The social organisation of chemotherapy treatment consultations Fe´ lix Dı´az Universidad Complutense de Madrid Abstract This paper analyses doctor-patient interaction at the outpatients consultations of a Medical Oncology Service in a Spanish public hospital. First, it introduces the cultural and institutional setting of the research. It then describes some details of the sequential organisation of the routine encounters between patients undertaking chemotherapy and their doctors. Three conventionalised doctors’ utterances (‘How are you’, ‘How are you tolerating the treatment’, and ‘The tests are fine’) are shown to be crucial for assessment and treatment activities. It then discusses how the use of these tokens affects the dimension of casual/institutional talk, and doctor-patient interactional asymmetry. The analysis pays special attention to the way in which treatment decisions are grounded in and projected by the assessment activities in the encounter. The discussion considers how the interactive resources deployed in the consultation relate to the incorporation of patients’ views in routine decisions. Keywords: doctor-patient interaction, oncology, professional dominance Introduction This paper reports an analysis of specific aspects of doctor-patient interaction at the outpatients consultations of a Medical Oncology Service in a Spanish public hospital. The analysis reported here is embedded in a wider project on the communication of symptoms and diagnoses in the medical institution, involving ethnographic and historical research. After introducing the cultural and institutional setting of the research, I will describe some details of the sequential organisation of chemotherapy treatment consultations in the Service. Treatment consultations are routine encounters between patients undertaking chemotherapy and their doctors to monitor the patient’s progress and take routine decisions regarding treat- ment and the patient’s general state. As my general description of these Sociology of Health & Illness Vol. 22 No. 3 2000 ISSN 0141–9889, pp. 364–389 # Blackwell Publishers Ltd/Editorial Board 2000. Published by Blackwell Publishers, 108 Cowley Road, Oxford OX4 1JF, UK and 350 Main Street, Malden MA 02148, USA.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The social organisation of chemotherapytreatment consultations
Fe lix Dõ az
Universidad Complutense de Madrid
Abstract This paper analyses doctor-patient interaction at the outpatientsconsultations of a Medical Oncology Service in a Spanish publichospital. First, it introduces the cultural and institutional settingof the research. It then describes some details of the sequentialorganisation of the routine encounters between patientsundertaking chemotherapy and their doctors. Threeconventionalised doctors' utterances (`How are you', `How areyou tolerating the treatment', and `The tests are fine') are shownto be crucial for assessment and treatment activities. It thendiscusses how the use of these tokens affects the dimension ofcasual/institutional talk, and doctor-patient interactionalasymmetry. The analysis pays special attention to the way inwhich treatment decisions are grounded in and projected by theassessment activities in the encounter. The discussion considershow the interactive resources deployed in the consultation relateto the incorporation of patients' views in routine decisions.
Keywords: doctor-patient interaction, oncology, professional dominance
Introduction
This paper reports an analysis of specific aspects of doctor-patientinteraction at the outpatients consultations of a Medical Oncology Servicein a Spanish public hospital. The analysis reported here is embedded ina wider project on the communication of symptoms and diagnoses in themedical institution, involving ethnographic and historical research.
After introducing the cultural and institutional setting of the research,I will describe some details of the sequential organisation of chemotherapytreatment consultations in the Service. Treatment consultations are routineencounters between patients undertaking chemotherapy and their doctors tomonitor the patient's progress and take routine decisions regarding treat-ment and the patient's general state. As my general description of these
Sociology of Health & Illness Vol. 22 No. 3 2000 ISSN 0141±9889, pp. 364±389
# Blackwell Publishers Ltd/Editorial Board 2000. Published by Blackwell Publishers, 108 Cowley Road,Oxford OX4 1JF, UK and 350 Main Street, Malden MA 02148, USA.
encounters will show, treatment decisions are grounded in and projected bythe assessment activities in the encounter.
My particular interest is with how the features of interaction in theconsultation relate to the incorporation of patients' views in routine treat-ment decisions. Pervasive features of the clinical institution, such as doctors'and patients' differential orientation to medical knowledge, together withthe doctor's lead in the sequential organisation of the encounter, may limitmany chances for patient participation. My analysis will focus on specificinteractional resources which are available to all participants in the inter-action to ensure (or, sometimes, avoid) patients' participation in the routinemanagement of their disease.
By means of this analysis, I hope to offer some directions for improvingthe quality of social relations in the clinic (and particularly in oncologycare), while illustrating the methodological and practical advantages of adetailed analysis of conversational interaction in clinical settings.
Researching social interaction in the medical institutionThe methodological procedures and principles guiding this analysis areinspired by the contributions of ethnomethodological theory and practice tosocial research throughout the last 30 years (see Button 1991, Boden andZimmerman 1991). I use conversation analysis as a method suitable for theinvestigation of situated action in an applied setting and with an ethno-methodological commitment (see Drew and Heritage 1992, Hutchby andWooffit 1998). Conversation analysis and ethnomethodology are incorpor-ated here as resources for reflection on the applied concerns mentioned above.
The research methods deployed here also incorporate other resourcesinherited from the ethnographic tradition, which I regard as always usefuland often necessary for any analytical consideration. These include therecording of descriptions of action in context by writing notes in the courseof the action observed, or shortly after, and the recording of accounts givenby members of the institution about the issues which are the focus of theresearch project (see Charmaz and Olesen 1997). These techniques ofobserving and registering action are equally applied to the description ofcontexts (such as a service, a hospital, or a national health network) whichconstitute members' resources in the interaction analysed.
The consideration and use of data not collected through automaticrecording instruments are a precondition for the possibility of researchingan institution. Accounting for the analyst's availability of the `commonknowledge' or `medical technicalities' needed to understand what is going onin interaction is a researcher's responsibility (see also Cicourel 1992, 1995).This responsibility emerges from the fact that many `commonsensicalstandpoints' can be available to the analyst who confronts transcripts ofinteraction, and adhering to one is a precondition for the analysis.
In this study, my concern is with the interactional aspects of a certainkind of conversational encounter (treatment consultations) in a specific
The social organisation of chemotherapy treatment consultations 365
# Blackwell Publishers Ltd/Editorial Board 2000
institutional setting, which is organised to serve a social purpose (an OncologyService in a public hospital). Whatever occurs in the consultation can onlybe discussed with reference to the organisational and cultural contexts inwhich the specific encounter makes sense and plays a role. Indeed, theconsultation encounters display a practical orientation to other activities inthe Medical Oncology Service to which the encounters are subordinated;they also produce effects on those other settings and, by and large, on thepatients' lives and wellbeing. Thus, this investigation combines the analysisof transcripts of interaction with interpretative notes based on the obser-vation of other environments.
Observation and analysis were carried out with the support of the medicalpractitioners in the Medical Oncology Service of the hospital. BetweenFebruary and July 1998, I attended the Service several days a week. I wouldroutinely sit in one of the outpatients consultation rooms1, wearing a whitecoat and silently observing and taking notes. After a few weeks, I alsostarted to visit the Oncology ward, and the day hospital area wherechemotherapy treatment is given to outpatients. In these visits I would chatinformally with patients, relatives and practitioners I already knew.
In March 1998, I started to explain the research project to specific out-patients taking chemotherapy and their relatives, in order to request theirconsent to audio-record their consultations, giving them an informationsheet about the purpose, method and ethical guarantees of the recording.I requested the participation of 17 patients with their relatives; all of themagreed to participate in the research, except for a patient whose son posedobjections. After acceptance, I would switch the recorder on whenever oneof these patients entered the consultation room, and switch it off when theyleft.
The Medical Oncology Service and the consultationThe Hospital La Paz was constructed in the 1960s as a model for themodernisation of the Spanish hospital system. This system developedthrough the last 30 years in a process that gave the `general hospital' apivotal role in public specialised care, integrating care, research and trainingin complex organisations. This involves reducing in-ward stays to theminimum necessary for acute patients, and increasing the resources andexploitation of specialised areas for outpatient visits. In this context, theMedical Oncology Service of the Hospital La Paz is devoted to providingcare and assistance to cancer patients, on an ambulatory basis, with theavailability of about 30 ward beds.
