The valvular anatomy of the iliac venous system and its clinical implications Paul A. LePage, MD, J. Leone1 Villavicencio, MD, Edward R. Gomez, MD, Michael N. Sheridan, PhD, and Norman M. Rich, MD, Bethesda, Md., and Washington D. C. Clinical and phlebographic evidence exists that correlates the presence of varices of the vulva, posterior thigh, and the pelvic congestion syndrome with insufliciency of the internal iliac venous system (pelvic dumping syndrome). Information in the modem medical literature regarding the valvular anatomy of the internal iliac veins and its tributaries is limited. We dissected 82 iliac venous system specimens in 42 human cadavers (29 men, 13 women) to gain information on the relationship between the disease described and the anatomy of the region. Each specimen contained common, external, and internal iliac veins, including the tributaries of the latter. We recorded the anatomic variations of the internal iliac vein trunk and the location of valves in the complete iliac venous system, including 485 tributaries of the internal iliac veins. Five specimens of internal iliac vein had calcified thrombosis or were extensively involved with pelvic carcinoma and were not suitable for valve study, which left 79 specimens for analysis. The internal iliac vein drained into the external iliac venous system by means of a single trunk in 73% of the specimens and by two well-formed and separated trunks in 27O/6 of the specimens. In one specimen (1.2%) the internal iliac vein drained directly into the inferior vena cava (parallel internal and external iliac veins). One specimen had a well-developed valve in the common iliac vein (1.2%). The external iliac vein had one valve in 26.2% of the specimens. This vein had three times as many valves on the right side as in the left (39.6% vs 14.6%: p = 0.0106). The internal iliac vein had valves present in 10.1% of its main trunks and in 9.1% of the 485 tributaries dissected. This is the first time that well-developed valves have been demonstrated in the internal iliac vein and their location described in a series of human cadaver dissections. The scarcity of valves in the pelvic veins, however, led us to consider that varicose veins in the vulva or elsewhere develop not only because of valvular insufficiency but also because of genetic structural venous wall anomalies as well as hormonal and hemodynamic factors present during pregnancy. (J VAX SURG 1991;14: 678-83.) The importance of valves in the hemodynamics of the venous circulation and in the pathophysiology of varicose veins has been long recognized. The current textbooks of descriptive and topographic anatomy From the Departments of Surgery and Anatomy, Uniformed Services University of the Health Sciences, Bethesda, and the General and Vascular Surgery Services, Walter Reed Army Medical Center, Washington, D.C. The opinions or assertions contained herin are the private ones of the authors and are not to be construed as official or as reflecting the views of the Department of Defense, Department of the Army, or the Uniformed Services University of the Health Sciences. Presented at the Second Annual Meeting of The American Venous Forum, Coronado, Calif., Feb. 2-i-23, 1990. Reprint requests: J. Leone1 Villavicencio, MD, FACS, Professor of Surgery, Department of Surgery, Uniformed Services Univer- sitv of the Health Sciences. 4301 Tones Bridge Rd.. Bethesda. Mi) 20814-4799. ’ ’ 24/l/31717 678 and related publications offer a detailed description of the location and distribution of valves in the veins of practically every anatomic territory with exception of the internal iliac vein.‘-6 Because of its recognized clinical implications, the anatomy and valve distribu- tion in the veins of the lower extremities and its possible relation with the development of varicose veins have been the subject of important reports published during the decades of the 1940s and 1950~.~-~ We became interested in the valvular system of the internal iliac vein through the observation of vulvar and gluteal varices and the analysis of retro- grade venograms performed on patients with vulvar varices and symptoms of pelvic congestion syn- drome. We found that information in the medical literature on the valvular system of the internal iliac vein and its tributaries was very scarce. A thorough search of the literature on the subject was carried out,

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
The valvular anatomy of the iliac venous system and its clinical implications Paul A. LePage, MD, J. Leone1 Villavicencio, MD, Edward R. Gomez, MD, Michael N. Sheridan, PhD, and Norman M. Rich, MD, Bethesda, Md., and Washington D. C.
