Journal of Psychosocial Oncology, 27:1–24, 2009 Copyright © Taylor & Francis Group, LLC ISSN: 0734-7332 print / 1540-7586 online DOI: 10.1080/07347330802614634 The Role of Social Support in Families Coping with Childhood Brain Tumor ALUN C. JACKSON, PhD Melbourne Graduate School of Education, Melbourne, Australia; and Centre on Behavioural Health, University of Hong Kong KATE ENDERBY, DPsych Community Group Programs, Mental Health Service, Royal Children’s Hospital, Melbourne, Australia MAREE O’TOOLE, BSW Royal Children’s Hospital, Melbourne, Australia SHANE A. THOMAS, PhD School of Primary Health Care, Monash University, Melbourne, Australia DAVID ASHLEY, MD Children’s Cancer Centre, Royal Children’s Hospital, Melbourne, Australia JEFFREY V. ROSENFELD, MBBS Neurosurgery, the Alfred Hospital, Melbourne, Australia EMMA SIMOS, BSW (Hon) Swinburne University, Melbourne, Australia NICOLE TOKATLIAN, BSW Psychosocial Services, Children’s Cancer Centre, Royal Children’s Hospital, Melbourne, Australia RANEE GEDYE, BSW (Hon) Auckland Starship Hospital, Auckland, New Zealand Primary funding for this study was provided by the Bluey Day Foundation. Additional funding was provided by the Besen Family Trust, Child Cancer Foundation New Zealand, Starship Foundation, and The Alfred Hospital Neurosurgery Department. Emma Simos was formerly affiliated with Social Work Practice Research Unit, University of Melbourne/Royal Children’s Hospital, Melbourne, Australia. Address correspondence to Alun C. Jackson, PhD, Melbourne Graduate School of Edu- cation, University of Melbourne, Parkville, Victoria 3010, Australia. E-mail: aluncj@unimelb. edu.au 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Journal of Psychosocial Oncology, 27:1–24, 2009Copyright © Taylor & Francis Group, LLCISSN: 0734-7332 print / 1540-7586 onlineDOI: 10.1080/07347330802614634
The Role of Social Support in Families Copingwith Childhood Brain Tumor
ALUN C. JACKSON, PhDMelbourne Graduate School of Education, Melbourne, Australia;
and Centre on Behavioural Health, University of Hong Kong
KATE ENDERBY, DPsychCommunity Group Programs, Mental Health Service, Royal Children’s Hospital,
Melbourne, Australia
MAREE O’TOOLE, BSWRoyal Children’s Hospital, Melbourne, Australia
SHANE A. THOMAS, PhDSchool of Primary Health Care, Monash University, Melbourne, Australia
DAVID ASHLEY, MDChildren’s Cancer Centre, Royal Children’s Hospital, Melbourne, Australia
JEFFREY V. ROSENFELD, MBBSNeurosurgery, the Alfred Hospital, Melbourne, Australia
EMMA SIMOS, BSW (Hon)Swinburne University, Melbourne, Australia
NICOLE TOKATLIAN, BSWPsychosocial Services, Children’s Cancer Centre, Royal Children’s Hospital,
Melbourne, Australia
RANEE GEDYE, BSW (Hon)Auckland Starship Hospital, Auckland, New Zealand
Primary funding for this study was provided by the Bluey Day Foundation. Additionalfunding was provided by the Besen Family Trust, Child Cancer Foundation New Zealand,Starship Foundation, and The Alfred Hospital Neurosurgery Department. Emma Simos wasformerly affiliated with Social Work Practice Research Unit, University of Melbourne/RoyalChildren’s Hospital, Melbourne, Australia.
Address correspondence to Alun C. Jackson, PhD, Melbourne Graduate School of Edu-cation, University of Melbourne, Parkville, Victoria 3010, Australia. E-mail: [email protected]
1

2 A. C. Jackson et al.
Previous studies suggest that support from social networks is a pro-tective factor buffering the negative effects of stressful events, suchas having a child with a chronic illness. The literature highlightsthe need for more systematic examination of parents’ social supportnetworks across the disease trajectory, to obtain a more completeunderstanding of how a family’s support system affects adjustmentover time. This was attempted in this study of 88 parents of childrenwith brain tumors, recruited from hospitals in Australia, Singapore,and New Zealand. It employed a longitudinal design, tracking fam-ilies for 2 years postdiagnosis to examine the relationship betweensocial support and coping. As in previous research this study showedthat different types of support are needed at different stages in theillness trajectory. The study also identified the use of various copingstrategies by families, directed at the maintenance and enhance-ment of existing supports and the securing of new supports. Thestudy failed to establish a statistically significant relationship be-tween level of coping and social support, however, suggesting thatparents were using primarily “internal” familial modes of coping,including preexisting patterns of coping, with external social sup-port being an adjunct to their coping rather than being a majorcontributor.
KEYWORDS social support, family coping, pediatric brain tumors
INTRODUCTION
The diagnosis and treatment of a childhood brain tumor has immediateand long-term implications for the child and family. The experiences ofthese families have often been overlooked in childhood cancer research dueto the additional complications of impairments in brain function, differingtreatment regimes, and poor prognosis (Overholser & Fritz, 1990; Phipps &Mulhern, 1995; Radcliffe, Bennett, Kazak, Foley, & Phillips, 1996; Sawyer,Antoniou, Toogood, & Rice, 1997). This is despite the fact that the inci-dence of central nervous system (CNS) tumors (i.e., brain and spinal cordtumors) is second only to leukemia among childhood cancer, accounting forapproximately 20% of all newly diagnosed pediatric malignancies (Mulhern,Hancock, Fairclough, & Kun, 1992).
Aspects of family functioning have only recently been included as vari-ables in the study of behavioral and cognitive outcomes for children withbrain tumors (Carlson-Green, Morris, & Krawiecki, 1995).
Research in the more general area of childhood cancer has shifted froman emphasis on the psychopathology of family functioning to a focus onthe resilience of families in coping with the challenges associated with their
Social Support and Coping with Pediatric Brain Tumor 3
child’s illness (Kazak & Nachman, 1991; Kupst, 1992). It appears that mostfamilies are able to adjust to their child’s illness through the use of variouscoping strategies and supports (Kazak & Nachman, 1991; Kupst, 1992; Kupst& Shulman, 1988; Speechley & Noh, 1992). Certain demographic variablessuch as low socioeconomic status (Kupst et al., 1995; Mulhern, Fairclough,Smith, & Douglas, 1992; Speechley & Noh, 1992), age of parents (Mulhernet al., 1992), and marital status (Mulhern et al., 1992; Speechley & Noh, 1992)appear to affect the adjustment of parents of children with cancer. Familyadjustment has also been related to social support, few concurrent stressors,and use of open communication in the family (Kupst et al., 1995).
Many studies, however, have been restricted by the use of cross-sectional designs that fail to offer insight into how families adapt over timeand the impact of different phases of illness (diagnosis, treatment, longerterm) on family coping and adjustment.
The current study aimed to address some of the oversights of pastresearch by focusing on children with brain tumors, including fathers andmothers, and using the increasingly favored method of a longitudinal orprospective design (Hoekstra-Weebers, Jaspers, Kamps, & Klip, 2001; Kazaket al., 2003; Svavarsdottir, 2005; Wijnberg-Williams, Kamps, Klip, Hoekstra-Weebers, 2006) to examine the relationship between impact, social support,and coping in families having a child with a brain tumor. Previous researchon impact of childhood chronic illness on families and the role of socialsupport in family coping is presented below.
THE IMPACT OF CHILDREN’S CHRONIC ILLNESS ON FAMILIES
Chronic childhood conditions fall along a continuum ranging from those thathave essentially no impact on the child, to those that profoundly affect thechild and family (Newacheck & Taylor, 1992). Several studies have reportedthat the presence of chronic illness places the well-being of the entire familyat risk as the burden of care increases vulnerability to major psychologicaland social disturbances (Hoddap, Dykens, & Masino, 1997; Martin & Nisa,1996; Woods, Haberman, & Packard, 1993), with diagnosis recognised asa particular point of vulnerability (Sloper, 1996; Swallow & Jacoby, 2001).Graetz, Schute, and Sawyer (2000) also noted the range of new familial ad-justment tasks postdiagnosis. Sawyer et al. (1997) went further in identifyingdiagnosis, the commencement of treatment, transition from hospital to home,and relapse as all being potential points of elevated stress, even in familieswho are otherwise coping well, which Sawyer and Spurrier (1996) believe isthe majority of families.
At least four dimensions of the impact of chronic illness on the familyhave been identified in previous studies: financial burden, which is the ex-tent to which the illness changes the economic status of the family; social

4 A. C. Jackson et al.
impact, which is concerned with the quality of interaction with those outsidethe immediate household; familial impact, which is the interaction withinthe family unit including parental and sibling relationships; and subjectivedistress, or the strain experienced by the primary caregiver directly related tothe demands of the illness (Stein & Reissman, 1980). Significant correlationsbetween the four dimensions of impact have been noted (Mailick, Holden,& Walther, 1994). One of the key findings emerging from previous researchis the extent to which the impact of childhood chronic conditions on thefamily is determined by the perception of the illness as a stressor, and bythe cultural context in which it occurs (Zahr, Khoury, & Saoud, 1994).
