Original Article Proc IMechE Part H: J Engineering in Medicine 2014, Vol. 228(12) 1258–1263 Ó IMechE 2014 Reprints and permissions: sagepub.co.uk/journalsPermissions.nav DOI: 10.1177/0954411914562490 pih.sagepub.com The relationship between maximal hip abductor strength and resultant loading at the knee during walking Ryan T Lewinson 1,2,3 , Jay T Worobets 1 and Darren J Stefanyshyn 1,2 Abstract The peak external knee adduction moment (KAM) is implicated in progression of knee osteoarthritis (OA). Recently, hip abductor weakness has also been found in patients with knee OA; however, it remains unknown as to howor if this weakness is a consequence of OA, or a predisposing factor. If it is the latter, a direct relationship between hip strength and KAM magnitude would be expected. The purpose of this study was to evaluate the relationship between hip abduc- tor strength and KAM magnitude during walking. In fourteen adults, maximal isometric hip abductor strength was mea- sured, and the KAM was quantified during gait. Additionally, internal hip abductor moments, vertical and medial ground- reaction-forces (GRFs), and GRF to knee joint center lever-arms were quantified during gait. The relationship between hip strength and GRFs, lever-arms and KAM were assessed using correlation. Internal hip abductor moments were compared to maximum hip strength by paired samples t-test. Correlations between hip strength and the vertical GRF (r = –0.05, p = 0.87), medial GRF (r = –0.24, p = 0.41), lever arm (r = –0.01, p = 0.97), and KAM (r = –0.24, p = 0.41) were not statistically significant. Peak internal hip abductor moments during gait (1.1 6 0.2 Nm/kg) were significantly lower than maximal hip abductor strength (1.8 6 0.3 Nm/kg, p \ 0.001). It is concluded that hip abductor strength is not related to KAM magnitude. It seems more likely that hip abductor weakness is a consequence of OA rather than a predisposing factor. Keywords Biomechanics, gait, muscle, osteoarthritis, walking, joint loading Date received: 7 July 2014; accepted: 11 November 2014 Introduction Large frontal plane resultant loads at the knee have been identified as a risk factor for the onset and pro- gression of knee osteoarthritis (OA)—a disease charac- terized by progressive degeneration of articular cartilage leading to pain and loss of function. 1,2 These frontal plane resultant loads are commonly expressed as the peak external knee adduction moment (KAM) and develop during the stance phase of gait. Biomechanically, they are often calculated using an inverse dynamics procedure but are often explained in terms of the magnitudes of the frontal plane ground reaction force (GRF) and the perpendicular distance from the GRF vector to the knee joint center. 2 While not an exact measurement of medial tibiofe- moral load itself, it is believed that with elevated peak KAMs, the loads on the medial compartment tend to increase, contributing to development and progression of OA. 2,3 This notion is supported by the fact that KAMs have been shown to be negatively correlated with tibial cartilage thickness 3 and positively correlated with Kellgren–Lawrence OA severity grade. 3,4 Additionally, studies using instrumented knee replace- ments have found that medial contact forces increase with elevated KAMs. 5 Therefore, one potential strategy 1 Human Performance Laboratory, Faculty of Kinesiology, University of Calgary, Calgary, AB, Canada 2 Biomedical Engineering, Schulich School of Engineering, University of Calgary, Calgary, AB, Canada 3 Faculty of Medicine, University of Calgary, Calgary, AB, Canada Corresponding author: Ryan T Lewinson, Human Performance Laboratory, Faculty of Kinesiology, University of Calgary, 2500 University Drive N.W., Calgary, AB T2N 1N4, Canada. Email: [email protected] by guest on December 16, 2014 pih.sagepub.com Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Original Article
