The Vascular The Vascular Lab and the Lab and the Angiographic Angiographic Assessment Assessment of PAD of PAD John C. Lantis II, MD John C. Lantis II, MD Assistant Professor of Assistant Professor of Surgery – Columbia Surgery – Columbia Director of Clinical Director of Clinical Research Research St Lukes-Roosevelt St Lukes-Roosevelt Hospital Hospital

The Vascular Lab and the Angiographic Assessment of PAD The Vascular Lab and the Angiographic Assessment of PAD John C. Lantis II, MD John C. Lantis II,
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The Vascular The Vascular Lab and the Lab and the Angiographic Angiographic Assessment Assessment of PADof PAD
John C. Lantis II, MDJohn C. Lantis II, MD Assistant Professor of Assistant Professor of
Surgery – ColumbiaSurgery – Columbia Director of Clinical Director of Clinical
ResearchResearch St Lukes-Roosevelt St Lukes-Roosevelt
HospitalHospital
The QuestionsThe Questions
Does the patient have enough blood Does the patient have enough blood flow to heal their wound / or the flow to heal their wound / or the intervention ?intervention ?
Does the patient have PAD, and Does the patient have PAD, and should I be helping them to find should I be helping them to find coordinated care ?coordinated care ?
Is the patients circulation Is the patients circulation compromised to the point that I am compromised to the point that I am highly concerned about tissue loss ?highly concerned about tissue loss ?

The Answers!The Answers! (Obviously) A good physical exam(Obviously) A good physical exam Physiologic testingPhysiologic testing
• Ankle brachial indexAnkle brachial index• Pulse volume recordingPulse volume recording• Duplex/MRI – NOVADuplex/MRI – NOVA• TCPO2 (Transcutaneous Oxygen Tension)TCPO2 (Transcutaneous Oxygen Tension)
Anatomic testingAnatomic testing• DuplexDuplex• MRAMRA• AngiogramAngiogram• CTACTA

The Ankle Brachial IndexThe Ankle Brachial Index
Measurement of Measurement of segmental leg segmental leg pressure compared to pressure compared to the highest brachial the highest brachial artery pressureartery pressure• Can be done at the Can be done at the
bedsidebedside• Requires little Requires little
equipmentequipment• Helps determine level Helps determine level
of diseaseof disease

