Documenta Ophthalmologica 43,1 : 31-44, 1977 THE USE OF MINI- AND MICRO-COMPUTERS IN EYE CLINICAL PRACTICE G. FRUGONE, E. GIANNOTTI, P. MORASSO, V. TAGLIASCO & T. VERNAZZA (Genoa, Italy) ABSTRACT In an ophthalmological department there are many sectors in which the use of computers can give useful support. We have singled out three major areas of interest: 1. the rationalization of the flow of patients; 2. the management of clinical records; 3. the automatization of ophthalmological devices. Instead of using different dedicated computational systems we preferred to focus our attention on a unique system based on a minicomputer driving several parallel micro- processors. Preliminary results are given. INTRODUCTION The Bioengineering Unit of the Electrical Engineering Department is at present working with the Eye Clinic Department of Genoa University on problems connected with the introduction of computer techniques in clinical practice. The technical and scientific aspects that will be dealt with refer only to a situation where university eye clinics may constitute ophthal- mological centers organized on a regional basis, as in the Italian Health System: for that reason our approach is strongly biased and perhaps lacks generality. Our main objective was to use only one computational system as a uni- fying element for several methodologies and applications in the eye clinic environment. In Fig. 1 the three major areas of interest are singled out: the automation of some ophthalmological devices, the automation of clinical records and the automation of other services (e.g. accounting, out-patient scheduling, etc.). In the following only the first two points will be discussed in detail. Instead of using differently dedicated computational systems, our attention was focused on the use and design of devices without any com- putational or logical capability, by giving the computer these tasks. There- fore, we have chosen a computer configuration based on a minicomputer connected to a set of microprocessors (Fig. 2); this set of microprocessors 31

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Documenta Ophthalmologica 43,1 : 31-44, 1977
THE USE OF MINI- AND MICRO-COMPUTERS IN EYE CLINICAL PRACTICE
G. FRUGONE, E. GIANNOTTI, P. MORASSO, V. TAGLIASCO & T. VERNAZZA
( Genoa, Italy)
ABSTRACT
In an ophthalmological department there are many sectors in which the use of computers can give useful support. We have singled out three major areas of interest: 1. the rationalization of the flow of patients; 2. the management of clinical records; 3. the automatization of ophthalmological devices. Instead of using different dedicated computational systems we preferred to focus our attention on a unique system based on a minicomputer driving several parallel micro- processors. Preliminary results are given.
INTRODUCTION
The Bioengineering Unit of the Electrical Engineering Department is at present working with the Eye Clinic Department of Genoa University on problems connected with the introduction of computer techniques in clinical practice. The technical and scientific aspects that will be dealt with refer only to a situation where university eye clinics may constitute ophthal- mological centers organized on a regional basis, as in the Italian Health System: for that reason our approach is strongly biased and perhaps lacks generality.
