The status of the myocardial arterioles in angina pectoris Briatz M. More, M.D.* Sheldon C. Sommers, M.D. La Jolla, Calif. T he symptom complex of angina pec- toris is nowadays public knowledge and a medical commonplace. It is surpris- ing that the first clear reference to the disease in the literature appeared as late as the seventeenth century.’ In the latter half of the eighteenth century, William Heberden2 wrote a classic description of the symptomatology of angina of effort and placed it among the spasmodic com- plaints. Some years later, Parry3 uncovered the association of angina with ischemia of heart muscle. Authorities now agree that the angina1 syndrome is due to myocardial anoxemiaG4J Osler6 described a number of diseases as- sociated with angina1 pain, but degener- ative coronary artery disease is by far the most common etiological agent. LenPgre and Himbert found significant coronary atherosclerosis in 80 per cent of necropsy hearts in an unselected angina1 group; and when angina had been the only clinical abnormality, significant atherosclerosis was present in 100 per cent of the cases. The important investigations of Blum- gart, Schlesinger and Davis,8 and Zoll, Wessler and Blumgartg involved injecting the coronary system with a radiopaque mass but did not include a systematic study of the walls of the small arteries and arterioles. The conclusion was that the theory that arterial spasm produced relative myocardial ischemia was unproved, but that spasm and vasomotor effects which reduce coronary flow are in no way incompatible with the widespread patho- logic effects demonstrated. There is a paucity of descriptive or quantitative morphologic studies of the small intramural coronary arteries in patients with angina1 heart disease. For years, one of us (S. C. Sommers) had noted that the myocardial arteriolar walls were thicker than usual in patients with angina. The senior author was uncertain whether this relationship existed. Consequently, these vessels have now been measured in order to determine whether they exhibited a muscular hypertrophy that would be consistent with a spastic tendency in life, and whether they demonstrated any unusual thickening or significant luminal narrowing that would contribute to the adverse effects of obliterative and sclerotic disease of the larger vessels. The statistical an- alyses subsequently performed were not utilized to establish that differences existed, but to estimate the degree of the arteriolar alterations in angina that had become evident from the histopathologic study. Materials and methods Histologic sections were made from 50 necropsy hearts. The angina1 group con- sisted of 20 hearts taken from subjects with Received for publication Nov. 2, 1961 *Present address: 12A Columbia Road, Edinburgh, Scotland. 323

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The status of
the myocardial arterioles in angina pectoris
Briatz M. More, M.D.*
Sheldon C. Sommers, M.D.
La Jolla, Calif.
T he symptom complex of angina pec- toris is nowadays public knowledge
and a medical commonplace. It is surpris- ing that the first clear reference to the disease in the literature appeared as late as the seventeenth century.’ In the latter half of the eighteenth century, William Heberden2 wrote a classic description of the symptomatology of angina of effort and placed it among the spasmodic com- plaints. Some years later, Parry3 uncovered the association of angina with ischemia of heart muscle.
Authorities now agree that the angina1 syndrome is due to myocardial anoxemiaG4J Osler6 described a number of diseases as- sociated with angina1 pain, but degener- ative coronary artery disease is by far the most common etiological agent. LenPgre and Himbert found significant coronary atherosclerosis in 80 per cent of necropsy hearts in an unselected angina1 group; and when angina had been the only clinical abnormality, significant atherosclerosis was present in 100 per cent of the cases.
The important investigations of Blum- gart, Schlesinger and Davis,8 and Zoll, Wessler and Blumgartg involved injecting the coronary system with a radiopaque mass but did not include a systematic study of the walls of the small arteries and arterioles. The conclusion was that the theory that arterial spasm produced
relative myocardial ischemia was unproved, but that spasm and vasomotor effects which reduce coronary flow are in no way incompatible with the widespread patho- logic effects demonstrated.
There is a paucity of descriptive or quantitative morphologic studies of the small intramural coronary arteries in patients with angina1 heart disease. For years, one of us (S. C. Sommers) had noted that the myocardial arteriolar walls were thicker than usual in patients with angina. The senior author was uncertain whether this relationship existed. Consequently, these vessels have now been measured in order to determine whether they exhibited a muscular hypertrophy that would be consistent with a spastic tendency in life, and whether they demonstrated any unusual thickening or significant luminal narrowing that would contribute to the adverse effects of obliterative and sclerotic disease of the larger vessels. The statistical an- alyses subsequently performed were not utilized to establish that differences existed, but to estimate the degree of the arteriolar alterations in angina that had become evident from the histopathologic study.
Materials and methods
Histologic sections were made from 50 necropsy hearts. The angina1 group con- sisted of 20 hearts taken from subjects with
Received for publication Nov. 2, 1961 *Present address: 12A Columbia Road, Edinburgh, Scotland.
