The Pharmacist Registration Examination Rebecca Elvey (BA, MA (Econ)) Research Associate Samuel D Jee (BSc) Research Assistant Penny Lewis (PhD, MRPharmS) Research Associate Harsha Parmar (MRPharmS) Teaching Fellow Ellen I Schafheutle (PhD, MRes, MSc, MRPharmS) Lecturer in Law & Professionalism in Pharmacy Mary Tully (PhD, MRPharmS) Clinical Senior Lecturer Sarah Willis (BA, MA) Research Fellow Jason Hall (PhD, MSc, BSc, PGCE, MRPharmS) Senior Lecturer School of Pharmacy and Pharmaceutical Sciences 1 st The University of Manchester Floor Stopford Building Oxford Road Manchester M13 9PT Correspondence Dr Jason Hall [email protected] 0161 275 2720

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
The Pharmacist Registration Examination
Rebecca Elvey (BA, MA (Econ)) Research Associate
Samuel D Jee (BSc) Research Assistant Penny Lewis (PhD, MRPharmS) Research Associate Harsha Parmar (MRPharmS) Teaching Fellow Ellen I Schafheutle (PhD, MRes, MSc, MRPharmS) Lecturer in Law & Professionalism in Pharmacy Mary Tully (PhD, MRPharmS) Clinical Senior Lecturer Sarah Willis (BA, MA) Research Fellow Jason Hall (PhD, MSc, BSc, PGCE, MRPharmS) Senior Lecturer
School of Pharmacy and Pharmaceutical Sciences 1st
The University of Manchester Floor Stopford Building
Oxford Road Manchester M13 9PT
Correspondence Dr Jason Hall [email protected] 0161 275 2720
The Pharmacist Registration Examination – September 2010 i
Abstract
The aim of this study was to review the registration examination and compare
it with alternative methods of assessing professional competence. We carried
out the following three pieces of work. Firstly, we reviewed the procedures for
registration of selected other health professionals (optometry, medicine,
dentistry) within Great Britain to determine the range of methods employed for
assessing suitability for registration. Secondly, we reviewed the procedures
for registration of pharmacists in a selection of English speaking countries
outside Great Britain to determine the range of methods employed for
assessing suitability for registration. Thirdly, we mapped out the registration
examination questions against the pre-registration syllabus.
There were differences between the professions and differences between
countries in terms of the training and assessment of candidates seeking to
obtain professional registration. Pharmacy was the only profession in our
review with formal written examinations at the end of the postgraduate pre-
registration training period whilst the other professions relied on practice
based assessments to a greater extent. In pharmacy in GB the supervisor and
assessor functions were not separated which was not the case in most other
professions or countries. Our assessment of the registration examination
suggests that it particularly focuses on the assessment of knowledge which
means that particular emphasis and importance rests on the regular
performance reports to assess a broad range of competences and
understanding.
The Pharmacist Registration Examination – September 2010 ii
Acknowledgements We would firstly like to give thanks to the General Pharmaceutical Council
(GPhC)/Royal Pharmaceutical Society of Great Britain (RPSGB) who funded
this research and provided us with pharmacy registration examination data.
This research started in May 2010 when the RPSGB was the regulator in
Great Britain and was completed after 27th
September 2010 when the GPhC
became the pharmacy regulator.
Many thanks go to Professor Val Wass from the School of Medicine at Keele
University (formerly from the School of Medicine at the University of
Manchester) for her advice about registration requirements in medicine and
other healthcare professions in Great Britain and abroad.
We are also very grateful to our expert panel consisting of:
• Ian Smith – Boots Teacher Practitioner University of Manchester; Boots
Pre-registration coordinator for north of England
• Alison Littlewood – Lead Pre-registration Facilitator, NHS north west;
• Professor Chris Dickinson – Optometry Programme Director, University
of Manchester;
• Andrea Owen – University Medical Assessment Partnership (UMAP).;
and
• Iain Mackie – Head of School of Dentistry, University of Manchester
The expert panel offered their time and expertise about registration
requirements in pharmacy, medicine and other healthcare professions in
Great Britain and abroad. We would particularly like to thank Ian Smith and
Alison Littlewood for helping members of the research team with the
registration examination mapping exercises.
The Pharmacist Registration Examination – September 2010 iii
Contents 1 Introduction ............................................................................................... 1
1.1 Membership of a profession ................................................................ 1
1.2 Membership of the pharmacy profession ............................................ 2
1.3 Aims of this study ................................................................................ 3
1.4 Layout of this report ............................................................................ 4
2 Comparing registration of pharmacists in GB with registration requirements
for other GB healthcare professions and for pharmacists abroad .................... 5
2.1 Introduction ......................................................................................... 5
2.2 Method ................................................................................................ 5
2.3 Results ................................................................................................ 7
2.3.1 Pharmacy ..................................................................................... 7
2.3.2 Optometry .................................................................................. 12
2.3.3 Medicine ..................................................................................... 16
2.3.4 Dentistry ..................................................................................... 22
2.3.5 Summary/comparison of the different professions ..................... 28
2.3.6 Australia ..................................................................................... 32
2.3.7 New Zealand .............................................................................. 37
2.3.8 Canada ....................................................................................... 38
2.3.9 USA ............................................................................................ 43
2.3.10 Summary/comparison of the different countries ...................... 48
3 The effectiveness of the pharmacist registration examination ................ 51
3.1 Introduction ....................................................................................... 51
3.2 Method .............................................................................................. 51
3.3 Results .............................................................................................. 53
3.3.1 Closed book examination paper ................................................. 53
3.3.2 Open book examination paper ................................................... 57
3.3.3 Summary/Comparison of the closed and open book papers ...... 62
4 Discussion .............................................................................................. 64
4.1 Registration requirements for other healthcare professions in the UK.. 64
4.2 Registration requirements for pharmacists in selected other countries .66
The Pharmacist Registration Examination – September 2010 iv
4.3 The effectiveness of the pharmacist registration examination:
mapping of examination questions against syllabus & knowledge versus
understanding ............................................................................................. 68
5 Recommendations .................................................................................. 72
6 References ............................................................................................. 73
Appendices 7.1 Appendix 1: Comparison of registration requirements for healthcare
professionals in GB ........................................................................................ 77
7.2 Appendix 2: Comparison of registration requirements for pharmacists
in GB and abroad ........................................................................................... 80
7.3 Appendix 3: Coding of the registration examination syllabus ............ 82
7.4 Appendix 4: Mapping of closed and open book registration
examination questions to knowledge and/or understanding and examination
syllabus .......................................................................................................... 88
List of tables Table 3.1: Number of times syllabus entries were assessed in the closed
book examination ........................................................................................... 54
Table 3.2: Number of times syllabus entries assessed knowledge and/or
understanding (number of questions) in the closed book ............................... 57
Table 3.3: Number of times syllabus entries are assessed in the open book
examination .................................................................................................... 59
Table 3.4: Number of times syllabus entries assessed knowledge and/or
understanding (number of questions) in the open book ................................. 61
The Pharmacist Registration Examination – September 2010 1
1 Introduction
1.1 Membership of a profession
Members of a profession tend to have a monopoly on their area of expertise
or practice and many have a restricted title. Membership of a profession may
bring a number of rewards such as job security, above average salary,
interesting work and respect from society. Such benefits make membership
attractive and there is usually competition1
for entry.
Historically, members of professions were generally keen to preserve the
social standing and reputation of their profession and sought to guard entry to
their profession.2
Entry to a profession was usually via the successful
completion of a period of study at a higher education institution on an
approved programme of study and in some cases following a period of
apprenticeship and further assessment.
More recently, the motive for controlling entry to the health professions has
been to promote health, safety and wellbeing of patient and the public.3 Many
of the health professions either have their own regulator, or are jointly
regulated by the Health Professions Council (HPC), which deal with entry to
their profession. Within the UK the Council for Healthcare Regulatory
Excellence (CHRE) is the organisation that oversees the regulators for nine
health professions including medicine, dentistry, optometry and pharmacy.4
They review how the health profession regulators carry out a range of
activities including education and training, fitness to practise and registration.
The Pharmacist Registration Examination – September 2010 2
1.2 Membership of the pharmacy profession
To become a pharmacist in Great Britain (GB), it is a requirement to
successfully undertake a four-year full time Master of Pharmacy (MPharm)
degree course in a UK university. This is followed by 52 weeks of pre-
registration training, usually in one of the main pharmacy sectors (i.e.
community or hospital), but sometimes split between more than one sector
(e.g. between the pharmaceutical industry and hospital pharmacy). Besides
entrance to the pre-registration year via an MPharm degree, a one-year
Overseas Pharmacists Assessment Programme (OSPAP) diploma is also in
place and is offered at five schools of pharmacy in GB. The latter needs to be
passed by internationally trained pharmacists from outside the European
Economic Area (EEA) before they are eligible to enter pre-registration training.
All pre-registration applicants have to sign declarations of good conduct and
good health, agree to abide by the Standards of conduct, ethics and
performance5
(previously the RPSGB Code of Ethics) and pay the appropriate
fee.
The pre-registration training itself involves a minimum of 26 weeks (and
usually 52 weeks) of supervised practice in employment in a clinical
(pharmacy practice) environment. Outcomes of training are assessed using
two distinct methods. Firstly, trainees must demonstrate competence in
eleven areas of practice by providing evidence that they have complied with
performance standards related to these eleven areas.6
A pre-registration tutor
acts as supervisor and also assessor for compliance with the standards in a
series of assessments made during the training year (at 13, 26 and 39 weeks)
leading up to a final assessment at the end of the year. The second aspect of
assessment is the formal registration examination, a uniform test for all pre-
registration trainees, set centrally by the General Pharmaceutical Council
(GPhC), and previously the Royal Pharmaceutical Society of Great Britain
(RPSGB). A trainee cannot sit the examination until their tutor has signed
them off as fit to undertake the examination at the 39 week assessment and
provided the trainee has completed at least 45 weeks of pre-registration
training.
The Pharmacist Registration Examination – September 2010 3
The requirement for pharmacists to undertake a 12-month period of pre-
registration training prior to registration has been in place for a long time. The
system of pre-registration competencies and the completion of a related
portfolio, as well as a written exam, has been in place for a number of years.
Nevertheless, we have little insight into the effectiveness of current
arrangements for in practice training and assessment, or the effectiveness of
the written exam. Nevertheless, similar arrangements for in practice training
are in place in the education of other healthcare professions, or pharmacists
in other countries. Further insight may also be gained from exploring how
current assessment maps against the existing examination syllabus.6
1.3 Aims of this study
The aim of this study was to review the registration examination and compare
it with alternative methods of assessing professional competence
In order to meet the research aims we carried out the following pieces of work
that together contribute to this report:
• A review of the procedures for registration of selected other health
professionals (optometry, medicine, dentistry) within Great Britain to
determine the range of methods employed for assessing suitability for
registration
• A review of the procedures for registration of pharmacists in a selection
of English speaking countries outside Great Britain to determine the
range of methods employed for assessing suitability for registration
(section 2)
• Mapping out examination questions against the pre-registration
syllabus1
(section 3)
1 Previously this was the preregistration standards, but this was not feasible (c.f. section 2)

The Pharmacist Registration Examination – September 2010 4
1.4 Layout of this report
As there were two main parts to this study each part is presented in turn, with
an individual ‘introduction and method’, ‘results’, and ‘summary’ section.
Following this an overall discussion highlights some of the key issues raised
from the findings from each part of the study. Based on these findings,
recommendations related to assessments are then made.
The Pharmacist Registration Examination – September 2010 5
2 Comparing registration of pharmacists in GB with registration requirements for other GB healthcare professions and for pharmacists abroad
2.1 Introduction
There are a range of healthcare professions in GB, each having different
requirements set out for prospective registrants to fulfil so they can be placed
on the register. Differences also exist in registration requirements for
pharmacists in other countries. It is useful to gain insight into these different
requirements, as they may shed light on which aspects of, or approaches to,
training, supervision and assessment the registration bodies for those
professions or countries consider to be particularly effective. This could inform
potential changes
to achieve a more effective means of assessment and
registration in GB pharmacy.
This part of the study aims to:
• compare the methods used for assessing the suitability for registration
as a pharmacist in GB, with methods used by optometry, medicine and
dentistry in GB;
• compare the methods used for assessing the suitability for registration
as a pharmacist in GB to a selection of English speaking countries with
similar systems/policies outside GB: Australia, Canada, New Zealand
and the USA.
2.2 Method
For each profession, and for each country, we reviewed the training
programmes and assessment methods in place for each profession prior to
full registration as a health professional, in order to answer the following
questions:
The Pharmacist Registration Examination – September 2010 6
• Who conducts the assessment?
• Where is it assessed?
• When is it assessed?
• What is assessed?
• How is it assessed (by what methods)?
Numerous internet searches were carried out to identify relevant websites
relating to the regulatory and professional bodies and training/educational
organisations (such as professional societies and colleges) of health care
professions in Great Britain as well as identifying similar organisations for the
pharmacy profession abroad. Some of these websites included:
• The Royal Pharmaceutical Society of Great Britain (prior to split):
http://www.rpsgb.org
• General Optical Council: http://www.optical.org/
• General Medical Council: http://www.gmc-uk.org/
• General Dental Council: http://www.gdc-uk.org/
• Australian Pharmacy Council: http://www.pharmacycouncil.org.au/
• New Zealand Pharmacy Council:
http://www.pharmacycouncil.org.nz/cms_display.php
• The Pharmacy Examining Board of Canada:
(http://www.pebc.ca/EnglishPages/General/HomePage.html)
• National Association of Boards of Pharmacy in the USA:
http://www.nabp.net/
The websites were examined for documentation pertaining to registration
which mainly consisted of registration programme training curricula,
workbooks and similar materials. The documents were read and the relevant
information was extracted. Members of the expert panel summarised relevant
information regarding registration and helped identify relevant documents and
websites.
The Pharmacist Registration Examination – September 2010 7
2.3 Results
This section reviews the different methods used to train and assess an
individual to prove that they are qualified to register to practise in their
discipline. Specifically, pharmacy in GB will be compared to optometry,
medicine and dentistry. A comparison table of the registration processes for
these professions is provided in appendix 1. This section of the report also
provides details about the different methods used, and requirement laid out,
for a pharmacist to register in a selection of other countries besides GB:
Australia, New Zealand, Canada and USA. A comparison table of the
registration processes of countries is available in appendix 2.
Findings for healthcare professionals including pharmacy To provide the main comparator, this section will begin by setting out the
requirements for registration as a pharmacist in GB.
2.3.1 Pharmacy
2.3.1.1 Basic training requirements and different types of registration
In the main, pharmacy undergraduate degree programmes consist of a four-
year Masters course, the MPharm, although a five-year sandwich course is
also available. Following attainment of the MPharm degree, pharmacy pre-
registration trainees undertake a one-year pre-registration post, most
commonly in either a community or hospital pharmacy practice setting, usually
with two weeks ‘cross sector’ experience. After successful completion of the
pre-registration year, and passing the required assessments, trainees can
apply for registration as a pharmacist with the GPhC.
2.3.1.2 Details of training and assessment methods
Information presented in this section was taken/adapted from the 2009/10
version of the pre-registration trainee workbook (previously available from the
RPSGB website) 2009/106, unless otherwise indicated. During the course of
this programme of work the GB pharmacy regulator changed from the RPSGB
The Pharmacist Registration Examination – September 2010 8
to the GPhC. The most up to date version of the workbook is available from
the GPhC website7
. When referring to the current regulations reference will be
made to the GPhC and when a historical perspective is taken the RPSGB will
be referred to.
People involved in the assessment of pre-registration trainees
Pre-registration training can only be undertaken in premises approved by, and
registered with, the GPhC. Each pre-registration trainee is assigned to a pre-
registration tutor. The pre-registration tutor is the key contact for trainees
during their pre-registration year. The tutor assesses whether or not the
trainee has reached the standard of competence required and makes the final
decision as to whether the trainee is a fit and proper person to be registered.
Requirements for being a tutor include being:
• a practising pharmacist and have been working in the field of pharmacy
in which they wish to tutor for at least three years
• able to work for a minimum of 28 hours a week over a minimum of four
days with the trainee
In community pharmacy, for example, there is usually a one-to-one
relationship of tutor to trainee. In some training sites that employ several
trainees, there may not be enough pharmacists, who meet all of the criteria to
be tutors, to enable every trainee to have their own tutor. In these cases one
of the tutors or the pre-registration manager will take on the role of tutor for
more than one trainee.
Currently, the GPhC does not specify any compulsory training for tutors, but
states that tutors ‘have an ethical obligation to be adequately and
appropriately trained, prepared and experienced to take on the role’. GPhC
issues distance learning materials as part of the tutor workbooks and other
material sent to tutors. The materials also contain references to other sources
of information and guidance and tutors should follow these up. Most large
The Pharmacist Registration Examination – September 2010 9
employers will also run in-house training for tutors. Some universities run
‘training for trainers’ courses (previously available from the RPSGB website).8
Besides the tutor, there are also other individuals that play a role in the
training of pre-registration trainees. In the workplace these are trainers and
mentors. The GPhC does not specify requirements for those fulfilling these
roles, but, as stipulated in the pre-registration trainee workbook:
• trainers are often pharmacists but may be other pharmacy personnel.
Trainers have the greatest input when a tutor has responsibility for
more than one trainee and when a trainee is working away from the
tutor's place or section of work (primarily this relates to different
sections of a hospital pharmacy or different parts of a hospital trust).
Trainers may then undertake some of the roles of the pre-registration
tutor;
• a mentor is a person who is able to guide and support the trainee in a
non-judgemental way, for example, a recently registered pharmacist or
a more experienced colleague. Trainees, along with their tutors, are
encouraged to identify a suitable person, either within the workplace or
elsewhere, to be their mentor.
2.3.1.3 Assessment – what is assessed and how
Skills and behaviours are assessed in the workplace by the pre-registration
tutor or trainer. Knowledge is assessed by satisfactory performance and
behaviour whilst in the workplace, and in the registration examination.
To successfully complete the pharmacy pre-registration year, trainees have to
demonstrate competence in the ‘pre-registration standards’. These standards
are set out in the pre-registration workbook. The performance standards are
grouped into three areas – personal effectiveness, interpersonal skills and
medicines & health. The standards can be assessed in any order and the
timing of assessments is agreed between the tutor and trainee. Trainees must
collect evidence which demonstrates their competence against each standard
and build up a portfolio of evidence. Evidence of the trainee’s competence
The Pharmacist Registration Examination – September 2010 10
against each standard is then assessed by the tutor. There are three staged
assessments (every 13 weeks). The tutor acts as an assessor and completes
progress reports for each assessment, which are submitted to the GPhC.
Competence in the pre-registration standards is confirmed through the three
progress reports plus a ‘final declaration’ completed by the pre-registration
tutor.
Observation is the main method of assessment against the performance
standards. As stated in the pre-registration trainee workbook, there are
different types of observation that can be used:
• Formal observation – the assessor observes the trainee undertaking a
particular activity and then provides feedback. If performance is of the
required standard the assessor records this, if not, they will discuss
areas for improvement with the trainee. Trainees should be observed
on more than one occasion to ensure consistent performance.
Observation can be undertaken for a short period i.e. whilst
undertaking a particular task, or over a longer period i.e. over a week of
giving advice over the pharmacy counter, or of fielding queries in the
medicines information centre.
• Informal observation - tutors and others will observe trainees in the
workplace and can give the trainee feedback and highlight areas where
improvement is needed; this is an ongoing, formative process.
• Role play, case study, simulation – tutors, trainers or study day
facilitators can provide ‘mock’ situations for trainees to deal with.
Where the tutor is not involved, others can provide a report for the
portfolio. Video evidence showing how the trainee performs in certain
tasks e.g. preparing aseptic products, demonstrating how to use an
appliance may also be used.
In addition to observation, other forms of evidence are collected by trainees to
show how they meet the performance standards and are filed in the portfolio,
The Pharmacist Registration Examination – September 2010 11
with an annotation to show which standards they relate to. The main forms of
evidence as noted in the pre-registration trainee workbook are:
• testimonials - statements provided by a person who has worked with
the trainee and observed their performance. Trainees are encouraged
to ask others who provide training for them when their tutor is absent,
to complete testimonials for the tutor to review;
• projects and assignments that the trainee can write up to show what
they did and what they learned in a certain area, as demonstration of
competence in that area;
• records of evidence – brief notes of work situations e.g. diaries or
notebooks of work experiences, conversations and so on that are
cross-referenced to the relevant performance standards;
• prior experience – e.g. a valid first aid certificate or a workbook/portfolio
from undergraduate work experience. Evidence from this source is
most likely to be appropriate for 'technical' areas;
• other documentation - examples of other evidence could include copies
of medicines administration records; copy of a problem prescription
with notes of action taken.
The pre-registration workbook does not specify what type of or how much
evidence is required for each competency, but states that trainees ‘probably
need to produce a minimum of five pieces of evidence for each standard’ to
satisfy the tutor of their competence. One piece of evidence, e.g. the record of
observation of a particular scenario, could be used to demonstrate
competence against more than one standard.
The registration examination
Besides performing adequately in accordance with the tutors’ performance
reports and subsequently being signed off, pre-registration trainees also have
to pass the registration examination. Trainees are eligible to sit the registration
examination after a satisfactory 39-week Progress report and after completing
45 weeks of training. The registration examination assesses knowledge and
The Pharmacist Registration Examination – September 2010 12
understanding by asking candidates to analyse and evaluate practise-based
problems. There are two papers in the examination both of which use multiple
choice questions (MCQs). In the first paper candidates should attempt all 90
questions in 90 minutes and the examination is closed book. In the second
paper candidates should attempt all 80 questions in 150 minutes and the
examination is open to selected reference sources (British National Formulary
– BNF, Drug Tariff and Medicines Ethics and Practice – MEP). Twenty of the
questions in the second paper are calculation style and electronic calculators
are not permitted in this examination. Trainees must achieve 70% across all
questions and 70% in the calculation style questions.
2.3.2 Optometry
2.3.2.1 Basic training requirements and different types of registration
Following a three-year undergraduate degree, pre-registration optometrists
undertake a one-year ‘Scheme for Registration’ (SfR) post in a high street or
hospital practice, usually with some ‘cross-sector’ experience. The SfR is run
by the College of Optometrists.
Optometry students are required to register with the General Optical Council
(GOC) from the start of their undergraduate training. After successful
completion of the pre-registration year, and passing the required
assessments, trainees can apply for full registration. The GOC also holds
registers for specialty practitioners and corporate bodies. Registrants with a
specialty entered against their name in the opticians register are qualified to
perform additional duties to those of a normal optometrists or dispensing
optician. Once qualified, optometrists can develop their interests in specialist
areas.9 There are currently three specialties for which optometrists can be
registered: ‘Additional Supply’, ‘Supplementary Prescribing’ and ‘Independent
Prescribing’. Following completion of a training course and approval by the
GOC, a register entry is added to the registrant’s record allowing them to
practise their specialty.
The Pharmacist Registration Examination – September 2010 13
2.3.2.2 Details of training and assessment methods
Information presented in this section has been taken/adapted from The SfR
handbook10
unless otherwise indicated.
People involved in the assessment of pre-registration optometrists
The supervisor is the key contact for the pre-registration optometrist and is
responsible for supporting them throughout their SfR training. Supervisors
work with trainees on a day-to-day basis, directly supervising them on the
premises. Supervisors must have been practising optometry for at least three
years. No formal training is provided.
The SfR competency assessments are conducted by two separate
independent assessors – one for each stage of the assessments. Assessors
are appointed by the College of Optometrists.
Assessment – what is assessed and how
The core activity of trainee optometrists’ work is carrying out sight tests on
patients, and this is done from the start of their training. At first the trainee is
only expected to see ‘simple’ cases, and the supervisor checks their work
closely. As they progress, the trainee is expected to see more complex cases,
and supervisor makes fewer checks on their work. The assessment
framework specifies particular ‘patient episodes’ that a trainee must see
during the pre-registration year.
During the year, the trainee keeps a ‘logbook’, where they record:
• details about each patient seen – this consists of a table where
information about each case is entered into a row;
• a weekly dispensing summary for spectacles;
• any additional comments, unusual occurrences or ‘learning points’.
The Pharmacist Registration Examination – September 2010 14
The trainee has monthly reviews of their work with their supervisor. During the
review the supervisor checks the logbook and patient records and completes
a review sheet which provides the assessor with an overview of the trainee’s
professional development. The supervisor also gives the trainee a score for
each competency.
To successfully complete the SfR, trainees have to satisfy the assessors with
their level of ‘competence’ in their work. The skills required are set out as a
number of ‘competencies’ falling under categories such as ‘communication
skills’, ‘professional conduct’ and ‘ocular examination and technique’11
which
the trainee has to pass. These are assessed through a process of ‘work
based assessment’, which has two stages.