Clinical and phlebographic evidence exists that correlates the presence of varices of the vulva, posterior thigh, and the pelvic congestion syndrome with insufliciency of the internal iliac venous system (pelvic dumping syndrome). Information in the modem medical literature regarding the valvular anatomy of the internal iliac veins and its tributaries is limited. We dissected 82 iliac venous system specimens in 42 human cadavers (29 men, 13 women) to gain information on the relationship between the disease described and the anatomy of the region. Each specimen contained common, external, and internal iliac veins, including the tributaries of the latter. We recorded the anatomic variations of the internal iliac vein trunk and the location of valves in the complete iliac venous system, including 485 tributaries of the internal iliac veins. Five specimens of internal iliac vein had calcified thrombosis or were extensively involved with pelvic carcinoma and were not suitable for valve study, which left 79 specimens for analysis. The internal iliac vein drained into the external iliac venous system by means of a single trunk in 73% of the specimens and by two well-formed and separated trunks in 27O/6 of the specimens. In one specimen (1.2%) the internal iliac vein drained directly into the inferior vena cava (parallel internal and external iliac veins). One specimen had a well-developed valve in the common iliac vein (1.2%). The external iliac vein had one valve in 26.2% of the specimens. This vein had three times as many valves on the right side as in the left (39.6% vs 14.6%: p = 0.0106). The internal iliac vein had valves present in 10.1% of its main trunks and in 9.1% of the 485 tributaries dissected. This is the first time that well-developed valves have been demonstrated in the internal iliac vein and their location described in a series of human cadaver dissections. The scarcity of valves in the pelvic veins, however, led us to consider that varicose veins in the vulva or elsewhere develop not only because of valvular insufficiency but also because of genetic structural venous wall anomalies as well as hormonal and hemodynamic factors present during pregnancy. (J VAX SURG 1991;14: 678-83.)
The importance of valves in the hemodynamics of the venous circulation and in the pathophysiology of varicose veins has been long recognized. The current textbooks of descriptive and topographic anatomy
From the Departments of Surgery and Anatomy, Uniformed Services University of the Health Sciences, Bethesda, and the General and Vascular Surgery Services, Walter Reed Army Medical Center, Washington, D.C.
The opinions or assertions contained herin are the private ones of the authors and are not to be construed as official or as reflecting the views of the Department of Defense, Department of the Army, or the Uniformed Services University of the Health Sciences.
Presented at the Second Annual Meeting of The American Venous Forum, Coronado, Calif., Feb. 2-i-23, 1990.
Reprint requests: J. Leone1 Villavicencio, MD, FACS, Professor of Surgery, Department of Surgery, Uniformed Services Univer- sitv of the Health Sciences. 4301 Tones Bridge Rd.. Bethesda. Mi) 20814-4799. ’ ’
24/l/31717
678
