1 Title: The prevalence and correlates of supportive care needs in testicular cancer survivors: A cross-sectional study Running head: Testicular cancer survivors’ unmet needs Authors: Allan ‘Ben’ Smith 1 , Madeleine King 1,2 , Phyllis Butow 1 , Tim Luckett 3 , Peter Grimison 2,4 , Guy C. Toner 2,5 , Martin Stockler 2,4 , Elizabeth Hovey 2,6 , John Stubbs 2,7 , George Hruby 8 , Howard Gurney 9 , Sandra Turner 9 , Mahmood Alam 10 , Keith Cox 4 , Ian Olver 11 Affiliations: 1. Psycho-Oncology Co-operative Research Group (PoCoG), University of Sydney, Sydney, NSW, Australia 2. Australian and New Zealand Urogenital and Prostate Cancer Trials Group (ANZUP), Sydney, NSW, Australia 3. Improving Palliative Care through Clinical Trials (ImPaCCT), South Western Sydney Clinical School, The University of New South Wales, Sydney, NSW, Australia 4. Sydney Cancer Centre, Sydney, NSW, Australia 5. Peter MacCallum Cancer Centre and University of Melbourne, Melbourne, VIC, Australia 6. Prince of Wales Hospital, Sydney, NSW, Australia 7. Cancer Voices Australia, Sydney, NSW, Australia 8. Royal Prince Alfred Hospital, Sydney, NSW, Australia 9. Crown Princess Mary Cancer Centre, Westmead Hospital, Sydney, NSW, Australia 10. Liverpool Hospital, Sydney, NSW, Australia 11. Cancer Council Australia, Sydney, NSW, Australia Corresponding author: Allan ‘Ben’ Smith PoCoG, School of Psychology Transient Building (F12) University of Sydney NSW 2006 AUSTRALIA Ph: +61 2 9351 4518 Fax: +61 2 9036 5292 Email: [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
Title: The prevalence and correlates of supportive care needs in testicular cancer survivors: A cross-sectional study Running head: Testicular cancer survivors’ unmet needs Authors: Allan ‘Ben’ Smith1, Madeleine King1,2, Phyllis Butow1, Tim Luckett3, Peter Grimison2,4, Guy C. Toner2,5, Martin Stockler2,4,
Elizabeth Hovey2,6, John Stubbs2,7, George Hruby8, Howard Gurney9, Sandra Turner9, Mahmood Alam10, Keith Cox4, Ian Olver11
Affiliations: 1. Psycho-Oncology Co-operative Research Group (PoCoG), University of Sydney, Sydney, NSW, Australia 2. Australian and New Zealand Urogenital and Prostate Cancer Trials Group (ANZUP), Sydney, NSW, Australia
3. Improving Palliative Care through Clinical Trials (ImPaCCT), South Western Sydney Clinical School, The University of New South Wales, Sydney, NSW, Australia
4. Sydney Cancer Centre, Sydney, NSW, Australia 5. Peter MacCallum Cancer Centre and University of Melbourne, Melbourne, VIC, Australia 6. Prince of Wales Hospital, Sydney, NSW, Australia 7. Cancer Voices Australia, Sydney, NSW, Australia 8. Royal Prince Alfred Hospital, Sydney, NSW, Australia 9. Crown Princess Mary Cancer Centre, Westmead Hospital, Sydney, NSW, Australia 10. Liverpool Hospital, Sydney, NSW, Australia 11. Cancer Council Australia, Sydney, NSW, Australia
Corresponding author: Allan ‘Ben’ Smith PoCoG, School of Psychology Transient Building (F12) University of Sydney NSW 2006 AUSTRALIA Ph: +61 2 9351 4518 Fax: +61 2 9036 5292 Email: [email protected]
2
Abstract Objective: This cross-sectional study aimed to identify the prevalence and correlates of supportive care needs in testicular cancer (TC) survivors. Methods: Men who had completed active anti-cancer treatment for TC between 6 months and 5 years previously showing no evidence of recurrence were recruited from 14 Australian cancer centres (September 2009 - February 2011). Participants completed a self-report questionnaire measuring sociodemographics, disease and treatment information, supportive care needs (CaSUN), psychological distress (DASS21) and health-related quality of life (HRQOL; SF36v2). Results: Of the 486 eligible TC survivors invited to participate, 244 completed the questionnaire. Sixty-six percent reported one or more unmet supportive care needs. The mean number of unmet needs was 4.73 (SD=7.0, Range=0-34). The most common unmet needs related primarily to existential survivorship issues (e.g. life stress) and relationships (e.g. sex life). Younger age and presence of chronic illness other than TC were significantly associated with higher number of unmet needs. Number of unmet needs was more highly correlated with psychological distress and HRQOL than unmet need strength. Conclusions: The majority of TC survivors reported one or more unmet needs. Unmet needs regarding existential survivorship issues were frequently reported by TC survivors despite their favorable prognosis. Relationships unmet needs were less prevalent, but still more common than in breast and gynecological cancer survivors. These findings appear to be related to the young age of TC survivors. As higher number of unmet needs is significantly associated with psychological morbidity and impaired HRQOL, interventions addressing this constellation of issues are needed. Keywords Testicular cancer, Survivor, Supportive care needs, Psychological distress, Health-related quality of life, Oncology
3
Introduction Testicular cancer (TC) is the most prevalent cancer (excluding skin) in men aged 15-35 years [1] and its incidence is rising, particularly among Caucasians [2]. Advances in diagnosis and treatment, particularly cisplatin-based chemotherapy, have achieved cure rates exceeding 95% [3], resulting in increasing numbers of TC survivors. There is a growing awareness of cancer survivors’ supportive care needs [4], commonly defined as “the requirement of some action or resource that is necessary, desirable, or useful to attain optimal well-being” [5; p227]. Needs are considered met if the required action/resource has been provided, or unmet if not. Identification of unmet needs can guide assessment, planning and delivery of services to improve TC survivors’ psychological wellbeing and health-related quality of life (HRQOL) [6]. Testicular cancer survivors may have needs relating to enduring impacts of their diagnosis and treatment and their relative youth. The long-term physical effects of TC treatments include potential infertility, altered neurological and respiratory function, plus increased risk of secondary malignancy and cardiovascular disease [7, 8]. Testicular cancer can raise practical challenges (e.g. difficulty getting life insurance) and psychological/existential issues (e.g. fear of cancer recurrence) largely unexpected by young men and with considerable personal and professional implications [9]. Additionally, TC affects an organ inherently linked to masculine and sexual identity, potentially exacerbating concerns regarding body image, sexuality and intimate relationships [10]. While less common than more global health concerns, masculinity/sexuality issues have been linked to higher depression levels [11]. Research investigating TC survivors’ psychological wellbeing and HRQOL indicates poorer patient-reported outcomes (PROs) are related to young age, single relationship status, unemployment and chronic illness [12-14]. The only study of TC survivors’ supportive care needs [15] was from a single urban cancer centre with an established patient education and survivorship program and most participants (56%) were managed with only surveillance post-orchidectomy. Consequently, their results may under-represent the prevalence of TC survivors’ unmet needs generally. Research objectives and hypotheses This study aimed to identify the prevalence and correlates of supportive care needs in a multi-centre sample of TC survivors. We expected the majority of TC survivors would report unmet needs, particularly regarding:
1) Existential survivorship, due to being diagnosed with a life-threatening illness at a relatively early and formative life stage; 2) Relationships, because of TC’s impact on sexuality and many TC survivors being at an age where they are developing long-term intimate
relationships. Another objective was to explore factors associated with higher number and strength of unmet needs in TC survivors. Due to limited prior research, we thought sociodemographic (e.g. younger age), disease (e.g. metastatic disease) and treatment (e.g. chemotherapy) variables, may provide a good foundation for identifying those likely to experience greater number or strength of unmet needs. We also anticipated that higher number and strength of unmet needs would be associated with poorer psychological wellbeing and HRQOL. Methods
4
Participants Eligibility criteria were:
1) completion of active anti-cancer treatment for TC 0.5-5 years previously; 2) no evidence of recurrence; 3) older than 18 years; 4) sufficient English for questionnaire completion.