Stage 1 of the work-based assessment involves the assessment of 75
competencies over a minimum of three visits (usually quarterly throughout the
year). For the assessment of competencies, direct observation is the preferred
method, and is compulsory for 13 specified skills. Where direct observation is
not compulsory, or as a second form of evidence, anything relevant from the
following ‘evidence types’ is acceptable:
• examples of patient records
• logbook signed by supervisor, ophthalmologist or hospital optometrist
• witness testimony
• case scenarios provided by assessor
• questioning by assessor
• field plots
• images provided by assessor
• keratometry readings taken
• prescription interpretation
• referral letters
• verification of supplied spectacles
The Pharmacist Registration Examination – September 2010 15
During the assessments, the Stage 1 assessor:
• observes the trainee carrying out procedures with patients (e.g. a
routine eye examination on a presbyopic patient) – these are planned
with the trainee and they book in appropriate patients in advance so
that the assessor can observe them during the assessment;
• discusses cases from the logbook with the trainee;
• discusses with the trainee the records they have provided as evidence
and ask them questions about photographs of abnormal eye conditions
or visual field plot results which he or she will provide.
Demonstration of the understanding of some skills can be assessed by the
assessor discussing cases with the trainee – where possible these will be
‘real’ cases the trainee has seen, otherwise the assessor will use hypothetical
scenarios. The assessor will review evidence from patient records and
witness testimonies. The assessor will require at least two, and preferably
three, pieces of evidence before they will be satisfied of a trainee’s
competence in any area.
When the Stage 1 Assessor has judged the trainee to be competent in all 75
Stage 1 competencies, they enter Stage 2 of the work-based assessment
process and are allocated a Stage 2 Assessor who is different from the first
assessor.12
The Stage 2 Assessor judges whether the trainee has maintained
their competence in all eight core subjects by assessing:
• the trainee’s ability to carry out an eye examination on a presbyopic
patient - by undertaking this on a simulated patient
• the trainee’s ability to fit soft contact lenses and provide aftercare to a
soft lens wearer – by undertaking these on a simulated patient
• The over-arching competencies – by having case-based discussions
The assessor also confirms that the trainee has completed the GOC’s
refractions and dispensings (spectacles) requirement of a minimum of 350
refractions and 250 dispensings (spectacles).
The Pharmacist Registration Examination – September 2010 16
The final assessment
Once assessed as competent by the Stage 2 assessor, trainees may enter
the final assessment. This is now an Objective Structured Clinical
Examination (OSCE) comprising 14 stations. (This is new for trainees starting
from June 2009, and was previously a two-day final assessment in
examination conditions). Candidates must pass the OSCE before being
eligible for registration with the GOC.
2.3.3 Medicine
2.3.3.1 Basic training requirements and different types of registration
Medical undergraduate degree programmes consist of a five-year degree
course, the Bachelor of Medicine (MBChB). Following attainment of the
MBChB degree, medical trainees enter a two-year ‘foundation training’
programme, during which they are called ‘foundation doctors.’ Provisional
registration with the GMC is required from the start of foundation training.
Successful completion of the first year of foundation training (F1), and passing
the required assessments, allows trainees to apply for full registration with the
GMC. This is followed by a second year of foundation training (F2).
Successful completion of this does not lead to any change in registration
status. After the F2 year, doctors can go on to undertake either GP training or
specialist training, leading to registration as a GP or specialist (consultant).13
2.3.3.2 Details of training and assessment methods
Information presented in this section is taken/adapted from the Foundation
curriculum 2010 14
, unless otherwise indicated.
People involved in the assessment of pre-registration doctors
There is an educational supervisor who is a trainer that is selected to be
responsible for the overall supervision and management of a specified
The Pharmacist Registration Examination – September 2010 17
foundation doctor’s educational progress during a training placement or series
of placements. Local education providers must ensure that educational
supervisors have adequate support and resources to undertake their training
role. This will include training in equality and diversity.
There is also a clinical supervisor who is a trainer that is selected and
appropriately trained to be responsible for overseeing a specified foundation
doctor’s clinical work and providing constructive feedback during a training
placement. Clinical supervisors may change on a day-to-day basis depending
on the rota for each foundation doctor. A clinical supervisor will usually be the
consultant or principal in general practice to whom a foundation doctor is
directly accountable for their clinical work. Some training schemes appoint an
educational supervisor for each placement. The roles of clinical and
educational supervisor may then be fulfilled by the same person.
Other people are also involved in the assessment of trainee doctors; some of
the assessment methods used on the foundation programme specify who can
be involved (for example, see the ‘multi-source feedback’ tool outlined below).
The foundation curriculum states that:
Within any attachment an individual assessor is unlikely to build up a coherent
picture of competences, let alone performance of an individual foundation
doctor. To prevent any individual having undue influence over a doctor’s
progression the educational/clinical supervisor’s overall assessment and
judgement of the foundation doctor must be based on multiple assessments
by many observers.
Assessment – what is assessed and how
Foundation year one takes place entirely in secondary care settings, usually
with three, four-month attachments in medical and surgical settings. Most
learning takes place in clinical areas, but there is protected time for
educational activity.
The Pharmacist Registration Examination – September 2010 18
The foundation programme is designed to work through a process of
continuous assessment, with a formative approach. The programme
curriculum emphasises that assessments should be spread evenly throughout
the year and that assessments should be followed by constructive feedback.
The foundation curriculum states that:
"Feedback is a key component of the interactions between supervisors and
foundation doctors. Giving and receiving feedback and engaging in
constructive conversations about learning, successes, difficulties and
progress are all part of an effective professional learning environment.
Improvement in clinical practice will only happen if regular review leads to
constructive feedback. Unscheduled assessments are a good opportunity for
immediate feedback. This is particularly true of Direct Observation of
Procedural Skills (DOPS) and mini-Clinical Evaluation Exercise (mini-CEX)
which may be opportunistic. It is essential that trainers provide, and
foundation doctors receive, structured feedback.”
The foundation doctor, with the support of the supervisor(s), is responsible for
arranging assessments, having them signed off and recording results. The
evidence should be used to stimulate immediate or early feedback and to
provide a basis for discussion with the clinical and/or educational supervisor.
Foundation doctors undertake assessments and document them in their e-
portfolio. The GMC requires demonstration of competence in a series of
procedures in order for a provisionally registered doctor with a licence to
practise to be eligible for full registration. These are recorded and signed off in
a log book, which is found in the e-portfolio. A completed log book is also
required for successful completion of the foundation programme.
There are five main assessment methods used during the foundation year:
1) Multi-source feedback
2) Direct observation of doctor/patient encounter
3) Case-based discussion
The Pharmacist Registration Examination – September 2010 19
4) Developing the clinical teacher
5) Final assessment
1) Multi-source feedback:
• usually takes place at least once a year; Deaneries have the option of
increasing the frequency;
• incorporates Team Assessment of Behaviour (TAB) which consists of
the collated views from a range of co-workers (previously described as
360-degree assessment). It will be mapped to a self-assessment tool
with identical domains. It is suggested that both F1 and F2 TAB be
taken in the first four months of the year’s training. If there is a risk of
‘rater fatigue’, i.e. overburdening of a small number of colleagues, then
F2 TAB could be undertaken in the second four months of training. If
there are concerns about any foundation doctor, TAB can be repeated
in the last four months of training;
• for each assessment, the foundation doctor should nominate 15 raters.
A minimum of 10 returns are required. No other foundation doctor can
be a rater. The recommended mix of raters/assessors is as follows:
• 2–8 doctors more senior than F2, including at least one
consultant or GP principal;
• 2–6 senior nurses (band 5 or above);
• 2–4 allied health professionals;
• 2–4 other team members including ward clerks, secretaries and
auxiliary staff.
2) Direct observation of doctor/patient encounter
Two tools can be used to assess doctor/patient encounters: the Direct
Observation of Procedural Skills (DOPS) and the mini-Clinical Evaluation
Exercise (mini-CEX).
The Pharmacist Registration Examination – September 2010 20
The DOPS is a structured checklist for assessing the foundation doctor’s
interaction with the patient when performing a practical procedure. Foundation
doctors may submit up to three DOPS as part of the minimum requirements
for evidence assessing doctor-patient encounters; there should also be a
minimum of six mini-CEX per annum. Different assessors should be used for
each encounter wherever possible and each DOPS could represent a different
procedure and may be specific to the specialty. Although DOPS was
developed to assess procedural skills, its primary purpose in foundation years
is to assess the doctor/patient interaction.
The mini-CEX is a structured assessment of an observed clinical encounter.
Foundation doctors should complete a minimum of six mini-CEXs in F1 and
another six in F2. These should be spaced out during the year with at least
two mini-CEX completed in each four month period. A different assessor
should be used for each mini-CEX wherever possible, including at least one of
consultant or GP level, per four month placement. Each mini-CEX must
represent a different clinical problem, sampling one of the acute care, chronic
illness, psychiatric care, etc. (categories listed in the Syllabus and
competences).
Foundation doctors are required to undertake a minimum of nine observed
encounters in both F1 and in F2. At least six of these encounters each year
should use mini-CEX.
3) Case-based discussion (CBD)
The CBD a structured discussion of clinical cases managed by the foundation
doctor. Its strength is assessment and discussion of clinical reasoning. A
minimum of six CBDs should be completed with at least two CBDs undertaken
in any four month period. Different assessors should be used for each CBD
wherever possible. Assessors should have sufficient experience of the area
under consideration, typically higher specialty training, with variations between
specialties. Each CBD must represent a different clinical problem, sampling

The Pharmacist Registration Examination – September 2010 21
one of the acute care, chronic illness, psychiatric care etc (categories listed in
Syllabus and competences).
4) Developing the clinical teacher
Foundation doctors need to demonstrate the knowledge, skills, attitudes and
behaviours to undertake a teaching role. Some of the competencies required
of a clinical teacher include undertaking teaching in under or post-graduate
education in a one-to-one setting, assessing students and other non medical
colleagues in training and contributing to the assessment or review of
students and other colleagues with whom they work. A form is used to aid the
assessment of a foundation doctor’s skill in teaching and/or making a
presentation.
5) Final assessment
Towards the end of a placement, the foundation doctor and educational
supervisor will meet again for an overall assessment. They will review the e-
portfolio and the results of assessments made during the placement. This
process will involve reviewing evidence from colleagues who have observed
the doctor’s performance in practice and/or in individual assessments. This
should include a ‘sign off’ document confirming satisfactory performance and
progress. It should detail any outstanding issues that still need to be
addressed.
The educational supervisor’s role includes having an overview of the
foundation doctors’ assessments. The results of these assessments will be
drawn together and included in a formal structured report by the educational
supervisor. This will cover the overall performance of the doctor in a
placement. Whilst workplace-based assessments (WPBAs) will be taken into
account, the overall judgement will include a triangulated view of the doctor’s
performance. This includes the doctor’s attendance and participation in
educational activities, appraisals, and the assessment process as well as the
recording of all of these activities in an e-portfolio.
The Pharmacist Registration Examination – September 2010 22
The outcome of the final assessment discussion should be agreed by both the
foundation doctor and the educational supervisor and recorded in the doctor’s
e-portfolio ‘end of placement review’ form. Placement reports put together in
an annual report will form the basis of the foundation training programme
director/tutor’s recommendations of satisfactory completion of F1 and the
foundation programme.
2.3.4 Dentistry
2.3.4.1 Basic training requirements and different types of registration
On completion of a five-year Bachelor of Dental Surgery (BDS), dental
graduates can apply for full registration with the General Dental Council
(GDC). Full registration allows the practice of dentistry without supervision.
This means that it is legal for a dentist to practise privately with no further
training following their BDS; however, many dentists will continue with further
training before practice. The GDC also holds 13 ‘specialist lists’ for particular
branches of dentistry.15
Once registered, dentists can undertake further
training in specialist areas to allow them to apply for registration on the 13
‘specialist lists’ held by the GDC. Any registered dentist can work in a
particular field of dentistry (such as orthodontics or oral surgery), but only
those on a specialist list can call themselves a 'specialist'.
In October 2005, the Department of Health asked the General Professional
Training (GPT) Liaison Group UK to take forward the development of a
curriculum for foundation programmes in dentistry in the UK. The proposed
two-year dental foundation programme is broadly comparable to the
structured two year GPT programme which has been available for a
proportion of graduates in the UK.
The proposed curriculum for dental foundation training was published by the
Committee of Postgraduate Dental Deans and Directors (COPDEND) which
sets out a two-year foundation programme. The first year is equivalent to the
The Pharmacist Registration Examination – September 2010 23
one year ‘vocational training’ and is spent in primary care, providing NHS
general dental services. The remainder of the two year programme can be
completed in a variety of primary and secondary care settings. The
COPDEND policy statement specifies that the aim of dental foundation
training is: ‘To enable the acquisition and demonstration of dental foundation
training competences, the evidence of which could, in the future, contribute to
that required for a first validation with the GDC following initial registration.’
The curriculum was formally launched by the Chief Dental Officer (England)
on 15 November 2006.
2.3.4.2 Details of training and assessment methods
People involved in the assessment of pre-registration dentists
The Bachelor of Dental Surgery (BDS):
The BDS is a five year course provided by higher education institutions. The
GDC specified ‘learning outcomes’ which must be achieved in order to
register as a dentist and the GDC accredits BDS programmes. There is
variation between the BDS courses in the different dental schools, but they all
meet the requirements for the outcomes. The examinations and any other
assessments that have to be passed as part of the BDS can therefore be
called ‘professional examinations’ in the sense that they are the gateway to
registration.
Foundation training:
The proposed curriculum (described above) states that: Individuals
responsible for judging the performance of dental foundation programme
trainees should be appropriately qualified, have relevant expertise and be
adequately prepared for their role through training.
The Pharmacist Registration Examination – September 2010 24
Assessment – what is assessed and how
The Bachelor of Dental Surgery (BDS):
For the BDS, the GDC defines the overarching outcomes that span four
domains.16
The overarching outcomes should be demonstrated throughout
education and training.
Overarching outcomes:16
Upon registration with the GDC the Registrant will be able to:
• Practise safely and effectively, making the high quality long term care
of patients the first concern
• Apply an evidence-based approach to learning, practice, clinical
judgment and decision making
• Accurately assess own capabilities and limitations, demonstrating
reflective practice, in the interest of high quality patient care and act
within these boundaries
• Recognise the role and responsibility of being a registrant and
demonstrate professionalism throughout education, training and
practice in accordance with GDC guidance
These four domains are; clinical, communication, management and leadership
and professionalism. Registrants must be able to demonstrate a variety of
outcomes that include activities such as describing, explaining, discussing,
recognising, implementing, managing, assessing, monitoring and evaluating.
The GDC state that assessments must be ‘rigorous, appropriate and reliable
as a gateway for students to become qualified to practise independently’, but
it is open to each HEI as to how they perform the assessment.16
Foundation training:
The proposed curriculum states that the type of assessment used should
reflect the stage in training (i.e. postgraduate). Also, the dental foundation
The Pharmacist Registration Examination – September 2010 25
programme is more focussed on assessing ‘performance outcomes’ and less
on the achievement of individual competencies. The curriculum states:
…it is recommended that within postgraduate dental training, assessment
should be at the highest level of Miller’s pyramid wherever possible i.e. what
the practitioner ‘does’. At this level, we are looking at the assessment of
‘performance’ rather than ‘competence’, which is an appropriate approach for
training within the workplace where the integration of individual competencies
into the ‘whole task’, and a consistent approach to practice is required for the
delivery of high quality patient care. 17
The curriculum outlines to a number of assessment methods which are
considered potentially appropriate for dental foundation training. These are
outlined below.
Workplace-based assessment using observation of performance:
Assessment methods using direct observation of performance in the
workplace frequently have high validity. There are two main approaches to
scoring performance – checklists and the use of global ratings. In brief,
methods using checklists are usually specific to the task being assessed. The
task is divided procedurally into stages or skills and the evaluator identifies
whether or not each stage has been performed correctly. The advantages of
this approach are that very detailed and structured feedback can be provided
on individual tasks. This may be particularly useful at earlier stages of
professional development such as undergraduate training, the mastery of
more complex tasks at postgraduate training, or for targeted training when
addressing poor performance. The use of global ratings to measure observed
performance has been shown to have many advantages at the postgraduate
level, including more flexibility, and enhanced validity. Ratings are usually
provided along a scale (e.g., 6, 8 or 9 points) with performance descriptors,
and across several broad areas of performance that may be clinically-
orientated (e.g. ‘history taking’, ‘clinical judgement’) or generic (e.g.
The Pharmacist Registration Examination – September 2010 26
‘professionalism’, ‘communication skills’). The majority of methods that are
currently being piloted, in postgraduate dental education, use global ratings.
LEP (Longitudinal Evaluation of Performance)
The LEP uses global ratings on a 9-point scale (1-3 = ‘Need Improvement’, 4-
6 = ‘Satisfactory’, 7-9 = ‘Superior’ performance) to score trainees’
performance in several clinical and generic areas. This approach was adapted
from the mini-CEX, specifically for use within postgraduate dental training (VT
and GPT). Evaluation of the LEP to date has indicated high validity and a
positive educational impact. Specific features of the tool include:
• high flexibility (can be used across the whole curriculum)
• continuous assessment
• judgements are made against a reference point that is the standard
expected upon completion of the training, allowing the demonstration of
progress and the identification of strengths and weaknesses at an early
stage.
• high quality feedback for trainees and trainers.
• a ‘no penalty’ approach to assessments where scores are awarded in
the ‘need improvement’ range, reducing the likelihood of leniency/halo
effect and the potential for demotivation of trainees.
Mini-CEX (Clinical Evaluation Exercise)
Developed in the U.S.A. by Dr John Norcini, this tool has had wide
international success, and was one of the first methods of this kind, from
which many others (including the LEP) have been developed. Evolving from
the more detailed and time consuming ‘CEX’, the mini-CEX was designed to
take a ‘snapshot’ of performance and enhance feasibility and flexibility within
the workplace. Recent changes to the tool, for its use within medical
foundation programme pilots, include the move from a 9-point to a 6-point
scale, with descriptors highlighting that evaluators judgements are made
The Pharmacist Registration Examination – September 2010 27
against the standard expected upon completion of F1 or F2. Previously,
judgements were made in relation to the trainee’s current stage in training.
DOPS (Direct Observation of Procedural Skills)
Originally developed and evaluated by the Royal College of Physicians,
DOPS is a method similar to the mini-CEX that has been designed specifically
for the assessment of practical skills. This tool uses the same rating scale and
descriptors as the mini-CEX used in medical foundation programme pilots, but
against areas that resemble more of a structured checklist for practical
procedures.
CbD (Case-based discussion)
Also being used within medical foundation pilots, CbD allows case
presentation and subsequent discussions with evaluators/trainers to be
recorded. CbD assesses clinical judgement and the application of knowledge
with regard to patient care. It is also used in the USA for poorly performing
doctors, as it allows the decisions and thought processes of practitioners to be
probed by the evaluator.
PAQ (Patient Assessment Questionnaire)
Designed specifically for the assessment of dentists in postgraduate training,
the PAQ has good validity and reliability in primary care (vocational training)
and is now being piloted in the SDS and HDS. The PAQ asks patients to
anonymously provide ratings on a 5-point scale (poor, fair, good, very good
and excellent) for areas of communication skills and professionalism. This
data can be triangulated with that from other assessments such as the LEP, to
compare the trainers and patients views of these areas of performance.
The Pharmacist Registration Examination – September 2010 28
Mini-PAT/Min e-PAT (Peer Assessment Tool)
A method of multi-source feedback for trainees, the mini-PAT is also being
piloted at present in medical foundation programmes. Multi source feedback
can assess multiple components of performance.
Dental VT/GPT ‘Test of Knowledge’
Used alongside the LEP and PAQ in Scotland, within the system of
assessment for satisfactory completion of VT and GPT, this test is computer-
based and focuses on aspects of knowledge that are developed within this
training such as health and safety in practice, practice organisation, NHS rules
and regulations etc. It does not include clinically related questions that may
have previously been assessed at an undergraduate level.
2.3.5 Summary/comparison of the different professions
By comparing pharmacy, optometry, medicine and dentistry in GB we have
been able to draw out some of the similarities and differences between the
processes of registration between these healthcare professions. All of the
training programmes use portfolios and there is a focus on ‘continuous
assessment.’ The trainee collects pieces of evidence and has to record these
and ‘map’ them onto the competencies that they have to achieve. With all the
postgraduate training programmes, trainees spend most of their time in a
practice setting. The amount of time they spend in university varies, for
example pharmacy pre-registration trainees attend ‘study days’ at the
university whereas optometry trainees do not come to the university for
anything. There are, however, a number of differences in terms of the
implementation of formative and summative assessments.
In pharmacy, the specific assessment methods for each competency are less
strictly prescribed than they are in the medical foundation programme. For
example, the medical foundation curriculum states that ‘competence 2.1 –
Eliciting a history’ is assessed via mini-CEX and CBD. Throughout the
curriculum most competencies have methods of assessment specified. In the
The Pharmacist Registration Examination – September 2010 29
pharmacy pre-registration workbook, the focus seems to be more on providing
proof that a competence has been ‘met’, and the workbook specifies forms of
documentary evidence that can be used, but is less specific about the actual
assessment tools that can be employed.
There is less specification in the assessment tools that pharmacy trainees
could be ‘subject’ to for example, the final assessment for all optometry
trainees is an OSCE, whereas the pharmacy pre-registration programme does
not specify that trainees will be assessed through OSCEs. However, in
practice, they may take part in OSCEs as part of a university study day, and
the results from this could form part of the evidence used to achieve the
competencies.
In terms of the timings of assessments, the pharmacy and optometry
programmes are similar in that they have scheduled quarterly assessments,
whereas medical foundation trainees are responsible for organising their own
assessments, by finding suitable cases and asking colleagues to assess
them. This puts more onus on the trainee to manage their own time (and
learning).
In terms of who assesses the trainee, pharmacy pre-registration trainees have
a tutor who acts as their supervisor on the work premises and also takes the
role of the assessor (through performance reports). In optometry there is a
supervisor on the premises, but an independent assessor goes in quarterly to
‘sign off’ the trainee’s evidence against the competencies. Medical foundation
trainees are ‘formally’ assessed by a greater range of people. For example,
for team-based assessment, there are recommendations on who should be
included in this, including other health care professionals. Furthermore, there
is a clinical as well as an educational supervisor. While a pre-registration
trainee could potentially include a testimonial from a nurse who had observed
their work on a hospital ward as evidence in their portfolio, this is not a
requirement in medicine. The process of obtaining feedback from a wider
range of colleagues is much more formal and established in medicine.
The Pharmacist Registration Examination – September 2010 30
Pharmacy is the only profession with formal written examinations at the end of
the postgraduate pre-registration training period, although if we include the
methods of assessment used on the BDS, then pharmacy and dentistry have
the most similar assessment methods in place – trainees are assessed using
written examinations in MCQ format (dentistry also has short answers).
The training programme for dentistry is unique among the professions
included in this review in that a bachelor degree, which is not ‘graded’ but
simply awarded with a ‘pass’, allows registration with the regulatory body.
Therefore, postgraduate trainees are already members of the profession from
the start of their postgraduate training. At the moment, dental vocational
training is not formally assessed, although a curriculum for dental foundation
training has been published, which sets out the assessment methods that are
likely to be used for this. However, whereas doctors must successfully
complete their F1 year to be eligible for full professional registration, this is not
the case for dentists. 18
The proposed foundation programme for dentistry has been designed to
follow the medical training model in that it is a two year practice-based
programme, using many of the same assessment tools. However a key
difference is that whereas the majority of medical postgraduate training takes
place in hospitals, it is compulsory for dentists to complete a year of
postgraduate training in primary care. (The majority of dentists practise in
general or personal dental practice.) Also, the dental foundation programme is
more focussed on assessing ‘performance outcomes’ and less on the
achievement of individual competencies.
Pharmacy and dentistry have only one ‘level’ or type of registration, whereas
medicine has four types on three levels – provisional (F1), full and then GP or
specialist (following specialist training). Student optometrists have to register
with the GOC from the start of their undergraduate training, and then apply for
full registration after passing the scheme for registration. While all practising
pharmacists have to undertake continuing professional development to
maintain their registration, and there are ‘higher’ qualifications which

The Pharmacist Registration Examination – September 2010 31
pharmacists can undertake, such as the hospital diploma, there is only one
level of professional registration.
With medicine, trainees have to successfully complete their F1 year to be
eligible for full registration. However, the assumption is that their ‘training’ will
not stop there, as the F2 curriculum sets out a further year of competencies
that doctors must achieve, with the aim of going on to specialist training,
which leads to specialist registration. This model provides a clear path that
medical trainees follow which suggests a higher level of practice, and
eventually (on completion of specialist training) a higher level of registration.
