Click here to load reader

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

R
Tmr
Ma
b
c
a
ARR2AA
KrTASBEC
C
T
h0
Neuroscience and Biobehavioral Reviews 47 (2014) 592–613
Contents lists available at ScienceDirect
Neuroscience and Biobehavioral Reviews
journa l h om epa ge: www.elsev ier .com/ locate /neubiorev
eview
he use of repetitive transcranial magnetic stimulation forodulating craving and addictive behaviours: A critical literature
eview of efficacy, technical and methodological considerations
. Grall-Bronneca,b,c, A. Sauvageta,c,∗
Addictology and Psychiatry Department, Nantes University Hospital, FranceEA 4275 “Biostatistics, Clinical Research and Subjective Measures in Health Sciences”, University of Nantes, FranceClinical Investigation Unit 18 - BALANCED “BehaviorAL AddictioNs and ComplEx mood Disorders”, University Hospital of Nantes, France
r t i c l e i n f o
rticle history:eceived 20 November 2013eceived in revised form5 September 2014ccepted 15 October 2014vailable online 24 October 2014
eywords:
a b s t r a c t
Objectives: Repetitive transcranial magnetic stimulation (rTMS) is a potential therapeutic intervention forthe treatment of addiction. This critical review aims to summarise the recent developments with respectto the efficacy of rTMS for all types of addiction and related disorders (including eating disorders), andconcentrates on the associated methodological and technical issues.Methods: The bibliographic search consisted of a computerised screening of the Medline and ScienceDirectdatabases up to December 2013. Criteria for inclusion were the target problem was an addiction, a relateddisorder, or craving; the intervention was performed using rTMS; and the study was a clinical trial.
TMSranscranial magnetic stimulationddictionubstance use disorderehavioural addiction
Results: Of the potential 638 articles, 18 met the criteria for inclusion. Most of these (11 of the 18) sup-ported the efficacy of rTMS, especially in the short term. In most cases, the main assessment criterionwas the measurement of craving using a Visual Analogue Scale.Discussion: The results are discussed with respect to the study limitations and, in particular, the manymethodological and technical discrepancies that were identified. Key recommendations are provided.
ating disorderraving
© 2014 The Authors. Published by Elsevier Ltd. This is an open access article under the CC BY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/3.0/).
ontents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5932. Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 595
2.1. Search strategy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5952.2. Eligibility criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5952.3. Study selection. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5952.4. Data extraction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 595
3. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5963.1. Efficacy of rTMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 596
3.1.1. rTMS and nicotine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5963.1.2. rTMS and alcohol . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5963.1.3. rTMS and cocaine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5963.1.4. rTMS and methamphetamine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5963.1.5. rTMS and food . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 596
3.2. rTMS technical procedures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3.2.1. The rTMS device . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3.2.2. Stimulation site and identification of the target site . . . . .3.2.3. General design of the sessions and rTMS parameters . . . .
∗ Corresponding author at: Addictology and Psychiatry Department, Hôpital St Jacquesel.: +33 0240846116; fax: +33 0240846118.
E-mail address: [email protected] (A. Sauvaget).
ttp://dx.doi.org/10.1016/j.neubiorev.2014.10.013149-7634/© 2014 The Authors. Published by Elsevier Ltd. This is an open access article un
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 596
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 596 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 596
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 605
, CHU de Nantes, 85, rue Saint Jacques, 44093 Nantes Cedex 1, France.
der the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/3.0/).
M. Grall-Bronnec, A. Sauvaget / Neuroscience and Biobehavioral Reviews 47 (2014) 592–613 593
3.2.4. Sham procedures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6053.2.5. Safety and tolerance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 605
4. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6054.1. Methodological issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 605
4.1.1. Sample size and scope of application. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6054.1.2. Characteristics of the participants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6064.1.3. Main exclusion criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6064.1.4. Cortical excitability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6064.1.5. Design . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 607
4.2. Technical issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6074.2.1. General considerations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6074.2.2. The rTMS device . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6074.2.3. Stimulation site and identification of target site . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6074.2.4. General design of the sessions and rTMS parameters . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6074.2.5. Sham procedure. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6084.2.6. Safety and tolerance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 608
5. Future directions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 608Conflict of interest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 610
. . . . . .
1
rtrAtafcsgdcr(nfvsDmbwk
Ibnetgicnagd5sletl
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. Introduction
Addictions are complex illnesses, and are the subject of manyesearch studies. A recent review paper suggested that over halfhe adult population of the United States reported symptomseminiscent of current addictive disorders (Sussman et al., 2011).ddictions can be defined as “a condition in which a behaviour
hat can function both to produce pleasure and to reduce painfulffects is employed in a pattern that is characterised by two keyeatures: (1) recurrent failure to control the behaviour, and (2)ontinuation of the behaviour despite significant harmful con-equences” (Goodman, 1990, 2008). Despite this minimalist butenerally agreed upon behavioural definition, different addictionsisplay many similarities in terms of risk factors, the frequency ofomorbidities and the trajectory, which is marked by periods ofelative control or abstinence alternating with periods of relapseGoodman, 2008). Finally, different types of addiction share aumber of clinical symptoms such as drug-seeking behaviour,
eelings or thoughts directed towards pathological behaviour per-ading the mind and impulsive action followed by periods oftruggle with anxiety of varying length (Le Moal and Koob, 2007;ickson et al., 2011). Compulsivity and impulsivity are the twoain factors involved in a composite addiction cycle, which can
e characterised by three successive stages: binge/intoxication,ithdrawal/negative affect, and preoccupation/anticipation, also
nown as the “craving stage” (Koob and Volkow, 2010).Addictions are not only limited to substance use disorders (SUD).
ndeed, it is now widely agreed that they also relate to non-drugehaviours (e.g. gambling or shopping) and substances that haveot traditionally been viewed as addictive (e.g. food) (Gearhardtt al., 2011). Whether they are linked to SUD or behavioural addic-ions, also known as “related disorders” (RD), they actually have areat deal in common despite their apparent clinical heterogene-ty and mainstream thinking increasingly views SUD and RD as aoherent whole. This is highlighted in the latest version of the Diag-ostic and Statistical Manual of Mental Disorders (DSM-5), where
new category entitled “Addiction and RD” combines SUD andambling disorders and drops the former categories of abuse andependence (O’Brien, 2011). Although not included in the DSM-, several other disorders were considered relating to the Internet,ex, exercise and shopping (Potenza, 2014a). It is expected that this
ist is non-exhaustive. Addiction relating to food was not consid-red by the research workgroup, due to existing debates on theopic (Potenza, 2014a), and grouping eating disorders under theabel “addictions” remains controversial. Despite this, more and. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 610
more authors support this idea (Speranza et al., 2012; Potenza,2014b). The umbrella term of eating disorders encompasses a broadspectrum, with anorexia nervosa (AN) at one end and binge eat-ing disorder (BED) at the other, and also includes bulimia nervosa(BN) and other specified feeding and eating disorder (OSFED). BN,BED and, to a lesser extent, OSFED share behavioural and clini-cal characteristics with other types of addictive disorders (Volkowand O’Brien, 2007; Kinzl and Biebl, 2010; Gearhardt et al., 2011;Speranza et al., 2012; Davis, 2013; Curtis and Davis, 2014). In par-ticular, they meet the diagnostic criteria proposed by Goodman(Goodman, 2008; Speranza et al., 2012). They also share neurobio-logical processes with other addictive disorders (Cota et al., 2006;Cowin et al., 2011; Gearhardt et al., 2011; Avena and Bocarsly, 2012;Umberg et al., 2012; Kaye et al., 2013; Volkow et al., 2013). Con-ceptualising AN as a behavioural addiction is perhaps somewhatmore complicated. Indeed, people with AN are not addicted to foodbut quite the opposite, they are addicted to food deprivation, andthey show real determination instead of losing control. Because ofthese opposing behavioural features, AN and BN could be regardedas two sides of the same coin. In particular, they are characterisedby a persistent preoccupation with food and dysfunctional cogni-tion related to body weight and body image (Avena and Bocarsly,2012), and by the same brain alterations, for example, increasedgrey matter volume of the medial orbitofrontal cortex and reducedwhite matter in the right temporal and parietal areas relativeto healthy individuals (Frank et al., 2013). The neural molecularevents driving self-restriction are detected in the nucleus accum-bens, strengthening the idea of the addictive facet of restrictive dietunderpinned by a rewarding effect associated with energy expen-diture (Jean et al., 2012). For all of these reasons, AN could alsobe considered as a behavioural addiction or a RD, especially of thebinge-eating/purging type.
Craving is one of the most striking symptoms of addiction andRD, as emphasised by the composite addiction cycle previouslymentioned (Koob and Volkow, 2010). It has been the subject ofgrowing attention, to the extent that it is listed as one of the diag-nostic criteria in the category “Addiction and RD” (O’Brien, 2011).Craving is defined as a pressing, urgent and irrepressible desire togive in to an addictive behaviour, and results in the loss of con-trol in most cases (Skinner and Aubin, 2010). In addition to theextensive literature in the field of drug craving, there is also a wide
range of information about food craving (Bou Khalil and El Hachem,2013; Jansen et al., 2013). Beyond the mere desire to take a drug orfood or to gamble, for example, craving also includes the expecta-tion of positive effects and the relief of negative effects as a result
5 e and
otttasdrpBn(2ibste22u(etnchfciHi
tapm3veni2ne
fiuictc((dtsehdmeadLa
94 M. Grall-Bronnec, A. Sauvaget / Neuroscienc
f this action (Young and Wohl, 2009). It is a persistent symp-om that can arise spontaneously or be cue-induced by exposinghe subject to various stimuli related to the addictive behaviourhrough classical conditioning (Watson, 1913). Incidentally,nimal models of craving are based on two behaviours: drug-eeking induced by drugs or stimuli previously associated withrug-taking, and drug-seeking induced by an acute stressor or aesidual negative emotional state (Koob and Volkow, 2010). It isossible to generalise this phenomenon to food craving (Avena andocarsly, 2012; Marco et al., 2012). Despite long periods of absti-ence, craving can reappear and increase the likelihood of relapseKoob and Volkow, 2010; Skinner and Aubin, 2010; Marhe et al.,013). Special attention must therefore be paid to managing crav-
ngs during the treatment of an addicted subject. Craving can alsoe cue-induced in an experimental setting to gain a better under-tanding of the role it plays in the decision-making process ando determine its neuro-cognitive correlates, as well as to test thefficacy of medication in reducing craving scores (Franklin et al.,011; Potenza et al., 2012; Goldman et al., 2013; McGrath et al.,013; Veilleux et al., 2013). Studies have shown that cravings arenderpinned by activation of the reward and motivation circuitsMcBride et al., 2006; Wang et al., 2007; Wing et al., 2012; Goldmant al., 2013; Jansen et al., 2013; Volkow et al., 2013). Accordingo these authors, the main neural structures involved are: theucleus accumbens, dorsal striatum, orbitofrontal cortex, anterioringulate cortex, dorsolateral prefrontal cortex (DLPFC), amygdala,ippocampus and insula. While the left DLPFC, as determined by
MRI, appears to play a crucial role in increasing self-control overravings (Hayashi et al., 2013), the right DLPFC may be involvedn the inhibitory control of affective impulses (Pripfl et al., 2013a).owever, a lack of empirical evidence for hemispheric differences
n DLPFC in addiction excludes definitive conclusions.Aside from the many features these disorders share, as men-
ioned above, there are also similarities in the therapeuticpproaches (Goodman, 2008). These are most often based onsychotherapy, which is administered using a range of differentethods (Goodman, 1990; Potenza et al., 2011). For more than
0 years, researchers have been developing methods for adju-ant care, particularly in the field of pharmacotherapy (Potenzat al., 2011). Many different molecules have been tested. Unfortu-ately, the results of such trials have not been completely successful
n meeting expectations (Achab and Khazaal, 2011; Muller et al.,011; Bolt et al., 2012; Mariani and Levin, 2012). More recently,ew treatment modalities such as brain stimulation have beenxplored.
Transcranial magnetic stimulation (TMS) is a medical tool thatrst appeared over 20 years ago (Barker, 1999). This neuromod-lation technique is based on the principle of electromagnetic
nduction and consists of magnetic pulses to induce electricalurrents in the brain via a coil placed on the scalp. This leadso cerebral neuromodulation through the modification of corti-al excitability (Daskalakis et al., 2006), of blood flow to the areaBestmann et al., 2005), of the frequency of neuronal dischargeBarr et al., 2009), and of the release of neurotransmitters such asopamine (Strafella et al., 2003; Cho and Strafella, 2009). In addi-ion to its cortical action, TMS is said to act remotely on deepertructures, via brain circuits and interhemispheric connections (Foxt al., 1997). Initially, TMS was used to study motor conductivity;owever, the effect of stimulation was extremely short-lived andisappeared almost instantaneously. Later, the ability to deliverultiple pulses via repetitive TMS (rTMS) enabled longer lasting
ffects and investigations into cognition, brain-behaviour relations
nd the pathophysiology of various neurologic and psychiatricisorders (Wassermann and Lisanby, 2001; Kobayashi and Pascual-eone, 2003; Tassinari et al., 2003; Rossi and Rossini, 2004; Riddingnd Rothwell, 2007). High frequency (HF) stimulation (>5 Hz)Biobehavioral Reviews 47 (2014) 592–613
is considered to have excitatory effects on the cortical activitywhereas low frequency (LF) stimulation (<1 Hz) is considered tohave inhibitory effects (Pascual-Leone et al., 1994). Animal andhuman studies have concluded that rTMS may have a therapeu-tic effect by altering cortical excitability through the modulationof neurotransmitters including dopamine and GABA (Barr et al.,2011). Successive studies have broadened the range of therapeuticapplications in the field of neurological, re-educational and psychi-atric pathologies. One line of research to emerge recently examinesthe efficacy of rTMS on addiction and RD by targeting craving inparticular.
Experimental studies suggest that there is indeed a dopaminer-gic dysfunction of the mesolimbic systems in addicts (Goodman,2008). According to some authors, symptoms of addiction andRD could be alleviated by “boosting” dopaminergic transmission(Diana, 2011), which may be achieved via TMS.
Because of their deep brain localisation, dopaminergic neuronsare indirectly stimulated during rTMS, through their more superfi-cial projections, especially in the DLPFC (Diana, 2011). The DLPFC isinvolved in cognitive control and the physiopathology of impulsecontrol disorders, such as addiction and RD (Crockford et al., 2005;Wang et al., 2007; Van Holst et al., 2010). rTMS applied to theDLPFC may therefore indirectly modulate dopaminergic pathways(Addolorato et al., 2012) and may consequently have an impacton the symptoms of addiction (Keck et al., 2002; Feil and Zangen,2010): cognitive control could be improved and/or cravings couldbe reduced (Jansen et al., 2013).
