www.ejbps.com 89 THE STATUS OF SERUM LIPID PROFILE IN STRESS-RELATED PRE-INSOMNIA Uba A.I 1,2 *, Abdullahi I.L 2 , Abdullahi, S.A 2 and Adamu H 2 1 Department of Biochemistry, Bayero University, Kano, P.M.B 3011, Kano-Nigeria 2 Centre for Biotechnology Research, Bayero University, Kano P.M.B 3011, Kano-Nigeria Article Received on 03/12/2014 Article Revised on 24/12/2014 Article Accepted on 15/01/2015 ABSTRACT Understanding of the correlation between stress, pre-insomnia and serum lipid profile status may provide clues toward the management of stress- related cardiovascular diseases. This study assessed the serum lipid profile on a total of thirty seven (37) male and female subjects; twenty eight (28) of which are students selected from different departments and nine (9), within Kano city. Twenty five (25) served as experimental subjects and twelve (12) as control subjects. Their blood pressure was taken and information on general life style, sleeping as well as reading habits was recorded by means of well-structured questionnaire prior to sample collection. Venous blood (5ml) was collected from each subject, centrifuged and the sera stored. Serum lipid profile was assayed using commercial kit from fortress diagnostics limited. When the Mean serum Total Cholesterol, High Density Lipoprotein Cholesterol, Low Density Lipoprotein Cholesterol and Triglyceride levels of test subjects were compared with those of the control subjects the difference was not significant (p˃0.05). When comparison was made within the study group, based on borderline risk of high and normal blood pressure, the serum lipid profile level was found to differ significantly (p˂0.05). Thus our st udy showed that acute sleep deprivation (pre- insomnia) does not alter serum lipid profile, however, is associated with mild hypertension which is a risk factor for cardiovascular diseases. KEYWORDS: Pre-insomnia, Stress, Lipid profile. European Journal of Biomedical AND Pharmaceutical sciences http://www.ejbps.com ISSN 2349-8870 Volume: 2 Issue: 1 89-98 Year: 2015 Research Article ejbps, 2015, Volume 2, Issue 1, 89-98. *Correspondence for Author Uba A.I PhD (In view) Department of Biochemistry, Bayero University, Kano, P.M.B 3011, Kano-Nigeria.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
www.ejbps.com
89
Uba A.I et al. European Journal of Biomedical and Pharmaceutical Sciences
THE STATUS OF SERUM LIPID PROFILE IN STRESS-RELATED
PRE-INSOMNIA
Uba A.I1,2
*, Abdullahi I.L2, Abdullahi, S.A
2 and Adamu H
2
1Department of Biochemistry, Bayero University, Kano, P.M.B 3011, Kano-Nigeria
2Centre for Biotechnology Research, Bayero University, Kano P.M.B 3011, Kano-Nigeria
Article Received on 03/12/2014 Article Revised on 24/12/2014 Article Accepted on 15/01/2015
ABSTRACT
Understanding of the correlation between stress, pre-insomnia and
serum lipid profile status may provide clues toward the management of
stress- related cardiovascular diseases. This study assessed the serum
lipid profile on a total of thirty seven (37) male and female subjects;
twenty eight (28) of which are students selected from different
departments and nine (9), within Kano city. Twenty five (25) served as experimental
subjects and twelve (12) as control subjects. Their blood pressure was taken and
information on general life style, sleeping as well as reading habits was recorded by means of
well-structured questionnaire prior to sample collection. Venous blood (5ml) was collected
from each subject, centrifuged and the sera stored. Serum lipid profile was assayed using
commercial kit from fortress diagnostics limited. When the Mean serum Total Cholesterol,
High Density Lipoprotein Cholesterol, Low Density Lipoprotein Cholesterol and Triglyceride
levels of test subjects were compared with those of the control subjects the difference was not
significant (p˃0.05). When comparison was made within the study group, based on
borderline risk of high and normal blood pressure, the serum lipid profile level was found to
differ significantly (p˂0.05). Thus our study showed that acute sleep deprivation (pre-
insomnia) does not alter serum lipid profile, however, is associated with mild hypertension
which is a risk factor for cardiovascular diseases.
