
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
The Permanente Journal / Spring 2000 / Volume 4 No. 2
The Permanente Journal, 500 NE Multnomah St, Suite 100, Portland, OR 97232
Mission...The PermanenteJournal is written andpublished by theclinicians of thePermanente MedicalGroups and KFHP topromote the delivery ofsuperior health carethrough the principlesand benefits ofPermanente Medicine.
Where to find ThePermanente Journal...A full-text version isavailable on our Web site(www.kaiserpermanente.org/permanentejournal.html).In addition, copies of theJournal are available inKaiser Permanentelibraries Programwide.
How to Contact ThePermanente Journal…E-mail us [email protected]
Call us at (503) 813-4387
Fax us at (503) 813-2348
If you have any questionsregarding distribution ofthis journal, pleasecontact Amy Eakin at(503) 813-2623, ore-mail: [email protected]
48 Asthma Disease Management Program. Colorado Region
This program included registry development, guideline dissemination, classes, and management by nursesof pediatric and adult asthma patients. Planned measures of the impact of the program are utilization,patient and physician satisfaction, appropriateness of medications and cost-effectiveness. The preliminarydata suggest improved quality, satisfaction and utilization outcomes. Noteworthy among the results isreduced overuse of beta-agonist medication. Similar programs are rapidly becoming standard of care.
57 Emergency Contraception Research and Demonstration Project. Southern California Region
This project, a collaboration between Southern California Kaiser Permanente and others, evaluated theacceptability and feasibility of emergency contraception (EC, or “morning-after pills”). Aspects describedinclude packaging and availability problems, education and training of staff, and ensuring adequate patientunderstanding. All objectives were met with high patient satisfaction and probable cost savings.
66 The Breast Health and Cancer Detection Program. Georgia Region
With a target population of all women in the Kaiser Permanente Georgia Region 50 years of age or older, thisprogram includes attempts to improve member access, member and practitioner awareness, and practitioneradherence. The screening rates in the targeted group rose from 74% in 1996 to 84% in 1999 (p < 0.0001).Telephone calls and mailings to women overdue for mammography screening seemed to be especially effective.Reduced breast cancer morbidity and mortality are among the probable long-term expected results.
78 Improvement of Cardiac Outcomes in Kaiser Permanente of Ohio. Ohio Region
This project involved the use of reminder notices to practitioners caring for patients with coronary disease(CAD) as a means of improving care. The specific targets were four interventions proven beneficial forCAD; these were regular aspirin use, smoking cessation, cholesterol lowering, and use of beta-blockerdrugs. Substantial increase in compliance was demonstrated as well as concomitant decrease inhospitalizations for CAD.
Soul of the Healer8 Cats’ Hill Criterium. J. Richard Gaskill, MD
16 Peacock at the Window. J. Richard Gaskill, MD
84 A Bunker in the Storm. Anonymous.
A Word from the Medical Directors85 Can Managing Cost Be Part of Managing Care? Donald L. McGuirk, MD
Health Systems87 Potential Abuses of Group Visits. Edward B. Noffsinger, PhD; John C. Scott, MD
Since this exciting new model for patient encounters is spreading across the Program, this article will beextremely valuable to those Permanente Groups who are beginning their Group Visit programs.

tab
le o
f co
nte
nts
99 Understanding Today’s Group-Visit Models. Edward B. Noffsinger, PhD; John C. Scott, MD
While there has been much written recently on group visits, this article may be the best overall discussionof this exciting new innovation.
113 What does the STAR Survey mean to a Permanente Physician?Interview with David Glass, National Director of Market Research
This interview with David Glass, the National Director of Market Research, addresses this survey tool andthe important information that it can provide to the Permanente Medical Groups.
External Affairs115 Primum Non Nocere: Safety, Medical Errors, and Congressional Intent. Donald W. Parsons, MD
After the Institute of Medicine report on medical errors in hospitals, patient safety has become a hotpolitical topic. Kaiser Permanente has been a leader in improving patient safety. Our integrated health caresystem and our previous track record give us an enviable position in being able to be a leader inimproving patient safety.
117 Kaiser Permanente’s Response to JCAHO’s Sentinel Event Standards:Our Significant Event Root-Cause Analysis Program Leads to Preventing Medical Errors.Ricki Stajer, RN, MA, CPHQ; Bud Pate, REHS
This article is one of Kaiser Permanente practical approaches to improving patient safety. KaiserPermanente’s policy on significant events is reviewed and how it meets the JCAHO policy regardingsentinel events. We have learned that blaming individuals has the effect of decreasing our ability to find theroot cause of the significant event.
Book Reviews124 “The Back Pain Revolution,” by Gordon Waddell, Alf L. Nachemson (Introduction), Reed B.
Phillips (Introduction). Gary Stein, MD
125 “God Unmasked; the Full Life Revealed,” by Ernest Lane, MD. Albert Ray, MD
Announcements126 Free Hemochromatosis Information ◆ National Primary Care Conference Audio Tape Order Form ◆
San Diego Physician Chairs California’s Young Physician Group ◆ In Memoriam
Instructions for Authors128 We want you to submit your work. Look here to find out how.
CME131 Complete this form to receive Category 1 Credit.
?

3The Permanente Journal /Spring 2000 / Volume 4 No. 2
ed
itor’s co
mm
en
ts
Editor’s Comments
Healing Physicians: Physicians HealingTom Janisse, Editor-in-Chief
In Western medicine, as a discipline andprofession, physicians practice science, nothealing. Attention to the “art” of medicinehas waxed and waned over time in an at-
tempt to characterize the other part of what physicianspractice with patients—that interpersonal dimension,that feeling state, the caring for a patient who is illwith a disease. This artful practice can be viewedwithin the realm of a healing practice.
The word “healing” has recently surfaced withinthe practice of medicine. Though still peripheral,healing is heard in healthcare conversation, and isvisible in articles and in books related to medicine.Actual healing practice is more common in alterna-tive medicine, and appears foremost in the ancientpractice of shamanism—a spiritual practice. The sha-man—better recognized in the Western world as the“medicine man” or the “spirit doctor”—aids the trans-formation of a person from illness to health, often ina ceremonial setting. Using ritualistic practices, theshaman invokes the spirits (within humans, and fromthe non-ordinary, spiritual plane) to diagnose thecausative factor, then heals the person, restoring bal-ance or “wholeness.” Based on the original derivationof the word, to heal is to make whole.
In his book, “The Spirit of Healing,” David Cumes,a Stanford-trained surgeon, raised in South Africa,introduces to Western medicine the Kalahari desertshamans’ practice of healing medicine. He cites fourfactors involved in shamanic healing, that are simi-larly present in today’s doctor–patient encounter:
1. The healer2. The patient’s inner healer,3. The place, and4. The universal field.1
Stanley Krippner, psychologist and paranormal ex-pert, author of many books including “SpiritualDimensions of Healing: From Tribal Shamanism toContemporary Health Care,” offers a confirmatoryperspective, based upon his experience with alter-native practices. He describes four basic reasons whytreatments in any therapeutic setting work:
1. The practitioner’s personal qualities,2. The person’s expectations,3. The treatment, and4. A shared world view.2
Viewing these two sets of four components side-by-side broadens our understanding of the interactivenature of these aspects on effective healing.
Physicians may have lost a sense of the importancethey play as a person in their interactions with theirpatients. A purely intellectual exchange with only aphysical outcome is often ineffectual in treating apatient’s condition, which has both a physical com-ponent and a personal component (psychological,emotional, social, spiritual). Knowledge of theshaman’s practice can assist redirecting a physician’spractice toward a more balanced approach. This doesnot require physicians to learn completely knew skills,or practice unfamiliar ceremonial rituals in their of-fice. Rather, the physician’s personal self (the healer)can connect in “the human moment”3 with thepatient’s personal self (the inner healer) in an officeor hospital environment (the place) when both havea common understanding, or better, a common be-lief system (the universal field).
Before we further discuss the components of thisshaman-native or doctor-patient relationship, it isimportant to explore the difference between curingand healing.
Curing vs Healing: Disease vs IllnessDifferent than curing—ridding the patient of dis-
ease symptoms and the body of the physicalcause—healing not only alleviates physical symp-toms, but, more importantly, resolves a person’sillness—those psychological, emotional, social andspiritual aspects that cause distress. In addition,healing practices prepare a person to prevent theillness and disease from returning, and attempt, ina larger life context, to heal the family and eventhe community.
Illness has a very personal description and mean-ing. Psychologist and Native American storyteller,Terry Tafoya, cites an example: “Tomorrow in youroffice you see a Shoshonee Native American forworsening diabetes. If you ask, ‘Why did you be-come sick?’ He may say, ‘I am sick because yourpeople took my sacred mountain, built over our cer-emonial burial ground, or clear-cut my forest.’ Anyof these acts could spiritually wound this Shoshoneenative who believes he is part of nature, and hisnature has been violated.”4 This illness may worsenhis diabetic physical condition.
Cultural practice can be the dominant determi-nant of an ethnic patient’s behavior. Overlookingthis context, diagnosis is a futile exercise. The fol-lowing story paints a vivid image. A middle-agedHaitian immigrant woman was brought into one ofour Kaiser Permanente mental health offices by a

4 The Permanente Journal / Spring 2000 / Volume 4 No. 2
ed
ito
r’s
com
men
ts
concerned neighbor. Her husband had recentlypassed away after a long illness. She spoke English,but not very well. Her summary statement was, “Idon’t want to do anything; I don’t want to see any-one.” She would not go out of the house; shewouldn’t talk to her friends; she wouldn’t have any-one into her house; and she wore only black. Basedon her behavior, the therapist believed she was suf-fering from complicated and severe depression. Thetherapist treated her for several months, finding anybreakthrough difficult. He suggested that she go out,see friends, have someone over for dinner. She re-fused any suggestions. Finally, he resorted to anexploration of her cultural belief system that mightbe interfering with her recovery. He asked if shewould be better going back to Haiti. She said no.The breakthrough came when he asked her howother Haitian women would handle the death oftheir husband. She replied that a year must passfirst. That only after one year of mourning—wear-ing black and staying inside—could she againparticipate in community activities. This was a nor-mal Haitian ritual of year-long mourning. At yearendshe would put on a red dress and dancing shoesand go out with friends to celebrate. Her depres-sive-appearing behavior was a self-imposedsociocultural belief and grieving process. She was“ill” without disease. In fact, her emotional state wasone of mourning, not illness.
Stanford physician, Alan Barbour, and author of thebook, “Caring For Patients,” describes in the follow-ing diagram “the elements of the doctor’s responsibility
for the disease (the medical model) and those of thedoctor’s responsibility for the ill person.”5
Curing a disease is a reductionist approach, frag-menting the organ from the whole person. It is anexpression of the biomedical model of the body as amachine with a broken part. People are more thanthe sum of their parts.
1. HealerThe words “healer” and “healing” sound strange
and unfamiliar to physicians since they were rarelyspoken or referenced in medical school. The onlyreference I can recall is to “wound healing.” We weretrained to restore organ function, but not in the con-text of restoring balance, personal or family, emotionalor spiritual.
Internist-author of the book “Healing Words,” LarryDossey also wrote, as editor of the journal “Alterna-tive Therapies,” an article called, “Whatever Happenedto Healers?” He commented on physician training:“Medical school, instead of nurturing and develop-ing the natural healing talents of gifted young studentswho have sought to help people, seem adept at ex-tinguishing them.
The first two years seem to desensitize studentswith the endless lectures and information and dataand memorization and the sparse contact with pa-tients.” A medical student, in a letter written to him,exclaimed that medical school “…crushed the hu-man person into the spiritless formula of science.”6
How can we expect compassionate physicians toemerge from such a dispassionate training program?
Addressing a more widespread phenomenon in ourmodern culture, New Yorker cartoonist, Cheney,draws out an image applicable to medicine. The sceneis a hallway in any office building. Several peoplegather around a man who just dropped a sheaf ofpapers that lay strewn on the floor at his feet. Hepresses his left hand against his chest and his righthand braces him against the wall. He says, “Really,I’m fine. It was just a fleeting sense of purpose…I’msure it will pass.“7 This fleeting sense of purpose fora doctor is the caring for a person who is ill, ratherthan our frenetic, headlong rush to cure a patient’sdisease or just ameliorate their symptoms with a drug.
To accomplish this, physicians must reconnect withtheir own personal, emotional, and spiritual self. DrDavid Cumes comments on this: “It is ego that leadsphysicians to believe they know best. It is ego thatenjoys the patient who shuts up, follows instructions,and falls into the role of passive victim with the dis-ease. Many physicians become disconnected fromtheir spiritual self because of the rigors of their pro-fession, and are thus incapable of ‘seeing’ the soulsof their patients. Some physicians are wounded inthe medical training process and so this becomes adeterrent to their ability to heal themselves or theirpatients. Some of the best Western physicians haveshamanic abilities and often put them to good use
Patients PersonsDisease IllnessUnderstanding the Understanding the Biological Situation Personal SituationDiagnosis Clinical JudgmentCuring HealingTreatment CollaborationEradicating Sickness Achieving Health
Doctor
Barbour, A. Caring for Patients. Stanford, CA: Stanford University Press; 1995:32.

5The Permanente Journal /Spring 2000 / Volume 4 No. 2
ed
itor’s co
mm
en
ts
without realizing it. However, Western medicine hasdifficulty validating these nonobjective methods thatare not easily measured. The portal to this alterna-tive healing is the right brain, and, for this, we needto open the heart. We need more heart in our mod-ern system and a little less intellect.”1
If we recall the yearning we had to become doc-tors; the desire we had to help other people; thechance, through our work, to perform a greater good,to achieve a higher purpose, how does that expressitself today? Has medical school and modern medi-cal practice dropped the enormous, dense, complexscience of medicine onto the physician’s heart, caus-ing shortness of breath and profound fatigue? Howcan the spirit of the art of medicine energize the prac-tice of medicine to restore the balance necessary forphysicians to simultaneously treat the physical dis-ease of diabetes and the personal distress of beingan ill diabetic? Curing addresses the former, healingis what addresses both.
Even for the most intellectual scientist among us, ifwe are considering simple ways to connect with pa-tients that have value for them, then the electronicmedical record (accessible at the time of visit), oreven the paper chart (if available at the visit), can beused to advantage. Recording several words in a so-cial history about personal aspects of a patient orcomments about family members, or important lifeepisodes, can remind you about your patient.8 Re-calling a personal moment with your patient canreconnect you at the personal level. This is true evenif the patient knows you remember only becauseyou made a note in their record. That you thoughtenough to note something personal, and then men-tion it later, demonstrates you care about them as aperson, or at least that you are attempting to relateon a personal level. This is one way to act like aphysician healer.
What are the qualities that a shaman (or physicianhealer) possesses? Rolling Thunder, a nationallyknown Native American shaman, describes a differ-ence in our peoples: “Primitive people have naturalhuman capacity, ability and powers which exceedmodern humans. Moderns experience less of ourhuman potential—in sight, sound, touch and smell—than ever before. We do so many unnatural thingsnow, we don’t know what is natural anymore.”9 Ouremphasis on the external and material world resultsin a reduced sensitivity to the internal and spiritual.Dr Cumes says: “The shaman embraces mystiquerather than methodology, the compassionate and the
empathic rather than the objective and impersonal,the intuitive rather than the rational. The marriage ofscience and shamanism creates equilibrium and ful-fills the requirement of balancing the opposites formore complete healing.”1
In a more mundane sense, shamanic healing at-tributes would fall generally into the areas ofawareness, beliefs, personal qualities, practice—whatwe say and do. Dr Dossey notes: “Because there maybe no such thing as a perfect fit between the beliefsof a physician and a patient, two of the most valu-able qualities a physician can cultivate are those offlexibility and tolerance. These capacities make itpossible for a physician to honor a patient’s point ofview, even though it may not be his or her own; andthey permit the physician to consider a variety ofapproaches to a particular problem.”10
Peter Silberfarb, psychiatrist and director of theAmerican Board of Family Practice, says, “You’ll neverfind out what worries patients unless you listen, andlistening doesn’t take a lot of time, for a good doctor.You don’t have to spend a lot of time, but you haveto spend time being totally focused on the person.Many patients are not looking for anything but reas-surance that they’ll be okay in our hands.”11
These and other personal qualities of composureand confidence, appropriate emotion and body lan-guage, all build toward an endpoint of developing asense of trust. Ultimately, it is to get beyond the purelyintellectual and cognitive. It is to be a person withanother person.
2. PatientThe patient is the focus of healing. Both the physi-
cian and the patient are focused on improving thepatient’s medical condition and on enhancing thepatient’s well being. Even as physicians must movepast the scientist and search their inner personal self,so patients need to be in touch with their emotions,psyche, social context, and spirituality because ulti-mately people heal themselves. A patient who onlyadmits his physical symptoms and seeks relief with apill or procedure will not effectively treat his illness.Components of the patient’s inner self include: theirexpectations, beliefs about the doctor, the treatment,the potential for improvement, the ability to interactwith the doctor in a human moment, and their inten-tion to get better. “The belief that therapy can dosomething to cure a problem is so powerful that thisfaith has to be taken into account when evaluatingthe ‘actual effect’ of different treatments.”1

6 The Permanente Journal / Spring 2000 / Volume 4 No. 2
ed
ito
r’s
com
men
ts
Figure 1.
In addition, the support and intentions offamily and friends assist the patient’s efforts to heal.One of the strengths a person has is a family they areconnected to and that supports them. In some fami-lies it is the grandparents who are the decision-makersand who must be consulted. When their opinion isconsistent with the patient’s wishes, synergy occurs.
Belief and Hope
Much has been said about the placebo response,usually to malign it, discount it, or fancifully invokeits effects out of frustration for lack of medical alter-natives. Researchers are annoyed with placebo effectswhich, if present, must be accounted for or compen-sated for in the experimental group. Despite variousopinions most people associate the placebo responsewith belief. If belief is powerful then the responsecan be dramatic. Shaman know the power of beliefand use it to great advantage forthe person they are healing.
“If healers disturb the belief sys-tem of the patient by the impositionof their own belief, they will com-promise the magical ability of thesystem to work. Faith or belief inthe healer is critical, and there mustbe a consistency between thepatient’s notion of healing and thedoctor’s approach. A Westerner maybe satisfied with a written prescription and explanationas to how the medication is going to work; a San(Kalahari desert) native would trust a hands-on approachcombined with some sweat from a San dancer in apost-trance state. Similarly, if physicians dispense treat-ments they do not believe in, this weakens the placeboeffect by contracting the field of possibilities, and worksagainst a desired outcome by both doctor and patient.”1
How can this approach be applied in a Westernmedical office? “Some doctors exude a sense of un-ruffled calm, certainty, trust, composure, andconfidence, that augments the placebo effect.”1
To offer a perspective on this from paranormal re-search, psychologists Braud and Schlitz demonstratedin a study that one person (an influencer) could cre-ate a reproducible physiologic change (calming oractivation) in another distant person (the subject)through intention and visualizing images. “Certainpsychological conditions in the influencer appear toplay a role in the success of the intentions and imag-ery: confidence, belief, positive expectation,motivation, level of spontaneity, mood, and rapport.”12
3. Place“Bedside manner,” the metaphor for a physician’s
comforting personal presence, if not compassion,lacks visual potency in the now more common out-patient setting in the doctor’s office in a large medicaloffice. If we examine for a moment the “exam room,”what pleasing aesthetics are present there to com-fort, or to lend a sense of “place,” important as contextfor a meaningful interaction between doctor andpatient? Are we expecting too much from the physi-cian in conversation or in empathy to overcome thesterility of the setting? Barren, white rooms with coldsurfaces and jarring metal sounds served well to com-municate that no germs lived here. But it’s also difficultto find heart here. How can we expect a doctor tohave an artful encounter?
Of course, healing occurs in many other places. Sha-man perform their ceremonies in the wilds of nature,
in communal gathering places, orin a native’s residence. Place is asmuch about a comfortable environ-ment of any kind. What is a strainto imagine, however, is how anexam room can achieve a sense ofplace. Nonetheless, many wonder-ful encounters occur here betweenpatient and doctor. It is actually atribute to the ability of two peopleto overcome physical structure in
reaching a state of mutual benefit.What physicians could at least attend to is the envi-
ronment of their offices and exam rooms. Look atthem with a new awareness and with an eye forcomforting and engaging pictures and mementos,with diversity that appeals to many, and with someattention to the furniture. What is the patient’s chairlike? What is the room setup that allows you and thepatient to interact most comfortably?
4. The FieldThe fourth component of healing is the field, which
can be described variously as a spiritual plane, collec-tive unconscious, a common consciousness, or moreeasily understandable as: a common culture, commonexperiences, similar belief systems, a shared feelingstate, or a shaman-native or physician-patient relation-ship. Ultimately, the desired state (field) is aninterpersonal relationship of trust and understanding.
What complicates this, however, is the unidimen-sional perspective people possess in Western culture.Tafoya notes, “When we are trained to see something

7The Permanente Journal /Spring 2000 / Volume 4 No. 2
ed
itor’s co
mm
en
ts
in a certain way we are also trained to ignore thealternate. For example, look at the image in Figure 1.
We are trained to see the black ink on the page—the wave—but we don’t see the white space—thespiral—or the black wave and white spiral together asa whole image.”4 For many physicians to reach thefield of a common consciousness with their patientsrequires both an alternate and a holistic perspective.
Interdependent FactorsAll four of the healing factors are interdependent, with
one or more of greater importance depending on thephysical condition or illness, or personal relationship.The shaman or physician has great power to heal, oreven to make things worse. Tafoya says, “If you try tohave someone sing a song that doesn’t belong to themor that doesn’t fit them then we may do them a disser-vice, and they may not respond.”4 Finding the rightsong has benefits for both. Joan Halifax, psychologistauthor of “Shamanism Voices: A Survey of VisionaryNarratives,” notes that, “The power of song to heal thesinger as well as the listener is a persistent and remark-able feature of shamanistic songs.”13
Chanting produces a field effect and can facilitatedevelopment of a calming state of mind by triggeringalpha brain rhythm, and even a trance state. Some formof chanting is ubiquitous among Shamanic healing cer-emonies14 to support the four healing factors by addingto the field effect and enhancing interconnectedness.
SummaryPhysicians can improve the doctor-patient encoun-
ter by attending to personal qualities that enhancerelationship and trust, and by recognizing their valueas a healer in patients’ eyes. If physicians can clearlyunderstand their patients’ expectations, and align withthose, they can then import the power of the beliefresponse to magnify the effect of their shared treat-ment plan. Within this dialogue, behaviors with caringintention may influence patients’ healing responsemore than had ever been thought possible. By what-ever method, creating a sense of place for thisinteraction adds another potent component; and fi-nally, the field of common understanding of beliefsystems can create further positive benefit for pa-tients in this patient-physician encounter.
A Moment in Time and PlaceFrom the modern perspective of the corporate
business of medicine the bottom line dictates howthe doctor-patient relationship plays out. This dis-turbs many physicians. Edward Hallowell ,psychiatrist and author of “Connect,” comments onthis: “The public still wants to have a doctor. Itdoesn’t want to have a brand. It wants to have some-thing more than a corporate image. It wants to turnto a person in the human moment.”3 Achieving thishuman moment can be enhanced through a highlypersonal interaction between two people. If thatpersonal interaction can be further enhanced as anancient healing interaction, then we can hopefully“…arrive where we started, and know the place forthe first time.”15 ❖
References1. Cumes D. The Spirit of Healing, Llewellyn Publications,Minnesota, 1999.2. Krippner S. Medicine and the Inner Realities. AlternativeTherapies, 3:6, 1997.3. Hallowell E. The Value of the Human Moment in Medicine.Group Practice Journal, October, 1999.4. Tafoya T. Mental Health in the New Millennium. MulticulturalHealth Conference, Portland, Oregon, April, 2000.5. Barbour A, Caring For Patients. Stanford University Press, 1995.6. Dossey L, Whatever Happened to Healers? AlternativeTherapies, 1:5, 1995.7. Cheney, The New Yorker, January, 2000.8. Chin H, Asst. Regional Medical Director, Clinical InformationSystems, Northwest Permanente. Personal communication,March, 2000.9. Rolling Thunder, Interview, New Dimensions Radio, 1999.10. Dossey L. Healing Words. HarperSanFrancisco Publishers,1993.11. Silberfarb P. A Partisan for Psychiatry. Dartmouth Medicine,Winter, 1999.12. Braud WG, Schlitz M. A Method for the Objective Study ofTranspersonal Imagery. Journal of Scientific Exploration 3, no.1, 1989, 43-63.13. Halifax J. Shamanic Voices: A Survey of Visionary Narratives.Arkana:Penguin Group, New York, 1991.14. Moffit Cook P. Shaman, Jhankiri & Nele: Music Healers ofIndigenous Cultures. Ellipsis Arts, New York, 1997.15. Elliott TS. The Four Quartets.
Bibliography1. Alvord LA, “The Scalpel and the Silver Bear,” Bantam Books,1999.2. Hallowell E, “Connect.” Pantheon Books, 1999.3. Montour L, “The Medicine Wheel: Understanding ‘Problem’Patients in Primary Care,” The Permanente Journal, 4:1, 2000.4. Remen R, “Kitchen Table Wisdom,” Riverhead Books, NewYork, 1996.
8 The Permanente Journal / Spring 2000 / Volume 4 No. 2
sou
l o
f th
e h
eale
r
“Cats’ Hill Criterium”by J. Richard Gaskill, MD

9The Permanente Journal / Spring 2000 / Volume 4 No. 2
perm
an
en
te a
bstra
cts
Evaluating Hypertension Control in aManaged Care SettingAlexander M, Tekawa I, Hunkeler E, Fireman B, Rowell R,et al. Arch Intern Med 1999 Dec 13-27;159(22):2673-7.
BACKGROUND: We conducted a retrospective cohortstudy on a random sample of adult patients withhypertension in a large health maintenance organi-zation to assess the feasibility of documenting bloodpressure (BP) control and to compare different mea-sures for defining BP control.
METHODS: Three criteria for BP control were assessed:systolic BP less than 140 mm Hg; diastolic BP less than90 mm Hg; and combined BP control, with systolic BPless than 140 mm Hg and diastolic BP less than 90 mmHg. Four methods of assessing hypertension control bythe above criteria were examined: proportion of pa-tients with BP under control at 75% and 50% or more oftheir office visits; the mean of all pressures during thestudy period; and the BP from the last visit during thestudy period.
RESULTS: The proportion of patients meeting each cri-terion for control was similar whether we used the meanBP for all visits, the last recorded BP, or control at 50%or more of visits. Control rates were substantially lowerwhen the more stringent assessment, 75% of visits, wasused. The proportion of patients with combined BPcontrol at 75% or more of their visits was half that of theother methods.
CONCLUSIONS: In this health maintenance organizationpopulation, results with the use of the simplest approach,the last BP measurement recorded, were similar to re-sults with the mean BP. Our findings indicate thatevaluation of BP control in a large health maintenanceorganization will find substantial room for improvement,and clinicians should be encouraged to be more ag-gressive in their management of hypertension, especiallywith regard to the systolic BP, which until recent yearshas been underemphasized.
Copyright 1999, American Medical Association.
Diabetes Management in a Health MaintenanceOrganization. Efficacy of Care ManagementUsing Cluster VisitsSadur CN, Moline N, Costa M, Michalik D, Mendlowitz D,et al. Diabetes Care 1999 Dec 22(12):2011-7.
OBJECTIVE: To evaluate the effectiveness of a clustervisit model led by a diabetes nurse educator for de-livering outpatient care management to adult patientswith poorly controlled diabetes.
RESEARCH DESIGN AND METHODS: This study involved arandomized controlled trial among patients of KaiserPermanente’s Pleasanton, CA, center who were aged16-75 years and had either poor glycemic control(HbA
1c > 8.5%) or no HbA
1c test performed during
the previous year. Intervention subjects receivedmultidisciplinary outpatient diabetes care manage-ment delivered by a diabetes nurse educator, apsychologist, a nutritionist, and a pharmacist in clus-ter visit settings of 10-18 patients/month for sixmonths. Outcomes included change (from baseline)in HbA
1c levels; self-reported changes in self-care
practices, self-efficacy, and satisfaction; and utiliza-tion of inpatient and outpatient health care.
RESULTS: After the intervention, HbA1c levels declined
by 1.3% in the intervention subjects versus 0.2% inthe control subjects (p < 0.0001). Several self-carepractices and several measures of self-efficacy im-proved significantly in the intervention group.Satisfaction with the program was high. Both hospi-tal (p = 0.04) and outpatient (p < 0.01) utilizationwere significantly lower for intervention subjects af-ter the program.
CONCLUSIONS: A six-month cluster visit group modelof care for adults with diabetes improved glycemiccontrol, self-efficacy, and patient satisfaction and re-sulted in a reduction in health care utilization afterthe program.
Copyright 1999 by the American Diabetes Association.
Lack of Correlation of Symptoms with Special-ist-Assessed Long-Term Asthma SeverityOsborne ML, Vollmer WM, Pedula KL, Wilkins J, Buist AS,O’Hollaren M, Chest 1999 Jan;115(1):85-91.
STUDY OBJECTIVES: To validate three indicators of asthmaseverity as defined in the National Asthma EducationProgram (NAEP) guidelines (ie, frequency of symptoms,degree of airflow obstruction, and frequency of use oforal glucocorticoids), alone and in combination, againstseverity as assessed by pulmonary specialists providedwith 24-month medical chart data.
DESIGN: Cross-sectional comparison of questionnaireand clinical-based markers of asthma severity withphysician-assessed severity based on chart review.The pulmonologists did not have access to the re-sults of the baseline evaluations when making theirseverity assessments.
SETTING AND PARTICIPANTS: Study participants were 193asthmatic members (age range, 6 to 55 years) of a
Permanente Abstracts

10 The Permanente Journal / Spring 2000 / Volume 4 No. 2
perm
an
en
te a
bst
ract
s
large health maintenance organization who under-went a baseline evaluation as part of a separatelongitudinal study. This evaluation consisted ofspirometry, skin prick testing, and a survey that in-cluded questions on symptoms and medication use.The participants in the ancillary study were selected,based on their baseline evaluation, to reflect a broadrange of asthma severity.
RESULTS: Based on the chart review, 86 of the studysubjects (45%) had mild disease, 90 (45%) had mod-erate disease, and 17 (9%) had severe disease. Thisphysician-assessed severity correlated highly (p ≤0.013) with NAEP-based indices of severity based onoral glucocorticoid use (never, infrequently for at-tacks, frequently for attacks, and daily use) and onspirometry (FEV1 > 80% predicted, 60 to 80% pre-dicted, and <60% predicted). It did not, however,correlate with current asthma symptoms (≤ once/week, 2 to 6 times/week, daily) (p = 0.87). A com-posite severity score based on spirometry and theglucocorticoid use data still provided an overall agree-ment of 63%, with a weighted kappa of 0.40.
CONCLUSIONS: While current symptoms are the mostimportant concern of patients with asthma, they re-flect the current level of asthma control more thanunderlying disease severity. Investigators must there-fore use caution when comparing groups of patientsfor whom severity categorization is based largely onsymptomatology. This observation, that symptomsalone do not reflect disease severity, becomes evenmore important as health-care delivery moves closerto protocols/practice guidelines and “best treatment”programs that rely heavily on symptoms to guidesubsequent treatment decisions.
Effect of a Pediatric Self-Care Book onUtilization of Services in a Group Model HMOFrance EK, Selna MJ, Lyons EE, Beck AL, Calonge BN,Clin Pediatr (Phila) 1999 Dec;38(12):709-15.
The purpose of this study was to determine theeffect of a pediatric self-care book (SCB) with nursetelephone support on use of health services. The studywas performed in a pediatric department of KaiserPermanente in a suburb of Denver, Colorado. Wellpatients seen at age 2 weeks to 2.5 months (infantgroup) or 14 to 19 months (toddler group) were en-rolled. Intervention families received a copy of thebook, Your Child’s Health, and were oriented on itsuse. Rates of sick visits, advice nurse calls, pharmacyprescriptions, emergency department visits, and hos-
pital admissions were assessed. Visit and call rateswere calculated, and mean rates of the SCB groupand the control group were then compared. Of 1104enrol[lee]s, 527 received the SCB; the other 577 servedas controls. The SCB group had 14.0% fewer totalvisits (excluding well-baby visits) than controls did(p = 0.018). For infants and toddlers who were notfirst-borns, the intervention was associated with astatistically significant decrease in sick visits (23%),advice nurse phone calls (24%), and pharmacy pre-scriptions (26%); no statistically significant differencesin study outcomes were seen among first-born studysubjects. Promotion of self-care in a group modelhealth maintenance organization can decrease useof services by families of young children.
Exploring Indicators of TelephoneNursing QualityHoare K, Lacoste J, Haro K, Conyers C, J Nurs Care Qual1999 Oct;14(1):38-46.
To explore whether documentation, use of clini-cal guidelines, and nurse competency are the bestindicators of quality telephone nursing, this studyexamined the relationship between these com-monly cited indicators and the characteristics of atelephone nursing call. This study, done at a largehealth maintenance organization (HMO), found: ac-companying symptoms played a major role intelephone nursing assessment; call length was re-lated to documentation process and to number ofvisits to a health care facility after a call; nurses’interpersonal skills and ability to determine urgencyof a call are related to the documentation processbut not to outcomes of the call; time of a call isrelated to disposition; and disposition is related tonumber of visits after a call.Reprinted with permission from Hoare K; Lacoste J; Haro K; Conyers C;
J Nurs Care Qual 1999 Oct;14(1):38-46, ©1999 Aspen Publishers, Inc.
HMO Physicians’ Use of ReferralsBachman KH, Freeborn DK, Soc Sci Med 1999Feb;48(4):547-57.
Clinical uncertainty is a source of variation in medi-cal decision-making as well as a source ofwork-related stress. Increasing enrollment in orga-nized health care systems has intensified interest inunderstanding referral utilization as well as issuessuch as physician dissatisfaction and burnout. Weexamined whether primary care physicians’ affective

11The Permanente Journal / Spring 2000 / Volume 4 No. 2
perm
an
en
te a
bstra
cts
reactions to uncertainty and their job characteristicswere associated with use of referrals and burnout.Data came from mail surveys of primary care physi-cians practicing in two large group model healthmaintenance organizations (HMOs) in the USA. Con-sistent with past research, we found that youngerphysicians had higher referral rates than older physi-cians, and that general internists had higher rates thaneither family practitioners or pediatricians. Greaterstress from uncertainty increased referrals and refer-rals were negatively correlated with heavier workdemands (patient visits per hour). Greater stress fromuncertainty, perceived workload (too high) and asense of loss of control over the practice environ-ment were associated with higher levels of burnout.Reprinted from Soc Sci Med: Bachman KH, Freeborn DK, HMO
physicians’ use of referrals, 48(4):p 547-57, 1999, with permis-
sion from Elsevier Science.
Cost of Care for Patients inCancer Clinical TrialsFireman BH, Fehrenbacher L, Gruskin EP, Ray GT, J NatlCancer Inst 2000;92(2):136-42.
BACKGROUND: Information on the costs of medicalcare for patients enrolled in clinical trials is neededby policymakers evaluating ways to facilitate clinicalresearch in a managed care environment. We exam-ined the direct costs of medical care for patientsenrolled in cancer clinical trials at a large health main-tenance organization (HMO).
METHODS: Costs for 135 patients who entered 22cancer clinical trials (including 12 breast cancer tri-als) at Kaiser Permanente in Northern California, from1994 through 1996, were compared with costs for135 matched control subjects who were not enrolledin such trials. Cancer registry data and medical chartswere used in matching the control subjects to thetrial enrollees with respect to cancer site, stage, dateof diagnosis, age, sex, and trial eligibility. The directcosts of medical care were compared between trialenrollees and the control subjects for a one-year pe-riod, with data on costs and utilization of servicesobtained from Kaiser Permanente databases andmedical charts.
RESULTS: Mean one-year costs for the enrollees intrials were 10% higher than those for the control sub-jects ($17,003 per enrollee compared with $15,516per control subject; two-sided p = .011). The primarycomponent of this difference was a $1376 differencein chemotherapy costs ($4815 per trial enrollee ver-
sus $3439 per control subject; two-sided p < .001).Costs for the 11 enrollees in trials that had a bonemarrow transplant (BMT) arm were approximatelydouble the costs for their matched control subjects(borderline significance: two-sided p = .054). The$15,041 mean cost for the enrollees in trials withoutBMT was similar to the $15,186 mean cost for theirmatched control subjects.
CONCLUSIONS: Participation in cancer clinical trials ata large HMO did not result in substantial increases inthe direct costs of medical care.Reprinted with permission from Oxford University Press.
Spousal Concordance for Cancer Incidence:a Cohort StudyFriedman GD, Quesenberry CP Jr, Cancer 1999 Dec1;86(11):2413-9.
BACKGROUND: Because married couples share at leasttheir home environment, spousal aggregation of can-cer might provide clues to unsuspected etiologicfactors. The authors sought to measure the concor-dance of cancer occurrence in married couples andexplore factors that might explain greater-than-ex-pected concordance.
METHODS: The authors identified 25,670 cancer-freemarried couples in Northern California who werefollowed for up to 31 years for the development ofcancer. In Cox proportional hazards analysis, thedevelopment of cancer in a spouse was treated as atime-dependent, independent variable, and spouse-with/spouse-without risk ratios were determined,controlling for age and gender. For selected concor-dant espoused pairs, additional explanatoryinformation was sought in their medical records.
RESULTS: There was no excess concordance for allcancers combined; the spouse-with/spouse-withoutrisk ratio was 0.97 (95% confidence interval, 0.90-1.05). Statistically significant husband-wifeassociations were found only for cancer of the tongueand stomach and for non-Hodgkin lymphoma. Ex-cept for cancer of the penis/endometrium and testis/vulva, based on one couple with each combination,gender specific cancers did not aggregate withinmarried couples. Established and suspected risk fac-tors, not necessarily related to the marriage, werefound for some individuals who had concordancewith their spouses.
CONCLUSIONS: Little spousal concordance for canceroccurrence was found. The study of spousal aggrega-tion does not appear useful in identifying unsuspected

12 The Permanente Journal / Spring 2000 / Volume 4 No. 2
perm
an
en
te a
bst
ract
s
environmental causes of cancer in heterogeneous popu-lations in urban areas of affluent Western countries. Acohort study would have to be much larger than thisone to detect weak spousal concordance reliably.Copyright 1999, American Cancer Society. Reprinted by permis-
sion of Wiley-Liss, Inc, a subsidiary of John Wiley & Sons, Inc.
Changing Paternity and the Risk of Preeclampsia/Eclampsia in the Subsequent PregnancyLi DK, Wi S, Am J Epidemiol 2000 Jan 1;151(1):57-62.
To determine whether changing paternity affects therisk of preeclampsia or eclampsia in the subsequentpregnancy and whether the effect depends on awoman’s history of preeclampsia/eclampsia with herprevious partner, a cohort study was conducted basedon 140,147 women with two consecutive births during1989-1991, identified through linking of annual Califor-nia birth certificate data. Among women withoutpreeclampsia/eclampsia in the first birth, changing part-ners resulted in a 30% increase in the risk ofpreeclampsia/eclampsia in the subsequent pregnancycompared with those who did not change partners (95%confidence interval: 1.1, 1.6). On the other hand, amongwomen with preeclampsia/eclampsia in the first birth,changing partners resulted in a 30% reduction in therisk of preeclampsia/eclampsia in the subsequent preg-nancy (95% confidence interval: 0.4, 1.2). The differenceof the effect of changing paternity on the risk of preec-lampsia/eclampsia between women with and thosewithout a history of this condition was significant (p <0.05 for the interaction term). The above estimates wereadjusted for potential confounders. These findings sug-gest that the effect of changing paternity depends onthe history of preeclampsia/eclampsia with the previ-ous partner and support the hypothesis that parentalhuman leukocyte antigen sharing may play a role inthe etiology of preeclampsia/eclampsia.Reprinted by permission of Oxford University Press.
Second-Trimester Serum Chorionic Gonadot-ropin Concentrations and Complications andOutcome of PregnancyWalton DL, Norem CT, Schoen EJ, Ray GT, Colby CJ, NEngl J Med 1999 Dec 30;341(27):2033-8.
BACKGROUND: Maternal serum chorionic gonadotro-pin is measured to screen for fetal chromosomalabnormalities. Whether the results can also be usedto predict the risk of complications or an adverseoutcome of pregnancy is not known.
METHODS: We reviewed the medical records of 28,743girls and women in whom chorionic gonadotropinwas measured during the second trimester of preg-nancy (between July 1, 1995, and January 31, 1997),seeking information about the complications and out-come of their pregnancies. We excluded girls andwomen who had preexisting risk factors for compli-cations or an adverse outcome of pregnancy.
RESULTS: Higher serum chorionic gonadotropin con-centrations were associated with higher rates of stillbirth(odds ratio for every increase in chorionic gonadotro-pin of one multiple of the median, 1.4; 95 percentconfidence interval, 1.1 to 1.9). There was no relationbetween higher serum chorionic gonadotropin con-centrations and the risk of gestational diabetes,premature rupture of membranes or intrauterine growthretardation or small size for gestational age (odds ra-tio, 1.1; 95 percent confidence interval, 0.9 to 1.2).Higher serum chorionic gonadotropin concentrationswere associated with a risk of placental abnormalities(odds ratio, 1.5; 95 percent confidence interval, 1.3 to1.7), pregnancy-induced hypertension (odds ratio, 1.4;95 percent confidence interval, 1.3 to 1.5), and pretermdelivery without pregnancy-induced hypertension(odds ratio, 1.1; 95 percent confidence interval, 1.0 to1.2). Inclusion in certain racial or ethnic categories(black, Filipino or Pacific Islander, unknown race orethnic group, and “other,” which included those ofMiddle Eastern descent and Native Americans) was abetter predictor of the risk of an adverse outcomethan serum chorionic gonadotropin values.
CONCLUSIONS: Measurements of serum chorionic go-nadotropin are of little clinical value for predicting therisk of complications and the outcome of pregnancy.Copyright 1999, Massachusetts Medical Society. All rights reserved.
Effect of Age on Reasons for Initiationand Discontinuation of HormoneReplacement TherapyEttinger B, Pressman A, Silver P, Menopause 1999Winter;6(4):282-9.
OBJECTIVE: The purpose of this study was to exam-ine age-related differences in reasons thatpostmenopausal women began and stopped hormonereplacement therapy (HRT).
DESIGN: Two identical telephone surveys were con-ducted of women members of Kaiser FoundationHealth Plan who had begun HRT within the previ-ous three years. The first, in 1997, was of 604 olderwomen aged 65 years or older; the second, in 1998,

13The Permanente Journal / Spring 2000 / Volume 4 No. 2
perm
an
en
te a
bstra
cts
was of 866 younger women aged 50-55 years. Pre-scription records for both groups provided the meansfor determining continuation of therapy.
RESULTS: Among older women, 35% reported preven-tion or treatment of osteoporosis as the primary reasonfor starting HRT. Younger women were less likely (14%)to report this (p < 0.001). Relief of vasomotor meno-pausal symptoms was the most frequently reportedreason that younger women gave for starting HRT; itwas the primary reason in 34%. In contrast, only 7% ofolder women reported relief of vasomotor symptomsas the primary reason for starting HRT (p < 0.001). Olderwomen were more likely than younger women to dis-continue HRT; after 12 months, the probabilities ofdiscontinuation were 62% and 48% (relative risk = 1.4;95% confidence interval = 1.2-1.6). Treatment-relatedside effects were most often the reason given for stop-ping HRT; 87% of older women and 64% of youngerwomen who stopped reported that a treatment sideeffect was their primary reason (p < 0.001). Amongtreatment side effects, vaginal bleeding was the mostfrequently reported reason for stopping HRT; it wasthe primary reason for stopping in 52% of older womenand 29% of younger women (p < 0.001).
CONCLUSIONS: Older women differ from youngerwomen in their reasons for starting and stopping HRT.Whereas osteoporosis is the predominant reason thatolder women begin HRT, relief of vasomotor symp-toms is the major reason that younger women begin.Early discontinuation of HRT is common and is greateramong older women. Intolerance of treatment, par-ticularly vaginal bleeding, is the predominant reasonfor stopping HRT.
Psychosocial Treatments forAdolescent DepressionLewinsohn PM, Clarke GN, Clin Psychol Rev 1999Apr;19(3):329-42.
Major Depressive Disorders affect between 2% and5% of adolescents at any one point in time. Depres-sion in adolescence is associated with seriouspsychosocial deficits and has negative effects on func-tioning during young adulthood. Starting with thepioneering work of Lenore Butler and her colleagues,many psychosocial interventions have been developedand studied, with generally positive results. On thebasis of a meta-analysis of the existing cognitive-be-havioral therapy (CBT) studies, we estimate an overalleffect size of 1.27 and that 63% of patients show clini-cally significant improvement at the end of treatment.
It seems reasonable to conclude that CBT has beendemonstrated to be an effective treatment for depressedadolescents. In this article we describe these interven-tions, most of which are meant to address the problemsshown by depressed adolescents. The purpose of ourarticle is to bring this literature to the attention of clini-cians in a manner which quickly and clearlysummarizes the key features of the interventions tomake it easy for clinicians to take advantage of thiswealth of information and to avail themselves of theexisting resources. We conclude by suggesting futuredirections and several additional areas of applicationfor adolescent depression treatments.Reprinted from Clinical Psychology Review, Vol 19(3), Lewinsohn
PM, Clarke GN: Psychosocial treatments for adolescent depression.
Clin Psychol Rev 19(3): 329-42. Copyright 1999, with permission
from Elsevier Science.
Cigarette Smoking, Alcohol Consumption, andRisk of ARDS: a 15-Year Cohort Study in aManaged Care SettingIribarren C, Jacobs DR Jr, Sidney S, Gross MD, Eisner MD,Chest 2000 Jan;117(1):163-8.
STUDY OBJECTIVE: To examine the association ofcigarette smoking and alcohol consumption withhospital presentation of ARDS in a well-defined,multiethnic population.
DESIGN: Retrospective cohort study.SETTING: Health maintenance organization in North-
ern California.PARTICIPANTS: A total of 121,012 health plan sub-
scribers (54.2% women), aged 25 to 89 years.OUTCOME MEASURE: Hospital presentation of ARDS (vali-
dated by medical chart review) from baseline in 1979to 1985 through the end of 1993 (median, 9.9 years).
RESULTS: There were 56 cases of ARDS (33 in men,23 in women). The case fatality rate was 39% in bothgenders. ARDS was independently related to increas-ing age (rate ratio of ten years, 1.38; 95% confidenceinterval [CI], 1.12 to 1.71), to current smoking of < 20cigarettes/d (rate ratio vs never cigarette smokers, 2.85;95% CI, 1. 23 to 6.60), and to current cigarette smok-ing of ≥ 20 cigarettes/d (rate ratio vs never smokers,4.59; 95% CI, 2.13 to 9.88). No association was ob-served between alcohol consumption and ARDS.
CONCLUSIONS: The results of this study suggest a re-lationship (with evidence of dose-response effect)between cigarette smoking and ARDS. Assuming acausal relationship, approximately 50% of ARDS caseswere attributable to cigarette smoking.