For example, the foundation curriculum states: ‘A key feature of the F2
curriculum is that all doctors must develop competencies at a significantly
higher level than those acquired in the F1 year’.14
The Pharmacist Registration Examination – September 2010 32
Findings for pharmacy in countries outside GB
This section of the report focuses on pharmacy registration requirements for a
selection of countries outside GB, specifically: Australia, New Zealand,
Canada and USA. These were selected as they are English speaking and
have similar healthcare systems and particularly arrangements for pharmacy
education and training, and registration.
2.3.6 Australia
2.3.6.1 Basic training requirements and different types of registration
Australian pharmacy undergraduate degree programmes consist of a four-
year bachelor’s degree, the BPharm. Following attainment of the BPharm
degree, the graduate must register with the Pharmacy Board of Australia and
undertake a period of supervised practice of 1824 hours (e.g. 38 hours per
week for 48 weeks) and also pass an examination. They can then apply for
‘general registration’.
Previously, there was a registering authority (a Pharmacy Board) in each state
and territory of Australia that was responsible for registration and regulation of
pharmacy within that jurisdiction. As of 1st July 2010 the state registering
authorities were decommissioned and all registration and regulation issues
are now the responsibility of the newly established Pharmacy Board of
Australia. Registrants have national registration that enables them to work
anywhere in Australia without having to re-register (and pay a fee) in each
state they wish to practise. This is part of the Intergovernmental Agreement on
the Australian health workforce, which has created a single national
registration and accreditation system for 10 health professions (chiropractors,
dental care practitioners, medical practitioners, nurses and midwives,
optometrists, osteopaths, pharmacists, physiotherapists, podiatrists, and
psychologists).19
The internship year (the year following the BPharm – similar to the pre-
registration year in Great Britain) is generally undertaken in a hospital or
The Pharmacist Registration Examination – September 2010 33
community setting; a small number undertake their training in an industry
setting. Graduates of the BPharm in Australia are required to hold provisional
registration in order to complete an internship. Interns must complete
supervised practice and pass the Board Registration Examination.
2.3.6.2 Details of training and assessment methods
People involved in the assessment of pre-registration trainees
The Pharmacy Board of Australia stipulates the following requirements for
supervised practice:
• each period of supervised practice is undertaken under the direction
and/or supervision of a preceptor approved by the Board for a minimum
period of 152 hours;
• it must be under the direct supervision of a pharmacist who holds
general registration (not necessarily the approved preceptor).
Note that some of the assessment methods outlined below include additional
specifications for the training of those carrying out certain types of
assessment.
Assessment – what is assessed and how
Supervised practice is undertaking pharmacy practice under the direct
supervision of a pharmacist who holds general registration (a preceptor), while
the pharmacist is providing pharmacy services in pharmacy premises or other
circumstances as determined by the Board.
Previously, each state had its own ‘Intern training programme’. The
Pharmaceutical Society of Australia is the largest provider of Intern training
programmes in Australia, and has now developed a National Intern Training
Program. The National Intern Training Program will be rolled out in most
states and territories of Australia in 2010 and 2011.20 At the time of writing,
The Pharmacist Registration Examination – September 2010 34
there was no guidance available specifying the detail of this national
programme. Without this, a description of the pharmacy intern programme
was taken from a paper by Marriott et al. in the American Journal of
Pharmaceutical Education.21
Requirements of the intern programme include:
• completion of an accredited education programme such as that
provided by the Pharmaceutical Society of Australia, Monash
University, and others;
• passing the competency-based pharmacy board examinations. The
structure of the pharmacy board examination used to vary somewhat
between states but generally took the form of an oral examination at
the end of the internship and could involve an OSCE;
• pass a law and ethics examination;
• a calculations examination;
• an Australian Pharmacists Competency Assessment Test (APCAT);
• a demonstration of satisfying the competency standards for
pharmacists in Australia (see below).
The competency standards are grouped into eight ‘functional areas’:
•
•
practise pharmacy in a professional and ethical manner
•
manage work issues and interpersonal relationships in pharmacy
practice
•
promote and contribute to optimal use of medicines
•
dispense medicines
•
prepare pharmaceutical products
•
provide primary health care
•
provide medicines and health information and education
apply organisational skills in the practise of pharmacy
The Pharmacist Registration Examination – September 2010 35
The competency standards for pharmacists in Australia documentation22
outline six ‘suggested’ assessment methods for the required competencies
which are outlined below.
1) Supervisor observation
(Following training) Supervisors observe the trainee in the workplace to
assess competence. A prepared checklist over a period of time, taking into
account varying conditions in the workplace, is often used. Appraisals of
aspects of competency may also be conducted. Appraisal can include:
•
•
application to work;
•
quality of work;
•
attitude to clients;
•
attitude to co-workers;
personal behaviour/professional attitude.
2) Written assignments/examinations
Written assignments/examinations can include practice-based reports, open-
book assignments and written examinations. These are outlined below:
Practice-based reports Can include case studies relating to:
• prescriptions;
• primary health care;
• consumer medication records;
• reports of extemporaneous preparations undertaken.
(In industrial placements, involvement in manufacturing process of products
may be reported.)
Open-book assignments
A series of practice-based questions covering broad areas of competence to be
answered and submitted for assessment.
The Pharmacist Registration Examination – September 2010 36
Written examinations
Practice-based questions may be closed- or open-book and can be in the form of:
• short answers;
• multiple-choice questions;
• essays.
3) Oral interview
The oral interview is an interview that consists of practice-based questions.
Prescription and primary care cases can be used to assess:
• knowledge;
• communication skills;
• application of theory to practice;
• professional decision making, judgement and attitudes.
An oral interview relies on experienced practitioners who are trained
assessors for objectivity, reliability and validity. Preferably, two assessors
should examine together and come to an agreed interpretation of the
candidate’s competence with reference to the Performance Criteria and pre-
established decision rules.
4) Objective structured examination
The objective structured examination is a series of stations structured to each
assess an aspect of competence. The objective structured examination is a
method of assessing practical and clinical skills which brings together several
testing methods. There are two broad categories of stations:
• At procedure stations an activity or practical procedure is carried out
e.g. dispensing a prescription; counselling a ‘consumer’. (A marker with a
checklist and scoring card notes the candidate’s performance.)
• At question stations written answers to open-ended or multiple choice
questions are given. After a given period, candidates move on to the next
station in response to a given signal. The time allowed should be the
The Pharmacist Registration Examination – September 2010 37
same for each station to simplify the rotation. All candidates rotate
through the same stations.
5) Practical examination
The practical examination focuses on candidates’ ability at dispensing
simulated prescriptions for proprietary and/or extemporaneous preparations
under examination conditions.
6) Evidence of prior learning
This is assessed by having candidates provide evidence of aspects of
competency previously assessed satisfactorily by other sources. Evidence
may include:
• certification of courses successfully undertaken;
• record of hours of practical training undertaken;
• log book of practical experiences.
2.3.7 New Zealand
2.3.7.1 Basic training requirements and different types of registration
Pharmacy undergraduate degree programmes in New Zealand consist of a
four-year bachelor’s degree, the BPharm. Graduates must then register as an
intern with the Pharmacy Council of New Zealand and complete a minimum of
44 weeks practical training in a pharmacy alongside an intern programme run
by the Pharmaceutical Society of New Zealand (named EVOLVE)23
. The
EVOLVE Intern Programme runs concurrently with the practical training period
and is the training and assessment that occurs around that work experience.
Successful completion of these allows application for full registration as a
pharmacist.
The Pharmacist Registration Examination – September 2010 38
2.3.7.2 Details of training and assessment methods
People involved in the assessment of pre-registration trainees in New Zealand
All New Zealand graduate interns must undertake supervised practice, under
an approved preceptor pharmacist in an approved site. Preceptors must:
• be pharmacists with three years post-registration experience
• have completed the training for a preceptor as currently required by the
Pharmacy Council. Currently this is Workplace Assessor Training Unit
Standard 4098 on the New Zealand Qualifications Authority (NZQA)
framework; ‘Use standards to assess candidate performance’. (The
NZQA is a national organisation that oversees qualifications.)
Assessment – what is assessed and how
The EVOLVE Intern Programme24
, run through the Pharmaceutical Society of
New Zealand, is an achievement based programme based on a set of
competence standards that describe the knowledge, skills and attitudes
required of a newly registered pharmacist. The preceptor conducts three
assessments during the year, against the competence standards.
The final assessment
Trainees attend an Assessment Centre where they are assessed by trained
assessors.25
The final assessment involves an oral interview conducted by
two assessors and a five station OSCE assessing application of clinical
knowledge and professional competence for a range of practice scenarios.
2.3.8 Canada
There are 12 regulatory authorities with responsibility for the registration or
licensing of pharmacists within their areas in Canada – one for each province
or territory, apart from Nunavut, which is included within the remit of the
The Pharmacist Registration Examination – September 2010 39
Northwest Territories Department of health and social services. This
department specifies that to be ‘licensed’ pharmacists must have passed the
Pharmacy Examining Board of Canada (PEBC) examination, but there are no
other requirements regarding practical experience etc. No other details about
registration of pharmacists in the territories were found.
2.3.8.1 Basic training requirements and different types of registration
The number and type of registration categories varies between provinces, for
example, Alberta has five: clinical, associate (non-practising), retired, student
(undergraduates) and provisional (interns) while Ontario has three: student,
intern and registered pharmacist.
The National Association of Pharmacy Regulatory Authorities (NAPRA) has a
‘national model licensing programme’ which sets core requirements for initial
licensure of pharmacists. These are:
• a degree in pharmacy (BSc); Canadian undergraduate degree
programmes consist of a four-year course, however, these require
completion of a one-year ‘pre-pharmacy’ university course to be
undertaken before entry;
• passing the ‘Pharmacist Qualifying Examination’ set by the PEBC;
• pharmacy jurisprudence requirements – assessed by a ‘jurisprudence
examination’ set by the provincial regulatory authority;
• practical experience/training period, during which time the professional
competencies are assessed.
There are also language fluency requirements, but applicants who have
received an accredited Canadian or American university degree in pharmacy
will not be required to undergo further testing unless a ‘trigger’ suggests that a
test for language proficiency is necessary.
The Pharmacist Registration Examination – September 2010 40
2.3.8.2 Details of training and assessment methods
People involved in the assessment of pre-registration trainees in Canada
For structured practical training, each pre-registration trainee or candidate is
supervised and assessed by a recognized preceptor. To be recognized as a
preceptor, the pharmacist must:
• be a member in good standing of a Provincial or Territorial Regulatory
Authority;
• have at least 12 months experience as a licensed pharmacist;
• hold a ‘practising’ or ‘active’ licence and be practising in a patient care
setting with direct patient interaction;
• have undertaken a preceptor training program offered by an accredited
university or the Regulatory Authority.26
Assessment – what is assessed and how
The profession of pharmacy is regulated on a provincial level. The provincial
regulatory authorities are directly responsible for granting pharmacist licenses,
assessing the competency of pharmacists and ensuring public safety.
NAPRA defined a set of seven competencies required of pharmacists at the
point of licensure. Each competency has a number of elements, of which
there are 37 in total. 27
1) Patient Care
2) Professional Collaboration and Team Work
3) Ethical, Legal and Professional Responsibilities
4) Drug, Therapeutic and Practice Information
5) Communication and Education
6) Drug Distribution
7) Management Knowledge and Skills
The Pharmacist Registration Examination – September 2010 41
In early 1998, NAPRA's National Licensing Standards Committee (NLSC)
identified 19 of the 37 Competency Elements as being optimally assessed
through a structured practical training program. It was recommended that
these particular competencies require observation of performance to
determine the ability of the pre-registration trainee or candidate and that
further, the observations should occur over a period of time to ensure that
performance can be sustained. Accordingly, a structured practical training
framework was developed.
The framework for assessing competencies states that:
The structured practical training experience and assessment should ideally be
incorporated into the undergraduate academic program. However, it is
acknowledged that the Canadian Council for Accreditation of Pharmacy
Programs' (CCAPP) current minimum criterion of 16 weeks practical training
experience may not provide sufficient time to assess all the required
competencies. In such cases, an internship program administered and
supervised by the Provincial Regulatory Authority would be required. The total
practical training experience with assessment could be carried out through a
partnership arrangement between the Provincial Regulatory Authority and the
Faculty, determined on a province-by-province basis.
Programs should be focused on measuring or assessing the actual attainment
of competencies, which is not directly related to time spent. Therefore, the
group's further suggestion that the total time required for completion of a
structured practical training program prior to licensure be not less than 24
weeks (840 hours) is offered as an example. Using this example, the following
schedule of internship training is offered as a possible option to consider for
candidates enrolled in accredited in-province and domestic pharmacy
programs.
The candidate might complete 280 hours of practical experience over eight or
more weeks during the first three years of enrolment, as follows:

The Pharmacist Registration Examination – September 2010 42
• Year 1: 70 hours over at least 2 weeks
• Year 2: 70 hours over at least 2 weeks
• Year 3: 140 hours over at least 4 weeks
Practical experience obtained over an extended period of time allows for
integration with the didactic program and can result in an optimal learning
opportunity. In Year 4 the period of structured practical training might be 560
hours over sixteen weeks, scheduled in blocks of at least 140 hours/four
weeks duration and involve sites that offer different types of experiences.
In practice, each pharmacy regulatory body has its own provincial
requirements. Before gaining a license to practise, trainees may gain practical
experience which is included within their undergraduate programme, or they
may be required to undertake an ‘internship’ which takes place after they have
graduated. The requirements for how much time is required in each of these
types of training varies between provinces.
For example, in Alberta, the undergraduate degree programme includes 900
hours of structured practical training (SPT). After graduating, trainees must
complete 100 of SPT as an intern and follow the Post-Graduate Structured
Practical Training and Evaluation Guide for Alberta Pharmacist Interns which
assesses the entry to practice competencies of the pharmacist intern in a
structured, 100 hour timeframe while practising in a typical practice setting. In
Ontario, in the fourth year of the degree programme, undergraduates
participate in 16-weeks of supervised training in field placements where they
apply in-class learning and are evaluated with university-affiliated pharmacists
in actual pharmacy settings. Following graduation, to register with the Ontario
College of Pharmacists, graduates must successfully complete a minimum 12-
week SPT internship while registered with OCP as an intern.
The jurisprudence examination
Provincial requirements vary, but the examinations are generally based on the
regulatory body’s standards and policies, and Federal and Provincial acts and
their regulations, which control the production, distribution, advertising, sales
The Pharmacist Registration Examination – September 2010 43
and use of drugs in a particular province and assess the pre-registration
trainee knowledge, ability to interpret and apply all legislation that impacts on
current pharmacy practice. For example, in Alberta, the ethics and
jurisprudence examination is undertaken online, at a testing centre, is closed
book, in MCQ format and lasts for two hours. In Ontario, alternatively, the
examination is a written, MCQ format, lasting two and a half hours.
The PEBC examination
This examination has two parts, a written component in MCQ format and an
OSCE. Part I consists of two MCQ papers, taken in two sittings over two
consecutive days. Each sitting (examination period) is 3.75 hours in length.
Part II is a 16-station (plus four rest stations) OSCE, undertaken over a
maximum of six hours, with breaks. The examinations are undertaken on the
same days throughout the whole of Canada.
2.3.9 USA
2.3.9.1 Basic training requirements and different types of registration
Each of the 51 states in the USA has its own board of pharmacy, and there
are some variations in requirements for registration between states, however,
generally, these are:
• Attainment of a Doctor of Pharmacy (PharmD) - there are pre-
pharmacy requirements which precede entry to the PharmD, which
usually involve at least one year of university education;
• passing the North American Pharmacist Licensure Examination
(NAPLEX) examination;
• passing a jurisprudence examination (44 states and the District of
Columbia require that applicants pass the Multistate Pharmacy
Jurisprudence Examination (MPJE), while those states that do not
require the MPJE have their own law examination);
• fulfilling practical experience requirements.
The Pharmacist Registration Examination – September 2010 44
The categories of ‘licence’ vary between states but include student, intern,
‘standard’ and speciality categories.
2.3.9.2 Details of training and assessment methods
People involved in the assessment of pre-registration trainees in the USA
According to standard number 14 of the accreditation guidelines stipulated by
the Accreditation Council for Pharmacy Education (ACPE)28
, throughout the
practical training (i.e. practice based experience) of a pharmacist in the USA
there is a preceptor on site that can work with the trainee. According to the
guidelines a ‘Preceptor should hold full, shared, adjunct, or other defined
positions in the college or school and should be well versed in the outcomes
expected of students and the pedagogical methods that best enhance
learning. In this regard, the college or school must ensure that preceptors
receive orientation, especially for first-time preceptors prior to assuming their
responsibilities, ongoing training, and development. Preceptors should provide
close supervision of and significant interaction with students. The student-to
preceptor ratio for the pharmacy practice experiences should be adequate to
provide individualized instruction, guidance, supervision, and assessment.’
Assessment – what is assessed and how
The NAPLEX
The NAPLEX was designed to measure a candidate’s knowledge of the
practice of pharmacy. It is one component of the licensure process and is
used by the boards of pharmacy as part of their assessment of a candidate’s
competence to practise as a pharmacist. The 185-question examination tests
a prospective pharmacist’s ability to measure pharmacotherapy and
therapeutic outcomes, prepare and dispense medications, and implement and
evaluate information for optimal health care. Many of the questions are asked
The Pharmacist Registration Examination – September 2010 45
in a scenario-based format. For example, a patient profile is provided, and the
candidate must answer a series of questions related to the profile.
The NAPLEX is computer-based and uses adaptive technology to deliver
selected-response and constructed-response questions. Computer adaptive
testing (CAT) successively selects questions so as to maximize the precision
of the examination based on what is known about the examination from
previous questions. From the examinee's perspective, the difficulty of the
examination seems to tailor itself to his or her level of ability. For example, if a
candidate performs well on an item of intermediate difficulty, they will then be
presented with a more difficult question. Or, if they performed poorly, they
would be presented with a simpler question. Compared to static tests, with a
fixed set of items administered to all examinees, computer-adaptive tests
require fewer test items to arrive at equally accurate scores.29
The Multistate Pharmacy Jurisprudence Examination (MPJE)
The MPJE combines federal- and state-specific questions to test the
pharmacy jurisprudence knowledge of prospective pharmacists. It serves as
the pharmacy law examination in participating jurisdictions. Each board of
pharmacy approves questions applicable in that state or jurisdiction. The
MPJE is a two-hour, computer-adaptive examination that consists of 90
multiple-choice test questions. The MPJE tests candidates on:
• legal aspects of pharmacy practice, including responsibilities with
regard to the distribution and dispensing of pharmaceuticals and for the
care of patients;
• licensure, registration, certification, and operational requirements;
• regulatory structure and terms of the laws and rules that regulate or
affect pharmacists, pharmacies, manufacturers, and distributors.30
The Pharmacist Registration Examination – September 2010 46
Practical experience requirements
Requirements are set by each state pharmacy board. There may be slight
differences in the requirements for the number of hours spent in practice.
The ACPE is the national agency for the accreditation of professional degree
programs in pharmacy and providers of continuing pharmacy education. The
ACPE specifies a number of ‘Professional competencies’ and ‘Outcome
expectations’ for PharmD programmes.28
Professional competencies that
must be achieved by graduates through the professional degree program
curriculum are the ability to:
• Provide patient care in cooperation with patients, prescribers, and other
members of an inter-professional health care team based upon sound
therapeutic principles and evidence-based data, taking into account
relevant legal, ethical, social, cultural, economic, and professional
issues, emerging technologies, and evolving biomedical,
pharmaceutical, social/behavioural/administrative, and clinical sciences
that may impact therapeutic outcomes;
• Manage and use resources of the health care system, in cooperation
with patients, prescribers, other health care providers, and
administrative and supportive personnel, to promote health; to provide,
assess, and coordinate safe, accurate, and time-sensitive medication
distribution; and to improve therapeutic outcomes of medication use;
• Promote health improvement, wellness, and disease prevention in
cooperation with patients, communities, at-risk populations, and other
members of an inter-professional team of health care providers.
These professional competencies must be used to guide the development of
stated learning outcome expectations for the pre-registration curriculum. To
anticipate future professional competencies, outcome statements must
incorporate the development of the skills necessary to become self-directed
lifelong learners. These competencies can, however, be difficult to assess.
The Pharmacist Registration Examination – September 2010 47
The issue of ‘pharmacy’ competencies and their assessment has received
attention from those concerned with the assessment of pre-registration
trainees in the USA. A paper by Ried and colleagues reports work undertaken
to develop a standardised performance measure for ‘practical experiences’ at
three colleges in Florida.31
Each college had used a different tool for
assessing students' clinical competencies. This was burdensome and
confusing for the preceptors. In response, some preceptors developed and
used their own forms instead of the colleges' forms. This lead to faculty from
the state's three colleges of pharmacy collaborating to develop a standardized
assessment tool: the System of Universal Clinical Competency Evaluation in
the Sunshine State (SUCCESS).
Graduates must possess the basic knowledge, skills, attitudes, and values to
practise pharmacy independently at the time of graduation. In this regard, the
college or school must ensure that graduates are competent to:
• provide patient-centred care, through the ability to design, implement,
monitor, evaluate, and adjust pharmacy care plans that are patient-
specific; address health literacy, cultural diversity, and behavioural
psychosocial issues; and are evidence-based;
• manage a successful patient-centred practice (including establishing,
marketing, and being compensated for medication therapy
management and patient care services rendered);
• provide population-based care, through the ability to develop and
implement population-specific, evidence-based disease management
programs and protocols based upon analysis of epidemiologic and
pharmacoeconomic data, medication use criteria, medication use
review, and risk-reduction strategies;
• manage human, physical, medical, informational, and technological
resources, through the ability to ensure efficient, cost-effective use of
these resources in the provision of patient care;
• manage medication use systems, through the ability to apply patient-
and population-specific data, quality improvement strategies,
medication safety and error reduction programs, and research
The Pharmacist Registration Examination – September 2010 48
processes to minimize drug misadventures and optimize patient
outcomes; to participate in the development of drug use and health
policy; and to help design pharmacy benefits;
• promote the availability of effective health and disease prevention
services and health policy through the ability to apply population-
specific data, quality improvement strategies, informatics, and research
processes to identify and solve public health problems and to help
develop health policy.
To be capable of the above, pharmacy graduates also must be able to:
• communicate and collaborate with patients, care givers, physicians,
nurses, other health care providers, policy makers, members of the
community, and administrative and support personnel to engender a
team approach to patient care;
• retrieve, analyze, and interpret the professional, lay, and scientific
literature to provide drug information and counselling to patients, their
families or care givers, and other involved health care providers;
• demonstrate expertise in informatics;
• carry out duties in accordance with legal, ethical, social, economic, and
professional guidelines;
• maintain professional competence by identifying and analyzing
emerging issues, products, and services.
2.3.10 Summary/comparison of the different countries
This section draws out some of the similarities and differences between the
training and registration procedures for pharmacy across the different
countries.
Our research has found that the length of time required to become a qualified
pharmacist is typically five years. In the USA it may also take six years if a
pre-pharmacy course is carried out for two years prior to the four year doctor
of pharmacy. The way that these years are formatted differs between the
The Pharmacist Registration Examination – September 2010 49
countries that were compared. For example, the systems existent in GB,
Australia and New Zealand generally require students to complete a
pharmacy degree, followed by a year of supervised practice. The USA seems
somewhat different, in that practice experience is integrated more with links to
colleges and schools of pharmacy, and courses may indeed differ depending
on the college or state one is training in. In Canada there appears to be more
integration of practice into the earlier years of the course rather than
segmenting the educational (taught in university/college) and practical side of
pharmacy.
Findings from this research also highlight differences in terms of the people
who are involved in the practical training of pre-registration trainees. There is
at least one individual that is intimately involved in the training and
assessment of pre-registration pharmacists: a tutor or ‘preceptor’ with a
required amount of experience in practising pharmacy. Although there is an
indication that these individuals may receive some orientation and support in
their role as a preceptor (as stipulated in the accreditation guidelines of the
USA), New Zealand demands the most requirements of their preceptors. This
includes ensuring they have a minimum of three years post-registration
experience and have completed preceptor training in accordance with the
pharmacy council. One year of practice experience seems to be the norm in
the other countries that were examined, though in GB the tutor also needs
three years experience in the field they are working and tutoring in.
The amount of assessment taking place within each of the pre-registration
systems between the countries varied. In comparison to the GB system,
Australia New Zealand, Canada and the USA appear to have in place a wider
range of measures to assess competences and performance. The newly
formed National Intern Training Program that is being rolled out in Australia21
has a comprehensive range of assessments including observations from
supervisors, written examinations, oral interviews, and practical examinations,
to name but a few. In New Zealand and Canada there are observation
assessments that take place throughout the practice training such as OSCEs.
