The Role of Health Information Technology in Medication Safety Wednesday, April 25, 2007 12:00 – 1:00 p.m. EDT

The Role of Health Information Technology in Medication Safety Wednesday, April 25, 2007 12:00 – 1:00 p.m. EDT.
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The Role of Health Information Technology in Medication Safety
Wednesday, April 25, 200712:00 – 1:00 p.m. EDT

Moderator: Paul Sharek, MD, MPH, FAAPAssistant Professor of Pediatrics, Stanford School of
MedicineMedical Director of Quality ManagementChief Clinical Patient Safety OfficerLucile Packard Children’s HospitalPalo Alto, California

This activity was funded through an educational grant from the Physicians’
Foundation for Health Systems Excellence.

Disclosure of Financial Relationships and Resolution of Conflicts of Interest for AAP CME Activities
Grid
The AAP CME program aims to develop, maintain, and increase the competency, skills, and professional performance of pediatric healthcare professionals by providing high quality, relevant, accessible and cost-effective educational experiences. The AAP CME program provides activities to meet the participants’ identified education needs and to support their lifelong learning towards a goal of improving care for children and families (AAP CME Program Mission Statement, August 2004).
The AAP recognizes that there are a variety of financial relationships between individuals and commercial interests that require review to identify possible conflicts of interest in a CME activity. The “AAP Policy on Disclosure of Financial Relationships and Resolution of Conflicts of Interest for AAP CME Activities” is designed to ensure quality, objective, balanced, and scientifically rigorous AAP CME activities by identifying and resolving all potential conflicts of interest prior to the confirmation of service of those in a position to influence and/or control CME content. The AAP has taken steps to resolve any potential conflicts of interest.
All AAP CME activities will strictly adhere to the 2004 Updated Accreditation Council for Continuing Medical Education (ACCME) Standards for Commercial Support: Standards to Ensure the Independence of CME Activities. In accordance with these Standards, the following decisions will be made free of the control of a commercial interest: identification of CME needs, determination of educational objectives, selection and presentation of content, selection of all persons and organizations that will be in a position to control the content, selection of educational methods, and evaluation of the CME activity.
The purpose of this policy is to ensure all potential conflicts of interest are identified and mechanisms to resolve them prior to the CME activity are implemented in ways that are consistent with the public good. The AAP is committed to providing learners with commercially unbiased CME activities.

DISCLOSURES Activity Title: Safer Health Care for Kids - Webinar The Role of Health Information Technology in Medication Safety Activity Date: April 25, 2007
DISCLOSURE OF FINANCIAL RELATIONSHIPS All individuals in a position to influence and/or control the content of AAP CME activities are required to disclose to the AAP and subsequently to learners that the individual either has no relevant financial relationships or any financial relationships with the manufacturer(s) of any commercial product(s) and/or provider of commercial services discussed in CME activities.
Name Name of Commercial Interest(s)*
(*Entity producing
health care goods
or services)
Nature of Relevant Financial
Relationship(s) (If yes, please list: Research Grant,
Speaker’s Bureau, Stock/Bonds
excluding mutual funds, Consultant,
Other - identify)
CME Content Will Include
Discussion/ Reference to Commercial
Products/Services
Disclosure of Off-Label (Unapproved)/Investigational Uses of Products
AAP CME faculty are required to disclose to the AAP and to learners when they plan to discuss or
demonstrate pharmaceuticals and/or medical devices that are not approved
Rainu Kaushal, MD, MPH
No No No No

DISCLOSURESSAFER HEALTH CARE FOR KIDS - PROJECT ADVISORY COMMITTEE AND STAFF DISCLOSURE OF FINANCIAL RELATIONSHIPS All individuals in a position to influence and/or control the content of AAP CME activities are required to disclose to the AAP and subsequently to learners that the individual either has no relevant financial relationships or any financial relationships with the manufacturer(s) of any commercial product(s) and/or provider of commercial services discussed in CME activities.
Name Name of Commercial Interest(s)*
(*Entity producing health care goods
or services)
Nature of Relevant Financial Relationship(s)
(If yes, please list: Research Grant, Speaker’s
Bureau, Stock/Bonds excluding mutual funds,
Consultant, Other - identify)
CME Content Will Include Discussion/
Reference to Commercial Products/Services
Disclosure of Off-Label (Unapproved)/Investigational Uses
of Products AAP CME faculty are required to
disclose to the AAP and to learners when they plan to discuss or
demonstrate pharmaceuticals and/or medical devices that are not approved
Karen Frush, MD, FAAP (PAC Member)
No No No No
Uma Kotagal, MD, MBBS, MSc, FAAP (PAC Member)
No No No No
Christopher Landrigan, MD, MPH, FAAP (PAC Member)
No No No No
Marlene R. Miller, MD, MSc, FAAP (PAC Chair)
No No No No
Paul Sharek, MD, MPH. FAAP (PAC Member)
No No No No
Erin Stucky, MD, FAAP (PAC Member)
No No Not sure No
Nancy Nelson (AAP Staff) No No No No
Melissa Singleton, MEd (Project Manager – AAP Consultant)
No No No No
Junelle Speller (AAP Staff) No No No No
Linda Walsh, MAB (AAP Staff)
No No No No

