The Role of Parent Stress and Parenting Behaviors in Cognitive Function in Children with Sickle Cell Disease By Janet Yarboi, M.S. Dissertation Submitted to the Faculty of the Graduate School of Vanderbilt University in partial fulfillment of the requirements for the degree of DOCTOR OF PHILOSOPHY in PSYCHOLOGY August 10, 2018 Nashville, Tennessee Approved: Bruce Compas, Ph.D. Michael DeBaun, M.D., M.P.H. Sarah Jaser, Ph.D. Sohee Park, Ph.D. Megan Saylor, Ph.D.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The Role of Parent Stress and Parenting Behaviors in Cognitive Function in Children with Sickle Cell Disease
By
Janet Yarboi, M.S.
Dissertation
Submitted to the Faculty of the
Graduate School of Vanderbilt University
in partial fulfillment of the requirements
for the degree of
DOCTOR OF PHILOSOPHY
in
PSYCHOLOGY
August 10, 2018
Nashville, Tennessee
Approved:
Bruce Compas, Ph.D.
Michael DeBaun, M.D., M.P.H.
Sarah Jaser, Ph.D.
Sohee Park, Ph.D.
Megan Saylor, Ph.D.

ii
TABLE OF CONTENTS
Page
LIST OF TABLES…………………………………………………………………….....iii LIST OF FIGURES……………………………………………………………………….v Chapter I. BACKGROUND………………………………………………………………………..1 Sickle cell disease…………………………………………………………………2 Cognitive problems in children with SCD…………………………………….......5 Disease-related correlates of cognitive function in SCD………………………….8 Social-environmental correlates of cognitive function…………………………..10 From environment to child: The mediating role of caregivers…………………..12 Characteristics of children with SCD and families………………………………15 Present research and hypotheses…………………………………………………20 II. METHOD……………………………………………………………………………..24 Participants…………………………………………………………………….....24 Procedure………………………………………………………………………...25 Measures…………………………………………………………………………27 Data analytic strategy………………………………………………………….....32 III. RESULTS……………………………………………………………………………35 Preliminary analyses……………………………………………………………..35 Comparison of means…………………………………………………………....36 Bivariate correlational analyses……………………………………………….....37 Multivariate regression analyses…………………………………………………39 IV. DISCUSSION………………………………………………………………………..42 Appendix A. Pediatric Inventory for Parents (PIP)…………………………………………………72 B. Perceived Stress Scale (PSS)……………………………………………………….....77 C. Supplementary Analyses……………………………………………………………...79 REFERENCES…………………………………………………………………………..89

iii
LIST OF TABLES
Table Page 1. Demographic Characteristics of Children and Caregivers in Sample………………...58 2a. Definitions and Examples of Macro-Level IFIRS Codes in Responsive Parenting Composite……………………………………………………………………..59 2b. Definitions and Examples of Macro-Level IFIRS Codes in Warm Parenting Composite………………………………………………………………………………..60 2c. Definitions and Examples of Macro-Level IFIRS Codes in Withdrawn Parenting Composite……………………………………………………………………..61 2d. Definitions and Examples of Macro-Level IFIRS Codes in Overinvolved Parenting Composite……………………………………………………………………..62 3. Definitions and Examples of Micro-Level Contingency Codes………………………63 4. Bivariate Correlations Between Micro- and Macro-Level Observed Parenting Codes……………………………………………………………………………………..64 5. Means, Standard Deviations, and One-Sample t tests of Child Cognitive Function………………………………………………………………………………….65 6. Bivariate Correlations Among Sociodemographic and Disease Risk, Parent Stress, and Child Cognitive Function………………………………………….....66 7. Bivariate Correlations Between Parent Stress and Observed Parenting………………67 8. Bivariate Correlations Between Observed Parenting and Child Cognitive Function………………………………………………………………………………….68 9. Summary of Linear Regression Analyses for Variables Predicting Child Cognitive Function…………………………………………………………………….....69 10. Intercorrelations Among Macro-Level Codes Included in Responsive Parenting Composite……………………………………………………………………..80 11. Intercorrelations Among Macro-Level Codes Included in Warm Parenting Composite………………………………………………………………………………..81 12. Intercorrelations Among Macro-Level Codes Included in Withdrawn Parenting Composite……………………………………………………………………..82

iv
13. Intercorrelations Among Macro-Level Codes Included in Overinvolved/ Intrusive Parenting Composite…………………………………………………………...83 14. Intercorrelations Among Micro-Level Parenting Codes……………………………..84 15. Linear Regression Analyses for Variables Predicting Child VCI and PRI………….85 16. Linear Regression Analyses for Variables Predicting Child Cognitive Function with PIP Total……………………………………………………………….....86

v
LIST OF FIGURES
Figure Page 1. Heuristic Model Depicting Proposed Pathway Between Parent Stress, Observed Parenting and Cognitive Function in Children with SCD………………….....71
1
CHAPTER I
BACKGROUND
Recent estimates indicate that over 4 million children in the United States live
with a chronic health condition, which represents a significant increase in recent decades
(van der Lee, Mokkink, Grootenhuis, Heymans & Offringa, 2007). One reason for this
increase is that, with advancements in early identification and treatment, more children
are surviving and living with their conditions through adolescence and into adulthood
(e.g., Halfon & Newacheck, 2010). Consequently, new research is aimed at better
understanding the long-term effects of pediatric disease on health and development. One
significant consequence, and the focus of the current study, is impairment in brain
development and cognitive function. In a recent review, Compas, Jaser, Reeslund, Patel,
and Yarboi (2017) provided the first synthesis of evidence of significant neurocognitive
problems in children with a wide range of chronic health conditions, including traumatic
brain injury, leukemia, congenital heart disease, and type 1 diabetes among others.
As highlighted by Compas et al. (2017), one chronic health condition that places
patients at an increased risk for considerable cognitive impairment is sickle cell disease
(SCD). This potentially life-threatening condition affects more than one in every 400
African-American newborns (Lorey, Arnopp, & Cunnigham, 1996). As screening and
treatment options improve and greater numbers of pediatric SCD patients are surviving
into adulthood, there is a renewed interest and urgency in identifying the underlying
causes of these marked decrements in cognitive functioning (Compas et al., 2017).
Although prior research has primarily focused on disease-related risk factors, emerging

2
evidence suggests it is also important to consider the influence of sociodemographic
factors, especially given the challenges associated with economic disadvantage that face
many children with SCD and their families (e.g., King et al., 2014). Research with
healthy, typically developing children suggests that parents serve as one of the
cornerstones of this pathway, mediating the relationship between disease burden and
sociodemographic disadvantage and cognitive impairment in children (e.g., Doan &
Evans, 2011).
The goal of the present research is to examine the role of parent stress and
parenting behaviors and their association with cognitive function in this high-risk, yet
understudied, population. In this introduction, I begin by reviewing the biomedical
characteristics of SCD and the current evidence of cognitive impairment in patients.
Next, I present findings in support of both disease-related and sociodemographic
correlates of cognitive function. I then summarize the literature regarding the role of
parents in children’s cognitive development and present the rationale and hypotheses for
the current study.
Sickle Cell Disease
Sickle cell disease (SCD) refers to a group of chronic genetic blood disorders that
are among the most common inherited monogenic disorders in the world (Weatherall,
Hofman, Rodgers, Ruffin & Hrynkow, 2005). SCD is caused by a genetic mutation
resulting in the production of sickle hemoglobin (HbS), which causes red blood cells to
become hard and abnormally shaped. There are several hemoglobinopathies in the SCD
family, with sickle cell anemia (HbSS) identified as the most common and the most
severe (Ashley-Kock, Yang & Olney, 2000). Other major types of sickle cell disease

3
include hemoglobin SC disease (HbSC) and hemoglobin S-beta thalassemia (Rees,
Williams & Gladwin, 2010). SCD most commonly affects those of African descent, but
cases have also been reported in those of Mediterranean, Indian and Arab descent
(Driscoll, 2007). These disorders are characterized by recurrent pain crises, chronic
anemia and other debilitating complications.
In the United States, 44 states and the District of Columbia currently include
hemoglobinopathy testing as part of newborn screening, which allows for early diagnosis
before clinical onset of symptoms. The first symptoms of SCD generally appear within
the first year of life with disease presentation varying based on age. In early childhood,
SCD patients are most likely to experience infection, spleen enlargement, and
neurological complications. As patients enter adolescence and adulthood, they are more
likely to suffer from retinopathy, leg ulcers, renal insufficiency, pulmonary hypertension,
and other chronic organ damage. Some SCD complications, however, occur throughout
the lifespan. The most common symptom of SCD is severe acute pain caused by the
entrapment of sickled blood cells and the consequent interruption of blood flow.
Considered the hallmark of SCD, these vaso-occlusive pain crises are experienced by
70% of all patients and account for 30% of SCD-related hospital admissions (Platt et al.,
1991). Acute chest syndrome is another common complication of SCD and is caused by
the obstruction of pulmonary vasculature. Symptoms of acute chest syndrome include
pain, fever, cough and hypoxia (Driscoll, 2007).
A recent report using census population data estimated that nearly 100,000 people
in the U.S. are living with an SCD disorder, even after accounting for early mortality
(Hassell, 2010). However, this number is likely an underestimation by up to 37%, as it

4
includes the Black and Hispanic population but excludes White (including
Mediterranean) and Asian (including Indian and Arab) individuals. In the U.S., it is
estimated that approximately one in less than 400 African-American newborns is affected
with HbSS, HbSC or Hb S-beta thalassemia (Hassell, 2010). It is well established that
individuals with SCD have a shortened life expectancy (e.g., Platt et al., 1994). However,
due to improvements in screening and diagnostic procedures as well as advancements in
treatment options, life expectancy has increased significantly over the last four decades.
More specifically, life expectancy for individuals with sickle cell anemia (HbSS) has
increased from approximately 14 years in 1973 to 42 years for males and 48 years for
females in 1994 (Hamideh & Alvarez, 2013).
More recently, a study of 940 patients in the Dallas Newborn Cohort ranging in
age from less than 1 month to 20 years, estimated the 18-year survival rate to be 93.9%
for patients with more severe forms of the disease, such as HbSS, and 98.4% for patients
with milder forms of SCD, such as HbSC (Quinn, Rogers, McCavit & Buchanan, 2010).
This is an improvement from the estimated survival rates of the same cohort several years
earlier (Quinn, Rogers & Buchanan, 2004). Hamideh and Alvarez (2013) observed a
similar trend in SCD-related mortality. The authors found that, when compared to 1979-
1998, SCD mortality during 1999-2009 significantly decreased by 61% for infants, 67%
for young children and 22-35% for 5-19 year olds.
Collectively, these studies show that, over the last several decades, survival has
increased and mortality has decreased in children with SCD. It should be noted, however,
that both studies show that these trends are not as encouraging for young adults; these
individuals are actually at a greater risk for early SCD-related death than they were

5
several years ago. Hamideh and Alvarez (2013) suggest that certain barriers including
limited access to providers, poor communication between providers, and insufficient
insurance coverage mark the transition period between pediatric and adult care. These
findings demonstrate that more SCD patients are surviving through childhood while
simultaneously struggling with the transfer of care between late adolescence and early
adulthood. Consequently, there has been a push to redirect research efforts towards
understanding if and how children with SCD are adapting to the psychosocial,
psychological, and cognitive effects of living with the disease (Helps, Fuggle, Udwin &
Dick, 2003).
Cognitive Problems in Children with SCD
Impaired cognitive function is one of the most significant negative developmental
outcomes faced by individuals with SCD. More specifically, a growing body of evidence
indicates that children with SCD experience cognitive deficits across several domains
when compared to healthy peers and normative samples (e.g., Hijmans et al., 2011a; King
et al., 2014; Schatz, 2004; Steen et al., 2005). In the most comprehensive meta-analysis to
date, Schatz, Finke, Kellett and Kramer (2002) computed and compared the Cohen’s d
effect sizes for 14 previously published studies examining impairments in cognitive
function in children with SCD. With regard to general intelligence, the authors found that
the average IQ of children with SCD was 4.3 standard score points lower (d = -0.31) than
that of healthy comparison samples. The effect was notably larger for studies that also
examined differences in domain-specific cognitive areas. Seventy-one percent of the
included studies found significant deficits in specific cognitive domains including
attention, executive function, language and memory. No data were provided for the

6
magnitude of the effects in these domains.
Since 2002, the body of research related to cognitive deficits in pediatric SCD
patients has continued to grow with results generally replicating those found by Schatz et
al. (2002). For example, Steen et al. (2005) found that pediatric SCD patients with normal
magnetic resonance imaging (MRI) results (that is, without any evidence of
cerebrovascular damage) showed significant deficits in general intelligence when
compared to healthy controls matched to patients by age, gender and race with a reported
Cohen’s d effect size of -.72. When all patients were considered, including those with
MRI abnormalities, the effects were even greater (d = -1.11). Additional analyses of
patients with HbSS, the most severe form of SCD, showed that this group experienced
the greatest impairment in tasks related to verbal intelligence. Hijmans et al. (2011a)
found similar results, demonstrating that, on average, children with SCD obtained
significantly lower IQ scores than controls matched by socioeconomic status
(SES) with a mean full-scale IQ that was more than d = 1.5 standard deviations below
population norms. Specifically, the authors reported that more than 1 in 3 children with
SCD had an IQ lower than 75 standard points1 compared to 1 in 10 children in the
comparison group. They also found that children with SCD scored lower than controls on
tasks related to both performance and verbal intelligence (Hijmans et al., 2011a). In a
recent study of infants and toddlers living with SCD, patients scored, on average, a full
standard deviation (d = 1.0) below population norms on a measure of cognitive
development (Glass et al., 2013). These results suggest that functional deficits in
cognition in children with SCD may begin at a very young age, placing patients at risk
1 Current criteria for a diagnosis of intellectual disability includes an IQ standard score of 70 ± 5 for measurement error (American Psychiatric Association, 2013).

7
for early developmental delay.
Recent evidence has also shown that children with SCD experience domain-
specific cognitive impairment in areas such as memory, language, and executive function.
For example, Schatz and Roberts (2007) also found that toddlers and early preschoolers
with SCD make more incorrect responses and perseverative errors on a delayed response
working memory task. Additionally, there is evidence to suggest that children with SCD
experience language-processing deficits that are not accounted for by tasks designed to
measure verbal intelligence. For example, one study showed that children with the most
severe cases of SCD scored significantly lower than demographically matched healthy
controls on semantic, syntactic and phonological tasks (Schatz, Puffer, Sanchez, Stancil
& Roberts, 2009). Pediatric SCD patients also show deficits in executive functions,
including skills related to working memory, sustained attention, selective attention, and
planning (e.g., Hijmans et al., 2011a; Yarboi et al., 2017).
In addition to general intelligence and specific cognitive domains, researchers
have also explored the effect of cognitive impairment on academic achievement and
school performance. School-aged children with SCD score lower than peers on
psychometric tests of academic achievement, including tasks and tests related to reading,
writing and math (Schatz, 2002; 2004). More specifically, Schatz (2004) found medium
effects on tests of reading decoding (r = -.31) and math calculations (r = -.37). While
these findings are useful for detecting and classifying functional impairments in students
with SCD, a closer examination of non-psychometric outcome variables (i.e., measures of
academic attainment) provides additional information. For example, a conservative
estimate shows that more than 31% of students with SCD (44% when considering only

8
participants who successfully enrolled in the study) received special services at school
and/or had a reported history of grade retention. This estimate is compared to 14% of
demographically matched comparison students recruited from the same community.
Children with SCD were also more likely to repeat multiple grades with several
participants repeating a grade past the third grade (Schatz, 2004). Some evidence
suggests that issues with academic achievement in children with SCD may be detected as
early as initial school entry. For example, Steen et al. (2005) found that kindergarten
students with SCD displayed deficits in certain kindergarten-readiness skills, which are
generally required for long-term success in reading and math learning.
Disease-Related Correlates of Cognitive Function in SCD
Although it is well established that children with sickle cell disease are at risk for
significant decrements in cognitive functioning, there is a limited understanding of the
underlying causes. To date, most research has focused on disease-related factors that have
a direct effect on cognition. One of the most highly studied among these factors is
cerebral infarction, or stroke. Patients with SCD are at an increased risk of experiencing
neurological damage, the most common and severe of which is the result of stroke. It is
estimated that approximately 7% of children with sickle cell anemia will suffer from one
or more overt cerebrovascular events before the age of 15 years, with incidence peaking
between the ages of 2 and 5 years (Hogan, Pitten Cate, Vargha-Khadem, Prengler, &
Kirkha, 2006; Schatz & Buzan, 2006). Pediatric SCD patients with a clinical history of
overt stroke experience, on average, a 10-15 point decline in IQ as well as difficulties
with academic achievement and attainment (Schatz & McClellan, 2006).
Children with SCD may also experience cerebral infarction without any overt

9
symptoms, resulting in brain damage that is only detectable with MRI. Advancements in
imaging technology have allowed for earlier and more accurate detection of these “silent”
strokes, resulting in an estimated prevalence of 21.8% in children with SCD (Pegelow et
al., 2002). While patients with a history of overt stroke are typically at the greatest risk
for cognitive impairment, there is evidence that children with MRI-detected silent strokes
are also vulnerable to mild deficits in cognitive function in comparison to both SCD
patients with no MRI abnormalities and healthy controls without SCD (e.g., Brown et al.,
2000; Hogan et al., 2006). For example, in a recent meta-analysis, King et al. (2014)
compared children with SCD with and without silent strokes based on brain MRI and
showed that although all participants displayed deficits in FSIQ (M = 86.54), those with
silent strokes were more severely impaired, with an overall effect of -4.76 IQ points.
Given that pediatric SCD patients without a history of cerebral infarction, either
overt or silent, also experience notable cognitive impairment (e.g., Brown et al., 2000;
Hogan et al., 2006), it is important to consider the impact of other biomedical factors.
For example, research shows that children with SCD with normal MRI results, but
elevated cerebral blood flow (CBF) velocity, perform poorly on measures of language
functioning, general intelligence and attention (Sanchez, Schatz & Roberts, 2010; Strouse
et al., 2006). CBF velocity is also closely tied to occurrence of stroke in SCD patients and
has been utilized to identify those at the highest risk (Adams et al., 1992).
Sleep-disordered breathing represents another important disease-related predictor
of cognitive function in this population (Hill et al., 2006). One estimate suggests that as
many as 40% of children with SCD are affected by sleep-disordered breathing, which
results in frequent sleep disruption and nocturnal oxygen desaturation (Needleman et al.,

