The “three M’s”: Muscles, malformation, and malocclusion T. M. GRABER, D.D.S., M.S.D., Ph.D. Kenilworth, Ill. I T w o u L D be hard to convince the neophyte that fashions flourish in ortho- dontics even as they do in interior decorating and clothes design. A quick glance at the programs of the various sectional components of the American Associa- tion of Orthodontists and a summary perusal of the literature of the past 10 years would, indeed, indicate that there is a time-linked subject orientation. Ten years ago editors were surfeited with papers on cephalometrics. The ma- jority of theses being written by graduate students were cephalometrically oriented and, as one observer has put it, “the numbers racket was in high gear. ” Most appliance articles 10 years ago were on the Angle edgewise appliance if they dealt with mechanothera,py. The tenor of most of these articles was that the problems were really quite simple if you had the proper mechanism and observed the commandments emanat,ing from above. For one group of disciples, the most important commandments were the following: 1. Never take out teeth; to do so means compromise, and failure is only a matter of degree. 2. You have been given an appliance that is capable of any movement you choose. Use it properly and you shall not fail. Remember, you are one of the “chosen people, ” following in His footsteps. 3. The only true research is that being done by those who have inherited His mantle; there is no other God but He. 4. Do not degrade thyself by comminglin, 0 with disbelievers. You have been given the divine message. 5. Obey and do not question. 6. If you put the teeth in their proper relationship to each other, nor- mal function will result and stimulate the development of support- ing bone. 7. Ignore the soft tissues; t,hcy will move out of your way. From the Department of Orthodontics, University of Michigan School of Dentistry. Presented at the thirty-third annual meeting of the Great Lakes Societ,y of Ortho- dontists, Detroit, Mich., Dec. 11, 1962. 418

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
The “three M’s”: Muscles, malformation, and malocclusion T. M. GRABER, D.D.S., M.S.D., Ph.D.
Kenilworth, Ill.
I T w o u L D be hard to convince the neophyte that fashions flourish in ortho- dontics even as they do in interior decorating and clothes design. A quick glance at the programs of the various sectional components of the American Associa- tion of Orthodontists and a summary perusal of the literature of the past 10 years would, indeed, indicate that there is a time-linked subject orientation. Ten years ago editors were surfeited with papers on cephalometrics. The ma- jority of theses being written by graduate students were cephalometrically oriented and, as one observer has put it, “the numbers racket was in high gear. ” Most appliance articles 10 years ago were on the Angle edgewise appliance if they dealt with mechanothera,py. The tenor of most of these articles was that the problems were really quite simple if you had the proper mechanism and observed the commandments emanat,ing from above. For one group of disciples, the most important commandments were the following:
1. Never take out teeth; to do so means compromise, and failure is only a matter of degree.
2. You have been given an appliance that is capable of any movement you choose. Use it properly and you shall not fail. Remember, you are one of the “chosen people, ” following in His footsteps.
3. The only true research is that being done by those who have inherited His mantle; there is no other God but He.
4. Do not degrade thyself by comminglin, 0 with disbelievers. You have been given the divine message.
5. Obey and do not question. 6. If you put the teeth in their proper relationship to each other, nor-
mal function will result and stimulate the development of support- ing bone.
7. Ignore the soft tissues; t,hcy will move out of your way.
From the Department of Orthodontics, University of Michigan School of Dentistry. Presented at the thirty-third annual meeting of the Great Lakes Societ,y of Ortho- dontists, Detroit, Mich., Dec. 11, 1962.
418

S. Don’t worry about the amount of force you WC. Twth will I~OV~ one way or the other.
9. Read extensively in comparative anatomy, anthropolop,v, and art, for an erudite display of such knolx-ledge will assist you in times ot travail.
10. Hctain the orthodontic results indefinitely. This \vill allow function to take OWP and stabilize the results.
If thcsr commandments did not instill the fear of the deit;\V in the: t~agcr young orthodontist, he was somewhat perplexed when ht ran into another wt ol precepts, also emanating from an oracle on high. These ~olunnandments----I’r!)nI a slight1.v different cult, of course--were as f’ollows:
1. Thou shalt not expand. 2. lIonor thy paGent and practice and strixxl for perfection alld a picas-
ing profile. 3. Rrmcmbcr that the master has said that the lowr incisors must lw
90 tlegrccs to t,he mandibular plam, or 65 dcgrces to the E’rankf’ort horizontal. 110 not deviate!
1. Ijo not hesitate to estract first premolars. Only in this \\a>- (‘ill1 ,votl
achiwe the objectives required by our master. 5. Band as many teeth as possible ; to do less indicat,os sloth, inde-
cisions and lack of comprehension of 1 htl only roatl to orthodonti(~ Sal\-ation.
6. lgnow muscles, particularly those of thtb tongue, as you strive For the magic mathematical formula.
7. lgnorr morphogcnetic pattern and gronth gradients. Occlusion is the Iwall and the c>nd-all of our existence.
8. Ignorr root resorption, but do not show the roent,grnograms to your confrCrc>s because they might interpret this as a sign of wcakntlss.
!I. Take your “finished” records as soon as you remove appliances. 1 f you have not achieved the objectives as outlined by the master. the cast’ is not to lot> considered “finished.”
10. Retain the case indefinitely. Never discuss failures with nonbc4ic\-ws, for you may sow the seeds of ugly suspicion and mistrust.
It is ohvions from looking at both sets of’ the ” ~a~r~tl tchn” that thtb atl- lierent, to citlicr set of commandments had to liarc “religion.” Conflicting as some of the admonitions seem, however, there wre some common drnominators. In both past’s, it \V~S assumed that the applianws \VOU~~ automatically proclucca the desired result it’ used properly. In both cast’s, OIW just did not think about failure or the accomplishment of less than idcal results. In both CasCs, to II’IC something tliffcrent meant to compromise, and compromise was ;I, therapeutic disgrace. I~‘ollowe~~s of both sets ol’ rules paid lip wrviw to I’unt~tionai t’or~s but ignowd the role of niusclt~s.
In this U-ondcrful world of fashion, musclrs w’l’t’ bonntl to haw thclir* I-1;1,v.
The patient ‘S f’ailurtl to wc‘ar his rctainrr conIt not be hlametl for illI tilt? I’(‘-
1il~WS. IXvrll the 1110st zcalons operator CtJlIltl St’t’ that his JW?+td Irl~llri~~~~lilliorri:
at times produced very imperCect results. Third molars provided a good alibi, as did that nebulous ent,ity known as “growth and development, ” but thcrc still must be something else.
There was a rude awakening as clinicians suddenly saw that the patient had a tongue. From the pulpit came the sonorous declaration that “90 per cent of all patients are reverse swallowers!” Disciples gulped a bit when they heard this. Such a statement was, indeed, hard to swallow. Had not the master said to ignore the tongue? At least, he had said this in effect when he said that for every degree over 25 degrees for the Frankfort-mandibular plane angle, the lower incisors should be tipped 1 degree lingually past the magic 90 degree norm. In the spirit of the immortal Tennyson poem, “Theirs not to make reply, theirs not to reason why, theirs but to do and die.” So now there was at least, the perfect scapegoat-the tongue!
The fine work of CYrwynne-Evans,26 Ballard,? H~vcll,~~~~ 31 and T~lley,~” studg- ing the role of the musculature, was ‘ ’ discovered ’ ’ and the numerous graphs and curves associated wit,h the cephalometric contribution to the literature gave way to the curves and contours of the orofacial soft-tissue environment. Speech therapists became tongue tamers. They soon found that lion taming was more succe&X.” Improper nursing, poor design of artificial nipples, retention of in- fantile mechanisms, and nonnutritive sucking were blamed for orthodontic relapses. These tenuous connections arc in much the same category as those used by armchair psychologists who often attribute every adult neurosis to imagined childhood frustrations. Many a physiologist has raised an cyebro\\ as budding “muscle-bound” orthodontists delve in fanciful flights of teleology to explain their failures.
This facetious critique is exaggerated, but, we cannot deny the basic fact that,, from a complete disregard of muscle activity and habit patterns, we have jumped to a belief that muscle plays a dominant role, affecting our manipulations whether we like it or not. One almost senses a feeling of hopelessness or pessimism in sharp contrast t,o the great optimism of the early 1950’s when orthodontists could move teeth as they desired. Perhaps this reflects a belated recognition by our orthodontic engineers that the results produced by the most precise tech- niques and the most efficient armamentaria will not stand the test of time when there is a conflict between the morphologic pattern attained and the physiologic structure of t,he stomatognathic system. Fortunately, the fundamental phe- nomenon of homeostasis, or the organism’s ability to adapt to change, does give the orthodontist some leeway, reducing the air of gloom and pessimism that pervades the lair of the muscle men t,cday.
The orthodontic vernacular has been greatly expanded recently with the inclusion of such terms as reverse swdlowing, hereditary incompetence, endog- enous pattern,, vis~o~rl swalloll~, somatic pottern, retained infantile swal.lou~, simlde tongue-thrust, complex ton’gue-thrust, transitional swallowers, etc. Where do muscles ilnd malocclusion stand with rcaspect, to this IIXIHS of verdant verbiagr ? Arc 111~ answers to bc found in caurrt‘nt myometric and clect,romyogmphic research and basic muscle physiology? Ts it, not, possible that thcrc are many facets to this problem?
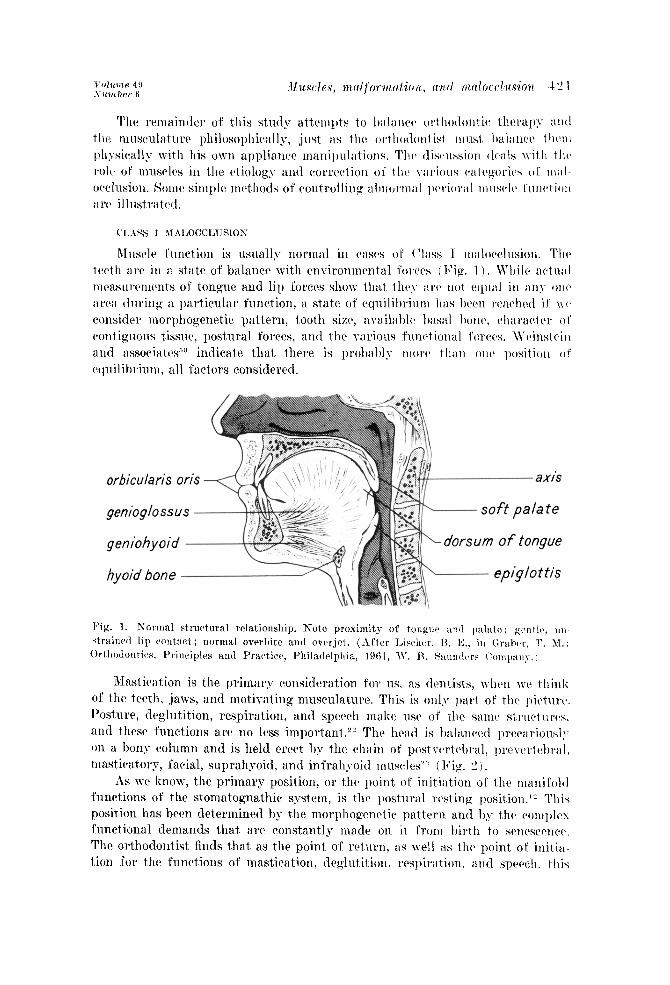
Rlr~sclc t’nnction is usually normal in cast3 01’ (‘lass 1 nr:ilocclnsion. 1’11~ twth aw in a state of bnlnnct? with en\-ironnicntal Cor~ws [ I’ip. 1 ). While wtn;ll rncasurcirncWs of tongue and lip forces show that tlivy arc not equal iii ;~ii~’ OII(’ aiw tluring a particular function, a state of cquilihAuiir has lwn rwchctl if I\ 0 cwnsidvr inorpliogenetic pattern, tooth sixc, iIYLlil:lhl(~ hsiitl hick, clkaractctr 01 cwitigiious tissue, postural forws, and the various Rinct ional forws. \\‘cGrstein and iissociat($” indicate that. there is prohil~l~ n10w thati onv positioii o! c~c~uilibrinm, all factors consider-cd.
orbicularis oris
Izig. 1. Kormal structural rclntionship. Note proximity of tongue ant1 p:~1:1tc; gentIt>, uw strainwl lip cwnt~:tct ; normal 0vrrl)ite and ovcrjet. (After Idischc~r. 13. E.. in Grahr, T. 11.:
f )rtllotloutiw, Priwiples and Pract,iw, Philnilelphia, 1961, IV. H. Saurltl~~rs ~‘onqwy. /
Mastication is the primary consideration for, us. as tlcntists, when wc thitlli of the teeth, jaws, and motivating musculature. This is only part of the picturcb. Posture, dcglutition, respiration, and speech make use of the same sttwetur~c~s, and t.hestl t’unctions arc no less important .?” The head is balnnwd precariously on a bony column and is held crwt by the chain of postwrtebral, I)r’c\.rr.tc,l)r.;lI. tnasticatory, facial, suprahyoid, and infrahyoid muwlesY” ( Fig. 2 j.