Our main objective was to use only one computational system as a uni-
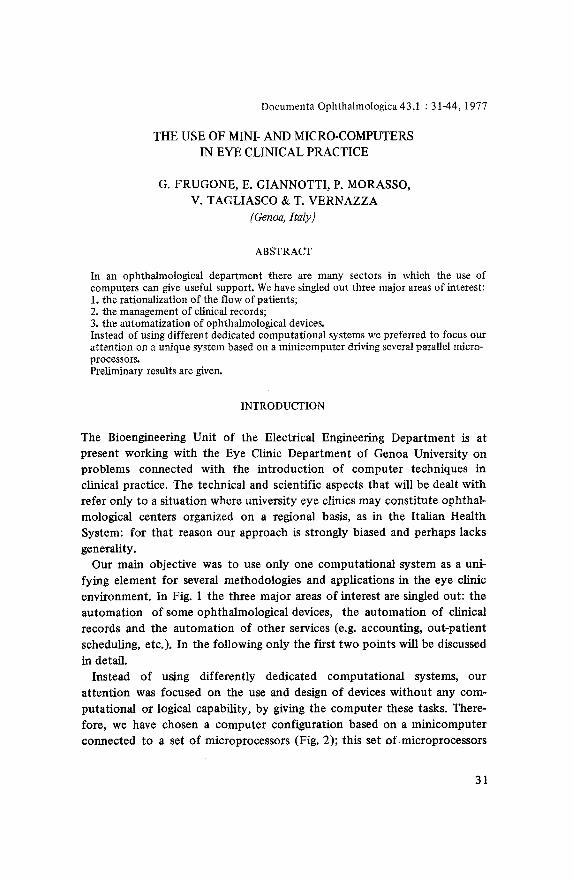
fying element for several methodologies and applications in the eye clinic environment. In Fig. 1 the three major areas of interest are singled out: the automation of some ophthalmological devices, the automation of clinical
records and the automation of other services (e.g. accounting, out-patient scheduling, etc.). In the following only the first two points will be discussed
in detail. Instead of using differently dedicated computational systems, our
attention was focused on the use and design of devices without any com-
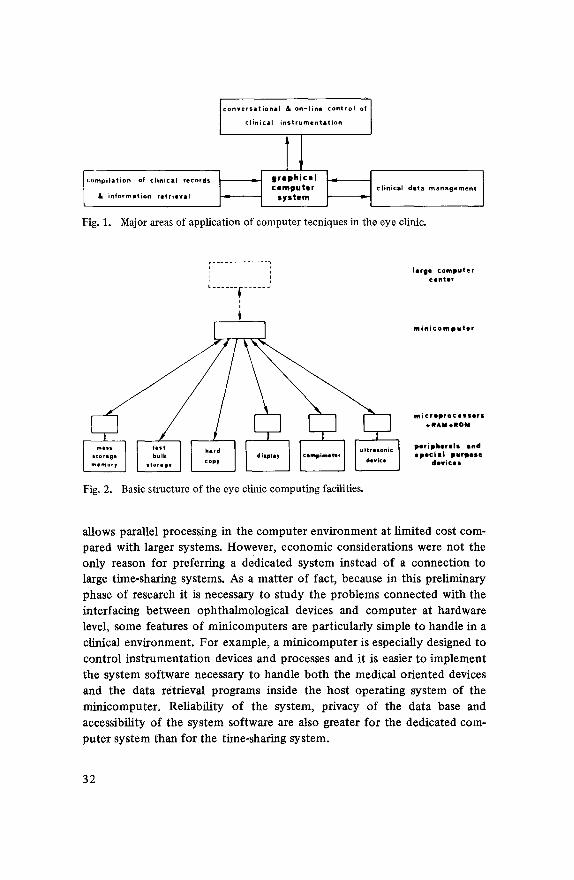
putational or logical capability, by giving the computer these tasks. There- fore, we have chosen a computer configuration based on a minicomputer connected to a set of microprocessors (Fig. 2); this set of microprocessors
31
c o n v e r s a t i o n a l & on-line control of I c in ica nstrumentat on I
I TI c o m p u t e r clinical deta management
L & in fo rma t ion wetrieval s y s t e m
Fig. 1. Major areas of application of computer tecniques in the eye clinic.
r . . . . . . . . . . . . . 1 I i
I
t . . . . . . ~- . . . . . "
,,
Fig, 2. Basic structure of the eye clinic computing facilities.
large computer Ceflter
m i n i c o m p u t e r
microprocessors §
peripherals and spec ia l purpose
devices
allows parallel processing in the computer environment at limited cost com- pared with larger systems. However, economic considerations were not the only reason for preferring a dedicated system instead of a connection to large time-sharing systems. As a matter of fact, because in this preliminary phase of research it is necessary to study the problems connected with the interfacing between ophthalmological devices and computer at hardware level, some features of minicomputers are particularly simple to handle in a clinical environment. For example, a minicomputer is especially designed to
control instrumentation devices and processes and it is easier to implement the system software necessary to handle both the medical oriented devices and the data retrieval programs inside the host operating system of the minicomputer~ Reliability of the system, privacy of the data base and accessibility of the system software are also greater for the dedicated com-
puter system than for the time-sharing system.