Social support systems and interactions with the health care systemare of particular importance to the families of chronically ill children, andstudies of the availability and perceived adequacy of support between moth-ers of healthy children and those with chronic illness have indicated that,though there may be no difference in the availability of support, the mothersof chronically ill children reported significantly lower perceived adequacyof support (Hamlett, Pellegrini, & Katz, 1992). Furthermore, the ability offamilies to access relevant services can be restricted by lack of knowledgeand emotional capacity (James, 1991), and whether the parents’ definitionsand expectations of support match those of the service provider (McGee &Burkett, 1998).
SOCIAL SUPPORT AND COPING
A large empirical and clinical literature suggests that social support from so-cial networks is a protective factor that buffers the negative effects of stressfullife events, and enhances physical and emotional well-being (Garwick, Pat-terson, Bennett, & Blum, 1998; Lynam, 1987; Patterson, Garwick, Bennett, &Blum, 1997), while less social support is associated with greater burden incarers (Kim, Duberstein, Sorenson, & Larson, 2005). The illness-buffering ef-fects of social support have most frequently been associated with measuresof perceived social support, as distinct from structural measures of socialties or networks (Speechley & Noh, 1992). It must be noted, however, thatseveral researchers have questioned the use of social support as an explana-tory concept, claiming there to be either a lack of evidence or conflictingfindings, and calling for a better understanding of what aspects of socialrelationships affect adaptation (Lo-Biondo-Wood, Bernier-Henn, & Williams,1992; Noll et al., 1995; Tomlinson & Mitchell, 1992). This includes situationswhere support utilization and meaning may be seen to differ between theparents of a child with cancer (Goldbeck, 2001).
Patterson et al. (1997) explored the definitional issues surrounding socialsupport and it is their definition that was adopted for this study. They defined“social network” as the persons one has contact with who could potentially

Social Support and Coping with Pediatric Brain Tumor 5
provide support. Two distinct types of network group are identified: informalsupports such as family and friends, and formal supports including medicaland allied health professionals, social workers; teachers, and so forh who getpaid for the services they provide (Patterson et al., 1997; Pelletier, Lepage,& Dussault, 1994). Thus, “social network” should be viewed as distinct from“social support” which usually refers to “the subjective sense of receivingsomething from network members” (Patterson et al., 1997). The type ofsupport network members provide may be: emotional—providing trust, em-pathy, and love; instrumental—the provision of practical assistance such asloaning money, giving of time, skills, and so forth; and informational—thegiving of advice; or appraisal, providing evaluative feedback (Pelletier et al.,1994).
Many studies fail to acknowledge the distinction between social net-work and social support and look solely at the existence of a social network,assuming that the presence of network members automatically indicates thatthe person is receiving support (Patterson et al., 1997; Speechley & Noh,1992). Secco and Moffat (1994) also noted that even where such distinctionsare made, there is often a lack of conceptual precision in the way “support”is defined. Network members have not always been found to be supportive(Lynam, 1987; Patterson et al., 1997; Tomlinson & Mitchell, 1992). In theirstudy of supportive and nonsupportive behaviors experienced by parentsof children with a chronic illness, Patterson et al. (1997) found that 78%of mothers and 61% of fathers had experienced at least one nonsupportiveincident from network members. Extended family members were identifiedas the most predominant source of nonsupportive behaviors with a commontheme being the perceived inability or unwillingness of extended family tounderstand the family’s situation (Patterson et al., 1997). Parents highlightedthe tendency for extended family to avoid having contact with, or discus-sions about, the ill child, while others identified problematic communicationpatterns, including unhelpful advice, conflict over the best provision of care,and invasive and inappropriate questioning, with a lack of practical assis-tance also being noted (Patterson et al., 1997). In addition, parents suggestthat some extended family members were themselves so distressed that,they were not only unable to provide any form of support, but also actuallyrequired it themselves.
Within the chronic illness and cancer literature, a number of studies ofparental perceptions of social support have found informal supports to bethe greatest source of emotional and practical support for parents (Florian& Krulik, 1991; Garwick et al., 1998; Molinari & Freeborn, 2006; Pattersonet al., 1997; Pellitier et al., 1994; Sloper, 1996) and children and adolescents(Trask et al., 2003; von Weiss et al., 2002). Patterson et al. (1997), Florian andKrulik (1991), and Pelletier et al. (1994) found spouses/partners to be themost frequently mentioned source of informal support, followed by extendedfamily and friends.

6 A. C. Jackson et al.
There are mixed findings regarding the role of formal supports, as per-ceived by parents of children with cancer and/or chronic conditions. Ina number of studies, service providers have been identified as the ma-jor source of helpful information or support, with physicians and nursesmost frequently named, along with facilitated support groups for parents(Garwick et al., 1998; McGee & Burkett, 1998; Patterson et al., 1997). No-tably, in the Pelletier et al. (1994) study, mothers identified professionalsin the top three sources of perceived support, alongside immediate familymembers and spouses. Furthermore, when social supports were not meetingtheir needs, mothers identified professionals as the first source of supportfrom which help was wanted. The findings of Pelletier et al. (1994) divergefrom those of Florian and Krulik (1991) who observed that there was anabsence of formal support, from medical and allied health and mental healthprofessionals, in the networks of parents of chronically ill children. However,Pelletier et al. (1994) noted that the fact that the participants in their studywere interviewed as they came in for an outpatient clinic appointment, mayhave inflated their rating of the importance of health care professionals as asource of support.
Morrow, Hoagland, and Morse (1981) discovered a significant associa-tion between the amount of parental contact, and the degree of perceivedhelpfulness. Although parents failed to identify allied health and mentalhealth professionals as an important source of support in their existing net-works, exploration of unmet need in a number of studies has revealed coun-selling to be one of the most desired supports identified by parents (Morrowet al., 1981; Sloper, 1996). Thus, it may be suggested that a low level ofperceived support from allied health and mental health professionals couldbe a product of unmet need, rather than of the quality of support provided.
Interestingly, the relative emphasis parents placed on particular types ofsupport from specific sources was reflected in the emphasis they placed onnonsupportive behaviors, suggesting that parents have certain expectationsregarding the types of support they should receive from specific sources. Asnoted above, the absence of emotional support and inadequate practical helpwere common problems attributed to family members, whereas inadequateand insufficient information was highlighted as the greatest area of nonsup-port from service providers (Garwick et al., 1998; Patterson et al., 1997).
Tomlinson and Mitchell (1992) contend that the type and amount ofsupport most useful in an immediate crisis, such as at the point of diagnosisor relapse, may not be what is most useful at other stages in the disease tra-jectory. Consequently, available support or the form support takes may varyover time. Tomlinson and Mitchell (1992, p. 388) contend that “social supportchanges over time, influences different aspects of the crisis experience andcan have both direct and indirect influence on certain forms of adjustment.”This was not reflected in the findings of Morrow et al. (1981) who failed tofind differences in patterns of social support among parents with children at
Social Support and Coping with Pediatric Brain Tumor 7
different stages of treatment. Morrow’s study was, however, a cross-sectionaldesign encompassing parents of children at various stages of the illness, andas such, did not systematically follow families across the disease trajectory(Morrow et al., 1981). Similar findings were also evident in the Garwicket al. (1998) study, in which perceived social support stayed relatively con-stant across the two interviews, with the exception of fathers’ perceptionsof emotional support from family members, which was significantly higher.The subjects of this study were, however, parents of preadolescents (aged8–11 years), the majority of whom had been living with a chronic illness ordisability for several years. Hence, the subjects had had a significant periodof time to adjust to the illness of their child.
Patterson et al. (1997) found that parents’ perceptions of the amountof support received increased significantly 12 months following the firstinterview. Mothers reported an increase in emotional support from family andinformal community support, whereas fathers reported a significant increasein emotional and practical help from informal community supports. Theysuggest that this perceived increase in support may reflect a change in theratio of the perceived need for support.
A later study of the temporal need for social support for parents was re-ported by Hoekstra-Weebers et al. (2001) utilizing a longitudinal design, withthe Social Support List Interactions (SSL-I) and Discrepancies (SSL-D) usedto measure social support. Parents in this study reported a diminishing in theamount of support received over time, after the high levels of “crisis support”at diagnosis. Fathers reported more negative interactions related to support,most likely related to perceived lack of support in their workplaces, andnegative experiences of support for fathers was associated with higher levelsof distress over time. Overall, this study confirmed the usefulness of distin-guishing clearly between amount, type, and perceived usefulness of support.
The existing literature highlights the need for a more systematic ex-amination of parents’ social support networks across the disease trajectory,to obtain a more complete gauge of how a family’s support system affectscoping and adjustment overtime. This was attempted in the current studythrough the prospective design.
CONCEPTUAL FRAMEWORK FOR THE STUDY
The conceptual framework for the study was guided by the Resiliency Modelof Family Stress, Adjustment and Adaptation developed by McCubbin andMcCubbin (1996), a model that had emerged from numerous studies of fam-ilies of different backgrounds, cultures, and experiences, including studiesof families faced with chronic stress and illness.