The first articles to assess the value of rTMS to treat addictivedisorders date back to 2003 (Eichhammer et al., 2003; Johann et al.,2003). Uncovering a role for rTMS treatment for addiction and RDhas been approached from a number of different perspectives andin many different ways (original research, reviews, and comprehen-sive work), namely by focusing on case studies (Hausmann et al.,2004; De Ridder et al., 2011; Downar et al., 2012; McClelland et al.,2013b; Baczynski et al., 2014); one substance at a time (Hoppneret al., 2011; Nardone et al., 2012; Wing et al., 2013); including allSUDs (Barr et al., 2008; Feil and Zangen, 2010; Barr et al., 2011;Addolorato et al., 2012; Bellamoli et al., 2014); eating disorders(Van den Eynde and Guillaume, 2012; McClelland et al., 2013a);one symptom of addiction at a time, such as craving (Jansen et al.,2013); dependence, or cognitive impairment (Knoch et al., 2006);comprehensive physiopathological approaches (Keck et al., 2002;Strafella et al., 2003; Barr et al., 2008; Camus et al., 2009; Cho andStrafella, 2009; Diana, 2011; Hayashi et al., 2013); one neuromod-ulation technique at a time (Barr et al., 2008, 2011; Hoppner et al.,2011; Addolorato et al., 2012; Bellamoli et al., 2013; Rosenberget al., 2013) or several techniques investigated simultaneously (Feiland Zangen, 2010; Van den Eynde and Guillaume, 2012; Jansenet al., 2013; Wing et al., 2013). Several “magnetic techniques”have also been tested in addiction and RD such as transcranialdynamic magnetotherapy (TcDMT) in the complex treatment ofalcohol withdrawal syndrome (Staroverov et al., 2009) and deepTMS in pathological gambling (Rosenberg et al., 2013). Althoughthese techniques use magnetic fields, they are not completely com-parable to rTMS. Their mechanistic properties, working on theprinciple of electromagnetic induction are similar. However, theydiffer regarding their depth of penetration and the focality of themagnetic field, mainly because they use different coils. rTMS mostoften uses a figure-8 coil, which induces an electric field restrictedto superficial cortical targets, up to 3 cm (Rossi et al., 2009) dueto its rapid attenuation in depth. Deep TMS is designed to reachgreater depths than rTMS, reaching up to 6 cm (Bersani et al., 2013)
via an H-coil. Figure-8 coils produce a more focal and shallowerstimulation compared to H-coils.First and foremost, we support the idea that all types ofaddiction can be compared using a comprehensive approach that

M. Grall-Bronnec, A. Sauvaget / Neuroscience and Biobehavioral Reviews 47 (2014) 592–613 595
Number of studies identified
through searches = 638
Included studies = 18
Screening inclusion criteria
- The target problem w as a SUD or
related disorder
- The intervention consisted of rTMS
- The study was a clinical trial
Screening exclusion criteria
- Animal models
- Studies into risk-taking behaviour or decision-making
- Lack of methodological data
- Addictions with mood and psychotic comorbidities in particular
- Studies with only a physiopathological aim
- Case reports
- Reviews
Unduplicated research = 484
ch str
cttjnCnis
iaislTtfocrt
2
2
i2G“h“ob
The data extraction work was divided between the twoauthors. Extracted data included clinical, general, and technicalconsiderations.
Fig. 1. Flow diagram of the sear
onsiders physiopathological, clinical and therapeutic aspects. Inhis paper, we consider both addiction and RD. We also supporthe idea that behavioural changes ought to be considered, notust craving. Finally, we think that a systematic comparison of allon-invasive neuromodulation techniques (e.g., transcranial Directurrent Stimulation and rTMS) is not plausible because these tech-iques do not share the same procedures and because research
n this field is too recent and heterogeneous to currently performpecific meta-analyses.
The purpose of this article is to critically review the progressn the use of rTMS since its inception to treat addiction and RD,nd in particular the developments in its therapeutic efficacy. Thiss particularly important as it will allow us to identify the mostuccessful approaches, summarise the progress made, and high-ight the lessons to be learned from the difficulties encountered.his review will first discuss the methodological issues, followed byhe technical issues of rTMS applied to addiction and RD. Finally,uture directions and key recommendations will be proposed. Tour knowledge, this work is the first to provide a summary thatovers all types of addiction, including SUD and RD in the field ofTMS and to offer a critical assessment of the methodological andechnical issues raised.
. Methods
.1. Search strategy
We identified articles for inclusion in this review by search-ng the MEDLINE and ScienceDirect databases up to December013, limiting the search to articles published in English anderman (one article). The key words used were “TMS” or
rTMS” AND one of the following terms: “addiction”, “alco-
ol”, “amphetamine”, “methamphetamine”, “anorexia nervosa”,behavioural addiction”, “benzodiazepine”, “binge eating dis-rder”, “bulimia nervosa”, “cannabis”, “cocaine”, “compulsiveuying/shopping”, “craving”, “DLPFC”, “dopamine”, “drug”, “eatingategy and selection procedure.
disorder”, “ecstasy”, “EDNOS”1, “exercise”, “food craving”, “impuls-ivity”, “LSD”, “nicotine”, “opiate”, “pathological gambling”, “sexaddiction”, “smoking”, “sport addiction”, and “tobacco”. A manualsearch and a screening of the bibliography of the selected studieswere performed in addition to the computerised screening. Dupli-cate searches were eliminated. The search strategy is summarisedin Figure 1.
2.2. Eligibility criteria
Studies had to fulfil the following criteria to be included:
- The target problem was an addiction, a RD or craving- The intervention was performed using rTMS- The study was a clinical trial (e.g., any research study concerning
human beings, including pilot studies and randomised clinicaltrials) (WHO, 2014).
2.3. Study selection
First, all studies were screened based on their titles andabstracts. Second, the two authors read the full text of all studiesidentified in this search process. They carried out this work inde-pendently using the same bibliographic search. In the event of adisagreement between them, the relevant studies were discussed.
2.4. Data extraction
1 In the rest of the text, we refer to the DSM-IV because the studies we haveselected have been carried out prior to the DSM-5 publication. “EDNOS” (eatingdisorder not otherwise specified) (DSM-IV) was replaced by “OSFED” (DSM-5).
5 e and
3
minease
3
3
o(aotciAsTt(catmstdacs(bcDe
3
ablhs(dtcrfera
3
w
96 M. Grall-Bronnec, A. Sauvaget / Neuroscienc
. Results
Eighteen articles met the criteria for inclusion.The disorders tested were nicotine, alcohol, cocaine and
ethamphetamine dependence, and eating disorders (food crav-ng, AN, BN and EDNOS). Of the 18 studies included, only one was aon-controlled study (Politi et al., 2008). To the best of our knowl-dge, we assume that rTMS has not yet been tested in the followingddictive disorders: ecstasy, LSD or opiate use disorders, compul-ive buying/shopping, pathological gambling, sex addiction andxercise addiction.
.1. Efficacy of rTMS
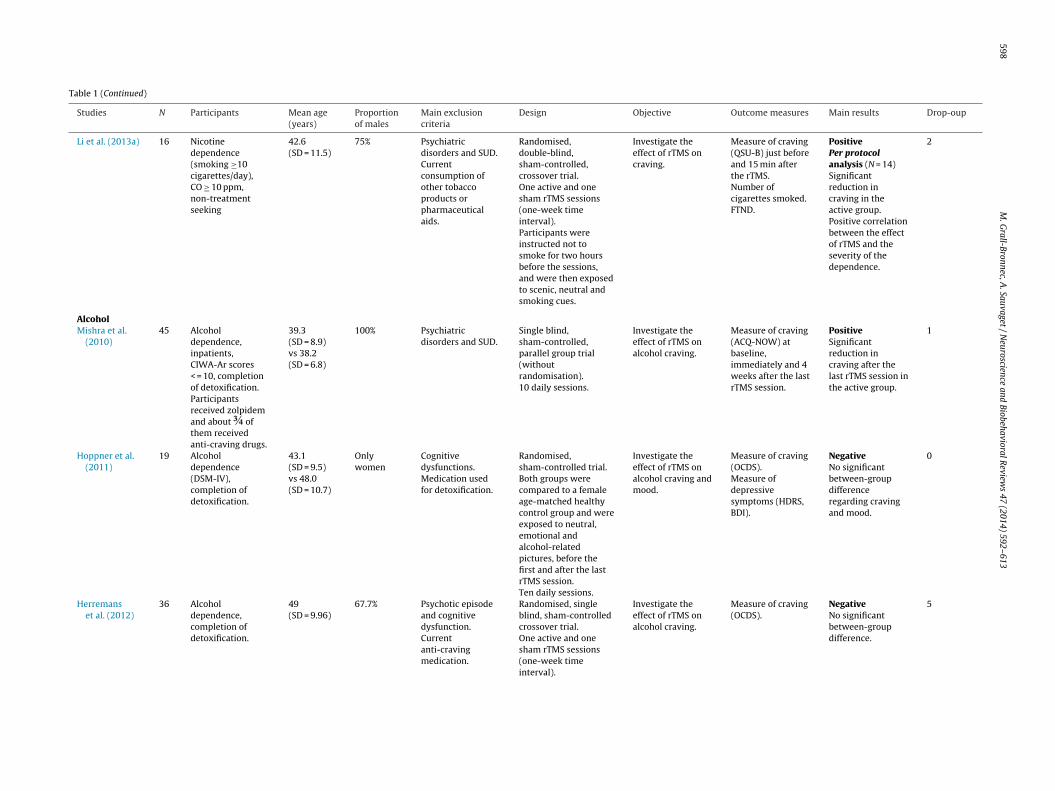
The results are summarised in Table 1.
.1.1. rTMS and nicotineThe first studies to test the efficacy of rTMS in the sphere
f addictions were carried out in nicotine-dependent subjectsEichhammer et al., 2003; Johann et al., 2003). Both studies adopted
crossover design. In one of the studies, two sessions were carriedut, compared to four sessions in the other study. Compared tohe placebo, real stimulation produced a significant reduction inravings (Johann et al., 2003) and in cigarette consumption dur-ng the hours that followed rTMS (Eichhammer et al., 2003). Later,miaz and colleagues used a design with parallel groups of 10 dailyessions followed by a maintenance period (Amiaz et al., 2009).he authors observed significant reductions in cigarette consump-ion (assessed by urine cotinine levels) and nicotine dependenceassessed by the Fagerström test). Exposure to smoking-relatedues followed by active rTMS produced a specific positive effectfter 10 sessions by reducing the craving for nicotine, which tendedo disappear after 6 months. Another trial offered additional infor-
ation to improve our understanding of the influence of theuperior frontal gyrus on nicotine craving rather than being a realest of the efficacy of rTMS (Rose et al., 2011). These studies areescribed in the literature review by Wing et al. (2013). This reviewlso reports preliminary work with the aim of studying the effi-acy of rTMS combined with nicotine replacement in subjects withtrong nicotine dependence but also suffering from schizophreniaWing et al., 2012). This study was not included in our analysisecause of this specific comorbidity. Finally, the last study suc-essfully demonstrated that a single session of HF rTMS over theLPFC could significantly reduce cigarette craving induced by cuexposure (Li et al., 2013a).
.1.2. rTMS and alcoholDespite the strong prevalence of alcohol use disorders and the
bsence of effective treatment for some patients, rTMS has onlyeen tested on alcohol-dependent patients very recently. We have
isted three studies that included alcohol-dependent subjects whoad just completed detoxification. Two of the studies used 10 dailyessions of rTMS, applied to the right (Mishra et al., 2010) or leftHoppner et al., 2011) DLPFC. The third study adopted a crossoveresign with two rTMS sessions, one active and one placebo, appliedo the right DLPFC (Herremans et al., 2012). The study by Mishra andolleagues was carried out as a single blind trial and indicated thateal stimulation was superior, with a reduction in craving lasting forour weeks after the completion of the active rTMS sessions (Mishrat al., 2010). Conversely, the next two studies reported negativeesults as they failed to show a significant reduction in craving afterctive rTMS (Hoppner et al., 2011; Herremans et al., 2012).
.1.3. rTMS and cocaineAs far as we are aware, only two studies have been published
ith the aim of evaluating the efficacy of rTMS on craving among
Biobehavioral Reviews 47 (2014) 592–613
cocaine-dependent subjects. All of the patients studied had previ-ously completed their cocaine detoxification. In both studies, theauthors concluded that rTMS had a positive effect. Nevertheless,there were a number of important differences between these stud-ies. The aim of the first study was to compare the effects of rTMSaccording to the side of the brain it was applied to (Camprodonet al., 2007). The results showed that rTMS had only a transienteffect. In contrast, the other study was not controlled but was ofinterest because it showed that 10 daily sessions of rTMS deliveredto the left DLPFC produced a significant reduction in craving overtime (Politi et al., 2008). Despite these promising results, no furtherstudies have been reported.
3.1.4. rTMS and methamphetamineIn a single-blind, sham-controlled crossover study, Li and
colleagues recently suggested that LF rTMS on the left DLPFCtransiently increased cue-induced craving in methamphetamineparticipants (Li et al., 2013b).
3.1.5. rTMS and foodThe body of literature in the field of eating disorders, and more
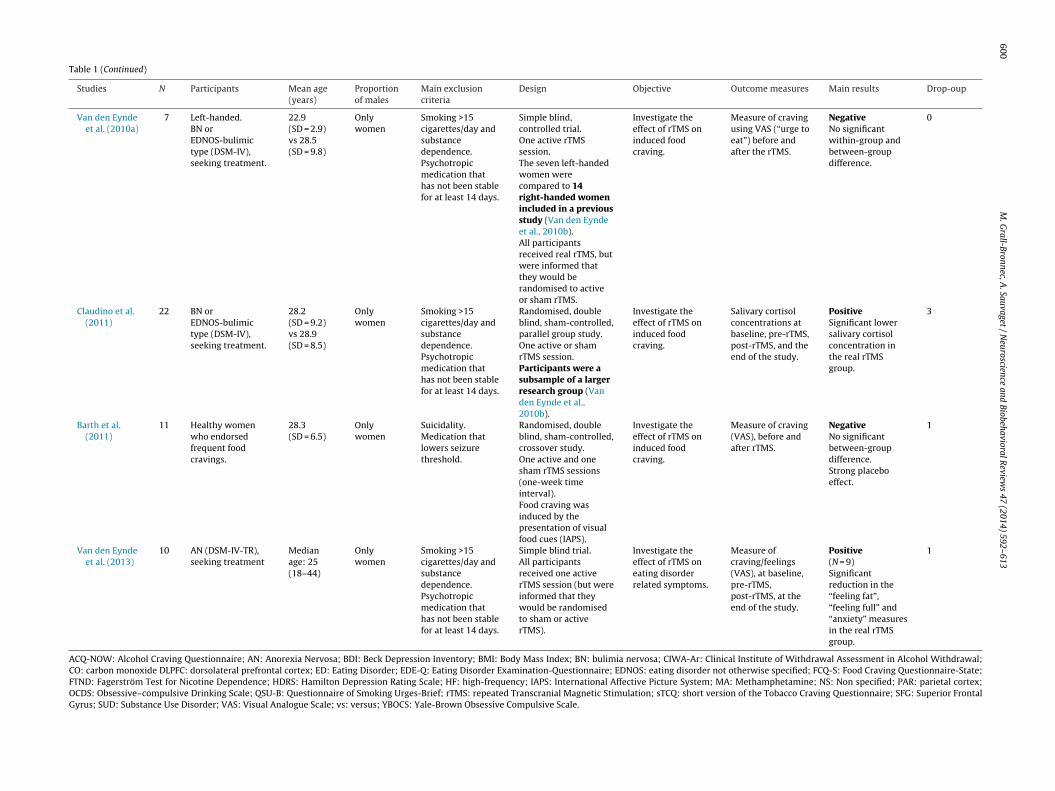
broadly that of food craving, provides the most evidence of rTMStreatment efficacy. Seven studies have been published to date. Fiveof these were carried out by the same team (Uher et al., 2005; Vanden Eynde et al., 2010a, 2010b, 2013; Claudino et al., 2011), whichprobably explains their similarities, and two of them were basedon patients included in a previous study (Van den Eynde et al.,2010b). All of these studies except one (Van den Eynde et al., 2010b)included only women who had a history of BN or EDNOS-bulimictype (Walpoth et al., 2008; Van den Eynde et al., 2010a, 2010b;Claudino et al., 2011). For the most part, the studies were ran-domised, double-blind, sham-controlled, parallel group trials. Allexcept one (Walpoth et al., 2008) aimed to investigate the efficacyof a single rTMS session delivered to the left DLPFC on inducedfood craving. In most of the studies the assessment criteria werescore variations on Visual Analogue Scales. One study used a moreobjective physiological measurement of craving, by repeating sali-vary cortisol assays (Claudino et al., 2011), while another chose touse an indirect reflection of craving based on the change in fre-quency of binges and purges (Walpoth et al., 2008). As shown insummary Table 1, four of the seven studies listed concluded thatrTMS is effective.
3.2. rTMS technical procedures
The results are summarised in Table 2.
3.2.1. The rTMS deviceThe equipment most frequently used was MagStim (12 studies),
far ahead of Neuronetics (three studies). Only three studies failedto specify the equipment used. Most of the studies in which theequipment was specified used focal coils, such as the 8-figured coil.