KEYWORDS: Pre-insomnia, Stress, Lipid profile.
European Journal of Biomedical AND
Pharmaceutical sciences http://www.ejbps.com
ISSN 2349-8870
Volume: 2
Issue: 1
89-98
Year: 2015
Research Article ejbps, 2015, Volume 2, Issue 1, 89-98.
*Correspondence for
Author
Uba A.I PhD (In view)
Department of Biochemistry,
Bayero University, Kano,
P.M.B 3011, Kano-Nigeria.
www.ejbps.com
90
Uba A.I et al. European Journal of Biomedical and Pharmaceutical Sciences
1.1 INTRODUCTION
Insomnia is a subjective feeling of having difficulty initiating, maintaining or restoring sleep,
or having poor sleep quality (Roth, 2007). It was reported to be associated with substantial
impairments of an individual’s quality of life (Leger et al., 2012), depression (Sarsour, et al.,
2010) and accident occurrence (Chiang, et al., 2012). Insomnia is the most common sleep
disorder, affecting one in four people (Kessler 2011; Shatzmiller 2012; American Academy
of sleep medicine 2001). Many people may not realize that insomnia and short sleep duration
correlate with various health problems including cardiovascular disease, anxiety, and
potentially cancer (Terauchi 2012; Chayon 1998; Kakizaki 2008; Verkasalo 2005; Philips
2007). Insomnia also increases mortality in adults (Chien, 2010 and Hublin 2011). Although
the cause and physiology of insomnia have not been completely understood, it is generally
considered as one kind of hyperarousal disorder related to increased activity of hypothalamic
pituitary adrenal-axis (Roth, 2007). During this process cortisol (Vgontzas et al.,2001) will be
secreted excessively. Elevated cortisol is able to induce higher cholesterol (Fraser et al.,
1999).
Pre-insomnia (onset of insomnia) may be a consequence of another underlying medical
problem e.g. mental health issue, physical health issue, hormonal imbalance, medication, and
stimulant. Recently, it was demonstrated that paradoxical sleep deprivation for four days has
significant effect on lipid metabolism such as increasing Low Density Lipoproteins
(Anderson et al.,2004). In addition, cholesterol concentration was significantly decreased in
rats exposed to cold environmental temperatures, indicating increase corticosterone synthesis
and activation of HPA system (Cvijic, Davidovic and Jordjevic, 2003). Recent study
suggested that short sleep duration was associated with higher risks of hypercholesterolaemia
in the adults of U.S (Gangswisch et al.,2010) and japan (Kaneita et al, 2008) likewise reduce
sleep duration was found to be related to dyslipidemia in other studies (Chen, and Zhang,
2014).
During the past two decades, considerable evidence has accumulated showing an association
between cardiovascular disease (especially adverse coronary artery disease) and markers of
stress and other psychological factors, such as anxiety, depression and somatization (Artham
et al., 2008; Hemingway and Marmot, 1999; Rozansk et al.,2005). Recent studies have
shown that disturbed sleep and sleep deprivation are associated with subsequent occurrence
of cardiovascular alterations (Stickgold and Walker, 2007; Cintra et al.,2005; Perry et
www.ejbps.com
91
Uba A.I et al. European Journal of Biomedical and Pharmaceutical Sciences
al.,2007), behavoural changes (Anderson et al., 2005; Spiegel, Sheridan, and Van Cauter,
2002; Andersen et al., 2006) as a result of weight loss; however, unlike the decrease in LDL,
the reduction of triglyceride concentration is not related to this weight reduction (Perry et
al.,2007). Another ones have shown that habitual sleep duration <5hr per night is associated
with an increased prevalence of arterial hypertension (Gangwischet al., 2006; Gottlieb et
al.,2006; Cappuccio et al.,2007). Some articles have proposed that activation of the
sympathetic nervous system by sleep deprivation may be involved in triggering
cardiovascular events in the morning hours (Tochikubo et al., 1996 and Lusardi et al., 1999).