DISCLOSURESAAP COMMITTEE ON CONTINUING MEDICAL EDUCATION (COCME) DISCLOSURE OF FINANCIAL RELATIONSHIPS All individuals in a position to influence and/or control the content of AAP CME activities are required to disclose to the AAP and subsequently to learners that the individual either has no relevant financial relationships or any financial relationships with the manufacturer(s) of any commercial product(s) and/or provider of commercial services discussed in CME activities.
Name Name of Commercial Interest(s)*
(*Entity producing health care goods
or services)
Nature of Relevant Financial Relationship(s)
(If yes, please list: Research Grant, Speaker’s
Bureau, Stock/Bonds excluding mutual funds,
Consultant, Other - identify)
CME Content Will Include Discussion/
Reference to Commercial Products/Services
Disclosure of Off-Label (Unapproved)/Investigational Uses
of Products AAP CME faculty are required to
disclose to the AAP and to learners when they plan to discuss or
demonstrate pharmaceuticals and/or medical devices that are not approved
Ellen Buerk, MD, FAAP
No No No No
Meg Fisher, MD, FAAP
No No No No
Robert A. Wiebe, MD, FAAP
No No Not sure No
Jack Dolcourt, MD, FAAP
No No No No
Thomas W. Pendergrass, MD, FAAP
No No No No
Beverly P. Wood, MD, FAAP No No No No

CME CREDIT
The American Academy of Pediatrics (AAP) is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
The AAP designates this educational activity for a
maximum of 1.0 AMA PRA Category 1 Credit™. Physicians should only claim credit commensurate with the extent of their participation in the activity.
This activity is acceptable for up to 1.0 AAP credit.
This credit can be applied toward the AAP CME/CPD Award available to Fellows and Candidate Fellows of the American Academy of Pediatrics.

OTHER CREDIT
This webinar is approved by the National Association of Pediatric Nurse Practitioners (NAPNAP) for 1.2 NAPNAP contact hours of which 0.3 contain pharmacology (Rx) content. The AAP is designated as Agency #17. Upon completion of the program, each participant desiring NAPNAP contact hours should send a completed certificate of attendance, along with the required recording fee ($10 for NAPNAP members, $15 for nonmembers), to the NAPNAP National Office at 20 Brace Road, Suite 200, Cherry Hill, NJ 08034-2633.
The American Academy of Physician Assistants
accepts AMA PRA Category 1 Credit(s)TM from organizations accredited by the ACCME .

Rainu Kaushal, MD, MPHAssociate Professor of Pediatrics and Public Health,Weill Medical College of Cornell UniversityDirector of Pediatric Quality and Safety, KCCH at NYPHNew York, New York

11
The Role of Health Information Technology
in Medication Safety
April 25, 2007
12:00 – 1:00 p.m. EDT

12
Learning Objectives
Upon completion of this activity, you will be able to:
Review the epidemiology of ambulatory medication safety in pediatrics.
Describe the role of health information technology in improving medication safety.
Utilize specific health information technology applications.
13
Historical Perspective
In 1925, 4 main types of adverse events identified for hospitalized patients: Burns due to hot water Delirious patients jumping from hospital
windows Accidents connected with hospital elevators Mistakes in the use of drugs
Aikens C. Study in the Ethics for Nurses. Philadelphia: Saunders; 1925

14
Patient Safety and Medical Errors Become a National Concern
November 29, 1999

15

16
IOM Report: Preventing Medication Errors
One medication error per day per inpatient Variation across institutions
At least 25% of injuries from medications are preventable
Annual preventable injuries from medications 380,000-450,000 in hospitals for $3.5 billion 800,000 in long-term care 530,000 in Medicare ambulatory patients for $887 million