14 The Permanente Journal / Spring 2000 / Volume 4 No. 2
perm
an
en
te a
bst
ract
s
Warfarin Use among Ambulatory Patients withNonvalvular Atrial Fibrillation: the Anticoagu-lation and Risk Factors in Atrial Fibrillation(ATRIA) StudyGo AS, Hylek EM, Borowsky LH, Phillips KA, Selby JV, Singer DE:
Ann Intern Med 1999 Dec 21;131(12):927-34
BACKGROUND: Warfarin dramatically reduces the riskfor ischemic stroke in nonvalvular atrial fibrillation,but its use among ambulatory patients with atrial fi-brillation has not been widely studied.
OBJECTIVE: To assess the rates and predictors ofwarfarin use in ambulatory patients with nonvalvularatrial fibrillation.
DESIGN: Cross-sectional study.SETTING: Large health maintenance organization.PATIENTS: 13,428 patients with a confirmed ambula-
tory diagnosis of nonvalvular atrial fibrillation andknown warfarin status between 1 July 1996 and 31December 1997.
MEASUREMENTS: Data from automated pharmacy,laboratory, and clinical-administrative databases wereused to determine the prevalence and determinantsof warfarin use in the three months before or afterthe identified diagnosis of atrial fibrillation.
RESULTS: Of 11,082 patients with nonvalvular atrialfibrillation and no known contraindications, 55% re-ceived warfarin. Warfarin use was substantially lowerin patients who were younger than 55 years of age
(44.3%) and those who were 85 years of age orolder (35.4%). Only 59.3% of patients with one ormore risk factors for stroke and no contraindicationswere receiving warfarin. Among a subset of “ideal”candidates to receive warfarin (persons 65 to 74years of age who had no contraindications and hadprevious stroke, hypertension, or both), 62.1% hadevidence of warfarin use. Among our entire co-hort, the strongest predictors of receiving warfarinwere previous stroke (adjusted odds ratio, 2.55 [95%CI, 2.23 to 2.92]), heart failure (odds ratio, 1.63[CI, 1.51 to 1.77]), previous intracranial hemorrhage(odds ratio, 0.33 [CI, 0.21 to 0.52]), age 85 years orolder (odds ratio, 0.35 [CI, 0.31 to 0.40]), and pre-vious gastrointestinal hemorrhage (odds ratio, 0.47[CI, 0.40 to 0.57]).
CONCLUSIONS: In a large, contemporary cohort ofambulatory patients with atrial fibrillation who re-ceived care within a health maintenance organization,warfarin use was considerably higher than in otherreported studies. Although the reasons why physi-cians did not prescribe warfarin could not beelucidated, many apparently eligible patients withatrial fibrillation and at least one additional risk fac-tor for stroke, especially hypertension, did not receiveanticoagulation. Interventions are needed to increasethe use of warfarin for stroke prevention among ap-propriate candidates. ❖

15The Permanente Journal / Spring 2000 / Volume 4 No. 2
Introduction and HistoryOur commitment to improving the health
of our members is a driving force in theKaiser Permanente (KP) dedication to qual-ity improvement. With our integratedhealth system and defined population ofmembers, we are in a unique position tocontinually explore opportunities to refinethe care we provide. By focusing on newor improved ways to deploy the right careat the right time, we enhance the healthof our members, build upon our existingreputation as a provider of quality healthcare, and improve service and cost-effec-tiveness of care for our members andgroup customers.
During his 17 years as President, CEO,and Chairman of the Boards of KaiserFoundation Health Plan, Inc, and KaiserFoundation Hospitals, James A. Vohs con-tinually emphasized the moral and strategicimportance of quality and quality improve-ment. On the event of his retirement asChairman of the Board, the James A. VohsAward for Quality was established by theBoards to recognize and honor projectsthat advance the quality of care, show-case innovat ive techniques andknowledge that can be transferredthroughout the Program, and underscorethe value of multidisciplinary teamwork.
The Vohs Award recognizes exceptionalKP efforts to address quality-of-care issuesand acknowledges multidisciplinary teamefforts representing Kaiser FoundationHealth Plan, Inc, Kaiser Foundation Hospi-tals, and the Medical Groups. As before,the criteria for selecting a winner assure thatthe project measurably improves patientcare and has the potential for transfer as a“successful practice,” thereby benefitingmany members across the Program. TheVohs Award is designed to encourageprojects that demonstrate leadership withinKP and the health care industry, and thatdevelop and apply new approaches to im-prove quality of care.
Annually, each KP Division is invited tonominate one or two projects for consider-ation for the James A. Vohs Award forQuality. The award is presented for theproject that best represents a well-estab-lished effort to significantly improve qualitythrough substantial, objectively docu-mented, and institutionalized changes indirect patient care, through either new pro-grams or significant improvements inexisting ones.
We present here the 2000 winners of theVohs award: the first-place winner, “BrightSystems®: A Total Quality ManagementProject to Improve Children’s Health,” fromKPNC of the California Division; the onethat received honorable mention, “TheChildhood/Adolescent Immunization Pro-gram with accompanying ImmunizationToolkit,” from the Denver/Boulder LocalMarket of the KP Colorado Region; and sev-eral other outstanding Quality ProgramDescriptions which were submitted, includ-ing “Achieving Positive Outcomes throughCollaborative Pharmaceutical Care—theKPNW Medication Management Program,”“Improvement of Cardiac Outcomes fromthe KP Ohio Region,” “Asthma Disease Man-agement” from the Denver/Boulder LocalMarket of the KP Colorado Region, and “TheBreast Health and Cancer Detection Pro-gram” from the KP Georgia Region.
In addition to presenting the basic ele-ments of each program, we hope to remindthe reader of the Vohs Award applicationprocess to stimulate similar project devel-opment on diverse topics throughout ourorganization. Multidisciplinary involvementand strong team leadership is critical to thesuccess of these projects. Just as the qualityplanning process and methods for makingprograms operational served as the frame-work for several other successful programrollouts within the Local Markets, all pro-grams described should serve as a modelfor quality improvement programs through-out Kaiser Permanente nationally.
The James A. Vohs Award for QualityThe second annual Permanente Journal special issue
Incentive is provided to all TPMG/KP pro-fessional staff to apply for the James A. VohsQuality Improvement Award. There is nomonetary gift with this award. The winningDivision receives an engraved award, andproject team members receive awards. The“real” award is recognition for good work.Winners and runners-up are invited topresent their projects at a reception hostedby the Boards of Directors, Division Presi-dents, and other Program Officers. Theawardees also receive publicity through theQuality Notes newsletter and through local,state, and national press releases.
The local level process for nominationvaries. Each Division has contact liaisons,who can be located through their qualityrepresentative. Each Division also has ascreening and review process for potentialnominees. Nominations are signed off bythe Division President and Medical Direc-tor. Nominations and applications are dueSeptember 1st each year.
A Vohs Award Selection Committee con-sists of two to three Boards of Directorsmembers, a Vohs family member, Chair-man Bob Crane, two to three ProgramOffice quality representatives, one Perman-ente Federation representative, and twonon-voting Program Office quality repre-sentatives, who serve as staff to theCommittee. This Committee announces itsselection at the Board of Directors meet-ing in December. Notification is made tothe Division President and Medical Direc-tor by phone after that meeting. Teammembers are contacted by phone withinthe next day or two. The recognition cer-emony takes place at the March Board ofDirectors’ meeting.
We thus hope that the following entriesfor this year’s James A. Vohs Award willserve as models to motivate all KP staff topresent projects for consideration and mo-tivate us to continually improve the processof providing direct patient care and accessto health information for our members. ❖
clinica
l con
tribu
tion
s

16 The Permanente Journal / Spring 2000 / Volume 4 No. 2
sou
l o
f th
e h
eale
r
“Peacock at the Window”by J. Richard Gaskill, MD

17The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
Bright Systems®, the 2000 winner of theJames A. Vohs Award for Quality, is a set of com-puter- and paper-based tools that has changedthe way Kaiser Permanente (KP) pediatriciansconduct health supervision visits within KPNorthern California. The multicomponent systemincorporates Speed Charting forms for physi-cians, health education information fordistribution to parents and patients, and “patientencounter tools” explaining a variety of healthtopics, especially injury prevention and counsel-ing about exposure to environmental tobaccosmoke (ETS). Use of Bright Systems® has resultedin more accurate visit documentation, more per-sonalized patient care and greater satisfactionfor parents and health care professionals.
It’s a typical scene in the pediatrics department of anymedical center: mothers (and a few fathers) wait withtheir children to see the doctor for an ailment or ahealth supervision visit. Children sit, play, or run around.Parents page through copies of popular magazines,keeping an eye on the children’s activity. Nurses andfront office staff shuttle parents and children with theirforms and records into and out of examination rooms.
In the examination room, a medical assistant checksthe child’s weight and height. The pediatrician en-ters the room with a blank sheet of pink paper at-tached to a clipboard and jots down notes while run-ning through his own list of questions from memory.If he gets involved in talking about the importanceof car seat belts, the pediatrician may never get aroundto asking whether the child wears a bike helmet. Iftime permits and the pediatrician remembers, he’llreturn to a question that concerned the parent andprobe for more information. In the meantime, screen-ing tests and immunizations must be given. All toosoon, the parent and child are out the door, and thephysician’s attention turns to the next patient.
It doesn’t have to be that way. Picture a waitingroom where parents arrive knowing that the exami-nation will be tailored to their child’s needs. Whenthey register, parents receive and complete a shorthealth questionnaire that covers standard, age-appro-priate risk assessment issues. The medical assistantnotes the child’s weight and height on a health infor-mation sheet tailored to the child’s age and gives thesheet to the parent. During the visit, the pediatricianuses a printed form that prompts her to address age-
specific topics related to child development, safety,and parenting and to conduct an appropriate physicalexamination. The physician also reviews the completedhealth questionnaire and discusses any areas of riskthat are revealed. The parent, child, and physician allleave the visit reassured that their individual concernswere addressed along with all the fundamentals.
The secret to health supervision visits that resemblethat second scenario is Bright Systems®, the 2000 win-ner of the James A. Vohs Award for Quality. Thebasic system includes five tools: the Physician Prac-tice Survey, a spreadsheet of health supervision guide-lines; Speed Charting, a set of age-specific forms toassist physicians at the patient visit; Healthy Kids-Healthy Futures, age-specific information for parents;Health Questionnaires, an age-specific risk assess-ment tool; and Safety Questionnaires, a data collec-tion tool. (The Permanente Medical Group registeredthe name “Bright Systems®” as a trademark and re-tains ownership of related copyrights.)
Bright Systems® is the brainchild of Scott Gee, MD,the Project Director and Associate Director for Preven-tive Medicine, Regional Health Education, Kaiser Per-manente (KP) Northern California Region, as well as apediatrician at the KP Pleasanton Medical Offices. DrGee wanted to streamline the routine parts of healthsupervision visits and thereby create more opportunityfor meaningful interaction with parents and patients.
“I want to be able to talk with parents about thetopics that are most appropriate or are of greatestconcern for them and that will reap the greatestbenefits for them and their child. Standardizing whencertain information is provided and giving doctorsan easy way to document the discussion frees themup to engage in more meaningful, individual dia-logue with parents and children,” he explains.
The importance of adding efficiency and meaning tohealth supervision visits becomes clear when you con-sider that this type of visit represents half of all visits toKP Pediatrics Departments. These visits focus on pre-venting injuries and disease, guidance for parents, andadministering screening tests and immunizations. Thevalue of comprehensive pediatric care has been shownnot only to improve children’s health but also to re-duce the need for hospital admissions, operations, andillness-related visits. Comprehensive pediatric care alsocontributes to improved parent satisfaction, increasedmaternal compliance with health instructions, and im-proved diet and maternal self-confidence.1-7
DIANE FRASER is a health care and business writer based in the San Francisco Bay Area. She has written for the Garfield Memorial Fund, andmost recently wrote about the Depression Initiative for The Permanente Journal.
Review:Bright Systems® Sheds Light and Lightens the Loadat Pediatric Health Supervision Visits
By Diane Fraser
The parent, child,and physician all
leave the visitreassured that their
individualconcerns were
addressed alongwith all the
fundamentals.

18 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
Despite the demonstrated effectiveness of compre-hensive health supervision visits, studies show thatonly a small fraction of the visit time (8.4%) is de-voted to counseling and anticipatory guidance forparents.8 Studies show that injury prevention is dis-cussed only half the time and that few pediatriciansroutinely obtain family smoking histories. Further-more, pediatricians often don’t take advantage ofthese visits as opportunities to discuss behavioralconcerns with parents.9-12
Yet injuries are the leading cause of death in chil-dren and adolescents and account for 600,000 hospitaladmissions and 16 million emergency departmentvisits per year. The total cost associated with theseinjuries exceeds $7.5 million.13-15 The issue of expo-sure to environmental tobacco smoke (ETS) is equallycritical. ETS is estimated to contribute to 6200 child-hood deaths and $4.6 million in direct medicalexpenses annually.16-17
Bright Systems® was conceived to remedy manyof these deficiencies by incorporating health caredelivery tools for practitioners and front office staff;educational information for parents, patients, andhealth care professionals; and “patient encountertools” on a variety of health topics, especially injuryprevention and ETS counseling. Bright Systems®’objectives were to:
• Create an office system that deliversconsistent and comprehensive healthsupervision;
• Improve the quality and consistency ofanticipatory guidance given to parents athealth supervision visits;
• Improve parent safety behaviors;• Improve physician satisfaction by
reducing unnecessary work.According to David Sobel, MD, MPH, Director of
Patient Education and Health Promotion, RegionalHealth Education in KP Northern California, BrightSystems® isn’t only a win/win proposition–-it’s a win/win/win. “Parents win because they are happier withthe quality and thoroughness of their health supervi-sion visits and more confident thanks to the healtheducation handouts. Physicians win because they areable to move through the routine parts of the visitefficiently allowing them to focus on individual needsand questions. And the organization wins becauseBright Systems® is a cost-effective, proactive systemthat supports our focus on prevention and healthimprovement. Bright Systems® seamlessly integrateshealth education into ongoing clinical care.”
A Complete Set of ToolsBright Systems® used Total Quality Management
(TQM)18 methodologies to develop an office system(a series of routines and tools supported by all prac-tice personnel19), staff training, and continuousimprovement mechanisms to improve health super-vision visits. As noted earlier, the basic systemincludes a Physician Practice Survey, Speed Chartingforms, Healthy Kids-Healthy Futures sheets, andHealth/Safety Questionnaires.
Physician Practice Survey
Early in Bright Systems®’ development, the PhysicianPractice Survey helped determine and track health su-pervision visits at which physicians delivered specificcare (eg, immunizations) or information (eg, aboutbreastfeeding or use of child car seats). The survey wasan important tool for assembling an overview of howdifferent physicians, even within a single facility, tookindividual approaches to health supervision visits. Thisinformation was used to design the Bright Systems®
Speed Charting forms and health information sheets.Today, the survey incorporates the KP Northern
California Region’s clinical practice guidelines andserves as a convenient visual reminder for medicalassistants and front office staff to prepare for andconduct health supervision visits. A quick glance at aspreadsheet reminds staff which immunizations mustbe given at the four-year visit, for example. In thisway, the office staff knows what to be prepared forand what to prepare the parent for.
Dewey Woo, MD, a pediatrician with TPMG,examines a patient.
Yet injuries are theleading cause ofdeath in childrenand adolescentsand account for600,000 hospital
admissions and 16million emergencydepartment visits
per year.

19The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
Speed Charting FormsThese age-specific, structured encounter forms give
physicians a streamlined way to document the topicscovered at each health supervision visit. A separateform is used at each visit from birth to age 18 years.Forms are divided into sections that include interimand social histories, nutrition, development, physicalexamination, health assessment, and planning. Eachsection contains space for written comments, but anequally important feature of the forms is a series ofchecklists that allow physicians to annotate themedical chart quickly, accurately, and thoroughly.Symbols are used to indicate the parent’s responsesto specific questions.
For example, the Development section of the formgiven at the 18-month visit prompts the physician toask about and note the baby’s ability to:
• Kick/throw a ball• Use a spoon or fork• Climb stairs (with hand held)• Scribble• Speak ___ words.
Like all practitioners, pediatricians have an increas-ing paperwork burden. It is not uncommon for themto complete six or seven pieces of paper per childper visit—not just for internal use but also for pro-grams such as the US Department of Agriculture’sWomen, Infants, and Children (WIC) Program, schooladministrators, and US immigration authorities. “Thecheckoff boxes are a great timesaver, and since phy-sicians aren’t known for clear handwriting, they im-prove the accuracy of the documentation as well,”says Deborah L. Gould, MD, Chair, Chiefs of Pediat-rics, The Permanente Medical Group.
The sections and topics included in the forms anddiscussed at visits change as the patient ages. Forexample, a section about school appears on the formused for children at age six years, when questionsabout TV and video games also make their appear-ance on the forms. The social history section tracksparental marital status and the presence of smokersin the house. Prompts to ask about whether the childis in daycare or is a latchkey child and about thechild’s drug or tobacco use and sexual activity areadded to the form as the child develops.
Although the Bright Systems®’ Speed Charting formsare currently paper-based, they could readily be com-puterized. As KP Northern California moves closerto implementing an electronic medical record sys-tem, Bright Systems® is well positioned to adapt tothis change.
Healthy Kids-Healthy Futures SheetsParents receive age-specific Healthy Kids-Healthy
Futures information sheets when they arrive for eachhealth supervision visit. These sheets contain basicinformation about feeding or eating habits, safety,healthy habits, and parenting skills. A highlightedsection on the front of the sheet lets parents knowwhat may happen at the next visit and alerts them tothe possible need for immunizations or the advis-ability (and correct dosage) of giving acetaminophendrops to a young child.
Since her daughter Eliza was born, in July 1999, newmother Ann Banchoff has received Healthy Kids-HealthyFutures information sheets at every health supervisionvisit with her pediatrician at the KP San Francisco MedicalCenter. “It’s reassuring to know that we’re getting infor-mation that’s been reviewed and approved by quali-fied doctors in an organization I trust,” she says. “Thesheets are a handy complement to the Healthwise Hand-book and other books I’m using.”
Parents are encouraged to share the health infor-mation sheets with others who are involved in car-ing for the child. Dr Gould observes, “We’re seeing alot more fathers bringing their children in for healthsupervision visits these days, which is great. But al-most all of them come prepared with a list of ques-tions the mother wants answered. The Healthy Kids-Healthy Futures sheets usually take care of the stan-dard questions, and the physician has more time toaddress individual concerns. Plus, it’s a reliable wayto get important information back to the home, nomatter who brings the child in.”
On the back of each sheet, one or more topics areexplored in more detail. These topics range from“childproofing” checklists (for use with children agedsix to ten months) to temper tantrums and potty train-ing (for toddlers) to violence prevention, puberty,and sexuality (for older children and teens).
The health information sheets also are appropriatefor older pediatric patients to use in guiding theirown health care choices. “It’s important for Leah toget information about her own body from a reliablesource other than her parents. When someone otherthan her mother tells her that she needs to have plentyof calcium in her diet, it’s welcome reinforcement,”observes Joy Carlson, who brings her 11-year-olddaughter to a pediatrician at the KP Oakland Medi-cal Center. “Even though I’m not a big fan of pam-phlets, I found the Bright Systems® information veryhelpful as a reminder, or forecaster, of what will behappening in Leah’s life in the coming months.”
“It’s important forLeah to get
information abouther own body from
a reliable sourceother than her
parents.”

20 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
Health and Safety QuestionnairesWhen parents register at the front desk, the recep-
tionist or other front office staff member gives thema health risk assessment survey to complete whilewaiting for the doctor. The survey asks many of theroutine age-specific questions a pediatrician wouldnormally ask during a health supervision visit. Hav-ing these questions already answered by the parent(or by the teenaged patient) frees the physician toexplore current issues of concern for the parent andpatient in greater depth during the visit.
Irene Takahashi, MD, Chief of Pediatrics at the KPSouth San Francisco Medical Center notes that thequestionnaires are helpful for certifying students toparticipate in school athletic programs. The answersto questions such as “Have you ever had chest painor severe difficulty breathing?” and “Have you everfainted during exercise?” often help physicians probefor underlying physical conditions that may preventparticipation and to identify the need for furthermedical investigation.
Separate safety questionnaires are used before andafter Bright Systems® is implemented at a KP facil-ity. As a data collection tool, these questionnairesgive parents the opportunity to self-report their ef-forts to create safe environments for the health andwell being of their children. The questionnairesquery items such as appropriate use of child carseats; infant’s sleeping position; efforts to“childproof” the home; and the presence and ac-
cessibility of firearms in the home. Comparing thebefore-and-after data measures Bright Systems®’ ef-fect in reducing safety risks.
A Culturally Sensitive ApproachThe Healthy Kids-Healthy Futures information
sheets are designed for people with limited literacyskills and incorporate cultural sensitivity. To reach abroad range of families, all information sheets havebeen translated into Spanish and Chinese. As theHealthy Kids-Healthy Futures Program is disseminatedto other parts of the country, where other languagesand cultures may be prominent in the Health Planmember population, local needs can be accommo-dated as well. In all languages, the content of theinformation sheets reflects a wide range of culturalpreferences; for example, the sheets list a number ofethnic foods as examples of healthy eating habits.
As an example of the ongoing evolution of BrightSystems®, Dr Gould cites the current discussion overadding to the forms questions about alternativeforms of medicine that parents might use. “Almostevery parent gives some kind of health care athome-–even if it’s only acetaminophen,” Dr Gouldsays. “Increasingly, we realize that some home rem-edies may include herbal therapies that could con-flict with the medical advice that we give. Askingabout home remedies not only gives us more in-formation, it validates the parent’s own actions inan appropriate way.”
Table 1. Multidisciplinary participation in Bright Systems
Kaiser Foundation HealthPlan/Hospitals
The Permanente Medical Group State of California
Care Management Institute consulted onmaterials and evaluation tools
Pediatrics Departments (doctors, nurses,behavioral health specialists, medicalassistants, receptionists, and healtheducators) consulted on materials
California State Department of HealthServices consulted on anticipatoryguidance and health risk assessment toolsfor Medi-Cal
Perinatal Services Study Group consultedon Integrated Perinatal Educationprogram
Chiefs of Pediatrics approved andendorsed the system
Child Health Disability Program consultedon anticipatory guidance and health riskassessment tools
Compliance and Risk Managementverified compliance with legal standards
Adolescent Medicine specialists approvedand endorsed the system
Temperament Program consulted onparental anticipatory guidelines
Documentation Management Committeeconsulted on medical records andstandards
Committee of Health InformationManagers and Physicians consulted onNCQA standards
The survey asksmany of theroutine age-
specific questions apediatrician would
normally askduring a health
supervision visit.

21The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
The program is meeting with success outside the KPorganization also. In California, the Public Health De-partments in Monterey and San Francisco Counties haveadopted Bright Systems®. “What is happening with BrightSystems® is a perfect example of how we can fulfill ourmission to improve the health of not just our members,but of the communities we serve,” says Dr Sobel.
A Commitment to “Meaningful Detailing”The impetus for creating Bright Systems® came when
Dr Gee read the Bright Futures report issued by theMaternal and Child Health Bureau of the US Departmentof Health and Human Services.1 That report, Dr Geeremembers, “gave us a vision of children’s health and ofwhat it will take for us to have healthier children. But weneeded tactics and practical tools to get there.”
On his own initiative, Dr Gee started to develop BrightSystems® in 1991. The next year, matching funding fromRegional Health Education in KP Northern Californiahelped Dr Gee expand the team to include a half-timehealth educator: Jodi Jessen, DPH. Together, Drs Geeand Jessen visited pediatricians at each KP facility toshow them the Bright Systems® process and tools. “Ineach facility we had to prove that Bright Systems® helpedphysicians and staff to work more efficiently, save time,and produce better health outcomes,” recalls PamelaLarson, MPH, Director of Prevention and Self-Care,Regional Health Education in KP Northern California.“We focused on the concept of ‘meaningful detailing,’convincing each physician that the information collectedand distributed was meaningful to parents, to patients,to physicians, and to the organization.”
Before any KP facility could implement Bright Sys-tems®, pediatricians had to agree on a common ap-proach to health supervision visits. “Practicing Per-manente Medicine means much more than practic-ing as a group of individuals. One of the challengesof working on a program like Bright Systems® is thatit requires the physicians in a department to cometogether and agree on what the charting and patienteducation forms should contain. A helpful byproductis that physicians across the Program learned howbetter collaboration and consensus building can im-prove medical practice,” says Dr Sobel, identifying akey learning from the implementation.
The KP South San Francisco Medical Center is a goodexample of a facility where pediatricians struggled withthe idea of using a preprinted, KP regional form to docu-ment health supervision visits. The pediatricians wereconcerned also about the logistics of parents completingquestionnaires and receiving handouts. “We had some
initial resistance,” Dr Takahashi recalls. “It was only afterBright Systems® personnel explained that our views wouldbe heard and acknowledged and that we could custom-ize the forms to meet our needs, that we decided to joinin.” Among the changes that the KP South San Franciscopediatricians sought and achieved was inclusion of ascreening protocol for autism at the 18-month visit. (Stan-dard speed-charting forms have now been implementedacross the KP Northern California Region.)
The KP South San Francisco facility took a phasedapproach to implementing Bright Systems®, using it firstonly for children younger than ten years of age. “Wehad some reservations about the usefulness and valid-ity of the questionnaires and forms for teens,” says DrTakahashi. Among those concerns were privacy issuesand having teens and parents complete separate healthquestionnaires. After a few physicians started using theteen materials, their value soon became apparent.
“I obtain much more valuable information from myadolescent patients now that I’m using Bright Sys-tems®. Teenagers are clearly more willing to truth-fully answer sensitive questions on a questionnairethan [when they are] being asked face-to-face. OnceI have their written answers, I can focus my conver-sations on what matters most to each individual pa-tient,” says Dr Takahashi. “That makes the entire visitmuch more meaningful to the patient and to me.”
Getting the front office staff actively engaged in theprocess was equally important to the success of BrightSystems®. “We were extremely fortunate to have theenthusiastic support of staff members who readily sawthe positive effects Bright Systems® had in their offices.We couldn’t have done it without them,” says Ms. Larson.
Developing and implementing Bright Systems®
called for the talents of a multidisciplinary team se-lected from Kaiser Foundation Health Plan/Hospi-
Table 2. Kaiser Permanente (KP) Northern CaliforniaBright Systems® Team Members
KP Department Team Member, Title
Regional Health Education Scott Gee, MD, Project DirectorPamela Larson, MPH, Project ManagerLinda Rieder, MPH, Pediatric Program ManagerValerie Sheehan, MPH, Pediatric Program CoordinatorKimmie Lee, RD, MPH, Publications Coordinator
Care Management Institute Rachelle Mirkin, MPH, Interregional Consultant
Teenagers areclearly more
willing to truthfullyanswer sensitivequestions on a
questionnaire than[when they are]
being asked face-to-face.
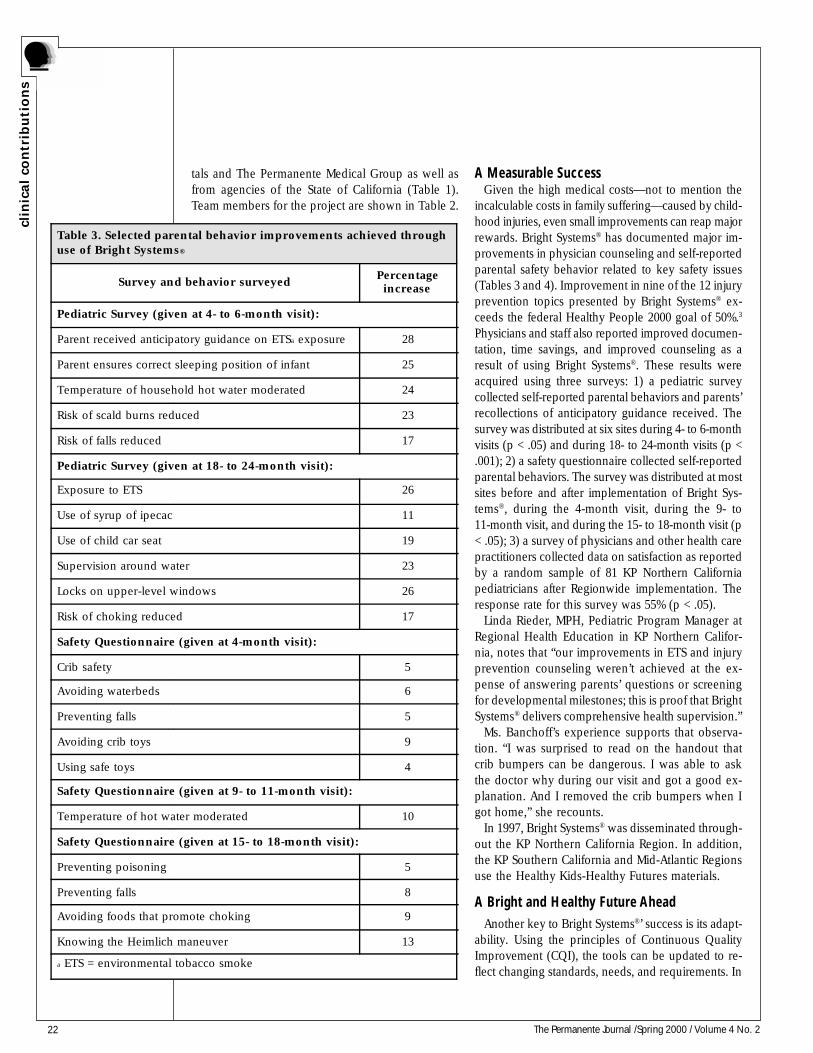
22 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
A Measurable SuccessGiven the high medical costs—not to mention the
incalculable costs in family suffering—caused by child-hood injuries, even small improvements can reap majorrewards. Bright Systems® has documented major im-provements in physician counseling and self-reportedparental safety behavior related to key safety issues(Tables 3 and 4). Improvement in nine of the 12 injuryprevention topics presented by Bright Systems® ex-ceeds the federal Healthy People 2000 goal of 50%.3
Physicians and staff also reported improved documen-tation, time savings, and improved counseling as aresult of using Bright Systems®. These results wereacquired using three surveys: 1) a pediatric surveycollected self-reported parental behaviors and parents’recollections of anticipatory guidance received. Thesurvey was distributed at six sites during 4- to 6-monthvisits (p < .05) and during 18- to 24-month visits (p <.001); 2) a safety questionnaire collected self-reportedparental behaviors. The survey was distributed at mostsites before and after implementation of Bright Sys-tems®, during the 4-month visit, during the 9- to11-month visit, and during the 15- to 18-month visit (p< .05); 3) a survey of physicians and other health carepractitioners collected data on satisfaction as reportedby a random sample of 81 KP Northern Californiapediatricians after Regionwide implementation. Theresponse rate for this survey was 55% (p < .05).
Linda Rieder, MPH, Pediatric Program Manager atRegional Health Education in KP Northern Califor-nia, notes that “our improvements in ETS and injuryprevention counseling weren’t achieved at the ex-pense of answering parents’ questions or screeningfor developmental milestones; this is proof that BrightSystems® delivers comprehensive health supervision.”
Ms. Banchoff’s experience supports that observa-tion. “I was surprised to read on the handout thatcrib bumpers can be dangerous. I was able to askthe doctor why during our visit and got a good ex-planation. And I removed the crib bumpers when Igot home,” she recounts.
In 1997, Bright Systems® was disseminated through-out the KP Northern California Region. In addition,the KP Southern California and Mid-Atlantic Regionsuse the Healthy Kids-Healthy Futures materials.
A Bright and Healthy Future AheadAnother key to Bright Systems®’ success is its adapt-
ability. Using the principles of Continuous QualityImprovement (CQI), the tools can be updated to re-flect changing standards, needs, and requirements. In
Table 3. Selected parental behavior improvements achieved throughuse of Bright Systems®
Survey and behavior surveyedPercentageincrease
Pediatric Survey (given at 4- to 6-month visit):
Parent received anticipatory guidance on ETSa exposure 28
Parent ensures correct sleeping position of infant 25
Temperature of household hot water moderated 24
Risk of scald burns reduced 23
Risk of falls reduced 17
Pediatric Survey (given at 18- to 24-month visit):
Exposure to ETS 26
Use of syrup of ipecac 11
Use of child car seat 19
Supervision around water 23
Locks on upper-level windows 26
Risk of choking reduced 17
Safety Questionnaire (given at 4-month visit):
Crib safety 5
Avoiding waterbeds 6
Preventing falls 5
Avoiding crib toys 9
Using safe toys 4
Safety Questionnaire (given at 9- to 11-month visit):
Temperature of hot water moderated 10
Safety Questionnaire (given at 15- to 18-month visit):
Preventing poisoning 5
Preventing falls 8
Avoiding foods that promote choking 9
Knowing the Heimlich maneuver 13
a ETS = environmental tobacco smoke
tals and The Permanente Medical Group as well asfrom agencies of the State of California (Table 1).Team members for the project are shown in Table 2.

23The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
addition to the changes made throughout the devel-opment phase, several modifications have been madesince full implementation of Bright Systems®. Sugges-tions for these improvements have come from physi-cians and parents and in response to regulations. Forexample, early in 1999, when KP Northern Californiaadded rotavirus immunization to the six-month healthsupervision visit, the Speed Charting forms were up-dated to include this preventive measure; and whenthe decision to vaccinate was rescinded later that year,the item was removed from the forms.
More recently, when California education authoritiesdecided to require hepatitis B vaccine for all studentsentering the seventh grade, the immunization was addedto the speed-charting form used at the visit for 12- to14-year-old patients. In addition, the feasibility of groupvisits for teens—a possibility suggested by physiciansat KP South San Francisco—is being investigated.
“We learned a tremendous amount about the pro-cess of change in a large organization through BrightSystems®,” says Dr Sobel. “It all started with one dedi-cated physician, was supported regionally in a sys-tematic way, and incorporated the principles of CQI.It is a model for other programs.”
Indeed, Bright Systems® has been extended to incor-porate the Healthy Beginnings perinatal program nowbeing used in KP Northern California. Healthy Begin-nings expands standard patient education informationby incorporating classes for expectant parents. Theapplicability of speed charting forms at perinatal visitsis being studied. And KP Northern California’s RegionalHealth Education Department is exploring how BrightSystems® might work in the adult care setting.
According to Ms. Rieder, a key to the adaptability ofBright Systems® to other settings is its simplicity. “Noneof the Bright Systems® tools is terribly complicated. Wepurposefully kept the materials simple and inexpensiveto produce. That way, we can adapt and update themeasily and cost-effectively.” Bright Systems® is a greatexample of a low-tech solution that has a high impact.
Looking back at what Bright Systems® has accom-plished and how much more it promises, Dr Gee isconvinced that “change doesn’t have to mean morework. It can—and should—mean a better, simplerway to practice, better relationships between practi-tioners and their patients, and better health.” ❖
References1. Green M, editor. Bright futures: guidelines for healthsupervision of infants, children and adolescents. Arlington, VA:National Center for Education in Maternal and Child Health; 1994.2. Guidelines for health supervision III. 3rd ed. Elk Grove
Village, IL: American Academy of Pediatrics; 1997.3. Healthy People 2000: national health promotion anddisease prevention objectives. Washington, DC: US PublicHealth Service: 1991. (US Dept Of Health and HumanServices publication PHS 91-50212)4. Alpert JJ, Robertson LS, Kosa J, Heagarty MC, Haggerty RJ.Delivery of health care for children: report of an experiment.Pediatrics 1976;57:917-30.5. Wasserman RC, Inui TS, Barriatua RD, Carter WB,Lippincott P. Pediatric clinician’s support for parents makes adifference: an outcome-based analysis of clinician-parentinteraction. Pediatrics 1984;74:1047-53.6. Hoekelman RA. What constitutes adequate well-baby care?Pediatrics 1975;55:313-26.7. Gutelius MF, Kirsch AD, MacDonald S, Brooks MR,McErlean T. Controlled study of child health supervision:behavioral results. Pediatrics 1977;60:294-304.8. Reisinger KS, Bires JA. Anticipatory guidance in pediatricpractice. Pediatrics 1980;66:889-92.9. Dodds M, Nicholson L, Muse B III, Osborn LM. Grouphealth supervision visits more effective than individual visitsin delivering health care information. Pediatrics1993;91:668-70.10. Korsch BM, Negrete F, Mercer AS, Freemon B. Howcomprehensive are well child visits? Am J Dis Child1971;122:483-8.11. Osborn LM. Effective well-child care. Curr Probl Pediatr1994;24:306-26.12. Frankowski BL, Weaver SO, Secker-Walker RH. Advisingparents to stop smoking: pediatricians’ and parents’ attitudes.Pediatrics 1993;91:296-300.13. National Center for Injury Prevention and Control. Tenleading causes of death, 1995. Atlanta, GA: Centers forDisease Control and Prevention; 1997.14. Rivara FP, Grossman DC. Prevention of traumatic deathsto children in the United States: how far have we come andwhere do we need to go? Pediatrics 1996;97(6Pt1):791-7.15. Childhood injuries in the United States. Division of InjuryControl, Center for Environmental Health and Injury Control,Centers for Disease Control. Am J Dis Child 1990;144:627-46.16. Pirkle JL, Flegal KM, Bernert JT, Brody DJ, Etzel RA,Maurer KR. Exposure of the US population to environmentaltobacco smoke: the Third National Health and NutritionExamination Survey, 1988-1991. JAMA 1996;275:1233-40.17. Environmental tobacco smoke: a hazard to children.American Academy of Pediatrics Committee on Environmen-tal Health. Pediatrics 1997;99:639-42.18. Walton M. The Deming management method. New York:Perigee; 1986.19. Carney PA, Dietrich AJ, Keller A, Landgraf J, O’ConnorGT. Tools, teamwork and tenacity: an office system forcancer prevention. J Fam Pract 1992;35:388-94.
Table 4. Satisfaction expressed by physicians and otherhealth care practitioners
Aspect of Bright Systems® you wouldrecommend to other physicians
Percentageresponding yes
Speed Charting materials? 88
Healthy Kids-Healthy Futures materials? 96
Health Questionnaires? 97
“It all started withone dedicatedphysician ...”

24 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
The pilot project for Bright Systems®:A Total Quality Management Project to ImproveChildren’s Health was initiated in Pleasantonin 1991 and 1992 and implemented Regionwidein Kaiser Permanente Northern California(KPNC) in 1997. Table 1 shows the Project Teamand Contact Person.
BackgroundPrimary pediatric care and comprehensive health
supervision have demonstrated improvements in re-ducing hospitalizations, operations, illness visits andmissed appointments. Comprehensive health super-vision visits also demonstrate improved parentsatisfaction, increased maternal compliance, improveddiet, and maternal self-confidence.1-4
Fifty percent of all visits to a pediatric departmentare considered preventive visits, or health supervi-sion visits. A health supervision visit focuses onprimary as well as secondary prevention through riskassessment, anticipatory guidance (provider counsel-ing), screening tests, and immunizations. Routinehealth supervision visits are an important way to keepchildren healthy.5-7
Office systems have been studied as a way to im-prove the delivery of preventive services and havedemonstrated effectiveness at improving cancerscreening and physician counseling.8-14 Office sys-tems have been defined as a series of routinessupported by the shared responsibilities of all prac-tice personnel as well as by various tools.9 Tools thathave been studied include flowsheets, chart stickers,structured encounter forms, patient information, andquestionnaires.15-27 Total Quality Management (TQM)has also been suggested as a way to improve thedelivery of preventive services.29,30
Injury prevention and environmental tobacco smokecounseling have been identified as high priorities forhealth supervision.31-34 Injuries are the leading causeof death in children and adolescents beyond the firstyear of life and in 1986, more than 22,000 US chil-dren aged 0 to 19 years died of injuries. Injuries areestimated to be responsible for 600,000 hospitaliza-tions and 16 million emergency department visits eachyear. The annual medical cost of childhood injuriesis estimated to be over $7.5 billion.35-37 The effective-ness of physician injury prevention counseling hasbeen demonstrated in several studies.33,34,38 In addi-t ion to injuries, smoking and exposure toenvironmental tobacco smoke (ETS) pose seriousthreats to children’s health. Approximately 43% ofchildren two months to 11 years of age live in homeswith at least one smoker. Exposure to environmen-tal tobacco smoke is associated with sudden infantdeath syndrome (SIDS), bronchiolitis, acute otitismedia, middle ear effusions, asthma, altered lipidprofiles, and cancer. Environmental tobacco smokecontributes to an estimated 6200 childhood deathsand $4.6 billion in direct medical expenses everyyear.31,32,39 The effectiveness of brief physician coun-seling reinforced by written patient information onchanging health behaviors has been demonstratedin several studies.40-42
Despite the demonstrated effectiveness of compre-hensive health supervision, studies have shown thatthe amount of time spent during the health supervisionvisit to deliver anticipatory guidance is often limited to8.4% of the total visit time.43 Other studies have demon-strated that injury prevention counseling is covered lessthan 50% of the time.44-46 Few pediatricians routinelytake parent smoking histories.47 Behavioral concernsfrom parents are also often not covered.44,45
Bright Systems®: A Total Quality Management Projectto Improve Children’s Health
Table 1. Team contributing to Bright Systems®: A Total QualityManagement Project to Improve Children's Health
Team member names/titles: Scott M. Gee, MD, Project Director,Associate Director for Preventive Medicine, Regional Health Education;Pamela Larson, MPH, Project Manager, Director of Prevention & Self-Care;Regional Health Education; Linda Rieder, MPH, Pediatric Program Manager,Regional Health Education; Valerie Sheehan, MPH, Pediatric ProgramCoordinator, Regional Health Education; Kimmie Lee, RD, MPH,Publications Coordinator, Regional Health Education; Rachelle Mirkin, MPH,Interregional Consultant, Care Management Institute.
Contact person: Scott M. Gee, MD, Regional Health Education, 1950Franklin Streeet, 13th Floor, Oakland, CA 94612 (e-mail: [email protected]).
ION
ION
®
Figure 1.
Northern California Region
Fifty percent of allvisits to a pediatric
department areconsidered
preventive visits, orhealth supervision
visits.