and related publications offer a detailed description of the location and distribution of valves in the veins of practically every anatomic territory with exception of the internal iliac vein.‘-6 Because of its recognized clinical implications, the anatomy and valve distribu- tion in the veins of the lower extremities and its possible relation with the development of varicose veins have been the subject of important reports published during the decades of the 1940s and 1950~.~-~ We became interested in the valvular system of the internal iliac vein through the observation of vulvar and gluteal varices and the analysis of retro- grade venograms performed on patients with vulvar varices and symptoms of pelvic congestion syn- drome. We found that information in the medical literature on the valvular system of the internal iliac vein and its tributaries was very scarce. A thorough search of the literature on the subject was carried out,
Volume 14 Number 5 November 1991 The ~alvulwanatumy ofthe iliacvenoussystem 679
beginning with the classic works of anatomists of the sixteenth century, when valves were first described, and extending to the modern anatomy textbooks and current publications. Our search revealed either no description of valves in the internal iliac vein or reports of absence of valves in its trunk.10-‘5
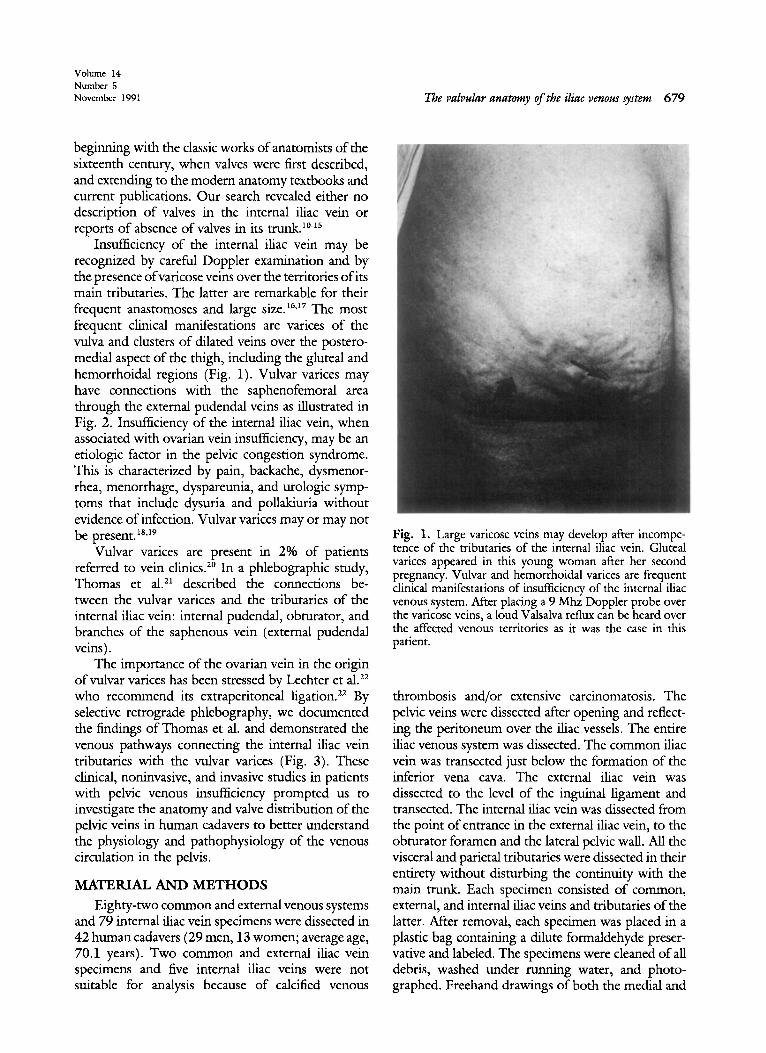
Insufliciency of the internal iliac vein may be recognized by careful Doppler examination and by the presence ofvaricose veins over the territories of its main tributaries. The latter are remarkable for their frequent anastomoses and large size.‘6~17 The most frequent clinical manifestations are varices of the vulva and clusters of dilated veins over the postero- medial aspect of the thigh, including the gluteal and hemorrhoidal regions (Fig. 1). Vulvar varices may have connections with the saphenofemoral area through the external pudendal veins as illustrated in Fig. 2. Insufliciency of the internal iliac vein, when associated with ovarian vein insufficiency, may be an etiologic factor in the pelvic congestion syndrome. This is characterized by pain, backache, dysmenor- rhea, menorrhage, dyspareunia, and urologic symp- toms that include dysuria and pollakiuria without evidence of infection. Vulvar varices may or may not be present.“,19
Vulvar varices are present in 2% of patients referred to vein clinics.2o In a phlebographic study, Thomas et a121 described the connections be- tween the vulvar varices and the tributaries of the internal iliac vein: internal pudendal, obturator, .and branches of the saphenous vein (external pudendal veins).
The importance of the ovarian vein in the origin of vulvar vat-ices has been stressed by Lechter et al.22 who recommend its extraperitoneal ligation.22 By selective retrograde phlebography, we documented the findings of Thomas et al. and demonstrated the venous pathways connecting the internal iliac vein tributaries with the vulvar varices (Fig. 3). These clinical, noninvasive, and invasive studies in patients with pelvic venous insufliciency prompted us to investigate the anatomy and valve distribution of the pelvic veins in human cadavers to better understand the physiology and pathophysiology of the venous circulation in the pelvis.