17
Preventing Medication Errors: Recommendations Patient’s rights and enhancing consumer
information Utilizing HIT
Prescribing and transmission of all prescriptions electronically by 2010
Appropriate clinical decision support Adopt other appropriate technology (eMAR, bar
coding, smart iv pumps) Monitor for medication errors Standards for HIT
More research Pediatrics a prime focus area

18
Overview
Why medication errors occur in children Pediatric medication error epidemiology
Inpatient Outpatient
Prevention strategies HIT
Safety and qualityFinancial

19
Why medication errors occur in children
Weight based dosing Stock medicine dilution Ten fold errors Decreased communication abilities Inability to self-administer medications Increased vulnerability of young, critically ill
children Immature renal and hepatic systems

20
Definitions
Near Misses
ADEs
Medication Errors

21
Comparisons of Adult and Pediatric Inpatients
Pediatrics Adults**
Orders reviewed 10,778 10,070
Medication errors 616 (5.7%) 530 (5.3%)
Near Misses 115 (1.1%) 35 (0.35%) *
ADEs 26 (0.24%) 25 (0.25%)
Preventable ADEs 5 (0.05%) 5 (0.05%)
*p value <0.05
**Study performed at Brigham and Women’s Hospital in 1992 using similar methods Kaushal et al, JAMA 2001

22
Error Stage for Medication Errors
Ordering74%
Administer2%
Monitor1%
Dispense13%
Transcribe10%

23
Near Misses in the NICU per 100 orders
2.8
1.3
0.77
0.35
0
0.5
1
1.5
2
2.5
3
NICU PICU Med/Surg Adult
**
* P<0.001JAMA 2001;285;2114-20
*

24
Ambulatory Setting: Medication Errors
2952 medication 2952 medication errorserrors 1.6 errors per 1.6 errors per
patientpatient 1.3 errors per 1.3 errors per
prescriptionprescription 521 (12%) rx 521 (12%) rx
inappropriate inappropriate abbreviationabbreviation
1389 (64%) rx 1389 (64%) rx partially illegiblepartially illegible
WeightOtherDoseRouteAmountStrength

25
Preliminary Results For Six Office Practices
Rate N 95% CI
Preventable ADEs 3% 57 3-4
Non-preventable ADEs
13% 226 11-15
Ameliorable ADEs 9% 152 7-10
Non-intercepted Near Misses
25% 455 22-29

26
Stages
Administering
Ordering
Dispensing
Transmitting
Administering
Ordering
Dispensing
Transmitting
Preventable ADEs Near Misses
27
Why Do Errors Occur?
Physician writes an order Nursing, pharmacist, and clerical staff
mechanisms are in place to carry out orders What occurs in reality?

28
We deliver medications in hospitals in a manner that essentially hasn’t changed in 60 years.
physician writes order
secretary transcribes
secretary faxes
nurse double checks
pharmacist checksdrug interactions
pharmacist checksorder/allergies
pharmacist enter order
pharmacist receives fax
nurse checks drugagainst med sheets
nurse obtains drugfrom delivery system
pharmacy tech placesdrawer in delivery system
pharmacy tech loadsdrawer
nurse checks patient,drug, dose, route, time
nurse administersdrug
Is a double checknecessary?
Is drug administeredvia pump
If order incorrect:multiple other steps

