The Relationship between Vitamin B, Metabolism, Asthma, and Theophylline Therapy JOHAN B. UBBINK,“ W. J. HAYWARD VERMAAK, RHENA DELPORT, AND WILLEM J. SERFONTEIN Department of Chemical Pathology University of Pretoria Pretoria 0001, South Africa PETER BARTEL Section of Neurology University of Pretoria Pretoria 0001, South Africa INTRODUCTION Asthma can be broadly defined as enhanced reactivity of the airways to specific and nonspecific stimuli, resulting in diffuse airways obstruction with clinical symptoms like dyspnea, cough, and a tight chest. Stimuli that may provoke asthmatic responses include environmental allergens, respiratory infection, certain drugs such as nonsteroi- dal anti-inflammatory drugs, and exercise.’ An important aspect of asthma treatment is the administration of bronchodilators of which theophylline is most commonly used.2 As will be reviewed in this paper, vitamin B, status and asthma have been studied by several researchers3^’; however, the effect of medication per se on vitamin B, status has not been investigated. Because it would be practically impossible to study vitamin B, status in asthmatics without the use of bronchodilators, we opted for the alternative: to study the effect of bronchodila- tors on vitamin B, metabolism in healthy volunteers. We therefore investigated the effect of theophylline on vitamin B, metabolism in healthy volunteers, and our results are summarized and reviewed in the second part of this paper. VITAMIN B, STATUS AND ASTHMA In 1975, Collipp and coworkers reported increased urinary xanthurenic and kynurenic acid excretion in asthmatic children following oral tryptophan l ~ a d i n g . ~ . ~ Because tryptohan metabolism is vitamin B,-dependent, Collipp and coworkers postu- lated that asthmatic children may suffer from a “pyridoxine dependency,” which might explain the apparent disturbed tryptophan metabolism. Increased tryptophan “Address for correspondence: Dr. J. B. Ubbink, Department of Chemical Pathology, University of Pretoria, P.O. Box 2034, Pretoria 0001, South Africa. 285

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The Relationship between Vitamin B, Metabolism, Asthma, and Theophylline
Therapy JOHAN B. UBBINK,“ W. J. HAYWARD VERMAAK, R H E N A DELPORT, AND WILLEM J . SERFONTEIN
Department of Chemical Pathology University of Pretoria
Pretoria 0001, South Africa
PETER BARTEL Section of Neurology University of Pretoria
Pretoria 0001, South Africa
INTRODUCTION
Asthma can be broadly defined as enhanced reactivity of the airways to specific and nonspecific stimuli, resulting in diffuse airways obstruction with clinical symptoms like dyspnea, cough, and a tight chest. Stimuli that may provoke asthmatic responses include environmental allergens, respiratory infection, certain drugs such as nonsteroi- dal anti-inflammatory drugs, and exercise.’
An important aspect of asthma treatment is the administration of bronchodilators of which theophylline is most commonly used.2 As will be reviewed in this paper, vitamin B, status and asthma have been studied by several researchers3^’; however, the effect of medication per se on vitamin B, status has not been investigated. Because it would be practically impossible to study vitamin B, status in asthmatics without the use of bronchodilators, we opted for the alternative: to study the effect of bronchodila- tors on vitamin B, metabolism in healthy volunteers. We therefore investigated the effect of theophylline on vitamin B, metabolism in healthy volunteers, and our results are summarized and reviewed in the second part of this paper.
VITAMIN B, STATUS AND ASTHMA
In 1975, Collipp and coworkers reported increased urinary xanthurenic and kynurenic acid excretion in asthmatic children following oral tryptophan l ~ a d i n g . ~ . ~ Because tryptohan metabolism is vitamin B,-dependent, Collipp and coworkers postu- lated that asthmatic children may suffer from a “pyridoxine dependency,” which might explain the apparent disturbed tryptophan metabolism. Increased tryptophan
“Address for correspondence: Dr. J. B. Ubbink, Department of Chemical Pathology, University of Pretoria, P.O. Box 2034, Pretoria 0001, South Africa.
285
286 ANNALS NEW YORK ACADEMY OF SCIENCES
metabolism to xanthurenic acid owing to vitamin B, deficiency could normally be corrected by relatively small doses of pyridoxine'; however, Collipp et al. found that three months of pyridoxine supplementation in asthmatic children (50 mg/day) did not normalize urinary xanthurenic acid excretion after oral tryptophan l ~ a d i n g . ~ These results indicated impaired pyridoxine utilization in asthmatics, but the reason for the impaired vitamin B, metabolism was not identified. However, Hall and coworkers,* using erythrocyte aspartate aminotransferase activity with and without in vitro PLP stimulation as an indirect test for vitamin B, status, found no evidence of a vitamin B, deficiency in asthmatic children.