As we know, the primary position, or the point of initiation of the manifold functions of the stomatognathic systctn, is thv postural wsting position.” This position has been determined by the rnorphogwrctic pattern and by the c~orn~~lrs functional demands that arc constantly made on it t’ront birth to scnesc~rrw. The orthodontist finds that as the point of wtum, as well i\s the point of init,ia tion for the functions of mastication, dcglutition. rvspiration, and sptwh. this
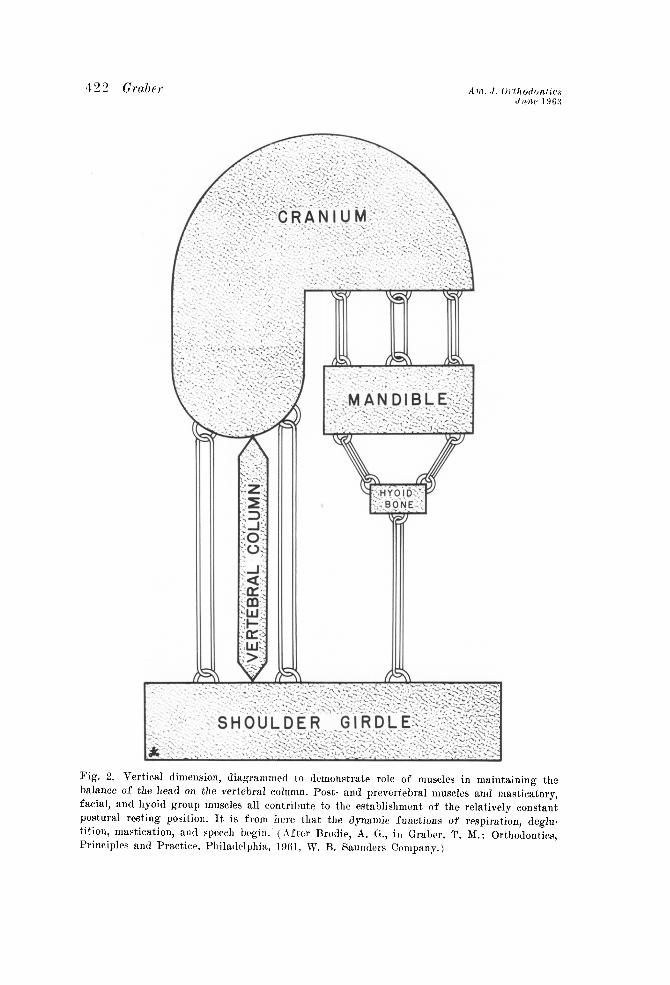
Fig. 2. Vertical dimension, diagrammed to demonstrate role of muscles in maintaining the balance of the head on the vertebral column. Post- and prevertebral muscles and masticatorp, facial, and hyoid group muscles all contribute to the establishment of the relatively constant postural resting position. It is from hrrc that the dynamic functions of respiration, deglu. tition, mastication, and speech begin. (After Rrodir, A. G., in Grabcr, T. M.: Orthodontics,
Principlrs and Practice, Philatlrlphia, lW1, W. R. Saunders Company.)
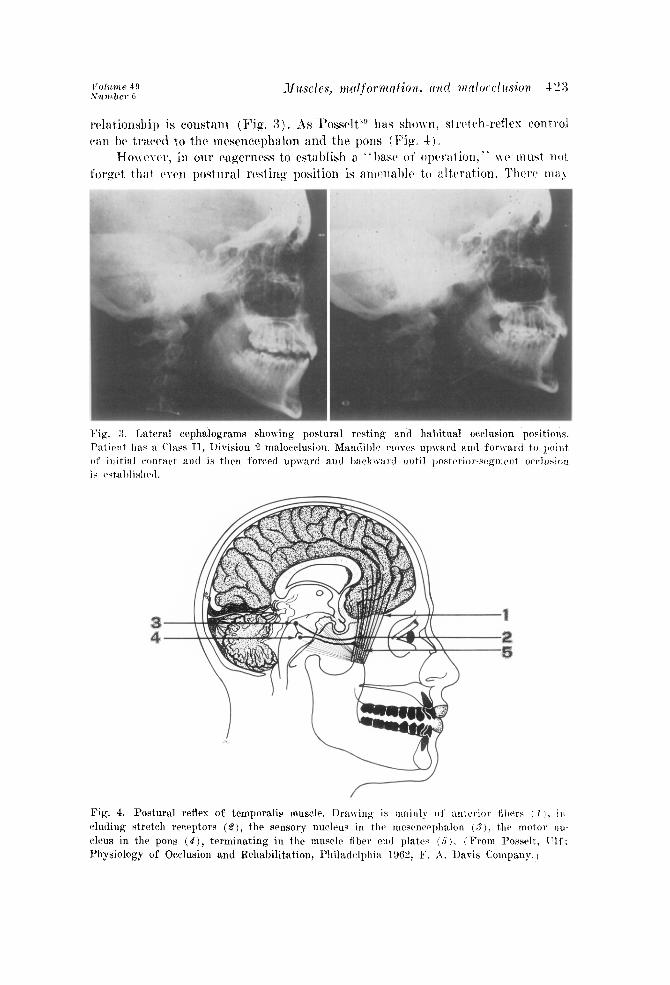
Fig. 3. TAsteral cephalograms showing postural resting and habitual occlusion posit,ions.
Patient has il Class 11, 1)ivision !? malocclusion. Mandible moves upward and forwwl to point of initial contart and is thrn foxed upwar and I)ac~k\\.:lrrl until 1lostc~l,iol-sc,glrlc~nt or~lu~:ic~n
is wtal)lishtd.
Fig. 4. Postural reflex of t,emporalis muscle. Drawing is m:linl) 01’ anterior tilwrs 1 I I, ill- duding stretch receptors (8), the sensory nu~lrus in tlw rl~esen~cl)llalon (‘I), the motor nw cleus in the pons (4)) terminating in the muscle fiber end plates (5 ). ( From I’osselt, 1’1C: Physiology of Occlusion and Rehabilitation, l’hiladclphi:~ 1962, K. A. Davis Company. 1

4“4 tklber I
be a measurable change from mornin g to night. Ncr~ous tension, prcmaturt: contacts, tcrnporomandibula~ *joint distur%ances, and homeostasis may all pro- duce variation, and these possihilitics should be checked whenever a postural rest registration is made.‘” I:sually such \-ariations as are produced are rninor and do not mitigate any more against the concept of postural resting position than does inherent variability in other areas of the body. Constant peripheral rc- cruitment of muscle fibers and tonus maintains the head in the position of best advantage, from which the active functions may be initiated with minimum effort.30 Thus, postural restin% position is hardly a system at rest in the truest sense. JVherr WC measure the total forces acting on the dental arches, i1 significant amount must bc credited to these subclinical, relatively minimal and y*t potent
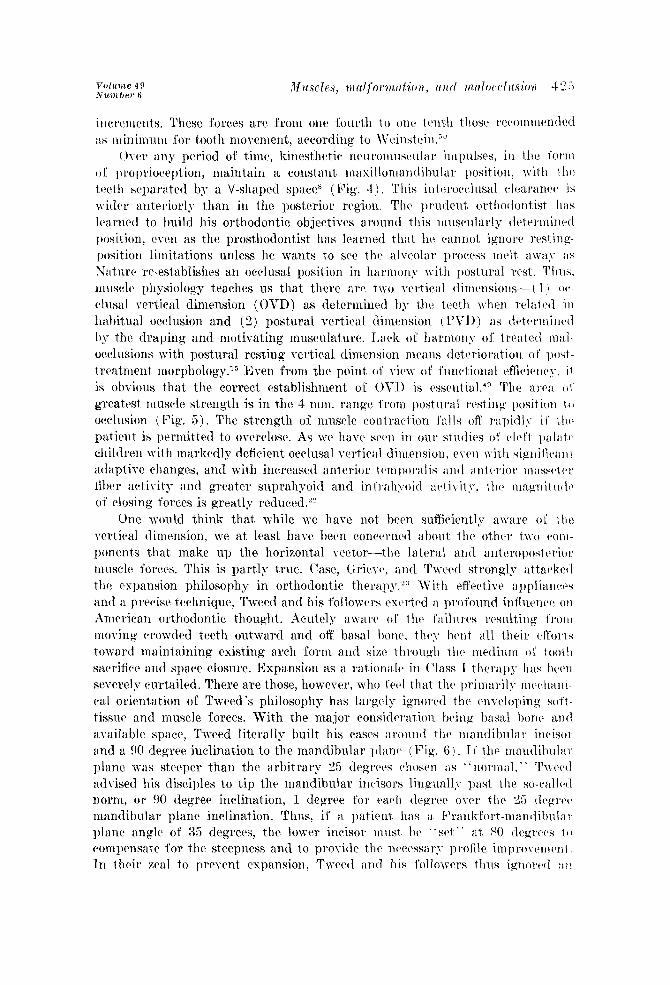
m AREA OF GREATEST MUSCLE STRENGTH
Fig. 6. Lateral eephalomctric tracings of mandible in open-mouth (1) and postural rest- ing (2) positions, occlusion (8 ), and overclosure (4). Positional influence of mandible on strength of muscle contraction is shown by the fact, that between 2 and 3 the greatest force is created. Magnitude falls off rapidly between 3 and 4.