25The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
ProcessBright Systems® began as a TQM Project at the De-
partment of Pediatrics at Pleasanton in 1991. Surveysof doctors, nurses, and administrators from both TPMGand KFH were used to develop the customer needsspreadsheets (Figure 1) along with surveys of HealthPlan members. Customer needs were transferred tothe Bright Systems® products and processes through aseries of Juran quality planning spreadsheets. Con-struction of the office system began with the PhysicianPractice Survey and was followed by Speed Charting,Healthy Kids–Healthy Futures, and Safety Question-naires projects. The Safety Questionnaires are used tocollect age-specific parent safety behavior data. Thequestionnaires are distributed in the waiting room andcollected anonymously. The data from these question-naires are used for the continuous quality improvementand quality control activities of Bright Systems®. Thecompleted office system was implemented and evalu-ated at Pleasanton in 1992.
The success of the program spread rapidly, andfour clinics implemented the program in 1993. Re-gional Health Education (RHE) Matching Grant fundswere obtained in 1994 to support the disseminationof the program. The dissemination of Bright Systems®
followed the process described by Rogers in “Diffu-sion of Innovations.”48-50 The early adopters wouldnot use the program without adaptation and madesignificant improvements in the office system toolsas part of the adaptation process. It became clearthat adaptation would have to occur to achieve wide-spread dissemination. RHE staff provided on-sitefacilitation to overcome local barriers to implemen-tation and support for local adaptation. Later it wasdecided to use the entire PRECEDE model of change(Figure 2)51-52 and utilize predisposing, enabling, andreinforcing strategies at each new site. Customer con-tracts were used to set limits on the degree of localadaptation. The Safety Questionnairepreimplementation data were used to focus the in-jury prevention counseling (Speed Charting) andwritten parent information (Healthy Kids—HealthyFutures) on the specific safety issues identified bythe service population. Physician consensus was alsoused to adapt the office system to each clinic. Theadaptation of the office system through the combineduse of parent safety behavior data and physician con-sensus had four significant outcomes:
1. It improved acceptance of the officesystem by physicians and nonphysicianstaff, which facilitated dissemination.
2. Physicians learned more about healthsupervision and quality improvement byparticipating in the adaptation of theoffice system.
3. The system had a greater effect atimproving parent safety behaviors.
4. The office system tools were continuouslyimproved, and new tools were developed.
The adaptability of Bright Systems® clearly sepa-rated this office system from other “out-of-the-box”office systems such as “Put Prevention into Practice,”which has had difficulty gaining acceptance.13,14 Ad-aptation of the office system was followed byimplementation and postimplementation Safety Ques-tionnaire data collection and analysis. On-site surveysand chart reviews were also performed at all facili-ties to determine the actual use of the system.Postimplementation Safety Questionnaire data werepresented to each facility with suggestions for con-tinued improvement.
With the improvements of the office system fromthe “early adopters” and refinement of the implemen-tation process, dissemination entered the “middleadopters” phase of diffusion.47 This phase was charac-terized by rapid dissemination. In order to meet theincreased customer demands, additional funding wasacquired from the Successful Practices Implementa-tion Program in 1996. The Health Questionnaires (forhealth risk assessment) were added to the basic officesystem in 1996 as part of the “Guidelines for Preven-tion and Health Promotion” implementation strategy.
Figure 2.
The early adopterswould not use theprogram withoutadaptation and
made significantimprovements inthe office system
tools as part of theadaptation process.
It became clearthat adaptationwould have to
occur to achievewidespread
dissemination.
26 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
The “late adopters” phase was characterized bya slower pace of dissemination.48 Outreach (aca-demic detai l ing) was used to encourageparticipation. The last six sites participated in alarge parent survey (Pediatric Survey), which pro-vided the data on improved physician counseling.Complete KP Northern California dissemination wasachieved in 1997.
Objectives• Design an office system that delivers
consistent and comprehensive healthsupervision;
• Improve the quality and consistency ofthe anticipatory guidance given at healthsupervision visits;
• Improve parent safety behaviors;• Improve physician satisfaction by
reducing unnecessary work;• Demonstrate the effectiveness and cost-
effectiveness of the program;• Disseminate the program to all facilities in
Northern California.
MethodologyScope
Bright Systems® targets all children from birth to 19years as well as their families. In Northern California, thisprogram addresses the preventive health needs of nearlyhalf of all members. Although this application focuseson pediatrics, products and processes of the programhave been expanded to include perinatal and adult healthcare delivery (Figure 3). The perinatal program, HealthyBeginnings—Integrated Perinatal Education (Figure 4)was developed as a TPMG and KFH collaboration and iscurrently being disseminated. In a 1998 collaborationwith Children Now,53 KP identified routine health super-vision visits as a potential strategy to improve earlychildhood development. Bright Systems® is now main-tained, managed, and improved by KPNC Regional HealthEducation staff. The Chiefs of Pediatrics and AdolescentMedicine provide oversight for the pediatric program.The adult program is currently being evaluated.
The development and diffusion of Bright Systems®
involved a multidisciplinary team (Table 1) span-ning a range of departments and committeesthroughout TPMG, KFHP/H, and the California StateGovernment, including:
Kaiser Foundation Health Plan/Hospitals
• Program Offices (Care Management Institute):Provided consultation on development of the mate-rials and evaluation tools.
• Perinatal Services Study Group: Provided consul-tation on development of the Integrated PerinatalEducation Program.
• Compliance and Risk Management: Verified that allmaterials met legal standards and regulatory requirements.
• Temperament Program: Provided consultation onparental anticipatory guidance tool.
Risk AssessmentQuestionnaires
BrightSystemsPediatric
HealthyBeginnings
Perinatal
BrightSystems
Adult
Yes Yes Yes
StructuredEncounter Forms
Yes Yes Yes
Written PatientInformation
Yes Yes Yes
Staff Training Yes Yes Yes
Patient EducationCurriculum
Yes
Group Visits Yes Yes
Continuous QualityImprovement
Yes
Bright Systems - Products & Processes
Figure 3.
HealthybeginningsPERINATAL OFFICE SYSTEM
Figure 4.
Bright Systems®
targets all childrenfrom birth to 19years as well astheir families. In
NorthernCalifornia, this
program addressesthe preventivehealth needs ofnearly half of all
members.
27The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
The Permanente Medical Group• Facility Pediatrics Departments: Doctors, nurses,
behavioral health specialists, medical assistants, re-ceptionists, and health educators providedconsultation on development of the materials andtheir integration into care.
• Chiefs of Pediatrics: Granted approval and en-dorsement of materials and system.
• Adolescent Specialists: Granted approval and en-dorsement of materials and system.
• Documentation Management Committee: Pro-vided consultation on medical records standards forKaiser Permanente.
• Committee of Health Information Managers andPhysicians: Provided consultation on medical recordstandards for NCQA.
California State Government
• Department of Health Services: Provided con-sulting on parental anticipatory guidance and healthrisk assessment tools for MediCal.
• Child Health and Disability Prevention (CHDP)Program: Provided consulting on parental anticipa-tory guidance and health risk assessment tools.
ProductsBright Systems® used TQM methodologies to develop
a complete office system, staff training, and continuousimprovement in quality of health supervision visits. Thebasic office system (Figure 5) includes:
• The Physician Practice Survey (healthsupervision guidelines spreadsheet);
• Speed Charting (age-specific structuredencounter forms);
• Healthy Kids–Healthy Futures (age-specific parent information);
• Safety Questionnaires (data collection tool).Bright Systems® covers a wide variety of health top-
ics and particularly stresses injury prevention andenvironmental tobacco smoke counseling. The of-fice system was extensively evaluated anddemonstrated improvements in physician counsel-ing, parent safety behaviors, and physiciansatisfaction. Dissemination of the program to KPNCand four other KP Regions used the cutting-edge strat-egies from Green51 and Rogers.48-50
MeasuresThe Bright Systems® comprehensive program includes
delivery of preventive services to infants, children, teens,and adults. Alternative care models such as group and
cluster visits were also developed. An overview of theproducts and processes are shown in Figures 1 to 3.These tools are all designed to deliver a consistent pre-vention message and reinforce self-care. Bright Systems®
tools are reviewed, updated, and improved annually aspart of the Guidelines for Prevention and Health Pro-motion revision process and to meet NCQA standardsfor documentation. The Bright Systems® staff manageall the products and processes and keep the office sys-tem consistent with new recommendations from externalgroups such as the Centers for Disease Control andPrevention (CDC) and the American Academy of Pedi-atrics (AAP). All the content is evidence-based and hasbeen approved by the relevant Chiefs groups. All mate-rials are designed for limited literacy and culturalsensitivity. Bright Systems® utilized three different sur-vey instruments to evaluate effectiveness.
Pediatric Survey
This instrument collected self-reported parent be-haviors and parent recall of anticipatory guidancegiven at health supervision visits. This survey wasapplied at six sites in conjunction with the 4- to 6-month visits. Chi-square tests were used for statisticaltesting. For the 4- to 6-month visit survey, findingswere considered statistically significant at p < .05.For the 18- to 24-month visit survey, findings wereconsidered statistically significant at p < .001. Whenno statistically significant difference between the pro-portions was found, the abbreviation NS was used.
PHYSICAL 2 W
HEIGHTWEIGHTHEAD CIR.B. P.VISION
2 M 4 M 6 M 9 M 12 M 15 M 18 M 2 Y 3 Y 4 Y 5 Y 6 Y 8 Y 10 Y 11-1 4 Y 15-17 Y 18-21 Y
HEARING
APDTHDPTTdTOPVIPVMMRHIBHEP BV - ZT.B.
CBCUALEADCHOL
PHYSICIAN PRACTICE SURVEYPHYSICIAN: SCOTT GEE, M.D.
12 MO NTH WELL CHILD VISIT
AGE: __________months old
W EIGHT: __________pound/oz
HEIGHT: __________inches
HEAD CIRC: __________inches
Co ncerns:
Nu trition:
Developme nt:
Elim ina tion:
Sle ep:
NO PROBLE MS
NO PROBLE MS
_____ ___WORDS
PA T- A-CAKE
PINCER G RASP
CRUISES
SEE DE NVER
DATE Phone #:
C UP
EYES SOMETIMES APPEAR TO CROSS
Accompanied By: M OM
D AD
B RIGHT SYSTEMST M
" Speed Cha rting"
OT HER
RE LATIVE
X = YES OR DISCUSSED * O = NO * BLA NK = NOT ASKED OR DISCUSSED
N ONE
Inte rim History :
Social Histo ry:
WHOLE MILK
RE ASONABLY BALANCED
TAB LE FOODS
NO PROBLEMS
DAY CARESINGLE PARENT
SMOKERS IN THE HOUS E
NO PROBLEMS
SIGNIFICA NT ILLNESS OR I NJURY:
IMPRINT AREA
PEDIATRIC OFFICE SYSTEM
Do you always place yo ur child in a ca r sea t for every ride? ... ... . ... ... ... . ... ... ... . ... ... . ... ... ... . ... .. � � �
Do you have Syrup of Ip ecac in the house?.... ... . ... ... ... . ... ... ... . ... ... ... . ... ... ... . ... ... ... . ... ... . ... ... ... . . � � �
Hav e you turne d your water heater temperature down to low or warm (<120¡�F.)?.. ... ... . ... ... � � �
Do you place ga tes at the entrance to stairways?.. ... ... . ... ... ... . ... ... ... . ... ... ... . ... ... ... . ... ... . ... ... ... . .. � � �
Do you feed yo ur child formula with i ron, iron fo rti fied cereal, or me at ev ery day?.... ... ... . . � � �
Do you avo id putting your child to bed wi th a bo ttle? (can cause serious tooth decay). . ... ... . � � �
Do you have a swimming po ol, ho t tub, spa or fish pond in yo ur backyard? ... . ... ... . ... ... ... . ... .� � �
Do es anyone smoke in yo ur home?. . . ... ... ... . ... ... ... . ... ... ... . ... ... ... . ... ... ... . ... ... ... . ... ... . ... ... ... . ... ... ..� � �
Do es your child l ive in or regularly visi t a house or other location wi th p eeling or chipping paint built before 1960? . . . ... ... ... . ... ... ... . ... ... ... . ... ... ... . ... ... ... . ... ... . ... ... ... . ... .� � �
Do es your child l ive in or regularly visi t a house bu ilt before 19 60 with
rec ent or ongoing renovation or re modeling? . . ... ... . ... ... ... . ... ... ... . ... ... ... . ... ... ... . ... ... . ... ... ... . ... ... .� � �
Do es your child have a parent, sibling, housemate, or playmate who is being t reated or followed for lead po iso ning? ... . ... ... ... . ... ... ... . ... ... ... . ... ... ... . ... ... ... . ... ... ... . ... ... . ... ... ... . .� � �
Do es your child l ive wi th someo ne whose job or ho bby inv olves exposure to lead? . . ... . ... ... .� � �
Do es your child l ive near an active lead smelter or battery rec ycling plant? . . . ... ... . ... ... ... . ... ..� � �
Has an y household memb er or caregiver eve r ha d active TB or a posi tive TB sk in test? . . ... .� � �
Has an y household memb er or caregiver l ived or frequently t raveled outside the U. S .? . . ... . .� � �
Do es any ho usehold me mber or caregive r ha ve HIV or AIDS? ... ... . ... ... ... . ... ... ... . ... ... . ... ... ... . .� � �
Has yo ur family ev er lived in a ho meless sh elter or i s your child a foster child? . . . ... ... ... . ... ..� � �
Is there anything you wo uld like to discuss today?
BRIGHT SY STEMSTM
DA TE I MPRINT AREA
Yes NoDoesn' tApply
MD / PNP
Lea
d P
ois
on
ing
Ris
k F
acto
rsT
B R
isk
Fac
tors
NOT FOR SALE OR REPRODUCTI ON WITHOUT PERMISSIONFRO M THE PERMA NENTE MEDICAL GROUP, I NC.
Healthy Kids - Healthy Futures
Safety
Parenting
SIDS (c rib death): put y our baby to s leep on h is/her side or back (not stomach) on a f irm, f lat mattre ss.
Ca r Seat: use for every ri de. In stall properl y.Falls: do not l eave y our b aby alo ne on a bed, sofa o r ta ble.Bu rns: tu rn your wate r heater tempera ture down to wa rm or low (<1 20 deg. F). Insta ll smoke d etectors a nd check regul arl y. Don’t dri nk hot l iquids near baby. Al ways check water temperature before putt ing baby in bath.
Safe Toy s: (see oth er side) .
Do n’�t wo rry about spoili ng your baby.Ne ver l eave your baby a lone in your home, car o r bath tub.
He lp your baby develop good sleep habits (o ther s ide).T ry to set time aside for older sibl ings.Ho ld, ta lk and sing to your baby.Sh akin g or spanking a b aby may cause serious i njury and death .
Bre astmilk is th e best food fo r your ba by.Feed y our baby breastm ilk or formula with iron (consult your doctor if using low iron fo rmula ).
Bre ast fe ed your ba by "on demand" (let your baby decide when a nd how long to nurse).Formula fed bab ies usua lly eat 4 -6 ounc es every 4 hours .Do not warm bottles in a m icrowave.Always c heck how hot th e formula is before feed ing your ba by.Wait unti l 4 -6 months old to s tart solid fo od.
Sm oking a round y our baby increases his /he r r isk fo r SIDS, ear infections and a sthma. Ca ll He alth Education (510-8 47-5172) if you would
lik e to qu it.W ash your hands before fe eding and after c hanging dia pers.Do n’t d rive after drinking a lcohol and we ar y our s eat be lt.Ta ke your ba by for wa lks.
Dat e:_________ _ Weight :_________ _ Height :__________
2 Month Check Up
Feeding
Healthy Habits
Figure 5.
Bright Systems®
covers a widevariety of health
topics andparticularly
stresses injuryprevention andenvironmentaltobacco smoke
counseling.
28 The Permanente Journal / Spring 2000 / Volume 4 No. 2
Safety QuestionnairesThese questionnaires collected self-reported parent safety behaviors. This
survey was applied at four months, 9 to 11 months, and 15 to 18 months ofage, before and after implementation at most sites. Chi-square tests wereused, and findings were considered statistically significant at p < .05.
Physician and Practitioner SurveyThis survey collected data on provider satisfaction with
the office system. This questionnaire was sent to a randomsample of 81 pediatricians in KPNC after Regionwide imple-mentation of Bright Systems®. The response rate was 67%(55 of 81 surveys were returned). A t test was used, andfindings were considered statistically significant at p < .05.
ResultsImproved Quality of Patient CarePediatric Survey
Three hundred twenty-one parents of children agedfour to six months completed the preimplementation sur-vey, and 202 completed the postimplementation survey.Parent recall of the anticipatory guidance given by thephysicians at the four- to six-month health supervisionvisits are shown in Figure 6. Significant improvements (p< 0.05) in delivery of anticipatory guidance were reportedfor environmental tobacco smoke (↑28%), correct sleep-ing position (↑25%), hot water temperature < 120 ° F(↑24%), reducing the risk of scald burns (↑23%), andreducing the risk of falls (↑17%).
Seven hundred forty-one parents of children aged 18to 24 months completed the preimplementation survey,and 575 completed the postimplementation survey. Par-ent recall of the anticipatory guidance given by thephysicians at the 18- to 24-month health supervision vis-its are shown in Figure 7. Significant improvements (p <0.001) in the delivery of anticipatory guidance were re-ported for environmental tobacco smoke (↑26%), syrupof ipecac use (↑11%), car seat use (↑19%), supervisionaround water (↑23%), window locks on upper-story win-dows (↑26%), and reducing risk of choking (↑17%).
Safety Questionnaires
Three hundred sixty-seven parents of children aged fourmonths completed the preimplementation survey, and 417completed the postimplementation survey (Figure 8). Sig-nificant improvements (p < 0.05) in parents’ self-reportedsafety behaviors at the four-month health supervision visitwere demonstrated for crib safety (↑55%), avoidingwaterbeds (↑6%), preventing falls (↑5%), avoiding cribtoys (↑9%), and using safe toys (↑4%).
Three hundred thirty-one parents of children aged 9 to11 months completed the preimplementation survey, and440 completed the postimplementation survey (Figure9). Parents at the 9- to 11-month visit reported improve-ment (p < 0.05) in turning down the water temperatureto less than 120°F (↑10%). This improvement correspondswith the 24% increase in provider counseling for riskreduction noted at the 4- to 6-month visit (Figure 6).
Self-ReportedBehaviors at 4
Month Visit87
92
90
96
91
96
90
94
84
93
78
80
82
84
86
88
90
92
94
96
% o
f P
aren
ts
Crib Saf
ety
Avoid
Wat
erbed
Preve
nting F
alls
Safe T
oys
Crib T
oys
Pre: n=367Post: n=417
p < 0.05
Figure 8.
9496
85 86
34
60
43
54
42
61
32
55
20
46 44
61
01020
304050
6070
8090
100
% o
f P
aren
ts
Answer
ed Q
uest (
NS)
Develo
pmen
t (NS)
Enviro
nmen
tal S
mok
e
Poison
ing
Car S
eat
Drownin
gFall
s
Chokin
g
Pre: n=741Post: n=575
p < 0.001
AnticipatoryGuidance at
18-24 Month Visit
Figure 7.
AnticipatoryGuidance at
4-6 Month Visit
97989092
41
69
55
80
56
69
21
45
20
4347
64
0102030405060708090
100
% o
f P
aren
ts
Answer
ed Q
uest (
NS)
Develo
pmen
t (NS)
Enviro
nmen
tal S
mok
e
Sleepin
g Pos
ition
Car S
eat (
NS)
Wat
er T
emp <
120 D
eg
Scald
Burn
sFall
s
Pre: n=321Post: n=202
p < 0.05
Figure 6.
clin
ical
con
trib
uti
on
s
-

29The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
Three hundred seventy parents of children aged15 to 18 months completed the preimplementationsurvey, and 513 completed the postimplementationsurvey (Figure 10). Significant improvements (p <0.05) in parents’ self-reported safety behaviors at the15- to 18-month visit were demonstrated for prevent-ing poisoning (↑5%), preventing falls (↑8%), avoidingchoking foods (↑9%), and knowing the Heimlichmaneuver (↑13%).
Improved Physician and Practitioner Satisfaction
Physician & Practitioner Survey
Physicians and practitioners reported benefits, in-cluding improved documentation, time-saving, andimproved counseling (Table 2).
Improved Member Satisfaction
Member Satisfaction (part of the Pediatric Survey)
Seven hundred forty-one parents of children ages18 to 24 months completed the preimplementationsurvey, and 575 completed the postimplementationsurvey. Although not statistically significant, smallimprovements were demonstrated for questions aboutsatisfaction with the doctor or nurse practitioner (NP)(Table 3).
EvaluationRelevance to Patient Care
Bright Systems® increased physician counselingon environmental tobacco smoke by 26% to 28%and injury prevention counseling by 11% to 26%.The improvements in parents’ self-reported safetybehaviors of 5% to 13% provide further evidenceof the effectiveness of physician counseling at im-proving safety behaviors. In a recent article,Quinlan et al,38 reported on the outcomes of atelephone survey of US households used to de-termine the rate of injury prevention counselingreceived among US children. The rates of injuryprevention counseling reported by parents fromthe Bright Systems® program were much higherthan the national average for having syrup of ip-ecac in the home (37% higher) and use of a carseat (30% higher). Nine of the 12 injury preven-tion topics for anticipatory guidance (Figures 6and 7) exceeded the Healthy People 2000 goal of50%.7 Improvements in environmental tobaccosmoke and injury prevention counseling did notcome at the expense of answering all of the par-ents’ questions or screening for developmentalmilestones. We believe this achievement consti-tutes evidence that we succeeded in developinga single office system that delivers comprehen-sive health supervision while at the same timeemphasizes key issues. We estimate that routinephysician injury prevention counseling combinedwith written patient information could save $5.50in medical costs per health supervision visit forchildren aged 0 to 4 years.54 At a cost of $0.09 inmaterials per health supervision visit, Bright Sys-tems® is a highly cost-effective intervention.
Innovation and Leadership
Bright Systems®, the only fully integrated office sys-tem entirely designed using TQM methodologies, hasdemonstrated significant improvements in quality andachieved large-scale dissemination. This program usesoffice systems, staff training, and continuous qualityimprovement to form a data-driven health care de-livery system for improving health outcomes. BrightSystems® has demonstrated the effectiveness of thesystematic application of a multifaceted approach toimproving physician performance and satisfaction.As a “grassroots” TQM project driven from bottom totop, Bright Systems® has been a breakthrough in or-ganizational learning for KPNC.
Table 2. Results of Physician/Practioner Survey
Would you recommend to other physicians? Yes
Speed charting 88%
Healthy Kids—Healthy Futures 96%
Health questionaires 97%
Table 3. Parental survey responses showingimproved satisfaction
Survey question
Percent ofparents
answering "Yes"
Before After
Did the doctor/NP answer allof your questions andaddress your concerns?
94% 96%
Did the doctor/NP seemconcerned about you andyour child?
85% 88%
Did the doctor/NP spendenough time with you?
86% 89%
At a cost of $0.09in materials per
health supervisionvisit, Bright
Systems® is ahighly cost-
effectiveintervention.
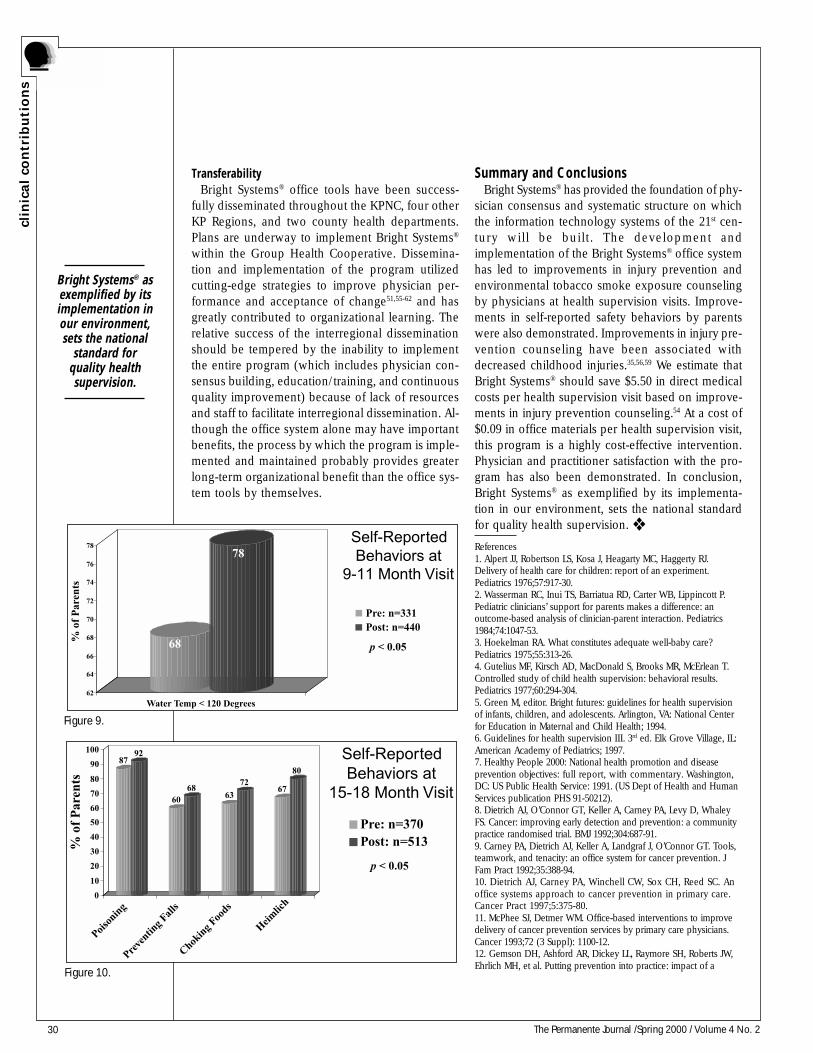
30 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
TransferabilityBright Systems® office tools have been success-
fully disseminated throughout the KPNC, four otherKP Regions, and two county health departments.Plans are underway to implement Bright Systems®
within the Group Health Cooperative. Dissemina-tion and implementation of the program utilizedcutting-edge strategies to improve physician per-formance and acceptance of change51,55-62 and hasgreatly contributed to organizational learning. Therelative success of the interregional disseminationshould be tempered by the inability to implementthe entire program (which includes physician con-sensus building, education/training, and continuousquality improvement) because of lack of resourcesand staff to facilitate interregional dissemination. Al-though the office system alone may have importantbenefits, the process by which the program is imple-mented and maintained probably provides greaterlong-term organizational benefit than the office sys-tem tools by themselves.
Summary and ConclusionsBright Systems® has provided the foundation of phy-
sician consensus and systematic structure on whichthe information technology systems of the 21st cen-tury will be built. The development andimplementation of the Bright Systems® office systemhas led to improvements in injury prevention andenvironmental tobacco smoke exposure counselingby physicians at health supervision visits. Improve-ments in self-reported safety behaviors by parentswere also demonstrated. Improvements in injury pre-vention counseling have been associated withdecreased childhood injuries.35,56,59 We estimate thatBright Systems® should save $5.50 in direct medicalcosts per health supervision visit based on improve-ments in injury prevention counseling.54 At a cost of$0.09 in office materials per health supervision visit,this program is a highly cost-effective intervention.Physician and practitioner satisfaction with the pro-gram has also been demonstrated. In conclusion,Bright Systems® as exemplified by its implementa-tion in our environment, sets the national standardfor quality health supervision. ❖
References1. Alpert JJ, Robertson LS, Kosa J, Heagarty MC, Haggerty RJ.Delivery of health care for children: report of an experiment.Pediatrics 1976;57:917-30.2. Wasserman RC, Inui TS, Barriatua RD, Carter WB, Lippincott P.Pediatric clinicians’ support for parents makes a difference: anoutcome-based analysis of clinician-parent interaction. Pediatrics1984;74:1047-53.3. Hoekelman RA. What constitutes adequate well-baby care?Pediatrics 1975;55:313-26.4. Gutelius MF, Kirsch AD, MacDonald S, Brooks MR, McErlean T.Controlled study of child health supervision: behavioral results.Pediatrics 1977;60:294-304.5. Green M, editor. Bright futures: guidelines for health supervisionof infants, children, and adolescents. Arlington, VA: National Centerfor Education in Maternal and Child Health; 1994.6. Guidelines for health supervision III. 3rd ed. Elk Grove Village, IL:American Academy of Pediatrics; 1997.7. Healthy People 2000: National health promotion and diseaseprevention objectives: full report, with commentary. Washington,DC: US Public Health Service: 1991. (US Dept of Health and HumanServices publication PHS 91-50212).8. Dietrich AJ, O’Connor GT, Keller A, Carney PA, Levy D, WhaleyFS. Cancer: improving early detection and prevention: a communitypractice randomised trial. BMJ 1992;304:687-91.9. Carney PA, Dietrich AJ, Keller A, Landgraf J, O’Connor GT. Tools,teamwork, and tenacity: an office system for cancer prevention. JFam Pract 1992;35:388-94.10. Dietrich AJ, Carney PA, Winchell CW, Sox CH, Reed SC. Anoffice systems approach to cancer prevention in primary care.Cancer Pract 1997;5:375-80.11. McPhee SJ, Detmer WM. Office-based interventions to improvedelivery of cancer prevention services by primary care physicians.Cancer 1993;72 (3 Suppl): 1100-12.12. Gemson DH, Ashford AR, Dickey LL, Raymore SH, Roberts JW,Ehrlich MH, et al. Putting prevention into practice: impact of a
Self-ReportedBehaviors at
9-11 Month Visit
68
78
62
64
66
68
70
72
74
76
78
% o
f P
aren
ts
Water Temp < 120 Degrees
Pre: n=331Post: n=440
p < 0.05
Figure 9.
Self-ReportedBehaviors at
15-18 Month Visit
8792
6068
63
7267
80
0
10
20
30
40
50
60
70
80
90
100
% o
f P
aren
ts
Poison
ing
Preve
nting F
alls
Chokin
g Foo
ds
Heimlic
h
Pre: n=370Post: n=513
p < 0.05
Figure 10.
Bright Systems® asexemplified by itsimplementation inour environment,sets the national
standard forquality healthsupervision.
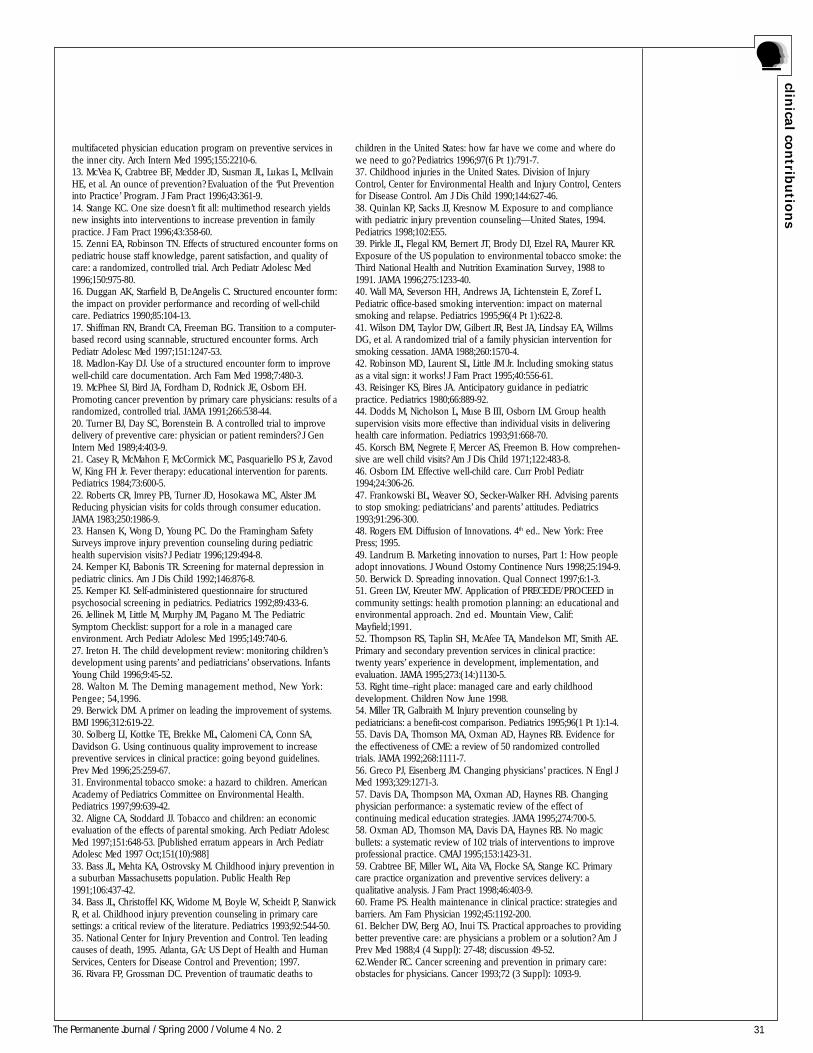
31The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
multifaceted physician education program on preventive services inthe inner city. Arch Intern Med 1995;155:2210-6.13. McVea K, Crabtree BF, Medder JD, Susman JL, Lukas L, McIlvainHE, et al. An ounce of prevention? Evaluation of the ‘Put Preventioninto Practice’ Program. J Fam Pract 1996;43:361-9.14. Stange KC. One size doesn’t fit all: multimethod research yieldsnew insights into interventions to increase prevention in familypractice. J Fam Pract 1996;43:358-60.15. Zenni EA, Robinson TN. Effects of structured encounter forms onpediatric house staff knowledge, parent satisfaction, and quality ofcare: a randomized, controlled trial. Arch Pediatr Adolesc Med1996;150:975-80.16. Duggan AK, Starfield B, DeAngelis C. Structured encounter form:the impact on provider performance and recording of well-childcare. Pediatrics 1990;85:104-13.17. Shiffman RN, Brandt CA, Freeman BG. Transition to a computer-based record using scannable, structured encounter forms. ArchPediatr Adolesc Med 1997;151:1247-53.18. Madlon-Kay DJ. Use of a structured encounter form to improvewell-child care documentation. Arch Fam Med 1998;7:480-3.19. McPhee SJ, Bird JA, Fordham D, Rodnick JE, Osborn EH.Promoting cancer prevention by primary care physicians: results of arandomized, controlled trial. JAMA 1991;266:538-44.20. Turner BJ, Day SC, Borenstein B. A controlled trial to improvedelivery of preventive care: physician or patient reminders? J GenIntern Med 1989;4:403-9.21. Casey R, McMahon F, McCormick MC, Pasquariello PS Jr, ZavodW, King FH Jr. Fever therapy: educational intervention for parents.Pediatrics 1984;73:600-5.22. Roberts CR, Imrey PB, Turner JD, Hosokawa MC, Alster JM.Reducing physician visits for colds through consumer education.JAMA 1983;250:1986-9.23. Hansen K, Wong D, Young PC. Do the Framingham SafetySurveys improve injury prevention counseling during pediatrichealth supervision visits? J Pediatr 1996;129:494-8.24. Kemper KJ, Babonis TR. Screening for maternal depression inpediatric clinics. Am J Dis Child 1992;146:876-8.25. Kemper KJ. Self-administered questionnaire for structuredpsychosocial screening in pediatrics. Pediatrics 1992;89:433-6.26. Jellinek M, Little M, Murphy JM, Pagano M. The PediatricSymptom Checklist: support for a role in a managed careenvironment. Arch Pediatr Adolesc Med 1995;149:740-6.27. Ireton H. The child development review: monitoring children’sdevelopment using parents’ and pediatricians’ observations. InfantsYoung Child 1996;9:45-52.28. Walton M. The Deming management method, New York:Pengee; 54,1996.29. Berwick DM. A primer on leading the improvement of systems.BMJ 1996;312:619-22.30. Solberg LI, Kottke TE, Brekke ML, Calomeni CA, Conn SA,Davidson G. Using continuous quality improvement to increasepreventive services in clinical practice: going beyond guidelines.Prev Med 1996;25:259-67.31. Environmental tobacco smoke: a hazard to children. AmericanAcademy of Pediatrics Committee on Environmental Health.Pediatrics 1997;99:639-42.32. Aligne CA, Stoddard JJ. Tobacco and children: an economicevaluation of the effects of parental smoking. Arch Pediatr AdolescMed 1997;151:648-53. [Published erratum appears in Arch PediatrAdolesc Med 1997 Oct;151(10):988]33. Bass JL, Mehta KA, Ostrovsky M. Childhood injury prevention ina suburban Massachusetts population. Public Health Rep1991;106:437-42.34. Bass JL, Christoffel KK, Widome M, Boyle W, Scheidt P, StanwickR, et al. Childhood injury prevention counseling in primary caresettings: a critical review of the literature. Pediatrics 1993;92:544-50.35. National Center for Injury Prevention and Control. Ten leadingcauses of death, 1995. Atlanta, GA: US Dept of Health and HumanServices, Centers for Disease Control and Prevention; 1997.36. Rivara FP, Grossman DC. Prevention of traumatic deaths to
children in the United States: how far have we come and where dowe need to go? Pediatrics 1996;97(6 Pt 1):791-7.37. Childhood injuries in the United States. Division of InjuryControl, Center for Environmental Health and Injury Control, Centersfor Disease Control. Am J Dis Child 1990;144:627-46.38. Quinlan KP, Sacks JJ, Kresnow M. Exposure to and compliancewith pediatric injury prevention counseling—United States, 1994.Pediatrics 1998;102:E55.39. Pirkle JL, Flegal KM, Bernert JT, Brody DJ, Etzel RA, Maurer KR.Exposure of the US population to environmental tobacco smoke: theThird National Health and Nutrition Examination Survey, 1988 to1991. JAMA 1996;275:1233-40.40. Wall MA, Severson HH, Andrews JA, Lichtenstein E, Zoref L.Pediatric office-based smoking intervention: impact on maternalsmoking and relapse. Pediatrics 1995;96(4 Pt 1):622-8.41. Wilson DM, Taylor DW, Gilbert JR, Best JA, Lindsay EA, WillmsDG, et al. A randomized trial of a family physician intervention forsmoking cessation. JAMA 1988;260:1570-4.42. Robinson MD, Laurent SL, Little JM Jr. Including smoking statusas a vital sign: it works! J Fam Pract 1995;40:556-61.43. Reisinger KS, Bires JA. Anticipatory guidance in pediatricpractice. Pediatrics 1980;66:889-92.44. Dodds M, Nicholson L, Muse B III, Osborn LM. Group healthsupervision visits more effective than individual visits in deliveringhealth care information. Pediatrics 1993;91:668-70.45. Korsch BM, Negrete F, Mercer AS, Freemon B. How comprehen-sive are well child visits? Am J Dis Child 1971;122:483-8.46. Osborn LM. Effective well-child care. Curr Probl Pediatr1994;24:306-26.47. Frankowski BL, Weaver SO, Secker-Walker RH. Advising parentsto stop smoking: pediatricians’ and parents’ attitudes. Pediatrics1993;91:296-300.48. Rogers EM. Diffusion of Innovations. 4th ed.. New York: FreePress; 1995.49. Landrum B. Marketing innovation to nurses, Part 1: How peopleadopt innovations. J Wound Ostomy Continence Nurs 1998;25:194-9.50. Berwick D. Spreading innovation. Qual Connect 1997;6:1-3.51. Green LW, Kreuter MW. Application of PRECEDE/PROCEED incommunity settings: health promotion planning: an educational andenvironmental approach. 2nd ed. Mountain View, Calif:Mayfield;1991.52. Thompson RS, Taplin SH, McAfee TA, Mandelson MT, Smith AE.Primary and secondary prevention services in clinical practice:twenty years’ experience in development, implementation, andevaluation. JAMA 1995;273:(14:)1130-5.53. Right time–right place: managed care and early childhooddevelopment. Children Now June 1998.54. Miller TR, Galbraith M. Injury prevention counseling bypediatricians: a benefit-cost comparison. Pediatrics 1995;96(1 Pt 1):1-4.55. Davis DA, Thomson MA, Oxman AD, Haynes RB. Evidence forthe effectiveness of CME: a review of 50 randomized controlledtrials. JAMA 1992;268:1111-7.56. Greco PJ, Eisenberg JM. Changing physicians’ practices. N Engl JMed 1993;329:1271-3.57. Davis DA, Thompson MA, Oxman AD, Haynes RB. Changingphysician performance: a systematic review of the effect ofcontinuing medical education strategies. JAMA 1995;274:700-5.58. Oxman AD, Thomson MA, Davis DA, Haynes RB. No magicbullets: a systematic review of 102 trials of interventions to improveprofessional practice. CMAJ 1995;153:1423-31.59. Crabtree BF, Miller WL, Aita VA, Flocke SA, Stange KC. Primarycare practice organization and preventive services delivery: aqualitative analysis. J Fam Pract 1998;46:403-9.60. Frame PS. Health maintenance in clinical practice: strategies andbarriers. Am Fam Physician 1992;45:1192-200.61. Belcher DW, Berg AO, Inui TS. Practical approaches to providingbetter preventive care: are physicians a problem or a solution? Am JPrev Med 1988;4 (4 Suppl): 27-48; discussion 49-52.62.Wender RC. Cancer screening and prevention in primary care:obstacles for physicians. Cancer 1993;72 (3 Suppl): 1093-9.

32 The Permanente Journal / Spring 2000 / Volume 4 No. 2
IntroductionThe Childhood and Adolescent Immunization Program was de-
veloped for the Kaiser Permanente Colorado (KPCO) Denver/Boulder Local Market in response to our commitment to our pre-vention program and improving the health status of the childrenand adolescents. Team Members are listed in Table 1.
BackgroundIn 1996, the combination of new vaccines and new data, which
changed the ages at which vaccines are known to be efficacious,made it necessary to revise our immunization schedules. The re-sult of these changes was a decline in our overall immunizationrates for two-year-old infants from 1995 through 1996 as measuredby the HEDIS (Health-Plan Employer Data and Information Set).Further, effectively communicating and coordinating new sched-ules and vaccines to our providers and staff proved to be aformidable challenge.
Process
In late 1996, a small group of staff and providers reviewed therecords of all delinquent children in our HEDIS subset. In this pro-cess, we identified several opportunities for improvement. Amongour discoveries, we found that a significant percentage of delinquen-cies occurred because of missed opportunities and providers followingoutdated schedules or incorrect “relative” contraindications. Problemswith information and communication were identified. These prob-lem areas became the focus of our new initiatives. These discoverieschallenged all of us to achieve a higher level of quality improvement,and our team quickly embraced the new immunization initiatives.
ObjectivesThe objective of our project was to improve the immunization
rates of our children and to assure that these children were immu-nized accurately and on schedule. The foundation of our enhancedprogram was formal adoption of the Centers for Disease Controland Prevention (CDC) Standards for Pediatric Immunization Prac-tices.1 As a result, we initiated an aggressive population-basedimmunization campaign that included tracking and outreach toevery delinquent child aged 14 months, 20 months, and 12.5 yearswithin our KP Region. Our 1998 regional performance goal was toachieve the top quartile for all HEDIS quality measures.
MethodologyScope
Kaiser Permanente operates 15 medical offices in the Denver/Boulder Local Market, and more than 145 providers within ourorganization are involved with caring for children. Our Immuniza-tion Program within KPCO targets our entire population of children,not just the HEDIS subset. Although most of our work has beenwith infants and toddlers aged 0 to two years, the focus on achiev-ing higher coverage rates for all children has greatly intensifiedbecause of this initiative. Our Departments of Pediatrics, FamilyPractice, and Prevention jointly developed an implementation planfor this new effort. Molly Burchell, MD, Chief of Pediatrics, led theproject and currently champions the Immunization Program. Thelocal health care team champions, who perform all the detailedoutreach to members, are critical to improvements. The champi-ons are MAs, LPNs, RNs, or nursing supervisors, in cooperationwith physicians, depending on the interests and skills of the team.
Quality Measures
The primary measure of the success of the interventions is im-proved immunization coverage rates. If our interventions areworking, we should see a decrease in variation and improvedrates both at individual medical offices and as a program. As aregional quality assurance priority, the Primary Care Quality Councilreviews all HEDIS quality measures, including childhood immuni-zation rates. We created a clear channel of communication andaccountability by integrating our efforts with our Primary CareQuality Council. Feedback and new ideas are collated to developimproved processes that are adopted, along with our best prac-tices, across our KP Region. Childhood immunization coveragerates are critical HEDIS quality indicators for our KP Regional aswell as the national KP Program. This initiative and the strikingresults coincide with our focus on HEDIS measures as a founda-tion of our quality program.
Process ImplementationIn 1997, we formally adopted the Standards for Pediatric Immu-
nization Practices as recommended by the CDC and used this asa template for our improvement plan. In our review of existingpractices, we identified four critical areas as opportunity for im-provement. These four areas represented improvement
opportunities in six of the CDC standards.1. Assess immunization status at every encounter, and
follow only true contraindications (CDC Standards 4and 7). We implemented printing of the immunizationrecord throughout our KP Region from our computer-ized immunization tracking system for every child at allprimary care, urgent care, and trauma visits, includingweekend care visits. This strategy further helped us cap-ture missed opportunities, which has been identifiednationally as one of the greatest barriers to achieving
Table 1. Childhood/Adolescent Immunization Program Team Members
Molly Burchell, MD; Regional Department Chief of PediatricsJanet Nelson, RN, MS; Business Manager, Primary CareEmily Sharp, RN, MSN; Nursing SupervisorSharon Castro; Administrative Secretary, Primary CarePrimary Care Health TeamsContact Person: Molly Burchell, MD, RDC, Pediatrics, Primary CareAdministration; 2500 South Havana Street; Aurora, CO 80014; 303/338-3552;303/338-3565 (fax); [email protected]
The Childhood/Adolescent Immunization Program
clin
ical
con
trib
uti
on
s
Colorado Region
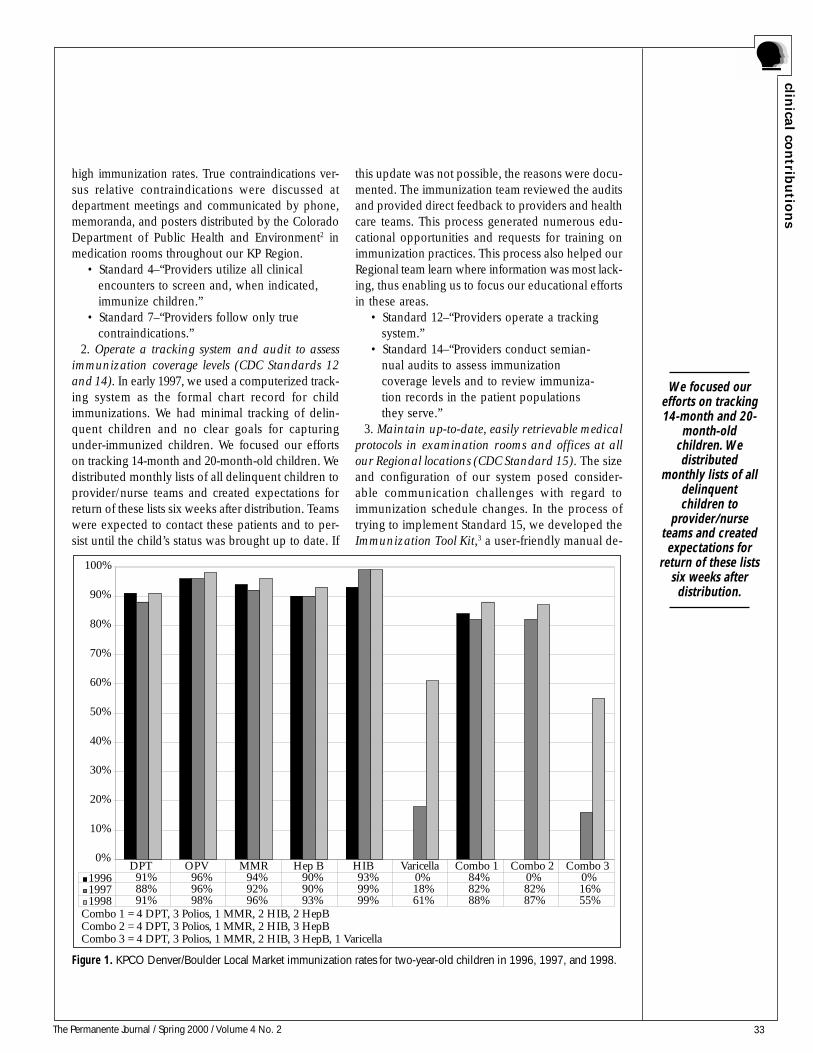
33The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
high immunization rates. True contraindications ver-sus relative contraindications were discussed atdepartment meetings and communicated by phone,memoranda, and posters distributed by the ColoradoDepartment of Public Health and Environment2 inmedication rooms throughout our KP Region.
• Standard 4–“Providers utilize all clinicalencounters to screen and, when indicated,immunize children.”
• Standard 7–“Providers follow only truecontraindications.”
2. Operate a tracking system and audit to assessimmunization coverage levels (CDC Standards 12and 14). In early 1997, we used a computerized track-ing system as the formal chart record for childimmunizations. We had minimal tracking of delin-quent children and no clear goals for capturingunder-immunized children. We focused our effortson tracking 14-month and 20-month-old children. Wedistributed monthly lists of all delinquent children toprovider/nurse teams and created expectations forreturn of these lists six weeks after distribution. Teamswere expected to contact these patients and to per-sist until the child’s status was brought up to date. If
this update was not possible, the reasons were docu-mented. The immunization team reviewed the auditsand provided direct feedback to providers and healthcare teams. This process generated numerous edu-cational opportunities and requests for training onimmunization practices. This process also helped ourRegional team learn where information was most lack-ing, thus enabling us to focus our educational effortsin these areas.
• Standard 12–“Providers operate a trackingsystem.”
• Standard 14–“Providers conduct semian-nual audits to assess immunizationcoverage levels and to review immuniza-tion records in the patient populationsthey serve.”
3. Maintain up-to-date, easily retrievable medicalprotocols in examination rooms and offices at allour Regional locations (CDC Standard 15). The sizeand configuration of our system posed consider-able communication challenges with regard toimmunization schedule changes. In the process oftrying to implement Standard 15, we developed theImmunization Tool Kit,3 a user-friendly manual de-
Combo 1 = 4 DPT, 3 Polios, 1 MMR, 2 HIB, 2 HepBCombo 2 = 4 DPT, 3 Polios, 1 MMR, 2 HIB, 3 HepBCombo 3 = 4 DPT, 3 Polios, 1 MMR, 2 HIB, 3 HepB, 1 Varicella
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1996 91% 96% 94% 90% 93% 0% 84% 0% 0%1997 88% 96% 92% 90% 99% 18% 82% 82% 16%1998 91% 98% 96% 93% 99% 61% 88% 87% 55%
DPT OPV MMR Hep B HIB Varicella Combo 1 Combo 2 Combo 3
Figure 1. KPCO Denver/Boulder Local Market immunization rates for two-year-old children in 1996, 1997, and 1998.
We focused ourefforts on tracking14-month and 20-
month-oldchildren. Wedistributed
monthly lists of alldelinquentchildren to
provider/nurseteams and createdexpectations for
return of these listssix weeks afterdistribution.
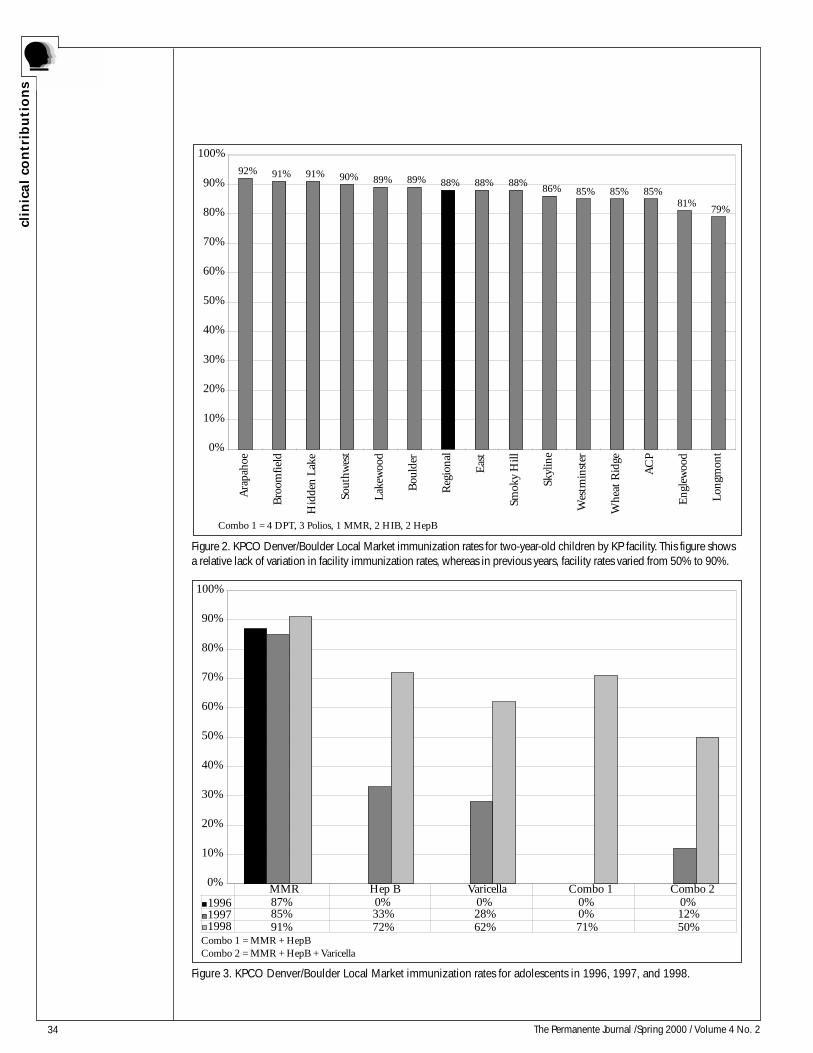
34 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
Combo 1 = 4 DPT, 3 Polios, 1 MMR, 2 HIB, 2 HepB
92% 91% 91% 90% 89% 89% 88% 88% 88%86% 85% 85% 85%
81%79%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Ara
paho
e
Bro
omfie
ld
Hid
den
Lake
Sout
hwes
t
Lake
woo
d
Bou
lder
Reg
iona
l
Eas
t
Smok
y H
ill
Skyl
ine
Wes
tmin
ster
Whe
at R
idge
AC
P
Eng
lew
ood
Long
mon
t
Combo 1 = MMR + HepBCombo 2 = MMR + HepB + Varicella
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1996 87% 0% 0% 0% 0%1997 85% 33% 28% 0% 12%1998 91% 72% 62% 71% 50%
MMR Hep B Varicella Combo 1 Combo 2
Figure 2. KPCO Denver/Boulder Local Market immunization rates for two-year-old children by KP facility. This figure showsa relative lack of variation in facility immunization rates, whereas in previous years, facility rates varied from 50% to 90%.
Figure 3. KPCO Denver/Boulder Local Market immunization rates for adolescents in 1996, 1997, and 1998.
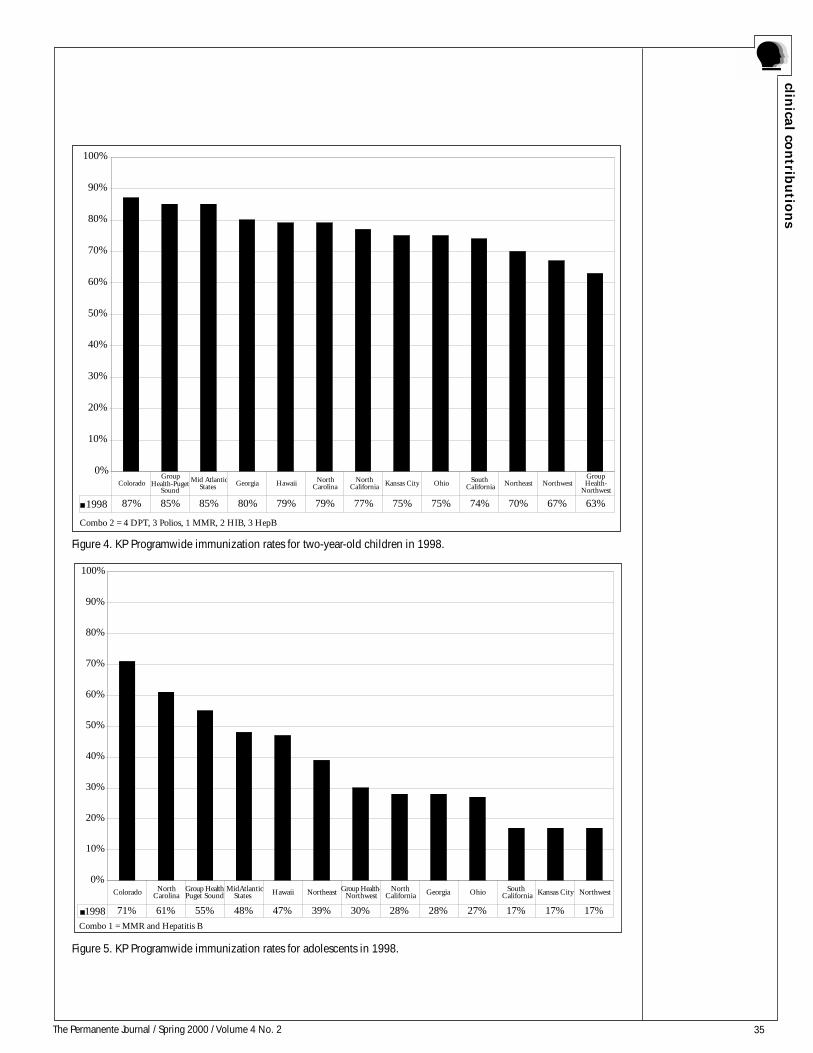
35The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
Combo 2 = 4 DPT, 3 Polios, 1 MMR, 2 HIB, 3 HepB
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1998 87% 85% 85% 80% 79% 79% 77% 75% 75% 74% 70% 67% 63%
ColoradoGroup
Health-PugetSound
Mid AtlanticStates Georgia Hawaii North
CarolinaNorth
California Kansas City Ohio South California Northeast Northwest
Group Health-
Northwest
Combo 1 = MMR and Hepatitis B
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1998 71% 61% 55% 48% 47% 39% 30% 28% 28% 27% 17% 17% 17%
Colorado North Carolina
Group Health-Puget Sound
MidAtlantic States Hawaii Northeast Group Health-
NorthwestNorth
California Georgia Ohio South California Kansas City Northwest
Figure 4. KP Programwide immunization rates for two-year-old children in 1998.
Figure 5. KP Programwide immunization rates for adolescents in 1998.