MATERLAL AND METHODS
Eighty-two common and external venous systems and 79 internal iliac vein specimens were dissected in 42 human cadavers (29 men, 13 women; average age, 70.1 years). Two common and external iliac vein specimens and five internal iliac veins were not suitable for analysis because of calcified venous
Fig. 1. Large varicose veins may develop after incompe- tence of the tributaries of the internal iliac vein. Gluteal vat-ices appeared in this young woman after her second pregnancy. Vulvar and hemorrhoidal varices are frequent clinical manifestations of insufficiency of the internal iliac venous system. After placing a 9 Mhz Doppler probe over the varicose veins, a loud Valsalva reflux can be heard over the affected venous territories as it was the case in this patient.
thrombosis and/or extensive carcinomatosis. The pelvic veins were dissected after opening and reflect- ing the peritoneum over the iliac vessels. The entire iliac venous system was dissected. The common iliac vein was transected just below the formation of the inferior vena cava. The external iliac vein was dissected to the level of the inguinal ligament and transected. The internal iliac vein was dissected from the point of entrance in the external iliac vein, to the obturator foramen and the lateral pelvic wall. All the visceral and parietal tributaries were dissected in their entirety without disturbing the continuity with the main trunk. Each specimen consisted of common, external, and internal iliac veins and tributaries of the latter. After removal, each specimen was placed in a plastic bag containing a dilute formaldehyde preser- vative and labeled. The specimens were cleaned of all debris, washed under running water, and photo- graphed. Freehand drawings of both the medial and
680 LePage et al.
Journal of VASCULAR
SURGERY
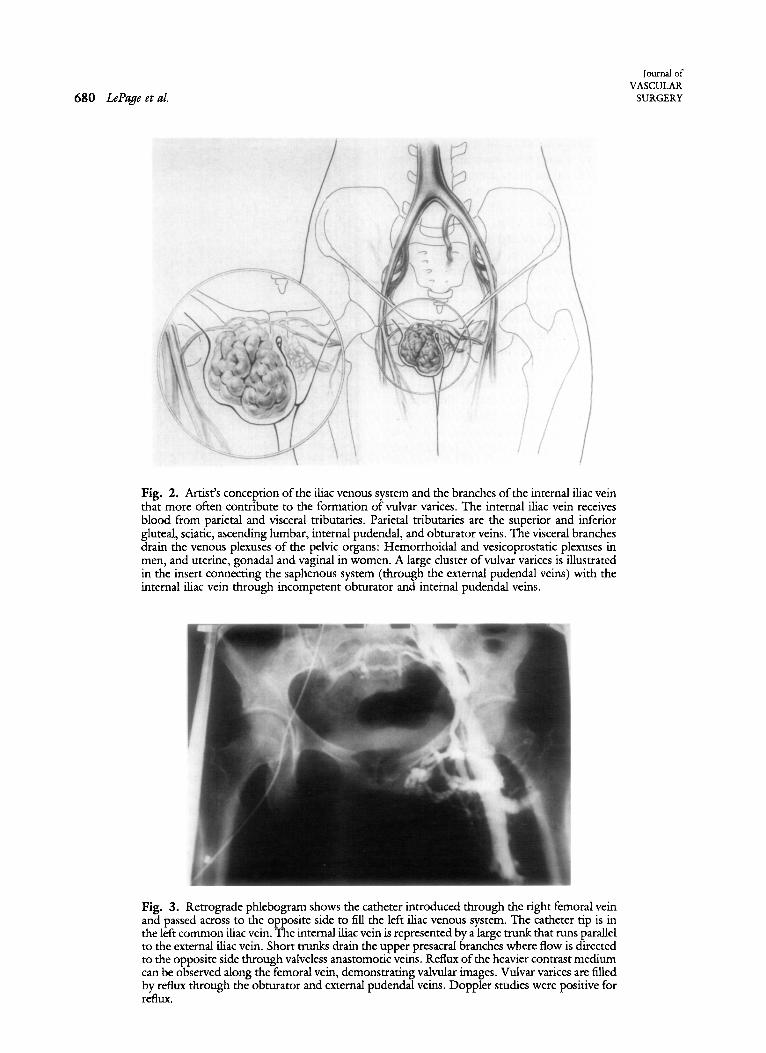
Fig. 2. Artist’s conception of the iliac venous system and the branches of the internal iliac vein that more often contribute to the formation of vulvar vat-ices. The internal iliac vein receives blood from parietal and visceral tributaries. Parietal tributaries are the superior and inferior gluteal, sciatic, ascending lumbar, internal pudendal, and obturator veins. The visceral branches drain the venous plexuses of the pelvic organs: Hemorrhoidal and vesicoprostatic plexuses in men, and uterine, gonadal and vaginal in women. A large cluster of vulvar varices is illustrated in the insert connecting the saphenous system (through the external pudendal veins) with the internal iliac vein through incompetent obturator and internal pudendal veins.