10
1999). Research with non-SCD patients has shown that children with obstructed
breathing during sleep experience subtle but significant impairments in processing speed,
attention, and executive function (e.g., Beebe et al., 2004; Hill et al., 2006). In a recent
study with children with SCD, Hollocks et al. (2012) found that sleep disordered
breathing, which is associated with low hemoglobin oxygen saturation, may negatively
impact general intelligence and specific executive domains.
Another reported biomedical predictor of cognitive function in young SCD
patients is anemia, or the deficiency of red blood cells in the blood. Anemia is often
considered an indicator of overall severity in SCD (Ohene-Frempong et al., 1998).
Evidence suggests that anemia severity, which is determined by hemoglobin level, is
inversely correlated with performance on certain domains of cognitive function,
including short-term and working memory, verbal comprehension, and overall
intelligence (Hijmans et al., 2011b; Steen et al., 2003). In one example, Steen and
colleagues (2003) found that anemia explained 23% of the variance in overall IQ in
pediatric SCD patients without a history of stroke. As with sleep-disordered breathing,
these effects are likely due to insufficient cerebral oxygenation.
Collectively, these findings demonstrate the major impact that disease-related
factors have on the cognitive development of children with SCD. Nevertheless,
biomedical characteristics of the disease only explain a portion of the variance in
children’s cognitive function. This suggests that there may be other important, but not yet
explored, factors contributing to the observed effect.
Social-Environmental Correlates of Cognitive Function
To date, research on cognitive impairment in children with SCD has primarily

11
focused on the disease-related risk factors discussed above. However, there is evidence to
suggest that sociodemographic factors may also be implicated in children’s cognitive
development, yet these issues have received relatively little attention in SCD research in
comparison.
There is an extensive body of research demonstrating the damaging effects of
chronic poverty on neurocognitive development in healthy children. In their review of the
relationship between socioeconomic status and brain development, Hackman and Farah
(2009) described pronounced economic disparities in several areas of cognitive ability,
including language ability, executive function, and memory. Findings on the effect of
economic deprivation on other domains, including visual/spatial cognition, are
inconclusive, suggesting that financial hardship affects neurocognitive systems
differently (Farah et al., 2006; Hackman & Farah, 2009).
The impact of growing up in persistent poverty is also apparent through more
global measures of cognitive ability, such as IQ and academic achievement (e.g., Bradley
& Corwyn, 2002; Sirin, 2005). One report showed that children as young as 5 years old
from low-income families were already performing worse than their more affluent peers
on tasks related to verbal intelligence, performance intelligence, and overall intelligence
(Duncan, Brooks-Gunn & Klebanov, 1994). On average, children raised in poverty obtain
IQ scores 5-10 points lower than those of children raised in middle class families (Kaiser
& Delaney, 1996). The growing literature on the relationship between economic status
and academic achievement has produced similar results. In a meta-analytic review of
articles published between 1990 and 2000, Sirin (2005) calculated medium to large
effects, with children raised in poorer families or attending disadvantaged schools

12
experiencing greater academic difficulty. It is important to acknowledge that exposure to
persistent poverty during childhood has lasting effects, predicting cognitive impairment
into adulthood (Kaplan et al., 2001).
From Environment to Child: The Mediating Role of Caregivers
In examining the route through which sociodemographic disadvantage and
financial strain may affect children, I draw on models supported by social-environmental
theories of development, which hold that the child is at the center of a large and dynamic
system of environmental influences that interact with one another to shape early
development (e.g., Bronfenbrenner, 1977; Sameroff & Fiese, 2000). These influences are
often categorized either as operating proximally, exerting a direct effect on the individual,
or distally, exerting an effect via an indirect mechanism involving more proximal factors.
Importantly, children’s caregivers represent one of the most salient proximal factors
impacting the course of child development, including cognitive function. Indeed, Kaiser
and Delaney (1996) refer to the parent-child relationship as “the primary developmental
context in which early cognitive, social, and behavioral development will occur” (p. 69).
Thus, in an effort to better comprehend the mechanisms through which sociodemographic
disadvantage impacts cognitive functioning in children, the field has turned its attention
to the caregiver as a possible mediator.
There is evidence to suggest that parenting behaviors are implicated in the
cognitive development of offspring (e.g., Lugo-Gil & Tamis-LeMonda, 2008; Tamis-
LeMonda, Shannon, Cabrera, & Lamb, 2004). For example, in a large study of 2,089
children and their families, Lugo-Gil and Tamis-LeMonda (2008) found that observed
parenting quality when children were 14 months of age was linked to concurrent
13
cognitive development (r = .26) as well as later cognitive development both at 24 months
(r = .40) and at 36 months of age (r = .39). Additional analyses showed that parenting
quality mediated the effects of family resources on children’s Mental Development Index
scores at all ages, demonstrating that factors such as family income and parental living
arrangement influence children indirectly through parents’ behaviors. In a noteworthy
examination of parenting as a mediator of the effect between income, cumulative risk,
and effortful control in preschoolers, Lengua et al. (2014) found that all domains of
parenting (i.e., warmth, negativity, scaffolding, limit setting and responsiveness) were
associated with children’s executive control concurrently at 36 months of age (r = .15 to r
= .35) as well as executive control scores 9 months and 18 months later (r = .13 to r =
.35).
However, in order to better understand the effect of economic disadvantage on the
parent-child relationship, it is crucial to understand how poverty directly affects parents
and caregivers. One pathway through which socioeconomic disadvantage may affect
parents of children with SCD is through levels of actual and perceived stress. For
example, in an exploration of parents’ perceptions of life in economically poor
environments, Ghate and Hazel (2002) found that economically disadvantaged parents
experienced a complex set of stressors at the level of the individual, the family, and the
community. Parents raising families in impoverished conditions are often faced with the
challenges of unemployment, physical health difficulties, and a lack of vital resources
including food, water and heat (Guo & Harris, 2000). Additionally, parents from low-
income households more frequently report low levels of familial and community support
(Middlemiss, 2003). As described by Conger and Donnellan (2007), it is the experience

14
of such social-environmental strain that “gives psychological meaning to economic
hardship” (p. 179). This notion is supported by a comprehensive body of research which
shows that persistent exposure to financial hardship and limited social support are
associated with chronic stress and distress in parents, including elevated rates of
depression and maladjustment (Kaiser & Delaney, 1996).
The role or responsive parenting. The stress and negative emotions associated
with poverty weaken interpersonal relationships and compromise parents’ abilities to
engage in responsive interactions with their children (Bradley & Corwyn, 2002). Indeed,
research has shown that socioeconomically disadvantaged caregivers engage in parenting
behaviors that lack consistency, support, and sensitivity to children’s needs (e.g.,
Hackman, Farah & Meaney, 2010; Kaiser & Delaney, 1996; Luby et al., 2013). These
patterns of parenting behaviors and values are often manifested in disruptions in parent-
child interactions. For example, Hart and Risley (1995) found that parents with lower
incomes use less complex and diverse language when interacting with their children.
Such communication styles are typically associated with parenting behaviors that are less
nurturing and less responsive (Hart & Risley, 1995). This is consistent with findings from
Guo and Harris (2000) who showed that exposure to poverty exerted a strong negative
effect on parent-child interactions, such that disadvantaged mothers were less likely to
engage in recurrent conversation with their child and were less likely to answer their
child’s questions with verbal responses.
Evans and colleagues have examined this concept of parental responsiveness
extensively, demonstrating that psychological stress, limited social support, and chaotic
environments partially account for the relationship between poverty and responsiveness

15
(e.g., Doan & Evans, 2011; Evans, Boxhill & Pinkava, 2008; Evans et al., 2010).
Conversely, the resilience displayed by some children raised in chronically disadvantaged
environments may be attributed to parenting that is responsive and attuned to the child’s
needs. More specifically, Doan and Evans (2011) suggest that mothers who are highly
responsive are more likely to exhibit child-centered teaching skills and create a more
enriching environment. In addition to stimulating cognitive development, these types of
parenting behaviors may also indirectly compensate for the direct effects of long-standing
poverty and stress on children’s functioning (Doan & Evans, 2011). Additionally, the
work produced by Evans and colleagues has emphasized the relationship between
duration of poverty and cumulative risk exposure. In other words, the longer children are
exposed to poverty, the greater their accumulation of adverse physical (e.g., crowding,
noise, substandard housing) and psychosocial (e.g., family discord, violence) risk factors.
Over time, this is related to greater distress and more impaired functioning for both
children and caregivers (Evans, 2003; Evans & Kim, 2007).
Characteristics of Children with SCD and Families
The above findings have significant implications for the predominantly African-
American population of SCD patients in the U.S. For perspective, the most recent report
from the U.S. Census Bureau (DeNavas-Walt & Proctor, 2015) indicates that while the
national poverty rate is 15%, the African-American population is disproportionately
represented with an estimated 26% of all Black families living below the poverty
threshold (US$24,008 annual income for households with two adults and two children).
Indeed, many individuals with SCD face poverty and chronic financial hardship
(Barbarin, Whitten, Bond & Conner-Warren, 1999). In a multi-site study, King et al.

16
(2014) found that over 50% of individuals with SCD enrolled in the study at sites in the
U.S. lived at or below poverty, and nearly 70% received Medicaid healthcare coverage.
Given that children with SCD experience disease-related effects on cognitive ability and
many grow up in economically disadvantaged homes, a significant portion of these
children may be facing a double burden of both biological risks and adverse
environmental conditions.
Importantly, when considering the impact of poverty and parenting on cognitive
development in children with sickle cell disease, it is also important to consider the
additional stress exerted on parents when raising a child with a potentially life-
threatening, chronic illness. Brown et al. (2008) proposed that parents of chronically ill
children are exposed to a number of different stressors including financial strain,
disruptions to daily routine, and an increase in and persistently high levels of caretaking
responsibilities. A recent synthesis of the literature on parenting stress found that
caregivers of children experiencing pediatric illness (including asthma, cancer, and
diabetes among others) reported greater parenting stress than caregivers of healthy
children (Cousino & Hazen, 2013). The authors also found that greater parenting stress
was associated with poorer psychological adjustment (e.g., depression and anxiety
symptoms) in caregivers of chronically ill children, which, as highlighted earlier, is
similar to outcomes experienced by parents facing chronic economic disadvantage.
In the context of SCD, research has shown that there is a significant inverse
relationship between disease-related parenting stress and family functioning among
families with children with SCD, particularly with regard to communication about sickle-
cell related issues (Barakat, Patterson, Tarazi & Ely, 2007). Consistent with the findings

17
reported above, family income was also a significant predictor of disease-related
parenting stress in this population (Barakat et al., 2007). Importantly, evidence shows that
illness parameters such as disease severity and duration may contribute more to parenting
stress among caregivers of children with SCD than in other illness populations. For
example, greater frequency of pain episodes and more frequent use of routine and urgent
health care services have been linked to greater disease-related parenting stress in
caregivers of children and adolescents with SCD (e.g., Barakat et al., 2007; Logan,
Radcliffe & Smith-Whitley, 2002). In contrast, disease-specific illness parameters are
unrelated to parenting stress among diabetes, epilepsy, and juvenile rheumatoid arthritis
populations (Cousino & Hazen, 2013). Collectively, these results suggest that parents of
children with sickle cell disease, many of whom are also socioeconomically
disadvantaged, may be facing a double hit to their capacity to be warm, supportive, and
responsive parents due to additional stress surrounding their child’s physical health
condition.
Although findings are limited, emerging evidence supports a link between
parental characteristics and cognitive problems in children with SCD. For example, King
et al. (2014) found that although disease-related factors such as cerebral infarction and
hemoglobin oxygen saturation played a significant role in the cognitive function of
children with SCD, a considerable amount of the additional variance was due to
sociodemographic factors such as parental education and income. Similarly, Yarboi et al.
(2017) found that maternal financial strain is negatively associated with positive
parenting and children’s cognitive function across several domains.
While promising, these preliminary findings are limited in several ways. First, at

18
the stressor level, recent evidence from pediatric oncology research demonstrates that it
may be best to examine sociodemographic status by utilizing a variable that aggregates
the multiple, distinct factors that comprise SES (Bemis et al., 2015). Despite these
findings, previous studies assessing SES in pediatric populations have typically utilized a
single variable as a proxy for sociodemographic disadvantage (e.g., family income), thus
failing to account for the collective impact of exposure to multiple markers of risk.
Second, at the parent stress level, existing studies have failed to incorporate a
self-reported assessment of caregiver’s perceived stress regarding the challenges of
caring for a child with a chronic health condition and/or the burden of chronic financial
hardship. In order to make inferences about the impact of these stressors on parenting
behaviors, it will be important to measure caregivers’ subjective experiences.
Third, at the parenting level, Yarboi et al. (2017) measured parenting using a self-
report measure that may have been vulnerable to sources of bias inherent in parents’
reports on their own behavior. Future work would benefit greatly from a more direct and
comprehensive assessment of parenting behaviors that captures more information than is
typically gathered from caregivers’ self-reports alone. One approach would be to code
specific parenting behaviors during observed parent-child interactions. Aspland and
Gardner (2003) encouraged the use of observational measures in assessing parenting
behavior as these methods are more closely aligned with real-world processes. Further,
the use of a comprehensive, detailed coding system allows for a more thorough
assessment of specific aspects of responsive parenting, including parental sensitivity to
and stimulation of children’s thinking skills.
Observed parent-child interactions can be assessed at two different levels of

19
analysis. At the macro-level, global coding systems are utilized to quantify dyadic or
parenting behaviors (e.g., responsiveness, warmth, intrusiveness) on scales that indicate
overall frequency and intensity throughout an interaction (e.g., Iowa Family Interaction
Rating Scale; IFIRS; Melby & Conger, 2001), but do not quantify the exact sequence of
behaviors between caregivers and children. For example, a global coding system might
rate a caregiver on how warm he or she was based on verbal and nonverbal behavior
towards the child during the interaction, but would not directly measure the number of
warm behaviors (e.g., hugging the child) or statements (e.g., “I love you”). Macro-level
coding systems are widely used and well validated; as a result, several composite codes
comprised of individual macro codes have been used in the literature and have been
shown to reliably predict child outcomes. In one example, Watson et al. (2014) measured
parental responsiveness using an empirically supported composite of macro-level parent
behaviors (e.g., listener responsiveness, communication, child-centeredness), and found
that parental responsiveness was related to use of adaptive coping strategies in children.
In contrast, the micro-level of analysis is able to capture the number of times a
caregiver uses a certain type of response (e.g., validation, repetition, question) and the
exact content of the response by relying on the structure of language as well as
conversational discourse between speakers (e.g., Hart & Risley, 1992; Lasky & Klopp,
1982). While widely used in developmental psychology research, micro-level systems are
not as commonly used in clinical psychology research and, as a result, the relationship
between parent language and child outcomes is often best understood by examining
individual codes in isolation rather than with composites reflecting a more global pattern
of behavior (as with macro-level coding). Thus, while no specific theory-driven

20
definition for responsive parenting exists at the micro-level, studies have shown that
certain categories of parental responses, including topic maintenance, validations,
reflections, expansions, and imperatives are related to psychosocial outcomes in children
(Murphy et al., 2015; Rodriguez et al., 2013).
Importantly, few studies have utilized both macro- and micro-level coding
systems to analyze the same parent-child interactions. Previous research suggests that
integrative analyses are beneficial in identifying micro-level components of parent
language that are associated with more global measures of parental behavior and that,
when used together, these systems may more reliably detect teachable parenting skills to
target in interventions aimed at improving psychosocial outcomes in children (Rodriguez
et al., 2013).
Present Research and Hypotheses
To date, research has established that children with sickle cell disease are at risk
for considerable cognitive impairment across several domains. In the push to identify the
underlying mechanisms responsible for these deficits, prior research has focused on
disease-related risk factors (e.g., cerebral infarction, cerebral blood flow velocity, sleep-
disordered breathing, and anemia severity) and their effect on cognition. A separate, but
related, body of research provides evidence to suggest that sociodemographic factors
such as income and home environment may also be implicated in the cognitive
development of children with SCD. Given the particular demographic characteristics of
children with SCD and their families (i.e., chronically ill, largely African-American and
disproportionately low-income), it is important to understand the relationship between
parent stress, parenting and child cognitive function in this complex, underrepresented

21
population.
Indeed, research indicates that caregivers of children with SCD may be unique in
their exposure to two distinct areas of parenting hardship: sociodemographic
disadvantage and chronic health problems in their children. The stress experienced in
response to these stressors may impair the ability to provide responsive, cognitively
stimulating parenting to children who are already at increased risk for cognitive
impairment. The few studies that have specifically examined these potential effects in the
context of pediatric SCD have found promising preliminary evidence, but future work
will benefit greatly from a more comprehensive methodological approach with focused
research aims.
Based on Evans and colleagues’ theoretical framework of parent-mediated
cognitive development in the face of environmental stressors (e.g., Doan & Evans, 2011),
one purpose of the present research is to extend the existing literature on parent stress
(specifically related to sociodemographic hardship and medical care), parenting, and
cognitive function and to unite these concepts in the context of pediatric SCD. I examine
how certain sociodemographic and disease factors are related to caregivers’ perceived
stress, and, in turn, if stress impacts how parents parent, and if any of these components
serve as unique predictors of cognitive function in children with SCD (see Figure 1). I do
so by exploring the following aims and hypotheses:
Aim 1: Replicate previous findings, which show that children with SCD
experience deficits in cognitive function across multiple domains when compared to
same-age peers.
22
• Hypothesis 1: Children with SCD will score lower than normative samples
on measures of cognitive function, including those in the domains of
intelligence, working memory and academic achievement.
Aim 2: Use a cumulative risk framework to determine the relationship between
children’s disease characteristics, caregivers’ sociodemographic disadvantage, and parent
stress.
• Exploratory analyses will determine the level of disease severity,
sociodemographic disadvantage, and parental stress in the current sample.
• Hypothesis 2: Greater sickle cell disease severity will be associated with
higher levels of both disease-related parenting stress and general perceived
stress.
• Hypothesis 3: Greater sociodemographic disadvantage will be associated
with higher levels of both disease-related parenting stress and general
perceived stress.
Aim 3. Determine the relationship between parent stress, observed parenting
behaviors and cognitive function in children with SCD, accounting for disease severity
and sociodemographic disadvantage.
• Hypothesis 4: Higher levels of parent stress will be associated with lower
levels of responsive parenting behaviors at the macro- and micro-levels
and with lower scores on measures of cognitive function in children with
SCD.

23
• Hypothesis 5: Lower levels of responsive parenting behaviors will be
associated with lower scores on measures of cognitive function in children
with SCD.
• Hypothesis 6: Parent stress and responsive parenting behaviors will serve
as significant predictors of cognitive function in children with SCD, above
and beyond the variance accounted for by disease severity and
socioeconomic disadvantage alone.