illcrcwents. These forces arc from one fourth to onc1 tctnih I host ~c~c~olo~llc,rlclcItl
as minimuin for tooth movement, according to \Vcinstvin .“’ ( )JY~V any period ol’ time, kincsth~tic IIC’II~‘O~ILIIS(‘I~~~~~’ iltll)u lses, iu the fo1*111
of l~roprioctytion, maintain a constant iuwsilloii~alltlil,uli~~r position, with tlrca ttvdlr separated by a V-shaped space8 (Fig. 4). This iut~~~w~lus~il cl~avancc~ is wider anteriorly than in the posterior region. The pru(lent, orthodontist IlitS lwrncd to build his orthodontic objectives around this muscularly clt%rrnlinod position, cvtw as the prosthodontist has learned that hc vannot ignore rcM&- position limit,ations unless he wants to sw thch alV?Olar I)rOC’eSS lrl?lt a\\‘a>- ilS
Nat we re-establishes an occlusal position in harmony with postural wst. ‘~‘II~Is. muscle physiology teaches us that thcrc are two vertical ditncnsions--( 1 I (IV- ClUSill vertical dimension (OVD) as determined by thv twtli when relaicvl itI habitual occlusion and (2) postural vertical dimension (, L’\7D) as tlvt riix\i nwl 1)~ the draping and motivating musculature. I,ack of harmony of’ trcutt~tl l\tirl- occlusions with postural resting vertical dimension m~aris deterioration 0 f post - trcatnient n~orphology.15 Even from the point of view of func%ional efficic~rrq~, i l is obvious that the correct establishment of OVI) is csscnt ial.‘” The arw 01 greatest muscle st,rength is in the 4 mm. range i’rom l)ostural resting posil ion to occlusion (<Fig. 5). The strength of muscle contract ion i’alls off rapidly il’ t Ir(z piltiNlt is perxiittcd to overdose. As wc liavc ww in 0u1* stllciics 01’ ~lrfi pal;ltl~ children with markedly deficient occlusal vertical dimcwsion, even \\-ith sigllificwn I adapti\-e chang;cs, and with increased antcrior tcwlwrulis ant1 anterior maw~t (~1’ fil)er activity and greater suprahyoitl and inl’rah>-aid activity. thcl r\~;lgrrit\lci~~ of closing forces is greatly reduced.22
One would think that while wc have not hwn suffivicntlg aware oI’ the ycrtical dirnmsion, we at least haw been concerned i\bout the ot.hrr t\\o W~I-
ponrnts t,hat make up the horizontal vxtor-the latwal and autwopostwior muscle forces. This is partly t,rue. Case, Gric\c, anti Twed strongl>~ attwkr(l thtl expansion philosophy in ort,hodontic therapy.2:S With rffcctivc appliarrws and a prwisc trchniyue! Tweed and his followers cxcrtod :I profound inflwnw OH Amrrican orthodontic thought. hcutcly awaw ol’ t hc t’ailurcs rcsltlting YI’OIII moving crowded teeth outward and off hsal hone, thy- hcrrt ill1 their c>ffor~ s t~oward maintaining existin, 0‘ arch form and size throligh tlic medium (,I’ ioot!l sacrifice and space closure. Expansion as a rationale in (‘lass 1 thc~rul)y IlilS hew severely rurt,ailed. There are those, however, who frcl that the primaril>- mwhani- cal oricnt,ation of Tweed’s philosophy has largely ignored the t~nvc~loping so1’t- tissw and muscle forces. With the major considwation lwing lursal how ;Irltl arailable space, Tweed literally built his cases arolllltl the nmndihular incisor and a 90 degree inclination to the mandibular ~~l;rnc~ (Fig. 6 1. IC the tn;rntlihul;ll~ plant? \vas st,ecper than the arbitrary ‘II-, de$yws cllost~n ZIS + * norlnal, - ’ ‘r\wc~tl
advised his disciples to tip thr mandibular incisors 1inpuall;v I)ast the so-call~l norm, or 90 degree inclination, 1 degree for viwli t1rg.r~~~ owr t hr 25 tlrgwi~ mandibular plane inclination. Thus, it’ a patient, has a Fr.anlr fol.t-rnandihul;r I’ plane angle of 35 degrees, the lower incisor must. hv “SCI ” at 80 tl~gww I~J compensate for thr steepness and to provide thcl llPWsSi~I',T' p rofilr improwmc~nl In their ma1 to prcvcnt expansion, Twwl ar~tl his t’ollmwrs thus ignclwct at?

Tweed Triangle
Fig. 6. Cephalometric analysis by Charles Tweed. The larger the angle at 4 (the greater the Frankfort-mandihular plane angle), the smaller the angles formed at 1, .S and 3 must be to compensate for the genial olrtusenrss. The treatment objective is a 65 degree angle formed by the long axis of the mandibular incisors and the Frankfort horizontal plane at 5, 6, and ‘7. Mandibular incisors must he moved lingually to compensate for steep mandibular plane. The maxilla (shaded area) is ignored in this analysis, regardless of category of malocclusion.
equally important muscle force and mass--the t,ongue. The 90 degree incisor inclination by itself was a fict,ion, nonexistent as a “norm” in Nature; it was a convenient clinical creation that was obtainable by appliance manipulation but empiric and mathematical and unphysiologic. As Winders and others have shown, the functional forces of the tongue can be three t,o four times as great in some areas as the opposing lip and cheek muscles and can hardly he ignored (Fig. 7).
To expansion must be added contraction in Class I malocclusion, or in any category of malocclusion in which the teeth are tipped to arbitrary inclinations t,hat ignore the contiguous functioning muscle masses. For the extractionist, there is ample posttreatment evidence in the form of spaces in t,he extraction site, deepened overbite, crowding mandibular incisors, soft-tissue proliferation and all-too-frequent root resorption, and temporomandibular joint disturbances.‘” These sequelae arc of no less concern than the untoward effects of injudicious expansion. With expansion, we are at least moving the teeth in the direction in

whit*h normal growth and development nlity take thaw as the stomatognat hit. system develops its fullest potential through growth. Routitw twpiric tooth sacrifice at times gives the opposite impression of’ a general shrinking p~wcss.
Those who favor differential light-force trchniqnes qwnd a great dtwl 01’ time discussing the optimum force for moving a tooth, but many 01’ them havtx been no less guilty than proponents of the edgewise techniyucs in ignoring thus I)alant+ing &ret of contiguous muscle and the role of growth and devrloptwnt Teeth art’ often tipped to bizarre inclinations during one stag!> of treatment. lSwcssi\c lingual tippin, 0’ of incisors freyucntl~w wmains to cvicroach on ihc fotlgue space.
The thretv~imensional nature of muscle forces as they act on the dentition k
thns iipparcnt. In the rertical plane the postural considerations are dominant, :1nt1 \-et thtl orthodontist must also hc conwrnrd with the functions of wspira- lion, dcglutition, mastication, and speech-all ot’ which use the silmtx struc+tnws.
9/cm2 T !
; 3 4 5 7 7 p 9’pH’pl3’p15 30 50 70 90 II0 130 150 zoo 400 600 20,401 60180 ,I001 120~140~ 1
80q00~20~40~600,e002000 1 , ,
< \I
Mandibular .a..__
Depends on Overbkte
- Resting Pressures
Swallowing Pressures
Maximum Effort Pressures
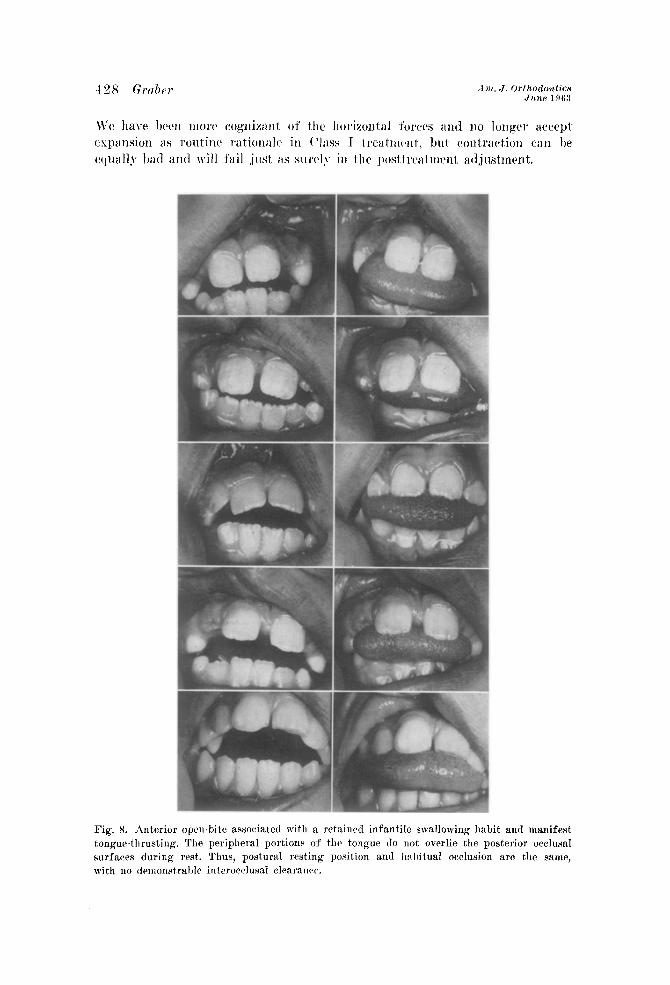
Fig.
surf: with
8. Anterior open-bite associated with a. rctaind infantile swallowing habit and mani ue-thrusting. The peripheral portions of the tongue do not overlie the posterior occl wes during rest. Thus, postural resting position and habitual occlusion arc the SE
no rl~monstral~le interocclusal clearanrr.
fest USRI

It, has been pointed out that muscle activity is normal in Class I I&OW~\I- sions in general, that Nature has given us the mold, and that we must vork within this frame of reference. In other \vords~ we start wit,h normal muaclc activity and we must maintain it. Some import;knt c~scq)tions, however. arv s(wI in the \arious types of open-bite (I*‘ig. 8).
The greatest, share of (‘lass I open-bite prohl(ws may 1)~ attributed to thumb- and finger-sucking, a rctainctl visceral or infantile swallowing llil hit, or a combination of both.“, 17. 3”. 31 This typo ol’ nlalocclusion providw an esccllcnt. example ot’ applied muscle phpsiology. The infant bcyins life with a wt~ll-d~~- vrloprd tongue-thrusting mechanism (Fig. 9). This nursing instinct is ow ot the best devcloped of all infantile movements and is qnitv a contrast, to t Ilc akimbo and apparently meaningless activities of thv cstremitics.‘” It is SD cfficicnt mwhanism, too, as the tongue darts forward innumc~rablc timw to obtain milk from the mother’s hrcast or from 21 rcwonahlc t’acsimilv thvrcwt’.
INFANTILE (VISCERAL) SWALLOW
ELONSATED TONBUE \
k MANDISULAR fRRU8T
MAXILLARY SUM PAD DEPRESSW CeNTRAL FURRDW
YANDIWLAR BUM PA LOWER TONSUE POIITION
NARROW TONBUE
Fig. 9. Iufantile swallowing mrchaoism. Plun~rrlikc wtion is assoriatrcl with nursing. (Ihrrli pads flow between posterior gum pads during nursing, unopposc~tl 1)~ pripheral portious (11 tongue. Associated with the tongue-thrust is the ant&or positioning of the mandible. The condyle may be felt gliding rhythmically forward aud l~:~~~lrwartL in the nursing act. Note concave midline contour of dorsum of tongue.

There are no teeth to get in the way, and the dominant posture of the tongue is one in which the center is depressed, the peripheral portions are raised, and the mass is elongated, ready for plungerlike action. The instinct is so powerful that the infant usually engages in the suckling act even when there is no nipple present. There is very little in the way of an articular eminence, so the mandible moves forward readily to assist in the nursing act. Lips purse and move rhythmically in unison.14
At about 5 to 6 months of age, as the incisors begin to erupt, certain proprioceptive impulses come into play and the peripheral portion of the
MATURE (SOMATIC) SWALLOW
HUMPED
REDUCED PERI-ORAL SPltlkCTER MOMENTARY INCISOR CONTACT
1 -j- NO MANDIBULAR THRUST
B
SHALLOW CEWTRAL FURROW
Hl0HER TONSUE POSITION
Fig. 10. Somatic swallowing mechanism. The dorsum is less concave and approximates the palate during deglutition. The tip of the tongue is contained behind the incisors; peripheral portions flow between opposing posterior segments. Anterior mandibular thrust has dis- appeared,
I~olume 4!) Muscles, nLcrlfot~nztrtio7~, wt1tl m~rlfmlusion -I:‘, 1 NlLTn her 6
tongue st,arts t,o spread laterally. This change in tongue function is a gradual one, and it is called the transitional stage.:” & the incisors erupt more fully, the peripheral portions of the tongue occupy t,he space between the remainin$z cdentulous areas of the upper and lower gum pads. and the rnorr rnatuw
somatic swallow is the result (Fig. IO). The lips closit~, and the incisors comtS together momentarily as the tip of the tongue lies behind thr incisors during tht> swallowing act. Actually, all postural muscles arc brought into play during this activity, as electromyographic studies hnvc sho~~.:‘~ i. 14. 13. IS. ?.i. ‘41. :x:. LII. 4!4
-1s the deciduous canines and molars erupt, the peripheral portions of the tongllr’ still overlie the occlusal surfaces during rest, as th(l mandible is mnintainctl at post,ural resting position. Thus, the tongue assists in maintaining the intc,roc‘- clusal space or clearance.