The first criterion enabled identification of TC-related issues beyond acute effects of diagnosis and treatment, but at a time when TC could still be expected to have a relatively strong influence on psychosocial wellbeing. Recruitment Men were invited to participate by their treating clinician during follow-up consultations or via posted invitation letters. Participants were recruited from 14 Australian metropolitan cancer centres over 18 months (September 2009 - February 2011). Participating centres’ ethics committees approved the study and all participants provided written informed consent. Sample size A target of 250 survivors was calculated to allow estimation of mean levels of unmet needs, anxiety, depression and HRQOL with 95% confidence intervals within ±0.12 of a standard deviation and proportions of patients with clinically important levels of anxiety/depression with 95% confidence intervals of ±5% (assuming underlying prevalence of 20%). Questionnaire Participants completed either a postal or online self-report questionnaire, which produced data of comparable quality [16]. The questionnaire measured sociodemographics, disease and treatment information, and PROs using measures with well-established validity and reliability listed below. Supportive care needs were evaluated using the Cancer Survivors’ Unmet Needs measure (CaSUN) [17]. The CaSUN contains 28 items assessing needs over the preceding month across five domains: Existential Survivorship - 14 items (e.g. help to move on with life), Comprehensive Cancer Care - 6 items (e.g. local health care services), Information - 3 items (e.g. understandable information), Relationships - 3 items (e.g. problems with sex life) and Quality of Life (QOL) - 2 items (e.g. changes to QOL). Domain Cronbach’s alphas ranged from .75-.92 in our sample, indicating acceptable to excellent internal consistency. A further 7 items cover complementary/alternative therapies, fertility, employment, financial support, insurance, legal services, and ongoing service provision. Respondents indicate whether needs are “not applicable”, “met”, or “unmet”. The strength of unmet needs is rated as “weak” (1), “moderate” (2) or “strong” (3). Unmet needs can range in number from 0-35 and strength from 1-3.
5
Psychological distress was measured using the Depression Anxiety Stress Scales short-form (DASS21) [18], which contains three seven-item subscales measuring depression, anxiety and stress over the past week. Subscale scores can range from 0-42. Higher scores indicate greater morbidity. Cronbach’s alpha for the DASS21 subscales in our sample were .93, .83, and .91 respectively, signifying good to excellent internal consistency. The SF-36v2 [19] was used to measure HRQOL. Eight domains of HRQOL are assessed over the preceding month: physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health. Domain Cronbach’s alphas ranged from .82-.93 in our sample, representing good to excellent internal consistency. Australian population norms and weights [20] were used to calculate Physical Component Summary (PCS) and Mental Component Summary (MCS) scores. Higher domain and component summary scores indicate better HRQOL. Statistical analysis Responses for the CaSUN, DASS21 and SF-36v2 were scored following standard algorithms [17-19]. Missing CaSUN items were counted as zeros when calculating domain or total needs scores. However, if all items contributing to a domain or total score were missing then the corresponding summary score was also considered missing. Missing DASS21 and SF-36v2 items were replaced using the within-person average score of completed items on the same scale, provided participants had answered at least 50% of scale items. Unmet need prevalence was evaluated with several descriptive statistics: proportion of participants reporting one or more unmet needs; mean number of unmet needs reported in each domain and in total; proportion of TC survivors endorsing each unmet need; and mean strength rating of each unmet need among men with that unmet need. Univariate and multiple regression was used to identify explanatory variables associated with the dependent variables, total number of unmet needs and average unmet need strength. Explanatory variables entered individually into univariate regressions and simultaneously into the multiple regression model were the sociodemographic, disease and treatment variables in Table 1, plus age and time since treatment completion. Categorical variables with more than two groups were dummy coded. The reference group for education level was “year 10 or below” and for treatment “surveillance/surgery alone”. Bivariate and partial Pearson correlations were calculated to explore associations of number and strength of unmet needs with psychological distress and HRQOL. Partial correlations were adjusted for the abovementioned explanatory variables. Data analysis was performed using SPSS version 17 (IBM, Somers, NY, USA), with p-values of <.05 considered statistically significant. Results Of 486 eligible TC survivors invited to participate, 139 (29%) could not be contacted to confirm receipt of the study invitation and 50 (10%) declined to participate. Of 297 TC survivors who agreed to participate, 244 returned the questionnaire (125 by post and 119 online), giving a response rate of 70% of 347 contactable or 50% of 486 eligible. A significantly higher proportion of TC survivors recruited in clinic (110/140) returned questionnaires compared to those recruited by invitation letter (134/346; χ2=61.7, p<.001). As all data were self-reported, participants and non-participants could not be compared. The mean age of diagnosis for participating TC survivors (34.9 years, SD=10.0, Range=16-69), was comparable to that of Australian men diagnosed with TC in general (35.3 years; t(240)=-.577, p=.564) [21]. While treatment data were unavailable for all Australian TC survivors, oncologists on the research team confirmed the treatments reported in this sample were reasonably consistent with what they observed in clinical practice.