The Service provides chemotherapy to ambulatory and internal patients,and is co-ordinated with other Services in the hospital related to cancer care:these mainly include several surgery services, the Radiotherapy OncologyService, and a Home Palliative Care Unit for terminal patients. Medicalpractitioners in the Service rotate their duties between the outpatientsconsultation and the hospital ward. The medical staff includes seven
366 Fe lix Dõ az
# Blackwell Publishers Ltd/Editorial Board 2000

oncologists with a permanent position, and four residents in advancedapprenticeship specialising in oncology.
The medical encounters in the consultation can be classified into threetypes with distinctive features; these types are recognised by participants,and the distinction between them is used as an organisational resource. Thestaff refer to these three kinds in forms and reports used in the day-to-daymanagement of the consultation, and in their routine spoken reference tothat management, using the labels New, Treatment, and Follow-up.
The first contact of a patient with the Service is performed through a Newencounter. The patient normally comes to the Service referred from thesurgery service where s/he was operated on (usually in the same hospital),from a district outpatients clinic2, or from their general practice consulta-tion. A New encounter is normally performed dedicating special attentionto the formulation of the diagnosis, as patients often do not know thediagnostic details of their illness, and may be eager to resolve doubts andanxieties about it. It is also common that relatives know more than patientsabout the diagnosis and may be worried about the appropriate disclosure orconcealment of information to the patient (see DõÂ az 1998).
After a general assessment interview and the delicate sequence in whichthe diagnosis is delivered, a New encounter proceeds with the explanation ofthe therapeutic alternatives, and their prognostic possibilities. If the doctoris recommending chemotherapy treatment, s/he will explain its organisationin cycles, the likely side effects, and the decision-making process it implies3.Specifically, depending on the way in which the patient tolerates treatment(known by reference to the patient's symptomatology and to blood teststaken before chemotherapy) and depending on the efficiency of the treat-ment (tested through various methods), the chemotherapy will be continued,changed or suspended throughout the process. The risks and side effects ofthe specific chemotherapy proposed to the patient are summarised in aninformed consent form, which the doctor offers to the patient on a Newencounter, to be returned with the patient's signature.
If a patient agrees to be treated with chemotherapy, s/he will attend theconsultation regularly for a period that ranges between three months andseveral years, taking part in Treatment encounters. Whether the chemicalsare administered through intravenous devices in the day hospital, or pre-scribed to be taken orally at home, the consultation will be the site wheredoctors, patients and relatives consider the general state of the patient, theirtolerance of treatment and the general illness process. As I will illustratelater in a more detailed analysis, these considerations become grounds formost decisions concerning the regulation of treatment and other forms ofintervention for the wellbeing of the patient. The treatment options are thefocus of the consultation.
Normally, the patient attending a Treatment encounter takes an `urgentblood test' (as it is called in the consultation) first thing in the morning.These tests are analysed in a laboratory located elsewhere in the hospital,
The social organisation of chemotherapy treatment consultations 367
# Blackwell Publishers Ltd/Editorial Board 2000
and the results returned to the consultation a few hours after. A Treatmentencounter occurs after these blood tests arrive, so that they can be taken intoaccount for decisions concerning treatment. The remaining sections of thispaper are devoted to describing and analysing Treatment encounters.
If treatment is completed successfully, the patient enters a schedule ofFollow-up encounters, which will occur every several months, and thenyearly, unless complications in the illness suggest new treatment plans.Follow-up encounters are aimed at keeping track of the patient's progress,monitoring her or him for the possible appearance of new tumours, andadvising her or him on general issues of diet, wellbeing, etc.
The standard organisation of chemotherapy treatment consultations
Treatment consultations at the Medical Oncology Service are the site for acontinuing relation between the patient and the Service for a consistentperiod of time. The purpose of dealing with a specific problem known toboth parties in the interaction ± namely, the treatment of the patient's cancer± constitutes a shared background throughout. For a consistent period oftime, the patient attends the consultation to get on with the management ofan illness whose diagnosis has been formerly established (her or his specificcancer) through an intervention which has been agreed (her or his specificchemotherapy treatment). Pilnick (1998) has noted that the clinical relationinvolving chronic patients bears peculiarities that distinguish it from theclassical relation between doctors and episodic patients. The current studycan be read as an investigation of some of these distinctive features.
In this section I provide a very basic account of what goes on in Treat-ment consultations, in terms of a variety of activities or sequences, based onthe close examination of a series of Treatment consultations throughout amonth. My purpose now is to share with the reader a general gloss of theorganisation of these activities, which will help in understanding the analysisin the following section. Some of the details which entitle me to this overalldescription will receive more attention in further sections.
A Treatment consultation will normally involve an assessment of thepatient's general state with respect to both the illness and the ongoingtreatment; I will term these assessment (A) sequences. These include`informings' (i.e. sequences devoted to inform one another) between thepatient and the doctor, and I later describe the way in which theseinformings are produced. The assessment activity is consequentially relatedto the prescription and explanation of treatment by the doctor, such thatsequences focusing on treatment (T sequences) occur after assessmentsequences and rely on them as evidential grounds and practical justification.
There are two other kinds of sequence which serve important functions inthe continuing relation between the patient and the Service, and particularlyin a Service among other services which the patient uses in the public and
368 Fe lix Dõ az
# Blackwell Publishers Ltd/Editorial Board 2000

private health system. Many consultations include what I call Casualinsertions (CI), which resemble greeting sequences in that they show theparticipants' interest and attention to their everyday lives beyond thepatient's illness. The frequency and character of these insertions vary withthe development of a personal relationship between doctor and patient.These insertions reflect features of both institutional and casual talk.
Also, the organisation of the public and private health services, and thatof the hospital itself, require patient and relatives to move from one serviceto another for various purposes, and to learn how to move around thesystem and where to find solutions to occasional troubles. A good part ofthe Treatment consultation may be devoted to informing and assisting theusers about the most efficient management of these procedures. I label theseactivities as Bureaucratic Management (BM) sequences.
In some of their features, chemotherapy treatment consultations aresimilar to counselling medical encounters. They are encounters in whichdoctor and patient maintain a continuing relation with a distinct orientationto a series of routine practices linked to a specific disease and its cor-responding treatment. Counselling encounters with adolescent diabetics(Silverman 1993) would be an analogous case.
To sum up, the general organisation of chemotherapy treatmentconsultations would comprise the following activities:
Initial greetings (IG)The consultation starts with greetings, which may involve personalintroductions if the participants do not remember having met one another,or a `familiarity sequence' (Coupland et al. 1994: 98±9) to connect thecurrent encounter with former ones. The doctor shows interest in thepatient's condition, and comments on the patient's life and their generalappearance may follow, as well as comments on the appointment, how longthe patient had to wait and so on.
Assessment and discussion of the patient's condition (A)The doctor shows interest in the general state and symptomatology of thepatient, and the patient responds. These sequences also include informingsabout the medicines the patient is taking. Sometimes, there may be a directreference to the way in which the patient is tolerating treatment. The patientmay initiate sequences with specific complaints, inviting a physical exam-ination by the doctor. Within these sequences, the doctor also informs thepatient about the results of the examination, or interprets the relevance ofthe patient's symptoms.
Discussion and prescription of treatment and/or further investigations (T)The discussion and prescription of treatment makes use of former Asequences. The doctor may produce extended explanations about themanagement of oral medication. The medication for side effects is discussed.
The social organisation of chemotherapy treatment consultations 369
# Blackwell Publishers Ltd/Editorial Board 2000

The treatment's general organisation in cycles, and the relevant transitionsbetween them, are discussed with reference to evaluations based on scansand endoscopies. On occasions, the doctor will explain the relation betweenthe blood tests, the treatment and the side effects. And the doctor may offereveryday remedies for some problems presented by the patient.
Casual insertions (CI)In these sequences, the doctor may show interest in the patient's leisuretime; the participants' holidays and everyday life are a common topic ofcomment. The main distinction between these activities and the initial andfinal greetings is that participants actively insert CIs in between other moretechnically oriented activities. Ten Have (1991) has referred to this con-versational practice in medical encounters as `small talk'. Frankel (1983)demonstrated the use of these informal comments as a way of distracting thepatient's attention from the doctor's technical action through the physicalexamination. Here they are used for a similar purpose.
Issues of bureaucratic management (BM)In BM sequences, doctors may assist patients in applying for scans andradiographs, and in filling out documents. Participants may discuss the needto make appointments with other services in the hospital, or with the generalpractitioner, and the appropriate management of the relation of the patientwith those other services. Doctors may also need to explain the relation ofthe consultation to the day hospital.