In contrast, Reynolds and Natta, compared 15 adult patients with bronchial asthma to 16 controls and found significantly depressed plasma and erythrocyte pyridoxal-5'-phosphate (PLP) levels in asthmatic patients. Pyridoxine supplementa- tion failed to produce uniform and consistent elevations in plasma PLP levels in asthmatics, while control subjects showed dramatic elevations of plasma PLP concen- trations on the same pyridoxine treatment regimen. From their results, Reynolds and Natta concluded that asthmatics may have altered metabolism of vitamin B,; however, the scientific base for the impaired pyridoxine utilization remained unknown. In a follow-up study, Simon and Reynolds' found that pyridoxine supplementation (1 00 mgfday) resulted in plasma PLP levels that were approximately 30% lower in asthmatics when compared to controls, again indicating altered vitamin B, metabolism in asthmatics.
Delport et al.' confirmed depressed plasma PLP levels in asthmatic patients, but showed that plasma pyridoxal levels were normal, thus suggesting that the depressed plasma PLP levels in asthmatics were not nutritionally induced.
THEOPHYLLINE THERAPY AND VITAMIN B, METABOLISM
Several drugs are known to have an antagonistic effect on vitamin B,. Hydrazine derivatives like phenelzine"." and i s ~ n i a z i d ' ~ ~ ' ' - ' ~ react with PLP and pyridoxal to form hydrazones, resulting in functional inactivation of PLP. Penicillamine has been shown to inactivate PLP by forming a thiazolidine deri~ative,". '~ while the anti- vitamin B, effect of cycloserine" could be explained by Schiff-base formation of the antibiotic with PLP.
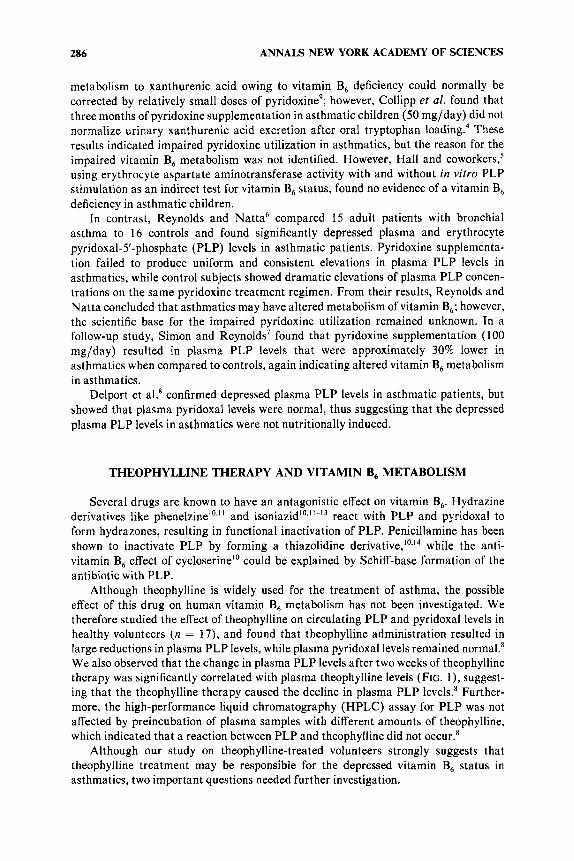
Although theophylline is widely used for the treatment of asthma, the possible effect of this drug on human vitamin B, metabolism has not been investigated. We therefore studied the effect of theophylline on circulating PLP and pyridoxal levels in healthy volunteers ( n = 17), and found that theophylline administration resulted in large reductions in plasma PLP levels, while plasma pyridoxal levels remained normal.' We also observed that the change in plasma PLP levels after two weeks of theophylline therapy was significantly correlated with plasma theophylline levels (FIG. l ) , suggest- ing that the theophylline therapy caused the decline in plasma PLP levels.' Further- more, the high-performance liquid chromatography (HPLC) assay for PLP was not affected by preincubation of plasma samples with different amounts of theophylline, which indicated that a reaction between PLP and theophylline did not occur.'
Although our study on theophylline-treated volunteers strongly suggests that theophylline treatment may be responsible for the depressed vitamin B, status in asthmatics, two important questions needed further investigation.
