1 The Use of Albumin for the Prevention of Hepatorenal Syndrome in Patients with Spontaneous Bacterial Peritonitis and Cirrhosis http://www.funnyjunk.com/funny_pictures/1743659/Enlarged/ Daniel Giddings, PharmD PGY-1 Pharmacy Practice Resident St. David's South Austin Medical Center October 4, 2013 Learning Objectives: 1. Describe the diagnostic criteria, pathogenesis and epidemiology of hepatorenal syndrome and spontaneous bacterial peritonitis (SBP). 2. Compare treatment guidelines for the use of albumin for the prevention of hepatorenal syndrome in SBP. 3. Examine the evidence base for use of albumin in these patients. 4. Determine albumin's role in the prevention of hepatorenal syndrome in SBP patients.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
The Use of Albumin for the Prevention of Hepatorenal
Syndrome in Patients with Spontaneous Bacterial Peritonitis
and Cirrhosis
http://www.funnyjunk.com/funny_pictures/1743659/Enlarged/
Daniel Giddings, PharmD
PGY-1 Pharmacy Practice Resident
St. David's South Austin Medical Center
October 4, 2013
Learning Objectives:
1. Describe the diagnostic criteria, pathogenesis and epidemiology of hepatorenal syndrome and
spontaneous bacterial peritonitis (SBP).
2. Compare treatment guidelines for the use of albumin for the prevention of hepatorenal syndrome in
SBP.
3. Examine the evidence base for use of albumin in these patients.
4. Determine albumin's role in the prevention of hepatorenal syndrome in SBP patients.

2
Hepatorenal Syndrome
Introduction
1
Renal failure in patients with cirrhosis is relatively common, and can be attributed in some to dehydration or
intrinsic renal parenchymal disease such as glomerulonephritis. In other cases, however, renal failure is not
accompanied by any underlying renal pathology and cannot be attributed to other factors; this is known as
hepatorenal syndrome.
Diagnosis
1
Entirely a diagnosis of exclusion in patients with cirrhosis and ascites with associated renal impairment
Treatment guidelines both reference diagnostic criteria put out by the International Ascites Club,
updated last in 2007
The six criteria are:
o Presence of cirrhosis with ascites
o Renal impairment, as indicated by a serum creatinine of greater than 1.5mg/dL
o No improvement in renal impairment (reduction in serum creatinine to < 1.5mg/dL) despite
diuretic withdrawal and volume expansion with albumin (1g/kg actual body weight up to 100g)
for 2 days
o Absence of shock
o No current or recent treatment with nephrotoxic drugs, such as aminoglycosides
o Absence of parenchymal kidney disease as indicated by proteinuria of more than 500mg/day,
microhematuria (> 50 RBC/hpf), and/or abnormal renal ultrasound
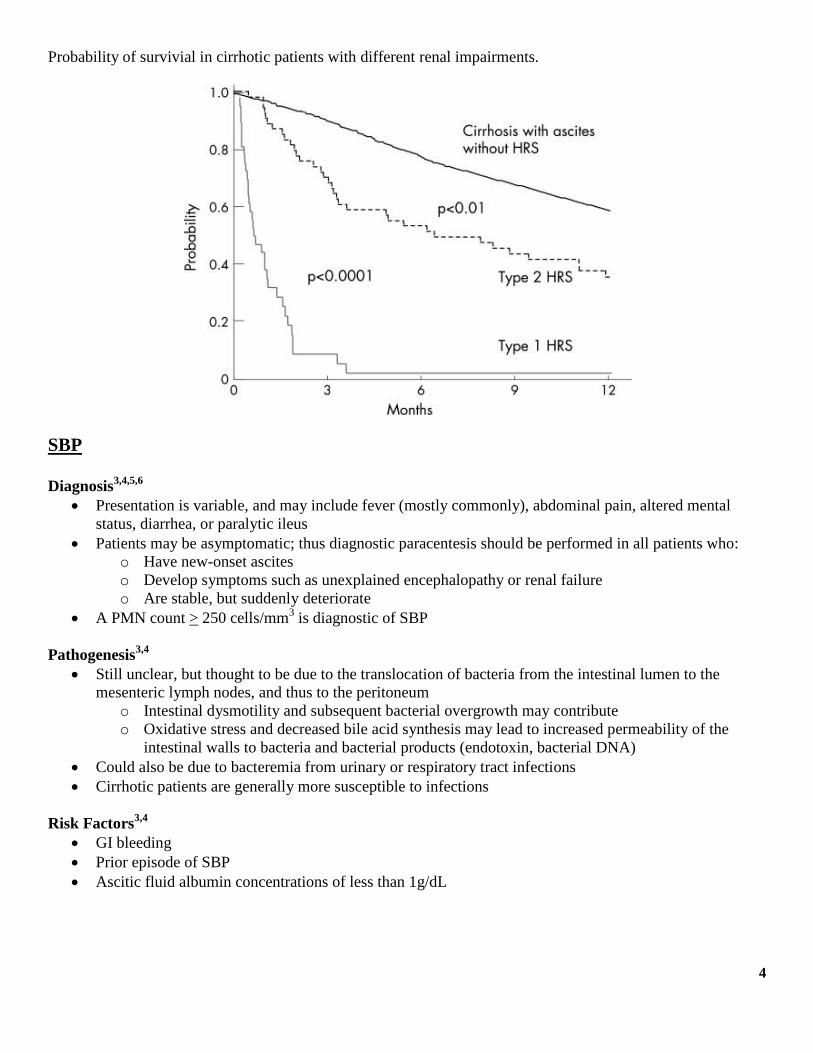
Can be separated into two dynamic classes
o Type 1 - A doubling in serum creatinine that reaches at least 2.5mg/dL over the course of at least
two weeks
o Type 2 - Cases that meet diagnostic criteria without meeting the criteria for Type 1 hepatorenal
syndrome
Pathogenesis1,2
Centers around extreme renal vasoconstriction as a result of pathological splanchnic vasodilation
The underlying cirrhotic process causes increased splanchnic vascular resistance and portal hypertension
This leads to a decrease in systemic vascular resistance (SVR) through local release of vasodilators,
including nitric oxide (NO), carbon monoxide, and endogenous cannabanoids
o Bacterial translocation from the intestines may also play a role through the inflammatory
response (could explain the relationship to SBP)
Initially, cardiac output is increased to compensate for this decrease in vascular resistance (recall the
formula: BP = SVR x CO)
As portal hypertension and decrease in SVR progress, vasoconstrictor systems activate to keep blood