3.2.2. Stimulation site and identification of the target siteThe cortical target most often selected was the left DLPFC (14
studies) with the right DLPFC being chosen much less frequently(two studies). Just one study compared the efficacy of both targetregions (Camprodon et al., 2007). Another chose to compare SFGand MOC (Rose et al., 2011). The DLPFC was most often located usingthe “5 cm” or “6 cm” empirical method (10 studies), by moving thecoil 5 or 6 cm anterior to the motor cortex, along a parasagittal
line (Herbsman et al., 2009; George and Post, 2011). Two studiesused the international EEG system or “10–20 method” (Hoppneret al., 2011; Rose et al., 2011). Only one study used neuronavigationwith 3D-MRI (Herremans et al., 2012). Only four studies failed to
M.
Grall-Bronnec,
A.
Sauvaget /
Neuroscience
and Biobehavioral
Review
s 47
(2014) 592–613
597
Table 1Clinical trials of rTMS for addiction and related disorders: clinical and general considerations.
Studies N Participants Mean age(years)
Proportionof males
Main exclusioncriteria
Design Objective Outcome measures Main results Drop-oup
NicotineJohann et al.
(2003)11 Nicotine
dependence(FTND), motivationto quit smoking.
35 (23–55) 18.2% Psychiatricdisorders and SUD.
Randomised,double-blind,sham-controlled,crossover trialOne active and onesham rTMS sessions on2 consecutive days.
Investigate theeffect of rTMS oncigarette craving.
Measure of craving(VAS)
PositiveSignificantreduction incraving after thereal rTMS for 9participants.
0
Eichhammeret al. (2003)
14 Nicotinedependence(FTND), motivationto quit smoking.
35.4(SD = 8.9)
14.2% Psychiatricdisorders and SUD.Benzodiazepinesmedication.
Randomised,double-blind,sham-controlled,crossover trial.Two active and twosham rTMS sessions on4 consecutive days.
Investigate theeffect of rTMS oncigarette smokingand craving.
Measure of craving(VAS) and smoking.
PositiveSignificantreduction insmoking in theactive group.
NS
Amiaz et al.(2009)
52 Nicotinedependence(DSM-IV), smoking>20 cigarettes/day,motivation to quitsmoking.
47.9 43.7% Psychiatricdisorders.Current psychiatricmedication.
Randomised,double-blind andsham-controlled trial(four subgroups: activevs shamrTMS/smoking-relatedvs neural picture cues).10 daily sessionsfollowed by a 4-weekmaintenance phase.
Investigate theeffect of rTMS oncigarette smoking,dependence andcraving.
Levels of cotininein urine.Number ofcigarettes smoked.FTND, sTCQ.VAS.
PositivePer protocolanalysis (N = 48).Significantreduction incigarette smokingand dependence.
18
Rose et al.(2011)
15 Smoking >20cigarettes/day,CO ≥ 10 ppm,craving increase ≥1point uponexposure to cues.
40.7(SD = 9.56)
53.3% Psychiatricdisorders and SUD.Current psychiatricmedication.
Randomised,sham-controlled trialAt the beginning ofeach session, subjectssmoked a cigarette.One hour later, theyunderwent rTMSconcurrently duringexposure to (1) neutral(2) smoking cues (3)smoking a cigarette.
Test hypothesesabout the causalrole of SFG inmodulatingcraving.
Cue reactivity.Cigaretteevaluationquestionnaire
Does not provideevidence of theutility of rTMS.
NS
598
M.
Grall-Bronnec,
A.
Sauvaget /
Neuroscience
and Biobehavioral
Review
s 47
(2014) 592–613
Table 1 (Continued)
Studies N Participants Mean age(years)
Proportionof males
Main exclusioncriteria
Design Objective Outcome measures Main results Drop-oup
Li et al. (2013a) 16 Nicotinedependence(smoking ≥10cigarettes/day),CO ≥ 10 ppm,non-treatmentseeking
42.6(SD = 11.5)
75% Psychiatricdisorders and SUD.Currentconsumption ofother tobaccoproducts orpharmaceuticalaids.
Randomised,double-blind,sham-controlled,crossover trial.One active and onesham rTMS sessions(one-week timeinterval).Participants wereinstructed not tosmoke for two hoursbefore the sessions,and were then exposedto scenic, neutral andsmoking cues.
Investigate theeffect of rTMS oncraving.
Measure of craving(QSU-B) just beforeand 15 min afterthe rTMS.Number ofcigarettes smoked.FTND.
PositivePer protocolanalysis (N = 14)Significantreduction incraving in theactive group.Positive correlationbetween the effectof rTMS and theseverity of thedependence.
2
AlcoholMishra et al.
(2010)45 Alcohol
dependence,inpatients,CIWA-Ar scores< = 10, completionof detoxification.Participantsreceived zolpidemand about ¾ ofthem receivedanti-craving drugs.
39.3(SD = 8.9)vs 38.2(SD = 6.8)
100% Psychiatricdisorders and SUD.
Single blind,sham-controlled,parallel group trial(withoutrandomisation).10 daily sessions.
Investigate theeffect of rTMS onalcohol craving.
Measure of craving(ACQ-NOW) atbaseline,immediately and 4weeks after the lastrTMS session.
PositiveSignificantreduction incraving after thelast rTMS session inthe active group.
1
Hoppner et al.(2011)
19 Alcoholdependence(DSM-IV),completion ofdetoxification.
43.1(SD = 9.5)vs 48.0(SD = 10.7)
Onlywomen
Cognitivedysfunctions.Medication usedfor detoxification.
Randomised,sham-controlled trial.Both groups werecompared to a femaleage-matched healthycontrol group and wereexposed to neutral,emotional andalcohol-relatedpictures, before thefirst and after the lastrTMS session.Ten daily sessions.
Investigate theeffect of rTMS onalcohol craving andmood.
Measure of craving(OCDS).Measure ofdepressivesymptoms (HDRS,BDI).
NegativeNo significantbetween-groupdifferenceregarding cravingand mood.
0
Herremanset al. (2012)
36 Alcoholdependence,completion ofdetoxification.
49(SD = 9.96)
67.7% Psychotic episodeand cognitivedysfunction.Currentanti-cravingmedication.
Randomised, singleblind, sham-controlledcrossover trial.One active and onesham rTMS sessions(one-week timeinterval).
Investigate theeffect of rTMS onalcohol craving.
Measure of craving(OCDS).
NegativeNo significantbetween-groupdifference.
5

M.
Grall-Bronnec,
A.
Sauvaget /
Neuroscience
and Biobehavioral
Review
s 47
(2014) 592–613
599
Table 1 (Continued)
Studies N Participants Mean age(years)
Proportionof males
Main exclusioncriteria
Design Objective Outcome measures Main results Drop-oup
CocaineCamprodon
et al. (2007)6 Cocaine
dependence(DSM-IV), inpatientcompletion ofdetoxification.
19–23 100% Currentdependence onother substanceand psychiatricdisorders.Psychiatricmedication.
Randomised, crossovertrial (one-week timeinterval).Two rTMS sessionsover left and rightDLPFC.
Investigate theeffect of rTMS oncocaine craving.
Measure of craving(VAS).Measure of anxiety,happiness, sadnessand discomfort(VAS).
PositiveSignificant, buttransient,reduction of thecraving with the“right” rTMS (butno effect with the“left” rTMS).
0
Politi et al.(2008)
36 Cocainedependence(DSM-IV),completion ofdetoxification.
NS 86.1% NS No controlled study.Ten daily sessions.
Investigate theeffect of rTMS oncocaine craving.
Gambling taskSCID IIWAIS-R
PositiveSignificant overtime reduction ofthe craving.
0
MethamphetamineLi et al. (2013b) 17 MA dependence
(DSM-IV-TR)10 MA-dependentusers non-seekingtreatment and 8healthy controls
34.7(SD = 10.6)vs 32.5(SD = 12.6)
50% Psychiatricdisorders.Psychiatricmedication.
Randomised,single-blind,sham-controlledcrossover trial andhealthy controlled trial(one-hour timeinterval).One active and onesham rTMS sessions(one-hour timeinterval).
Investigate theeffect of rTMS onmethamphetaminecraving.
Measure of craving(VAS).
Significant, buttransient, increaseof the craving.
0
FoodUher et al.
(2005)30 Women with
normal averageBMI, with strongurges.
25.2(SD = 5.4)vs 26.4(SD = 4.9)
Onlywomen
ED, currentpsychiatricdisorders andsmoking > 5cigarettes/day.Psychiatricmedication.
Randomised, doubleblind, sham-controlled,parallel group trial.One active or shamrTMS session.
Investigate theeffect of rTMS onfood craving.
Measure of craving(VAS), immediatelyafter food exposure(before and afterrTMS).
PositivePrevention of anincrease of foodcraving in the realrTMS group.
2
Walpoth et al.(2008)
14 BN (DSM-IV). 27.4(SD = 4.8)vs 22.6(SD = 2.6)
Onlywomen
Severe depressivesymptoms,BMI < 17.5.Psychotherapy andpsychiatricmedication for thepast 3 months.
Randomised, doubleblind, sham-controlled,parallel group trial.One week of placebowash-out, then 15daily active or shamrTMS sessions.
Investigate theeffect of rTMS onbinges and purges.
Reduction of atleast 50% in thefrequency of bingesand purges.
NegativeNo significantbetween-groupdifference.
0
Van den Eyndeet al. (2010b)
37 BN orEDNOS-bulimictype (DSM-IV),seeking treatment.
30.5(SD = 11.2)vs 29.5(SD = 8.4)
13.1% Smoking >10cigarettes/day andsubstancedependence.Psychotropicmedication thathas not been stablefor at least 14 days.
Randomised, doubleblind, sham-controlled,parallel group trial.One active or shamrTMS session.
Investigate theeffect of rTMS oninduced foodcraving.
Measure of craving(VAS: “urge to eat”)before and afterthe rTMS.
PositiveSignificantreduction incraving and in thenumber ofbinge-eatingepisodes over the24-hour follow-upin the real rTMSgroup.
5
600
M.
Grall-Bronnec,
A.
Sauvaget /
Neuroscience
and Biobehavioral
Review
s 47
(2014) 592–613
Table 1 (Continued)
Studies N Participants Mean age(years)
Proportionof males
Main exclusioncriteria
Design Objective Outcome measures Main results Drop-oup
Van den Eyndeet al. (2010a)
7 Left-handed.BN orEDNOS-bulimictype (DSM-IV),seeking treatment.
22.9(SD = 2.9)vs 28.5(SD = 9.8)
Onlywomen
Smoking >15cigarettes/day andsubstancedependence.Psychotropicmedication thathas not been stablefor at least 14 days.
Simple blind,controlled trial.One active rTMSsession.The seven left-handedwomen werecompared to 14right-handed womenincluded in a previousstudy (Van den Eyndeet al., 2010b).All participantsreceived real rTMS, butwere informed thatthey would berandomised to activeor sham rTMS.
Investigate theeffect of rTMS oninduced foodcraving.
Measure of cravingusing VAS (“urge toeat”) before andafter the rTMS.
NegativeNo significantwithin-group andbetween-groupdifference.
0
Claudino et al.(2011)
22 BN orEDNOS-bulimictype (DSM-IV),seeking treatment.
28.2(SD = 9.2)vs 28.9(SD = 8.5)
Onlywomen
Smoking >15cigarettes/day andsubstancedependence.Psychotropicmedication thathas not been stablefor at least 14 days.
Randomised, doubleblind, sham-controlled,parallel group study.One active or shamrTMS session.Participants were asubsample of a largerresearch group (Vanden Eynde et al.,2010b).
Investigate theeffect of rTMS oninduced foodcraving.
Salivary cortisolconcentrations atbaseline, pre-rTMS,post-rTMS, and theend of the study.
PositiveSignificant lowersalivary cortisolconcentration inthe real rTMSgroup.
3
Barth et al.(2011)
11 Healthy womenwho endorsedfrequent foodcravings.
28.3(SD = 6.5)
Onlywomen
Suicidality.Medication thatlowers seizurethreshold.
Randomised, doubleblind, sham-controlled,crossover study.One active and onesham rTMS sessions(one-week timeinterval).Food craving wasinduced by thepresentation of visualfood cues (IAPS).
Investigate theeffect of rTMS oninduced foodcraving.
Measure of craving(VAS), before andafter rTMS.
NegativeNo significantbetween-groupdifference.Strong placeboeffect.
1
Van den Eyndeet al. (2013)
10 AN (DSM-IV-TR),seeking treatment
Medianage: 25(18–44)
Onlywomen
Smoking >15cigarettes/day andsubstancedependence.Psychotropicmedication thathas not been stablefor at least 14 days.
Simple blind trial.All participantsreceived one activerTMS session (but wereinformed that theywould be randomisedto sham or activerTMS).
Investigate theeffect of rTMS oneating disorderrelated symptoms.
Measure ofcraving/feelings(VAS), at baseline,pre-rTMS,post-rTMS, at theend of the study.
Positive(N = 9)Significantreduction in the“feeling fat”,“feeling full” and“anxiety” measuresin the real rTMSgroup.
1
ACQ-NOW: Alcohol Craving Questionnaire; AN: Anorexia Nervosa; BDI: Beck Depression Inventory; BMI: Body Mass Index; BN: bulimia nervosa; CIWA-Ar: Clinical Institute of Withdrawal Assessment in Alcohol Withdrawal;CO: carbon monoxide DLPFC: dorsolateral prefrontal cortex; ED: Eating Disorder; EDE-Q: Eating Disorder Examination-Questionnaire; EDNOS: eating disorder not otherwise specified; FCQ-S: Food Craving Questionnaire-State;FTND: Fagerström Test for Nicotine Dependence; HDRS: Hamilton Depression Rating Scale; HF: high-frequency; IAPS: International Affective Picture System; MA: Methamphetamine; NS: Non specified; PAR: parietal cortex;OCDS: Obsessive–compulsive Drinking Scale; QSU-B: Questionnaire of Smoking Urges-Brief; rTMS: repeated Transcranial Magnetic Stimulation; sTCQ: short version of the Tobacco Craving Questionnaire; SFG: Superior FrontalGyrus; SUD: Substance Use Disorder; VAS: Visual Analogue Scale; vs: versus; YBOCS: Yale-Brown Obsessive Compulsive Scale.

M.
Grall-Bronnec,
A.
Sauvaget /
Neuroscience
and Biobehavioral
Review
s 47
(2014) 592–613
601
Table 2Clinical trials of rTMS for addiction and related disorders: technical considerations.
Studies Handedness rTMSdevice
Stimulationsite (brainregion)
Method forlocatingcorticaltarget
F (Hz) Method fordetermin-ingRMT
% of RMT Number oftrains
ITI (s) Totalpulses persession
Sessionduration
Sham-TMSprocedures(devices andmethods)
Tolerance/adverseeffects
NicotineJohann et al.
(2003)NS Magstim
active coilandsham-coilsystem
Left DLPFC NS 20 (HF) NS 90% 20 trains(2.5 s each)
NS 1000 NS Sham-coilsystem
NS
Eichhammeret al. (2003)
RH Magstimactive coilandsham-coilsystem
Left DLPFC 5 cmmethod
20 (HF) NS 90% 20 trains(2.5 s each)
42,5 1000 14 min Shamstimulation atthe samelocation andfrequency,using asham-coilsystem
Mild headachesin 2 cases afteractivestimulation
Amiaz et al.(2009)
NS Double70-mm(figure-8)coil(Magstim)
Left DLPFC 5 cmmethod
10 (HF) S◦ of themotorstrip-examiningthe rightAPBM
100% 20 15 NS NS Mu-metalplates attachedto the activecoil
NS
Rose et al.(2011)
NS NeuroneticsModel2100 CRS
SFG or MOC(side notspecified)
International10–20system forEEG
10 (HF)(SFG)1 (LF) (SFG)1 (LF)(MOC)
S◦ of themotorstrip-examiningthe rightAPBM
90% NS NS Greaternumber ofpulses forthe 20 HzS◦
2 min 30 sfor eachsession
No shamsession
NS
Li et al. (2013a) RH NeuroneticsModel3600 witha solid focalcoil TMSmachine
Left DLPFC 6 cmmethod
10 (HF) S◦ of themotorstrip-examiningthe rightAPBM
100% 60 trains(5 s each)
10 3000 15 min Sham systemusing a shamrTMS coilTwo scalpelectrodeswere locatedjust below thehairline,connected to aTENSD.Participantswore the scalpelectrodes inbothconditions.During realTMS, there wasno currentflowingthrough thescalpelectrodes.
