Fetal and Maternal Medicine Review http://journals.cambridge.org/FMR Additional services for Fetal and Maternal Medicine Review: Email alerts: Click here Subscriptions: Click here Commercial reprints: Click here Terms of use : Click here THE PRENATAL MANAGEMENT OF NEURAL TUBE DEFECTS: TIME FOR A RE-APPRAISAL MASAYUKI ENDO, TIM VAN MIEGHEM, ELISENDA EIXARCH, PAOLO DE COPPI, GUNNAR NAULAERS, FRANK VAN CALENBERGH, LUC DE CATTE, ROLAND DEVLIEGER, LIESBETH LEWI, ALEX EGGINK, KYPROS NICOLAIDES, EDUARDO GRATACOS and JAN DEPREST Fetal and Maternal Medicine Review / Volume 23 / Issue 3-4 / November 2012, pp 158 - 186 DOI: 10.1017/S0965539512000083, Published online: 02 July 2012 Link to this article: http://journals.cambridge.org/abstract_S0965539512000083 How to cite this article: MASAYUKI ENDO, TIM VAN MIEGHEM, ELISENDA EIXARCH, PAOLO DE COPPI, GUNNAR NAULAERS, FRANK VAN CALENBERGH, LUC DE CATTE, ROLAND DEVLIEGER, LIESBETH LEWI, ALEX EGGINK, KYPROS NICOLAIDES, EDUARDO GRATACOS and JAN DEPREST (2012). THE PRENATAL MANAGEMENT OF NEURAL TUBE DEFECTS: TIME FOR A RE- APPRAISAL. Fetal and Maternal Medicine Review, 23, pp 158-186 doi:10.1017/ S0965539512000083 Request Permissions : Click here Downloaded from http://journals.cambridge.org/FMR, IP address: 89.106.234.22 on 11 Dec 2013

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Fetal and Maternal Medicine Reviewhttp://journals.cambridge.org/FMR
Additional services for Fetal and Maternal Medicine Review:
Email alerts: Click hereSubscriptions: Click hereCommercial reprints: Click hereTerms of use : Click here
THE PRENATAL MANAGEMENT OF NEURAL TUBEDEFECTS: TIME FOR A RE-APPRAISAL
MASAYUKI ENDO, TIM VAN MIEGHEM, ELISENDA EIXARCH, PAOLO DE COPPI, GUNNARNAULAERS, FRANK VAN CALENBERGH, LUC DE CATTE, ROLAND DEVLIEGER, LIESBETHLEWI, ALEX EGGINK, KYPROS NICOLAIDES, EDUARDO GRATACOS and JAN DEPREST
Fetal and Maternal Medicine Review / Volume 23 / Issue 3-4 / November 2012, pp 158 - 186DOI: 10.1017/S0965539512000083, Published online: 02 July 2012
Link to this article: http://journals.cambridge.org/abstract_S0965539512000083
How to cite this article:MASAYUKI ENDO, TIM VAN MIEGHEM, ELISENDA EIXARCH, PAOLO DE COPPI, GUNNARNAULAERS, FRANK VAN CALENBERGH, LUC DE CATTE, ROLAND DEVLIEGER, LIESBETHLEWI, ALEX EGGINK, KYPROS NICOLAIDES, EDUARDO GRATACOS and JAN DEPREST(2012). THE PRENATAL MANAGEMENT OF NEURAL TUBE DEFECTS: TIME FOR A RE-APPRAISAL. Fetal and Maternal Medicine Review, 23, pp 158-186 doi:10.1017/S0965539512000083
Request Permissions : Click here
Downloaded from http://journals.cambridge.org/FMR, IP address: 89.106.234.22 on 11 Dec 2013

Fetal and Maternal Medicine Review 2012; 23:3–4 158–186 C© Cambridge University Press 2012doi:10.1017/S0965539512000083 First published online 2 July 2012
THE PRENATAL MANAGEMENT OF NEURAL TUBEDEFECTS: TIME FOR A RE-APPRAISAL
1, 2, 3MASAYUKI ENDO, 1, 3TIM VAN MIEGHEM, 2, 5ELISENDA EIXARCH, 2, 6PAOLO DE COPPI,1GUNNAR NAULAERS, 4FRANK VAN CALENBERGH, 1LUC DE CATTE,1, 2ROLAND DEVLIEGER, 1LIESBETH LEWI, 7ALEX EGGINK, 2, 8KYPROS NICOLAIDES,2, 5EDUARDO GRATACOS AND 1, 2, 3JAN DEPREST
1Division Woman and Child, University Hospital Gasthuisberg, Leuven, Belgium. 2Experimental Programme onPrenatal Management of Neural Tube Defects, Centre for Surgical Technologies, Faculty of Medicine, KULeuven, Leuven, Belgium. 3Laboratory Experimental Gynaecology, Research Unit Fetus Placenta Neonate,Department of Development and Regeneration, Faculty of Medicine, KU Leuven, Leuven, Belgium.4Department of Neurosurgery, University Hospital Gasthuisberg, Leuven, Belgium. 5Department of Obstetricsand Gynaecology, Hospital Clinic-Idibaps, University of Barcelona and CIBER-ER, Barcelona, Spain.6Department of Paediatric Surgery, Great Ormond Street Hospital, London, United Kingdom. 7Department ofObstetrics and Gynaecology, Erasmus Medical Center, University Medical Center Rotterdam, The Netherlandsand representing the Dutch PROSPER consortium. 8Fetal Medicine Unit, King’s College, London, UnitedKingdom.
INTRODUCTION
The prevalence of neural tube defects (NTD) in Europe is around 9 per 10,000 birthsmaking it one of the most frequent congential anomalies affecting the central nervoussystem1. NTD encompass all anomalies that are secondary to failure of closure ofthe neural tube. In this review, we will first summarize the embryology and someepidemiologic aspects related to NTDs. The review focuses on myelomeningocele(MMC), which is the most common distal closure defect. We will describe thesecondary pathologic changes in the central and peripheral nervous system thatappear later on in pregnancy and contribute to the condition’s morbidity. Thepostnatal impact of MMC mainly depends on the upper level of the lesion. In Europe,the vast majority of parents with a fetus with prenatally diagnosed NTDs, includingMMC, opt for termination of pregnancy, as they are apparently perceived as verydebilitating conditions. Animal experiments have shown that prenatal surgery canreverse this sequence. This paved the way for clinical fetal surgery resulting inan apparent improvement in outcome. The results of a recent randomized trialconfirmed better outcomes after fetal repair compared to postnatal repair2; with
Jan Deprest, MD PhD, Clinical Department of Obstetrics and Gynaecology, University Hospitals Leuven,Academic Department of Development and Regeneration, Faculty of Medicine, KU Leuven, Herestraat 49,3000 Leuven, Belgium. [email protected]

The prenatal management of neural tube defects 159
follow up for 30 months. This should prompt fetal medicine specialists to reconsidertheir position towards this condition as well as its prenatal repair. The fetal surgerycentre in Leuven did not have a clinical programme for fetal NTD repair until thepublication of the MOMS trial. In order to offer this procedure safely and effectively,we allied to a high volume centre willing to share its expertise and assist us inthe first procedures. Given the maternal side effects of current open fetal surgicaltechniques, we have intensified our research programmes to explore minimallyinvasive alternatives. Below we will describe how we are implementing this.
EMBRYOLOGY RELATED TO CLOSURE DEFECTS OF THE NEURAL TUBE
The earliest morphologic response to neural induction in the embryonic ectodermis an increase in height of the cells that later will form the central nervous system.Eighteen days after conception these cells emerge as the ‘neural plate’. The plateinitially becomes narrower and longer and neurulation involves the lateral foldingof this plate along a midline neural groove. This acts as an anchoring point aroundwhich the two sides hinge and fold towards each other. Both sides fuse posteriorly andseparate from the overlying ectodermal sheath, to form the neural tube. Closure ofthe neural tube starts 21–22 days after conception in the region of the earliest somitesand then spreads cranially and caudally. The cranial (anterior) and caudal (posterior)neuropore close at 24 and 26 days respectively. By then, the future central nervoussystem looks like a cylinder sealed at both ends. This cylinder is irregularly shapedand will undergo region-specific changes to form what will later be the brain andspinal cord.
The early spinal cord has a central canal and undergoes a segmental arrangement.The exiting nerve roots indicate this segmental organisation. Each level is dividedinto alar and basal plate regions, which correspond to later sensory and motor regions.In the first trimester of pregnancy, the spinal cord extends over the entire length of theembryo. The spinal nerves pass through the intervertebral spaces at the level of theirorigin. Later, the posterior part of the body outgrows the spinal cord and to a lesserextent the vertebral column. Traditionally, it has been assumed that at birth, the spinalcord terminates at lumbar vertebra 3 (L3), and by adulthood at L2. The lumbar and sac-ral spinal nerve roots therefore elongate significantly, causing the appearance of a horsetail or ‘cauda equina’. Below that, the filum terminale connects the end of the spinalcord to the end of the dural sac. In the early fetal period, the primordial meninx is thecondensed mesenchyme around the neural tube and consists of two layers. The thickerouter mesodermal layer forms the dura mater. The thinner inner (pia-arachnoid) layeris of neural crest origin and closely apposed to the neural tissue. It is composedof the pia and arachnoid mater (together referred to as leptomeninges). Within theleptomeninges, fluid filled spaces appear that will coalesce to form the subarachnoidspace. Embryonic cerebrospinal fluid (CSF) is already present from 5 weeks.
Failure of closure of the cranial and caudal neuropores leads to birth defects at thelevel of the brain and the spinal cord, respectively. The best known manifestation of

160 Masayuki Endo et al
Figure 1 A: In spina bifida occulta, the spinal cord and meninges remain in place, and are coveredby soft tissues. Actually the neural arch, the bony coverage is missing, which are normally induced by theroof plate of the neural tube. It is speculated that inductive factors from the neural tube or meninges causethe typical local hair growth; the barrier of the neural arches normally prevent this from happening. Spinabifida aperta is a more pronounced lesion. B: In meningocele, the dura may be locally missing, so thatthe arachnoid layer is bulging beneath the skin. The sac actually contains meninges and cerebrospinal fluid.The spinal cord remains in place though there may be cord abnormalities. C: In myelo-meningocele thespinal cord is bulging through the defect into the subarachnoid space. This causes more displacement andtraction on spinal roots. D: Myeloschisis: the spinal cord is splayed open, with the wall of the central canalconstituting the outer surface.Colour codes: yellow line is dura mater; blue line is the arachnoid membrane, blue shading refers to cerebro-spinal fluid. Drawing by Myrthe Boymans (www.myrtheboymans.nl) for, and copyright by UZ Leuven, Belgium).
failure at the cranial end is anencephaly, but milder variations such as encephalocelesalso exist. This review however focuses on the consequences of failure of closure atthe caudal end. This again includes a range of anomalies that affect the spinal cordcaused by defects in the formation of the bony and soft tissue coverage overlying thespinal cord. The degree of non fusion of the embryonic halves of the vertebral archesmay be quite variable. It can range from a relatively local and closed defect (spinabifida occulta - Figure 1 A) with minimal changes in the spinal cord to an ‘open’lesion. Spina bifida occulta is relatively frequent in the population and often remainsundiagnosed. Of relevance here are more extensive lesions, collectively referred to as