6
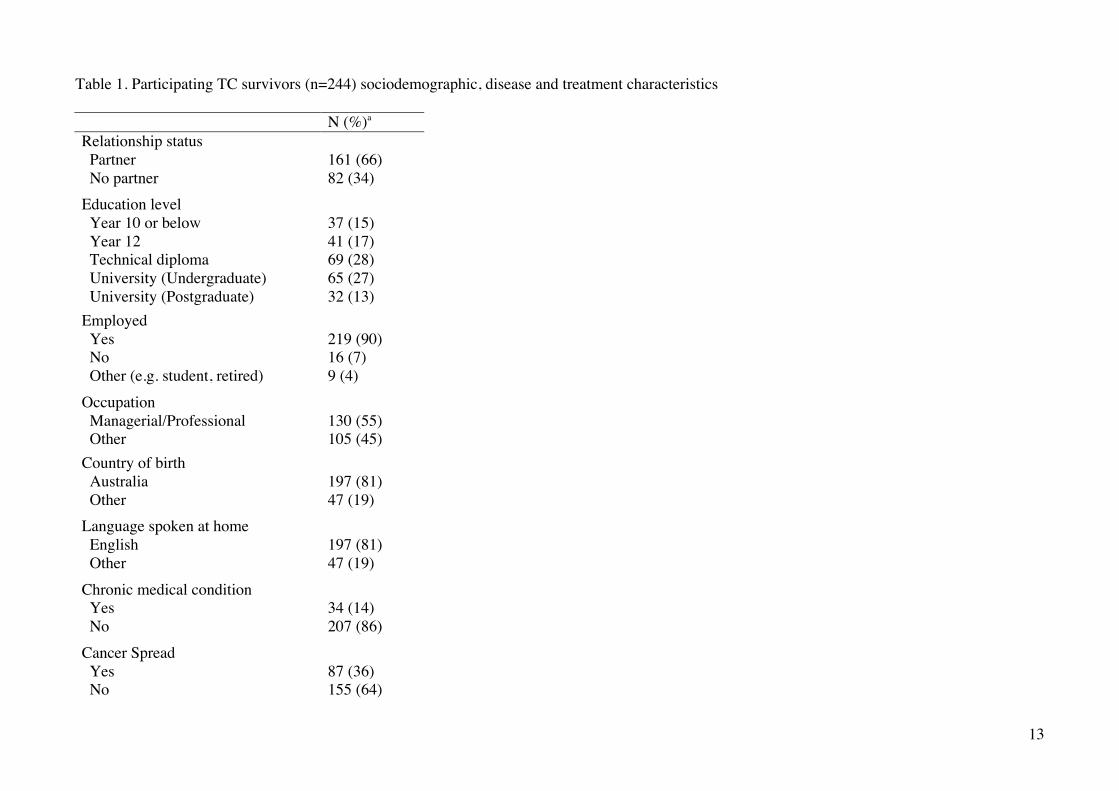
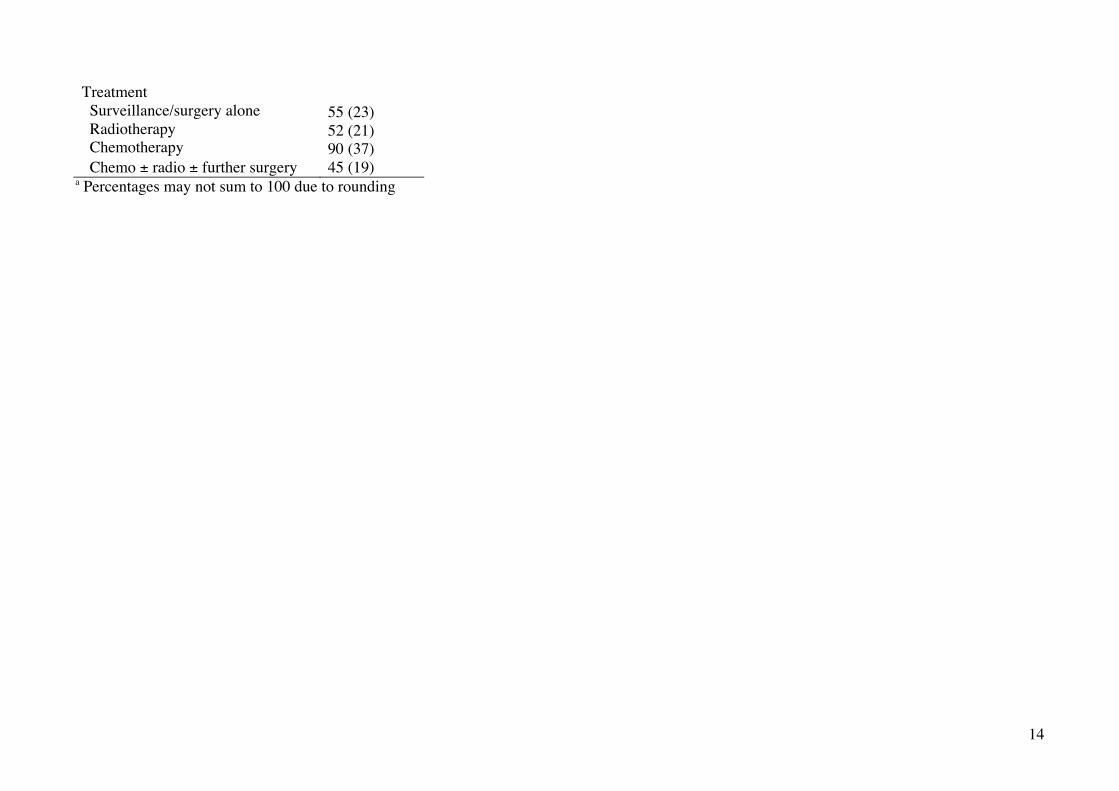
Mean participant age at study assessment was 38.3 years (SD=10.3, Range=21-68). Mean time since treatment completion was 2.3 years (SD=1.4, Range=0.5-5). Metastatic disease was reported by 36%, and 77% had received chemotherapy and/or radiotherapy. Chronic disease was reported by 34 participants (14%), the most commonly reported chronic medical conditions being testosterone deficiency (n=6) and cardiovascular diseases particularly hypertension (n=6), which may both be caused by TC and its treatment. Table 1 shows additional sociodemographic, disease and treatment characteristics.