Proc IMechE Part H:J Engineering in Medicine2014, Vol. 228(12) 1258–1263� IMechE 2014Reprints and permissions:sagepub.co.uk/journalsPermissions.navDOI: 10.1177/0954411914562490pih.sagepub.com
The relationship between maximal hipabductor strength and resultantloading at the knee during walking
Ryan T Lewinson1,2,3, Jay T Worobets1 and Darren J Stefanyshyn1,2
AbstractThe peak external knee adduction moment (KAM) is implicated in progression of knee osteoarthritis (OA). Recently,hip abductor weakness has also been found in patients with knee OA; however, it remains unknown as to how or if thisweakness is a consequence of OA, or a predisposing factor. If it is the latter, a direct relationship between hip strengthand KAM magnitude would be expected. The purpose of this study was to evaluate the relationship between hip abduc-tor strength and KAM magnitude during walking. In fourteen adults, maximal isometric hip abductor strength was mea-sured, and the KAM was quantified during gait. Additionally, internal hip abductor moments, vertical and medial ground-reaction-forces (GRFs), and GRF to knee joint center lever-arms were quantified during gait. The relationship betweenhip strength and GRFs, lever-arms and KAM were assessed using correlation. Internal hip abductor moments werecompared to maximum hip strength by paired samples t-test. Correlations between hip strength and the vertical GRF(r = –0.05, p = 0.87), medial GRF (r = –0.24, p = 0.41), lever arm (r = –0.01, p = 0.97), and KAM (r = –0.24, p = 0.41)were not statistically significant. Peak internal hip abductor moments during gait (1.1 6 0.2 Nm/kg) were significantlylower than maximal hip abductor strength (1.8 6 0.3 Nm/kg, p \ 0.001). It is concluded that hip abductor strength isnot related to KAM magnitude. It seems more likely that hip abductor weakness is a consequence of OA rather than apredisposing factor.
KeywordsBiomechanics, gait, muscle, osteoarthritis, walking, joint loading
Date received: 7 July 2014; accepted: 11 November 2014
Introduction
Large frontal plane resultant loads at the knee havebeen identified as a risk factor for the onset and pro-gression of knee osteoarthritis (OA)—a disease charac-terized by progressive degeneration of articularcartilage leading to pain and loss of function.1,2 Thesefrontal plane resultant loads are commonly expressedas the peak external knee adduction moment (KAM)and develop during the stance phase of gait.Biomechanically, they are often calculated using aninverse dynamics procedure but are often explained interms of the magnitudes of the frontal plane groundreaction force (GRF) and the perpendicular distancefrom the GRF vector to the knee joint center.2
While not an exact measurement of medial tibiofe-moral load itself, it is believed that with elevated peakKAMs, the loads on the medial compartment tend toincrease, contributing to development and progression
of OA.2,3 This notion is supported by the fact thatKAMs have been shown to be negatively correlatedwith tibial cartilage thickness3 and positively correlatedwith Kellgren–Lawrence OA severity grade.3,4
Additionally, studies using instrumented knee replace-ments have found that medial contact forces increasewith elevated KAMs.5 Therefore, one potential strategy
1Human Performance Laboratory, Faculty of Kinesiology, University of
Calgary, Calgary, AB, Canada2Biomedical Engineering, Schulich School of Engineering, University of
Calgary, Calgary, AB, Canada3Faculty of Medicine, University of Calgary, Calgary, AB, Canada
Corresponding author:
Ryan T Lewinson, Human Performance Laboratory, Faculty of
Kinesiology, University of Calgary, 2500 University Drive N.W., Calgary,
AB T2N 1N4, Canada.
Email: [email protected]
by guest on December 16, 2014pih.sagepub.comDownloaded from

for prevention and slowing the progression of OA isto reduce the peak KAM. To do this, it is necessaryto identify factors that contribute to elevated KAMsso that targeted intervention strategies may bedefined.