pressure normal, including the RAAS system, the sympathetic nervous system, and the release of ADH
These systems cause intense vasoconstriction in the renal arteries, leading to renal hypoperfusion, salt
and water retention, and renal failure

3
Precipitating Factors1
Bacterial infection, including spontaneous bacterial peritonitis (SBP)
o SBP is the only infection with a clearly demonstrated relationship to hepatorenal syndrome
Large-volume paracentesis without volume repletion
Gastrointestinal bleeding
Hypovolemic shock
Over-diuresis (no study evidence for this)
Epidemiology and Prognosis
Overall incidence of hepatorenal syndrome was estimated to be 40% at 5 years in one study
Renal failure in patients with cirrhosis and ascites is associated with a poor prognosis, but the
development of hepatorenal syndrome indicates an even poorer one
• Portal Hypertension
• Caused by underlying cirrhosis, leads to increased vascular resistance in splanchnic system
• Splanchnic Vasodilation
• Reponse to underlying cirrhosis and portal hypertension
• Compensatory Response
• Includes increased cardiac output and activation of vasoconstricting systems, including RAAS, ADH, and sympathetic nervous system activation
• Renal failure and Hepatorenal Syndrome
• Due to extreme vasoconstriction of the renal arteries mediated by the compensatory response
4
Probability of survivial in cirrhotic patients with different renal impairments.
SBP Diagnosis
3,4,5,6
Presentation is variable, and may include fever (mostly commonly), abdominal pain, altered mental
status, diarrhea, or paralytic ileus
Patients may be asymptomatic; thus diagnostic paracentesis should be performed in all patients who:
o Have new-onset ascites
o Develop symptoms such as unexplained encephalopathy or renal failure
o Are stable, but suddenly deteriorate
A PMN count > 250 cells/mm3 is diagnostic of SBP
Pathogenesis3,4
Still unclear, but thought to be due to the translocation of bacteria from the intestinal lumen to the
mesenteric lymph nodes, and thus to the peritoneum
o Intestinal dysmotility and subsequent bacterial overgrowth may contribute
o Oxidative stress and decreased bile acid synthesis may lead to increased permeability of the
intestinal walls to bacteria and bacterial products (endotoxin, bacterial DNA)
Could also be due to bacteremia from urinary or respiratory tract infections
Cirrhotic patients are generally more susceptible to infections
Risk Factors3,4
GI bleeding
Prior episode of SBP
Ascitic fluid albumin concentrations of less than 1g/dL
5
Epidemiology and Mortality3,4,5,6
Prevalence studies from the 1970's showed a prevalence of 5-10%, but newer studies using modern
diagnostic criteria show a prevalence of roughly 10-30% of patients admitted to hospitals with cirrhosis
In-hospital mortality rates have fallen from 90% to around 10-30%
o Renal impairment is a strong predictor of mortality; progressive renal failure was associated with
an in-hospital mortality of 100% in one study, with stable renal impairment being associated
with a 31% mortality rate and no renal impairment only 7%
o Other predictors of mortality include elevated BUN and serum bilirubin, positive ascitic fluid
cultures, and age
Treatment Guidelines5,6
Two regularly updated guidelines that address the treatment and prevention of hepatorenal syndrome:
o The American Association for the Study of Liver Diseases (AASLD)
o The European Association for the Study of the Liver (EASL)
AASLD Guidelines
Class IIa, Level B
EASL Guidelines
Class I, Level B
Patients with ascitic fluid PMN counts greater than or
equal to 250 cells/mm3 (0.25 x 10
9/L) and clinical
suspicion of SBP, who also have a serum creatinine
>1 mg/dL, blood urea nitrogen >30 mg/dL, or total
bilirubin >4 mg/dL should receive 1.5 g albumin per
kg body weight within 6 hours of detection and 1.0
g/kg on day 3.