Fig. 3. Retrograde phlebogram shows the catheter introduced through the right femoral vein and passed across to the opposite side to fill the left iliac venous system. The catheter tip is in the left common iliac vein. The internal iliac vein is represented by a large trunk that runs parallel to the external iliac vein. Short trunks dram the upper presacral branches where flow is directed to the opposite side through valveless anastomotic veins. Reflux of the heavier contrast medium can be observed along the femoral vein, demonstrating valvular images. Vulvar varices are filled by reflux through the obturator and external pudendal veins. Doppler studies were positive for refhrx.
Volllmr 14 Number 5 November 1991 The valvular anatomy of the iliac vmous ytem 681
lateral aspects of each specimen were made. The veins were carefully opened longitudinally, thrombus and dry blood was gently removed, and the presence, number, and location of valves was recorded. Statis- tical analysis of the recorded data was performed by use of Fisher’s exact test.
RESULTS Single and double internal iliac vein trunks
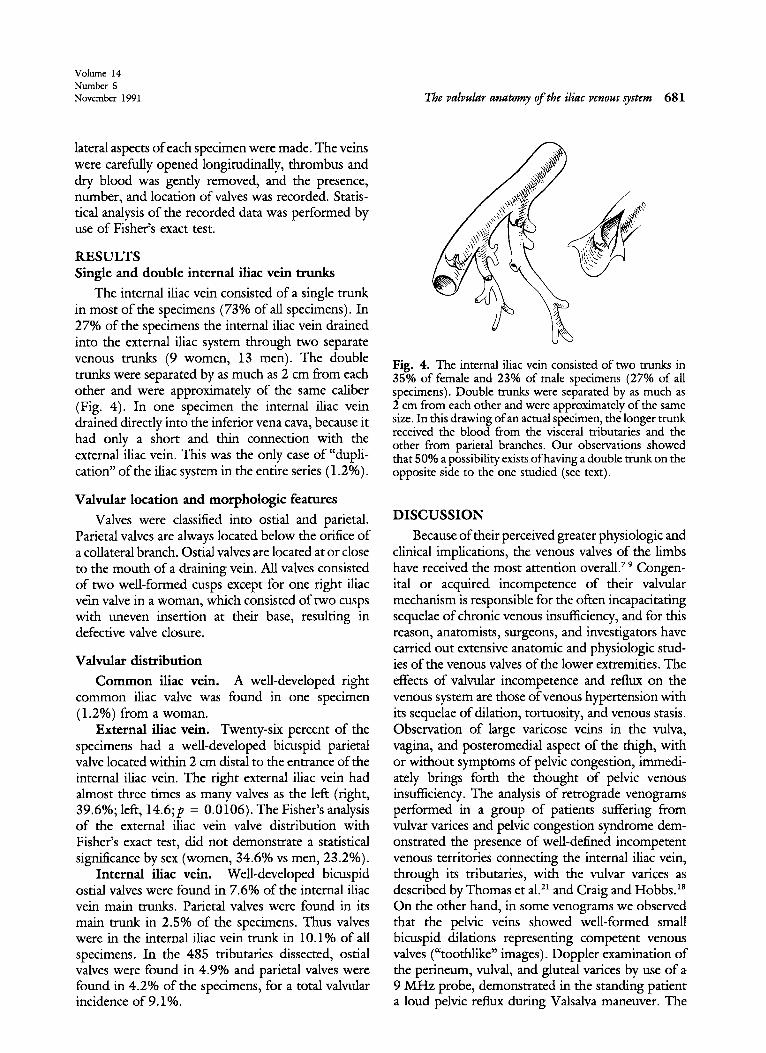
The internal iliac vein consisted of a single trunk in most of the specimens (73% of all specimens). In 27% of the specimens the internal iliac vein drained into the external iliac system through two separate venous trunks (9 women, 13 men). The double trunks were separated by as much as 2 cm from each other and were approximately of the same caliber (Fig. 4). In one specimen the internal iliac vein drained directly into the inferior vena cava, because it had only a short and thin connection with the external iliac vein. This was the only case of “dupli- cation” of the iliac system in the entire series (1.2%).
