The Ritvo Autism Asperger The Ritvo Autism Asperger Diagnostic Diagnostic Scale Revised (RAADS-R) Scale Revised (RAADS-R) A scale to assist the diagnosis of autistic spectrum disorder in adults- An international validation study with nine participating centers Ariella Riva Ritvo, Ph.D., Yale Edward R. Ritvo, MD., UCLA Donald Guthrie, Ph.D., UCLA Max Ritvo, Yale University Demetra Hufnagel, Yale University Daniela Markovic, MS., UCLA Participating Centers: Ami Klin, Ph.D., Yale; Latha Soorya, Ph.D. Mt. Sinai; William McMahon, MD, Kim Moody, U of Utah; David Mataix-Cols, Ph.D., King’s Collge; Bruce Tonge, MD, Avril Brereton, PhD, Monash University; Trevor Clark, Ph.D, Vicki Gibbs, Fiona Aldridge, Megan Williams, ASPECT, Sydney; Tony Attwood, Ph.D, J. Eloff, Ph.D. Griffith University; Stephanie Moeser-Warren, Geneva Center, Toronto; Lisa Andersen, Susanne Bejerot, MD, PhD. Karolinska Institute IMFAR 2010 IMFAR 2010 PHILADELPHIA PHILADELPHIA

The Ritvo Autism Asperger Diagnostic Scale Revised (RAADS-R) A scale to assist the diagnosis of autistic spectrum disorder in adults- An international.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
The Ritvo Autism Asperger DiagnosticThe Ritvo Autism Asperger DiagnosticScale Revised (RAADS-R)Scale Revised (RAADS-R)
A scale to assist the diagnosis of autistic spectrum disorder in adults-An international validation study with nine participating centers
Ariella Riva Ritvo, Ph.D., Yale Edward R. Ritvo, MD., UCLADonald Guthrie, Ph.D., UCLA
Max Ritvo, Yale UniversityDemetra Hufnagel, Yale University
Daniela Markovic, MS., UCLA
Participating Centers: Ami Klin, Ph.D., Yale; Latha Soorya, Ph.D. Mt. Sinai; William McMahon, MD, Kim Moody, U of Utah;David Mataix-Cols, Ph.D., King’s Collge; Bruce Tonge, MD, Avril Brereton, PhD, Monash University;
Trevor Clark, Ph.D, Vicki Gibbs, Fiona Aldridge, Megan Williams, ASPECT, Sydney;Tony Attwood, Ph.D, J. Eloff, Ph.D. Griffith University; Stephanie Moeser-Warren, Geneva Center, Toronto;
Lisa Andersen, Susanne Bejerot, MD, PhD. Karolinska Institute
IMFAR 2010IMFAR 2010PHILADELPHIAPHILADELPHIA
IMFAR 2010IMFAR 2010PHILADELPHIAPHILADELPHIA

© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 2
BackgroundBackground The RAADS-R is a modified version of the Ritvo Autism Asperger
Diagnostic Scale. The rationale for its development, its method of construction, and its comparison to other similar scales have been published in JADD in 2008 .
The first version of the RAADS contained 78 questions. Published data demonstrated it had high validity, reliability, sensitivity, and specificity in a limited number of subjects.
Questions on the initial RAADS assess developmental pathology in three symptom areas: language, social relatedness, and sensory-motor (re. DSM-IV-TR). After critical review and the results of a factor analysis, a revised 80-item version was developed (the RAADS-R) with the addition of a fourth symptom area (circumscribed interests), two questions, and several word clarifications.

© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 3
ObjectivesObjectives
To describe the methods and present the results of the nine university international standardization study of the new 80-item RAADS-R.
© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 4
MethodsMethods1. A uniform protocol was used by all centers
2. IRB consent was obtained by each center
3. All subjects signed informed consent
Participating Subject Groups: Autism Spectrum Disorder Subjects N = 201
1. 66 subjects with a diagnosis of Autistic Disorder
2. 135 subjects with a diagnosis of Asperger’s Disorder
Comparison Subjects N = 5781. 276 subjects with no DSM-IV-TR diagnosis
2. 302 subjects with other DSM-IV-TR diagnoses
© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 5
MethodsMethods ASD Subjects (groups 1 and 2 n = 201)
Uniformly diagnosed by research criteria : 1. A clinical interview (DSM-IV-TR diagnostic criteria met) 2. ADI/ADOS Scale (ADOS module IV at least) to establish
concurrent validity3. Standardized IQ test, (WAIS or WASI) full IQ of =/> 80 4. Constantino Social Responsiveness Scale-Adult (SRS-A)
to assess concurrent validity when available (69 subjects) 5. Repeat testing to assess reliability
Comparison subjects (groups 3 and 4 n = 578 ):1. Volunteers without a DSM-IV-TR diagnosis2. Volunteers with current DSM-IV-TR diagnosis other than
ASD

© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 6
MethodsMethods Administration of RAADS-R:
1. ASD subjects: Following initial screening, a clinician interviewed each subject to confirm the diagnostic information and IQ data, completed the ADI/ADOS or ADOS module IV, and then introduced the scale and explained how to answer the questions. The clinician remained with each subject as the questions were being answered to offer clarifications when asked, and to make sure answers were entered in the proper columns on the Likert scale. An SRS–A scale was obtained from cooperating accompanying adults when available.