Until more information is available, we recommend
that all patients who develop SBP should be treated
with broad spectrum antibiotics and intravenous
albumin (1.5 g/kg at diagnosis and 1g/kg on day 3).
Albumin7,8
Overview
Albumin is an endogenous protein 66,500 kDa in molecular weight that exerts most (70-80%) of the
colloid oncotic pressure in blood plasma
Derived for pharmaceutical use from pooled human plasma
Distributes widely in the vasculature and extravascular space
Acts as a transport molecule for a variety of endogenous substances and drugs, including:
o Nitric oxide
o Fatty acids
o Metals
o Cholesterol
o Phenytoin (recall corrected phenytoin level in hypoalbuminemia)
o Digoxin
Exerts a strong oncotic pressure and can serve as a vascular volume expander (this is its FDA labeled
indication)
Serves as a thiol sink and is the major contributor of extracellular thiols, which are scavengers of
reactive oxygen and nitrogen species
Available in the US as a 5% and 25% solution
Mechanism of Action in the Prevention of Hepatorenal Syndrome
6
Albumin's function as a plasma volume expander may serve to compensate for the decrease in SVR
caused by cirrhosis and portal hypertension (this is likely the primary mechanism of action in the
prevention of hepatorenal syndrome)
Antioxidant effects may play a role by decreasing the release of vasodilators from cirrhotic liver tissue
Albumin may bind bacterial endotoxins and DNA fragments that contribute to hepatorenal syndrome via
bacterial translocation