24
CHAPTER II
METHOD
Participants
Demographic characteristics of the sample are presented in Table 1. Participants
included 48 children and adolescents with SCD ages 6 to 16 (M = 9.30; SD = 3.08 years).
Participants were 56.8% male and represented a variety of sickle cell disease subtypes:
70.5% were diagnosed with HbSS; 20.5% and 9.1% were diagnosed with HbSC, and
variations of S-beta thalassemia, respectively. Results from patients’ most recent MRI
studies indicated that the majority of children (77.3%) displayed no evidence of an overt
cerebral infarct. Of the remaining 22.7%, 7 patients presented with a history of silent
stroke and 3 with a history of overt stroke. As expected, the majority of the sample
(97.7%) identified as African American. With regard to school attendance, caregivers
reported that children missed a mean of 5.30 days (SD = 6.75) of school in the last year
due to illness. Furthermore, 6.8% of the sample had repeated a grade and 22.7% received
special services (e.g., Individualized Education Program, 504 plan).
Participants also included 48 primary caregivers of youth with SCD. Caregivers
were predominantly biological parents (n = 42); the sample also included adopted parents
(n = 1), grandparents (n = 3), and other primary caregivers (n = 2). Despite representing a
wide range of familial relatedness, 92.3% of caregivers reported spending daily face-to-
face time with their child; thus, the terms “parent” and “caregiver” will be used
interchangeably throughout. Overall, caregivers ranged in age from 25 to 60 years old (M
= 39.57, SD = 9.43), and 79.5% were female. Self-report indicated that only one

25
caregiver carried his/her own diagnosis of sickle cell disease. Caregivers came from a
range of educational backgrounds (11th grade to 3rd year of graduate school; M = 13.7
years of education) as well as annual family income levels (40.4% earned $25,000 or
less, 29.8% earned $25,001 to $50,000, 14.9% earned $50,001 to $75,000, 8.5% earned
$75,001 to 100,000, and 6.4% earned $100,000 or above).
Procedure
Families were recruited to participate as part of a larger descriptive study,
Thinking and Learning in Children with Sickle Cell Disease, with the aim of determining
whether the environmental factors of stress and parenting influence cognitive functioning
in children with SCD above and beyond the effect of medical characteristics. Eligibility
requirements included: (a) confirmed diagnosis of sickle cell disease, (b) child age of 6-
16 years at study entry, and (c) participation of a caregiver who has legal guardianship
and is primarily responsible for the child. Children with a history of co-morbid
neurologic disorder (e.g., neurofibromatosis, lead poisoning, tuberous sclerosis) were
excluded from participating. Informed consent was obtained from caregivers and
informed assent was obtained from children prior to study entry and participation. The
study protocol was reviewed and approved by the Vanderbilt University Institutional
Review Board.
All recruitment occurred at the Monroe Carell Jr. Children’s Hospital at
Vanderbilt Sickle Cell Clinic and the Matthew Walker Comprehensive Health center,
where participants received their hematological care. Members of the medical team aided
in identifying families that would be eligible for research participation in advance of their
scheduled clinic appointments. During these routine appointments, familiar medical

26
personnel introduced the study to caregivers. After receiving verbal consent to be
approached by a member of the research team, families were given additional
information and were recruited for participation if interested. During the laboratory-based
study visit, children completed a brief cognitive assessment battery while caregivers
completed a series of questionnaires on family demographics and self-reported social-
environmental stress and parenting stress.
During the study visit, caregiver-child dyads also completed a video recorded
interaction task. As part of the 10-minute task, dyads were asked to work together to
complete a series of 15 tangram puzzles of increasing difficulty. Specifically, participants
were instructed to “talk to each other and ask each other questions in order to solve the
puzzles” as a measure of “how you and your child communicate and solve problems
together.” This direct observation of parenting is derived from similar paradigms used in
previous studies of parenting and cognitive function (e.g., Compas et al. 2010; Deater-
Deckard et al., 2010; Dunn et al., 2011).
Trained graduate and undergraduate students coded all video recordings of parent-
child interactions. All coders were required to pass a written test of code definitions and
examples and to train to 80% reliability on a series of standard recordings that had been
previously recorded by expert raters. Videos of parent-child interactions were double-
coded independently by two coders who then met to discuss scores and reach consensus
when needed. For macro-level IFIRS coding, the higher of two discrepant ratings was
used when coders’ ratings differed by one point. When ratings differed by two or more
points, coders reached agreement through discussion. For micro-level contingency

27
coding, any discrepancy in individually assigned codes was discussed until coders
reached agreement on the assignment of one code.
Measures
Sociodemographic and medical information. Parents provided demographic
information, including age, education level, race, annual family income, and marital
status. Parents gave permission for the research staff to access children’s electronic
medical records, where patients’ hemoglobin level, disease type, stroke status, and
history of acute chest syndrome and emergency department visits were extracted.
Disease-related parenting stress. Caregivers completed the Pediatric Inventory
for Parents (PIP; Streisand, Braniecki, Tercyak & Kazak, 2001; see Appendix A), a 42-
item parent-report questionnaire to assess both frequency and difficulty of disease-related
parenting stress. For each item, caregivers were instructed to use a 5-point Likert scale to
indicate how often an event has occurred (1 = never to 5 = very often) and how difficult
the event has been (1 = not at all to 5 = extremely) during the past seven days. In addition
to separate Frequency and Difficulty Total scores, the PIP also produces scores across
four domains: Communication (e.g., “speaking with my child about his/her illness”),
Emotional Distress (e.g., “seeing my child sad or scared”), Medical Care (e.g., “watching
my child during medical visits/procedures”), and Role Function (e.g., “having
money/financial troubles”). For the purpose of the present study, only difficulty scores
were used as difficulty with an event is believed to be a better indicator of perceived
stress than the frequency of the event. Adequate validity and internal consistency have
been previously demonstrated (α = 0.80 - 0.96) (Streisand et al., 2001). Internal
consistency in the present sample was α = 0.96.

28
General perceived stress. Caregivers also completed the Perceived Stress Scale
(PSS; Cohen, Kamarck & Mermelstein, 1983; see Appendix B), a brief, 10-item measure
of the degree to which non-specific situations in one’s life are appraised as stressful,
particularly with regard to predictability and controllability. For each item, caregivers are
instructed to use a 5-point Likert scale (0 = never, 4 = very often) to rate how often they
have experienced certain feelings and thoughts (e.g., “how often have you felt confident
about your ability to handle your personal problems”; “how often have you felt
difficulties were piling up so high that you could not overcome them”) within the last
month. Internal consistency in the present sample was α = 0.69.
Intellectual functioning. Children with SCD completed the Wechsler
Abbreviated Scale of Intelligence, Second Edition (WASI-II; Wechsler & Hsiao-pin,
2011). The WASI-II is widely used to assess intelligence in children and adults. The
measure consists of four subtests: Block Design, Vocabulary, Matrix Reasoning, and
Similarities. The total combined performance on these subtests is used to generate the
Full-Scale Intelligence Quotient (FSIQ), a broad estimate of general intellectual ability. It
is also possible to interpret subtest scores based on specific components of intelligence
including verbal intelligence and non-verbal intelligence. The Verbal Comprehension
Index (VCI) is comprised of the Vocabulary and Similarities subtests and is designed to
measure verbal comprehension. The Perceptual Reasoning Index (PRI), comprised of the
Block Design and Matrix Reasoning subtests, is intended to assess non-verbal intellectual
abilities, specifically perceptual organization of visual stimuli.
Working memory. In order to assess a core indicator of executive function,
children were also administered two subtests that make up the Working Memory Index

29
(WMI) from the Wechsler Intelligence Scale for Children, Fourth Edition (WISC-IV;
Wechsler, 2003). The WISC-IV is the benchmark test used to assess intelligence in
children. The WMI, composed of the Digit Span and Letter-Number Sequencing subtests,
is a measure of the ability to concentrate, sustain attention, and exert mental control, a
skillset that comprises one of the core areas of executive function (Miyake & Friedman,
2012).
Academic achievement. Children also completed the Wide Range Achievement
Test, Fourth Edition (WRAT4; Wilkinson & Robertson, 2006). The WRAT4 is a widely
used assessment of the fundamental academic skills of reading, spelling and math in
children and adults. The measure includes four brief subtests: Word Reading, Sentence
Comprehension, Spelling and Math Computation. The test produces five derived standard
scores: one for each of the four subtests as well as a Reading Composite score, which is a
combination of examinees’ performance on the Word Reading and Sentence
Comprehension subtests.
Observed parenting. The video-recorded interactions between caregivers and
children with SCD were quantified using macro- and micro-level coding of caregivers’
parenting behavior and communication. The coding systems used at each level are
described in greater detail below.
(1) Macro-level. The Iowa Family Interaction Rating Scales (IFIRS) is a macro-
level coding system used to code caregivers’ verbal and non-verbal communication,
behaviors, and emotions in a videotaped interaction (Melby & Conger, 2001). Codes are
assigned values from 1 to 9, with 1 reflecting the absence of the behavior or emotion and
9 indicating a behavior or emotion is “mainly characteristic” of the caregiver during the

30
interaction. Twenty-five parenting codes were scored. For the current study, a subset of
16 codes was used to create four composite scores: Responsive Parenting, Warm
Parenting, Withdrawn Parenting and Overinvolved/Intrusive Parenting. See Tables 2a –
2d for code definitions and examples drawn from the IFIRS manual (Melby & Conger,
2001). Responsive Parenting was included to test the a priori hypothesis that this specific
parenting behavior would be related to cognitive function in children with SCD. Warm
Parenting was included post hoc to test the potential interaction between responsive and
warm parenting in predicting children’s cognitive abilities. Withdrawn and
Overinvolved/Intrusive Parenting were also included post hoc to explore the relationship
between other non-responsive parenting behaviors and cognitive function.
The Responsive Parenting composite was derived by summing scores from the
following codes: stimulates cognitive development, encourages independence, listener
responsiveness, communication, and sensitive/child-centered (Table 2a). Bivariate
Pearson intercorrelations for the individual codes included in this composite were all
significant at the p < .05 level and ranged from r = 0.33 to r = 0.71 (M = 0.57); see Table
10 in Appendix C for summary. The Warm Parenting composite was derived by
summing scores from the following codes: warmth/support, pro-social, and positive
mood (Table 2b). Bivariate Pearson intercorrelations for the individual codes included in
this composite were all significant at the p < .05 level and ranged from r = 0.37 to r =
0.67 (M = 0.49); see Table 11 in Appendix C for summary. Both the Responsive and
Warm Parenting composites were adapted based on a similar aggregation of IFIRS codes
used in previous research to assess responsive parenting behaviors among parents with a

31
history of depression (Watson et al., 2014). Internal consistency for the Responsive and
Warm Parenting composites were α = 0.87 and α = 0.74, respectively.
Based on previous research (Gruhn et al., 2016), a Withdrawn Parenting
composite was derived by summing scores from the following codes: externalized
negative, avoidant, indulgent/permissive, and inconsistent discipline (Table 2c).
Collectively, these codes capture parenting behaviors that are unresponsive to children’s
needs. Bivariate Pearson intercorrelations for the individual codes included in this
composite were all significant at the p < .05 level and ranged from r = 0.50 to r = 0.89 (M
= 0.70); see Table 12 in Appendix C for summary. Internal consistency for the composite
was α = 0.75.
Finally, an Overinvolved/Intrusive Parenting composite was derived by summing
scores from the following codes: parental influence, intrusive, and lecture/moralize
(Table 2d). This composite was adapted based on a similar aggregation of IFIRS codes
previously used in research with adolescents with type 1 diabetes (Gruhn, Lord & Jaser,
2016) to capture specific parenting behaviors that are more controlling and less
collaborative in nature. Bivariate Pearson intercorrelations for the individual codes
included in this composite ranged from r = 0.23 to r = 0.25 (M = 0.24); see Table 13 in
Appendix C for summary. Internal consistency for the composite was α = 0.43. Given the
non-significant relationship between included codes and poor internal consistency, this
composite score was not used in subsequent analyses.
(2) Micro-level. The Contingency Coding System (CSS) is a micro-level coding
system used to code caregivers’ conversational discourse with their children
(Contingency Coding Manual; Rodriguez, Zuckerman, Saylor, Schuele & Compas,

32
2011). Caregivers and children’s speech during the interaction task was transcribed and
divided into utterances. An utterance is defined as “a unit of speech with complete
semantic and syntactic content” (McLaughlin, Schutz, & White, 1980). The first two
parent utterances following each utterance by the child were coded and percentages of
each code were calculated out of the total number of coded utterances. Each utterance
received a topic maintenance code (i.e., whether the caregiver “maintained” or “changed”
the topic of conversation) as well as one of the following contingency codes: reflection,
expansion, reframe, solicit, provision of information, disclosure, imperative, validation,
or other (see Table 3 for code definitions and examples). Parent utterances after child
utterances that were non-verbal or lacked sufficient content were coded as uncodeable
and were excluded from the present analyses. Although micro-level codes have not been
used previously to create composites of responsive parenting, parents’ use of more
maintains, reflections, expansions, and validations and fewer imperatives were predicted
to be most reflective of responsive parenting based on prior use of the CSS to capture
micro-level parenting in pediatric populations (e.g., Murphy et al., 2016; Rodriguez et al.,
2013).2
Data Analytic Strategy
The collective impact of sociodemographic and disease risk factors were
examined with two cumulative risk (CR) variables. Based on an approach described by
Bemis et al. (2015), each sociodemographic variable was dichotomized such that
participants received a score of 0 or 1, indicating lesser or greater risk: caregiver
partnered (0) versus single (1); annual family income > $25,000 (0) versus ≤ $25,000 (1);
2Supplemental bivariate correlational analyses were run to examine the intercorrelation of individual micro-level parenting codes (see Table 14, Appendix C). The results did not provide sufficient evidence for the creation of a composite and supported the use of individual codes in the following analyses.

33
and caregiver education level > 12th grade (0) versus ≤ 12th grade (1). The cutoff for
annual family income was chosen to best approximate those above versus below the
poverty line for a family of four with two children (US$24,036 according to 2015 census
data). The education level cutoff was chosen following guidelines set by previous CR
research (e.g., Brody et al., 2013). The sociodemographic CR variable is the sum of
scores across these three dichotomized measures, with CR scores ranging from 0 to 3.
A similar approach was used to aggregate illness-related risk factors into a single
CR variable to demonstrate SCD disease severity: no history of stroke (0) versus prior
stroke event (1); no history of acute chest syndrome (0) versus prior acute chest event (1);
hemoglobin level > 9.45 g/dL (0) versus < 9.45 g/dL (1) at most recent clinic
appointment; and no visits to the emergency department (0) versus 1 or more visits to the
emergency department (1) within the last year. These specific risk factors and cutoffs
were chosen based on guidelines from previous research assessing pediatric SCD disease
severity with multiple indicators (Logan, Radcliffe & Smith-Whitley, 2002; Tweel et al.,
2010) and availability of data in participants’ medical records. The disease CR variable
represents the sum of each participants score across these four dichotomized measures,
with CR scores ranging from 0 to 4.
Means and standard deviations of children’s scores on cognitive function
measures including the WASI-II, WISC-IV and WRAT4 were calculated. Additionally,
one sample t-tests were used to compare pediatric SCD patients’ performance on these
measures to that of the normative sample presented for each test to examine how children
with SCD function cognitively in comparison to same-age peers. Means and standard
deviations were also used to determine the caregiver sample’s level of reported parent

34
stress. A series of Pearson bivariate correlations were also calculated to determine
associations between cumulative sociodemographic and disease risk (described above),
parent stress (reported on the PIP and PSS), observed parenting behaviors (coded at the
macro- and micro-levels), and measures of children’s cognitive function. Bivariate
correlations were conducted to allow for an evaluation of the associations between
variables before examining these associations in the multivariate regression analyses, in
part to identify possible suppressor effects that can emerge in regression analyses.
Finally, the unique impact of parent stress and parenting behaviors on children’s
cognitive function were evaluated using a series of linear multiple regression analyses.
To account and control for disease-related and sociodemographic factors, indicators of
cumulative risk were entered in Step 1 of each model. In Step 2, caregivers’ scores on
self-reported measures of general perceived stress (PSS) and disease-related parenting
stress (PIP) were entered. Finally, observed parenting behavior ratings were entered in
Step 3. This ordering of independent variables represents a progression from predictors
that are physically and psychologically distal to the dependent variables (that is, measures
of cognitive function in children with SCD) to those that are most proximal as depicted
by the model in Figure 1. Regression analyses were repeated for each dependent
cognitive function variable (i.e., IQ, working memory, and academic achievement).
All statistical analyses were conducted using IBM SPSS Statistics (Version 24). A
series of power analyses were performed using G Power (Faul, Erdfelder, Lang &
Buchner, 2007) to determine the minimal detectable effect size. Given an alpha of .05,
and a sample size of 48 participants, the current study has an 80% probability of detecting

35
an effect size of d = .41 or greater for one sample t-tests and r = .39 or greater for
bivariate correlations.
36
CHAPTER III
RESULTS
Preliminary Analyses
On the sociodemographic CR measure, 28.3% of parents had zero risk factors,
21.7% had one risk factor, 43.5% had two risk factors, and 6.5% had three risk factors.
On the disease CR measure, 12.5% of children had zero risk factors, 27.1% had one risk
factor, 22.9% had two risk factors, 35.4% had three risk factors, and 2.1% had four risk
factors. The association between cumulative sociodemographic and disease risk (r =
0.20) was not statistically significant.
With regard to the two domains of parent stress (general and disease-related),
caregivers’ mean PSS Total score was 14.42 (SD = 6.98) while their mean PIP Total
scores was 84.39 (SD = 36.59). Additionally, a series of exploratory bivariate correlation
analyses were conducted to examine the association between the two domains of parent
stress used in the current study. Scores on the PSS were significantly positively correlated
with all subscale scores on the PIP, including communication (r = 0.54, p < .001),
medical care (r = 0.57, p < .001), emotional distress (r = 0.56, p < .001), role function (r
= 0.60, p < .001), and total difficulty (r = 0.61, p < .001), such that parents who reported
higher levels of general perceived stress also reported elevated levels of disease-related
parent stress.
Similarly, a series of exploratory bivariate analyses were run to examine the
association between the two levels (micro and macro) of observed parenting behaviors
used in the current study. Results are presented in Table 4. As described in the Method

37
section, composite codes were created using macro-level codes from the IFIRS (i.e.,
responsive, warm and withdrawn parenting), while micro-level codes from the CCS were
analyzed as individual variables. Macro-level responsive parenting and warm parenting
were each positively correlated with micro-level solicits (r = 0.32 and r = 0.31, p < .05;
respectively) and validations (r = 0.57 and r = 0.46, p < .001; respectively), and were
negatively associated with micro-level provisions of information (r = -0.30 and r = -0.31,
p < .05; respectively). In contrast, parents who exhibited more withdrawn parenting at the
macro-level used significantly fewer topic maintenances (r = -0.33, p < .05) and more
imperatives (r = 0.30, p < .05) at the micro-level.
Comparison of Means
Child cognitive function. Mean scores, standard deviations, and results of one-
sample t-tests of children’s cognitive functioning are reported in Table 5. When
compared to the normative sample of same-age peers on measures of cognitive function,
children with SCD significantly underperformed on nearly all domains of intelligence,
working memory, and academic achievement. Specifically, children’s mean scores were
significantly lower than the standardized mean of 100 on indices measuring verbal
comprehension (M = 94.00, SD = 12.50), perceptual reasoning (M = 90.85, SD = 12.12),
full scale IQ (M = 91.56, SD = 10.98)3, working memory (M = 93.65, SD = 14.58), math
(M = 93.83, SD = 13.65), sentence completion (M = 92.83, SD = 15.34), and reading (M
= 93.98, SD = 14.43). Significant Cohen’s d effect sizes ranged from d = -0.41 to -0.67,
indicating a medium effect on average. Children’s scores on spelling and word reading
(both within the domain of academic achievement) were not significantly different from
3 Significant impairment was observed across all three scales of the WASI-II (VCI, PRI, FSIQ). Given that full scale IQ reflects combined performance across both verbal comprehension and perceptual reasoning indices, only FSIQ was used as an indicator of overall intelligence in the following analyses.