2. Comparison Subjects: All were given the RAADS-R to complete in the presence of a clinician. All comparison subjects were clinically evaluated to determine that their IQ was 80 or above.
3. Each of the 9 participating centers was asked to score, review and mail in full packets of ASD subjects. Some of the participating centers contributed data to the comparison group subject pool.
© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 7
TranslationsTranslations Translations took into account cultural/idiomatic variations.
Questions addressed core symptoms regardless of language, which will allow for standardization of results and assessment of validity and reliability. Some studies are well on their way (Swedish and Japanese) while others (French and Hindi) are in early stages. Standard protocol and translation methods are being followed.
Studies are being conducted in:1. Swedish: Lisa Andersen, Ph.D, Susanne Bejerot, MD,
PhD, Karolinska Institute2. Japanese: Prof. Masatsugu Tsujii, Kaori Matsumoto, Kenji
Tsuchiya, Nagoya, Japan3. Hindhi4. French
© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 8
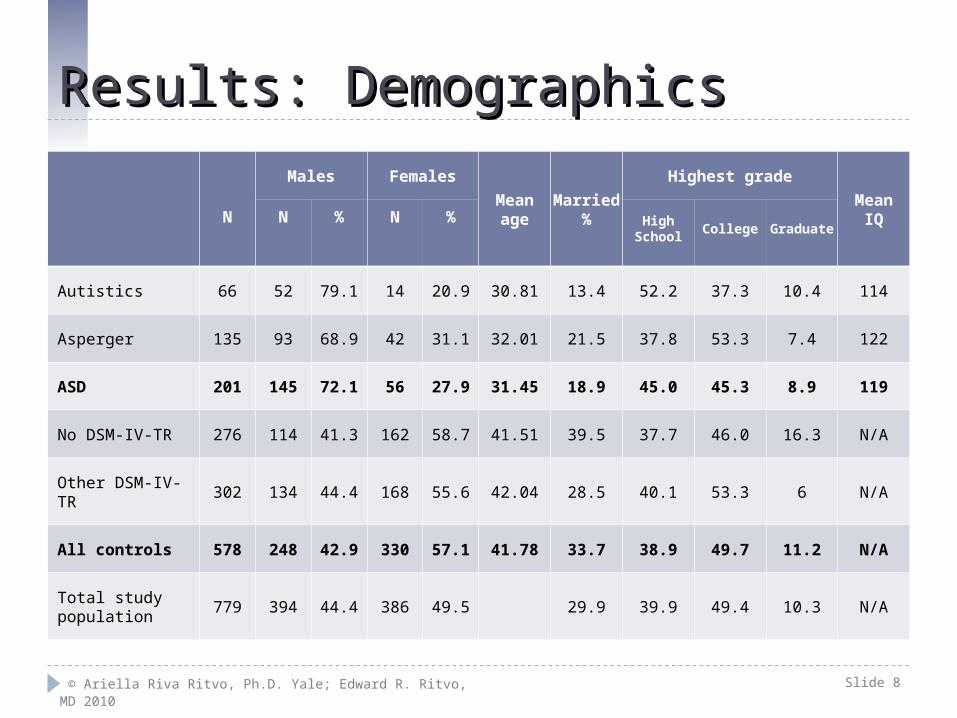
Results: DemographicsResults: Demographics
N
Males Females
Meanage
Married%
Highest grade
MeanIQN % N % High
SchoolCollege Graduate
Autistics 66 52 79.1 14 20.9 30.81 13.4 52.2 37.3 10.4 114
Asperger 135 93 68.9 42 31.1 32.01 21.5 37.8 53.3 7.4 122
ASD 201 145 72.1 56 27.9 31.45 18.9 45.0 45.3 8.9 119
No DSM-IV-TR 276 114 41.3 162 58.7 41.51 39.5 37.7 46.0 16.3 N/A
Other DSM-IV-TR 302 134 44.4 168 55.6 42.04 28.5 40.1 53.3 6 N/A