UBBINK et al.: B,, ASTHMA, THEOPHYLLINE THERAPY 287
1 . Because plasma pyridoxal levels were not affected in either asthmatics or volunteers on theophylline therapy, this could indicate that overall vitamin B, status during theophylline therapy is not seriously impaired. Plasma pyridoxal, being a less polar compound than PLP, is directly available for cellular and is considered the transport form of vitamin B,. Therefore, as cellular supply of pyridoxal remained normal, this could indicate that theophylline therapy had no overall adverse effect on patients’ vitamin B, status.
2. By what mechanism does theophylline lower plasma PLP levels?
9 6
80
6 4
4 8 c5
5 Y
a a 1 32
U
1 6
0
.
. 0 . .
0 0 . . .
0. . 0 . . .
I I
2 6 1 0 14 18
P L A S M A T H E O P H Y L L I N E L E V E L ( m g l P )
FIGURE 1. Scatter diagram of plasma theophylline levels and the change in plasma pyridoxal-5’- phosphate (PLP) levels after two weeks of theophylline therapy in a group of 17 healthy volunteers. Spearman rankcorrelation coefficient (r) = 0.68 ( p < 0.01). (Reprinted from Delport eta[.* with permission of the publisher).
We performed a placebo-controlled, double-blind study to investigate vitamin B, status during a four-week period of theophylline therapy. In addition to plasma PLP and pyridoxal levels, erythrocyte PLP levels and urinary xanthurenic acid excretion after oral tryptophan loading were also used as indexes of vitamin B, status.18
TABLE 1 indicates that theophylline-treated subjects had significantly lower plasma PLP levels, when compared to placebo-treated controls. Plasma pyridoxal, erythrocyte
288 ANNALS NEW YORK ACADEMY OF SCIENCES
TABLE 1. Parameters of Vitamin B, Status in Placebo or Theophylline-Treated Subjects
Parameter
___ ~
Placebo Treatment Theophylline Treatment Before After Before After
Plasma PLP (nanomol/l)
Plasma PL (nanomol/l)
Erythrocyte PLP (picomol/g Hb)
Erythrocyte PL kinase (nanomol PLP/gHb hr)
Urinary XA (wmo1/24hr)
mean SD mean SD mean SD mean SD mean SD
44.9 46.5 41.9 19.6 9.1 15.4 15.0 12.0 14.3 5.8 3.3 4.4
171.1 160.0 172.7 41.9 60.7 43.3 25.2 26.1 24.2 15.2 13.4 9.0 20.1 22.1 18.3 14.2 17.4 12.3
24.9“.b 12.1 12.1 3.7
145.5’ 34.7 46.9“.b
7.3 30.1 19.0
NOTE: Placebo or theophylline treatment was administered for four weeks and parameters of vitamin B, status were measured before and directly after the four-week treatment period. The placebo group did not differ from the theophylline group before treatment was started. After the four-week treatment period, plasma pyridoxal-5’-phosphate (PLP) and erythrocyte pyridoxal (PL) kinase levels were significantly different when the theophylline group was compared to the placebo group. (“p < 0.001). Compared to pretreatment levels, posttreatment erythrocyte PLP levels of the theophylline group showed a significant decrease, while urinary xanthurenic acid excretion was significantly higher (bp < 0.05). Urinary xanthurenic acid excretion was measured after tryptophan loading (2 g) and corrected for basal xanthurenic acid excretion. Data reported in this table was summarized from Ubbink et at.’’
PLP, and urinary xanthurenic acid (after oral tryptophan loading) levels did not differ significantly when the two groups were compared. However, posttreatment erythrocyte PLP levels of the theophylline-treated group were significantly lower ( p = 0.03) when compared to pretreatment erythrocyte PLP levels. Similarly, the tryptophan load test resulted in significantly ( p = 0.007) increased urinary xanthurenic acid excretion after four weeks of theophylline therapy in comparison with pretreatment urinary xanthurenic acid excretion. These results indicated that although plasma PLP declined rapidly with theophylline therapy, intracellular indexes of vitamin B, status (erythro- cyte PLP, tryptophan load test) were more resistant to change. One week of pyridoxine supplementation was sufficient to normalize biochemical parameters of vitamin B, status.”