38
standardized norms.4
Bivariate Correlational Analyses
Sociodemographic risk, disease risk and parent stress. Bivariate analyses
examining associations of exposure to sociodemographic and disease risk to both general
and illness-related parent stress are presented in Table 6. Parents experiencing greater
cumulative sociodemographic risk reported significantly higher levels of general
perceived stress as measured with the PSS (r = 0.46, p < .01). In contrast, child illness
severity, as represented by the cumulative disease risk variable, was not significantly
correlated with disease-related parenting stress on any subscales of the PIP. However, it
is noteworthy that cumulative disease risk was significantly correlated with the PSS (r =
0.34, p < .05), such that parents of children with greater disease burden reported higher
levels of general stress.
Parent stress and child cognitive function. Bivariate analyses examining
associations of general and disease-related parent stress to cognitive function in children
with SCD are also presented in Table 6. Scores on the PSS were significantly negatively
correlated with children’s Reading Composite scores (r = -0.34, p < .05), meaning that
parent reports of greater general stress are associated with poorer reading ability in
children with SCD. There were no significant associations between PSS scores and other
domains of cognitive function, including intellectual ability and working memory.
The relationship between the PIP and measures of cognitive function varied by
subscales of disease-related parenting stress. Specifically, all subscales of the PIP were
significantly negatively correlated with children’s Reading Composite scores (r = -0.30 to
4 For the purpose of data reduction, scores on Word Reading and Sentence Completion from the WRAT4 were not used in the following analyses; the composite of these scores (Reading Composite) was used instead.

39
r = -0.43, p < .05). The Medical Care subscale of the PIP was also significantly
negatively correlated with working memory on the WISC-IV (r = -0.40, p < .01) as well
as with Spelling on the WRAT4 (r = -0.36, p < .05), such that parent report of greater
difficulty related to managing their child’s medical care was were associated with lower
working memory and spelling scores in children; this relationship also approached
significance for full scale IQ and math achievement. The correlations between the
Emotional Distress and Role Function subscales of the PIP and children’s Working
Memory approached significance (r = -0.22, p < .10). There were no significant
associations between any subscales of the PIP and full scale IQ.
Parent stress and observed parenting. Bivariate analyses examining the
correlations between parent stress and observed parenting are presented in Table 7. With
regard to general perceived stress, scores on the PSS were significantly negatively
correlated with micro-level imperatives (r = -0.40, p < .01), such that parents who
reported greater general stress utilized fewer direct commands in interactions with their
children. Scores on the PSS were not related to other micro-level or macro-level codes.
With regard to disease-related parent stress, Total scores on the PIP were significantly
negatively correlated with micro-level topic maintenance codes (r = -0.27, p < .05), such
that parent who reported greater levels of disease-related stress used fewer utterances that
maintained the topic of conversation in interactions with their children. This pattern was
also observed across several subscales of the PIP, including Communication (r = -0.24, p
< .05), Emotional Distress (r = -0.25, p < .05), and Role Function (r = -0.27, p < .05).
Parent stress was not related to any other type of micro-level parenting from the CCS.
Additionally, Medical Care (r = -0.30, p < .05), Role Function (r = -0.29, p < .05)

40
and Total (r = -0.24, p < .05) disease-related parent stress on the PIP were significantly
negatively associated with macro-level Responsive Parenting behaviors from the IFIRS;
parents who reported greater stress in these domains demonstrated less responsive
parenting during interactions with their children. In contrast, caregivers who reported
more Emotional Distress on the PIP exhibited significantly more Withdrawn Parenting (r
= 0.24, p < .05) at the macro-level.
Observed parenting and child cognitive function. The relationship between
parenting and cognitive function in children with SCD varied as a function of the type of
observed parent behavior (see Table 8). Specifically, macro-level Responsive Parenting
was significantly positively correlated with children’s math (r = 0.25, p < .05) and
reading (r = 0.27, p < .05) scores on a standardized measure of academic achievement5.
In contrast, the correlations approached significance for Withdrawn Parenting with
children’s academic skills in spelling (r = -0.18, p < .10), math (r = -0.24, p < .10), and
reading (r = -0.19, p < .10). At the micro-level, parents’ use of expansions in response to
their children’s utterances was significantly positively related with children’s score across
a range of cognitive function domains including full scale IQ (r = 0.35, p < .05), working
memory (r = 0.37, p < .05), and academic skills related to spelling (r = 0.29, p < .05) and
reading (r = 0.26, p < .05). It is noteworthy that parents’ use of reflective utterances at the
micro-level approached significance for negative associations with children’s academic
achievement in spelling (r = -0.21, p < .10), math (r = -0.19, p < .10), and reading (r = -
0.18, p < .10).
Multivariate Regression Analyses
5Post hoc analyses to test the interaction between Responsive and Warm Parenting in their relationship to cognitive function in children were all non-significant.

41
Multiple regression analyses were used to predict cognitive function in children
with SCD from sociodemographic and disease risk (Step 1), general and disease-related
parent stress (Step 2), and indicators of observed parenting behaviors at the macro- and
micro-levels (Step 3). In the final step, Responsive Parenting and Expansions were
included as indicators of macro- and micro-level parenting, respectively, based on their
significant relationship with child cognitive function as confirmed by the preceding
bivariate analyses. Each model was run twice: first with the PIP Total score as a global
indicator of disease-related stress, and again including the Medical Care subscale score
from the PIP to determine the associations with this specific domain of parent stress. In
general, using a specific indicator of parent stress (i.e., PIP Medical Care Difficulty)
provided more information about the effect of stress on children’s cognitive function than
using a more global indicator (i.e., PIP Total Difficulty). Thus, only those results from
regressions run using the Medical Care score were included in Table 9. For more
information regarding the effect of including the PIP Total to predict cognitive function,
please see Table 16 in Appendix C.
As shown in Table 9, neither sociodemographic nor disease risk emerged as
significant predictors in any step of the linear regressions for children’s cognitive
function. In the model predicting full scale IQ, parent disease-related stress (ß = -0.46, p
< .05) emerged as a significant predictor in Step 2, but was no longer significant (ß = -
0.36, p < .10) when parenting behaviors were added to the model in Step 3. In the final
step, parents’ use of micro-level expansions significantly predicted full scale IQ (ß =

42
0.35, p < .05)6. A similar pattern occurred in the regression model predicting children’s
working memory ability: parent disease-related stress emerged as a significant predictor
in Step 2 (ß = -0.43, p < .05), but was no longer significant in Step 3 (ß = -0.34, p < .10),
whereas micro-level expansions were a significant predictor (ß = 0.40, p < .05). This final
model explained 35% of the total variance in working memory ability in children with
SCD, F(6, 35) = 2.59, p < .05. The same pattern occurred in the regression model
predicting reading achievement: parent disease-related stress emerged as a significant
predictor in Step 2 (ß = -0.45, p < .05), but was no longer significant in Step 3, whereas
micro-level expansions were a significant predictor (ß = 0.37, p < .05). This final model
explained 39% of the total variance in children’s reading skills, F(6, 34) = 3.01, p < .05.
A different set of patterns emerged in the linear regression models predicting
children’s spelling and math. As observed in the previous set of regressions, neither
sociodemographic nor disease risk emerged as significant predictors in any step, while
parent disease-related stress emerged as a significant predictor in Step 2 (ß = -0.47 and
-0.44, p < .05). When parenting was added in the final step, none of the included
independent variables served as significant predictors of children’s academic
achievement.
6 Post hoc regression analyses were also conducted to test for unique patterns among the two subscales that constitute full scale IQ (Verbal Comprehension and Perceptual Reasoning). For a summary of findings, please see Table 15 and Table 16 in Appendix C.

43
CHAPTER IV
DISCUSSION
There is strong evidence that children with sickle cell disease are at risk for
significant impairments in intellectual ability, executive function and academic
achievement (e.g. King et al., 2014; Schatz et al., 2002). Efforts to better understand the
underlying cause of these deficits have focused on the direct effect of disease-related
factors on cognition; however, disease characteristics only account for a portion of the
variance in children’s cognitive performance. In order to account for the additional
impact of distal environmental factors on cognitive function in children with SCD, it is
important to consider the role of the caregiver as one of the most salient proximal factors
impacting the course of cognitive development in offspring. In particular, caregivers of
children with SCD may be unique in their exposure to two distinct areas of parenting
hardship (i.e. sociodemographic disadvantage and chronic health problems in children),
and may experience significant stress that impairs the ability to provide responsive,
cognitively stimulating parenting to this population of vulnerable, high risk children.
Thus, the purpose of the present study was to extend the existing literature on
stress, parenting, and cognitive function, and to unite these concepts in the context of
pediatric sickle cell disease. This study is the first of its kind to integrate research on the
combined association of sociodemographic and medical care burden with parent
functioning, and, subsequently, to explore how parenting is related to cognitive
performance in a group of children also at risk for significant deficits in functioning. In

44
doing so, this research aims to provide direction for future efforts to assist children with
SCD and their families.
Summary of Findings and Interpretations
The first aim of the current study was to replicate previous findings which
demonstrate that children with SCD experience deficits in cognitive function compared to
same-age peers (e.g., Schatz et al., 2002). Indeed, children with SCD in the current
sample significantly underperformed relative to normative data on measures assessing
intelligence (WASI-II), executive function (WISC-IV), and academic achievement
(WRAT4). Specifically, on the WASI-II, children scored significantly lower than
national norms on the Verbal Comprehension Index, the Perceptual Reasoning Index, and
Full-Scale IQ, with the range of effect sizes representing a medium effect. Children’s
mean score on the Working Memory Index of the WISC-IV was also significantly lower
than the normative sample mean, representing a notable deficit in ability in this core
domain of executive function. Similarly, children with SCD in the present sample also
demonstrated significant difficulty in several domains of academic achievement,
including math and reading. Collectively, these results replicate previous findings,
provide new evidence for observed deficits across multiple indices of cognitive function
in pediatric SCD patients, and further highlight the magnitude of the problem faced by
this population.
The second aim of the current study was to determine the relationship between
children’s disease characteristics, caregivers’ sociodemographic disadvantage, and parent
stress. Preliminary analyses reveal that characteristics of this sample corroborate previous
work demonstrating the multiple challenges faced by children with SCD and their

45
parents. With regard to sociodemographic risk factors, 40% of caregivers had annual
family incomes of $25,000 or less, 52% were single parents (i.e., single, divorced, or
separated), and had, on average, 13 years of formal education (i.e., one year post-
secondary). When assessed cumulatively, results showed that 50% of parents endorsed
exposure to multiple of these risk factors. With regard to disease-related risk factors, over
70% of children in the current sample presented with a diagnosis of HbSS, typically
regarded as the most severe type of SCD (Ashley-Kock, Yang & Olney, 2000). A closer
examination of more specific indicators of disease severity revealed that 23% of children
had a history of stroke, 52% had a history of acute chest syndrome, and nearly half of all
children had made an SCD-related visit to the emergency department in the year prior to
study enrollment. When assessed cumulatively, results showed that more than 60% of
children had experienced multiple of these disease-related risk factors. Thus, as supported
by Bemis et al. (2015), utilization of a multiple, cumulative-risk framework shows that
both children and parents in the current sample are exposed to an accumulation of
stressors that are chronic in nature, demonstrating the unique vulnerability afflicting
caregivers of youth with SCD.
Despite this evidence for significant exposure to sociodemographic and disease-
related stressors, past studies have failed to incorporate self-reported assessments of
caregivers’ perception of these burdens as subjectively stressful. In the current study,
parents of children with SCD provided self-reports of both their general perceived stress
(PSS) and stress related to parenting a chronically ill child (PIP). Descriptive analyses
showed that, on average, participants reported a moderate level of general stress on the
PSS (Cohen, Kamarck & Mermelstein, 1983). Further, total scores on the PIP were

46
comparable to those obtained from previous studies of parents of youth with SCD
(Barakat, Patterson, Tarazi & Ely, 2007; Logan, Radcliffe & Smith-Whitley, 2002).
Results from a series of correlational analyses showed that parents with greater
cumulative sociodemographic risk reported experiencing greater general stress on the
PSS. Greater cumulative disease risk was also related to higher levels of parents’ general
stress, but to a lesser degree than was sociodemographic risk. Interestingly, disease risk
was not related to greater disease-related stress on the PIP, a finding which is inconsistent
with past research demonstrating a link between SCD illness parameters and parent stress
(e.g., Barakat et al., 2007). This suggests that while disease-related parenting stress may
be an important indicator of parent functioning and its relation to child functioning
(further discussion below), the PSS as a measure of general stress that is not specifically
related to parenting may provide a clearer picture of how caregivers perceive the
experience of managing not only sociodemographic disadvantage, but also their child’s
illness.
The third, and perhaps most important, aim of the current study was to determine
the relationship between parent factors (specifically, parent stress and parenting
behaviors) and cognitive function in children with SCD. In examining the link between
parent stress and cognitive function, two key findings emerged. First, both general stress
on the PSS and disease-related parent stress on the PIP are significantly correlated with
children’s reading achievement on the WRAT4, such that the children of parents who
reported higher levels of stress scored lower on a standardized test of reading skills. In an
interesting contrast, both types of parent stress were unrelated to overall intelligence as
measured by the WASI-II, with the exception of the PIP Medical Care domain which

47
approached significance with overall intelligence. While both the WASI-II and WRAT4
attempt to capture aspects of an individual’s verbal functioning, the measures are distinct
in that the WASI-II is primarily concerned with underlying intellectual ability, whereas
the WRAT4, a test of achievement, is primarily concerned with the acquisition of
information and mastery of a learned skillset. Thus, this pattern of findings may
demonstrate the differential effect of parent stress on children’s achieved learning versus
their capacity for learning, highlighting a potential area for intervention.
Another key finding in examining the relationship between parent stress and
cognitive function in children was that of the parent stress domains assessed, the Medical
Care subscale of the PIP was the most consistently related to cognitive function in
pediatric SCD patients. Specifically, of the five correlations tested for this subscale of the
PIP with measures of children’s cognitive functioning and achievement, three were
statistically significant (working memory, spelling achievement, and reading
achievement) and two approached significance (full scale IQ and math achievement).
This pattern demonstrates the pervasiveness of an ill child’s medical care on parent
functioning and its impact across multiple domains of child cognitive performance.
Compared to other subscales of the PIP that capture more broad examples of parenting
stress (e.g., difficulty sleeping, feeling helpless, arguing with family), the items that
comprise the Medical Care subscale are specifically designed to measure parenting stress
related to helping with, observing and making decisions about children’s medical
appointments and procedures. In this sense, the Medical Care subscale is the most
medically oriented and context-specific and, consequently, the most sensitive in its ability

48
to detect impaired interactions between a parent and an ill child (in comparison to a
parent and a healthy sibling or a parent and a spouse, for example).
An examination of the association between self-reported parent stress and
observed parenting behaviors produced mixed findings. Caregivers who reported more
disease-related stress on the PIP exhibited significantly fewer Responsive Parenting
behaviors and a trend towards more nonresponsive parenting behaviors (i.e., Withdrawn
Parenting) at the macro-level. In the current study, Responsive Parenting was
characterized by parenting that prioritizes awareness of and sensitivity to children’s
needs; balances active listening with communication of new ideas; encourages
independence that is matched to children’s abilities; and uses cognitive stimulation to
enhance children’s thinking and learning. In contrast, Withdrawn Parenting was used as
an indicator of nonresponsive parenting and was characterized by negativity and criticism
towards the task; avoidance; inconsistency; and independence and freedom that is
inappropriately matched to children’s abilities.
At the micro-level, greater disease-related stress on the PIP was related to fewer
instances of parent topic maintenance. An utterance is coded as a Maintain if the parent
continues the topic of the preceding child utterance and/or develops the general topic of
conversation as opposed to completely changing the topic of conversation by deflecting
or redirecting from the child’s previous utterance(s). Effective topic maintenance requires
caregivers to track the course of the conversation and provide a response or set of
responses that reflect at least a portion of the child’s contribution, an ability that is
consistent with responsive parenting. Taken together, these findings provide evidence for

49
the negative impact of parent stress on parent-child interactions, specifically with regard
to problem solving and collaboration on a cognitively demanding task.
The final set of bivariate correlational analyses examined the relationship between
observed parenting and cognitive function in children with SCD. Although many of the
parenting behaviors measured in the current study were unrelated to child cognitive
function, two key findings did emerge. First, as hypothesized, the composite of macro-
level Responsive Parenting was related to children’s academic achievement. Specifically,
children whose caregivers demonstrated responsiveness in a brief parent-child interaction
scored significantly higher on tests of math and reading achievement. Second, also as
hypothesized, at the micro level of analysis, parents’ use of Expansions was related to
children’s performance across all cognitive domains including general intellectual
functioning (IQ), working memory, and academic achievement. An Expansion is a
complex, two-step discourse strategy that requires caregivers to first repeat some or all of
the child’s preceding utterance and then provide additional content. As such, expansive
language inherently incorporates aspects of other micro-level codes including
Reflections, Validations and Provisions of Information, and would take precedence over
these codes in the coding process. Thus some, but not all, specific parenting behaviors
(i.e., responsive parenting and expansive language) appear to be linked to cognitive
performance in pediatric SCD patients, highlighting concrete, teachable parenting skills
as potential targets for intervention.
While correlational analyses were essential in elucidating the magnitude and
direction of the bivariate relationships between the variables of interest (i.e.,
sociodemographic and disease risk, general and disease-related parent stress, and micro-