Valvular location and morphologic features
Valves were classified into ostial and parietal. Parietal valves are always located below the orifice of a collateral branch. Ostial valves are located at or close to the mouth of a draining vein. All valves consisted of two well-formed cusps except for one right iliac ve?n valve in a woman, which consisted of two cusps with uneven insertion at their base, resulting in defective valve closure.
Valvular distribution
Common iliac vein. A well-developed right common iliac valve was found in one specimen (1.2%) from a woman.
External iliac vein. Twenty-six percent of the specimens had a well-developed bicuspid parietal valve located within 2 cm distal to the entrance of the internal iliac vein. The right external iliac vein had almost three times as many valves as the left (right, 39.6%; left, 14.6;~ = 0.0106). The Fisher’s analysis of the external iliac vein valve distribution with Fisher’s exact test, did not demonstrate a statistical significance by sex (women, 34.6% vs men, 23.2%).
Internal iliac vein. Well-developed bicuspid ostial valves were found in 7.6% of the internal iliac vein main trunks. Parietal valves were found in its main trunk in 2.5% of the specimens. Thus valves were in the internal iliac vein trunk in 10.1% of all specimens. In the 485 tributaries dissected, ostial valves were found in 4.9% and parietal valves were found in 4.2% of the specimens, for a total valvular incidence of 9.19/o.
Fig. 4. The internal iliac vein consisted of two trunks in 35% of female and 23% of male specimens (27% of all specimens). Double trunks were separated by as much as 2 cm from each other and were approximately of the same size. In this drawing of an actual specimen, the longer trunk received the blood from the visceral tributaries and the other from parietal branches. Our observations showed that 50% a possibility exists of having a double trunk on the opposite side to the one studied (see text).
DISCUSSION
Because of their perceived greater physiologic and clinical implications, the venous valves of the limbs have received the most attention overall.7-9 Gmgen- ital or acquired incompetence of their valvular mechanism is responsible for the often incapacitating sequelae of chronic venous insufficiency, and for this reason, anatomists, surgeons, and investigators have carried out extensive anatomic and physiologic stud- ies of the venous valves of the lower extremities. The effects of valvular incompetence and reflux on the venous system are those of venous hypertension with its sequelae of dilation, tortuosity, and venous stasis. Observation of large varicose veins in the vulva, vagina, and posteromedial aspect of the thigh, with or without symptoms of pelvic congestion, immedi- ately brings forth the thought of pelvic venous insufficiency. The analysis of retrograde venograms performed in a group of patients suffering from vulvar varices and pelvic congestion syndrome dem- onstrated the presence of well-defined incompetent venous territories connecting the internal iliac vein, through its tributaries, with the vulvar varices as described by Thomas et aLzl and Craig and Hobbs.ls On the other hand, in some venograms we observed that the pelvic veins showed well-formed small bicuspid dilations representing competent venous valves (“toothlike” images). Doppler examination of the perineum, vulval, and gluteal varices by use of a 9 MHz probe, demonstrated in the standing patient a loud pelvic reflux during Valsalva maneuver. The

682 LePge et al.
Journal of VASCULAR
SURGERY
anatomic areas of Doppler reflux correlated well with that occurs during pregnancy. In these cases the the territories of radiologic reflux. These observations femoral vein dilates to more than twice its normal stimulated our interest in the study of the anatomy size. Under these conditions the valve cusps separate and distribution of valves in the pelvic veins. and become incompetent.23
Little attention has been paid to the valvular system of the internal iliac vein. The internal iliac or hypogastric vein, as described in modern texts of anatomy, consists of a single large trunk draining into the external iliac vein to form the common iliac vein (Fig. 2). It receives the blood from parietal and visceral tributaries. The parietal tributaries are supe- rior and inferior gluteal, sciatic, sacral, ascending lumbar, internal pudendal, and obturator veins. The visceral tributaries carry blood from the pelvic organs: hemorrhoidal and vesicoprostatic plexuses in men, and the uterine, gonadal, and vesicovaginal plexus in women. These veins are extensively inter- connected through a system of valveless veins capable of bidirectional blood flow.