A review reported by Dimsdale and Herd showed that the level of free fatty acids and total
cholesterol increases in acute and chronic stress (Dimsdale, 1982), which may be attributed to
insomnic condition. Similarly a study conducted by Fakhari and colleagues in 2004
demonstrated increased triglyceride in individuals who had experienced high levels of stress
in the preceding 6-12 months (Fakhari et al.,2007). This may be attributed to the finding that
cortisol causes the mobilization of fats (lipids) deposited in the adipose and other tissues,
leading to an increased levels of lipids in the blood (Bower and Sergerstrom, 2001). More
recently, our previous work on stress has shown that the higher the examination stress the
higher the serum Cholesterol, Low Density Lipoprotein Cholesterol and Triglycerides levels
and lower the serum High Density Lipoprotein levels, suggesting an increased risk of
hyperlipidaemia in stress condition (Uba et al.,2014). The response to examination stress may
be related to the enhanced utilisation of cholesterol in the andrenal cortex for steriodogenesis
(Bijlani et al., 1986). Increase catecholamine levels result in up regulation of lipoprotein
lipase, leading to increased concentrations of free fatty acids(FFA) in the serum that are
transformed by the liver into cholesterol and triglycerides. Cortisol,on the other hand,
increases the deposition of abdorminal fat, which is more sensitive to lipolitic agents and
related to insulin resistance (Resmond, 2005), elevated lipid profiles in turn may mediate
longer term deleterious effects on physical health including heart disease and stroke.
The studies cited above have not been able establish proper correlation between stress, pre-
insomnia, lipid profile and cardiovascular disease. This study is aimed at determining serum
lipid profile status in pre-insomnic individuals in stress condition. The specific objectives are
(1) To find if pre-insomnic condition is enough to cause lipid profile alteration (2) To observe
whether an acute insomnia (pre-insomnia) is the risk factor for or the consequence of lipid
profile alteration..
www.ejbps.com
92
Uba A.I et al. European Journal of Biomedical and Pharmaceutical Sciences
2.1 MATERIAL AND METHOD
2.1.1 Study Site, Subjects and Sample Collection
The study was carried out at Bayero University, Kano, Department of Biochemistry. A total
of thirty seven (37) male and female subjects; twenty eight (28) of which are students
selected from different departments and nine (9), within Kano city. Twenty five (25) served
as experimental subjects and 12 as control subjects.Their blood pressure was taken and
information on their general life style, including dietary habit was recorded by of means of
structured questionnaire prior to sample collection. Venous blood (5ml) was collected from
each subject, centrifuged and the sera stored.
The study was approved by the ethical committee of the institution and the informed consent
was obtained from the study subjects.
2.1.2 Methodology
2.1.2.1Estimation of Serum Lipid Profile
Serum total cholesterol was assayed by Tindar’s reaction (Evans and Stein, 1986; NIH,
1990), Serum Triglyceride level was determined as described by Fossati and Precipe (1982),
HDL-C, using commercial kit from fortress diagnostics limited and the serum LDC-L level
was calculated by Friedwald’s formular (Friedwald et al., 1972).
2.1.3 Statistical analysis
The result were expressed as means ± standard deviation. One – way analysis of variance
ANOVA was used to analyse Lipid Profile data followed by Student T-Test to calculate
statistical significance difference between the various groups.
