs who were confirmedas diabetic patients. 507c of whom had good glycemiccontrol (Table l). The mean (and standard deviarion) ofage for subjects who had good control of DM were 47.0(1,1.8) years. compared wirh 51.5 (13.8) years for those\{ i'ro had poor conuol (T=3.88. DF=61 l. P=0.0001 ).
There u'as normal age distriburion, hence there was no:l:ri ibr transformation or categorizarion. and the variablerr< u'as used as a continuous one. The dlsrribution of aeerras as follows: median, mean (SD) 49.48.92 (12.8) ),ears.nrode 45 years. standard error 0.48 years. variance 163.E9\ears squares. skewness and kunosis 0.06 and 0.2.
There was no specific difference of means of BMIbettreen good and poor glycemic control patienrs, 28.7(5.4) and 28.3 (5-5), respectively. The prevalence ofol)esrty sas high among the parients of the two groups.39c,t and 349a for good and poor glycemic control patients.respectively. There was. however. no significantdifTerence.
There rvas no specific pattern for mcans of RBS forcach aee eroup of male and female patients rvith gccd andpoor glycemic control There was no significant differencebet\\een means of RBS of male and female parients of eachage group. whether among good or poor glycemic groups.
There was a signiftcant relationship between glycemiccontrol and age (Table l.). and treatmenr modaliries of DM(Table 2). Subjects who had good glycemic control of DMwere younger and following a diet regimen, while thosewho had poor glycemic control were older and on insulintrcatment.
IUultiYariate analysis comprising 415 individuals wasconducted to find out the factors that can potentiallvinfluence or are associated wirh the control of DM. and-15 SrZ rvcrc found to have good glycemic control. Thcinl:ial model ircluded the follou'ing factors; agc. gender.BMl. region. placc ol rcsidence. urban vs rural. durationof DN'I. and trcatment modalities of DM. Thc treatmentmodality of DM was the only lcctor which had srgnificanrassociation with glycemic control. Compared to patients onthe diet rcgimen, those on insulin and oral agent treatmentwerc at 1647r and 657. more nsk o[ having poor glycemrccontrol. respectively (Table 3).
CLYCEMIC CONTROL OII DIAIJETIC PATIENTS
T^Br-r I Co,'tftri$ ttlo,,ornt hn..u,t t hlsi.tt dah t,l snot anttpoo. sl,'.n <o ftnldiul'uit l,otit, s
G(xi currrol -lrnrup Poor conlft,l gn,up{mcan1sDr (nrcanlsD) P-vahc
AEc ()'c.rxi)BMIPre!alencc otobcsir]
-'t(N51.5 ( l:1.8) <o.(firlItt I (5 -5) 0.:r.r
71.* 0_ 19
:ltI).17 0 t t-l s,26.7 (5 J)
79.n
'Numbi-.r of recordr u ith availablc dfll
T^Btt- 2. Conpa.ison oI lifi}rc t luctot' \'hich c a[fcct sbc?Dti.
Clyc.mic conuol
Good control group Poor conlrol groupno ( ) no. (+) I. dF*
Rcgion
NonhSoudrCcnrralEast
Resid€nc)UrbanRural
Sex
MaleFcmal.
Treatmcntmodaliircs
lnsulinOral agcnrDicr
90 (52.3)21 110.',l)1-7 6l.O)55 (46.6)
93 (56.1t
lll (50.6)96 i50 0)
158 (49,1)l5t5l5)
23 (29.r)I l3 (42.8)112 (61.7)
6.2482 (47.?)35 (59,3)5l (53.0)63 (53 4)7l (43.31
0.0220E (49.a,
(50 0)
0.29r62 (50.6)I42 (48.5)
10.77
56 (70.9)r5l (57.2)% (35.8)
2 0.0(x)
018
*Chi-squared: "degree of frcedom
Discussion
This is an epidemiological population-based studyrvhich reflects the partern and factors which can potentially-affect glycemic control of Saudi diabetic patients at thenational leve!. Several obsen'ations can be made withrespect to the glycernic control: the high rate of parientswith poor glycenlic control. which amounts to 507c of thestudy diabetic population. is rather an alarnring rate whichprobably reflects the inadeguacy of services provided.including education. and lack of insight into theimportance of eood glvcemic control. whether from thephysicians. patients or both. lnsulin-rreared diabeticpirticnrs amounl ro l3?. comparcd rvith 43% ar,d 44cl tororal agents and diel. respectivell, ln spite of having a
significantly higlrcr ratc o[ insulin users among the poorglycenlic control group whcn compared rvith soodglycemic control diabetic patients (719i vs. 29clo). the rateof insulin users u'as lower than that of oral agents arnongpaticnls \.\,ith poor glycerric conrrol (187. vs. 507r). Poorglycemic diabcrrc patients were significantly oldcr thangood glycemic control diabetic patients.