Recently, hip abductor muscle weakness has beenfound in patients with knee OA.6 Attempts have beenmade to improve hip strength for OA patients and havefound that while this does seem to help reduce pain, ithas no effect on the peak KAM.7 In a recent cross-sectional study, it was also shown that hip musclestrength was not related to peak KAM magnitude inpatients with knee OA.8 Together, these data suggestthat hip weakness is something experienced by patientswith OA, that can worsen pain symptoms, but that it isof no consequence to KAM magnitude, and thus, it isunlikely to be associated with further OA progression.Consequently, it seems plausible that hip weakness isan outcome of OA, rather than a predisposing factor toOA development; however, to confirm this notion, testsmust be performed on individuals with no OA present.Specifically, if hip weakness is a predisposing factor toOA development, then (1) a direct relationship betweenhip abductor strength and peak KAM magnitudewould be expected in healthy individuals, and (2) indi-viduals with lower hip strength would be more likely todevelop OA over the course of their life. The purpose ofthis study was to evaluate the first criteria above, wherethe relationship between hip abductor strength andpeak KAM magnitude during walking was assessed inhealthy individuals. Based on previous studies high-lighting that hip strength was not related to peak KAMmagnitude in an OA population, it was hypothesizedthat hip abductor strength would not be correlated withpeak KAMmagnitude.
Methods
Participants
A total of 14 healthy participants (six females and eightmales) volunteered to participate in this study. The par-ticipants had a mean (standard deviation (SD)) age of25.1 years (4.5 years), height of 171.9 cm (8.8 cm), andbody mass of 70.0 kg (14.9 kg). All participants werefree from any musculoskeletal pain at the time of thestudy, and none indicated any musculoskeletal injurywithin the past 3months. All participants gaveinformed consent, and ethics approval was obtainedfrom the University’s Conjoint Health Research EthicsBoard prior to subject recruitment.
Hip strength data collection
Participants were first asked to stand in the anatomicalposition, and the hip angle of their right leg was mea-sured using a handheld goniometer. This was done byplacing the center of the goniometer in line with thegreater trochanter, one goniometer arm directed
toward the posterior superior iliac spine and the otherarm directed toward the knee joint center (Figure 1).Participants were then placed on the bed of a BiodexSystem 3 dynamometer (Biodex Medical Systems, Inc.,Shirley, NY, USA) on their left side with their right legfacing upward. The right thigh was strapped tightly inplace and raised to an angle of 5� more adducted thanwhat was measured during the anatomical position.This was done to simulate the frontal plane hip anglethat is typically experienced at the instance of the peakKAM during walking.9
A resting limb weight trial was recorded first for 5 sat a sampling frequency of 100Hz. In this trial, the legremained stationary without any muscle contraction,and the passive moment acting on the Biodex wasrecorded. Following this, participants performed fivemaximal isometric hip abduction contractions, each of5-s duration with 10-s rest periods between trials. A
Figure 1. A schematic diagram showing the measurement ofthe standing frontal plane hip joint angle for the muscle strengthtesting protocol. While the subject stood in the anatomicalposition, the goniometer center was placed in line with thegreater trochanter (GT), and the arms were directed towardthe posterior superior iliac spine (PSIS) and the knee jointcenter (KJC).
Lewinson et al. 1259
by guest on December 16, 2014pih.sagepub.comDownloaded from

sampling frequency of 100Hz was also used for theactive conditions.
Hip strength data processing
The moment recorded from the resting limb weight trial(negative value) was calculated as the mean momentacross the 5-s trial. From each of the five active trials,peak moments were identified (positive values) and aver-aged to give the mean maximal active moment. Since theresting limb moment acts in the opposite direction to theactive abduction moments, hip abductor strength wascalculated by adding the absolute magnitude of the rest-ing moment to the magnitude of the active moment.10
This was done using a custom-coded script in MATLABr2010a (MathWorks, Natick, MA, USA).