The anatomic finding that the internal iliac venous system consists of two completely separate trunks in 27% of all specimens, is relevant for the radiologist trying to catheterize selectively the inter- nal iliac vein trunk, since both trunks may need to be visualized to elucidate the pathways of venous reflux. For the vascular surgeon trying to interrupt pelvic venous reflux through an extraperitoneal approach,X-26 it is important to recognize that more than one quarter of the patients may have a double internal iliac venous trunk.
Our cadaver dissections clearly demonstrated the presence of well-developed valves in the internal iliac vein and its tributaries. The observation of rich anastomotic plexuses among the different visceral components of the pelvis, and the relative scarcity of valves in the pelvic venous system, have contributed to the understanding or the pathophysiology of reflux of the pelvic veins into the gluteal, vulvar, and lower extremity venous systems (pelvic dumping syndrome). However, it poses the following impor- tant question: if 90% of the individuals do not have valves in the internal iliac system, why do we not see more women with vulvar varices and symptoms of pelvic venous insufficiency? Twenty percent of preg- nant women will develop varicose veins, but only one out of three will have vulvar varices.” These obser- vations lead us to consider that varicose veins may develop not only as a result of valvular incompetence, but also as a result of genetic anomalies and disturbances in the collagen structure of the venous wall. Aside from the genetic, hormonal and valvular disorders, important anatomic and physiologic fac- tors occur in the pregnant woman, which contribute to produce hypertension in the pelvic veins. Com- pression of the left common iliac vein by the right common iliac artery may be significant in nearly 20% of the patients and may lead to venous hypertension in the distal territories. Another factor is the direct compression of the pelvic veins and specifically the inferior vena cava by the pregnant uterus. This compression against the vertebral column is aggra- vated by the lumbar lordosis in pregnancy and the dextrorotation of the uterus. An important physio- logic consideration is the large increase in pelvic flow
The presence of well-developed valves in the common and external iliac veins must be taken into consideration in the interpretation of a retrograde venogram, since the presence of parietal valves in the vein trunks produce images of interrupted flow that may resemble venous thrombosis, especially in the area of the left common iliac vein where the right common iliac artery may compress the vein. A competent common iliac or external iliac venous valve produce an image of complete flow interrup- tion during the retrograde injection of contrast material. In these cases, the observation of the bicuspid dilation of the valve sinuses may explain the apparent obstruction.
The parietal valve encountered in the external iliac vein in approximately one third of the specimens is worth discussing. We have described that the right external iliac has almost three times as many valves as the left (right, 39.6% vs left, 14.6%). The scarcity of valves in the left external iliac leaves the saphenofem- oral area of a relatively high number of patients without protection against the high thoracoabdom- inal pressures. These findings may offer objective support to the reported higher incidence of varicose veins in the left lower extremity. On the other hand, it is important to keep in mind the absence or presence of the external iliac valve during the interpretation of Doppler reflux at the saphenofem- oral junction. If the Doppler probe is placed over the common femoral vein, we will hear a loud reflux during Valsalva maneuver if there is no external iliac valve. In this case we could make an erroneous diagnosis of saphenofemoral incompetence if we fail to place the Doppler probe directly over the saphe- nous vein distal to the junction. On the other hand, if there is an iliac valve present, and we place the Doppler probe over the greater saphenous vein, we will not hear reflux even though there might be an

VolLIme 14 Number 5 November 1991
incompetent saphenofemoral junction. These pitfalls in the examination of the saphenofemoral junction will be the subject of a separate communication.
The internal iliac vein and its numerous visceral and parietal tributaries serve as an important collat- eral pathway in cases of obstruction of the ilio caval segment. In these cases blood will flow after the hemodynamic laws, from the territory of high pressure to the territories of lower pressure. The relative scarcity of valves encountered in the pelvic plexuses will thus be beneficial and contribute to the development of collateral circulation, since blood could flow in practically any direction.
We thank Mr. George S. Holborow and Mr. John Brunette, Curator and Assistant Curator, respectively of the Department of Anatomy at the Uniformed Services Uni- versity of the Health Sciences, and Drs. William Holbrook, Anton Sidawy, Joseph Giordano, Charles G. Rob, Charles Hufnagel, and Adel Elham for their valuable assistance in the Anatomy Laboratory.