Bureaucratic management also involves sequences concerned with arrangingnext appointments; explanations by the doctor about the importance ofkeeping reports, and the interactional work done to ensure that patientskeep copies of documents. Finally, other bureaucratic management sequencesare aimed at explaining how to get receipts for medication, or the medi-cation itself.
The occurrence of these sequences in the clinical institution is obviouslylinked to what Strong (1979) has called `Bureaucratic Medicine'. It isimportant to note, though, that my reference to bureaucratic managementpertains simply to a particular kind of activity identifiable within consul-tations. The forms of institutional organisation this activity indexicalises arebeyond the scope of this paper.
Final exchanges (FE)The consultation ends with a standard goodbye sequence, which may bepreceded by a mention of the next relevant activity after the patient leavesthe room. It is also common for the final greeting to include references to thegeneral progress of the patient, and their expectations from the treatment. Ifthe patient is not in a positive mood, the doctor may try to cheer them up.The final farewell may be accompanied by the patient and relatives thankingthe doctor.
370 Fe lix Dõ az
# Blackwell Publishers Ltd/Editorial Board 2000
CI and BM sequences may be occasioned at any moment along theconsultation. Assessment sequences normally occur before discussions oftreatment, but the flexibility of the consultation allows for several tran-sitions between these different activities in each consultation. Because of thisflexibility, I avoid talking about these activities or conversational sequencesas established `phases' ordered in a consistent and systematic way (see Byrneand Long 1976). In the following section, I will illustrate how some tran-sitions between activities are performed in a relatively negotiated way.
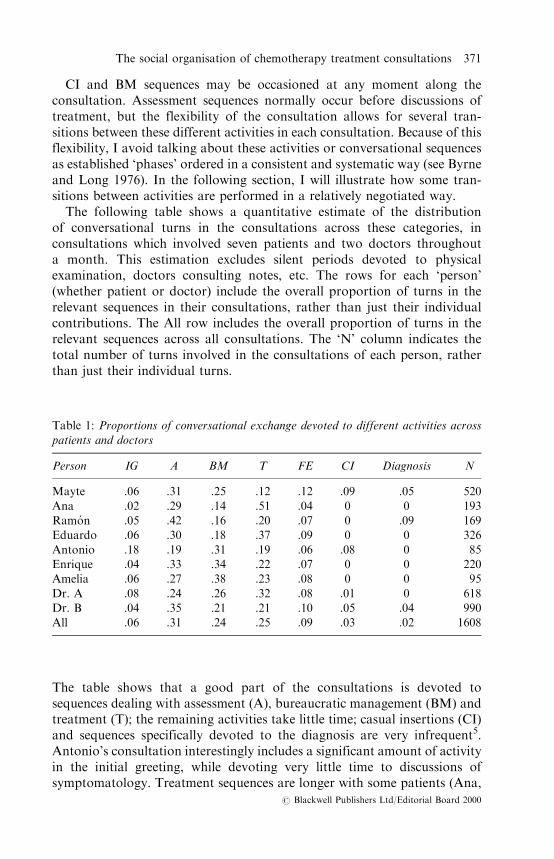
The following table shows a quantitative estimate of the distributionof conversational turns in the consultations across these categories, inconsultations which involved seven patients and two doctors throughouta month. This estimation excludes silent periods devoted to physicalexamination, doctors consulting notes, etc. The rows for each `person'(whether patient or doctor) include the overall proportion of turns in therelevant sequences in their consultations, rather than just their individualcontributions. The All row includes the overall proportion of turns in therelevant sequences across all consultations. The `N' column indicates thetotal number of turns involved in the consultations of each person, ratherthan just their individual turns.
The table shows that a good part of the consultations is devoted tosequences dealing with assessment (A), bureaucratic management (BM) andtreatment (T); the remaining activities take little time; casual insertions (CI)and sequences specifically devoted to the diagnosis are very infrequent5.Antonio's consultation interestingly includes a significant amount of activityin the initial greeting, while devoting very little time to discussions ofsymptomatology. Treatment sequences are longer with some patients (Ana,
Table 1: Proportions of conversational exchange devoted to different activities across
patients and doctors
Person IG A BM T FE CI Diagnosis N
Mayte .06 .31 .25 .12 .12 .09 .05 520
Ana .02 .29 .14 .51 .04 0 0 193Ramo n .05 .42 .16 .20 .07 0 .09 169Eduardo .06 .30 .18 .37 .09 0 0 326
Antonio .18 .19 .31 .19 .06 .08 0 85Enrique .04 .33 .34 .22 .07 0 0 220Amelia .06 .27 .38 .23 .08 0 0 95
Dr. A .08 .24 .26 .32 .08 .01 0 618Dr. B .04 .35 .21 .21 .10 .05 .04 990All .06 .31 .24 .25 .09 .03 .02 1608
The social organisation of chemotherapy treatment consultations 371
# Blackwell Publishers Ltd/Editorial Board 2000

Eduardo); other patients' consultations focus more on bureaucraticmanagement (Enrique, Amelia). My general impression is that more timeis devoted to treatment in interactions with patients from higher `culture orclass' backgrounds, while BM takes up more time with patients from lowersocio-cultural backgrounds (Enrique and Amelia), although the analysisbrought to this report is insufficient to assert this with any certainty.
Three conventionalised tokens, and their sequential placement
Most assessments and decisions emerging from treatment consultations aremanaged either in A sequences, or in transitions between A and Tsequences. In this section I describe the sequential occurrence of threestandardised doctors' actions which, I argue, play a crucial role in theaccomplishment of treatment decisions.
How are you?Around the opening of a treatment consultation, the doctor shows interestabout the patient's general state, offering the patient the opportunity to startwith a description of it. Following Coupland et al. (1992, 1994) I label thestandard tokens used for this purpose as How are you (HAY) tokens:
Excerpt 1 6:
1 Dr A: Antonio, buenos dõ as ((un segundo, mientras Antonio se sienta))¿Co mo estamos?
1 Dr A: Antonio, good morning ((1 second, while Antonio sits down))How are we?
1 Dr A: Good morning, Antonio ((1 second, while Antonio sits down))How are we?
2 Antonio: Bien
2 Antonio: Fine2 Antonio: Fine
3 Dr A: Los ana lisis esta n esple ndidos ((Antonio sonrõ e)). ¿Usted co mo seencuentra?
3 Dr A: The tests are splendid ((Antonio smiles)). You how do youfind yourself?
3 Dr A: The tests are splendid ((Antonio smiles)). How are youfeeling?
4 Antonio: Yo bien, he estado. he estado fuera
4 Antonio: I fine, I have been. I have been out4 Antonio: I'm fine, I've been. I've been out
Former research on `How are you' tokens has paid attention to theambiguity between their `casual' and their `clinical' use, and the way inwhich that ambiguity is resolved (see Silverman 1987: 166±169, Coupland
372 Fe lix Dõ az
# Blackwell Publishers Ltd/Editorial Board 2000
et al. 1992, 1994). Schegloff (1968, 1986) has suggested that greetings incasual conversation serve two basic functions: establishing the identity ofthe speakers, and re-aligning their states of knowledge relative to theencounter at hand. Sacks (1975) discussed the normative requirement that,primarily, a `How are you' is used casually, as a greeting, without involvingthe participants into assessing one another's condition (without them beingexpected to say literally `how they are').
In a clinical conversational environment, the casual use of HAY ispreserved, while its clinical use (assessing the patient's condition) is alsorelevant. A straightforward HAY at the beginning of the encounter opensup the possibility of taking it up in either way. Heath (1981) found that,in general practice consultations, patients normally hear the HAY as aninitiation of the inquiry into the problem that brings them to the con-sultation. Frankel (1990) offers a range of possible responses to HAY inclinical interviews, such that the clinical use can be delayed until the casualtake-up is completed.
This excerpt, drawn from the very beginning of a consultation, shows aninstance of that ambiguity. Dr A's first move makes the two optionsavailable, and the pair 1±2 can, in principle, be read in both senses. `How arewe?' is an interesting formulation in that it chooses the first person plural toaddress a second person. In Spanish, this can be used to mark informalitywhen the interlocutors are well known acquaintances. But here, it ratherseems to indexicalise the institutional alignment between both participants:`How are we?' can be heard as `How are you, with respect to the businessthat brings us together?', where it is Dr A, and not Antonio, that can defineand regulate that business.