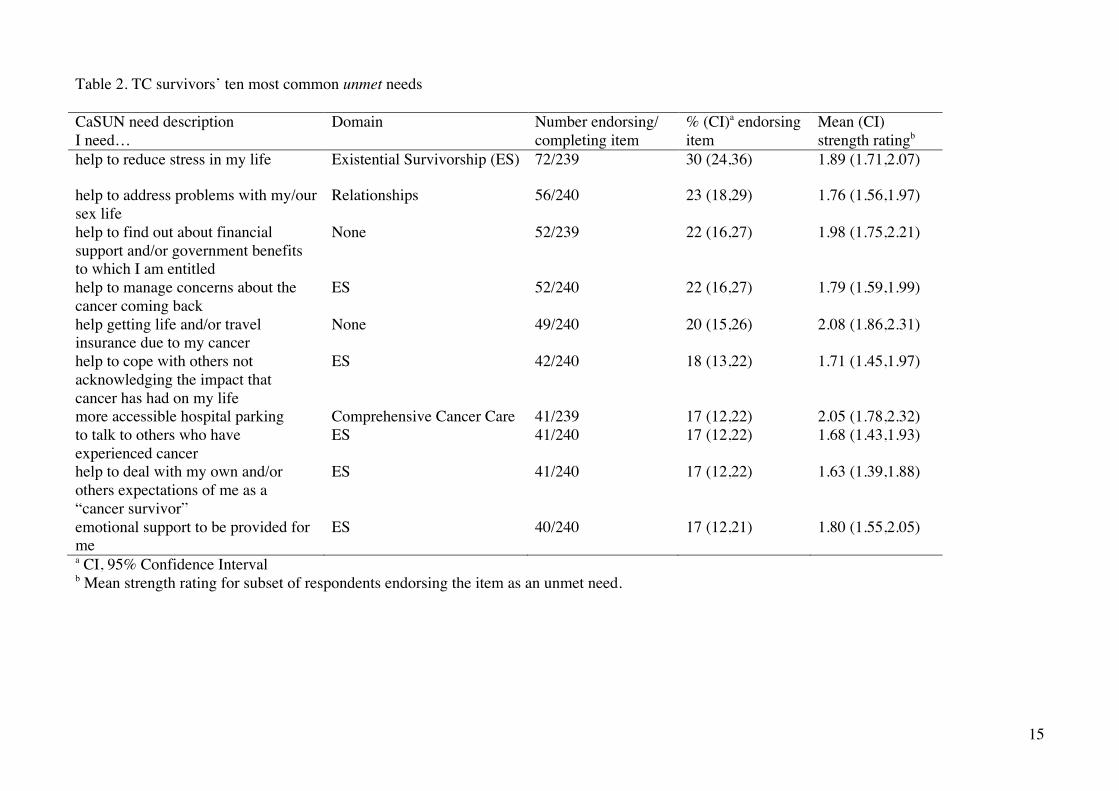
Table 1 Prevalence and type of supportive care needs Sixty-six percent of participants reported one or more unmet supportive care needs. Mean total number of unmet needs was 4.73 (SD=7.0, Range=0-34). Mean number of unmet needs in each CaSUN domain was: Existential Survivorship - 2.12 (SD=3.44), Comprehensive Cancer Care - 0.67 (SD=1.32), Information - 0.32 (SD=.76), Relationships - 0.50 (SD=.90) and QOL - 0.26 (SD=.61). More than 20% of respondents had unmet needs related to life stress, sex life problems, finances and fear of cancer recurrence (Table 2). Six of the ten most common unmet needs were in the existential survivorship domain.
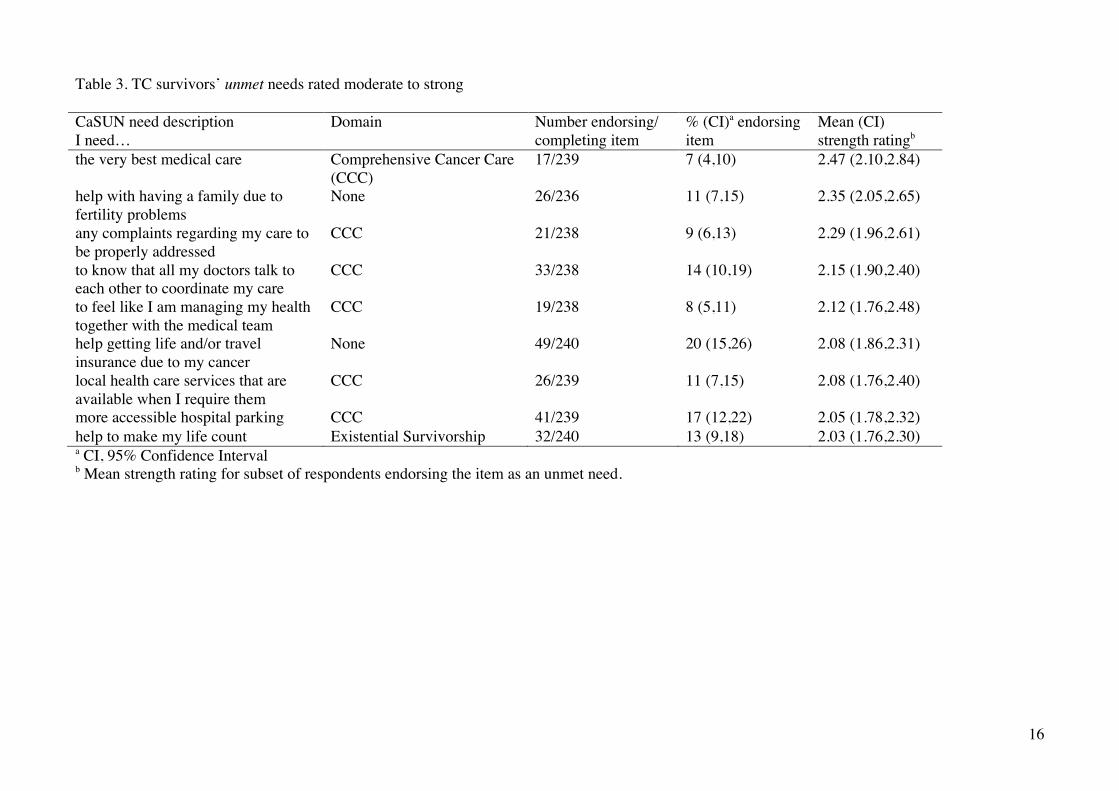
Table 2 The nine strongest unmet needs (mean strength rating of two or more among the subsample of participants endorsing those items) related to six comprehensive cancer care issues, fertility, insurance, and needing help to make life count (Table 3). However, except for insurance and hospital parking, these were considered unmet by under 15% of respondents.