The prenatal management of neural tube defects 161
spina bifida cystica or aperta. Through a bony defect, the meninges and/or spinal cordprotrude as a cyst filled with cerebrospinal fluid.
Meningocele refers to herniation of the meninges through the open vertebral archeswithout obvious herniation of neural tissue (Figure 1B), myelomeningocele (MMC) ischaracterized by extrusion of the meninges and the spinal cord ( = myelum; Figure 1C).Myeloschisis is the most severe form, where the spinal cord itself actually remainsopen, because of failing fusion of the neural folds (Figure 1D).
IN THE PRENATAL PERIOD SPINA BIFIDA IS A PROGRESSIVE DISEASE
The majority of NTD are isolated and considered multifactorial in origin, thoughthe exact aetiology remains unknown. We refer for aetiologic mechanisms to reviewselsewhere28. To explain the subsequent phenotype a two hit hypothesis has beenproposed. The first hit or the primary failure in the closure of the spinal canal early inembryonic life (4th week of gestation) exposes the spinal cord and nerves to directtrauma and neurotoxic agents in the amniotic fluid. These can be considered assecond hits, that progressively damage the developing nervous system. A progressivedestruction of neural tissue has been confirmed by serial prenatal observations andstarts with local ependymal degeneration and subsequent tissue loss at the level ofthe defect from 16 weeks of gestation onwards3–5. Typically, the cord proximal to thedefect remains normal6,7. However, it may be tethered at the site of the defect, leadingto traction on the developing neural tissue8,9.
Effects are both “under” or peripheral to the lesion, as well as “above”, affectingthe brain. Motor and sensory deficits develop beyond the level of the defect, typicallyaffecting the lower limbs in case of thoraco-lumbar lesions. The clinical impact ishighly dependent on the level and extension of the lesion10,11. Whereas local damage tothe spinal cord and peripheral nerves becomes evident at birth, it remains irreversibledespite immediate postnatal surgical repair. In long-term survivors major disabilitiesinclude paralysis, bowel, bladder and sexual dysfunction. The motor deficit leads toprogressive orthopaedic deformities of the spine (scoliosis) and the lower limbs.
Myelomeningocele also induces progressive changes above the level of the lesion.The most important one is the Chiari II malformation, formerly referred to as the“Arnold-Chiari II” or simply CM II. This is the downward displacement of thecerebellar vermis and brain stem into the spinal canal. Moreover, elongation andcompression of the brain stem, compression of the fourth ventricle and downwarddisplacement of the venous sinuses is often seen12. The Chiari malformation mayhave a hydrostatic origin (CSF leakage at the level of the defect, leading to a ‘suctiongradient’)12 and has been invariably described between 19 and 25 weeks of gestation.However, as diagnosis has been shifting to the first trimester, it seems signs arealready present early on. CM II can cause cerebellar, respiratory and cranial nervedysfunction. Moreover the hindbrain herniation impairs normal circulation of CSFthrough the fourth ventricle, leading to secondary hydrocephalus, which in turn

162 Masayuki Endo et al
affects neurocognitive prognosis and late morbidity. Over 80% of children requirelifelong shunting, diverting CSF to the peritoneal cavity. This procedure has wellidentified risks from malfunction and infection, as well as the requirement forreinsertion13. Around 50% of children will have shunt complications in the firstyear of life14. The majority (70%) of children with MMC have an IQ above 80, and halfof them are able to live independent lives15. Parents nevertheless have to be preparedfor a child with a significant need for care. Some health systems offer a wide rangeof resources, but families typically do not receive the full potential benefits16. We donot have recent European estimates of health costs of MMC, but in 2009, life-timemedical costs in the US for a single child with a NTD were 460,923 US$, plus another52,415 US$ for non-medical educational and developmental services17.
PRENATAL DIAGNOSIS AND SCREENING
The ultrasound appearance of the various manifestations of NTD are very specific,but beyond the scope of this paper18. The most important direct clue to MMC is acystic mass protruding from the dorsal vertebral bodies, which show locally splayedossification centres19. Lumbar lesions account for the vast majority of cases, followedby sacral, thoracic and cervical lesions. Spinal abnormalities are usually combinedwith variable secondary signs in the brain. These are often the first anomalies to bepicked up by the ultrasonographer. They include ventriculomegaly, microcephaly, aconcave shape of the frontal calvarium (lemon sign), and obliteration of the cisternamagna with either an apparently “absent” cerebellum or abnormal anterior curvatureof the cerebellar hemispheres (banana sign) (Figure 2)18,20. The lemon sign is presentin about 1% of normal pregnancies and in up to 98% of cases with open spinal defectbefore 24 weeks, and gradually disappears thereafter20. The distortion or absence ofthe cerebellum as part of the CM II is observed in 95% of spina bifida aperta, butdoes not resolve with advancing gestation. Among 6 sonographic diagnostic signs forspina bifida, D’Addario et al21 observed a small cerebellum, a small fossa posteriorand an effaced cisterna magna in respectively 96%, 96% and 93% of cases. Ultrasoundscreening in the second trimester includes those sections of the fetal head in which thecranial signs related to open neural tube defects are clearly visible, resulting in a highdetection rate even in non tertiary care centres22,23. To determine the upper level,landmarks on transverse views of the spine are the most caudal rib (correspondingto T12) and the superior edge of the iliac crest (L5). Such evaluation is best done ata reference centre, as experience and case load are important factors for accuracy.More advanced imaging techniques including 3-D multiplanar, 3-D tomographicultrasound, 4D-volume contrast imaging, and MRI may be useful, especially laterin pregnancy24. (Figure 3)
In the 1980s, the combination of ultrasound and maternal serum �-fetoprotein(MSAFP) around 16 to 18 weeks was introduced to optimize prenatal detection ratein screening programs (reviewed in25). In such programmes, elevated MSAFP led to

The prenatal management of neural tube defects 163
Figure 2 Second trimester ultrasound images.A: Midsagittal view of the lumbosacral area, with the conus medullaris ending at L2–3 in a more ventralposition. B: Pathologic case, with meningolipoma, tethered cord, and conus medullaris now at L4 and ina dorsal position. Note also the raised skin area above the meningolipoma (arrowhead). C: A cystic massprotruding from the lumbo-sacral vertebral bodies on a midsagittal section. D: Transversa section with U-shaped splayed vertebrum, the meningeal sac bulging through the defect, and some nervous tissue protrudingin the sac. E: 3D surface rendered image of the numerous nervous tissue strands emerging from the spinalcanal (arrows). F: Secondary signs in the brain such as ventriculomegaly and the lemon sign.
targeted ultrasound, and amniocentesis for measurement of AFP, acetylcholinesteraselevels and karyotyping. Most European countries have now moved to first trimesterscreening, combining ultrasound measurement of the nuchal translucency (NT),assessment of the nasal bone, blood flow in the ductus venosus, in combination withmaternal serum screening, which is effective in picking up 95% of major aneuplodiesas well as a range of major structural anomalies. These may also include fetal spinalanomalies. From a first trimester screening viewpoint, an easily detectable markerof open spina bifida is localized within the brain in the same mid-sagittal plane ofthe fetal face used for assessment of NT and the nasal bone. In normal fetuses thefourth cerebral ventricle presents as an intracranial translucency (IT) parallel to theNT, while in fetuses with open spina bifida IT may be absent26 (Figure 4). This isbelieved to be due to caudal displacement of the cerebellum, compressing the fourthventricle, hence it is an early manifestation of the CM II. This sign should prompt

164 Masayuki Endo et al
Figure 3 Magnetic Resonance Images: A: Prenatal at 30 weeks in a fetus with sacral meningomyelocoele.B: Same fetus, ventriculomegaly. C: MRI can also be used for postmortem examination, here in a 33 week fetus,demonstrating ventriculomegaly, with heterotopic foci in the ventricular walls, and the Chiari malformation.Courtesy Prof F Claus, medical imaging department.
further investigation of the fetal spine and posterior brain. In the majority of openspina bifida cases there will be an increased diameter of the brain stem, as well asa decrease in the distance between the brain stem and occipital bone27. Prospectivestudies need to evaluate the value of using these first trimester features as a screeningtest for NTD.
EPIDEMIOLOGY OF NTD
The incidence of NTD varies worldwide, with the highest incidences in NorthernChina and Mexico29. Typical risk factors for NTD include previous history of aNTD in a sibling, maternal obesity, poorly controlled diabetes and maternal useof antiepileptic drugs. The true role of ethnicity and socio-economic factors maybe difficult to distinguish, but it is clear that preventive measures play a role3.For instance, folic acid fortification of flour has decreased the incidence of NTDin the USA to 2–3/10,000 live births8,30. The failure to completely abolish NTDs

The prenatal management of neural tube defects 165
Figure 4 Intracranial translucency or 4th ventricle (∗), with choroid plexus of the 4th ventricle (arrows).MO: medulla oblongata, B: brainstem, T: thalamus, and M: midbrain.
demonstrates that other poorly understood factors are also at play. The number of liveborn babies with MMC in the USA totals 1/3,00031.
In Europe, where food is not fortified with folic acid, the prevalence of NTD(9/10.000 births) has not declined substantially over the last decade (Table 1). Thissuggests failure of the preventive policy32. Although care providers are well aware ofthe need for preconceptual folic acid supplementation, the majority of fertile womenare either unaware of it or start supplementation only after a positive pregnancy test,which is too late from an embryologic point of view33. Though fortification has thesupport of most parent support groups contacted in Europe, there remains disbelief ofthe scientific evidence and doubts about safety32,34.
The Eurocat registry systematically records the incidence of birth defects in arepresentative selection of European regions (Table 2), allowing insights into regionaldifferences in incidence. Knowledge of the national screening policy is informativewith respect to the pick-up rates by prenatal ultrasound. Outcome data includeinformation on termination of pregnancy (TOP) rates which are dependent on nationallegal limitations10. Eurocat registration data are typically considered as representativeof wider areas, rather than centres of excellence in that area35. The majority ofEuropean countries in 2004 offered routine prenatal screening ultrasound (one or