However explicit 1 may be as regards the medical relevance of HAY, in 3Dr A reformulates `How are we?' into `How are you feeling?', prefacing itthis time with an optimistic assessment of `the tests'. By doing this, Dr A hasoffered a first assessment and an opportunity for Antonio to respond with asecond. Antonio's response to 3 repeats `fine', and moves into a brief storyabout a recent journey (such that his capacity to go on a journey works toattest that he is fine). So, while Antonio's first `fine' (2) can be understood asresponding either to the casual or the clinical meaning of HAY, the second(4) can only be taken as a relevant response to Dr A's first assessment. It isAntonio's uptake that confirms the second HAY as a clinical one.
The HAY token is commonly introduced at the beginning of theconsultation, often managing to establish the evaluation of the patient'scondition as the first relevant activity. This sequential position opens HAYto ambiguity, as general interest for a newcomer to an encounter is alsoappropriate in greetings. The doctor may deal with this ambiguity byrespecifying the HAY, as above; in this case, the response to the first HAYcan be treated as casual or clinical, while the second response is bound tothe clinical formulation of the first HAY, and can only be understood asclinical.
The social organisation of chemotherapy treatment consultations 373
# Blackwell Publishers Ltd/Editorial Board 2000
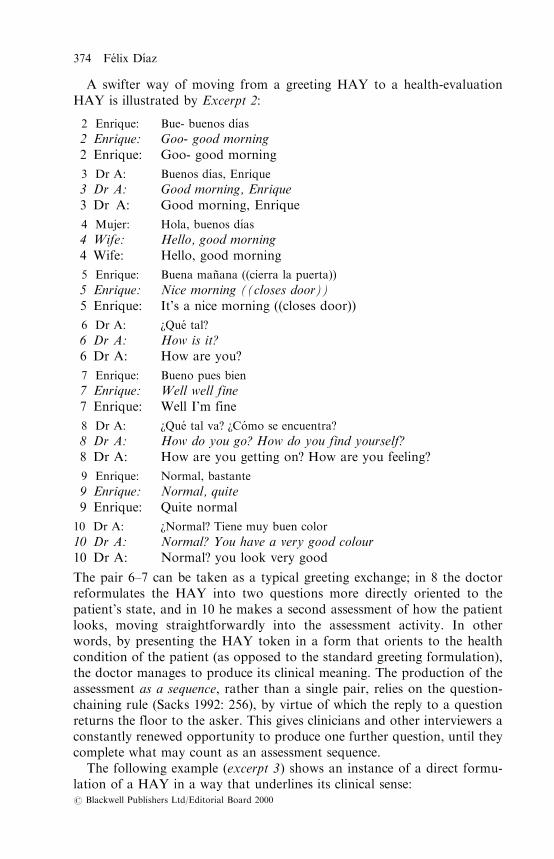
A swifter way of moving from a greeting HAY to a health-evaluationHAY is illustrated by Excerpt 2:
2 Enrique: Bue- buenos dõÂ as
2 Enrique: Goo- good morning2 Enrique: Goo- good morning
3 Dr A: Buenos dõÂ as, Enrique
3 Dr A: Good morning, Enrique3 Dr A: Good morning, Enrique
4 Mujer: Hola, buenos dõÂ as
4 Wife: Hello, good morning4 Wife: Hello, good morning
5 Enrique: Buena manÄ ana ((cierra la puerta))
5 Enrique: Nice morning ((closes door))5 Enrique: It's a nice morning ((closes door))
6 Dr A: ¿Que tal?
6 Dr A: How is it?6 Dr A: How are you?
7 Enrique: Bueno pues bien
7 Enrique: Well well fine7 Enrique: Well I'm fine
8 Dr A: ¿Que tal va? ¿Co mo se encuentra?
8 Dr A: How do you go? How do you find yourself?8 Dr A: How are you getting on? How are you feeling?
9 Enrique: Normal, bastante
9 Enrique: Normal, quite9 Enrique: Quite normal
10 Dr A: ¿Normal? Tiene muy buen color
10 Dr A: Normal? You have a very good colour10 Dr A: Normal? you look very good
The pair 6±7 can be taken as a typical greeting exchange; in 8 the doctorreformulates the HAY into two questions more directly oriented to thepatient's state, and in 10 he makes a second assessment of how the patientlooks, moving straightforwardly into the assessment activity. In otherwords, by presenting the HAY token in a form that orients to the healthcondition of the patient (as opposed to the standard greeting formulation),the doctor manages to produce its clinical meaning. The production of theassessment as a sequence, rather than a single pair, relies on the question-chaining rule (Sacks 1992: 256), by virtue of which the reply to a questionreturns the floor to the asker. This gives clinicians and other interviewers aconstantly renewed opportunity to produce one further question, until theycomplete what may count as an assessment sequence.
The following example (excerpt 3) shows an instance of a direct formu-lation of a HAY in a way that underlines its clinical sense:
374 Fe lix Dõ az
# Blackwell Publishers Ltd/Editorial Board 2000

1 Hija: Hola
1 Daughter: Hello1 Daughter: Hello
2 Dra B: Hola, adelante. ¿Que tal, Ana? . ¿Mejor?
2 Dr B: Hello, come in . How is it, Ana? . Better?2 Dr B: Hello, come in . How are you, Ana? . Any better?
3 Ana: Sõ . Un poco ma s . estable . (. . .)
3 Ana: Yes . A bit more . stable . (. . .)3 Ana: Yes . A bit more . stable . (. . .)
`Any better?' orients to the shared knowledge that Ana was not feeling verywell in former encounters. Juxtaposed to a HAY, it constructs the meaningof HAY as related to whatever was wrong before and now could be better,initiating an assessment sequence. As a whole, line 2 conflates the greetingwith the clinical inquiry.
Even if participants start talking about the patient's condition throughany other procedure, explicit HAYs mark the initiation of a standardceremony of assessment of the patient's condition. In the following excerpt(excerpt 4), the doctor's HAY does some interactional work in this sense:
16 Dra B: Pues le estaba diciendo a [Fe lix que:
16 Dr B: Well I was telling [FeÂlix that:16 Dr B: Well I was telling [Fe lix that
17 Marido: [( ) doctora
17 Husband: [( ) doctor17 Husband: [( ) doctor
18 Dra B: que te ha visto hoy, que te ha visto con ((riendo:)) buena cara
18 Dr B: that he has seen you today, that he has seen you with((laughing:)) good face
18 Dr B: that he's seen you today, that he's seen you ((laughing:))looking good
19 Mayte: ¿SõÂ ? ((rõÂ e))
19 Mayte: Yes? ((laughs))19 Mayte: Has he? ((laughs))
20 Marido: SõÂ , hoy . hoy es otro: panorama
20 Husband: Yes, today . today it is anothe:r panorama20 Husband: Yes, today . today it's a differe:nt picture
21 Dra B: Bueno, ¿que tal? ¿Co mo te encuentras?
21 Dr B: Well, how is it? How do you find yourself?21 Dr B: Well, how are you? how are you feeling?
22 Mayte: Pues bien, volvõ a la: normalidad . vamos . ((explicacio n extendida))
22 Mayte: Well fine, I went back to the: normality . let's go .((lengthy account))
22 Mayte: Well I'm fine, I returned to: normality . I mean .((lengthy account))
The social organisation of chemotherapy treatment consultations 375
# Blackwell Publishers Ltd/Editorial Board 2000

Up to 20, several comments have been made informally about Mayte'scondition, but she has not had the chance to make her own (19 is just arepeat of 18). By introducing a HAY in 20, the doctor offers the next turn toMayte, inaugurating a more formal assessment sequence in which she willreceive direct attention. Also, note that 20 is designed with two alternativeformulations of HAY, the second one (`how are you feeling?') being moreclearly clinical.