36 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
signed to provide current, accurate information andrecommendations for immunization of children. Themanual also serves as a reference for materials fromthe Advisory Committee on Immunization Practices(ACIP) and from the CDC and provides other criti-cal information such as Vaccine Information Sheetsand Adverse Events Reporting forms (AVERS). Post-ing the current immunization schedule in eachexamination room used for children is now a partof our primary care quality assurance measures. Fi-nally, the system provides a process for thereplacement of outdated schedules and vaccine in-formation, which allows us to keep current withpractices and protocols. The Immunization Tool Kitreceived rave reviews from staff and providers andcontinues to be used widely on a daily basis.
• Standard 15 – “Providers maintain up-to-date, eas-ily retrievable medical protocols at all locations wherevaccines are administered.”
4. Provide ongoing education to staff and physicians(CDC Standard 18). Specifically targeted educationand training was delivered to local facility teams andto large departments. In addition, specific feedbackwas given to individual providers when schedules werenot followed or when relative contraindications wereused instead of true contraindications. Through theabove tracking and auditing process, we were able toidentify local areas of concern (providers not follow-ing the proper schedule) as well as regional problems(eg, low Varivax compliance). We customized localteam education and feedback to the specific need whiledirecting our KP Regional interdepartmental educa-tion programs to the more global problem areas.
• Standard 18 –“Providers receive ongoingeducation and training on currentimmunization recommendations.”
Quantitative Analysis
Statistical analysis does not apply to this project.
ResultsThe result of these initiatives has been not only the
reversal of a declining trend but the achievement of ourhighest rate ever for diphtheria-tetanus-pertussis (DTP),polio, HIB, and hepatitis B vaccinations. In fact, for child-hood immunization rates, we surpassed our previoustarget and are in the top decile of all KP Regions.
CommentThe Healthy People 20004 national goal is to assure
that 90% of our children are fully immunized. Our
results support the evidence that when the CDC’s Stan-dards for Immunization Practice are implemented fully,such high coverage rates can be achieved. The objec-tive to improve our immunization rates was achievedby combining tools, skills, and education with account-ability to our Primary Care Quality Council.
This immunization program with intensive track-ing and outreach, coupled with our ImmunizationTool Kit as a vehicle for quality processes and com-munication, has been shared widely across thecountry. We have given Immunization Tool Kits anddiscussed the program with the KP Northwest, Ha-waii, Kansas City, and Colorado Springs Regions. Thestaff emphasizes the user-friendly, hands-on formatof the Tool Kit as a manual used daily in the clinicalsetting. We have also shared materials with manyorganizations outside KP. This proactive population-based program exemplifies the goals and valuesthroughout KP, and its “health state management”process can be transferred and adopted in many ven-ues as “disease state management” for our population.The project truly required a multidisciplinary approachbecause it was critical to have the physician/providerknowledge and expertise as well as diligent, detailedimplementation by the nursing staff.
ConclusionIn conclusion, even as vaccine technology contin-
ues to expand, we have a system in place to immunizeour children efficiently and accurately despite advancesand increasing complexity of the technology. Ourquality improvement process of measuring, analyzingthe data, formulating an improvement plan, imple-menting, and remeasuring can be generalized to anysuch problem. Any dedicated team with time, energy,and a clear, specific goal can be successful. The suc-cess of the Childhood/Adolescent ImmunizationProgram has been possible only through true owner-ship and commitment at all levels of the organizationand passion for the care of children. ❖
References1. National Immunization Program, Centers for Disease Controland Prevention. Standards for Pediatric ImmunizationPractices. Atlanta, GA: Center for Disease Control andPrevention; February 1996; Seventh Printing.2. Colorado State Department of Public Health and Environment.Guide to Contraindication in Childhood Vaccination. April 1996.3. Burchell MF, Sharp EA. Kaiser Permanente Medical CareProgram. Immunization Tool Kit. Denver, CO: Kaiser PermanenteMedical Care Program, Colorado Region; September 1999[available from the authors].4. National Center for Health Statistics. Healthy People 2000review, 1998-99. Hyattsville, MD: US Public Health Service; 1999.
The ImmunizationTool Kit receivedrave reviews fromstaff and providersand continues to
be used widely ona daily basis.
37The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
BackgroundA major challenge in health care today is to pro-
vide high-quality, cost-effective pharmaceutical carein a climate of skyrocketing prices (nationwide,spending for medications increased 84% from 1993through 1998). To help meet this challenge, KaiserPermanente Northwest (KPNW) in 1996 developed a
quality improvement project known as the ClinicalPharmacy Services Restructure, which in 1998 be-came the Medication Management Program (MMP)—acentrally managed model for population-based clini-cal pharmacy services that are integrated into thedelivery system. Onsite pharmacy staff and localhealth care teams collaborate to implement clinical
Achieving Positive Outcomes through Collaborative PharmaceuticalCare: The KPNW Medication Management Program
Table 1. Team members
Pharmacy Department: Rob Ashley, RPh, Pharmacist, MMP & Fisher's Landing MOB; Gene Boschee, RPh, Pharmacist, MMP &Beaverton MOB; Anne Bracy, Analyst; Donna Caldwell, MS, RPh, Pharmacist, Drug Information (DI); Jeanette Chardon, Education& Publications Specialist; Karen Carter, RPh, Pharmacy Improvement Program Team; Renee Christiansen, Pharmacy Technician,MMP; Sharon Cunningham, RPh, Pharmacist, Mt. Scott MOB; Marge Diment, RPh, Pharmacist-in-Charge, Vancouver Pharmacy;Diane Ditmer, PharmD, Pharmacist-in-Charge, DI; Jim Dunscomb, RPh, Supervisor, Sunnyside Pharmacy; Mike Eldredge, MS, RPh,Pharmacist, Optimal Renal; Suzanne Gauen, RPh, Pharmacist, Drug Information; Larry Gayton, RPh, Pharmacist, MMP & VancouverMOB; Cheryl Geisler, RPh, Pharmacist, MMP & Cascade Park MOB; Marie Grant, RPh, Pharmacist, MMP & Longview Kelso MOB;Michelle Hall, RPh, Pharmacist, MMP & Rockwood MOB; Ken Hansel, RPh, MMP & Salmon Creek MOB; Anita Hampton, RPh,Supervisor, North Lancaster Pharmacy; Mike Harding, RPh, Supervisor, Longview Kelso Pharmacy; Dave Heffner, RPh, Supervisor,Skyline Pharmacy; Kent Higginbotham, RPh, Supervisor, Division Pharmacy; Val Johnson, Pharmacy Benefits & KP Online; TriciaKahut, Communications & Database Specialist; Larry Klika, RPh, Pharmacist, MMP & Rockwood MOB; Dean Klopfenstein, RPh,CDE, Pharmacist-in-Charge, MMP; Mike Kinard, MS, RPh, Regional Pharmacy Manager; Evie Kralman, Pharmacy Secretary; StacyLandes, Pharmacy Benefits, Pharmacy Alert Services & KP Online; Jackie Larson, RPh, Pharmacy Improvement Program Team;Sally Logan, RPh, Pharmacist, MMP, & EpicCare (CIS) Liaison; Steve Logan, RPh, East Central Service Area Manager; CarolynLuettgerodt, RPh, Pharmacy Improvement Program Team; Norm Muilenburg, RPh, Pharmacist, Drug Information; LisaNakashimada, RPh, Pharmacist, MMP & Sunset MOB; Gary Nelson, RPh, Pharmacist, Division MOB; Terry Parsons, RPh,Pharmacist, Skyline MOB; Pat Perry, RPh, Pharmacist, MMP, and East Interstate MOB; Fred Powers, RPh, Acting Supervisor, SunsetPharmacy; Judy Ramage, Pharmacy Technician, MMP; Chris Ramsey, PharmD, Pharmacist, Longview Kelso MOB; Tanya Ramsey,PharmD, Pharmacist, MMP, & Longview Kelso MOB; Mike Regner, MS, RPh, Pharmacist, Drug Information; Kathryn Ring, RPh,Pharmacist, MMP, Sunset MOB & KP Online; Kati Rowe, RPh, Pharmacist, MMP & Sunnyside MOB; Cathy Sbur, PharmD,Supervisor, Salmon Creek Pharmacy; Cindy Sieck, PharmD, Pharmacist, MMP & Salmon Creek MOB; Sandra Teeny, RPh,Supervisor, Automated Refill Center; Theresa Terry, PharmD, Pharmacist, Rockwood MOB; LouAnn Thorsness, RPh, Pharmacist,MMP, & Pharmacy Alert Services; Don Tsukamaki, RPh, Pharmacist, MMP & Beaverton MOB; Bernie Walker, PharmD, Pharmacist,MMP, Rockwood MOB, & EpicCare (CIS) Liaison; Bob White, RPh, Pharmacist, MMP & Vancouver MOB; Ginny Wilborn, RPh,Westside and Salem Service Area Manager; Lisa Wilson, RPh, Supervisor, Rockwood Pharmacy; Tami Wilson, RPh, Supervisor,Cascade Park Pharmacy; Donna Wolfer, RPh, Pharmacist, MMP & Mt Scott MOB; Gary Woodson, RPh, Pharmacist, DI (retired);Tom Wright, RPh, Supervisor, MMP; Colette Yamaguchi, RPh, Clark & Longview Kelso Service Area ManagerContact Person: Nancy Louie Lee, MS, RPh, Clinical Pharmacy Services Manager
Northwest Permanente Medical Group: John Chen, MD, Service Area Director, Central PCSA, Member, Diabetes SteeringCommittee; Richard Dykstra, MD, Co-Chair, Senior & Disabled Care Committee; Harry Glauber, MD, Endocrinology, Member,Diabetes Steering Committee; Michael Herson, MD, Endocrinology, Member, Diabetes Steering Committee; Robin Lake, MD,Cardiology, Member, Cardiovascular Steering Committee; Jim Norris, MD, Chairman, Regional Formulary & TherapeuticsCommittee; Paul Wallace, MD, Chairman, Clinical Strategies Integration Group; Rick Wise, MD, Co-Chair, Cardiovascular SteeringCommittee; Maureen Wright, MD, Former Co-chair, Cardiovascular Steering Committee
KNPW Health Plan Operations: Sue Caulfield, RN, KSMC Director of Patient/Family Education, Member, Diabetes SteeringCommittee; John Crawford, Regional Health Education; Donna Forsberg, RN, Clinic Coordinator, Care Manager Strategy, Manager,Westside PCSA; Bill Hurst, Regional Call Center; Carla Johnson, MS, RN, Westside PCSA Manager, Co-chair, Cardiovascular SteeringCommittee; Connie Keyes, RN, MSN, Regional Nursing Consultant; Peggy McClure, MS, MBA, Manager, Health Systems & CallCenter, Co-chair, Diabetes Steering Committee; Ray Robertson, Director, Shared Services; Kate Scott, Regional Call Center;Kimberly Smith, Formerly: Analyst, Consulting & Analytical Services; Kati Traunweiser, Clinical Implementation Specialist; JanWeerts, RN, Implementation Specialist, Health Systems; Shirley Welch, PhD, Director of Chemistry, Regional Lab
Center for Health Research: Jonathan Brown, PhD, Co-chair, Diabetes Steering Committee; Lucy Nonnenkamp, MS, Co-chair,Senior & Disabled Care Committee
Northwest Region
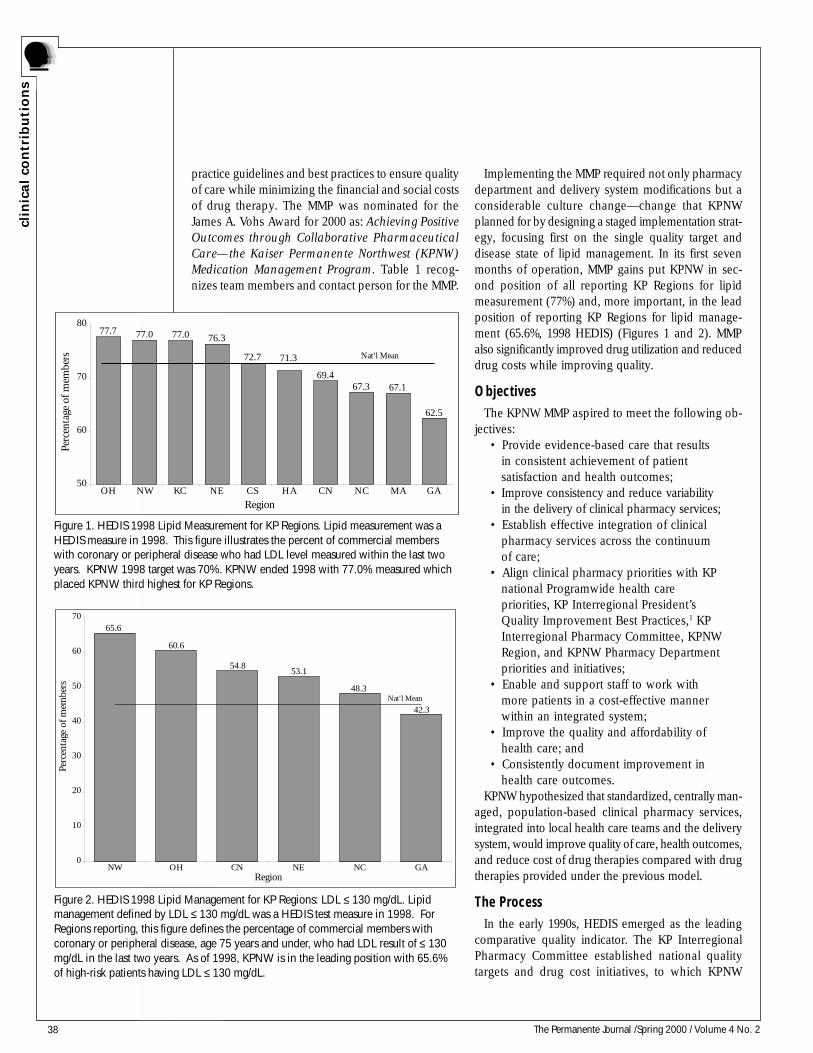
38 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
practice guidelines and best practices to ensure qualityof care while minimizing the financial and social costsof drug therapy. The MMP was nominated for theJames A. Vohs Award for 2000 as: Achieving PositiveOutcomes through Collaborative PharmaceuticalCare—the Kaiser Permanente Northwest (KPNW)Medication Management Program. Table 1 recog-nizes team members and contact person for the MMP.
Implementing the MMP required not only pharmacydepartment and delivery system modifications but aconsiderable culture change—change that KPNWplanned for by designing a staged implementation strat-egy, focusing first on the single quality target anddisease state of lipid management. In its first sevenmonths of operation, MMP gains put KPNW in sec-ond position of all reporting KP Regions for lipidmeasurement (77%) and, more important, in the leadposition of reporting KP Regions for lipid manage-ment (65.6%, 1998 HEDIS) (Figures 1 and 2). MMPalso significantly improved drug utilization and reduceddrug costs while improving quality.
ObjectivesThe KPNW MMP aspired to meet the following ob-
jectives:• Provide evidence-based care that results
in consistent achievement of patientsatisfaction and health outcomes;
• Improve consistency and reduce variabilityin the delivery of clinical pharmacy services;
• Establish effective integration of clinicalpharmacy services across the continuumof care;
• Align clinical pharmacy priorities with KPnational Programwide health carepriorities, KP Interregional President’sQuality Improvement Best Practices,1 KPInterregional Pharmacy Committee, KPNWRegion, and KPNW Pharmacy Departmentpriorities and initiatives;
• Enable and support staff to work withmore patients in a cost-effective mannerwithin an integrated system;
• Improve the quality and affordability ofhealth care; and
• Consistently document improvement inhealth care outcomes.
KPNW hypothesized that standardized, centrally man-aged, population-based clinical pharmacy services,integrated into local health care teams and the deliverysystem, would improve quality of care, health outcomes,and reduce cost of drug therapies compared with drugtherapies provided under the previous model.
The ProcessIn the early 1990s, HEDIS emerged as the leading
comparative quality indicator. The KP InterregionalPharmacy Committee established national qualitytargets and drug cost initiatives, to which KPNW
Figure 2. HEDIS 1998 Lipid Management for KP Regions: LDL ≤ 130 mg/dL. Lipidmanagement defined by LDL ≤ 130 mg/dL was a HEDIS test measure in 1998. ForRegions reporting, this figure defines the percentage of commercial members withcoronary or peripheral disease, age 75 years and under, who had LDL result of ≤ 130mg/dL in the last two years. As of 1998, KPNW is in the leading position with 65.6%of high-risk patients having LDL ≤ 130 mg/dL.
42.3
48.3
53.154.8
60.6
65.6
0
10
20
30
40
50
60
70
NW OH CN NE NC GA
Nat'l Mean
Region
Perc
enta
ge o
f mem
bers
Figure 1. HEDIS 1998 Lipid Measurement for KP Regions. Lipid measurement was aHEDIS measure in 1998. This figure illustrates the percent of commercial memberswith coronary or peripheral disease who had LDL level measured within the last twoyears. KPNW 1998 target was 70%. KPNW ended 1998 with 77.0% measured whichplaced KPNW third highest for KP Regions.
77.7 77.0 77.0 76.3
72.7
62.5
69.4
71.3
67.167.3
50
60
70
80
OH NW KC NE CS HA CN NC MA GA
Nat'l Mean
Region
Perc
enta
ge o
f mem
bers

39The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
committed. When the pressure to document the valueof clinical pharmacy services increased, the old model(where individual pharmacists set patient care prioritiesbased on daily requests for service) was not sufficient.KPNW’s historical model of providing clinical pharmacyservices was no longer viable. A new model ofpharmaceutical care delivery was needed—anintegrated, population-based model that would supportKPNW’s health outcome goals, HEDIS and other qualitygoals, achieve drug cost initiatives, and provide datato demonstrate the effectiveness and value of clinicalpharmacy services. The process to develop integrated,cost-effective clinical pharmacy services was drivenby a shared vision to support physicians and healthcare teams to improve health care outcomes.
In 1996, the KPNW Regional Pharmacy Departmentinitiated a quality improvement project to: 1) evaluateclinical pharmacy service delivery models inside andoutside of KP, 2) evaluate the strengths and weaknesses
of the current ‘reactive’ process of providing clinicalpharmacy services, and 3) identify quality attributes andservice features critical to a new model for the deliveryof pharmaceutical care. Although no single best modelemerged, the Pharmacy Department, in collaborationwith Northwest Permanente physicians, Health Plan,and KPNW clinical committees, used the identified bestpractices to design the population-based MMP model.The Northwest Permanente physicians involved in theprocess were instrumental in soliciting support fromfellow physicians, without whom MMP would not havebeen a success. Cardiovascular Steering Committee lead-ers helped to hone the focus for the initial stage of theimplementation plan to an emphasis on high-risk, sec-ondary-prevention patients. Other KPNW clinicalcommittees continue to help focus priorities and shapethe MMP program in vital, ongoing ways.
Eight key best practices emerged for the new MMPmodel:
Table 2. 1998-1999 Pharmacy MMP Cumulative Priorities
Initiated Priorities Responsibility shared by
2Q98 Quality: Lipid Measurement and Management
Regional Formulary & TherapeuticsCommittee (RFTC), Cardiovascular SteeringCommittee (CVSC), Clinical StrategiesIntegration Group (CSIG), HEDIS
4Q98 Gastrointestinal Drug Therapy RFTC, Interregional Pharmacy (IRP)
4Q98 Lipid Drug Therapy RFTC, IRP, CVSC
4Q98 Anticoagulation Conversion RFTC, IRP
4Q98 Pilot Glycemic ControlRFTC, Diabetes Mellitus SteeringCommittee (DMSC)
4Q98 Pilot Eldercare High-Risk Drug Therapy Senior & Disabled Care Committee, CSIG
1Q99 Aspirin Documentation RFTC, CVSC
1Q99 Allergy Drug Therapy RFTC, IRP
1Q99 Plan Multidisciplinary Model Westside Leadership
1Q99 ACE-Inhibitor Drug Therapy RFTC, IRP, CVSC
3Q99 Aspirin Initiation RFTC, CVSC
3Q99 Quality: Glycemic Control RFTC, DMSC
3Q99 Implementation of Multidisciplinary Model Westside Leadership
3Q99 Plan for expansion of Multidisciplinary Model Clark County Leadership
3Q99 Plan Asthma & Depression Drug TherapyRFTC, Asthma Steering Committee,Depression Steering Committee
The process todevelop integrated,
cost-effectiveclinical pharmacy
services was drivenby a shared vision
to supportphysicians and
health care teamsto improve healthcare outcomes.
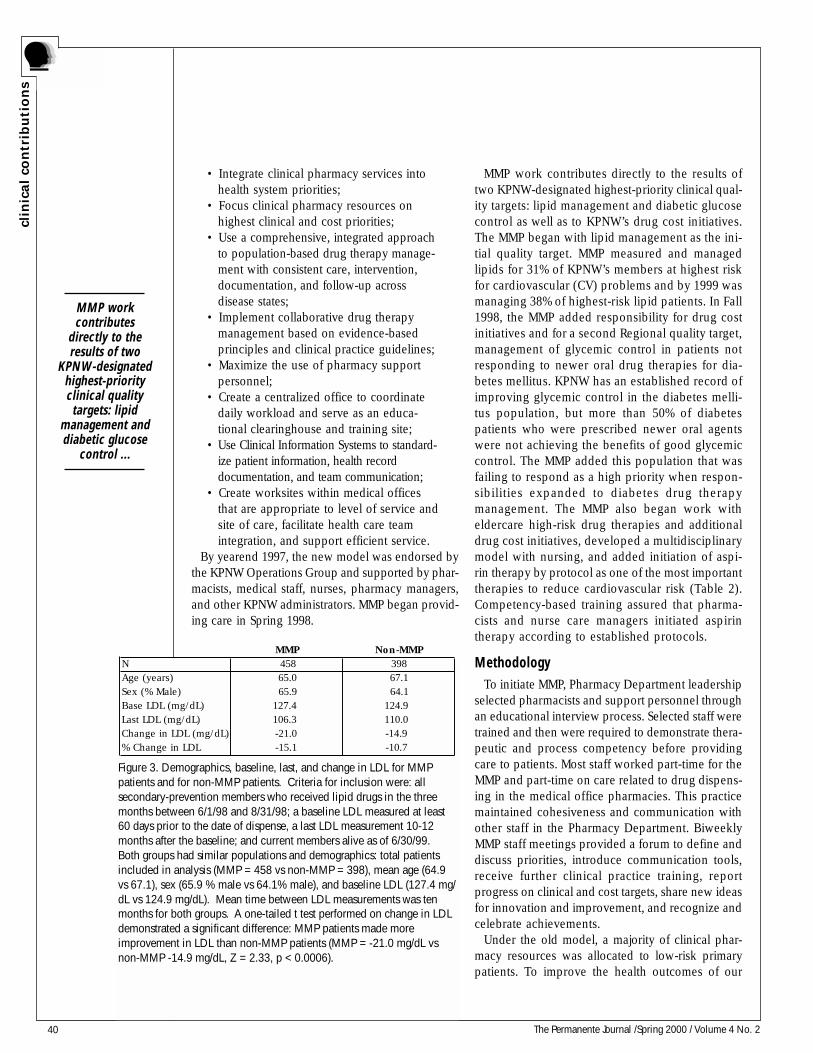
40 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
• Integrate clinical pharmacy services intohealth system priorities;
• Focus clinical pharmacy resources onhighest clinical and cost priorities;
• Use a comprehensive, integrated approachto population-based drug therapy manage-ment with consistent care, intervention,documentation, and follow-up acrossdisease states;
• Implement collaborative drug therapymanagement based on evidence-basedprinciples and clinical practice guidelines;
• Maximize the use of pharmacy supportpersonnel;
• Create a centralized office to coordinatedaily workload and serve as an educa-tional clearinghouse and training site;
• Use Clinical Information Systems to standard-ize patient information, health recorddocumentation, and team communication;
• Create worksites within medical officesthat are appropriate to level of service andsite of care, facilitate health care teamintegration, and support efficient service.
By yearend 1997, the new model was endorsed bythe KPNW Operations Group and supported by phar-macists, medical staff, nurses, pharmacy managers,and other KPNW administrators. MMP began provid-ing care in Spring 1998.
MMP work contributes directly to the results oftwo KPNW-designated highest-priority clinical qual-ity targets: lipid management and diabetic glucosecontrol as well as to KPNW’s drug cost initiatives.The MMP began with lipid management as the ini-tial quality target. MMP measured and managedlipids for 31% of KPNW’s members at highest riskfor cardiovascular (CV) problems and by 1999 wasmanaging 38% of highest-risk lipid patients. In Fall1998, the MMP added responsibility for drug costinitiatives and for a second Regional quality target,management of glycemic control in patients notresponding to newer oral drug therapies for dia-betes mellitus. KPNW has an established record ofimproving glycemic control in the diabetes melli-tus population, but more than 50% of diabetespatients who were prescribed newer oral agentswere not achieving the benefits of good glycemiccontrol. The MMP added this population that wasfailing to respond as a high priority when respon-sibilities expanded to diabetes drug therapymanagement. The MMP also began work witheldercare high-risk drug therapies and additionaldrug cost initiatives, developed a multidisciplinarymodel with nursing, and added initiation of aspi-rin therapy by protocol as one of the most importanttherapies to reduce cardiovascular risk (Table 2).Competency-based training assured that pharma-cists and nurse care managers initiated aspirintherapy according to established protocols.
MethodologyTo initiate MMP, Pharmacy Department leadership
selected pharmacists and support personnel throughan educational interview process. Selected staff weretrained and then were required to demonstrate thera-peutic and process competency before providingcare to patients. Most staff worked part-time for theMMP and part-time on care related to drug dispens-ing in the medical office pharmacies. This practicemaintained cohesiveness and communication withother staff in the Pharmacy Department. BiweeklyMMP staff meetings provided a forum to define anddiscuss priorities, introduce communication tools,receive further clinical practice training, reportprogress on clinical and cost targets, share new ideasfor innovation and improvement, and recognize andcelebrate achievements.
Under the old model, a majority of clinical phar-macy resources was allocated to low-risk primarypatients. To improve the health outcomes of our
Figure 3. Demographics, baseline, last, and change in LDL for MMPpatients and for non-MMP patients. Criteria for inclusion were: allsecondary-prevention members who received lipid drugs in the threemonths between 6/1/98 and 8/31/98; a baseline LDL measured at least60 days prior to the date of dispense, a last LDL measurement 10-12months after the baseline; and current members alive as of 6/30/99.Both groups had similar populations and demographics: total patientsincluded in analysis (MMP = 458 vs non-MMP = 398), mean age (64.9vs 67.1), sex (65.9 % male vs 64.1% male), and baseline LDL (127.4 mg/dL vs 124.9 mg/dL). Mean time between LDL measurements was tenmonths for both groups. A one-tailed t test performed on change in LDLdemonstrated a significant difference: MMP patients made moreimprovement in LDL than non-MMP patients (MMP = -21.0 mg/dL vsnon-MMP -14.9 mg/dL, Z = 2.33, p < 0.0006).
MMP Non-MMPN 458 398Age (years) 65.0 67.1Sex (% Male) 65.9 64.1Base LDL (mg/dL) 127.4 124.9 Last LDL (mg/dL) 106.3 110.0 Change in LDL (mg/dL) -21.0 -14.9 % Change in LDL -15.1 -10.7
MMP workcontributes
directly to theresults of two
KPNW-designatedhighest-priorityclinical qualitytargets: lipid
management anddiabetic glucose
control ...
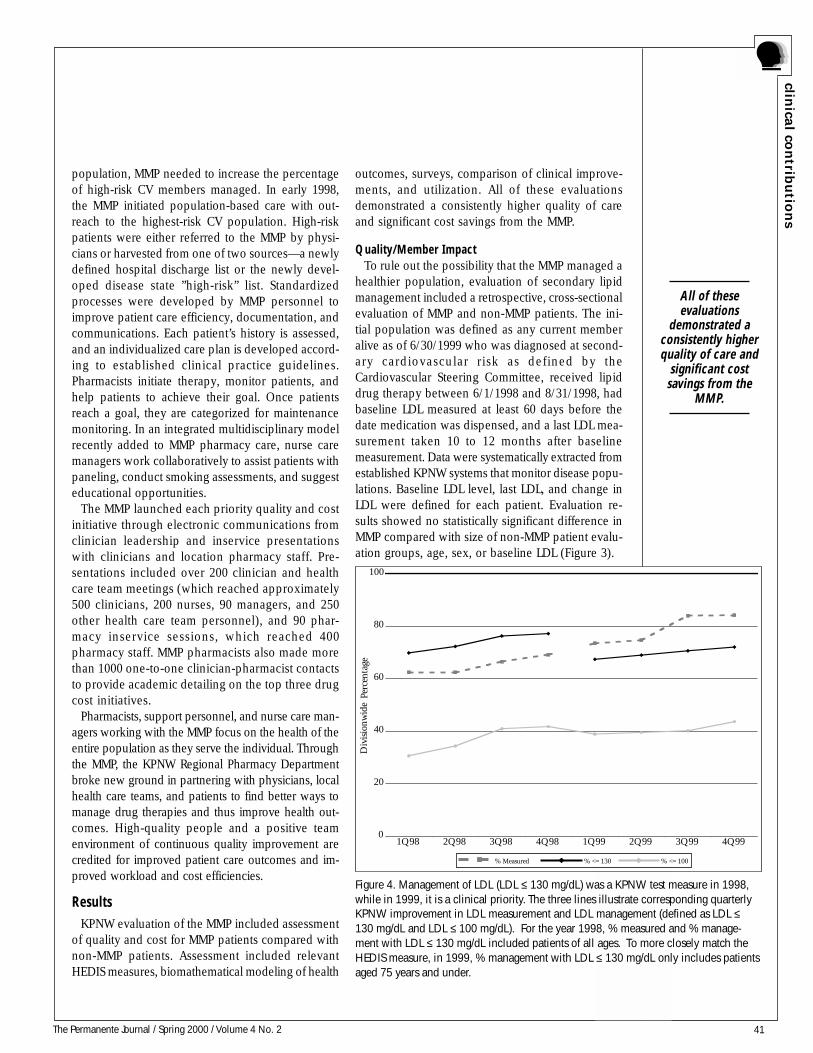
41The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
population, MMP needed to increase the percentageof high-risk CV members managed. In early 1998,the MMP initiated population-based care with out-reach to the highest-risk CV population. High-riskpatients were either referred to the MMP by physi-cians or harvested from one of two sources—a newlydefined hospital discharge list or the newly devel-oped disease state ”high-risk” list. Standardizedprocesses were developed by MMP personnel toimprove patient care efficiency, documentation, andcommunications. Each patient’s history is assessed,and an individualized care plan is developed accord-ing to established clinical practice guidelines.Pharmacists initiate therapy, monitor patients, andhelp patients to achieve their goal. Once patientsreach a goal, they are categorized for maintenancemonitoring. In an integrated multidisciplinary modelrecently added to MMP pharmacy care, nurse caremanagers work collaboratively to assist patients withpaneling, conduct smoking assessments, and suggesteducational opportunities.
The MMP launched each priority quality and costinitiative through electronic communications fromclinician leadership and inservice presentationswith clinicians and location pharmacy staff. Pre-sentations included over 200 clinician and healthcare team meetings (which reached approximately500 clinicians, 200 nurses, 90 managers, and 250other health care team personnel), and 90 phar-macy inservice sessions, which reached 400pharmacy staff. MMP pharmacists also made morethan 1000 one-to-one clinician-pharmacist contactsto provide academic detailing on the top three drugcost initiatives.
Pharmacists, support personnel, and nurse care man-agers working with the MMP focus on the health of theentire population as they serve the individual. Throughthe MMP, the KPNW Regional Pharmacy Departmentbroke new ground in partnering with physicians, localhealth care teams, and patients to find better ways tomanage drug therapies and thus improve health out-comes. High-quality people and a positive teamenvironment of continuous quality improvement arecredited for improved patient care outcomes and im-proved workload and cost efficiencies.
ResultsKPNW evaluation of the MMP included assessment
of quality and cost for MMP patients compared withnon-MMP patients. Assessment included relevantHEDIS measures, biomathematical modeling of health
outcomes, surveys, comparison of clinical improve-ments, and utilization. All of these evaluationsdemonstrated a consistently higher quality of careand significant cost savings from the MMP.
Quality/Member ImpactTo rule out the possibility that the MMP managed a
healthier population, evaluation of secondary lipidmanagement included a retrospective, cross-sectionalevaluation of MMP and non-MMP patients. The ini-tial population was defined as any current memberalive as of 6/30/1999 who was diagnosed at second-ary cardiovascular risk as defined by theCardiovascular Steering Committee, received lipiddrug therapy between 6/1/1998 and 8/31/1998, hadbaseline LDL measured at least 60 days before thedate medication was dispensed, and a last LDL mea-surement taken 10 to 12 months after baselinemeasurement. Data were systematically extracted fromestablished KPNW systems that monitor disease popu-lations. Baseline LDL level, last LDL, and change inLDL were defined for each patient. Evaluation re-sults showed no statistically significant difference inMMP compared with size of non-MMP patient evalu-ation groups, age, sex, or baseline LDL (Figure 3).
Figure 4. Management of LDL (LDL ≤ 130 mg/dL) was a KPNW test measure in 1998,while in 1999, it is a clinical priority. The three lines illustrate corresponding quarterlyKPNW improvement in LDL measurement and LDL management (defined as LDL ≤130 mg/dL and LDL ≤ 100 mg/dL). For the year 1998, % measured and % manage-ment with LDL ≤ 130 mg/dL included patients of all ages. To more closely match theHEDIS measure, in 1999, % management with LDL ≤ 130 mg/dL only includes patientsaged 75 years and under.
0
20
40
60
80
100
1Q98 2Q98 3Q98 4Q98 1Q99 2Q99 3Q99 4Q99
Div
isio
nwid
e Pe
rcen
tage
% Measured % <= 130 % <= 100
All of theseevaluations
demonstrated aconsistently higherquality of care and
significant costsavings from the
MMP.
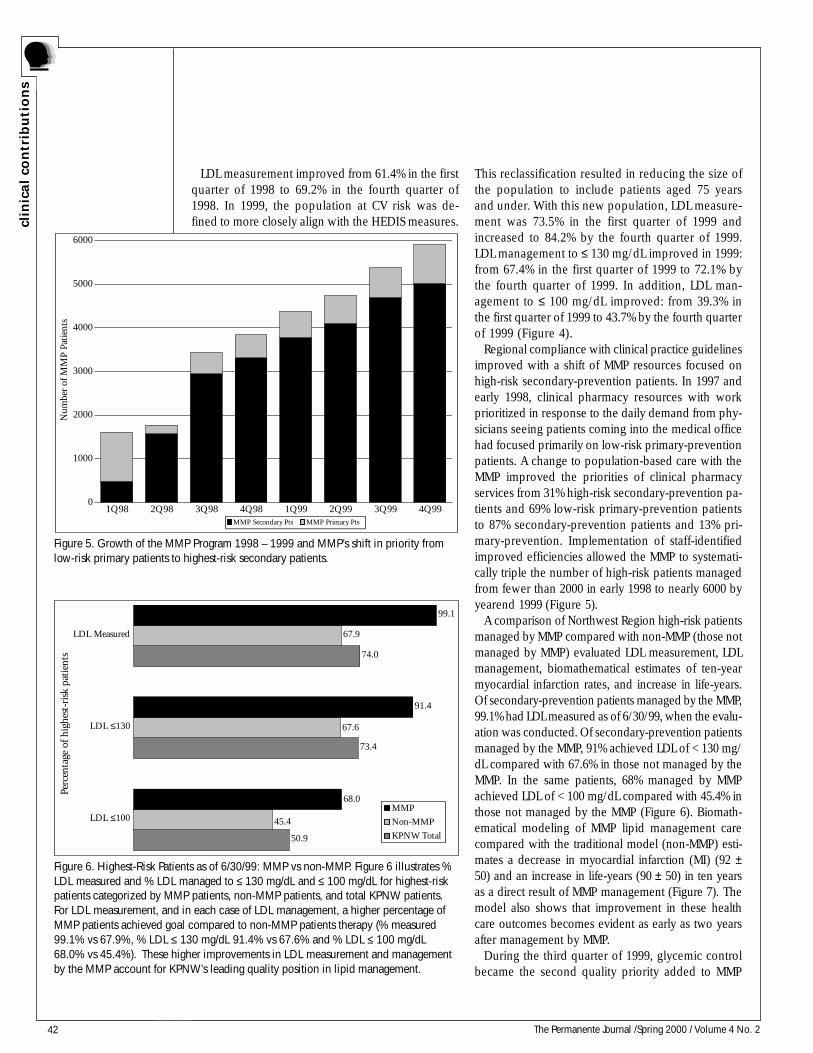
42 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
LDL measurement improved from 61.4% in the firstquarter of 1998 to 69.2% in the fourth quarter of1998. In 1999, the population at CV risk was de-fined to more closely align with the HEDIS measures.
This reclassification resulted in reducing the size ofthe population to include patients aged 75 yearsand under. With this new population, LDL measure-ment was 73.5% in the first quarter of 1999 andincreased to 84.2% by the fourth quarter of 1999.LDL management to ≤ 130 mg/dL improved in 1999:from 67.4% in the first quarter of 1999 to 72.1% bythe fourth quarter of 1999. In addition, LDL man-agement to ≤ 100 mg/dL improved: from 39.3% inthe first quarter of 1999 to 43.7% by the fourth quarterof 1999 (Figure 4).
Regional compliance with clinical practice guidelinesimproved with a shift of MMP resources focused onhigh-risk secondary-prevention patients. In 1997 andearly 1998, clinical pharmacy resources with workprioritized in response to the daily demand from phy-sicians seeing patients coming into the medical officehad focused primarily on low-risk primary-preventionpatients. A change to population-based care with theMMP improved the priorities of clinical pharmacyservices from 31% high-risk secondary-prevention pa-tients and 69% low-risk primary-prevention patientsto 87% secondary-prevention patients and 13% pri-mary-prevention. Implementation of staff-identifiedimproved efficiencies allowed the MMP to systemati-cally triple the number of high-risk patients managedfrom fewer than 2000 in early 1998 to nearly 6000 byyearend 1999 (Figure 5).
A comparison of Northwest Region high-risk patientsmanaged by MMP compared with non-MMP (those notmanaged by MMP) evaluated LDL measurement, LDLmanagement, biomathematical estimates of ten-yearmyocardial infarction rates, and increase in life-years.Of secondary-prevention patients managed by the MMP,99.1% had LDL measured as of 6/30/99, when the evalu-ation was conducted. Of secondary-prevention patientsmanaged by the MMP, 91% achieved LDL of < 130 mg/dL compared with 67.6% in those not managed by theMMP. In the same patients, 68% managed by MMPachieved LDL of < 100 mg/dL compared with 45.4% inthose not managed by the MMP (Figure 6). Biomath-ematical modeling of MMP lipid management carecompared with the traditional model (non-MMP) esti-mates a decrease in myocardial infarction (MI) (92 ±50) and an increase in life-years (90 ± 50) in ten yearsas a direct result of MMP management (Figure 7). Themodel also shows that improvement in these healthcare outcomes becomes evident as early as two yearsafter management by MMP.
During the third quarter of 1999, glycemic controlbecame the second quality priority added to MMP
Figure 6. Highest-Risk Patients as of 6/30/99: MMP vs non-MMP. Figure 6 illustrates %LDL measured and % LDL managed to ≤ 130 mg/dL and ≤ 100 mg/dL for highest-riskpatients categorized by MMP patients, non-MMP patients, and total KPNW patients.For LDL measurement, and in each case of LDL management, a higher percentage ofMMP patients achieved goal compared to non-MMP patients therapy (% measured99.1% vs 67.9%, % LDL ≤ 130 mg/dL 91.4% vs 67.6% and % LDL ≤ 100 mg/dL68.0% vs 45.4%). These higher improvements in LDL measurement and managementby the MMP account for KPNW’s leading quality position in lipid management.
50.9
73.4
74.0
67.6
67.9
68.0
91.4
99.1
45.4LDL ≤100
LDL ≤130
LDL Measured
MMP
Non-MMP
KPNW Total
Perc
enta
ge o
f hig
hest
-ris
k pa
tien
ts
Figure 5. Growth of the MMP Program 1998 – 1999 and MMP’s shift in priority fromlow-risk primary patients to highest-risk secondary patients.
0
1000
2000
3000
4000
5000
6000
1Q98 2Q98 3Q98 4Q98 1Q99 2Q99 3Q99 4Q99
Num
ber
of M
MP
Pati
ents
MMP Secondary Pts MMP Primary Pts
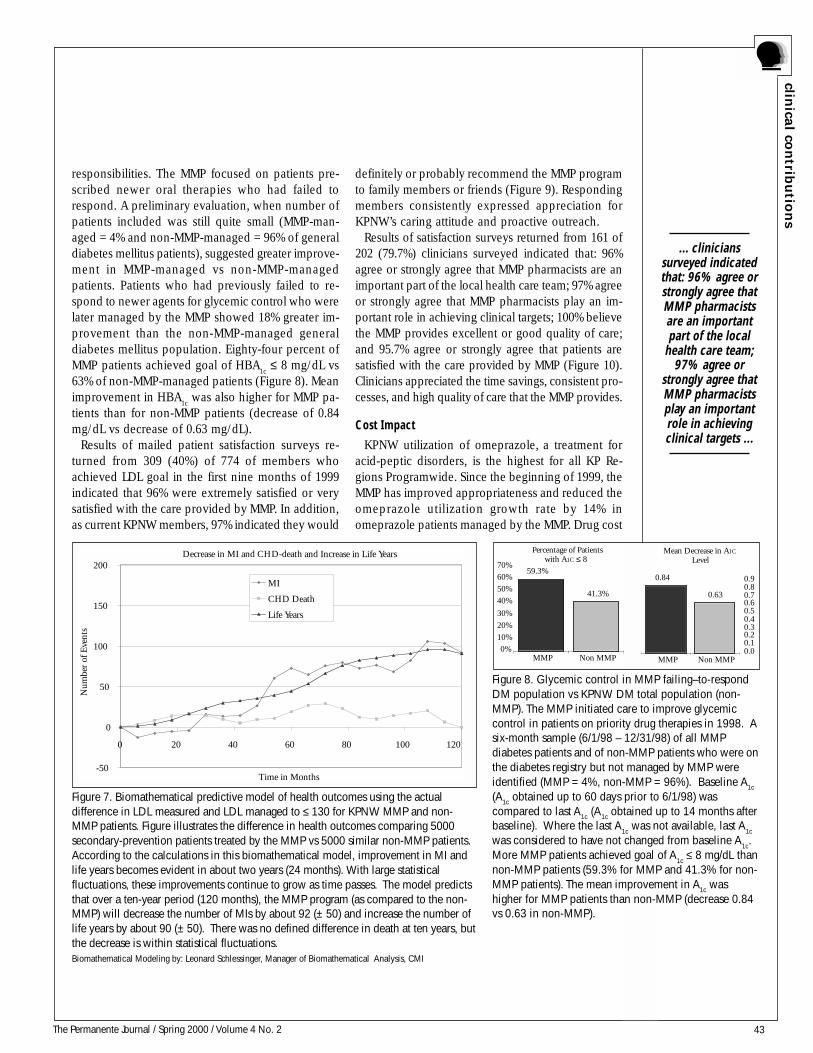
43The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
responsibilities. The MMP focused on patients pre-scribed newer oral therapies who had failed torespond. A preliminary evaluation, when number ofpatients included was still quite small (MMP-man-aged = 4% and non-MMP-managed = 96% of generaldiabetes mellitus patients), suggested greater improve-ment in MMP-managed vs non-MMP-managedpatients. Patients who had previously failed to re-spond to newer agents for glycemic control who werelater managed by the MMP showed 18% greater im-provement than the non-MMP-managed generaldiabetes mellitus population. Eighty-four percent ofMMP patients achieved goal of HBA
1c ≤ 8 mg/dL vs
63% of non-MMP-managed patients (Figure 8). Meanimprovement in HBA
1c was also higher for MMP pa-
tients than for non-MMP patients (decrease of 0.84mg/dL vs decrease of 0.63 mg/dL).
Results of mailed patient satisfaction surveys re-turned from 309 (40%) of 774 of members whoachieved LDL goal in the first nine months of 1999indicated that 96% were extremely satisfied or verysatisfied with the care provided by MMP. In addition,as current KPNW members, 97% indicated they would
Decrease in MI and CHD-death and Increase in Life Years
-50
0
50
100
150
200
0 20 40 60 80 100 120
Time in Months
Num
ber
of E
vent
s
MI
CHD Death
Life Years
Figure 7. Biomathematical predictive model of health outcomes using the actualdifference in LDL measured and LDL managed to ≤ 130 for KPNW MMP and non-MMP patients. Figure illustrates the difference in health outcomes comparing 5000secondary-prevention patients treated by the MMP vs 5000 similar non-MMP patients.According to the calculations in this biomathematical model, improvement in MI andlife years becomes evident in about two years (24 months). With large statisticalfluctuations, these improvements continue to grow as time passes. The model predictsthat over a ten-year period (120 months), the MMP program (as compared to the non-MMP) will decrease the number of MIs by about 92 (± 50) and increase the number oflife years by about 90 (± 50). There was no defined difference in death at ten years, butthe decrease is within statistical fluctuations.Biomathematical Modeling by: Leonard Schlessinger, Manager of Biomathematical Analysis, CMI
definitely or probably recommend the MMP programto family members or friends (Figure 9). Respondingmembers consistently expressed appreciation forKPNW’s caring attitude and proactive outreach.
Results of satisfaction surveys returned from 161 of202 (79.7%) clinicians surveyed indicated that: 96%agree or strongly agree that MMP pharmacists are animportant part of the local health care team; 97% agreeor strongly agree that MMP pharmacists play an im-portant role in achieving clinical targets; 100% believethe MMP provides excellent or good quality of care;and 95.7% agree or strongly agree that patients aresatisfied with the care provided by MMP (Figure 10).Clinicians appreciated the time savings, consistent pro-cesses, and high quality of care that the MMP provides.
Cost Impact
KPNW utilization of omeprazole, a treatment foracid-peptic disorders, is the highest for all KP Re-gions Programwide. Since the beginning of 1999, theMMP has improved appropriateness and reduced theomeprazole utilization growth rate by 14% inomeprazole patients managed by the MMP. Drug cost
41.3%
59.3%
0%
10%
20%
30%
40%
50%
60%
70%
MMP Non MMP
Percentage of Patientswith A1C ≤ 8
Mean Decrease in A1C
Level
0.84
0.63
0.00.10.20.30.40.50.60.70.80.9
MMP Non MMP
Figure 8. Glycemic control in MMP failing–to-respondDM population vs KPNW DM total population (non-MMP). The MMP initiated care to improve glycemiccontrol in patients on priority drug therapies in 1998. Asix-month sample (6/1/98 – 12/31/98) of all MMPdiabetes patients and of non-MMP patients who were onthe diabetes registry but not managed by MMP wereidentified (MMP = 4%, non-MMP = 96%). Baseline A1c
(A1c obtained up to 60 days prior to 6/1/98) wascompared to last A1c (A1c obtained up to 14 months afterbaseline). Where the last A
1c was not available, last A
1c
was considered to have not changed from baseline A1c
.More MMP patients achieved goal of A
1c ≤ 8 mg/dL than
non-MMP patients (59.3% for MMP and 41.3% for non-MMP patients). The mean improvement in A1c washigher for MMP patients than non-MMP (decrease 0.84vs 0.63 in non-MMP).
... clinicianssurveyed indicatedthat: 96% agree orstrongly agree thatMMP pharmacistsare an importantpart of the local
health care team;97% agree or
strongly agree thatMMP pharmacistsplay an importantrole in achievingclinical targets ...
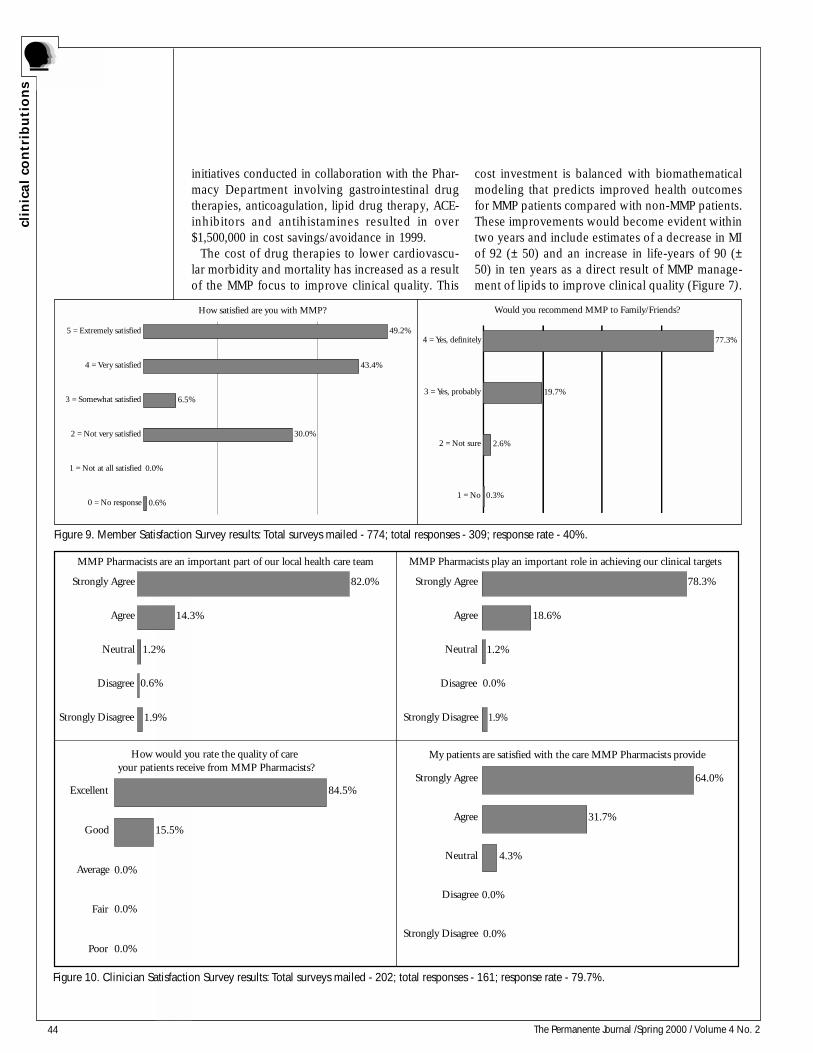
44 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
initiatives conducted in collaboration with the Phar-macy Department involving gastrointestinal drugtherapies, anticoagulation, lipid drug therapy, ACE-inhibitors and antihistamines resulted in over$1,500,000 in cost savings/avoidance in 1999.
The cost of drug therapies to lower cardiovascu-lar morbidity and mortality has increased as a resultof the MMP focus to improve clinical quality. This
cost investment is balanced with biomathematicalmodeling that predicts improved health outcomesfor MMP patients compared with non-MMP patients.These improvements would become evident withintwo years and include estimates of a decrease in MIof 92 (± 50) and an increase in life-years of 90 (±50) in ten years as a direct result of MMP manage-ment of lipids to improve clinical quality (Figure 7).
How satisfied are you with MMP?
49.2%
43.4%
30.0%
0.0%
0.6%
6.5%
5 = Extremely satisfied
4 = Very satisfied
3 = Somewhat satisfied
2 = Not very satisfied
1 = Not at all satisfied
0 = No response
Would you recommend MMP to Family/Friends?
77.3%
19.7%
2.6%
0.3%
4 = Yes, definitely
3 = Yes, probably
2 = Not sure
1 = No
Figure 9. Member Satisfaction Survey results: Total surveys mailed - 774; total responses - 309; response rate - 40%.
1.9%
1.2%
14.3%
82.0%
Strongly Disagree
Disagree
Neutral
Agree
Strongly Agree
MMP Pharmacists are an important part of our local health care team
0.6%
1.9%
1.2%
18.6%
78.3%
Strongly Disagree
Disagree
Neutral
Agree
Strongly Agree
MMP Pharmacists play an important role in achieving our clinical targets
0.0%
How would you rate the quality of care your patients receive from MMP Pharmacists?
15.5%
84.5%
Poor
Fair
Average
Good
Excellent
0.0%
0.0%
0.0%
My patients are satisfied with the care MMP Pharmacists provide
4.3%
31.7%
64.0%
Strongly Disagree
Disagree
Neutral
Agree
Strongly Agree
0.0%
0.0%
Figure 10. Clinician Satisfaction Survey results: Total surveys mailed - 202; total responses - 161; response rate - 79.7%.
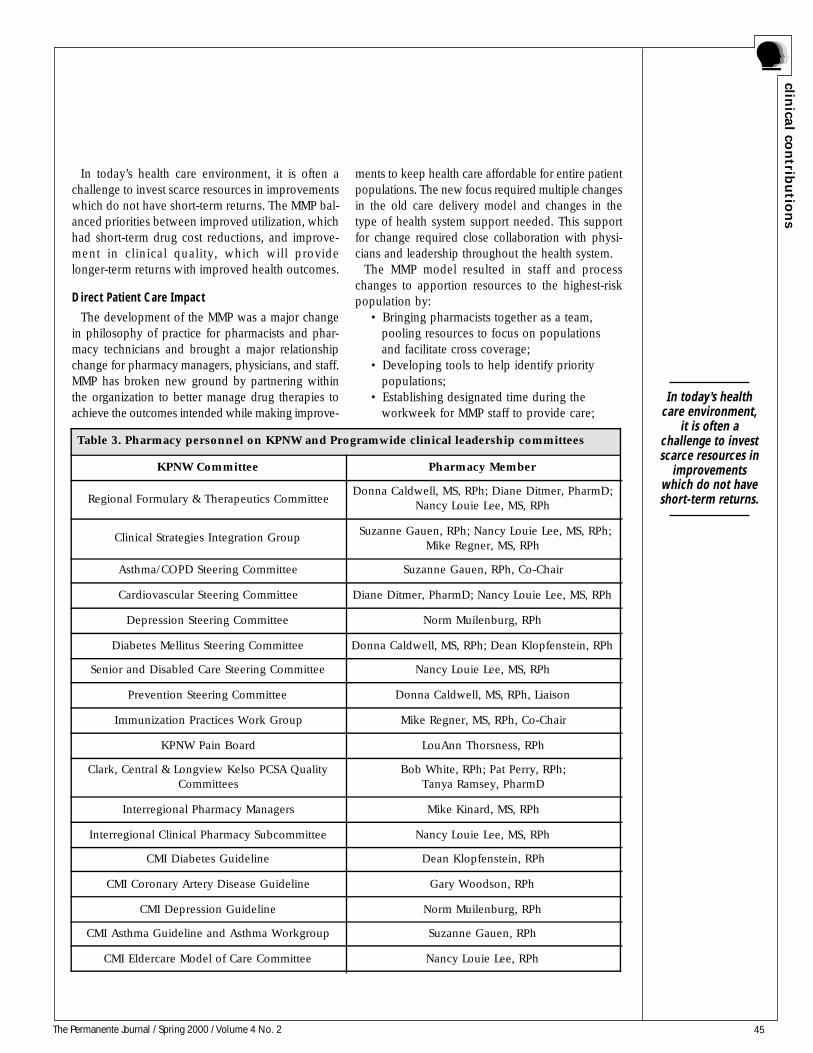
45The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
In today’s health care environment, it is often achallenge to invest scarce resources in improvementswhich do not have short-term returns. The MMP bal-anced priorities between improved utilization, whichhad short-term drug cost reductions, and improve-ment in clinical quality, which will providelonger-term returns with improved health outcomes.
Direct Patient Care Impact
The development of the MMP was a major changein philosophy of practice for pharmacists and phar-macy technicians and brought a major relationshipchange for pharmacy managers, physicians, and staff.MMP has broken new ground by partnering withinthe organization to better manage drug therapies toachieve the outcomes intended while making improve-
ments to keep health care affordable for entire patientpopulations. The new focus required multiple changesin the old care delivery model and changes in thetype of health system support needed. This supportfor change required close collaboration with physi-cians and leadership throughout the health system.
The MMP model resulted in staff and processchanges to apportion resources to the highest-riskpopulation by:
• Bringing pharmacists together as a team,pooling resources to focus on populationsand facilitate cross coverage;
• Developing tools to help identify prioritypopulations;
• Establishing designated time during theworkweek for MMP staff to provide care;
Table 3. Pharmacy personnel on KPNW and Programwide clinical leadership committees
KPNW Committee Pharmacy Member
Regional Formulary & Therapeutics CommitteeDonna Caldwell, MS, RPh; Diane Ditmer, PharmD;
Nancy Louie Lee, MS, RPh
Clinical Strategies Integration Group Suzanne Gauen, RPh; Nancy Louie Lee, MS, RPh;
Mike Regner, MS, RPh
Asthma/COPD Steering Committee Suzanne Gauen, RPh, Co-Chair
Cardiovascular Steering Committee Diane Ditmer, PharmD; Nancy Louie Lee, MS, RPh
Depression Steering Committee Norm Muilenburg, RPh
Diabetes Mellitus Steering Committee Donna Caldwell, MS, RPh; Dean Klopfenstein, RPh
Senior and Disabled Care Steering Committee Nancy Louie Lee, MS, RPh
Prevention Steering Committee Donna Caldwell, MS, RPh, Liaison
Immunization Practices Work Group Mike Regner, MS, RPh, Co-Chair
KPNW Pain Board LouAnn Thorsness, RPh
Clark, Central & Longview Kelso PCSA QualityCommittees
Bob White, RPh; Pat Perry, RPh;Tanya Ramsey, PharmD
Interregional Pharmacy Managers Mike Kinard, MS, RPh
Interregional Clinical Pharmacy Subcommittee Nancy Louie Lee, MS, RPh
CMI Diabetes Guideline Dean Klopfenstein, RPh
CMI Coronary Artery Disease Guideline Gary Woodson, RPh
CMI Depression Guideline Norm Muilenburg, RPh
CMI Asthma Guideline and Asthma Workgroup Suzanne Gauen, RPh
CMI Eldercare Model of Care Committee Nancy Louie Lee, RPh
In today’s healthcare environment,
it is often achallenge to investscarce resources in
improvementswhich do not haveshort-term returns.