50
and macro-level parenting behaviors), the multivariate regression analyses informed the
most important take-home messages of the current study. First, there were differences in
the degree to which the two types of parent stress accounted for variance in cognitive
function in children with SCD. Specifically, when both general perceived stress on the
PSS and Medical Care-related stress on the PIP were added as independent predictors
after accounting for sociodemographic status and disease severity, parents’ disease-
related stress was a significant and consistent predictor of children’s intellectual ability,
working memory, and academic achievement. In contrast, parents’ general stress did not
account for a significant amount of variance in children’s cognitive performance. This
pattern further underlines the PIP’s robust sensitivity in capturing the interplay between
parent and child functioning.
In the final and most stringent test of the study hypotheses, multivariate
regression analyses also showed that when both macro-level Responsive Parenting and
micro-level Expansions were added as independent predictors in the final step of the
regression models, parent stress was no longer a significant predictor of children’s
cognitive function for all five dependent variables. Additionally, parents’ use of
expansive language emerged as a significant predictor of three dependent variables (full
scale IQ, working memory, and reading achievement). Taken together, these two
outcomes suggest that variance in cognitive performance as a function of parent stress –
which was seen in the previous step of the regression models – is at least partially
accounted for by the relationship between observed parenting behaviors and children’s
cognitive function. More specifically, the relationship between disease-related parent
stress and intelligence, working memory, and reading achievement may be explained, in

51
part, by differences in parents’ use of expansive language under conditions of chronic
stress.
Although parents’ use of micro-level Expansions accounted for greater variance
in children’s cognitive function than did macro-level Responsive Parenting, it is worth
noting that adding both parenting predictors in the final step of the regression analyses
significantly improved the predictive value of the overall model in explaining differences
in working memory and reading achievement. Specifically, the final model (with
cumulative risk, parent stress and parenting included) accounted for 35% and 39% of
variance in children’s working memory and reading achievement scores, respectively.
Strengths of the Current Study
This study is the first of its kind to examine cognitive ability as a function of
biomedical, sociodemographic and parent characteristics, specifically within the context
of pediatric sickle cell disease. Relatively few studies have explored the impact of non-
disease related correlates of cognitive function, and even fewer have emphasized the
potential role of parents and parenting behaviors in explaining differences in cognitive
performance in this high-risk yet understudied population. Emerging evidence has
supported a link between parental characteristics and cognitive problems in children with
SCD (e.g., King et al., 2014, Yarboi et al., 2017), but interpretations from these studies
are limited by a number of conceptual and methodological weaknesses.
In conceptualizing the relationship between sociodemographic disadvantage and
cognitive impairment, previous studies of children with SCD have proposed associations
among financial strain, impaired parenting and cognitive deficits without sufficiently
accounting for the mechanism through which social-environmental burden may impact

52
parent-child interactions and, subsequently, child functioning. By drawing on a
theoretical framework established by Evans and colleagues, which has consistently
incorporated biological and self-reported indicators of actual and perceived stress (e.g.,
Evans, Boxhill & Pinkava, 2008; Evans & Kim, 2007), the current study is strengthened
by explicitly measuring and accounting for parents’ perception of exposure to
sociodemographic and illness factors as subjectively stressful. This approach is also
consistent with Lazarus’s seminal work on stress appraisal (e.g., Lazarus & Folkman,
1984).
Several key strengths of the study sample and methodological design also support
the contribution of the current study to the existing literature. First, the sample contained
a wide range and was relatively heterogeneous with regard to caregivers’
sociodemographic characteristics (including annual income, parent education, and marital
status) as well as children’s disease characteristics (including disease type and history of
stroke), which improves the generalizability of the reported findings. Furthermore, the
current study utilized a more complex and comprehensive method to measure
sociodemographic disadvantage and disease severity than most prior studies with
pediatric populations. The decision to use a cumulative risk approach was supported by
recent evidence that shows that the impact of accumulating stressors and risk factors
exceeds the influence of any singular risk factor in understanding physiological and
psychological processes (e.g., Bemis et al., 2015; Evans & Kim, 2013).
An additional strength of the present study was the use of well-validated, multi-
method measures that assess key study variables across multiple domains. Specifically,
analyses were based on objective medical data, self-report questionnaires, standardized

53
and norm-referenced cognitive data, and direct observation of parenting. Utilizing a
multi-method design has been shown to reduce the potential effect of common method
variance and is widely regarded as the most rigorous methodological approach,
particularly in cross-sectional research (Lindell & Whitney, 2001). In particular, the use
of a direct observation paradigm to measure parenting is a significant improvement from
past research with this population, which has primarily relied on parent and child self-
reports. Furthermore, quantifying parenting across two levels of analysis (i.e., macro and
micro) helps clarify the mechanism of the effect on child functioning and allows for more
specific targets for intervention.
Limitations of the Current Study and Future Directions
Exploring limitations of the current study provides opportunity and direction for
future research on this topic. First, despite recruiting participants from an active pediatric
hospital in a large metropolitan area, the relatively small sample size reflects the
challenge of recruiting and enrolling families who are faced with the chronic burden of
both disease-related and sociodemographic stress. Interestingly, this appears to be a
common difficulty among pediatric SCD researchers (e.g., Barakat, Patterson, Tarazi &
Ely, 2007). When possible, future research on cognitive and psychosocial functioning in
children with SCD and their families would greatly benefit from recruiting participants
across multiple sites or aggregating data across multiple samples to increase sample size
and statistical power.
Given the nature of genetic transmission and that the gene variant for SCD is
protective against malaria infection (Ashley-Koch, Yang & Olney, 2000), SCD is known
to most commonly affect those of African descent. Indeed, 98% of participants in the

54
current sample identified as Black/African-American, which is consistent with past
research. Given that race is highly correlated with exposure to other markers of
sociodemographic disadvantage (e.g., education, employment, income), the proposed
research questions were largely driven by the expectation that the sample would be
demographically representative of a larger population that is historically high-risk, yet
alarmingly understudied. However, this significant skew in distribution might limit the
generalizability of the findings to other more racially diverse patient populations. For
example, some studies have found group differences in parenting practices by race, a
phenomenon that is typically interpreted from a cultural and contextual perspective
(Brody & Flor, 1998). Limited studies have specifically measured responsive parenting
among African American caregivers (e.g., Burchinal, Follmer & Bryant, 1996), and it
remains unclear how the conceptualization and utility of parental responsiveness may
differ by race. Similarly, it is unclear if and how different iterations of responsive
parenting might be related to differential outcomes in child. Thus, there is an opportunity
for future work to explore the relationship between parenting and cognitive function in a
more racially heterogeneous pediatric population.
Third, interpretations of the findings are considerably restricted by the cross-
sectional design of the study. Specifically, temporal precedence was not established and
mediation among key study variables could not be tested, thus limiting any inferences
about causality and direction of effects. This is especially important given emerging
evidence of bi-directionality, which shows that children’s cognitive function (among
other child characteristics) influences the type of parenting they receive (e.g., Tucker-
Drob & Harden, 2012; Wagner et al. 2015). From a bi-directional perspective, a plausible

55
alternative interpretation of the current findings is that children with cognitive difficulties
elicit less expansive conversation and responsiveness from caregivers; over time, this
may disrupt parent-child interactions and result in greater parenting stress. Future work
will benefit from a more thorough assessment of child characteristics embedded within a
longitudinal design in order to better understand the dynamic, transactional relationship
between parent stress, parenting behaviors and cognitive function in children with SCD
across time.
Implications for intervention. Further exploratory research with a revised
methodology as described above may be beneficial to advance this understudied topic
within the field of pediatric psychology, with the long-term goal of identifying concrete,
teachable parenting and coping skills that may improve functioning in this population.
Despite the limitations of the current study design, the results of the present study
do provide early evidence in support of the concurrent development and testing of a
targeted intervention for parents of children with SCD that combines stress management
with parenting skills training. The next steps in this line of research are informed by
recent findings which show that (a) teaching adaptive coping strategies has beneficial
effects on managing caregiver stress and (b) incorporating responsive parenting skills has
beneficial effects on improving cognitive function in low-income families, albeit in
children without SCD (Neville et al., 2013; Raviv & Wadsworth, 2010).
With regard to parent stress, it will be important to synthesize research on
psychological interventions for parents and families coping with a child’s chronic illness
(e.g. Barlow & Ellard, 2004; Kazak, 2005) with interventions to reduce psychosocial
stress in families faced with economic hardship (e.g., Wadsworth et al., 2011). An

56
effective program for caregivers of children with SCD might focus on identifying sources
of stress in parents’ lives and mastering key coping strategies to manage the stress related
to sociodemographic hardship and parenting a child with a chronic illness. Integrating
interventions in these two areas will increase the likelihood of developing a program that
is feasible and efficacious for families dealing with childhood sickle cell disease.
Importantly, an effective program will aim to address elevations in parent stress prior to
teaching adaptive parenting skills.
With regard to parenting skills, evidence from parent skills programs shows that
caregiver behavior is amenable to change (e.g., Scott et al., 2001), making it a potential
avenue for intervention in the case of impaired or compromised cognitive function in
children. In a seminal study with healthy children, Neville et al. (2013) tested the effects
of an 8-week parenting skills intervention aimed at improving cognitive function in
economically disadvantaged children. Children of parents assigned to the training
program demonstrated significantly greater improvements in neural responses to a
selective training task and greater gains in nonverbal IQ and language than children in the
active control group (Head Start alone). Further, parents reported decreased parenting
stress and increased turn-taking in observed conversations with their children. An
effective intervention for parents of children with SCD might specifically focus on
building skills for responsive parenting and scaffolding of a child’s cognitive skills by
incorporating expansive language (i.e., first validating and reflecting the child’s
statement, then expanding on the child’s content with new information).
While more work is needed to replicate findings from the above interventions and
to fully understand the underlying mechanisms of change, existing research with

57
comparable populations presents a novel and promising opportunity to improve outcomes
for both children and parents with SCD. To date, research aimed specifically at
enhancing cognitive function in pediatric SCD has been limited, and has focused
primarily on home-based computerized cognitive training programs such as Cogmed. In a
recent test of the feasibility of Cogmed in children with SCD, Hardy et al. (2016)
observed significant improvements in working memory in participants who completed
the program. However, adherence to the program was poor, with less than half of the
sample completing all 25 training sessions. Importantly, the authors note that certain
socioeconomic and psychosocial variables including parent stressors and daily hassles,
family functioning, and the caregiver’s workload may have influenced the level of
support the child received and, subsequently, the child’s ability to complete the program.
This suggests that incorporating a parent component to increase caregiver responsiveness
and support for children completing a cognitively demanding task may result in greater
adherence to the intervention and more pronounced effects.
Conclusion
The present study utilized a multi-method design with comprehensive and well-
validated measures to replicate and expand on previous research on cognitive
development in children with sickle cell disease to provide evidence for the relationship
between parent and child functioning. Specifically, this work shows that caregivers of
children with SCD are exposed to and report experiencing considerable levels of stress
related both to sociodemographic disadvantage and caring for a child with a chronic
health condition. In turn, parent stress is related to how caregivers interact and
communicate with their children. Preliminary evidence from the integration of two

58
coding systems reveals that parenting behaviors, especially parents’ use of expansive
language, is a reliable and consistent predictor of multiple domains of cognitive function
in children with SCD. These findings demonstrate the need to consider the impact of
parent functioning on cognitive development in this vulnerable population. Furthermore,
findings highlight the need to develop a targeted intervention for parents of children with
SCD that combines stress management with parenting skills training with the aim of
improving functioning in both caregivers and youth.

59
Table 1. Demographic Characteristics of Children and Caregivers in Sample.
Characteristic M SD N % Child age 9.1 3.0 Caregiver age 39.2 9.1 Caregiver education (years) 13.7 1.9 Child gender Female 22 45.8 Male 26 54.2 Child SCD diagnosis HbSS 34 70.8 HbSC 9 18.8 Hb beta-thalassemia 5 10.4 Child history of stroke No stroke 37 77.1 Stroke 11 22.9 Caregiver gender Female 38 79.2 Male 10 20.8 Caregiver relationship to child Biological parent 42 87.5 Adoptive parent 1 2.1 Grandparent 3 6.3 Other 2 4.2 Caregiver marital status Married 22 45.8 Single 15 31.3 Divorced 8 16.7 Separated 2 4.2 Living with someone 1 2.1 Annual family income ≤ $25,000 19 40.4 $25,001 - $50,000 14 29.8 $50,001 - $75,000 7 14.9 $75,001 - $100,000 4 8.5 ≥ $100,001 3 6.4

60
Table 2a. Definitions and Examples of Macro-Level IFIRS Codes in Responsive Parenting Composite. Responsive Parenting Composite Codes
Definition Examples
Stimulates Cognitive Development (SC)
Parent’s use of activities to foster and enhance child’s thinking, achievement, and learning in areas of perceptual, cognitive and linguistic development.
Verbal: “See the rounded corners? Where is there a spot for that?”; “Why don’t you try the edges first? Which piece would go on the ends?”
Encourages Independence (EI)
Parental demonstrations of trust in and encouragement of the child’s independence in thought and actions.
Verbal: “I know you can do it, just give it another try”; “That’s it, you’ll get it done soon.”
Listener Responsiveness (LR)
The parent’s nonverbal and verbal responsiveness as a listener to the verbalizations of the child through behaviors that validate and indicate attentiveness to the child.
Non-verbal: Eye contact, head-nods when child is speaking Verbal: “Yeah, mm-hmm.”
Communication (CO) The parent’s ability to neutrally or positively express his/her own point of view, needs, wants, etc. in a clear, appropriate away, and reasonable manner, and to demonstrate consideration of the child’s point of view. The good communicator promotes rather than inhibits exchange of information.
Verbal: “That is an interesting idea.”
Sensitive/Child Centered (CC)
Parent’s responses to child are appropriate and based on the child’s behavior and speech; they offer the right mix of support and independence so child can experience mastery, success, pride and develop effective self-regulatory skills.
Non-verbal: Managing activity pace, handing child next puzzle piece when ready. Verbal: “You seem frustrated, what’s wrong?”
Positive Reinforcement (PO)
The extent to which the parent responds positively to the child’s appropriate behavior or behavior that meets specific parental standards.
Verbal: “You’re doing such a good job”; “I like how you cleaned up after yourself.”

61
Table 2b. Definitions and Examples of Macro-Level IFIRS Codes in Warm Parenting Composite. Warm Parenting Composite Codes
Definition Examples
Warmth/Support (WM)
Expressions of care, concern, support, or encouragement toward the child.
Non-verbal: Hugs, holding hands, warm smiles Verbal: “You did that well, I’m really proud of you.”
Prosocial (PR) The extent to which the parent relates competently and effectively with the child; it includes demonstrations of cooperation, sensitivity, helpfulness, willingness to change own behavior for the child, and willingness to comply with needs and wishes of the child.
Non-verbal: Focusing on and participating in the task. Verbal: “I’m sorry, I didn’t know that bothered you”; “Thanks for putting away the puzzle pieces”
Positive Mood (PM) The degree to which the parent appears happy and optimistic and/or demonstrates a positive attitude and behavior toward self, the child, and things in general.
Non-verbal: Smiling, laughing, being involved positively in the interaction, animated expressions and gestures Verbal: “This is fun!”; “I’m good at puzzles”; “We can do this!”

62
Table 2c. Definitions and Examples of Macro-Level IFIRS Codes in Withdrawn Parenting Composite. Withdrawn Parenting Composite Codes
Definition Examples
Externalized Negative (EX)
The extent to which the parent displays negativity in the form of complaints or critical comments regarding people, things, or events outside of the interaction task, as well as complaints or negative comments about the task itself.
Verbal: “When is this stupid task going to be over?”; “This is a dumb puzzle”
Avoidant (AV)
The extent to which the parent physically orients self away from the child in such a manner as to avoid interaction.
Non-verbal: Looking down or away in embarrassment.
Indulgent/Permissive (IP)
The extent to which the parent gives the child considerable and often times an inappropriate degree of freedom to regulate or control his/her own behavior; parent is characterized by a “laissez faire,” anything goes attitude and is excessively lenient.
Non-verbal: Child hits mother, mother ignores. Child repeats the behavior, mother does nothing Verbal: “Do what you want to do. You don’t listen to me anyway.”
Inconsistent Discipline (ID)
Parental inconsistency and failure to follow through on an expected consequence or punishment, as well as failure to maintain and adhere to rules and standards of conduct set for the child’s behavior.
Non-verbal: Parent laughs when child fails to obey instructions. Verbal: “Fine, I’ll clean up this time”

63
Table 2d. Definitions and Examples of Macro-Level IFIRS Codes in Overinvolved Parenting Composite. Overinvolved Parenting Composite Codes
Definition Examples
Parental Influence (PI) The parent’s direct and indirect attempts to influence, regulate, or control the child’s life according to commonly accepted, age-appropriate standards.
Verbal: “We always clean up after we play”; “Finish one, then start the next.”
Intrusive (NT) The extent to which the parent is domineering and over-controlling during interactions with their child; parent’s behavior is adult-centered rather than child-centered.
Non-verbal: Taking a puzzle piece from child’s hands. Verbal: “Use this piece instead. Do it now.”
Lecture/Moralize (LM) The degree to which the parent presents information in a didactic, superior-wisdom manner that may be lectury, preachy, intrusive, pushy, and/or moralizing; rather than discuss issues, the parent may simply lecture the child and/or tell him/her how things really are or should be.
Verbal: “You should know better”; “She said do it together”; “You have to help me”

64
Table 3. Definitions and Examples of Micro-Level Contingency Codes. Contingency Code
Definition Examples
Maintains Caregiver continues the topic of the preceding utterance and/or develops the general topic of the conversation.
Child: “This one looks like a tree.” Parent: “What else could it be?”
Non-example:
Child: “This one looks like a tree.” Parent: “I wonder how much time is left.”
Reflections Caregiver repeats some or all of the child’s utterance with no additional content.
Child: “This piece.” Parent: “That piece.”
Reframes Caregiver corrects or disagrees with the child, or states an alternate viewpoint.
Child: “This one looks like a tree.” Parent: “Actually I think it’s supposed to be a giraffe.”
Expansions Caregiver repeats some or all of the child’s utterance but also adds additional content.
Child: “This way.” Parent: “You want to turn it this way?”
Disclosures Caregiver expresses something about his/her own emotional experience.
Child: “I can’t do this.” Parent: “I hate when you’re hard on yourself.”
Solicits Caregiver asks a question in order to elicit a response from the child.
Child: “We did it!” Parent: “Which one should we try next?”
Provisions of Information
Caregiver conveys a fact or opinion to the child.
Child: “What?” Parent: “Now we have to find the square.”
Imperatives Caregiver directs the child to do something or stop doing something.
Child: “That doesn’t look right.” Parent: “Turn that piece around.”
Validations Caregiver confirms, empathizes, or praises the child’s utterance without adding new content.
Child: “The triangle goes there.” Parent: “That’s right.”