So, normatively, HAYs are positioned at the beginning of theconsultation, within or immediately after the initial greeting sequence, andoperating a transition from the greeting sequence to an assessment sequence.On occasions, the assessment sequence can be postponed, but the rule ofoffering a HAY at the beginning will be preserved:
Excerpt 5:
1 Dr A: ((a aprendices:)) Este es un ca ncer de pulmo n de sesenta y dos anÄ os,
. en principio esta : con tratamiento, (1) tolero muy mal el primerciclo de quimio[terapia y la querõ an
1 Dr A: ((to trainees:)) This is a cancer of lung of a 62 year old, . inprinciple she is with treatment, (1) she tolerated very badly thefirst cycle of chemo[therapy and they wantedher to
1 Dr A: ((to trainees:)) This is a 62-year-old lung cancer, . in principleshe's taking treatment, (1) she tolerated the first cycle ofchemotherapy [very badly and they wanted her to
2 Amelia: ((entrando)) [doctor
2 Amelia: ((entering)) [doctor2 Amelia: ((entering)) [doctor
3 Dr A: ingresar ¿Que tal Amelia? . Ya la he visto antes por ahõ fuera .¿Co mo estamos, hija?
3 Dr A: get in, How is it Amelia? . Already I have seen you beforearound there outside . How are we, daughter?
3 Dr A: come onto the ward . How are you Amelia? . I saw youbefore out there . How are we, my child?
4 Amelia: Pues y- yo creo que bien ahora de momento
4 Amelia: Well I- I think that fine now for the moment4 Amelia: Well I- I think I'm fine now for the moment
5 Dr A: Vamos [a ver
5 Dr A: We are going [to see5 Dr A: Let's [see
6 Amelia: [Yo vengo a ver las cosas
6 Amelia: [I come to see the things6 Amelia: [I'm coming to see how things are
7 Dr A: Estaba: aguantando un poquito . y no se si si: hay cama . si hubieracama ¿le gustarõ a ingresar para hacerse el pro ximo ingresada?
376 Fe lix Dõ az
# Blackwell Publishers Ltd/Editorial Board 2000

7 Dr A: I was holding a little bit . and I don't know if i:f there is bed . ifthere were bed, would you like to go in to do the next oneinside?
7 Dr A: I was waiting for a little while . and I don't know if if there isa bed . If there is a bed, would you like to come onto theward to do the next one in the ward?
8 (3)
So, after the initial formal sequence in which the doctor shows interest in thepatient's condition through a HAY (3±6), the interaction moves on to thedecision about whether Amelia will enter the ward or not ± one of the maintopics in this specific encounter. After the decision is taken, the doctor willoffer a new HAY:
Excerpt 6:
26 Dr A: (. . .) . El primero ya sabe que lo paso mal
26 Dr A: (. . .) . The first you already know that you passed it bad26 Dr A: (. . .) . You already know that your first (cycle) was bad
27 Amelia: mh . [sõÂ , sõÂ es verdad
27 Amelia: mh . [yes, yes it is true27 Amelia: mh . [Yes, it was
28 Dr A: [ambulatoriamente, entonces vamos a ver si ingresada co mo lo pasa
. ¿Co mo se ha encontrado estos quince dõ as?
28 Dr A: [the ambulatory way, then we are going to see if inside howyou pass it . How have you found yourself these fifteen days?
28 Dr A: [as an outpatient, then let's go into the ward and see howyou are. How have you felt this last fortnight?
29 Amelia: Pues estos bien
29 Amelia: Well these fine29 Amelia: Well these I've been fine
30 (1) ((assessment interview))
This time, the HAY does initiate an assessment sequence.To sum up so far: normally, the doctor offers a HAY token to the patient
at the onset of the technically-oriented activity in the consultation, andnormally this generates an assessment sequence. If necessary, assessmentHAYs are formulated in a distinctive way to distinguish them from greetingHAYs. Still, the possible ambiguity between clinical and casual uses of HAYdoes not produce disruption, as a casual uptake of HAY is also legitimate,and the clinical use can follow the courteous exchange. This compatibilitycontradicts Silverman's (1987: 166) suggestion that ambiguity between thecasual and clinical uses of HAY `creates interactional problems in manymedical encounters'.
The doctor's HAY establishes the patient's self-assessment of their healthcondition as the next relevant action in a standard ceremonial way. The
The social organisation of chemotherapy treatment consultations 377
# Blackwell Publishers Ltd/Editorial Board 2000
doctor may act to limit this relevant next action, and then recover it througha further HAY token to reintroduce an assessment sequence.
The tests are fineIn excerpt 1 above, the HAY token appeared interlocked with an assessmentof `the tests' by the doctor. This is common practice in the beginning ofassessment sequences. As the patient is offered the opportunity to offer anassessment of his or her condition, the doctor gives a parallel assessmentbased on a technical measure: the blood tests taken first thing in themorning, the results of which the consultation has been waiting for. Thisdoctor's action is a form of medical information delivery to which Byrneand Long (1976) refer as `assessing the patient's condition'.
A `The tests are fine' (TTAF) token is commonly presented in theconversational environment of a HAY token to mirror the patient's self-assessment; in turn, it also contributes to establishing the medical relevanceof the HAY. My interest now is with how and when the TTAF issequentially produced, and what work is accomplished by producing it insuch a manner and on such occasions. In excerpt 1, the TTAF works as asecond assessment of Antonio's `Fine' (2), and is followed by a re-assertionby Antonio (4). In other words, it is a doctor's assessment in between twoassessments by the patient, both elicited by the doctor.
Excerpt 1 is also an instance of the Perspective Display Series (PDS)(Maynard 1991a, 1991b, 1992), by means of which the doctor solicits anassessment from the patient before providing his or her own version. So thatDr A's HAY (1) elicits Antonio's `Fine' (2), and immediately after, Dr Aproduces an assessment of the tests (3) which, in this case, is perfectly tunedwith Antonio's self-assessment. According to Maynard, the PDS is a deviceby means of which doctors can co-implicate the patient's self-assessment inthe delivery of diagnostic information (Maynard 1992). It also marks thedifferential position of doctor and patient with respect to the clinicalinstitution, by facilitating the production of the doctor's clinical assessmentas the most exhaustive one, and the definitive one (Maynard 1991b).
Nevertheless, an account of the PDS solely in terms of the tactics ofinformation delivery might divert our attention from the fact that doctorsuse the information they receive from their patients, and not just to designthe delivery of their assessment. This information is also crucial to thepurpose of taking decisions about treatment (a task for which theconsultation is designed). In chemotherapy treatment consultations, doctorsproduce third parts of PDS that display alignment with the patient'sassessment. This has been found to be exceptional in clinical practice (seeFrankel 1984), where doctors omit any comment regarding the validity oftheir patient's responses. What is noteworthy in our assessment-mirroringsequences is the organisation of the assessment sequence so as to establishthe grounds for a decision; these grounds need to cover both the doctor'sassessment of the tests and the patient's self-assessment.
378 Fe lix Dõ az
# Blackwell Publishers Ltd/Editorial Board 2000
In other words, the patient's self-assessment, together with the doctor'spresentation of the results of the tests, will establish the basis for a decisionon the continuation, change or suspension of treatment. But the presen-tation of an actual decision by the doctor will normally be prefaced by anassessment of the tests, rather than the patient's self-assessment. Let usreturn to Antonio's consultation. After the sequence shown in excerpt 1, aseries of comments about Antonio's condition (which is constructed asnormal), and a Casual Insertion follow; then, the doctor introduces anotherTTAF token to move into a Treatment sequence:
Excerpt 7:
52 Dr A: ah, aquõ ha llovido ma s
52 Dr A: Oh, here it has rained more52 Dr A: oh, it's been raining more here
53 Antonio: mh
53 Antonio: mh53 Antonio: mh
54 Dr A: Muy bien, bueno pues los ana lisis esta n muy bien . Hoy vamos apor el octavo
54 Dr A: Very good, well well the tests are very good . Today we go forthe eighth
54 Dr A: Okay, well the tests are very good . Today we are going forthe eighth
55 Antonio: mh
55 Antonio: mh55 Antonio: mh
56 Dr A: Entonces la idea que tenõ amos . es que se le va a poner otra vez paradarle . otro ma s . hasta un noveno . y luego ya
56 Dr A: Then the idea that we had . is that you are going to be putanother time to give you . another one . to a ninth . and thenalready