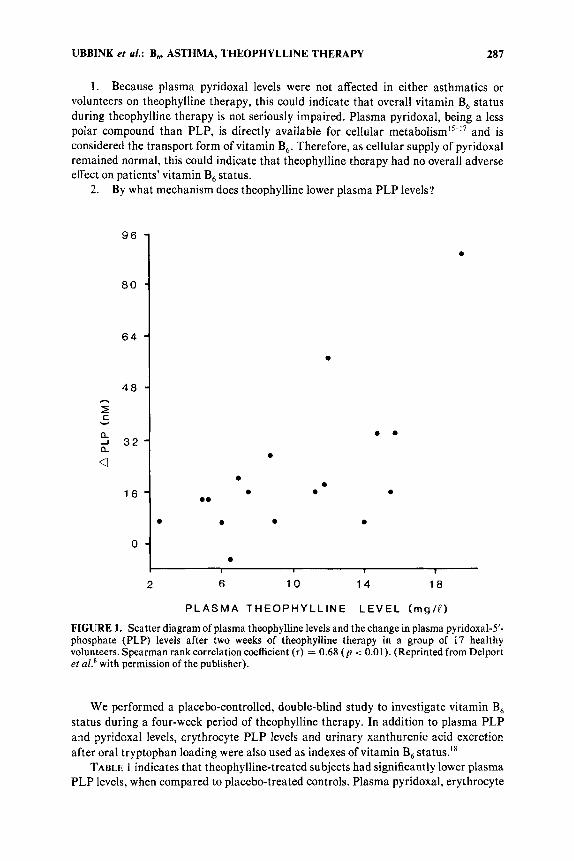
The above-mentioned clinical trial confirmed that theophylline interfered with vitamin B, metabolism; however, it provided no information on the possible mecha- nism(s) of the theophylline-induced interference. Using a sensitive HPLC assay” for the enzyme pyridoxal kinase (EC 2.7.1.35), we found that theophylline treatment induced significantly higher erythrocyte pyridoxal kinase activity levels (TABLE 1).18 We subsequently performed kinetic experiments directly in erythrocyte hemolysates and monitored PLP production in the presence of low, variable pyridoxal concentra- tions (0.4-2.0 bmol/l) and saturating ATP levels (2.21 mmol/l). Results indicated that theophylline is a powerful inhibitor for pyridoxal kinase (FIG. 2 ) . Respective to the substrate pyridoxal, the kinetic data fit the noncompetitive model of enzyme inhibition.I8
The observation that erythrocyte pyridoxal kinase levels during theophylline therapy increased nearly twofold should be considered in context of the extrahepatic tissues’ dependency on intracellular pyridoxal kinase activity and circulating pyridoxal
UBBINK et al.: B , ASTHMA, THEOPHYLLINE THERAPY 289
for adequate PLP supply. Presumably, inhibition of pyridoxal kinase by theophylline stimulates de novo synthesis of pyridoxal kinase in an attempt to maintain certain minimum intracellular levels of PLP. Other inhibitors of pyridoxal kinase have been shown to have a similar effect: daily administration of 4-deoxypyridoxine to rabbits increased cerebral activity of pyridoxal kinase sixfold within seven days.20 The in- creased erythrocyte levels of pyridoxal kinase after four weeks of theophylline treat- ment may indicate that the body is able to adapt to theophylline therapy. Since plasma pyridoxal levels remained normal, it should be theoretically possible that the vitamin B, status during theophylline therapy could return to normal if intracellular pyridoxal kinase levels increase sufficiently to overcome the inhibitory effect of theophylline.