JYith any physiologic phenomenon there is a wid(L range of variations thiIt can lx.2 called “normal.” An average infant would show a dominant, and cx- clnsirc thrusting Ssceral swallow for the first 6 months of life, a transition;11 thrusting and lateral spread of the tongue during the next !-WY, and a dominanr somatic type of swallow, with the tongnc contained within the tlentition, thcal*ck. after.
It is considered normal for children to rngage in nonnntritivcb sucking during infancv.‘R Thr most common form is thumb- or finger-sucking (F’ip. 11) . Sinvc the mouth is the initial avenue of communication with the outside world. ant1 since the orofacial musculature is relatively ~~41 dcvclopcd, this nonnutrit ivcl sucking apparently gives the infant a fczling of warmth, a glow, a suw of satis- faction or euphoria that is closely linked to the infantile or visceral swallowing mechanism. As other avenues of communication with thtl outside world devclop~ as other muscle systems mature, and as visual and auditory stimuli Incomes meaningful, the euphoria induced by the oral activity assumt’s Itlss importan(~c. Tn the avcragc child, the nonnutritive sucking habits spontaneously tlisappc*al sometime bctwec‘n the sixth and cightecnth months 01’ life. In some childwo these habits may be normal for at least another year or so. That the thwsting action of the tongue is a primary instinct is shown by a stud\- of the c+hild with
athctoitl cerebral palsy who returns to primitive de~(~lopmcnt;ll ;lctirit irs anal
exhibits the monotonous thrusting of the tonglIe through most of his xlking l1oul’s.
There is a considerable body of opinion linking the nonnntritivr sucking habits with inadequate nursing and with poor nipple substitutcas alltl :l~t ifi& I nursing trchniqucs. I have reached t,his conclusion after ii stady ol’ II~OYC thitli 600 children with thumb- and finger-sucking problems in the last 17 ~(‘it~s.”
Whatt~ver the reason for the pcrsistcncc ot’ the finger-slicking habit (slov
physiologic maturation, inadequate or impropcv nllrsing methods, nipplr d(4gns which cnllancc the infantile thrusting and do not ;~llo~ thca dcv~~1opnrc~r1t 0:’ mo1~1 l~lilt\lrc somatic SW~~O\V during the tr.arlsitioll;ll st:lgtb. 01’ ])ossil)ly iI hvwdi t;ri*y (.Xiss II, 1)ivision 1 type of malocclnsio~~ \~hicll svcnis to dcmar~,l mo13-
nonnutr-itivc snrking bccansr of the child’s inability to thrust the uurrdihlc- forward sufficiently), the infant begins with a fing:ckr’ habit of sufficient intmsity. frequency, and duration to dcforrn the maxillary anterior segment. forcing this

432 GraOet
Fig IIlXJ pre;
the
. 11. Malocclusions associated with finger-sucking. 13ilatcJral narrowing of maxillary a 7 lw attributed to tongue-thrusting, lower wxting tougw posture, and excwsivr: but 3sures that arc a part of the infantilo swallowing mwhanism. Unilateral cross-bites result of a ‘( convenience swing’ : of the mandil~le to one side, with tooth guidance f~
.rch acal are
point of initial contact to habitual occlusion.
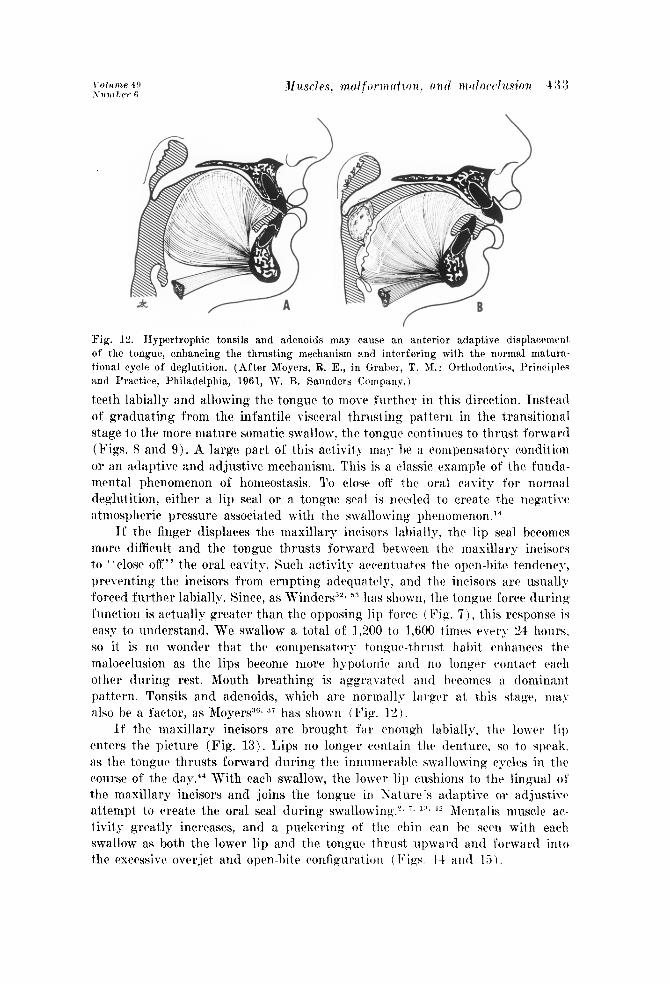
Fig. 12. Hypertrophic tonsils and adenoids may cause ai anterior adaptive displacement of the tongue, enhancing the thrusting mechanism and interfering with the normal mat,ura- tional cycle of deglutition. (After Meyers, R. E., in Graljer, T. M.: Orthodontiw, Principlrs and Przacticr, Philadelphia, 1961, IV. B. Saunders Company. I
teeth labially and allowing the tongue to move further in this direction. Tnsteati of graduating from the infantile visceral thrusting pattern in t,he transitional stage to t,hr more mature somatic swallow, the tongue continues to thrust forward (Figs. 8 and 9). A large part of this activity may be a compensatory rondit.ion or an adaptive and adjustive mechanism. This is a classic, rsamplc of the fnnda- mcrnal phenomenon of homeostasis. TO ~10s~ off the oral cavity for ncJm:il
deglutition, either a lip seal or a tongue seal is needed to create the ncgativc at,mospheric pressure associated with the swallowing pht~nonunon.14
It’ thr finger displaces the maxillary incisors labially, the lip sea,1 bccomcs more difficult and the tongue thrusts forward between the maxillary incisors to “close off” the oral cavity. Such activity accentuates the oprn-hite tendency, prcvcnting the incisors from erupting adequately, and the incisors arc nsuall~ forced further labially. Since, as Winders”“, 53 has shown, the tongue force during function is actually greater than the opposing lip force (Fig. 7)) this response is easy to understand. We swallow a total of 1,200 to 1,600 times cvrr>* 2-I hours. so it is no wonder that the compensatory tongtrc-thrust habit enhances thr malocclusion as the lips become more hypotonic and no longer contact each other during rest. Mouth breathing is aggraratctl i\Ild becomes a dominant pattern. Tonsils and adenoids, which are normall,v larger at this stage. ma\ also he a factor, as Meyers”“, 37 has shown (Fig. 12 )
If the maxillary incisors are brought far wough labially, the lower lip ent,rrs the picture (Fig. 13). Lips no longer contain the denture, so to speak. as the tongue thrusts forward during the innmr~crablc swallowing cycles in the course of the day.+’ With each swallow, the louver lip cushions t,o the lingual ot the maxillary incisors and joins the tongue in Xaturc’s adaptive or adjust,ivc attempt to create the oral seal during swallowing.‘. i. *13. ‘? Mentalis muselc ac- tivity greatly increases, and a puckering of the chin can be seen with each swallow as hot,h the lower lip and the tongnc thrust upward and forward into
the excrssivc ovcrjct and open-bite configuratic)n (, Pigs. 14 and 15).
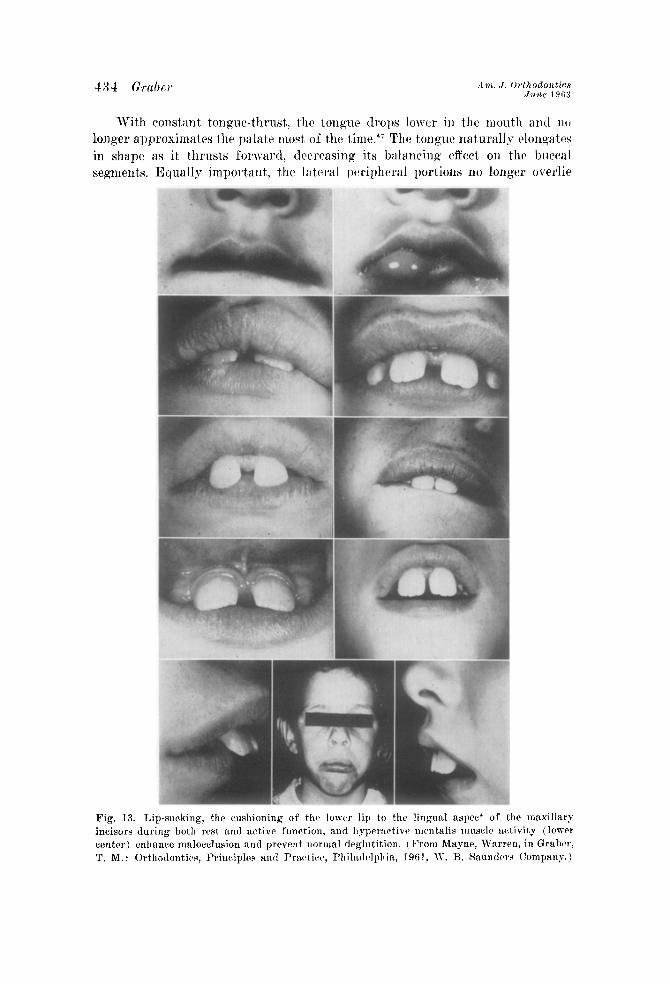
With constant tongue-thrust, th(l tongue drops lower in the mouth and no longer approximates the palate most of the time. 47 The tongue naturally elongates in shape as it thrusts forward, decreasing its hi~lancing effect on the buccal segments. Equally important, the lateral peripheral portions no longer overlie
Fig. 13 incisors center) T. M.:
. Lip-sucking, thr cwshioning of the lower lip to the lingual aspect of th f ma1 tillary during both rest and active function, and hypcractiw mrntalis musslc acti vity ( (IOJVCI
enhance malocclusion and prevent normal drglutition. (From Mayne, Warrtr I, in G rshw, Orthodontics, Prinriplrs and Practice, Pl~ilatlr~lpl~in, 1961, K. R. Baundcrs Corn1 my.)