The model is based on five fundamental assumptions about family life:(1) families face hardships and changes as a natural part of family life;

8 A. C. Jackson et al.
(2) families develop basic competencies, patterns of functioning, and capa-bilities designed to foster the growth and development of family membersand to protect the family from major disruptions in the face of change; (3)families develop basic and unique competencies, patterns of functioning,and capabilities designed to protect the family from unexpected stressorsand to foster the family’s recovery following a family crisis or major transi-tion; (4) families draw from the network of relationships and resources in thecommunity, including its ethnicity and cultural heritage, particularly duringperiods of family stress and crises; and (5) families faced with crisis situa-tions demanding changes in the family’s functioning work to restore order,harmony, and balance even in the midst of change (McCubbin, Thompson,& McCubbin, 1996).
METHODS
As noted, this was a prospective study involving a within-group design withrepeated measures over time. Participants in the study were involved ina questionnaire interview at four different points in time: (1) at diagnosis;(2) 6 months postdiagnosis; (3) 12 months postdiagnosis; and (4) 2 yearspostdiagnosis. The first occasion involved a face-to-face interview conductedat the hospital. Participants were then given the choice of a face-to-faceinterview or a telephone interview for the following three testing occasions.The questionnaire took between 45 minutes and 11
2 hours to complete andincluded multiple choice questions, and a small number of short answerquestions. The Norbeck Social Support Questionnaire (see below) was sentto participants to be completed at home and mailed to the research team,as it contained a series of half pages that had to be visually aligned in orderto complete the questions. A slight change to the method of completionof this instrument, following poor initial returns and consultation with theparent participants who had experienced difficulty with the questionnaire,involved a member of the research team assisting parents to complete thequestionnaire over the phone.
In terms of the effectiveness of telephone interviewing in this type ofresearch, there have been numerous studies since the late 1960s comparingthe difference between various modes of data collection. Most studies so farhave indicated that there are few major differences in the quality of infor-mation between telephone and face-to-face/household interviews in surveyresearch (Fenig, Levav, Kohn, & Yelin, 1993; Rohde, Lewinsohn, & Selley,1997; Weeks, Kulka, Lessler, & Whitmore, 1983), and that telephone inter-views are equivalent to face-to-face interviews in terms of validity, reliability,precision of estimates, and response rates (Paulsen, Crowe, Noyes, & Pfohl,1988; Slutske et al., 1998), and in their capacity to elicit qualitative data(Sweet, 2002). In the current study, the research team judged that the qualityof response in the telephone interviews was no less than for the face-to-face

Social Support and Coping with Pediatric Brain Tumor 9
interviews, and exceeded them in effective completion of the Norbeck SocialSupport Questionnaire.
Measures Used in the Study
Variables described in the Resiliency model and the instruments used tomeasure them included:
Concept Measure
Family resources Norbeck Social Support Questionnaire (NSSQ)Specific Support Grid
Problem solving and coping Coping Health Inventory for Parents (CHIP)Family bonadjustment,
maladjustmentFamily Adaptability and Cohesion Evaluation and Crises Scale
(FACES 11)
The Norbeck Social Support Questionnaire (NSSQ; Norbeck, 1995), oneof the two measures of support used for this study, is a 9-item self-reportmeasure designed to capture the multiple dimensions of social support.Scores are given for “total functional support,” comprising emotional andtangible support; and for “total network.” Reported test-retest reliability at1 week ranged from .85–.92 (Norbeck, Lindsey, & Carrieri, 1983). Reportedconcurrent validity testing with the Personal Resource Questionnaire showedmoderate intercorrelations with the NSSQ (p <.01) (Norbeck et al., 1983).
In addition to completing the NSSQ, participants were provided witha list of social support services and asked to indicate which services theyhad accessed throughout the time since their child was diagnosed. Thisinstrument, the Specific Support Grid (SSG), was specifically designed forthis study by members of the study team (O’Toole & Enderby).
Family coping was measured with the Coping Health Inventory forParents (CHIP), a 45-item measure developed to assess parents’ appraisal oftheir coping responses to the management of family life when they have achild member who is seriously and/or chronically ill (McCubbin, McCubbin,Nevin, & Cauble, 1981). The CHIP is a self-report measure consisting of achecklist of 45 specific behaviors. Parents are asked to record how helpful(on a scale of 0–3), each behavior was in their particular family situation.
1. Coping Pattern 1: Family integration, cooperation, and an optimistic defi-nition of the situation. These items focus on strengthening family life andrelationships, and the parents’ outlook on life with an ill child.
2. Coping Pattern 2: Maintaining social support, self-esteem, and psycholog-ical stability. These 18 items involve parents’ efforts to develop relation-ships with others, engage in activities which enhance feelings of individualidentity and self-worth, plus behaviors to manage psychological pressuresand tensions.

10 A. C. Jackson et al.
3. Coping Pattern 3: Understanding the health care situation through com-munication with other parents and consultation with the health careteam. This subscale consists of eight behaviors directed at the parents’relationships with health care professionals and other parents of chron-ically ill children. These behaviors include developing more knowledgeand understanding of the illness, and mastering any homecare treatmentsand prescribed medical regimens.
Cronbach’s alpha reliabilities for the three coping patterns are .79, .79,and .71, respectively (McCubbin & McCubbin, 1996).
Adaptability and cohesion were measured using the Family Adaptabilityand Cohesion Evaluation Scale (FACES II), a 30-item self-report measure de-veloped to measure two critical family constructs: adaptability (14 items) andcohesion (16 items) (Olson, Portner, & Bell, 1982). The scale was developedas a revision of the original FACES scale to provide a shorter instrument, toreduce the number of double negative items and to include a 5-point Likert-type scale (almost never to almost always). Two items address each of thefollowing dimensions of cohesion: emotional bonding, family boundaries,coalitions, time, space, friends, decision making, interests, and recreation.Items measuring cohesion include “family members feel very close to eachother” and “family members like to spend free time together.” Two to threeitems measure each of the following dimensions of adaptability: assertive-ness, leadership, discipline, negotiations, roles, and rules. Family adaptabilityitems include “it is difficult to get a rule changed in our family” and “familymembers discuss problems and feel good about solutions.” Cronbach’s alphareliabilities for the cohesion subscale, adaptability subscale, and total scaleare .87, .78, and .90, respectively.
Demographic and severity of illness information (as rated by medicalstaff) on parents and children was collected, and included name, age, sex,place of birth, and residential status. Specific details from parents includedsocioeconomic status, occupation, education level, number of dependents,marital status, ethnic background, and involvement in a religious/spiritualorganization.
Qualitative Data
Two open-ended questions were also included in the questionnaire, in thebelief that such qualitative information would enrich the data and validatethe quantitative findings (Frank-Stromborg & Olsen, 1997):
• How has your experience with the hospital been so far?• Is there anything else you would like to tell us about your family’s expe-
riences since your child was diagnosed with a brain tumor?

Social Support and Coping with Pediatric Brain Tumor 11
Qualitative data derived from semistructured interviews conductedwith every fifth respondent instead of survey questionnaires, and the twoopen-ended questions asked of all respondents were formed into cate-gories and analyzed thematically using a sociological perspective combin-ing narrative and thematic analysis. The data were also interpreted usingan anthropological perspective in that the analysis aimed primarily to re-main faithful to the respondents’ view and information provided to the re-searchers. This was achieved by keeping responses in context with regardto meaning and terms of expression (i.e., concepts and language used byrespondents).
The semistructured interviews were undertaken primarily to provide ameans of comparison with how parents conceptualized the key elements ofthe study, such as coping, with how these elements were conceptualizedin the instruments selected to measure them. This will be the subject of afurther analysis.
Following analysis of the quantitative and the qualitative data, an im-portant additional element of the treatment of the data was introduced. Thisinvolved “work shopping” the data with the oncology social work team atthe Royal Children’s Hospital, to determine the extent to which the data de-rived from the theory-driven measures reflected their clinical experience ofthe psycho-social impacts of childhood brain tumors on families.
Participant Population
Participants were enrolled into the study during initial hospital admission forinvestigation and diagnosis of a brain tumor in their child, between 2001 and2002, with the study having been granted approval from the Royal Children’sHospital Human Research Ethics Committee on April 27, 2000 (approvalnumber 99125A). Mothers and fathers were invited to participate, andparticipants whose child died during the 3-year study, on the advice of theChild Brain Tumour Association, a parent association, who were consultedon the study design, were to be offered the opportunity to remain in thestudy.
Eighty-eight parents were recruited into the study at six participatinghospitals: Royal Children’s Hospital, Melbourne (N = 53); the Women’s andChildren’s Hospital, Adelaide (N = 6); Princess Margaret Hospital, Perth(N = 7); KK Women’s and Children’s Hospital, Singapore (N = 7); andAuckland Starship Hospital (N = 15). The children comprised 50 girls and38 boys with a mean age of seven years (age range 2 months to 16 years11 months).
The following tumor types were represented in the study population.These figures relate to the Royal Children’s Hospital sample (N = 31) onlybut are representative of the study population.