In the USA there was more emphasis on examination-based assessment
The Pharmacist Registration Examination – September 2010 50
such as the NAPLEX and MPJE. As with the USA, a written examination-
based assessment – as opposed to a more practical assessment such as an
OSCE – is the final assessment for pre-registration trainees in GB. However,
while the GB examination is paper based, the NAPLEX and the MJPE are
administered using ‘computer-adaptive’ technology. This means that all
candidates do not answer the same questions; the examination papers sat by
pre-registration trainees during the month of testing (June or September) will
be the same.
Assessing the competencies of practical-based experience may create
problems for some preceptors monitoring pre-registration trainees as has
been found in research in the USA.31 Other work has demonstrated similar
findings. For example, Hill et al. conducted a review of the assessment
methods of an Advanced Pharmacy Practice Experiential (APPE) Program. 32
The review of the school’s assessments methods suggested that the existing
forms were cursory and did not allow for detailed assessment of students’
competence in performing clinical responsibilities. They lacked objective
criteria, were not competency related, did not require midpoint grading, and
provided little guidance to preceptors in grading. After reviewing assessment
instruments from several other pharmacy schools as well as guidelines
published by the Accreditation Council for Pharmaceutical Education and the
American Association for Colleges of Pharmacy, the authors decided to
develop a competency-based assessment process with detailed grading
rubrics. Studies such as this highlight some of the complexities of assessing
practice-based placements in pharmacy.
Lastly, there are some differences between the countries examined in terms
of regulatory boards. Canada, for example, has 12 regulatory authorities. In
the USA there are also a number of pharmacy boards which may create
problems in terms of consistency in the training and development of future
pharmacists. These countries do however outline general guidelines for
subordinate authorities in terms of requisites for the registration of
pharmacists. One could argue that a national system of regulation, such as in
GB may provide a more consistent means of regulating registration.
The Pharmacist Registration Examination – September 2010 51
3 The effectiveness of the pharmacist registration examination
3.1 Introduction
The registration examination takes place twice per year (in June and
September) and consists of written closed and open book papers which
assess knowledge and understanding using MCQs. In the closed book paper
candidates attempt 90 questions in 90 minutes. In the open book paper –
open to selected reference sources (BNF, Drug Tariff and Medicines Ethics
and Practice) – candidates attempt 80 questions in 150 minutes. Twenty of
these questions require calculations, though electronic calculators are not
allowed to be used.
The aim of this part of the study is to assess how effective the closed and
open book examinations are in assessing pre-registration trainees in a range
of competencies, knowledge and understanding.
3.2 Method
It was initially proposed that the questions from past papers of the registration
examination would be mapped against the pre-registration performance
standards, and, the questions in the registration examination would be
reviewed to determine what they were assessing in terms of competencies,
knowledge and/or understanding. Initially, a number of questions from the July
2009 examination were mapped against the pre-registration performance
standards,6
by a pharmacist member of the research team (PL). This involved
assigning the relevant performance standards, of which there are 76, to each
examination question. However, this task proved unsuccessful as few
questions mapped straightforwardly onto a performance standard directly.
As a result of this, PL met with two members of the expert panel (IS & AL) to
discuss and review the mapping already undertaken. (These members of the
expert panel are from The University of Manchester and have specialised
knowledge and experience in pre-registration training and assessment in
The Pharmacist Registration Examination – September 2010 52
community and hospital pharmacy respectively.) Following this joint reviewing
of the examination questions, in terms of what performance standards were
being covered, PL and the expert panel concluded that many of the
examination questions underpinned some the performance standards but did
not directly examine them. Following consultation with the commissioner at
the RPSGB, it was therefore decided to map the examination questions onto
the examination syllabus instead6
– of which there are 35 elements.
The elements were coded and mapped by another pharmacist member of the
research team (HP). Each element was coded (see appendix 1) and
subsequently mapped to the examination questions from the open and closed
book papers in June 2008, September 2008, June 2009 and September 2009.
In order to ‘map’ a question onto the examination syllabus, the content of each
question was analysed and then mapped onto the appropriate element(s) of
the syllabus. For example, if a question assessed the action and use of a
drug, as well as assessing knowledge on the side effects of the drug, it was
mapped onto both elements 14 and 17 of the examination syllabus (i.e.
actions and uses of a drug and adverse effects of medicines, respectively).
The coding of the four examination papers was tabulated in order to obtain
descriptive statistics about what elements of the examination syllabus could
be mapped to the registration examination. If the content of the question did
not map onto the examination syllabus, it was recorded as ‘did not map’ (see
appendix 4). Questions that were missing from the examination papers
obtained from the RPSGB were also accounted for when tabulating the data.
The questions in the registration examination were also reviewed to determine
what they assessed in terms of knowledge and/or understanding. Definitions
of knowledge and understanding were obtained from the Oxford English
Dictionary:33
Knowledge:
• Acquaintance with a fact; perception, or certain information of, a fact or
matter; state of being aware or informed; consciousness (of anything).
• Acquaintance with facts, range of information,
The Pharmacist Registration Examination – September 2010 53
Understanding:
• To comprehend; to apprehend the meaning or import of; to grasp the
idea of.
• Comprehension of something
The content of each question was analysed by two members of the research
team (PL and HP), and once again, where necessary, members of the expert
panel were consulted for advice in this exercise. In order to classify a question
that assessed knowledge, knowledge was interpreted as ‘facts and concepts
that pre-registration trainees would know from their undergraduate degree and
pre-registration experience’. In order to classify a question that assessed
understanding, understanding was interpreted as ‘the ability to use and apply
knowledge and concepts to answer a question correctly’. In some cases, a
question could be classified as assessing both knowledge and understanding.
The classification of the four examination papers was tabulated in order to
obtain descriptive statistics about the assessment of knowledge and/or
understanding in the four examination papers. If the content of the question
did not map onto knowledge and/or understanding, it was recorded as ‘did not
map’ (see appendix 4).
In some instances questions had been removed by the RPSGB from some of
the examination papers due to errors / problems with specific questions, and
these were noted and recorded as ‘removed from paper’ (see appendix 4).
3.3 Results
This section reviews the findings from both the closed book and the open
book examination papers in sequence.
3.3.1 Closed book examination paper
This section of the report focuses on the closed book registration examination
paper in 2008 and 2009. Table 3.1 displays the number of times the
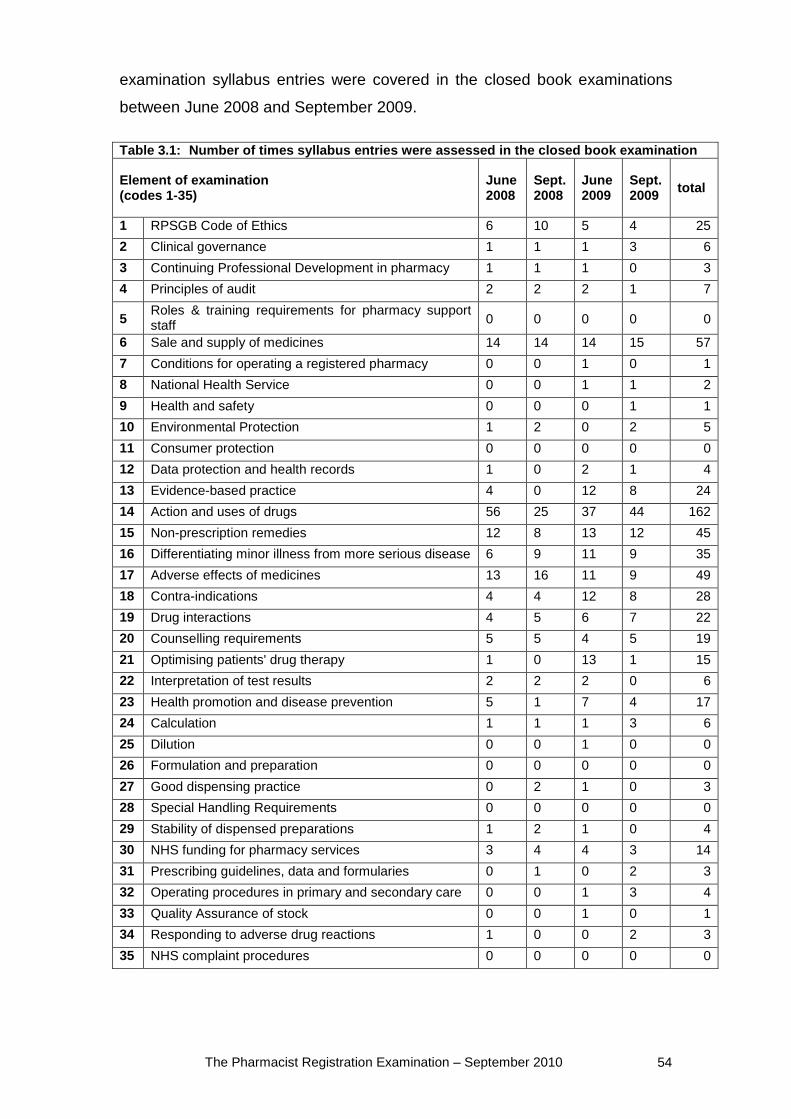
The Pharmacist Registration Examination – September 2010 54
examination syllabus entries were covered in the closed book examinations
between June 2008 and September 2009.
Table 3.1: Number of times syllabus entries were assessed in the closed book examination
Element of examination (codes 1-35)
June 2008
Sept. 2008
June 2009
Sept. 2009 total
1 RPSGB Code of Ethics 6 10 5 4 25 2 Clinical governance 1 1 1 3 6 3 Continuing Professional Development in pharmacy 1 1 1 0 3 4 Principles of audit 2 2 2 1 7
5 Roles & training requirements for pharmacy support staff 0 0 0 0 0
6 Sale and supply of medicines 14 14 14 15 57 7 Conditions for operating a registered pharmacy 0 0 1 0 1 8 National Health Service 0 0 1 1 2 9 Health and safety 0 0 0 1 1 10 Environmental Protection 1 2 0 2 5 11 Consumer protection 0 0 0 0 0 12 Data protection and health records 1 0 2 1 4 13 Evidence-based practice 4 0 12 8 24 14 Action and uses of drugs 56 25 37 44 162 15 Non-prescription remedies 12 8 13 12 45 16 Differentiating minor illness from more serious disease 6 9 11 9 35 17 Adverse effects of medicines 13 16 11 9 49 18 Contra-indications 4 4 12 8 28 19 Drug interactions 4 5 6 7 22 20 Counselling requirements 5 5 4 5 19 21 Optimising patients' drug therapy 1 0 13 1 15 22 Interpretation of test results 2 2 2 0 6 23 Health promotion and disease prevention 5 1 7 4 17 24 Calculation 1 1 1 3 6 25 Dilution 0 0 1 0 0 26 Formulation and preparation 0 0 0 0 0 27 Good dispensing practice 0 2 1 0 3 28 Special Handling Requirements 0 0 0 0 0 29 Stability of dispensed preparations 1 2 1 0 4 30 NHS funding for pharmacy services 3 4 4 3 14 31 Prescribing guidelines, data and formularies 0 1 0 2 3 32 Operating procedures in primary and secondary care 0 0 1 3 4 33 Quality Assurance of stock 0 0 1 0 1 34 Responding to adverse drug reactions 1 0 0 2 3 35 NHS complaint procedures 0 0 0 0 0
The Pharmacist Registration Examination – September 2010 55
The examination syllabus entry that was assessed most frequently in all of the
four closed book papers (2008-09) was syllabus entry 14 (‘action and uses of
drugs’). Its assessment ranged between 26 and 56 times amongst the set of
89/90 questions (one question had been omitted from the June 2009
examination paper). The other most commonly assessed syllabus entries
were syllabus entries 6 (sale & supply of medicines), 17 (adverse effects of
medicines), and 1 (RPSGB Code of Ethics)
One question (question 58) in June 2008 did not fall into any of the
examination syllabus entries and could therefore not to be mapped. In
September 2008, five questions (14, 30, 31, 32, and 61) did not map well onto
any of the examination syllabus entries and could therefore not be mapped.
3.3.1.1 Areas of duplication of assessment
As noted above, in all examination papers, from June 2008 to September
2009 inclusive, the examination syllabus entry that was been assessed most
frequently was syllabus entry 14. Across the four examinations, the mean
number of times this element was assessed in the closed book paper was 41,
in comparison to the overall mean for the other entries which was 4.1. In
addition to this particular element of the syllabus, many questions mapped
onto other codes as well at the same time. Those syllabus entries that were
frequently mapped to questions that also mapped onto syllabus entry 14 were:
• Evidence-based practice (code 13)
• Non-prescription remedies (code 15)
• Differentiating minor illness from more serious disease (code 16)
• Adverse effects of medicines (code 17)
• Contra-indications (code 18)
• Drug interactions (code 19)
• Counselling requirements (code 20)
• Health promotion and disease prevention (code 23)
The Pharmacist Registration Examination – September 2010 56
3.3.1.2 Areas of under assessment
In comparison to the highly assessed syllabus entries, in particular entries 1,
6, 14, and 17, all other elements of the examination syllabus are consistently
assessed considerably less frequently. The mean number for the assessment
of all elements of the examination syllabus was 4.1 times per examination.
Those entries which were assessed less than four times were therefore
considered to be under assessed (excluding ‘Calculation’ (code 24) which is
not part of the closed book examination). Those that were assessed at least
once but less than four times are:
• Continuing Professional Development (CPD) in pharmacy (code 3)
• Conditions for operating a registered pharmacy (code 7)
• National Health Service (code 8)
• Health and safety (code 9)
• Good dispensing practice (code 27)
• Prescribing guidelines, data and formularies (code 31)
• Quality Assurance of stock (code 33)
• Responding to adverse drug reactions (code 34)
Five elements of the examination syllabus were never assessed in the closed
book examination between June 2008 and September 2009:
• Roles and training requirements for pharmacy support staff (code 5)
• Consumer protection (code 11)
• Formulation and preparation (code 26)
• Special Handling Requirements (code 28)
• NHS complaint procedures (code 35)
3.3.1.3 Differences between years
As can be seen from Table 1, there are differences in the number of times
syllabus entries were examined in the closed book papers in 2008 and 2009.
Five elements from the examination syllabus have only been assessed in the
2009 examination papers:
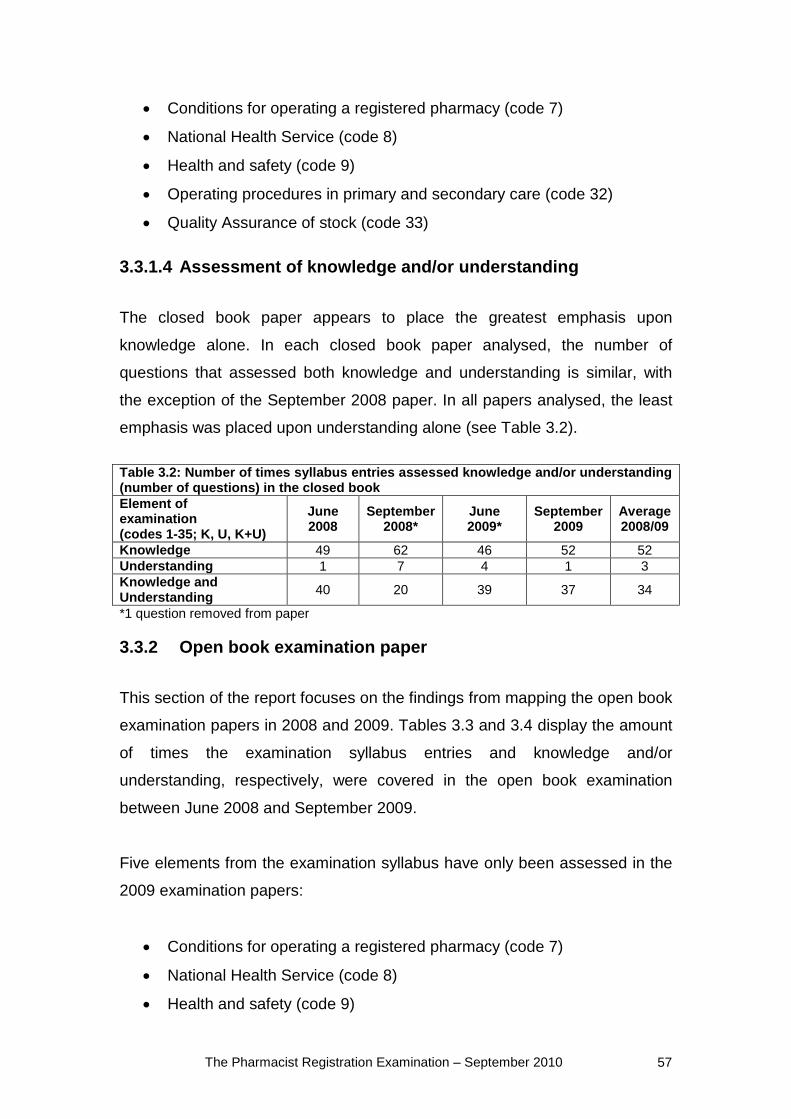
The Pharmacist Registration Examination – September 2010 57
• Conditions for operating a registered pharmacy (code 7)
• National Health Service (code 8)
• Health and safety (code 9)
• Operating procedures in primary and secondary care (code 32)
• Quality Assurance of stock (code 33)
3.3.1.4 Assessment of knowledge and/or understanding
The closed book paper appears to place the greatest emphasis upon
knowledge alone. In each closed book paper analysed, the number of
questions that assessed both knowledge and understanding is similar, with
the exception of the September 2008 paper. In all papers analysed, the least
emphasis was placed upon understanding alone (see Table 3.2).
Table 3.2: Number of times syllabus entries assessed knowledge and/or understanding (number of questions) in the closed book Element of examination (codes 1-35; K, U, K+U)
June 2008
September 2008*
June 2009*
September 2009
Average 2008/09
Knowledge 49 62 46 52 52 Understanding 1 7 4 1 3 Knowledge and Understanding 40 20 39 37 34
*1 question removed from paper
3.3.2 Open book examination paper
This section of the report focuses on the findings from mapping the open book
examination papers in 2008 and 2009. Tables 3.3 and 3.4 display the amount
of times the examination syllabus entries and knowledge and/or
understanding, respectively, were covered in the open book examination
between June 2008 and September 2009.
Five elements from the examination syllabus have only been assessed in the
2009 examination papers:
• Conditions for operating a registered pharmacy (code 7)
• National Health Service (code 8)
• Health and safety (code 9)
The Pharmacist Registration Examination – September 2010 58
• Operating procedures in primary and secondary care (code 32)
• Quality Assurance of stock (code 33)
3.3.2.1 Areas of under assessment
The elements of the examination syllabus which have a mean result for the
number of times an entry has been assessed of less than three (the average)
are considered to be under assessed. Those that were assessed at least once
but less than three times include:
• Principles of audit (code 4)
• Roles and training requirements for pharmacy support staff (code 5)
• Conditions for operating a registered pharmacy (code 7)
• Environmental Protection (code 10)
• Differentiating minor illness from more serious disease (code 16)
• Prescribing guidelines, data and formularies (code 31)
• Operating procedures in primary and secondary care (code 32)
• NHS complaint procedures (code 35)
There are eleven elements of the examination syllabus that were not
assessed during any of the four open book examination papers in 2008 and
2009:
• Clinical governance (code 2)
• CPD in pharmacy (code 3)
• National Health Service (code 8)
• Health and safety (code 9)
• Consumer protection (code 11)
• Data protection and health records (code 12)
• Dilution (code 25)
• Formulation and preparation (code 26)
• Good dispensing practice (code 27)
• Special Handling Requirements (code 28)
• Quality assurance of stock (code 33)
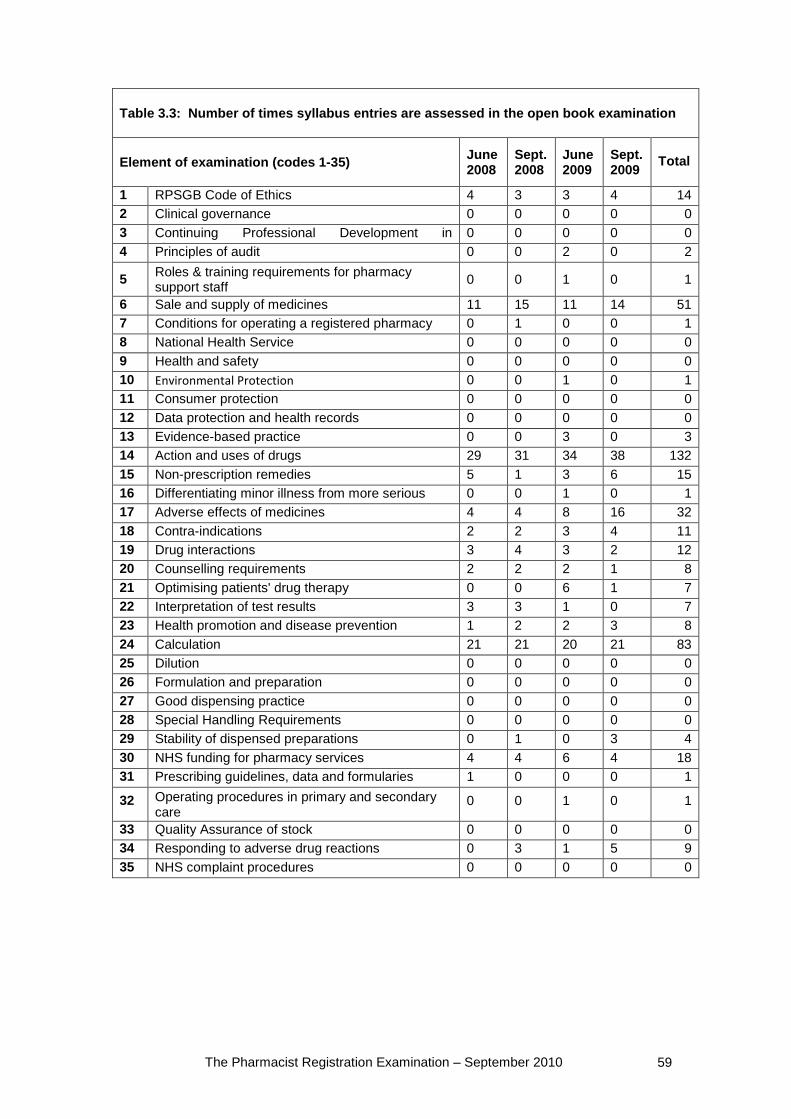
The Pharmacist Registration Examination – September 2010 59
Table 3.3: Number of times syllabus entries are assessed in the open book examination
Element of examination (codes 1-35) June 2008
Sept. 2008
June 2009
Sept. 2009
Total
1 RPSGB Code of Ethics 4 3 3 4 14 2 Clinical governance 0 0 0 0 0 3 Continuing Professional Development in
h 0 0 0 0 0
4 Principles of audit 0 0 2 0 2
5 Roles & training requirements for pharmacy support staff 0 0 1 0 1
6 Sale and supply of medicines 11 15 11 14 51 7 Conditions for operating a registered pharmacy 0 1 0 0 1 8 National Health Service 0 0 0 0 0 9 Health and safety 0 0 0 0 0 10 Environmental Protection 0 0 1 0 1 11 Consumer protection 0 0 0 0 0 12 Data protection and health records 0 0 0 0 0 13 Evidence-based practice 0 0 3 0 3 14 Action and uses of drugs 29 31 34 38 132 15 Non-prescription remedies 5 1 3 6 15 16 Differentiating minor illness from more serious
di 0 0 1 0 1
17 Adverse effects of medicines 4 4 8 16 32 18 Contra-indications 2 2 3 4 11 19 Drug interactions 3 4 3 2 12 20 Counselling requirements 2 2 2 1 8 21 Optimising patients' drug therapy 0 0 6 1 7 22 Interpretation of test results 3 3 1 0 7 23 Health promotion and disease prevention 1 2 2 3 8 24 Calculation 21 21 20 21 83 25 Dilution 0 0 0 0 0 26 Formulation and preparation 0 0 0 0 0 27 Good dispensing practice 0 0 0 0 0 28 Special Handling Requirements 0 0 0 0 0 29 Stability of dispensed preparations 0 1 0 3 4 30 NHS funding for pharmacy services 4 4 6 4 18 31 Prescribing guidelines, data and formularies 1 0 0 0 1
32 Operating procedures in primary and secondary care
0 0 1 0 1
33 Quality Assurance of stock 0 0 0 0 0 34 Responding to adverse drug reactions 0 3 1 5 9 35 NHS complaint procedures 0 0 0 0 0
The Pharmacist Registration Examination – September 2010 60
3.3.2.2 Questions in the registration examination mapped against the examination syllabus
Just like in the closed book examinations, syllabus entry 14 (‘action and uses
of drugs’) was also assessed most frequently in the open book papers. This
element of the syllabus was assessed between 29 and 41 times in the four
examination papers (mean = 33.5.). The second most frequently assessed
syllabus entry was 24 (‘calculations’), which was assessed between 20 and 21
times in 2008 and 2009. Syllabus entry 6 (‘sale and supply of medicines’)
followed in frequency and was assessed between 11 and 15 times.