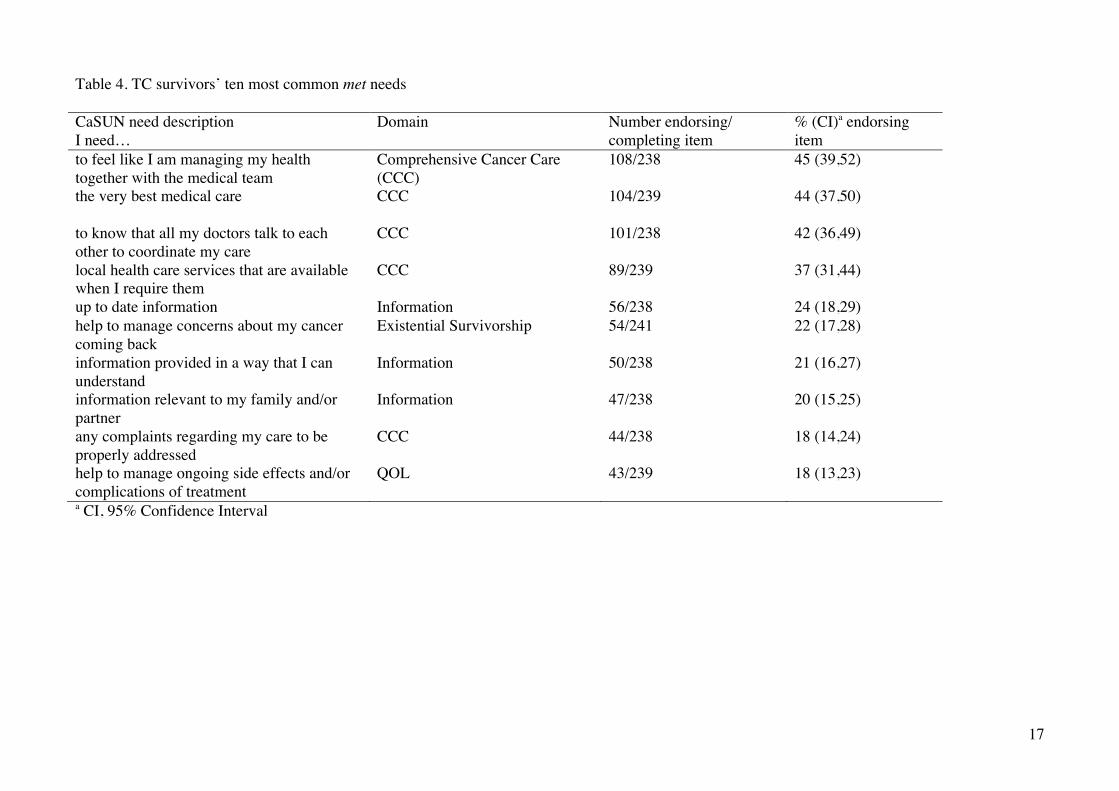
Table 3 Seventy-five percent of participants reported one or more met needs. Mean number of met needs was 4.76 (SD=5.0, Range=0-30). The most common met needs related to comprehensive cancer care and information provision (Table 4).
Table 4
Correlates of unmet needs The only explanatory variable significantly associated with higher number of unmet needs in univariate regression was chronic illness (β=.209, p=.001, r2=.04). In multiple regression, where other explanatory variables were controlled for, chronic illness remained significantly associated with higher number of unmet needs (β=.189, p=.01, sr2=.03); younger age was also significantly associated with higher number of unmet needs (β=-.188, p=.04, sr2=.02). Higher mean unmet need strength was associated with radiotherapy treatment (β=.161, p=.04, r2=.03) in univariate regression, while
7
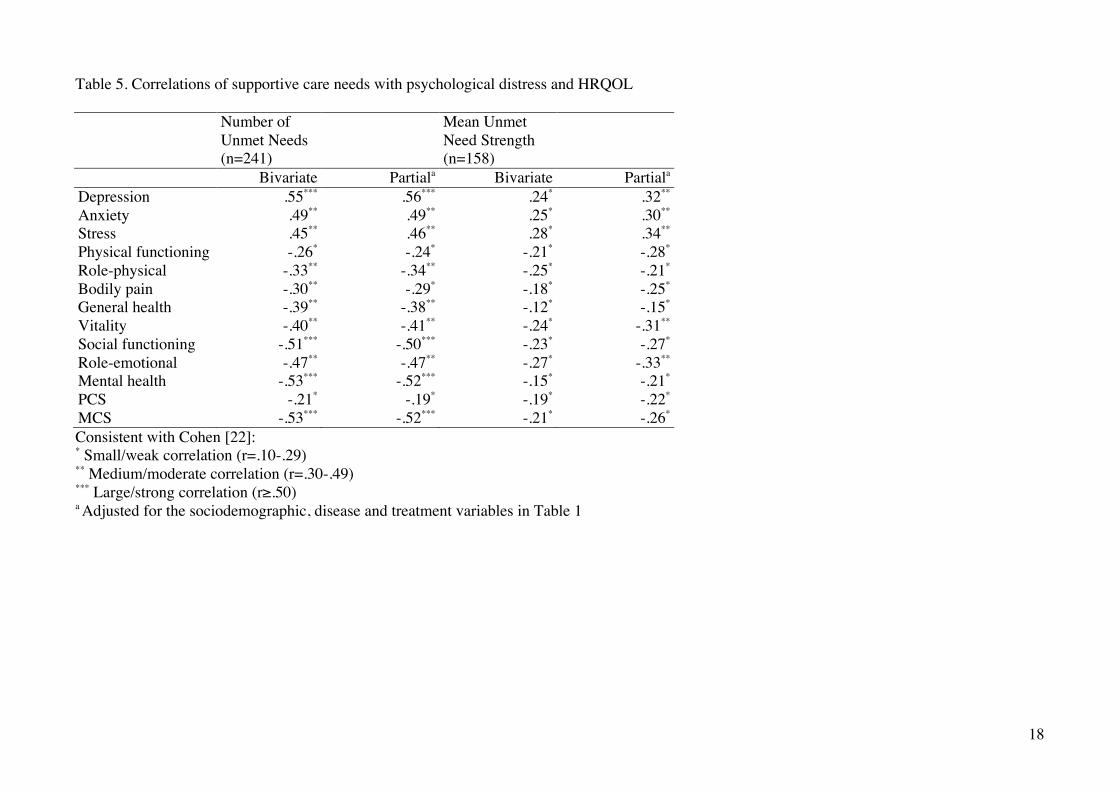
chemotherapy treatment was associated with lower mean unmet need strength (β=-.196, p=.01, r2=.04). However, in multiple regression, no sociodemographic, disease or treatment variables showed significant associations with average unmet need strength. Associations between unmet needs and other PROs Greater total number of unmet needs was significantly correlated with higher levels of depression, anxiety and stress, and poorer HRQOL across all domains (Table 5), and particularly strongly correlated with higher depression levels, poorer social functioning, mental health and mental aspects of HRQOL generally (MCS score). Conversely, average unmet need strength was only weakly correlated with most psychological distress and HRQOL outcomes.
Table 5 [22] Discussion This study offers the most comprehensive exploration to date of the prevalence and correlates of TC survivors’ supportive care needs. Two-thirds of our sample reported one or more unmet needs, while three-quarters reported one or more met needs. The most common unmet needs related to existential survivorship issues such as life stress and fear of cancer recurrence. Younger age and chronic illness additional to TC were associated with higher number of unmet needs. A minority of men experienced moderate to strong unmet needs, largely related to comprehensive cancer care issues like needing the best medical care and complaints being properly addressed. Total number of unmet needs was at least moderately associated with most psychological distress and HRQOL outcomes, and strongly correlated with higher depression levels, poorer social functioning and worse mental health. Among men with unmet needs, average unmet need strength showed mostly weak associations with psychological distress and HRQOL. The proportion of TC survivors reporting one or more unmet needs (66%) was similar to that observed in previous research using the CaSUN on testicular (63%) [15] and breast (61%) [23] cancer survivors, but somewhat higher than studies of gynecological (52-56%) [24, 25] and mixed cancer survivors (47-54%) [17, 26]. The mean total number of unmet needs reported by TC survivors (4.73) was towards the middle of the range of means/medians (2.0-8.6) reported previously [15, 17, 23-25, 27]. The younger age of TC survivors may explain the higher proportion reporting unmet needs in our study and Bender et al [15]. The mean age of TC survivors participating in both studies was at least 15 years lower than any of the other abovementioned studies and lower age was associated with greater number of unmet needs in our study. Our hypothesis that unmet needs reported by TC survivors would largely relate to existential survivorship issues and relationships was partially supported. Six of the ten most common unmet needs related to existential survivorship, similar to previous findings in other cancer survivor populations. The relationship supportive care need for “help to address problems with my/our sex life” was the second most common unmet need in our sample, but no other relationship unmet needs featured among the ten most common. However, the mean number of relationship unmet needs was still higher than in breast [23] and gynaecological [25] cancer survivors, where a need for help to address sex life issues did not feature in the ten most frequent unmet needs, potentially reflecting gender differences.