Walking biomechanics data collection
Three retroreflective tracking markers were placed oneach of the shoe, shank, and thigh segments of the rightlower extremity of each participant. Additional retrore-flective markers were placed over the medial and lateralmalleoli, medial and lateral epicondyles, and the rightand left greater trochanters. Following a warmupperiod, participants were asked to complete five trialswalking along a 20-m runway within 5% of the targetspeed of 1.6m/s, which was monitored by two photo-cells. As they did this, eight Motion Analysis cameras(Motion Analysis Corp., Santa Rosa, CA, USA)recorded the three-dimensional (3D) trajectories ofeach retroreflective marker at a frequency of 240Hz,and a Kistler force platform (Kistler AG, Winterthur,Switzerland) mounted flush with the lab floor recorded3D GRF data at a frequency of 2400Hz. Each partici-pant wore the same model of footwear (adidas adiZeroMana) to eliminate the influence of different footwearmodels on resultant joint loads.
A standing neutral trial was also recorded for each par-ticipant. In this trial, the participant stood on the forceplatform in the anatomical position for 3 s. The neutraltrial was used to define the ankle joint center as the mid-way point between the malleoli markers,11 the knee jointcenter as the midway point between the epicondyle mar-kers,11 and the hip joint center as the point 25% of thedistance between the greater trochanter markers.12 Inaddition, the neutral trial was used to determine segmentlengths, which were then used to estimate segment centersof mass. Segment masses, centers of mass, and momentsof inertia were taken from the literature.13,14
Walking biomechanics data processing
Kinetic and kinematic data were imported into Kintrak7.0 (University of Calgary, Calgary, AB, USA) andsmoothed using fourth-order Butterworth low-pass fil-ters with cutoff frequencies of 50 and 12Hz, respec-tively.15 Embedded segment coordinate systems weredefined for the foot, shank, and thigh, and a Newton–
Euler inverse dynamics approach was then used to cal-culate KAMs and internal hip abduction moments dur-ing walking.11,16 The peak KAM and hip abductionmoment were extracted for each trial, averaged acrosstrials for each participant, and normalized to the parti-cipant’s mass.
GRFs and GRF lever arms were also studied to pro-vide indication of the mechanism, if any, by whichKAMs were altered across varying hip strength pro-files. At the instant of the peak KAM, vertical andmedial GRF magnitudes were also extracted fromKintrak for each trial and averaged and normalized tobody mass for each participant. Frontal plane GRF toknee joint center lever arms were found for each trialby multiplying the medial and vertical GRFs by theirrespective perpendicular distances from the GRF origin(i.e. center of pressure) to the knee joint center in thevertical and mediolateral directions and then dividingby the resultant frontal plane force.
Statistical analysis
Correlations were used to assess the relationship betweenhip abductor strength and peak KAM, vertical GRF,medial GRF, GRF lever arm, and the peak hip abduc-tion moment during walking. In addition, a two-tailedpaired samples t-test was used to compare the magnitudeof hip abductor strength (i.e. maximum available hipabductor moment) and the magnitude of the peak hipabduction moment during walking (i.e. maximum uti-lized hip abductor moment) within subjects. For all sta-tistical tests, an alpha level of 0.05 was used.
Results
Throughout stance phase, the utilized hip abductionmoment during walking was less than maximum hipabductor strength, that is, the available hip abductormoment (Figure 2). Statistically, the peak utilized hipabduction moment was significantly less than maxi-mum hip strength (p \ 0.001, 95% confidence interval
Figure 2. Internal hip abduction moment during gait (blue,with SD bars) is shown relative to maximum hip abductorstrength (red, with SD bars). It can be seen that the utilized hipmoment during gait remains well below maximum hip abductorstrength or the available moment.