In June 2008, five questions (question 49-51 and 61-62) were missing from
the examination paper and were therefore unable to be mapped onto the
syllabus. In June 2009 one question (question 14) was unable to be mapped
onto the examination syllabus as it did not correspond to any of the elements
assessment.
3.3.2.3 Areas of duplication of assessment
Some elements of the registration examination syllabus were being assessed
much more than others; there was clearly some over assessment/duplication
in this respect. The mean result for the number of times an entry was in the
open book papers from June 2008-September 2009 was 3. In all examination
papers from June 2008-September 2009 inclusive, the examination syllabus
entry that was assessed most frequently was entry 14 (‘action and uses of
drugs’). In addition to this particular element of the syllabus, many questions
mapped onto other codes as well at the same time. Syllabus entries that were
frequently mapped to questions that also mapped onto syllabus entry 14 were:
• Adverse effects of medicines (code 17)
• Contra-indications (code 18)
• Drug interactions (code 19)
• Counselling requirements (code 20)
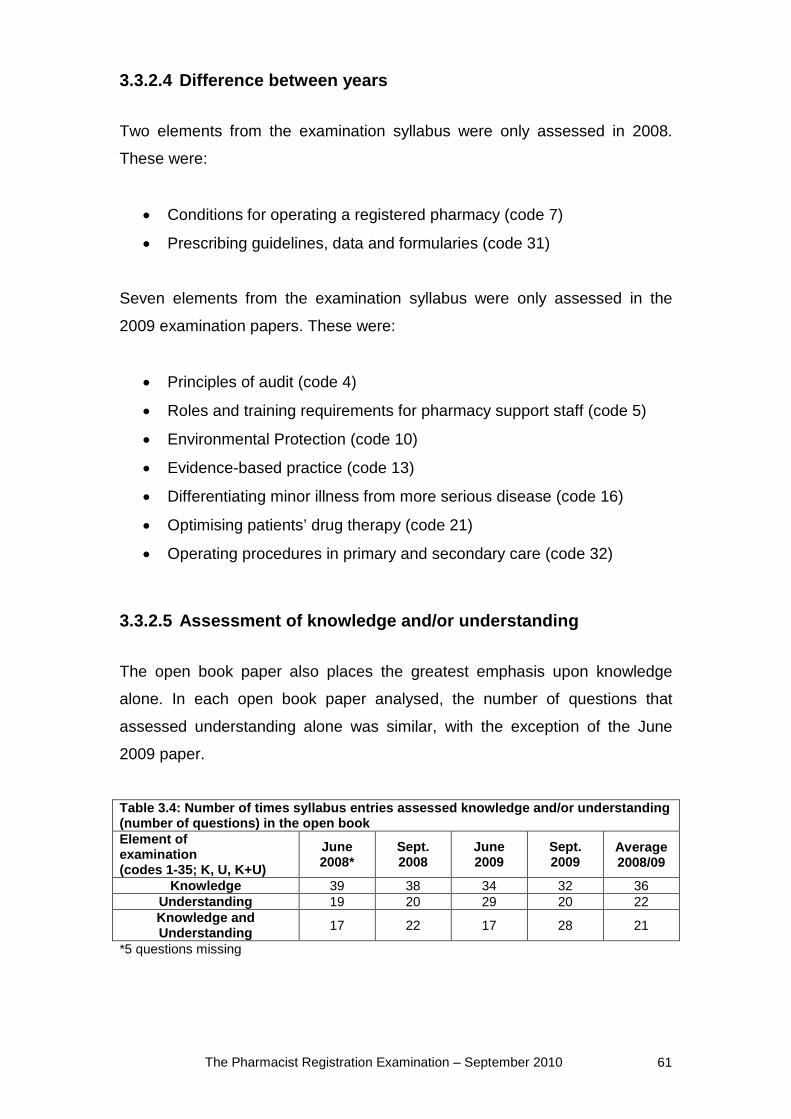
The Pharmacist Registration Examination – September 2010 61
3.3.2.4 Difference between years
Two elements from the examination syllabus were only assessed in 2008.
These were:
• Conditions for operating a registered pharmacy (code 7)
• Prescribing guidelines, data and formularies (code 31)
Seven elements from the examination syllabus were only assessed in the
2009 examination papers. These were:
• Principles of audit (code 4)
• Roles and training requirements for pharmacy support staff (code 5)
• Environmental Protection (code 10)
• Evidence-based practice (code 13)
• Differentiating minor illness from more serious disease (code 16)
• Optimising patients’ drug therapy (code 21)
• Operating procedures in primary and secondary care (code 32)
3.3.2.5 Assessment of knowledge and/or understanding
The open book paper also places the greatest emphasis upon knowledge
alone. In each open book paper analysed, the number of questions that
assessed understanding alone was similar, with the exception of the June
2009 paper.
Table 3.4: Number of times syllabus entries assessed knowledge and/or understanding (number of questions) in the open book Element of examination (codes 1-35; K, U, K+U)
June 2008*
Sept. 2008
June 2009
Sept. 2009
Average 2008/09
Knowledge 39 38 34 32 36 Understanding 19 20 29 20 22 Knowledge and Understanding 17 22 17 28 21
*5 questions missing
The Pharmacist Registration Examination – September 2010 62
3.3.3 Summary/Comparison of the closed and open book papers
Our analysis of four pharmacist registration examination open and closed
book examination questions (from 2008 and 2009) suggests that the closed
book paper assesses a wider range of elements from the examination
syllabus than the open book paper. The mean number of questions based on
‘actions and uses of drugs’ in the four closed book papers analysed was 42,
compared to a mean of 34 in the four open book papers analysed. In the
closed book papers analysed, the entry ‘action and uses of drugs’ was
consistently assessed in conjunction with ‘CPD in pharmacy, sale and supply
of medicines, optimising patients’ drug therapy, interpretation of test results
and calculation’. In the open book papers analysed, the elements that were
consistently assessed in conjunction with ‘action and uses of drug’ were
adverse effects of medicines, contra-indications, drug interactions and
counselling requirements. It should be noted, however, that in the closed and
open book papers, ‘action and uses of drugs’ has never consistently been
assessed with a particular entry. The number of times it is assessed with a
particular element of the examination syllabus is variable. For example, in the
June 2008 closed book paper, it was assessed ten times in conjunction with
‘non-prescription remedies’, but only assessed twice in conjunction with the
same element in the September 2008 paper.
Besides syllabus entry 14, there were a number of other entries which were
assessed frequently in all four reviewed examinations. They were entries 6
(sale & supply of medicines), 17 (adverse effects of medicines), and 1
(RPSGB Code of Ethics) in the closed book examination, and 24
(‘calculations’) in the closed book examination. These syllabus entries are
ones encompassing pharmacists’ keys competencies and roles, so would be
expected to be adequately and sufficiently assessed. Some syllabus entries
were assessed rather less frequently, others were not assessed at all during
one or more of the four reviewed examination papers.
Both the closed and open book papers placed the highest emphasis upon
assessing knowledge alone. The closed book paper assessed knowledge and

The Pharmacist Registration Examination – September 2010 63
understanding to a similar level as knowledge alone, whereas, the open book
paper assesses understanding to a similar level as knowledge alone.
The Pharmacist Registration Examination – September 2010 64
4 Discussion
In this report, we have compared registration requirements for pharmacist
registration in GB with requirements in other countries, as well as
requirements for other healthcare professionals in the UK. We have also
reviewed the final written registration examination required for GB pharmacist
registration in detail, to identify which elements of the examination syllabus
are being assessed, and to what extent, and whether questions assess
knowledge and/or understanding. This discussion section will summarise the
findings from these different parts (see sections 2 and 3) and discuss their
implications.
Our findings from comparing registration requirements for pharmacists
elsewhere (namely in Australia, Canada, New Zealand, and the USA), as well
as other UK healthcare professionals (optometrist, doctor or dentist) have
shown that there are both similarities and differences. Both provide us with a
better understanding of possible different approaches, and also give some
insight into potential benefits and/or drawbacks within these.
4.1 Registration requirements for other healthcare professions in the UK
The training of the healthcare professions in Great Britain we looked at
(dentistry, medicine and optometry) were chosen because they all have an
undergraduate mostly university based degree course, followed by more
practice based training pre- or post graduation. For the purpose of this study,
we focussed on training, supervision and assessment during practice based
learning. None of the other healthcare professional registrations required a
written examination comparable to the GB pharmacist registration
examination, but they were much more focussed on practice based
assessments.
One important finding that is worth noting here was the difference in the
number of individuals or tutors involved in the supervision and assessment of
The Pharmacist Registration Examination – September 2010 65
pre-registration trainees in the different professions. In pharmacy there is one
tutor who is integral to the pre-registration year of a trainee. They serve as
both a colleague and mentor, supervisor, and as an assessor. By assessing
and signing the pre-registration performance reports on the trainee’s
progression, they ultimately dictate to a large extent whether a trainee has
performed to a satisfactory standard and is ready to sit the registration
examination. Likewise, in optometry there is one supervisor who acts as the
key contact for the trainee optometrist during their SfR training. However,
separate external assessors are involved in the assessment of the student.
In medicine, an even larger number of individuals are involved in contributing
towards both the training and measurement of performance (assessment) of
foundation doctors. Trainees are assigned an educational supervisor and a
clinical supervisor, so they essentially have two key points of contact
throughout their foundation training. They will receive feedback and undergo
assessment from them, who in turn draw on regular assessments from other
sources that liaise with the foundation doctors, such as colleagues (doctors
and other healthcare professionals such as nurses) and patients – they
essentially receive ‘multi-source’ feedback.34 This is arguably advantageous
over the one-to-one feedback and supervision more likely to be encountered
for pre-registration pharmacy trainees and optometry students.34;35
Dentistry stands out as somewhat of an anomaly because dentistry graduates
register with the GDC following graduation. Although many dentists do tend to
undergo further training and supervised practice after registering, and this is
indeed a requirement for NHS practice, this is not a registration requirement. It
appears that the system in place within pharmacy is most similar to that in
place within optometry whereas dentistry and medicine have more unique
features.
Our research findings from comparing the registration requirements of
different healthcare professions in GB also highlighted some of the differences
in the amount – and type – of assessment undertaken by pre-registration
trainees from the various healthcare sectors. Pharmacy trainees are subjected
The Pharmacist Registration Examination – September 2010 66
to routine monitoring and quarterly progress reports prior to a final written
examination. This differs from the assessment methods in place in the other
professions. In optometry for example there is an emphasis on students
meeting a number of competencies which are verified through visits from an
external assessor. If proven to be competent students will proceed to the next
stage of the SfR which assesses more practical abilities (e.g. undertaking an
eye examination). The final assessment is an OSCE which again assesses
practical (including communication) skills that are routinely carried out by an
optometrist.
Foundation doctors undergo continuous and regular assessment (and
formative feedback) by multiple (and multidisciplinary) assessors.
Assessments such as the mini-CEX and DOPS are carried out during the
foundation and results are provided and ratified by a number of different
people. This is useful in gaining a broad range of insight into the performance
of a foundation doctor. Other forms of assessment aim to develop other skills
such as becoming a clinical tutor.
Drawing a comparison between dentistry and the other healthcare professions
just described is difficult due to the peculiar system of allowing registration
without a ‘pre-registration’ or ‘foundation’ year of supervised practise. The
BDS course undertaken by dentistry students will, however, assess a range of
practical skills and performance throughout the five year undergraduate
course in a similar fashion. Pharmacy may lack some useful features that are
present in the pre-registration training year in optometry and medicine such as
having independent assessors and more practical assessments overseen by
appropriately trained (and independent) assessors. Pharmacy pre-registration
trainees will inevitably undertake a great deal of work during their pre-
registration year which is monitored and developed by their tutor, but formal
and objective tests seem to be lacking.
4.2 Registration requirements for pharmacists in selected other countries
The Pharmacist Registration Examination – September 2010 67
When we examined the pharmacy registration processes internationally, we
discovered that there were a number of similarities in the way the regulators
control pharmacist registration. Commonly, it takes a total of five years’
training to become a pharmacist in GB, Australia, New Zealand and Canada.
In the USA it often takes more than five years. All candidates studying for their
pharmacy qualification in GB, Australia and New Zealand are required to
undertake a degree in pharmacy followed by a year of supervised practice.
Throughout the degree programme there may be practice-based experience
but the majority of real-world practice will take place in the year following the
degree (i.e. the pre-registration year in GB). In Canada and the USA there
appears to be more variation in terms of the amount of practical experience
that pre-registration trainees undertake according to the province or state they
are training in. There is also no ‘set’ year of practising pharmacy under
supervision after completing a pharmacy degree. It seems that such work
experience in distributed through the period of study.
The idea of distributing practical experience throughout the undergraduate
course is something that is already in place in Bradford University in GB36;
here, students do two six-month blocks of supervised practice at different
stages rather than having a one-year block at the end of their degree.
Perhaps the incorporation of more supervised practice throughout a pharmacy
degree, rather than merged into one year at the end of the degree, provides
students with a better grasp and knowledge of practical experience which is
conducive to learning practical-based subjects in the MPharm. This is indeed
what was recommended in the Pharmacy White Paper.37
Having one individual as a student or pre-registration trainee’s tutor/preceptor
seems to be common place in each country, though the experience and
requirements of these individuals varies. However, as previously discussed,
there may be some subjectivity in assessments of pre-registration trainees if
this comes from one individual acting as a supervisor and an assessor. This of
course may be more of an issue in GB whereby tutors fill in progress reports –
one of the main ways trainees are measured and assessed throughout their
pre-registration training; they do not have external monitors assessing them,
The Pharmacist Registration Examination – September 2010 68
nor do they undergo different assessments, apart from the registration
examination at the end of supervised practice. In New Zealand, and Canada,
for example, OSCEs are used which may be considered a more superior
assessment of someone’s competencies or fitness to practise.38
Perhaps in
GB there can be more assessment during the pre-registration year which will
focus both on areas of practice and additionally on areas which cannot be
feasibly assessed in the registration examination.
4.3 The effectiveness of the pharmacist registration examination: mapping of examination questions against syllabus & knowledge versus understanding
In another part of this study39
, the research team carried out an examination
of the closed and open book examination papers between 2008 and 2009 and
mapped the examination questions against the pre-registration syllabus.
Findings from this research showed that both the open and closed book
examination papers do not place the same amount of emphasis on each
element of the pre-registration examination syllabus. This is clear from our
findings that many questions map onto specific elements such as ‘action and
uses of drugs,’ ‘sale & supply of medicines,’ and ‘adverse effects of
medicines,’ whereas some elements of the syllabus are not covered at all by
any questions. These are areas which are of particular importance in
pharmacy practice, particularly in community and hospital practice, where the
majority of newly registered pharmacists will practise. The elements of the
pre-registration syllabus that went unassessed in both the open and closed
papers were consumer protection (code 11), dilution (code 25), formulation
and preparation (code 26) and special handling requirements (code 28). Our
findings suggest there is an unequal amount of focus on the elements of the
pre-registration examination syllabus in the pre-registration examination
papers. Perhaps it can be expected that some elements may be more
assessed than others, particularly if these are deemed to be very important
aspects of a pharmacist’s future role upon becoming registered.
The Pharmacist Registration Examination – September 2010 69
Our assessment of the registration examination suggests that it particularly
focuses on the assessment of knowledge which is not surprising considering
the aims stated in the pre-registration trainee workbook.6 Assessments have
the ability to direct learning in a particular direction.40
This relatively narrow
focus on the assessment of knowledge in the registration exam means that
particular emphasis and importance rests on the appropriate assessment of a
broad range of competences and understanding in the regular performance
reports.
Indeed, the written registration examination is currently only part of the
registration assessment which is otherwise assessed continuously and signed
off / passed by the tutor in quarterly progress reports. Understanding may be
much better and more appropriately assessed in practice, but how objectively
and independently this is done in different pharmacy sectors and settings
cannot be commented on based on this project. Other healthcare professions
separate supervisory and assessment functions, and others (medicine in
particular) put particular emphasis on not only obtaining regular assessment,
but involving numerous assessors in this process. How effective these
approaches are in the other healthcare professions, and how some relevant
features could be incorporated into pharmacist pre-registration assessment,
would require further study. Equally, the effectiveness, validity and objectivity
of the current assessment using the completion of progress reports by tutors
for pharmacy pre-registration trainees would require further exploration.
In fact, there has been some research over the last decade, which has
highlighted potential problems with in-practice assessments. This has
indicated that some students or trainees in healthcare professions such as
nursing and medicine are progressing through their clinical training without
encountering failure in assessments that measure performances in abilities
they struggle with. Evidence from nursing has demonstrated a ‘failure to fail’
students even though they may be underperforming.41 Assessment of clinical
competency is complex and is generally based on direct observations from a
mentor which will involve subjective value judgements that vary from person
to person.41 There have been findings of nurse mentors passing students on
The Pharmacist Registration Examination – September 2010 70
clinical assessments even when there were doubts about their performance.42
This could be, in part, due to mentors being unprepared to assess the
competency of students in practice placements.42 Further evidence coming
from the medical setting has also demonstrated the ‘failure to fail’ tendencies
mentors may have. A recent study43
has shown that medical tutors may not
fail medical students due a number of factors such as attitudes towards a
student, attitudes about failing a student and motivation to comply with norms,
such as what they think they should do, or what other tutors were doing. In
that study, focus groups were conducted with a number of medical educators
(GPs, hospital doctors and non-clinical tutors) to understand what was behind
the decision process of passing students that may not possess satisfactory
skills and competencies in medicine. Attitudes and beliefs played a major role
in the process whereby, for example, a tutor may not fail a student because
their attitudes toward that student were positive; the student may be well-like
by tutors or was perceived to be aware of their difficulties.
Other factors may play a role in not failing students as another study in
Canada has shown. In this study, conducted by Dudek et al.,44
semi-
structured interviews were conducted with 21 clinical supervisors at the
University of Ottawa. A number of barriers were identified that prevent
supervisors from reporting a trainee who has been performing poorly. These
include lack of documentation (supporting evidence for judgements), lack of
knowledge of what to document, the anticipation of an appeal process, and
lack of remediation options. The failure to fail students who may not be
meeting the necessary requirements for progressing in their chosen field,
such as nursing and medicine, may be widespread. With these issues
appearing to be prevalent in nursing and medicine, it is likely that they are
also occurring in pharmacy.
This research has ultimately identified some possible shortcomings of the
registration examination and its potential implications for the pharmacist
registration process in GB. This research has also considered the registration
systems in place within other healthcare professions in GB and other systems
of pharmacy registration outside of GB and how they may offer a different
The Pharmacist Registration Examination – September 2010 71
approach to assessing and registering pharmacists. With this information, we
are able to make a number of recommendations concerning the registration
assessment of pharmacists in Great Britain. Many of these would need to be
informed by further research, which we also highlight.
At the time of writing, Modernising Pharmacy Careers (MPC) (part of Medical
Education England (MEE)) is reviewing pharmacy undergraduate education
and pre-registration training. They are assessing the content and continuing
relevance of pharmacy training and identifying options for change. Their report
is expected to be published late 2010.
The Pharmacist Registration Examination – September 2010 72
5 Recommendations
We would like to provide the following recommendations to be considered
concerning the pre-registration examination. As stated in our discussion,
these would need to be informed and supported by further evaluation and
research.
• The tutor should continue to undertake formative assessment of the
trainee and provide feedback to support their professional development
• Separate the supervisor (tutor) and summative assessor function to
improve objectivity and consistency between different tutors
• Review who can be a tutor: The training requirements for tutors should
be addressed. Standards for tutors should be developed. Appropriate
training would need to be developed, with which tutors would need to
be accredited, to ensure they can comply with the appropriate
standards.
• Increase the number and type of formative assessments during the
pre-registration year. Increase the number of people and disciplines
involved in these assessments. These assessments should focus on
skills, understanding and competencies central to the practice of
pharmacy.
• The final registration assessment should not just focus on the
assessment of knowledge but should also assess a wider range of
skills and competencies.
• Further training, support and/or mentoring during the first year following
registration could be considered, following the medical model of
foundation 1 & 2 training
The Pharmacist Registration Examination – September 2010 73
6 References
(1) Fazackerley A. Contest hots up for medical places. Times Higher Education Online. 2004.
(2) Larson MS. The Rise of Professionalism: A Sociological Analysis. Berkeley: University of California Press; 1977.
(3) Department of Health. Trust, assurance and safety - the regulation of health professionals in the 21st century. 2010.
(4) Council for Healthcare Regulatory Excellence. Assuring patient safety through regulation. 2009.
(5) General Pharmaceutical Council. Standards of conduct, ethics and performance. Accessed 10/09/10; available from: http://www.pharmacyregulation.org/pdfs/other/gphcstandardsofconductethicsandperflo.pdf
(6) Royal Pharmaceutical Society of Great Britain. Preregistration trainee workbook 2009/10. 2009
(7) Royal Pharmaceutical Society of Great Britain. Preregistration trainee workbook 2010/2011. Accessed 10/09/10; available from: http://www.pharmacyregulation.org/pdfs/preregistrationpharmacists/2ctraineeworkbook201011.pdf
(8) Royal Pharmaceutical Society of Great Britain. Frequently Asked Questions (FAQs) for Pre-registration Tutors. 2010.
(9) General Optical Council. Opticians' registers. 2010. Accessed 15/06/10; available from: http://www.optical.org/en/our_work/Registration/Opticians'_Registers.cfm
(10) The College of Optometrists. Scheme for registration trainee handbook. 2009.
(11) General Optical Council. GOC optometry core curriculum, core competencies and learning outcomes. 2010 Accessed 25/09/10; available from: http://www.optical.org/goc/filemanager/root/site_assets/educational_curricula/goc_optometry_core_curriculum.pdf
(12) Association of Optometrists. Work based assessment visits 2010/11.2010. Accessed 24/09/10; available from: http://www.assoc-optometrists.org/uploaded_files/work_based_assessment_visits_280410.pdf
The Pharmacist Registration Examination – September 2010 74
(13) General Medical Council. The medical register. 2010. Accessed 15/06/10; available from: http://www.gmc-uk.org/doctors/medical_register.asp
(14) Academy of Royal Medical Colleges, Department of Health, NHS Scotland, Department of Health, NHS Wales. The UK foundation curriculum. 2010. Cardiff, Crown copyright.
(15) General Dental Council. Who we regulate. 2010. Accessed 15/06/10; available from: http://www.gdcuk.org/About+us/Who+we+regulate/
(16) General Dental Council. Outcomes for registration. 2010. Accessed 25/09/10; available from: http://www.gdc-uk.org/NR/rdonlyres/4D5C3858-0F32-4EFD-B0E4-A3F79A991D30/0/Learningoutcomesdraftpublication.pdf
(17) Committee of Postgraduate Dental Deans and Directors, Scottish Executive, Department of Health, Department of health Welsh Assembly Government. A curriculum for UK Dental Foundation Programme Training. 2010.
(18) Committee of Postgraduate Dental Deans and Directors. COPDEND Dental Foundation Training Policy Statement . 2010. Accessed 04/06/10; available from: http://www.copdend.org.uk/
(19) Australian Health Practitioner Regulation Agency. Pharmacy Board of Australia. 2010. Accessed 12/07/10; available from: http://www.ahpra.gov.au/Health-Professions.aspx
(20) Pharmaceutical Society of Australia. Intern training programme. 2010. Accessed 12/07/10; available from: http://www.psa.org.au/site.php?id=4291
(21) Marriott JL, Nation RL, Roller L, Costelloe M, Galbraith K, Stewart P et al. Pharmacy Education in the Context of Australian Practice. American Journal of Pharmaceutical Education 2008; 72(6 (Article 131)).