65
Table 4. Bivariate Correlations Between Micro- and Macro-Level Observed Parenting Codes.
Micro-Level Codes Macro-Level Composite Codes
Responsive Parenting
Warm Parenting
Withdrawn Parenting
Topic Maintenance .14 -.05 -.33* Reflections .19 .15 .01 Expansions .15 .00 .12 Reframes .03 -.10 .27† Solicits .32* .31* -.16 Disclosures -.03 .18 -.04 Provisions of Information -.30* -.31* .02 Validations .57*** .46*** -.12 Imperatives -.03 -.10 .30*
† p <.10. *p <.05. **p <.01. ***p <.001.
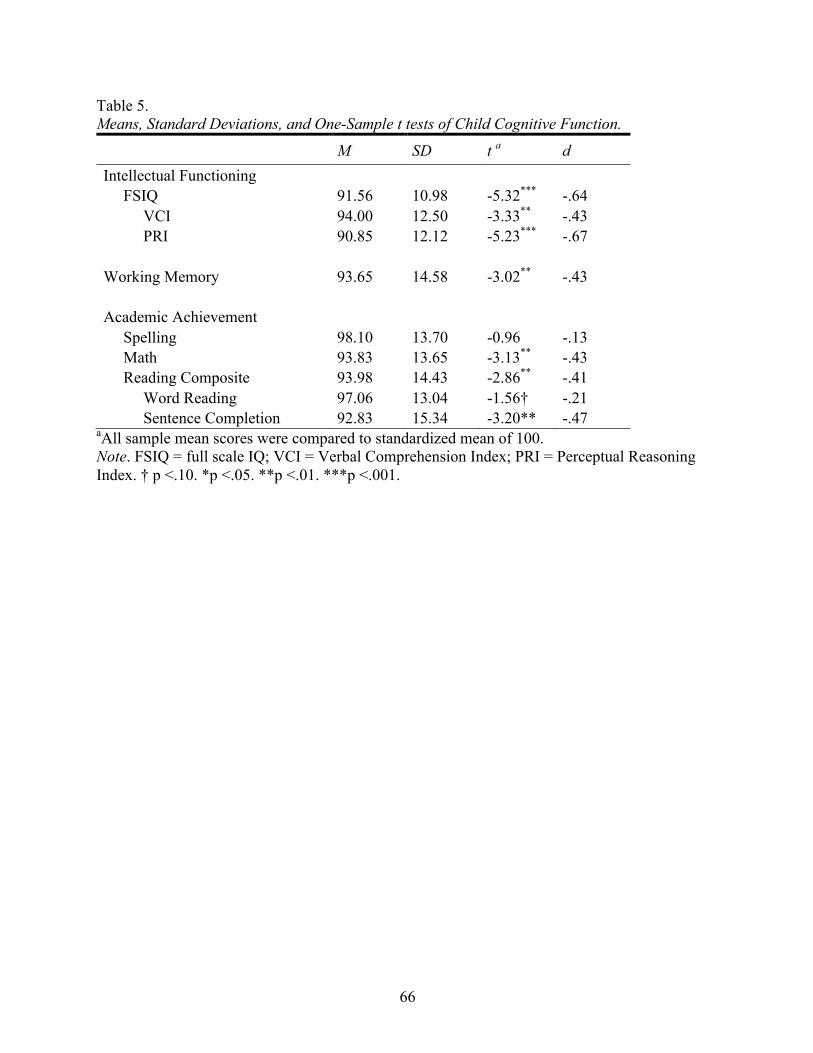
66
Table 5. Means, Standard Deviations, and One-Sample t tests of Child Cognitive Function.
M SD t a d Intellectual Functioning FSIQ 91.56 10.98 -5.32*** -.64 VCI 94.00 12.50 -3.33** -.43 PRI 90.85 12.12 -5.23*** -.67 Working Memory 93.65 14.58 -3.02** -.43 Academic Achievement Spelling 98.10 13.70 -0.96 -.13 Math 93.83 13.65 -3.13** -.43 Reading Composite 93.98 14.43 -2.86** -.41 Word Reading 97.06 13.04 -1.56† -.21 Sentence Completion 92.83 15.34 -3.20** -.47
aAll sample mean scores were compared to standardized mean of 100. Note. FSIQ = full scale IQ; VCI = Verbal Comprehension Index; PRI = Perceptual Reasoning Index. † p <.10. *p <.05. **p <.01. ***p <.001.
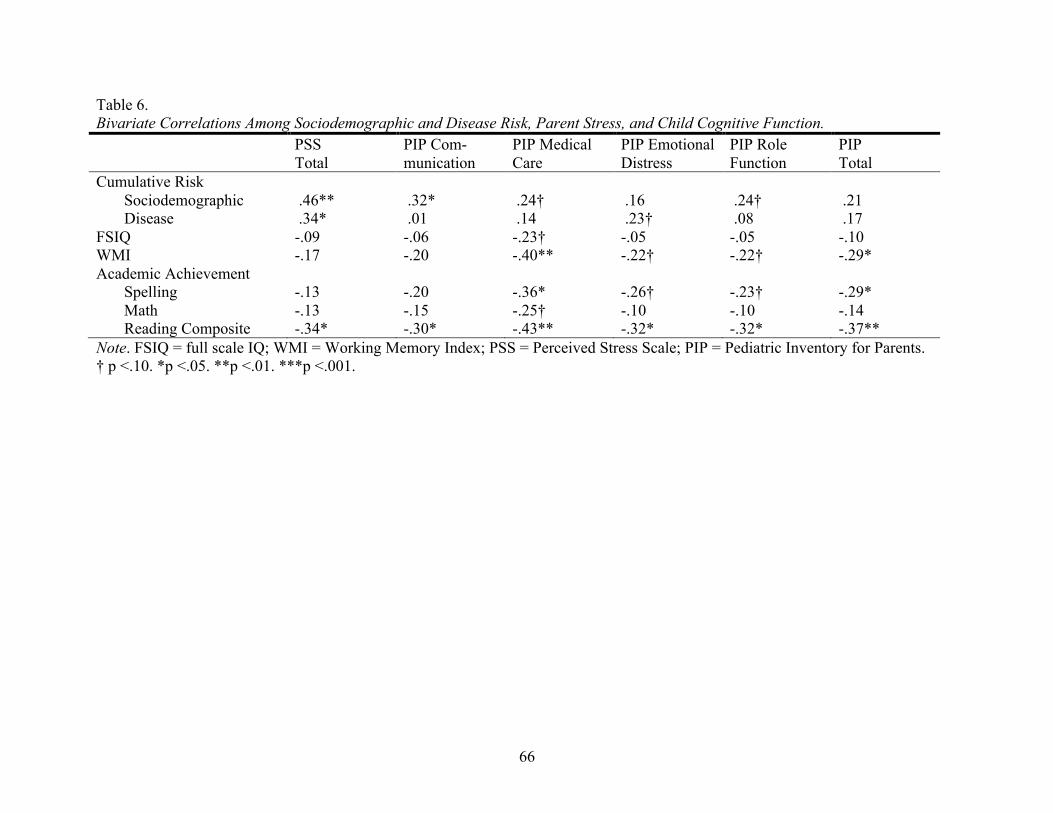
66
Table 6. Bivariate Correlations Among Sociodemographic and Disease Risk, Parent Stress, and Child Cognitive Function. PSS
Total PIP Com- munication
PIP Medical Care
PIP Emotional Distress
PIP Role Function
PIP Total
Cumulative Risk Sociodemographic .46** .32* .24† .16 .24† .21 Disease .34* .01 .14 .23† .08 .17 FSIQ -.09 -.06 -.23† -.05 -.05 -.10 WMI -.17 -.20 -.40** -.22† -.22† -.29* Academic Achievement Spelling -.13 -.20 -.36* -.26† -.23† -.29* Math -.13 -.15 -.25† -.10 -.10 -.14 Reading Composite -.34* -.30* -.43** -.32* -.32* -.37** Note. FSIQ = full scale IQ; WMI = Working Memory Index; PSS = Perceived Stress Scale; PIP = Pediatric Inventory for Parents. † p <.10. *p <.05. **p <.01. ***p <.001.

67
Table 7. Bivariate Correlations Between Parent Stress and Observed Parenting.
Parenting Codes PSS Total
PIP
Communic. Medical Care
Emotional Distress
Role Function Total
Macro-Level Responsive -.07 -.19 -.30* -.17† -.29* -.24* Warm .13 -.12 -.12 -.02 -.17† -.09 Withdrawn .14 .12 .21† .24* .21† .22† Micro-Level Maintains -.07 -.24* -.22† -.25* -.27* -.27* Reflections .25† .01 .11 .07 -.07 .04 Expansions .19† .04 -.15 -.01 .12 -.06 Reframes -.25† -.20† -.17 -.17 -.18† -.18† Solicits .21† .03 .02 -.06 -.13 -.04 Disclosures .10 -.08 -.04 .02 -.06 -.02 Provisions of Info. .03 .04 .10 .17 .23† .16 Validations .22† .03 -.06 .06 -.02 .01 Imperatives -.40** -.14 -.08 -.14 -.15 -.13
Note. PSS = Perceived Stress Scale; PIP = Pediatric Inventory for Parents. † p <.10. *p <.05. **p <.01. ***p <.001.

68
Table 8. Bivariate Correlations Between Observed Parenting and Child Cognitive Function.
Parenting Codes FSIQ WMI Spelling Math Reading Composite
Macro-Level Responsive .16 .11 .15 .25* .27* Warm .04 -.08 .12 .07 .23† Withdrawn -.06 -.14 -.18† -.24† -.19† Micro-Level Maintains -.17† -.01 -.04 .09 .01 Reflections -.15 -.16 -.21† -.19† -.18† Expansions .35* .37* .29* .16 .26* Reframes .01 .08 .10 -.04 .11 Solicits .19† .22† .15 .13 .12 Disclosures .11 .00 -.04 .08 .13 Provisions of Info. -.09 -.20† -.11 -.09 -.12 Validations .08 -.11 .02 .06 .01 Imperatives .09 .02 .02 -.07 .04
Note. FSIQ = full scale IQ; WMI = Working Memory Index. † p <.10. *p <.05. **p <.01. ***p <.001.

69
Table 9. Summary of Linear Regression Analyses for Variables Predicting Child Cognitive Function.
aMacro-level. bMicro-level. Note. CR = cumulative risk; PSS = Perceived Stress Scale; PIP = Pediatric Inventory for Parents. † p <.10. *p <.05. **p <.01. ***p <.001.
Predictor Full Scale IQ Working Memory
β F R2 ΔR2 β F R2 ΔR2 Step 1 .71 .04 1.06 .06 CR Sociodemographic -.21 -.04 CR Disease .02 -.23 Step 2 1.61 .17 .13† 2.06† .21 .15† CR Sociodemographic -.31 -.06 CR Disease .08 -.12 PSS Total .27 .07 PIP Medical Care -.46* -.43* Step 3 1.92† .28 .11† 2.59* .35 .14† CR Sociodemographic -.32† -.05 CR Disease .01 -.21 PSS Total .19 -.04 PIP Medical Care -.36† -.34† Responsive Parentinga .03 -.05 Expansionsb .35* .40*

70
Table 9 continued. Summary of Linear Regression Analyses for Variables Predicting Child Cognitive Function.
aMacro-level. bMicro-level. Note. CR = cumulative risk; PSS = Perceived Stress Scale; PIP = Pediatric Inventory for Parents. † p <.10. *p <.05. **p <.01. ***p <.001.
Predictor Spelling Math Reading Composite
β F R2 ΔR2 β F R2 ΔR2 β F R2 ΔR2 Step 1 .17 .01 .63 .04 1.34 .08 CR Sociodemographic -.10 -.10 -.15 CR Disease -.01 -.13 -.19 Step 2 1.71 .18 .17* 1.69 .18 .14† 3.29* .31 .23* CR Sociodemographic -.12 -.14 -.09 CR Disease .11 -.04 -.04 PSS Total .08 .12 -.10 PIP Medical Care -.47* -.44* -.45* Step 3 1.42 .23 .05 1.23 .20 .03 3.01* .39 .09 CR Sociodemographic -.13 -.17 -.15 CR Disease .06 -.06 -.11 PSS Total .02 .09 -.15 PIP Medical Care -.40† -.39† -.34† Responsive Parenting .02 .10 .16 Expansions .23 .13 .37*

71
Figure 1. Heuristic Model Depicting Proposed Pathway Between Parent Stress, Observed Parenting and Cognitive Function in Children with SCD.

72
Appendix A. Pediatric Inventory for Parents (PIP)

PEDIATRIC INVENTORY FOR PARENTS Below is a list of difficult events which parents of children who have (or have had) a serious illness sometimes face. Please read each event carefully, and circle HOW OFTEN the event has occurred for you in the past 7 days, using the 5 point scale below. Afterwards, please rate how DIFFICULT it was/or generally is for you, also using the 5 point scale. Please complete both columns for each item. HOW
OFTEN? HOW
DIFFICULT?
EVENT
1=Never, 2=Rarely,
3=Sometimes, 4=Often,
5=Very often
1=Not at all, 2=A little,
3=Somewhat, 4=Very much, 5=Extremely
1. Difficulty sleeping ........................................................................ 1 2 3 4 5 1 2 3 4 5 2. Arguing with family member(s) ................................................... 1 2 3 4 5 1 2 3 4 5 3. Bringing my child to the clinic or hospital ................................... 1 2 3 4 5 1 2 3 4 5 4. Learning upsetting news ............................................................... 1 2 3 4 5 1 2 3 4 5 5. Being unable to go to work/job .................................................... 1 2 3 4 5 1 2 3 4 5 6. Seeing my child’s mood change quickly ...................................... 1 2 3 4 5 1 2 3 4 5 7. Speaking with doctor .................................................................... 1 2 3 4 5 1 2 3 4 5 8. Watching my child have trouble eating ........................................ 1 2 3 4 5 1 2 3 4 5 9. Waiting for my child’s test results ............................................... 1 2 3 4 5 1 2 3 4 5 10. Having money/financial troubles ............................................... 1 2 3 4 5 1 2 3 4 5 11. Trying not to think about my family’s difficulties ..................... 1 2 3 4 5 1 2 3 4 5 12. Feeling confused about medical information ............................. 1 2 3 4 5 1 2 3 4 5 13. Being with my child during medical procedures ........................ 1 2 3 4 5 1 2 3 4 5 14. Knowing my child is hurting or in pain ..................................... 1 2 3 4 5 1 2 3 4 5 15. Trying to attend to the needs of other family members ............. 1 2 3 4 5 1 2 3 4 5 16. Seeing my child sad or scared .................................................... 1 2 3 4 5 1 2 3 4 5 17. Talking with the nurse ................................................................ 1 2 3 4 5 1 2 3 4 5 18. Making decisions about medical care or medicines ................... 1 2 3 4 5 1 2 3 4 5 19. Thinking about my child being isolated from others ................. 1 2 3 4 5 1 2 3 4 5 20. Being far away from family and/or friends ................................ 1 2 3 4 5 1 2 3 4 5 21. Feeling numb inside ................................................................... 1 2 3 4 5 1 2 3 4 5 22. Disagreeing with a member of the health care team .................. 1 2 3 4 5 1 2 3 4 5

Randi Streisand, Ph.D.
HOW OFTEN?
HOW DIFFICULT?
EVENT
1=Never, 2=Rarely,
3=Sometimes, 4=Often,
5=Very often
1=Not at all, 2=A little,
3=Somewhat, 4=Very much, 5=Extremely
23. Helping my child with his/her hygiene needs ............................ 1 2 3 4 5 1 2 3 4 5 24. Worrying about the long term impact of the illness ................... 1 2 3 4 5 1 2 3 4 5 25. Having little time to take care of my own needs ........................ 1 2 3 4 5 1 2 3 4 5 26. Feeling helpless over my child’s condition ................................ 1 2 3 4 5 1 2 3 4 5 27. Feeling misunderstood by family/friends as to the severity of
my child’s illness ......................................................................... 1 2 3 4 5
1 2 3 4 5
28. Handling changes in my child’s daily medical routines ............. 1 2 3 4 5 1 2 3 4 5 29. Feeling uncertain about the future .............................................. 1 2 3 4 5 1 2 3 4 5 30. Being in the hospital over weekends/holidays ........................... 1 2 3 4 5 1 2 3 4 5 31. Thinking about other children who have been seriously ill ....... 1 2 3 4 5 1 2 3 4 5 32. Speaking with my child about his/her illness ............................. 1 2 3 4 5 1 2 3 4 5 33. Helping my child with medical procedures (e.g. giving shots,
swallowing medicine, changing dressing) ................................... 1 2 3 4 5
1 2 3 4 5
34. Having my heart beat fast, sweating, or feeling tingly ............... 1 2 3 4 5 1 2 3 4 5 35. Feeling uncertain about disciplining my child ........................... 1 2 3 4 5 1 2 3 4 5 36. Feeling scared that my child could get very sick or die ............. 1 2 3 4 5 1 2 3 4 5 37. Speaking with family members about my child’s illness ........... 1 2 3 4 5 1 2 3 4 5 38. Watching my child during medical visits/procedures ................ 1 2 3 4 5 1 2 3 4 5 39. Missing important events in the lives of other family members 1 2 3 4 5 1 2 3 4 5 40. Worrying about how friends and relatives interact with my
child ............................................................................................. 1 2 3 4 5
1 2 3 4 5
41. Noticing a change in my relationship with my partner .............. 1 2 3 4 5 1 2 3 4 5 42. Spending a great deal of time in unfamiliar settings .................. 1 2 3 4 5 1 2 3 4 5

Randi Streisand, Ph.D.
PEDIATRIC INVENTORY FOR PARENTS SCORING SHEET
PIP item number and brief description of event within each domain
(F = Frequency, D = Difficulty)
COMMUNICATION (CM: 9 items) F D MEDICAL CARE (MC: 8 items) F D
2. Arguing ................................................. 3. Bringing my child to the clinic .............
7. Speaking with doctor ............................ 8. Watching/eating ....................................
12. Feeling confused ................................. 13. Being with my child ...........................
17. Talking with the nurse ........................ 18. Making decisions ................................
22. Disagreeing ......................................... 23. Helping/hygiene needs .......................
27. Feeling misunderstood ........................ 28. Handling changes ...............................
32. Speaking with child ............................ 33. Helping/procedures .............................
37. Speaking with family .......................... 38. Watching/procedures ..........................
40. Worrying .............................................
CM TOTAL MC TOTAL
EMOTIONAL DIST. (ED: 15 items) F D ROLE FUNCTION (RF: 10 items) F D
1. Difficulty sleeping ................................ 5. Being unable to go to work ..................
4. Learning upsetting news ....................... 10. Having money ....................................
6. Seeing mood change ............................. 15. Trying to attend/other .........................
9. Waiting for test results .......................... 20. Being far away from family ...............
11. Trying not to think/difficulties ........... 25. Having little time ................................
14. Knowing/hurting ................................. 30. Being in the hospital ...........................
16. Seeing child sad .................................. 35. Feeling uncertain ................................
19. Thinking about/isolated ...................... 39. Missing important events ...................
21. Feeling numb inside ........................... 41. Noticing a change ...............................
24. Worrying about/impact ....................... 42. Spending a great deal of time .............
26. Feeling helpless ..................................
29. Feeling uncertain ................................
31. Thinking about/other ill
34. Having my heart beat fast ...................
36. Feeling scared .....................................
ED TOTAL RF TOTAL
CM+ED+MC+RF TOTAL:F
CM+ED+MC+RF TOTAL:D

Randi Streisand, Ph.D.
Pediatric Inventory for Parents Scoring Instructions
The PIP is scored separately for each of the 4 domains (Communication, Emotional Distress,
Medical Care, Role Function), across 2 scales: Frequency (F) and Difficulty (D). There is also a
total score comprised of the sum for each of the 4 domains, yielding Total F and Total D scores.
Items are scored as endorsed by respondents, ranging from 1-5. The range for each of the Total F
and Total D scores is 42-210.
Using the item number across domains as listed on the preceding page, sum the items to yield a
score for each domain. For example, for the Communication Domain, summing the Frequency
scores for items 2, 7, 12, 17, 22, 27, 32, 37, 40 results in the Communication Frequency score.
Summing the Difficulty scores for the same item numbers results in the Communication Difficulty
score. These scores are then combined with the scores from each of the other domains to yield the
PIP Total Frequency, and PIP Total Difficulty scores; the scoring sheet provided will facilitate this
process.