323
324 More and Sommers .4m. Heart .I. Sc~~trmbcv, 1962
Table I. Age, sex, duration oj’ angina and diseases in control cases
A nginal CO?itiol / Normu
-.___
$ 1 Lse.y~Lc$i~~r,.. g sexl~~ Diseesc if;’ &.+g, Di.seusr
43 hl 340 1 44 A4 410 Lymphoma 23 F 180 Injuq 47 M 700 6 44 i\l 380 Mesenteric infarct 24 M 320 Thymic
carcinoma 51 M 400 “Recent” 52 M 230 Lymphoma 2.5 M 320 Injures 54 hl 460 4 55 M 340 Carcinoma of colon 25 M 4.50 Injuq 54 M -~- Long stancl- 57 ikl 440 Cirrhosis 28 M 280 Brain tumor
ing 58 hl 4.50 “Some” 58 Al 490 Mediastinal goiter 31 F 30.5 Polio 6 3 h,l 370 l’,i 59 WI 310 Carcinoma of lung 34 M 400 Polio 66 hl 450 2 64 M 170 Carcinoma of esophagus 3.5 F 350 Polio 67 M 610 10 67 M 190 Lymphoma 35 F 270 Polio 67 M 570 5 67 M 290 Carcinoma of stomach 38 M 360 Polio 69 F 450 15 68 M 500 Carcinoma of lung 70 F 380 8 71 F 290 Transverse myelitis 70 M 600 “ullknown” 71 M 380 Carcinoma of lung 72 h,l 570 10 72 M 370 Reticulum cell sarcoma 73 R/z 870 17 72 M 510 Septicemia 74 M 440 2 73 hl 280 Carcinoma of stomach 75 M 550 7 74 h4 .-~ Carcinoma of appendix 77 F 600 5 75 F 410 Carcinoma of breast 78 F 420 12 76 F 320 Carcinoma of stomach 78 F 470 Long stand- 76 F 340 Carcinoma of bile duct
ing
Mean 6.5 511* 130 65 350f 97 30 324, 74
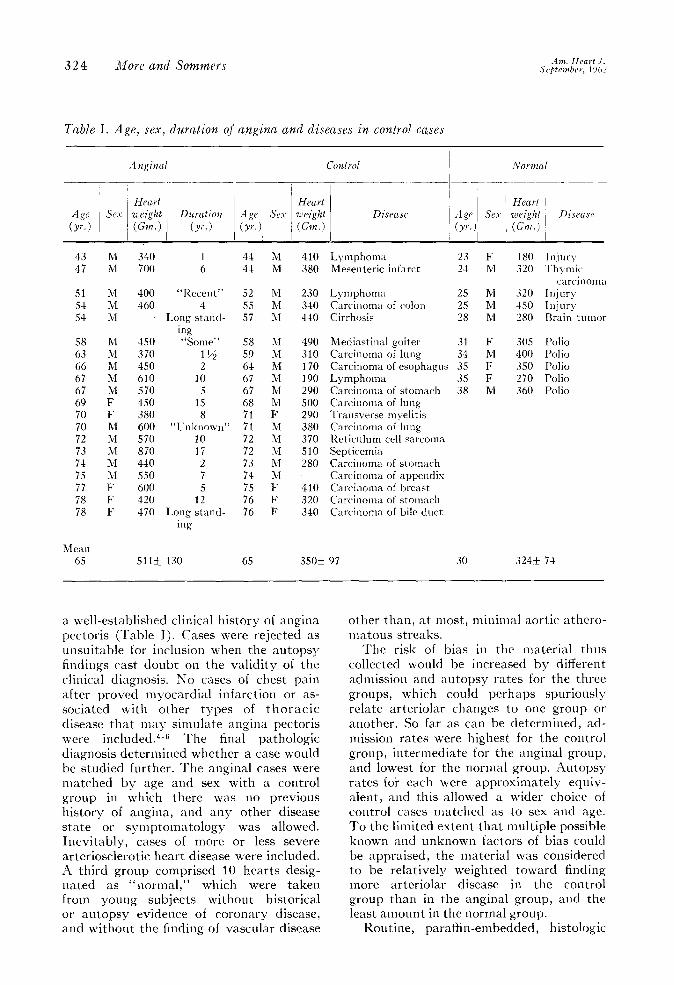
a well-established clinical history of angina pectoris (Table I). Cases were rejected as unsuitable for inclusion when the autopsy findings cast doubt on the validity of the clinical diagnosis. No cases of chest pain after proved myocardial infarction or as- sociated with other types of thoracic disease that may simulate angina pectoris were included.4-6 The final pathologic diagnosis determined whether a case would be studied further. The angina1 cases were matched by age and sex with a control group in which there was no previous history of angina, and any other disease state or symptomatology was allowed. Inevitably, cases of more or less severe arteriosclerotic heart disease were included. A third group comprised 10 hearts desig- nated as “normal,” which were taken from young subjects without historical or autopsy evidence of coronary disease, and without the finding of vascular disease
other than, at most, minimal aortic athero- matous streaks.
The risk of bias in the material thus collected would be increased by different admission and autopsy rates for the three groups, which could perhaps spuriousl> relate arteriolar changes to one group or another. So far as can be determined, ad- mission rates were highest for the control group, intermediate for the angina1 group, and lowest for the normal group. Autopq rates foi each were approximately equiv- alent, and this allowed a wider choice of control cases matched as to sex and age. To the limited extent that multiple possible known and unknown factors of bias could be appraised, the material was considered to be relatively weighted toward finding more arteriolar disease in the control group than in the angina1 group, and the least amount in the normal group.
Routine, paraffin-embedded, histologic
Status of myocardial arterioles in angina pectoris 325
sections were examined from both Zenker and formalin-fixed material. Some sections were those made by the original prosectors. lisually, additional sections were cut from preserved stock tissue. A majority of the sections were stained by the Masson trichrome method. A minority were stained with routine hematoxylin and eosin. The Masson trichrome stain facilitated the identification of the muscle components of the vessel walls. The specimens were derived from many different parts of the myocardium.
Variations in the histopathologic ma- terial ascribable to postmortem intervals, duration and type of fixation, and methods of tissue processing and staining influenced the appearance of the myocardium, but the walls of the myocardial arterioles were not appreciably affected. The sections nere regularly cut perpendicular to the epicardial surface; and in all three groups studied, grossly evident foci of atrophy, fibrosis, degeneration, or hypertrophy of the myocardial fibers were occasionally included. The technique used by the pro- sectors provided, practically exclusively, pieces of left ventricular and interventricu- lar septal myocardium not otherwise se- lected grossly or microscopically.
Measurements were made using an optical micrometer with medium magni- fication (X320). Twenty vessels were measured from each heart. They were located largely in the substance of the myocardium in interstitial planes. An at- tempt was made to include only vessels that had apparently been cut substantially
perpendicular to their course, but many vessels were not wholly circular in outline, so that some estimations of total diameters were necessary. Limitations of material, time, and money were responsible for the decision to measure only 20 arterioles per heart.