The study was approved by the ethical committee of the institution and the informed consent
of the study subjects was obtained prior to experimentation.
www.ejbps.com
93
Uba A.I et al. European Journal of Biomedical and Pharmaceutical Sciences
3.0 RESULT AND DISCUSSION
3.1 RESULT
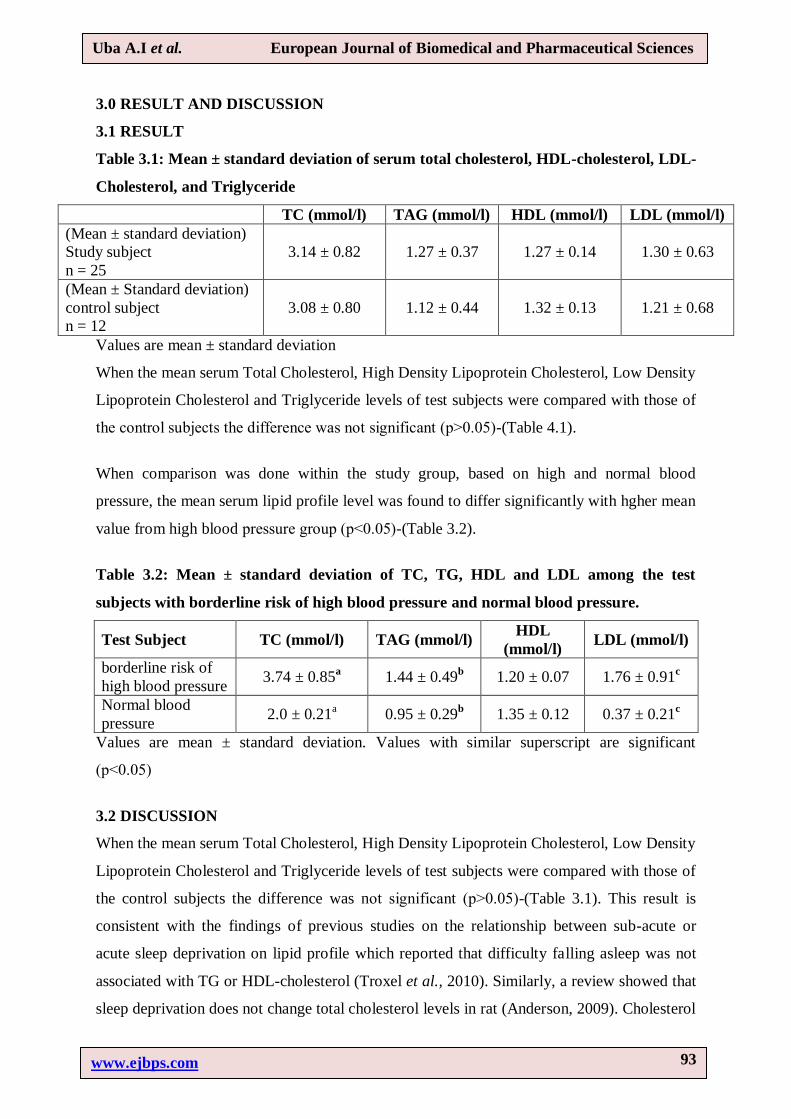
Table 3.1: Mean ± standard deviation of serum total cholesterol, HDL-cholesterol, LDL-
Cholesterol, and Triglyceride
TC (mmol/l) TAG (mmol/l) HDL (mmol/l) LDL (mmol/l)
(Mean ± standard deviation)
Study subject
n = 25
3.14 ± 0.82 1.27 ± 0.37 1.27 ± 0.14 1.30 ± 0.63
(Mean ± Standard deviation)
control subject
n = 12
3.08 ± 0.80 1.12 ± 0.44 1.32 ± 0.13 1.21 ± 0.68
Values are mean ± standard deviation
When the mean serum Total Cholesterol, High Density Lipoprotein Cholesterol, Low Density
Lipoprotein Cholesterol and Triglyceride levels of test subjects were compared with those of
the control subjects the difference was not significant (p˃0.05)-(Table 4.1).