77
Appendix B. Perceived Stress Scale (PSS)

version: 05/15/2017 PSS 1 of 1
INSTRUCTIONS:
The questions in this scale ask you about your feelings and thoughts during THE LAST MONTH. In each case, please indicate your response by placing an “X” over the circle representing HOW OFTEN you felt or thought a certain way.
1. In the last month, how often have you been upset because of something that happened unexpectedly?
2. In the last month, how often have you felt that you were unable to control the important things in your life?
3. In the last month, how often have you felt nervous and “stressed”?
4. In the last month, how often have you felt confident about your ability to handle your personal problems?
5. In the last month, how often have you felt that things were going your way?
6. In the last month, how often have you found that you could not cope with all the things that you had to do?
7. In the last month, how often have you been able to control irritations in your life?
8. In the last month, how often have you felt that you were on top of things?
9. In the last month, how often have you been angered because of things that were outside your control?
10. In the last month, how often have you felt difficulties were piling up so high that you could not overcome them?
Almost Fairly Very Never Never Sometimes Often Often 0 1 2 3 4
PSS

79
Appendix C. Supplementary Analyses

80
Table 10. Intercorrelations Among Macro-Level Codes Included in Responsive Parenting Composite. SC EI LR CO CC
SC --
EI .61*** --
LR .58*** .43*** --
CO .61*** .36** .68*** --
CC .69*** .61*** .72*** .63*** --
PO .71*** .56*** .43*** .33** .57***
Note. See table 2a for code abbreviations. † p <.10. *p <.05. **p <.01. ***p <.001.

81
Table 11. Intercorrelations Among Macro-Level Codes Included in Warm Parenting Composite. WM PR
WM --
PR .43*** --
PM .67*** .37**
Note. See table 2b for code abbreviations † p <.10. *p <.05. **p <.01. ***p <.001.

82
Table 12. Intercorrelations Among Macro-Level Codes Included in Withdrawn Parenting Composite. EX AV IP
EX --
AV .50*** --
IP .58*** .79*** --
ID .54*** .89*** .89***
Note. See table 2c for code abbreviations † p <.10. *p <.05. **p <.01. ***p <.001.
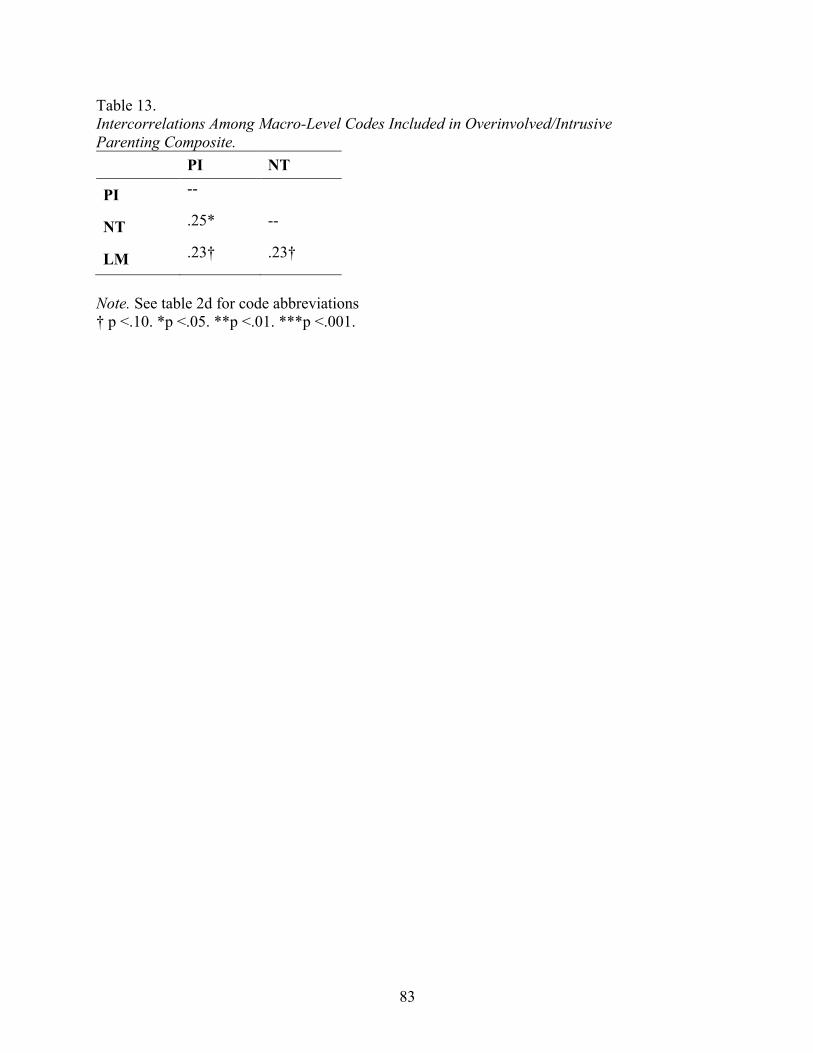
83
Table 13. Intercorrelations Among Macro-Level Codes Included in Overinvolved/Intrusive Parenting Composite. PI NT
PI --
NT .25* --
LM .23† .23†
Note. See table 2d for code abbreviations † p <.10. *p <.05. **p <.01. ***p <.001.

84
Table 14. Intercorrelations Among Micro-Level Parenting Codes. Maintains Reflections Expansions Reframes Solicits Disclosures Provisions
of Info. Imperatives
Maintains -- Reflections .23† -- Expansions .00 -.02 -- Reframes -.24† -.14 .31* -- Solicits -.14 -.02 .07 -.09 -- Disclosures -.18 .02 -.02 .01 -.07 -- Provisions of Info. -.17 -.08 .22 .12 -.36** .27† -- Validations .21 .22† -.09 -.16 -.06 -.02 -.22† -- Imperatives -.30* -.16 -.03 .34* -.20 -.04 -.06 -.03
† p <.10. *p <.05. **p <.01. ***p <.001.

85
Table 15. Linear Regression Analyses for Variables Predicting Child VCI and PRI.
Note. CR = cumulative risk; PSS = Perceived Stress Scale; PIP = Pediatric Inventory for Parents. † p <.10. *p <.05. **p <.01. ***p <.001
Verbal Comprehension Perceptual Reasoning
Predictor β F R2 ΔR2 β F R2 ΔR2 Step 1 1.57 .09 .02 .00 CR Sociodemographic -.30† .03 CR Disease .03 -.03 Step 2 1.48 .16 .07 2.03† .21 .21* CR Sociodemographic -.28 -.20 CR Disease .11 -.02 PSS Total -.04 .56* PIP Medical Care -.26 -.52* Step 3 1.66 .26 .10 2.43* .33 .13† CR Sociodemographic -.34† -.13 CR Disease .07 -.10 PSS Total -.08 .47* PIP Medical Care -.15 -.49* Responsive Parenting .22 -.24 Expansions .23 .31†

86
Table 16. Linear Regression Analyses for Variables Predicting Child Cognitive Function with PIP Total.
Note. CR = cumulative risk; PSS = Perceived Stress Scale; PIP = Pediatric Inventory for Parents. † p <.10. *p <.05. **p <.01. ***p <.001
Verbal Comprehension Perceptual Reasoning
Predictor β F R2 ΔR2 β F R2 ΔR2 Step 1 1.57 .09 .02 .00 CR Sociodemographic -.30† .03 CR Disease .03 -.03 Step 2b 1.14 .13 .04 .70 .08 .08 CR Sociodemographic -.25 -.14 CR Disease .09 -.06 PSS Total -.11 .43† PIP Total -.14 -.29 Step 3b 1.61 .25 .12† 1.55 .24 .16† CR Sociodemographic -.34† -.11 CR Disease .06 -.14 PSS Total -.10 .36 PIP Total -.11 -.30 Responsive Parenting .23 -.19 Expansions .26† .39*

87
Table 16 continued. Linear Regression Analyses for Variables Predicting Child Cognitive Function with PIP Total.
Note. CR = cumulative risk; PSS = Perceived Stress Scale; PIP = Pediatric Inventory for Parents. † p <.10. *p <.05. **p <.01. ***p <.001
Full Scale IQ Working Memory
Predictor β F R2 ΔR2 β F R2 ΔR2 Step 1 .71 .04 1.06 .06 CR Sociodemographic -.21 -.04 CR Disease .02 -.23 Step 2b .63 .08 .03 1.11 .13 .07 CR Sociodemographic -.26 -.01 CR Disease .04 -.15 PSS Total .15 -.04 PIP Total -.24 -.25 Step 3b 1.53 .24 .17† 2.23† .32 .19* CR Sociodemographic -.31 -.04 CR Disease -.02 -.24 PSS Total .12 -.08 PIP Total -.23 -.24 Responsive Parenting .06 -.02 Expansions .41* .45**
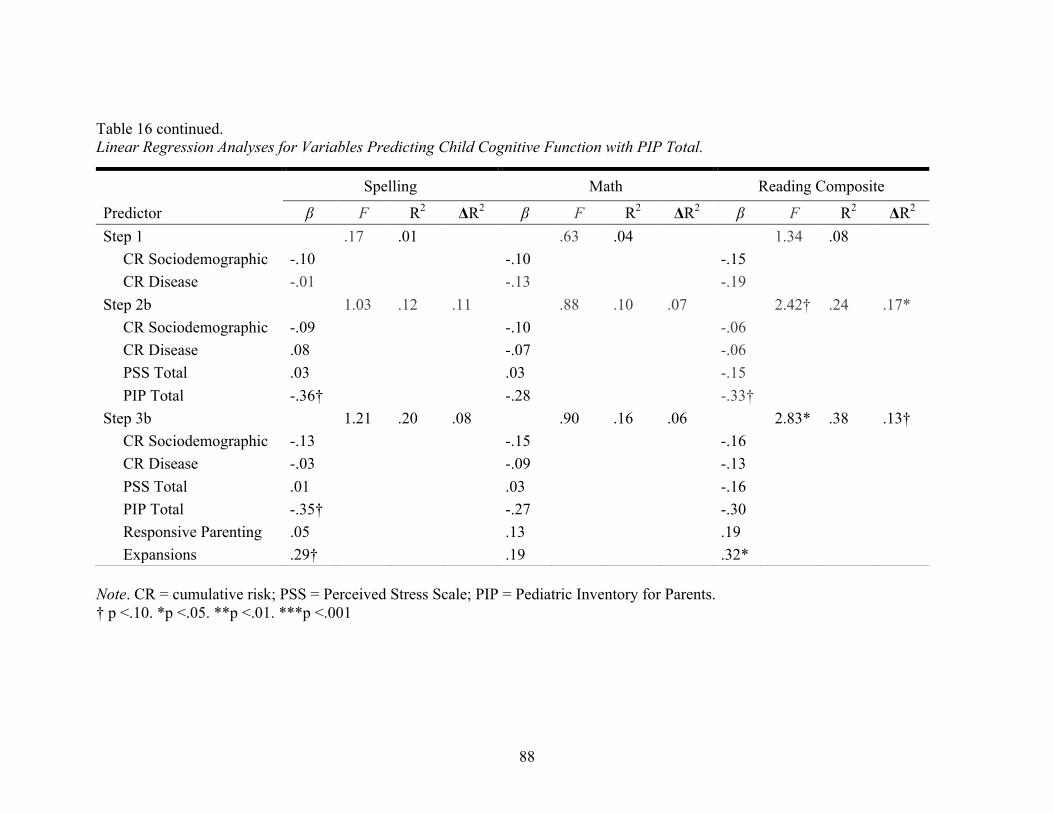
88
Table 16 continued. Linear Regression Analyses for Variables Predicting Child Cognitive Function with PIP Total.
Note. CR = cumulative risk; PSS = Perceived Stress Scale; PIP = Pediatric Inventory for Parents. † p <.10. *p <.05. **p <.01. ***p <.001
Spelling Math Reading Composite
Predictor β F R2 ΔR2 β F R2 ΔR2 β F R2 ΔR2 Step 1 .17 .01 .63 .04 1.34 .08 CR Sociodemographic -.10 -.10 -.15 CR Disease -.01 -.13 -.19 Step 2b 1.03 .12 .11 .88 .10 .07 2.42† .24 .17* CR Sociodemographic -.09 -.10 -.06 CR Disease .08 -.07 -.06 PSS Total .03 .03 -.15 PIP Total -.36† -.28 -.33† Step 3b 1.21 .20 .08 .90 .16 .06 2.83* .38 .13† CR Sociodemographic -.13 -.15 -.16 CR Disease -.03 -.09 -.13
PSS Total .01 .03 -.16 PIP Total -.35† -.27 -.30 Responsive Parenting .05 .13 .19 Expansions .29† .19 .32*

89
REFERENCES
Adams, R., McKie, V., Nichols, F., Carl, E., Zhang, D. L., McKie, K., ... & Hess, D. (1992). The
use of transcranial ultrasonography to predict stroke in sickle cell disease. New England
Journal of Medicine, 326(9), 605-610.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders
(DSM-5®). Arlington, VA: American Psychiatric Publishing.
Ashley-Koch, A., Yang, Q., & Olney, R. S. (2000). Sickle hemoglobin (Hb S) allele and sickle
cell disease: a HuGE review. American Journal of Epidemiology, 151(9), 839-845.
Aspland, H., & Gardner, F. (2003). Observational Measures of Parent‐Child Interaction: An
Introductory Review. Child and Adolescent Mental Health, 8(3), 136-143.
Barakat, L. P., Patterson, C. A., Tarazi, R. A., & Ely, E. (2007). Disease-related parenting stress
in two sickle cell disease caregiver samples: Preschool and adolescent. Families, Systems,
& Health, 25(2), 147.
Barbarin, O. A., Whitten, C. F., Bond, S., & Conner-Warren, R. (1999). The social and cultural
context of coping with sickle cell disease: II. The role of financial hardship in adjustment
to sickle cell disease. Journal of Black Psychology, 25(3), 294-315.
Barlow, J. H., & Ellard, D. R. (2004). Psycho‐educational interventions for children with chronic
disease, parents and siblings: An overview of the research evidence base. Child: Care,
Health and Development, 30(6), 637-645.
Beebe, D. W., Wells, C. T., Jeffries, J., Chini, B., Kalra, M., & Amin, R. (2004).
Neuropsychological effects of pediatric obstructive sleep apnea. Journal of the
International Neuropsychological Society: JINS, 10(7), 962-975.
Bradley, R. H., & Corwyn, R. F. (2002). Socioeconomic status and child development. Annual

90
Review of Psychology, 53(1), 371-399.
Brody, G. H., & Flor, D. L. (1998). Maternal resources, parenting practices, and child
competence in rural, single‐parent African American families. Child Development, 69(3),
803-816.
Bronfenbrenner, U. (1977). Toward an experimental ecology of human development. American
Psychologist, 32(7), 513.
Brown, R. T., Davis, P. C., Lambert, R., Hsu, L., Hopkins, K., & Eckman, J. (2000).
Neurocognitive functioning and magnetic resonance imaging in children with sickle cell
disease. Journal of Pediatric Psychology, 25(7), 503-513.
Brown, R. T., Wiener, L., Kupst, M. J., Brennan, T., Behrman, R., Compas, B. E., ... & Zeltzer,
L. (2008). Single parents of children with chronic illness: An understudied phenomenon.
Journal of Pediatric Psychology, 33(4), 408-421.
Burchinal, M. R., Follmer, A., & Bryant, D. M. (1996). The relations of maternal social support
and family structure with maternal responsiveness and child outcomes among African
American families. Developmental Psychology, 32(6), 1073.
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress.
Journal of Health and Social Behavior, 385-396.
Compas, B.E., Champion, J.E., Forehand, R., Cole, D.A., Reeslund, K.L., Fear, J., Hardcastle,
J., Keller, G., Rakow, A., Garai, E., Merchant, M.J., & Roberts, L. (2010). Coping and
Parenting: Mediators of 12-month outcomes of a family group cognitive-behavioral
preventive intervention with families of depressed parents. Journal of Consulting and
Clinical Psychology, 78, 623-634.
Compas, B. E., Jaser, S. S., Reeslund, K., Patel, N., & Yarboi, J. (2017). Neurocognitive deficits