All controls 578 248 42.9 330 57.1 41.78 33.7 38.9 49.7 11.2 N/A
Total study population
779 394 44.4 386 49.5 29.9 39.9 49.4 10.3 N/A

© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 9
ResultsResults Diagnostic Accuracy (Sensitivity and Specificity):
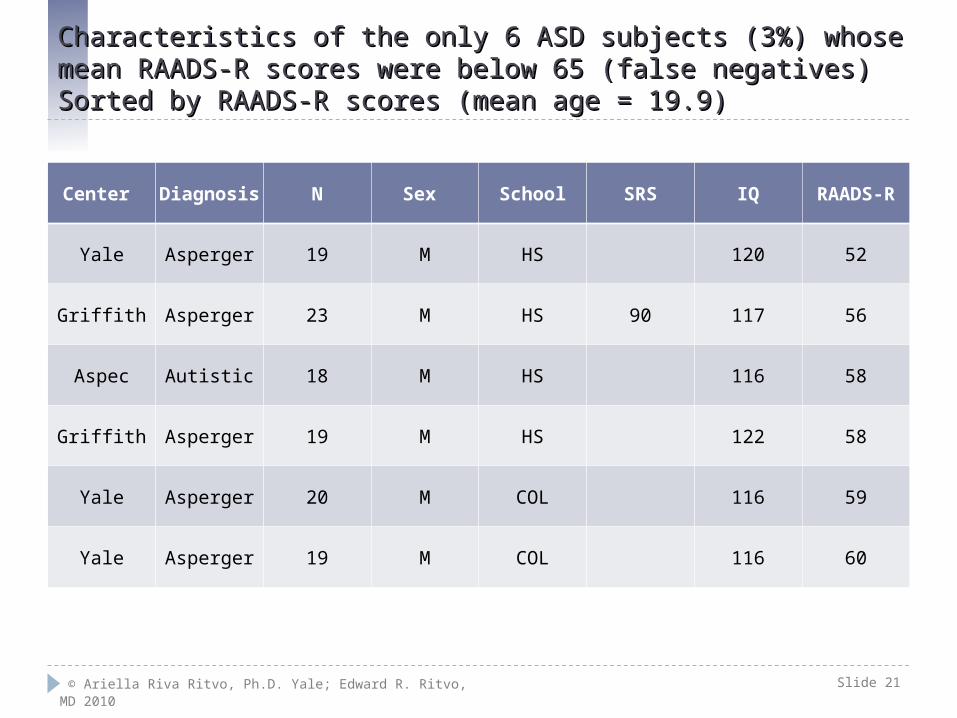
Utilizing a cut off RAADS-R score of 65, six ASD subjects from three of the nine centers scored below, and thus were in the non ASD range. They are labeled “false negatives,” yielding sensitivity for the RAADS-R of 97%. None of the comparison subjects scored above 65, so there were no false positives. Thus the specificity for the RAADS-R is 100%.
Pair-wise comparison of each of the 80 questions Post-hoc unequal variance t-tests were performed for pair-wise comparison of
each of the 80 questions. The ASD subjects differed significantly from the comparison groups on all 80 questions (p < 0.0001 for all questions).
The mean RAADS-R scores of the ASD, the Autistic, and the Asperger groups from all nine centers are significantly different (p < 0.0001) from the combined mean of the comparison groups, and the mean for each of the nine research centers.
Cronbach Alpha coefficients demonstrate good internal consistency.
© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 10 © Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 10
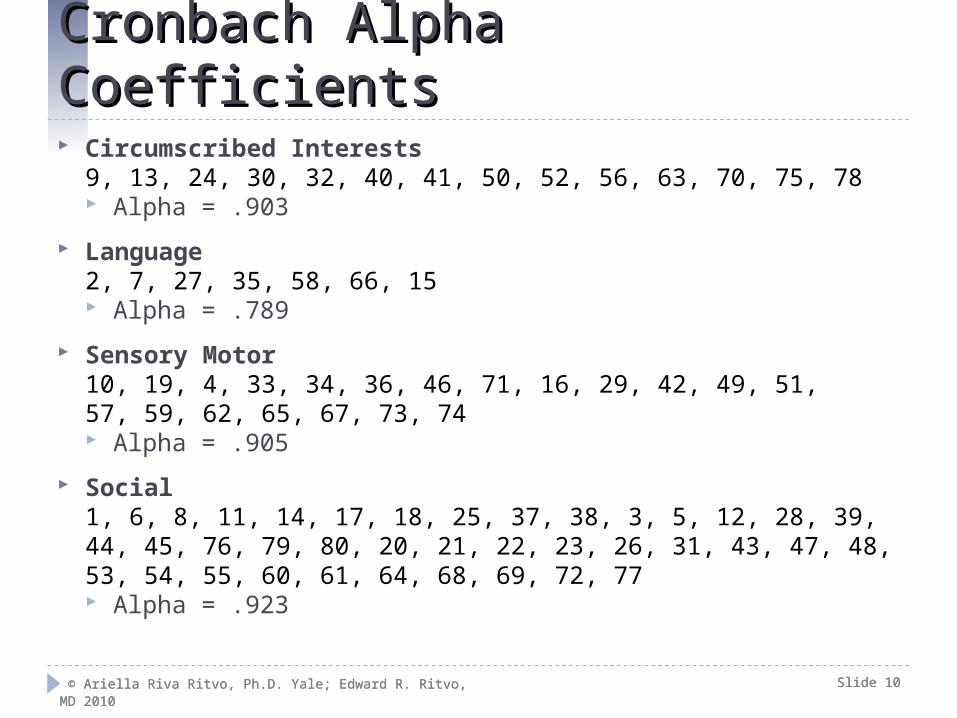
Cronbach Alpha CoefficientsCronbach Alpha Coefficients Circumscribed Interests
9, 13, 24, 30, 32, 40, 41, 50, 52, 56, 63, 70, 75, 78 Alpha = .903
Language2, 7, 27, 35, 58, 66, 15 Alpha = .789