As discussed in guidelines, albumin must be combined with a vasoconstrictor to maximize effectiveness
in the treatment of SBP
Costs and Adverse Effects
Available as a generic: AWP for 25g of 25% albumin is $64.50
For reference, a guideline-recommended course of albumin in a 70kg SBP patient would cost roughly
$450 at AWP
Contraindications and Precautions
o Contraindicated in cardiac failure: leads to circulatory overload
o Use with caution in patients with renal or hepatic impairment, as protein load may precipitate
azotemia or encephalopathy
o Pulmonary or peripheral edema may result from overly rapid infusion
o Hypersensitivity reactions have occurred
o Blood product: though pasteurized, cannot rule out transmission of infective agents
Literature Review
Effect of intravenous albumin on renal impairment and mortality in patients with
cirrhosis and spontaneous bacterial peritonitis9
Objective: To determine whether plasma volume expansion with albumin could prevent the impairment of
renal function and reduce mortality in patients with SBP.
Methods
Multicenter, randomized, controlled trial
Inclusion and exclusion criteria (notice parallels to hepatorenal syndrome and SBP diagnostic criteria)
o Ascitic fluid PMN count > 250 cells/mm3
o Absence of findings suggestive of secondary peritonitis
o Absence of shock, GI bleed, grade 3 or 4 hepatic encephalopathy, HIV infection, cardiac failure,
and other infections
o Serum creatinine no more than 3 mg/dL
o Severe dehydration within one week of diagnosis of peritonitis, as evaluated clinically or by