12 A. C. Jackson et al.
Tumor type No. %
Pilocytic astrocytoma grd 1 13 42Medulloblastoma 5 16Pontine Glioma 3 10Germinoma 2 6.5GBM 2 6.5Anaplastic astrocytoma 1 3PNET 1 3Choroid Plexus Papilloma 1 3Immature teratoma 1 3Pituitary tumor 1 3Ependymoma 1 3
GBM = Glioblastoma multiforme; PNET = Primitive neuroectodermal tumor
RESULTS
Respondents
Of the parents participating in the study, 53 were mothers, whereas 35 werefathers. Of these parents, 17% were aged between 21 and 30; 51.1% wereaged between 31 and 40, while 26.1% were aged between 41 and 50. Ageswere not provided by 5.7% of parents. Eighty-eight parents started the study,of whom 83 completed the NSSQ at some point in the study.
Types of Support Received
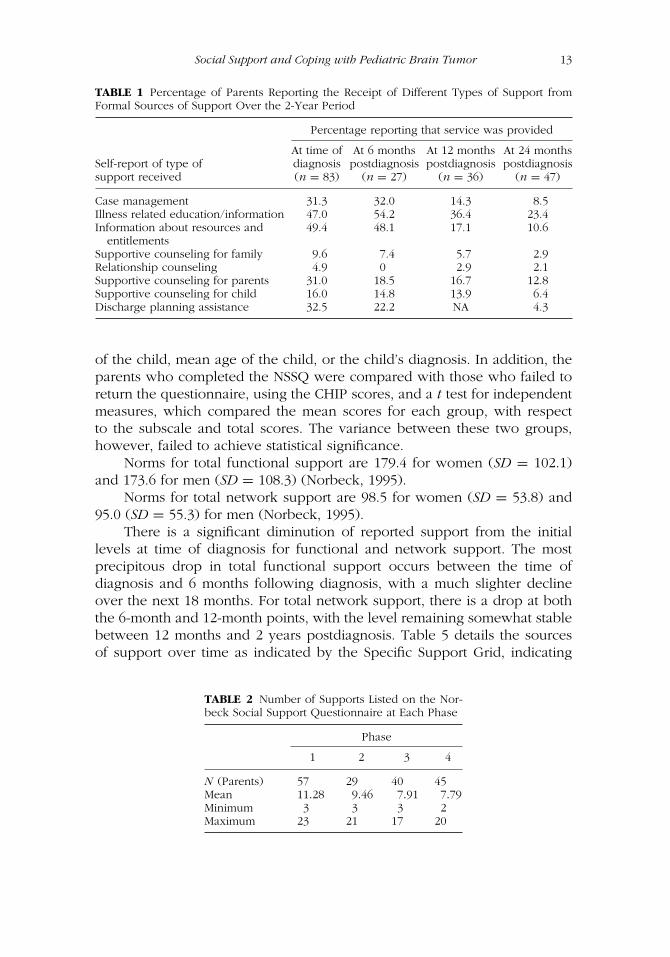
Using the Specific Support Grid, comparison of type of support (as reportedby parents) at diagnosis and up to 2 years postdiagnosis, shows persistencein the use of all three forms of support—informational, emotional andtangible—although there is an expected decline in all forms of supportused, but a persisting need for informational support over the 2 year period(Table 1).
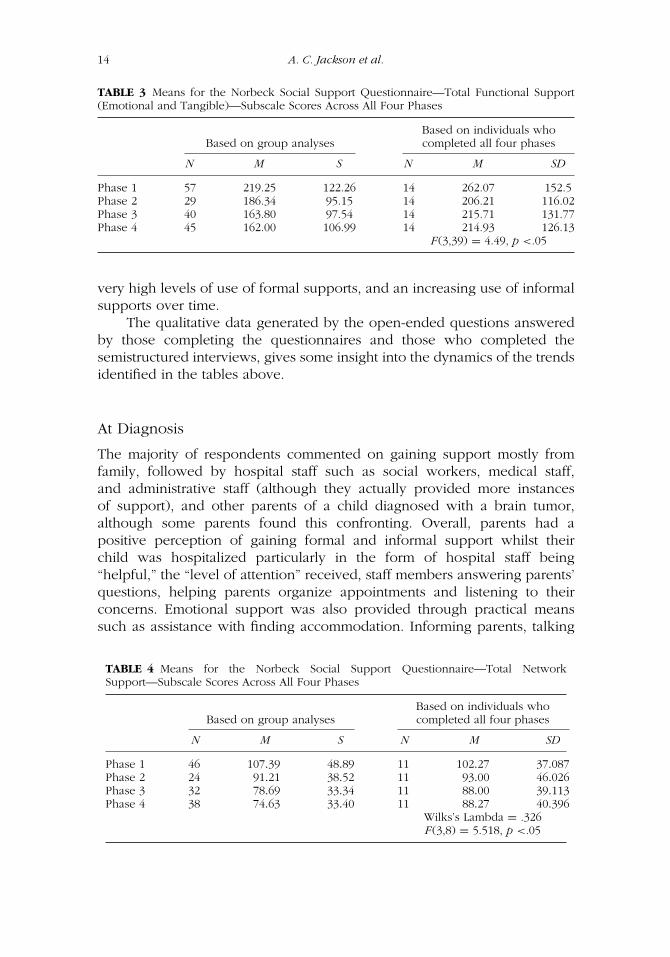
Table 2 details the number of supports, as measured by the NSSQ, andTables 3 and 4 detail the means of the NSSQ across the four phases. As Table3 shows, although between 29 and 57 parents completed the NSSQ at eachphase of the study, only 14 parents completed the NSSQ at all four phases.
A comparative assessment was undertaken to ascertain whether theparents who returned the social support measures could be considered rep-resentative of participants in the larger study. Those who returned the NSSQwere compared with those who either failed to return the survey, or thosewho participated in the semistructured interviews and who did not completethe NSSQ. This comparison, considering various demographic variables, wasconducted using a chi-square test for independence. No statistically signifi-cant differences were found between the two groups with respect to the sexor age of parents; their educational levels and religious affiliation, the sex
Social Support and Coping with Pediatric Brain Tumor 13
TABLE 1 Percentage of Parents Reporting the Receipt of Different Types of Support fromFormal Sources of Support Over the 2-Year Period
Percentage reporting that service was provided
At time of At 6 months At 12 months At 24 monthsSelf-report of type of diagnosis postdiagnosis postdiagnosis postdiagnosissupport received (n = 83) (n = 27) (n = 36) (n = 47)
Case management 31.3 32.0 14.3 8.5Illness related education/information 47.0 54.2 36.4 23.4Information about resources and 49.4 48.1 17.1 10.6
entitlementsSupportive counseling for family 9.6 7.4 5.7 2.9Relationship counseling 4.9 0 2.9 2.1Supportive counseling for parents 31.0 18.5 16.7 12.8Supportive counseling for child 16.0 14.8 13.9 6.4Discharge planning assistance 32.5 22.2 NA 4.3
of the child, mean age of the child, or the child’s diagnosis. In addition, theparents who completed the NSSQ were compared with those who failed toreturn the questionnaire, using the CHIP scores, and a t test for independentmeasures, which compared the mean scores for each group, with respectto the subscale and total scores. The variance between these two groups,however, failed to achieve statistical significance.
Norms for total functional support are 179.4 for women (SD = 102.1)and 173.6 for men (SD = 108.3) (Norbeck, 1995).
Norms for total network support are 98.5 for women (SD = 53.8) and95.0 (SD = 55.3) for men (Norbeck, 1995).
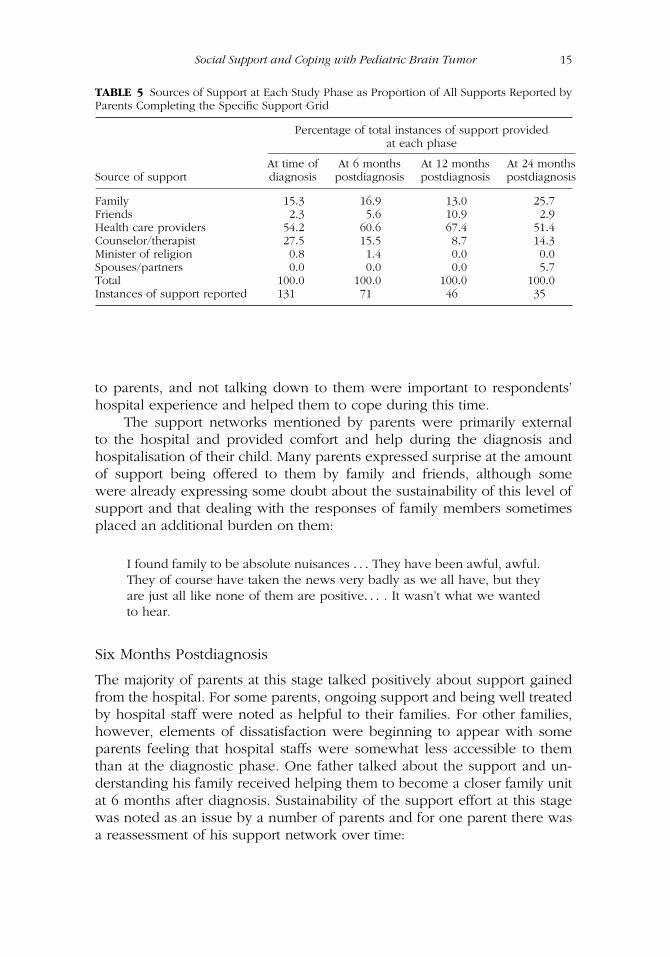
There is a significant diminution of reported support from the initiallevels at time of diagnosis for functional and network support. The mostprecipitous drop in total functional support occurs between the time ofdiagnosis and 6 months following diagnosis, with a much slighter declineover the next 18 months. For total network support, there is a drop at boththe 6-month and 12-month points, with the level remaining somewhat stablebetween 12 months and 2 years postdiagnosis. Table 5 details the sourcesof support over time as indicated by the Specific Support Grid, indicating
TABLE 2 Number of Supports Listed on the Nor-beck Social Support Questionnaire at Each Phase
Phase
1 2 3 4
N (Parents) 57 29 40 45Mean 11.28 9.46 7.91 7.79Minimum 3 3 3 2Maximum 23 21 17 20