(22) Pharmaceutical society of Australia. Competency standards for pharmacists in Australia. 2010 Available from: http://www.psa.org.au/site.php?id=1123
(23) Pharmaceutical Society of New Zealand. Requirements of the EVOLVE Intern Training Programme. 2010. Accessed 21/09/10; available from: http://psnz.org.nz/public/evolve/documents/RequirementsoftheInternTrainingProgramme.pdf
(24) Pharmaceutical Society of New Zealand. EVOLVE intern programme. 2010. Accessed 21/09/10; available from: http://www.psnz.org.nz/public/evolve/training_an_intern_pharmacist/training.aspx
(25) Royal Pharmaceutical Society of New Zealand. Guidelines for employing an intern. 2010. Accessed 21/09/10; available from:
The Pharmacist Registration Examination – September 2010 75
http://psnz.org.nz/public/evolve/training_an_intern_pharmacist/documents/GuidelinesforemployinganIntern2011.pdf
(26) National Association of Pharmacy Regulatory Authorities. A framework for assessing Canadian pharmacists' competencies at entry-to- practice through structured practical training programs. 2010. Accessed 10/07/10; available from: http://www.napra.org/Content_Files/Files/Framework_for_Assessing_Canadian_Pharmacists_Competencies.pdf
(27) National Association of Pharmacy Regulatory Authorities. Professional competencies for Canadian pharmacists at entry to practice. 2007.
(28) Accreditation Council for Pharmacy Education. Accreditation standards and guidelines for the professional program in pharmacy leading to the doctor of pharmacy degree. 2006.
(29) National Association of Boards of Pharmacy. NAPLEX. 2010. Accessed 12/07/10; available from: http://www.nabp.net/programs/examination/naplex/
(30) National Association of Boards of Pharmacy. MJPE. Accessed 12/07/10; available from: http://www.nabp.net/programs/examination/mpje/
(31) Ried LD, Nemire R, Doty R, Brickler MP, Anderson HH, Frenzel-Shepherd E, Larose-Pierre M, Dugan D. An automated competency-based student performance assessment program for advanced pharmacy practice experiential programs. American Journal of Pharmaceutical Education 2007; 71(6):128.
(32) Hill LH, Delafuente JC, Sicat BL, Kirkwood CK. Development of a competency-based assessment process for advanced pharmacy practice experiences. American Journal of Pharmaceutical Education 2006; 70(1).
(33) Oxford English Dictionary. 2010. Accessed 21/09/10; available from: http://oxforddictionaries.com/
(34) Lockyer J. Multisource feedback in the assessment of physician competencies. Journal of Continuing Education in Health Professions 2003; 23(1):4-12.
(35) Violato C, Lockyer J, Fidler H. Multisource feedback: a method of assessing surgical practice. BMJ 2003; 326(7388):546-548.
(36) Bradford University. Pharmacy MPharm 5 years practice-integrated. 2010. Accessed 23/09/10; available from: http://www.brad.ac.uk/pharmacy/our-courses/undergraduate/pharmacy-mpharm-5-year-practice-integrated/
(37) Department of Health. Pharmacy in England: Building on strengths - delivering the future. 2010.
The Pharmacist Registration Examination – September 2010 76
(38) Sloan DA, Donnelly MB, Schwartz RW, William S. The objective structured clinical examination: The new gold standard for evaluating postgraduate clinical performance. Annals of Surgery 1995; 222(6).
(39) Jee SD, Willis S, Elvey R, Lewis P, Parmar H, Schafheutle EI, Tully M, Hall J. Re-sitting assessments and competence. The University of Manchester. 2010.
(40) Ofsted. Assessment for learning: the impact of National Strategy support. 2008. Accessed 20/09/10; available from: http://www.ofsted.gov.uk/Ofsted-home/Publications-and-research/Browse-all-by/Documents-by-type/Thematic-reports/Assessment-for-learning-the-impact-of-National-Strategy-support
(41) Dolan G. Assessing student nurse clinical competency: Will we ever get it right? Journal of Clinical Nursing 2003; 12(1):132-141.
(42) Duffy K. Failing students: a qualitative study of factors that influence the decisions regarding assessment of students' competence in practice. Caledonian Nursing and Midwifery Research Centre, School of Nursing, Midwifery and Community Health, Glasgow Caledonian University. 2003.
(43) Cleland JA, Knight LV, Rees CE, Tracey S, Bond CM. Is it me or is it them? Factors that influence the passing of underperforming students. Medical Education 2008; 42(8):800-809.
(44) Dudek NL, Marks MB, Regehr G. Failure to fail: The perspectives of clinical supervisors. Academic Medicine 2005; 80 (10 SUPPL.).
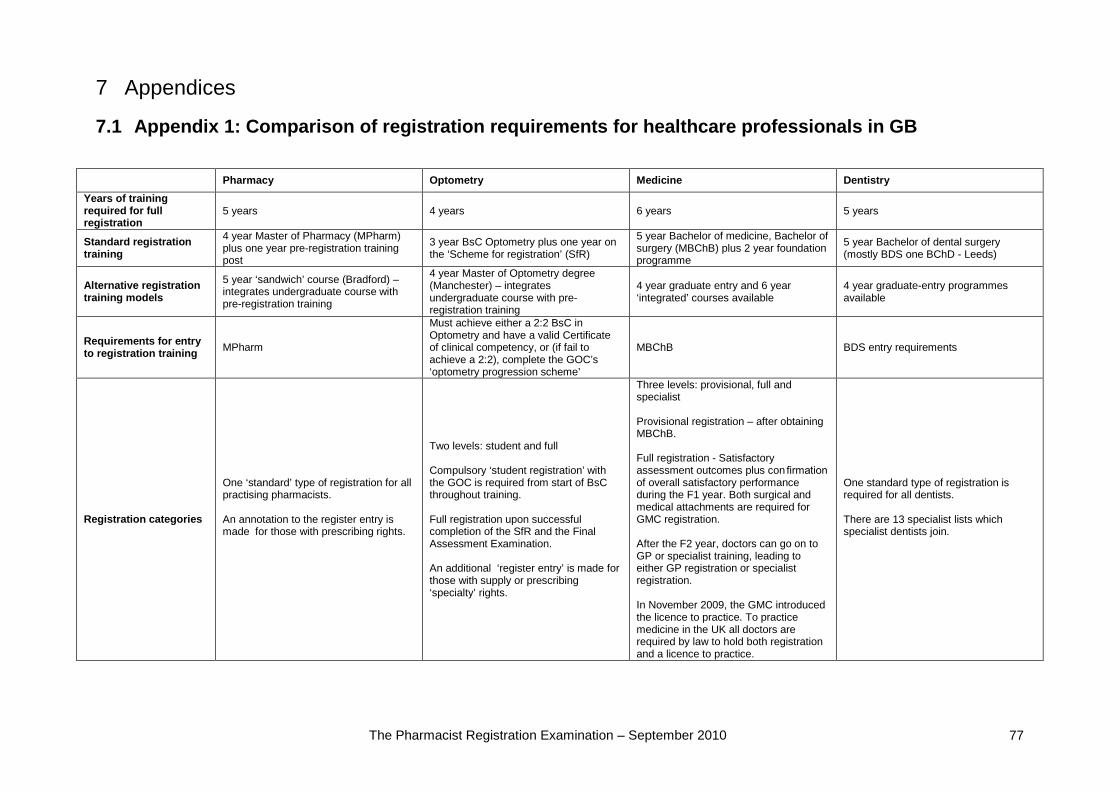
The Pharmacist Registration Examination – September 2010 77
7 Appendices
7.1 Appendix 1: Comparison of registration requirements for healthcare professionals in GB
Pharmacy Optometry Medicine Dentistry Years of training required for full registration
5 years 4 years 6 years 5 years
Standard registration training
4 year Master of Pharmacy (MPharm) plus one year pre-registration training post
3 year BsC Optometry plus one year on the ‘Scheme for registration’ (SfR)
5 year Bachelor of medicine, Bachelor of surgery (MBChB) plus 2 year foundation programme
5 year Bachelor of dental surgery (mostly BDS one BChD - Leeds)
Alternative registration training models
5 year ‘sandwich’ course (Bradford) – integrates undergraduate course with pre-registration training
4 year Master of Optometry degree (Manchester) – integrates undergraduate course with pre-registration training
4 year graduate entry and 6 year ‘integrated’ courses available
4 year graduate-entry programmes available
Requirements for entry to registration training MPharm
Must achieve either a 2:2 BsC in Optometry and have a valid Certificate of clinical competency, or (if fail to achieve a 2:2), complete the GOC’s ‘optometry progression scheme’
MBChB BDS entry requirements
Registration categories
One ‘standard’ type of registration for all practising pharmacists. An annotation to the register entry is made for those with prescribing rights.
Two levels: student and full Compulsory ‘student registration’ with the GOC is required from start of BsC throughout training. Full registration upon successful completion of the SfR and the Final Assessment Examination. An additional ‘register entry’ is made for those with supply or prescribing ‘specialty’ rights.
Three levels: provisional, full and specialist Provisional registration – after obtaining MBChB. Full registration - Satisfactory assessment outcomes plus confirmation of overall satisfactory performance during the F1 year. Both surgical and medical attachments are required for GMC registration. After the F2 year, doctors can go on to GP or specialist training, leading to either GP registration or specialist registration. In November 2009, the GMC introduced the licence to practice. To practice medicine in the UK all doctors are required by law to hold both registration and a licence to practice.
One standard type of registration is required for all dentists. There are 13 specialist lists which specialist dentists join.
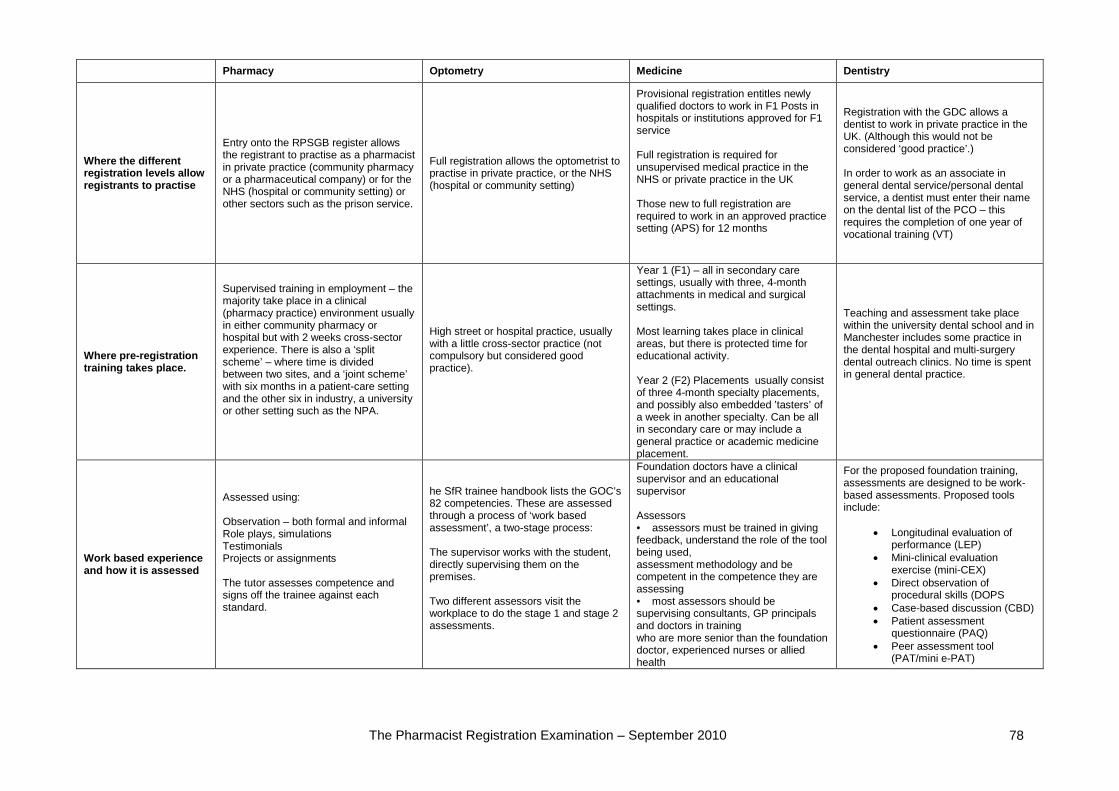
The Pharmacist Registration Examination – September 2010 78
Pharmacy Optometry Medicine Dentistry
Where the different registration levels allow registrants to practise
Entry onto the RPSGB register allows the registrant to practise as a pharmacist in private practice (community pharmacy or a pharmaceutical company) or for the NHS (hospital or community setting) or other sectors such as the prison service.
Full registration allows the optometrist to practise in private practice, or the NHS (hospital or community setting)
Provisional registration entitles newly qualified doctors to work in F1 Posts in hospitals or institutions approved for F1 service Full registration is required for unsupervised medical practice in the NHS or private practice in the UK Those new to full registration are required to work in an approved practice setting (APS) for 12 months
Registration with the GDC allows a dentist to work in private practice in the UK. (Although this would not be considered ‘good practice’.) In order to work as an associate in general dental service/personal dental service, a dentist must enter their name on the dental list of the PCO – this requires the completion of one year of vocational training (VT)
Where pre-registration training takes place.
Supervised training in employment – the majority take place in a clinical (pharmacy practice) environment usually in either community pharmacy or hospital but with 2 weeks cross-sector experience. There is also a ‘split scheme’ – where time is divided between two sites, and a ‘joint scheme’ with six months in a patient-care setting and the other six in industry, a university or other setting such as the NPA.
High street or hospital practice, usually with a little cross-sector practice (not compulsory but considered good practice).
Year 1 (F1) – all in secondary care settings, usually with three, 4-month attachments in medical and surgical settings. Most learning takes place in clinical areas, but there is protected time for educational activity. Year 2 (F2) Placements usually consist of three 4-month specialty placements, and possibly also embedded ’tasters’ of a week in another specialty. Can be all in secondary care or may include a general practice or academic medicine placement.
Teaching and assessment take place within the university dental school and in Manchester includes some practice in the dental hospital and multi-surgery dental outreach clinics. No time is spent in general dental practice.
Work based experience and how it is assessed
Assessed using: Observation – both formal and informal Role plays, simulations Testimonials Projects or assignments The tutor assesses competence and signs off the trainee against each standard.
he SfR trainee handbook lists the GOC’s 82 competencies. These are assessed through a process of ‘work based assessment’, a two-stage process: The supervisor works with the student, directly supervising them on the premises. Two different assessors visit the workplace to do the stage 1 and stage 2 assessments.
Foundation doctors have a clinical supervisor and an educational supervisor Assessors • assessors must be trained in giving feedback, understand the role of the tool being used, assessment methodology and be competent in the competence they are assessing • most assessors should be supervising consultants, GP principals and doctors in training who are more senior than the foundation doctor, experienced nurses or allied health
For the proposed foundation training, assessments are designed to be work-based assessments. Proposed tools include:
• Longitudinal evaluation of performance (LEP)
• Mini-clinical evaluation exercise (mini-CEX)
• Direct observation of procedural skills (DOPS
• Case-based discussion (CBD) • Patient assessment
questionnaire (PAQ) • Peer assessment tool
(PAT/mini e-PAT)
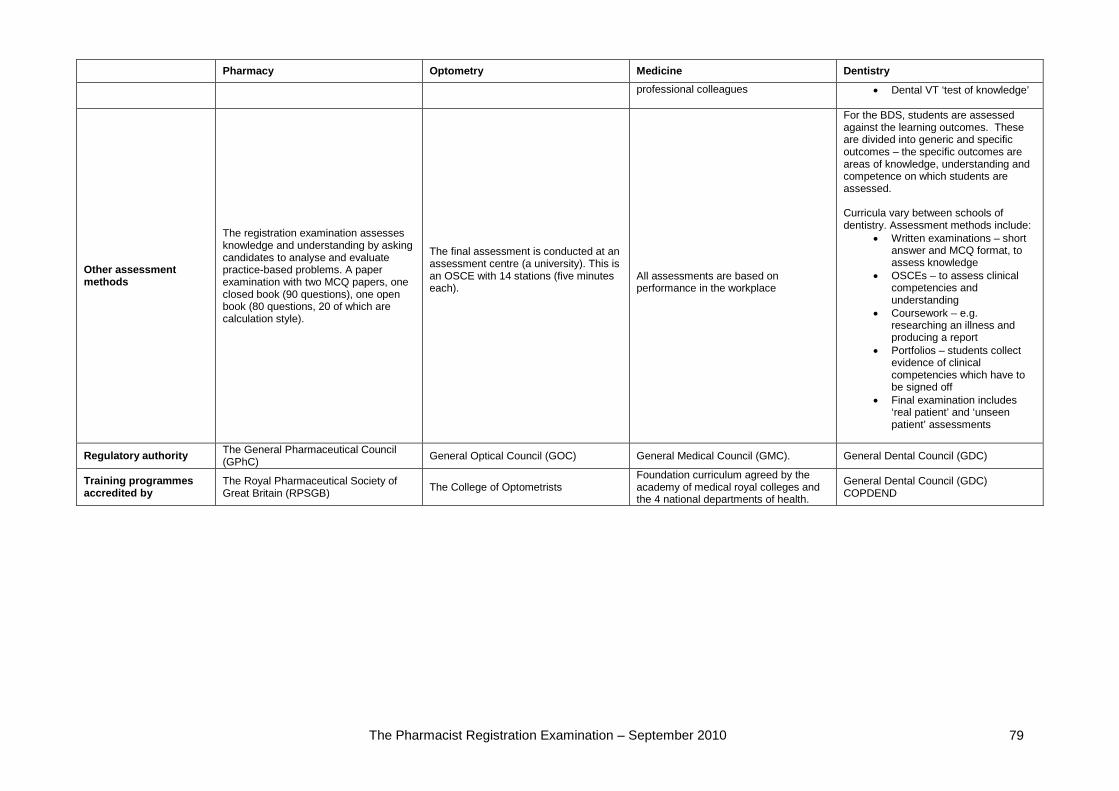
The Pharmacist Registration Examination – September 2010 79
Pharmacy Optometry Medicine Dentistry professional colleagues • Dental VT ‘test of knowledge’
Other assessment methods
The registration examination assesses knowledge and understanding by asking candidates to analyse and evaluate practice-based problems. A paper examination with two MCQ papers, one closed book (90 questions), one open book (80 questions, 20 of which are calculation style).
The final assessment is conducted at an assessment centre (a university). This is an OSCE with 14 stations (five minutes each).
All assessments are based on performance in the workplace
For the BDS, students are assessed against the learning outcomes. These are divided into generic and specific outcomes – the specific outcomes are areas of knowledge, understanding and competence on which students are assessed. Curricula vary between schools of dentistry. Assessment methods include:
• Written examinations – short answer and MCQ format, to assess knowledge
• OSCEs – to assess clinical competencies and understanding
• Coursework – e.g. researching an illness and producing a report
• Portfolios – students collect evidence of clinical competencies which have to be signed off
• Final examination includes ‘real patient’ and ‘unseen patient’ assessments
Regulatory authority The General Pharmaceutical Council (GPhC) General Optical Council (GOC) General Medical Council (GMC). General Dental Council (GDC)
Training programmes accredited by
The Royal Pharmaceutical Society of Great Britain (RPSGB) The College of Optometrists
Foundation curriculum agreed by the academy of medical royal colleges and the 4 national departments of health.
General Dental Council (GDC) COPDEND
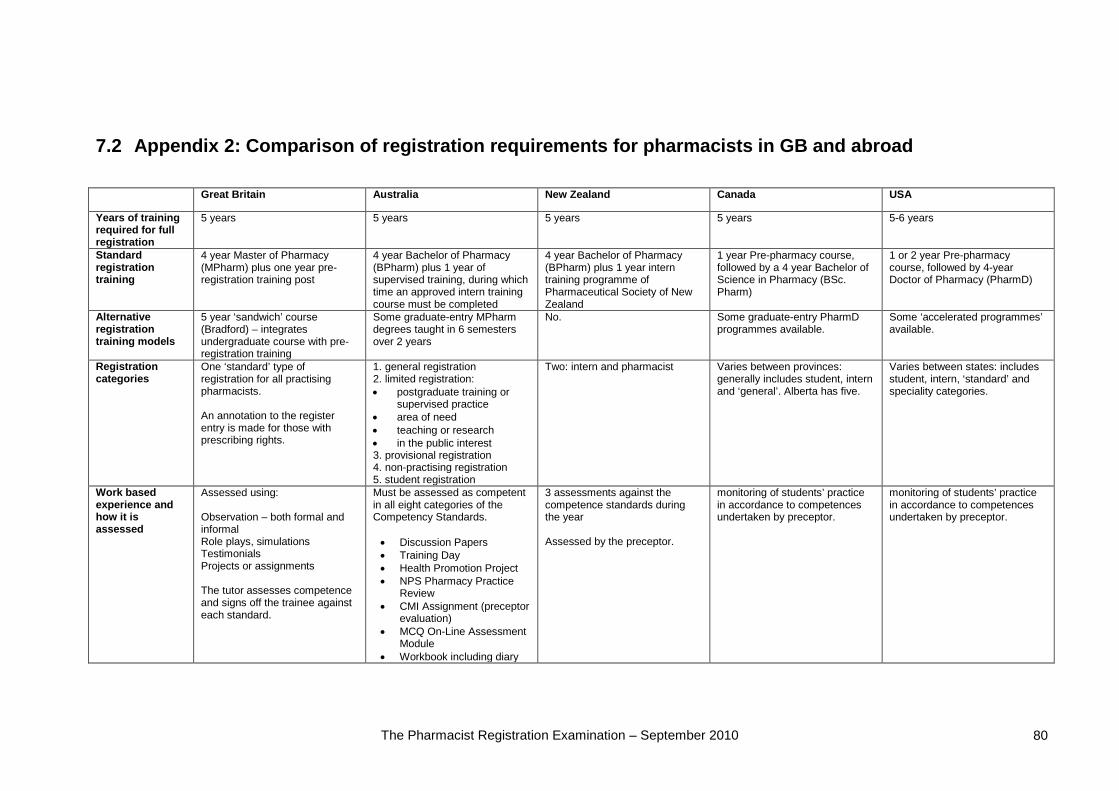
The Pharmacist Registration Examination – September 2010 80
7.2 Appendix 2: Comparison of registration requirements for pharmacists in GB and abroad Great Britain Australia New Zealand Canada USA
Years of training required for full registration
5 years 5 years 5 years 5 years 5-6 years
Standard registration training
4 year Master of Pharmacy (MPharm) plus one year pre-registration training post
4 year Bachelor of Pharmacy (BPharm) plus 1 year of supervised training, during which time an approved intern training course must be completed
4 year Bachelor of Pharmacy (BPharm) plus 1 year
1 year Pre-pharmacy course, followed by a 4 year intern
training programme of Pharmaceutical Society of New Zealand
Bachelor of Science in Pharmacy
1 or 2 year Pre-pharmacy course, followed by 4-year Doctor of Pharmacy (PharmD) (BSc.
Pharm)
Alternative registration training models
5 year ‘sandwich’ course (Bradford) – integrates undergraduate course with pre-registration training
Some graduate-entry MPharm degrees taught in 6 semesters over 2 years
No. Some graduate-entry PharmD programmes available.
Some ‘accelerated programmes’ available.
Registration categories
One ‘standard’ type of registration for all practising pharmacists. An annotation to the register entry is made for those with prescribing rights.
1. general registration 2. limited registration: • postgraduate training or
supervised practice • area of need • teaching or research • in the public interest 3. provisional registration 4. non-practising registration 5. student registration
Two: intern and pharmacist Varies between provinces: generally includes student, intern and ‘general’. Alberta has five.
Varies between states: includes student, intern, ‘standard’ and speciality categories.
Work based experience and how it is assessed
Assessed using: Observation – both formal and informal Role plays, simulations Testimonials Projects or assignments The tutor assesses competence and signs off the trainee against each standard.
Must be assessed as competent in all eight categories of the Competency Standards. • Discussion Papers • Training Day • Health Promotion Project • NPS Pharmacy Practice
Review • CMI Assignment (preceptor
evaluation) • MCQ On-Line Assessment
Module • Workbook including diary
3 assessments against the competence standards during the year Assessed by the preceptor.
monitoring of students’ practice in accordance to competences undertaken by preceptor.
monitoring of students’ practice in accordance to competences undertaken by preceptor.