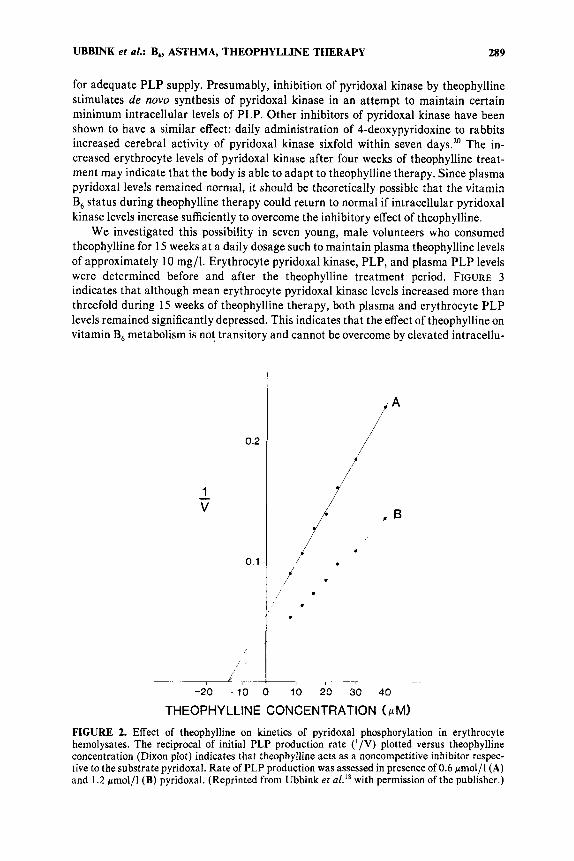
We investigated this possibility in seven young, male volunteers who consumed theophylline for 15 weeks at a daily dosage such to maintain plasma theophylline levels of approximately 10 mg/l. Erythrocyte pyridoxal kinase, PLP, and plasma PLP levels were determined before and after the theophylline treatment period. FIGURE 3 indicates that although mean erythrocyte pyridoxal kinase levels increased more than threefold during 15 weeks of theophylline therapy, both plasma and erythrocyte PLP levels remained significantly depressed. This indicates that the effect of theophylline on vitamin B, metabolism is not transitory and cannot be overcome by elevated intracellu-
/ '
Y -
-20 -10 0 10 20 30 40
THEOPHYLLINE CONCENTRATION (pM)
FIGURE 2. Effect of theophylline on kinetics of pyridoxal phosphorylation in erythrocyte hemolysates. The reciprocal of initial PLP production rate (' /V) plotted versus theophylline concentration (Dixon plot) indicates that theophylline acts as a noncompetitive inhibitor respec- tive to the substrate pyridoxal. Rate of PLP production was assessed in presence of 0.6 pmol/l (A) and 1.2 pmol/l (B) pyridoxal. (Reprinted from Ubbink et ~ 1 . ' ~ with permission of the publisher.)

290 ANNALS NEW YORK ACADEMY OF SCIENCES
h
2 75- I rn 1 0
5
ii 2 5
c 50-
a
m c Y
lar levels of pyridoxal kinase. Long-term theophylline therapy in asthmatics will therefore lead to a chronic depressed vitamin B, status. Although all aspects of vitamin B, metabolism in asthmatic patients have not yet been investigated, we suggest that theophylline therapy is a major, if not the only, factor responsible for the depressed vitamin B, status of asthmatics.
100
75 - 0 5 50 ld C v
a 2 25
0
4 ~
\ - 1 2
A
500.
CI 375 n I rn . - 250
0 0 P
a J 125 a
.- Y
0
1 100
u O L 1 2
B
~
u 1 2 C
FIGURE 3. Indicators of vitamin B, status (1) before and (2) after 15 weeks of theophylline therapy in seven healthy, male volunteers. (A) Plasma pyridoxal-5’-phosphate (PLP) levels, (B) erythrocyte PLP levels and (C) total erythrocyte pyridoxal kinase levels measured in vitro in presence of saturating amounts of ATP and pyridoxal. Pyridoxal kinase levels are expressed in nanomole PLP formed per gram hemoglobin (Hb) per hour. Although total erythrocyte pyridoxal kinase levels increased substantially during theophylline therapy, a significant decline in erythro- cyte PLP levels could not be prevented. This indicates that in vivo the increased erythrocyte pyridoxal kinase levels are largely inhibited by theophylline.
POSSIBLE CLINICAL IMPLICATIONS OF PYRIDOXAL KINASE INHIBITION BY THEOPHYLLINE
Although theophylline has been used in the treatment of asthma since 1937;’ the mechanism of theophylline-induced bronchodilation is still uncertain. Theophylline is an effective adenosine antagonist a t therapeutic plasma level^,^^-^^ and it has been suggested that adenosine receptor blockade may be the mechanism by which theophyl- line mediates b r o n c h o d i l a t i ~ n . ~ ~ ~ ~ ~ On the other hand, enprofylline (3-propylxanthine) is a poor adenosine an tag~nis t , ’~ yet it is about fivefold more potent than theophylline as a bronchodilator in man and other specie^.^^.^' This may indicate that adenosine receptor antagonism is not the explanation for theophylline-induced bronchodi la t i~n .~~ Although adenosine receptor antagonism appears unimportant in explaining the effect
UBBINK et al.: B,, ASTHMA, THEOPHYLLINE THERAPY 291
of theophylline on bronchodilation, this mechanism may explain theophylline-induced central nervous system stimulation. Different parts of the brain are presumably under depressant influences of therefore, adenosine receptor antagonism has been suggested to explain the stimulatory effect of theophylline on the central nervous
As severe pyridoxine deficiency has been documented to cause convulsions in the question now arises if a theophylline-induced pyridoxine deficiency could enhance the central nervous system excitability associated with theophylline therapy.