Someparticipantsexperiencedmilddiscomfort atthe start ofstimulation.Twoparticipantsdropped outbecause ofschedulingconflicts.

602
M.
Grall-Bronnec,
A.
Sauvaget /
Neuroscience
and Biobehavioral
Review
s 47
(2014) 592–613
Table 2 (Continued)
Studies Handedness rTMSdevice
Stimulationsite (brainregion)
Method forlocatingcorticaltarget
F (Hz) Method fordetermin-ingRMT
% of RMT Number oftrains
ITI (s) Totalpulses persession
Sessionduration
Sham-TMSprocedures(devices andmethods)
Tolerance/adverseeffects
AlcoholMishra et al.
(2010)RH Magstim
rapiddeviceactive andshamfigure-8coils
RightDLPFC
5 cmmethod
10 (HF) MEP 110% 20 trains(4.9 s each)
30 1000 NS Sham figure-8coils
Seizure forpatient withsham (butrecentlystoppedlorazepam),one scalp pain,five transientheadaches,pain duringdelivery of thestimulationtrain, anxietyfor fourpatients at firstsession
Hoppner et al.(2011)
NS NS Left DLPFCfor theactive coil
F3 (Inter-national10–20system forEEG)
20 (HF) NS 90% 20 trains(2.5 s each)
42,5 1000 NS No sham coilbut shamstimulationwith active coilapplied abovethe lefttemporalmuscle, angledat 45◦ , 5 cmlateral to F3, S◦
intensityreduced to 60%RMT
Good/None
Herremanset al. (2012)
NS Double70-mm(figure-8)coil(Magstim)
RightDLPFC
3D-MRI 20 (HF) Singlepulse TMSwith MEP
110% 40 trains(1.9 s each)
12 1560 NS Active coil heldangled at 90◦
Single blindSubjects woreearplugs andwereblindfolded
Good/None
CocaineCamprodon
et al. (2007)RH NS Left DLPFC
or rightDLPFC
NS 10 (HF) NS 90% 20 trains(10 s each)
60 NS NS No shamsession
Good/None
Politi et al.(2008)
NS Active coil Left DLPFC NS 15 (HF) NS 100% 20 trains(2 s each)
30 NS NS No shamsession
NS
MethamphetamineLi et al. (2013b) NS Double
70-mm(figure-8)coil(Magstim)
Left DLPFC 6 cmmethod
1 (LF) S◦ of themotorstrip-examiningthe rightAPBM
100% NS NS 900 15 min Active coil heldangled at 45◦
Single blindElectricalstimulationthrough theskin on thesubjects’forehead
Transient mildscalpdiscomfort atthe start ofstimulation insomeparticipants

M.
Grall-Bronnec,
A.
Sauvaget /
Neuroscience
and Biobehavioral
Review
s 47
(2014) 592–613
603
Table 2 (Continued)
Studies Handedness rTMSdevice
Stimulationsite (brainregion)
Method forlocatingcorticaltarget
F (Hz) Method fordetermin-ingRMT
% of RMT Number oftrains
ITI (s) Totalpulses persession
Sessionduration
Sham-TMSprocedures(devices andmethods)
Tolerance/adverseeffects
FoodUher et al.
(2005)RH Magstim
rapiddevice realand shamfigure-8coils
Left DLPFC 5 cmmethod
10 (HF) S◦ of themotorstrip-examiningthe rightAPBM
110% 20 trains(5 s each)
55 1000 20 min Same locationand frequencyusing thesham-coilsystem
Physicaldiscomfort forone patient(real session)
Walpoth et al.(2008)
NS Magstimrapiddevice realand shamfigure-8coils
Left DLPFC NS 20 (HF) NS 120% 10 trains(10 s each)
60 2000 NS Sham coilsystem
No seizure-likephenomenawere observed
Van den Eyndeet al. (2010b)
RH Magstimrapiddevice realand shamfigure-8coils
Left DLPFC 5 cmmethod
10 (HF) S◦ of themotorstrip-examiningthe rightAPBM
110% 20 trains(5 s each)
55 1000 20 min Same locationand frequencyusing thesham-coilsystemBlindingsuccess isreported (moresuccessful insham-groupthan in the realrTMS group)
- Physicaldiscomfort forone patient(real session)- Transientslight headachefor five patientsin each group
Van den Eyndeet al. (2010a)
LH vs RH Magstimrapiddevice andfigure-8coils
Left DLPFC 5 cmmethod
10 (HF) S◦ of themotorstrip-examiningthe rightAPBM
110% 20 trains(5 s each)
55 1000 20 min NS NS
Claudino et al.(2011)
RH Magstimrapiddevice realand shamfigure-8coils
Left DLPFC 5 cmmethod
10 (HF) S◦ of themotorstrip-examiningthe rightAPBM
110% 20 trains(5 s each)
55 1000 20 min Same locationand frequencyusing thesham-coilsystemBlindingsuccess isreported (bothsuccessful inbothsham-groupand real rTMSgroup)
NS

604
M.
Grall-Bronnec,
A.
Sauvaget /
Neuroscience
and Biobehavioral
Review
s 47
(2014) 592–613
Table 2 (Continued)
Studies Handedness rTMSdevice
Stimulationsite (brainregion)
Method forlocatingcorticaltarget
F (Hz) Method fordetermin-ingRMT
% of RMT Number oftrains
ITI (s) Totalpulses persession
Sessionduration
Sham-TMSprocedures(devices andmethods)
Tolerance/adverseeffects
Barth et al.(2011)
NS Solid focalcoilNeuronetics®
Left PFC 5 cmmethod
10 (HF) S◦ of themotorstrip-examiningthe rightAPBM
100% NS (10 seach)
20 3000 15 min Scalpelectrodesconnected toEpix VT®TENSDSham rTMS coilBlindingsuccessreported(successful,only 40% ofparticipantsguessedcorrectly)
NS
Van den Eyndeet al. (2013)
RH Magstimrapiddevice realfigure-8coil
Left DLPFC 5 cmmethod
10 (HF) S◦ of themotorstrip-examiningthe rightAPBM
110% 20 trains(5 s each)
55 1000 20 min NB: patientswere informedthey would berandomised toeither to shamor real TMS. Atleast, allreceived realTMSBlindingsuccessreported (notsuccessful: allparticipantscorrectlyguessed theirallocation toreal rTMS)
- Physicaldiscomfort forone patient- Description of“slight buzzingin the head”
APBM: Abductor Pollicis Brevis Muscle; DLPFC: DorsoLateral Prefrontal Cortex; EEG: Electro Encephalography Electrode; F: Frequency; HF: High Frequency; ITI: Intertrain Interval; LF: Low Frequency; LH: Left-handed; MC: MotorCortex; MEP: Motor Evoked Potentials; MOC: Motor Cortex; NS: Non Specified; PFC: Prefrontal Cortex; RH: Right-handed; RMT: Resting Motor Treshold; rTMS = repetitive Transcranial Magnetic Stimulation; S◦: Stimulation; SFG:Superior Frontal Gyrus; TENSD: Transcutaneous Electrical Nerve Stimulation Device; vs: versus; 3D-MRI: 3D Magnetic Resonance Imaging.

M. Grall-Bronnec, A. Sauvaget / Neuroscience and Biobehavioral Reviews 47 (2014) 592–613 605
Table 3Main sources of bias in the studies of rTMS in addiction and related disorders.
Selection biasMethod of recruiting subjects (in particular, with or without treatment participants).Duration and severity of the addiction or related disorder.Stage of treatment prior to rTMS (detoxification or continuation of substance use).
Observation biasThe Hawthorne effect.Over or underestimating the intensity of craving.Placebo effect of rTMS itself.Placebo effect of therapeutic trials carried out in the field of addiction and related disorders.Order of the placebo session and active session in a crossover study.Poor targeting of the cerebral area.Insufficient number of pulses and number of sessions.Attrition bias (drop out).Running statistical analyses per protocol.
Confounding biasSociodemographic characteristics: age, gender, ethnicity.Hormonal status.Volume of grey matter.Psychiatric and somatic comorbidities.Handedness.Psychotropic treatments (in particular, continuation of anti-craving drugs during the trial).Duration of the session, which may overlap with the duration required for the craving to subside naturally.Cumulative and persistent effects of rTMS when the interval between two sessions is very short.Sample size.Ability of the treatment-seeking participants to use relapse prevention techniques during cue-induced craving procedure.
N
sC
3
MsiscLmdoeefriA2wncss
3
iTiBa4s
B: All these biases are discussed in Section 4.
tate that identification method that was used (Johann et al., 2003;amprodon et al., 2007; Politi et al., 2008; Walpoth et al., 2008).
.2.3. General design of the sessions and rTMS parametersThe number of sessions also varied from one study to the next.
ost of them (12) studied the effect of rTMS in a single activeession compared with a placebo. One third of the studies exam-ned the effect of rTMS over several sessions, often around a dozenessions. HF was used in most cases, with 10 Hz being the mostommon (10 studies). Only two studies tested LF (Rose et al., 2011;i et al., 2013b). The motor threshold (MT), which in turn deter-ines the intensity of the rTMS was, in most cases (10 of 18),
etermined using the visual method (i.e., by watching mobilisationf the long thumb abductor), a less accurate method than using anlectromyogram (EMG), which was used in two studies (Mishrat al., 2010; Herremans et al., 2012). Six studies did not list detailsor this parameter. The intensity used, as a percentage of resting MT,anged from 90% (5 studies) to 120% (1 study). The majority of stud-es used intensities between 100% (5 studies) and 110% (7 studies).
considerable majority of the studies (12) divided stimulation into0 trains. The inter-train interval, which is also a safety parameter,as greater than 20 s (a maximum of 60 s) in 12 studies. The totalumber of pulsations, which is an essential parameter for rTMS effi-acy (Gershon et al., 2003), was most often set at 1000 or above peression (13 studies). The duration of the session (15–20 min) wastipulated in half of the studies.
.2.4. Sham proceduresThe placebo method is most often described and in most cases
s based on the use of a sham coil (7 studies). Four studies usedranscutaneous Electrical Nerve Stimulation (TENS) as well, whichncreases the effectiveness of the placebo (Walpoth et al., 2008;
arth et al., 2011; Li et al., 2013a, 2013b). Four studies used anctive coil, reducing its activity either by inclination at an angle of5◦–90◦, or by applying a metallic plate to the surface to limit thepread of the magnetic signal. Only four studies noted the efficacyof blinding (Van den Eynde et al., 2010b, 2013; Barth et al., 2011;Claudino et al., 2011).
3.2.5. Safety and toleranceFinally, eight studies did not specify rTMS tolerance, which was
generally good, as shown in four studies in which no side effectswere reported. Only one study reported a case of serious side effects(seizure, probably due to discontinuing benzodiazepine too soon)(Mishra et al., 2010).
4. Discussion
Most studies supported rTMS efficacy, especially in the shortterm, regardless of the comparison with a sham stimulation. A veryrecent meta-analysis argued that non-invasive neurostimulationof the DLPFC decreases craving levels in substance dependence(Jansen et al., 2013). However, its efficacy deserves to be dis-cussed in light of many methodological and technical disparities.All sources of bias, shown in Table 3, will be discussed.
4.1. Methodological issues
4.1.1. Sample size and scope of applicationThe scope of application of rTMS is vast and all of the studies
were limited by small sample sizes. The study completed by Amiazand colleagues had the highest number of subjects (N = 52), but thesample was divided into four groups (Amiaz et al., 2009). To com-pensate for this disadvantage, many studies were carried out witha crossover design to generate greater power. Some articles do notstate the duration or severity of the disorder (Camprodon et al.,2007; Politi et al., 2008; Herremans et al., 2012), whereas thesesame variables could not be taken into consideration statisticallyin the other studies due to their small sample sizes. In particu-
lar, a study of the link between the measurement of craving andthese dimensional variables, or subgroup analyses (i.e., rTMS effi-cacy in “short” versus “long duration of the illness” subgroups),was not performed. Only the study by Li et al. (2013a) found a
6 e and
pncesfies2
4
ghwpdto2etnictmamr2owOttcaowtr
4m2iygeTrc
4whSetawcdf
06 M. Grall-Bronnec, A. Sauvaget / Neuroscienc
ositive correlation between reduced craving and the severity oficotine dependence. Age, gender, the neurotoxic effects of psy-hoactive substances (in particular alcohol) and the neurocognitiveffect of being underweight are all factors that can influence theeverity of the disorder. Some patients had completed detoxi-cation prior to start of the studies (for example: Eichhammert al., 2003), when others had been exposed to cues with thepecific aim of increasing their craving (for example: Uher et al.,005).
.1.2. Characteristics of the participantsThe populations studied were heterogeneous, and this hetero-
eneity may explain the differences in results. Some participantsad a characterised disorder (for example: Mishra et al., 2010),hile others only had a symptom (food craving in healthy peo-le, for example: Uher et al., 2005). Some of them were previouslyetoxified (for example: Herremans et al., 2012), while others con-inued to use a substance (for example: Amiaz et al., 2009). Somef them were undergoing treatment (for example: Hoppner et al.,011), while others were recruited through advertisements (forxample: Eichhammer et al., 2003). In this particular case, the par-icipants wished to quit smoking, but their demand for care wasot entirely spontaneous. They were only enrolled in an exper-
mental protocol using rTMS, and not in a traditional smokingessation programme. The main selection bias was primarily linkedo the way the subjects were recruited. Indeed, noting the treat-
ent status of the participants is a crucial issue, and some authorsrgued that non-treatment seeking addicted participants showedore cue-induced craving than those who were seeking treatment,
esulting in an overestimation of intensity (Wertz and Sayette,001; Wilson et al., 2004). When the participants were seekingr undergoing treatment, it may be assumed that their disordersere more severe and long-standing, alleviating the effect of rTMS.n the other hand, it may be argued that participants undergoing
reatment had learned to self-control their cravings. This was allhe more true when they had received prior psychotherapy. In thisontext, participants could use relapse prevention techniques, suchs thought-stoppage or urge surfing, leading to an underestimationf craving intensity (Wanigaratne et al., 1990). This may interfereith the interpretation of the results, concluding that rTMS is effec-
ive. To our knowledge, participants were not asked to avoid usingelapse prevention techniques during cue-induced craving tasks.
.1.2.1. Age. Elderly subjects and a smaller volume of frontal greyatter are associated with a poorer response to rTMS (Jorge et al.,
008) for patients with vascular depression. Although patientsncluded in the studies we reviewed were rather young (under 60ears old), some of their addictive disorders are known to reducerey matter and cortical thickness (Gallinat et al., 2006; Nakamat al., 2011; Frank et al., 2013; Grodin et al., 2013; Ide et al., 2014).his consequence may falsely diminish rTMS efficacy. Indeed, theTMS magnetic field may not be powerful enough to reach theortical layer.
.1.2.2. Gender. Apart from specific aspects of addiction and RD inomen, which is not the topic of this review, gender differencesave yet to be widely studied in the field of rTMS and addiction.ome gender differences have been shown in depressed rats (Yangt al., 2007) and in schizophrenic humans, with a better responseo rTMS in females (Huber et al., 2003). Moreover, hormonal statusffects the response of treatment-resistant depression to rTMS in
omen (Huang et al., 2008). It may also have an influence on thelinical expression of some addictive conditions, such as bulimicisorders (Lester et al., 2003), and may therefore introduce a con-ounding bias for discussion (Claudino et al., 2011).