32
ON LINE CONTROL OF OPHTHALMOLOGICAL TESTS
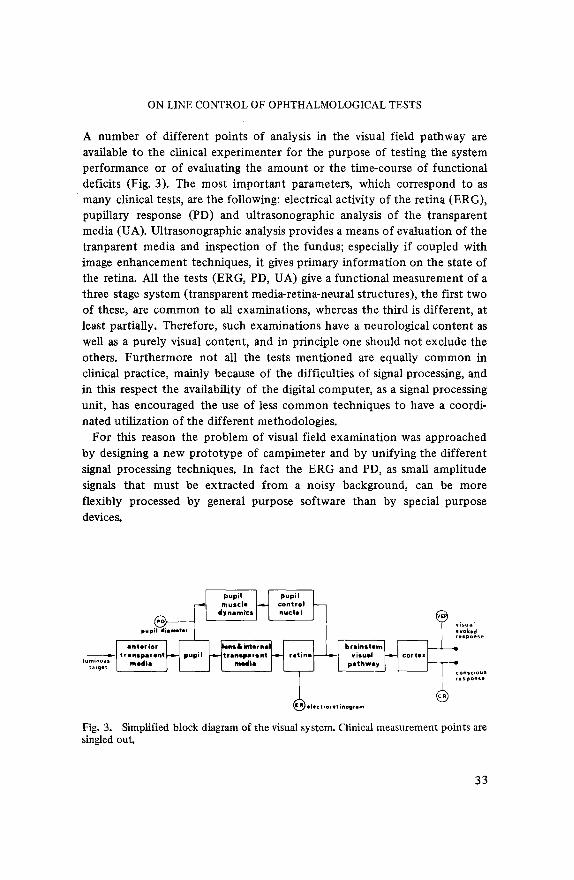
A number of different points of analysis in the visual field pathway are available to the clinical experimenter for the purpose of testing the system performance or of evaluating the amount or the time-course of functional deficits (Fig. 3). The most important parameters, which correspond to as many clinical tests, are the following: electrical activity of the retina (ERG), pupillary response (PD) and ultrasonographic analysis of the transparent media (UA). Ultrasonographic analysis provides a means of evaluation of the tranparent media and inspection of the fundus; especially if coupled with image enhancement techniques, it gives primary information on the state of the retina. All the tests (ERG, PD, UA) give a functional measurement of a three stage system (transparent media-retina-neural structures), the first two of these, are common to all examinations, whereas the third is different, at least partially. Therefore, such examinations have a neurological content as well as a purely visual content, and in principle one should not exclude the others. Furthermore not all the tests mentioned are equaUy common in clinical practice, mainly because of the difficulties of signal processing, and in this respect the availability of the digital computer, as a signal processing unit, has encouraged the use of less common techniques to have a coordi- nated utilization of the different methodologies.
For this reason the problem of visual field examination was approached by designing a new proto type of campimeter and by unifying the different signal processing techniques. In fact the ERG and PD, as small amplitude signals that must be extracted from a noisy background, can be more flexibly processed by general purpose software than by special purpose devices.
pupil iameter evoked response
cortex I �9
conscious response
t~.~/electroretlnogram
Fig. 3. Simplified block diagram of the visual system. Clinical measurement points are singled out.