Further indirect support for this hypothesis is derived from the observation that symptoms of vitamin B, deficiency and theophylline side effects resemble each other. The effects of theophylline on brain electrical activity have been investigated, to a limited extent, by means of visual and spectral analysis of the electroencephalogram (EEG). While an increased incidence of EEG abnormalities has been reported in asthma patients receiving theophylline therapy,33 EEG abnormalities have also been reported in pyridoxine-deficient ~hi ldren.~’ In the latter study, pyridoxine supplementa- tion was associated with normalization of the EEG. Data reported in the above- mentioned two studies are, however, not directly comparable, and no further informa- tion is yet available on the effect of pyridoxine supplementation on theophylline- induced EEG changes.
Both theophylline therapy and vitamin B, deficiency may lead to changes in sleep patterns. Theophylline treatment may cause increased restlessness during sleep, less active (REM) sleep, and a shift towards shallower stages of non-REM ~ l e e p . ~ ~ - ~ ’ A chronic vitamin B, deficiency in rats resulted in depressed brain serotonin level^,'^^^^ as well as shortened phases of both REM and the deeper stages of non-REM sleep.40 It remains to be investigated whether a vitamin B, deficiency may aggravate theophylline- induced sleep disturbances by inducing a functional deficiency in brain serotonin levels.
Both a severe vitamin B, and theophylline may lead to convulsions. Keniston and Weir44 reported that intravenous administration of amino- phylline to vitamin B,-deficient dogs resulted in central nervous system (CNS) effects including muscular twitching, eyelid fluttering, and tremors. Pyridoxine supplementa- tion reportedly reversed the C N S effects mentioned above. It is well known that theophylline toxicity is not a close function of plasma theophylline level^,^'*^^ and it has been suggested that the vitamin B, status may influence the threshold of theophylline- induced seizures.44 In view of theophylline’s inhibitory effect on pyridoxal kinase, the possible use of pyridoxine therapy in theophylline overdose should be investigated.
Finally, it is also noteworthy that certain N7-substituted theophylline derivatives (P-hydroxyethyltheophylline, 7-(2,3-dihydroxypropyltheophylline and 7-(P-hydroxypro- pyltheophylline) have notably fewer side effects when compared to t h e ~ p h y l l i n e . ~ ~ . ~ ~ . ~ ~ None of the above-mentioned products have an inhibitory effect on pyridoxal kinase (unpublished observations), again suggesting that vitamin B, deficits may contribute to theophylline side effects.
CONCLUSIONS
Asthmatic patients present with a depressed vitamin B, status owing to theophyl- line inhibition of pyridoxal kinase. Increased intracellular pyridoxal kinase levels were
292 ANNALS NEW YORK ACADEMY OF SCIENCES
unable to reverse the relative vitamin B, deficiency induced by theophylline therapy. Pyridoxine supplementation (1 0 mg/day) normalized vitamin B, status in theophylline- treated volunteers. T h e possible therapeutic effects of pyridoxine supplementation during theophylline therapy should be subjected to closer scientific scrutiny.
1.
2.
3.
4.
5 .
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
REFERENCES
HOLGATE, S. T. 1984. In Bronchodilator Therapy. T. J . H. Clark & G . M. Cochrane, Eds.:
SHENFIELD, G. M. & R. N. BROGDEN. 1984. In Bronchodilator Therapy. T. J. H. Clark & 1-16. ADIS Press. Auckland, New Zealand.
G. M. Cochrane, Eds.: 17-37. ADIS Press. Auckland, New Zealand.
treatment of childhood bronchial asthma. Ann. Allergy 3 5 93-97. COLLIPP, P. J., S . Y. CHEN, R. K. SHARMA, V. BALANCHANDAR & V. T. MADDAIAH. 1975.
Tryptophan metabolism in bronchial asthma. Ann. Allergy 35 153-158. HALL, M. A,, H. THOM & G. RUSSELL. 1981. Erythrocyte aspartate aminotransferase
activity in asthmatic and nonasthmatic children and its enhancement by vitamin B,. Ann. Allergy 47: 464-466.
REYNOLDS, R. D. & C. L. NATTA. 1985. Depressed plasma pyridoxal phosphate concentra- tions in adult asthmatics. Am. J. Clin. Nutr. 41: 684-688.
SIMON R. A. & R. D. REYNOLDS. 1988. Vitamin B, and asthma. In Current topics in Nutrition and Disease: Clinical and Physiological Applications of Vitamin B,. J. E. Leklem & R. D. Reynolds, Eds. Vol. 19 307-315. Alan R. Liss. New York.