Biobehavioral Reviews 47 (2014) 592–613
4.1.3. Main exclusion criteriaPsychiatric and somatic comorbidities may be confounding fac-
tors in assessing rTMS efficacy in addictive conditions. Fortunately,medical conditions are often an exclusion criterion, because theycan be absolute or relative contraindications for rTMS (Rossi et al.,2009). Psychiatric conditions may also interfere. For example, ineating disorders, improving depressive and obsessive–compulsivesymptoms as well as bingeing and purging symptoms may high-light a common physiopathological process rather than the specificefficacy of rTMS (Walpoth et al., 2008).
4.1.3.1. Associated treatments. While some of the studies exam-ined in our review were careful to exclude patients receivingpsychotropic treatments, others included such patients on the con-dition that treatment had been stable for at least two weeks andeven stipulated that ¾ of the patients received anti-craving drugs(such as naltrexone, acamprosate, disulfiram, carbamazepine, orfluoxetine) after completion of the rTMS sessions (Mishra et al.,2010). Prescribing this type of treatment may interfere with theassessment of craving even when the rTMS is carried out some timelater.
4.1.3.2. Handedness. Just one study highlighted the importance ofthis parameter in their results (Van den Eynde et al., 2010a). Halfof the studies do not specify the subjects’ handedness, while theother half looked at right-handed subjects only. This choice is sel-dom justified. Some authors (Mishra et al., 2010) argued that theapplication of HF rTMS to the right DLPFC has been hypothesised toproduce trans-synaptic suppression of the left DLPFC (i.e., the dom-inant hemisphere in right-handed individuals) (Fox et al., 1997).However, others found that applying HF rTMS to the left DLPFCin right-handed individuals also reduced craving (Uher et al., 2005;Van den Eynde et al., 2010b; Li et al., 2013a). These findings suggestthat handedness may not be as important a criterion as has beensuggested. Moreover, in some cases the dominant hemisphere maybe the right one in right-handed individuals. According to someauthors, approximately 95–99% of right-handed individuals haveleft-hemispheric language dominance, as is the case with approxi-mately 70% of left-handed individuals (Corballis, 2014). In contrast,some authors have suggested that left-handed people are morelikely to suffer from mental disorders from childhood (van derHoorn et al., 2010) and addictive disorders later in life (Sperlinget al., 2000). When applied to the left DLPFC, rTMS produces dif-ferent effects in right-handed and left-handed subjects (Van denEynde et al., 2010a). Including left-handed individuals in furtherstudies involves taking these last two facts, clinical and ethicalissues, into account. Indeed, left-handed people should be includedin this research, especially because they may be more likely to sufferfrom mental disorders (van der Hoorn et al., 2010).
4.1.4. Cortical excitabilityrTMS aims to modulate cortical excitability. Its effectiveness
greatly depends on the state of neuronal activation in the targetedbrain region at the time of stimulation (Silvanto and Pascual-Leone,2008). Cortical excitability is determined by a number of factors(Feil and Zangen, 2010), which, alone or in combination, helpchange the level of neuronal activity, thereby changing the resultingeffects of rTMS. It is precisely for this reason that age, gender, men-strual cycle, level of anxiety or mood, sleep deprivation, substance
abuse, thickness of skull layers or brain atrophy, and psychotropictreatments must be accounted for before the start of a study (Rossiet al., 2009). Moreover, ethnicity should be taken into consideration(Yi et al., 2014).
e and
4
rmmsiiIspfi
bieu
iad(etc
4
4
wtasiasthpp
4
esotecwoITn
4
ScmearwW
M. Grall-Bronnec, A. Sauvaget / Neuroscienc
.1.5. DesignMost of the studies carried out to date assessed the efficacy of
TMS in reducing craving as assessed by Visual Analogue Scales (forore detail, see Table 1). While this tool provides a fast measure-ent of craving that can easily be repeated, the measurement is
ubjective and fluctuates over time, as well as being subject to thenfluence of other variables. Less often, the main objective was tonvestigate the effect of rTMS on substance use or eating behaviour.n these cases, the outcome measures were the number of cigarettesmoked or the number of binges and purges. From a therapeuticoint of view, the latter type of studies is more relevant, while therst type may be useful as an exploratory study.
The procedures for inducing craving also varied, sometimeseing controlled by exposure to neutral cues, especially in stud-
es relating to nicotine dependence. Participants may have beenxposed to cues before and after the rTMS session or during stim-lation.
Moreover, attrition bias has also been observed in trials includ-ng several rTMS sessions. One of the most ambitious studies had
design closest to the protocol used to test rTMS efficacy in majorepression and included measurement of the long-term effectAmiaz et al., 2009). It also had the largest number of subjects. How-ver, its results were limited by a high drop-out rate and notably byhe authors’ decision to run statistical analyses per protocol, whichan lead to false positive results.
.2. Technical issues
.2.1. General considerationsFirst, rTMS protocols vary immensely. Sometimes the protocol
as not specified or the description was rather vague, whereashe parameters used can have a direct impact on rTMS efficacynd the results of the study. This may partly explain the occa-ionally contradictory results that emerge from these studies. Its therefore difficult to compare the protocols from different tri-ls, which authors often fail to justify or discuss, especially in oldertudies. Second, the more recent the study was, the more accuratehe description of the protocol. This means that broad comparisonsave to be drawn. Similarly, the same team tends to use the samerotocol, which makes more accurate comparison of the resultsossible.
.2.2. The rTMS deviceThe equipment used may influence the results depending on its
ase of handling and intrinsic characteristics. The coil design is alsoignificant and may interfere with the efficacy of rTMS. The depthf penetration and focality on the clinical target are the two mainechnical features of the coil. Up to now, figure-8 type coils havexhibited the best depth–focality trade-off, compared with circularoils (Deng et al., 2013). Because most of the studies used this veryidespread coil, we think this technical point enhanced the efficacy
f rTMS and is not likely to explain the differences between studies.nterestingly, researchers also recently tested the efficacy of deepMS in behavioural addictions (Rosenberg et al., 2013), which hasot yet been proven.
.2.3. Stimulation site and identification of target siteIn almost all cases, the brain area stimulated was the left DLPFC.
timulation of the DLPFC can induce the release of dopamine in theaudate nucleus (Strafella et al., 2001). Thus, repeated stimulationay induce neuroadaptation in the dopaminergic system (Strafella
t al., 2003). Other target regions such as the right DLPFC or DMPFC
re also starting to be tested (Downar and Daskalakis, 2013). Theight DLPFC was rarely chosen; however, testing this target may bearranted as it is involved in decision making (Knoch et al., 2006).e hypothesise that the left DLPFC was more often tested than theBiobehavioral Reviews 47 (2014) 592–613 607
right DLPFC or others targets because researchers built their firststudies on studies of rTMS and depression. The choice of targetregion, however, is only of relative significance when one consid-ers that rTMS also produces remote effects (Fox et al., 1997; Mishraet al., 2010). rTMS not only produces local effects facing the coilbut also on the ipsi- and contralateral (inter-hemispheric) corti-cal side, either inhibiting (Ferbert et al., 1992; Fox et al., 1997) orfacilitating cortical activity (Fox et al., 1997; Hanajima et al., 2001).Stimulating a target region may also modulate the excitability ofanother one rather than directly stimulating the latter (Rizzo et al.,2004). These findings are also supported by neuroimaging evidence(Bestmann et al., 2005). Moreover, the remote effects of rTMS onfrontal cortical regions have been noticed in deeper cerebral struc-tures, especially in the mesostriatal system, increasing the releaseof dopamine (Keck et al., 2002), and subcortical regions (Hanlonet al., 2013). For example, stimulation of the DLPFC potentiallyincreases dopamine excretion in the ventral striatum (Strafellaet al., 2001). In the same way, SFG is also connected to subcorticalstructures such as the amygdala and striatum (Croxson et al., 2005).Therefore, stimulating the DLPFC or SFG may ultimately both haveremote effects on dopamine release, depending of course on the fre-quency of stimulation. Because dopamine is particularly involved inthe physiopathological processes of addictions and RD, any modu-lation of its neurotransmission activity is probably more importantthan the initial target where the stimulation takes place.
Nevertheless, the link with the decision making process mustbe kept in mind (Bechara, 2005; Redish et al., 2008). The prefrontalcortex is involved in many aspects of cognitive processes includingdecision-making to achieve goal directed behaviours. Moreover, itsactivity depends on motivation to seek treatment (Wilson et al.,2004) and inter-temporal drug availability (McBride et al., 2006;Hayashi et al., 2013), both related to the issue of self-control.
The methods for identifying the target site have varying levelsof precision. The most commonly used, the “5-cm method”, hasbeen criticised because it does not take into account interindivid-ual skull size and anatomical variations in the prefrontal cortex(Herbsman et al., 2009; Johnson et al., 2013). Neuronavigationproved to be a superior target location method for DLPFC com-pared with the “5-cm method” and the “10–20 method” or theinternational EEG system (Rusjan et al., 2010; Bradfield et al., 2012;Kim et al., 2013). Thus, neuronavigational coil positioning seems toincrease the therapeutic effects of rTMS in several diseases such asdepression (Fitzgerald et al., 2009; Schonfeldt-Lecuona et al., 2010;Nauczyciel et al., 2011), auditory hallucinations (Klirova et al., 2013)and pain (Ahdab et al., 2010). However, the research has yet to showevidence for the greater efficacy of rTMS in addictions or RD usingneuronavigation, compared with other coil-positioning methods.
4.2.4. General design of the sessions and rTMS parameters4.2.4.1. Number of sessions. The number of rTMS sessions receivedby the participants ranged from 1 to 15, and was influenced bythe aim of the study and the chosen outcome measures. Changes inbehaviour and long-lasting effects were more often seen in patientsundergoing repeated rTMS sessions. Similar evidence is seen in thetreatment of major depression (Lam et al., 2008). If participantsunderwent several sessions, the interval between the two sessionsvaried from one hour to one week. Little is known about the cumu-lative and persistent effects of rTMS over time in the treatment ofaddictions and RD. These particular effects are usually identified byparallel group trials; however, they may result in misinterpretationif a crossover design is used, particularly when the interval is short(Eichhammer et al., 2003; Johann et al., 2003) or even very short (Li
et al., 2013b).4.2.4.2. Frequency. HF was used in all of the studies, except two(Rose et al., 2011; Li et al., 2013b). As previously mentioned, HF

6 e and
sastwaotbtd(rtbfieiawFiiLt2op
4attsaistpdMpib2
4atiowsIesa2oltarufi
08 M. Grall-Bronnec, A. Sauvaget / Neuroscienc
timulation is considered to have excitatory effects on both leftnd right cortical activity. Regarding the frequency and targetite, most of the studies we reviewed showed that HF appliedo the left DLPFC had positive results on craving or dependence,hereas others found negative results on craving. When HF is
pplied to the right DLPFC, two studies showed a positive effectn craving and only one study found a negative effect. It is unfor-unate that this decision (HF or LF) was not always motivatedy underlying physiopathological hypotheses. When mentioned,he main hypothesis is that HF rTMS has been shown to alteropaminergic neurotransmission in subcortical structuresEichhammer et al., 2003). Researchers sometimes tend toeplicate parameters used by previous teams, without explainingheir own hypothesis. It is only recently that LF protocols haveegun to be tested. Li et al. (2013b) chose LF for two reasons, therst being safety because individuals with a history of MA usuallyxhibit significantly increased cortical excitability and often showncreased seizure susceptibility, and the second was listed simplys “exploratory”. They assumed that LF rTMS, which is inhibitory,ould modulate cravings and perhaps even worsen cravings.
inally, they showed that LF rTMS on the left DLPFC transientlyncreased cue-induced craving in MA participants. Hence, reducingnhibitory control might be one of the possible mechanisms of theF rTMS. Stimulating the right DLPFC with HF rTMS may result inrans-synaptic suppression of the left DLPFC (Camprodon et al.,007; Mishra et al., 2010). Thus we support the idea that the choicef HF or LF in any trial should be made in consideration of otherarameters, especially the target site.
.2.4.3. Motor threshold and the intensity of stimulation. Although visual determination of MT should preferably be avoided, as itends to overestimate the minimal intensity required to activatehe motor cortex (Lefaucheur et al., 2011), it was widely used in thetudies. While rather troublesome to use, the EMG method is moreccurate and, more importantly, can be accurately reproduced. Thentensity of stimulation thus determines rTMS efficacy. Even if thetimulation intensity at the motor cortex gives an accurate result,here is no evidence that this is more optimal than that at therefrontal cortex for therapeutic purposes. However, using visualetermination of the MT could artificially increase the patient’s realT, and lead to a higher intensity rTMS than that predicted by the
rotocol. This could thus result in incorrect interpretations and maynterfere with the safety of rTMS. Over 100% intensity is thought toe a predictive rTMS response factor in depression (Gershon et al.,003). It seems that this is also the case for addiction and RD.
.2.4.4. The number of trains, intertrain interval, numbers of pulses,nd number and duration of sessions. The number of trains, inter-rain intervals and pulses per train should be described more often,n line with safety regulations (Rossi et al., 2009). The total numberf pulses per session was between 1000 and 2000 in most trials,hich seems to be suitable for ensuring effective rTMS. Two recent
tudies actually used 3000 pulses (Barth et al., 2011; Li et al., 2013a).n fact, a figure higher than 1000 is thought to be predictive of rTMSfficacy in depression (Gershon et al., 2003), while the number ofessions is said to determine the efficacy of rTMS in the mediumnd long term (Gershon et al., 2003; Khedr et al., 2005; Amiaz et al.,009). In most of the studies examined here, rTMS was carriedut in a single session. The effects thus seemed to be very short-ived, lasting from a few seconds to a few minutes. The duration ofhe session, which was not always stipulated, is nevertheless also
determining factor in regard to assessing the specific effect of
TMS on craving. The natural progression of craving remains poorlynderstood. According to some authors, craving may be sustainedor 30 min following exposure to cues, with a gradual decreasen intensity (Heishman et al., 2010). It may be hypothesised thatBiobehavioral Reviews 47 (2014) 592–613
under certain conditions (for example, during an excessively longsession), craving intensity may actually diminish naturally over thecourse of a few minutes, and it may instead have been incorrectlyattributed to a specific effect of the rTMS. While this risk does exist,it has largely been mitigated through the design of studies withcontrol groups.
4.2.5. Sham procedureThe quality of the placebo method is a crucial issue. The reliabil-
ity of the results is substantially undermined when authors fail todescribe the placebo method used or to optimise it. Using a shamcoil alone does not create optimum placebo conditions (Loo et al.,2000) because, among other reasons, it does not produce a tac-tile sensation on the face or scalp. Fortunately, the placebo methodhas been gradually improved over time. First, some research teamsused electrical stimulation through the skin on the subjects’ fore-head, over the prefrontal cortex, triggered by the rTMS machineto correspond to sham rTMS pulses (Li et al., 2013a). Second, theelectrical current was titrated to a level matching participants’ rat-ings of real rTMS (Barth et al., 2011; Li et al., 2013a). Third, someresearchers also tested the validity of the sham system at the end ofthe study by asking participants to guess which rTMS session wasreal and which was sham (Barth et al., 2011).
The Hawthorne effect is probably at work when subjects candistinguish between the placebo and the active method. Expres-sions of craving are eminently subjective, and its intensity maybe overestimated or underestimated if the placebo method hasnot been optimised (Brunoni et al., 2009). This was the case formost of the studies, especially where the sham method consistedof simply applying the active coil to the target area at an angleof 45◦–90◦. In this situation, there is probably still slight activity,possibly modulating cortical excitability. There are still too fewstudies examining the reliability of the placebo method througha patient survey (Broadbent et al., 2011). Furthermore, the rTMSplacebo effect may be linked to the disorder being studied and thestudy design rather than the treatment itself (Brunoni et al., 2009).A strong placebo effect is often reported in therapeutic trials carriedout in the field of addiction and RD (Hodgins et al., 2011). Moreover,it has been shown that in crossover studies, a placebo session priorto the active session artificially increases the effect of the latter(Andre-Obadia et al., 2011).
Although blinding efficacy is seldom reported, it is neverthe-less a critical component in determining the magnitude of placeboeffects in controlled rTMS studies. Assessing the efficacy of blindingshould be very helpful for further studies.