33
Role o f the computer in visual field examination
The rationale in the use of a computer as a controller for the campimeter
can be summarized as follows. The visual field test must have a short duration, but this time reduction
must not cause any deterioration of the reliability of the test: the attributes of sensitivity and repeatability must be maintained. Finally, for correct differential diagnosis and for a more accurate characterization of initial
pathological trends, the results have to be memorized in numerical form. The first improvement induced by the introduction of computers is the
elimination of the systematic errors due to the operator. Secondly, the computer can partially suppress, in kinetic campimetry, the error due to the latency time of the subject's response (which consists of pressing a push
button). Nevertheless, the main task of the computer refers to the possibility to
choose the optimal strategy for target projection. An operator who analyzes the maps, acts as a pattern recognizer; he compares the new map with some stereotyped maps previously organized, even if this organization and classifi- cation is very often not established on mathematical bases. If standard maps categorized according to refractive state, pupil diameter, age etc., are stored
in the computer system, the appropriate strategies for target presentation can be chosen and the test can offer more data for the same time duration. According to the strategy of the target presentation, the trajectories are initially chosen as functions of the patient's parameters, but they can be modified during the test, depending on the results. The last task of the computer consists of memorization, comparison and quantification of the graphical results. In this context a display connected to the computer can promptly interact with the medical operator by allowing comparison of the last campimetric test with the previous tests (in order to study the develop- ment of the patient's state in quantitative terms) or with some pre-defined
normal situation.
Implementation o f a controller o f the campimeter using a microprocessor INTEL 8080
To implement the automatization of the campimetric examination we have used a small dedicated system (based on a microprocessor) connected with the central minicomputer. In the subdivision of functions between the two computing units we have used the criteria of delegating the real time control to the microprocessor and the information storage and retrieval to the mini- computer. Accordingly the minicomputer is provided with all the necessary
34
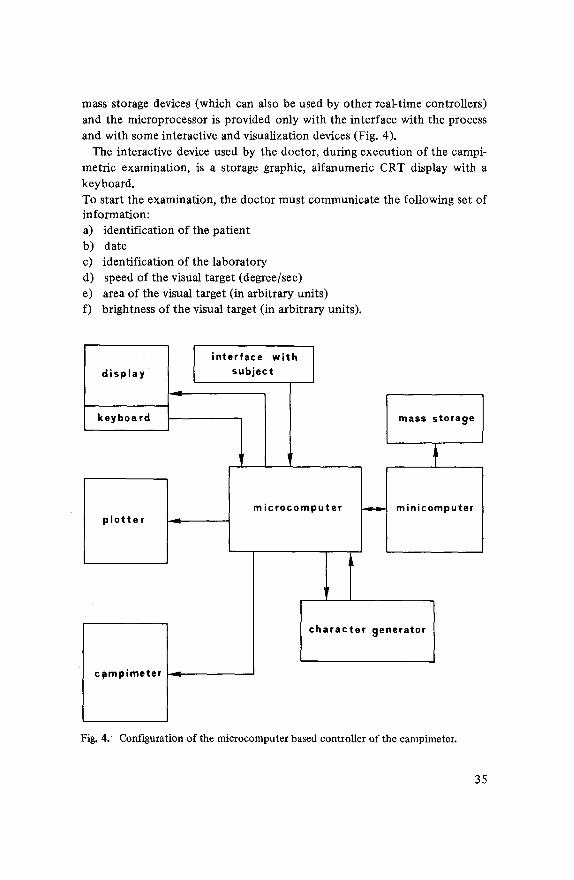
mass storage devices (which can also be used by other real-time controllers) and the microprocessor is provided only with the interface with the process and with some interactive and visualization devices (Fig. 4).
The interactive device used by the doctor, during execution of the campi- metric examination, is a storage graphic, alfanumeric CRT display with a keyboard. To start the examination, the doctor must communicate the following set of information: a) identification of the patient b) date c) identification of the laboratory d) speed of the visual target (degree/sec) e) area of the visual target (in arbitrary units) f) brightness of the visual target (in arbitrary units).
interface with display I subject
keyboard
plotter I---~
c~mpimeter ~.~
mass storage
microcomputer ~ minicomputer
character 9enerator
Fig. 4. Configuration of the microcomputer based controller of the campimeter.
35
Data a), b), c) are used only as labels of the examination to be displayed on the CRT display and on the plot ter at the end of the examination and are transmitted to the minicomputer for permanent storage. Data d), e), f) are parameters for the real t ime controller. If more than one level of bright- ness is indicated, the levels are sorted and the examination is repeated from the highest to the lowest level.