Sensory Motor10, 19, 4, 33, 34, 36, 46, 71, 16, 29, 42, 49, 51, 57, 59, 62, 65, 67, 73, 74 Alpha = .905
Social1, 6, 8, 11, 14, 17, 18, 25, 37, 38, 3, 5, 12, 28, 39, 44, 45, 76, 79, 80, 20, 21, 22, 23, 26, 31, 43, 47, 48,53, 54, 55, 60, 61, 64, 68, 69, 72, 77 Alpha = .923
© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 11
Factor AnalysisFactor Analysis Factor Analysis was carried out using both Varimax (orthogonal) and Oblique (non
orthogonal) rotation. Results were compared between the two rotational strategies. The Oblique rotational method was chosen because we assume the underlying constructs are interrelated.
We identified four factors. To compare the model derived factors versus the assigned four subdomains (DSM-IV-TR), we computed the Pearson correlation. Factors I and IV correlated most strongly with the social construct (r =.80). Factor II correlated most strongly with circumscribed interests (r =.78), factor III with sensory motor (r =.88).
The language construct was not picked up with the four factor model. However, the factor analysis is a mathematical computation of clusters and picks up on key words, missing the nuances in these questions. For instance, the question: “the phrase ‘I’ve got you under my skin’ makes me feel uncomfortable” is clearly a language construct question and targets concrete language and lack of understanding symbolic language. The factor analysis loaded it as a sensory motor question, most likely because it contained the words “skin” and “uncomfortable”.