8
The identified need for help with relationship/sexuality issues is consistent with a previous finding that 67% of TC survivors needed information concerning sexuality and 22% still needed support regarding sexuality a median of 5.9 years post-treatment [28]. TC survivors who did not undergo radiotherapy or chemotherapy were the least likely to need support [28]. This may explain the greater number of relationship/sexuality needs reported in our sample compared to Bender et al’s [15], the majority of whom underwent only surveillance post-orchidectomy. The met needs most commonly reported by TC survivors in our study were similar to those in Bender et al’s study [15], the majority relating to comprehensive cancer care or information. However, Bender’s sample reported a higher number of met needs (median=8.0 versus mean=4.8 in our study) and the ten most common met needs were endorsed by 37-80% of respondents versus 18-45% in our study. This discrepancy may indicate support services provided by Bender’s Canadian recruiting centre more effectively addressed TC survivors supportive care needs than the Australian health system. However, since there were similar unmet need levels in both studies, it is more likely that Canadian TC survivors simply reported more needs in general. Exactly why is unclear, but it may be due to the use of an amended CaSUN measure by Bender et al, with fewer items and a modified response scale. Our results and those of Bender et al [15] suggest that generally TC survivors do not report many needs and most reported needs are adequately addressed. However, the small but noteworthy proportion of men with moderate to strong unmet needs highlights the importance of identifying characteristics associated with greater unmet needs, so that interventions can be targeted at these individuals. Of the sociodemographic, disease and treatment variables assessed, only lower age and chronic illness/comorbidity in addition to TC were associated with higher number of unmet needs in multiple regression, although these variables only explained a small amount of variance. Bender et al similarly found that younger age was associated with number of met, but not unmet needs. Younger TC survivors should be carefully screened for unmet needs and offered tailored supportive care services. Additionally, those experiencing ongoing morbidity potentially related to TC and its treatment, such as testosterone deficiency and hypertension, should be carefully monitored and managed. Unmet need strength was not as highly correlated with other PROs as number of unmet needs, which was strongly associated with psychological distress and mental rather than physical HRQOL, confirming previous findings [25]. This may be due to the prevalence of existentially related unmet needs, which are more likely to be associated with impaired psychological versus physical functioning [29]. The predominance of existential and relationship needs suggests supportive care for TC survivors should focus more on psychosocial than physical aspects of HRQOL. The optimal way of providing supportive care to TC survivors is still unclear. Bender et al [15] found the most common source of support for TC survivors was their partner/spouse (62%) followed by parents (17%) and friends (8%), while only 4% sought help from health professionals. It is unclear why TC survivors do not generally seek help from health professionals, psychologists especially, seeing as many of their unmet needs are psychological/existential in nature and appear to lead to reduced mental HRQOL. Perhaps most needs are adequately addressed via support from partners, friends and family. Alternatively, maybe TC survivors, like many other younger men, are concerned about the stigma attached to seeking professional help. Or perhaps the frequently reported unmet need for more accessible hospital parking is indicative of difficulties TC survivors experience accessing health services. The cost of obtaining help may also be prohibitive; 22% of our sample reported an unmet need for help finding
9
out about financial support and/or government benefits, despite free or subsidised treatment by health professionals being available through Medicare in Australia. In light of these possibilities, a low-intensity tailored intervention that does not require face-to-face contact and is free to access such as an Internet intervention may be well suited to addressing TC survivors’ needs. Forty-four percent of TC survivors in Bender et al’s [15] study said they would use a TC online support community offered by their institution and a further 43% possibly would. Testicular cancer survivors’ strongest unmet needs largely related to comprehensive cancer care, however, they were also relatively uncommon. This suggests a minority of TC survivors were dissatisfied with their medical care and consequently perceived this as their greatest area of need. The remaining majority of TC survivors whose medical care needs were satisfied, reported other needs. This provides support for a potential hierarchy of needs, with existential issues only endorsed once lower-level needs, such as for information and comprehensive care, are satisfied [17]. This finding has important implications for clinical practice and intervention design, as lower-level needs may need to be satisfied before higher-level needs can be addressed. Limitations Our cross-sectional design means we cannot infer causality or describe how outcomes change over time. While the large number of participants from multiple cancer centres around Australia is a strength, our low response rate may limit generalisability. Comparison of participants and non-participants to check for sampling bias was not feasible, but evaluation against age data for all Australian TC survivors [21] and clinical experience suggests our sample was representative of Australian TC survivors generally. The cancer-specific nature of the CaSUN prevented comparison of unmet needs in TC survivors and the general population. Normative data from a modified non-cancer-specific version of the CaSUN would facilitate future comparisons. Only a small amount of variance in the number of unmet needs was explained by individual sociodemographic, disease and treatment variables. Psychological variables such as neuroticism or meaning making, shown to be related to somatic and mental morbidity [30] and psycho-social wellbeing [31] respectively, may be more pertinent risk factors for poor psychosocial outcomes after a diagnosis of TC. The goal of future research is to: 1) determine further risk factors that can identify high-risk individuals; 2) develop effective interventions for vulnerable at-risk subgroups. Finally, given the relatively high mean number of relationship unmet needs reported in this study, investigating the supportive care needs of TC survivors’ partners using an instrument such as the Cancer Survivors’ Partners Unmet Needs measure [32] may be worthwhile. Conclusion Most TC survivors reported one or more unmet needs. Unmet needs regarding existential survivorship issues were frequently reported by TC survivors despite their favorable prognosis. Relationships unmet needs were not as prevalent, but were still more common than in breast and gynecological cancer survivors. These findings appear to be related to the young age of TC survivors. As higher number of unmet needs is significantly associated with psychological morbidity and impaired HRQOL, interventions addressing this constellation of issues are needed. Acknowledgements
10
This study was co-funded by beyondblue and Cancer Australia (grant number 507961). Allan ‘Ben’ Smith is supported by an Australian Rotary Health Ian Scott Scholarship. Professor Butow holds a NHMRC Senior Principal research fellowship and Professor King is supported by the Australian Government through Cancer Australia. The study was conducted by the Psycho-Oncology Co-operative Research Group (PoCoG) in collaboration with the Australian and New Zealand Urogenital and Prostate Cancer Trials Group (ANZUP). PoCoG were responsible for study development, funding, coordination, analysis and reporting. ANZUP contributed to study development, funding, recruitment, analysis, and reporting. The authors would like to thank all the patients who participated in the study, as well as investigators and trials staff at Border Medical Oncology (Richard Eek, Lauren Callow), The Canberra Hospital (Gane Pranavan, Olive Doig), Concord Repatriation Hospital (Martin Stockler), Flinders Medical Centre (Bogda Koczwara, Alison Richards), Liverpool Hospital (Mahmood Alam, Suyen Moncada), Princess Alexandra Hospital (Damien Thompson, Steph Le), Peter MacCallum Cancer Centre (Guy Toner), Prince of Wales Hospital (Elizabeth Hovey, Christine Norris), Royal Adelaide Hospital (Nimit Singhal, Hazel Bourke), Royal North Shore Hospital (Nick Pavlakis, Julia Hunter), Royal Prince Alfred Hospital (Michael Boyer, Keith Cox), St George Hospital (Joe Bucci, Xiaolu Wang), Tweed Hospital (Ehtesham Abdi, Sharon Clark) and Westmead Hospital (Howard Gurney, Sandra Turner). Conflicts of interest The authors have no conflicts of interest to disclose. All authors have full control of all primary data and agree to allow the journal to review their data if requested.