56 Dr A: So our idea . was that you're going to be given again to giveyou . one more . up to a ninth . and then (. . .)
This second TTAF token (54) completes the former sequence to initiate atreatment sequence. It is presented as the grounds for continuing withtreatment. But, what exactly do `the tests' test? What is their technical use?In the following sequence, a patient makes an attempt at giving an answer tothis question; the doctor corrects her, giving an account that glosses thepractical meaning of the tests in and for the Medical Oncology Service:
Excerpt 8:
80 Mayte: y con lo:s ana lisis ustedes van viendo . lo que retrocede-
80 Mayte: and with the: tests you go seeing . what it moves back-80 Mayte: and with the: tests you keep track of . how it recedes-
The social organisation of chemotherapy treatment consultations 379
# Blackwell Publishers Ltd/Editorial Board 2000

81 Dra B: No, los ana lisis nos sirven como control
81 Dr B: No, the tests serve us as control81 Dr B: no, the tests serve as a control
82 Mayte: No, le quiero decir=
82 Mayte: No, I want to say to you=82 Mayte: no, what I mean is=
83 Dra B: =de las ce lulas de la sangre para ver
83 Dr B: =of the cells of the blood to see83 Dr B: =of the blood cells to see
84 Mayte: [sõÂ
84 Mayte: [yes84 Mayte: [yes
85 Dra B: [si el tratamiento se puede . poner . si las cosas van mal . Tenemos
un riesgo que es el de la:s plaquetas . bajas, que ya como estamos .Y: y le pongo el tratamiento a dosis . reducidas, a menos dosis de laque le corresponde, por esa razo n . Si vemos que lo tolera bien, pues
le podemos . subir un poquito .[Eso ya
85 Dr B: [if the treatment can be . put . if the things go wrong . We havea risk which is that of the: low . platelets, which already as weare . A:nd and I put you the treatment at reduced . dosage, atlower dosage than that which corresponds to you, for thatreason . If we see that you tolerate it fine, then we can . riseyou a little bit .
[That then85 Dr B: [if treatment can be . given . if things go wrong . We
have a risk which is that of low . platelets, which as we arealready- . And I am giving you the treatment at reduced .dosages, at a lower dosage than we would normally give you,for that reason . If we see that you are tolerating it fine, thenwe can . raise it a little bit . [That is-
86 Mayte: [no, lo decõÂ a porque como
dice que a lo mejor con tres ciclos era bastante,
86 Mayte: [No, I was saying itbecause as you say that maybe with three cycles it was enough,
86 Mayte: [no, I was saying itbecause as you are saying that maybe three cycles would beenough,
87 Dra B: Tenemos que hacer para eso un:- un esca ner . (. . .)
87 Dr B: We have to do for that a:- a scan . (. . .)87 Dr B: We have to do a- a scan for that . (. . .)
In this sequence, the patient starts displaying an understanding that `thetests' are used to `keep track of how it recedes', where `it' refers to thetumour. The doctor denies the patient's guess, and clarifies that blood tests
380 Fe lix Dõ az
# Blackwell Publishers Ltd/Editorial Board 2000

are actually meant to keep track of the state of blood cells in relation totreatment. The growth or retreat of the tumour can only be measured bymeans of other tests, such as scanners. It is important to note that, althoughthis basic explanation of the practical meaning of the tests is given in everyNew encounter, patients recurrently ask about their meaning in Treatmentencounters, and sometimes display the wrong understanding shown here byMayte. On the other hand, and as I will discuss below, the asymmetricalstructure of the doctor±patient relation may be keeping some patients fromasking about this issue.
Of course, the blood tests can give good and bad results; they are notalways fine. A bad result in the tests gives grounds for the doctors toinvestigate the relation between the tests and the patient's general state,producing an extended assessment sequence:
Excerpt 9:
9 Dr A: Bueno Eduardo, ¿co mo estamos hoy? ¿mh?
9 Dr A: Well Eduardo, how are we today? mh?9 Dr A: Well Eduardo, how are we today? uh?
10 Eduardo: Pue:s . flojito
10 Eduardo: We:ll . a bit weak10 Eduardo: We:ll . a bit weak
11 Dr A: Sigue muy bajo de leucocitos hoy . ¿Co mo va esa: ese catarro?
11 Dr A: You go on very low of leukocytes today . How goes that: thatcold?
11 Dr A: Your leukocytes are still very low today . How is that: thatcold going?
12 Eduardo: Bueno el catarro iba bastante bien . ((explicacio n extendida))
12 Eduardo: Well the cold was going quite well . ((lengthy account))12 Eduardo: Well the cold was going quite well . ((lengthy account))
This extract exemplifies the use of the Perspective Display Series as a devicethat enables the doctor to co-implicate the patient's perspective in the thirdpart of the series (Maynard 1992). So Dr A can produce his assessment thatEduardo's `leukocytes are still very low' and show concern about his `cold'as a topical continuation of his claim to feel `a bit weak'. Thus, the badassessment of the tests and the participants' comments on Eduardo'sweakness and other symptoms are bound together and used reciprocally tomake sense of one another.
On the other hand, this example exposes a certain peculiarity in the designof the delivery of bad tests results. Compare the following doctor's assess-ments of test results:
3 Dr A: The tests are splendid ((Antonio smiles)). How are youfeeling?
(excerpt 1)
The social organisation of chemotherapy treatment consultations 381
# Blackwell Publishers Ltd/Editorial Board 2000
54 Dr A: Okay, well the tests are very good. Today we are going forthe eighth
(excerpt 7)
11 Dr A: Your leukocytes are still very low today. How is that thatcold going?
(excerpt 9)
In excerpts 1 and 7, the delivery is produced with a straightforwardstatement designed in a patterned way: `The tests are [splendid/very good/better]'. In excerpt 9, the doctor does not say straightforwardly `the tests arebad'. Rather, he designs his turns in ways that show the dispreferredcharacter of giving a test result which is not as good as it could or should be.He refers to the specific information in the tests which is presented asproblematic (low leukocytes). He also shows orientation to the temporallocation of this measure (still, today), displaying his knowledge that theleukocytes have been low on previous appointments. And he follows with aquestion that attends to a specific process in the patient that might berelated to the bad results (that cold).
Summing up, the doctor's reference to `the tests' can play two sequentialfunctions; in the environment of a HAY, it introduces the blood tests asa new standard of evaluation of the patient's condition, which will becompared with other kinds of assessment. And, later in the consultation, itprompts the initiation of a proposal regarding treatment, being the maincriterion for such decisions. As I will discuss in the next section, the tests aretreated as sounder evidence for clinical decisions than the other consider-ations with which they can be contrasted.
How are you tolerating the treatment?Another conventional token, linked to HAYs in the opening of assessmentsequences, is How are you tolerating the treatment? (HAYTT). By means ofa HAYTT, the doctor invites the patient to comment on his or her healthcondition, but circumscribing the relevant field of comment to thesymptoms normally associated with treatment.
Excerpt 10 :
12 Dr A: ¿Que tal va tolerando el tratamiento? . ¿Bien?
12 Dr A: How do you go tolerating the treatment? . Fine?12 Dr A: How are you tolerating the treatment? . Fine?
13 (1)
14 Mujer: Un poquillo cansao, esta y no come como comõ a . el otro dõ a ladoctora le dijo que le iba a dar un . un reconstituyente y e l no
quiso
14 Wife: A little bit tired, he is and he doesn't eat as he was eating . theother day the doctor said to him that she was going to give hima . a reconstituent and he didn't want
382 Fe lix Dõ az
# Blackwell Publishers Ltd/Editorial Board 2000

14 Wife: He is a little bit tired, and he's not eating normally . theother day the doctor said she was going to give him a . atonic and he refused
A relevant response to a HAYTT by the patient or relative should focus onthe relevant topical field: symptoms and problems associated with chemo-therapy. In this case, the wife of the patient mentions tiredness and lack ofappetite, which refer to the kind of problems known to be correlative withchemotherapy. Note that the doctor addressed the HAYTT to the patient,and that it is his wife who answers after a lapse of one second. The patientmay not have understood the doctor's HAYTT (as commonly happens inconsultations with patients from lower social-cultural backgrounds). If thepatient shows problems in understanding the HAYTT, or if s/he gives aminimal response, the doctor will normally continue with more specificquestions, referring to the particular symptoms associated with chemo-therapy treatment:
Excerpt 11:
(1)