14 A. C. Jackson et al.
TABLE 3 Means for the Norbeck Social Support Questionnaire—Total Functional Support(Emotional and Tangible)—Subscale Scores Across All Four Phases
Based on group analysesBased on individuals whocompleted all four phases
N M S N M SD
Phase 1 57 219.25 122.26 14 262.07 152.5Phase 2 29 186.34 95.15 14 206.21 116.02Phase 3 40 163.80 97.54 14 215.71 131.77Phase 4 45 162.00 106.99 14 214.93 126.13
F(3,39) = 4.49, p <.05
very high levels of use of formal supports, and an increasing use of informalsupports over time.
The qualitative data generated by the open-ended questions answeredby those completing the questionnaires and those who completed thesemistructured interviews, gives some insight into the dynamics of the trendsidentified in the tables above.
At Diagnosis
The majority of respondents commented on gaining support mostly fromfamily, followed by hospital staff such as social workers, medical staff,and administrative staff (although they actually provided more instancesof support), and other parents of a child diagnosed with a brain tumor,although some parents found this confronting. Overall, parents had apositive perception of gaining formal and informal support whilst theirchild was hospitalized particularly in the form of hospital staff being“helpful,” the “level of attention” received, staff members answering parents’questions, helping parents organize appointments and listening to theirconcerns. Emotional support was also provided through practical meanssuch as assistance with finding accommodation. Informing parents, talking
TABLE 4 Means for the Norbeck Social Support Questionnaire—Total NetworkSupport—Subscale Scores Across All Four Phases
Based on group analysesBased on individuals whocompleted all four phases
N M S N M SD
Phase 1 46 107.39 48.89 11 102.27 37.087Phase 2 24 91.21 38.52 11 93.00 46.026Phase 3 32 78.69 33.34 11 88.00 39.113Phase 4 38 74.63 33.40 11 88.27 40.396
Wilks’s Lambda = .326F(3,8) = 5.518, p <.05
Social Support and Coping with Pediatric Brain Tumor 15
TABLE 5 Sources of Support at Each Study Phase as Proportion of All Supports Reported byParents Completing the Specific Support Grid
Percentage of total instances of support providedat each phase
At time of At 6 months At 12 months At 24 monthsSource of support diagnosis postdiagnosis postdiagnosis postdiagnosis
Family 15.3 16.9 13.0 25.7Friends 2.3 5.6 10.9 2.9Health care providers 54.2 60.6 67.4 51.4Counselor/therapist 27.5 15.5 8.7 14.3Minister of religion 0.8 1.4 0.0 0.0Spouses/partners 0.0 0.0 0.0 5.7Total 100.0 100.0 100.0 100.0Instances of support reported 131 71 46 35
to parents, and not talking down to them were important to respondents’hospital experience and helped them to cope during this time.
The support networks mentioned by parents were primarily externalto the hospital and provided comfort and help during the diagnosis andhospitalisation of their child. Many parents expressed surprise at the amountof support being offered to them by family and friends, although somewere already expressing some doubt about the sustainability of this level ofsupport and that dealing with the responses of family members sometimesplaced an additional burden on them:
I found family to be absolute nuisances . . . They have been awful, awful.They of course have taken the news very badly as we all have, but theyare just all like none of them are positive. . . . It wasn’t what we wantedto hear.
Six Months Postdiagnosis
The majority of parents at this stage talked positively about support gainedfrom the hospital. For some parents, ongoing support and being well treatedby hospital staff were noted as helpful to their families. For other families,however, elements of dissatisfaction were beginning to appear with someparents feeling that hospital staffs were somewhat less accessible to themthan at the diagnostic phase. One father talked about the support and un-derstanding his family received helping them to become a closer family unitat 6 months after diagnosis. Sustainability of the support effort at this stagewas noted as an issue by a number of parents and for one parent there wasa reassessment of his support network over time:
16 A. C. Jackson et al.
You learn who your friends are. It’s interesting watching people’s reac-tions. Some people stopped contacting us. We’ve been lucky with thesupport we’ve been given.
Twelve Months Postdiagnosis
Discussion of the support respondents received from the hospital at12 months postdiagnosis showed that many respondents were positive,particularly about the continuity of support and reliability. The continuity ofcompassion and support was noted as reassuring for one father, although,again, it should be noted that there was an increase in complaints regardingother aspects of the hospital, such as communication with some medicalstaff, lack of coordination of appointments, waiting times, and inadequateresources. One mother linked her child’s positive prognosis with less needto talk with others.
We didn’t go to any of the other parent groups. We had a good prognosis.We didn’t want to hear or tell. We didn’t need that.
Twenty-Four Months Postdiagnosis
Many families at this stage are facing the physical and psycho-social long-term effects of their child’s brain tumor. Two families noted the importanceof practical support through a philanthropic trust to finance, for example,a tutor for a child with cognitive impairment. For one mother, there was aloss of friends to contend with, as they were not able to provide the type ofsupport needed:
I have lost friends over the time and that was very difficult at the timewith everything I felt I had to cope with that I was losing friends as well.And also just because I felt that I had to—and I did have to—explainand hold my ground with what was going on in my life and just somuch happening with dealing and coping with what had happened to(daughter) and the ups and downs of your marriage and then, of course,all the other relationships in your life so things have crumbled.
For another mother with no extended family support, the role of formalsupport gained more significance:
It’s a part of my personality change, I have had to be very strong and justsimply get people to, for want of a better word, perhaps leave me to domy mothering and lean very much on my GP and the Maternal Healthand Child Nurse.
Social Support and Coping with Pediatric Brain Tumor 17
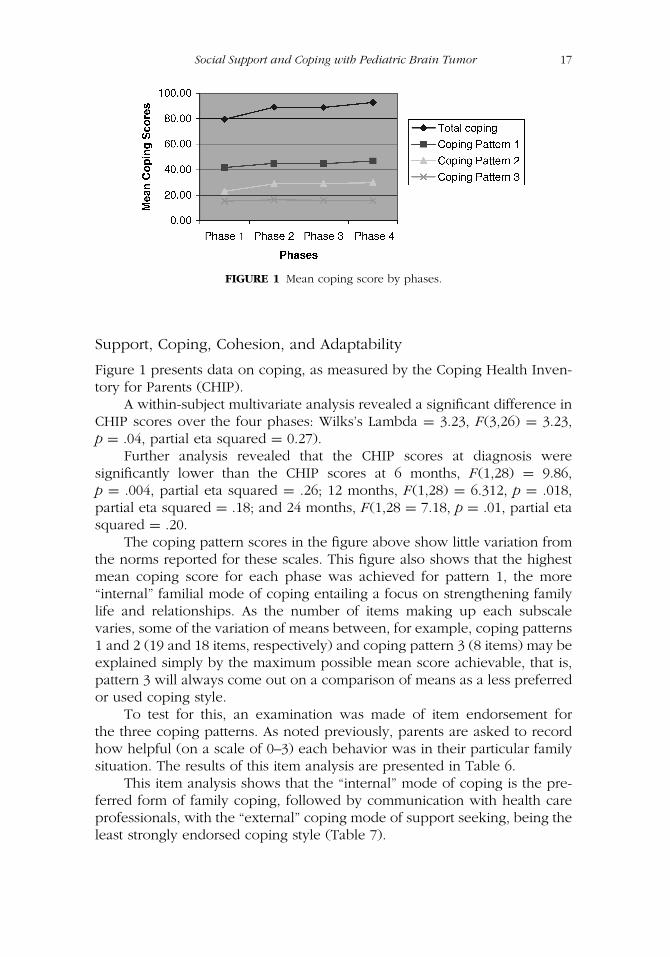
FIGURE 1 Mean coping score by phases.
Support, Coping, Cohesion, and Adaptability
Figure 1 presents data on coping, as measured by the Coping Health Inven-tory for Parents (CHIP).
A within-subject multivariate analysis revealed a significant difference inCHIP scores over the four phases: Wilks’s Lambda = 3.23, F(3,26) = 3.23,p = .04, partial eta squared = 0.27).