During the execution of the examination the microprocessor moves the spot along one of 24 equally spaced meridians which are chosen at random. Perception of the target is communicated by the patient by means of a push-button, which gives access to the computer through an interface in interrupt mode. For any percepted target the microprocessor stores the parameters of the trajectory (in polar coordinates) and of the target (bright- ness and area) and proceeds to trace another trajectory.
The computer also performs a congruence check of the patient 's response. If some response is 'strange' (which can be due to a lesion but also to a lack of attention), the same trajectory is presented several times, and the re- sponse is stored for good if repeated at least three times.
At the end of the examination the system draws (using a bidimensional interpolat ion routine) the campimetric map on the CRT display and/or the plot ter (for a hard copy).
The doctor can then issue additional commands for the storage of the examination, or for retrieval and display of previous examinations and of the patient 's clinical record.
If some part of the generated map is ambiguous and the doctor decides to have further details, he can restart the examination which will be executed as it was described above, with the additional specification of a new central posit ion from which the trajectories must be initiated.
COMPUTER AUTOMATION OF OPHTHALMOLOGICAL CLINICAL RECORDS
The need for computer management of clinical records was first raised by the introduct ion of the computer in the control of complex ophthalmolo- gical tests (like campimetry) and by the problem of storing and retrieving such information in an appropriate way. Therefore, we have to stress that our approach to the problem of clinical records is strongly biased toward the eye clinic.
The two main functions that we at tr ibuted to the system were: (a ) the conversational retrieval of single clinical records (including graphical in- formation) in a simplified t ime-shared environment, which allows a few doctors (less than eight) to act simultaneously, and ( b ) t h e statistical
36
retrieval from tile data base, according to a conversational inquiry system. The basic constraints which guided our implementat ion were both economic (the use of a minicomputer with less than 32K words of core memory) and psychological, i.e. the need of having an appropriate interface between the system and the medical personnel.
Codification of clinical records
In general, the information which is stored in a clinical record falls into one of the following classes: (a) information that can be expressed using a fixed format, whether numerical (e.g. quantitative results of laboratory analysis) or hteral (eog. anagraphical information); (b)graphic information, deriving from medical test instruments; (c) descriptive information, that needs the use of natural language (e.g. diagnosis, anamnesis, etc.).
From the point of view of the computer only the fixed-format informa- tion of the first class needs a careful standardization, after which pro- gramming becomes a trivial routine. In the case of graphic information, without discussing the possibility of microfilm reproduction and retrieval, it is necessary to convert such information to a numerical (first class) form or to a descriptive one (third class). The former solution, of course, is prefer- able and its implementation is very much facilitated if the clinical examina- tions are managed directly by the computer, but this is not always possible. The information of the third class (descriptive information) is the hardest to deal with, from the point of view of computer automation, because it uses natural language.
The compIexity of the problem would be drastically reduced if we could list all the possible descriptive phrases or if we could find a convenient way to express them with well-defined sequences of fixed format units. How- ever, if this approach is workable in the case of general purpose clinical records, which can be considered as a set formed by a large amount of items of small complexity, it seems more difficult in the case of the eye clinic records, characterized by a relatively small amount of rather complex items.
Therefore, we chose to save much of the free-format structure of the records, as they are now, by introducing as few restrictions as possible. Basically, restrictions can be set either at syntactical level or at lexical level. Both solutions were studied and we found that the more acceptable one, for the clinical environment, was to use a hmited vocabulary for the descriptive parts of the records and to allow, at the same time, natural language syntax.
In this context a first dictionary of medical terms for glaucoma was developed: From statistical analysis performed on a set of clinical records it was found that the number of dictionary entries extends to about two
37

hundred. They consist of substantives, adjectives, verbs and adverbs. Each entry of the dictionary is formed by three parts: (a) the word itself, (b) its internal coding, (c) its class (verb, adjective, etc.).
Codification of clinical records is actually carried out by an Interpreter whose functions are the following: a) articles are deleted in a preprocessing phase b) verbs are identified and, depending on the information gathered from dictionary, the Interpreter decides whether to maintain or to delete them c) prepositions, conjunctions and other syntactic connectives are used to build a corresponding tree whose leaves point to the information (i.e. nouns, adjectives, adverbs, etc.) Contained in the parsed sentence.