1260 Proc IMechE Part H: J Engineering in Medicine 228(12)
by guest on December 16, 2014pih.sagepub.comDownloaded from
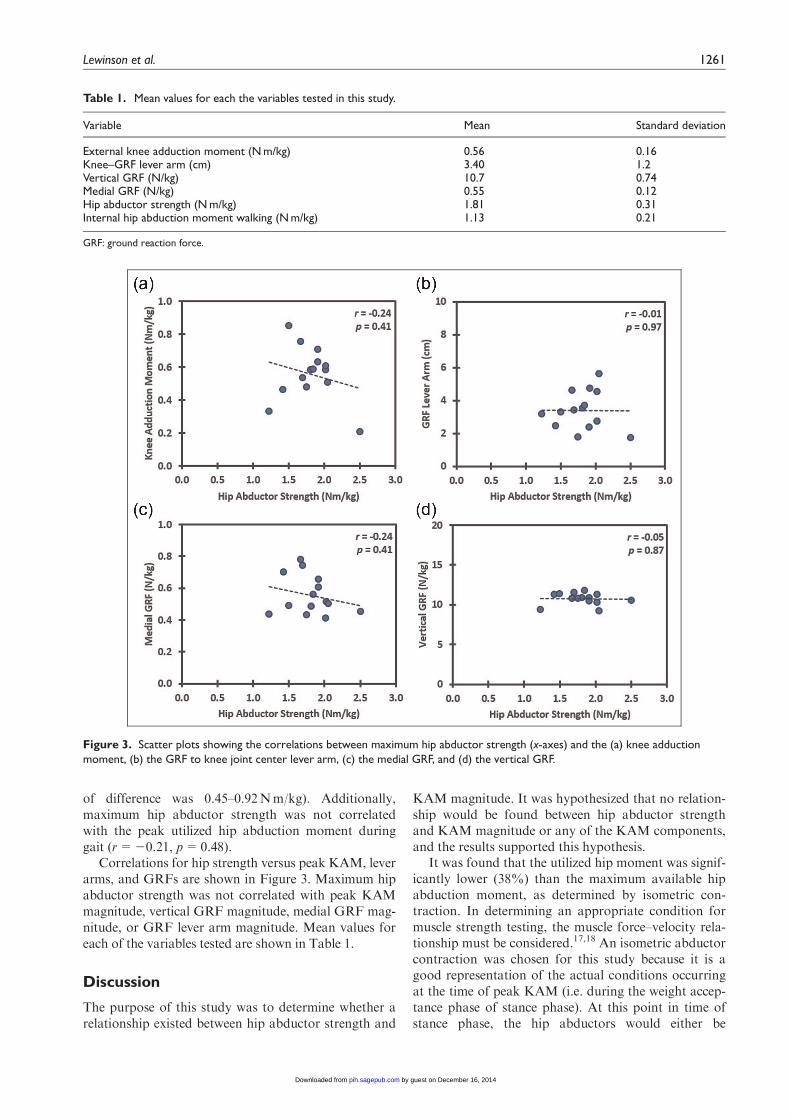
of difference was 0.45–0.92Nm/kg). Additionally,maximum hip abductor strength was not correlatedwith the peak utilized hip abduction moment duringgait (r=20.21, p=0.48).
Correlations for hip strength versus peak KAM, leverarms, and GRFs are shown in Figure 3. Maximum hipabductor strength was not correlated with peak KAMmagnitude, vertical GRF magnitude, medial GRF mag-nitude, or GRF lever arm magnitude. Mean values foreach of the variables tested are shown in Table 1.
Discussion
The purpose of this study was to determine whether arelationship existed between hip abductor strength and
KAM magnitude. It was hypothesized that no relation-ship would be found between hip abductor strengthand KAM magnitude or any of the KAM components,and the results supported this hypothesis.
It was found that the utilized hip moment was signif-icantly lower (38%) than the maximum available hipabduction moment, as determined by isometric con-traction. In determining an appropriate condition formuscle strength testing, the muscle force–velocity rela-tionship must be considered.17,18 An isometric abductorcontraction was chosen for this study because it is agood representation of the actual conditions occurringat the time of peak KAM (i.e. during the weight accep-tance phase of stance phase). At this point in time ofstance phase, the hip abductors would either be
Figure 3. Scatter plots showing the correlations between maximum hip abductor strength (x-axes) and the (a) knee adductionmoment, (b) the GRF to knee joint center lever arm, (c) the medial GRF, and (d) the vertical GRF.