4.2.6. Safety and toleranceApart from conventional safety recommendations and respec-
ting the exclusion criteria for rTMS, specific points related toaddictions must be noted (Rossi et al., 2009). First, patients exposedto drugs of abuse often show increased seizure susceptibility, andsecond withdrawal from alcohol or benzodiazepines increases therisk of developing a seizure threshold (Kawasaki et al., 2012; Leachet al., 2012; Ghezzi et al., 2014). Safety, more than tolerance, whichis often good, needs to be balanced with the parameters, especiallythe frequency, number of pulses, intensity, and number of sessions,required to provide rTMS efficacy.
5. Future directions
Overall, the use of rTMS in patients with addictions and RD does
seem to be a promising treatment that merits further research.Nevertheless, this critical review leads us to propose key recom-mendations (Table 4). Neuromodulation may increase cognitivecontrol in various ways, opening up new treatment prospects to
M. Grall-Bronnec, A. Sauvaget / Neuroscience and Biobehavioral Reviews 47 (2014) 592–613 609
Table 4Key recommendations for further studies on rTMS in addiction and related disorders.
Main issues Key recommendations
Clinical and general considerationsLack of treatment and intervention in
addictions and related disordersTesting neuromodulation through rTMS of each addiction and related disorder.
Knowledge of the physiopathology ofaddictions and related disorders
Coupling neuroimaging and functional investigations with rTMS to enhance the knowledge of physiopathology andthen argue the choice of parameters.
Design Developing controlled, randomised, double-blind studies, based on larger sample groups.Replicating trials.Discussing all sources of bias.
Inducing craving procedures Better understanding of the natural fluctuations of craving.Justifying the choice of instant of cue-inducing craving in relation with the rTMS session and assessment.Asking seeking-treatment participants to avoid using relapse prevention techniques during the cue-induced cravingprocedure.
Outcome and assessment criteria Coupling subjective assessment and objective and physiological measurements.Developing other criteria (such as changes in behaviour).Increasing study follow-up to examine the long-lasting effect of rTMS.
Potential indications for rTMS inaddictions and related disorders
Developing clinical (and eventually biological) predictors of treatment outcome.
Technical considerationsComprehensive assessment of the
treatment effect andphysiopathological hypothesis
Measuring neurophysiological and neuroimaging variables regularly throughout the rTMS trial.
Lack of details of rTMS procedures Describing rTMS parameters accurately and justifying them.Handedness Determining handedness carefully using an appropriate questionnaire.
Including left-handed individuals in the studies.rTMS device: type of coil Choosing the appropriate type of coil for the target site (based on its depth of penetration and focality).Stimulation site Testing regions other than the DLPFC.
Using individualised techniques to locate the target site (international EEG system, neuronavigation) to conductreproducible and reliable studies.
rTMS parameters Using a reproducible method to determine the motor threshold, such as the EMG method.Increasing the number of sessions, number of pulses and intensity within a safety context.Choosing HF or LF according to the target site, basing oneself on a physiopathological hypothesis.Specifying session duration so as to discuss it in the light of craving evolution if craving is the main outcome.Giving all the rTMS parameters accurately so as to conduct replicating trials and further meta-analyses.
Sham procedure Using an electrical stimulation.Reporting and discussing blinding success.
Safety and tolerance Systematically reporting safety and tolerance.ng the
h2
hrCpci
AturipsetvwA(
otdds
Considering safety when choosi
elp addicted patients by reducing their craving levels (Jansen et al.,013).
Both the efficacy of this method and real indications for its useas yet to be confirmed. Research should therefore continue byeplicating the trials, with particular attention given to their design.ontrolled, randomised, double-blind studies, based on larger sam-le groups should be standard practice. Some authors recommendarrying out international multicentre studies as a way of overcom-ng recruitment difficulties (Van den Eynde and Guillaume, 2012).
In addition, the choice of main assessment criteria is crucial.ssessing craving using a VAS is extremely subjective and fluc-
uates over time under the influence of many factors. A betternderstanding of the natural fluctuations in cravings is key toeducing factors of confusion. Moreover, the measurement of crav-ng intensity could be coupled with approximate but objective andhysiological measurements of craving (Claudino et al., 2011). Mea-urement of indirect criteria might also be added to this, such asvaluations of a change in behaviour (for example, a reduction inhe number of cigarettes smoked or in the number of binges), pro-ided that the effect of rTMS is evaluated in the medium term, asas done in some of the described studies (Walpoth et al., 2008;miaz et al., 2009) and as is recommended by some researchers
Wing et al., 2012).As previously mentioned, the beneficial effect observed in most
f the studies is only a short-term effect, limiting the interven-
ion’s usefulness. Some authors have conducted studies with theesign used in the treatment of major depression, with repeatedaily sessions of rTMS over a period of several weeks. This designhould provide a long-lasting effect. Several authors argue thatrTMS parameters.
studies should be developed according to this model based on thehypothesis that repeated, frequent sessions will result in changesin cerebral neuroplasticity and generate a long-lasting effect (Vanden Eynde and Guillaume, 2012). Moreover, the use of multiplerTMS sessions per day may also be a promising therapeutic devel-opment, as shown very recently in depression (Baeken et al., 2013).The efficacy of rTMS should be greatly enhanced when the numberof pulses is high (Gershon et al., 2003). In patients with addictionsand RD, several rTMS sessions per day may alleviate efficacy byincreasing the number of pulses. We also hypothesise that it mayreduce craving, a key symptom in addiction, which may occur sev-eral times a day. Safety concerns related to giving several rTMSsessions a day should also be assessed.
Handedness should be considered as one of the inclu-sion/exclusion criteria and subject handedness should be carefullyresearched using an appropriate questionnaire. Including left-handed individuals may improve our understanding of brainfunctioning (Willems et al., 2014).
Developing better knowledge of brain mapping in patients withaddiction may help determine which brain regions other than theDLPFC could be tested. This may not be as important as it appearsbecause of the remote effects of rTMS, which have been discussedabove. Finally, the hemispheric differences of the DLPFC in addic-tion should also be a matter of debate. These unresolved issuesshould be clarified in future studies. They are all the more important
because hemispheric differences in human beings are still beingdiscussed (Corballis, 2014). For this reason, both left- and right-sided rTMS could be compared in the same trial to clarify the roleof the two sides in regulating craving. In the future, identification
6 e and
omicaatIicw
ctpm2ptfta
cncepdciemm
ccmte
ron
C
t
L
R
A
A
A
A
A
10 M. Grall-Bronnec, A. Sauvaget / Neuroscienc
f the target area may rely on methods other than the “5-cm”ethod, as evidenced by the superior efficacy of neuronavigation
n the treatment of depression. This statement must be taken veryarefully because to date, no evidence of the superiority of neuron-vigation has yet been found for rTMS in patients with addictionsnd RD. LF rTMS on both the right and left DLPFC should be testedo specify more precisely whether it might influence craving or not.nhibition by LF in regions in which hyperactivity is discovered dur-ng craving induction, especially the right DLPFC (Wang et al., 2007)ould be interesting. LF is all the more interesting for safety reasons,ith a lower risk of seizure compared with HF.
The intensity of treatment and the number of pulses per sessionould be increased and still remain in line with safety regula-ions (Rossi et al., 2009). Optimising and standardising stimulationarameters does present a challenge but is a necessary step thatany authors have called for (Barr et al., 2008; Feil and Zangen,
010; Diana, 2011; Wing et al., 2012). Detailed descriptions of therotocols used in the articles would enhance the repeatability ofhese trials and thus facilitate comparisons of the results of dif-erent studies. This would be a first step towards meta-analyseshat would be useful for interpreting results as suggested by someuthors (Van den Eynde and Guillaume, 2012).
Moreover, clinical and non-clinical predictors of treatment out-omes must be determined to provide more detailed indications ofeuromodulation. To our knowledge, only one study reached theonclusion that rTMS had a more intense effect on heavy smok-rs than light smokers (Li et al., 2013a) (for a description of thearameters, see Table 2). In other areas, work on outcome pre-ictors identified exogenic and endogenic factors. Variability inortical excitability may also be linked to genetic characteristics,n the same way that responses to medications can be influ-nced by genetic variability (Sturgess et al., 2011). In contrast, theodulation of several genes may be involved in the therapeuticechanisms of rTMS (Ikeda et al., 2013).Finally, physiological measurements, such as electroen-
ephalography, PET-scan or fMRI, should be associated withlinical studies to enhance our knowledge of the underlyingechanisms of both addictions and RD, particularly concerning
he dopaminergic brain reward systems and rTMS action (Pripflt al., 2013b).
Implementation of these recommendations would allow neu-omodulation through rTMS to take its place in the spectrumf therapeutic strategies, alongside other neuromodulation tech-iques, psychotherapies and pharmacotherapies.
onflict of interest
The authors report no financial or other relationship relevant tohe subject of this article.
We thank Gaëlle Challet-Bouju, Anne-Franc oise Goalic, Tiannaoose and Véronique Sébille-Rivain for their help.
eferences
chab, S., Khazaal, Y., 2011. Psychopharmacological treatment in pathological gam-bling: a critical review. Curr. Pharm. Des. 17, 1389–1395.
ddolorato, G., Leggio, L., Hopf, F.W., Diana, M., Bonci, A., 2012. Novel therapeu-tic strategies for alcohol and drug addiction: focus on GABA, ion channels andtranscranial magnetic stimulation. Neuropsychopharmacology 37, 163–177.
hdab, R., Ayache, S.S., Brugieres, P., Goujon, C., Lefaucheur, J.P., 2010. Compari-son of standard and navigated procedures of TMS coil positioning over motor,premotor and prefrontal targets in patients with chronic pain and depression.Neurophysiol. Clin. 40, 27–36.
miaz, R., Levy, D., Vainiger, D., Grunhaus, L., Zangen, A., 2009. Repeated high-frequency transcranial magnetic stimulation over the dorsolateral prefrontalcortex reduces cigarette craving and consumption. Addiction 104, 653–660.
ndre-Obadia, N., Magnin, M., Garcia-Larrea, L., 2011. On the importance of placebotiming in rTMS studies for pain relief. Pain 152, 1233–1237.
Biobehavioral Reviews 47 (2014) 592–613
Avena, N.M., Bocarsly, M.E., 2012. Dysregulation of brain reward systems in eat-ing disorders: neurochemical information from animal models of binge eating,bulimia nervosa, and anorexia nervosa. Neuropharmacology 63, 87–96.
Baczynski, T., de Aquino Chaim, C., Nazar, B., Carta, M., Arias-Carrion, O., Silva, A.,Machado, S., Nardi, A.E., 2014. High-Frequency rTMS to Treat Refractory BingeEating Disorder and Comorbid Depression: A Case Report. CNS Neurol DisordDrug Targets.
Baeken, C., Vanderhasselt, M.A., Remue, J., Herremans, S., Vanderbruggen, N.,Zeeuws, D., Santermans, L., De Raedt, R., 2013. Intensive HF-rTMS treatmentin refractory medication-resistant unipolar depressed patients. J. Affect. Disord.151, 625–631.
Barker, A.T., 1999. The history and basic principles of magnetic nerve stimulation.Electroencephalogr. Clin. Neurophysiol. Suppl. 51, 3–21.
Barr, M.S., Farzan, F., Rusjan, P.M., Chen, R., Fitzgerald, P.B., Daskalakis, Z.J., 2009.Potentiation of gamma oscillatory activity through repetitive transcranialmagnetic stimulation of the dorsolateral prefrontal cortex. Neuropsychophar-macology 34, 2359–2367.
Barr, M.S., Farzan, F., Wing, V.C., George, T.P., Fitzgerald, P.B., Daskalakis, Z.J., 2011.Repetitive transcranial magnetic stimulation and drug addiction. Int. Rev. Psy-chiatry 23, 454–466.
Barr, M.S., Fitzgerald, P.B., Farzan, F., George, T.P., Daskalakis, Z.J., 2008. Transcra-nial magnetic stimulation to understand the pathophysiology and treatment ofsubstance use disorders. Curr. Drug Abuse Rev. 1, 328–339.
Barth, K.S., Rydin-Gray, S., Kose, S., Borckardt, J.J., O’Neil, P.M., Shaw, D., Madan,A., Budak, A., George, M.S., 2011. Food cravings and the effects of left prefrontalrepetitive transcranial magnetic stimulation using an improved sham condition.Front Psychiatry 2, 9.
Bechara, A., 2005. Decision making, impulse control and loss of willpower to resistdrugs: a neurocognitive perspective. Nat. Neurosci. 8, 1458–1463.
Bellamoli, E., Manganotti, P., Schwartz, R.P., et al., 2014. rTMS in the treatment ofdrug addiction: an update about human studies. Behav. Neurol. 2014, Article ID815215, 11 pages.
Bersani, F.S., Minichino, A., Enticott, P.G., Mazzarini, L., Khan, N., Antonacci, G., Rac-cah, R.N., Salviati, M., Delle Chiaie, R., Bersani, G., Fitzgerald, P.B., Biondi, M., 2013.Deep transcranial magnetic stimulation as a treatment for psychiatric disorders:a comprehensive review. Eur. Psychiatry 28, 30–39.
Bestmann, S., Baudewig, J., Siebner, H.R., Rothwell, J.C., Frahm, J., 2005. BOLD MRIresponses to repetitive TMS over human dorsal premotor cortex. Neuroimage28, 22–29.
Bolt, D.M., Piper, M.E., Theobald, W.E., Baker, T.B., 2012. Why two smoking cessationagents work better than one: role of craving suppression. J. Consult. Clin. Psychol.80, 54–65.
Bou Khalil, R., El Hachem, C., 2013. Potential role of repetitive transcra-nial magnetic stimulation in obesity. Eat. Weight Disord., http://dx.doi.org/10.1007/s40519-013-0088-x, Epub 2013 Dec 11.
Bradfield, N.I., Reutens, D.C., Chen, J., Wood, A.G., 2012. Stereotaxic localisation of thedorsolateral prefrontal cortex for transcranial magnetic stimulation is superiorto the standard reference position. Aust. N. Z. J. Psychiatry 46, 232–239.
Broadbent, H.J., van den Eynde, F., Guillaume, S., Hanif, E.L., Stahl, D., David, A.S.,Campbell, I.C., Schmidt, U., 2011. Blinding success of rTMS applied to the dor-solateral prefrontal cortex in randomised sham-controlled trials: a systematicreview. World J. Biol. Psychiatry 12, 240–248.
Brunoni, A.R., Lopes, M., Kaptchuk, T.J., Fregni, F., 2009. Placebo response of non-pharmacological and pharmacological trials in major depression: a systematicreview and meta-analysis. PLoS ONE 4, e4824.
Camprodon, J.A., Martinez-Raga, J., Alonso-Alonso, M., Shih, M.C., Pascual-Leone, A.,2007. One session of high frequency repetitive transcranial magnetic stimula-tion (rTMS) to the right prefrontal cortex transiently reduces cocaine craving.Drug Alcohol Depend. 86, 91–94.
Camus, M., Halelamien, N., Plassmann, H., Shimojo, S., O’Doherty, J., Camerer, C.,Rangel, A., 2009. Repetitive transcranial magnetic stimulation over the rightdorsolateral prefrontal cortex decreases valuations during food choices. Eur. J.Neurosci. 30, 1980–1988.
Cho, S.S., Strafella, A.P., 2009. rTMS of the left dorsolateral prefrontal cortexmodulates dopamine release in the ipsilateral anterior cingulate cortex andorbitofrontal cortex. PLoS ONE 4, e6725.
Claudino, A.M., Van den Eynde, F., Stahl, D., Dew, D., Andiappan, M., Kalthoff, J.,Schmidt, U., Campbell, I.C., 2011. Repetitive transcranial magnetic stimula-tion reduces cortisol concentrations in bulimic disorders. Psychol. Med. 41,1329–1336.
Corballis, M.C., 2014. Left brain, right brain: facts and fantasies. PLoS Biol. 12,e1001767.