Further analysis revealed that the CHIP scores at diagnosis weresignificantly lower than the CHIP scores at 6 months, F(1,28) = 9.86,p = .004, partial eta squared = .26; 12 months, F(1,28) = 6.312, p = .018,partial eta squared = .18; and 24 months, F(1,28 = 7.18, p = .01, partial etasquared = .20.
The coping pattern scores in the figure above show little variation fromthe norms reported for these scales. This figure also shows that the highestmean coping score for each phase was achieved for pattern 1, the more“internal” familial mode of coping entailing a focus on strengthening familylife and relationships. As the number of items making up each subscalevaries, some of the variation of means between, for example, coping patterns1 and 2 (19 and 18 items, respectively) and coping pattern 3 (8 items) may beexplained simply by the maximum possible mean score achievable, that is,pattern 3 will always come out on a comparison of means as a less preferredor used coping style.
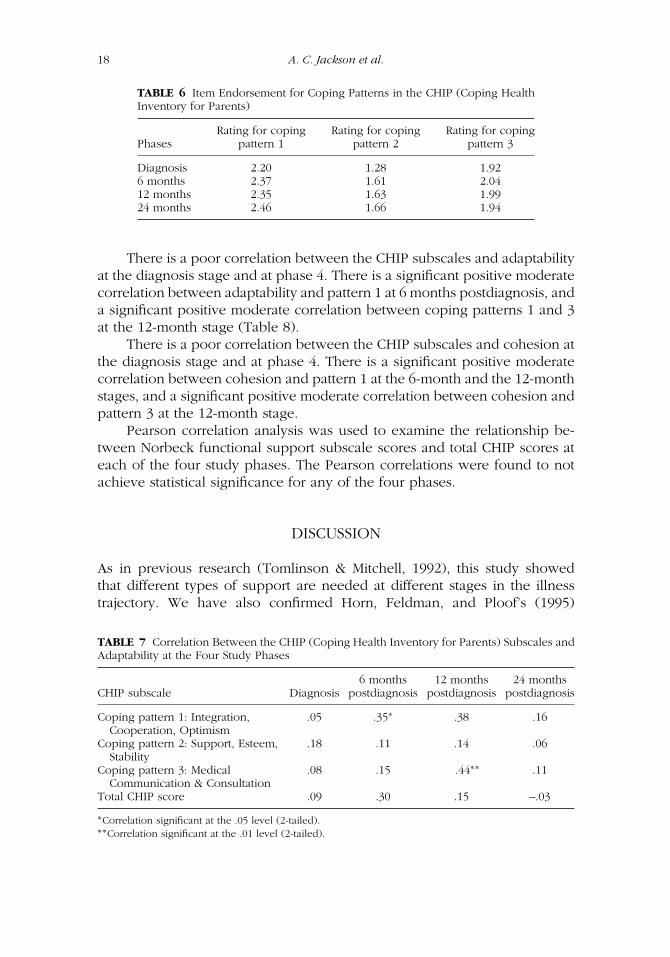
To test for this, an examination was made of item endorsement forthe three coping patterns. As noted previously, parents are asked to recordhow helpful (on a scale of 0–3) each behavior was in their particular familysituation. The results of this item analysis are presented in Table 6.
This item analysis shows that the “internal” mode of coping is the pre-ferred form of family coping, followed by communication with health careprofessionals, with the “external” coping mode of support seeking, being theleast strongly endorsed coping style (Table 7).
18 A. C. Jackson et al.
TABLE 6 Item Endorsement for Coping Patterns in the CHIP (Coping HealthInventory for Parents)
Rating for coping Rating for coping Rating for copingPhases pattern 1 pattern 2 pattern 3
Diagnosis 2.20 1.28 1.926 months 2.37 1.61 2.0412 months 2.35 1.63 1.9924 months 2.46 1.66 1.94
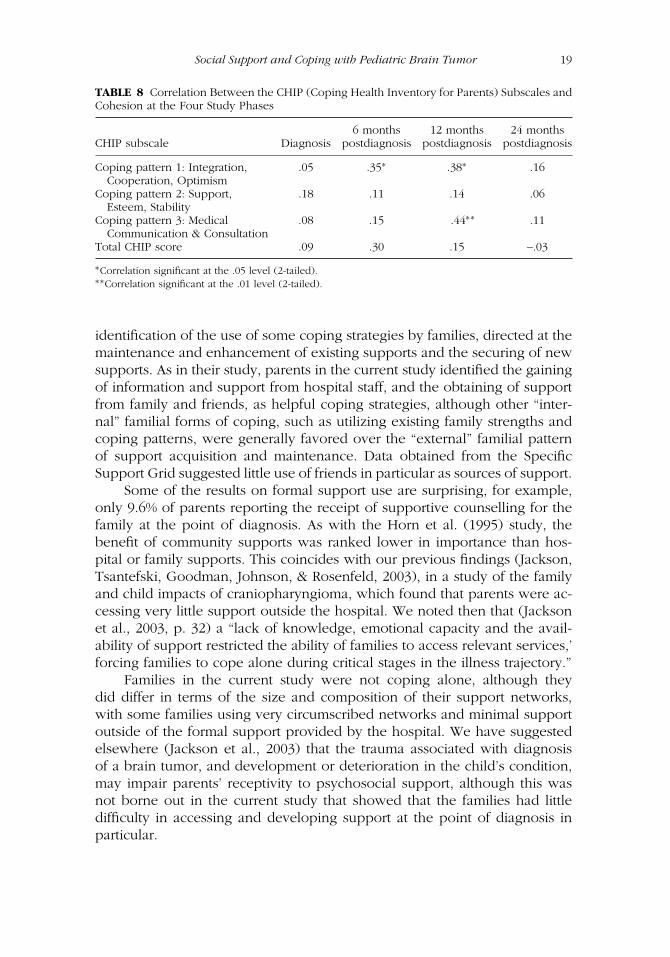
There is a poor correlation between the CHIP subscales and adaptabilityat the diagnosis stage and at phase 4. There is a significant positive moderatecorrelation between adaptability and pattern 1 at 6 months postdiagnosis, anda significant positive moderate correlation between coping patterns 1 and 3at the 12-month stage (Table 8).
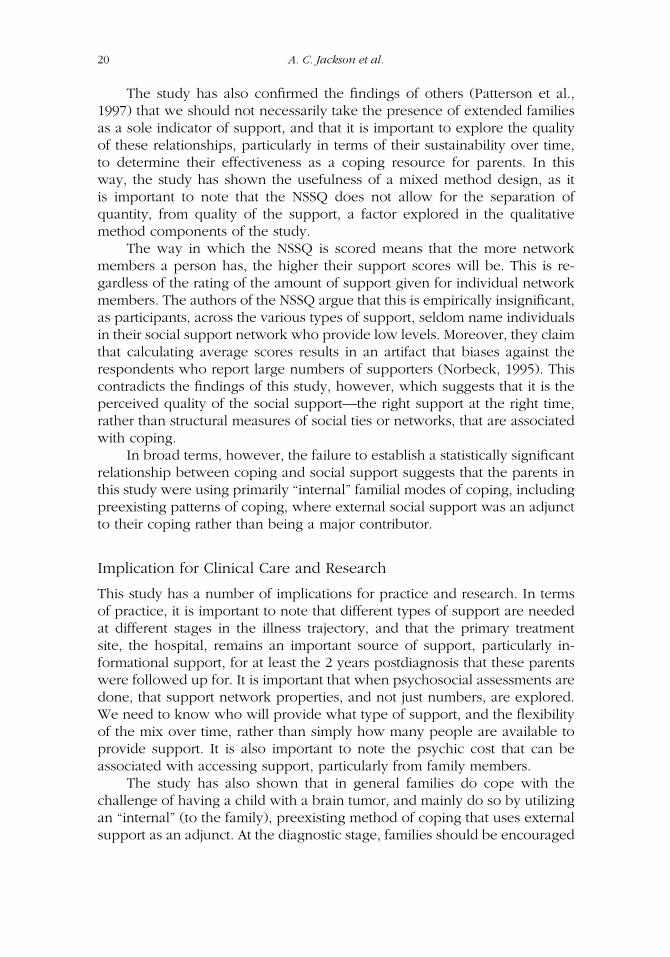
There is a poor correlation between the CHIP subscales and cohesion atthe diagnosis stage and at phase 4. There is a significant positive moderatecorrelation between cohesion and pattern 1 at the 6-month and the 12-monthstages, and a significant positive moderate correlation between cohesion andpattern 3 at the 12-month stage.
Pearson correlation analysis was used to examine the relationship be-tween Norbeck functional support subscale scores and total CHIP scores ateach of the four study phases. The Pearson correlations were found to notachieve statistical significance for any of the four phases.
DISCUSSION
As in previous research (Tomlinson & Mitchell, 1992), this study showedthat different types of support are needed at different stages in the illnesstrajectory. We have also confirmed Horn, Feldman, and Ploof’s (1995)
TABLE 7 Correlation Between the CHIP (Coping Health Inventory for Parents) Subscales andAdaptability at the Four Study Phases
6 months 12 months 24 monthsCHIP subscale Diagnosis postdiagnosis postdiagnosis postdiagnosis
Coping pattern 1: Integration,Cooperation, Optimism
.05 .35∗ .38 .16
Coping pattern 2: Support, Esteem,Stability
.18 .11 .14 .06
Coping pattern 3: MedicalCommunication & Consultation
.08 .15 .44∗∗ .11
Total CHIP score .09 .30 .15 –.03
∗Correlation significant at the .05 level (2-tailed).∗∗Correlation significant at the .01 level (2-tailed).