28 Dra B: ¿Que tal tolero el: el ciclo del otro dõ a?
28 Dr B: How did you tolerate the: the cycle of the other day?28 Dr B: How did you tolerate the the cycle the other day?
29 Ana: Muy bien
29 Ana: Very well29 Ana: Very well
30 Dra B: ¿No vomita?
30 Dr B: You don't vomit?30 Dr B: No vomiting?
31 Ana: Nada
31 Ana: Nothing31 Ana: Nothing at all
32 Dra B: No vomita na[da, ¿no?
32 Dr B: You don't vomit no[thing, no?32 Dr B: You don't vomit at [all, do you?
33 Ana: [pero nada
33 Ana: [but nothing33 Ana: [well nothing at all
34 Dra B: ¿Las pastillas entran bien?
34 Dr B: Do the pills get in well?34 Dr B: No problem swallowing the pills?
35 Hija: Muy bien muy bien
35 Daughter: Very well very well35 Daughter: No problem at all
The social organisation of chemotherapy treatment consultations 383
# Blackwell Publishers Ltd/Editorial Board 2000
By developing HAYTTs into question-answer chains, such that the ques-tions refer to the common problems linked to chemotherapy, the doctorestablishes a field of relevant problems to review in the assessment. Thesequential features of question±answer chains (Sacks 1992: 256) allow thedoctor to complete an exploration of the relevant domain. To summarise,HAYTTs accompany HAYs in the conversational environment wheresymptom-assessment sequences are initiated, focusing on a set of problemstypically associated with treatment.
Conclusions
On the whole, the ways in which different kinds of knowledge are used andhandled in the consultation are directly linked to the ways in which speakersare positioned with respect to the institution. Patients and relatives canprovide assessments that will be treated as descriptions of feeling or opinion.These are useful resources for the doctor, together with the results of bloodtests, but the latter play a more direct role in resolutions regarding treat-ment. By monitoring the insertion of HAY, HATT and TTAF tokens, andby virtue of the structural properties of question-answer chains (Sacks 1992:256, Frankel 1990), the doctor has direct control over the process of assess-ment, which often relies on a comparison between the patient's reports andthe blood tests.
Before ending, I will briefly comment on the patients' cultural backgroundas regards the structural organisation of assessment in the consultation. AsAmelia suggests in excerpt 5, and as former studies of interaction in medicalencounters have illustrated, many patients come to see the doctor with theassurance that the doctor knows all that needs to be known (see Charleset al. 1998, for a review). Also, in Western cultures it may be regarded asimpolite or unnecessary to ask questions of the doctor (Fisher 1984). Westhas offered evidence that physicians tend to monopolise the right to askquestions in consultations (West 1984), and that questions asked by patientsare designed as dispreferred turns (West 1983).
This limited evidence of patients' questioning is in spite of the right ofpatients to information advocated by the socialisation and liberalisation ofmedicine, which is given secondary relevance in ethics handbooks. As far asI have observed, it is much more common for patients from a lower socio-cultural background (Enrique and Amelia in the sample presented here) toassume this passive footing in the consultation. In turn, this footing iscomplemented with the doctors' active role in monitoring the interaction(see also Fisher 1983).
Patient participation in the ongoing process of decision-making throughtheir chemotherapy is not only a matter of competing rights at the level ofethics handbooks. Through the day-to-day management of the delivery ofa service, the patient's participation is locally related to their self-awareness
384 Fe lix Dõ az
# Blackwell Publishers Ltd/Editorial Board 2000
and education regarding how to use the service efficiently (Charles et al.1998). Participation also impinges on their ability to confront a chronicillness which is still loaded with stigma, significant silences and fatalisticmetaphors (see Sontag 1979). And (perhaps the most common worry formedical practitioners), it is directly connected with the ease of relationshipbetween the patient and the Service.
But the possible correlation between `patient participation' and othermeasures valued by practitioners loses relevance in the light of an ethicalposition that promotes patients' rights. My analytical work addresses thelocal workings of the accomplishment of participation in the relevantapplied settings; correlational research provides little help to this end.
The main analytical outputs of this paper can be summarised asfollows:
1. Treatment consultations cover a series of activities which can beidentified and described. These include greetings, the assessment of thepatient's condition, the prescription of treatment, the explanation ofbureaucratic matters and, occasionally, diagnostic informings and casualinsertions. The sequential organisation of these activities is such that,although they are identifiable as patterns of action orientation, they areclosely bound with one another in the course of their production.Although there are certain binding rules of order between the sequences,the transition from one activity to another is a participants' accomplish-ment, and thus it is negotiable.
2. The most predominant kinds of activity in the consultations are discussionsof the patient's condition (31 per cent), prescriptions of treatment (25 percent), and explanations about the management of bureaucratic tasks(24 per cent). The amount of time devoted to bureaucratic issues, and thepractical orientation to them, make sense in a health system that makesthe patient responsible for the organisation of appointments, the acqui-sition of medication and many other activities to do with the remediationof their health problem. I see this organisational feature as an effect ofthe way in which the socialisation and liberalisation of medicine havetaken form in Spain.
3. The `How are you' (HAY) token at the beginning of the medicalencounter can be perceived as giving relevance to either its casual or itsclinical meaning. This ambiguity is not problematic, as it is immediatelyresolved in the subsequent turns, and both meanings can and do play apart in the consultation. By virtue of the question-chaining rule, HAYsbecome the formal onset of assessment sequences. They can also be usedto mark the initiation of an assessment sequence, ending some otheractivity. The `How are you tolerating the treatment' (HAYTT) token is aversion of the clinical use of HAY which restricts the topical domain ofthe assessment of the patient's condition to the culture of `toleratingchemotherapy'.
The social organisation of chemotherapy treatment consultations 385
# Blackwell Publishers Ltd/Editorial Board 2000
4. When doctors inform the patient about the blood tests, they locate anddesign the informing to compare them with the patient's self-assessmentsof their condition. The Perspective display series (PDS) is a deviceavailable for this purpose, while retaining the functions Maynard (1992)ascribes to it as a strategy for diagnostic communication. On the otherhand, bad test results are given in ways that show the dispreference forthem as opposed to the normal, good results. Both the PDS and thedesign of bad news deliveries are doctors' devices that invoke a sense ofsolidarity between doctor and patient.
5. The sequences in which HAYs, HAYTTs and assessments of the tests areclosely bound together work to establish the crucial evidence fordecisions on treatment. It is common that a good assessment of the testswill mark the initiation of a treatment sequence. An institutional relationof subordination between the general assessment produced by inform-ings by the patient and the objective measurement of the tests seems to bein operation in the consultations, such that the tests preponderate assounder evidence (where sounder evidence is that which accomplishesobjectivity).
A relevant question concerning these analytical outcomes is: Where do thesestructures of social interaction belong? Are they contingent on encounters inthe clinical institution, in oncology care, in Spanish oncology care, or in thisparticular Service? I would suggest that we consider the issue of general-isation with scrupulous attention to the specifics of the contexts analysed.Since studies of this sort have been predominant in English-speakingsocieties, the reader may be tempted to regard the analysis presented here asparticularly providing `Spanish results'. But this analysis should rather beread as a case study in an organisation which bears many peculiarities otherthan the language used or the State that rules above it.
I would like to end with a reflection which is more practical thananalytical, in the sense that it orients to the ways in which oncology staff canconsider improving their practice. Patients may, on occasion, display mis-understandings as to what `the tests' are for, how important their feelingsand impressions are, and which feelings and impressions in particular. Yet,they do not always know whether these confusions are relevant enough to bemade explicit. While doctor±patient asymmetry is an ever-present accom-plishment of interaction in the medical institution (see also Ten Have 1991,Maynard 1991a), the routines through which the doctor monitors theconsultation should include explicit procedures for ensuring that the patientknows how decisions regarding treatment are taken.
Specific action addressed to empowering the patient with knowledgeabout the routine tasks in the consultation may compensate for the limitsthat professional dominance imposes on their knowledge of such tasks.Doing routines is doctors' work. It makes doctors' work economic, practicaland feasible within given space-time limits. If the routines are making it
386 Fe lix Dõ az
# Blackwell Publishers Ltd/Editorial Board 2000

difficult for patients to participate, a possible solution may be to pay specialattention to the slots the routines provide for patient participation, and tomanage these slots appropriately.