166 Masayuki Endo et al
Table 1 Total prevalence (per 10,000 births) of neural tube defects among full member EUROCATregistries in the period 2003–200732,99. Numbers include live births, terminations of pregnancy because ofthe anomaly and still births.
Prevalence of neural tube defectsand subtypes
Prevalence of neural tube defectsand subtypes, after exclusion ofchromosomal anomalies
Category 2003–2007 2005–2009 2003–2007 2005–2009
Neural tube defects 9.4 9.74 9.0 9.35Anencephaly and similar 3.2 3.59 3.1 3.51Encephalocele 1.2 1.17 1.1 1.11Spina bifida 5.1 4.98 4.8 4.74
Table 2 Neural tube defects in Eurocat registries; percentage of prenatally diagnosed cases, mediangestational age at prenatal diagnosis, legislation on termination of pregnancy and percentage of casesundergoing termination of pregnancy. From: Boyd P, et al 35. Eurocat registries are operating in Styria(Austria), Antwerp and Hainaut (Belgium), Zagreb (Croatia), Odense (Denmark), Isle de la Reunionand Paris (France), Saxony-Anhalt (Germany), Dublin (Ireland), Emilia Romagna (Italy), Tuscany (Italy),Malta, N Netherlands (NL), Wielkopolska (Poland), Vaud (Switzerland), East Midlands & South Yorkshire(UK).
Country3Number ofRoutine scans
Prenataldiagnosis (%of total)
Gestational ageat diagnosis(weeks)
Legalterminationgestational agelimit
TOP (% ofprenatallydiagnosed)
Belgium 3 scans 83% 16 None 89%Croatia 3 scans1 80% 12 None 100%Denmark 2 scans 89% 16 None if lethal 88%England – Wales 2 scans 94% 17 None 92%France 3 scans 94% 14 None 98%Germany 3 scans 90% 18 None 44%Italy 3 scans 87% 18 <28 wks 94%Switzerland 2 scans 83% 13 <28 wks 100%Ireland 1 scan2 56% 22 Not legal 0%Malta 2 scans2 25% 19 Not legal 0%Spain 3 scans2 94% 16 <28 wks 98%Netherlands None routine2,3 78% 31 <24 wks 29%
Total 88% 17 88%
[1 Two scans official policy, but 3 usually performed; 2 no national screening policy, but routine screeningoffered; 3at the time of this registration there was neither a national ultrasound screening policy norroutine screening (this has changed since).]
more; Table 2). In those where no such recommendations are present (like Ireland,Spain and Malta), scans and/or MSAFP screening are still routinely performed. In theEurocat registry areas listed in Table 2, 88% of NTD were detected prenatally, at

The prenatal management of neural tube defects 167
a median gestational age of 17 weeks. This led to termination of pregnancy (TOP)in 88% of prenatally diagnosed cases (77% of all cases). Excluding countries wheretermination is illegal, the prenatal diagnosis and termination rate were 91% and 84%,respectively.
One factor potentially important for patients when considering TOP is the gestationat diagnosis. For instance, in the Netherlands the gestational age at diagnosis was31 weeks at that time (the screening policy has subsequently changed). Late diagnosiswas associated with a termination rate of only 29%. It will be interesting to see howsecond, and more recently, first trimester screening and diagnosis change TOP rates.Other factors must influence decision making; in Germany, where prenatal diagnosiswas made at 18 weeks, only 44% of cases underwent termination. The majority ofthe European regions however have relatively high detection and termination rates,reflecting the public’s perception of the morbidity of this condition. This is furtherillustrated by the fact that 7.3% of NTDs undergo late termination; also 11% oflate TOPs are for NTD36. The high termination rates may contribute to the falseperception that NTDs are uncommon, in turn causing lack of political support forfood fortication programs.
Spina bifida, without other anomalies, remains the most frequent NTD in Europewith around 4.8 cases per 10,000 births (between 2005–2009). The numbers varyamong regions, from 2.16 (Portugal) to 11.6/10,000 births (Germany). Of all spinabifida cases registered in the Eurocat registry, 60.5% underwent termination, 2.5%were stillborn, leaving 37% of cases live born. The recurrence risk for MMC is usuallyquoted to be 1.5–3%; with two affected siblings it is 5.7–12%28,37. The presence ofspina bifida occulta in a sibling does not increase the risk for MMC.
BRIEF HISTORY OF EXPERIMENTAL FETAL SURGERY
The combination of an early onset first hit and additional progressive damage (secondhit) to otherwise largely normal neural elements led researchers to consider antenataltherapy. Fetal intervention essentially aims at isolating the defect in a leak proof wayfrom the toxic and traumatic intrauterine environment. The potential of such a fetalintervention is confirmed by an experiment of nature. Indeed, when a spinal columndefect remains covered rather than being an open lesion (as in spina bifida occulta orin the presence of a lipomyelomeningocele), fetuses do not develop the same severesequelae as in open defects38. With the ability to diagnose MMC early and with highaccuracy in the prenatal period, this is an attractive concept if it was shown to beeffective.
Researchers started to explore the potential of fetal surgery by developing animalmodels for NTDs as well as surgical techniques for its repair. Finally, they documentedthe effects of in utero intervention as compared to controls managed after birth.Initial primate models involved the creation of a lumbar defect, which was either leftuntreated or closed primarily39. Fetal surgery avoided the occurrence of cystic lesionsand neurologic deficit, but primary surgery obviously did not mimic the progressive

168 Masayuki Endo et al
in utero acquired changes between occurrence of the defect and an eventual repair.Meuli et al40 at the University of San Francisco in California (UCSF) established alamb model, where MMC was recreated by the microsurgical excision of the skin, theparaspinal mucles, the vertebral arches and the dura mater at level L1-L4 at 75 days ofgestation. The lambs were then returned to the uterine cavity with reestablishment ofthe amniotic fluid volume. At birth these lambs had an MMC-like cystic fluid lesion,complete flaccid sensori-motor paraplegia and were incontinent of stools and urine.They lost normal neural ultrastructure (disruption of neural bundles, cord necrosis,neural tissue loss) distal to the lesion, but not proximally, comparable to what is seenin humans. Somatosensory evoked potentials were absent in the hind limbs, but theyhad normal latency in the forelimbs. Such observations were also made in other lowerspecies, such as pigs, rats and rabbits with MMC-like lesions41–46. In a second step,lambs with a surgically induced MMC underwent secondary repair 25 days after theinitial lesion was created (day 100 of pregnancy) by reversed latissimus dorsi muscleflap and skin coverage. This resulted in near normal motor function, intact sensationand urinary and stool continence after term caesarean section47,48. On histology thespinal cord, nerve roots and spinal ganglia appeared nearly normal. The teams in SanFrancisco and Philadelphia also showed that the CM II was reversed by intra-uterineclosure49,50. These experiments laid the experimental basis for fetal surgery for MMC,as they demonstrated that exposure to the intra-uterine environment reproducedsimilar damage as seen in clinical cases, and that prenatal closure preserved neurologicfunction and structural integrity. Animal experimental evidence of a fetal surgicalprocedure was and still is an absolute prerequisite prior to embarking on humanclinical trials51,52.
FIRST FETAL SURGERY FOR A NON-LIFE-THREATENING ANOMALY
Although MMC is associated with significant and irreversible morbidity, thecondition is not lethal in the vast majority of cases. Contemplating fetal surgeryonly to prevent morbidity rather than mortality would be a paradigm shift for thefetal surgical community53. Indeed, any potential fetal benefit could be outweighedby procedure related complications in an otherwise healthy mother. At the moment ofstarting these clinical programmes, the experience with open fetal surgery had alreadyshown that there were inherent maternal side effects of tocolysis, haemorrhage andobstetrical consequences of hysterotomy and membrane rupture, as well as fetal risks(mainly prematurity)54,55. Given these risks, it would seem acceptable only to targetthe fetuses with NTD that have the worst prognosis, yet who could still benefitfrom a prenatal intervention. Fetuses without obvious established damage, e.g. thosewith CM II and hence at the highest risk for posterior fossa symptoms and laterhydrocephaly, would therefore seem logical fetal surgery candidates.
At that time operative fetoscopy was booming, mainly to treat complicationsof monochorionic twins51. It was believed that minimally invasive access to thefetus would overcome most, if not all of the risks of open surgery56,57. Several

The prenatal management of neural tube defects 169
Figure 5 Artist impression of a fetoscopic myelomeningocele repair using multiple ports by percutaneousaccess. Initially the fetoscopic procedure was described via laparotomy by Bruner et al in 199961
and Farmer et al.62 Fetoscopic repair is still practised by Kohl et al63. Drawing by Myrthe Boymans(www.myrtheboymans.nl) for and copyright by UZ Leuven, Belgium.
teams demonstrated the feasibility of very complex fetoscopic procedures involvingdissection, suturing and ligation58–60. This might be one of the reasons why endoscopiccoverage of MMC after maternal laparotomy, was attempted, first by Bruner et albetween 1994 and 1997 (Figure 5)61. Unfortunately, two out of four fetuses died duringor following an operation under carbon dioxide insufflation. Farmer et al62 from SanFrancisco also reported one out of three successful attempts of fetoscopic coverage ofthe defect using an Alloderm (LifeCell Corporation, Branchburg, NJ) patch. Despite asuccessful antenatal intervention, that baby still required a standard repair because ofpatch release and ended up with a VP-shunt. The other two attempts failed technically,leading to demise of one fetus, and standard postnatal surgery and VP-shunting in theother. In Europe, the group in Bonn had a comparable experience, which was onlyrecently independently reported in detail63,64. Of 19 fetoscopic procedures performedbetween 20 and 25 weeks, 3 procedures were abandoned and 3 fetuses or neonateseventually died. This left 13 (68%) fetuses that were successfully operated on andsurvived, who were matched for the level of lesion and same gestational age topostnatal repairs. In summary, the complication rate was higher in the fetal surgerygroup (membrane rupture, olighydramnios, chorioamnionitis), the gestational age atdelivery earlier (32 vs. 39 weeks, respectively, p = 0.001), leading to a higher chance forrespiratory distress syndrome. In concordance with observations after open surgery,the neurologic outcome after fetoscopic surgery was better (two gained segments,better preserved knee-jerk and anal reflexes). Despite proving the benefit of fetal