When comparison was done within the study group, based on high and normal blood
pressure, the mean serum lipid profile level was found to differ significantly with hgher mean
value from high blood pressure group (p˂0.05)-(Table 3.2).
Table 3.2: Mean ± standard deviation of TC, TG, HDL and LDL among the test
subjects with borderline risk of high blood pressure and normal blood pressure.
Test Subject TC (mmol/l) TAG (mmol/l) HDL
(mmol/l) LDL (mmol/l)
borderline risk of
high blood pressure 3.74 ± 0.85
a 1.44 ± 0.49
b 1.20 ± 0.07 1.76 ± 0.91
c
Normal blood
pressure 2.0 ± 0.21
a 0.95 ± 0.29
b 1.35 ± 0.12 0.37 ± 0.21
c
Values are mean ± standard deviation. Values with similar superscript are significant
(p˂0.05)
3.2 DISCUSSION
When the mean serum Total Cholesterol, High Density Lipoprotein Cholesterol, Low Density
Lipoprotein Cholesterol and Triglyceride levels of test subjects were compared with those of
the control subjects the difference was not significant (p˃0.05)-(Table 3.1). This result is
consistent with the findings of previous studies on the relationship between sub-acute or
acute sleep deprivation on lipid profile which reported that difficulty falling asleep was not
associated with TG or HDL-cholesterol (Troxel et al., 2010). Similarly, a review showed that
sleep deprivation does not change total cholesterol levels in rat (Anderson, 2009). Cholesterol
www.ejbps.com
94
Uba A.I et al. European Journal of Biomedical and Pharmaceutical Sciences
level and Low Density Lipoprotein Cholesterol had no significant change in sub-chronic
sleep deprivation (Perry et al., 2007). Research showed that there is no significant changing
in cholesterol level in sleep deprived male rats (Antunes, 2007). A study on the effect of sleep
deprivation on 18 – 65 years old men and women, proved that short sleep deprivation had no
effect on total cholesterol levels (Adamkova, 2009). Thus acute sleep deprivation may be due
to acute effect of cardiovascular physiology arising from changes in the autonomic nervous
system, rather than Lipid profile (Artham et al., 2008).
However, our study is inconsistent with a report by Dimsdale and Herd that, the level of free
fatty acids and total cholesterol increases in chronic stress (Dimsdale and Herd, 1982), which
may be attributed to insomnia. Similarly a study conducted by Fakhari and colleagues in
2004 demonstrated increased triglyceride in individuals who had experienced high levels of
stress in the preceding 6-12 months (Fakhari et al.,2007). A very recent study has shown that
the higher the examination stress the higher the serum Cholesterol, Low Density Lipoprotein
Cholesterol and Triglycerides levels and lower the serum High Density Lipoprotein levels,
suggesting an increased risk of hyperlipidaemia in stress condition (Uba et al.,2014).
However, these reports evaluated effects of chronic sleep deprivation rather than acute or
sub-acute sleep deprivation (Pre-insomnia) being reported by our study.
Upon comparison within experimental subjects with borderline risk high blood pressure and
normal blood pressure groups, a significant increase (p˂0.05)-(Table 3.2) in total cholesterol,
triglyceride, low density lipoprotein cholesterol and a decrease (p˂0.05)-(Table 3.2) in high
density lipoprotein cholesterol levels in individuals with borderline risk of high blood
pressure was observed compared with normal blood pressure individuals, suggesting that
acute insomnia is associated with prevalence of arterial hypertension. The individuals with
border line risk of high blood pressure were thought to be more stressed compared to those
with normal blood pressure, indicating an increase in electroencephalogram beta wave
activity of the brain, making it harder for the brain to achieve the state of relaxation needed
for sleep ( the brain still remain alert ). The body circadian rhythm and time may be
disconnected, resulting in disruption of normal sleeping pattern.