The ankle brachial IndexThe ankle brachial Index Prognostic capabilitiesPrognostic capabilities
• Forefoot amputations are likely to heal, if the ankle pressure is Forefoot amputations are likely to heal, if the ankle pressure is > 70 mmHg, or if the ABI > 0.45> 70 mmHg, or if the ABI > 0.45
• Toe amputations are likely to heal with ankle pressures of > 35 Toe amputations are likely to heal with ankle pressures of > 35 mmHg or toe pressures > 55 mmHg mmHg or toe pressures > 55 mmHg
LimitationsLimitations• Ankle pressures can be artificially inflated in patients with Ankle pressures can be artificially inflated in patients with
diabetes mellitus and ESRDdiabetes mellitus and ESRD• Toe pressures are therefore relied uponToe pressures are therefore relied upon
Pressure less than 50 mm Hg and a toe-to-arm ratio of less than Pressure less than 50 mm Hg and a toe-to-arm ratio of less than 0.6 is indicative of ischemic arterial disease0.6 is indicative of ischemic arterial disease
Foot lesions usually heal if toe pressures exceed 30 mmHG in non-Foot lesions usually heal if toe pressures exceed 30 mmHG in non-diabetic patients and 55 mmHG in diabetic patientsdiabetic patients and 55 mmHG in diabetic patients
Ipsilateral ankle to toe pressures can be used to assess for Ipsilateral ankle to toe pressures can be used to assess for obstructive pedal vascular disease obstructive pedal vascular disease
• AVG 0.65 in normalsAVG 0.65 in normals• AVG 0.23 in patients with rest pain of tissue lossAVG 0.23 in patients with rest pain of tissue loss
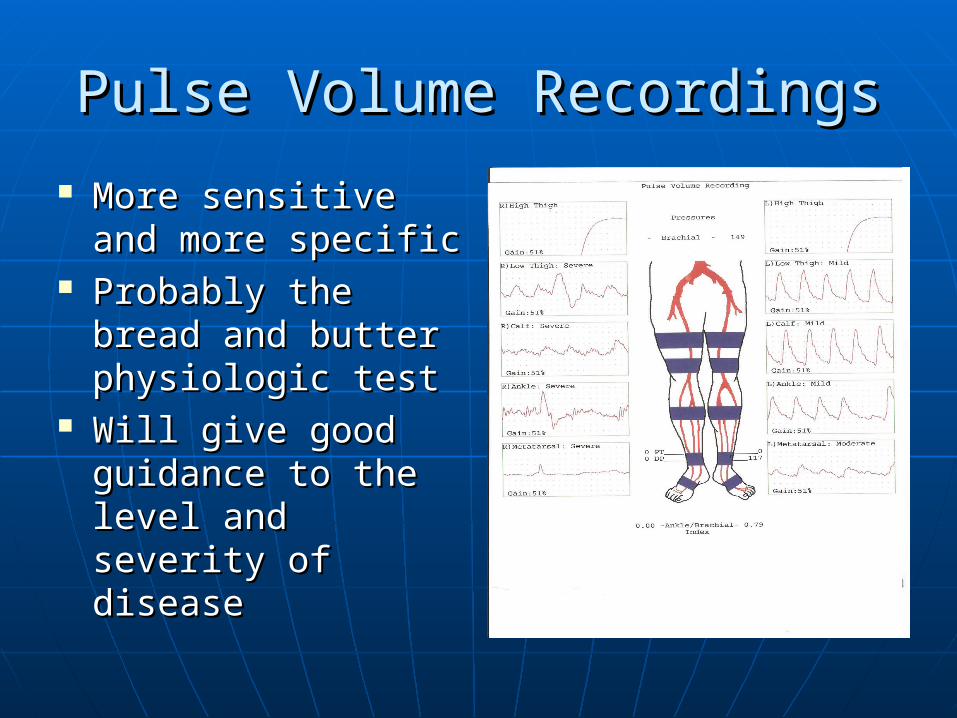
Pulse Volume RecordingsPulse Volume Recordings
More sensitive and More sensitive and more specificmore specific
Probably the bread Probably the bread and butter and butter physiologic testphysiologic test
Will give good Will give good guidance to the guidance to the level and severity level and severity of diseaseof disease
Pulse Volume RecordingsPulse Volume Recordings(with ABI and exercise)(with ABI and exercise)
Treadmill walking test Treadmill walking test • Walking at 1.8 mphWalking at 1.8 mph• 10 % incline10 % incline• Uncovers more subtle lesionsUncovers more subtle lesions
Especially proximal lesions in the iliac and Especially proximal lesions in the iliac and SFA vesselsSFA vessels
A fall in the ABI of 0.2 or a recovery to A fall in the ABI of 0.2 or a recovery to baseline pressure that is greater than 1 baseline pressure that is greater than 1 minute is significantminute is significant
Categories of Chronic Limb Categories of Chronic Limb IschemiaIschemia
Clinical DescriptionClinical Description• Normal AsymptomaticNormal Asymptomatic• Mild ClaudicationMild Claudication
(ABI - < 0.7)(ABI - < 0.7)• Moderate ClaudicationModerate Claudication• Severe claudicationSevere claudication
• Rest PainRest Pain (ABI - < 0.4)(ABI - < 0.4)
• Minor Tissue LossMinor Tissue Loss
• Major Tissue LossMajor Tissue Loss
Pressure CriteriaPressure Criteria• Normal Treadmill testNormal Treadmill test• Completes test, ankle pressure Completes test, ankle pressure
drops > 20 mmHg, absolute ankle drops > 20 mmHg, absolute ankle pressure > 50 mmHgpressure > 50 mmHg
• Between mild and severeBetween mild and severe
• Cannot complete treadmill test Cannot complete treadmill test and ankle pressure after exercise and ankle pressure after exercise < 50 mm Hg< 50 mm Hg
• Resting ankle pressure < 60 Resting ankle pressure < 60 mmHG or toe pressure < 40 mmHG or toe pressure < 40 mmHGmmHG
• Resting ankle pressure less than Resting ankle pressure less than 40 mmHg or toe pressure less 40 mmHg or toe pressure less than 30 mmHgthan 30 mmHg
• Same as minorSame as minor

Duplex UltrasoundDuplex Ultrasound(Combination of B mode imaging and (Combination of B mode imaging and
doppler velocity criteria)doppler velocity criteria) Doppler waveform Doppler waveform
analysis of the analysis of the femoral, popliteal and femoral, popliteal and tibial vessels can be tibial vessels can be carried outcarried out
Waveforms are Waveforms are evaluated similarly to evaluated similarly to the PVR tracingsthe PVR tracings
More accurate at More accurate at localizing disease than localizing disease than PVRsPVRs
Very labor intensiveVery labor intensive