Social Support and Coping with Pediatric Brain Tumor 19
TABLE 8 Correlation Between the CHIP (Coping Health Inventory for Parents) Subscales andCohesion at the Four Study Phases
6 months 12 months 24 monthsCHIP subscale Diagnosis postdiagnosis postdiagnosis postdiagnosis
Coping pattern 1: Integration,Cooperation, Optimism
.05 .35∗ .38∗ .16
Coping pattern 2: Support,Esteem, Stability
.18 .11 .14 .06
Coping pattern 3: MedicalCommunication & Consultation
.08 .15 .44∗∗ .11
Total CHIP score .09 .30 .15 –.03
∗Correlation significant at the .05 level (2-tailed).∗∗Correlation significant at the .01 level (2-tailed).
identification of the use of some coping strategies by families, directed at themaintenance and enhancement of existing supports and the securing of newsupports. As in their study, parents in the current study identified the gainingof information and support from hospital staff, and the obtaining of supportfrom family and friends, as helpful coping strategies, although other “inter-nal” familial forms of coping, such as utilizing existing family strengths andcoping patterns, were generally favored over the “external” familial patternof support acquisition and maintenance. Data obtained from the SpecificSupport Grid suggested little use of friends in particular as sources of support.
Some of the results on formal support use are surprising, for example,only 9.6% of parents reporting the receipt of supportive counselling for thefamily at the point of diagnosis. As with the Horn et al. (1995) study, thebenefit of community supports was ranked lower in importance than hos-pital or family supports. This coincides with our previous findings (Jackson,Tsantefski, Goodman, Johnson, & Rosenfeld, 2003), in a study of the familyand child impacts of craniopharyngioma, which found that parents were ac-cessing very little support outside the hospital. We noted then that (Jacksonet al., 2003, p. 32) a “lack of knowledge, emotional capacity and the avail-ability of support restricted the ability of families to access relevant services,’forcing families to cope alone during critical stages in the illness trajectory.”
Families in the current study were not coping alone, although theydid differ in terms of the size and composition of their support networks,with some families using very circumscribed networks and minimal supportoutside of the formal support provided by the hospital. We have suggestedelsewhere (Jackson et al., 2003) that the trauma associated with diagnosisof a brain tumor, and development or deterioration in the child’s condition,may impair parents’ receptivity to psychosocial support, although this wasnot borne out in the current study that showed that the families had littledifficulty in accessing and developing support at the point of diagnosis inparticular.
20 A. C. Jackson et al.
The study has also confirmed the findings of others (Patterson et al.,1997) that we should not necessarily take the presence of extended familiesas a sole indicator of support, and that it is important to explore the qualityof these relationships, particularly in terms of their sustainability over time,to determine their effectiveness as a coping resource for parents. In thisway, the study has shown the usefulness of a mixed method design, as itis important to note that the NSSQ does not allow for the separation ofquantity, from quality of the support, a factor explored in the qualitativemethod components of the study.
The way in which the NSSQ is scored means that the more networkmembers a person has, the higher their support scores will be. This is re-gardless of the rating of the amount of support given for individual networkmembers. The authors of the NSSQ argue that this is empirically insignificant,as participants, across the various types of support, seldom name individualsin their social support network who provide low levels. Moreover, they claimthat calculating average scores results in an artifact that biases against therespondents who report large numbers of supporters (Norbeck, 1995). Thiscontradicts the findings of this study, however, which suggests that it is theperceived quality of the social support—the right support at the right time,rather than structural measures of social ties or networks, that are associatedwith coping.
In broad terms, however, the failure to establish a statistically significantrelationship between coping and social support suggests that the parents inthis study were using primarily “internal” familial modes of coping, includingpreexisting patterns of coping, where external social support was an adjunctto their coping rather than being a major contributor.
Implication for Clinical Care and Research
This study has a number of implications for practice and research. In termsof practice, it is important to note that different types of support are neededat different stages in the illness trajectory, and that the primary treatmentsite, the hospital, remains an important source of support, particularly in-formational support, for at least the 2 years postdiagnosis that these parentswere followed up for. It is important that when psychosocial assessments aredone, that support network properties, and not just numbers, are explored.We need to know who will provide what type of support, and the flexibilityof the mix over time, rather than simply how many people are available toprovide support. It is also important to note the psychic cost that can beassociated with accessing support, particularly from family members.
The study has also shown that in general families do cope with thechallenge of having a child with a brain tumor, and mainly do so by utilizingan “internal” (to the family), preexisting method of coping that uses externalsupport as an adjunct. At the diagnostic stage, families should be encouraged
Social Support and Coping with Pediatric Brain Tumor 21
to identify their coping patterns, in terms of what may be transferred to thisnew situation.
The study has shown the usefulness of a mixed method prospectivestudy design. It is also worth noting that the NSSQ does not allow for theseparation of quantity, from quality of the support, a feature of the tool thatshould be borne in mind when using it to assess support.
REFERENCES
Carlson-Green, B., Morris, R., & Krawiecki, N. (1995). Family and illness predictorsof outcome in pediatric brain tumors. Journal of Pediatric Psychology, 20(6),769–784.
Fenig, S., Levav, I., Kohn, R., & Yelin, N. (1993). Telephone vs. face-to-face inter-viewing in a community psychiatric survey. American Journal of Public Health,83(6), 896–898.
Florian, V., & Krulik, T. (1991). Loneliness and social support of mothers of chroni-cally ill children. Social Science Medicine, 32(11), 1291–1296.
Frank-Stromborg, M., & Olsen, S, J. (1997). Instruments for clinical health-care re-search (2nd ed.). Boston: Jones & Bartlett Publishers.
Garwick, A. W., Patterson, J. M., Bennett, F. C., & Blum, R. W. (1998). Parents’perceptions of helpful vs unhelpful types of support in managing the careof preadolescent’s with chronic conditions. Archives of Paediatric AdolescentMedicine, 152, 665–671.
Goldbeck, L. (2001). Parental coping with the diagnosis of childhood cancer: Gendereffects, dissimilarity within couples, and quality of life. Psycho-Oncology, 10(4),325–335.
Graetz, B. W., Shute, R. H., & Sawyer, M. G. (2000). An Australian study of adoles-cents with cystic fibrosis: Perceived supportive and non-supportive behavioursfrom family and friends and psychological adjustment. Journal of AdolescentHealth, 26, 64–67.
Hamlett, K. W., Pellegrini, D. S., & Katz, K. S. (1992). Childhood chronic illness as afamily stressor. Journal of Pediatric Psychology, 17(1), 33–47.
Hoddap, R., Dykens, E., & Masino, L. (1997). Families of children with Prader-Willi syndrome—stress-support and relations to child characteristics. Journal ofAutism and Development Disorders, 27(1), 11–24.
Hoekstra-Weebers, J. E., Jaspers, J. P., Kamps, W. A., & Klip, E. C. (2001). Psycho-logical adaptation and social support of parents of pediatric cancer patients:A prospective longitudinal study. Journal of Pediatric Psychology, 26(4), 225–235.
Horn, J. D., Feldman, H. M., & Ploof, D. L. (1995). Parent and professional percep-tions about stress and coping strategies during a child’s lengthy hospitalisation.Social Work in Health Care, 21(1), 107–127.
Jackson, A. C., Tsantefski, M., Goodman, H., Johnson, B., & Rosenfeld, J. (2003).The psychosocial impacts on families of low-incidence, complex conditions inchildren: The case of craniopharyngioma. Social Work and Health Care, 38(1),81–107.
22 A. C. Jackson et al.
James, C. S. (1991). Practice research in social work: Applications for people livingwith HIV/AIDS. Australian Social Work, 44(4), 15–22.
Kazak, A. E., Cant, M. C., Jensen, M. M., McSherry, M., Rourke, M. T., Hwang, W. T.,et al. (2003). Identifying psychosocial risk indicative of subsequent resource usein families of newly diagnosed pediatric oncology patients. Journal of ClinicalOncology, 21(17), 3220–3225.
Kazak, A. E., & Nachman, G. S. (1991). Family research on childhood chronic illness:Pediatric oncology as an example. Journal of Family Psychology, 4(4), 462–483.
Kim, Y., Duberstein, P. R, Sorenson, S., & Larson, M. R. (2005). Levels of depressivesymptoms in spouses of people with lung cancer: Effects of personality, socialsupport, and caregiving burden. Psychosomatics, 46(2), 123–130.
Kupst, M. (1992). Long-term family coping with acute lymphoblastic leukemia inchildhood. In A. M. La Greca, L. J. Siegel, J. L. Wallander, & C. E. Walker (eds.),Stress and coping in child health, New York: Guilford Press.
Kupst, M., Natta, M. B., Richardson, C. C., & Sculman, J. L., Lavigne, J. V., & Das,L. (1995). Family coping with pediatric leukemia: Ten years after treatment.Journal of Pediatric Psychology, 20(5), 601–617.