We will report the variances accounted for by each factor and the Cronbach alpha coefficients, but upon review of the loadings, we remain confident that the original assignments of questions reflect the clinical picture with more clinical relevance. Either way, the instrument has good internal consistency.
© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 12
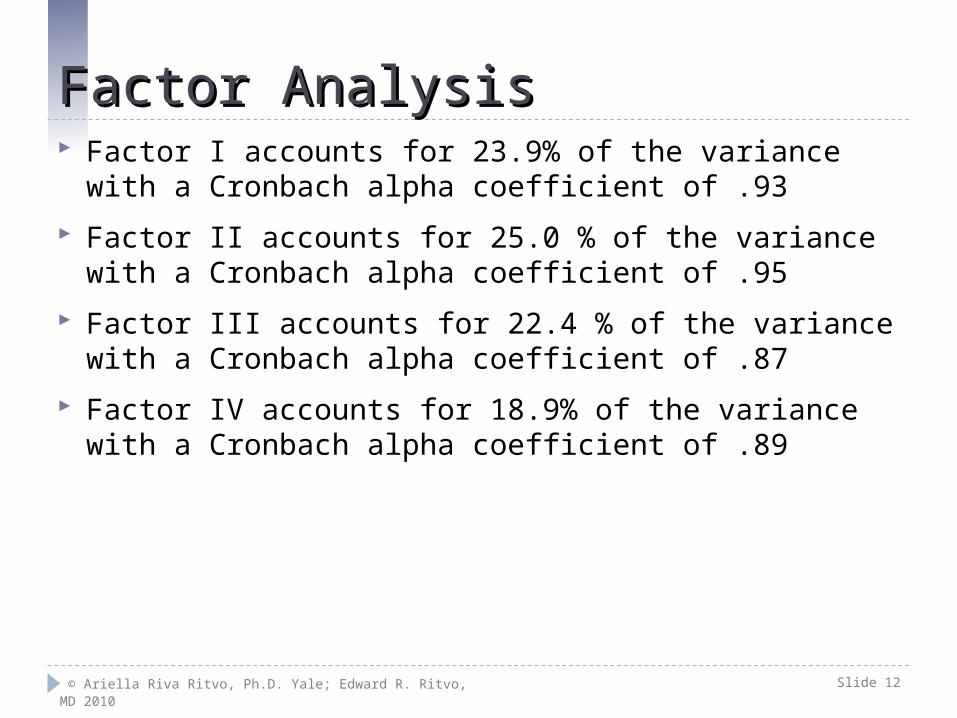
Factor AnalysisFactor Analysis Factor I accounts for 23.9% of the variance with a Cronbach
alpha coefficient of .93
Factor II accounts for 25.0 % of the variance with a Cronbach alpha coefficient of .95
Factor III accounts for 22.4 % of the variance with a Cronbach alpha coefficient of .87
Factor IV accounts for 18.9% of the variance with a Cronbach alpha coefficient of .89
© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 13
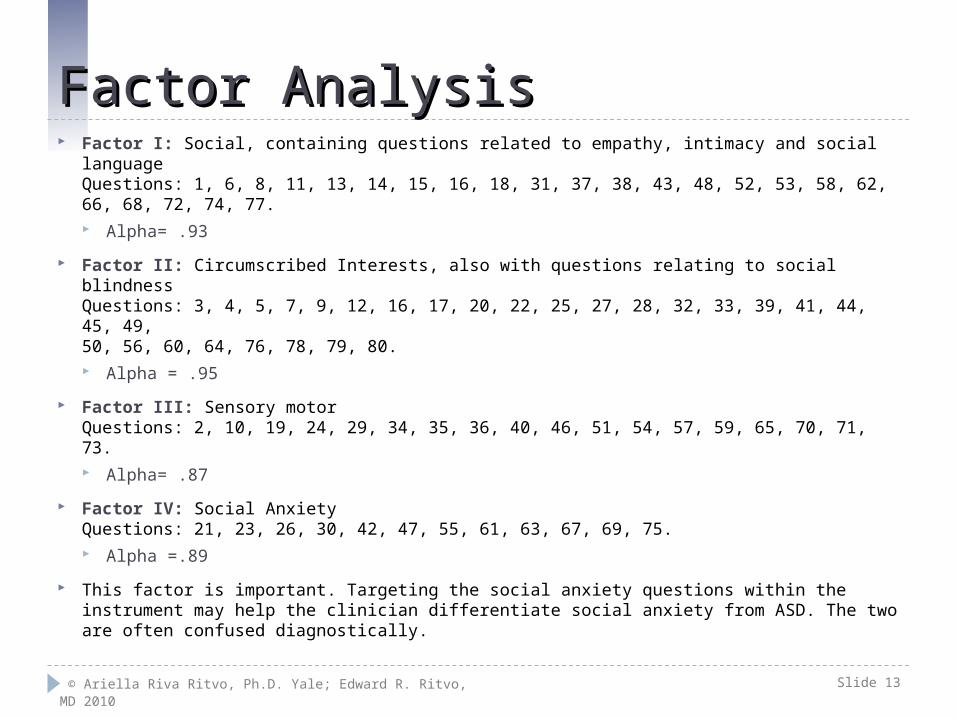
Factor AnalysisFactor Analysis Factor I: Social, containing questions related to empathy, intimacy and social language
Questions: 1, 6, 8, 11, 13, 14, 15, 16, 18, 31, 37, 38, 43, 48, 52, 53, 58, 62, 66, 68, 72, 74, 77. Alpha= .93
Factor II: Circumscribed Interests, also with questions relating to social blindnessQuestions: 3, 4, 5, 7, 9, 12, 16, 17, 20, 22, 25, 27, 28, 32, 33, 39, 41, 44, 45, 49, 50, 56, 60, 64, 76, 78, 79, 80. Alpha = .95
Factor III: Sensory motorQuestions: 2, 10, 19, 24, 29, 34, 35, 36, 40, 46, 51, 54, 57, 59, 65, 70, 71, 73. Alpha= .87
Factor IV: Social AnxietyQuestions: 21, 23, 26, 30, 42, 47, 55, 61, 63, 67, 69, 75. Alpha =.89
This factor is important. Targeting the social anxiety questions within the instrument may help the clinician differentiate social anxiety from ASD. The two are often confused diagnostically.

© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 14
Test – Retest ReliabilityTest – Retest Reliability mean interval between tests = 15 months
SubjectsN
Mean RAADS-R1st Test
Mean RAADS-R2nd Test
ASD subjects 15 155 149
Comparison subjects 15 20 21

© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 15
Test – Retest Data Statistical Analysis Test – Retest Data Statistical Analysis
Subject group Number Pearson r= Spearman Rho=
All subjects 30 .987 .956
Autistic 7 1.0 1.0
Asperger 8 .939 .952
Comparisons 15 .874 .764
© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 16
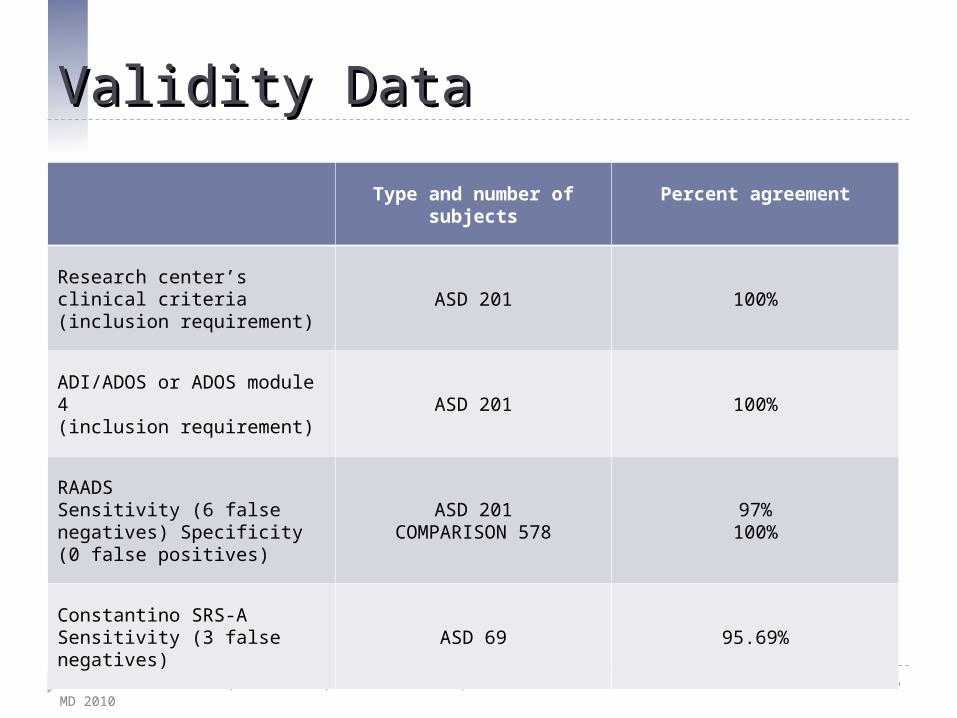
Validity DataValidity Data
Type and number of subjects
Percent agreement
Research center’s clinical criteria (inclusion requirement)
ASD 201 100%
ADI/ADOS or ADOS module 4(inclusion requirement)
ASD 201 100%
RAADSSensitivity (6 false negatives) Specificity (0 false positives)
ASD 201COMPARISON 578
97%100%
Constantino SRS-ASensitivity (3 false negatives)
ASD 69 95.69%
© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 17
Validity Data-Constantino Social Responsiveness Scale, Adult (SRS-A)Validity Data-Constantino Social Responsiveness Scale, Adult (SRS-A)
69 SRS-A were administered to a 3rd party (e.g. parent, spouse).
SRS-A cutoff t score is 59. Three subjects (4.31 percent) scored below the cutoff (55, 57 and 58). This is a 95.59% concordance rate with RAADS-R subjects.

© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 18
Mean RAADS-R Scores and Ranges by Research Center: ASD SubjectsMean RAADS-R Scores and Ranges by Research Center: ASD Subjects
Research center NRAADS-R Scores
Mean Min Max
UCLA 53 146 84 222
Yale 31 115 48 178
Mount Sinai 19 123 73 166
University of Utah 7 92 72 109
Monsah University, Australia 13 138 62 172
Aspect, Sydney 14 118 58 193
Griffith University, Australia 42 146 56 227
Geneva Center, Canada 8 148 107 216
University of London 14 135 67 205
© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 19
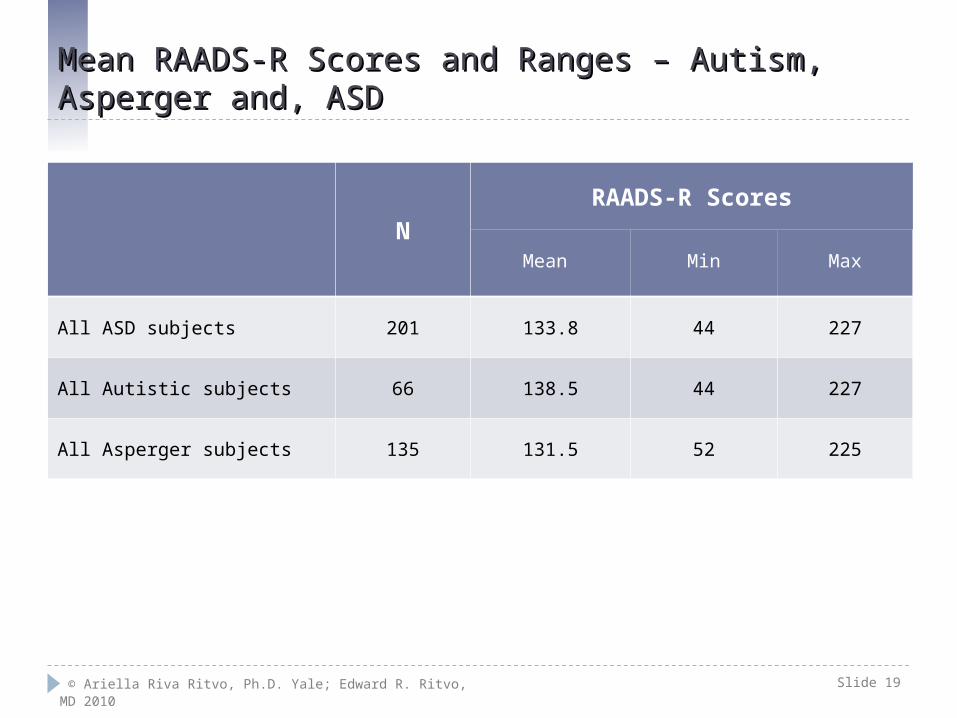
Mean RAADS-R Scores and Ranges – Autism, Asperger and, ASDMean RAADS-R Scores and Ranges – Autism, Asperger and, ASD
N
RAADS-R Scores
Mean Min Max
All ASD subjects 201 133.8 44 227
All Autistic subjects 66 138.5 44 227
All Asperger subjects 135 131.5 52 225

© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 20
Mean RAADS-R Scores and Ranges – Comparison SubjectsMean RAADS-R Scores and Ranges – Comparison Subjects
N
RAADS
Mean Min Max
No DSM-IV-TR diagnosis 275 22 0 64
Other DSM-IV-TR diagnoses 302 30 0 65
Total All Comparison subjects 578 25 0 65
© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 21