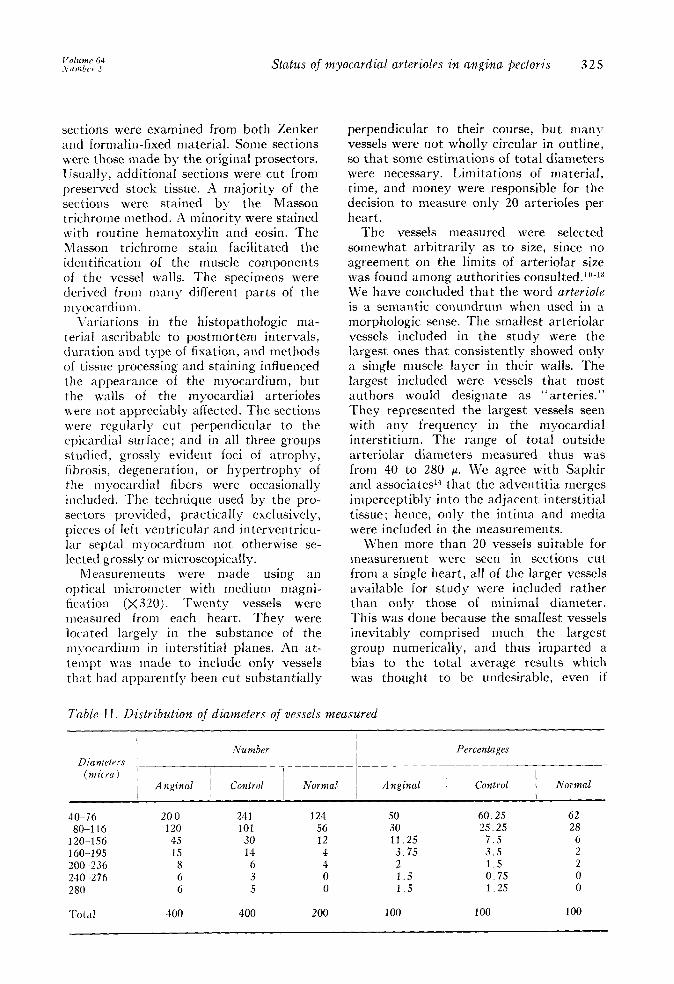
The vessels measured were selected somewhat arbitrarily as to size, since no agreement on the limits of arteriolar size was found among authorities consulted.‘n-13 We have concluded that the word arteriole is a semantic conundrum when used in a morphologic sense. The smallest arteriolar vessels included in the study were the largest ones that consistently showed only a single muscle layer in their walls. The largest included were vessels that most authors would designate as “arteries.” They represented the largest vessels seen with any frequency in the myocardial interstitium. The range of total outside arteriolar diameters measured thus was from 40 to 280 ~1. We agree with Saphir and associates14 that the adventitia merges imperceptibly into the adjacent interstitial tissue; hence, only the intima and media were included in the measurements.
When more than 20 vessels suitable for measurement were seen in sections cut from a single heart, all of the larger vessels available for study were included rather than only those of minimal diameter. This was done because the smallest vessels inevitably comprised much the largest group numerically, and thus imparted a bias to the total average results which was thought to be undesirable, even if
Table II. Distribution of diameters of vessels measured
1
Diameters ’ Number Percentages
-___ (?llicra I
I Anyinal Normal Angina1 Control Novelal
40-76 200 241 124 50 a-1 16 120 101 56 30
120-156 45 30 12 11.25 160-195 1.5 14 4 3.75 200.-236 8 6 4 2 24om-276 6 3 0 1.5 280 6 5 0 1.5
‘rot<ll 400 400 200 100
60.25 25.25
7.5 3.5 1.5 0.75 1.25
62 28
6 2 2 0 0
100 100
326 More and Sommers Am. Heart 3. septt?odJcr, i962
Table III. Distribution of thicknesses of vessel walls
Number Percentages Thickness _____
(micra) Angina1 Control Nornlal Angina1 Control I Normal
4 2 0 0 0.5 0.0 0.0 8 92 127 32 23 31.75 16
12 117 122 66 29.25 30.5 33 16 70 72 56 17.5 18.0 28 20 56 39 29 14.0 9.75 14.5 24 21 12 12 5.25 3.0 6.0 28 10 9 4 2.5 2.25 2.0 32 7 9 0 1.75 2.25 0.0 36 5 1 0 1.25 0.25 0.0 40 10 6 1 2.5 1 5 0.5 44 1 0 0 0.25 0.0 0.0 48 4 1 0 1.0 0.25 0.0 52 0 0 0 0.0 0.0 0.0 56 0 0 0 0.0 0.0 0.0 60 2 1 0 0.5 0.25 0.0 80 3 0 0 0.75 0.0 0.0
100 0 1 0 0.0 0.25 0.0
Total 400 400 200 100 100 100
Table IV. Number of muscle layers in vessel walls for each group
Layers (number) I 1 I 2 1 3 ) 4 1 5 1 6 1 7 1 8 1 14 1 None 1 Total
Number angina1 90 146 72 33 12 7 5 8 1 26 400 Number control 127 136 60 17 15 2 1 0 0 42 400 Number normal 38 94 46 18 2 0 1 0 0 1 200 Per cent angina1 22.5 36.5 18 8.25 3 1.75 1.25 2 0.25 6.5 100 Per cent control 31.75 34 15 4.25 3.75 0.5 0.25 0 0 10.5 100 Per cent normal 19 47 23 9 1 0 0.5 0 0 0.5 100
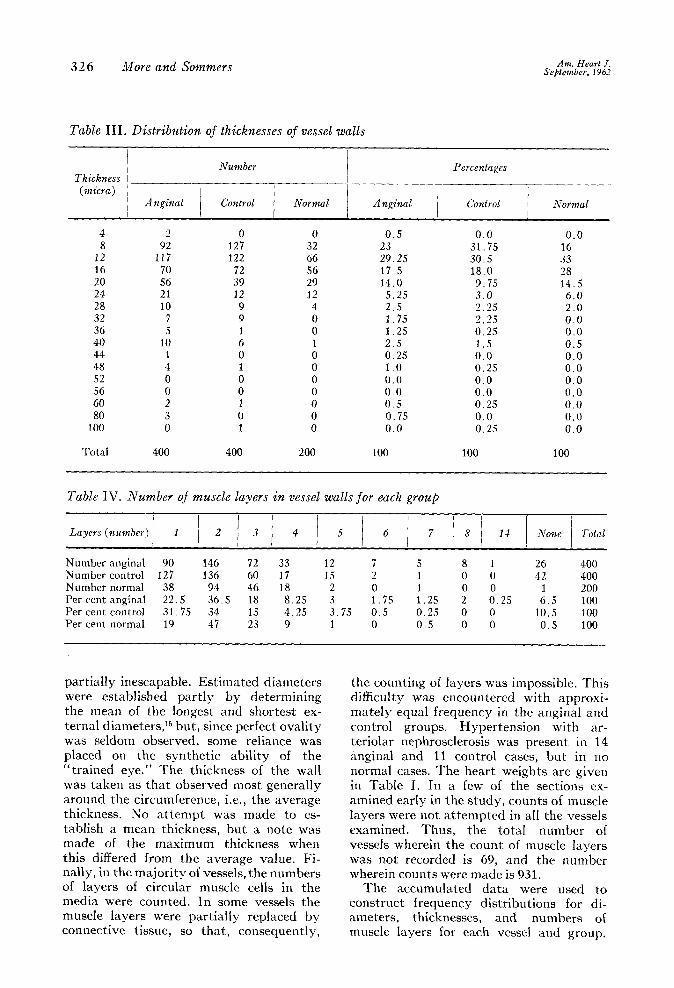
partially inescapable. Estimated diameters were established partly by determining the mean of the longest and shortest ex- ternal diameters,15 but, since perfect ovality was seldom observed, some reliance was placed on the synthetic ability of the “trained eye.” The thickness of the wall was taken as that observed most generally around the circumference, i.e., the average thickness. No attempt was made to es- tablish a mean thickness, but a note was made of the maximum thickness when this differed from the average value. Fi- nally, in the majority of vessels, the numbers of layers of circular muscle cells in the media were counted. In some vessels the muscle layers were partially replaced by connective tissue, so that, consequently,
the counting of layers was impossible. This difficulty was encountered with approxi- mately equal frequency in the angina1 and control groups. Hypertension with ar- teriolar nephrosclerosis was present in 14 angina1 and 11 control cases, but in no normal cases. The heart weights are given in Table I. In a few of the sections ex- amined early in the study, counts of muscle layers were not attempted in all the vessels examined. Thus, the total number of vessels wherein the count of muscle layers was not recorded is 69, and the number wherein counts were made is 931.