VY
DERATE
SHT
@TJ$FJj Mental Muscle
Lateral Pterygoid Muscle Anterior Temporal Muscle Fibers
BEEI Middle Temporal Muscle Fibers Posterior Temporal Muscle Fibers Ant. 81 Post. Masseter Muscte Fibers
EZ3 Medial Pterygoid Muscle‘ Fibers m Supra 81 Infra- hyoid Muscle Action
Labii Superloris 81 lnferloris
the occlusal surfaces of the posterior teeth tllwing lwstural resting position. 1Iorphologic and functional changes go hand in ha~~tl, coach augmenting tl11~ other. \\‘ith changes in thc1 tongue, check, a11t1 lip ntusc~lv iunct,ions, thr net cffwt is a significant~ narrowing of the maxillary arch antI ovcreruption of th(l postwioy twth. Occlasal vertical dimension antI postural v(31*tical dimension ( OVl) and PVD) become one and the saiiie as thv intc~wcclusal space is elimi- natcd. A cross-bite condition is frequently crcwtc4 b,v the bilateral narrowing 01 the ruasill;~r~ arch, and the con\.micncc wilg 01’ nlantlibular displacerwr~l results in a deflection to one side or the otht,r from the point of initial cont;lct (Fig. 1 1). The open-bite is accentuated by this “ vicious c~irclr” activity. I’nlrss normal activity can be rcstorrd and a matuw soma tic swallowing habit, achirwct, the malocrlusion may well hc perpetuated and apgi*a~atc~d until Katnw ha< wtablishrd a condition of balance with hcretlitary pattern, basal bone limits, tooth size, contiguous tissue, the functions of mastication. respiration. sptwltl and post,urc as well as deglutition, and other as yet uneyuated factorxS”
As xc have dra\vn this pictuw of a tlcr~lopinp nialocelusion, it is easy to

‘Y
iRATE
HT
Mental Muscle Lateral Pterygoid Muscle Anterior Temporal Muscle Fibers Middle Temporal Muscle Fibers Posterior Temporal Muscle Fibers Anterior Masseter Muscle Fibers Posterior Masseter Muscle Fibers Medial Pterygoid Muscle Fibers Supra 81 Infra-hyold Muscle Action Labii Superioris 81 Inferioris
Fig. 15. Bar graph illustrating comparative muscle pressures associated with abnormal smal- loming. Note heavy mentalis and ‘lip activity, dominance of posterior temporalis and masseter fibers, and increased hyoid muscle action. (See Fig. 14.)
incorrect. It is entirely correct to say that the finger habit was the first assault on the integrity of the dentition and that the adaptive and compensatory activi- ties of the tongue and lip teamed up to provide a much more significant deform- ing mechanism. Without the original deforming activity by the finger, however, the subsequent lip and tongue a,ction might never have occurred. For this reason, it is considered a good interceptive orthodontic procedure to place an appliance which eliminates the finger habit before the arch is deformed sufficiently to require homeostatic muscle act,ion during deglutition (F’ig. 16).
The optimal time for appliance placement is between the ages of 31/1 and 41/ years, preferably during the spring or summer when the child’s health is at its peak and the sucking desires can be sublimated in outdoor play and social act,ivity. The appliance serves several purposes. .P’irst, it, renders the finger
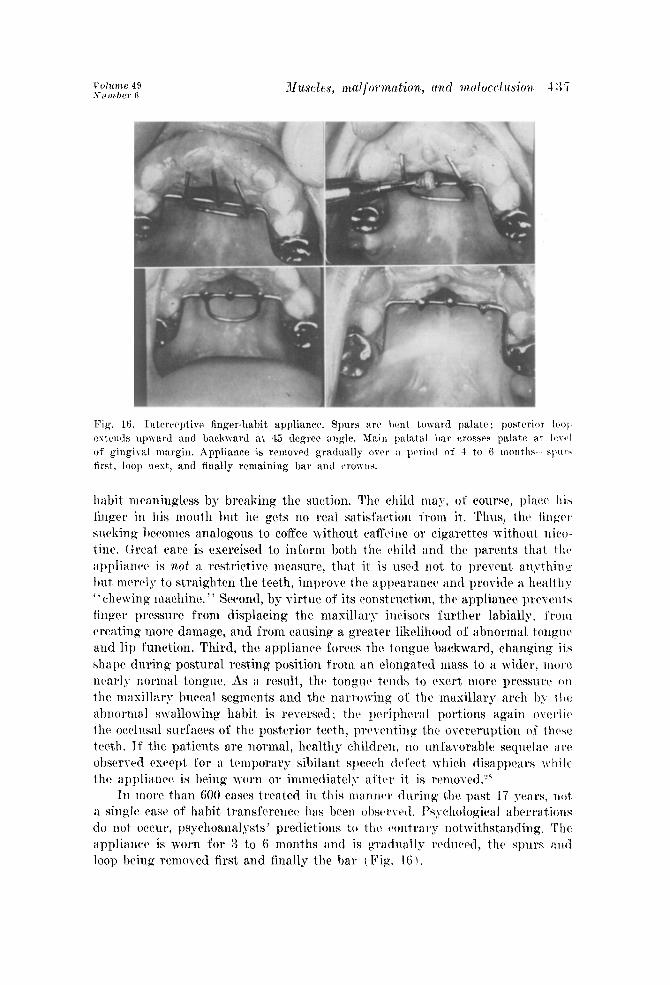
habit nl~~aningl<~ss by breaking the suction, The rhild may, of course, placx: ltis finger in his mouth but hc gets no real satisfaction I’rom it. Thus, the finger sucking l~ec~mes analogous to cofYee without caffrinc or cigarcttcs without, nicct- tint. (ireat care is exercised to inform both the child and the pa.rents that. t Irt* ilppliancc is not a restrictive measure, that it is used not to prevent anythinz but mcrcl1.y to st,raighten the teeth, improTe the appcarancc~ and provide a, health> ‘ ’ chewing machine. ” Second, by virtue of its construction, the appliance prrvcnts finger pressure from displacing the maxillary incisors further labially. frorll careating more damage, and from causing a greater likelihood of abnormal t,onguc and lip function. Third, the appliance forces the tongue ba.ckward, chanKing its shape during postural resting position from an elongated mass to a wider. ~OIY! nearly normal tongue. As a result, the tonpucl tends to csert more prcssnrc: on the mnxillar~ buccal segmcnt,s and t,hv narrowing of the maxillary arch by 1 tic> abnormal s\vallowing habit is reversrd; thti poriphcral portions again ovc*t*licb the occlnsal surfaces of the posterior teeth, prevc~ntin g t-hc owrernpt,ion of f.lrcw trcth. If’ the patients are normal, healthy children, no unfa~orahle sequela(~ a1-t: obscrvcd csccpt. for a temporary sibilant speech tlcfcct which disappears while the appliance is being worn or immediately at’tvr it is rrmo\~ed.y*
In morfl than 600 cases treated in this manntlr dnring t.hc past, 17 years, not a singIt> ease of habit transfcrencc has been obscrvtvl. Psychological aherrat.iorrs do not, occur, psychoanalysts’ predictions to the contrary not~~~ithst,andirl,. The appliance is worn for 3 to 6 months and is gradnally rc~~n~tl, tht> sln~rs :IH~ loop being ~wnoved first and finally the bar ( Fig. 16 1.
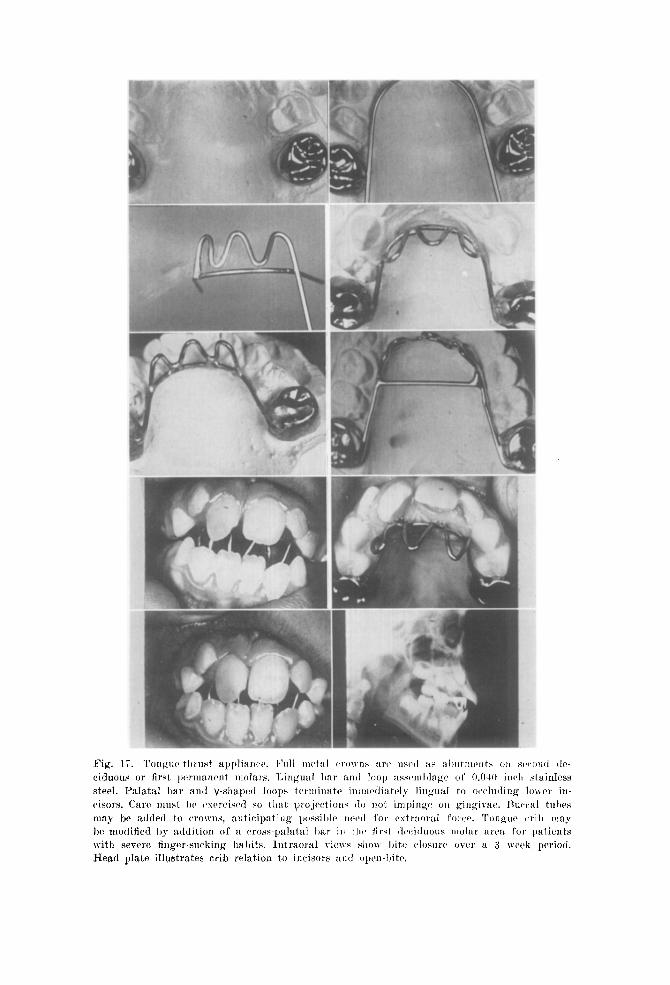
Fig. ciduc steel. cisor:
may be In with Head

F’ig. 18. Tongue and finger appliances incorporating cstraoral force auxiliary. If incLisors :w not I~anded (and this is usually the case), a 0.0411 iuch awlr J\-ire with vertical spriu~ loc~p- at molars :~nd soldered extraoral arm loops is fahricattvl. If iucisow are I,antM, ~v~rrid
anc~llorap assists in elongating incisors anti closing lli te. Lingu:tl crib is then cul oil’ :\n~l hands itw polisl~c~d down to permit finishing of the I.:I~(I witil tlstraoral for~c.
I f the occlusion has bcon sufficiently dcformt~d by the finger habit-, if ;I morphogcnetir pattern of incisor protrusion has bwn aggTUYi1tOtl i-b)- tllr finger habit to a degree requiring abnormal lip and tongnc function of an adapt iuc* nature, or if there is merely a retained infantile ton~?~t~-th~nsting habit instca(l of the more mature somatic swallow, a tongue-thrust appliance is used ( Fig. l’i). Its function and action arc similar to those 01’ the finger appliance just. described. The main purpose is to prevent the tongue from being insettetl into the open-bite 1,200 to 1,600 times a day, as it would bc if no applinnw wcr~’ present. The child is cncouragcd to learn the somatk swallowing habit by crawl- ing back of tht tongue and by the change in rrstin p shape. I’criphcral porliorrr of the tongue Occupy the intrrocclusal ClPtLrilll(‘e and rcstorc iI normal inl.ero+ clusal space and occlusal vertical dimension in harrtrorl~ with the postural vert iwi dimension. The anterior open-bite closes down as the incisors or*upt tmv;~ rtl ~(211
other and as the teeth are molded by the lip action. The strong action of the tongue working against the appliance may carise
the ov?rjct to lx increased, and it. is god pl’ilctif%~ to place ;t simple lill~i~ll :Iwh

and to use cervical extraoral I’orcc to rcducc the pro1 rusioik, thus oflsetting the: potent tongue forw (Fig. 18).
If’ the open-bitt is combined with au cwcssi~c ovor,jct and the: lower lil) 11;1s already entcrcd tht? picture, forcing llic maxillary incisors further labially because of hyperactivity of the mentalis muscle, and if a flattening or crowding of the mandibular anterior segment is in progress, a lip appliance is constructed
Fig. 19. Lip-habit appliance. A 0.040 inch I~ar is soldcrctl to full metal rrowns on stcond deciduous or first permanent molars. Bar may (‘row from lingual to labial eit,her mesial 01 distal to canine, depending on occlusion and anterior spacing. The operator should be sure that labial assemblage is 2 to 3 mm. anterior to labial aspect of lower incisors. Model is foiled first before endothermic acrylic is adapted to wire framework. Appliance is cemented in place for a period of 3 to 6 months, depending on severity of lip habit and amount of overjet.