Mukiple logistic regression analysis has shown thaitreatment modalities arc the only significanl factors whrchcan be associared with <legree of glycemic control. wherc
,\nnuk t'[ Soudi Lr.licttt. l'ol 13. No 2, l94t lll
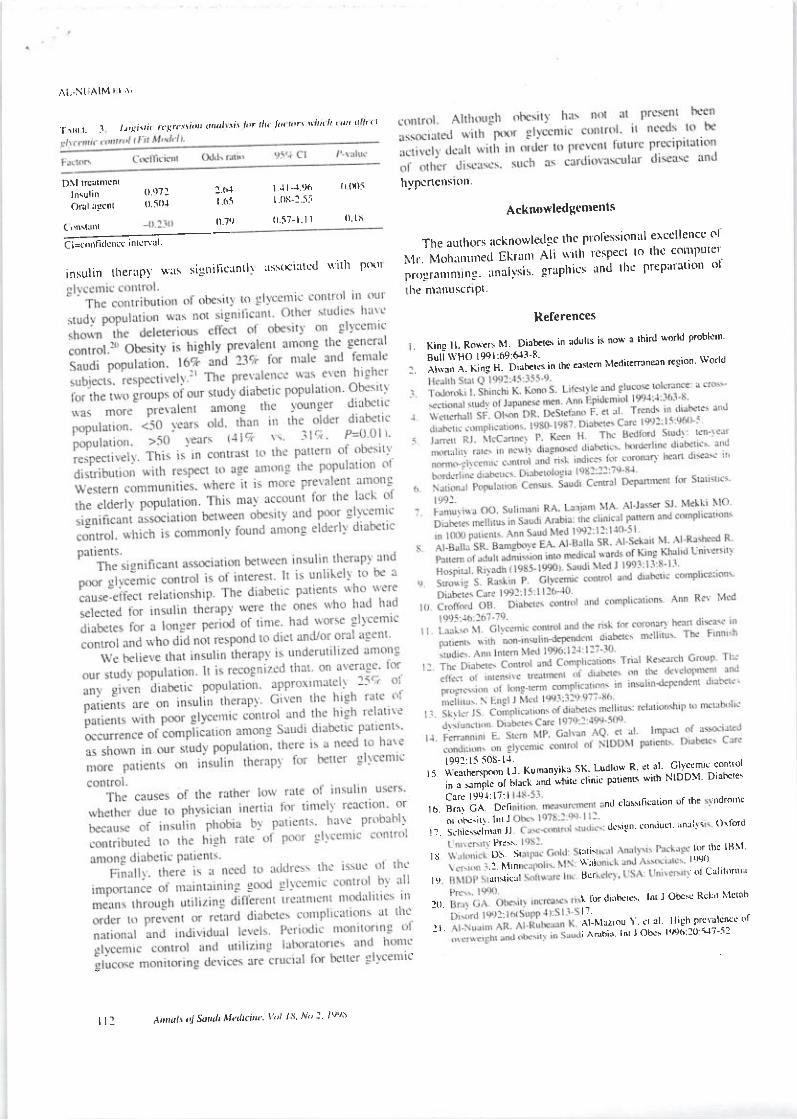
't\r'lI. :l /r,!n,i(,1sr(rln'ri'xdl\ritl'rIl( ttrkt\\'lt h tt trtt
r\t.-Nt iAlM I I \i
D\l rrcurnrcnr I .l t--r.96 {r (x)5 hypcncnston.ln\ulin (l.t)7' l'(iil';1.", 0 soj r'(ri I oli-l'-ss
Acknowledgcnrents0-79 (l-57 l.ll 0 lr
(,'n\lx'rl
E-i =r',,rr fi acucc ; n rcn I tci=confidcncc;nrcn'rl' The authQrs acknowledge thc Ptolessional erccllencc ol
insurin the*,p) $xr, sisnirrcuntr\ nssocirted *ith p*rt ll-Xllll"*llill tlt}lll''"'i5'iLJ'n'li""HH':thc mirnuscrlPt
References
' Kin! H' Ro'teh ltt' Diabct6 in adulLs is no\x r lhird u'orld problcrn'
B'rll\\ HO lgql:6q:Sl'8 - '
't"-"; 'l'*iil;:''o;Lrcs in *r ca*rcm tulcaircrrrnern region world
t0q1.li 50S- ll.
'' tJ]".t,'"]-i1,]., l Kumanvil'r sK Ludlos R' er 31. olvccmic coitrol
"i";li"
Itn"i;;'*t'i'" ai^.. pitrenrs wirh h-lDD:u Di'rhcre\
CrrL I9' I I?: I
't 'lli 3i ij"i nr crirs{ncation or lhe tdronlc
or oe..'rrr ' lnt I,r. t'.i'iL*",i"', d'{!n conducr' rnrr}\ o\rord
'' ol s' lili: ror rhc lrl\l'ii, ",
\\ xl r(,er)
'' '""i"i Bcr oi Cuiilomin
l0 I tor diuhLrcs l^r J Ob'st Rclrr i\'lcrrb
ll'It' Al'Nlurou \" cr al' llith prcY'rlcnct of
i Aahix' lnr 'l Obcs lt,l96r20 irl_52
l A,t,tlll! 4 Soutli tttdt.i'k" li]/ /s Nr) : /t)r/r
Related Documents