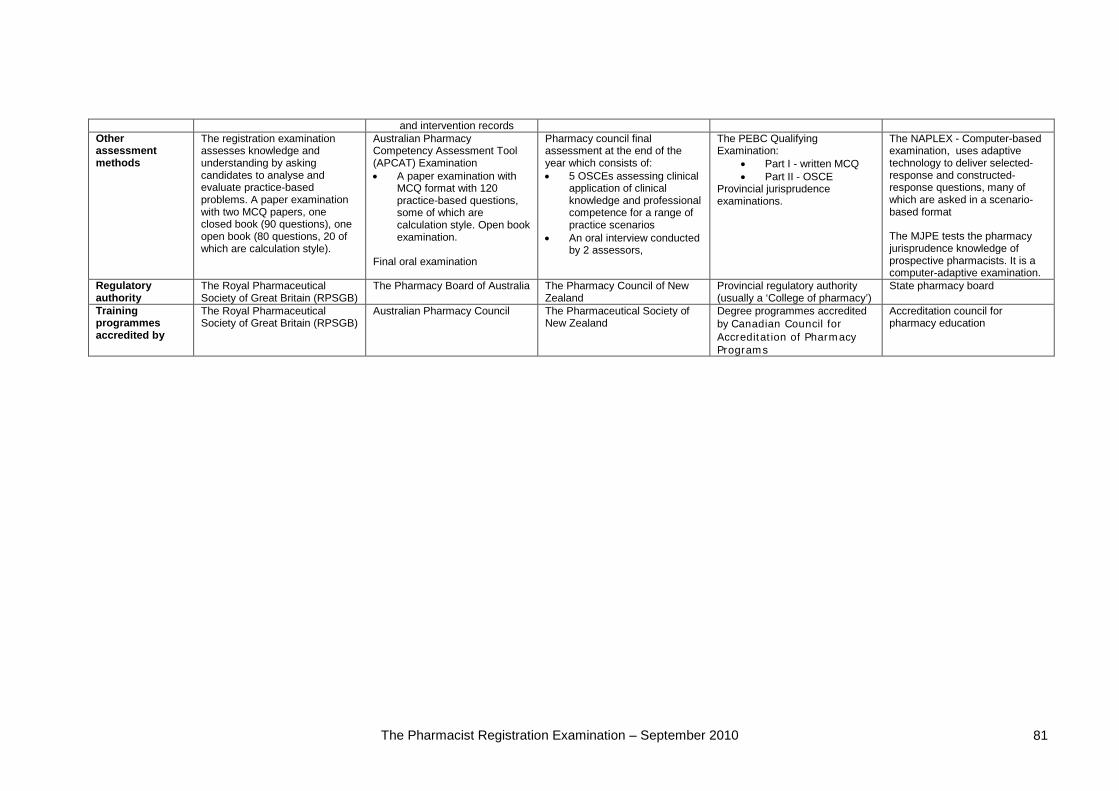
The Pharmacist Registration Examination – September 2010 81
and intervention records Other assessment methods
The registration examination assesses knowledge and understanding by asking candidates to analyse and evaluate practice-based problems. A paper examination with two MCQ papers, one closed book (90 questions), one open book (80 questions, 20 of which are calculation style).
Australian Pharmacy Competency Assessment Tool (APCAT) Examination • A paper examination with
MCQ format with 120 practice-based questions, some of which are calculation style. Open book examination.
Final oral examination
Pharmacy council final assessment at the end of the year which consists of: • 5 OSCEs assessing clinical
application of clinical knowledge and professional competence for a range of practice scenarios
• An oral interview conducted by 2 assessors,
•
The PEBC Qualifying Examination:
• Part I - written MCQ Part II - OSCE
The NAPLEX - Computer-based examination, uses adaptive technology to deliver selected-response and constructed-response questions, many of which are asked in a scenario-based format
Provincial jurisprudence examinations.
The MJPE tests the pharmacy jurisprudence knowledge of prospective pharmacists. It is a computer-adaptive examination.
Regulatory authority
The Royal Pharmaceutical Society of Great Britain (RPSGB)
The Pharmacy Board of Australia Provincial regulatory authority (usually a ‘College of pharmacy’)
The Pharmacy Council of New Zealand
State pharmacy board
Training programmes accredited by
The Royal Pharmaceutical Society of Great Britain (RPSGB)
Australian Pharmacy Council The Pharmaceutical Society of New Zealand
Degree programmes accredited by
Accreditation council for pharmacy education Canadian Council for
Accreditation of Pharmacy Programs
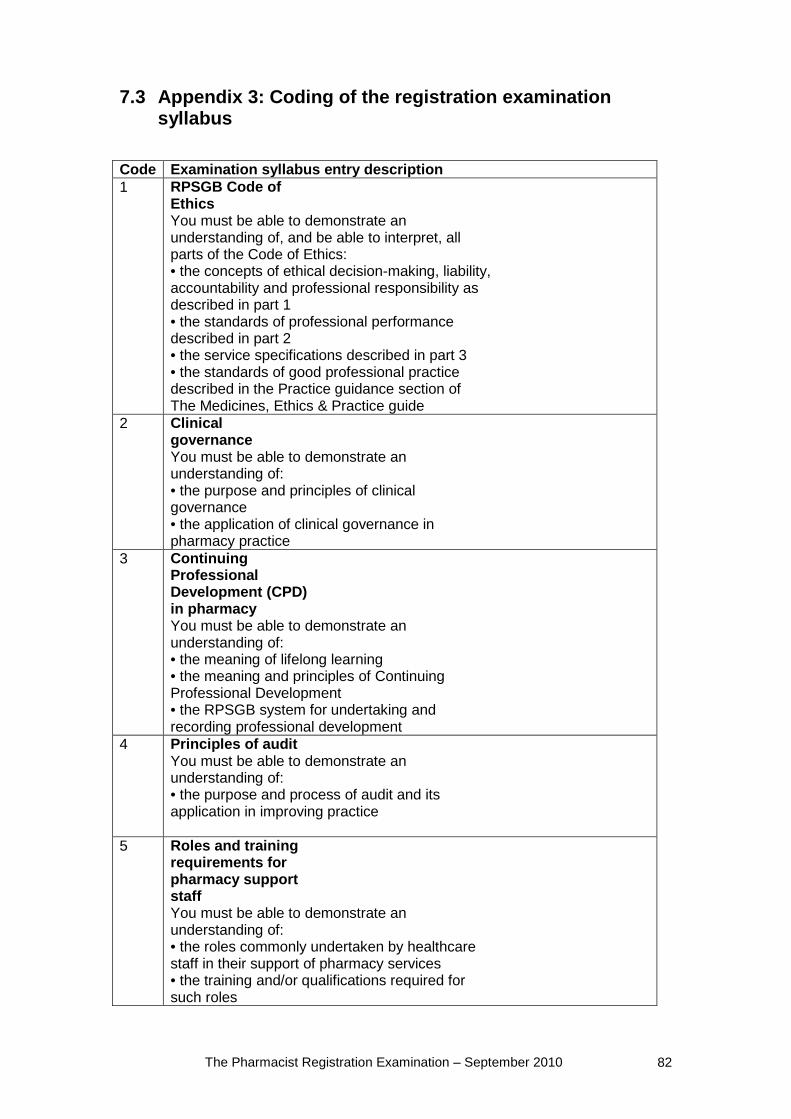
The Pharmacist Registration Examination – September 2010 82
7.3 Appendix 3: Coding of the registration examination syllabus
Code Examination syllabus entry description 1 RPSGB Code of
Ethics You must be able to demonstrate an understanding of, and be able to interpret, all parts of the Code of Ethics: • the concepts of ethical decision-making, liability, accountability and professional responsibility as described in part 1 • the standards of professional performance described in part 2 • the service specifications described in part 3 • the standards of good professional practice described in the Practice guidance section of The Medicines, Ethics & Practice guide
2 Clinical governance You must be able to demonstrate an understanding of: • the purpose and principles of clinical governance • the application of clinical governance in pharmacy practice
3 Continuing Professional Development (CPD) in pharmacy You must be able to demonstrate an understanding of: • the meaning of lifelong learning • the meaning and principles of Continuing Professional Development • the RPSGB system for undertaking and recording professional development
4 Principles of audit You must be able to demonstrate an understanding of: • the purpose and process of audit and its application in improving practice
5 Roles and training requirements for pharmacy support staff You must be able to demonstrate an understanding of: • the roles commonly undertaken by healthcare staff in their support of pharmacy services • the training and/or qualifications required for such roles
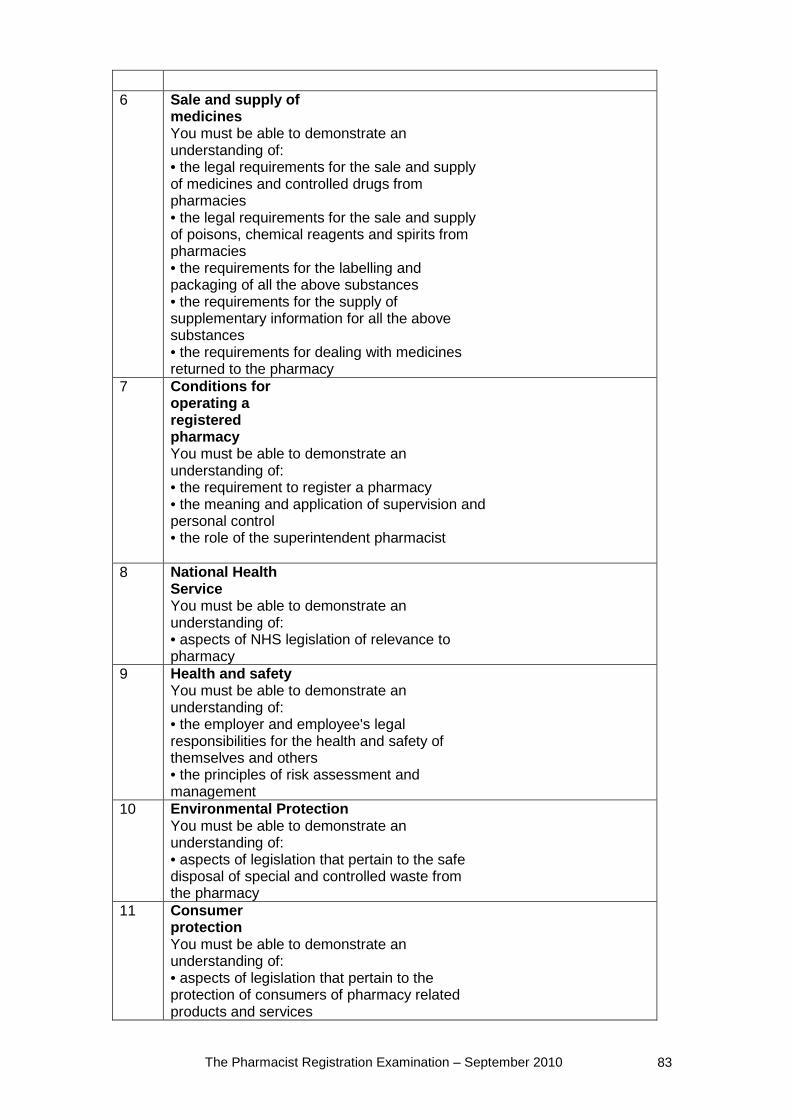
The Pharmacist Registration Examination – September 2010 83
6 Sale and supply of
medicines You must be able to demonstrate an understanding of: • the legal requirements for the sale and supply of medicines and controlled drugs from pharmacies • the legal requirements for the sale and supply of poisons, chemical reagents and spirits from pharmacies • the requirements for the labelling and packaging of all the above substances • the requirements for the supply of supplementary information for all the above substances • the requirements for dealing with medicines returned to the pharmacy
7 Conditions for operating a registered pharmacy You must be able to demonstrate an understanding of: • the requirement to register a pharmacy • the meaning and application of supervision and personal control • the role of the superintendent pharmacist
8 National Health Service You must be able to demonstrate an understanding of: • aspects of NHS legislation of relevance to pharmacy
9 Health and safety You must be able to demonstrate an understanding of: • the employer and employee's legal responsibilities for the health and safety of themselves and others • the principles of risk assessment and management
10 Environmental Protection You must be able to demonstrate an understanding of: • aspects of legislation that pertain to the safe disposal of special and controlled waste from the pharmacy
11 Consumer protection You must be able to demonstrate an understanding of: • aspects of legislation that pertain to the protection of consumers of pharmacy related products and services
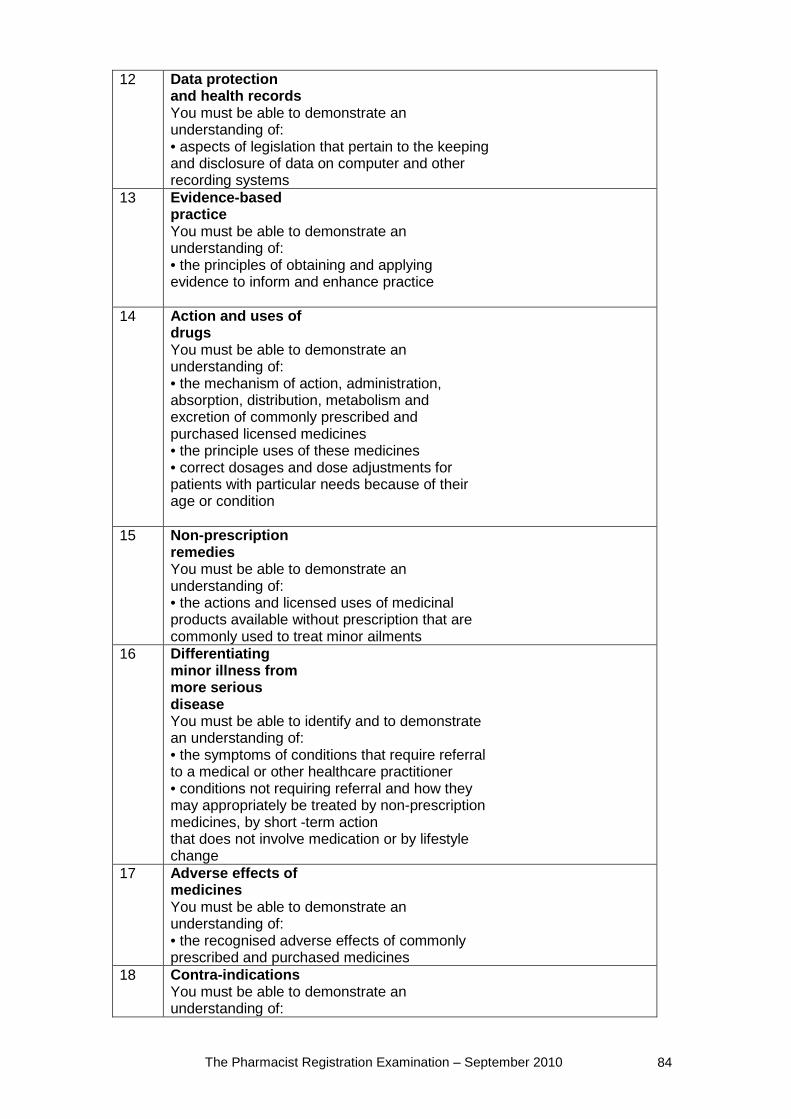
The Pharmacist Registration Examination – September 2010 84
12 Data protection and health records You must be able to demonstrate an understanding of: • aspects of legislation that pertain to the keeping and disclosure of data on computer and other recording systems
13 Evidence-based practice You must be able to demonstrate an understanding of: • the principles of obtaining and applying evidence to inform and enhance practice
14 Action and uses of drugs You must be able to demonstrate an understanding of: • the mechanism of action, administration, absorption, distribution, metabolism and excretion of commonly prescribed and purchased licensed medicines • the principle uses of these medicines • correct dosages and dose adjustments for patients with particular needs because of their age or condition
15 Non-prescription remedies You must be able to demonstrate an understanding of: • the actions and licensed uses of medicinal products available without prescription that are commonly used to treat minor ailments
16 Differentiating minor illness from more serious disease You must be able to identify and to demonstrate an understanding of: • the symptoms of conditions that require referral to a medical or other healthcare practitioner • conditions not requiring referral and how they may appropriately be treated by non-prescription medicines, by short -term action that does not involve medication or by lifestyle change
17 Adverse effects of medicines You must be able to demonstrate an understanding of: • the recognised adverse effects of commonly prescribed and purchased medicines
18 Contra-indications You must be able to demonstrate an understanding of:
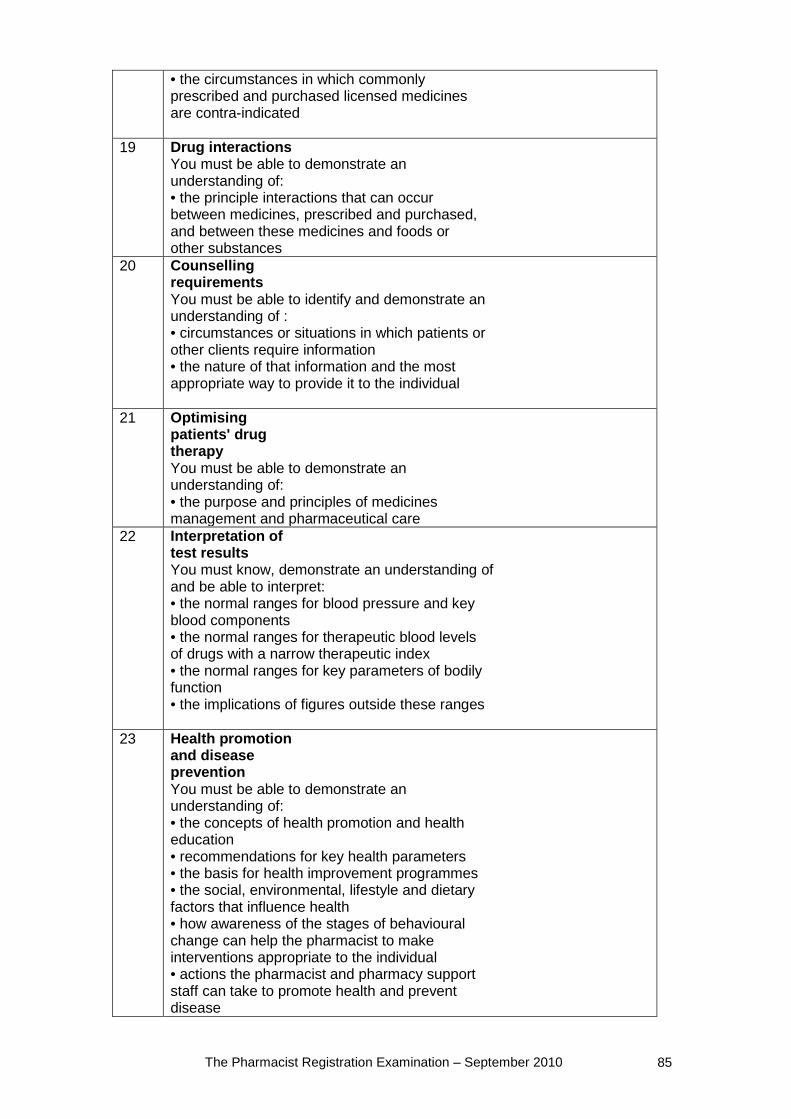
The Pharmacist Registration Examination – September 2010 85
• the circumstances in which commonly prescribed and purchased licensed medicines are contra-indicated
19 Drug interactions You must be able to demonstrate an understanding of: • the principle interactions that can occur between medicines, prescribed and purchased, and between these medicines and foods or other substances
20 Counselling requirements You must be able to identify and demonstrate an understanding of : • circumstances or situations in which patients or other clients require information • the nature of that information and the most appropriate way to provide it to the individual
21 Optimising patients' drug therapy You must be able to demonstrate an understanding of: • the purpose and principles of medicines management and pharmaceutical care
22 Interpretation of test results You must know, demonstrate an understanding of and be able to interpret: • the normal ranges for blood pressure and key blood components • the normal ranges for therapeutic blood levels of drugs with a narrow therapeutic index • the normal ranges for key parameters of bodily function • the implications of figures outside these ranges
23 Health promotion and disease prevention You must be able to demonstrate an understanding of: • the concepts of health promotion and health education • recommendations for key health parameters • the basis for health improvement programmes • the social, environmental, lifestyle and dietary factors that influence health • how awareness of the stages of behavioural change can help the pharmacist to make interventions appropriate to the individual • actions the pharmacist and pharmacy support staff can take to promote health and prevent disease
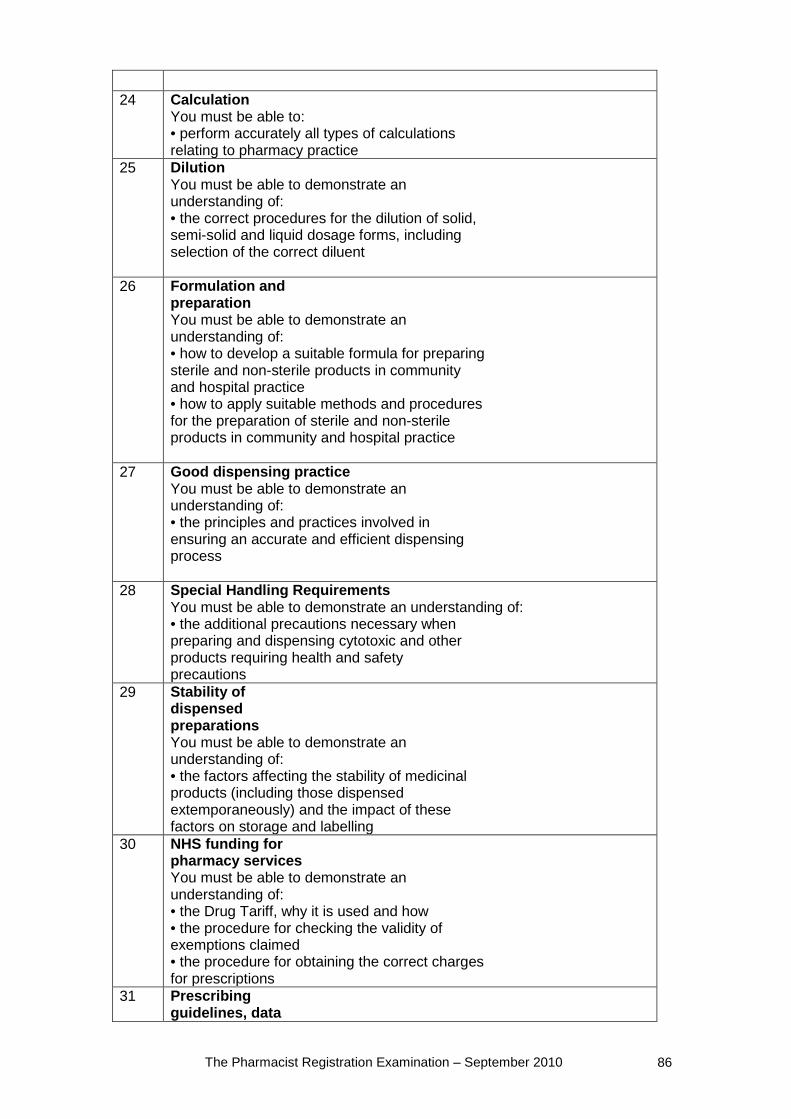
The Pharmacist Registration Examination – September 2010 86
24 Calculation
You must be able to: • perform accurately all types of calculations relating to pharmacy practice
25 Dilution You must be able to demonstrate an understanding of: • the correct procedures for the dilution of solid, semi-solid and liquid dosage forms, including selection of the correct diluent