Then this tree, which is a memory structured core image of the input string, is temporal ly stored in the core memory. All trees are linked together and only in the last phase dumped on magnetic tape with the other pieces of information. Numeric strings, which are written according to the rules of a regular language ( type 3 language according to the well-known Chomsky's classification), are processed by another module of the Interpreter (a simple finite state automaton) which accepts input strings as: 'TONO := 66 MMHG PILO 2% hfa 2;' and outputs a structure fulfilling the rules adopted by the Interpreter in the processing of the purely textual strings. The structure arising from the above mentioned sentence, is shown in Fig. 5.
Mass storage support
The criterion we used was to choose a support which could contain at least one year of patients ' records (i.e. about 2000 new records) and the choice was for a 9-track magnetic tape. The most straightforward way to code and store the clinical records on the tape is to reserve a file for each patient and
Fig. 5.
torlo /
66 p tono
hfa m m H g ] 66 mmH~ pilo ~-~---~ meas un "
2 % 2 hfa
Example of codification and storage of clinical records.
38
to accumulate in it the information (fixed and free-format) of all visits as out-patient and of all hospitalizations, ordered by date.
From the hardware point of view at least two tape transports are neces- sary to allow for retrieval of records from different tapes. Since the com- puter must contemporaneously serve the queuing of medical doctors' requests, the searching process of records on tapes and the control of special devices, such as campimeters, it is necessary to decentralize the simple, but time consuming processes like tape-searching to microprocessors driven by programs resident in ROMs (or PROMs)~ A fast storage of limited capacity is also useful to hold dictionaries (medical term dictionary and connective term dictionary), the patients' directory and so on. A new attractive solu- tion to this problem, alternative to the classical use of fixed head disks (high price) or moving head disks (low reliability for the clinical environment) is to use banks of RAMs or of shift registers, organized for example in such a way to simulate a fixed head disk.
Retrieval o f clinica ! records and inquiry system
Answering questions about the data base, formed by the whole set of coded clinical records, is perhaps the most useful application of the computer in the eye clinic. A delicate point in the inquiry system is the interface be-
tween the medical doctor and the computer. Such interface must be as flexible as possible and it must allow the doctor to ask questions in a very simple way. To this purpose we are presently working on the definition of a special language according to which the data base can be enquired.
Basically, the phrases of the inquiry language are commands written according to the production rules of a type-2 grammar. The lexicon which is used is the same restricted medical term dictionary, according to which medical records are compiled by doctors. The information, which can be referred by the commands, falls into three classes: integer or real numeral quantities, string variables and conditional boolean variables.
Whilst syntax techniques have been widely employed for translating general purpose language programming, less attention has been paid up to now the use of these methods for other purposes, such as on-line inter- rogation of data bases. In the clinical environment, where we are faced with the need for a highly flexible retrieval language, a fixed format query does not seem suitable to fulfil our requirements. Therefore, it is perfectly reasonable to try other techniques; syntax techniques, both for translating query language and for issuing appropriate directives to the computer, appear more and more promising.
Our design was to provide a partial on line retrieval system for simple
39
questions while, for more difficult questions, a more economical use of the computer can only be achieved by batching enquiries and answering all of them in a single sweep of the data base. Of course, this implies an off-line retrieval system~
Data structure in clinical records
The concept of a record in the form of a list of trees has been introduced. Each piece of information (i.e. a string of letters concerning something about the clinical record) is stored within the patient 's file as a leaf of a tree, whose physical structure depends on the hierarchical relations existing among the words of the given sentence. These relations depend on the syntactic connectives that are present in the parsed sentence. Also, numeric information is stored with this method, therefore - as regards the inquiry s y s t e m - there is no difference between textual and numeric data. This allows the inquiry system to treat the whole content of a patient 's file in the s a m e m a n n e r .