Table 1. Mean values for each the variables tested in this study.
Variable Mean Standard deviation
External knee adduction moment (N m/kg) 0.56 0.16Knee–GRF lever arm (cm) 3.40 1.2Vertical GRF (N/kg) 10.7 0.74Medial GRF (N/kg) 0.55 0.12Hip abductor strength (N m/kg) 1.81 0.31Internal hip abduction moment walking (N m/kg) 1.13 0.21
GRF: ground reaction force.
Lewinson et al. 1261
by guest on December 16, 2014pih.sagepub.comDownloaded from

contracting isometrically or eccentrically because thethigh angular velocity in the frontal plane would likelyeither be near zero or slightly toward adduction.9 Ifcontracting isometrically, the strength of the hip abduc-tors presented here would be representative of theiractual strength capacity during gait. If contractingeccentrically, the strength of the hip abductors pre-sented here would be slightly lower than their actualstrength capacity during gait, as muscles are able toproduce more force when contracting eccentrically.17,18
Therefore, the conclusions drawn from the hip strengthdata in this article can be considered externally valid,as the hip abductor strength data would either be simi-lar to or slightly lower than the actual hip abductorstrength at the time of the peak KAM.
In patients with knee OA, it has been found that hipabductor strength is lower than healthy controls byapproximately 24%.6 Applying this reduction instrength to this study would result in a maximum avail-able hip abductor moment of about 1.38Nm/kg. Still,the utilized hip abduction moment during gait observedin this study would be lower by 0.25Nm/kg or 18%than the available moment. This indicates that even if acertain degree of error is assumed with isometricdynamometer or gait biomechanics testing,10,11,16,18 itis unlikely that the required peak hip abductor momentduring gait would approach the available hip abductormoment under normal nonfatiguing conditions. Thisnotion is further supported by the findings in OA indi-viduals where hip strength is not related to peak KAMmagnitude;8 however, long-term prospective studies inboth healthy and OA populations are required to deter-mine whether factors such as obesity, age, and diseaseseverity affect either the required or utilized hipmoments. For instance, while hip strength may declinewith age and disease, if the utilized moment alsodecreases, then KAMs would not be expected to beaffected. Based on current data, it appears that no rela-tionship exists between hip abductor strength andKAM magnitude nor any of the components (verticalGRF, medial GRF, or GRF lever arm magnitudes)that influence KAM magnitude.
Supporting these results, a study by Geiser et al.19
found that when participants underwent a hip abductorfatiguing protocol, where hip strength was reduced byapproximately 40%, the internal knee abductionmoment during running was actually reduced.Additionally, studies aimed at strengthening the hipabductors in knee OA populations have found thatthese training programs do not have any effect onKAM magnitude.7,20,21 Therefore, it is concluded thathip abductor weakness does not contribute to KAMmagnitude and thus likely does not directly influenceOA development or progression. Instead, it seemslikely that hip abductor weakness may be a conse-quence of OA, and therefore, interventions aimed atstrengthening hip abductors may not be ideal. Futureattention should be focused toward identifying otherfactors that could affect KAM magnitude.
As a consequence of knee OA, hip muscle weaknesscould develop from a number of mechanisms. The first isdue to generalized muscle weakness simply due to reducedmobility and reduced muscle use as a result of chronicpain. The second is that patients with knee OA may adoptalternative gait strategies in attempt to unload the knee.One such example is lateral trunk lean. In this case, theGRF is shifted laterally and reduces the KAM.22 By lean-ing laterally, and shifting the body’s center of mass, therecould be less need to contract hip abductor muscles, andweakness could develop over time.