Characteristics of the only 6 ASD subjects (3%) whose mean RAADS-R scores Characteristics of the only 6 ASD subjects (3%) whose mean RAADS-R scores were below 65 (false negatives) Sorted by RAADS-R scores (mean age = 19.9)were below 65 (false negatives) Sorted by RAADS-R scores (mean age = 19.9)
Center Diagnosis N Sex School SRS IQ RAADS-R
Yale Asperger 19 M HS 120 52
Griffith Asperger 23 M HS 90 117 56
Aspec Autistic 18 M HS 116 58
Griffith Asperger 19 M HS 122 58
Yale Asperger 20 M COL 116 59
Yale Asperger 19 M COL 116 60
© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 22
ConclusionsConclusions No difficulties were reported in administration even though subjects were evaluated at
nine medical centers on three continents.
The RAADS-R proved to be highly accurate in discriminating between subjects with ASD and those without a DSM-IV-TR diagnosis and with another DSM-IV-TR diagnosis (Sensitivity = 97%. Specificity = 100).
Mean RAADS-R scores were significantly different (p < 0.0001) between ASD and comparison subjects at each of the nine centers and in all centers combined.
All eighty questions significantly differentiated between ASD and comparison subjects. The fact that this was true even when the comparison cases had a variety of DSM-IV-TM diagnoses other than ASD makes the RAADS-R particularly useful in adult clinic clinical settings.
The RAADS-R also demonstrated high test – retest reliability (Pearson Correlation Coefficient = .987, Spearman Correlation Coefficients = .956).
Concurrent validity with ADI/ADOS was 100% and with Constantino SRS-A concordance rate was 95.59%.
© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 23
ConclusionsConclusions Cronbach alphas were good for the four DSM-IV-TR domains, suggesting a good
internal consistency of the RAADS-R.
Factor analysis with oblique rotation to account for assumed correlation between constructs yielded four factors, also with good internal consistency.
Because ASD is a behaviorally defined syndrome with subtle nuances and factor analysis is mathematically based, picking up key words, we prefer to remain with the original question assignment, which reflects the clinical picture more accurately. That being said, the Cronbach alpha coefficients are good either way, and the original subdomains as well as the factors differentiate ASD from non-ASD subjects in a statistically significant way. The instrument was designed to be used as a whole, and all questions ultimately have one measurement—ASD symptomatology.
© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 24
SummarySummary The results from nine medical centers, based on 201
ASD subjects and 578 comparison subjects, demonstrated that the RAADS-R is highly valid, highly reliable, and it is easy to administer and to score. Thus we conclude that it can serve as a valuable asset to assist clinicians diagnosing ASD in adults eighteen years and older.
© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 25
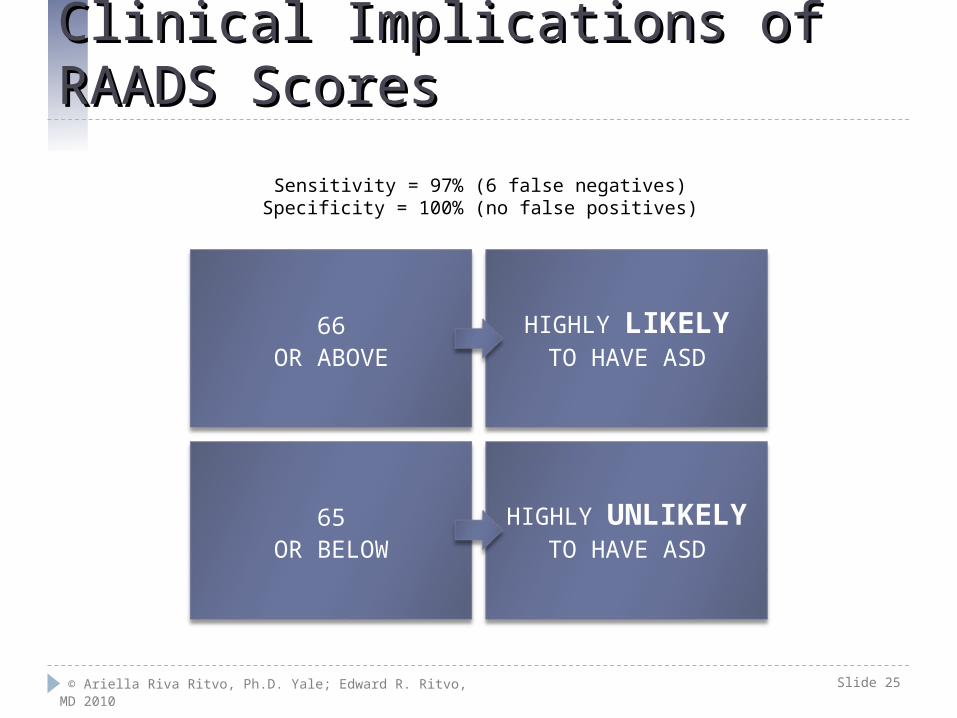
Clinical Implications of RAADS ScoresClinical Implications of RAADS Scores
66OR ABOVE
HIGHLY LIKELYTO HAVE ASD
65OR BELOW
HIGHLY UNLIKELYTO HAVE ASD
Sensitivity = 97% (6 false negatives)Specificity = 100% (no false positives)
© Ariella Riva Ritvo, Ph.D. Yale; Edward R. Ritvo, MD 2010 Slide 26
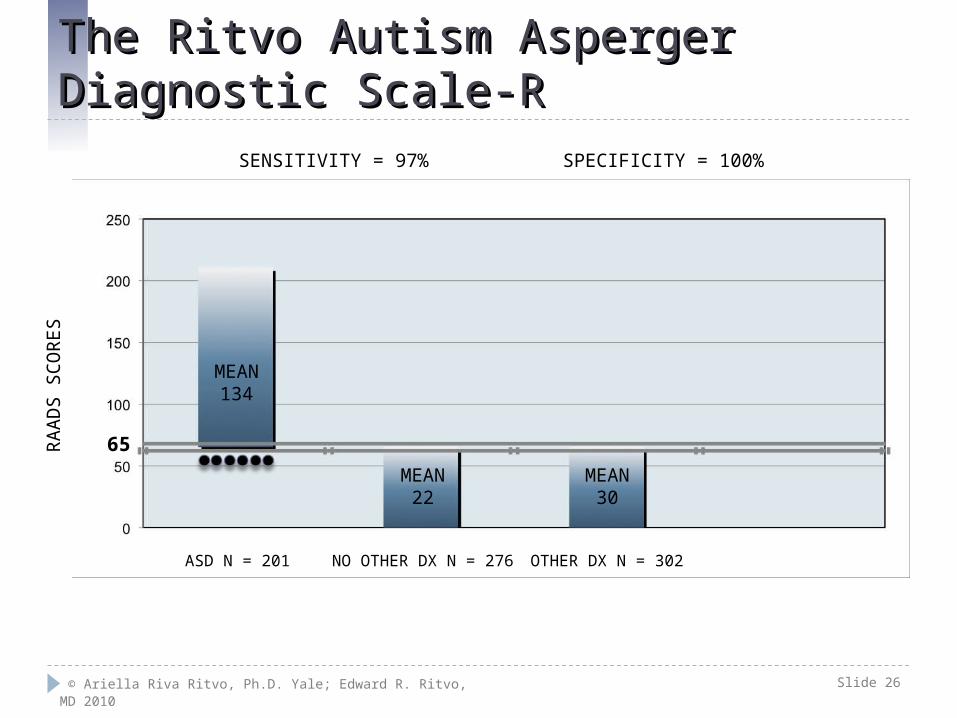
The Ritvo Autism Asperger Diagnostic Scale-R The Ritvo Autism Asperger Diagnostic Scale-R R
AA
DS
SC
OR
ES
ASD N = 201 OTHER DX N = 302NO OTHER DX N = 276
SENSITIVITY = 97% SPECIFICITY = 100%
MEAN134
MEAN22
MEAN30
65
© The Ritvo Autism Asperger Diagnostic Scale Revised (RAADS-R) 2010
Thank you.
Related Documents