Cortisol is a stress hormone secreted at higher level during stress for appropriate stress
response. Although the secretion may not be so significant to cause a vast alteration in pre-
insomnic individuals, these subjects tend to have an increased blood sugar level thought to
be produced by gluconeogenesis through the activation of pyruvate carboxylase, an enzyme
www.ejbps.com
95
Uba A.I et al. European Journal of Biomedical and Pharmaceutical Sciences
that generate oxaloacetate, an important precursor of glucose in the pathway. The glucose
produced provides energy to the brain. This high glucose metabolism leads to the inability of
the brain to get full relaxation even during sleep. (Uba et al.,2014). The pre-insomnic
condition can thus be attributed to stress as far as our study subjects are concerned.
3.3 CONCLUSION
Our study shows that acute sleep deprivation (pre-insumnia) does not alter serum TC, TG,
HDL and LDL cholesterol significantly, however, in stress condition borderline of high blood
pressure subjects showed low risk of developing cardiovascular diseases.
4.4 RECOMMENDATION
We recommend further research to investigate cardiac enzymes, blood glucose, cerebrospinal
fluid levels of individuals with chronic insomnia.
4.5 ACKNOWLEDGEMENT
We acknowledge the technical assistance of the laboratory technicians, Department of
Biochemistry, Bayero University, Kano and S.S Usman for critical reading of the manuscript
and making suggestions.
REFERENCE
1. Roth T and Roehrs T. (2003). Insomnia: epidemiology, characteristics, and consequences.
Clin Cornerstone, 2003; 5(3):5-15.
2. Leger D, Morin C.M, Uchiyama M, Hakimi Z, Cure S, Walsh J.K. (2012).
Chronicinsomnia, quality-of-life, and utility scores: comparison with goodsleepers in a
cross-sectional international survey. Sleep Med, 2012; 13(1):43 51.
3. Sarsour K, Morin CM, Foley K, Kalsekar A, Walsh J.K. (2010). Association of insomnia
severity and comorbid medical and psychiatric disorders in a health plan-based sample:
Insomnia severity and comorbidities. Sleep Med, 2010; 11(1):69–74.
4. Kessler R.C, Berglund P.A et al. (2011). Insomnia and the Performance of US Workers:
Results from the American Insomnia Survey. Sleep, 2011; 34(9): 1161-1171.
5. Shatzmiller RA and Benbadis S.R. Insomnia. Available at:
http://emedicine.medscape.com/article/1187829-overview Revised 2/12/2012; Accessed
4/19/2012.
6. American Academy of Sleep Medicine (2011). The International Classification of Sleep
Disorders, Revised.
www.ejbps.com
96
Uba A.I et al. European Journal of Biomedical and Pharmaceutical Sciences
7. Terauchi M, Hiramitsu S, Akiyoshi M, et al. (2012). Associations between anxiety,
depression and insomnia in peri- and post-menopausal women. Maturitas, May, 2012;
72(1):61-5.
8. Chiang Y.Y, Tsai P.Y, Chen P.C, Yang M.H, Li C.Y, Sung F.C, Chen K.B (2012). Sleep
disorders and traffic accidents. Epidemiology, 2012; 23(4):643–644.
9. Kakizaki M, Inoue K, Kuriyama S, et al. (2008). Sleep duration and the risk of prostate
cancer: the Ohsaki Cohort Study. Br J Cancer. Jul 8; 99(1):176-8. Epub 2008 Jun 10.
10. Verkasalo P.K, Lillberg K, Stevens R.G, et al. (2005). Sleep duration and breast cancer: a
prospective cohort study. Cancer, 2005; 15; 65(20):9595-600.
11. Philips B, Mannino D.M. (2007). Do insomnia complaints cause hypertension or
cardiovascular disease? J Clin Sleep Med. 2007; Aug 15;3(5):489-94.
12. Hublin C, Partinen M, Koskenvuo M, et al. (2011). Heritability and mortality risk of
insomnia-related symptoms: a genetic epidemiologic study in a population-based twin
cohort. Sleep, Jul, 2011; 1; 34(7):957-64.