Address for correspondence: FeÂlix DõÂaz, C/Puerto de Lumbreras, 15-38B,28031-Madrid, Spaine-mail: [email protected]
Acknowledgements
This research is supported by a postdoctoral fellowship from the Regional Council ofMadrid to the author. I am grateful to the clinical assistants at the Medical OncologyService of the Hospital La Paz, and to Dr. Javier de Castro, Dr. Marisa GarcõÂ a de
Paredes and Dr. BegonÄ a de las Heras for their availability and support through thefieldwork process. Dr. Amalio Ordo nÄ ez had the courage to open the doors of theService for me. Charles Antaki, Derek Edwards, Geraldine Leydon, Beatriz Martõ n,
David Silverman and an anonymous reviewer offered very helpful comments onformer versions of this paper which make this a much better final version. I am alsograteful to Janet Smithson for her competent linguistic suggestions.
Notes
1 The outpatients consultations in this Service are divided up into two teams ofpractitioners, one devoted to patients with malignancies from the respiratory
and digestive systems, as well as lymphomas, and the other devoted to patientswith head, neck, breast, urinary and prostate malignancies. All the analysis wascarried out on the first team.
2 District outpatients clinics are public health centres where patients may bereferred from their GP for specialised consultations. Most of them do not includean oncology section. Still, they may be the intermediate step between the general
practice consultation and the Medical Oncology Service in the Hospital.3 If the proposed treatment is surgical or radiological, the patient is transferred to
the relevant Service in the hospital, and will probably return to the MedicalOncology Service for further chemotherapy or for the follow-up. If no treatment
is possible, the patient may be offered the Home Palliative Care Unit.4 To respect participants' confidentiality, all names are fictitious.5 Here I am referring to `diagnostic informings' as a particular kind of information
delivery by the doctor; these consultations do include other forms of informationdelivery, such as assessments of the patient's general condition and explanationsof background information. The latter may occur within any sequence as I have
categorised them.6 Transcription conventions are adapted from Gail Jefferson's, given in Atkinson
and Heritage (1984). For each line of transcript, I provide the Spanish original (innormal characters), an extremely literal translation (in italics) and a pragmatic
colloquial English version. This can give the reader a sense of the transformationsinvolved in the translation, as well as showing some rhetorical forces in theSpanish original which cannot always be preserved.
The social organisation of chemotherapy treatment consultations 387
# Blackwell Publishers Ltd/Editorial Board 2000
References
Atkinson, J.M. and Heritage, J. (1984) Structures of Social Action: Studies inConversation Analysis. Cambridge: Cambridge University Press.
Boden, D. and Zimmerman, D.H. (1991) Talk and Social Structure: Studies in
Ethnomethodology and Conversation Analysis. Cambridge: Polity Press.Button, G. (ed) (1991) Ethnomethodology and the Human Sciences. Cambridge:Cambridge University Press.
Byrne, P.S. and Long, B.E. (1976) Doctors Talking to Patients. London: HMSO.Charles, C., Redko, C., Whelan, T., Gafni, A. and Reyno, L. (1998) Doing nothing isno choice, Sociology of Health and Illness, 20, 71±95.
Charmaz, K. and Olesen, V. (1997) Ethnographic research in medical sociology:
its foci and distinctive contributions, Sociological Methods and Research, 25, 4,452±94.
Cicourel, A. (1992) The interpenetration of communicative contexts: examples from
medical encounters. In Duranti, A. and Goodwin, C. (eds) Rethinking Context:Language as an Interactive Phenomenon. Cambridge: Cambridge University Press.
Cicourel, A. (1995) Medical speech events as resources for inferring differences in
expert-novice diagnostic reasoning. In Quasthoff, U.M. (ed) Aspects of OralCommunication. Berlin: Walter de Gruyter.
Coupland, J., Coupland, N. and Robinson, J.D. (1992) `How are you?': negotiatingphatic communion, Language in Society, 21, 207±30.
Coupland, J., Robinson, J.D. and Coupland, N. (1994) Frame negotiation indoctor±elderly patient consultations, Discourse and Society, 5, 1, 89±124.
DõÂ az, F. (1998) Buenas maneras de dar malas noticias en una consulta de oncologõÂ a.
Paper presented at the V Encuentro Internacional de LinguÈõÂstica en el Noroeste,Hermosillo (Me xico), November 1998.
Drew, P. and Heritage, J. (eds) (1992) Talk at Work: Interaction in Institutional
Settings. Cambridge: Cambridge University Press.Fisher, S. (1984) Institutional authority and the structure of discourse, DiscourseProcesses, 7, 201±24.
Fisher, S. (1983) Doctor talk/patient talk. In Fisher, S. and Todd, A.D. (eds) TheSocial Organization of Doctor±Patient Interaction. Norwood, NJ: Ablex.
Frankel, R. (1983) The laying on of hands. In Fisher, S. and Todd, A.D. (eds) TheSocial Organisation of Doctor±Patient Interaction. Norwood, NJ: Ablex.
Frankel, R. (1984) From sentence to sequence: understanding the medical encounterthrough micro-interactional analysis, Discourse Processes, 7, 135±70.
Frankel, R. (1990) Talking in interviews: a dispreference for patient-initiated
questions. In Psathas, G. (ed) Interactional Competence. New York: Irvington.Heath, C. (1981) The opening sequence in doctor±patient interaction. In Atkin-son, P. and Heath, C. (eds) Medical Work: Realities and Routines. Farnborough:
Gower.Hutchby, I. and Wooffit, R. (1998) Conversation Analysis. Cambridge: Polity Press.Maynard, D. (1991a) Interaction and asymmetry in clinical discourse, AmericanJournal of Sociology, 97, 2, 448±95.
Maynard, D. (1991b) The perspective±display series and the delivery and receipt ofdiagnostic news. In Boden, D. and Zimmerman, D.H. (eds) Talk and SocialStructure. Cambridge: Polity Press.
388 Fe lix Dõ az
# Blackwell Publishers Ltd/Editorial Board 2000
Maynard, D.W. (1992) On clinicians co-implicating recipients' perspective in the
delivery of diagnostic news. In Drew, P. and Heritage, J. (eds) Talk at Work:Interaction in Institutional Settings. Cambridge: Cambridge University Press.
Mishler, E. (1984) The Discourse of Medicine: Dialectics of Medical Interviews.
Norwood, NJ: Ablex.Pilnick, A. (1998) `Why didn't you say just that?' Dealing with issues of asymmetry,knowledge and competence in the pharmacist/client encounter, Sociology of
Health and Illness, 20, 29±51.Sacks, H. (1975) Everyone has to lie. In Blaunt, B. and Sanchez, M. (eds)Sociocultural Dimensions of Language Use. New York: Academic Press.
Sacks, H. (1992) Lectures on Conversation, Volume I. Oxford: Blackwell.
Schegloff, E. (1968) Sequencing in conversational openings, American Anthropolo-gist, 70, 1075±98.
Schegloff, E. (1986) The routine as achievement, Human Studies, 9, 111±51.
Silverman, D. (1987) Communication and Medical Practice: Social Relations in theClinic. London: Sage.
Silverman, D. (1993) Policing the lying patient. In Fisher, S. and Todd, A.D. (eds)
The Social Organisation of Doctor±Patient Interaction. Norwood, NJ: Ablex.Sontag, S. (1979) Illness as Metaphor. New York: Random House.Strong, P.M. (1979) The Ceremonial Order of the Clinic: Parents, Doctors, andMedical Bureaucracies. London: Routledge.
Ten Have, P. (1991) Talk and institution: a reconsideration of the `asymmetry' ofdoctor±patient interaction. In Boden, D. and Zimmerman, D.H. (eds) Talk andSocial Structure. Cambridge: Polity Press.
West, C. (1983) Ask me no questions. In Fisher, S. and Todd, A.D. (eds) The SocialOrganisation of Doctor±Patient Interaction. Norwood, NJ: Ablex.
West, C. (1984) Routine Complications: Trouble with Talk between Doctors and
Patients. Bloomington: Indiana University Press.
The social organisation of chemotherapy treatment consultations 389
# Blackwell Publishers Ltd/Editorial Board 2000
Related Documents