Transcutaneous Partial pressure of Transcutaneous Partial pressure of OxygenOxygen
Transcutaneous oxygen (tcPOTranscutaneous oxygen (tcPO2)2)
• Reflects the metabolic state of the Reflects the metabolic state of the target tissuetarget tissue
• Best for severe ischemiaBest for severe ischemia• Heated Clark electrode (very tech Heated Clark electrode (very tech
dependent, hard to reproduce)dependent, hard to reproduce)• < 20 mmHg – healing failure< 20 mmHg – healing failure• > 40 mmHg – healing success> 40 mmHg – healing success• Elevate limb > 30Elevate limb > 3000 /3 min – drop > 15 /3 min – drop > 15
mmHg – healing failuremmHg – healing failure

Other Methods of Assessing Blood Other Methods of Assessing Blood Supply Supply
Laser Doppler VelocimetryLaser Doppler Velocimetry• A relative index of cutaneous blood flowA relative index of cutaneous blood flow• With ischemia pulse waves are attenuated, mean With ischemia pulse waves are attenuated, mean
velocities are decreasedvelocities are decreased• If mean velocity is > 40 millivolts (mV) and pulse wave If mean velocity is > 40 millivolts (mV) and pulse wave
amplitude is > 4 mV – associated with healingamplitude is > 4 mV – associated with healing NOVANOVA
• Non-invasive Optimal Vessel Analysis (NOVA) a non-Non-invasive Optimal Vessel Analysis (NOVA) a non-invasive Magnetic Resonance Imaging (MRI) techniqueinvasive Magnetic Resonance Imaging (MRI) technique
• NOVA provides actual milliliter/minute blood flow data NOVA provides actual milliliter/minute blood flow data using specialized software analysis of standard MRI using specialized software analysis of standard MRI phase contrast imaging phase contrast imaging
• InvestigationalInvestigational
Back to the Questions….Back to the Questions….
Does the patient have enough blood flow Does the patient have enough blood flow to heal their wound / or the intervention ? to heal their wound / or the intervention ? NONO
Does the patient have PAD, and should I Does the patient have PAD, and should I be helping them to find coordinated care ? be helping them to find coordinated care ? YESYES
Is the patients circulation compromised to Is the patients circulation compromised to the point that I am highly concerned about the point that I am highly concerned about tissue loss ? YEStissue loss ? YES
Leads to the next two questions…Leads to the next two questions…
Where is the patients lesion?Where is the patients lesion?• Segmental PressuresSegmental Pressures• Segmental PVRsSegmental PVRs• Long leg duplexLong leg duplex
Can I get this patient revascularized?Can I get this patient revascularized?• What type of lesion?What type of lesion?• How many and where?How many and where?

MRAMRA
Non nephrotoxic contrastNon nephrotoxic contrast No arterial punctureNo arterial puncture However, claustrophobia limitedHowever, claustrophobia limited Sensitivity and specificity to level of Sensitivity and specificity to level of
disease 80-85%disease 80-85% Approximately 85 % concordance Approximately 85 % concordance
with Angiographywith Angiography

MRAMRA

AngiographyAngiography
Usually nephrotoxic dyeUsually nephrotoxic dye Arterial punctureArterial puncture Done with sedation (few issues with Done with sedation (few issues with
claustrophobia)claustrophobia) Able to intervene at time of Able to intervene at time of
procedureprocedure With subtraction capabilities With subtraction capabilities
probably able to see post-occluded probably able to see post-occluded vessels as well as MRAvessels as well as MRA

AngiographyAngiography
CT AngiogramCT Angiogram
Approaching MRAs capabilitiesApproaching MRAs capabilities Relatively large nephrotoxic dye loadRelatively large nephrotoxic dye load No arterial punctureNo arterial puncture Minimal claustrophobia issuesMinimal claustrophobia issues Distal vessel resolution still machine Distal vessel resolution still machine
and center dependentand center dependent

CT AngiogramCT Angiogram

A day in the life….A day in the life….
A patient limps in…A patient limps in… No palpable pulse…No palpable pulse… Small amount of Small amount of
tissue losstissue loss ABI/PVRs are ABI/PVRs are
obtainedobtained …….Obtain toe NIFs...Obtain toe NIFs..
Pt went onto heal..Pt went onto heal..

Or more likely…..Or more likely…..
We have flat line We have flat line tracingstracings
Which we follow Which we follow with a anatomic with a anatomic diagnostic ….diagnostic ….
Which leads us to Which leads us to our next our next speakers…speakers…
Related Documents