DELPORT, R., J. B. UBBINK, W. J. SERFONTEIN, P. J. BECKER & L. WALTERS. 1988. Vitamin B, nutritional status in asthma. The effect of theophylline therapy on plasma pyridoxal 5’-phosphate and pyridoxal levels. Int. J. Vit. Nutr. Res. 58: 67-72.
BROWN, R. R. 1981. The tryptophan load test as an index of vitamin B, nutrition. In Methods in Vitamin B, Nutrition. J. E. Leklem & R. D. Reynolds, Eds.: 321-340. Plenum Press. New York.
BHAGAVAN, H. N. 1985. Interaction between vitamin B, and drugs. In Current Topics in Nutrition and Disease. Vitamin B,: Its Role in Health and Disease. R. D. Reynolds & J. E. Leklem, Eds. Vol. 13: 401-415. Alan R. Liss. New York.
STEWART, J. W., W. HARRISON, F. QUITKIN & M. R. LIEBOWITZ. 1984. Phenelzine-induced pyridoxine deficiency. J. Clin. Psychopharmacol. 4 225-226.
PELLOCK, J. M., J. HOWELL, E. L. KENDIG & H. BAKER. 1985. Pyridoxine deficiency in children treated with isoniazid. 87: 658-661.
SNIDER, D. E. 1980. Pyridoxine supplementation during isoniazid therapy. Tubercle 61: 191-196.
JAFFE, A. I., K. ALTMAN & P. MERRYMAN. 1964. The antipyridoxine effect of penicillamine in man. J. Clin. Invest. 43: 1869-1873.
ANDERSON, B. B., C. E. FULFORD-JONES, J. A. CHILD, M. E. J. BEARD & C. J. T. BATEMAN. 197 1. Conversion of vitamin B, compounds to active forms in the red blood cell. J. Clin. Invest. 5 0 1901-1909.
LUMENG, L. & T. K. LI. 1980. Mammalian Vitamin B, metabolism: Regulatory role of protein-binding and the hydrolysis of pyridoxaL5’-phosphate in storage and transport. In Vitamin B, Metabolism and Role in Growth. G. P. Tryfiates, Ed.: 27-51. Food & Nutrition Press. Westport, CT.
MEHANSO, H. & L. V. M. HENDERSON. 1980. Transport and accumulation of pyridoxine and pyridoxal by erythrocytes. J. Biol. Chem. 255 11901-1 1907.
UBBINK, J. B., R. DELPORT, P. J. BECKER & S . BISSBORT. 1989. Evidence of a theophylline- induced vitamin B, deficiency caused by non-competitive inhibition of pyridoxal kinase. J. Lab. Clin. Med. 133 15-22.
UBBINK, J. B. & A. M. SCHNELL. 1988. Assay of erythrocyte enzyme activity levels involved in vitamin B, metabolism by high-performance liquid chromatography. J. Chromatogr. 431: 406412.
COLLIPP, P. J., S. GOLDZIER, N. WEISS, Y. SOLEYMANI & R. SNYDER. 1975. Pyridoxine

UBBINK et al.: B6, ASTHMA, THEOPHYLLINE THERAPY 293
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
31.
38.
39.
40.
41.
42.
43.
EBADI, M. S., E. E. McCoy & R. B. KUGEL. 1970. Interrelationships between pyridoxal and
BERTINO, J. S . & J. W. WALKER. 1987. Reassessment of theophylline toxicity. Serum
FREDHOLM, B. B. 1980. Are the action of methylxanthines due to antagonism of adenosine?
FREDHOLM, B. B. & C. G. A. PERSSON. 1982. Xanthine derivatives as adenosine receptor
SCHWABE, U. 1981. Direct binding studies of adenosine receptors. Trends Pharmacol. Sci. 2
PERSSON, C. G. A. 1987. The pharmacology of anti-asthmatic xanthines and the role of adenosine. I n Asthma Reviews. J. Morley, Ed. Vol 1: 61-94. Academic Press. New York.
LUNELL, E., N. SVEDMYR, K.-E. ANDERSON & C. G. A. PERSSON. Effects of enprofylline, a xanthine lacking adenosine antagonism, in patients with reversible obstructive lung disease. Eur. J. Clin. Pharmacol. 2 2 395-402.
PERSSON, C. G. A. 1986. Development of safer xanthine drugs for treatment of obstructive airway disease. J. Allergy Clin. Immunol. 7 8 817-824.