CVP < 4
199 patients were evaluated, 126 were included
Patients were randomized to either renally adjusted cefotaxime or renally adjusted cefotaxime plus 20%
albumin 1.5g/kg on day 1 and 1g/kg on day 3 of enrollment
Follow-up lasted 90 days from the enrollment period
Renal impairment at the time of enrollment was defined as a BUN of > 40 mg/dL or a serum creatinine
of > 1.5 mg/dL
In patients without renal impairment at baseline, a 50% increase in BUN or serum creatinine to levels
above 40 mg/dL and 1.5 mg/dL respectively was diagnostic for renal impairment during treatment
7
For patients with renal impairment at baseline, simply a 50% increase in BUN or serum creatinine was
diagnostic for worsening renal failure
50 patients in each group were required for an 80% power to detect a 25% difference in the rate of renal
failure
Results
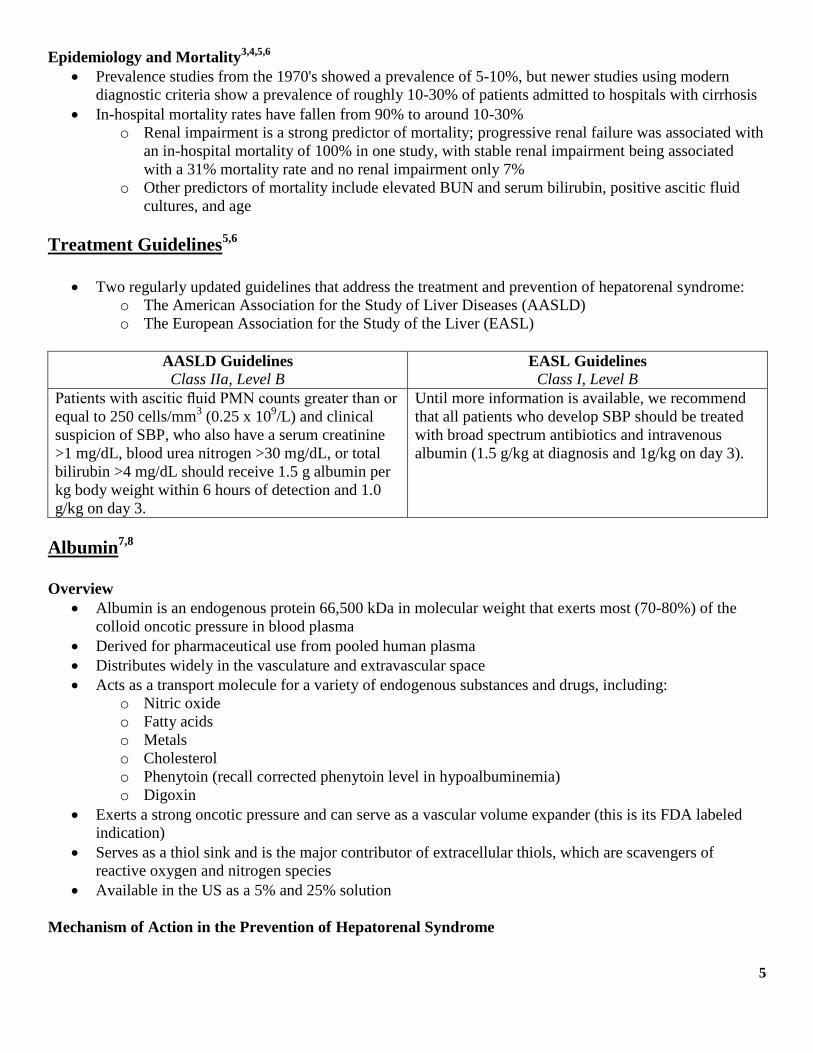
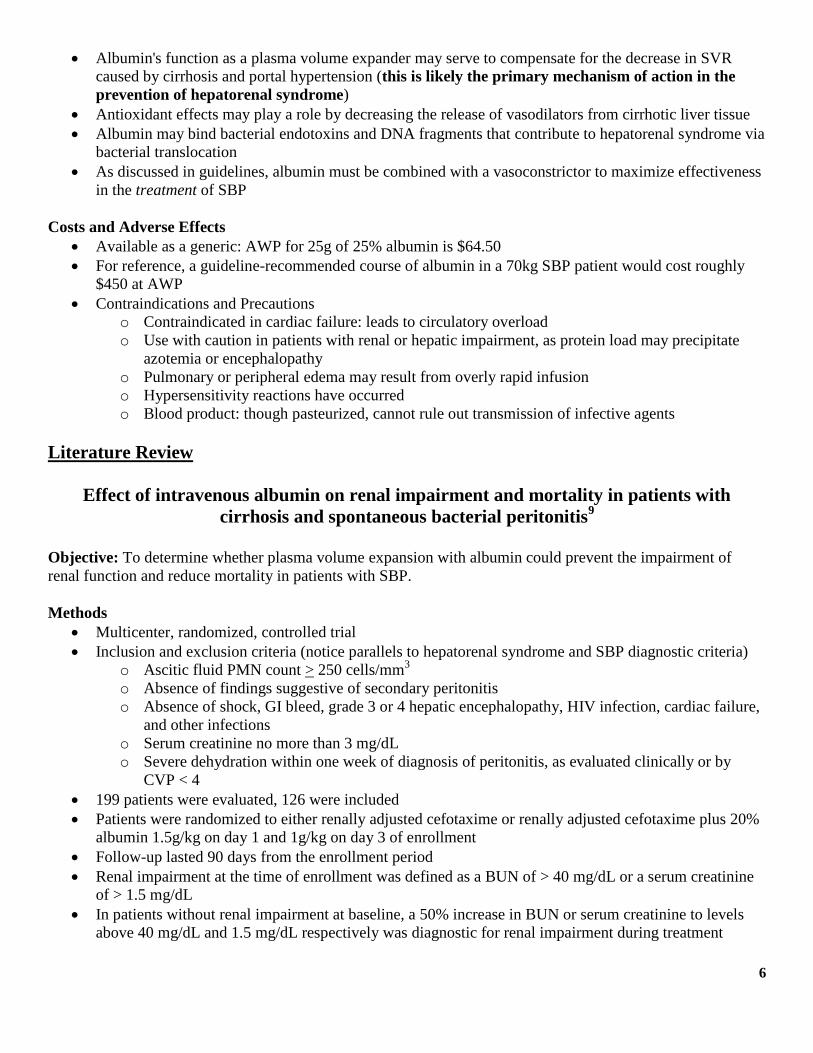
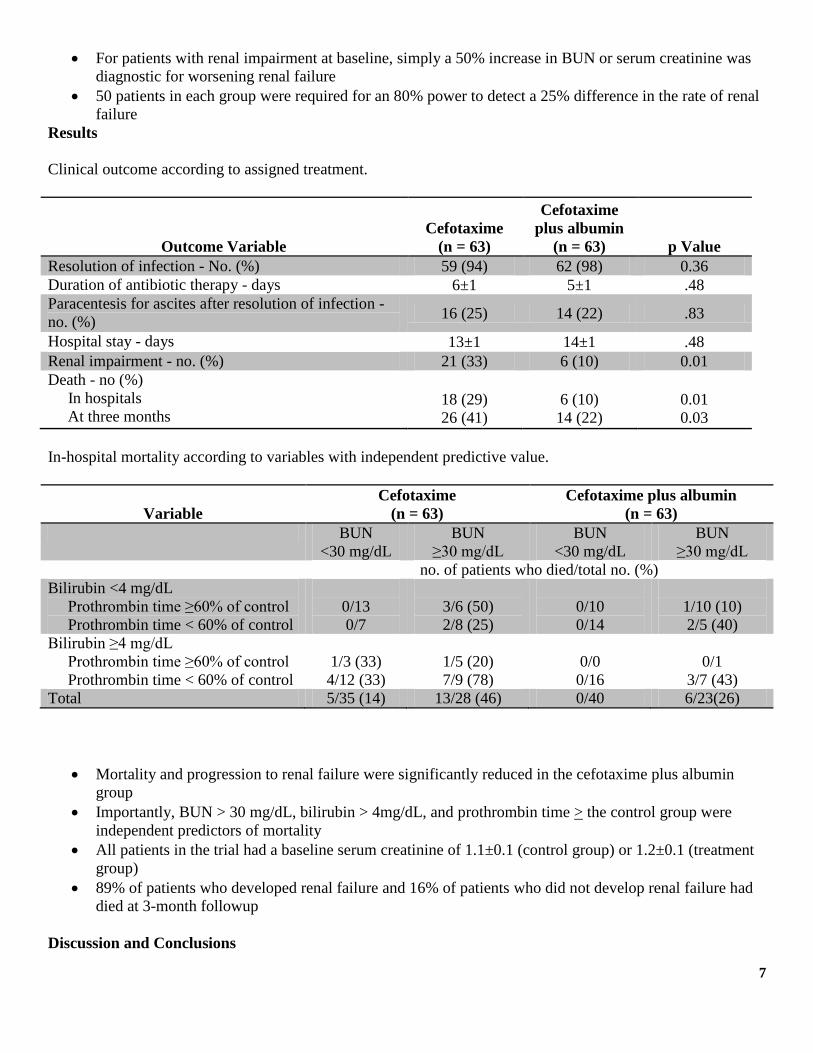
Clinical outcome according to assigned treatment.
Outcome Variable
Cefotaxime
(n = 63)
Cefotaxime
plus albumin
(n = 63) p Value
Resolution of infection - No. (%) 59 (94) 62 (98) 0.36
Duration of antibiotic therapy - days 6±1 5±1 .48
Paracentesis for ascites after resolution of infection -
no. (%) 16 (25) 14 (22) .83
Hospital stay - days 13±1 14±1 .48
Renal impairment - no. (%) 21 (33) 6 (10) 0.01
Death - no (%)
In hospitals
At three months
18 (29)
26 (41)
6 (10)
14 (22)
0.01
0.03
In-hospital mortality according to variables with independent predictive value.