29
We deliver medications in hospitals in a manner that essentially hasn’t changed in 60 years.
physician writes order
secretary transcribes
secretary faxes
nurse double checks
pharmacist checksdrug interactions
pharmacist checksorder/allergies
pharmacist enter order
pharmacist receives fax
nurse checks drugagainst med sheets
nurse obtains drugfrom meditrol
pharm. tech placesdrawer in meditrol
pharm. tech loadsdrawer
nurse checks patient,drug, dose, route, time
nurse administersdrug
Is a double checknecessary?
Is drug administeredvia pump
If order incorrect:multiple other steps
Consider: What’s the error rate in each one of
Consider: What’s the error rate in each one of
these steps - 5%, 1%, 0.1%, 0.01%
these steps - 5%, 1%, 0.1%, 0.01%
30
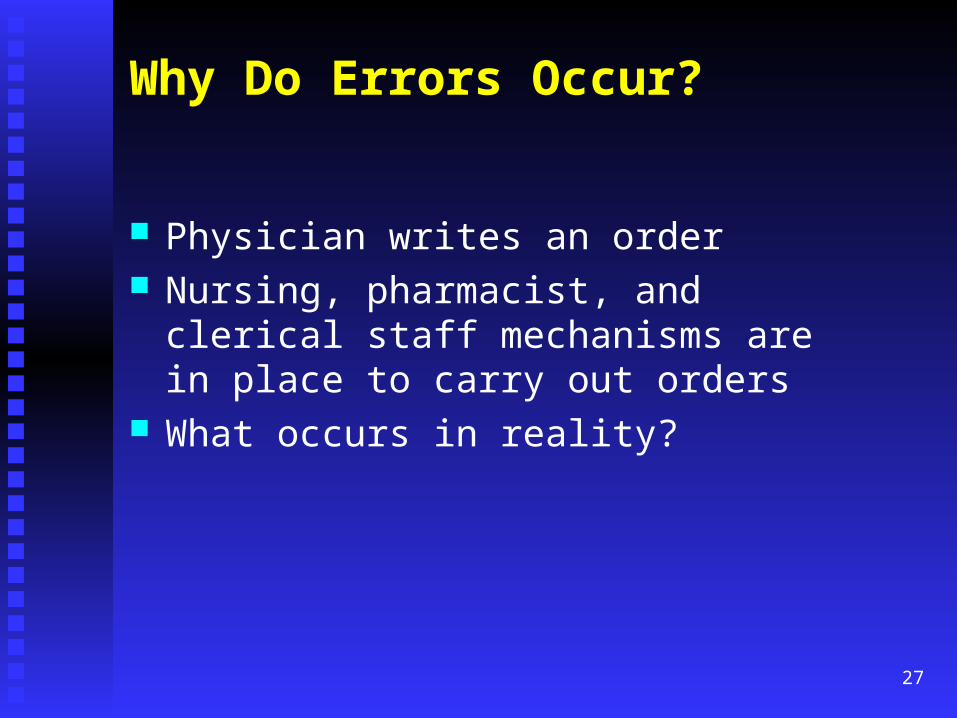
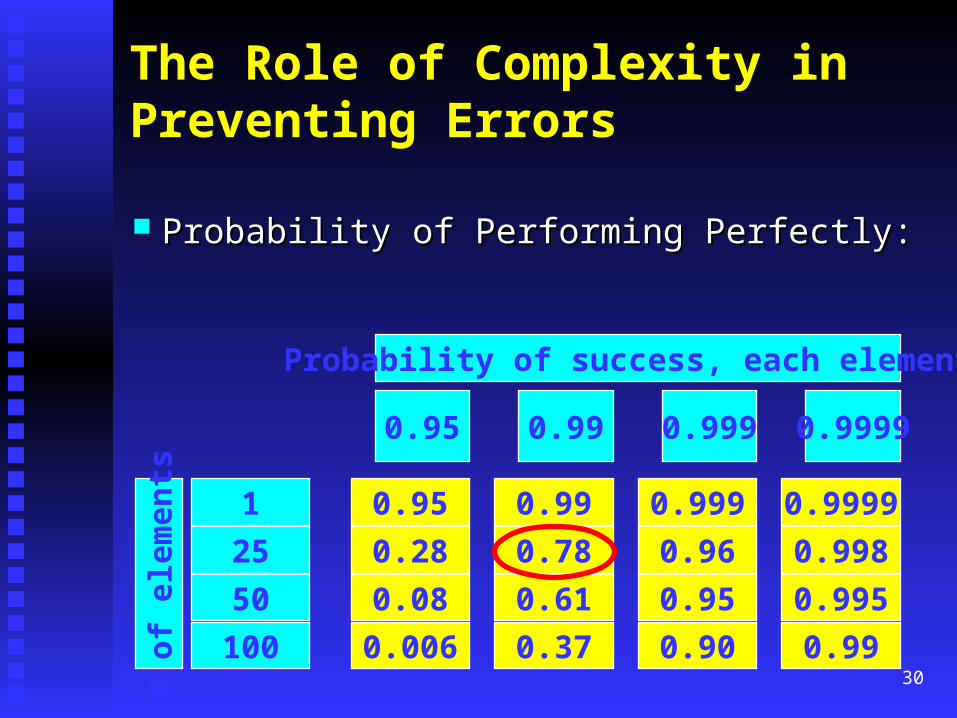
The Role of Complexity inPreventing Errors
Probability of Performing Perfectly:Probability of Performing Perfectly:
# of
ele
men
ts
100
50
1
25
0.006
0.08
0.95
0.28
0.37
0.61
0.99
0.78
0.90
0.95
0.999
0.96
0.99
0.995
0.9999
0.998
0.95 0.99 0.999 0.9999
Probability of success, each element:

31
No one makes an error on purpose.
Lucian LeapeLucian Leape
32
Everyone makes dumb mistakes every day.
33
No one admits an error if you punish them for it.