13. Chien K.L, Chen P.C, Hsu H.C, et al. (2010). Habitual sleep duration and insomnia and
the risk of cardiovascular events and all-cause death: report from a community-based
cohort. Sleep, Feb; 2010; 33(2):177-84.
14. Roth T. (2007) .Insomnia: definition, prevalence, etiology, and consequences. J Clin
Sleep Med, 2007; 3(5 Suppl):S7–S10.
15. Vgontzas A.N, Bixler E.O, Lin H.M, Prolo P, Mastorakos G, Vela-Bueno A, KalesA,
Chrousos G.P. (2011). Chronic insomnia is associated with nyctohemeral activationof the
hypothalamic-pituitary-adrenal axis: clinical implications. J ClinEndocrinol Metab, 2011;
86(8):3787–3794.
16. Fraser R, Ingram M.C, Anderson N.H, Morrison C, Davies E, Connell J.M. (2009).
Cortisol effects on body mass, blood pressure, and cholesterol in thegeneral population.
Hypertension, 2009; 33(6):1364–1368.
17. Anderson M.L, Bignotto M, Machado R.B, Tufik S. (2004). Different stress
modalitiesresult in distinct steroid responses by male rats. Braz J Med Biol, 2004; 37:791-
797.
18. Djordjević J, Cvijić G, Davidović V. (2003). Different activation of ACTH
andcorticosterone release in response to various stressors in rats. Physiol, 52:67-72.
19. Gangwisch J.E, Malaspina D, Babiss L.A, Opler M.G, Posner K, Shen S, Turner J.B,
Zammit G.K, Ginsberg H.N. (2010). Short sleep duration as a risk factor for
www.ejbps.com
97
Uba A.I et al. European Journal of Biomedical and Pharmaceutical Sciences
hypercholesterolemia: analyses of the National Longitudinal Study of Adolescent Health.
Sleep 2010; 33(7):956–961.
20. Kaneita Y, Uchiyama M, Yoshiike N, Ohida T. (2008). Associations of usual
sleepduration with serum lipid and lipoprotein levels. Sleep, 2008; 31(5):645–652.
21. Artham S.M, Lavie C.J, Milani R.V. (2008). Cardiac rehabilitation programs
markedlyimprove high-risk profiles in coronary patients with high psychologicaldistress.
South Med J., 2008; 101:262-7.
22. Hemingway H, Marmot M. (1999). Evidence based cardiology: psychosocial factorsin the
aetiology and prognosis of coronary heart disease. Systematicreview of prospective
cohort studies.BMJ. 1999; 318:1460-1467.
23. Rozanski A, Blumenthal J.A, Davidson K.W, et al. (2005). The epidemiology,
pathophysiology, and management of psychosocial risk factors in cardiacpractice: the
emerging field of behavioral cardiology. J Am Coll Cardiol, 2005; 45:637-651.
24. Stickgold R, Walker M.P. (2007).Sleep-dependent memory consolidation
andreconsolidation. Sleep Med, 2007; 8:331-43.
25. Cintra F, Poyares D, do Amaral A, de Marchi G, Barreto S, Tufik S, et al. (2005). Heart
rate variability during sleep in patients with vasovagal syncope.Pacing Clin
Electrophysiol, 2005; 28:1310-6.
26. Perry J.C, D’Almeida V, Souza F.G, Schoorlemmer G.H, Colombari E, TufikS. (2007).
Effects of subchronic and chronic exposure to intermittent hypoxia andsleep deprivation
on cardiovascular risk factors in rats. Respir PhysiolNeurobiol, 2007; 156:250-258.
27. Gangwisch J.E, Heymsfield S.B, Boden-Albala B, Buijs R.M, Kreier F,Pickering T.G, et
al. (2006). Short sleep duration as a risk factor for hypertension: analyses of the first
National Health and Nutrition Examination Survey. Hypertension, 2006; 47:833-9.