PERKINS, M. N. & T. W. STONE. 1980. Aminophylline and theophylline derivatives as antagonists of neuronal depression by adenosine: a microionophoretic study. Arch. fnt. Pharmacodyn. 246 205-214.
DUNWIDDIE, T. V. 1980. Endogenously released adenosine regulates excitability in the in vitro hippocampus. Epilepsia 21: 541-548.
COURSIN, D. B. 1969. Vitamin B, and brain function in animals and man. Ann. N.Y. Acad. Sci. 166 7-15.
BESSEY, 0. A., D. J. D. ADAM & A. E. HANSEN. 1957. Intake of vitamin B, and infantile convulsions. A first approximation of requirements of pyridoxine in infants. Pediatrics 2 0 33-44.
SNYDERMAN, S . E., L. E. HOLT, R. CARRETERO & K. JACOBS. 1953. Pyridoxine deficiency in the human infant. Am. J. Clin. Nutr. 1: 200-207.
SCHUCARD, D. W., S. L. SPECTOR, R. L. EUWER, K. R. CUMMINS, J. L. SCHUCARD & A. FRIEDMAN. 1985. Central nervous system effects of antiasthma medication-An EEG study. Ann. Allergy 54: 177-184.
ESPINOZA, H., R. ANTIC, A. T. THORNTON & R. D. McEvou. 1987. The effects of aminophylline on sleep and sleep-disordered breathing in patients with obstructive sleep apnea syndrome. Am. Rev. Respir. Dis. 136 80-84.
DENENBERG, V. H., L. P. ZEIDNER, E. B. THOMAN, P. KRAMER, J. C. ROWE, A. F. PHILIPPS & J. R. RAYE. 1982. Effects of theophylline on behavioral state development in the newborn rabbit. J. Pharmacol. Exp. Ther. 221: 604-608.
KORNER, A. F., E. M. RUPPEL & J. M. RHO. 1982. Effects of water beds on the sleep and motility of theophylline-treated preterm infants. Pediatrics 7 0 864-869.
RADULOVACKI, M. & R. M. VIRUS. 1988. Dose-response effects of 8-cyclopropyltheophyl- line on sleep and wakefulness in rats. Psychopharmacology 94 417-420.
DAKSHINAMURTI, K., W. D. LE BLANCQ, R. HERCHL & V. HAVLICEK. 1976. Nonparallel changes in brain monoamines of pyridoxine-deficient growing rats. Exp. Brain Res. 2 6
DAKSHINAMURTI, K. & C. S. PAULOSE. 1983. Consequences of decreased brain serotonin in the pyridoxine deficient young rat. Prog. Neuro-Pscyhopharmacol. Biol. Psychiatry 7:
DAKSHINAMURTI, K. 1982. Neurobiology of pyridoxine. I n Advances in Nutritional Re- search. H. H. Draper, Ed. Vol. 4 143-179. Plenum Press. New York.
ZWILLICH, C. W., F. D. SUTTON, T. A. NEFF, W. M. COHN, R. A. MAITHAY & M. M. WEINBERGER. 1975. Theophylline induced seizures in adults. Correlation with serum concentrations. Ann. Int. Med. 8 2 784-787.
SINGER, E. P. & A. KOLISCHENKO. 1985. Seizures due to theophylline overdose. Chest 87: 75 5-7 5 7.
PALOUCEK, F. P. & K. A. RODVOLD. 1988. Evaluation of theophylline overdose and toxicities. Ann. Emerg. Med. 17: 135-144.
phosphate pyridoxal kinase in rabbit brain. J. Neurochem. 17: 941-948.
concentrations, clinical course and treatment. Arch. Intern. Med. 147: 757-760.
Trends Pharmacol. Sci. 1: 129-132.
antagonists. Eur. J. Pharmacol. 81: 673-676.
229-303.
355-366.
743-746.

294 ANNALS NEW YORK ACADEMY OF SCIENCES
44.
45.
KENISTON, R. S. & M. R. WEIR. 1986. Aminophylline and gentamycin-2. Am. J . Clin. Nutr. 43 636-637.
MANEY, P. V., J. W. JONES, E. G. GROSS & H. M. KORNS. 1946. Dihydroxypropyl theophylline: Its preparation and pharmacological and clinical study. J. Am. Pharm.
MCCOLL, J. D., J. M. PARKER & J. K. W. FERGUSON. 1957. A comparison of the relative toxic, emetic and convulsive actions of a series of methylated xanthine derivatives. J. Pharmacol. Exp. Ther. 1 1 6 343-350.
ASSOC. 35 266-272. 46.
Related Documents