REFERENCES 1. Toldt C. An atlas of human anatomy, 2nd ed, vol II. New
York: The MacMillan Co, 1944:672-7. 2. Anson BJ. An atlas of human anatomy, Philadelphia: WB
Saunders Co, 1950:379-99. 3. Pemkopf E. Atlas of topographical and applied human
anatomy, vol II. In: Femer H. ed. Philadelphia: WB Saunders Co, 1963.
4. Sobotta. Atlas of human anatomy, vol 2. In: Hild WJ, ed. Blood vessels of the pelvic viscera in the female, 10th Engl ed. Baltimore, Munich: Urban and Schwarzenberg, 1983:204- 22.
5. Testut R, Jacob 0. Pelvic veins. In: Tratado de Anatomia Topografica, vol II, 8a ed, chap 6. Barcelona: Salvat, 1977:387-g.
6. Laufman H. Surgical anatomy of the venous system. In: Silvergirl’s Surgery: the veins. Austin, Tex: Silvergirl, 1986: 14-24.
7. Powell T, Lynn RB. The valves of the external iliac, femoral, and upper third of the popliteal vein. Surg Gynecol Obstet 1951;92:453-5.
8. Eger SA, Casper SL. Etiology of varicose veins from an anatomical aspect, based on a dissection of thirty-eight adult cadavers. JAMA 1943;123:148-9.
9. Basmajian JV. The distribution of valves in the femoral,
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
The vahlar anatomy of the iliac venous ~stem 683
external iliac, and common iliac veins and their relationship to varicose veins. Surg Gynecol Obstet 1952;95:537-42. Brown A. Old masterpieces in surgery. Privately printed, Omaha, 1928. De 1’Aulnoit AH. Recherches Anatomiques et Physiologiques sur les Valvules des Veines [thesis]. Paris, 1854. Aquapendente FA. De Venarum Ostiolis (1603), translation by KJ Franklin, Springfield, Ill: CC Thomas, 1933. Sappey PhC. Traite d’Anatomie Descriptive, first vol. Paris: V Masson, 1850:572. Dodd H, Cockert FB. Surgical anatomy of the veins of the lower limbs. In: The pathology and surgery of the veins of the lower limb. London: Churchill-Livingstone Ltd, 1976:47. Gray H. Anatomy, descriptive and surgical. London: John W. Parker & Son, 1858. Clemente CD. Gray’s anatomy, thirtieth American ed. Philadelphia: Lea and Febiger, 1985:839-61. Woodburne RT. Essentials of human anatomy, seventh ed. New York: Oxford University Press, Inc, 1983:507. Craig 0, Hobbs JT. Vulva1 phlebography in the pelvic congestion syndrome. Chin Radio1 1974;25:517-25. Dixon JA, Mitchell WA. Venographic and surgical observa- tions in vulvai varicose veins. Surg Gynecol Obstet 1979; 131:458-464. Dodd H, Payling-Wright H. Vulvai varicose veins in preg- nancy. Br Med (Clin Res) 1959;1:831-2. Thomas ML, Fletcher EWL, Andress MR, Cockett FB. The venous connections of v&al varices. Chin Radio1 1967; 18:313-7. Lechter A, Alvarez A, Lopez G. Pelvic varices and gonadal veins. Phlebology 1987, 2:181-S. Tamvakopoulos SK. Noninvasive estimation of lower limb venous dynamics in pregnant women [Abstract No. 02.31. Proceedings of the VI European American Symposium on Venous Diseases. Washington DC, 1987. Villavicencio JL. Evolution a large p&o (l-8 anos) de1 tratamiento quirurgico de insuficiencia venosa de las extrem- idades inferiores. GISA Publishers, Direction General de Education Militar. Escuela Medico Militar de Mexico. Mexico D/F/, 1968:77-87. Villavicencio JL, et al. Recurrent varicose veins. In: Trout III HH, Giordano JM, DePalrna RG, eds. Reoperative vascular surgery. New York: Marcel Dekker, Inc, 1987:255-302. Gomez ER, Viilavicencio JL, Coffey JA, Rich NM. Patho- genesis and surgical management of varicose veins of the vulva and upper thigh: the internal iliac venous insufficiency syndrome. In: Veith FJ, ed. Current critical problems in vascular surgery. St. Louis: Quality Med Pub& 1990:141-2.
Submitted July 6, 1990; accepted May 1, 1991
Related Documents