The accumulated data were used to construct frequency distributions for di- ameters, thicknesses, and numbers of muscle layers for each vessel and group.
V01wmc 64 Number 3 Status of myocardial arterioles in angina pectoris 327
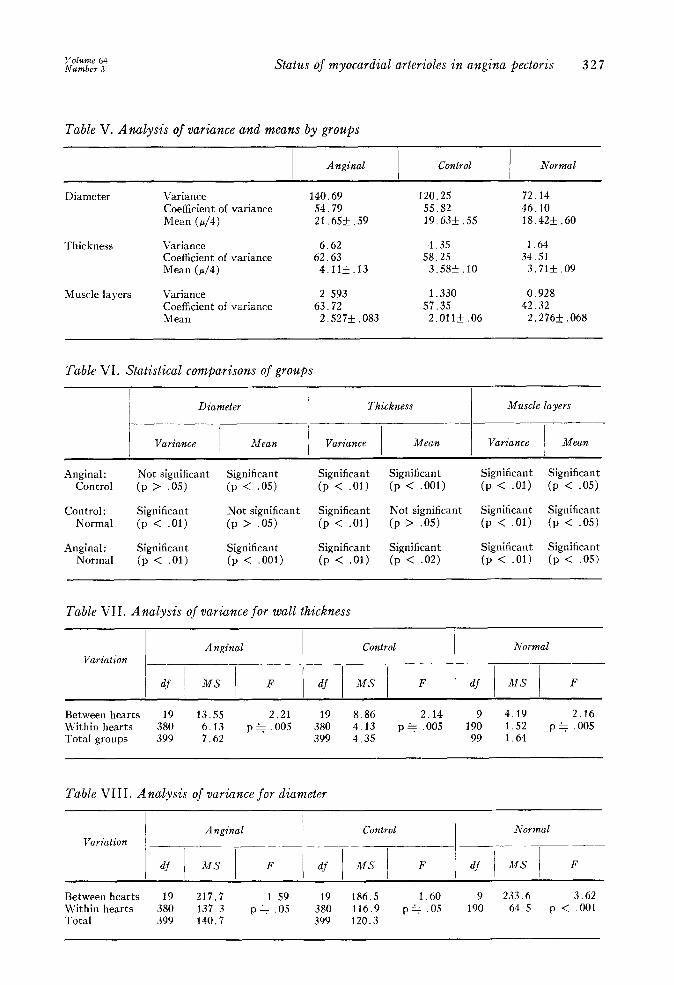
Table V. Analysis of variance and means by groups
I Angina1 Control I
Normal
Diameter Variance 140.69 120.25 72.14 Coefficient of variance 54.79 55.82 46.10 Mean (d4) 21.65&-.59 19.63+.55 18.42* .60
Thickness Variance 6.62 4.35 1.64 Coefficient of variance 62.63 58.25 34.51 Mean (d4) 4.11k.13 3.58* .lO 3.71* .09
Muscle layers Variance 2.593 1.330 0.928 Coefficient of variance 63.72 57.35 42.32 Mean 2.527+ ,083 2.011* .06 2.276* ,068
Table VI. Statistical comparisons of groups
Diameter Thickness Muscle layers -
Variance Mean Variance Mean Variance Mean
Angina1 : Not significant Significant Significant Significant Significant Significant Control (P > .05) (P < .OS) (P < .01) (p < ,001) (p < .Ol) (p < .05)
Control: Significant Not significant Significant Not significant Significant Significant Normal (P < .Ol) (P > .OS) (P < .Ol) (P > .05) (p < .Ol) (p < .05)
Angina1 : Significant Significant Significant Significant Significant Significant Normal (P < .Ol) (p < ,001) (P < .Ol) (P < .02) (p < .Ol) (p < .05)
Table VII. Analysis of variance for wall thickness
I I Angina1 Control Normal
Variation __
/ df 1 MS 1 F df / MS / F df / MS 1 F
Between hearts 19 13.55 2.21 19 8.86 2.14 9 4.19 2.16 U’ithin hearts 380 6.13 p + .005 380 4.13 p+ ,005 190 1.52 p + .005 Total groups 399 7.62 399 4.35 99 1.64
Table VIII. Analysis of variance for diameter
Variation Angina1 Control Normal
-__ -
F df MS I I
F F
Between hearts 19 217.7 1.59 19 186.5 1.60 9 233.6 3.62 Within hearts 380 137.3 p+ .o.s 380 116.9 p* .05 190 64.5 p < ,001 Total 399 140.7 399 120.3

328 More and Sommers Am. Hrart .I. .Scfitcmber, 1962
First, the vessels in each group were com- pared as individual observations (Tables II, III, and IV). Thereafter, the three groups were compared. Each analysis answered an appropriate, different ques- tion in regard to the material studied. Professional statisticians assisted with these tests.