170 Masayuki Endo et al
intervention, the authors concluded that the currently observed complications mustbe addressed before considering fetoscopic surgery as a clinical alternative for MMC64.
OPEN FETAL SURGERY EXPERIENCE ON PATIENTS OPERATED PRIOR TO THE MOMS TRIAL
In the USA, teams converted to an open approach. Adzick et al65 from The Children’sHospital of Philadelphia (CHOP) first reported a successful open repair in 1998. Brunerfrom Vanderbilt (Nashville, Tennessee) compared his first open cases to the earlierendoscopic ones, and concluded that open surgery was superior66. A working partyat the National Institutes of Health had meanwhile identified in total 27 reports onclinical procedures, with variable degrees of overlap67. The largest experience camefrom two groups. The group from CHOP reported on 50 selected patients, operatedbetween 20 and 25 completed weeks of gestation68,69. The indications and outcomesare displayed in Table 3. None of the fetal surgeries failed and the overall survivalrate was 94% (there were 3 prematurity related deaths). On follow up there was adramatic improvement in hindbrain herniation prior to birth, and postnatal neurologicoutcome compared to historical controls65,68,70,71. The need for VP-shunting washalved, for all levels of lesions (43% vs. 84%). Over half (57%) of fetuses withthoracic or lumbar lesions demonstrated better leg function than would have beenexpected for the anatomical level of the defect, although 17% had worse than expectedfunction. The Vanderbilt group initially operated on 29 patients between 24 and 30weeks, and by 2005 they reported a total of 178 patients (Table 3)70,72. In a matchedcontrol study, the rates of short term prematurity-related complications were identicalto the complications of premature infants born early for reasons other than fetalsurgery73.
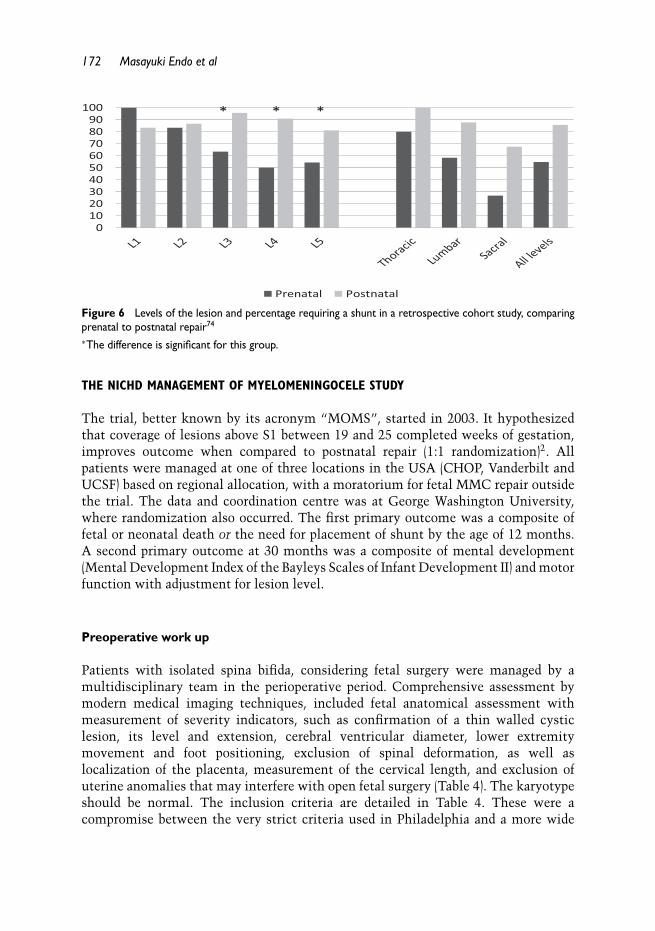
In preparation for a nationwide trial, these 2 centres designed a retrospective cohortstudy, with 104 fetal and 189 postnatal repairs, in which they obtained follow-up formore than a year. Cases were stratified according to the level of the lesion and thegestational age at surgery. Again, shunt dependent-hydrocephalus was reduced afterfetal repair, at least for fetuses with lesions below L2 (Figure 6)74. Conversely, lesionshigher than L3 did not appear to benefit from fetal surgery. The effect of fetal repairwas better when repair was done prior to or at 25 weeks, rather than later75.
The above findings were in part the basis for the design of a randomized trialcomparing prenatal to postnatal repair. During that trial there was a voluntarymoratorium on open fetal surgery outside the trial. During that period, longer termfollow up studies were carried out and an agreement was sought on standardization oflong term outcome measures. In a 2-year follow up report on 30 prenatally operatedchildren, the presence of a VP-shunt was correlated with a significant decrease in alltesting scores. The lower shunt rate after fetal repair, together with a better outcomewithout a shunt more likely resulted in normal cognitive development68. Danzeret al76,77 recently reported the 5-year follow up of children at CHOP. Their meanverbal intelligence, performance intelligence and full intelligence quotient were in thenormal population range. High or average scores for these were found in 90% or more,

The prenatal management of neural tube defects 171
Table 3 A comparison of indications for fetal surgery, obstetrical and short-term outcomes in two series(adapted from 51). Criteria for intervention were based on information from available papers from the samesurgical teams.
CHOP68 Vanderbilt72
(n = 50) (n = 178)
Inclusion criteria Between 20+0 and 25+6 weeks Varied over time – initially <30weeks80
Normal fetal karyotype Normal fetal karyotypeAbsence of other congenital
anomaliesAbsence of other major congenital
anomaliesLesion S1 and higher Not specified; all cases were S1 and
higherLateral ventricular size ≤17 mm Lateral ventricular diameter ≥ 10
mm66
Severe (grade III) Chiari IImalformation
Chiari II malformation66
Sonographic evidence of normalmovement of both lowerextremities without talipes
Establishment of lower legmovement not required.
ResultsGestation at surgery (wks) 23+ 0 (20+0–25+4) (19–30); later <26 wksGestation at delivery (wks) 34+4 (25+4–37)∗ 33+5 (25–38)Postnatal shunt (postnatal age) 46% (21 wks) 46% (12 wks)Perinatal losses 3/51 (5.8%; due to prematurity) 5/178 (2.8%; causes not specified)Length of hospital stay 4 days 3.3 days (3–7)Oligohydramnios Not specified 25 % early on
30 % readmission rateDelivery <30 wks 5/47 (10.6 %)∗∗ 11.8 %Delivery >32 wks 40/47 (85 %)∗∗ Not specifiedMaternal complications None reported; one amniotic fluid
leak through the hysterotomy scar9 (5.1 %) mild pulmonary oedema1 bowel obstruction4 (2.2%) dehiscence,asymptomatic in 3
∗: includes all patients; ∗∗denominator is survivors only.
and in 60 % for processing speed. Un-shunted children had better full intelligencequotient and processing speed than those requiring a shunt. Their functional statusregarding self-care, mobility and cognitive independence was lower than normal age-matched controls. Complete independency was achieved by 84% (cognition), 38% (selfcare), 62% (mobility), and 58% total functional outcome. Again outcomes were betterwhen no shunt was required76,77. The majority of children achieve neurocognitiveand neurofunctional independence. Nearly one third however continue to requiremaximal assistance when carrying out self-care tasks. Functional studies confirmedprevious findings by other centres that showed only minimal impact of prenatal MMCsurgery on continence function78,79.
172 Masayuki Endo et al
0102030405060708090
100
Prenatal Postnatal
* * *
Figure 6 Levels of the lesion and percentage requiring a shunt in a retrospective cohort study, comparingprenatal to postnatal repair74
∗The difference is significant for this group.
THE NICHD MANAGEMENT OF MYELOMENINGOCELE STUDY
The trial, better known by its acronym “MOMS”, started in 2003. It hypothesizedthat coverage of lesions above S1 between 19 and 25 completed weeks of gestation,improves outcome when compared to postnatal repair (1:1 randomization)2. Allpatients were managed at one of three locations in the USA (CHOP, Vanderbilt andUCSF) based on regional allocation, with a moratorium for fetal MMC repair outsidethe trial. The data and coordination centre was at George Washington University,where randomization also occurred. The first primary outcome was a composite offetal or neonatal death or the need for placement of shunt by the age of 12 months.A second primary outcome at 30 months was a composite of mental development(Mental Development Index of the Bayleys Scales of Infant Development II) and motorfunction with adjustment for lesion level.
Preoperative work up
Patients with isolated spina bifida, considering fetal surgery were managed by amultidisciplinary team in the perioperative period. Comprehensive assessment bymodern medical imaging techniques, included fetal anatomical assessment withmeasurement of severity indicators, such as confirmation of a thin walled cysticlesion, its level and extension, cerebral ventricular diameter, lower extremitymovement and foot positioning, exclusion of spinal deformation, as well aslocalization of the placenta, measurement of the cervical length, and exclusion ofuterine anomalies that may interfere with open fetal surgery (Table 4). The karyotypeshould be normal. The inclusion criteria are detailed in Table 4. These were acompromise between the very strict criteria used in Philadelphia and a more wide

The prenatal management of neural tube defects 173
Table 4 Inclusion and exclusion criteria for patients participating in the MOMS trial2.
Inclusion criteria• Maternal age ≥18y• Gestational age at randomization 19wks, 0d–25wks, 6d• Normal karyotype• S1-level lesion or higher• Confirmed CM type II malformation on prenatal ultrasound and magnetic resonance imaging
Exclusion criteria• Multiple pregnancy• Insulin-dependent pregestational diabetes• Additional fetal anomalies unrelated to MMC• Fetal kyphosis ≥30 degrees• History of incompetent cervix and /or short cervix <20mm by ultrasound scan• Placenta praevia• Other serious maternal medical condition• Obesity defined by body mass index of ≥35• Previous spontaneous singleton delivery <37wks gestation• Maternal–fetal Rh iso-immunization• Positive maternal human immunodeficiency virus or hepatitis B or known hepatitis C positivity• No support person to stay with the pregnant women at the centre• Uterine anomaly• Psychosocial limitations• Inability to comply with travel and follow-up protocols
approach used at Vanderbilt72,80. Both the anesthesiologist and the maternal-fetalmedicine specialists screened for physical maternal risks55,81. The results of thefetal assessment and its prognosis were then discussed with the family, as wellas the potential benefits and disadvantages of fetal surgery and the alternativeoptions. The well defined maternal risks were discussed, such as the side effectsof tocolysis, including the risk of pulmonary oedema, abruptio, uterine rupture, longhospitalization, as well as the need for future caesarean delivery, prior to obtaininginformed consent.
Surgical procedure
The following standardized procedure was agreed on for the MOMS trial, furtherdetailed in the on-line available additional material2. Prior to the operation, cefazolin(1000 mg I.V.) and indomethacin (50 mg rectal or PO) were administered. Maternalgeneral inhalational deep anaesthaesia and epidural anesthaesia provided adequatefetal anesthaesia and uterine relaxation for fetal surgery. In the postoperative phaseanalgesics were continued through the epidural catheter. A wide range of maternalmonitoring techniques were used81. A low transverse maternal laparotomy wasperformed to expose the uterus. In case of an anterior placenta, the muscle layerswere split so that the uterus could be exteriorized. Rarely a vertical skin incision

174 Masayuki Endo et al
Figure 7 Schematic drawing of open fetal surgical repair of a myelomeningocele. Drawing by MyrtheBoymans (www.myrtheboymans.nl) for and copyright by UZ Leuven, Belgium
was used in patients with a BMI>30. The hysterotomy was at least 6 cm awayfrom the placental edge. Intraoperative ultrasound determined the fetal and placentallocation (Figure 7). The fetus was manually positioned such that the MMC sac wasin the centre of the future hysterotomy. Two monofilamentary traction sutures werepassed under ultrasound guidance through the uterine wall and membranes. Withelectrocautery the myometrial layers were split and the cavity opened. A purposedesigned uterine stapling device, loaded with absorbable polyglycolic acid staples(Covidien Auto Suture, Norwalk CT) was used. This may be facilitated by a spear-like device, that snaps onto the lower limb of the uterine stapler. Prior to stapling,the operator excludes the incorporation of fetal elements or the cord by palpationand ultrasound. Two or more staplers were used to create a 6–8 cm uterine incision,large enough to expose the fetal myelomeningocele. In order to minimize the risks ofplacental separation, uterine contractions and expulsion of the fetus, warm Ringer’slactate was continuously infused into the cavity via a “level I” rapid infusion device(H-1200, Fast Flow Fluid Warmer, Smiths Medical ASD Incorporated, St. Paul, Minn.,USA). During the entire operation, the fetal heart rate and ventricular function werecontinuously monitored by fetal echocardiography. This was done by a fetal medicinespecialist or echocardiographer not involved in the actual surgery. The fetus was givenan intramuscular injection of fentanyl (20 mcg/kg) and vecuronium (0.2mg/kg) prior