Kupst, M., & Shulman, J. L. (1988). Long-term coping with pediatric leukemia: Asix-year follow-up study. Journal of Pediatric Psychology, 13(1), 7–22.
Lo-Biondo-Wood, G., Bernier-Henn, M., & Williams, L. (1992). Impact of the child’sliver transplant on the family: Maternal perspective. Paediatric Nursing, 18(5),461–466.
Lynam, J. (1987). The parent network in paediatric oncology: Supportive or not.Cancer Nursing, 10(4), 207–216.
Mailick, M. D., Holden, G. & Walther, V. N. (1994). Coping with childhood asthma.Health and Social Work, 19(3) 103–111.
Martin, C., & Nisa, M. (1996). Meeting the needs of children and families in chronicillness and disease: A greater role for the G.P.? Australian Family Physician,25(8), 1273–1281.
McCubbin, M. A., & McCubbin, H. I. (1996). Resiliency in families: A conceptualmodel of family adjustment and adaptation in response to stress and crises.In H. I. McCubbin, A. I. Thompson, & M. A. McCubbin (eds.), Family assess-ment: Resiliency, coping and adaptation—inventories for research and practice(pp. 1–64). Madison: University of Wisconsin System.
McCubbin, H. I., McCubbin, M. A., Nevin, R., & Cauble, E. (1996). Coping-HealthInventory for Parents (CHIP). In H. I. McCubbin, A. I. Thompson, & M.A. McCubbin (eds.), Family assessment: Resiliency, coping and adaptation—inventories for research and practice (pp. 407–454). Madison: University of Wis-consin System. (Original published in 1983.)
McCubbin, H. I., Thompson, A. I., & McCubbin, M. A. (1996). Family assessment:Resiliency, coping and adaptation—Inventories for research and practice. Madi-son: University of Wisconsin System.
McGee, S. J., & Burkett, K. W. (1998). Building a support group for parents ofchildren with brain tumours. Journal of Neuroscience Nursing, 30(6), 345–349.
Molinari, D. L., & Freeborn, D. (2006). Social support needs of families adoptingspecial needs children. Journal of Psychosocial Nursing and Mental HealthServices, 44(4), 28–34.
Social Support and Coping with Pediatric Brain Tumor 23
Morrow, G. R., Hoagland, A. C., & Morse, I. P. (1981). Sources of support per-ceived by parents of children with cancer: Implications for counselling. PatientCounselling and Health Education, 4(1), 36–39.
Mulhern, R. K., Fairclough, D. L., Smith, B., & Douglas, S. M. (1992). Maternaldepression, assessment methods, and physical symptoms affect estimates ofdepressive symptomology among children with cancer. Journal of PediatricPsychology, 17(3), 313–326.
Mulhern, R. K., Hancock, J., Fairclough, D. L., & Kun, L. (1992). Neuropsychologicalstatus of children treated for brain tumours: A critical review and integrativeanalysis. Medical and Pediatric Oncology, 20(3), 181–191.
Newacheck, W., & Taylor, W. R. (1992). Childhood chronic illness: Prevalence,severity, and impact. American Journal Public Health, 82(3), 64–71.
Noll, R. B., Garstein, M. A., Hawkins, A., Vannatta, K., Davies, W. H., & Bukowski,W. M. (1995). Comparing parental distress for families with children who havecancer and matched comparison families without children with cancer. FamilySystems Medicine, 13(1), 11–27.
Norbeck, J. S. (1995). Scoring instructions for the Norbeck Social SupportQuestionnaire (NSSQ) revised 1995. Unpublished manual. Available atwww.nurseweb.ucsf.edu
Norbeck, J. S., Lindsey, A. M., & Carrieri, V. L. (1983). Further development ofthe Norbeck Social Support Questionnaire: Normative data and validity testing.Nursing Research, 32(1), 4–9.
Olson, D. H., Portner, J., & Bell, R. Q. (1982). FACES II: Family Adaptability andCohesion Evaluation Scales. Minnesota: University of Minnesota, Family SocialScience.
Overholser, J., & Fritz, G. (1990). The impact of childhood cancer on the family.Journal of Psychosocial Oncology, 8(4), 71–85.
Patterson, J. M., Garwick, A. W., Bennett, F. C., & Blum, R. W. (1997). Social supportin families of children with chronic conditions: Supportive and nonsupport-ive behaviours. Journal of Developmental and Behavioural Psychology, 18(6),383–391.
Paulsen, A. S., Crowe, R. R., Noyes, R., & Pfohl, B. (1988). Reliability of the telephoneinterview in diagnosing anxiety disorders. Archives of General Psychiatry, 45(1),62–63.
Pelletier, G. G., Lepage, L., & Dussault, G. (1994). Social support received by mothersof chronically ill children. Child: Care, Health and Development, 20, 115–131.
Phipps, S., & Mulhern, R. (1995). Family cohesion and expressiveness promoteresilience to the stress of pediatric bone marrow transplant: A preliminary report.Developmental and Behavioral Pediatrics, 16(4), 257–263.
Radcliffe, J., Bennett, D., Kazak, A., Foley, B., & Phillips, P. (1996). Adjustment inchildhood brain tumor survival: Child, mother, and teacher report. Journal ofPediatric Psychology, 21(4), 529–539.
Rohde, P., Lewinsohn, P. M., & Seeley, J. R. (1997). Comparability of telephoneand face-to-face interviews in assessing Axis I and Axis II disorders. AmericanJournal of Psychiatry, 154(11), 1593–1598.
Sawyer, M., & Spurrier, N. (1996). Families, parents and chronic childhood illness.Family Matters, 44, 12–15.
24 A. C. Jackson et al.
Sawyer, M., Antoniou, G., Toogood, I., & Rice, M. (1997). Childhood cancer: A two-year prospective study of the psychological adjustment of children and parents.Journal of the American Academy of Child and Adolescent Psychiatry, 36(12),1736–1743.
Secco, M. L., & Moffatt, M. E. K. (1994). A review of social support theories and in-struments used in adolescent mothering research. Journal of Adolescent Health,15(7), 517–527.
Sloper, P. (1996). Needs and responses of parents following the diagnosis of child-hood cancer. Child: Care, Health and Development, 22(3), 187–202.
Slutske, W. S., True, W. R., Scherrer, J. F., Goldberg, J., Bucholz, K. K., Heath,A. C., et al. (1998). Long-term reliability and validity of alcoholism diagnoses andsymptoms in a large national telephone interview survey. Alcoholism: Clinicaland Experimental Research, 22(3), 553–558.
Speechley, K. N., & Noh, S. (1992). Surviving childhood cancer, social support,and parents’ psychological adjustment. Journal of Pediatric Psychology, 17(1),15–31.
Stein, R. E., & Reissman, C. K. (1980). The development of an impact-on-family scale.Medical Care, 18(4), 465–472.
Svavarsdottir, E. K. (2005). Caring for a child with cancer: A longitudinal perspective.Journal of Advanced Nursing, 50(2), 153–161.
Swallow, V. M., & Jacoby, A. (2001). Mother’s coping with childhood chronic ill-ness: The effect of presymptomatic diagnosis of vesicoureric reflux. Journal ofAdvanced Nursing, 33(1), 69–78.
Sweet, L. (2002). Telephone interviewing: Is it compatible with interpretive phe-nomenological research? Contemporary Nursing, 12(1), 58–63.
Tomlinson, P. S., & Mitchell, K. E. (1992). On the nature of social support for familiesof critically ill children. Journal of Paediatric Nursing, 7(6), 386–394.
Trask, P. C., Paterson, A. G., Trask, C. L., Bares, C. B., Birt, J., & Maan, C. (2003).Parent and adolescent adjustment to pediatric cancer: Associations with coping,social support, and family function. Journal of Pediatric Oncology Nursing,20(1), 36–47.
von Weiss, R. T., Rapoff, M. A., Varni, J. W., Lindsley, C. B., Olson, N. Y., Madson,K. L., & Bernstein, B. H. (2002). Daily hassles and social support as predictorsof adjustment in children with pediatric rheumatic disease. Journal of PediatricPsychology, 27(2), 155–165.
Weeks, M. F., Kulka, R. A., Lessler, J. T., & Whitmore, R. W. (1983). Personal ver-sus telephone surveys for collecting household health data at the local level.American Journal of Public Health, 73(12), 1389–1394.
Wijnberg-Williams, B. J., Kamps, W. A., Klip, E. C., & Hoekstra-Weebers, J. E. (2006).Psychological adjustment of parents of pediatric cancer patients revisited: Fiveyears later. Psycho-Oncology, 15(1), 1–8.
Woods, N. F., Haberman, M. R., & Packard, N. J. (1993). Demands of illness andindividual, dyadic, and family adaptation in chronic illness. Western Journal ofNursing Research, 15(1), 10–30.
Zahr, L. K., Khoury, R. N., & Saoud, N. B. (1994). Chronic illness in Lebanesepreschoolers: Impact of illness and child temperament on the family. AmericanJournal of Orthopsychiatry, 64(3), 396–403.
Related Documents