(Fig. 19). Usnally this type of appliance is not ~Ieccssary if extraoral forw has been employed with the tongue-thrusting appliance. The mere elimination 01’ the exccssi\-c overjet usually permits homeostatic changes in muscle fund-ion. The lip no longer cushions to the lingual of the upper incisors, and mentalis musclr actiTit,y disappears. If the problem is primarily a lip or menta.lis muscle: condition or a lip-sucking habit, a lip appliance proves t4fective.
The lip appliance is constructed so that the labial wire and tho acrylic mass. ilrc sufficic~ntly gingiyal to the mandibular in&al margin to permit t,hr masillaq incisors to carnpt into a normal overbite. C’arc must, he escrcised to make sur(’ that, the lingual surface of the appliance is at least. 2 to 3 111111. Ii~biill to thtt
mandibular incisors so that the tongue may move thcsr twth forward into 21 normal arc and contact relationship. This is necessary to rc-rstablish the integrit> of thv lowr anterior segment and reduce thti horizontal overjet. The goal ot therapy is to permit the mandibular incisors to mow fnr enough labially ;III(~ t,hc maxillary incisors to drop far enough lingually to eliminate tht: cxwssiw owrjjct and the spare provided for abnormal lip action. H$peractivr menta lis muscle function will not disappear until. csrcssivc o\-el~jct is eliminated. ‘t’h~~ lip appliance is worn for 6 to 12 months, tlcprnding or) the severity of thcb problrtn. Rrcause of the obvious lcwrage problems and the forces working against thr wire framework, regular orthodontic bands arc usually inatlcc~uat o. Full nwtal crowns serve as excellent abutments for thcsc habit appliances, a1lt1 thy arc tvyc to place. There is no need to grin(l down thr occlnsa1 surfaws 01 eitliw the t,wth or t,hc crowns. since the opelI-bitt c*rcutcvl by thcb placc~mc~nl 01 thaw crowns quickly closes down within a wkek.
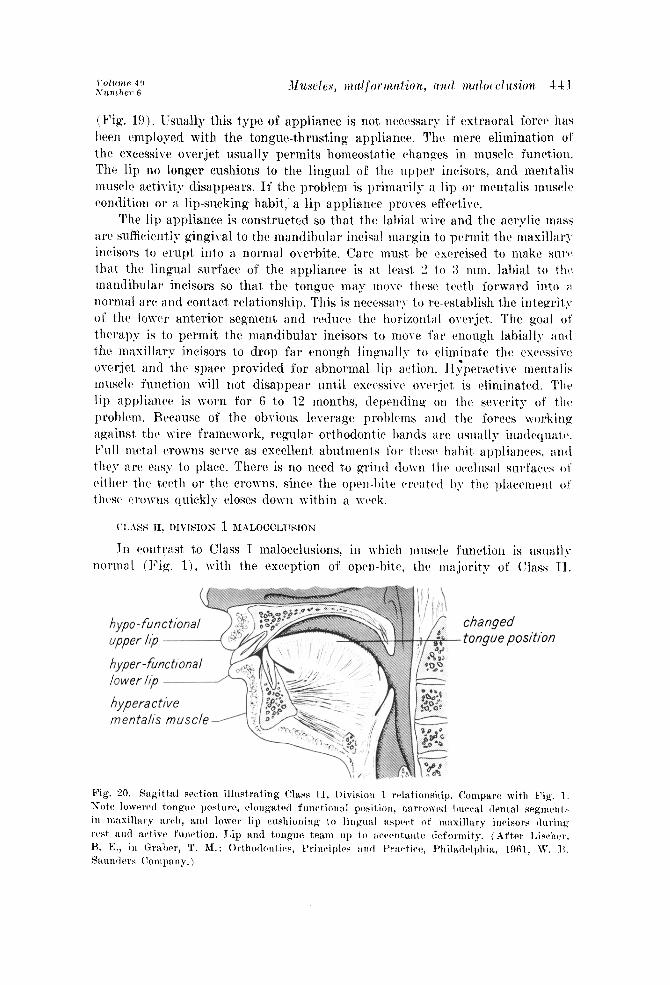
In caontr’ast t,o Class I malocclusions, in which lnuscle l’unct,ion is llsl~all> normal (Fig. l), with the exception of open-hito, thr ma.jority of (Ilass 11.
changed tongue position
Division 1 malocclusions do involve abnormal munclc a&\-it?- in the beginning (Fig. 20). In Class II, Division 1 therapy, a caliangc in muscle function is a requisite; expansion is a treatment objectirc. With a hereditary type of Class II malocclusion, the teeth merely reflect the abnormal anteroposterior da\\- w lationship, and the excessive overjet is a consequcncr. If we apply the same logic and the lessons that we learned in our analysis of the de\-elopment of open- bites in Class I malocclusions, it is easy to see why compensatory and adaptive muscle activity of an abnorrnal nature will enhance and perpetuate the Class 11 malocclusion.“4 The finger-suckin g habit or the retained I-isceral swallowing pattern is not a prerequisite to establishment of a favorable environment fox abnormal muscle activitp.‘a If a structural malrclationship exists, the muscle function adapts to t,his pattern as best it can in lint with the requirements of mastication, deglutition, respiration, and speech. The lower lip cushions to the lingual of the maxillary incisors, both at postural rest and during active func+- tion (Fig. 13). In some instances a lip-sucking habit develops, with the lowel lip mass almost constantly thrust into the cxccssivc ovcrjet. The lip itself map become hypertrophic as a result. The maxillary incisors move further labially, weakly resisted bp a hypotonic and relatively functionlcss upper lip (Fig. 8). The lower incisors buckle as the mandibular segment is flattened by continuousI> abnormal rnentalis muscle activity. The curbe of Spee increases. With the com- pensatory tongue-thrust,, loner tongue position, and increased buccinator muscle activity, the maxillary arch narrows and assumes the V shape so often associated with Class 11, Division 1 problems. Thus, the picture is similar to the open-bite problem just described in Class I malocclusions. 0 Open-bite occurs in Class II malocclusions also, but, it n-as described previously to emphasize thn fact that it can occur despite a normal jaw relationship. Abnormal muscle activity can thus create a pseudo Class II, Division 1 malocclusion, even wit,11 harmonious antcro- posterior jaw relations. A difference in true Class II, Mvision 1 problems is that the morphology and jaw relationship arc abnormal to begin with and muscle activity has only accentuated an existing pattern. In Class I open-bite and in pseudo Class II, Division 1 malocclusions, abnormal finger, tongue, and lip activity initiated the morphologic changes which, in turn, called on further abnormal muscle activity to meet functional demands and to compensate for the structural changes.
Orthodontic treatment of Class II, Division. 1 malocclusions should be di- rected first toward the creation of a ndrmal basal boric rrlationship which permits the muscles to function properly. The csta.blishrnent of a nortnal antcropostcrior jaw relationship, eliminating the excessive overjet and overbite conditions which have fostered adaptive muscle function, permits normal muscle activity.4” No longer is excessive buccal rnusclc pressure exerted on the posterior segment,s.’ Expansion of the buccal segments and an increase in maxillary intercanine width occur autonomously or can bc accomplished by means of orthodontic appliances. In line with our initial appraisal of the three-dimensional character of the muscle problem, this type of expansion is essential and qnitc stable :rft(>r the removal of all appliances. I~:lectrom~ographic research strongly substantiates this analysis.‘. I5

CLASS II, DIVISIOS il 3IALOCCI,U8IOS
The prccisc role of the musculature in Class II, Division :! malocclusion is more difficult to establish. A hereditary pattwn for the specific malocrlusion characteristics seems the predominant consideration. Activity of the c~hcrli anti lip muscles is usually normal, contrary to IXrision I. Thaw is some c~+ltwc~ to support thr contention that the tongue at lrast tends IO acwntuate the cxccs- sivc ~ww of Spee and that it interferes with the wuption of the postc~rior twtll by occupying the interocclusal space (E’ig. 21). If this is iiitlccd true, 1-h cow tlition would tend to increase the intcrocclusal clwrancc-and it is il fil('t tllilt in most, wsrs of Class Il, T)irision :! malocch~sion thcrcb is an c~sccssiw in1 (xl*- occlusal spaw. Because of the lingual inclination of the maxillary writ 1aal iti- cisors, combined with the excessive intcrocclusa I ~lcararw arid the in f~irc~l usiolt
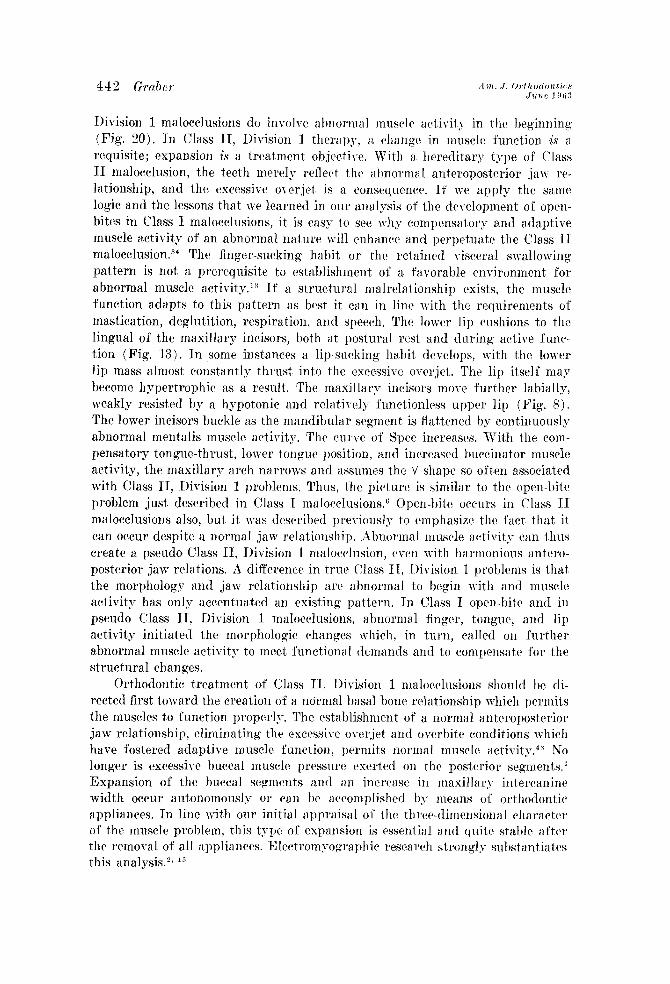
of the posterior teeth, functional guidance ot’ the tnandiblc is cpGic wmmo~~ (Pigs. 3 and 22). The mandible closes from postural rwting position to th(i point of initial contact. The lingually inclined maxillary incisors then guiclc> tht) mandible into a rrtruded position during the l~alancr of the closing 111onwc71t
to full orclusal contact~.~y!’ Electrompographica rrscarch shows that thcrc is ;I
compensator>- muscle a&v&p, with dominanw of thcx postrrior filw~ of’ both temporalis and masseter 11177sclcs from thca initial COIltilCt position to 1 hc posit ion of habitual occlusion (Fig. 23). The posterior-fiber dot~lin;~n(*r is c~liminatc~tl 1)~. properlv guided orthodontic therapy which rwtorw an o~*~~l~~sal wrt iral tlimc~rt - sion tllilt is in liarmon~ with the postural vortiwl dimc~nsion. Ihus c~liniii~:rlin~ tt1v ’ . forcod wtrusion ’ ’ phenomenon.