Distribution of variates. Proportionately more larger vessels were found in the angina1 group, and fewer vessels of the smallest measured diameters (40 to 76 pj (Table II). The distribution of vessel sizes in the angina1 group differed sig- nificantly from the d’istributions in the other two groups (chi square test; p <O.Ol). The distributions of vessel sizes in the control and normal groups were not sig- nificantly different from one another (p>O.3).
The vessels of the angina1 group showed the greatest range of variation in wall thickness. There were fewer vessels with thin walls (8 p) than in the control group, since fewer vessels of small diameter were present. The normal group had relatively more vessels of medium wall thickness (16 p) than did the other two groups. The distributions were all significantly different from one another (p <O.Ol or <O.OOl) (Table III).
The angina1 group, in addition, showed a greater range of variation in the numbers of muscle layers, and included fewer thin- walled vessels with one muscle layer than did the control group. This is again due to the difference in distribution of diameters, as shown in Table II. There were relatively more vessels with intermediate numbers of muscle layers and fewer vessels with only one muscle layer in the normal group than in either of the other two groups. The distributions all differed significantl\ from one another (p c.02 or <.OOl) (Table IV).
Variance and means of the independent variates. Analysis of the measurements gives the statistics shown in Table V for the three groups. A calculation of the levels of significance between any two groups is given in Table VI.
With angina, the arteriolar vessels as a group were wider and thicker and had more
muscle layers than the vessels in the other two groups. Moreover, they varied more in thickness and in numbers of muscle layers than in the other two groups. By way of contrast, normal vessels showed the least variation in diameter, thickness, and number of muscle layers. Normal vessels tended to have more muscle layers then control vessels, but fewer muscle layers than angina1 vessels.
To investigate whether a large part of the differences found between the vari- ates in the three groups \yas due to the fact that the hearts within each group were nonhomogeneous in respect to the variates measured, the variance found was analyzed for thickness and for di- ameter (see Tables VII and VIII).
The component of variance between hearts is 0.37, 0.24, and 0.27, respectively, for the anginal, control, and normal groups. Thus, the degree to which the thickness of vessels in any one heart displayed a dis- tinct difference from that of vessels in another heart in the same group is 0.06, 0.06, and 0.15, respectively, for the anginal, control, and normal groups, as measured by intraclass correlation. Thus, there is a significant between-heart variation in the average wall thickness of the myocardial vessels, but the magnitude of the variation is small. The over-all variations in vessel thickness, which were greatest for angina1 hearts, intermediate for control hearts, and least for normal hearts, are attributable almost entirely to variation within hearts, and there is a real difference between the three groups studied.
There are significant differences in di- ameter also between hearts (see Table VIII). The differences are less in the angi- nal and control hearts, but more in the normal hearts. The components of variance between hearts are 4.0, 3.5, and 16.9, and the intraclass correlations are 0.03, 0.03, and 0.21 for the anginal, control, and normal groups, respectively. Thus, the variation between hearts is very small in the angina1 and control groups. The in- creasing variability of diameters as one moves from the normal group to the con- trol group and then to the angina1 group thus has nothing to do with the mean diameters for the samples of hearts chosen. In fact, the normal sample of hearts seems
Status of myocardial arterioles in angina prctoris 329
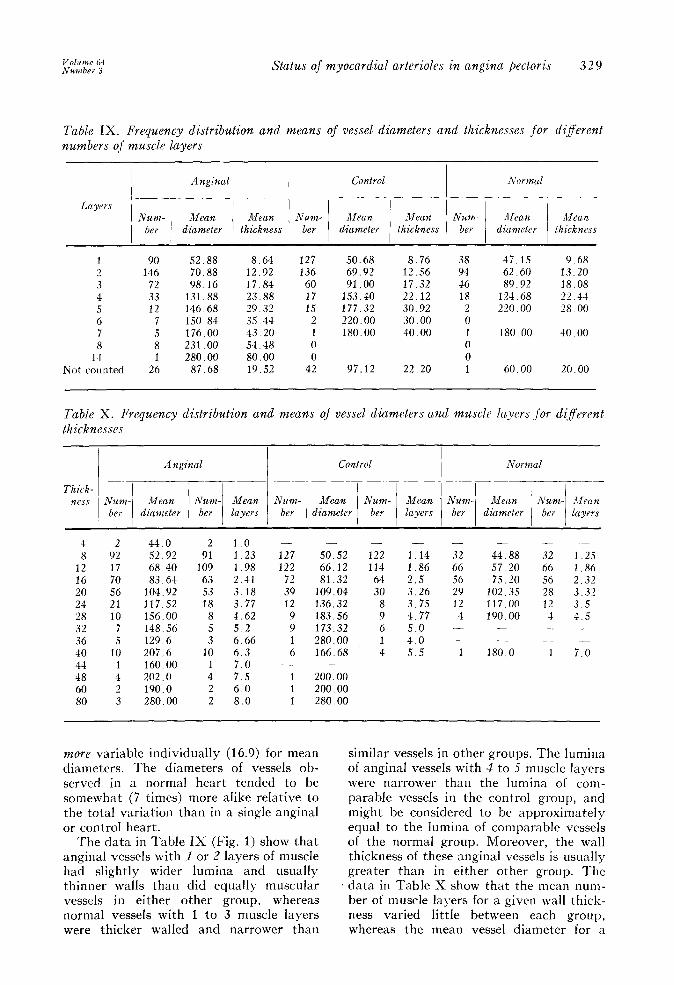
Table IX. Frequency distribution and means of vessel diameters and thicknesses for di’erent numbers of muscle layers
1 90 52.88 8.64 127 2 146 70.88 12.92 136 3 72 98.16 17.84 60 4 33 131.88 23.88 17 5 12 146.68 29.32 15 6 7 150.84 35.44 2 7 5 176.00 43.20 1 8 8 231 .oo 54.48 0
14 1 280.00 80.00 0 Not counted 26 87.68 19.52 42
50.68 8.76 69.92 12.56 91.00 17.32
153.40 22.12 177.32 30.92 220.00 30.00 180.00 40.00
97.12 22.20
38 47.15 9.68 94 62.60 13.20 46 89.92 18.08 18 124.68 22.44
2 220.00 28.00 0 1 180.00 40.00 0 0 1 60.00 20.00
Table X. Frequency distribution and means qf vessel diameters and mzrscle layers Jbr diflerent thicknesses
I I I Angina1
Thick- -__-__
Control Normal
4 2 44.0 2 1.0 - 8 92 52.92 91 1.23 127
12 17 68.40 109 1.98 122 16 70 83.64 63 2.41 72 20 56 104.92 53 3.18 39 24 21 117.52 18 3.77 12 28 10 156.00 8 4.62 9 32 7 148.56 5 5.2 9 36 5 129.6 3 6.66 1 40 10 207.6 10 6.3 44 1 160.00 1 7.0 2 48 4 202.0 4 7.5 1 60 2 190.0 2 6.0 1 80 3 280.00 2 8.0 1
- 50.52 66.12 81.32
109.04 136.32 183.56 173.32 280.00 166.68
-
200.00 200.00 280.00
- 122 1.14 32 44.88 32 1.25 114 1.86 66 57.20 66 1.86
64 2.5 56 75.20 56 2.32 30 3.26 29 102.35 28 3.32
8 3.75 12 117.00 12 3 5 9 4.77 4 190.00 1 4.5 6 5.0 - - -_ - 1 4.0 - - 4 5.5 1 180.0 1 7.0
more variable individually (16.9) for mean diameters. The diameters of vessels ob- served in a normal heart tended to be somewhat (7 times) more alike relative to the total variation than in a single angina1 or control heart.