46 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
• Defining patient-specific criteria to acceptreferrals into the program;
• Developing one centralized and multiplemedical office worksites to supportdelivery of appropriate levels of care;
• Standardizing patient care and documen-tation processes to support personnelefficiency and utilize the Clinical Informa-tion System in providing care;
• Creating a positive team environment ofcontinuous quality improvement.
In addition, the MMP enhanced the services pro-vided to patients by:
• Developing a cardiovascular risk list withthe Cardiovascular Steering Committee;
• Working with clinical leadership commit-tees to define priorities for MMP;
• Collaborating with the Regional Labora-tory to streamline ordering of directlymeasured LDL tests;
• Working with the Regional Call Center toschedule group appointments;
• Collaborating with Regional HealthEducation and using lifestyle modificationprograms and materials;
• Integrating pharmacist chronic diseasemedication management with chronicdisease nurse care managers.
Patients are highly satisfied with the proactive com-munication and ongoing availability of MMP staff toanswer questions via local and toll-free telephonenumbers. Patients understand that a team of expertsmanages their care, individualized to their specificdrug therapy needs, in collaboration with their clini-cians. Patients appreciate the positive recognition theyreceive when they achieve their therapeutic goalsand are comforted that the MMP continues to stay incontact through maintenance follow-up (Figure 9).
Innovation/Leadership
The key to successful implementation of centrallymanaged clinical pharmacy services is integrationacross the continuum of care within a health caresystem; this includes integration with local health careteams and participation in decisions about the clini-cal care of the populations. Local integration buildsand maintains relationships between pharmacy staffand medical office health care team members. KPNWestablished MMP worksites in each medical office,where MMP staff provide care as part of the localhealth care team. MMP staff may work in the central
MMP office and rotate shifts for telephone follow-upand member calls. Pharmacy Department and MMPstaff take an active role in leadership roles on com-mittees and at department meetings (Table 3) andprovide updates and education, participate in devel-opment of clinical practice guidelines, and lead healthcare team discussions on defining clinical targets. Thisrelationship facilitates integration of MMP work pri-orities with KP national, Regional, and departmentalpriorities (Table 2) and is essential to alignment ofMMP priorities within the KPNW Region and the na-tional KP Program.
In the new model, MMP personnel take an activerole in communicating with internal and externalcustomers. Communication tools to define MMP ser-vices and changes are centrally developed. MMPpharmacists use the tools at local health care teammeetings to facilitate discussion about the clinicaltargets or drug initiatives. In addition, the MMP usessatisfaction surveys to obtain ongoing feedback re-garding MMP services, quality of care, andopportunities for improvement.
Another innovation in the MMP model is designingprocesses to address varying needs of individual pa-tients as their health care needs evolve. MMPpopulation-based processes and resource allocationare designed to individualize care to meet the con-tinuum of needs of the individual. Resources areincreased or decreased depending on patient need.This flexibility supports most efficient use of resources.The individualized care for a patient not at goal isdifferent from the level of care for a patient who hasachieved goal and is in maintenance. The care for apatient who may be experiencing an adverse drugevent is different than the level of care for a patientwho tolerates the same medication without adverseeffects. In addition, the most appropriate type ofpatient interaction is also considered, ie, reminderletter, personal phone call, group appointment, orother appropriate interaction. Appropriate level ofcare is routinely considered in deciding on the best-qualified and least-costly process or personnel toemploy. The MMP makes ongoing improvements;this work environment requires that all personnelparticipate and function comfortably in an environ-ment of continuous change and improvement.
Summary and ConclusionsAs the MMP enters its 22nd month of existence,
quality and cost savings continue to improve. LDLlevels less than or equal to 130 mg/dL increased to
The key tosuccessful
implementation ofcentrally managedclinical pharmacy
services isintegration acrossthe continuum of
care within ahealth caresystem ...

47The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
72% at yearend 1999, up from the 66%, which hadalready placed KPNW in the lead position of HEDIS-reporting KP Regions in 1998. Glycemic controlamong MMP-managed therapy failure patients ishigher than general diabetes mellitus patients notmanaged by the MMP: 59.3% vs 41.3%. Patient sat-isfaction survey results show that 96% of MMPpatients are extremely or very satisfied with theircare. Clinician satisfaction survey results reveal that96% believe the MMP supports the health care teamand helps them to achieve clinical targets, and 100%say that the MMP provides excellent or good qual-ity of care. The MMP has helped KPNW achieveover $1,500,000 in drug cost savings. All of this hasbeen accomplished in less than two years—includ-ing tripling the number of patients managed (Figure5)—without hiring additional staff.
The MMP process is shaping state and nationalpharmaceutical care delivery models. KPNW has beenasked to discuss the MMP at:
• CMI Network Interregional Teleconference;• American Society of Health System
Pharmacists Meeting;2
• Interregional Clinical Pharmacy Meeting;• CMI Interregional Diabetes Models of
Care Teleconference;• Oregon Society of Health System Pharma-
cists Meeting;3,4
• CMI Interregional Eldercare Teleconference.
Now that the KPNW culture has changed, the MMPwill move forward by continuing to extend its scopeof care beyond lipid management, glycemic controlin selected diabetes mellitus therapies, and aspirintherapy. Focus will expand to improving outcomesand reducing costs of other drug therapies. Theinfrastructure is in place to continuously improveprocesses and further expand collaboration withclinicians, staff, and administrators to meet changingclinical and cost priorities. KPNW’s experience showsthat the MMP is a transferable model that can assistother integrated health systems in providing high-quality, cost-effective clinical pharmacy services toa large population. ❖
References1. Kaiser Permanente Interregional President's QualityImprovement Best Practices Recommendations for ClinicalPharmacy Services, 1997.2. Lee NL. Implementing Challenges from the ASHPConference "Pharmacy in Managed Care: Vision for theFuture": Prioritization and Implementation of Challenges;Pharmaceutical Care in Managed Care Pharmacy. SpecialSession of American Society of Health System PharmacistsMeeting, Las Vegas, NV, December, 1998.3. Wright TL. Population-based medication management of CVrisk: Dyslipidemias, Oregon Society of Health System PharmacistsAnnual Meeting, Skamania, Washington, May, 1999.4. Ashley R, Boschee G, Grant M, Johnson V, Perry P, RamageJ, et al. Improving the health of populations: An integratedMedication Management Program, Oregon Society of HealthSystem Pharmacists Annual Meeting, Skamania, Washington,May, 1999.
BeliefPerhaps the only limits to the human mind
are those we believe in.Willis Harman, “Global Mind”
Glycemic controlamong MMP-
managed therapyfailure patients is
higher than generaldiabetes mellitus
patients notmanaged by theMMP: 59.3%
vs 41.3%.

48 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
IntroductionThe Asthma Disease Management Program of the
Kaiser Permanente Colorado (KPCO) Denver/Boul-der Local Market began development in August 1995.Its pilot project was implemented in February 1997with full implementation in August 1998. A very largeteam of participants contributed to the initial andongoing success of this regionwide initiative. Table1 identifies the complete list of project supportersand contributors.
Asthma is recognized as a chronic inflammatorydisorder of the airways with symptomatic episodesthat range from mild and intermittent to severe andpersistent. Although the reasons are poorly under-stood, the prevalence of asthma has increasedsignificantly over the past 20 years in both chil-dren and adults.1 Undertreatment and inappropriatepharmaceutical therapy have been shown to bemajor contributors to asthma morbidity and mor-tality.2-4 In 1995, the prevalence of asthma withinKPCO was estimated to be 4% to 6% (13,600 to20,400 asthmatic members). Because of our largepopulation of asthmatic patients and the potentialfor relatively rapid improvement, asthma was oneof the diseases chosen for development of a dis-ease management program.5,6
BackgroundThe development of chronic disease management
programs began in 1995 with an assessment of themember population which identified that KPCO’smodel of care could be improved to meet the needsof chronically ill patients. Our traditional ambulatorycare model was designed to manage acute, episodicexacerbations of asthma. The following weaknesseswere identified: 1) inconsistent approaches acrossthe region to manage chronically ill patients; 2) in-consistent messages to these patients; and 3) no toolsto identify patients receiving inadequate care. Epide-miologic data, market climate, and utilization andcost data describing KPCO’s asthma population es-tablished the need for a redesign process. Employergroups such as PepsiCo, Coors Brewing Company,and Time/Warner Cable were asking about our ap-proach to chronic disease management. Likewise,regulatory and consumer reporting agencies such asthe National Committee for Quality Assurance (NCQA)and the Health Plan Employers Data Information Set(HEDIS) had established population-based standardsfor chronic diseases.7
ProcessThe Asthma Disease Management Program was
implemented as a pilot project in February 1997 fo-cusing on registry development, guidelinedissemination, limited asthma classes, and nursingcare management. Early in 1998, the registry wasrefined, care managers began limiting their inter-vention to high-risk patients under the age of 50years, and physician/staff education was instituted.In August, four additional asthma care managerswere hired, and a “real-time” notification processfor patient hospital and emergency department en-counters was introduced. Additionally, the CareManagement Institute (CMI) began supporting lo-cal disease management initiatives.
ObjectivesThe primary objectives of the Asthma Disease Man-
agement Program are to 1) improve quality outcomesof care, 2) equip patients to better self-manage theirchronic illness, 3) reduce costs of care through avoid-ance of acute episodes and complications, and 4)increase patient and physician satisfaction with con-tinuity of care. The purpose of the initial pilot projectevaluation was to compare the impact of the AsthmaDisease Management Program model with “care asusual” regarding quality outcomes, utilization patternswith related costs, and patient and physician satis-faction. Subsequent to the pilot program evaluation,additional analyses were performed to determine ifimprovements attributable to the Asthma DiseaseManagement Program could be sustained over time.
MethodologyScope
In 1995, analysis of KPCO’s total population of 340,000members revealed that 34.5% had one or more chronicdiseases, an amount that accounted for 60% of primarycare physician utilization. By initiation of the pilot projectin February 1997, the baseline number of asthmaticpatients was 19,784 regionwide. Twenty-two percentof our total asthma population (4708 patients) receivedtheir primary care at two of our medical offices,Westminster and Aurora Centrepoint, which were cho-sen as the pilot intervention sites.
Interventions
The Asthma Disease Management Program is a newmodel of care that addresses the needs of asthmapatients at a population level. The key program ele-
Asthma Disease Management Program
Colorado Region
Although thereasons are poorly
understood, theprevalence ofasthma hasincreased
significantly overthe past 20 years in
both childrenand adults.
49The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
ments described represent the primary changes from“care as usual.” Of particular note is the use of caremanagers—registered nurses—who are responsiblefor monitoring the population of asthma patients in
a specified geographic area, targeting high-risk pa-tients for intervention, and providing one-to-one andgroup care. The primary care physician retains ac-countability for directing and managing the patient’s
Table 1. Kaiser Permanente Colorado Denver/Boulder Local Market Asthma DiseaseManagement Program Project supporters/contributors
Disease Management Core Team Members• Jean Barker, MBA, Director, Strategy Development and Implementation—Team Co-Leader• David Berman, MD, CMI Physician Implementation Manager/Director, Disease Management—Team Co-Leader• Shelley Cooper, MBA, Consultant, Strategy Development and Implementation—Project Manager• Donna Beall, PharmD, Primary Care Services• Arne Beck, PhD, Director, Research and Development• Michael Bodily, MBA, Programmer/Analyst, Information Technology• Ned Calonge, MD, MPH, Chief, Preventive Medicine & Research• Pamela Cowan, BS, Analyst, Research and Development• Elizabeth Gay, MA, Director, Prevention• Alvin Goo, RPh, Pharmacy• Bill Good, MBA, Manager, Clinical Information Systems• Kent Nelson, PharmD, Primary Care Services
Asthma Work Team Members• Peter Cvietusa, MD, Allergy/Pediatrics• Alvin Goo, RPh, Pharmacy• Mary Jo Jacobs, MD, Emergency Medicine• William Marsh, MD, Associate Medical Director for Operations• James Mason, MD, Internal Medicine• Susan Merrill, MD, Pediatrics• Rebecca Mortensen, MD, Pulmonary Medicine• Carl Severin, MD, Family Practice• Betty Spiecher, RN, MS, Nursing Supervisor, Disease Management• John Williams, MD, Regional Department Chief, Allergy
Administrative support• Michael Alexander, Vice President and Executive Director• Connie Slaughter, RN, MS, Director, Quality and Resource Management• Linda Smith, RN, MS, MHA, Director, Operations Support• Andrew Wiesenthal, MD, Associate Medical Director, Medical Management
Physician Mentors• Peter Cvietusa, MD, Pediatrics/Allergy• Robert Harvey, MD, Allergy• Ross Westley, MD, MPH, Allergy• John Williams, MD, Regional Department Chief, Allergy
Pilot Project Asthma Care Managers• Karen Jahn, RN, BS, Asthma Care Manager• Cynthia Lamb, RN, BS, Asthma Care Manager
Research and Analytical Support• Jennifer Ellis, MBA, Programmer/Analyst, Research and Development• David Magid, MD, MPH, Investigator, Clinical Research Unit• Avery Wilson, MSPH, CMI Analyst
Contact persons• Emily Sandelin, RN, MS, CMI Implementation Specialist, Quality and Resource Management• Debra Pearson Ritzwoller, PhD, Health Care Economist, Disease Management
The primary carephysician retainsaccountability for
directing andmanaging thepatient’s care.Asthma care
managers extendphysicians’ ability
to monitor andeducate their
patients.

50 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
care. Asthma care managers extend physicians’ abil-ity to monitor and educate their patients. Key programelements include processes for registry and report-ing, “real-time” notification, care managerintervention, and KP Regionwide education.
Registry and Report Process
The Asthma Disease Identification, Registry, andReporting System is a set of software programs de-veloped by clinicians, programmers, and analysts atKPCO.8 This system extracts and compiles data fromclinical and administrative sources to produce a con-tinuously updated registry of patients with asthma.This system also generates monthly and quarterlyreports of patient levels in electronic and printed for-mats. These reports contain clinically relevant dataof interest to physicians and care managers. Patientsare risk-stratified by pharmaceutical dispensing andby Emergency Department (ED), observation/clini-cal decision unit (OBS/CDU), and inpatient utilization.
“Real-Time” Notification Process
Information about hospitalizations and ED encoun-ters for asthma is received and entered into an Accessdatabase every day. The appropriate care manager isnotified to contact patients shortly after discharge,when they are most likely to make behavior changesto better manage their asthma.
Care Manager Intervention
The care managers identify patients for proactiveoutreach using a combination of the panel report, real-time feedback from hospitals and EDs, and physicianreferral. The goal of intervention is to empower pa-tients to learn self-management skills and to makelifestyle changes to decrease asthma morbidity. Thecare manager follows patients enrolled in the programby in-person and telephone contact during a two- tothree-month period. When appropriate, patients arereferred to classes for additional asthma education.Upon discharge from active care management, patientsresume usual care with their primary care physicianbut may reenter the program if they again meet high-risk criteria. Population monitoring continues for allpatients in the Asthma Registry. Major functions andaccountabilities of care managers include:
• Assessment, treatment modification, andpatient education based on clinicalguidelines;
• Addressing patients’ psychologicalresponses to living with a chronic disease
using behavioral change strategies;• Providing telephone follow-up, trouble-
shooting, monitoring, and coaching toensure success of the patient’s self-management plan;
• Coordinating complex care of patientsand planning their transition back toprimary care as their condition permits;
• Reviewing and interpreting panel reportsand communicating with physicians aboutthe status of their asthma patients.
Regionwide Patient and Staff Education
Asthma management classes for patients (and fam-ily members) are offered monthly at all facilities.Asthma skills training sessions are offered to the staffto enhance their ability to conduct pulmonary func-tion tests and to provide education on medicationand equipment use, peak flow monitoring, environ-mental controls, and asthma pathophysiology. Inaddition, guidelines for asthma care, which are basedon the National Institutes of Health (NIH) recom-mended criteria for diagnosis and treatment, werewidely disseminated to physicians and mid-level pro-viders across the KPCO region.9
Subjects and Setting
In the initial pilot study, conducted from February1 to July 31, 1997, the Asthma Disease ManagementProgram model was compared with “care as usual.”Three hundred seventy-eight patients from a popu-lation of 19,784 members were enrolled in caremanagement during the pilot period. These patientscomprised the pilot intervention group. Patients wereeligible for enrollment if they received primary careservices at one of the two pilot sites and either wereidentified via registry report as being at high risk orwere referred to the program by their primary carephysician. High-risk asthma was defined as: 1) over-use of beta2-agonists, 2) high-dose beta2-agonistuse with no dispensed inhaled steroid, or 3) a re-cent asthma-related hospital or ED admission. Thepilot project was conducted at two medical offices:Westminster and Aurora Centrepoint. An additional976 intervention patients were enrolled into the pro-gram between August 1997 and January 1999.Patients not in the intervention groups received careas usual. Two asthma care managers (1.6 FTE) werehired to participate in the pilot project. Four caremanagers and 13 additional offices were added inAugust 1999.
Asthmamanagement
classes for patients(and family
members) areoffered monthly at
all facilities.

51The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
Study DesignA quasi-experimental pretest-posttest study de-
sign was used to examine changes in process ofcare and clinical outcomes measures for asthmaintervention patients. For some outcomes, multiplepre- or postintervention measurements were per-formed. Changes within a comparison group(composed of Asthma Registry members who hadnot been seen by the care managers) were alsoassessed on similar outcome measures. A pretest-posttest design was also used to evaluate changesin patient and physician satisfaction. Althoughplanned for the pilot evaluation, use of a morerigorous randomized case-control design was notfeasible because of pilot implementation issues.For example, during the pilot project, a large num-ber (48%) of all intervention patients were referredto asthma care managers by their primary care phy-sicians. Given that provider acceptance of theasthma care managers was an important key tosuccessful implementation of the Asthma Care Man-agement Program, referred patients were acceptedinto the Program at the expense of a more rigor-ous study design. Also, a great amount of refinementof the computer programs used for patient identi-fication and risk stratification took place duringthe pilot period. Statistical methods used in analy-ses of pilot and postpilot data included parametricand nonparametric within-group tests for signifi-cance (eg, chi-square, t, and Wilcoxon signed ranktests) as appropriate.
Patient Intervention Procedure
The asthma care managers contacted patients bytelephone and screened them for eligibility. Patientswere enrolled if they met entry criteria and werewilling to participate. A one-to-one initial visit wasscheduled. At the initial visit, the care manager re-corded a detailed history, performed pulmonaryfunction tests, and provided education about asthmaand its treatment. Small steps toward behavior changewere negotiated with the patient according to thepatient’s readiness to change, lifestyle, and areas (s)hewas willing to address. Patients were given a writtenhome care plan if their asthma was stable. Patientsexperiencing an asthma flare were appropriatelytreated and were scheduled for a second visit. Sub-sequent patient contacts occurred by telephone amean of three times during a three-month period.All face-to-face and phone contacts were recordedon coding sheets designed for the pilot project.
MeasuresThe project addressed the following outcomes, utili-
zation, and process of care measures: patient andphysician satisfaction, use of ambulatory and hospital-based health care services, overuse of beta2-agonistmedication, usage of prescribed anti-inflammatorymedication, dispensing of peak flow meters, preva-lence of spirometry testing, and the provision of ahome care plan.
Satisfaction Data
Pre- and postpilot patient satisfaction surveys wereadministered to 258 intervention and noninterven-tion asthma patients. Pre- and postpilot satisfactionsurveys were administered to 71 physicians at pilotand nonpilot medical offices. Survey questions useda five-point Likert scale response, where “1” definedthe negative pole and “5” defined the positive pole.Patient satisfaction data were collected from a ran-dom sample of nonintervention patients andintervention patients via telephone survey. Surveyresults were analyzed for patients who responded toboth the baseline and postpilot surveys. Questionsaddressed patient satisfaction with education, homecare planning, asthma management, and continuityof care. A written survey was administered in De-cember 1996 and again in August 1997 to a randomsample of physicians in primary care departments atpilot and nonpilot sites. Questions addressed satis-faction related to provision and monitoring of asthmapatient’s care, meeting patient expectations, and avail-ability of resources to manage asthma patients.Within-group and between-group changes in satis-faction were measured using Wilcoxon signed ranktests and Wilcoxon-Mann-Whitney U tests.
In March of 1998 and 1999, the CMI-sponsored ad-ministration of a survey to adults who were identifiedas having asthma. Eighty percent of patients whoresponded to the 1998 survey also responded to thefollow-up 1999 survey, for a total of 1225 patients.Data from a subsample of these respondents werepublished in the 1998 CMI Asthma Outcomes Re-port.10 Three of the 64 survey questions address issuesof patient satisfaction. Paired t tests and the Wilcoxonsigned rank test were used to assess changes be-tween the two time periods.
Utilization Data
Administrative databases were used to collect phar-macy, outpatient encounter, and hospital (inpatient,ED, and observation/clinical decision unit (OBS/
Patientsexperiencing an
asthma flare wereappropriately
treated and werescheduled for a
second visit.Subsequent patientcontacts occurred
by telephone amean of threetimes during athree-month
period.