The prenatal management of neural tube defects 175
to starting surgery. The actual MMC repair was not different from a postnatal repair.The neural placode was sharply dissected from surrounding tissue and allowed todrop back into the spinal canal. The dura was subsequently identified, reflected overthe placode and closed using a fine running suture. If there was insufficient dura forclosure, Duragen (Integra Life Sciences Corporation, Plainsboro, NJ) was used as asubstitute. Finally, skin flaps are mobilized and closed to complete the watertightMMC closure. If it was not possible to obtain skin closure, relaxing incisions weremade or Alloderm (Life Cell) was used. The uterus was closed in two layers, the firstone incorporating the absorbable staples and uterine membranes. As the last stitchesof this layer were being placed, warmed Ringer’s lactate, mixed with 2 g of oxacillinor 900 mg of clindamycin, was added to the uterus until the amniotic fluid indexappeared normal under ultrasound. A second imbricating layer of suture was tied.At uterine closure, intravenous magnesium sulfate was started, to be continued for24 hours thereafter. To help achieve a watertight hysterotomy closure, the uterinewound was covered with an omental patch. Finally, the abdominal wall was closedin layers. Postoperative medication included pain relief and cefazolin. Prophylactictocolytics included initial magnesium sulfate (24 hours), indomethacin (50 mg PR orPO 6 hourly, for 24 hours, then 25 mg 6 hourly for a total of 48 hours), with dailymonitoring of the ductus arteriosus. Maintenance tocolysis by oral nifedipine (10–20mg every 4–6 h) was initiated after discontinuiation of the magnesium until 37 weeks.Whenever needed, therapeutic tocolysis with magnesium sulfate and/or indomethacinwere considered. Patients remained in hospital for around 4 postoperative days,followed by modified bed rest for 2 weeks. Follow up visits included weekly ultrasoundassessment, which documented the amniotic fluid volume, the fetal membranes, thecervix, and biophysical profile. In the absence of problems, elective caesarean deliveryby lower uterine incision at 37 weeks was planned.
Trial results
In December 2010 the trial was concluded at a planned interim analysis of 183 outof the 200 anticipated patients because of efficacy2. The results are summarized inTable 5. In line with earlier clinical trials, fetal surgery improved MMC related infantoutcomes. The first primary outcome (death or need for shunt) occurred in 68% ofthe infants in the prenatal surgery group and in 98% of those postnatal surgery group(n = 158). Actual rates of shunt placement were 40% in the prenatal surgery group and82% in the postnatal surgery group. Prenatal surgery also resulted in improvement inthe composite score for mental development and motor function at 30 months (n =64; p = 0.007). On closer inspection, mental development score was not different, butthere was a marked improvement in motor function. There were also improvementsin several secondary outcomes, including hindbrain herniation by 12 months andambulation by 30 months (42% of patients could walk independently after fetalsurgery as compared to 21% after postnatal repair; p = 0.01). By serendipity, the

176 Masayuki Endo et al
Table 5 Summary of results of the MOMS trial (from Adzick et al2).
Prenatal Surgery Postnatal Surgery RR (CI) – p value
Pregnancies/fetuses 78 80Fetal profileGestational age at randomization 23.6 ± 1.4 23.9 ± 1.3Thoracic 4 (5%) 3 (4%)L1-L2 21 (27%) 10 (12%)L3-L4 30 (38%) 45 (56%)L5–S1 23 (29%) 22 (28%)
Maternal ComplicationsPulmonary edema 5 (6%) 0 (0%) P = 0.03Abruptio 5 (6%) 0 (0%) P = 0.03Chorioamnionitis 2 (3%) 0Dehiscence at hysterotomy site 8/76 (10%) 0 (0%)Haemorrhage requiring transfusion 7 (9%) 1 (1%) 7.18 (0.90–57.01) p = 0.03
Fetal/Neonatal outcomesOligohydramnios 16/78 (21%) 3/80 (4%) 5.47 (1.66–18.04) p = 0.001Chorioamniotic membraneseparation
20/78 (26%) 0/80 (0%) p < 0.001
Gestation at delivery (wks) 34.1 ± 3.1 37.3 ± 1.1 p < 0.001Spontaneous membrane rupture 46% 8% 6.15 (2.75–13.78) p < 0.001Delivery < 30 wks 10/78(13 %) 0/80 (0 %)Delivery >30 wks 68/78(87 %) 80/80 (100 %)Birth weight (gr) 2383 ± 688 3039 ± 469 P < 0.001Foot deformity 39/78 (50%) 36/80 (45%) 1.11 (0.80–1.54) p = 0.53Perinatal losses 2/78 (3%) 2/80 (2%) 1.03 (0.14–7.10) p = 1.00
Infant outcomes at 12 months 78 80Primary outcome 53 (68%) 78 (98%) 0.7 (0.58–0.84) p < 0.001Actual placement of shunt 31/78 (40%) 66/80 (82%) 0.48 (0.36–0.64) p < 0.001Any hindbrain herniation 45/70 (64%) 66/69 (96%) 0.67 (0.56–0.81) p < 0.001Surgery for tethered cord 6/77 (8) 1/80 (1) 6.15 (0.76–50.00) p = 0.06Chiari decompression surgery 1/77 (1) 4/80 (5) 0.26 (0.03–2.24) p = 0.37
Outcome of Children at30 months
64 70
Primary outcome score 148.6 ± 57.5 122.6 ± 57.2 0.007 P = 0.007Bayley Mental Development Index† 89.7 ± 14.0 87.3 ± 18.4 P = 0.53Difference between motor functionand anatomical levels‡
0.58 ± 1.94 -0.69 ± 1.99 P = 0.001
>Two levels better 20/62 (32%) 8/67 (12%)One level better 7/62 (11%) 6/67 (11%)No difference 14/62 (23%) 17/67 (25%)One level worse 13/62 (21%) 17/67 (25%)> Two levels worse 8/62 (13%) 19/67 (28%)
Walking independently onexamination
26/62 (42%) 14/67 (21%) 2.01 (1.16–3.48) p = 0.01

The prenatal management of neural tube defects 177
Table 5 Continued.
Prenatal Surgery Postnatal Surgery RR (CI) – p value
Walking status 0.03None 18/62 (29%) 29/67 (43%)Walking with orthotics or devices 18/62 (29%) 24/67 (36%)Walking without orthotics 26/62 (42%) 14/67 (21%)
WeeFIM score¥Self-care 20.5 ± 4.2 19.0 ± 4.2 p = 0.02Mobility 19.9 ± 6.4 16.5 ± 5.9 p = 0.003Cognitive 23.9 ± 5.2 24.1 ± 5.9 P = 0.67
†On the Bayley Scales of Infant Development II, the Mental Development Index and the PsychomotorDevelopment Index are both scaled to have a population mean (±SD) of 100 ± 15, with a minimum scoreof 50 and a maximum score 150. Higher scores indicate better performance. ‡ For the difference betweenthe motor function level and the anatomical level, positive values indicate function that is better thanexpected on the basis of the anatomical level. ¥ On the WeeFIM evaluation, the score on the self-caremeasurement ranges from 8 to 56, and scores on the mobility and cognitive measurements range from 5to 35, with higher scores indicating greater independence.
lesion level in the prenatal repair group was more severe than in the postnatal group(p = 0.02), which makes the results even more remarkable.
In essence fetal surgery resulted in a level of function that is two or more levelsbetter than what would be expected based on the anatomical lesion. These differencesare not only statistically significant but also clinically relevant82. Overall childrenborn after fetal surgery were less likely to have hindbrain herniation, and if theyhad, it was milder. Their need for surgical interventions after (fetal) coverage ofthe MMC was also lower, including decreased needs for VP-shunt insertion andrelease of tethered cord. The trial observations are consistent with earlier findingsin observational studies and are thus very likely to be constant. Though long termfollow up is not available yet, it is reasonable to hope for a durable outcome, as wasearlier demonstrated in observational studies. The follow up of the children fromthis study has started. MOMS II is funding an evaluation of trial children at ages5–9 years, hypothesizing that prenatal repair improves adaptive behaviour. Secondaryoutcomes of this study will be motor function, cognitive function, brain morphologyand function as determined by MRI, medical outcomes, quality of life, as well asmaternal reproductive functioning.
The procedure however comes at a price. There were two fetal deaths in the prenataltreatment group, one during surgery, the other due to prematurity. In a way, this wasbalanced in the postnatal surgery group by two additional deaths (RR: 1.03), whichwere due to the consequences of CM II. Delivery after fetal surgery took place ata mean of 34.1 weeks versus 37.3 weeks (p < 0.001) in the postnatal repair group,including 13% of deliveries <30 weeks versus none in controls.
There were also clinically relevant maternal complications and side effects.These included pulmonary oedema (6%; associated with aggressive tocolysis), and

178 Masayuki Endo et al
placental abruption. There were haemorrhagic complications at birth, requiring bloodtransfusion (9%). There were several prolonged hospitalizations and/or readmissionsfor oligohydramnios (21% vs. 4%; p = 0.001), membrane rupture (46% vs 0%;p < 0.001) and preterm delivery (79 % vs 15%; p < 0.001)83. One in three womenundergoing fetal surgery also had an area of thinning or dehiscence of the uterine scarat the time of caesarean delivery, although none of these women formally presentedwith clinically ruptured uterus. The presences of uterine dehiscence may have an (asyet undefined and quantified) effect both on the index as well as future pregnancies55
These complications are all unique to the fetal surgery group. They are seriouslimitations to the acceptability of fetal surgery, certainly in mothers consideringsubsequent pregnancies.
IMPLEMENTATION IN EUROPE
For us, the question therefore is not whether but how and how often one will offerprenatal repair in clinical practice. One potential limitation to a prompt uptake inEurope, is that the numbers will be relatively low, given the higher overall terminationrates. Based on the very high termination rates, it seems that the perception inEurope that MMC is a very morbid anomaly. Though outcome is improved byfetal intervention, the disease is not necessarily cured. When counseling parentsconsidering fetal surgery, the semantics are therefore very important. The MOMStrial has shown that outcomes are better following fetal surgery. However at the sametime, 26% of antenatal operated babies continue to have mild to moderate mentalretardation (mental developmental index less than 85). Also, 58 % of the children willnot be able to walk without help at 30 months. Yet this is significantly better thanafter postnatal repair, which will result in a 33% chance of a mental developmentalindex < 85 and a 79% chance of not being able to walk without help at 30 months. Asthe current fetal surgical technique does not cure the disease entirely, it seems fair tocounsel parents specifying the results using the percentages both ways (success andfailure rates) and leave all options open.
Another potential obstacle is that both patients and fetal medicine specialists arerelatively unfamiliar with open fetal surgery. In contrast, fetoscopy is widely accepted,but the data show that fetoscopic coverage of MMC at present does not yield similaroutcomes. Fetoscopic coverage is associated with a high number of complications andtechnical failures, though still improving outcome64. For us, the logical consequenceis therefore that fetal surgery should now be offered by open surgery, exactly asdescribed in the randomized trial. Traditionally, open fetal surgery per se has notbeen embraced in Europe. This may well be more a reflection of a physician’s attitudethan the patient’s perception of open fetal surgery51. We think this attitude shouldnow be reconsidered. Available data (Table 6) actually demonstrate that ruptureand preterm delivery rates after open fetal surgery are at least comparable to thosereported with what is obtained by fetoscopy in singletons in the early second half of