Variable
Cefotaxime
(n = 63)
Cefotaxime plus albumin
(n = 63)
BUN
<30 mg/dL
BUN
≥30 mg/dL
BUN
<30 mg/dL
BUN
≥30 mg/dL
no. of patients who died/total no. (%)
Bilirubin <4 mg/dL
Prothrombin time ≥60% of control
Prothrombin time < 60% of control
0/13
0/7
3/6 (50)
2/8 (25)
0/10
0/14
1/10 (10)
2/5 (40)
Bilirubin ≥4 mg/dL
Prothrombin time ≥60% of control
Prothrombin time < 60% of control
1/3 (33)
4/12 (33)
1/5 (20)
7/9 (78)
0/0
0/16
0/1
3/7 (43)
Total 5/35 (14) 13/28 (46) 0/40 6/23(26)
Mortality and progression to renal failure were significantly reduced in the cefotaxime plus albumin
group
Importantly, BUN > 30 mg/dL, bilirubin > 4mg/dL, and prothrombin time > the control group were
independent predictors of mortality
All patients in the trial had a baseline serum creatinine of 1.1±0.1 (control group) or 1.2±0.1 (treatment
group)
89% of patients who developed renal failure and 16% of patients who did not develop renal failure had
died at 3-month followup
Discussion and Conclusions

8
The authors conclude that albumin plus empiric antibiotic treatment is more effective at reducing
mortality and progression to renal failure in patients with SBP than empiric antibiotics alone
The trial helps confirm that progressive renal failure and hepatorenal syndrome are indicative of a poor
prognosis
Trial strengths
o Randomized and adequately controlled
o Endpoints and inclusion criteria consistent with the disease states being studied (PMN count in
ascitic fluid, serum creatinine cutoffs, etc.)
o Demonstrated a mortality benefit
o Appropriate statistical analysis
Trial weaknesses
o Benefit was most apparent in patients with BUN > 30 mg/dL and bilirubin > 4mg/dL, and only
patients with a serum creatinine above 1.0 were included in the trial
o Does not shed light on whether albumin is unique or other plasma volume expanders would be
effective for the same purpose (the authors address this in their discussion)
o Control patients may have been sicker
Restricted use of albumin for spontaneous bacterial peritonitis10
Objective: To assess whether albumin treatment is needed in all cases of SBP or whether a risk stratification
strategy is desirable.
Methods
A 28 patient prospective case series in two medical centers
Patients with a bilirubin > 4 or a serum creatinine > 1.0 were treated with albumin 1.5g/kg on day 1 and
1g/kg on day 3 of treatment along with empiric antibiotics
Low-risk patients (serum creatnine < 1.0 and bilirubin < 4) were treated only with empiric antibiotic
therapy
Results
Selected clinical characteristics of patients at diagnosis of spontaneous bacterial peritonitis episodes who did
receive (A) and who did not receive (B) albumin.
A
(n = 26)
B
(n = 18) p Value
Total bilirubin(mmol/L) 115 (12-395) 39 (14-67) <0.001
BUN (mg/dL) 28.5 (7-74) 18(5-48) 0.003
Creatinine (mmol/L) 124 (35-327) 80 (53-106) 0.001
In the low-risk group, SBP resolved in all patients and no patients developed renal impairment.
In the high-risk group, 12 patients developed renal impairment and five patients died.
Discussion and Conclusions
The authors conclude that albumin is not needed in all SBP patients
Strengths
o Used parameters based on the single randomized, controlled trial performed for this intervention
o Used established guidelines for diagnosis and treatment of SBP and hepatorenal syndrome

9
o Calculated p values
Weaknesses
o No control group
o Small case series
Albumin infusion improves outcomes of patients with spontaneous bacterial peritonitis: a
meta-analysis of randomized trials11
Objective: To quantify the effect of albumin infusion on renal impairment and mortality in patients with SBP.
Methods
A meta-analysis limited to only randomized, controlled trials evaluation albumin in SBP patients
o No language or time period restrictions
All three investigators independently determined trial inclusion eligibility
Endpoints of the analysis were renal impairment (as defined by the included trials) and mortality
Heterogeneity was judged using the Cochran Q test and the I2 test
Results of the trials were combined under a fixed-effects model
Results
Renal impairment. Confidence interval (CI) is shown by error bars. Data points for individual trials scaled
accordingly to meta-analytic weight.

10
Improvement in the incidence of renal impairment and mortality were shown
o Removing either of the two most heavily weighted studies did not change the overall conclusion
No differences shown between subgroups, however, a non-significant increase was seen in the incidence
of renal impairment and mortality in patients with BUN > 30 mg/dL and/or bilirubin > 4
Discussion and Conclusions
The authors conclude that albumin is effective for prevention of renal failure and mortality in SBP
patients with cirrhosis.
Strengths
o Relied only on randomized, controlled trials
o Appropriate statistical analysis
o Robust results
Weaknesses
o Small sample size
o 3 out of the 4 trials were not blinded
Albumin for bacterial infections other than spontaneous bacterial peritonitis in cirrhosis.
A randomized, controlled study12
Objective: To determine if albumin has beneficial effects outside of patients with cirrhosis that develop SBP.