52 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
CDU)) data for all patients identified with asthma. Tocontrol for seasonality and the effect of secular trendsin both clinical and data systems, utilization data wereextracted for several time periods before and afterthe pilot.
Outpatient utilization data were obtained fromclaims and encounter databases. Using paired t tests,the rate of asthma-related ambulatory care visits toprimary care departments was measured for severalperiods before and after the initial encounter with acare manager for intervention patients enrolled dur-ing the pilot and for a similar time period fornonintervention patients. During the postpilot phase,changes in ambulatory care utilization was measuredat the population level for patients identified in theregistry in both March 1998 and March 1999. Patientswere stratified into three age groups: 0-18 years (pe-diatric members), 19-49 years (adult members), and50+ years (older adult members). Paired t tests wereused to evaluate the change in mean number of vis-its per patient per year to Primary Care Departmentsfor asthma-related conditions and to the Pulmonologyand Allergy Departments.
Changes in hospital-based utilization rates (inpa-tient, ED, and OBS/CDU) were measured for apilot-specific cohort of intervention patients and forall asthma patients identified via the registry for sev-eral time periods. Paired t tests and repeated measuresANOVA were used to evaluate differences in meannumber of inpatient admissions, emergency depart-ment visits, and OBS/CDU visits per year for the initialpilot cohort of intervention patients. Paired t testswere used to evaluate the change in mean numberof inpatient admissions, emergency department vis-its, and OBS/CDU visits per patient per year. Nostatistical tests were performed on the likelihood ofa hospital event occurring.
Parametric and nonparametric statistical tests wereused to assess changes over time for four aspects ofpharmacy dispensing patterns for all asthma patients:1) number of beta2-agonists dispensed per patientin a six-month period; 2) percentage of patients withbeta2-agonist overuse; 3) percentage of patients tak-ing high-dose beta2-agonists with a dispensedinhaled anti-inflammatory; and 4) percentage ofasthma patients who had been dispensed a peakflow meter. Many of these measures were stratifiedby intervention status, by age category, or by both.In order to control for unmeasured seasonal varia-tion, the following four time periods were examinedfor the pilot evaluation: one-year prepilot, baseline
(or prepilot), end-of-pilot, and six-month postpilotperiods. Overuse is defined here as 12 or more me-tered dose inhalers (MDI), or 180 or more millilitersof nebulizer solution, or 2160 or more milliliters ofnebulizer premix solution of a beta2-agonist prod-uct dispensed in a six-month period. A patient whois a high-dose beta2-agonist user with an inhaledanti-inflammatory product is one who is dispensedsix or more MDIs or the equivalent of a beta2-agonist product in a six-month period and alsoreceives an inhaled anti-inflammatory product (eg,beclomethasone dipropionate, budesonide,fluticasone, cromolyn sodium, etc.).
Process of Care Measures
Dispensing of peak flow meters, administration ofspirometry tests, and development and documenta-tion of patient home self-care plans are all consideredto be process-of-care measures in this evaluation. InSeptember 1997, registered nurses performed retro-spective chart audits on all pilot intervention patientsand on a random sample of nonintervention patientsto document receipt of spirometry testing and exist-ence of a home care plan. Chi-square and Wilcoxonsigned rank tests were used to evaluate within-groupand between-group changes in these two measures.Data from the CMI-sponsored Survey of Adults withAsthma was used to describe changes in population-based measures of peak flow meter dispensing andreceipt of home self-care instructions.7 The Wilcoxonsigned rank test was used to examine changes in thedistribution of responses between March 1998 andMarch 1999 for a sample of 1222 documented asthmapatients who responded in both time periods.
ResultsSatisfaction
Seventeen physicians at pilot sites and 54 physi-cians at nonpilot sites completed baseline andpostpilot surveys. At baseline, no statistical differ-ence for any of the ten questions was noted betweenpilot and nonpilot physicians responding. Using theWilcoxon signed rank test, significant improvement(p < 0.05) in three of the satisfaction scores was foundfor the pilot site physicians. For the nonpilot sitephysicians, one measure improved significantly (p <0.05), and five measures declined significantly. Themagnitude of improvement was greater for the pilotgroup of physicians and staff for all questions. Themagnitude of improvement was greater for the pilotgroup of providers for all questions. Wilcoxon-Mann-
... significantimprovement (p <0.05) in three ofthe satisfaction
scores was foundfor the pilot site
physicians. For thenonpilot site
physicians, onemeasure improvedsignificantly (p <0.05), and five
measures declinedsignificantly.
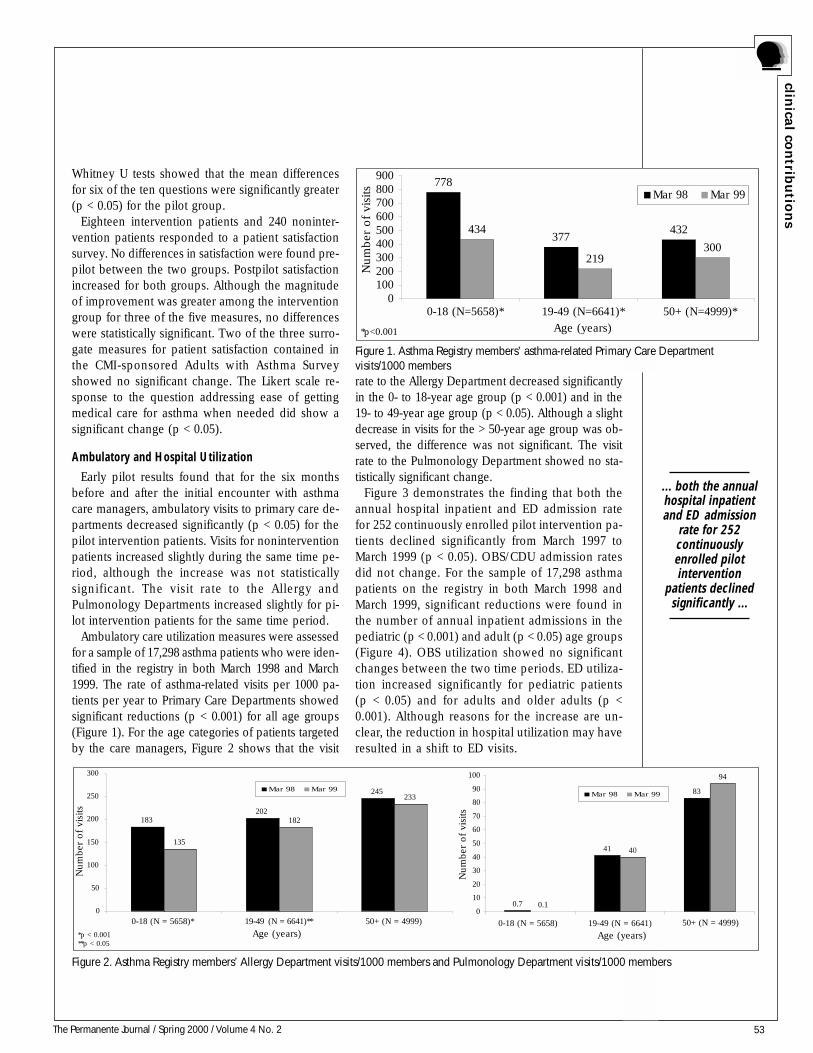
53The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
Whitney U tests showed that the mean differencesfor six of the ten questions were significantly greater(p < 0.05) for the pilot group.
Eighteen intervention patients and 240 noninter-vention patients responded to a patient satisfactionsurvey. No differences in satisfaction were found pre-pilot between the two groups. Postpilot satisfactionincreased for both groups. Although the magnitudeof improvement was greater among the interventiongroup for three of the five measures, no differenceswere statistically significant. Two of the three surro-gate measures for patient satisfaction contained inthe CMI-sponsored Adults with Asthma Surveyshowed no significant change. The Likert scale re-sponse to the question addressing ease of gettingmedical care for asthma when needed did show asignificant change (p < 0.05).
Ambulatory and Hospital Utilization
Early pilot results found that for the six monthsbefore and after the initial encounter with asthmacare managers, ambulatory visits to primary care de-partments decreased significantly (p < 0.05) for thepilot intervention patients. Visits for noninterventionpatients increased slightly during the same time pe-riod, although the increase was not statisticallysignificant. The visit rate to the Allergy andPulmonology Departments increased slightly for pi-lot intervention patients for the same time period.
Ambulatory care utilization measures were assessedfor a sample of 17,298 asthma patients who were iden-tified in the registry in both March 1998 and March1999. The rate of asthma-related visits per 1000 pa-tients per year to Primary Care Departments showedsignificant reductions (p < 0.001) for all age groups(Figure 1). For the age categories of patients targetedby the care managers, Figure 2 shows that the visit
rate to the Allergy Department decreased significantlyin the 0- to 18-year age group (p < 0.001) and in the19- to 49-year age group (p < 0.05). Although a slightdecrease in visits for the > 50-year age group was ob-served, the difference was not significant. The visitrate to the Pulmonology Department showed no sta-tistically significant change.
Figure 3 demonstrates the finding that both theannual hospital inpatient and ED admission ratefor 252 continuously enrolled pilot intervention pa-tients declined significantly from March 1997 toMarch 1999 (p < 0.05). OBS/CDU admission ratesdid not change. For the sample of 17,298 asthmapatients on the registry in both March 1998 andMarch 1999, significant reductions were found inthe number of annual inpatient admissions in thepediatric (p < 0.001) and adult (p < 0.05) age groups(Figure 4). OBS utilization showed no significantchanges between the two time periods. ED utiliza-tion increased significantly for pediatric patients(p < 0.05) and for adults and older adults (p <0.001). Although reasons for the increase are un-clear, the reduction in hospital utilization may haveresulted in a shift to ED visits.
Figure 2. Asthma Registry members’ Allergy Department visits/1000 members and Pulmonology Department visits/1000 members
183202
245
135
182
233
0
50
100
150
200
250
300
0-18 (N = 5658)* 19-49 (N = 6641)** 50+ (N = 4999)
Age (years)
Mar 98 Mar 99
0.7
41
83
0.1
40
94
0
10
20
30
40
50
60
70
80
90
100
0-18 (N = 5658) 19-49 (N = 6641) *p < 0.001**p < 0.05
Mar 98 Mar 99
Age (years)
Num
ber
of vi
sits
Num
ber
of vi
sits
50+ (N = 4999)
Figure 1. Asthma Registry members’ asthma-related Primary Care Departmentvisits/1000 members
778
377432434
219300
0100200300400500600700800900
0-18 (N=5658)* 19-49 (N=6641)* 50+ (N=4999)*
Age (years)
Mar 98 Mar 99
*p<0.001
Num
ber
of vi
sits
... both the annualhospital inpatientand ED admission
rate for 252continuouslyenrolled pilotintervention
patients declinedsignificantly ...
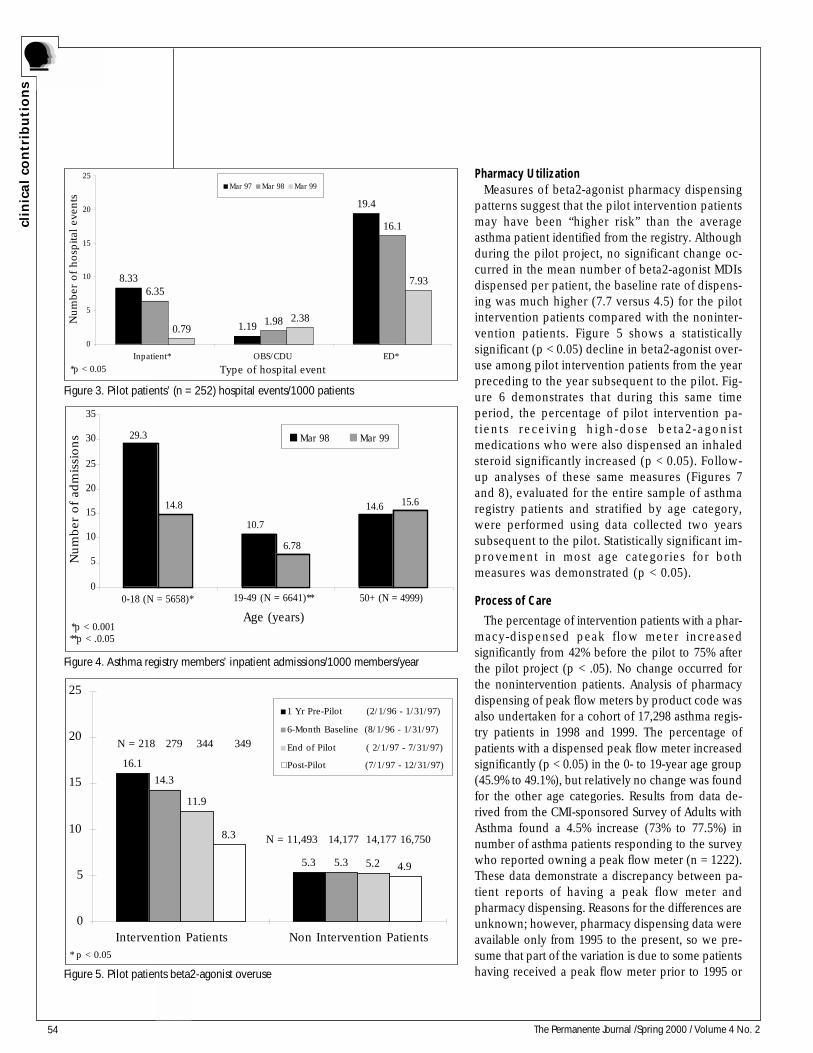
54 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
Pharmacy UtilizationMeasures of beta2-agonist pharmacy dispensing
patterns suggest that the pilot intervention patientsmay have been “higher risk” than the averageasthma patient identified from the registry. Althoughduring the pilot project, no significant change oc-curred in the mean number of beta2-agonist MDIsdispensed per patient, the baseline rate of dispens-ing was much higher (7.7 versus 4.5) for the pilotintervention patients compared with the noninter-vention patients. Figure 5 shows a statisticallysignificant (p < 0.05) decline in beta2-agonist over-use among pilot intervention patients from the yearpreceding to the year subsequent to the pilot. Fig-ure 6 demonstrates that during this same timeperiod, the percentage of pilot intervention pa-t ients r ece iv ing high-dose beta2-agonis tmedications who were also dispensed an inhaledsteroid significantly increased (p < 0.05). Follow-up analyses of these same measures (Figures 7and 8), evaluated for the entire sample of asthmaregistry patients and stratified by age category,were performed using data collected two yearssubsequent to the pilot. Statistically significant im-provement in most age categories for bothmeasures was demonstrated (p < 0.05).
Process of Care
The percentage of intervention patients with a phar-macy-dispensed peak flow meter increasedsignificantly from 42% before the pilot to 75% afterthe pilot project (p < .05). No change occurred forthe nonintervention patients. Analysis of pharmacydispensing of peak flow meters by product code wasalso undertaken for a cohort of 17,298 asthma regis-try patients in 1998 and 1999. The percentage ofpatients with a dispensed peak flow meter increasedsignificantly (p < 0.05) in the 0- to 19-year age group(45.9% to 49.1%), but relatively no change was foundfor the other age categories. Results from data de-rived from the CMI-sponsored Survey of Adults withAsthma found a 4.5% increase (73% to 77.5%) innumber of asthma patients responding to the surveywho reported owning a peak flow meter (n = 1222).These data demonstrate a discrepancy between pa-tient reports of having a peak flow meter andpharmacy dispensing. Reasons for the differences areunknown; however, pharmacy dispensing data wereavailable only from 1995 to the present, so we pre-sume that part of the variation is due to some patientshaving received a peak flow meter prior to 1995 or
8.33
1.19
19.4
1.98
16.1
0.792.38
7.936.35
0
5
10
15
20
25
Inpatient* OBS/CDU ED*
Type of hospital event
Mar 97 Mar 98 Mar 99
*p < 0.05
Num
ber
of hosp
ital
eve
nts
*p < 0.001**p < .0.05
29.3
10.7
14.614.8
6.78
15.6
0
5
10
15
20
25
30
35
0-18 (N = 5658)* 19-49 (N = 6641)** 50+ (N = 4999)
Age (years)
Mar 98 Mar 99
Num
ber
of ad
mis
sions
5.3
14.3
5.3
11.9
5.2
8.3
4.9
16.1
0
5
10
15
20
25
Intervention Patients Non Intervention Patients* p < 0.05
1 Yr Pre-Pilot (2/1/96 - 1/31/97)
6-Month Baseline (8/1/96 - 1/31/97)
End of Pilot ( 2/1/97 - 7/31/97)
Post-Pilot (7/1/97 - 12/31/97)
N = 218 279 344 349
N = 11,493 14,177 14,177 16,750
Figure 3. Pilot patients’ (n = 252) hospital events/1000 patients
Figure 4. Asthma registry members’ inpatient admissions/1000 members/year
Figure 5. Pilot patients beta2-agonist overuse
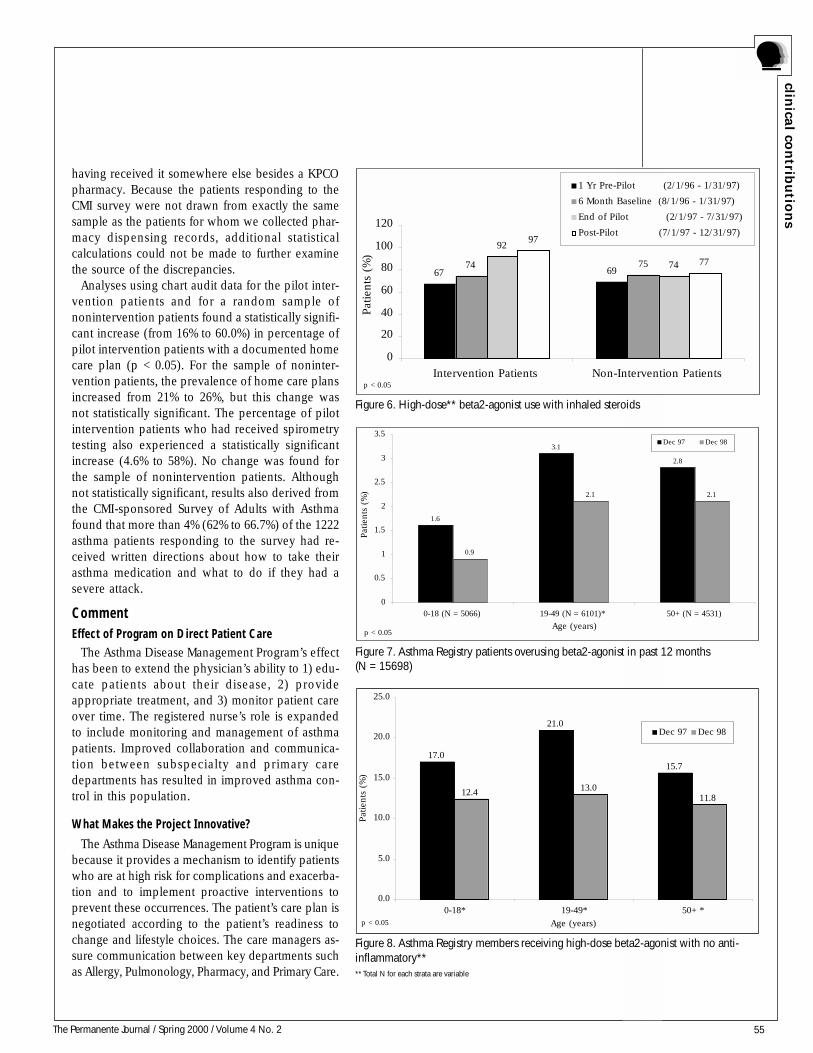
55The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
having received it somewhere else besides a KPCOpharmacy. Because the patients responding to theCMI survey were not drawn from exactly the samesample as the patients for whom we collected phar-macy dispensing records, additional statisticalcalculations could not be made to further examinethe source of the discrepancies.
Analyses using chart audit data for the pilot inter-vention patients and for a random sample ofnonintervention patients found a statistically signifi-cant increase (from 16% to 60.0%) in percentage ofpilot intervention patients with a documented homecare plan (p < 0.05). For the sample of noninter-vention patients, the prevalence of home care plansincreased from 21% to 26%, but this change wasnot statistically significant. The percentage of pilotintervention patients who had received spirometrytesting also experienced a statistically significantincrease (4.6% to 58%). No change was found forthe sample of nonintervention patients. Althoughnot statistically significant, results also derived fromthe CMI-sponsored Survey of Adults with Asthmafound that more than 4% (62% to 66.7%) of the 1222asthma patients responding to the survey had re-ceived written directions about how to take theirasthma medication and what to do if they had asevere attack.
CommentEffect of Program on Direct Patient Care
The Asthma Disease Management Program’s effecthas been to extend the physician’s ability to 1) edu-cate patients about their disease, 2) provideappropriate treatment, and 3) monitor patient careover time. The registered nurse’s role is expandedto include monitoring and management of asthmapatients. Improved collaboration and communica-tion between subspecialty and primary caredepartments has resulted in improved asthma con-trol in this population.
What Makes the Project Innovative?
The Asthma Disease Management Program is uniquebecause it provides a mechanism to identify patientswho are at high risk for complications and exacerba-tion and to implement proactive interventions toprevent these occurrences. The patient’s care plan isnegotiated according to the patient’s readiness tochange and lifestyle choices. The care managers as-sure communication between key departments suchas Allergy, Pulmonology, Pharmacy, and Primary Care.
17.0
21.0
15.7
12.4 13.011.8
0.0
5.0
10.0
15.0
20.0
25.0
0-18* 19-49* 50+ *
Pat
ients
(%
)
Dec 97 Dec 98
p < 0.05 Age (years)
Figure 8. Asthma Registry members receiving high-dose beta2-agonist with no anti-inflammatory**** Total N for each strata are variable
2.8
2.1
50+ (N = 4531)
1.6
3.1
0.9
2.1
0
0.5
1
1.5
2
2.5
3
3.5
0-18 (N = 5066) 19-49 (N = 6101)*
Age (years)
Pat
ients
(%
)
Dec 97 Dec 98
p < 0.05
Figure 7. Asthma Registry patients overusing beta2-agonist in past 12 months(N = 15698)
Pat
ients
(%
)
67 6974 75
92
74
97
77
0
20
40
60
80
100
120
Intervention Patients Non-Intervention Patients
1 Yr Pre-Pilot (2/1/96 - 1/31/97)
6 Month Baseline (8/1/96 - 1/31/97)
End of Pilot (2/1/97 - 7/31/97)
Post-Pilot (7/1/97 - 12/31/97)
p < 0.05
Figure 6. High-dose** beta2-agonist use with inhaled steroids
56 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
Has the Program Led to Development of New orImproved Processes That Can Be Considered“Best Practices”?
KPCO’s Primary Care Quality Council targetedasthma as one of its primary areas of focus for 1999.The Council adopted asthma quality measures rec-ommended by the Asthma Disease ManagementProgram and is piloting an asthma initiative in thePediatric Departments. In 1998, all KP Divisions col-laborated to create the CMI to disseminateknowledge and assist with local implementation ofevidence-based clinical best practices throughoutall regions. Our established Asthma Disease Man-agement Program has been highlighted ininterregional discussions and is being evaluated asa best practice.
Has the Project Resulted in Excellent PerformanceCompared with Other Programs orRelevant Benchmarks?
In October 1998, the CMI published data compar-ing the results for care processes and outcomes forall KP.10 For the period 8/1/96 through 7/31/97, whichincluded our six-month pilot period, the KPCO com-pared favorably with other KP Regions.
Benefits of Multidisciplinary Team Involvement
The volume and focus of the Program’s develop-ment required the skills of clinical and nonclinicalstaff. The Program is not viewed as replacing anypart of patient care but is well integrated into theprimary care milieu. The Program’s successful imple-mentation occurred because the viewpoints, concerns,and interests of the staff who would be affected wererepresented. These individuals continue to be on-site champions of the program.
Implications and ConclusionThe pilot project resulted in implementation of
asthma care management for all clinics in the Den-ver/Boulder Local Market and the addition of fourasthma care managers. KP Kansas City recently insti-
tuted an asthma care management program basedon the successful results of our Denver/Boulder Lo-cal Market project. The KPCO Colorado Springs LocalMarket is working collaboratively with the Denver/Boulder Disease Management Team to implementan asthma disease management program.
In conclusion, evaluation of the Asthma DiseaseManagement Program demonstrated improved pa-tient and physician satisfaction, improved treatment/care planning, and improved medication utilizationwith gains sustained over a two-year period. Theevaluation thus demonstrated that systematic, popu-lation-based asthma disease management can improvequality, satisfaction, and utilization outcomes and cansustain these gains over time. ❖
References1. National Heart, Lung and Blood Institute, National AsthmaEducation and Prevention Program. Global Initiative for Asthma:Global Strategy for Asthma Management and Prevention NHLBI/WHO Workshop Report National Institutes of Health Pub No.95-3659. Bethesda, MD, 1997.2. Pappas G, Hadden WC, Kozak LJ, Fisher GF. Potentiallyavoidable hospitalizations: inequalities in rates between USsocioeconomic groups. Am J Public Health 1997;87:811-6.3. Friday GA Jr, Khine H, Lin MS, Caliguiri LAA. Profile ofchildren requiring emergency treatment for asthma. Ann AllergyAsthma Immunol 1997;78:221-4.4. Hartert TV, Windom HH, Peebles RS Jr, Freidhoff LR, TogiasA. Inadequate outpatient medical therapy for patients withasthma admitted to two urban hospitals. Am J Med1996;100:386-94.5. van Essen-Zandvliet EE, Hughes MD, Waalkens HJ,Duiverman EJ, Pocock SJ, Kerrebijn KF. Effects of 22 months oftreatment with inhaled corticosteroids and/or beta2-agonist onlung function, airway responsiveness, and symptoms in childrenwith asthma. The Dutch Chronic Non-Specific Lung DiseaseStudy Group. Am Rev Respir Dis 1992;146:547-54.6. Solomon N, Steinbruegge J, Juhn P. White Paper: TheOpportunity of Disease Management at Kaiser Permanente,December 2, 1996, unpublished position statement.7. Bodily M. Disease Management System Specifications andDocumentation. Kaiser Permanente, 1999.8. HEDIS 2000 Technical Specifications. National Committee forQuality Assurance, Washington, DC, 1999, p. 98-100.9. National Heart, Lung and Blood Institute, National AsthmaEducation and Prevention Program. Expert Panel Report 2:Guidelines for the Diagnosis and Management of Asthma. NationalInstitutes of Health Pub No .97-4051. Bethesda, MD, 1997.10. Care Management Institute. 1998 Kaiser Permanente AsthmaOutcomes Report. October 1998.
The Program is notviewed as
replacing any partof patient care ...

57The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
Despite the availability of highly ef-fective methods of contraception, one half ofthe pregnancies in the United States are unin-tended, and 28% of all pregnancies end in abor-tion. Nearly one half of the approximatelythree million unintended pregnancies eachyear occur among women who report using acontraceptive method, suggesting that manyof these unintended pregnancies are a resultof contraceptive failure. It has been knownsince the early 1970s that oral contraceptivesgiven in high doses post-coitally are highlyeffective in preventing pregnancy, but theiruse has been limited.
In July 1996, Kaiser Permanente South-ern California (KPSC) began a research anddemonstration project on emergency contra-ceptive pills (ECP). The project was a collabo-ration between KPSC, the Pacific Institute forWomen’s Health (a Los Angeles-based nonprofitorganization specializing in research onwomen’s health), and the Program for Appro-priate Technology in Health (PATH, a Seattle-based not-for-profit group specializing in de-velopment of contraceptive health educationmaterials for consumers and providers). Theproject was designed to evaluate the feasibil-ity and acceptability of ECP within KP, to in-
crease the availability and use of ECP, and todevelop institutional templates, provider train-ing materials, and patient education materialsthat could be used to replicate the project inKP and elsewhere.
The demonstration and evaluation por-tions of the project were successfully completedin the San Diego Service Area of KPSC. Womenwho received ECP as part of the project werehighly satisfied with this service. There wassome evidence that abortion rates decreasedmore in San Diego than in other KPSC ServiceAreas, although this change cannot be attrib-uted solely to provision of ECP.
The repackaging of oral contraceptiveswas “institutionalized” in San Diego, and theECP kits that were developed and piloted in theproject are now available throughout the KPProgram. The Project has been replicatedthroughout KPSC, and ECPs are available andbeing provided in all KPSC Service Areas.The supporting materials (brochures, post-ers, templates) have been made widely avail-able both inside and outside KP. A cost analy-sis showed that provision of ECPs would becost-saving to KP even if a commercial prod-uct were substituted for the ECP kits used inthis project.
Emergency Contraception Research and Demonstration Project
Southern California Region
Table 1. Team members—Emergency Contraception Research and Demonstration Project
Kaiser PermanenteSouthern California
Pacific Institute forWomen's Health
Program for AppropriateTechnology in Health (PATH)
Contact person:Diana B. Petitti, MD, MPH
Director, Department of Research and Evaluation
Linda J. Beckman, PhDSenior Scientist
Elisa WellsSenior Program Officer
David Preskill, MDChief, Obstetrics and Gynecology, San Diego
S. Marie Harvey, PhDSenior Scientist
Scott WittetSenior Program Officer
Kathie HellerField Work Supervisor, Department of Research and Evaluation
Christy Sherman, PhDProject Manager
Michelle PaulDepartment Administrator, Obstetrics and Gynecology, San Diego
Debbie Postlethwaite,RNP, MPH, Project Coordinator, Obstetrics and Gynecology, San
Diego
Howard Switzky, RPh, FCSHPManager, Drug Distribution, California Division–South
The project wasdesigned toevaluate the
feasibility andacceptability of
ECP within KP ...

58 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
BackgroundThe project was initiated in response to the ob-
servation that in spite of the demonstrated efficacyof oral contraceptives as emergency contraception(EC), several problems prevented their widespreaddistribution and use. At the time that the projectwas initiated, no commercially available ECP prod-uct existed, provider knowledge of how to correctlyprescribe ECP was low, and obtaining ECP was in-convenient for women.
The project follows trends in patient care, both in-side and outside KP, that focus on womens’ health.The project is in keeping with initiatives in KPSC andelsewhere in the KP Program that seek to reduce therisk of unintended pregnancy. The project is in align-ment with the public’s desire to see contraceptivestreated in the same way as other medications by healthplans and insurers.
The ECP program had six components. The formalevaluation had five components. These are listed inTable 2 and described in the sections on Methodol-ogy and Evaluation.
ObjectivesThe project was designed to evaluate the feasibility
and acceptability of ECP within KP, to increase theavailability and use of ECP, and to develop institu-tional templates, provider training materials, and pa-tient education materials that could be used to repli-cate the project in KP and elsewhere.
Scope and SignificanceProblem Statement
Despite the availability of highly effective methodsof contraception, one half of the pregnancies in theUnited States are unintended, and 28% of all pregnan-cies end in abortion. Moreover, nearly one half of theapproximately three million unintended pregnancieseach year occur among women who report using acontraceptive method, suggesting that many of theseunintended pregnancies are a result of contraceptivefailure. Experts agree that increasing the menu of con-traceptive choices is desirable and that providingwomen a method of contraception that prevents preg-nancy after unprotected sexual intercourse orcontraceptive method failure is critically needed.
Emergency contraceptive pills (also known as “morn-ing-after pills”) are a form of postcoital hormonaltreatment intended to prevent pregnancy after unpro-tected sexual intercourse. It has been known sincethe mid 1970s that oral contraceptives (OCs) given inhigh doses postcoitally are effective in preventing preg-nancy. Studies done over the last two decades haveconfirmed that a specific regimen of emergency con-traception, known as the Yuzpe regimen, reduces therisk of pregnancy by about 75%. It is estimated thatamong 100 women who have unprotected intercourse,eight would be expected to become pregnant withoutECP whereas only two would be expected to becomepregnant with use of ECP. Other ECP regimens thatprovide only levonorgestrel in high doses reduce therisk of pregnancy by 90%.
Use of ECP has not been widespread in the UnitedStates for a number of reasons. Until very recently,provision of ECP required either provider knowledgeof exactly how to instruct patients to punch out theproper number of oral contraceptives from a pillpackage that was designed to facilitate daily use oforal contraceptives for fixed periods of 28 days orarrangement for repackaging of OCs into packets spe-cifically for use as ECPs. To repackage OCs in bulkrequires a repackaging license. In addition, provid-ers have been shown to lack detailed knowledge ofthe intricacies and complexities of ECP, includingtypes of products that can be used, dosing regimens,and recommended timing for use.
Relevance to Patient Care
About two million members (24%) KP Medical CareProgram are women of reproductive age (15-44 years)and are potentially in need of contraceptive services.
Table 2. Emergency contraception project
Program Components
• Repackaging of oral contraceptives as ECP kit• Development of provider and patient education materials• Development of environmental intervention materials to support program• In-service training of providers• Making ECP kits available at convenient locations• Packaging and distribution of "Replication Packs"
Evaluation Components
• Before/after survey of providers' knowledge and practices• Survey of members who received an emergency contraception kit in San Diego during the demonstration period• Assessment of rates of induced abortion for members in San Diego in comparison with the rest of KPSC• Monitoring of utilization of ECP kits• Analysis of the cost-effectiveness of provision of ECP• Analysis of induced-abortion rates
It has been knownsince the mid
1970s that oralcontraceptives
(OCs) given in highdoses postcoitally
are effective inpreventingpregnancy.

59The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
At least 25,000 KP members per year obtain an in-duced abortion (precise figures for abortions are notavailable) in spite of the fact that all members haveaccess to contraceptive services. The number of mem-bers who are potentially affected by the quality issueaddressed in this project—unintended pregnancy andthe need for a method to backup failure of condomsand other contraceptives—is much larger, becausethe male partners of women members and malemembers of the Health Plan are potentially affectedby the availability of ECP. All family members areaffected by unintended pregnancy.
External ImpactIn initiating this project, KP assumed a role of leader-
ship in the local community and nationally. The projecthad an important influence on other organizations’ will-ingness to provide ECP. The tools and templatesdeveloped in the project have been used as models orwithout modification in implementation of provision ofECP throughout the US. More than fifty EC TrainingToolboxes have been purchased by organizations out-side KP, including nursing schools, medical schools,and pharmacy schools; Planned Parenthood Federa-tion of America, the Departments of Health and HumanServices for Alaska, New Mexico, and Georgia; and aninternational health organization in Thailand. Projectmaterials and protocols have been adopted by localPlanned Parenthood affiliates, San Diego State Univer-sity, the University of California at San Diego, and manylocal and regional community clinics.
ECP project team members have become recognized,influential experts on provision of ECP and have beenspeakers at multiple national conferences on this topic.Project participants were consultants to the nationalmedia firm that developed Public Service Announce-ments concerning ECP that were aired in four citiesand public education materials used in several maga-zines with national circulation. Project team membershave been consulted by a California State Senator re-garding two submitted bills that would increase ac-cess to emergency contraception in California.
MethodologyRepackaging of Oral Contraceptives as ECP Kit
A cornerstone of the demonstration project was re-packaging of oral contraceptives as ECP. When theproject began, there was no commercially availableproduct packaged as ECP. Providers who wanted toprescribe OCs as ECP would first need to write a pre-scription for a full cycle of regular oral contraceptives.
They would then need to instruct the patient abouthow many of these pills to take at what interval. Oralcontraceptives that contain norethindrone, which arethe most commonly prescribed OCs given as regularoral contraception, have not been proven as effectiveas ECP. Even for OCs that contain norgestrel orlevonorgestrel, which have been shown effective asEC, the number of pills that need to be taken differsbetween different OC brands (eg, two pills every 12hours for Ovral; four pills every 12 hours for Levlen).These complexities meant that a provider would needto be very knowledgeable about some subtle issuesin OC formulation to prescribe ECP correctly.
To remove any problems that might arise from a needfor providers to have detailed knowledge of what kindand how many regular OCs needed to be given to beeffective as ECP, oral contraceptives were repackagedin the KPSC Regional Pharmacy. In the demonstrationphase, a combination oral contraceptive with 500 µg ofdL-norgestrel and 50 µg of ethinyl estradiol (Ovral) wasrepackaged because, at the time the project began, allof the published data on efficacy reflected the use ofthis type of product. In the replication phase, Phar-macy is repackaging Levlen, which is less costly andequally effective. It is anticipated that repackaging byKP will be replaced with a commercial product.
Table 3. Contents of Emergency Contraception "Tool Kit"
Provider-oriented Materials
• Department of Obstetrics and Gynecology policy and procedures for ECP provider service manual (18 pages)• Screening guidelines (3 pages)• Dispensing protocol (2 pages)
Environmental Intervention Tools
• "Once a Secret, Now an Option" poster (11 inches x 16 1/2 inches in lavender)• Appointment center notes for ECP (1 page)• Health Phone script (2 pages)• Dispensing form (half-page)
Patient-oriented Materials
• Information brochure for patients in English (blue) and Spanish (rose), wallet card with national ECP hotline number (English on one side/Spanish on the other) (2 1/4 inches x 3 1/4 inches in green)• Instructions to patients for using ECP as included in ECP Tool Kit (English and Spanish)
Other
• Order sheet for customized material
In initiating thisproject, KP
assumed a role ofleadership in thelocal communityand nationally.
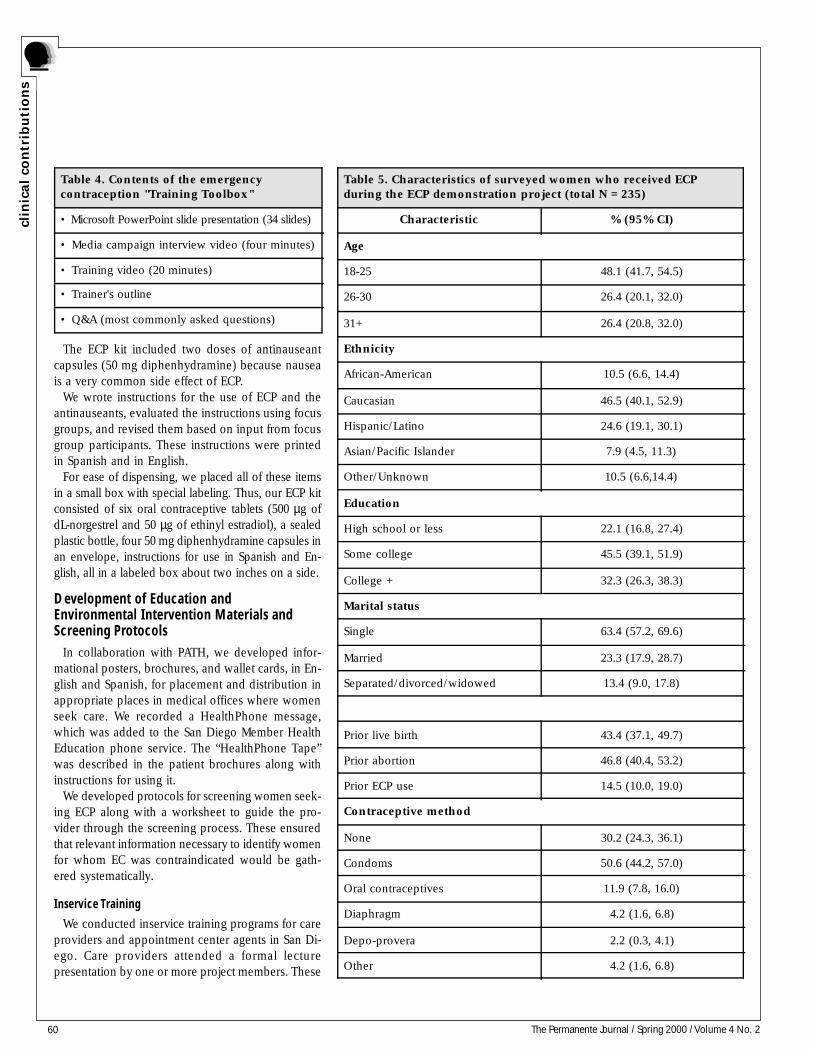
60 The Permanente Journal / Spring 2000 / Volume 4 No. 2
The ECP kit included two doses of antinauseantcapsules (50 mg diphenhydramine) because nauseais a very common side effect of ECP.
We wrote instructions for the use of ECP and theantinauseants, evaluated the instructions using focusgroups, and revised them based on input from focusgroup participants. These instructions were printedin Spanish and in English.
For ease of dispensing, we placed all of these itemsin a small box with special labeling. Thus, our ECP kitconsisted of six oral contraceptive tablets (500 µg ofdL-norgestrel and 50 µg of ethinyl estradiol), a sealedplastic bottle, four 50 mg diphenhydramine capsules inan envelope, instructions for use in Spanish and En-glish, all in a labeled box about two inches on a side.
Development of Education andEnvironmental Intervention Materials andScreening Protocols
In collaboration with PATH, we developed infor-mational posters, brochures, and wallet cards, in En-glish and Spanish, for placement and distribution inappropriate places in medical offices where womenseek care. We recorded a HealthPhone message,which was added to the San Diego Member HealthEducation phone service. The “HealthPhone Tape”was described in the patient brochures along withinstructions for using it.
We developed protocols for screening women seek-ing ECP along with a worksheet to guide the pro-vider through the screening process. These ensuredthat relevant information necessary to identify womenfor whom EC was contraindicated would be gath-ered systematically.
Inservice Training
We conducted inservice training programs for careproviders and appointment center agents in San Di-ego. Care providers attended a formal lecturepresentation by one or more project members. These
Table 4. Contents of the emergencycontraception "Training Toolbox"
• Microsoft PowerPoint slide presentation (34 slides)
• Media campaign interview video (four minutes)
• Training video (20 minutes)
• Trainer's outline
• Q&A (most commonly asked questions)
Table 5. Characteristics of surveyed women who received ECPduring the ECP demonstration project (total N = 235)
Characteristic % (95% CI)
Age
18-25 48.1 (41.7, 54.5)
26-30 26.4 (20.1, 32.0)
31+ 26.4 (20.8, 32.0)
Ethnicity
African-American 10.5 (6.6, 14.4)
Caucasian 46.5 (40.1, 52.9)
Hispanic/Latino 24.6 (19.1, 30.1)
Asian/Pacific Islander 7.9 (4.5, 11.3)
Other/Unknown 10.5 (6.6,14.4)
Education
High school or less 22.1 (16.8, 27.4)
Some college 45.5 (39.1, 51.9)
College + 32.3 (26.3, 38.3)
Marital status
Single 63.4 (57.2, 69.6)
Married 23.3 (17.9, 28.7)
Separated/divorced/widowed 13.4 (9.0, 17.8)
Prior live birth 43.4 (37.1, 49.7)
Prior abortion 46.8 (40.4, 53.2)
Prior ECP use 14.5 (10.0, 19.0)
Contraceptive method
None 30.2 (24.3, 36.1)
Condoms 50.6 (44.2, 57.0)
Oral contraceptives 11.9 (7.8, 16.0)
Diaphragm 4.2 (1.6, 6.8)
Depo-provera 2.2 (0.3, 4.1)
Other 4.2 (1.6, 6.8)
clin
ical
con
trib
uti
on
s

61The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
sessions took place at department meetings or spe-cially arranged education sessions. We presented acopy of a comprehensive clinical manual on ECP toeach participant and sent manuals to those unable toattend a presentation. The clinical manual providesdetailed information about ECP with specific recom-mendations for treatment, and a bibliography.
Making ECP Kits Available in Convenient Locations
We arranged to have ECP kits dispensed underphysician supervision in convenient locations withinthe San Diego Medical Center and at selected SanDiego medical office buildings. When a womancalled for advice and/or an appointment and thecall center determined that she wanted ECP, shewas directed to a screening/triage nurse, then toone of these locations to pick up an ECP Kit. Amessage was sent to the primary care provider toinform him/her of the request. If the provider or-dered an ECP kit, it was provided at the nurse’sstation or centralized nursing treatment centers inthe selected locations based on a physician ordergiven under a standard, written protocol that wasconsistent with California pharmacy law.
KP San Diego Pharmacy personnel stocked eachof the locations where ECP kits were provided andreplenished supplies when they ran out.
Packaging and Distribution of “Replication Packs”
We assumed from the beginning of the projectthat there would be interest in replicating theproject at other locations within KP as well as out-side KP. To facilitate replication, we developed a“Tool Kit,” whose contents are described in Table3. We arranged with a local printer to customizethe informational brochures, posters, and walletcards with information (eg logo, telephone num-bers) from the replication site. The printer has madethese materials available to those inside and out-side the organization.
We also developed the Training Toolbox (see Table 4for description of contents), consisting of the materialsa project manager would need to implement the projectfully in another site. The Toolbox included a videowritten by the project team, filmed at KP, and “starred”Dr Preskill and Debbie Postlethwaite, members of theproject team. Training Toolboxes have been distributedto the Chiefs of Obstetrics and Gynecology, FamilyMedicine, Internal Medicine, Pediatrics, and Pharmacyin all medical centers in all Regions of the KP Program(210 Toolboxes in all).
EvaluationBefore/After Survey of Provider Knowledgeand Practice
The evaluation included a pre/post survey of healthcare providers (physicians, NPs, CNMs, PACs in Depart-ments of Obstetrics and Gynecology, Family Medicine,Internal Medicine, Pediatrics, and Emergency Medicine)at baseline (September 1996, prior to training and avail-ability of ECP kits, and implementation of posters,HealthPhone messages, etc) and one year following fullimplementation (March 1998). Of 288 health care pro-viders who were asked to participate in the baselinesurvey, 164 (57%) completed it. The baseline surveyshowed that providers had a positive attitude about ECPbut that their knowledge of how to prescribe it was in-complete. Only one-third knew that treatment could beinitiated within 72 hours. Unavailability of a prepack-aged product was considered a barrier to provision ofECP by 90% of survey respondents.
A total of 101 providers responded both to thebaseline and follow-up survey, and showed improvedknowledge about ECP. Specific areas of significantlygreater knowledge included timing of doses for ECP,risk of teratogenic effects, rate of efficacy, mode ofaction, and contraindications. There were, however,no significant changes in global attitudes about ECPin respondents to both surveys.
Survey of Members Who Received an ECP KitDuring the Demonstration
Data were collected using structured telephone in-terviews conducted by trained female interviewersfrom January 1997 through February 1998. Eligible
Table 6. Sources of information about ECP for women who receivedECP during the demonstration project (N = 235)
Sources of information about ECP % (95% CI)
Kaiser Permanente materials (brochures, posters,Member Health News)
24.3 (18.8, 29.8)
Kaiser Permanente provider 19.1 (14.1, 24.1)
Friend or family member 17.2 (12.4, 22.0)
Newspapers, magazines, other media 11.6 (7.5, 15.7)
Kaiser Permanente staff 9.5 (5.8, 13.2)
Other 16.4 (11.7, 12.1)
Note: Total percentage exceeds 100.0 because women could report more than onesource of information.
... protocols ...ensured that
relevantinformationnecessary to
identify women forwhom EC was
contraindicatedwould be gathered
systematically.
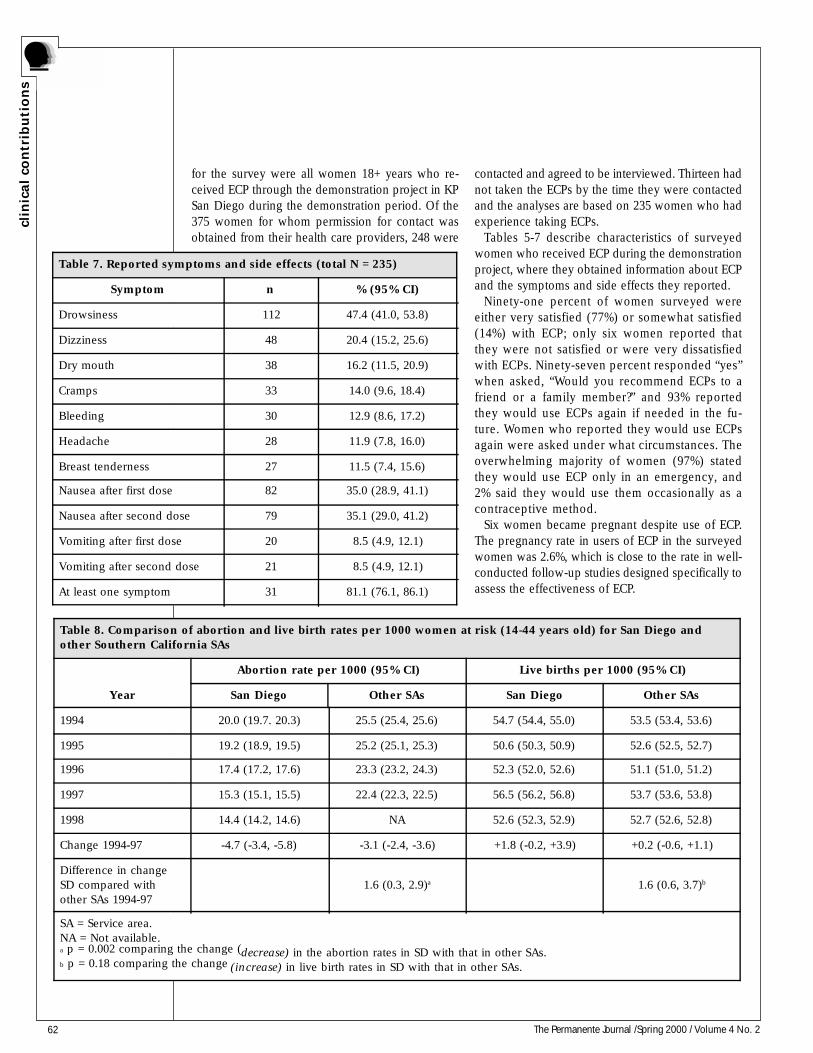
62 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
for the survey were all women 18+ years who re-ceived ECP through the demonstration project in KPSan Diego during the demonstration period. Of the375 women for whom permission for contact wasobtained from their health care providers, 248 were
contacted and agreed to be interviewed. Thirteen hadnot taken the ECPs by the time they were contactedand the analyses are based on 235 women who hadexperience taking ECPs.
Tables 5-7 describe characteristics of surveyedwomen who received ECP during the demonstrationproject, where they obtained information about ECPand the symptoms and side effects they reported.
Ninety-one percent of women surveyed wereeither very satisfied (77%) or somewhat satisfied(14%) with ECP; only six women reported thatthey were not satisfied or were very dissatisfiedwith ECPs. Ninety-seven percent responded “yes”when asked, “Would you recommend ECPs to afriend or a family member?” and 93% reportedthey would use ECPs again if needed in the fu-ture. Women who reported they would use ECPsagain were asked under what circumstances. Theoverwhelming majority of women (97%) statedthey would use ECP only in an emergency, and2% said they would use them occasionally as acontraceptive method.
Six women became pregnant despite use of ECP.The pregnancy rate in users of ECP in the surveyedwomen was 2.6%, which is close to the rate in well-conducted follow-up studies designed specifically toassess the effectiveness of ECP.
Table 8. Comparison of abortion and live birth rates per 1000 women at risk (14-44 years old) for San Diego andother Southern California SAs
Year
Abortion rate per 1000 (95% CI) Live births per 1000 (95% CI)
San Diego Other SAs San Diego Other SAs
1994 20.0 (19.7. 20.3) 25.5 (25.4, 25.6) 54.7 (54.4, 55.0) 53.5 (53.4, 53.6)
1995 19.2 (18.9, 19.5) 25.2 (25.1, 25.3) 50.6 (50.3, 50.9) 52.6 (52.5, 52.7)
1996 17.4 (17.2, 17.6) 23.3 (23.2, 24.3) 52.3 (52.0, 52.6) 51.1 (51.0, 51.2)
1997 15.3 (15.1, 15.5) 22.4 (22.3, 22.5) 56.5 (56.2, 56.8) 53.7 (53.6, 53.8)
1998 14.4 (14.2, 14.6) NA 52.6 (52.3, 52.9) 52.7 (52.6, 52.8)
Change 1994-97 -4.7 (-3.4, -5.8) -3.1 (-2.4, -3.6) +1.8 (-0.2, +3.9) +0.2 (-0.6, +1.1)
Difference in changeSD compared withother SAs 1994-97
1.6 (0.3, 2.9)a 1.6 (0.6, 3.7)b
SA = Service area.NA = Not available.a p = 0.002 comparing the change (decrease) in the abortion rates in SD with that in other SAs.b p = 0.18 comparing the change (increase) in live birth rates in SD with that in other SAs.
Table 7. Reported symptoms and side effects (total N = 235)
Symptom n % (95% CI)
Drowsiness 112 47.4 (41.0, 53.8)
Dizziness 48 20.4 (15.2, 25.6)
Dry mouth 38 16.2 (11.5, 20.9)
Cramps 33 14.0 (9.6, 18.4)
Bleeding 30 12.9 (8.6, 17.2)
Headache 28 11.9 (7.8, 16.0)
Breast tenderness 27 11.5 (7.4, 15.6)
Nausea after first dose 82 35.0 (28.9, 41.1)
Nausea after second dose 79 35.1 (29.0, 41.2)
Vomiting after first dose 20 8.5 (4.9, 12.1)
Vomiting after second dose 21 8.5 (4.9, 12.1)
At least one symptom 31 81.1 (76.1, 86.1)
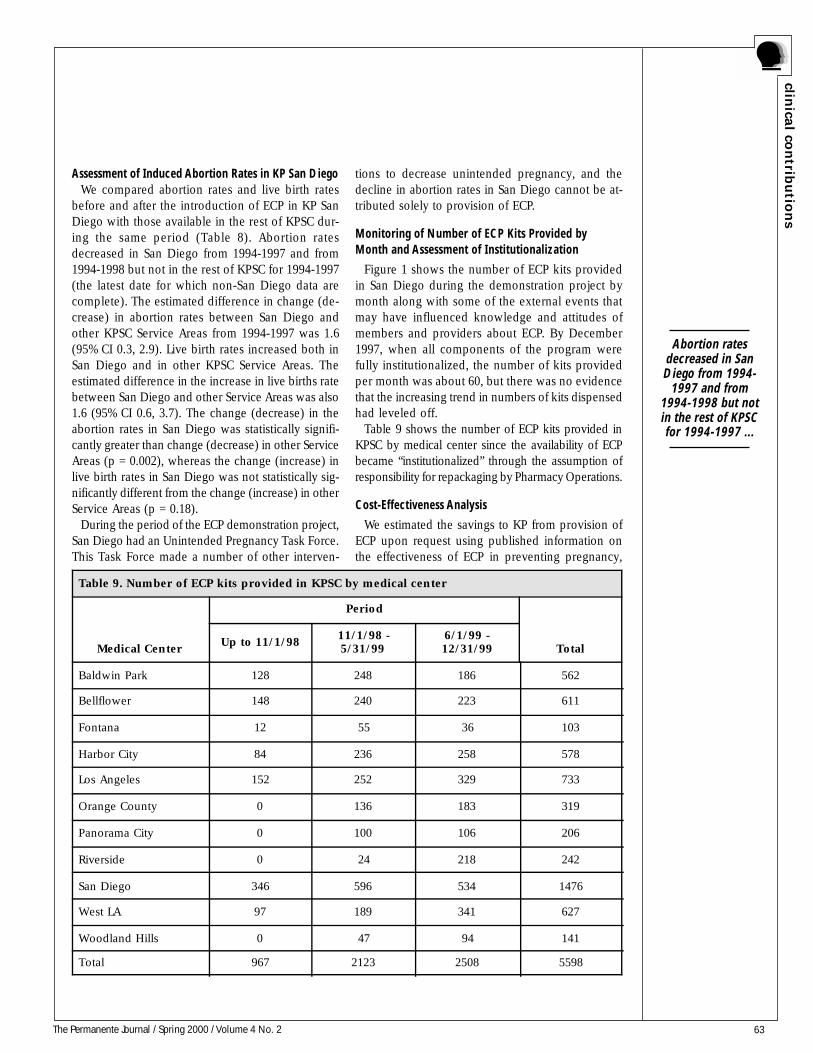
63The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
Assessment of Induced Abortion Rates in KP San DiegoWe compared abortion rates and live birth rates
before and after the introduction of ECP in KP SanDiego with those available in the rest of KPSC dur-ing the same period (Table 8). Abortion ratesdecreased in San Diego from 1994-1997 and from1994-1998 but not in the rest of KPSC for 1994-1997(the latest date for which non-San Diego data arecomplete). The estimated difference in change (de-crease) in abortion rates between San Diego andother KPSC Service Areas from 1994-1997 was 1.6(95% CI 0.3, 2.9). Live birth rates increased both inSan Diego and in other KPSC Service Areas. Theestimated difference in the increase in live births ratebetween San Diego and other Service Areas was also1.6 (95% CI 0.6, 3.7). The change (decrease) in theabortion rates in San Diego was statistically signifi-cantly greater than change (decrease) in other ServiceAreas (p = 0.002), whereas the change (increase) inlive birth rates in San Diego was not statistically sig-nificantly different from the change (increase) in otherService Areas (p = 0.18).
During the period of the ECP demonstration project,San Diego had an Unintended Pregnancy Task Force.This Task Force made a number of other interven-
tions to decrease unintended pregnancy, and thedecline in abortion rates in San Diego cannot be at-tributed solely to provision of ECP.
Monitoring of Number of ECP Kits Provided byMonth and Assessment of Institutionalization
Figure 1 shows the number of ECP kits providedin San Diego during the demonstration project bymonth along with some of the external events thatmay have influenced knowledge and attitudes ofmembers and providers about ECP. By December1997, when all components of the program werefully institutionalized, the number of kits providedper month was about 60, but there was no evidencethat the increasing trend in numbers of kits dispensedhad leveled off.
Table 9 shows the number of ECP kits provided inKPSC by medical center since the availability of ECPbecame “institutionalized” through the assumption ofresponsibility for repackaging by Pharmacy Operations.
Cost-Effectiveness Analysis
We estimated the savings to KP from provision ofECP upon request using published information onthe effectiveness of ECP in preventing pregnancy,
Table 9. Number of ECP kits provided in KPSC by medical center
Medical Center
Period
TotalUp to 11/1/98
11/1/98 -5/31/99
6/1/99 -12/31/99
Baldwin Park 128 248 186 562
Bellflower 148 240 223 611
Fontana 12 55 36 103
Harbor City 84 236 258 578
Los Angeles 152 252 329 733
Orange County 0 136 183 319
Panorama City 0 100 106 206
Riverside 0 24 218 242
San Diego 346 596 534 1476
West LA 97 189 341 627
Woodland Hills 0 47 94 141
Total 967 2123 2508 5598
Abortion ratesdecreased in SanDiego from 1994-
1997 and from1994-1998 but notin the rest of KPSCfor 1994-1997 ...
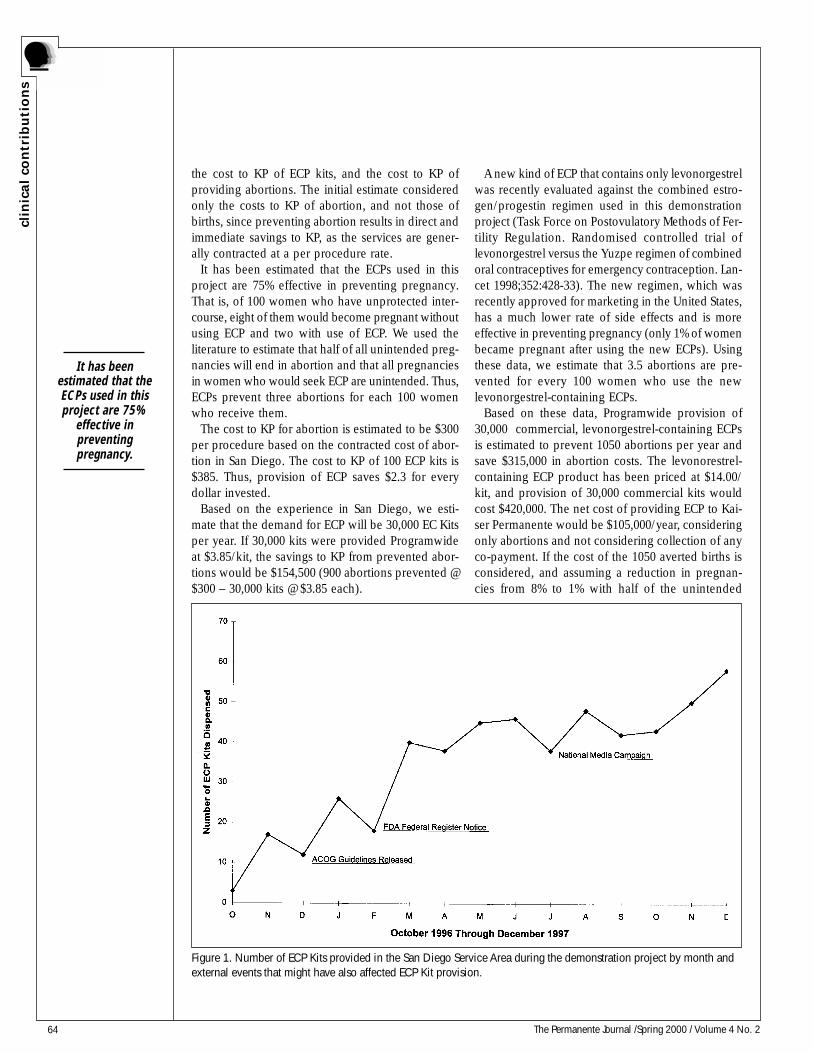
64 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
the cost to KP of ECP kits, and the cost to KP ofproviding abortions. The initial estimate consideredonly the costs to KP of abortion, and not those ofbirths, since preventing abortion results in direct andimmediate savings to KP, as the services are gener-ally contracted at a per procedure rate.
It has been estimated that the ECPs used in thisproject are 75% effective in preventing pregnancy.That is, of 100 women who have unprotected inter-course, eight of them would become pregnant withoutusing ECP and two with use of ECP. We used theliterature to estimate that half of all unintended preg-nancies will end in abortion and that all pregnanciesin women who would seek ECP are unintended. Thus,ECPs prevent three abortions for each 100 womenwho receive them.
The cost to KP for abortion is estimated to be $300per procedure based on the contracted cost of abor-tion in San Diego. The cost to KP of 100 ECP kits is$385. Thus, provision of ECP saves $2.3 for everydollar invested.
Based on the experience in San Diego, we esti-mate that the demand for ECP will be 30,000 EC Kitsper year. If 30,000 kits were provided Programwideat $3.85/kit, the savings to KP from prevented abor-tions would be $154,500 (900 abortions prevented @$300 – 30,000 kits @ $3.85 each).
A new kind of ECP that contains only levonorgestrelwas recently evaluated against the combined estro-gen/progestin regimen used in this demonstrationproject (Task Force on Postovulatory Methods of Fer-tility Regulation. Randomised controlled trial oflevonorgestrel versus the Yuzpe regimen of combinedoral contraceptives for emergency contraception. Lan-cet 1998;352:428-33). The new regimen, which wasrecently approved for marketing in the United States,has a much lower rate of side effects and is moreeffective in preventing pregnancy (only 1% of womenbecame pregnant after using the new ECPs). Usingthese data, we estimate that 3.5 abortions are pre-vented for every 100 women who use the newlevonorgestrel-containing ECPs.
Based on these data, Programwide provision of30,000 commercial, levonorgestrel-containing ECPsis estimated to prevent 1050 abortions per year andsave $315,000 in abortion costs. The levonorestrel-containing ECP product has been priced at $14.00/kit, and provision of 30,000 commercial kits wouldcost $420,000. The net cost of providing ECP to Kai-ser Permanente would be $105,000/year, consideringonly abortions and not considering collection of anyco-payment. If the cost of the 1050 averted births isconsidered, and assuming a reduction in pregnan-cies from 8% to 1% with half of the unintended
Figure 1. Number of ECP Kits provided in the San Diego Service Area during the demonstration project by month andexternal events that might have also affected ECP Kit provision.
It has beenestimated that theECPs used in thisproject are 75%
effective inpreventingpregnancy.