Although the results of this study indicate that hipmuscle weakness may not be a predisposing factor toknee OA, the results of experiments concerning quadri-ceps musculature seem to indicate that quadriceps mus-cle weakness may have a role in OA development. Forinstance, it has been shown that quadriceps muscleweakness rapidly induces cartilage damage in rabbits.23
This discrepancy between muscle groups may be partlyexplained by the fact that quadriceps muscles cross theknee joint and may directly alter loading in the tibiofe-moral compartment, whereas hip abductor muscles donot.24 Additionally, it is possible that the amount ofweakness induced in these rabbits (approximately 80%)resulted in the required force of the quadriceps duringnormal activity to exceed the available quadricepsstrength, resulting in further detrimental kinematic andkinetic changes.
A limitation of this study was that participantswere evaluated at a period where no OA was present.By using healthy subjects, the study was limited inthat conclusions cannot be directly applied to an OApopulation, where age, obesity, and disease severitymay have an impact on gait and muscle strength.However, since hip weakness has been proposed as apredisposing factor to OA, study of healthy popula-tions is a necessity. Additionally, a study that evalu-ated hip strength and KAM magnitudes in an OApopulation found similar results as those presentedhere.8
Another limitation of this study was that it wascross-sectional in design, which only allows for study atone instant in time. While a long-term prospectivestudy would be required to conclusively determinewhether hip weakness is a predisposing factor to OAdevelopment, a study like this would require anextremely large sample size and numerous years offollow-up to be performed correctly. Consequently, across-sectional design was used here to address the nec-essary prerequisite question to a prospective study: isthere a relationship between hip strength and KAMmagnitude in healthy individuals? This relationshipwould be expected in healthy individuals if hip strengthwas related to OA development but not expected if hipstrength was simply an outcome of OA. Therefore,although the data in the present study suggest that hipweakness is likely an outcome of OA rather than a pre-disposing factor, long-term prospective studies wouldbe required to confirm this notion.
1262 Proc IMechE Part H: J Engineering in Medicine 228(12)
by guest on December 16, 2014pih.sagepub.comDownloaded from

In conclusion, this study found no relationshipbetween hip abductor strength and KAM magnitudeduring gait. Additionally, hip strength was not corre-lated with the peak hip moment utilized during gait norwas it correlated with GRF magnitudes or lever armmagnitudes. Together, this suggests that hip weaknessis more likely a consequence of OA rather than a pre-disposing factor to OA.
Acknowledgements
R.T.L. recruited participants, collected and processedthe data, analyzed the data, and drafted the article. Allauthors were involved in the design of the study andinterpretation of the results, and J.T.W. and D.J.S. cri-tically reviewed the article. All authors read andapproved the final version of this article.
Declaration of conflicting interests
No conflicts of interest to report.
Funding
R.T.L. was funded by a Vanier Canada GraduateScholarship through the Canadian Institutes of HealthResearch, a Doctoral Award from the Natural Sciences& Engineering Research Council of Canada CREATEProgram, a Doctoral Award from the Killam Trusts,and an MD/PhD Studentship from Alberta Innovates-Health Solutions.
References
1. Bennell KL, Bowles KA, Wang Y, et al. Higher dynamicmedial knee load predicts greater cartilage loss over 12
months in medial knee osteoarthritis. Ann Rheum Dis
2011; 70: 1770–1774.2. Reeves ND and Bowling FL. Conservative biomechani-
cal strategies for knee osteoarthritis. Nat Rev Rheumatol
2011; 7: 113–122.3. Andriacchi TP, Mundermann AM, Smith RL, et al. A
framework for the in vivo pathomechanics of osteoar-thritis at the knee. Ann Biomed Eng 2004; 32: 447–457.
4. Sharma L, Hurwitz DE, Thonar EJMA, et al. Kneeadduction moment, serum hyaluronan level, and diseaseseverity in medial tibiofemoral osteoarthritis. Arthritis
Rheum 1998; 41: 1233–1240.5. Erhart JC, Dyrby CO, D’Lima DD, et al. Changes in in
vivo knee loading with a variable-stiffness interventionshoe correlate changes in the knee adduction moment. JOrthop Res 2010; 28: 1548–1553.