11
References 1. Cancer Incidence in Five Continents. Lyon: IARC; 2007. 2. Rosen A, Jayram G, Drazer M, Eggener SE. Global trends in testicular cancer incidence and mortality. Eur Urol 2011; 60: 374-9. 3. SEER Cancer Statistics Review, 1975-2007. Bethesda, MD: National Cancer Institute; 2010. 4. Committee on Cancer Survivorship: Improving C, Quality of L, Institute of M, National Research C. From Cancer Patient to Cancer Survivor: Lost
in Transition: The National Academies Press 2005. 5. Sanson-Fisher R, Girgis A, Boyes A et al. The unmet supportive care needs of patients with cancer. Supportive Care Review Group. Cancer 2000;
88: 226-37. 6. Pollock K, Wilson E, Porock D, Cox K. Evaluating the impact of a cancer supportive care project in the community: Patient and professional
configurations of need. Health Soc Care Community 2007; 15: 520-9. 7. Grossfeld GD, Small EJ. Long-term side effects of treatment for testis cancer. Urol Clin North Am 1998; 25: 503-15. 8. Travis LB, Curtis RE, Storm H et al. Risk of second malignant neoplasms among long-term survivors of testicular cancer. J Natl Cancer Inst 1997;
89: 1429-39. 9. Brodsky MS. Testicular cancer survivors impressions of the impact of the disease on their lives. Qual Health Res 1995; 5: 78-96. 10. Jonker-Pool G, Van De Wiel HBM, Hoekstra HJ et al. Sexual Functioning after Treatment for Testicular Cancer - Review and Meta-Analysis
of 36 Empirical Studies between 1975-2000. Arch Sex Behav 2001; 30: 55-74. 11. Siafaka V, Hyphantis TN, Alamanos I et al. Personality factors associated with psychological distress in testicular cancer survivors. J Pers
Assess 2008; 90: 348-55. 12. Fleer J, Hoekstra HJ, Sleijfer DT, Hoekstra-Weebers JEHM. Quality of life of survivors of testicular germ cell cancer: A review of the literature.
Support Care Cancer 2004; 12: 476-86. 13. Dahl AA, Mykletun A, Fossa SD. Quality of life in survivors of testicular cancer. Urologic Oncology: Seminars and Original Investigations
2005; 23: 193-200. 14. Luckett T, Butow PN, King MT, Olver IN. Psycho-social issues in long-term survivors of testicular cancer: Directions for future research. Asia
Pac J Clin Oncol 2008; 4: 125-31. 15. Bender JL, Wiljer D, To MJ et al. Testicular cancer survivors' supportive care needs and use of online support: a cross-sectional survey.
Support Care Cancer 2012: 1-10. 16. Smith AB, King M, Butow P, Olver I. A comparison of data quality and practicality of online versus postal questionnaires in a sample of
testicular cancer survivors. Psychooncology 2013; 22: 233-7. 17. Hodgkinson K, Butow P, Hunt GE et al. The development and evaluation of a measure to assess cancer survivors' unmet supportive care needs:
The CaSUN (Cancer Survivors' Unmet Needs measure). Psychooncology 2007; 16: 796-804. 18. Lovibond SH, Lovibond PF. Manual for the Depression Anxiety Stress Scales. Second Edition ed. Sydney: Psychology Foundation 1995. 19. Ware JE, Jr.,, Kosinski M, Bjorner JB et al. User's manual for the SF-36v2 Health Survey (2nd ed.). Lincoln, RI: Quality Metric Incorporated
2007.
12
20. Hawthorne G, Osborne RH, Taylor A, Sansoni J. The SF36 Version 2: Critical analyses of population weights, scoring algorithms and population norms. Qual Life Res 2007; 16: 661-73.
21. AIHW. Cancer in Australia 2010: an overview. Cancer series 2010 [cited 2013 8 March 2013]; Available from: http://www.aihw.gov.au/publication-detail/?id=6442472459
22. Cohen J. A power primer. Psychol Bull 1992; 112: 155-9. 23. Hodgkinson K, Butow P, Hunt GE et al. Breast cancer survivors' supportive care needs 2-10 years after diagnosis. Support Care Cancer 2007;
15: 515-23. 24. Urbaniec OA, Collins K, Denson LA, Whitford HS. Gynecological cancer survivors: Assessment of psychological distress and unmet
supportive care needs. Journal of Psychosocial Oncology 2011; 29: 534-51. 25. Hodgkinson K, Butow P, Fuchs A et al. Long-term survival from gynecologic cancer: Psychosocial outcomes, supportive care needs and
positive outcomes. Gynecol Oncol 2007; 104: 381-9. 26. Harrison SE, Watson EK, Ward AM et al. Primary health and supportive care needs of long-term cancer survivors: A questionnaire survey. J
Clin Oncol 2011; 29: 2091-8. 27. Lobb EA, Joske D, Butow P et al. When the safety net of treatment has been removed: Patients' unmet needs at the completion of treatment for
haematological malignancies. Patient Educ Couns 2009; 77: 103-8. 28. Jonker-Pool G, Hoekstra HJ, van Imhoff GW et al. Male sexuality after cancer treatment--needs for information and support: testicular cancer
compared to malignant lymphoma. Patient Educ Couns 2004; 52: 143-50. 29. Mazzotti E, Mazzuca F, Sebastiani C et al. Predictors of existential and religious well-being among cancer patients. Support Care Cancer 2011;
19: 1931-7. 30. Grov EK, Fossa SD, Bremnes RM et al. The personality trait of neuroticism is strongly associated with long-term morbidity in testicular cancer
survivors. Acta Oncol 2009; 48: 842-9. 31. Fleer J, Hoekstra HJ, Sleijfer DT et al. The role of meaning in the prediction of psychosocial well-being of testicular cancer survivors. Qual
Life Res 2006; 15: 705-17. 32. Hodgkinson K, Butow P, Hobbs KM et al. Assessing unmet supportive care needs in partners of cancer survivors: The development and
evaluation of the Cancer Survivors' Partners Unmet Needs measure (CaSPUN). Psychooncology 2007; 16: 805-13.