34
Error Reduction: Systems Approach Culture of Safety
Non-punitive systems Multidisciplinary error prevention
Involve parents and families Executive walk rounds Medication Safety Initiative
Strong, clear, visible attention to safety Avoid fatigue Minimize distractions Independent double checks
2nd checker will detect ~ 90% of errors made by first checker
HIT
35
How will HIT help?
Improve communication What has been done and by whom
Improve accessibility Paper records unavailable 1/3 of the time Physicians spend 20-30% of their time searching
for and organizing information Require key pieces of information Improve information retrieval
Impossible to store all needed clinical information in a physician’s head

36
How will HIT help? (cont)
“Just in time” decision support Assist with calculations Make the right thing the easiest to do Perform checks in real-time
Assist with monitoring Advance the quality agenda
Quality measurement Low cost way to diffuse evidence-based best
practices

37
Impact of HIT on Quality, Efficiency and Costs
4 Benchmark institutions4 Benchmark institutions QualityQuality
Increased adherence to guidelinesIncreased adherence to guidelines Enhanced surveillance and monitoringEnhanced surveillance and monitoring Medication errorsMedication errors
EfficiencyEfficiency Decreased utilization of careDecreased utilization of care
FinancialFinancial
Chaudhry B et al, Annals 2006

38
Types of HIT
EHR, Electronic health record CPOE, Computerized physician order entry Robots Smart IV systems Bar coding Telemedicine Automated drug delivery systems

39
CPOE: Low hanging fruit
Illegible handwriting Incomplete information Unacceptable Abbreviations Lack of leading zeros Inclusion of trailing zeros

40
Key Areas of Decision Support
Requiring complete ordersRequiring complete orders Default dosesDefault doses Drug-allergy checkingDrug-allergy checking DDI checkingDDI checking Renal dosingRenal dosing Geriatric dosingGeriatric dosing Drug-lab checkingDrug-lab checking Dose ceilingsDose ceilings

41
Handwriting example

42
“Corollary” order reminders reduce errors of omission
Target - corollary order pairs (n=87) NSAID – creatinine level Aminoglycoside – drug levels, creatinine Warfarin – routine protimes
Intervention -- display reminder at time of ordering
Overhage JAMIA 1997;4:364-375

43
Effect of alerts on compliance
Overhage JAMIA 1997;4:364-375

44
Proportion of doses exceeding recommended maximum
2.10%
0.60%
0.00%
0.50%
1.00%
1.50%
2.00%
2.50%
Paper-based Computer ordering
Teich Archives Int Med 2000;160:2741

45
Dosing appropriateness in patients with renal impairment
67%
54%59%
35%
0%10%20%30%40%50%60%70%
Doseappropriate
Frequencyappropriate
Intervention Control
Both resultsP < 0.001
Chertow JAMA 2001;286:2839-44

46
Effect of an antibiotic advisor
35
146
0
20
40
60
80
100
120
140
160
Orders for drugs to whichpatient is allergic
87
405
0
100
200
300
400
500
Excess drug dosages
12
206
0
50
100
150
200
250
Antibiotic-susceptibilitymismatches
4
28
0
5
10
15
20
25
30
ADEs caused by antiinfectiveagent
Intervention Control
All results statistically significantCosts, LOS also reduced
Evans NEJM 1998;338:232-238

Effect of Changing Default Dosing Frequency for Ceftriaxone
0
10
20
30
40
50
60
Week
Ord
ers/
wee
k BIDQD

48
Computer suggests300 mg every 8 hours for this patient; based
on age and weight
NYPH -- Pediatric dosing decision support
Evaluation•32% of suggestions accepted exactly•Good reasons for not following•Subjectively, physicians like it
(Killela B, et al; Pediatrics, 2007)

Results of Two Studies on Medication Error Prevention
CPOE reduced medication errors by 80% CPOE reduced serious medication errors by
55%
Bates et al, JAMA 1998