65The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
pregnancies resulting in abortion and half in birth,provision of commercial ECP at $14.00/kit will becost-saving as long as the cost of births to KP ex-ceeds $100 per birth.
Institutionalization, Replication and Dissemination
The repackaging of oral contraceptives has been“institutionalized,” and the ECP kits that were devel-oped and piloted in the project are now availablethroughout the KP program. The project has beenreplicated throughout KPSC, and ECP is available andbeing provided in all Service Areas in KPSC.
The Toolbox developed in the project was distrib-uted to Chiefs of Obstetrics and Gynecology, FamilyMedicine, Internal Medicine, Pediatrics, and Pharmacyin all Regions of KP throughout the KP Program.Altogether, 210 Toolboxes were distributed.
Over 200 tool kits, which have been made availableat cost to persons outside KP, have been distributedoutside KP. Over 100 toolboxes, also made availableat cost to persons outside Kaiser Permanente, havebeen distributed.
ConclusionThe objectives of the ECP Research and Demon-
stration Project were achieved. The project showedthe feasibility and acceptability of providing ECP di-rectly to women within KP. Providers exposed toproject materials increased their knowledge about
the correct use of ECP. ECP was delivered to womenin San Diego through the project. Women who re-ceived ECP were highly satisfied with this service.There was some evidence that abortion rates de-creased more in San Diego than in other Service Areasin KPSC, although this change cannot be attributedsolely to provision of ECP.
The repackaging of oral contraceptives was “insti-tutionalized” in KP San Diego and the ECP kits thatwere developed and piloted in the project are nowavailable throughout the KP program. The programhas been replicated throughout KPSC, and ECP areavailable and being provided in all KPSC ServiceAreas. Toolboxes, which contain all of the materialsto replicate the project, have been distributed through-out the Program. A cost analysis showed that provi-sion of ECP would be cost-saving to KP even if acommercial product were substituted for the ECP kitsused in this project. ❖
Publications
Petitti DB, Harvey SM, Preskill D, Beckman LJ, Postlethwaite D,
Switzky H, Sherman C. Emergency contraception: preliminary re-
port of a demonstration and evaluation project. J Am Med Womens
Assoc 1998;53(5 Suppl 2):251-4.
Harvey SM, Beckman LJ, Sherman C, Petitti D. Women’s experi-
ence and satisfaction with emergency contraception. Fam Plann
Perspect 1999:31:237-240, 260.
Find YourselfI expect that along the way you’ll uncover lost and
forgotten pieces of yourself that have been buried likevalleys filled in by years of accumulating snow.
Richard Stone, “The Healing Art of Storytelling”
The projectshowed the
feasibility andacceptability ofproviding ECP
directly to womenwithin KP.

66 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s The Breast Health and Cancer Detection Program
IntroductionThe Kaiser Permanente (KP) Georgia Region,
which includes The Southeast Permanente MedicalGroup (TSPMG) and Kaiser Foundation Health Plan(KFHP) of Georgia implemented its Breast Healthand Cancer Detection Program in November of 1994,when the organization’s Interdisciplinary PreventionCommittee (IPC) prevention priority was set as breastcancer screening.
BackgroundThe IPC was initiated as a part of the Quality Fo-
rum (the KP Georgia Region Quality ImprovementCommittee) in late 1994. A charge of IPC was to iden-tify priorities for quality improvement in preventivehealth services. The IPC conducted a review of sci-entific literature and considered both national andstate health initiatives in considering what servicesto establish as priorities. The IPC also consideredareas where low-cost interventions might achieve KPRegional goals to enable the Georgia Region to be-come a leader in delivery of medical care as measuredby HEDIS effectiveness-of-care measures.
Breast cancer is the leading cause of deaths in women aged 15-64 years: 48% of newbreast cancers and 56% of all breast cancer deaths occur in women aged 65 years and older. TheKaiser Permanente Georgia Region’s Breast Health and Cancer Detection Program, implementedin 1997, combines inreach and outreach activities designed to improve member access to breastcancer screening services as well as practitioner awareness for timely screening according topractice guidelines. The Program targets women aged 50 years and older. Inreach and outreachactivities implemented to improve access to mammography services included Saturday appoint-ments, van transportation of patients from centers without mammography services, self-referraland walk-in process, and adding mammography machines at high-use medical offices. Memberand provider educational and awareness activities included inserting colored chart remindersfor patients due for a mammogram; placing preventive service wall charts in exam rooms; estab-lishing a Radiology-based mammography tracking system to monitor and follow up patients withabnormal clinical breast exams or mammograms; conducting Call Center telephone outreach tocontact women aged 52-69 years past due for a mammogram; mailing postcard reminders and abrochure on clinical practice guidelines; and providing financial incentives to the health careteam (HCT) for improving screening rates and quarterly reporting of HCT results.
Measurable impact of the Program is reflected in the mammography screening rates (aged 52-69 years) based on HEDIS specifications: 1996 = 73.8%, 1997 = 74.5%, 1998 = 80.6%, 1999 = 84.3%. Theobserved improvement in mammography screening rates for the period 1996-99 was statistically sig-nificant (p < 0.0001). The Georgia Region’s 1997 performance for HEDIS breast cancer screening mea-sure was the second lowest in the Program. Its 1998 performance was among the top four KP Regions,and for 1999 was again among the top 10%. The interventions employed in this Program are common inmany KP Regions but with varying degrees of success. For example, in the Georgia Region, Call Centertelephone outreach to contact women aged 52-69 years who are past due for a mammogram was one ofthe most successful outreach methods, whereas the mobile mammography van outreach was the least
successful activity. Our practice results are trans-ferable among KP Regions but could show vary-ing results depending on how implemented.
Table 1. Team members for KP Georgia Region's Breast Health andCancer Detection Program
Program leaders:Adrienne Mims, MD, MPH, Chief of Prevention and Health Promotion,TSPMG; Leslie Litton, Director, Allied Health Services, KFHPProgram sponsors:Marcia Thompson, MD, Chief, Department of Radiology, TSPMG; DennisTolsma, MPH, Director, Clinical Quality Improvement, KFHPPatient Education Coordinator:Kecia Leatherwood, MS, Prevention and Health Promotion, KFHPBreast cancer screening work group members:Donna Deckard, Associate Manager, Health Care Operations, KFHP; DebraCarlton, MD, Associate Medical Director, Primary Care, TSPMG; CarrieSprenkle, RN, Quality Project Coordinator, Affiliated Care, TSPMG; LaurenPerkins, Outcomes Measurement Analyst, KFHP; Judy Griffith, RN, MS,Maternal Child Health Coordinator, Obstetrics/Gynecology, KFHP; ToniBest, RN, Advice Nurse Supervisor, Call Center, KFHP; Martha Wilber, MD,Chief, Department of Medicine, TSPMG (1995-98); Mark Hackman, MD,Chief, Department of Medicine, TSPMG (1999); Daria Fluker, RadiologySupervisor, Southwood Office, KFHP; Gail Kraft, Clinical InformationSystems Analyst, KFHPInterdisciplinary Prevention Committee (IPC) Contact Person:Thomas M. Judd, MS, PE, CCE, CPHQ Director, Quality Assessment,Improvement, and Reporting, Kaiser Permanente Georgia RegionNine Piedmont Center3495 Piedmont Road, NEAtlanta, GA 30305-1736
Georgia Region

67The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
Breast cancer screening was selected as a top-tenpriority for guideline development and for additionalintervention. Breast cancer will develop in one ofevery eight American women in her lifetime. Breastcancer is the leading cause of cancer deaths in womenaged 15 to 64 years. Forty-eight percent of new breastcancer cases and 56% of all breast cancer deaths oc-cur in women aged 65 years and older. Breast canceris most treatable and curable when it is found early,and the key to early detection is screening.
The national HEDIS result of 71%, reported in May1995, provided our baseline performance measure-ment. This result fell short of our goal of being in the90th percentile of performance on this and severalother HEDIS effectiveness-of-care measures.
In August 1995, the Quality Forum accepted theIPC recommendations, endorsed by the Departmentof Medicine, which emphasized the importance ofannual clinical breast examination and mammogra-phy for women of targeted age groups. In Novem-ber 1997, a new Excellence in Quality (EIQ) HEDISImprovement Team began work. Its charge was toundertake analyses of underlying causes of reducedperformance and to develop additional steps to im-pact yearend 1997 performance and for incorpora-tion into care delivery processes in 1998. In March1998, the Quality Forum Executive Committee des-ignated breast cancer screening one of the six orga-nizational quality priorities for 1998 and designated“owners” who would be accountable for this per-formance—the Chief of Radiology and the Directorof Radiology. At that time, the KP Georgia Region’sClinical Affairs Division designated mammographyas one of four priorities for improvement by thelocal Implementation Team—a collaborative effortwith KP’s Care Management Institute.
Program ObjectivesOne objective of the Breast Health and Cancer
Detection Program has been to assist our mem-bers and practitioners with information and treat-ment to facilitate adherence to practices that pro-mote early detection of potential breast cancer. Thesecond objective of the Program has been to sus-tain measurable improvement in the screening ratesto a level that meets or exceeds the 90th percentileof HEDIS breast cancer screening rates as reportedin Quality Compass.1
Program activities were implemented in 1997. The1996 screening rate therefore served as a baselinerate. If the program activities were efficacious in
increasing and sustaining the screening rate, thenthe 1999 rate could be expected to be much greaterthan the 1996 rate; and the screening rates shouldexhibit a trend of increasing rates from 1996 through1999. On the basis of the current screening rates,we expected to meet or exceed projected rates.
For the sample size used to calculate each year’smammography screening rate, we used administra-tive data only to calculate the screening rate. We didnot select samples: thus, 100% of the eligible popu-lation was used to calculate rates.
Thus, the 1999 predicted rate was developed byusing a simple linear projection from historical rates(Table 2). Yearend 1999 actual data showed a mam-mography screening rate of 84.3% (confirming thepredicted rate; not a statistically significant differencefrom 1998).
Program DescriptionThe EIQ’s designated Breast Cancer Screening Work
Group, in cooperation with the IPC, the Implemen-tation Team, and under the general direction of theQuality Forum, have implemented a broad array ofactivities to improve breast cancer screening rates.These activities have been intended to improve mem-ber access to screening services, member andpractitioner awareness for timely screening, and prac-titioner adherence to screening guidelines.
Improving Member AccessAccess was considered on the basis of 1996 HEDIS
results to be a key barrier to improved performance.The IPC Continuous Quality Improvement team (IPC/CQI) was convened in May 1997 to discuss ways toincrease access to mammography. Saturday hours andmobile mammography were identified as potentialactivities to overcome access barriers.
A mobile mammography pilot study was conductedin December 1997. Although 60 women werescreened and two previously undetected cancers werefound, the mobile mammography program was dis-continued because of mammogram quality problemsthat led to increased patient callbacks.
In November 1997, the EIQ recommended analy-sis of scheduling backlogs greater than threemonths that began the same month. Call Centerstaff examined wait lists, and primary care opera-tions began to provide backfill staffing to allowpractitioners with the longest wait lists to provideexaminations, including clinical breast examinationand referral to mammography.
Breast cancer ismost treatable andcurable when it isfound early, andthe key to early
detection isscreening.
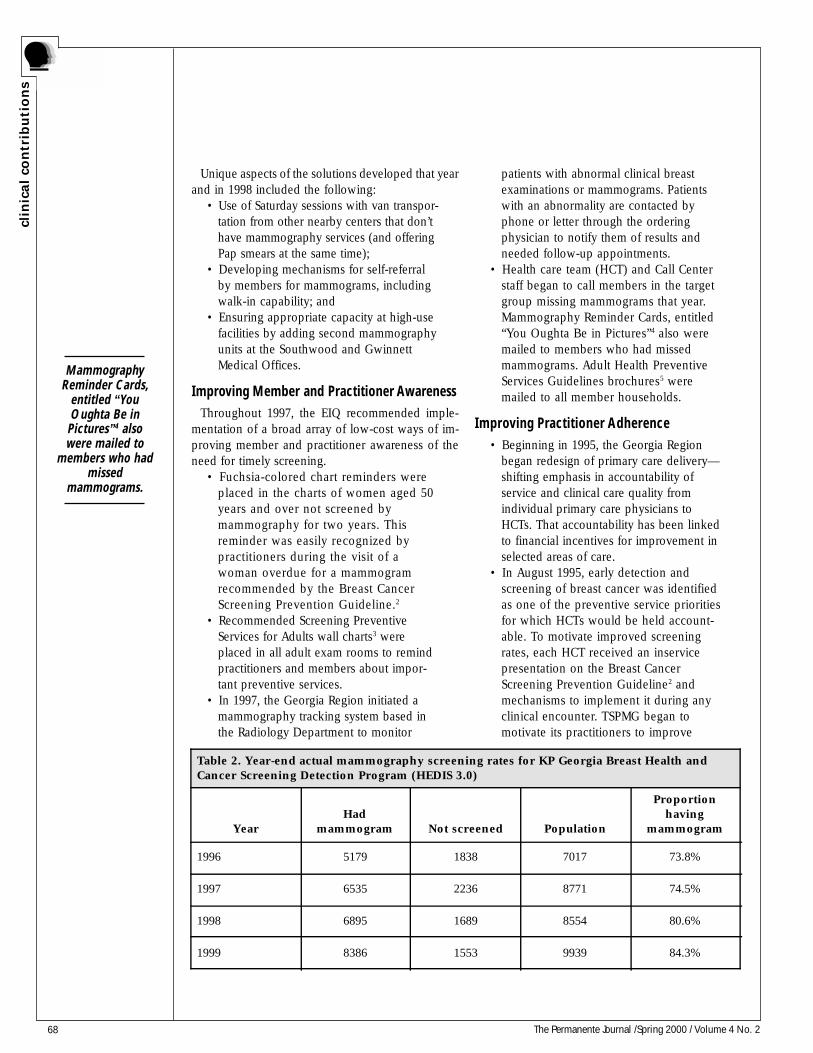
68 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
Unique aspects of the solutions developed that yearand in 1998 included the following:
• Use of Saturday sessions with van transpor-tation from other nearby centers that don’thave mammography services (and offeringPap smears at the same time);
• Developing mechanisms for self-referralby members for mammograms, includingwalk-in capability; and
• Ensuring appropriate capacity at high-usefacilities by adding second mammographyunits at the Southwood and GwinnettMedical Offices.
Improving Member and Practitioner AwarenessThroughout 1997, the EIQ recommended imple-
mentation of a broad array of low-cost ways of im-proving member and practitioner awareness of theneed for timely screening.
• Fuchsia-colored chart reminders wereplaced in the charts of women aged 50years and over not screened bymammography for two years. Thisreminder was easily recognized bypractitioners during the visit of awoman overdue for a mammogramrecommended by the Breast CancerScreening Prevention Guideline.2
• Recommended Screening PreventiveServices for Adults wall charts3 wereplaced in all adult exam rooms to remindpractitioners and members about impor-tant preventive services.
• In 1997, the Georgia Region initiated amammography tracking system based inthe Radiology Department to monitor
patients with abnormal clinical breastexaminations or mammograms. Patientswith an abnormality are contacted byphone or letter through the orderingphysician to notify them of results andneeded follow-up appointments.
• Health care team (HCT) and Call Centerstaff began to call members in the targetgroup missing mammograms that year.Mammography Reminder Cards, entitled“You Oughta Be in Pictures”4 also weremailed to members who had missedmammograms. Adult Health PreventiveServices Guidelines brochures5 weremailed to all member households.
Improving Practitioner Adherence• Beginning in 1995, the Georgia Region
began redesign of primary care delivery—shifting emphasis in accountability ofservice and clinical care quality fromindividual primary care physicians toHCTs. That accountability has been linkedto financial incentives for improvement inselected areas of care.
• In August 1995, early detection andscreening of breast cancer was identifiedas one of the preventive service prioritiesfor which HCTs would be held account-able. To motivate improved screeningrates, each HCT received an inservicepresentation on the Breast CancerScreening Prevention Guideline2 andmechanisms to implement it during anyclinical encounter. TSPMG began tomotivate its practitioners to improve
Table 2. Year-end actual mammography screening rates for KP Georgia Breast Health andCancer Screening Detection Program (HEDIS 3.0)
YearHad
mammogram Not screened Population
Proportionhaving
mammogram
1996 5179 1838 7017 73.8%
1997 6535 2236 8771 74.5%
1998 6895 1689 8554 80.6%
1999 8386 1553 9939 84.3%
MammographyReminder Cards,
entitled “YouOughta Be inPictures”4 alsowere mailed to
members who hadmissed
mammograms.
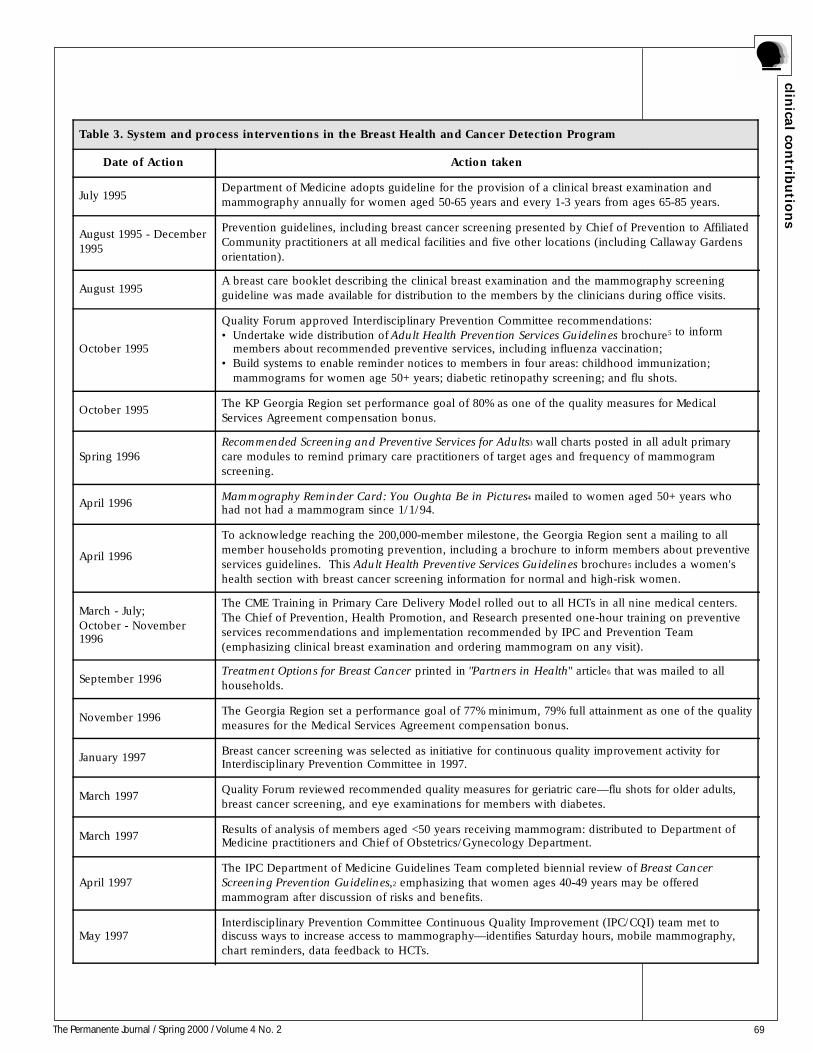
69The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
Table 3. System and process interventions in the Breast Health and Cancer Detection Program
Date of Action Action taken
July 1995Department of Medicine adopts guideline for the provision of a clinical breast examination andmammography annually for women aged 50-65 years and every 1-3 years from ages 65-85 years.
August 1995 - December1995
Prevention guidelines, including breast cancer screening presented by Chief of Prevention to AffiliatedCommunity practitioners at all medical facilities and five other locations (including Callaway Gardensorientation).
August 1995A breast care booklet describing the clinical breast examination and the mammography screeningguideline was made available for distribution to the members by the clinicians during office visits.
October 1995
Quality Forum approved Interdisciplinary Prevention Committee recommendations:• Undertake wide distribution of Adult Health Prevention Services Guidelines brochure5 to inform
members about recommended preventive services, including influenza vaccination;• Build systems to enable reminder notices to members in four areas: childhood immunization; mammograms for women age 50+ years; diabetic retinopathy screening; and flu shots.
October 1995The KP Georgia Region set performance goal of 80% as one of the quality measures for MedicalServices Agreement compensation bonus.
Spring 1996Recommended Screening and Preventive Services for Adults3 wall charts posted in all adult primarycare modules to remind primary care practitioners of target ages and frequency of mammogramscreening.
April 1996Mammography Reminder Card: You Oughta Be in Pictures4 mailed to women aged 50+ years whohad not had a mammogram since 1/1/94.
April 1996
To acknowledge reaching the 200,000-member milestone, the Georgia Region sent a mailing to allmember households promoting prevention, including a brochure to inform members about preventiveservices guidelines. This Adult Health Preventive Services Guidelines brochure5 includes a women'shealth section with breast cancer screening information for normal and high-risk women.
March - July;October - November1996
The CME Training in Primary Care Delivery Model rolled out to all HCTs in all nine medical centers.The Chief of Prevention, Health Promotion, and Research presented one-hour training on preventiveservices recommendations and implementation recommended by IPC and Prevention Team(emphasizing clinical breast examination and ordering mammogram on any visit).
September 1996Treatment Options for Breast Cancer printed in "Partners in Health" article6 that was mailed to allhouseholds.
November 1996The Georgia Region set a performance goal of 77% minimum, 79% full attainment as one of the qualitymeasures for the Medical Services Agreement compensation bonus.
January 1997Breast cancer screening was selected as initiative for continuous quality improvement activity forInterdisciplinary Prevention Committee in 1997.
March 1997Quality Forum reviewed recommended quality measures for geriatric care—flu shots for older adults,breast cancer screening, and eye examinations for members with diabetes.
March 1997Results of analysis of members aged <50 years receiving mammogram: distributed to Department ofMedicine practitioners and Chief of Obstetrics/Gynecology Department.
April 1997The IPC Department of Medicine Guidelines Team completed biennial review of Breast CancerScreening Prevention Guidelines,2 emphasizing that women ages 40-49 years may be offeredmammogram after discussion of risks and benefits.
May 1997Interdisciplinary Prevention Committee Continuous Quality Improvement (IPC/CQI) team met todiscuss ways to increase access to mammography—identifies Saturday hours, mobile mammography,chart reminders, data feedback to HCTs.
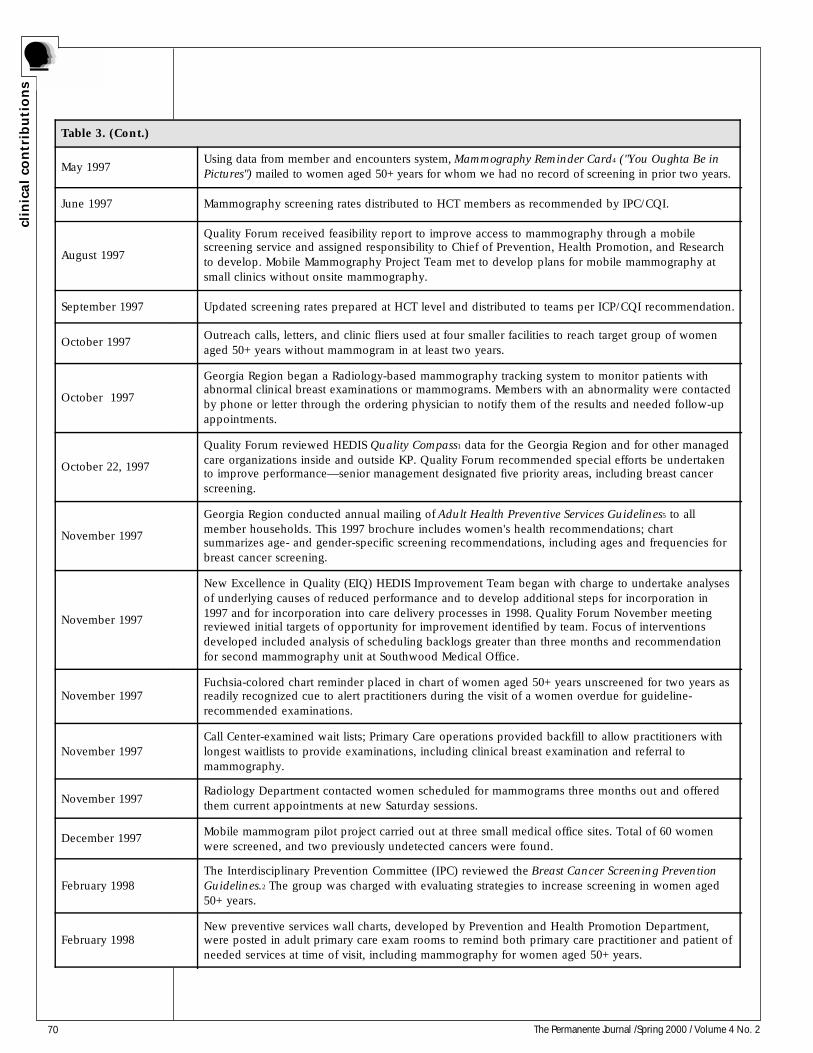
70 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
Table 3. (Cont.)
May 1997Using data from member and encounters system, Mammography Reminder Card4 ("You Oughta Be inPictures") mailed to women aged 50+ years for whom we had no record of screening in prior two years.
June 1997 Mammography screening rates distributed to HCT members as recommended by IPC/CQI.
August 1997
Quality Forum received feasibility report to improve access to mammography through a mobilescreening service and assigned responsibility to Chief of Prevention, Health Promotion, and Researchto develop. Mobile Mammography Project Team met to develop plans for mobile mammography atsmall clinics without onsite mammography.
September 1997 Updated screening rates prepared at HCT level and distributed to teams per ICP/CQI recommendation.
October 1997Outreach calls, letters, and clinic fliers used at four smaller facilities to reach target group of womenaged 50+ years without mammogram in at least two years.
October 1997
Georgia Region began a Radiology-based mammography tracking system to monitor patients withabnormal clinical breast examinations or mammograms. Members with an abnormality were contactedby phone or letter through the ordering physician to notify them of the results and needed follow-upappointments.
October 22, 1997
Quality Forum reviewed HEDIS Quality Compass1 data for the Georgia Region and for other managedcare organizations inside and outside KP. Quality Forum recommended special efforts be undertakento improve performance—senior management designated five priority areas, including breast cancerscreening.
November 1997
Georgia Region conducted annual mailing of Adult Health Preventive Services Guidelines5 to allmember households. This 1997 brochure includes women's health recommendations; chartsummarizes age- and gender-specific screening recommendations, including ages and frequencies forbreast cancer screening.
November 1997
New Excellence in Quality (EIQ) HEDIS Improvement Team began with charge to undertake analysesof underlying causes of reduced performance and to develop additional steps for incorporation in1997 and for incorporation into care delivery processes in 1998. Quality Forum November meetingreviewed initial targets of opportunity for improvement identified by team. Focus of interventionsdeveloped included analysis of scheduling backlogs greater than three months and recommendationfor second mammography unit at Southwood Medical Office.
November 1997Fuchsia-colored chart reminder placed in chart of women aged 50+ years unscreened for two years asreadily recognized cue to alert practitioners during the visit of a women overdue for guideline-recommended examinations.
November 1997Call Center-examined wait lists; Primary Care operations provided backfill to allow practitioners withlongest waitlists to provide examinations, including clinical breast examination and referral tomammography.
November 1997Radiology Department contacted women scheduled for mammograms three months out and offeredthem current appointments at new Saturday sessions.
December 1997Mobile mammogram pilot project carried out at three small medical office sites. Total of 60 womenwere screened, and two previously undetected cancers were found.
February 1998The Interdisciplinary Prevention Committee (IPC) reviewed the Breast Cancer Screening PreventionGuidelines.2 The group was charged with evaluating strategies to increase screening in women aged50+ years.
February 1998New preventive services wall charts, developed by Prevention and Health Promotion Department,were posted in adult primary care exam rooms to remind both primary care practitioner and patient ofneeded services at time of visit, including mammography for women aged 50+ years.
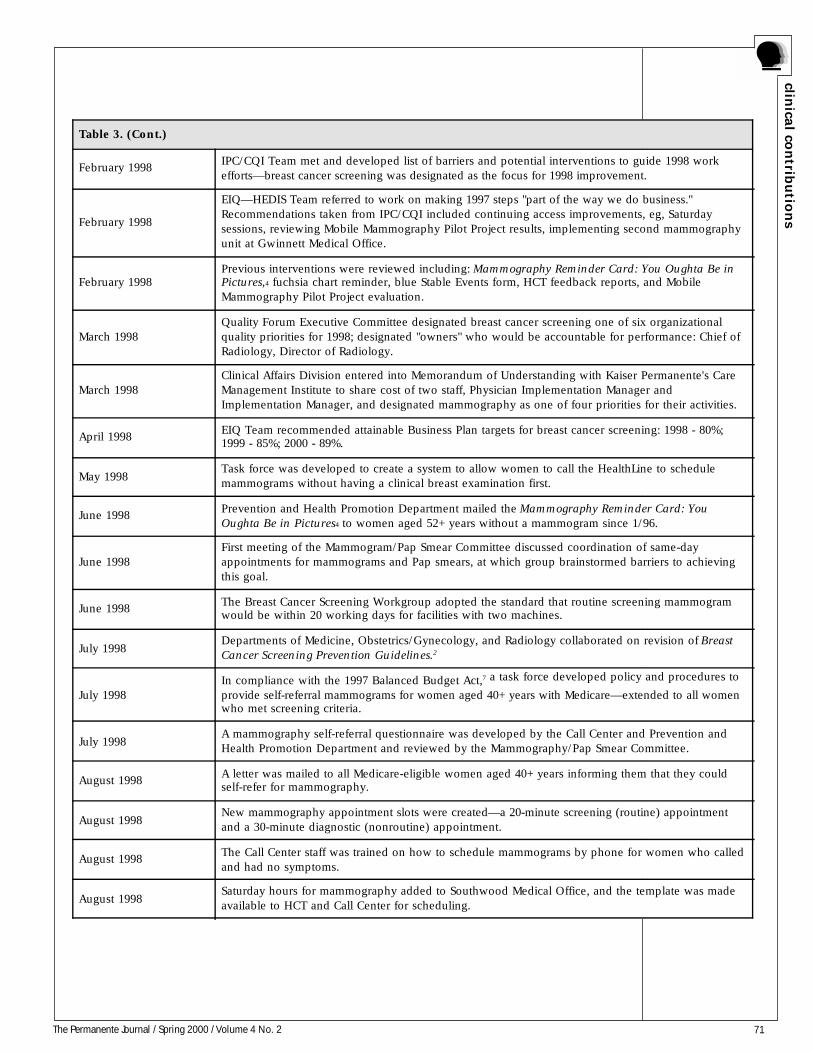
71The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
Table 3. (Cont.)
February 1998IPC/CQI Team met and developed list of barriers and potential interventions to guide 1998 workefforts—breast cancer screening was designated as the focus for 1998 improvement.
February 1998
EIQ—HEDIS Team referred to work on making 1997 steps "part of the way we do business."Recommendations taken from IPC/CQI included continuing access improvements, eg, Saturdaysessions, reviewing Mobile Mammography Pilot Project results, implementing second mammographyunit at Gwinnett Medical Office.
February 1998Previous interventions were reviewed including: Mammography Reminder Card: You Oughta Be inPictures,4 fuchsia chart reminder, blue Stable Events form, HCT feedback reports, and MobileMammography Pilot Project evaluation.
March 1998Quality Forum Executive Committee designated breast cancer screening one of six organizationalquality priorities for 1998; designated "owners" who would be accountable for performance: Chief ofRadiology, Director of Radiology.
March 1998Clinical Affairs Division entered into Memorandum of Understanding with Kaiser Permanente's CareManagement Institute to share cost of two staff, Physician Implementation Manager andImplementation Manager, and designated mammography as one of four priorities for their activities.
April 1998EIQ Team recommended attainable Business Plan targets for breast cancer screening: 1998 - 80%;1999 - 85%; 2000 - 89%.
May 1998Task force was developed to create a system to allow women to call the HealthLine to schedulemammograms without having a clinical breast examination first.
June 1998Prevention and Health Promotion Department mailed the Mammography Reminder Card: YouOughta Be in Pictures4 to women aged 52+ years without a mammogram since 1/96.
June 1998First meeting of the Mammogram/Pap Smear Committee discussed coordination of same-dayappointments for mammograms and Pap smears, at which group brainstormed barriers to achievingthis goal.
June 1998The Breast Cancer Screening Workgroup adopted the standard that routine screening mammogramwould be within 20 working days for facilities with two machines.
July 1998Departments of Medicine, Obstetrics/Gynecology, and Radiology collaborated on revision of BreastCancer Screening Prevention Guidelines.2
July 1998In compliance with the 1997 Balanced Budget Act,7 a task force developed policy and procedures to
provide self-referral mammograms for women aged 40+ years with Medicare—extended to all womenwho met screening criteria.
July 1998A mammography self-referral questionnaire was developed by the Call Center and Prevention andHealth Promotion Department and reviewed by the Mammography/Pap Smear Committee.
August 1998A letter was mailed to all Medicare-eligible women aged 40+ years informing them that they couldself-refer for mammography.
August 1998New mammography appointment slots were created—a 20-minute screening (routine) appointmentand a 30-minute diagnostic (nonroutine) appointment.
August 1998The Call Center staff was trained on how to schedule mammograms by phone for women who calledand had no symptoms.
August 1998Saturday hours for mammography added to Southwood Medical Office, and the template was madeavailable to HCT and Call Center for scheduling.