The data in Table IX (Fig. 1) show that angina1 vessels with 1 or 2 layers of muscle had slightly wider lumina and usually thinner walls than did equally muscular 9 vessels in either other group, whereas normal vessels with 1 to 3 muscle layers were thicker walled and narrower than
similar vessels in other groups. The lumina of angina1 vessels with 3 to 5 muscle layers were narrower than the lumina of com- parable vessels in the control group, and might be considered to be approximately equal to the lumina of comparable vessels of the normal group. Moreover, the wall thickness of these angina1 vessels is usually greater than in either other group. The data in Table X show that the mean num- ber of muscle layers for a given wall thick- ness varied little between each group, whereas the mean vessel diameter for a
330 More and Sommers Am. Heart J. September, 1962
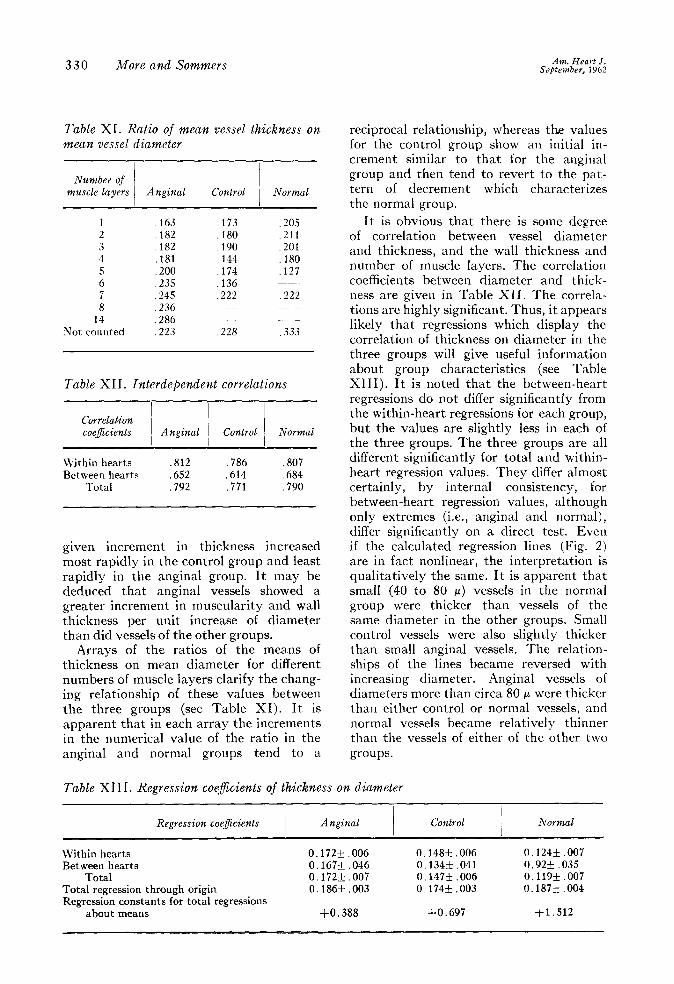
Table XI. Ratio of mean vessel thickness on mean vessel diameter
Number of muscle layers Angina1 Control Normal
1 ,163 ,173 ,205 2 182 180 ,211 3 :182 :190 ,201 4 181 ,144 .180 5 : 200 174 127 6 ,235 :136 i- 7 ,245 ,222 ,222 8 ,236 __
14 ,286 Not counted ,223 ,228 333
Table XII. Interdependent correlations
Correlation coeficients ) Angina1 1 Control 1 Normal
Within hearts ,812 786 807 Between hearts ,652 ,614 ,684
Total ,792 ,771 .790
given increment in thickness increased most rapidly in the control group and least rapidly in the angina1 group. It may be deduced that angina1 vessels showed a greater increment in muscularity and wall thickness per unit increase of diameter than did vessels of the other groups.
Arrays of the ratios of the means of thickness on mean diameter for different numbers of muscle layers clarify the chang- ing relationship of these values between the three groups (see Table XI). It is apparent that in each array the increments in the numerical value of the ratio in the angina1 and normal groups tend to a
reciprocal relationship, whereas tke values for the control group show an initial in- crement similar to that for the angina1 group and then tend to revert to the pat- tern of decrement which characterizes the normal group.