91
in children with chronic health conditions. American Psychologist, 72(4), 326.
Deater-Deckard, K. et al. (2010). Maternal working memory and reactive negativity in parenting.
Psychological Science, 21, 75-79.
DeNavas-Walt, C., & Proctor, B. D. U.S. Department of Commerce, U.S. Census Bureau.
(2015). Income and poverty in the United States: 2014. Retrieved from website:
http://www.census.gov/content/dam/Census/library/publications/2015/demo/p60-252.pdf
Doan, S. N., & Evans, G. W. (2011). Maternal responsiveness moderates the relationship
between allostatic load and working memory. Development and Psychopathology, 23(3),
873-880.
Driscoll, M. C. (2007). Sickle cell disease. Pediatrics in Review, 28(7), 259-268.
Duncan, G. J., Brooks-Gunn, J., & Klebanov, P. K. (1994). Economic deprivation and early
childhood development. Child Development, 65(2), 296-318.
Dunn, M.J., Rodriguez, E.M., Miller, K.S., Gerhardt, C.A., Vannatta, K., Saylor, M., Scheule,
M., & Compas, B.E. (2011). Direct observation of mother-child communication in
pediatric cancer: Assessment of verbal and non-verbal behavior and emotion. Journal of
Pediatric Psychology, 36, 565-575.
Evans, G. W. (2003). A multimethodological analysis of cumulative risk and allostatic load
among rural children. Developmental Psychology, 39(5), 924.
Evans, G. W., Boxhill, L., & Pinkava, M. (2008). Poverty and maternal responsiveness: The role
of maternal stress and social resources. International Journal of Behavioral Development,
32(3), 232-237.
Evans, G. W., Gonnella, C., Marcynyszyn, L. A., Gentile, L., & Salpekar, N. (2005). The role of
chaos in poverty and children's socioemotional adjustment. Psychological Science, 16(7),

92
560-565.
Evans, G. W., & Kim, P. (2007). Childhood poverty and health cumulative risk exposure and
stress dysregulation. Psychological Science, 18(11), 953-957.
Evans, G. W., Ricciuti, H. N., Hope, S., Schoon, I., Bradley, R. H., Corwyn, R. F., & Hazan, C.
(2010). Crowding and cognitive development the mediating role of maternal
responsiveness among 36-month-old children. Environment and Behavior, 42(1), 135-
148.
Farah, M. J., Shera, D. M., Savage, J. H., Betancourt, L., Giannetta, J. M., Brodsky, N. L., ... &
Hurt, H. (2006). Childhood poverty: Specific associations with neurocognitive
development. Brain Research, 1110(1), 166-174.
Faul, F., Erdfelder, E., Lang, A. G., & Buchner, A. (2007). G* Power 3: A flexible statistical
power analysis program for the social, behavioral, and biomedical sciences. Behavior
Research Methods, 39(2), 175-191.
Glass, P., Brennan, T., Wang, J., Luchtman-Jones, L., Hsu, L., Bass, C. M., ... & Gordeuk, V.
(2013). Neurodevelopmental Deficits Among Infants and Toddlers with Sickle Cell
Disease. Journal of Developmental & Behavioral Pediatrics, 34(6), 399-405.
Gruhn, M. A., Lord, J. H., & Jaser, S. S. (2016). Collaborative and overinvolved parenting
differentially predict outcomes in adolescents with Type 1 diabetes. Health
Psychology, 35(7), 652.
Guo, G., & Harris, K. M. (2000). The mechanisms mediating the effects of poverty on children’s
intellectual development. Demography, 37(4), 431-447.
Hackman, D. A., & Farah, M. J. (2009). Socioeconomic status and the developing brain. Trends
in Cognitive Sciences, 13(2), 65-73.

93
Hackman, D. A., Farah, M. J., & Meaney, M. J. (2010). Socioeconomic status and the brain:
mechanistic insights from human and animal research. Nature Reviews Neuroscience,
11(9), 651-659.
Halfon, N., & Newacheck, P. W. (2010). Evolving notions of childhood chronic illness. Journal
of the American Medical Association, 303(7), 665-666.
Hamideh, D., & Alvarez, O. (2013). Sickle cell disease related mortality in the United States
(1999–2009). Pediatric Blood & Cancer, 60(9), 1482-1486.
Hardy, S. J., Hardy, K. K., Schatz, J. C., Thompson, A. L., & Meier, E. R. (2016). Feasibility of
Home‐Based Computerized Working Memory Training With Children and Adolescents
With Sickle Cell Disease. Pediatric Blood & Cancer, 63(9), 1578-1585.
Hart, B. & Risley, T. R. (1992). American parenting of language-learning children: Persistent
differences in family-child interactions observed in natural home environments.
Developmental Psychology, 28, 1096-1105.
Hart, B., & Risley, T. R. (1995). Meaningful differences in the everyday experience of young
American children. Paul H Brookes Publishing.
Hassell, K. L. (2010). Population estimates of sickle cell disease in the US. American Journal of
Preventive Medicine, 38(4), S512-S521.
Helps, S., Fuggle, P., Udwin, O., & Dick, M. (2003). Psychosocial and neurocognitive aspects of
sickle cell disease. Child and Adolescent Mental Health, 8(1), 11-17.
Hijmans, C. T., Fijnvandraat, K., Grootenhuis, M. A., van Geloven, N., Heijboer, H., Peters, M.,
& Oosterlaan, J. (2011a). Neurocognitive deficits in children with sickle cell disease: a
comprehensive profile. Pediatric Blood & Cancer, 56(5), 783-788.
Hijmans, C. T., Grootenhuis, M. A., Oosterlaan, J., Heijboer, H., Peters, M., & Fijnvandraat, K.

94
(2011b). Neurocognitive deficits in children with sickle cell disease are associated with
the severity of anemia. Pediatric Blood & Cancer, 57(2), 297-302.
Hijmans, C. T., Grootenhuis, M. A., Oosterlaan, J., Heijboer, H., Peters, M., & Fijnvandraat, K.
(2011b). Neurocognitive deficits in children with sickle cell disease are associated with
the severity of anemia. Pediatric Blood & Cancer, 57(2), 297-302.
Hill, C. M., Hogan, A. M., Onugha, N., Harrison, D., Cooper, S., McGrigor, V. J., ... & Kirkham,
F. J. (2006). Increased cerebral blood flow velocity in children with mild sleep-
disordered breathing: a possible association with abnormal neuropsychological function.
Pediatrics, 118(4), e1100-e1108.
Hogan, A. M., Pit-ten Cate, I. M., Vargha-Khadem, F., Prengler, M., & Kirkham, F. J. (2006).
Physiological correlates of intellectual function in children with sickle cell disease:
hypoxaemia, hyperaemia and brain infarction. Developmental Science, 9(4), 379-387.
Hollocks, M. J., Kok, T. B., Kirkham, F. J., Gavlak, J., Inusa, B. P., DeBaun, M. R., & de Haan,
M. (2011). Nocturnal oxygen desaturation and disordered sleep as a potential factor in
executive dysfunction in sickle cell anemia. Journal of the International
Neuropsychological Society, 18(1), 168.
Kaiser, A. P., & Delaney, E. M. (1996). The effects of poverty on parenting young children.
Peabody Journal of Education, 71(4), 66-85.
Kaplan, G. A., Turrell, G., Lynch, J. W., Everson, S. A., Helkala, E. L., & Salonen, J. T. (2001).
Childhood socioeconomic position and cognitive function in adulthood. International
Journal of Epidemiology, 30(2), 256-263.
Kazak, A. E. (2005). Evidence-based interventions for survivors of childhood cancer and their
families. Journal of Pediatric Psychology, 30(1), 29-39.

95
King, A. A., Strouse, J. J., Rodeghier, M. J., Compas, B. E., Casella, J. F., McKinstry, R. C., ...
& Miller, J. P. (2014). Parent education and biologic factors influence on cognition in
sickle cell anemia. American Journal of Hematology, 89(2), 162-167.
Lasky, E. Z. & Klopp, K. (1982). Parent-child interactions in normal and language-disordered
children. Journal of Speech and Hearing Disorders, 47, 7-18.
Lazarus, R. S., & Folkman, S. (1984). Stress, Appraisal, and Coping. Springer Publishing
Company.
Lengua, L. J., Kiff, C., Moran, L., Zalewski, M., Thompson, S., Cortes, R., & Ruberry, E.
(2014). Parenting mediates the effects of income and cumulative risk on the development
of effortful control. Social Development, 23(3), 631-649.
Leyendecker, B., Harwood, R. L., Comparini, L., & Yalcinkaya, A. (2005). Socioeconomic
status, ethnicity, and parenting. Parenting: An Ecological Perspective, 2, 319-341.
Lindell, M. K., & Whitney, D. J. (2001). Accounting for common method variance in cross-
sectional research designs. Journal of Applied Psychology, 86(1), 114.
Lorey, F. W., Arnopp, J., & Cunningham, G. C. (1996). Distribution of hemoglobinopathy
variants by ethnicity in a multiethnic state. Genetic Epidemiology, 13(5), 501-512.
Luby, J., Belden, A., Botteron, K., Marrus, N., Harms, M. P., Babb, C., ... & Barch, D. (2013).
The Effects of Poverty on Childhood Brain Development: The Mediating Effect of
Caregiving and Stressful Life Events. JAMA Pediatrics, 167(12), 1135-1142.
Lugo-Gil, J., & Tamis-LeMonda, C. S. (2008). Family resources and parenting quality: Links to
children’s cognitive development across the first 3 years. Child Development, 79(4),
1065-1085.
McLaughlin, B., Schutz, C. & White, D. (1980). Parental speech to five-year-old children in a

96
game-playing situation. Child Development, 51, 580-582.
Melby, J. N., & Conger, R. D. (2001). The Iowa Family Interaction Rating Scales: Instrument
Summary. In P. Kerig and K. Lindahl (Eds.), Family observational coding systems:
Resources for systemic research. Mahwah, NJ: Lawrence Erlbaum Associates.
Middlemiss, W. (2003). Poverty, stress, and support: patterns of parenting behavior among lower
income black and lower income white mothers. Infant and Child Development, 12(3),
293-300.
Miyake, A., & Friedman, N. P. (2012). The nature and organization of individual differences in
executive functions four general conclusions. Current Directions in Psychological
Science, 21(1), 8-14.
Murphy, L. K., Rodriguez, E. M., Schwartz, L., Bemis, H., Desjardins, L., Gerhardt, C. A., ... &
Compas, B. E. (2015). Longitudinal associations among maternal communication and
adolescent posttraumatic stress symptoms after cancer diagnosis. Psycho‐Oncology.
Needleman, J. P., Franco, M. E., Varlotta, L., Reber-Brodecki, D., Bauer, N., Dampier, C., &
Allen, J. L. (1999). Mechanisms of nocturnal oxyhemoglobin desaturation in children and
adolescents with sickle cell disease. Pediatric Pulmonology, 28(6), 418-422.
Neville, H. J., Stevens, C., Pakulak, E., Bell, T. A., Fanning, J., Klein, S., & Isbell, E. (2013).
Family-based training program improves brain function, cognition, and behavior in lower
socioeconomic status preschoolers. Proceedings of the National Academy of
Sciences, 110(29), 12138-12143.
Ohene-Frempong, K., Weiner, S. J., Sleeper, L. A., Miller, S. T., Embury, S., Moohr, J. W., ... &
Cooperative Study of Sickle Cell Disease. (1998). Cerebrovascular accidents in sickle
cell disease: rates and risk factors. Blood, 91(1), 288-294.

97
Pegelow, C. H., Macklin, E. A., Moser, F. G., Wang, W. C., Bello, J. A., Miller, S. T., ... &
Kinney, T. R. (2002). Longitudinal changes in brain magnetic resonance imaging
findings in children with sickle cell disease. Blood, 99(8), 3014-3018.
Platt, O. S., Brambilla, D. J., Rosse, W. F., Milner, P. F., Castro, O., Steinberg, M. H., & Klug,
P. P. (1994). Mortality in sickle cell disease--life expectancy and risk factors for early
death. New England Journal of Medicine, 330(23), 1639-1644.
Platt, O. S., Thorington, B. D., Brambilla, D. J., Milner, P. F., Rosse, W. F., Vichinsky, E., &
Kinney, T. R. (1991). Pain in sickle cell disease: rates and risk factors. New England
Journal of Medicine, 325(1), 11-16.
Quinn, C. T., Rogers, Z. R., & Buchanan, G. R. (2004). Survival of children with sickle cell
disease. Blood, 103(11), 4023-4027.
Quinn, C. T., Rogers, Z. R., McCavit, T. L., & Buchanan, G. R. (2010). Improved survival of
children and adolescents with sickle cell disease. Blood, 115(17), 3447-3452.
Raviv, T., & Wadsworth, M. E. (2010). The efficacy of a pilot prevention program for children
and caregivers coping with economic strain. Cognitive Therapy and Research, 34(3),
216-228.
Rees, D. C., Williams, T. N., & Gladwin, M. T. (2010). Sickle-cell disease. The Lancet,
376(9757), 2018-2031.
Rodriguez, E. M., Dunn, M. J., Zuckerman, T., Hughart, L., Vannatta, K., Gerhardt, C. A., ... &
Compas, B. E. (2013). Mother–Child Communication and Maternal Depressive
Symptoms in Families of Children With Cancer: Integrating Macro and Micro Levels of
Analysis. Journal of pediatric psychology.
Rodriguez, E. M., Zuckerman, T., Saylor, M., Schuele, C. M., & Compas, B.E. (2011).

98
Contingency coding manual. Vanderbilt University, Department of Psychology and
Human Development.
Sameroff, A. J., & Fiese, B. H. (2000). Transactional regulation: The developmental ecology of
early intervention. Handbook of Early Childhood Intervention, 2, 135-159.
Sanchez, C. E., Schatz, J., & Roberts, C. W. (2010). Cerebral blood flow velocity and language
functioning in pediatric sickle cell disease. Journal of the International
Neuropsychological Society, 16(02), 326-334.
Schatz, J. (2004). Brief report: Academic attainment in children with sickle cell disease.
Journal of Pediatric Psychology, 29(8), 627-633.
Schatz, J., & Buzan, R. (2006). Decreased corpus callosum size in sickle cell disease:
relationship with cerebral infarcts and cognitive functioning. Journal of the International
Neuropsychological Society, 12(01), 24-33.
Schatz, J., Finke, R. L., Kellett, J. M., & Kramer, J. H. (2002). Cognitive functioning in children
with sickle cell disease: a meta-analysis. Journal of Pediatric Psychology, 27(8), 739-
748.
Schatz, J., & McClellan, C. B. (2006). Sickle cell disease as a neurodevelopmental disorder.
Mental Retardation and Developmental Disabilities Research Reviews, 12(3), 200-207.
Schatz, J., Puffer, E. S., Sanchez, C., Stancil, M., & Roberts, C. W. (2009). Language processing
deficits in sickle cell disease in young school-age children. Developmental
Neuropsychology, 34(1), 122-136.
Schatz, J., & Roberts, C. W. (2005). Short-term memory in children with sickle cell disease:
Executive versus modality-specific processing deficits. Archives of Clinical
Neuropsychology, 20(8), 1073-1085.

99
Schatz, J., & Roberts, C. W. (2007). Neurobehavioral impact of sickle cell disease in early
childhood. Journal of the International Neuropsychological Society, 13(06), 933-943.
Scott, S., Webster-Stratton, C., Spender, Q., Doolan, M., Jacobs, B., & Aspland, H. (2001).
Multicentre controlled trial of parenting groups for childhood antisocial behaviour in
clinical practice. Commentary: nipping conduct problems in the bud. British Medical
Journal, 323(7306), 194.
Sirin, S. R. (2005). Socioeconomic status and academic achievement: A meta-analytic
review of research. Review of Educational Research, 75(3), 417-453.
Steen, R. G., Fineberg-Buchner, C., Hankins, G., Weiss, L., Prifitera, A., & Mulhern, R. K.
(2005). Cognitive deficits in children with sickle cell disease. Journal of Child
Neurology, 20(2), 102-107.
Steen, R. G., Miles, M. A., Helton, K. J., Strawn, S., Wang, W., Xiong, X., & Mulhern, R. K.
(2003). Cognitive impairment in children with hemoglobin SS sickle cell disease:
relationship to MR imaging findings and hematocrit. American Journal of
Neuroradiology, 24(3), 382-389.
Streisand, R., Braniecki, S., Tercyak, K. P., & Kazak, A. E. (2001). Childhood illness-related
parenting stress: the pediatric inventory for parents. Journal of Pediatric
Psychology, 26(3), 155-162.
Strouse, J. J., Cox, C. S., Melhem, E. R., Lu, H., Kraut, M. A., Razumovsky, A., ... &
Casella, J. F. (2006). Inverse correlation between cerebral blood flow measured by
continuous arterial spin-labeling (CASL) MRI and neurocognitive function in children
with sickle cell anemia (SCA). Blood, 108(1), 379-381.
Tamis-LeMonda, C. S., Shannon, J. D., Cabrera, N. J., & Lamb, M. E. (2004). Fathers and

100
mothers at play with their 2-and 3-year-olds: contributions to language and cognitive
development. Child Development, 75(6), 1806-1820.
Tucker‐Drob, E. M., & Harden, K. P. (2012). Early childhood cognitive development and
parental cognitive stimulation: Evidence for reciprocal gene–environment
transactions. Developmental Science, 15(2), 250-259.
van der Lee, J. H., Mokkink, L. B., Grootenhuis, M. A., Heymans, H. S., & Offringa, M. (2007).
Definitions and measurement of chronic health conditions in childhood: a systematic
review. Journal of the American Medical Association, 297(24), 2741-2751.
Wadsworth, M. E., Raviv, T., Santiago, C. D., & Etter, E. M. (2011). Testing the adaptation to
poverty-related stress model: Predicting psychopathology symptoms in families facing
economic hardship. Journal of Clinical Child & Adolescent Psychology, 40(4), 646-657.
Wagner, N. J., Mills-Koonce, W. R., Willoughby, M. T., Zvara, B., & Cox, M. J. (2015).
Parenting and children’s representations of family predict disruptive and callous-
unemotional behaviors. Developmental Psychology, 51(7), 935.
Watson, K. H., Dunbar, J. P., Thigpen, J., Reising, M. M., Hudson, K., McKee, L., ... & Compas,
B. E. (2014). Observed parental responsiveness/warmth and children’s coping: cross-
sectional and prospective relations in a family depression preventive
intervention. Journal of Family Psychology, 28(3), 278.
Weatherall, D., Hofman, K., Rodgers, G., Ruffin, J., & Hrynkow, S. (2005). A case for
developing North-South partnerships for research in sickle cell disease. Blood, 105(3),
921-923.
Wechsler, D. (2003). Wechsler intelligence scale for children–Fourth Edition (WISC-IV). San
Antonio, TX: The Psychological Corporation.

101
Wechsler, D., & Hsiao-pin, C. (2011). WASI-II: Wechsler abbreviated scale of intelligence.
Pearson.
Wilkinson, G. S., & Robertson, G. J. (2006). Wide range achievement test (WRAT4).
Psychological Assessment Resources, Lutz.
Yarboi, J., Compas, B. E., Brody, G. H., White, D., Rees Patterson, J., Ziara, K., & King, A.
(2017). Association of social-environmental factors with cognitive function in children
with sickle cell disease. Child Neuropsychology, 23(3), 343-360.
Related Documents