The prenatal management of neural tube defects 179
Table 6 A comparison of selected outcome variables in larger clinical series on fetoscopic endoluminaltracheal occlusion (FETO) for severe congenital diaphragmatic hernia99, or on fetoscopic MMC coverage orrepair as well as open MMC repair2. For fetoscopic MMC repair, most of the data (n = 16) come from adetailed report (n = 16)100, unless specified. In that case the outcome variable could only be identified in alarger (n = 19) independent neurologic outcome report64.Notes and abbreviations: n.s. = not specified; 1 defined as the ability to complete the surgery as plannedat first attempt; 2 death around the time of surgery or as a result of it; 3 FETO involves an elective secondinvasive procedure around 34 weeks in 75% of cases. In another series without this second intervention,however, the gestational age at delivery was similar (35.6 (28–38) weeks)101; 4 cumulative; 5 at randomization;6
is a number at first attempt, when including a second attempt it is 209/210.
Fetoscopic endoluminaltracheal occlusion99 Fetoscopic MMC repair64,100 Open MMC repair2
N 210 16 78Anaesthesia Regional or local General anaesthesia General anaesthesiaAccess Percutaneous Percutaneous LaparotomyAccess diameter (mm) 3.3 mm 3 – 5.0 mm HysterotomyGestational age at
intervention (wks)27.1 (23.0–33.3) 24.0 (22–28) 23.6 ± 1.4 5
Operation time (min) 10 (3–93) 231 (50–480) n.s.Success rate1 203/210 (96.7%)6 8/16 (50%) n.s.Intra-operative
haemorrhagiccomplications
1/210 (0.5%) 4/16 (25%) n.s.
Perioperative death rate2 1/210 (0.5%) 2/16 (12.5%) 2/78 (2.6%)Chorioamnionitis 5/210 (2.4%) 3/13 (23.1%) 2/78 (3%)Oligohydramnios n.s. 9/16 (56%) 16/78 (21%)PPROM 99 (47.1%) 11/1364 36/78 (46%)Delivery prior to 30 weeks 13% (<32 wks) 9/16 (56%) 10/78 (13%)Delivery prior to 34
weeks465 (30.9%) 16/16 (100%) 36/78 (46%)
Gestational age at birth 35.3 wks (25.7–41.0)3 28 8 (21–33) 34.1 ± 3.1 wks (n.r.)
pregnancy. The best studied procedure in that respect is that for severe congenitaldiaphragmatic hernia, which also carries a significant risk for preterm delivery andpreterm membrane rupture.
We have therefore argued to “put open fetal surgery back on the European agenda”51.To our knowledge only a few European centres offer open surgical MMC-repair, withfew or no data being published in the peer reviewed literature84. Most fetal surgerycentres actually limit themselves to open procedures performed on placental support(EXIT procedure). Doing this may provide a certain basis of experience, includingthe use of inhalational anaesthesia for maximal uterine relaxation, gaining safe andeffective access to the uterus and keeping uteroplacental blood flow and gas exchangeadequate. Obviously this particular operation at mid gestation is very different,and training will be required. As for any other complex surgical technique, onecannot expect to have similar outcomes from the beginning85. The reported surgical

180 Masayuki Endo et al
technique and outcomes are the result of years of experience, careful standardizationand stringent case selection. The voluntary moratorium precluded other US centresfrom offering this procedure during the trial. Therefore other North-American centres,as well as most centres elsewhere, will have to be trained for what is to most a newprocedure. There are at present no guidelines, no consensus on which fetal surgicalprocedures should be offered regionally, nor how training should be structured andevaluated86. An NIH panel has published a white paper on this, and will soon comeout with recommendations for the expertise and experience required. In the absenceof criteria or recommendations, we, being a referral centre for congenital anomaliesincluding MMC, have decided to train our team in a model already in use in theUSA67. It consists of a mix of “in-house training”, whereby experienced physiciansinvite experts to learn from them, and, to a larger extent, “exported training”, wherebyour team travel to expert centres to train physicians and staff. We also have returnvisits to assist in the first experience. The fact that we have a high-volume fetal surgeryprogram, with an interdisciplinary board and team, offering a variety of procedures(including EXIT experience), as well as having a large experimental program, shouldreduce the learning curve. Regional availability of fetal MMC surgery in selectedEuropean centres will accommodate the impracticality and financial hurdles ofintercontinental travel for patients. We have discussed our plans with other regionalsocieties, so that turnover is sufficient to maintain proficiency both in evaluation andin fetal surgery.
OTHER LESSONS FROM FETAL SURGERY EXPERIENCE
Although there is a measurable and relevant benefit of fetal surgery, it is clear thatfetal surgery does not cure MMC82,85. There are significant morbidities in survivors,such as a substantial need for shunting with all its consequences and not all subjectsbenefit from the same degree of neuromotor improvement. It is conceivable that thecurrent technique, timing and/or selection criteria are not optimal85.
Selection criteria
The in utero effects are not identical for each case. For instance a number of fetusesdo not display reversal of hindbrain herniation. Future follow up studies may identifyprenatal predictors of inappropriate or poor response, such as extent of the lesion,ventricular diameter or limb function. One will however always have to accept thatthe response will be to a certain extent individual, i.e. that same severity fetuseswill not ultimately have the same outcome. It is therefore very difficult to use moregeneral prenatal predictors in the individual case. For instance, most studies pointto a level dependent outcome, though spectacular outcomes have been observed inindividual cases with very extensive lesions.

The prenatal management of neural tube defects 181
Technique
Technical limitations are obvious. First there is the need for laparotomy, whichby itself may cause fetal side effects. As mentioned, conversion to fetoscopy doesnot yield comparable postnatal outcomes. The present limitations of fetoscopy (e.g.operating times, membrane rupture and prematurity, feasibility and incompletenessof the surgery, need for multiple trocars) may ultimately be overcome by additionalexperimental work, technologic advancement and/or experience. A dramaticimprovement may come from a different technique of coverage, as already suggestedby several experiments87,88.
Timing
A trend for poorer outcomes with very late repairs is suggested80. Indeed, the defectis an embryologic one, which may of itself either be partly irreversible, or, by thetime repair is (currently) done, has already caused irreversible damage to the centralnervous system or peripheral nerves. Spina bifida will increasingly be diagnosed inthe first trimester, but very early repairs will call for alternative technical solutions,as the current surgical procedure is barely realistic on the frail tissues present duringthe first half of pregnancy89,90. Therefore rather than dissection of the neural placodeand layered suturing of the defect, it could be replaced by temporary effective sealingof the defect and surgical repair after birth91–95. Sealants could also serve as a matrixand/or carrier for factors that stimulate epidermal growth and neovascularization.The proof of principle of such a tissue engineered approach was demonstrated by theteam at CHOP, using a rodent model with retinoic acid induced fetal MMC90,96.
This, and other programmes97 are currently exploring the limits of what can bedone surgically for this disease. Extensive animal experience and good experimentalresults should be obtained to avoid premature implementation into clinical practice.Meanwhile, the standard of prenatal surgery at this moment remains open repair. Anyinnovative technique and protocol will have to be evaluated in a proper clinical trial,preferentially with a head-to-head comparison to the standard open technique in thehands of experienced operators.
Acknowledgements
We are greatly indebted to the Fetal Diagnosis and Treatment Center of the Children’sHospital of Philadelphia, PA (USA), for the research collaboration as well as exchangeprogramme supporting both teams in novel fetal surgical procedures (NS Adzick,A Flake, M Johnson, H Hedrick). ME and EE are beneficients of a Marie CurieIndustria-Academia Partnership and Pathways grant sponsored by the EuropeanCommission (251356). JPD and RDV are beneficients from a fundamental clinicalresearch grant of the Fonds Wetenschappelijk Onderzoek Vlaanderen (1.8.012.07.N.02