6. Hinman RS, Hunt MA, Creaby MW, et al. Hip muscleweakness in individuals with medial knee osteoarthritis.Arthritis Care Res 2010; 62: 1190–1193.
7. Foroughi N, Smith RM, Lange AK, et al. Lower limbmuscle strengthening does not change frontal planemoments in women with knee osteoarthritis: a rando-mized controlled trial. Clin Biomech 2011; 26: 167–174.
8. Rutherford DJ, Hubley-Kozey C and Stanish W. Hip
abductor function in individuals with medial knee
osteoarthritis: implications for medial compartment load-
ing during gait. Clin Biomech 2014; 29: 545–550.9. Kadaba MP, Ramakrishnan HK and Wooten ME. Mea-
surement of lower extremity kinematics during level
walking. J Orthop Res 1990; 8: 383–392.10. Herzog W. The relation between the resultant moments
at a joint and the moments measured by an isokinetic
dynamometer. J Biomech 1988; 21: 5–12.11. Robertson DGE, Caldwell GE, Hamill J, et al. Research
methods in biomechanics. Windsor, ON, Canada: Human
Kinetics, 2004.12. Weinhandl JT and O’Connor KM. Assessment of a
greater trochanter-based method of locating the hip joint
center. J Biomech 2010; 43: 2633–2636.13. Clauser CE, McConville JT and Young JW. Weight, vol-
ume, and center of mass of segments of the human body.
Dayton, OH: Wright-Patterson Air Force Base, 1969,
http://www.dtic.mil/dtic/tr/fulltext/u2/710622.pdf14. Dempster W. Space requirements of the seated operator.
Dayton, OH: Wright-Patterson Air Force Base, 1955,
http://www.smpp.northwestern.edu/savedLiterature/
DempsterEtAl.1955.pdf
15. Lewinson RT, Fukuchi CA, Worobets JT, et al. The
effects of wedged footwear on lower limb frontal plane
biomechanics during running. Clin J Sport Med 2013; 23:
208–215.16. Winter DA. Biomechanics and motor control of human move-
ment. 4th ed.Hoboken, NJ: John Wiley & Sons, 2009.17. Westing SH, Seger JY, Karlson E, et al. Eccentric and
concentric torque-velocity characteristics of the quadri-
ceps femoris in man. Eur J Appl Physiol Occup Physiol
1988; 58: 100–104.18. Nigg BM and Herzog W. Biomechanics of the musculos-
keletal system. 3rd ed.Hoboken, NJ: John Wiley & Sons,
2007.19. Geiser CF, O’Connor KM and Earl JE. Effects of iso-
lated hip abductor fatigue on frontal plane knee
mechanics. Med Sci Sports Exerc 2010; 42: 535–545.20. Sled EA, Khoja L, Deluzio KJ, et al. Effects of a home
program of hip abductor exercises on knee joint loading,
strength, function, and pain in people with knee osteoar-
thritis: a clinical trial. Phys Ther 2010; 90: 895–904.21. Bennell KL, Hunt MA, Wrigley TV, et al. Hip strengthen-
ing reduces symptoms but not knee load in people with med-
ial knee osteoarthritis and varus alignment: a randomized
controlled trial. Osteoarthritis Cartilage 2010; 18: 621–628.22. Hunt MA, Birmingham TB, Bryant D, et al. Lateral
trunk lean explains variation in dynamic knee joint load
in patients with medial compartment knee osteoarthritis.
Osteoarthritis Cartilage 2008; 16: 591–599.23. Youssef AR, Longino D, Seerattan R, et al. Muscle
weakness causes joint degeneration in rabbits. Osteoar-
thritis Cartilage 2009; 17: 1228–1235.24. Moore KL and Dalley AF. Clinically oriented anatomy.
5th ed.Philadelphia, PA: Lippincott Williams & Wilkins,
2005.
Lewinson et al. 1263
by guest on December 16, 2014pih.sagepub.comDownloaded from
Related Documents