Methods
Single center, randomized, controlled trial
Inclusion criteria
o Cirrhosis, diagnosed by liver biopsy or by clinical findings according to published guildelines
o Presence of infection, diagnosed by cultures or clinical suspicion with at least one of the
following:
PMN count > 10,000 cells/mm3 or 50% increase from baseline with a final value above
8,000 cells/mm3
5% or greater bands
Temperature > 37.5 C
Exclusion criteria
o GI bleed
o Previous antibiotic treatment
11
o Malignancy
o HIV infection
o Presence of shock
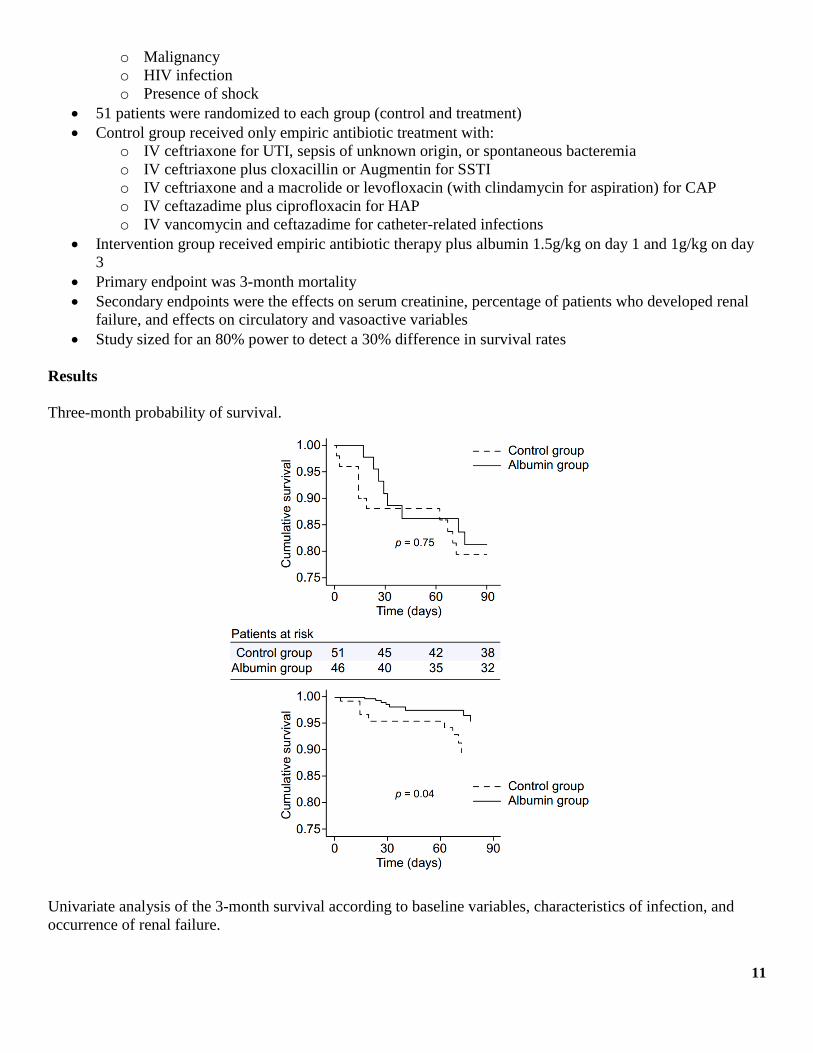
51 patients were randomized to each group (control and treatment)
Control group received only empiric antibiotic treatment with:
o IV ceftriaxone for UTI, sepsis of unknown origin, or spontaneous bacteremia
o IV ceftriaxone plus cloxacillin or Augmentin for SSTI
o IV ceftriaxone and a macrolide or levofloxacin (with clindamycin for aspiration) for CAP
o IV ceftazadime plus ciprofloxacin for HAP
o IV vancomycin and ceftazadime for catheter-related infections
Intervention group received empiric antibiotic therapy plus albumin 1.5g/kg on day 1 and 1g/kg on day
3
Primary endpoint was 3-month mortality
Secondary endpoints were the effects on serum creatinine, percentage of patients who developed renal
failure, and effects on circulatory and vasoactive variables
Study sized for an 80% power to detect a 30% difference in survival rates
Results
Three-month probability of survival.
Univariate analysis of the 3-month survival according to baseline variables, characteristics of infection, and
occurrence of renal failure.