Cota, D., Tschop, M.H., Horvath, T.L., Levine, A.S., 2006. Cannabinoids, opioids andeating behavior: the molecular face of hedonism? Brain Res. Rev. 51, 85–107.
Cowin, R.L., Avena, N.M., Boggiano, M.M., 2011. Feeding and reward: perspectivesfrom three rat models of binge eating. Physiol. Behav. 104, 87–97.
Crockford, D.N., Goodyear, B., Edwards, J., Quickfall, J., el-Guebaly, N., 2005. Cue-induced brain activity in pathological gamblers. Biol. Psychiatry 58, 787–795.
Croxson, P.L., Johansen-Berg, H., Behrens, T.E., Robson, M.D., Pinsk, M.A., Gross, C.G.,
Richter, W., Richter, M.C., Kastner, S., Rushworth, M.F., 2005. Quantitative inves-tigation of connections of the prefrontal cortex in the human and macaque usingprobabilistic diffusion tractography. J. Neurosci. 25, 8854–8866.Curtis, C., Davis, C., 2014. A qualitative study of binge eating and obesity from anaddiction perspective. Eat. Disord. 22, 19–32.
e and
D
D
D
D
D
D
D
D
E
F
F
F
F
F
F
G
G
G
G
G
G
G
G
G
H
H
H
H
H
M. Grall-Bronnec, A. Sauvaget / Neuroscienc
askalakis, Z.J., Moller, B., Christensen, B.K., Fitzgerald, P.B., Gunraj, C., Chen, R., 2006.The effects of repetitive transcranial magnetic stimulation on cortical inhibitionin healthy human subjects. Exp. Brain Res. 174, 403–412.
avis, C., 2013. A narrative review of binge eating and addictive behaviors: sharedassociations with seasonality and personality factors. Front Psychiatry 4, 183.
e Ridder, D., Vanneste, S., Kovacs, S., Sunaert, S., Dom, G., 2011. Transient alcoholcraving suppression by rTMS of dorsal anterior cingulate: an fMRI and LORETAEEG study. Neurosci. Lett. 496, 5–10.
eng, Z.D., Lisanby, S.H., Peterchev, A.V., 2013. Electric field depth-focality tradeoffin transcranial magnetic stimulation: simulation comparison of 50 coil designs.Brain Stimul. 6, 1–13.
iana, M., 2011. The dopamine hypothesis of drug addiction and its potential ther-apeutic value. Front Psychiatry 2, 64.
ickson, S.L., Egecioglu, E., Landgren, S., Skibicka, K.P., Engel, J.A., Jerlhag, E., 2011.The role of the central ghrelin system in reward from food and chemical drugs.Mol. Cell. Endocrinol. 340, 80–87.
ownar, J., Daskalakis, Z.J., 2013. New targets for rTMS in depression: a review ofconvergent evidence. Brain Stimul. 6, 231–240.
ownar, J., Sankar, A., Giacobbe, P., Woodside, B., Colton, P., 2012. Unanticipatedrapid remission of refractory bulimia nervosa, during high-dose repetitive trans-cranial magnetic stimulation of the dorsomedial prefrontal cortex: a case report.Front Psychiatry 3, 30.
ichhammer, P., Johann, M., Kharraz, A., Binder, H., Pittrow, D., Wodarz, N., Hajak,G., 2003. High-frequency repetitive transcranial magnetic stimulation decreasescigarette smoking. J. Clin. Psychiatry 64, 951–953.
eil, J., Zangen, A., 2010. Brain stimulation in the study and treatment of addiction.Neurosci. Biobehav. Rev. 34, 559–574.
erbert, A., Priori, A., Rothwell, J.C., Day, B.L., Colebatch, J.G., Marsden, C.D., 1992.Interhemispheric inhibition of the human motor cortex. J. Physiol. 453, 525–546.
itzgerald, P.B., Hoy, K., Daskalakis, Z.J., Kulkarni, J., 2009. A randomized trial ofthe anti-depressant effects of low- and high-frequency transcranial magneticstimulation in treatment-resistant depression. Depress. Anxiety 26, 229–234.
ox, P., Ingham, R., George, M.S., Mayberg, H., Ingham, J., Roby, J., Martin, C., Jer-abek, P., 1997. Imaging human intra-cerebral connectivity by PET during TMS.NeuroReport 8, 2787–2791.
rank, G.K., Shott, M.E., Hagman, J.O., Mittal, V.A., 2013. Alterations in brain struc-tures related to taste reward circuitry in ill and recovered anorexia nervosa andin bulimia nervosa. Am. J. Psychiatry 170, 1152–1160.
ranklin, T., Wang, Z., Suh, J.J., Hazan, R., Cruz, J., Li, Y., Goldman, M., Detre,J.A., O’Brien, C.P., Childress, A.R., 2011. Effects of varenicline on smoking cue-triggered neural and craving responses. Arch. Gen. Psychiatry 68, 516–526.
allinat, J., Meisenzahl, E., Jacobsen, L.K., Kalus, P., Bierbrauer, J., Kienast, T., Wit-thaus, H., Leopold, K., Seifert, F., Schubert, F., Staedtgen, M., 2006. Smoking andstructural brain deficits: a volumetric MR investigation. Eur. J. Neurosci. 24,1744–1750.
earhardt, A.N., White, M.A., Potenza, M.N., 2011. Binge eating disorder and foodaddiction. Curr. Drug Abuse Rev. 4, 201–207.
eorge, M.S., Post, R.M., 2011. Daily left prefrontal repetitive transcranial magneticstimulation for acute treatment of medication-resistant depression. Am. J. Psy-chiatry 168, 356–364.
ershon, A.A., Dannon, P.N., Grunhaus, L., 2003. Transcranial magnetic stimulationin the treatment of depression. Am. J. Psychiatry 160, 835–845.
hezzi, A., Krishnan, H.R., Atkinson, N.S., 2014. Susceptibility to ethanol with-drawal seizures is produced by BK channel gene expression. Addict. Biol. 19,332–337.
oldman, M., Szucs-Reed, R.P., Jagannathan, K., Ehrman, R.N., Wang, Z., Li, Y., Suh, J.J.,Kampman, K., O’Brien, C.P., Childress, A.R., Franklin, T.R., 2013. Reward-relatedbrain response and craving correlates of marijuana cue exposure: a preliminarystudy in treatment-seeking marijuana-dependent subjects. J. Addict. Med. 7,8–16.
oodman, A., 1990. Addiction: definition and implications. Br. J. Addict. 85,1403–1408.
oodman, A., 2008. Neurobiology of addiction. An integrative review. Biochem.Pharmacol. 75, 266–322.
rodin, E.N., Lin, H., Durkee, C.A., Hommer, D.W., Momenan, R., 2013. Deficits in cor-tical, diencephalic and midbrain gray matter in alcoholism measured by VBM:effects of co-morbid substance abuse. Neuroimage Clin. 2, 469–476.
anajima, R., Ugawa, Y., Machii, K., Mochizuki, H., Terao, Y., Enomoto, H.,Furubayashi, T., Shiio, Y., Uesugi, H., Kanazawa, I., 2001. Interhemispheric facil-itation of the hand motor area in humans. J. Physiol. 531, 849–859.
anlon, C.A., Canterberry, M., Taylor, J.J., DeVries, W., Li, X., Brown, T.R., George,M.S., 2013. Probing the frontostriatal loops involved in executive and limbicprocessing via interleaved TMS and functional MRI at two prefrontal locations:a pilot study. PLoS ONE 8, e67917.
ausmann, A., Mangweth, B., Walpoth, M., Hoertnagel, C., Kramer-Reinstadler,K., Rupp, C.I., Hinterhuber, H., 2004. Repetitive transcranial magnetic stimu-lation (rTMS) in the double-blind treatment of a depressed patient sufferingfrom bulimia nervosa: a case report. Int. J. Neuropsychopharmacol. 7, 371–373.
ayashi, T., Ko, J.H., Strafella, A.P., Dagher, A., 2013. Dorsolateral prefrontal andorbitofrontal cortex interactions during self-control of cigarette craving. Proc.
Natl. Acad. Sci. U. S. A. 110, 4422–4427.eishman, S.J., Lee, D.C., Taylor, R.C., Singleton, E.G., 2010. Prolonged duration ofcraving, mood, and autonomic responses elicited by cues and imagery in smok-ers: effects of tobacco deprivation and sex. Exp. Clin. Psychopharmacol. 18,245–256.
Biobehavioral Reviews 47 (2014) 592–613 611
Herbsman, T., Avery, D., Ramsey, D., Holtzheimer, P., Wadjik, C., Hardaway, F.,Haynor, D., George, M.S., Nahas, Z., 2009. More lateral and anterior prefrontal coillocation is associated with better repetitive transcranial magnetic stimulationantidepressant response. Biol. Psychiatry 66, 509–515.
Herremans, S.C., Baeken, C., Vanderbruggen, N., Vanderhasselt, M.A., Zeeuws, D.,Santermans, L., De Raedt, R., 2012. No influence of one right-sided prefrontalHF-rTMS session on alcohol craving in recently detoxified alcohol-dependentpatients: results of a naturalistic study. Drug Alcohol Depend. 120, 209–213.
Hodgins, D.C., Stea, J.N., Grant, J.E., 2011. Gambling disorders. Lancet 378 (9806),1874–1884.
Hoppner, J., Broese, T., Wendler, L., Berger, C., Thome, J., 2011. Repetitive transcranialmagnetic stimulation (rTMS) for treatment of alcohol dependence. World J. Biol.Psychiatry 12 (Suppl. 1), 57–62.
Huang, C.C., Wei, I.H., Chou, Y.H., Su, T.P., 2008. Effect of age, gender, menopausalstatus, and ovarian hormonal level on rTMS in treatment-resistant depression.Psychoneuroendocrinology 33, 821–831.
Huber, T.J., Schneider, U., Rollnik, J., 2003. Gender differences in the effect of repet-itive transcranial magnetic stimulation in schizophrenia. Psychiatry Res. 120,103–105.
Ide, J.S., Zhang, S., Hu, S., Sinha, R., Mazure, C.M., Li, C.S., 2014. Cerebral gray mattervolumes and low-frequency fluctuation of BOLD signals in cocaine dependence:duration of use and gender difference. Drug Alcohol Depend. 134, 51–62.
Ikeda, T., Kurosawa, M., Morimoto, C., Kitayama, S., Nukina, N., 2013. Multiple effectsof repetitive transcranial magnetic stimulation on neuropsychiatric disorders.Biochem. Biophys. Res. Commun. 436, 121–127.
Jansen, J.M., Daams, J.G., Koeter, M.W., Veltman, D.J., van den Brink, W., Goudriaan,A.E., 2013. Effects of non-invasive neurostimulation on craving: a meta-analysis.Neurosci. Biobehav. Rev. 37, 2472–2480.
Jean, A., Laurent, L., Bockaert, J., Charnay, Y., Dusticier, N., Nieoullon, A., Barrot, M.,Neve, R., Compan, V., 2012. The nucleus accumbens 5-HTR(4)-CART pathwayties anorexia to hyperactivity. Transl. Psychiatry 2, e203.
Johann, M., Wiegand, R., Kharraz, A., Bobbe, G., Sommer, G., Hajak, G., Wodarz, N.,Eichhammer, P., 2003. Transcranial magnetic stimulation for nicotine depend-ence. Psychiatr. Prax. 30 (Suppl. 2), S129L 131.
Johnson, K.A., Baig, M., Ramsey, D., Lisanby, S.H., Avery, D., McDonald, W.M., Li, X.,Bernhardt, E.R., Haynor, D.R., Holtzheimer 3rd, P.E., Sackeim, H.A., George, M.S.,Nahas, Z., 2013. Prefrontal rTMS for treating depression: location and intensityresults from the OPT-TMS multi-site clinical trial. Brain Stimul. 6, 108–117.
Jorge, R.E., Moser, D.J., Acion, L., Robinson, R.G., 2008. Treatment of vascular depres-sion using repetitive transcranial magnetic stimulation. Arch. Gen. Psychiatry65, 268–276.
Kawasaki, S.S., Jacapraro, J.S., Rastegar, D.A., 2012. Safety and effectiveness of afixed-dose phenobarbital protocol for inpatient benzodiazepine detoxification.J. Subst. Abuse Treat. 43, 331–334.
Kaye, W.H., Wierenga, C.E., Bailer, U.F., Simmons, A.N., Wagner, A., Bischoff-Grethe,A., 2013. Does a shared neurobiology for foods and drugs of abuse contributeto extremes of food ingestion in anorexia and bulimia nervosa? Biol. Psychiatry73, 836–842.
Keck, M.E., Welt, T., Muller, M.B., Erhardt, A., Ohl, F., Toschi, N., Holsboer, F., Sillaber,I., 2002. Repetitive transcranial magnetic stimulation increases the release ofdopamine in the mesolimbic and mesostriatal system. Neuropharmacology 43,101–109.
Khedr, E.M., Kotb, H., Kamel, N.F., Ahmed, M.A., Sadek, R., Rothwell, J.C., 2005.Longlasting antalgic effects of daily sessions of repetitive transcranial magneticstimulation in central and peripheral neuropathic pain. J. Neurol. Neurosurg.Psychiatry 76, 833–838.
Kim, W.J., Min, Y.S., Yang, E.J., Paik, N.J., 2013. Neuronavigated vs. conventionalrepetitive transcranial magnetic stimulation method for virtual lesioning on theBroca’s area. Neuromodulation 17, 16–21.
Kinzl, J.F., Biebl, W., 2010. Are eating disorders addictions? Neuropsychiatry 24,200–208.
Klirova, M., Horacek, J., Novak, T., Cermak, J., Spaniel, F., Skrdlantova, L., Mohr,P., Hoschl, C., 2013. Individualized rTMS neuronavigated according to regionalbrain metabolism ((18)FGD PET) has better treatment effects on auditory hal-lucinations than standard positioning of rTMS: a double-blind, sham-controlledstudy. Eur. Arch. Psychiatry Clin. Neurosci. 263, 475–484.
Knoch, D., Gianotti, L.R., Pascual-Leone, A., Treyer, V., Regard, M., Hohmann, M., Brug-ger, P., 2006. Disruption of right prefrontal cortex by low-frequency repetitivetranscranial magnetic stimulation induces risk-taking behavior. J. Neurosci. 26,6469–6472.
Kobayashi, M., Pascual-Leone, A., 2003. Transcranial magnetic stimulation in neu-rology. Lancet Neurol. 2, 145–156.
Koob, G.F., Volkow, N.D., 2010. Neurocircuitry of addiction. Neuropsychopharma-cology 35, 217–238.
Lam, R.W., Chan, P., Wilkins-Ho, M., Yatham, L.N., 2008. Repetitive transcranial mag-netic stimulation for treatment-resistant depression: a systematic review andmetaanalysis. Can. J. Psychiatry 53, 621–631.
Le Moal, M., Koob, G.F., 2007. Drug addiction: pathways to the disease and patho-physiological perspectives. Eur. Neuropsychopharmacol. 17, 377–393.