POSTKRIOR SUPKRIOR DlSbLAOKIYKNT
A,, ! A. \ 1: \ ; .i Fig. 22. Functional mandibular retrusion seen most commonly with a Class II, Division 2 malocclusion. Note overclosure and tooth guidance. 1, open-mouth position; 3, postural resting position; 3, initial contact; 4, habitual (retrudcd) occlusal position. With overclosure, the prospect is for reduced strength of muscle contraction and possibly reduced masticatory efficiency. (See Fig. 5.)
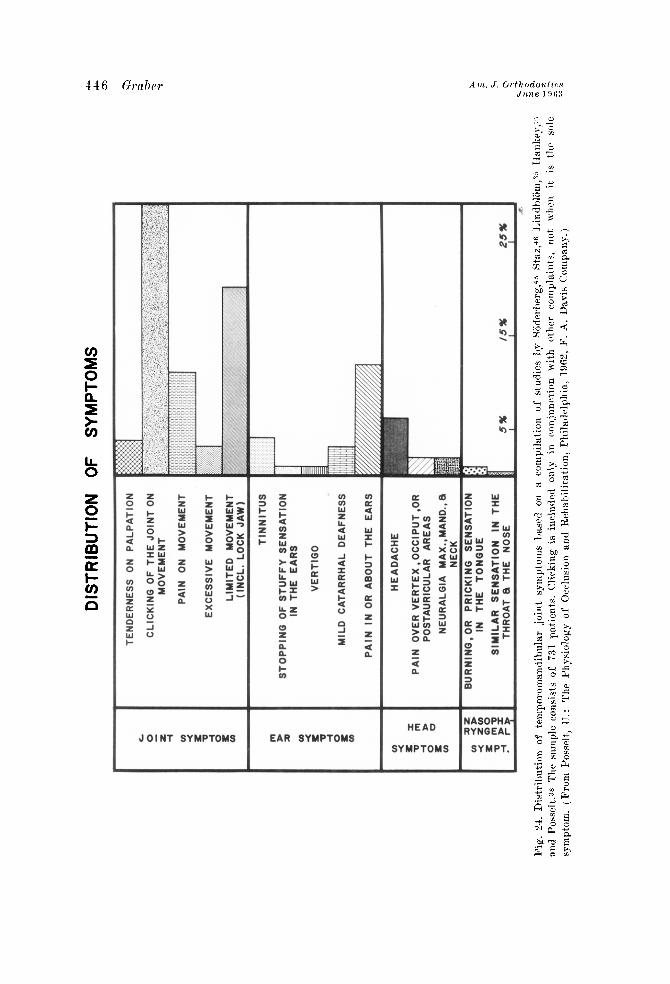
It is with tooth-guidanrc problems particularly, such as those encountered in Class II, Division 2 malocclusions, that temporomandibular joint problems arise,“, *SJ with clicking, crepitus, pain, and other vague but disturbing com- plaints. PosselP graphs the distribution (Fig. 24) and frequency (Fig. 25) of symptoms in 731. patients by combining the studies of Siiderberg,4” Staz,4” Lindbliim,:‘” Hankey,“’ and himself. 3S In the truest sense, tcmporomandibular joint, disorders may also bc considered muscle problems. From such nonhomeo- static phenomena as the inability of muscles to adapt to morphologic variation and changing functional demands, their sclectivc activity as shown by electro- myographic research, their occasional disregard for proprioceptive warnings of
Illc rcflcx arc, illld their occasional trismic or uncoordinated response? to t Ilvsc~ stimuli wmes the t~l~l~~o~0l~l~~dih~lli~ r joint s?-mpptomatolop!-.
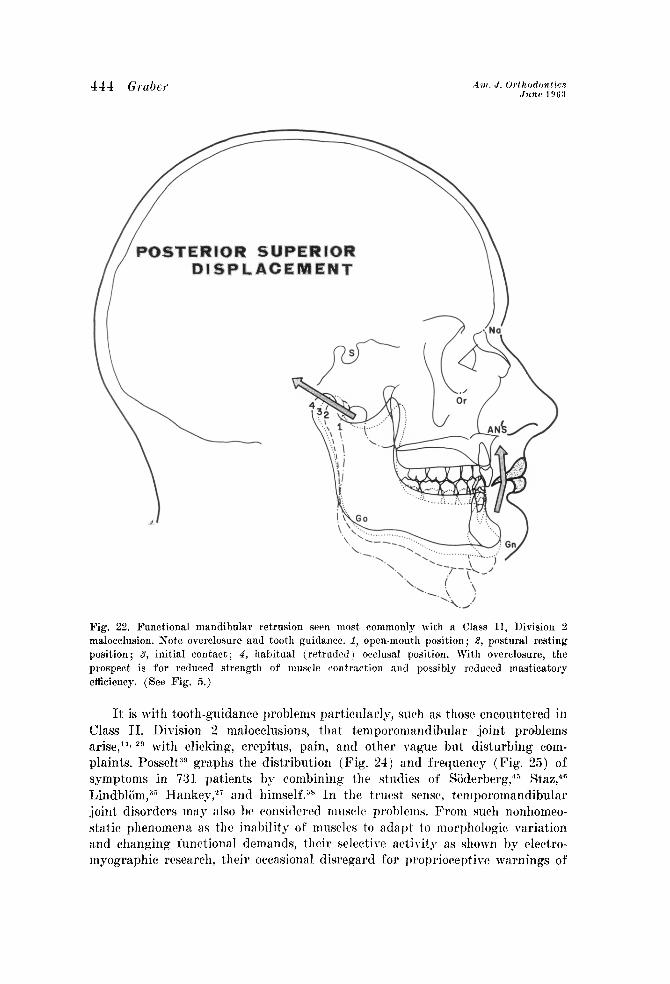
Tn Class 1II malocclusion, as in Class II, TXvision 1. wc arc dealing with a dominant bone dysplasia, with adaptive muscle function and tooth irregularit,ics reflect.ing a severe basal dysplasia. All three systc?nls-lwnc. ttlet,h, and musclw
-are involved. Here again, there is a stron p hereditary pattern. The upper lip is relatively short, though not necessa.rily h>-potonic. The lower lip is hypvr- trophic and redundant and appears to bc relatively passive during the tlegluti- tion cycle (Fig. 26). During swallowing, T-hew is actually a gwater activity ot the upper lip. The tongue is a potent force, although it is not, clear whether the tongue nmss or tongue function is the basis for the lingual “cupping out” l~h- neat11 t,hr mandibular teeth. The tongue does appear to lie lower in the floor 01 the mout,h. Since the maxillary arch does not llave the h;\l:~rl&~ t#ctt oi’ ton~w
\I A-
WL== I 5
Fig. 23. Muscles primarily responsible for mandibular functional movements. 2, Anterior ant1 posterior fibers of temporalis; 8, lateral pterygoid; 5. anterior, middle, and posterior com- ponents of masseter; 4, suprahyoid; 5, infrahyoid. Medial ptrrygoid not shown. In forced retrusion, electromyographic records shox a dominance of posterior temporalis, posterior masseter, and posterior suprahyoid muscles. Resistance to posterior condylar displacemrnt by the lateral pterygoid muscles (2) is apparently insufficient, since primary function is that of opening, not closing, and secondary stabilizing assignment on closure can result io txeessive forward movement of the articular disc on maximum contraction. (hfter Pox&t,, U. : The Physiology of Occlusion and Rehabilitation, Philadelphia, 1962, F. A. Davis Company. 1
DIS
TRIB
UTI
ON
O
F S
YM
PTO
MS
CLIC
KINB
OF
TH
E JO
INT
ON
MOVE
MENT
PAIN
ON
MO
VEME
NT
EXCE
SSIV
E MO
VEME
NT
STOP
PINO
OF
ST
UFFY
SE
NSAT
ION
IN
THE
EARS
MILD
CA
TARR
HAL
DEAF
NESS
PAIN
OV
ER
VERT
EX,
OCCI
PUT
,OR
POST
AURI
CULA
R AR
EAS
Pig.
24
. Di
stribu
tion
of te
nlpor
olllan
(libula
r joi
nt
symp
toms
base
d cm
a
comp
ilatio
n of
studie
s hy
Si
iderl)
erg,
43 S
taz,-‘e
IA
indhli
im,~
~ Ha
nkr\-
,a;
and
Poss
rlt.38
Th
e sa
mple
vons
ists
of 73
1 pa
tients
. Cl
irking
is
includ
ed
only
in co
njunc
tion
with
oth
er
c~om
plaint
s, no
t wh
en
it is
the
sole
symp
tom.
(From
Po
sselt
, TJ
.: Th
e Ph
ysiol
ogy
of Oc
clusio
n an
d Re
habil
itatio
n,
Phila
delph
ia,
1962
, I’.
A.
Davis
Co
mpan
y.)
mass, and since the peripheral portions of the tongue are less apparent betwixt the occlusal surfaces, the maxillary arch is usually narrow and the interocrlnsal space is either very small or entirely absent,. IDuring the deglutition cycle, there is greater mobility of the hyoid bone as the suprahgoid and infrahgoid muscit~s demonstrate greater activitv.
It is difficult to assess how much of’ the muwlc activit,v is homcostat ic, compensatory. or adaptive to the structural malrelationsl~ip and how murh ot’ it
CLICKINO OF THE JOINT ON MOVEMENT
LlWfED MOVEMENT (INCL. LOCK-JAW)
PAIN IN OR ABOUT THE EARS
PAIN ON MOVEMENT
HEADACHE
TENDERNESS ON PALPATION
TINNITUS
EXCESSIVE MOVEMENT
MILD CATARRHAL DEAFNESS
PAIN OVER VERTEX, OCCIPUT. OR POSTAURICULAR AREAS
NEURALQIA MAX., WAND.,a NECK
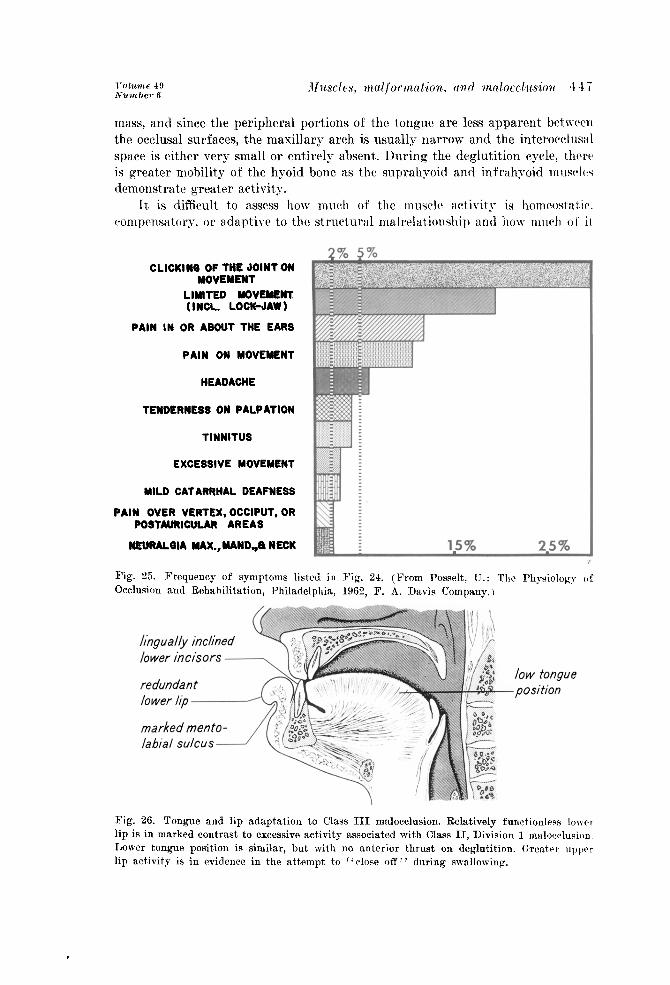
Fig. 25. Frequency of symptoms listed in Fig. 24. (From Posse& U.: The Physiology oi Occlusion and Rehabilitation, Philadelphia, 1964, F. A. Davis Company.)
redundant low tongue
-position
Fig. 26. Tongue and lip adaptation to Class III mdocclusion. Relatively functionless loner. lip is in marked contrast to excessive activity associated with Class II, Division 1 malocclusion. Lower tongue position is similar, but with no anterior thrust on deglutition. Greater upper lip activity is in evidence in the attempt to i ‘close 06’” during swallowing.