28. Gottlieb D.J, Redline S, Nieto F.J, Baldwin C.M, Newman A.B, Resnick H.E, et al.
(2006). Association of usual sleep duration with hypertension: theSleep Heart Health
Study. Sleep, 2006; 29:1009-14.
29. Cappuccio F.P, Stranges S, Kandala N.B, Miller M.A, Taggart F.M, Kumari M, et al.
(2007). Gender-specific associations of short sleep duration with prevalentand incident
hypertension: the Whitehall II Study. Hypertension, 2007; 50:693-700.
30. Tochikubo O, Ikeda A, Miyajima E, Ishii M. (1996). Effects of insufficient sleepon blood
pressure monitored by a new multibiomedical recorder.Hypertension, 1996; 27:1318-
1324.
www.ejbps.com
98
Uba A.I et al. European Journal of Biomedical and Pharmaceutical Sciences
31. Lusardi P, Zoppi A, Preti P, Pesce RM, Piazza E, Fogari R. (1999). Effects of
insufficientsleep on blood pressure in hypertensive patients.Am J Hypertens, 1999; 12:63-
68.
32. Dimsdale J.E, Herd J.A. (1982). Variability of plasma lipids in response to emotional
arousal. Psychosom Med., 1982; 44(5): 413 – 30.
33. Fakhari A, Ebrahimzadeh M, Shiva S, Fekrat S, Mohammadpoorasl A. (2007). Effect of
mental stress on serum triglyceride level. Research Journal of Biological Sciences,2007;
2(4): 476 – 78.
34. Bower J, and Sergerstrom S. (2011).Stress management; finding benefit and immune
fuction: positive effects on physiology. Journal of Psychosomatic Research, 2001; 56(1):
9 – 11.
35. Uba, A.I., Atiku, M.K., Wudil, A.M. and Aminu, M.S. (2014). Serum lipid profile status
in examination stress condition. Ejbpr, 2014; 1(2) : 551 – 557.
36. Bijlani R.L, Sud S, Gandhi B.M, Tandan B.N. (1986). Relationship of examination stress
to serum lipid profile, Indian J Physiol Pharmacol, 1986; 30(1): 22 – 30.
37. Rosmond R. (2005). Role of stress in the pathogenesis of the metabolicsyndrome.
Psychoneuroendocrinology, 2005; 30(1):1–10.
38. Evans A, Stein M.D. (1986). Lipids, lipoproteins and apolipoproteins: In: Textbook of
Clinical Chemistry (Tietz, W.W. ed) W.H. Saunders Co. Philadelphia: 1986, pp. 884-887.
39. Fossati P, Prencipe L (1982). Serum triglycerides determined colorimetrically with an
enzyme that produces hydrogen peroxide. Clin. Chem., 1982; 28: 2077-2080.
40. Friedewald W.T, et al., (1972). Clin Chem , 18:499
41. Troxel W.M, Buysse D.J, Matthews K.A, Kip K.E, Strollo P.J, Hall M, Drumheller
O,Reis S.E. (2010). Sleep symptoms predict the development of the metabolicsyndrome.
Sleep, 2010; 33(12):1633–1640.
42. Andersen M.L, Perry J.C, Bignotto M and Tufik S. (2009). Differential effect of sleep
loss and chronic stressors on lipid metabolism. Sleep Sci, 2009; 2(3): 135-140.
43. Antunes I.B, Andersen M.L, Alvarenga TAF and Tufik S. (2007). Effects of paradoxical
sleep deprivation on blood parameters associated with risk in intact and ovariectomized
rats compared with male rats behavioural. Behav Brain Res, 2007; 176(2): 187-192.
44. Adamkova V.H. (2009). Association between duration of the sleep and body weight.
Physiol Res, 2009; 1(58suppl): S 27-31.
Related Documents