50
Evidence of Reduction in Errors
CPOE Pittsburgh Children’s Harmful ADEs pre-CPOE 0.05/1000 doses Post-CPOE 0.03/1000 doses (p=0.05). CPOE prevents 1 ADE every 64 patient days
Upperman et al. J Pediatr Surg 2005;40:57-59

51
Evidence of Reduction in Errors
Mullett Stand alone anti-infective CDSS in PICU 59% decrease in the rate of pharmacy
interventions for wrong drug doses Potts
CPOE and medication ordering errors in PICU Medication errors reduced 96%
Near misses reduced 41%
Mullett CJ, et al. Pediatrics 2001;108:75-81
Potts AL, et al. Pediatrics 2004;113:59-63

52
So what’s the problem?
High federal and state policy interestHigh federal and state policy interest Leapfrog group identified as 1 of 3 patient safety Leapfrog group identified as 1 of 3 patient safety
‘leaps’‘leaps’ Only 10-15% of hospitals across the country have Only 10-15% of hospitals across the country have
active CPOE systemsactive CPOE systems Few primary care physicians have CPOEFew primary care physicians have CPOE High stakesHigh stakes
Enormous institutional investmentEnormous institutional investment Well-publicized ‘failures’Well-publicized ‘failures’

53
Unintended Consequences
““I have ordered the test that was right next I have ordered the test that was right next to the one I thought I ordered, you know, to the one I thought I ordered, you know, right below it that little thingie had come right below it that little thingie had come down and I clicked and I’m lookin’ at this down and I clicked and I’m lookin’ at this one but I in fact clicked on the thing before. one but I in fact clicked on the thing before. By that time I turned my head and I’m By that time I turned my head and I’m hitting return and typing my signature and hitting return and typing my signature and not seeing it.”not seeing it.”
Ash, JAMIA 2005

54
$$$,$$$,$$$ High cost and lack of capital
“The number one [barrier] is cost. I have been doing hospital software for 29 years, and this is the most expensive project I’ve ever done.”
Cost benefit mis-match “[CPOE] may save a lot of money [for] the health care
system overall, but [the money] is not being collected by the hospital.”
For ambulatory CPOE, assuming 11.6% capitation rate nationally 11% of ROI accrues to providers 89% to other stakeholders, primarily payers

55
Errors in AdministrationIV Infusions
Rule of 6’s intended for rapid dose calculation and drug preparation If:
conc of drug (mL/100 ml) = 6 x patient weight (kg) Then:
dose (µg/kg per min) = rate (mL/hour) Calculation intensive Numerous possible concentrations
If use standard drug concentrations, then rely on dosing charts

56
Errors in AdministrationIV Infusions
IV syringe pumps Traditional infusion pumps prone to ADEs Errors due to keypad data entry mistakes Free-flow phenomena

57
Smart Pumps
Library of medications with standard concentrations specific to patient population
Makes calculations
“Safety net”
Hard limits (range cannot be overridden)
Soft limits (can be overridden)
Pump alarms and halts infusion if medication dose is programmed outside preset limits

58
0
0.5
1
1.5
2
2.5
3
3.5
Reported Errors
PreinterventionErrors, per 1000
doses
PostinterventionErrors, per 1000
doses
Larsen et al. Pediatrics 2005
*
*p<0.001
Smart Pump with Standard Concentrations and Redesigned Labels

59
Safe Practices for Communicating Test Results
Critical ambulatory safety issue 75% of physicians did not notify patients
of normal results 33% of physicians did not even notify of
abnormal results (Boohaker et al, Archives 1996)
Approximately 1/3 of women with abnormal mammograms or pap smears do not receive appropriate follow-up care
60
Improving Result Management Systems
Can be integrated with Electronic Medical Records A tool that allows focus on truly abnormal test
results A tool that warns physicians if patients have missed
tests Use of standardized features, such as “ticklers” Paper systems can also be highly successful Standardized procedures rather than every physician
doing it his/her own way

61
Results Manager Application
Strategy: Automate CarefullyStrategy: Automate Carefully
EHREHR CPOECPOE Smart IV systemsSmart IV systems RobotsRobots Automated drug delivery systemsAutomated drug delivery systems Bar codingBar coding
Inexpensive technologyInexpensive technology 63% reduction in serious dispensing errors 63% reduction in serious dispensing errors
at BWHat BWH

63
Conclusions
Make safety top priority Move from a culture of blame to one of safety
Stop blaming people for making errors To err is human
Improve the system Utilize technology as it becomes available Involve patients/parents to the fullest extent Measure and iteratively refine
Related Documents