Leach, J.P., Mohanraj, R., Borland, W., 2012. Alcohol and drugs in epilepsy: patho-physiology, presentation, possibilities, and prevention. Epilepsia 53 (Suppl. 4),
48–57.Lefaucheur, J.P., Andre-Obadia, N., Poulet, E., Devanne, H., Haffen, E., Londero, A.,Cretin, B., Leroi, A.M., Radtchenko, A., Saba, G., Thai-Van, H., Litre, C.F., Vercueil,L., Bouhassira, D., Ayache, S.S., Farhat, W.H., Zouari, H.G., Mylius, V., Nicolier, M.,Garcia-Larrea, L., 2011. French guidelines on the use of repetitive transcranial

6 e and
L
L
L
L
M
M
M
M
M
M
M
M
M
N
N
N
OP
P
P
P
P
P
P
P
R
R
R
12 M. Grall-Bronnec, A. Sauvaget / Neuroscienc
magnetic stimulation (rTMS): safety and therapeutic indications. Neurophysiol.Clin. 41, 221–295.
ester, N.A., Keel, P.K., Lipson, S.F., 2003. Symptom fluctuation in bulimia ner-vosa: relation to menstrual-cycle phase and cortisol levels. Psychol. Med. 33,51–60.
i, X., Hartwell, K.J., Owens, M., Lematty, T., Borckardt, J.J., Hanlon, C.A., Brady, K.T.,George, M.S., 2013a. Repetitive transcranial magnetic stimulation of the dor-solateral prefrontal cortex reduces nicotine cue craving. Biol. Psychiatry 73,714–720.
i, X., Malcolm, R.J., Huebner, K., Hanlon, C.A., Taylor, J.J., Brady, K.T., George, M.S.,See, R.E., 2013b. Low frequency repetitive transcranial magnetic stimulation ofthe left dorsolateral prefrontal cortex transiently increases cue-induced crav-ing for methamphetamine: a preliminary study. Drug Alcohol Depend. 133 (2),641–646.
oo, C.K., Taylor, J.L., Gandevia, S.C., McDarmont, B.N., Mitchell, P.B., Sachdev, P.S.,2000. Transcranial magnetic stimulation (TMS) in controlled treatment studies:are some sham forms active? Biol. Psychiatry 47, 325–331.
arco, A., Schroeder, M., Weller, A., 2012. Feeding and reward: ontogenetic changesin an animal model of obesity. Neuropharmacology 62, 2447–2454.
arhe, R., Waters, A.J., van de Wetering, B.J., Franken, I.H., 2013. Implicit andexplicit drug-related cognitions during detoxification treatment are associatedwith drug relapse: an ecological momentary assessment study. J. Consult. Clin.Psychol. 81, 1–12.
ariani, J.J., Levin, F.R., 2012. Psychostimulant treatment of cocaine dependence.Psychiatr. Clin. N. Am. 35, 425–439.
cBride, D., Barrett, S.P., Kelly, J.T., Aw, A., Dagher, A., 2006. Effects of expectancyand abstinence on the neural response to smoking cues in cigarette smokers: anfMRI study. Neuropsychopharmacology 31, 2728–2738.
cClelland, J., Bozhilova, N., Campbell, I., Schmidt, U., 2013a. A systematic reviewof the effects of neuromodulation on eating and body weight: evidence fromhuman and animal studies. Eur. Eat. Disord. Rev. 21, 436–455.
cClelland, J., Bozhilova, N., Nestler, S., Campbell, I.C., Jacob, S., Johnson-Sabine,E., Schmidt, U., 2013b. Improvements in symptoms following neuronavigatedrepetitive transcranial magnetic stimulation (rTMS) in severe and enduringanorexia nervosa: findings from two case studies. Eur Eat Disord. Rev. 21,500–506.
cGrath, D.S., Dorbeck, A., Barrett, S.P., 2013. The influence of acutely administerednicotine on cue-induced craving for gambling in at-risk video lottery terminalgamblers who smoke. Behav. Pharmacol. 24 (2), 124–132.
ishra, B.R., Nizamie, S.H., Das, B., Praharaj, S.K., 2010. Efficacy of repetitive trans-cranial magnetic stimulation in alcohol dependence: a sham-controlled study.Addiction 105, 49–55.
uller, C.A., Geisel, O., Banas, R., Heinz, A., 2011. Current pharmacological treat-ment approaches for alcohol dependence. Expert Opin. Pharmacother. 15,471–481.
akama, H., Chang, L., Fein, G., Shimotsu, R., Jiang, C.S., Ernst, T., 2011. Metham-phetamine users show greater than normal age-related cortical gray matter loss.Addiction 106, 1474–1483.
ardone, R., Bergmann, J., Christova, M., Lochner, P., Tezzon, F., Golaszewski, S.,Trinka, E., Brigo, F., 2012. Non-invasive brain stimulation in the functional eval-uation of alcohol effects and in the treatment of alcohol craving: a review.Neurosci. Res. 74, 169–176.
auczyciel, C., Hellier, P., Morandi, X., Blestel, S., Drapier, D., Ferre, J.C., Barillot, C.,Millet, B., 2011. Assessment of standard coil positioning in transcranial magneticstimulation in depression. Psychiatry Res. 186, 232–238.
’Brien, C., 2011. Addiction and dependence in DSM-V. Addiction 106, 866–867.ascual-Leone, A., Valls-Sole, J., Wassermann, E.M., Hallett, M., 1994. Responses to
rapid-rate transcranial magnetic stimulation of the human motor cortex. Brain117 (Pt. 4), 847–858.
oliti, E., Fauci, E., Santoro, A., Smeraldi, E., 2008. Daily sessions of transcranial mag-netic stimulation to the left prefrontal cortex gradually reduce cocaine craving.Am. J. Addict. 17, 345–346.
otenza, M.N., 2014a. Non-substance addictive behaviors in the context of DSM-5.Addict. Behav. 39, 1–2.
otenza, M.N., 2014b. Obesity, food, and addiction: emerging neuroscience and clin-ical and public health implications. Neuropsychopharmacology 39, 249–250.
otenza, M.N., Hong, K.I., Lacadie, C.M., Fulbright, R.K., Tuit, K.L., Sinha, R., 2012.Neural correlates of stress-induced and cue-induced drug craving: influences ofsex and cocaine dependence. Am. J. Psychiatry 169, 406–414.
otenza, M.N., Sofuoglu, M., Carroll, K.M., Rounsaville, B.J., 2011. Neuroscience ofbehavioral and pharmacological treatments for addictions. Neuron 69, 695–712.
ripfl, J., Neumann, R., Kohler, U., Lamm, C., 2013a. Effects of transcranial directcurrent stimulation on risky decision making are mediated by ‘hot’ and ‘cold’decisions, personality, and hemisphere. Eur. J. Neurosci. 38, 3778–3785.
ripfl, J., Tomova, L., Riecansky, I., Lamm, C., 2013b. Transcranial mag-netic stimulation of the left dorsolateral prefrontal cortex decreasescue-induced nicotine craving and EEG delta power. Brain Stimul.,http://dx.doi.org/10.1016/j.brs.2013.11.003, Epub 2013 Nov 16.
edish, A.D., Jensen, S., Johnson, A., 2008. A unified framework for addiction: vul-nerabilities in the decision process. Behav. Brain Sci. 31, 415–437, discussion437–487.
idding, M.C., Rothwell, J.C., 2007. Is there a future for therapeutic use of transcranialmagnetic stimulation? Nat. Rev. Neurosci. 8, 559–567.
izzo, V., Siebner, H.R., Modugno, N., Pesenti, A., Munchau, A., Gerschlager, W., Webb,R.M., Rothwell, J.C., 2004. Shaping the excitability of human motor cortex withpremotor rTMS. J. Physiol. 554, 483–495.
Biobehavioral Reviews 47 (2014) 592–613
Rose, J.E., McClernon, F.J., Froeliger, B., Behm, F.M., Preud’homme, X., Krystal, A.D.,2011. Repetitive transcranial magnetic stimulation of the superior frontal gyrusmodulates craving for cigarettes. Biol. Psychiatry 70, 794–799.
Rosenberg, O., Klein, L.D., Dannon, P.N., 2013. Deep transcranial magnetic stimula-tion for the treatment of pathological gambling. Psychiatry Res. 206, 111–113.
Rossi, S., Hallett, M., Rossini, P.M., Pascual-Leone, A., 2009. Safety, ethicalconsiderations, and application guidelines for the use of transcranial mag-netic stimulation in clinical practice and research. Clin. Neurophysiol. 120,2008–2039.
Rossi, S., Rossini, P.M., 2004. TMS in cognitive plasticity and the potential for reha-bilitation. Trends Cogn. Sci. 8, 273–279.
Rusjan, P.M., Barr, M.S., Farzan, F., Arenovich, T., Maller, J.J., Fitzgerald, P.B.,Daskalakis, Z.J., 2010. Optimal transcranial magnetic stimulation coil placementfor targeting the dorsolateral prefrontal cortex using novel magnetic resonanceimage-guided neuronavigation. Hum. Brain Mapp. 31, 1643–1652.
Schonfeldt-Lecuona, C., Lefaucheur, J.P., Cardenas-Morales, L., Wolf, R.C., Kammer,T., Herwig, U., 2010. The value of neuronavigated rTMS for the treatment ofdepression. Neurophysiol. Clin. 40, 37–43.
Silvanto, J., Pascual-Leone, A., 2008. State-dependency of transcranial magneticstimulation. Brain Topogr. 21, 1–10.
Skinner, M.D., Aubin, H.J., 2010. Craving’s place in addiction theory: contributionsof the major models. Neurosci. Biobehav. Rev. 34, 606–623.
Speranza, M., Revah-Levy, A., Giquel, L., Loas, G., Venisse, J.L., Jeammet, P., Corcos,M., 2012. An investigation of Goodman’s addictive disorder criteria in eatingdisorders. Eur. Eat. Disord. Rev. 20, 182–189.
Sperling, W., Franck, H., Martus, P., Mader, R., Barocka, A., Walter, H., Lesch, M.,2000. The concept of abnormal hemispheric organization in addiction research.Alcohol Alcohol. 35, 394–399.
Staroverov, A.T., Zhukov, O.B., Raigorodskii, Y.M., 2009. Efficacy of transcranialmagnetotherapy in the complex treatment of alcohol withdrawal syndrome.Neurosci. Behav. Physiol. 39, 891–895.
Strafella, A.P., Paus, T., Barrett, J., Dagher, A., 2001. Repetitive transcranial magneticstimulation of the human prefrontal cortex induces dopamine release in thecaudate nucleus. J. Neurosci. 21, RC157.
Strafella, A.P., Paus, T., Fraraccio, M., Dagher, A., 2003. Striatal dopamine releaseinduced by repetitive transcranial magnetic stimulation of the human motorcortex. Brain 126, 2609–2615.
Sturgess, J.E., George, T.P., Kennedy, J.L., Heinz, A., Muller, D.J., 2011. Pharmaco-genetics of alcohol, nicotine and drug addiction treatments. Addict. Biol. 16,357–376.
Sussman, S., Lisha, N., Griffiths, M., 2011. Prevalence of the addictions: a problem ofthe majority or the minority? Eval. Health Prof. 34, 3–56.
Tassinari, C.A., Cincotta, M., Zaccara, G., Michelucci, R., 2003. Transcranial magneticstimulation and epilepsy. Clin. Neurophysiol. 114, 777–798.
Uher, R., Yoganathan, D., Mogg, A., Eranti, S.V., Treasure, J., Campbell, I.C.,McLoughlin, D.M., Schmidt, U., 2005. Effect of left prefrontal repetitivetranscranial magnetic stimulation on food craving. Biol. Psychiatry 58,840–842.
Umberg, E.N., Shader, R.I., Hsu, L.K., Greenblatt, D.J., 2012. From disordered eatingto addiction: the food drug in bulimia nervosa. J. Clin. Psychopharmacol. 32,376–389.
Van den Eynde, F., Broadbent, H., Guillaume, S., Claudino, A., Campbell, I.C., Schmidt,U., 2010a. Handedness, repetitive transcranial magnetic stimulation and bulimicdisorders. Eur. Psychiatry 27, 290–293.
Van den Eynde, F., Claudino, A.M., Mogg, A., Horrell, L., Stahl, D., Ribeiro, W., Uher,R., Campbell, I., Schmidt, U., 2010b. Repetitive transcranial magnetic stimula-tion reduces cue-induced food craving in bulimic disorders. Biol. Psychiatry 67,793–795.
Van den Eynde, F., Guillaume, S., 2012. Neuromodulation techniques and eatingdisorders. Int. J. Eat. Disord., http://dx.doi.org/10.1002/eat.22100.
Van den Eynde, F., Guillaume, S., Broadbent, H., Campbell, I.C., Schmidt, U., 2013.Repetitive transcranial magnetic stimulation in anorexia nervosa. A pilot study.Eur. Psychiatry 28, 98–101.
van der Hoorn, A., Oldehinkel, A.J., Ormel, J., Bruggeman, R., Uiterwaal, C.S., Burger, H.,2010. Non-right-handedness and mental health problems among adolescentsfrom the general population. The Trails Study. Laterality 15, 304–316.
Van Holst, R.J., Van den Brink, W., Veltman, D.J., Goudriaan, A.E., 2010. Brain imagingstudies in pathological gambling. Curr. Psychiatry Rep. 12, 418–425.
Veilleux, J.C., Conrad, M., Kassel, J.D., 2013. Cue-induced cigarette craving and mixedemotions: a role for positive affect in the craving process. Addict. Behav. 38,1881–1889.
Volkow, N.D., O’Brien, C.P., 2007. Issues for DSM-V: should obesity be included as abrain disorder? Am. J. Psychiatry 164, 708–710.
Volkow, N.D., Wang, G.J., Tomasi, D., Baler, R.D., 2013. The addictive dimensionalityof obesity. Biol. Psychiatry 73, 811–818.
Walpoth, M., Hoertnagl, C., Mangweth-Matzek, B., Kemmler, G., Hinterholzl, J.,Conca, A., Hausmann, A., 2008. Repetitive transcranial magnetic stimulation inbulimia nervosa: preliminary results of a single-centre, randomised, double-blind, sham-controlled trial in female outpatients. Psychother. Psychosom. 77,57–60.
Wang, Z., Faith, M., Patterson, F., Tang, K., Kerrin, K., Wileyto, E.P., Detre, J.A., Lerman,
C., 2007. Neural substrates of abstinence-induced cigarette cravings in chronicsmokers. J. Neurosci. 27, 14035–14040.Wanigaratne, S., Wallace, W., Pullin, J., Keaney, F., Farmer, R., 1990. Relapse Pre-vention For Addictive Behaviors: A Manual For Therapists. Blackwell ScientificPublishers, London.

e and
W
WW
WW
W
W
Yi, X., Fisher, K.M., Lai, M., Mansoor, K., Bicker, R., Baker, S.N., 2014. Differencesbetween Han Chinese and Caucasians in transcranial magnetic stimulation
M. Grall-Bronnec, A. Sauvaget / Neuroscienc
assermann, E.M., Lisanby, S.H., 2001. Therapeutic application of repetitive trans-cranial magnetic stimulation: a review. Clin. Neurophysiol. 112, 1367–1377.
atson, J.B., 1913. Psychology as the behaviorist views it. Psychol. Rev. 20, 158–177.ertz, J.M., Sayette, M.A., 2001. A review of the effects of perceived drug use oppor-
tunity of self-reported urge. Exp. Clin. Psychopharmacol. 9, 3–13.HO, 2014. Clinical Trials. http://wwwwhoint/topics/clinical trials/en/illems, R.M., der Haegen, L.V., Fisher, S.E., Francks, C., 2014. On the other hand:
including left-handers in cognitive neuroscience and neurogenetics. Nat. Rev.Neurosci. 15, 193–201.
ilson, S.J., Sayette, M.A., Fiez, J.A., 2004. Prefrontal responses to drug cues: a neu-rocognitive analysis. Nat. Neurosci. 7, 211–214.
ing, V.C., Bacher, I., Wu, B.S., Daskalakis, Z.J., George, T.P., 2012. High fre-quency repetitive transcranial magnetic stimulation reduces tobacco cravingin schizophrenia. Schizophr. Res. 139, 264–266.
Biobehavioral Reviews 47 (2014) 592–613 613
Wing, V.C., Barr, M.S., Wass, C.E., Lipsman, N., Lozano, A.M., Daskalakis, Z.J., George,T.P., 2013. Brain stimulation methods to treat tobacco addiction. Brain Stimul.6, 221–230.
Yang, Y., Li, W., Zhu, B., Liu, Y., Yang, B., Wang, H., Wang, Z., 2007. Sex differ-ences in antidepressant-like effect of chronic repetitive transcranial magneticstimulation in rats. Prog. Neuropsychopharmacol. Biol. Psychiatry 31, 735–740.
parameters. Exp. Brain Res. 232, 545–553.Young, M.M., Wohl, M.J., 2009. The Gambling Craving Scale: psychometric validation
and behavioral outcomes. Psychol. Addict. Behav. 23, 512–522.
Related Documents