Syntactic analyzer
The Interpreter of the inquiry system consists of a 'Syntactic analyzer routine' (SAR) which scans the input string and recognizes the logical rela- tionships among the words, and of a 'Data building routine' (DBR) which, following the instructions of the SAR, gets the appropriate tree and stores the collected codified information in its leaves. Finally, all trees are linked together and stored in the subsection of the patient 's f i le known as 'Objective examination' . Other sections of the record (fixed format informa- tion) are stored separately in the same file. This task is carried out by another modulus of the Interpreter which stores the string as well, as it is received. To save memory, each word belonging to this subsection, is codified internally as a real double precision number before its memoriza- tion. The employed method ensures a 'one-to-one correspondence' between the number and the word. The saving of memory is really very impressive even if this is paid for by the slow process of decoding each number into the relative word. Finally, the pat ient 's file which is still in core memory, is dumped on magnetic tape and the patient directory is updated.
Inquiry system
There are two major sections of the inquiry: the on-line modulus and the off-line modulus. The on-line modulus allows fast retrieval of data, but it
40
can execute only simple tasks such as retrieval of a specified patient 's record or sections of this record or his whole clinical history. More complex tasks are faced by the off-line modulus, when time considerations are not rele- vanto This job subdivision makes interleaving of multiple requests easier.
One of the shortcomings of the mass storage we have chosen stems from its sequentiality. Indeed, the simplest type of accessing data is sequential, but in this case each file is accessed in contiguous blocks equal to the logical record size. One cannot access or write logical record randomly; the next record to be accessed or written must immediately follow the one previous- ly accessed or written~ The system locates the file (i.e. its physical position) by the use of a table called 'File directory' . This table is stored in the beginning of the tape and, to increase search speed, it is part ly copied in the high core memory when the system is running. An important factor which affects the size of the core resident directory is the number of memory words available between the last word address of the currently running program and the address of the last user. This clearly depends on the size of the computer core memory.
To simplify these tasks, the system dumps the entries of the file directory relative to the most recent records as far as it is possible to fill the free memory. When a file is requested, whose directory entry is not core resi- dent, the system recognizes the search failure and then it dumps another section of the tape directory into core. This operation goes on until the requested file is located. Of course, each new section of the tape directory overlays the oldest entries of the core resident directory.
Requests which may be sent to the inquiry system are of two types: a) immediately executable orders (i.e. search of a pat ient 's record, etc.) b) boolean orders (orders whose execution depends on the validity of a compound boolean statement). Boolean directives are satisfied in batch processing.
The system recognizes the request type and takes appropriate actions. Requests of type (a) are immediately honoured while requests of type (b) are delayed until the system is in the executable state; i.e. they are satisfied only when the computer does not accomplish other priori ty tasks like patient monitoring, instrumentat ion control and data entry.
BNF syntax of the inquiry system
The syntax of the language employed by the inquiry system has the follow- ing structure:
~'~command) : : = ~retrieval command) [ ~etrieval command) <:boolean condition) I ~retrievat command)<'-.choice)
41
(retrieval command> : : = (o rder> (object of order> (o rder> : : = PRINT I LIST I APPEND [ . . . . (object of order> : : = I NAME AND SURNAME I DIRECTORY I ALL I
I ALL PATIENTS I /-.choice>: : = WITH (expression> (expression>:: = ( t e s t > I ( t es t><log op>(expression> ( t e s t > : : = ~qual i f ier>~quant> <'..qualifier> : : = SMALLEST [ GREATEST [ NORMAL [ ABNORMAL [ <boolean condition~: : =/--.log cond>l/--.boolean condition>/-.log cond> <log cond>: : = /-~rel cond><log o p > ( r e l cond>l <log op><log cond> I