182 Masayuki Endo et al
resp. 1803311N) and LDC from the “Klinische Opleidings- en Onderzoeks- Raad” ofthe University Hospitals Leuven. The experimental programme of the Leuven group issupported by the Flemish Instituut voor Wetenschap en Technologie (IWT/ 07/0715),as well as from the European Commission within the 6th Framework programmefor tissue engineering research for congenital birth defects (LSHC-CT-2006–037409;www.eurostec.eu). The latter in particular funds the experimental research of AE,EG, KN and JD. PROSPER is the Dutch consortium on prenatal management ofspina bifida. We thank L Pistorius, R Gooskens (Utrecht), R de Jong (Rotterdam), DSival (Utrecht), M Willemsen (Nijmegen), D Oepkes, C Peeters-Scholte and F Walther(Leiden) for setting up the PROSPER consortium.
REFERENCES
1 Garne E, Dolk H, Loane M, Boyd PA. EUROCAT website data on prenatal detection rates of congenitalanomalies. J Med Screening 2010; 17: 97–98.
2 Adzick NS, Thom EA, Spong CY, Brock JW, 3rd, Burrows PK, Johnson MP et al. A randomized trial ofprenatal versus postnatal repair of myelomeningocele. N Engl J Med 2011 17; 364: 993–1004.
3 Sival DA, Guerra M, den Dunnen WF, Batiz LF, Alvial G, Castaneyra-Perdomo A et al.Neuroependymal denudation is in progress in full-term human foetal spina bifida aperta. Brain Pathol2011; 21: 163–79.
4 Korenromp MJ, van Gool JD, Bruinese HW, Kriek R. Early fetal leg movements in myelomeningocele.Lancet 1986; 1: 917–18.
5 Sival DA, Begeer JH, Staal-Schreinemachers AL, Vos-Niel JM, Beekhuis JR, Prechtl HF. Perinatal motorbehaviour and neurological outcome in spina bifida aperta. Early Hum Dev 1997; 50: 27–37.
6 Meuli M, Meuli-Simmen C, Hutchins GM, Seller MJ, Harrison MR, Adzick NS . The spinal cordlesion in human fetuses with myelomeningocele: implications for fetal surgery. Pediatr Surg 1997; 32:448–52.
7 Hutchins GM, Meuli M, Meuli-Simmen C, Jordan MA, Heffez DS, Blakemore KJ. Acquired spinal cordinjury in human fetuses with myelomeningocele. Pediatr Path Lab Med 1996; 16: 701–12.
8 Bowman RM, McLone DG, Grant JA, Tomita T, Ito JA. Spina bifida outcome: a 25-year prospective.Pediatr Neurosurg 2001; 34: 114–20.
9 Maher CO, Goumnerova L, Madsen JR, Proctor M, Scott RM. Outcome following multiple repeatedspinal cord untethering operations. J Neurosurg 2007; 106: 434–38.
10 Mitchell LE, Adzick NS, Melchionne J, Pasquariello PS, Sutton LN, Whitehead AS. Spina bifida. Lancet2004; 364: 1885–95.
11 Bruner JP, Tulipan N. Tell the truth about spina bifida. Ultrasound Obstet Gynecol 2004; 24: 595–96.
12 McLone DG, Dias MS. The Chiari II malformation: cause and impact. Child’s Nerv Syst 2003; 19:540–50.
13 Rintoul NE, Sutton LN, Hubbard AM, Cohen B, Melchionni J, Pasquariello PS, et al. A new lookat myelomeningoceles: functional level, vertebral level, shunting, and the implications for fetalintervention. Pediatrics 2002; 109: 409–13.
14 Caldarelli M, Di Rocco C, La Marca F. Shunt complications in the first postoperative year in childrenwith meningomyelocele. Childs Nerv Syst 1996; 12): 748–54.
15 Hunt GM, Oakeshott P. Outcome in people with open spina bifida at age 35: prospective communitybased cohort study. BMJ 2003; 326: 1365–66.
16 Zipitis CS, Paschalides C. Caring for a child with spina bifida: understanding the child and carer. JChild Health Care 2003; 7: 101–12.
The prenatal management of neural tube defects 183
17 National Center on Birth Defects and Developmental Disabilities, US CDC. http://www.cdc.gov/ncbddd/spinabifida/data.html
18 Ghi T, Pilu G, Falco P, Segata M, Carletti A, Cocchi G et al. Prenatal diagnosis of open and closedspina bifida. Ultrasound Obstet Gynecol 2006; 28: 899–903.
19 Blumenfeld Z, Siegler E, Bronshtein M. The early diagnosis of neural tube defects. Prenat Diagn 1993;13: 863–71.
20 Nicolaides KH, Campbell S, Gabbe SG, Guidetti R. Ultrasound screening for spina bifida: cranial andcerebellar signs. Lancet 1986; 2: 72–74.
21 D’Addario V, Rossi AC, Pinto V, Pintucci A, Di Cagno L. Comparison of six sonographic signs in theprenatal diagnosis of spina bifida. Perinat Med 2008; 36: 330–34.
22 Shipp TD, Benacerraf BR. Second trimester ultrasound screening for chromosomal abnormalities.Prenat Diagn 2002; 22: 296–307.
23 Crane JP, LeFevre ML, Winborn RC, Evans JK, Ewigman BG, Bain RP, et al. A randomized trial ofprenatal ultrasonographic screening: impact on the detection, management, and outcome of anomalousfetuses. The RADIUS Study Group. Am J Obstet Gynecol 1994; 171: 392–99.
24 Bruner JP, Tulipan N, Dabrowiak ME, Luker KS, Walters K, Burns P, et al. Upper level of the spinabifida defect: how good are we? Ultrasound Obstet Gynecol 2004; 24: 612–17.
25 Shaer CM, Chescheir N, Schulkin J. Myelomeningocele: a review of the epidemiology, genetics, riskfactors for conception, prenatal diagnosis, and prognosis for affected individuals. Obstet Gynecol Surv2007; 62: 471–79.
26 Chaoui R, Benoit B, Mitkowska-Wozniak H, Heling KS, Nicolaides KH. Assessment of intracranialtranslucency (IT) in the detection of spina bifida at the 11–13-week scan. Ultrasound Obstet Gynecol2009; 34: 249–52.
27 Lachmann R, Chaoui R, Moratalla J, Picciarelli G, Nicolaides KH. Posterior brain in fetuses with openspina bifida at 11 to 13 weeks. Prenat Diagn 2011; 31: 103–106.
28 Au KS, Ashley-Koch A, Northrup H. Epidemiologic and genetic aspects of spina bifida and other neuraltube defects. Dev Disabil Res Rev 2010; 16: 6–15.
29 Botto LD, Moore CA, Khoury MJ, Erickson JD. Neural-tube defects. New Engl J Med 1999; 341:1509–19.
30 Boulet SL, Yang Q, Mai C, Kirby RS, Collins JS, Robbins JM, et al. Trends in the postfortificationprevalence of spina bifida and anencephaly in the United States. Birth Defects Res A Clin Mol Teratol2008; 82: 527–32.
31 Williams LJ, Rasmussen SA, Flores A, Kirby RS, Edmonds LD. Decline in the prevalence of spina bifidaand anencephaly by race/ethnicity: 1995–2002. Pediatrics 2005; 116: 580–86.
32 Dolk H, Loane M, Garne E. The prevalence of congenital anomalies in Europe. Exp Med Biol 2010;686: 349–64.
33 Busby A, Abramsky L, Dolk H, Armstrong B, Addor MC, Anneren G, et al. Preventing neural tubedefects in Europe: a missed opportunity. Reprod Toxicol 2005; 20: 393–402.
34 Abramsky L, Busby A, Dolk H. Promotion of periconceptional folic acid has had limited success. J RSoc Promot Health 2005; 125: 206–209.
35 Boyd PA, Devigan C, Khoshnood B, Loane M, Garne E, Dolk H. Survey of prenatal screening policiesin Europe for structural malformations and chromosome anomalies, and their impact on detectionand termination rates for neural tube defects and Down’s syndrome. BJOG 2008; 115: 689–96.
36 Wyldes MP, Tonks AM. Termination of pregnancy for fetal anomaly: a population-based study 1995to 2004. BJOG 2007; 114: 639–42.
37 Main DM, Mennuti MT. Neural tube defects: issues in prenatal diagnosis and counselling. ObstetGynecol 1986; 67: 1–16.
38 Husler MR, Danzer E, Johnson MP, Bebbington M, Sutton L, Adzick NS, et al. Prenatal diagnosis andpostnatal outcome of fetal spinal defects without Arnold-Chiari II malformation. Prenat Diagn 2009;29: 1050–57.
39 Michejda M. Intrauterine treatment of spina bifida: primate model. Z Kinderchir 1984; 39: 259–61.

184 Masayuki Endo et al
40 Meuli M, Meuli-Simmen C, Yingling CD, Hutchins GM, Hoffman KM, Harrison MR, et al. Creationof myelomeningocele in utero: a model of functional damage from spinal cord exposure in fetal sheep.J Pediatr Surg 1995; 30: 1028–32.
41 Heffez DS, Aryanpur J, Hutchins GM, Freeman JM. The paralysis associated with myelomeningocele:clinical and experimental data implicating a preventable spinal cord injury. Neurosurgery 1990; 26:987–92.
42 Heffez DS, Aryanpur J, Rotellini NA, Hutchins GM, Freeman JM. Intrauterine repair of experimentalsurgically created dysraphism. Neurosurgery 1993; 32: 1005–10.
43 Danzer E, Kiddoo DA, Redden RA, Robinson L, Radu A, Zderic SA et al. Structural and functionalcharacterization of bladder smooth muscle in fetal rats with retinoic acid-induced myelomeningocele.Am J Physiol Renal Physiol 2007; 292: F197–206.
44 Danzer E, Radu A, Robinson LE, Volpe MV, Adzick NS, Flake AW. Morphologic analysis ofthe neuromuscular development of the anorectal unit in fetal rats with retinoic acid inducedmyelomeningocele. Neurosci Lett 2008; 430: 157–62.
45 Danzer E, Zhang L, Radu A, Bebbington MW, Liechty KW, Adzick NS, et al. Amniotic fluid levels ofglial fibrillary acidic protein in fetal rats with retinoic acid induced myelomeningocele: a potentialmarker for spinal cord injury. Am J Obstet Gynecol 2011; 204: 178 e1–11.
46 Julia V, Sancho MA, Albert A, Conill J, Martinez A, Grande C, et al. Prenatal covering of the spinalcord decreases neurologic sequelae in a myelomeningocele model. J Pediatr Surg 2006; 41: 1125–129.
47 Meuli M, Meuli-Simmen C, Hutchins GM, Yingling CD, Hoffman KM, Harrison MR, et al. In uterosurgery rescues neurological function at birth in sheep with spina bifida. Nat Med 1995; 1: 342–47.
48 Meuli M, Meuli-Simmen C, Yingling CD, Hutchins GM, Timmel GB, Harrison MR, et al. In uterorepair of experimental myelomeningocele saves neurological function at birth. J Pediatr Surg 1996;31: 397–402.
49 Bouchard S, Davey MG, Rintoul NE, Walsh DS, Rorke LB, Adzick NS. Correction of hindbrainherniation and anatomy of the vermis after in utero repair of myelomeningocele in sheep. J PediatrSurg 2003; 38: 451–58.
50 Paek BW, Farmer DL, Wilkinson CC, Albanese CT, Peacock W, Harrison MR, et al. Hindbrainherniation develops in surgically created myelomeningocele but is absent after repair in fetal lambs.Am J Obstet Gynecol 2000; 183: 1119–123.
51 Deprest JA, Flake AW, Gratacos E, Ville Y, Hecher K, Nicolaides K, et al. The making of fetal surgery.Prenat Diagn 2010; 30: 653–67.
52 Harrison MR, Filly RA, Golbus MS, Berkowitz RL, Callen PW, Canty TG et al. Fetal treatment 1982.N Engl J Med 1982; 307: 1651–52.
53 Longaker MT, Whitby DJ, Adzick NS, Kaban LB, Harrison MR. Fetal surgery for cleft lip: a plea forcaution. Plast Reconstr Surg 1991; 88: 1087–92.
54 Adzick NS. Open fetal surgery for life-threatening fetal anomalies. Semin Fetal Neonatal Med 2010;15: 1–8.
55 Wilson RD, Lemerand K, Johnson MP, Flake AW, Bebbington M, Hedrick HL, et al. Reproductiveoutcomes in subsequent pregnancies after a pregnancy complicated by open maternal-fetal surgery(1996–2007). Am J Obstet Gynecol 2010; 203: 209 e1–6.
56 Luks FI, Deprest JA. Endoscopic fetal surgery: a new alternative? Eur J Obstet Gynecol Reprod Biol1993; 52: 1–3.
57 Luks FI, Peers KH, Deprest JA, Lerut TE, Vandenberghe K. The effect of open and endoscopic fetalsurgery on uteroplacental oxygen delivery in the sheep. J Pediatr Surg 1996; 31: 310–14.
58 Deprest JA, Luks FI, Peers KH, Vandenberghe K, Lerut TE, Brosens IA, et al. Intrauterine endoscopiccreation of urinary tract obstruction in the fetal lamb: a model for fetal surgery. Am J Obstet Gynecol1995; 172: 1422–426.
59 Gratacos E, Wu J, Devlieger R, Bonati F, Lerut T, Vanamo K, et al. Nitrous oxide amniodistentioncompared with fluid amniodistention reduces operation time while inducing no changes in fetal acid-base status in a sheep model for endoscopic fetal surgery. Am J Obstet Gynecol 2002; 186: 538–43.