12
Variable
Alive
(n = 79)
Death
(n = 18) p Value
Age (yr) 55 ± 11 60 ± 12 0.158
Ascites at inclusion 54 (68%) 17 (94%) 0.036
Hepatic encephalopathy at inclusion 24 (30%) 11 (61%) 0.027
Nosocomial infection 11 (14%) 10 (56%) <0.0001
Serum bilirubin (mg/dL) 3.5 ± 3.3 9.8 ± 8.6 0.007
Serum albumin (mg/dL) 29 ± 6 26 ± 4 0.024
Serum creatinine (mg/dL) 1.2 ± 0.6 1.3 ± 0.6 0.258
BUN (mg/dL) 24 ± 19 37 ± 21 0.010
Renal failure during infection 15 (19%) 10 (56%) 0.006
Overall, there were no significant differences in the unadjusted 3-month mortality rates between the
control and intervention groups (80% survival in the control group vs. 82.6% survival in the intervention
group)
Significance was shown when the results were adjusted for variables shown in univariate analysis to
have independent predictive value
Differences in the incidence of renal failure and in serum creatnine concentrations between the control
and intervention groups did not reach statistical significance
o Compared to SBP patients, renal failure did not occur as often in the control group of this study
o Mortality was also lower in the control group compared to SBP patients not treated with albumin
Discussion and Conclusions
The authors conclude that albumin treatment in patients with bacterial infections other than SBP is not
associated with a significant decrease in either 3 month mortality or the incidence of renal failure
The overall incidence of renal failure and mortality in the trial's control group reveals that the overall
difference in prognosis between SBP and other bacterial infections may help explain the negative results
of this trial
Strengths
o Randomized and controlled
o Used mortality as an endpoint
o Statistical analysis appropriate, including power calculation, and did not overstep with
conclusions based on post-hoc adjustment of results
Weaknesses
o Power estimate greatly overstated the actual effect size
o Needed to adjust results for statistical significance
Conclusions
Albumin is effective for the prevention of progression to hepatorenal syndrome and renal
failure in SBP patients
There is a small body of evidence that suggests that albumin is not needed in all SBP
patients, but more study is needed
No evidence to suggest that albumin is effective in other bacterial infections in cirrhotic
patients
More evidence is needed to inform about the optimal dose of albumin in SBP patients
o Trials underway (ClinicalTrials.gov: NCT00761098)

13
References
1. Diagnosis, prevention, and treatment of hepatorenal syndrome in cirrhosis. Salerno F, Gerbes A, Gines
P, et al. Gut. 2007;56:1310-1308.
2. Mechanisms promoting bacterial translocation from the gastrointestinal tract. Berg RD. Adv Exp Med
Biol 1999;473:11-30
3. Spontaneous bacterial peritonitis: recent data on incidence and treatment. Mansour PA, Atreja A, Zein
NN. Cleve Clin J Med. 2004;71(7):569-76.
4. Renal impairment after spontaneous bacterial peritonitis in cirrhosis: Incidence, clinical course,
predictive factors and prognosis. Follo A, Llovet JM, Navasa M, et al. Hepatology 1994;20:1495–1501.
5. Management of adult patients with ascites due to cirrhosis: update 2012. Runyon, BA for the AASLD.
Hepatology 2013;57(4):1651-3.
6. EASL clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and
hepatorenal syndrome in cirrhosis. EASL. Hepatology 2010;53:397-417.
7. Albumin. Lexi-Comp Online, Lexi-Drugs, Hudson, Ohio: Lexi-Comp, Inc.; Accessed September 22,
2013.
8. Albumin for end-stage liver disease. Lee JS. Korean J Intern Med 2012(27):13-19
9. Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and
spontaneous bacterial peritonitis. Sort P, Navasa M, Arroyo V, et al. N Engl J Med 1999;341:403-409.
10. Restricted use of albumin for spontaneous bacterial peritonitis. Sigal SH, Stanca SM, Fernandez J, et al.
Gut 2007;56(4):597-599
11. Albumin infusion improves outcomes of patients with spontaneous bacterial peritonitis: a meta-analysis
of randomized trials. Salerno F, Navickis RJ, Wilkes MM. Clin Gastroenterol Hepatol 2013;11(2):123-
130
12. Albumin for bacterial infections other than spontaneous bacterial peritonitis in cirrhosis. A randomized,
controlled study. Guevara M, Terra C, Nazar A, et al. Hepatology 2012;57:759-765

14
Appendix A: Included Trials in the Meta-analysis from Salerno et al.
Table 1.
Included Trials
Trial N Age
(SD)
Male, % Ethnicity Etiology Treatment regimen
Sort et al,
1999
126 61.0
(7.9)
64.3 Caucasian 29.4% alcohol,
70.6% other
Cefotaxime intravenously dosed
according to creatinine without vs
with 1.5g/kg 20% albumin within
first 6 h plus 1.0 g/kg on day 3
Xue et al,
2002
112 22-70 - Chinese - Ceftriaxone intravenously dosed
according to creatinine without vs
with 0.5-1.0 g/kg 20% albumin
within first 6 h and every third
day for 21 days
Fernandez
et al, 2005
20 61.0
(9.5)
55 Caucasian 60.0% HCV,
40.0% other
Ceftriaxone intravenously 2 g at
diagnosis and then 1 g/d plus 1.5
g/kg at baseline and 1.0g/kg on
day 3 of 20% albumin vs 6% HES
200/0.5
Chen et al,
2009
30 56.5
(11.5)
60 Chinese 60.0%
HBV<comma>
23.3%
HCV<comma>
16.7% alcohol
Cephalosporins without vs with
50 mL 20% albumin (0.14
g/kg−1 for a 70-kg patient) on
days 1–3
Related Documents