13
Table 1. Participating TC survivors (n=244) sociodemographic, disease and treatment characteristics N (%)a Relationship status Partner No partner
161 (66) 82 (34)
Education level Year 10 or below Year 12 Technical diploma University (Undergraduate) University (Postgraduate)
37 (15) 41 (17) 69 (28) 65 (27) 32 (13)
Employed Yes No Other (e.g. student, retired)
219 (90) 16 (7) 9 (4)
Occupation Managerial/Professional Other
130 (55) 105 (45)
Country of birth Australia Other
197 (81) 47 (19)
Language spoken at home English Other
197 (81) 47 (19)
Chronic medical condition Yes No
34 (14) 207 (86)
Cancer Spread Yes No
87 (36) 155 (64)
14
Treatment Surveillance/surgery alone Radiotherapy Chemotherapy Chemo ± radio ± further surgery
55 (23) 52 (21) 90 (37) 45 (19)
a Percentages may not sum to 100 due to rounding
15
Table 2. TC survivors’ ten most common unmet needs CaSUN need description I need…
Domain Number endorsing/ completing item
% (CI)a endorsing item
Mean (CI) strength ratingb
help to reduce stress in my life Existential Survivorship (ES) 72/239 30 (24,36) 1.89 (1.71,2.07)
help to address problems with my/our sex life
Relationships 56/240 23 (18,29) 1.76 (1.56,1.97)
help to find out about financial support and/or government benefits to which I am entitled
None 52/239 22 (16,27) 1.98 (1.75,2.21)
help to manage concerns about the cancer coming back
ES 52/240 22 (16,27) 1.79 (1.59,1.99)
help getting life and/or travel insurance due to my cancer
None 49/240 20 (15,26) 2.08 (1.86,2.31)
help to cope with others not acknowledging the impact that cancer has had on my life
ES 42/240 18 (13,22) 1.71 (1.45,1.97)
more accessible hospital parking Comprehensive Cancer Care 41/239 17 (12,22) 2.05 (1.78,2.32) to talk to others who have experienced cancer
ES 41/240 17 (12,22) 1.68 (1.43,1.93)
help to deal with my own and/or others expectations of me as a “cancer survivor”
ES 41/240 17 (12,22) 1.63 (1.39,1.88)
emotional support to be provided for me
ES 40/240 17 (12,21) 1.80 (1.55,2.05)
a CI, 95% Confidence Interval b Mean strength rating for subset of respondents endorsing the item as an unmet need.
16
Table 3. TC survivors’ unmet needs rated moderate to strong CaSUN need description I need…
Domain Number endorsing/ completing item
% (CI)a endorsing item
Mean (CI) strength ratingb
the very best medical care Comprehensive Cancer Care (CCC)
17/239 7 (4,10) 2.47 (2.10,2.84)
help with having a family due to fertility problems
None 26/236 11 (7,15) 2.35 (2.05,2.65)
any complaints regarding my care to be properly addressed
CCC 21/238 9 (6,13) 2.29 (1.96,2.61)
to know that all my doctors talk to each other to coordinate my care
CCC 33/238 14 (10,19) 2.15 (1.90,2.40)
to feel like I am managing my health together with the medical team
CCC 19/238 8 (5,11) 2.12 (1.76,2.48)
help getting life and/or travel insurance due to my cancer
None 49/240 20 (15,26) 2.08 (1.86,2.31)
local health care services that are available when I require them
CCC 26/239 11 (7,15) 2.08 (1.76,2.40)
more accessible hospital parking CCC 41/239 17 (12,22) 2.05 (1.78,2.32) help to make my life count Existential Survivorship 32/240 13 (9,18) 2.03 (1.76,2.30) a CI, 95% Confidence Interval b Mean strength rating for subset of respondents endorsing the item as an unmet need.
17
Table 4. TC survivors’ ten most common met needs CaSUN need description I need…
Domain Number endorsing/ completing item
% (CI)a endorsing item
to feel like I am managing my health together with the medical team
Comprehensive Cancer Care (CCC)
108/238 45 (39,52)
the very best medical care CCC 104/239 44 (37,50)
to know that all my doctors talk to each other to coordinate my care
CCC 101/238 42 (36,49)
local health care services that are available when I require them
CCC 89/239 37 (31,44)
up to date information Information 56/238 24 (18,29) help to manage concerns about my cancer coming back
Existential Survivorship 54/241 22 (17,28)
information provided in a way that I can understand
Information 50/238 21 (16,27)
information relevant to my family and/or partner
Information 47/238 20 (15,25)
any complaints regarding my care to be properly addressed
CCC 44/238 18 (14,24)
help to manage ongoing side effects and/or complications of treatment
QOL 43/239 18 (13,23)
a CI, 95% Confidence Interval
18
Table 5. Correlations of supportive care needs with psychological distress and HRQOL
Number of Unmet Needs (n=241)
Mean Unmet Need Strength (n=158)
Bivariate Partiala Bivariate Partiala Depression .55*** .56*** .24* .32** Anxiety .49** .49** .25* .30** Stress .45** .46** .28* .34** Physical functioning -.26* -.24* -.21* -.28* Role-physical -.33** -.34** -.25* -.21* Bodily pain -.30** -.29* -.18* -.25* General health -.39** -.38** -.12* -.15* Vitality -.40** -.41** -.24* -.31** Social functioning -.51*** -.50*** -.23* -.27* Role-emotional -.47** -.47** -.27* -.33** Mental health -.53*** -.52*** -.15* -.21* PCS -.21* -.19* -.19* -.22* MCS -.53*** -.52*** -.21* -.26* Consistent with Cohen [22]: * Small/weak correlation (r=.10-.29) ** Medium/moderate correlation (r=.30-.49) *** Large/strong correlation (r≥.50) a Adjusted for the sociodemographic, disease and treatment variables in Table 1
Related Documents






![Isolated Testicular Tuberculosis Mimicking Testicular ... involvement, but testicular involvement is an unusual clinical condition [3]. In this report, a case with isolated testicular](https://static.cupdf.com/doc/110x72/5f3d57bf74280d66ef795ba2/isolated-testicular-tuberculosis-mimicking-testicular-involvement-but-testicular.jpg)