26 Formulation and preparation You must be able to demonstrate an understanding of: • how to develop a suitable formula for preparing sterile and non-sterile products in community and hospital practice • how to apply suitable methods and procedures for the preparation of sterile and non-sterile products in community and hospital practice
27 Good dispensing practice You must be able to demonstrate an understanding of: • the principles and practices involved in ensuring an accurate and efficient dispensing process
28 Special Handling Requirements You must be able to demonstrate an understanding of: • the additional precautions necessary when preparing and dispensing cytotoxic and other products requiring health and safety precautions
29 Stability of dispensed preparations You must be able to demonstrate an understanding of: • the factors affecting the stability of medicinal products (including those dispensed extemporaneously) and the impact of these factors on storage and labelling
30 NHS funding for pharmacy services You must be able to demonstrate an understanding of: • the Drug Tariff, why it is used and how • the procedure for checking the validity of exemptions claimed • the procedure for obtaining the correct charges for prescriptions
31 Prescribing guidelines, data
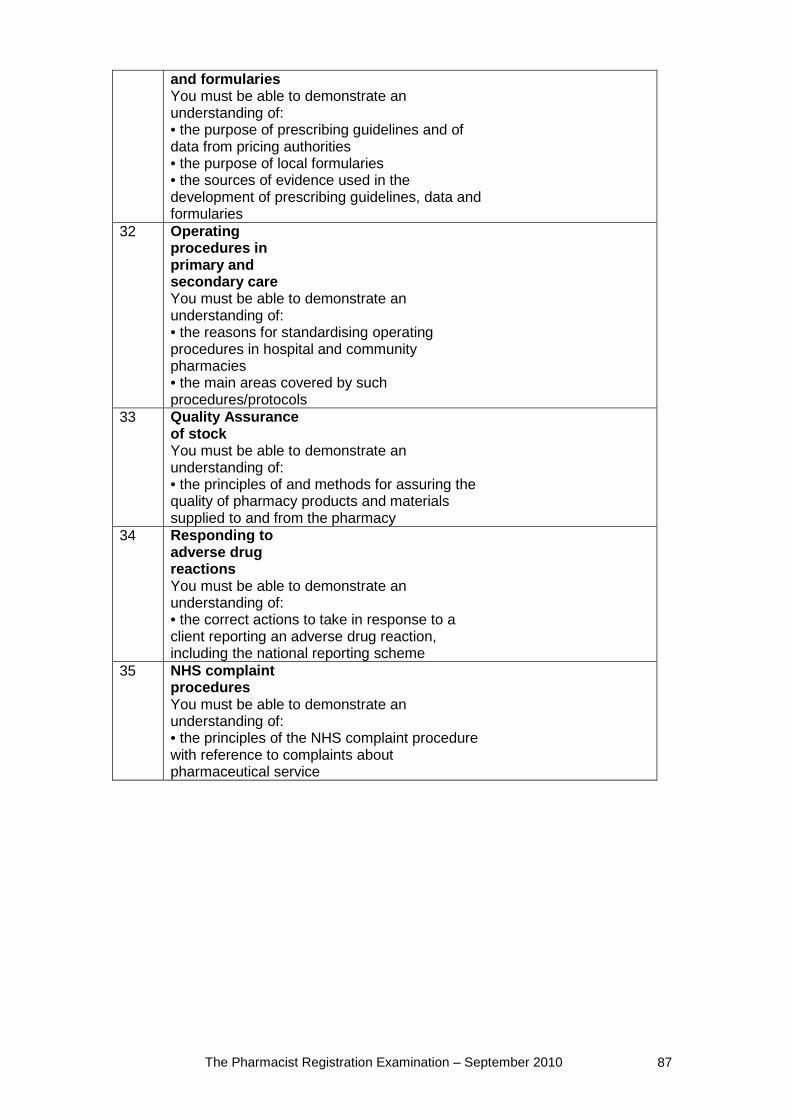
The Pharmacist Registration Examination – September 2010 87
and formularies You must be able to demonstrate an understanding of: • the purpose of prescribing guidelines and of data from pricing authorities • the purpose of local formularies • the sources of evidence used in the development of prescribing guidelines, data and formularies
32 Operating procedures in primary and secondary care You must be able to demonstrate an understanding of: • the reasons for standardising operating procedures in hospital and community pharmacies • the main areas covered by such procedures/protocols
33 Quality Assurance of stock You must be able to demonstrate an understanding of: • the principles of and methods for assuring the quality of pharmacy products and materials supplied to and from the pharmacy
34 Responding to adverse drug reactions You must be able to demonstrate an understanding of: • the correct actions to take in response to a client reporting an adverse drug reaction, including the national reporting scheme
35 NHS complaint procedures You must be able to demonstrate an understanding of: • the principles of the NHS complaint procedure with reference to complaints about pharmaceutical service
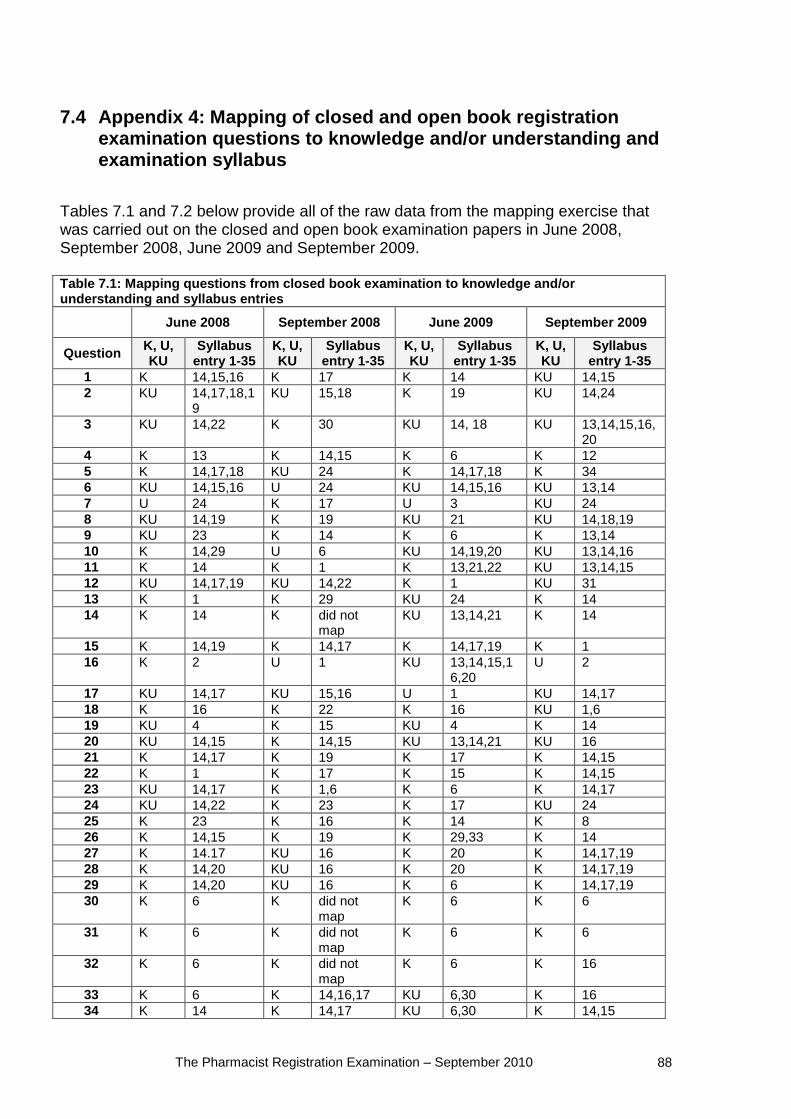
The Pharmacist Registration Examination – September 2010 88
7.4 Appendix 4: Mapping of closed and open book registration examination questions to knowledge and/or understanding and examination syllabus
Tables 7.1 and 7.2 below provide all of the raw data from the mapping exercise that was carried out on the closed and open book examination papers in June 2008, September 2008, June 2009 and September 2009. Table 7.1: Mapping questions from closed book examination to knowledge and/or understanding and syllabus entries
June 2008 September 2008 June 2009 September 2009
Question K, U, KU
Syllabus entry 1-35
K, U, KU
Syllabus entry 1-35
K, U, KU
Syllabus entry 1-35
K, U, KU
Syllabus entry 1-35
1 K 14,15,16 K 17 K 14 KU 14,15 2 KU 14,17,18,1
9 KU 15,18 K 19 KU 14,24
3 KU 14,22 K 30 KU 14, 18 KU 13,14,15,16,20
4 K 13 K 14,15 K 6 K 12 5 K 14,17,18 KU 24 K 14,17,18 K 34 6 KU 14,15,16 U 24 KU 14,15,16 KU 13,14 7 U 24 K 17 U 3 KU 24 8 KU 14,19 K 19 KU 21 KU 14,18,19 9 KU 23 K 14 K 6 K 13,14 10 K 14,29 U 6 KU 14,19,20 KU 13,14,16 11 K 14 K 1 K 13,21,22 KU 13,14,15 12 KU 14,17,19 KU 14,22 K 1 KU 31 13 K 1 K 29 KU 24 K 14 14 K 14 K did not
map KU 13,14,21 K 14
15 K 14,19 K 14,17 K 14,17,19 K 1 16 K 2 U 1 KU 13,14,15,1
6,20 U 2
17 KU 14,17 KU 15,16 U 1 KU 14,17 18 K 16 K 22 K 16 KU 1,6 19 KU 4 K 15 KU 4 K 14 20 KU 14,15 K 14,15 KU 13,14,21 KU 16 21 K 14,17 K 19 K 17 K 14,15 22 K 1 K 17 K 15 K 14,15 23 KU 14,17 K 1,6 K 6 K 14,17 24 KU 14,22 K 23 K 17 KU 24 25 K 23 K 16 K 14 K 8 26 K 14,15 K 19 K 29,33 K 14 27 K 14.17 KU 16 K 20 K 14,17,19 28 K 14,20 KU 16 K 20 K 14,17,19 29 K 14,20 KU 16 K 6 K 14,17,19 30 K 6 K did not
map K 6 K 6
31 K 6 K did not map
K 6 K 6
32 K 6 K did not map
K 6 K 16
33 K 6 K 14,16,17 KU 6,30 K 16 34 K 14 K 14,17 KU 6,30 K 14,15
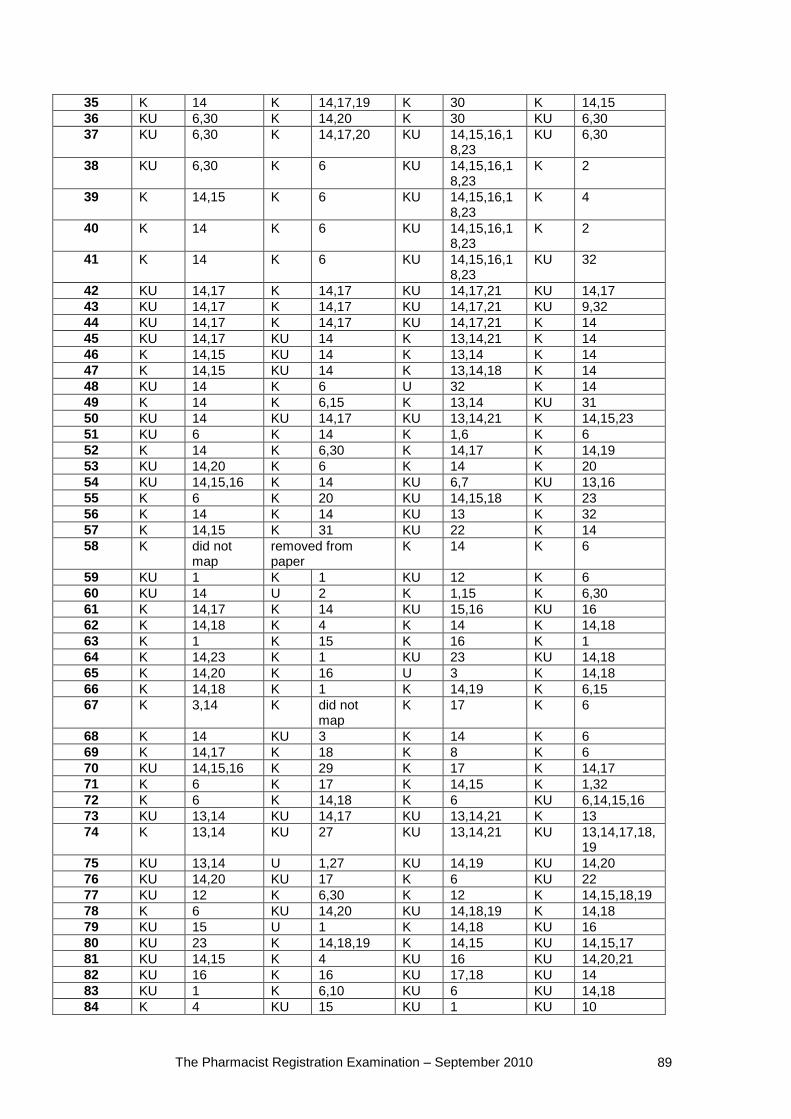
The Pharmacist Registration Examination – September 2010 89
35 K 14 K 14,17,19 K 30 K 14,15 36 KU 6,30 K 14,20 K 30 KU 6,30 37 KU 6,30 K 14,17,20 KU 14,15,16,1
8,23 KU 6,30
38 KU 6,30 K 6 KU 14,15,16,18,23
K 2
39 K 14,15 K 6 KU 14,15,16,18,23
K 4
40 K 14 K 6 KU 14,15,16,18,23
K 2
41 K 14 K 6 KU 14,15,16,18,23
KU 32
42 KU 14,17 K 14,17 KU 14,17,21 KU 14,17 43 KU 14,17 K 14,17 KU 14,17,21 KU 9,32 44 KU 14,17 K 14,17 KU 14,17,21 K 14 45 KU 14,17 KU 14 K 13,14,21 K 14 46 K 14,15 KU 14 K 13,14 K 14 47 K 14,15 KU 14 K 13,14,18 K 14 48 KU 14 K 6 U 32 K 14 49 K 14 K 6,15 K 13,14 KU 31 50 KU 14 KU 14,17 KU 13,14,21 K 14,15,23 51 KU 6 K 14 K 1,6 K 6 52 K 14 K 6,30 K 14,17 K 14,19 53 KU 14,20 K 6 K 14 K 20 54 KU 14,15,16 K 14 KU 6,7 KU 13,16 55 K 6 K 20 KU 14,15,18 K 23 56 K 14 K 14 KU 13 K 32 57 K 14,15 K 31 KU 22 K 14 58 K did not
map removed from paper
K 14 K 6
59 KU 1 K 1 KU 12 K 6 60 KU 14 U 2 K 1,15 K 6,30 61 K 14,17 K 14 KU 15,16 KU 16 62 K 14,18 K 4 K 14 K 14,18 63 K 1 K 15 K 16 K 1 64 K 14,23 K 1 KU 23 KU 14,18 65 K 14,20 K 16 U 3 K 14,18 66 K 14,18 K 1 K 14,19 K 6,15 67 K 3,14 K did not
map K 17 K 6
68 K 14 KU 3 K 14 K 6 69 K 14,17 K 18 K 8 K 6 70 KU 14,15,16 K 29 K 17 K 14,17 71 K 6 K 17 K 14,15 K 1,32 72 K 6 K 14,18 K 6 KU 6,14,15,16 73 KU 13,14 KU 14,17 KU 13,14,21 K 13 74 K 13,14 KU 27 KU 13,14,21 KU 13,14,17,18,
19 75 KU 13,14 U 1,27 KU 14,19 KU 14,20 76 KU 14,20 KU 17 K 6 KU 22 77 KU 12 K 6,30 K 12 K 14,15,18,19 78 K 6 KU 14,20 KU 14,18,19 K 14,18 79 KU 15 U 1 K 14,18 KU 16 80 KU 23 K 14,18,19 K 14,15 KU 14,15,17 81 KU 14,15 K 4 KU 16 KU 14,20,21 82 KU 16 K 16 KU 17,18 KU 14 83 KU 1 K 6,10 KU 6 KU 14,18 84 K 4 KU 15 KU 1 KU 10
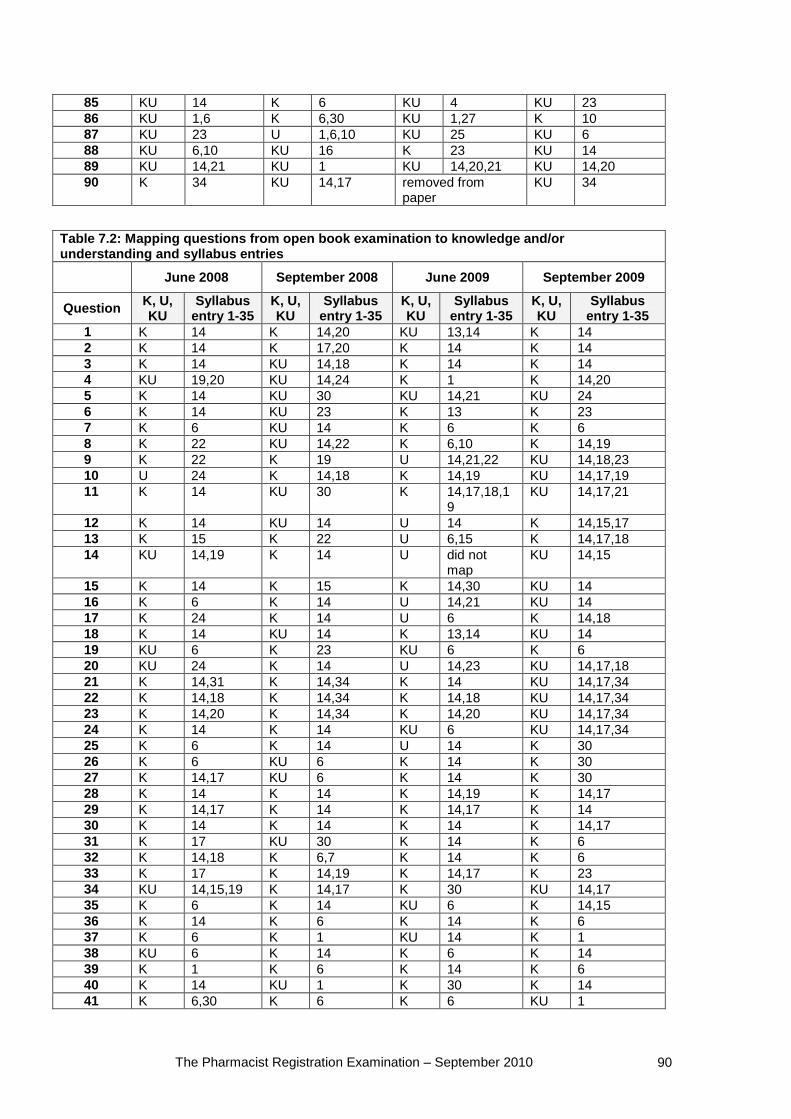
The Pharmacist Registration Examination – September 2010 90
85 KU 14 K 6 KU 4 KU 23 86 KU 1,6 K 6,30 KU 1,27 K 10 87 KU 23 U 1,6,10 KU 25 KU 6 88 KU 6,10 KU 16 K 23 KU 14 89 KU 14,21 KU 1 KU 14,20,21 KU 14,20 90 K 34 KU 14,17 removed from
paper KU 34
Table 7.2: Mapping questions from open book examination to knowledge and/or understanding and syllabus entries June 2008 September 2008 June 2009 September 2009
Question K, U, KU
Syllabus entry 1-35
K, U, KU
Syllabus entry 1-35
K, U, KU
Syllabus entry 1-35
K, U, KU
Syllabus entry 1-35
1 K 14 K 14,20 KU 13,14 K 14 2 K 14 K 17,20 K 14 K 14 3 K 14 KU 14,18 K 14 K 14 4 KU 19,20 KU 14,24 K 1 K 14,20 5 K 14 KU 30 KU 14,21 KU 24 6 K 14 KU 23 K 13 K 23 7 K 6 KU 14 K 6 K 6 8 K 22 KU 14,22 K 6,10 K 14,19 9 K 22 K 19 U 14,21,22 KU 14,18,23 10 U 24 K 14,18 K 14,19 KU 14,17,19 11 K 14 KU 30 K 14,17,18,1
9 KU 14,17,21
12 K 14 KU 14 U 14 K 14,15,17 13 K 15 K 22 U 6,15 K 14,17,18 14 KU 14,19 K 14 U did not
map KU 14,15
15 K 14 K 15 K 14,30 KU 14 16 K 6 K 14 U 14,21 KU 14 17 K 24 K 14 U 6 K 14,18 18 K 14 KU 14 K 13,14 KU 14 19 KU 6 K 23 KU 6 K 6 20 KU 24 K 14 U 14,23 KU 14,17,18 21 K 14,31 K 14,34 K 14 KU 14,17,34 22 K 14,18 K 14,34 K 14,18 KU 14,17,34 23 K 14,20 K 14,34 K 14,20 KU 14,17,34 24 K 14 K 14 KU 6 KU 14,17,34 25 K 6 K 14 U 14 K 30 26 K 6 KU 6 K 14 K 30 27 K 14,17 KU 6 K 14 K 30 28 K 14 K 14 K 14,19 K 14,17 29 K 14,17 K 14 K 14,17 K 14 30 K 14 K 14 K 14 K 14,17 31 K 17 KU 30 K 14 K 6 32 K 14,18 K 6,7 K 14 K 6 33 K 17 K 14,19 K 14,17 K 23 34 KU 14,15,19 K 14,17 K 30 KU 14,17 35 K 6 K 14 KU 6 K 14,15 36 K 14 K 6 K 14 K 6 37 K 6 K 1 KU 14 K 1 38 KU 6 K 14 K 6 K 14 39 K 1 K 6 K 14 K 6 40 K 14 KU 1 K 30 K 14 41 K 6,30 K 6 K 6 KU 1
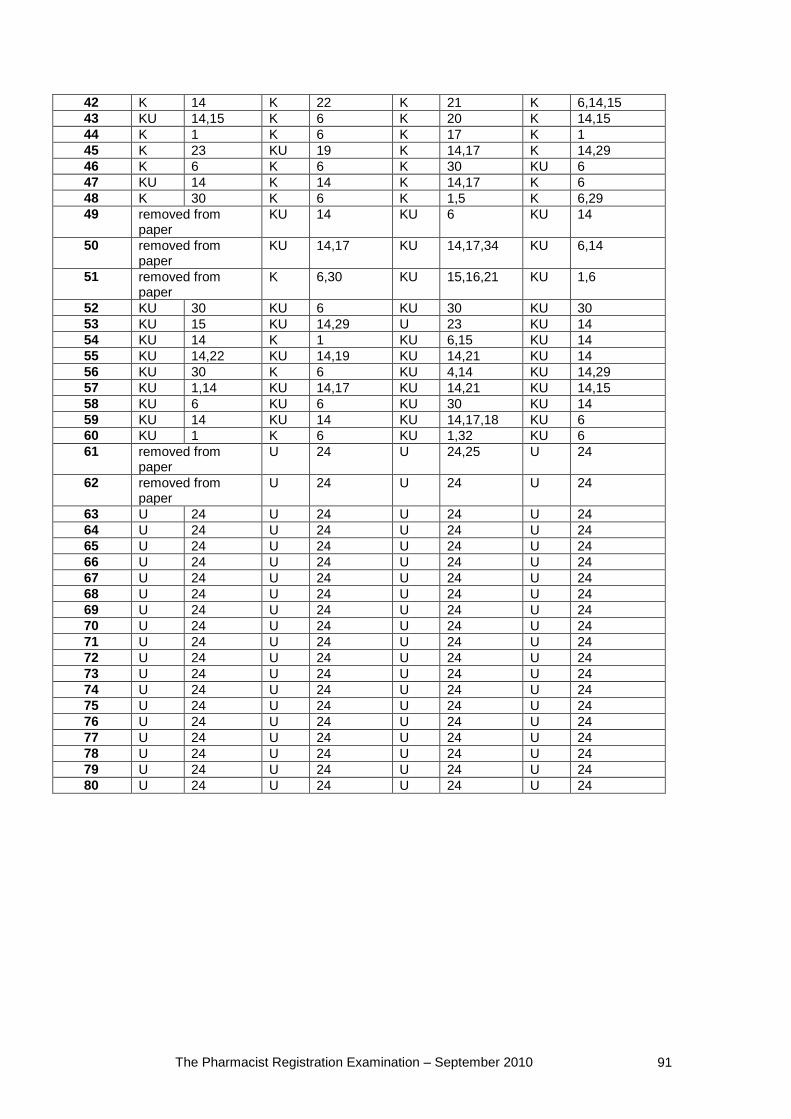
The Pharmacist Registration Examination – September 2010 91
42 K 14 K 22 K 21 K 6,14,15 43 KU 14,15 K 6 K 20 K 14,15 44 K 1 K 6 K 17 K 1 45 K 23 KU 19 K 14,17 K 14,29 46 K 6 K 6 K 30 KU 6 47 KU 14 K 14 K 14,17 K 6 48 K 30 K 6 K 1,5 K 6,29 49 removed from
paper KU 14 KU 6 KU 14
50 removed from paper
KU 14,17 KU 14,17,34 KU 6,14
51 removed from paper
K 6,30 KU 15,16,21 KU 1,6
52 KU 30 KU 6 KU 30 KU 30 53 KU 15 KU 14,29 U 23 KU 14 54 KU 14 K 1 KU 6,15 KU 14 55 KU 14,22 KU 14,19 KU 14,21 KU 14 56 KU 30 K 6 KU 4,14 KU 14,29 57 KU 1,14 KU 14,17 KU 14,21 KU 14,15 58 KU 6 KU 6 KU 30 KU 14 59 KU 14 KU 14 KU 14,17,18 KU 6 60 KU 1 K 6 KU 1,32 KU 6 61 removed from
paper U 24 U 24,25 U 24
62 removed from paper
U 24 U 24 U 24
63 U 24 U 24 U 24 U 24 64 U 24 U 24 U 24 U 24 65 U 24 U 24 U 24 U 24 66 U 24 U 24 U 24 U 24 67 U 24 U 24 U 24 U 24 68 U 24 U 24 U 24 U 24 69 U 24 U 24 U 24 U 24 70 U 24 U 24 U 24 U 24 71 U 24 U 24 U 24 U 24 72 U 24 U 24 U 24 U 24 73 U 24 U 24 U 24 U 24 74 U 24 U 24 U 24 U 24 75 U 24 U 24 U 24 U 24 76 U 24 U 24 U 24 U 24 77 U 24 U 24 U 24 U 24 78 U 24 U 24 U 24 U 24 79 U 24 U 24 U 24 U 24 80 U 24 U 24 U 24 U 24
Related Documents