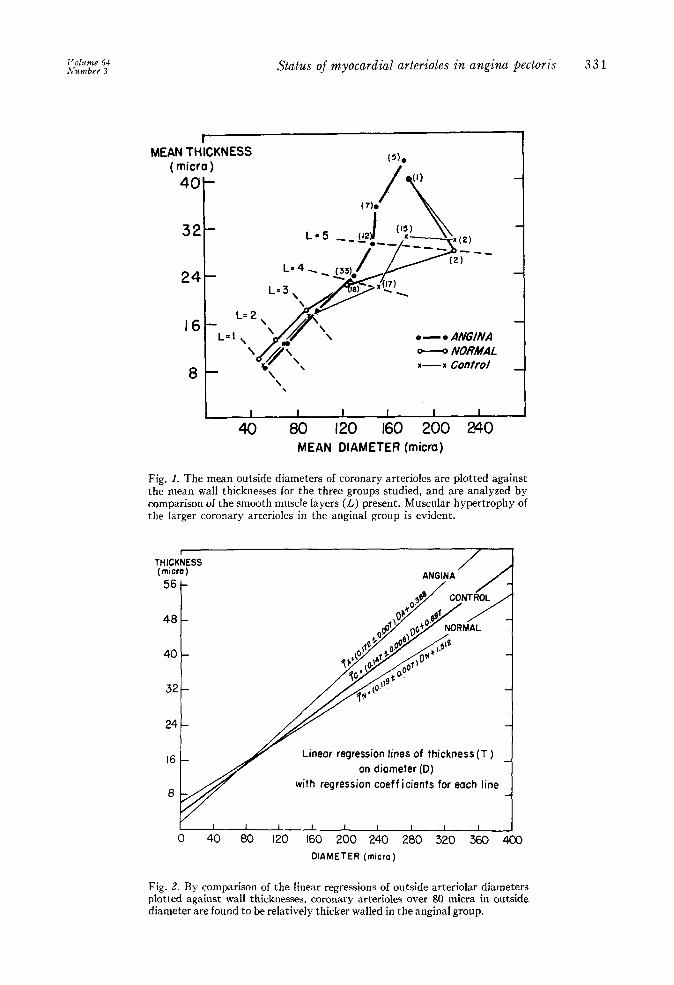
It is obvious that there is some degree of correlation between vessel diameter and thickness, and the wall thickness and number of muscle layers. The correlation coefficients between diameter and thick- ness are given in Table XII. The correla- tions are highly significant. Thus, it appears likely that regressions which display the correlation of thickness on diameter in the three groups will give useful information about group characteristics (see Table XIII). It is noted that the between-heart regressions do not differ significantly from the within-heart regressions for each group, but the values are slightly less in each of the three groups. The three groups are all different significantly for total and within- heart regression values. They differ almost certainly, by internal consistency, for between-heart regression values, although only extremes (i.e., angina1 and normal), differ significantly on a direct test. Even if the calculated regression lines (Fig. 2) are in fact nonlinear, the interpretation is qualitatively the same. It is apparent that small (40 to 80 p) vessels in the normal group were thicker than vessels of the same diameter in the other groups. Small control vessels were also slightly thicker than small angina1 vessels. The relation- ships of the lines became reversed with increasing diameter. Angina1 vessels of diameters more than circa 80 p were thicker than either control or normal vessels, and normal vessels became relatively thinner than the vessels of either of the other two groups.
Table XI I I. Regression coejicients of thickness on diameter
Regression coeficients Angina1 I
Control Normal
Within hearts 0.172+ ,006 0.148+ ,006 O.l241f:.OO7 Between hearts 0.167+.046 0.134* .041 0.92+ ,035
Total 0.172+ ,007 0.147+ ,006 0.119+ ,007 Total regression through origin 0.186f ,003 0.174+ ,003 0.187+ ,004 Regression constants for total regressions
about means +0.388 +0.697 +1.512
- - .-
1 'olrme 61 Number 3
Status of myocardial arterioles in angina pectoris 331
I MEAN THICKNESS
( micra ) (3).
40 / (1) (7).
24
t
L=4,_
16 L=2 \
t
. - . ANGINA - NORMAL
I I I I I 1 I I 40 80 120 160 200 240
MEAN DIAMETER (micra)
Fig. 1. The mean outside diameters of coronary arterioles are plotted against the mean wall thicknesses for the three groups studied, and are analyzed by comparison of the smooth muscle layers (L) present. Muscular hypertrophy of the larger coronary arterioles in the angina1 group is evident.
(micro) (micro)
56 56 -
48 48 -
40 40 -
32t- 32-
24
t
16 t
8 v Linear regression lines of thickness (T ) Linear regression lines of thickness (T )
on diameter(D) on diameter(D) with regression coefficients for each line with regression coefficients for each line
r I I I I I I I I I 0 40 80 120 160 200 240 280 320 360
DIAMETER (micra)
Fig. 2. By comparison of the linear regressions of outside arteriolar diameters plotted against wall thicknesses, coronary arterioles over 80 micra in outside diameter are found to be relatively thicker walled in the angina1 group.
332 More and Sommers Am. Heart J. Scptcmber, 1961
Discussion
The arteriolar vessels studied from patients with angina pectoris had dis- tinctive characteristics. There were rela- tively greater numbers of large vessels present than in the normal or control groups. Moreover, there was compara- tively more variation in the size of such vessels in the myocardium of the angina1 group. The smaller arteriolar vessels had relatively thinner walls than analogous vessels in the other groups, but with incre- ments in diameter the vessels in the angina1 group showed a greater increase in wall thickness than did vessels in the other groups. The arterioles of intermediate sizes from angina1 hearts were as thick and muscular as vessels from normal hearts, and more muscular and thicker than vessels of equal size from control hearts. Still larger vessels of the angina1 group were generally thicker and more muscular than vessels of equal size from the control or normal groups, but the number of such vessels measured was small.
We may suppose that in angina some of the smaller vessels (40 to 80 p) in the myo- cardium had been entirely obliterated by replacement fibrosis of the myocardium, and others may have dilated out of the range of small vessel diameters. The small (40 to 80 cl) arterioles which remained in the angina1 heart muscle were themselves generally somewhat dilated and, thus, had relatively thinner walls than similar vessels in other groups. Thus, the shift in the distribution may have been due to a com- bination of arteriolar obliteration and dilatation.
The distributions of vessel diameters were statistically skewed, being left asym- metrical. However, the distribution of means was considered to be within normal limits, and the levels of significance were, consequently, reasonably applicable. The significance of difference in variance should be treated with a little more caution in view of this asymmetry, although the “F” test used is robust for deviations from normality.