448 Graber Am. J. Orthodontacs June 1963
is in itself due to morphogenetic pattern. Very probably, depending 011 the case, the proportions vary. As in the Class I and Class II malocclusions, the threc- dimensional character of the muscle problem is again emphasized. Muscle forces are a significant factor of vertical, lateral, and anteroposterior dimensions.
An analysis has been made of muscles and their relationship to structural configuration in Class I, Class II, and Class III malocclusions. The effect of muscle forces is three-dimensional, although most orthodontists have considered it only in one vector-that of expansion. Whenever there is a struggle between muscle and bone, bone yields.5 Muscle function can be adaptive to morphogenetic pattern. A change in muscle function can initiate morphologic variation in the normal configuration of the teeth and supporting bone, or it can enhance an already existing malocclusion. In the latter instance, the inherent structural malrelationship calls for compensatory or adaptive muscle activity to perform the daily functions. The structural abnormality is increased by compensatory muscle activity to the extent that a balance is reached between pattern, environ- ment, and physiology. At times it is impossible to assign a specific cause-and- effect role to any one factor. It is imperative that the orthodontist appraise muscle activity and that he conduct his orthodontic therapy in such a manner that the finished result reflects a balance between the structural changes obtained and the functional forces acting on the teeth and investing tissues at that time.
REFERENCES
1. Alderisio, J. P., and Lahr, Roy: An Electronic Technique for Recording the Hypo- dynamic Forces of Lip, Cheek, and Tongue, J. D. Res. 32: 548-553, 1953.
2. Andersen, W. S.: The Relationship of the Tongue-Thrust Syndrome to Maturation and Othrr Factors, Aar. J. ORTHODONTICS 49: 264-275, 1963.
3. Angelone, L., Clayton, J. A., and Brandhorst, W. S.: An Approach to Quantitative Electromyography of the Masseter Muscle, J. D. Res. 39: 17-23, 1960.
4. Ardran, G. M., Kemp, F. H., and Lind, J.: A Cineradiographic Study of Bottle Feeding, Brit. J. Radio]. 31: 11-22, 1958.
5. Asling, C. W.: Recent Developments in Biologic Studies of the O&eous System, AM. J. ORTHODONTICS 47: 830-843, 1961.
6. Baker, R. E.: Tongue and Dental Function, AX J. ORTHODONTICS 4Q: 927-939, 1954. i. Ballard, C. F.: The Aetiology of Malocclusion-An Assessment, D. Practitioner 3: 42-50,
1957. 8. Baril, C., and Moyers, R. E.: An Electromyographic Analysis of the Temporalia Muscles
and Certain Facial Muscles in Thumb and Fingersucking Patients, J. D. Res. 39: 536- 553, 1960.
9. Barrett, R. H.: One Approach to Deviate Swallowing, AY. J. ORTHODONTICS 47: 726-736, 1961.
10. Bosma, J. F.: Maturation of Fun&ion of the Oral and Pharyngeal Region, AM. J. ORTHO- DONTICS 49: 94-104, 1963.
11. Choukas, N. C., and Sicher, H.: The Structure of the Temporomandibular Joint, Oral Surg., Oral Med. & Oral Path. 13: 1203-1213, 1960.
12. 1)i Salvo, N.: Neuromuscular Mechanisms Involved in Mandibular Movement and Pos- ture, AM. J. ORTHODONTICS 47: 330-342, 1961.
13. Dixon, D. A.: An Investigation Into the Influence of Soft Tissues on Tooth Position, T). Practitionrlr 10: 89-92, 1960.
14. Doty, R. W., and Bosma, J. F.: An Elcctrom~~ogral)llic ,\nalysis of Reflex 1)eglutition.
J. Neurophysiol. 19: 44-60, 1956. 15. Ekleberry, J. W., and Eggleston, W. B.: An Electroolyograpl~ic and Funet~iomal Evalut-
tion of Treated Orthodontic Cases, Master’s thesis, I-Ioraw EC. Rackham School of Graduate Studies, University of Michigan, Ann Arbor, Mich., 1961.
16. Eskcw, II., and Shcpard, E.: Congenital Aglossia, AM. .J. ORTHOUOETICS 35: 116-119, 19 k!). 17. Fletcher, X. G., Castreel, R. I,., and Bradley, I). 1’. : Tongue-Thrust S\rallow, Sp~‘~~‘li
Xrtic,ulation and age, J. Speech & Hearing Nrorders 26: %01-%0X, 1961. 18. Franks, A. 8. T. : Electromyography Relative to t hc Storll:ltogn:rthic System. I). l’i,:i.,-
titioner 8: 32-37, 1957. 19. Gardiner, J. II.: Congenital Partial Aglossia, 1). Practitioner 10: 83-87, 1960. 20. Graber, 7’. M.: Physiological Principles in Dentistry, Washington IInivcrsity 1). .I. 23:
35.43, 1957. 21. (?raIwr: T. M.,, Bzoch, K., and Aoba, T.: A Functional Sttnly of the IWatal and Plr:~r,vn-
geal Structures, Angle Orthodontist 29: 30-40, 1959. 22. Graber, ‘I’. M.: Orthodontics: Principles and Practiw, Philadelphia, 1961, \V. lx. ~;auii(lt~rs
company. 23. Grsber, T. M.: Role of Muscle in Malocclusion, Tr. European Orthodont. SW:. pp. I-?(‘.
1961. 24. Graber, T. M.: Current Concepts of Orthodontic Twntmc~nt in thf~ United States. .\w
t,ralian 1). J. 7: 355-362, 1962. 25. Grossman, W. J., Greenfield, 1% E., and Timms, 1). .J.: Elrctrolrl~ogra~~hy as an .\irl in
I)iagnosis and Treatment Analysis, AI\I. J. ORTHOIKIKTIW 47: 481~49i, 1961. 26. (;\\-?~II~,-~:~:~IIs, E., and Tulley, W. J.: Clinical Tyln’s, I). l’rac~titiowr 6: ZZZ-%i, l!),>H. 27. Ilaukry, (:. T. : Affections of the Tc~~~l~oron~~~ntlil~nl:rr .loint, I+ov. Roy. SOV. hl(l11. 49:
9S3094 1956 t.; . 28. Barrington, Robert, and Brrinholt, M. A.: The Rrhtion of tllch Ora1-1M~~~~llanisr,r >I::1
function to 1)cntal and Spcccli l)c~relopment, AM. .I. ORTHOIN~NTI~~S 49: ‘II-!I:+, l!lti:(. 29. fljorts,jo, C. : Studies on the Mechanics of the Tolrll~~)r”r~~:~r~~lil~lll:tr Joint, l,nn~I. S\Y~I~~~II.
1055, (1. W. 1~. Gleerup Publishers. 30. IIorell, J. 11. : Recent Advances in Orthodontics, Brit. 1). .I. 98: 11-L. 122, 1935. 31. Ilovt~ll, .T. 11. : The Relationship of the Oro-facial Musculature to Owlusion : (.‘uri~~~iii
13ritieh Thought. Zn Kraus, R. R., and Kictlrl, R. (tbtiitor3 / : Vistils in Orttlo~i~lirl ii.<:. l’l~ilx~l~~lplrin, 1962, Lea & Febigcr, pp. 328-313.
32. liaires. AY. I(.: Palatal Prrssurw of the Tongw in l'howti~~~ iin11 l)c~glutition, .l, l’l,~li. Bent. 7: 305-317, 1957.
33. Knw:mlul~at Y . . . Neuromuscular Mechanisms of Jar: ;rii~l ‘Tongue M~wwents, ,1 -A in. I lent A. 62: &j-551, 1961.
34. Kydd, VT. lb: Maximum Forces Exerted on the I)rwtition 1)~ the Perioral a1111 i,iiigu;il &Iusculature, J. Am. Dent. ,I. 55: 646.651, 1957.
35. Lin~lbliirn, 0. : 1 risordrrs of the Tcnll~oro~~1a~~tli~~ulxr Joint, .\rl;i atlout. w:irilliu:i~. 11: 61-94. 1953.
36. Moyrrs, R. E.: Handbook of Orthodontics, Chicago, 1958, Wearl)ook l’ul~lishwr, 111~. 37. Meyers, R. E. : The Role of Musculature in Orthodontic Triagnosia and ‘l’watmt~nt I’laii-
ning. In Kraus, Ii. H., and Riedel, R. (etlitow j : \‘istas in Ortliodontiw, I’l~il:~~l~~l~~l~i:~, 1962. I.(‘:~ B Febiaer, pp. 30%3%7.
38. Possrlt, C. : Ansikts- och liZkledssnlbrtor-diiagnc~s oeh ltt~hnn~lling (%itelwrgs ‘t’atull.. Sallskaps Arsbok 9: 104.124, 1958.
39. I’osselt, Ulf : The Physiology of Occlusion and Rehabilitation, I’liil:~delpliia, 1962. l’. -\. I)avis (:ompany.
40. Ralston, H. J.: Uses and Limitations of Electromyographg in the Quantitative Study ot Skeletal Muscle Function, AM. J. ORTHODONTICS 47: ;721-540. 1961.
41. Rogers, J. H. : Swallowing Patterns of a Normal l’opulation Sample Compared to ‘I’h~w~ of Patients From an Orthodontic Practice, ;\x .J. ~~KTHODI.~STIW 47: 674-6X9. 1961.
42. Sclaw. R.: The Trapped I,ower Lip, Rrit. 1). .T. 102: ?#--l(~3, 1937.
450 &abet Am. J. Orthodontics Jww 1963
43. Scott, J. H.: The Role of Soft Tissues in Determining Normal and Abnormal Dental Occlusion, D. Practitioner 11: 302-308, 1961.
44. Shelton, R. L., Bosma, J. F., and Sheets, B. V.: Tongue, Hyoid and Larynx Displace- ment in Swallow and Phonation, J. Applied Physiol. 15: 283-288, 1960.
45. SBderberg, F. : Malokklusion-arthrose-otalgie, Acta oto-laryng. scandinav. Supp. 95, pp. 85-98, 1950.
46. Staz, J.: The Treatment of Disturbances of the Temporomandibular Articulation, J. D. A. South Africa 6: 314-335, 1951.
47. Straub, W. J.: Malfunction of the Tongue, AM. J. ORTHODONTICS 47: 596-617, 1961. 48. Swindler, D. R., and Sassouni, V.: Open Bite and Thumbsucking in Rhesus Monkeys,
Angle Orthodontist 32: 27-37, 1962. 49. Tulley, W. J. : Adverse Muscle Forces: Their Diagnostic Significance, AM. J. ORTHO-
DONTICS 42: 801-814, 1956. 50. Weinstein, S., Haack, D. C., Morris, L. Y., Snyder, B. B., and -4ttaway, H. E.: On an
Equilibrium Theory of Tooth Position, Angle Orthodontist 33: l-26, 1963. 51. Wildman, A. J.: Analysis of Tongue, Soft Palate, and Pharyngeal Wall Movement, AhI.
J. ORTHODONTICS 47: 439-461, 1961. 52. Winders, R. V.: Forces Exerted on the Dentition by the Perioral and Lingual Muscula-
ture During Swallowing, Angle Orthodontist 28: 226-235, 1958. 53. Winders, R. V.: Recent Findings in Myometric Research, Angle Orthodontist 32: 38-43,
1962.
450 Green Bay &I.
Related Documents