/-dog cond>/---.log o p > ( r e l cond> ( t e l cond> : : = (member>/-4el op>/--.rnember> [ ~member> <~.jnember> : : = ~ a a m e > ( d a t e > [ ~"-.adj>~.name> ( n a m e > : : = (orgart~ [/--.status>[ ( q u a n t > [ ~"-.adj>~-aaame> /---.data~ : : = ( n u m string> I ( n u m st~ing>"--aneas un> ~rneas un~ : : = MMHG [ ANNI I GRADI I ORE (A) 1% ~-.num string>: : = ( n u m > I ~-aaum s t r i ng>(0> [ ( h u m s t r i n g > ( 9 > (orgart~ : : = CORNEA I BULBO I PUPILLA I . . . . . . ~/-status> : : = I ATROFIA [ GLAUCOMA [ STRABISMO I . . . . . . ~quant> : : = PRESSIONE I TONO I VISUS I DISTANZA I ~--adj> : : = OPACO I TRANSPARENTE I ATROFICO I TORBIDO I < a u m > : : = 0 1 1 1 2 I 314 1 5 1 6 1 7 1 8 1 9 I <log op> : : = NOT I AND I OR I ( r e l o p > : : = E Q I L E I L T I G E I G T [ (other commands> : : =/---directives> [ ~---system directives> /----directives>: : =FORGET [ NEXT [ STOP [ (system directives> : : = (various commands to implement specific tasks>
The meaning of the 'Forget ' directive is: forget the issued directive and wait
for another one. The meaning of the 'Next ' directive is: take the same directive on the next supplied entry of the pat ient directory. The meaning of the 'S top ' directive is: forget the issued directive and reload the super- visor (i.e. the min icompute r host operat ing system will resume control) .
Implementation techniques
The inquiry system we have designed is interpretat ive and holds the voca- bulary as data. It is possible to modify vocabulary to allow the user to
define new symbols for old symbols with the possibili ty of chaining of the dict ionary entries. This makes the al terat ion of vocabulary to define
synonyms possible and trivial. Appropriate ins t ruct ions have been inserted in the syntax to implement this new facility.
With regard to the problem of associating the parsed sentence with a set of actions to be implemented , many solut ions have been proposed. Among the most promising ones, the requested actions are embedded within the pro- duct ion rules in the syntax specifications. Our requirements are much less sophisticated for the present and we therefore turned to a direct interpreta- t ion for the immedia te ly executable requests; a template matching for the
42

other use is being considered. This technique consists of storing a series of templates against which the input string can be matched. Associated with each template is a pointer to a routine to be executed if a match occurs. The routine entered would extract the property (i.e. name, type. etc.) or the qualifier ( textual or numeric) and save it for future use, and the template matching process would again be invoked to identify the remainder of operations to be executed.
Interpretat ion of immediately executable directives requires a very simple state finite automaton, which gets the input string and commutes itself to the state corresponding to the action required. In its turn, this state, the identifier of an operative routine, takes the sequence of directives to accom- plish the given task.
Clearly very fast string processing is achieved in this way. To allow quick response to the user's request, data m a y be copied on a bank of RAMs (the so-called static disl~) and a microprocessor can read them from and print them on a line printer or a visual display~ Then the computer may be switched to other concurrent jobs.
In Fig. 6 an example, which shows how a request is processed by the Interpreter, is reported. The syntactic tree built by the SAR is pointed out. The request, written at the bo t tom of the figure in Italian means: search throughout the data base all files corresponding to patients who show symptoms of glaucoma and are fifty years old, and report them~
( $ E N T ENCIE ) ,
L!I<____
/ 77.,... 'r I .... rl I / ""r" ) ""T'" ~'"r"~ .... r ..... "\
.... i ....... T ..... i ...... 'i ....... ( ...... t ...... i ....... ~ ...... i"x cerca tu t t i sintomi .EO. glsucoma .AND. eta' . l O . 5 o
Fig. 6. Example of parsing of a command sentence accepted by the clinical data base inquixy system.
43
ACKNOWLEDGMENTS
This work is at present developing at the Eye Clinic Department of the University of Genova and we are grateful to Prof. A. Grignolo and Prof. Mo Zingirian for their support.
Authors' address: Istituto Electrotecnica Universita Viale Causa 13 16145 Genoa Italy
44
Related Documents