The figures for numbers of muscle layers are not considered to be very precise. Muscle cells are by no means disposed in perfectly concentric layers, but intermingle
to some extent. However, the same sources of error were present in both control and angina1 vessels. Thus, the difference ii) muscularity of arteriolar vessels in these groups is considered to be real, at least in a relative sense. Normal vessels had a rather more orderly media, so that the estimation of muscle cell layers was rather easier to make. When significant numbers of vessels, e.g., over 10, were present ii1 the plotted regressions of each group, normal vessels were found to be as muscu- lar as, or more muscular than, angina1 vessels. This suggests that the essential difference between the angina1 vessels and
control vessels is that angina1 vessels re- mained more reactive or more capable of muscle contraction than did control ves- sels. Consequently, a reason for the de- velopment of angina pectoris is that the arteriolar vascular bed retains constrictive reactivity in the face of a seriously di- minished arterial blood supply. It may not be true that when the arterjolar bed di- lates it is incapable of delivering the same amount of blood as in other arteriosclerotic hearts.
The three populations of arterioles ovcr- lap in some respects, but the three groups show differences in the degrees of associ- ation and the rates of change of association of the variates. Our findings tend to sup- port the accepted hypothesis that angina pectoris is due to vascular spasm and, hence, may be relieved by vasodilators that act directly on coronary vessels,“j*” thus increasing blood flow,” possibly part13 via collateral channels.‘*
This study represents a limited applica- tion of experimental histopathology to myocardial arterioles, which has involved measuring these vessels for, apparently, the first time. The usual evolution of medical knowledge that comprises the stages of observation, measurement, and mathematical analysis has been followed, but no claim of absolute accuraclr, great precision, certainty of proof, or universal application of the results is intended. The complex statistical analyses employed have not been made to prove that differences exist or that the simple measurements recorded are conclusive evidence of ar- teriolar alterations. The tests have evalu- ated the probabilit>- that the observed

Status of myocardial arterioles in angina pectoris 333
differences are due to chance, and the results are given to provide the reader with conclusions based on something be- yond mere experience and opinion.
The risk of bias from a conscious or un- conscious selection of material has not been ignored. Consideration of what un- related selective influences might operate to influence the size, number, muscular thickness, and diameter of myocardial arterioles in one group more than another is inconclusive, because more factors are unknown than known, and the direction and extent of these influences cannot be adequately analyzed. From a knowledge of hospital admissions, autopsy rates, and procedures, we are of the opinion that the group sizes and relative case fatalities, choice and selection of material for study, and the plan of study of the anginal, control, and normal series were not free from bias. Despite the various uncertain- ties, a search for influences which would introduce an element of bias that would invalidate the findings has not discredited the plausible relationship observed between myocardial arteriolar alterations and an- gina pectoris.
Summary
The wall thicknesses, the numbers of muscle layers in the media, and the di- ameters of 20 arterial vessels of arteriolar size (40 to 280 p) were measured or counted in microscopic sections of myocardium from each of 20 hearts taken from autopsied patients who had angina pectoris. The same measurements were made in 20 hearts from control subjects who were matched with the angina1 group by age and sex, but who were without angina, and in each of 10 hearts from young subjects who had no significant vascular disease. The meas- urements and counts in the three groups were analyzed statistically to provide com- parative data. The principal findings were: (1) There were fewer small and more large arterioles in the angina1 group than in the other two groups. (2) Vessels from angina1 hearts varied more in wall thick- ness and in numbers of muscle layvers. (3) The regression lines of vessel thickness on vessel diameter were significantly dif- ferent for each of the three groups. (4) Ves-
sels from angina1 hearts showed greater thickening of their walls with increase in diameter than that which occurred in either of the other groups. (5) Vessels of intermediate size from the angina1 hearts were more muscular than com- parable vessels from control hearts.
REFERENCES
1.
2.
1 s .
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
Albertini, H. F. (1618). Quoted by Levy.lG Heberden, W.: Commentaries on the history and cure of disease, p. 292. Quoted by Major, Ii. H.: Classic descriptions of disease, Spring- field, Ill., 1939, Charles C Thomas, Publisher, p. 4.55. Parry, C. H. (1799) : Xn inquiry into the symp- toms and causes of the syncope anginosa, com- monly called angina pectoris; illustrated by dissections. Quoted by Levy.lG Reefer, C. S., and Resnick, U’.: i-lnyina pectoris. A syndrome caused by anoxemia-of the myo- cardium. Arch. Int. Med. 41:769. 1928. Plotz, Ak.: Coronary heart disease, New York, 1957, Paul B. Hoeber Company. Osler, IV:.: The Lumleian Lectures on angina pectoris, Lancet 1:839, 1910. Len$gre, J., and Himbert, J.: Critical study of the relationship between angina pectoris and coronary atherosclerosis, AM. HEAKT J. S8:.539, 1959. Blumgart, II. L., Schlesinger, M. J., and Davis, D.: Studies on the relation of the clinical mani- festations of angina pectoris, coronary throm- bosis, and myocardinl infarction to the patho- logic findings, AM. HEART J. 19:1, 1940. Zoll. I’. M., Wessler, S., and Blumgart, H. L.: Angina pectoris, clinical and pathologic correla- tions, Am. J. Med. 11:331, 19.51. Gross, L., Rugel, M. .4., and Epstein, E. Z.: Lesions of coronary arteries and their branches in rheumatic fever, Am. J. Path. 11:253, 1935. Cowdry, E. 17.: Testbook of histology, ed. 4, PhiladelDhia. 1956. Lea & Febker. D. 141. Ham, A’. I+.: Histology, ed. ‘3, ‘Philadelphia, 1957, J. B. Lippincott Company, p. 246. Maximow, .4. ,4., and Bloom, W.: A textbook of histology, ed. 7, Philadelphia, 1957, W. B. Saunders Company, p. 234. Saphir, O., Ohringer, L., and Wong, R. : Changes in the intramural coronary branches in coronary arteriosclerosis, .4.M.A. Arch. Path. 62:159, 1956. Heath, n., and Best, P. V.: The tunica media of the arteries of the lung in pulmonary hyper- tension, J. Path. & Bact. 76:165, 1958. Levy, R. L.: Diseases of the coronary arteries and cardiac pain, New York, 1936, The Mac- millan Company. Mandelbaum, H., and Mandelbaum, Ii. A.: Ballistocardiographic response to nitroglycerin in coronary artery disease, ;\M. HF:.aR.r J. 44:257, 1952. Laurie, W., and 1Voods, J. D.: Anastomosis in the coronary circulation, Lancet 2:812, 19.58.
Related Documents