The prenatal management of neural tube defects 185
60 Skarsgard ED, Bealer JF, Meuli M, Adzick NS, Harrison MR. Fetal endoscopic (‘Fetendo’) surgery: therelationship between insufflating pressure and the fetoplacental circulation. J Pediatr Surg 1995; 30:1165–168.
61 Bruner JP, Richards WO, Tulipan NB, Arney TL. Endoscopic coverage of fetal myelomeningocele inutero. Am J Obstet Gynecol 1999; 180: 153–58.
62 Farmer DL, von Koch CS, Peacock WJ, Danielpour M, Gupta N, Lee H, et al. In utero repair ofmyelomeningocele: experimental pathophysiology, initial clinical experience, and outcomes. ArchSurg 2003; 138: 872–78.
63 Kohl T, Hering R, Heep A, Schaller C, Meyer B, Greive C, et al. Percutaneous fetoscopic patch coverageof spina bifida aperta in the human–early clinical experience and potential. Fetal Diagn Ther 2006; 21:185–93.
64 Verbeek RJ, Heep A, Maurits NM, Cremer R, Hoving EW, Brouwer OF, et al. Fetal endoscopicmyelomeningocele closure preserves segmental neurological function. Dev Med Child Neurol 2012;54: 15–22.
65 Adzick NS, Sutton LN, Crombleholme TM, Flake AW. Successful fetal surgery for spina bifida. Lancet1998; 21; 352: 1675–676.
66 Bruner JP, Tulipan NB, Richards WO, Walsh WF, Boehm FH, Vrabcak EK. In utero repair ofmyelomeningocele: a comparison of endoscopy and hysterotomy. Fetal Diagn Ther 2000; 15: 83–88.
67 Walsh WF, Chescheir NC, Gillam-Krakauer M, McPheeters ML, McKoy JN, Jerome R et al. Maternal-Fetal Surgical Procedures. Technical Brief No. 5. (Prepared by the Vanderbilt Evidence-based PracticeCenter under Contract No. 290–2007-10065.) AHRQ Publication No. 10(11)-EHC059-EF. Rockville,MD: Agency for Healthcare Research and Quality. April 2011.
68 Johnson MP, Gerdes M, Rintoul N, Pasquariello P, Melchionni J, Sutton LN, et al. Maternal-fetalsurgery for myelomeningocele: neurodevelopmental outcomes at 2 years of age. Am J Obstet Gynecol2006; 194: 1145–150.
69 Johnson MP, Sutton LN, Rintoul N, Crombleholme TM, Flake AW, Howell LJ, et al. Fetalmyelomeningocele repair: short-term clinical outcomes. Am J Obstet Gynecol 2003; 189: 482–87.
70 Bruner JP, Tulipan N, Paschall RL, Boehm FH, Walsh WF, Silva SR, et al. Fetal surgery formyelomeningocele and the incidence of shunt-dependent hydrocephalus. JAMA 1999; 282: 1819–825.
71 Tulipan N, Bruner JP. Fetal surgery for spina bifida. Lancet 1999; 353: 406.
72 Bruner JP, Tulipan N. Intrauterine repair of spina bifida. Clin Obstet Gynecol 2005; 48: 942–55.
73 Hamdan AH, Walsh W, Bruner JP, Tulipan N. Intrauterine myelomeningocele repair: effect on short-term complications of prematurity. Fetal Diagn Ther 2004; 19: 83–86.
74 Tulipan N, Sutton LN, Bruner JP, Cohen BM, Johnson M, Adzick NS. The effect of intrauterinemyelomeningocele repair on the incidence of shunt-dependent hydrocephalus. Pediatr Neurosurg2003; 38: 27–33.
75 Tulipan N. Intrauterine myelomeningocele repair. Clin Perinatol 2003; 30: 521–30.
76 Danzer E, Gerdes M, Bebbington MW, Koh J, Adzick SN, Johnson MP. Fetal myelomeningocele surgery:preschool functional status using the Functional Independence Measure for children (WeeFIM). ChildsNerv Syst 2011; 27: 1083–88.
77 Danzer E, Gerdes M, Bebbington MW, Zarnow DM, Adzick NS, Johnson MP. Preschoolneurodevelopmental outcome of children following fetal myelomeningocele closure. Am J ObstetGynecol 2010; 202: 450 e1–9.
78 Holzbeierlein J, Pope JI, Adams MC, Bruner J, Tulipan N, Brock JW, 3rd. The urodynamic profile ofmyelodysplasia in childhood with spinal closure during gestation. J Urol 2000; 164: 1336–339.
79 Holmes NM, Nguyen HT, Harrison MR, Farmer DL, Baskin LS. Fetal intervention formyelomeningocele: effect on postnatal bladder function. J Urol 2001; 166: 2383–386.
80 Tubbs RS, Chambers MR, Smyth MD, Bartolucci AA, Bruner JP, Tulipan N et al. Late gestationalintrauterine myelomeningocele repair does not improve lower extremity function. Pediatr Neurosurg2003; 38: 128–32.
81 Danzer E, Adzick NS. Fetal surgery for myelomeningocele: patient selection, perioperativemanagement and outcomes. Diagn Ther 2011; 30: 163–73.

186 Masayuki Endo et al
82 Bebbington MW, Danzer E, Johnson MP, Adzick NS. Open fetal surgery for myelomeningocele. PrenatDiagn 2011; 31: 689–94.
83 Wilson RD, Johnson MP, Crombleholme TM, Flake AW, Hedrick HL, King M, et al. Chorioamnioticmembrane separation following open fetal surgery: pregnancy outcome. Fetal Diagn Ther 2003; 18:314–20.
84 Sroka M, Swiatkowska-Freund M, Gołebiewski A, Piotr Czauderna P, Preis K. Fetal surgery: future orway leading to nowhere. First experiences. Przeglad Pediatryczny, 2007: 37: 7–9.
85 Danzer E, Johnson MP, Adzick NS. Fetal surgery for myelomeningocele: progress and perspectives.Dev Med Child Neurol 2012; 54: 8–14.
86 Moise KJ, Jr, Johnson A, Carpenter RJ, Baschat AA, Platt LD. Fetal intervention: providing reasonableaccess to quality care. Obstet Gynecol 2009; 113: 408–10.
87 Sanchez e Oliveira Rde C, Valente PR, Abou-Jamra RC, Araujo A, Saldiva PH, Pedreira DA.Biosynthetic cellulose induces the formation of a neoduramater following pre-natal correction ofmeningomyelocele in fetal sheep. Acta Cir Bras 2007; 22: 174–81.
88 Fontecha CG, Peiro JL, Sevilla JJ, Aguirre M, Soldado F, Fresno L, et al. Fetoscopic coverage ofexperimental myelomeningocele in sheep using a patch with surgical sealant. Eur J Obstet GynecolReprod Biol 2011; 156: 171–76.
89 Watanabe M, Jo J, Radu A, Kaneko M, Tabata Y, Flake AW. A tissue engineering approach for prenatalclosure of myelomeningocele with gelatin sponges incorporating basic fibroblast growth factor. TissueEng Part A. 2010; 16: 1645–55.
90 Watanabe M, Li H, Roybal J, Santore M, Radu A, Jo J, et al. A tissue engineering approach for prenatalclosure of myelomeningocele: comparison of gelatin sponge and microsphere scaffolds and bioactiveprotein coatings. Tissue Eng Part A. 2011; 17: 1099–110.
91 Sanchez e Oliveira Rde C, Valente PR, Abou-Jamra RC, Araujo A, Saldiva PH, Pedreira DA.Biosynthetic cellulose induces the formation of a neoduramater following pre-natal correction ofmeningomyelocele in fetal sheep. Acta Cir Bras 2007; 22: 174–81.
92 Fontecha CG, Peiro JL, Sevilla JJ, Aguirre M, Soldado F, Fresno L, et al. Fetoscopic coverage ofexperimental myelomeningocele in sheep using a patch with surgical sealant. Eur J Obstet GynecolReprod Biol 2011; 156: 171–76.
93 Fontecha CG, Peiro JL, Aguirre M, Soldado F, Anor S, Fresno L, et al. Inert patch with bioadhesive forgentle fetal surgery of myelomeningocele in a sheep model. Eur J Obstet Gynecol Reprod Biol 2009;146: 174–79.
94 Bilic G, Brubaker C, Messersmith PB, Mallik AS, Quinn TM, Haller C, et al. Injectable candidatesealants for fetal membrane repair: bonding and toxicity in vitro. Am J Obstet Gynecol 2010; 202: 85e1–9.
95 Abou-Jamra RC, Valente PR, Araujo A, Sanchez e Oliveira Rde C, Saldiva PH, Pedreira DA. Simplifiedcorrection of a meningomyelocele-like defect in the ovine fetus. Acta Cir Bras 2009; 24: 239–44.
96 Watanabe M, Jo J, Radu A, Kaneko M, Tabata Y, Flake AW. A tissue engineering approach for prenatalclosure of myelomeningocele with gelatin sponges incorporating basic fibroblast growth factor. TissueEng Part A. 2010; 16: 1645–55.
97 Hosper NA, Eggink AJ, Roelofs LA, Wijnen RM, van Luyn MJ, Bank RA et al. Intra-uterine tissueengineering of full-thickness skin defects in a fetal sheep model. Biomaterials 2010; 31: 3910–919.
98 http://www.eurocat-network.eu/accessprevalencedata/prevalencetables (prevalence rates of the last5 years) Accessed 19 February 2012.
99 Jani JC, Nicolaides KH, Gratacos E, Valencia CM, Done E, Martinez JM, et al. Severe diaphragmatichernia treated by fetal endoscopic tracheal occlusion. Ultrasound Obstet Gynecol 2009; 340: 304–10.
100 Kohl T, Tchatcheva K, Weinbach J, Hering R, Kozlowski P, Stressig R, et al. Partial amniotic carbondioxide insufflation (PACI) during minimally invasive fetoscopic surgery: early clinical experience inhumans. Surgical endoscopy. [Clinical Trial Research Support, Non-U.S. Gov’t]. 2010; 24: 432–44.
101 Ruano R, Duarte SA, Pimenta EJ, Takashi E, da Silva MM, Tannuri U, et al. Comparison betweenfetal endoscopic tracheal occlusion using a 1.0-mm fetoscope and prenatal expectant management insevere congenital diaphragmatic hernia. Fetal Diagn Ther 2011; 29: 64–70.
Related Documents