72 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
Table 3. (Cont.)
August 1998
IPC recommended orange (instead of fuchsia) chart reminders be placed in charts of unscreenedwomen aged 52+ years as a readily recognized cue to alert practitioners during the visit of a womanoverdue for guideline-recommended examinations. Prevention and Health Promotion Departmentdeveloped chart reminder and implemented process for reminders to be placed in medical records.
August 1998Call Center began outreach calls to women aged 52+ who had not had a mammogram since 1/1/95and scheduled mammograms during that call.
August 1998Prevention and Health Promotion Department supplied Obstetrics/Gynecology Department with adultprevention wall charts that were placed in all exam rooms.
September 1998Call Center staff began reminder calls to women scheduled for mammograms at Southwood, Glenlakeand Crescent Center Medical Offices to decrease the no-show rate.
September - December1998
Obstetrics/Gynecology Department held twice-monthly Women's Health Day on Saturdays, whenwomen had both Pap smear and mammogram (if indicated).
October 1998New Regionwide monthly e-mail newsletter, Ounce of Prevention8 featured the revised Breast CancerScreening Prevention Guidelines.2
October 1998Medical center staff placed posters promoting breast health and wore pins in celebration of BreastCancer Awareness Month.9
October 1998The Breast Health and Cancer Detection10 brochure was revised and printed by Prevention and HealthPromotion Department, then made available to HCTs for module distribution.
October 1998Adult Health Preventive Care Services Guidelines11 brochure was revised, printed, and mailed to all
subscriber households. The brochure includes reminders about frequency of mammography.
October 1998Procedure developed to expedite referral process for affiliated care members when contacted throughCall Center outreach efforts.
November 1998At the Affiliated Practitioners Advisory Council meeting, the Adult Health Preventive Care ServicesGuidelines11 mailer and the Healthwise Handbook12 were introduced, both of which include the
mammogram guidelines.
November 1998HEDIS mammogram results, goals, and the mammogram chart reminders were discussed at theAffiliated Practitioner Advisory Council Meeting, and practitioners were invited to participate in theguideline revisions.
November 1998 Affiliated Network chart data were abstracted to augment the administrative data.
November 1998Chart reminders were inserted into all Affiliated Care charts that did not contain evidence of aguideline-recommended mammogram.
November 1998Analysis of phone outreach calls and feedback from clinicians determined that some women in ourtarget group identified by our administrative records did have a mammogram within the last twoyears. A chart review was authorized to validate the negative administrative data at some sites.
November 21, 1998
Mammography Days event was held at Southwood Medical Office for Cascade female memberswithout transportation. Eligible women were transported by van to the facility on a Saturday toreceive mammogram and Pap smear if needed. Because of short notice of scheduling, only fourwomen took advantage of this service.
December 1998Call Center outreach to women aged 52+ years without a mammogram since 1/1/95 was extended tothe Affiliated Care members.
December 1998Primary care practitioner-specific 8/98 year-to-date performance rates for Pap smears, mammography,and diabetes retinopathy screening were provided to each physician in Adult Medicine Department.
December 1998 A mammography machine began service at Gwinnett Medical Office.
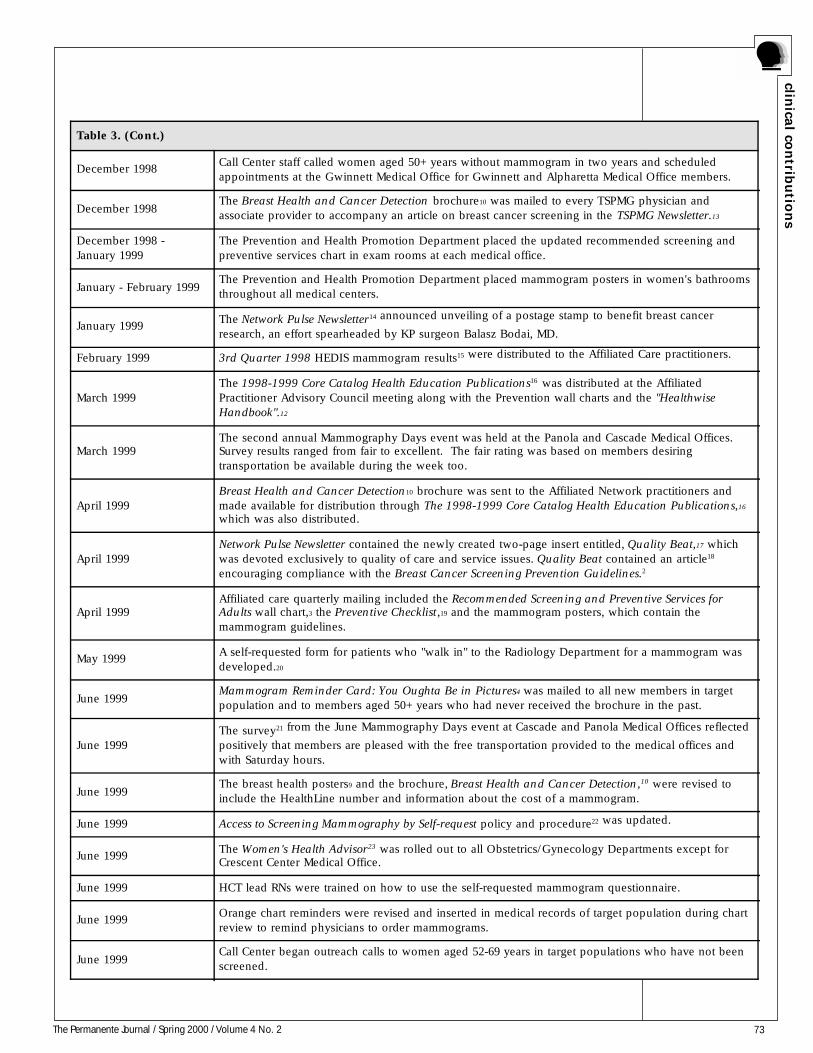
73The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
Table 3. (Cont.)
December 1998Call Center staff called women aged 50+ years without mammogram in two years and scheduledappointments at the Gwinnett Medical Office for Gwinnett and Alpharetta Medical Office members.
December 1998The Breast Health and Cancer Detection brochure10 was mailed to every TSPMG physician andassociate provider to accompany an article on breast cancer screening in the TSPMG Newsletter.13
December 1998 -January 1999
The Prevention and Health Promotion Department placed the updated recommended screening andpreventive services chart in exam rooms at each medical office.
January - February 1999The Prevention and Health Promotion Department placed mammogram posters in women's bathroomsthroughout all medical centers.
January 1999The Network Pulse Newsletter14 announced unveiling of a postage stamp to benefit breast cancer
research, an effort spearheaded by KP surgeon Balasz Bodai, MD.
February 1999 3rd Quarter 1998 HEDIS mammogram results15 were distributed to the Affiliated Care practitioners.
March 1999The 1998-1999 Core Catalog Health Education Publications16 was distributed at the AffiliatedPractitioner Advisory Council meeting along with the Prevention wall charts and the "HealthwiseHandbook".12
March 1999The second annual Mammography Days event was held at the Panola and Cascade Medical Offices.Survey results ranged from fair to excellent. The fair rating was based on members desiringtransportation be available during the week too.
April 1999Breast Health and Cancer Detection10 brochure was sent to the Affiliated Network practitioners andmade available for distribution through The 1998-1999 Core Catalog Health Education Publications,16
which was also distributed.
April 1999Network Pulse Newsletter contained the newly created two-page insert entitled, Quality Beat,17 whichwas devoted exclusively to quality of care and service issues. Quality Beat contained an article18
encouraging compliance with the Breast Cancer Screening Prevention Guidelines.2
April 1999Affiliated care quarterly mailing included the Recommended Screening and Preventive Services forAdults wall chart,3 the Preventive Checklist,19 and the mammogram posters, which contain themammogram guidelines.
May 1999A self-requested form for patients who "walk in" to the Radiology Department for a mammogram wasdeveloped.20
June 1999Mammogram Reminder Card: You Oughta Be in Pictures4 was mailed to all new members in targetpopulation and to members aged 50+ years who had never received the brochure in the past.
June 1999The survey21 from the June Mammography Days event at Cascade and Panola Medical Offices reflected
positively that members are pleased with the free transportation provided to the medical offices andwith Saturday hours.
June 1999The breast health posters9 and the brochure, Breast Health and Cancer Detection,10 were revised toinclude the HealthLine number and information about the cost of a mammogram.
June 1999 Access to Screening Mammography by Self-request policy and procedure22 was updated.
June 1999The Women's Health Advisor23 was rolled out to all Obstetrics/Gynecology Departments except forCrescent Center Medical Office.
June 1999 HCT lead RNs were trained on how to use the self-requested mammogram questionnaire.
June 1999Orange chart reminders were revised and inserted in medical records of target population during chartreview to remind physicians to order mammograms.
June 1999Call Center began outreach calls to women aged 52-69 years in target populations who have not beenscreened.
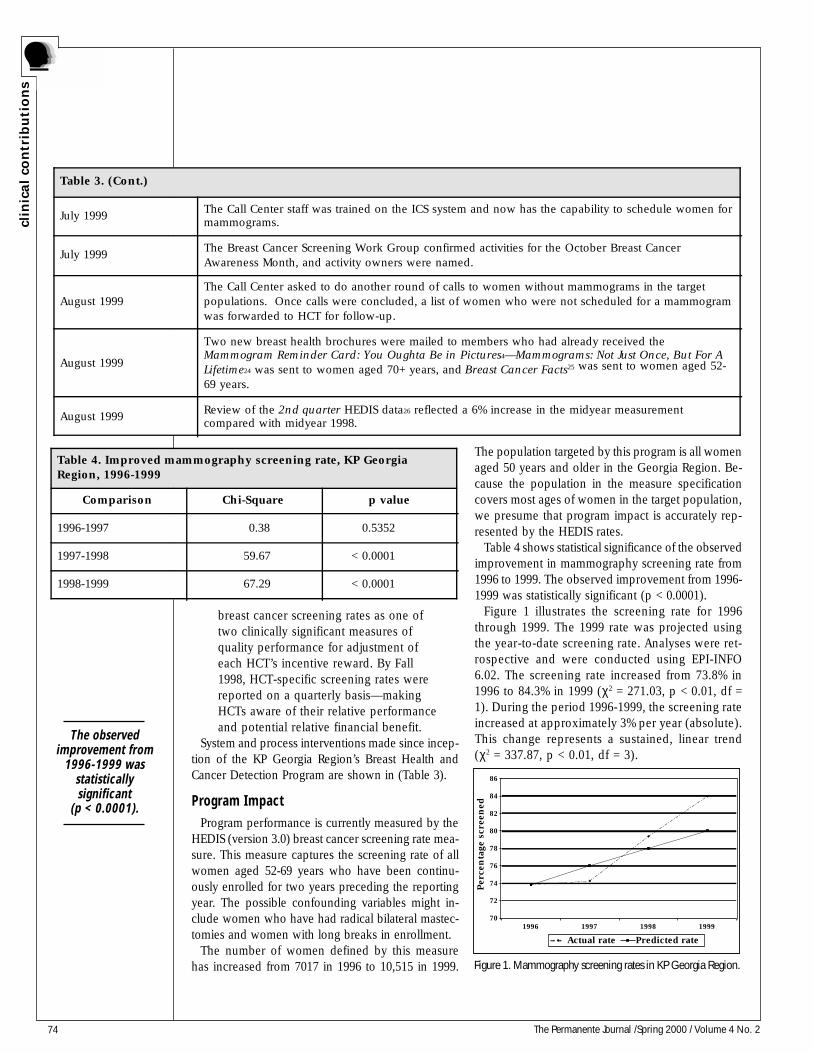
74 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
Table 3. (Cont.)
July 1999The Call Center staff was trained on the ICS system and now has the capability to schedule women formammograms.
July 1999The Breast Cancer Screening Work Group confirmed activities for the October Breast CancerAwareness Month, and activity owners were named.
August 1999The Call Center asked to do another round of calls to women without mammograms in the targetpopulations. Once calls were concluded, a list of women who were not scheduled for a mammogramwas forwarded to HCT for follow-up.
August 1999
Two new breast health brochures were mailed to members who had already received theMammogram Reminder Card: You Oughta Be in Pictures4—Mammograms: Not Just Once, But For ALifetime24 was sent to women aged 70+ years, and Breast Cancer Facts25 was sent to women aged 52-
69 years.
August 1999Review of the 2nd quarter HEDIS data26 reflected a 6% increase in the midyear measurementcompared with midyear 1998.
breast cancer screening rates as one oftwo clinically significant measures ofquality performance for adjustment ofeach HCT’s incentive reward. By Fall1998, HCT-specific screening rates werereported on a quarterly basis—makingHCTs aware of their relative performanceand potential relative financial benefit.
System and process interventions made since incep-tion of the KP Georgia Region’s Breast Health andCancer Detection Program are shown in (Table 3).
Program ImpactProgram performance is currently measured by the
HEDIS (version 3.0) breast cancer screening rate mea-sure. This measure captures the screening rate of allwomen aged 52-69 years who have been continu-ously enrolled for two years preceding the reportingyear. The possible confounding variables might in-clude women who have had radical bilateral mastec-tomies and women with long breaks in enrollment.
The number of women defined by this measurehas increased from 7017 in 1996 to 10,515 in 1999.
The population targeted by this program is all womenaged 50 years and older in the Georgia Region. Be-cause the population in the measure specificationcovers most ages of women in the target population,we presume that program impact is accurately rep-resented by the HEDIS rates.
Table 4 shows statistical significance of the observedimprovement in mammography screening rate from1996 to 1999. The observed improvement from 1996-1999 was statistically significant (p < 0.0001).
Figure 1 illustrates the screening rate for 1996through 1999. The 1999 rate was projected usingthe year-to-date screening rate. Analyses were ret-rospective and were conducted using EPI-INFO6.02. The screening rate increased from 73.8% in1996 to 84.3% in 1999 (χ2 = 271.03, p < 0.01, df =1). During the period 1996-1999, the screening rateincreased at approximately 3% per year (absolute).This change represents a sustained, linear trend(χ2 = 337.87, p < 0.01, df = 3).
70
72
74
76
78
80
82
84
86
1996 1997 1998 1999
Per
cen
tage
scr
een
ed
Actual rate Predicted rate
Figure 1. Mammography screening rates in KP Georgia Region.
Table 4. Improved mammography screening rate, KP GeorgiaRegion, 1996-1999
Comparison Chi-Square p value
1996-1997 0.38 0.5352
1997-1998 59.67 < 0.0001
1998-1999 67.29 < 0.0001
The observedimprovement from
1996-1999 wasstatisticallysignificant
(p < 0.0001).

75The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
CommentProgram Evaluation
The Breast Health and Cancer Detection Programhas achieved demonstrable results. In 1997 and 1998,the IPC/CQI team (and in 1999, the EIQ Breast Can-cer Work Group) systematically identified issuesimpeding performance improvement and have rec-ommended innovations to motivate and accelerateimprovement in breast cancer screening.
The program has achieved its objectives. The breastcancer screening rate for women rose from 74% in1996 to 84% for all insurance product lines in 1999.National benchmarks for 1998 were 81% (90th per-centile for commercial members) and 84% (90thpercentile for Medicare-eligible members). Our84.3% screening rate thus apparently makes theGeorgia Region a KP national leader and puts theGeorgia Region in the top 10% of all health plans inthe country.
The program has achieved these results with a broadarray of activities: Saturday hours, mobile mammog-raphy, medical record reminders, patient and physi-cian reminders, Call Center outreach, practitionerfeedback on performance, and practitioner financialincentives. Some of these activities are relatively lowin cost (eg, the fuchsia inserts in medical records).Several other innovations demonstrate the ability tointegrate improved care management into evolvingservice delivery within KP—such as use of Call Cen-ter technology and redesign of Primary Care deliv-ery. Although we cannot point to any one of theseinnovations as a key driver of improvement, imple-menting this cluster of innovations can substantiallyimprove care delivery.
In particular, the Call Center outreach was oneof the most successful methods implemented bythe Georgia Region. The purpose of this outreachtool was to call women aged 52-69 years whowere past due for a mammogram and to schedulean appointment for them. In some instances, theCall Center was not able to reach the patient; ifthat were the case, those names and phone num-bers were forwarded to the HCT for follow-up.At least three attempts at calling the patient weremade before involving the HCT. This activityshould be increased to maximize future return onthese efforts.
The least successful activity was the mobile mam-mography van outreach. Although the mobilemammography van did not have the turnout innumbers that we had anticipated, two women were
found in the early stages of cancer. The purposeof this outreach effort was to provide mammogra-phy services at sites without mammographyequipment. This intervention was directed atwomen who needed transportation to a medicalcenter to get a mammogram. The protocol for thisintervention was to process the films at the end ofthe day. A problem occurred in some cases whereincomplete views of the breast were taken, mak-ing the films inadequate. Forty (65%) of the womenhad to return for repeat views. No additional mo-bile mammography interventions have beenimplemented. However, one initiative that cameout of this outreach was the Mammography Daysevent, in which vans are used to transport womento medical offices with onsite mammography equip-ment. Mammography Days occurs on a quarterlybasis and has been successful. Plans to use themobile mammography van are uncertain. But theinitiative to provide van transportation should beincreased as a feasible alternative to the mobilemammography van outreach.
The impact of improved mammography screeningaccess on the rate of breast cancer diagnosis andbreast cancer stage at diagnosis were not availablewhen this article was prepared. The Georgia Regionbegan developing a Breast Cancer Registry with stage-at-diagnosis information in 1996. The 1996 and 1997data showed results comparable with other KP Re-gions. The 1998 and most recent data are currentlyundergoing data integrity checks related to our re-cently required state reporting and are not availableat this time.
Cost-effectiveness
Data from the Centers for Disease Control andPrevention27 suggest that screening women aged50-69 years for breast cancer every one to two yearscan lead to a 20% to 30% reduction in breast can-cer mortality. One study28 indicated that the com-bination of a clinical breast examination and anannual mammogram prevents premature death ata cost of $22,000 to $84,000 per life-year gained inwomen aged 55 to 65 years, depending on theeffectiveness of screening. Our Georgia Region’sdata on the evaluation of cost-effectiveness of thedescribed interventions are forthcoming. In themeantime, our annual budget for the KP-GeorgiaBreast Health and Cancer Detection Program is$71,000, a modest investment to achieve these sub-stantial gains.
The breast cancerscreening rate forwomen rose from74% in 1996 to84% ... in 1999.

76 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
ImplicationsThe following activities have already become the
normal practice for breast cancer screening outreachand are embedded in our ongoing processes of care.We therefore expect to sustain the gains made andpossibly even improve our results.
• Each summer, the Call Center phoneswomen aged 52-69 years who have notbeen screened for two or more years.
• Each May, the Prevention and HealthPromotion Department will mail the“Mammography Reminder Card: YouOughta Be in Pictures”4 or the“Mammograms: Not Just Once, But For ALifetime”24 brochure to women aged 50years and older.
• During the second quarter of each year,the Prevention and Health PromotionDepartment will place colorful “chartreminders” with the Breast CancerScreening Prevention Guidelines2 on themin the medical records charts of womenaged 50 years and older who have nothad a mammogram in two or more years.
• The breast health posters with the BreastCancer Screening Prevention Guidelines2
will be revised and placed in the bath-rooms during the second quarter of eachyear by the Prevention and HealthPromotion Department as needed.
• The “Recommended Screenings andPreventive Services for Adults”3 wall chartthat is placed in all medical center examrooms is revised every two years by theIPC and the Prevention and HealthPromotion Department. The wall chart issent to the network practitioners.
• The Radiology Department will continueto offer Saturday appointments thatsupport routine mammograms and “WellWomen” examinations and will providetransportation to the medical centers forwomen who need it.
TransferabilityNone of our changes in process of care (with the
possible exception of HCT incentives) are intrinsicto the Georgia Region. Some of the project processes,tools, and practices (eg, Saturday hours, self-referral,walk-in appointments, reminders) are common prac-tice in many KP Regions.
The Georgia Region’s Prevention and Health Pro-motion Department is dedicated to providinghigh-quality care to the members. In order to do this,this Department practices networking with other KPRegions and gleans from them initiatives that haveproved successful. Some of the initiatives that KPGeorgia uses for breast awareness were adapted fromthe KP Northwest Region. Specifically, the KP North-west Region’s EpicCare Health Maintenance Reminderbecame our paper version chart reminder; the North-ern California Region’s Clinic Visit Summary form toalert clinicians became our exam room wall chart,and the letter outreach became our “MammographyReminder Card: You Oughta be in Pictures”4 and“Mammograms: Not Just Once, But For A Lifetime”24
brochure mailer; and the KP Northwest Region’sWomen’s Safety Net gave us the idea to select a par-ticular population to target.
The nature of the innovations we used in theGeorgia Region make this Program a model of careboth for other medical conditions and for other KPRegions. In the absence of an electronic medicalrecord, medical record inserts are a low-costmethod for prompting behavior on the part of pa-tient and practitioner whenever a visit occurs. Thissimple activity can be used for promoting adher-ence to clinical practice guidelines for other dis-eases, such as asthma and diabetes. We have alsofocused recent efforts to develop a registry for ourprostate and colorectal cancers and melanomassimilar to our Breast Cancer Screening Registry. Inaddition, the Georgia Region mailed the large-printedition of the “Mammograms: Not Just Once, ButFor A Lifetime”24 brochure to women aged 70 yearsand older. Dr Adrienne Mims and Kecia Leather-wood presented our results at the Kaiser Perman-ente Third Prevention & Self-Care Symposium inDecember 1999 with an exhibit called “Implemen-tation of a Breast Health Screening Program forthe Hard-to-Reach Woman.”28
ConclusionIn conclusion, although we have no specific feed-
back information yet from other KP Regions that haveadopted aspects of our Georgia Region project (ei-ther regarding their experience or with respect toquality improvement results with the inreach andoutreach activities and educational programs), webelieve that any KP Region can apply a similar clus-ter of interventions to achieve measurable, sustain-able quality improvement. ❖
The breast cancerscreening rate forwomen rose from74% in 1996 to
84% for allinsurance product
lines in 1999.

77The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
References1. National Committee for Quality Assurance [HEDIS]. (http://www.ncqa.org/pages/communications/news/Compass.htm).Accessed on Feb. 18, 2000.2. The Southeast Permanente Medical Group. Breast cancerscreening recommendations: adult prevention guidelines. Atlanta,GA: Kaiser Permanente Medical Care Program; 1998. 3 p.3. The Southeast Permanente Medical Group. Recommendedscreenings and preventive services for adults [wall chart].Atlanta, GA: Kaiser Permanente Medical Care Program; Feb1998. 1 p.4. Mammography reminder card: you oughta be in pictures.Atlanta, GA: Kaiser Permanente Medical Care Program; June 1999.5. Adult Health Preventive Services guidelines brochures:preventive care for adults ages 18-44; Preventive care for adultsages 45-64; Preventive care for seniors ages 65+. Atlanta, GA:Kaiser Permanente Medical Care Program; December 1997.6. Treatment options for breast cancer. Partners in health. Fall1998:6-7.8. Breast cancer screening: an ounce of prevention [GeorgiaRegion] Oct 1999; n.d.9. Posters/pins. Screening mammography: guidelines for goodbreast health; Mammograms can save lives [Promotions forBreast Cancer Awareness Month]. Atlanta, GA: Kaiser Permanen-te Medical Care Program; n.d.10. Breast health & cancer detection. Atlanta, GA: KaiserPermanente Medical Care Program; Aug 1999.11. [Adult] preventive care services. Atlanta, GA: KaiserPermanente Medical Care Program; Nov 1999.12. Kaiser Permanente Medical Care Program. HealthwiseHandbook. Oakland, CA: Kaiser Permanente Medical CareProgram; 1994, 1999.13. Mims AD. Revised breast health & cancer detectionbrochure. TSPMG Newsletter. The Southeast PermanenteMedical Group; n.d.14. Kaiser Permanente Chief of Surgery helps stamp out breast
cancer. Network Pulse Newsletter; n.d.15. Outcomes Measurement Group. 3rd Quarter 1999 [HEDISData]. Breast cancer screening. Atlanta, GA: Kaiser PermanenteMedical Care Program; Oct 1999.16. The 1998-99 core catalog. Health Education Publications.Atlanta, GA: Kaiser Permanente Medical Care Program; n.d.17. Quality beat: when did you have your last mammogram?Network Pulse Newsletter; Spring 1999.18. Quality beat: article on compliance with Breast CancerScreening Prevention Guidelines.19. Preventive checklist. Atlanta, GA: Kaiser PermanenteMedical Care Program; December 1997. 4 p.20. Self–administered questionnaire for walk-in mammograms.Atlanta, GA: Kaiser Permanente Medical Care Program; Sep 1999.21. Mammography day survey. Atlanta, GA: Kaiser PermanenteMedical Care Program; n.d.22. Kaiser Permanente Medical Care Program, Georgia Region.Breast health and cancer detection,” Access to screeningmammography by self-request. Policy and Procedure, GeorgiaRegion, rev. Atlanta, GA: Kaiser Permanente Medical CareProgram; 1998.23. [The Women’s Health Advisor] 9 p. Breast cancer, 3 p;Mammography, 2 p; Breast self-examination, 1 p; Breast cancer,operable, 3 p. Clinical Reference Systems; 1998.24. Mammograms: not just once, but for a lifetime. WashingtonDC: US Department of Health and Human Services; 1998.25. Breast cancer and mammograms. Bethesda, MD: NationalInstitutes of Health, 1997.26. Outcomes Measurement Group. 2nd quarter 1999 [HEDISdata] Breast cancer screening. Atlanta, GA: Kaiser PermanenteMedical Care Program; Oct 1999.27. US Preventive Services Task Force. Guide to clinicalpreventive services, 2nd ed. Baltimore: Williams & Wilkins; 1996.28. Leatherwood KA, Mims A. Implementation of a breast healthscreening program for the hard-to-reach woman. KaiserPermanente Third Prevention & Self-Care Symposium, Dec 1999.
Experience Is InterpretiveAt its heart, what we call experience is an interpretive,
not a perceptive, encounter. Seeing is one thing. But howwe choose to interpret what we see will determine the
story we tell and the life we lead.Richard Stone, “The Healing Art of Storytelling”

78 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
IntroductionImproving cardiac outcomes was first defined
as an organizational goal in the Strategic QualityPlan of Kaiser Permanente of Ohio (KP Ohio) in1992. Table 1 lists the team members and contactperson for this project.
The literature indicates that the use of aspirin inpatients with known coronary artery disease (CAD)can decrease cardiac events by 25%.1 Lowering cho-lesterol to below 100 mg/dL in high-risk patientswith CAD can reduce morbidity and mortality byas much as 35%.2,3 Beta blockers after a myocar-dial infarction have also been shown to decreasecardiac events.4
Physician compliance with guidelines pertaining tothe use of aspirin and cholesterol-lowering drugs hasbeen low.5,6
BackgroundThis project was a joint effort between the Kai-
ser Foundation Health Plan and the PermanenteMedical Group of Ohio (OPMG). The team wasformed in 1993 to support the Strategic QualityPlan and was led by the Associate Medical Direc-tor for Medical Information and the AssistantMedical Director for Quality, Resource Manage-ment, and Continuity. The team included the In-ternal Medicine and Cardiology Departments;members of the Quality, Information Technology,and Clinical Innovation Departments. During thecourse of the project, individual team memberschanged, but the goals were maintained.
ProcessIn 1992, during a clinical strategic planning pro-
cess which reviewed effective interventions forprevalent diagnoses, we determined that four inter-ventions could have a measurable impact on ourmembers and could improve cardiac outcomes forCAD patients. We estimated that cardiac events couldbe reduced by as much as 20% if compliance with
established guidelines could be improved, with pos-sible further decreases if beta blocker and smokingcessation programs were successful.
The project was implemented in 1994 after the de-ployment of the Medical Automated Record System(MARS).7 In 1995, an analysis of data from KP Ohio,indicated that one half of admissions for ischemic heartdisease and one third of admissions for myocardial in-farction were in patients with known CAD, the groupat which the interventions described here were directed.
ObjectivesThe project goal was to improve cardiac outcomes
by using four interventions in patients with CAD:1. Increase aspirin use2. Increase the use of cholesterol-lowering drugs3. Encourage smoking cessation4. Increase beta blocker use after a myocar-
dial infarction.The specific objective of this project was to statisti-
cally decrease cardiac morbidity and mortality. A goalof reducing cardiac morbidity and mortality by 20%was set when this program began in 1994; half ofthis reduction would come from interventions directedat CAD patients (described here) and half from inter-ventions directed at patients with no CAD.
MethodologyScope
Cardiac disease is the most common cause of mor-bidity and mortality in the nation and in our HealthPlan membership. The cost of cardiac-related admis-sions and procedures in KP Ohio is about $20 millionper year, and approximately 4% of the membershiphave a diagnosis of CAD. This project was implementedwithin the normal duties of the Quality Chief of Inter-nal Medicine, the Chief of Internal Medicine, the MARSteam, the Quality, Resource Management, and Clini-cal Innovation Departments.
InterventionThe intervention consisted of computer-generated
reminders from MARS at the time of a visit. Re-minders suggested the use of aspirin for CADpatients, LDL cholesterol screening and control forpatients with a CAD diagnosis, and use of betablockers in patients who had a myocardial infarc-tion in the past two years (Figure 1). All OPMGphysicians use MARS to document treatment ofpatients. MARS prints a “paper intermediary” forall patients seen, which consists of a progress note
Improvement of Cardiac Outcomes in Kaiser Permanente of Ohio
Table 1. Team members for Improvement of Cardiac Outcomes inKaiser Permanente Ohio
Team member names: Wendy Dahar, MPH; Diana Dally; Gary DaMert,MD; Nick Dreher, MD; Allan Khoury, MD, PhD; Otfried Niedermaier, MD;Heidi Nystrom; Mark Roth, MD; Phyllis Powell; Ann Scott; Chuck Siemon;Bob Szczepanik; Linda Young; John Zuscik
Contact person: Allan Khoury, MD, PhD, 5400 Lancaster Dr., BrooklynHeights, OH 44131 (e-mail: [email protected])
Ohio Region
... use of aspirin inpatients with
known coronaryartery disease
(CAD) candecrease cardiacevents by 25%

79The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
that lists patients’ diagnoses, medications, allergiesand immunizations, and a reminder page that sug-gests changes in clinical care when patients arenot in compliance with guidelines.
Reminders were not generated for members withcontraindications. For example, people with a his-tory of aspirin allergy or side effects, gastritis, oresophagitis, warfarin use, or ticlopidine use were ex-cluded from the aspirin intervention. Approximately30% of the CAD patients were ineligible for the aspi-rin intervention due to these contraindications.
The intervention also included generation of com-parative reports of physician performance in guidelineareas. Literature validated the effectiveness of pro-viding clinical guideline reminders to physicians atthe moment of care.8 In addition, smoking status wascollected at every adult visit and was prominentlydisplayed on the progress note with the hope of trig-gering an education intervention in which clinicalstaff had been trained.
Quality Measures
Eight quality measures were used:• Percentage of patients with CAD on aspirin• Percentage of patients with CAD who
have had LDL cholesterol screening in thepast two years
• Percentage of patients with CAD whosecholesterol level is ≤100 mg/dL
• Percentage of patients receiving betablockers after a myocardial infarction
• Patient-reported smoking prevalence• Angina admission rate• Myocardial infarction admission rate• Death rate from CAD
Performance goals for these measures were adjustedover time. A performance goal of more than 80% ofeligible CAD patients receiving aspirin was set in 1993.The literature indicated that between 13% and 58% ofCAD patients take aspirin prophylactically and thatonly 10% to 15% of CAD patients are at target LDLlevels.5,6,9 Baseline measurements in KP Ohio foundthat 56% of CAD patients were receiving aspirin and10% were at target LDL levels.
A performance goal of 35% was set in 1996 forpatients reaching their target cholesterol level of ≤100 mg/dL. The literature indicates that in a researchsetting, 60% of patients reached goal.2 A performancegoal of 80% was set for cholesterol testing in the pasttwo years. The KP Ohio baseline for this measure in1997 was 70%.
No specific goals were set for beta blocker use orfor patient-reported smoking prevalence.
The system prompted the collection of smokingstatus and made that information evident at the mo-ment of care. The clinic smoking-cessation interven-tion is based on the TRAC program developed bythe Center for Health Research.10 This program fea-tures brief tobacco cessation advice and counseling.Videos, written materials, and phone calls providemembers with the support they need when they areready to quit.
A hospital discharge cardiac assessment programwas begun in 1995. The care path for this programincludes the use of beta blockers for members withmyocardial infarction.
In 1995, physician feedback reports were distrib-uted quarterly which detailed the percentage of panelmembers with CAD who were prescribed aspirin.Similar reports detailing LDL cholesterol screening inthe past two years, and LDL level controlled, werestarted in 1997.
Feedback reports also measured the percentage ofpanel members who smoked according to patientself-report.
The use of beta blockers after myocardial infarction,a HEDIS measure, was determined by chart review.
Beginning in 1993, hospital admissions for myocar-dial infarction and angina pectoris as well as CADdeath rates have been measured to determine if theinterventions have led to improvements in the cardiacmorbidity and mortality rates. The number of cardiacdeaths is determined through use of State of OhioVital Statistics death tapes. The number of hospitaladmissions is obtained through the billing systems.
Products
Clinical practice guidelines for cardiac disease weredeveloped, and provider education occurred at In-ternal Medicine Department meetings throughout thePermanente Medical Group of Ohio.
Figure 1.
Reminders werenot generated for
members withcontraindications.
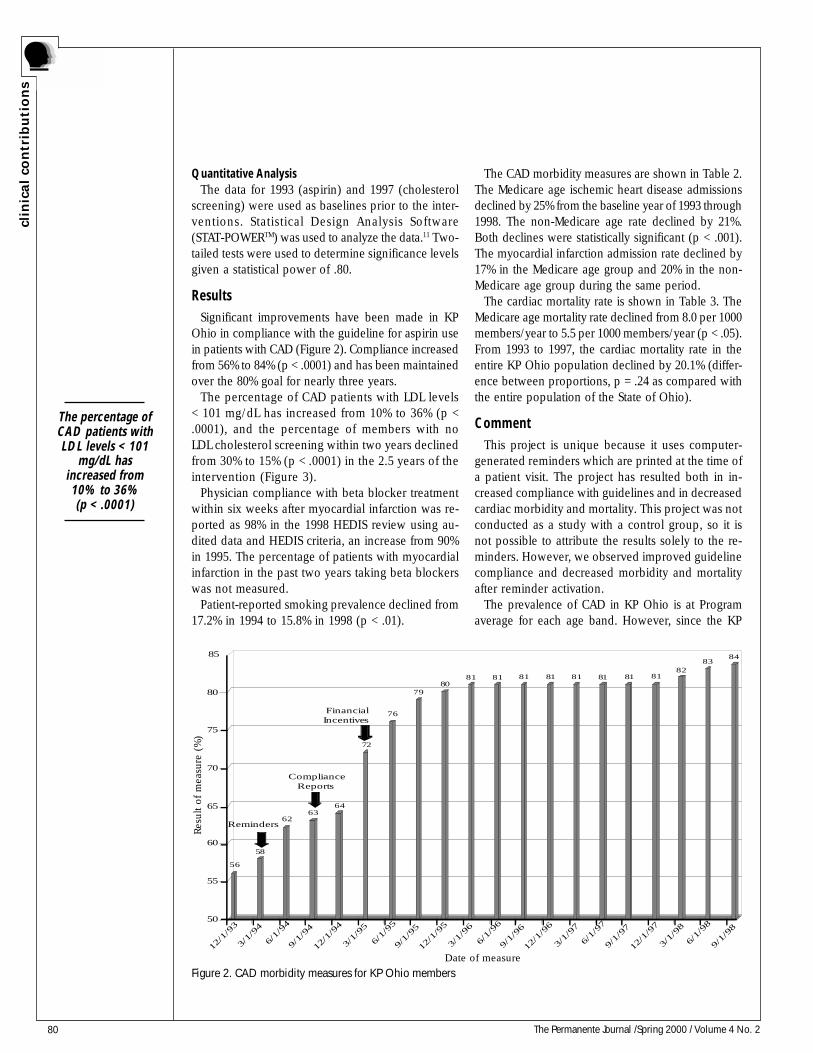
80 The Permanente Journal /Spring 2000 / Volume 4 No. 2
clin
ical
con
trib
uti
on
s
Figure 2. CAD morbidity measures for KP Ohio members
56
58
6263
64
72
76
7980
81 81 81 81 81 81 81 8182
8384
50
55
60
65
70
75
80
85
12/1
/93
3/1/
94
6/1/
94
9/1/
94
12/1
/94
3/1/
95
6/1/
95
9/1/
95
12/1
/95
3/1/
96
6/1/
96
9/1/
96
12/1
/96
3/1/
97
6/1/
97
9/1/
97
12/1
/97
3/1/
98
6/1/
98
9/1/
98
Reminders
ComplianceReports
FinancialIncentives
Res
ult of
mea
sure
(%
)
Date of measure
Quantitative AnalysisThe data for 1993 (aspirin) and 1997 (cholesterol
screening) were used as baselines prior to the inter-ventions. Statistical Design Analysis Software(STAT-POWERTM) was used to analyze the data.11 Two-tailed tests were used to determine significance levelsgiven a statistical power of .80.
ResultsSignificant improvements have been made in KP
Ohio in compliance with the guideline for aspirin usein patients with CAD (Figure 2). Compliance increasedfrom 56% to 84% (p < .0001) and has been maintainedover the 80% goal for nearly three years.
The percentage of CAD patients with LDL levels< 101 mg/dL has increased from 10% to 36% (p <.0001), and the percentage of members with noLDL cholesterol screening within two years declinedfrom 30% to 15% (p < .0001) in the 2.5 years of theintervention (Figure 3).
Physician compliance with beta blocker treatmentwithin six weeks after myocardial infarction was re-ported as 98% in the 1998 HEDIS review using au-dited data and HEDIS criteria, an increase from 90%in 1995. The percentage of patients with myocardialinfarction in the past two years taking beta blockerswas not measured.
Patient-reported smoking prevalence declined from17.2% in 1994 to 15.8% in 1998 (p < .01).
The CAD morbidity measures are shown in Table 2.The Medicare age ischemic heart disease admissionsdeclined by 25% from the baseline year of 1993 through1998. The non-Medicare age rate declined by 21%.Both declines were statistically significant (p < .001).The myocardial infarction admission rate declined by17% in the Medicare age group and 20% in the non-Medicare age group during the same period.
The cardiac mortality rate is shown in Table 3. TheMedicare age mortality rate declined from 8.0 per 1000members/year to 5.5 per 1000 members/year (p < .05).From 1993 to 1997, the cardiac mortality rate in theentire KP Ohio population declined by 20.1% (differ-ence between proportions, p = .24 as compared withthe entire population of the State of Ohio).
CommentThis project is unique because it uses computer-
generated reminders which are printed at the time ofa patient visit. The project has resulted both in in-creased compliance with guidelines and in decreasedcardiac morbidity and mortality. This project was notconducted as a study with a control group, so it isnot possible to attribute the results solely to the re-minders. However, we observed improved guidelinecompliance and decreased morbidity and mortalityafter reminder activation.
The prevalence of CAD in KP Ohio is at Programaverage for each age band. However, since the KP
The percentage ofCAD patients withLDL levels < 101
mg/dL hasincreased from10% to 36%(p < .0001)
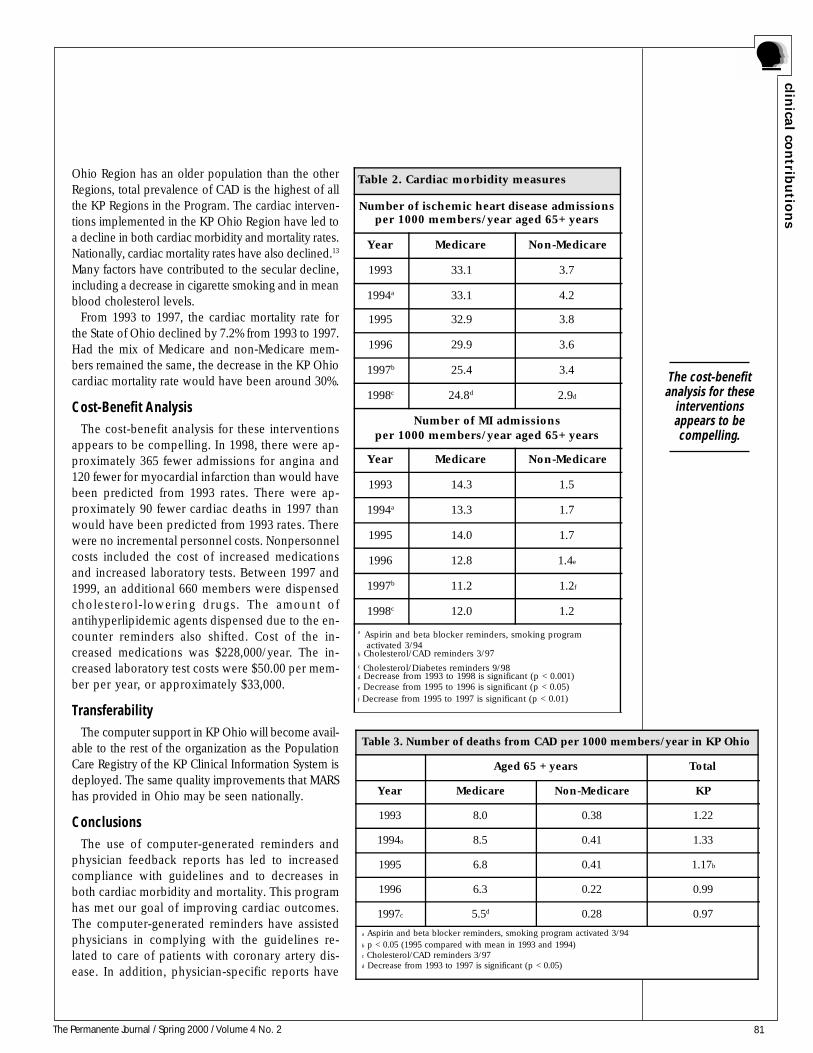
81The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
Ohio Region has an older population than the otherRegions, total prevalence of CAD is the highest of allthe KP Regions in the Program. The cardiac interven-tions implemented in the KP Ohio Region have led toa decline in both cardiac morbidity and mortality rates.Nationally, cardiac mortality rates have also declined.13
Many factors have contributed to the secular decline,including a decrease in cigarette smoking and in meanblood cholesterol levels.
From 1993 to 1997, the cardiac mortality rate forthe State of Ohio declined by 7.2% from 1993 to 1997.Had the mix of Medicare and non-Medicare mem-bers remained the same, the decrease in the KP Ohiocardiac mortality rate would have been around 30%.
Cost-Benefit AnalysisThe cost-benefit analysis for these interventions
appears to be compelling. In 1998, there were ap-proximately 365 fewer admissions for angina and120 fewer for myocardial infarction than would havebeen predicted from 1993 rates. There were ap-proximately 90 fewer cardiac deaths in 1997 thanwould have been predicted from 1993 rates. Therewere no incremental personnel costs. Nonpersonnelcosts included the cost of increased medicationsand increased laboratory tests. Between 1997 and1999, an additional 660 members were dispensedcholesterol-lowering drugs. The amount ofantihyperlipidemic agents dispensed due to the en-counter reminders also shifted. Cost of the in-creased medications was $228,000/year. The in-creased laboratory test costs were $50.00 per mem-ber per year, or approximately $33,000.
TransferabilityThe computer support in KP Ohio will become avail-
able to the rest of the organization as the PopulationCare Registry of the KP Clinical Information System isdeployed. The same quality improvements that MARShas provided in Ohio may be seen nationally.
ConclusionsThe use of computer-generated reminders and
physician feedback reports has led to increasedcompliance with guidelines and to decreases inboth cardiac morbidity and mortality. This programhas met our goal of improving cardiac outcomes.The computer-generated reminders have assistedphysicians in complying with the guidelines re-lated to care of patients with coronary artery dis-ease. In addition, physician-specific reports have
Table 2. Cardiac morbidity measures
Number of ischemic heart disease admissionsper 1000 members/year aged 65+ years
Year Medicare Non-Medicare
1993 33.1 3.7
1994a 33.1 4.2
1995 32.9 3.8
1996 29.9 3.6
1997b 25.4 3.4
1998c 24.8d 2.9d
Number of MI admissionsper 1000 members/year aged 65+ years
Year Medicare Non-Medicare
1993 14.3 1.5
1994a 13.3 1.7
1995 14.0 1.7
1996 12.8 1.4e
1997b 11.2 1.2f
1998c 12.0 1.2
a Aspirin and beta blocker reminders, smoking program activated 3/94b Cholesterol/CAD reminders 3/97c Cholesterol/Diabetes reminders 9/98d Decrease from 1993 to 1998 is significant (p < 0.001)e Decrease from 1995 to 1996 is significant (p < 0.05)f Decrease from 1995 to 1997 is significant (p < 0.01)
Table 3. Number of deaths from CAD per 1000 members/year in KP Ohio
Aged 65 + years Total
Year Medicare Non-Medicare KP
1993 8.0 0.38 1.22
1994a 8.5 0.41 1.33
1995 6.8 0.41 1.17b
1996 6.3 0.22 0.99
1997c 5.5d 0.28 0.97
a Aspirin and beta blocker reminders, smoking program activated 3/94b p < 0.05 (1995 compared with mean in 1993 and 1994)c Cholesterol/CAD reminders 3/97d Decrease from 1993 to 1997 is significant (p < 0.05)
The cost-benefitanalysis for these
interventionsappears to becompelling.
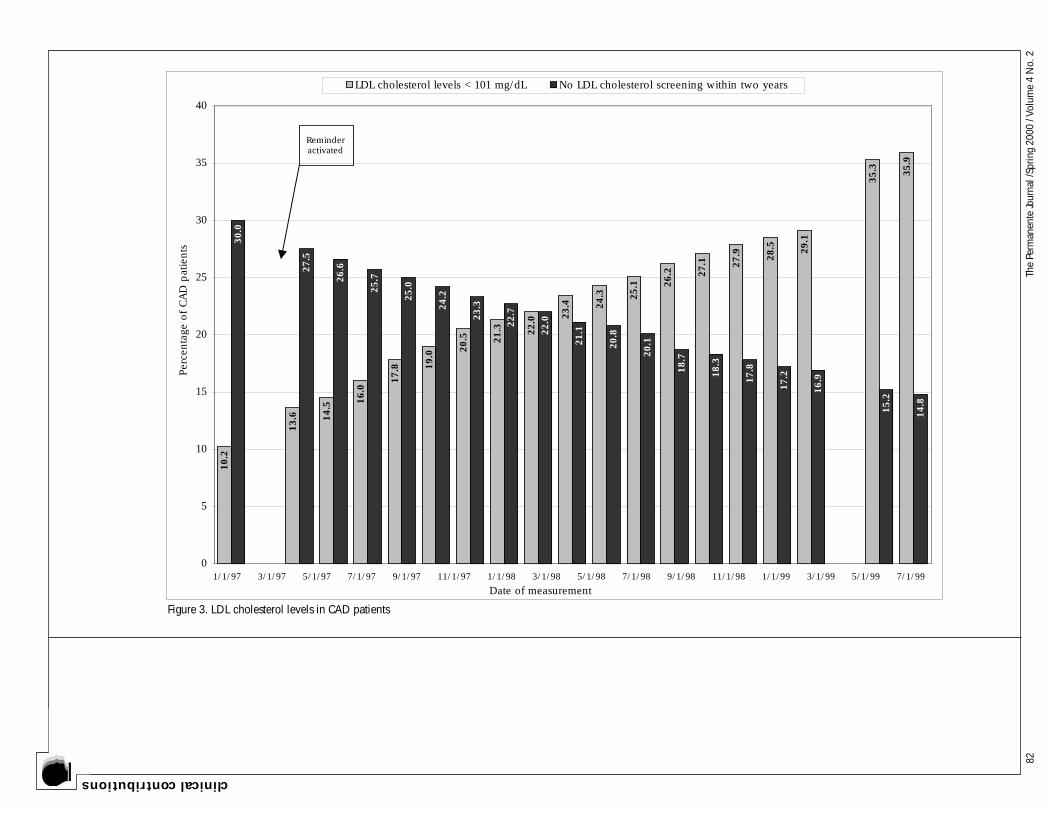
82Th
e Pe
rman
ente
Jour
nal /
Sprin
g 20
00 /
Volu
me
4 N
o. 2
clinical contributions
10.2
13.6 14.5
16.0
17.8 1
9.0
20.5 21.3 22.0 2
3.4 24.3 25.1 2
6.2 27.1 27.9 28.5 29.1
35.3 35.9
30.0
27.5
26.6
25.7
25.0
24.2
23.3
22.7
22.0
21.1
20.8
20.1
18.7
18.3
17.8
17.2
16.9
15.2
14.8
0
5
10
15
20
25
30
35
40
Per
centa
ge o
f CA
D p
atie
nts
LDL cholesterol levels < 101 mg/dL No LDL cholesterol screening within two years
Reminderactivated
1/1/97 3/1/97 5/1/97 7/1/97 9/1/97 11/1/97 1/1/98 3/1/98 5/1/98 7/1/98 9/1/98 11/1/98 1/1/99 3/1/99 5/1/99 7/1/99
Date of measurement
Figure 3. LDL cholesterol levels in CAD patients

83The Permanente Journal / Spring 2000 / Volume 4 No. 2
clinica
l con
tribu
tion
s
New York: Elsevier, 1991, p 205 (Current Topics inCardiology).5. Hoerger TJ, Bala MV, Bray JW, Wilcosky TC, LaRosa J.Treatment patterns and distribution of low-density lipoproteincholesterol levels in treatment-eligible United States adults. Am JCardiol 1998;82:61-5.6. Sueta CA, Petkun WM, Lulla A, Hart PL, Smith Jr. SC, SimpsonJr. RJ. Recommended management for hyperlipidemia and heartfailure: Are we following the guidelines? Circulation 1997;96Suppl 8:I362-I363.7. Schonfeld E. Can computers cure health care? Fortune, March30,1998.8. Johnston ME, Langston KB, Haynes RB, Mathieu A. Effects ofcomputer-based clinical decision support systems on clinicianperformance and patient outcome: a critical appraisal ofresearch. Ann Intern Med 1994;120:135-42.9. Vogel RA. Aspirin and coronary artery disease. N Engl J Med1996;335:1161-2.10. Hollis JF, Lichtenstein E, Vogt TM, Stevens VJ, Biglan A.Nurse-assisted counseling for smokers in primary care. AnnIntern Med 1993;118:521-5.11. Bavry JL. Statistical Design Analysis Software (Version 3):Getting Started. Portland, OR: QEI Systems, 1996.12. Kaiser Permanente Cardiovascular Outcomes Report; AnnualReport: Data from 1997. Oakland, CA: Care ManagementInstitute, February, 1999.13. Decline in deaths from heart disease and stroke–UnitedStates, 1900–1999. Morb Mortal Wkly Rep; 1999; 48:649-56.
alerted individual physicians to their performanceand have affected practice patterns. These remind-ers and reports appear to have decreased cardiacmortality more than the national trends. The suc-cess of the project is due to reminders and feed-back reports in combination with the usual physi-cian education efforts. Although a specific inter-vention may have had a greater impact than an-other, each component contributed to the overallsuccess of the KP Ohio Improvement of CardiacOutcomes project. ❖
References1. Willard JE. The use of aspirin in ischemic heart disease. NEngl J Med 1992;327:175-81.2 Randomised trial of cholesterol lowering in 4444 patients withcoronary heart disease: the Scandinavian Simvastatin SurvivalStudy (4S). Lancet 1994;344:1383-9.3. Sacks FM, Pfeffer MA, Moye LA, Rouleau JL, Rutherford JD,Cole TG, et al. The effect of pravastatin on coronary events aftermyocardial infarction in patients with average cholesterol levels.Cholesterol and Recurrent Events Trial Investigators. N Engl JMed 1996;335:1001-9.4. Gersh BJ, Rahimtoola SHE. Acute myocardial infarction.
The Stained-Glass PastViewing the past is like peering through a stained-glass
window from dawn to dusk. As the sun moves across thesky, the illumination of the many facets of glass changes. As Iwalk about the room, intricate patterns that were hidden in
darkness reveal themselves only from certain angles.Richard Stone, “The Healing Art of Storytelling”

84 The Permanente Journal / Spring 2000 / Volume 4 No. 2
sou
l o
f th
e h
eale
r
One-thirty in the morning.No seats were without bodies in the waiting room.ER Treatment One was smoking.Three ambulances arrive back to back,And the red phone rings again—two more coming in.One bringing an asthmatic, another with an MVA.“Sorry, Queens is closed,” they say.I collide with the day shift Team Coordinator—“You still here?”“Can’t leave now,” she says, “look at the board.”No one else could stay late to help.“We need sub-Q epi, solumedrol, and albuterol for the allergic reaction in F1.”The elderly man in Trauma C has EKG changes. “I need his old chart please.”“DOD needs an ICU bed.”The seizure patient in Trauma E pulls out his IV and attempts to get up, albeit intoxicated.“Why is the Tylenol OD in the GYN room?”“No other beds, Doc.”“Move him to the hallway, Psych can talk to him there…”“Doc, EPRP on the line…”“Get it out, get it out, oh my God, get it out!” introduced us to the woman hosting a frantically misguided bugin her ear canal.“Do we have a room?”“No—empty gurney against the back wall only.”“Put her there and get me some two percent lidocaine.”The ultrasound result handed to me shows acute cholecystitis.“Call the surgeon on call for me please.”“Doc, you may want to take a look at the allergic reaction—he’s getting worse…”
Suddenly, everything stopped. The lady in Trauma D dismissed the curtain like a strong wind through anopen window. In slow motion, she led her well-appearing child with a probable viral syndrome past the ERNurses’ Station. She used his arm as a leash. He was being towed with embarrassment. With agility anddisgust, she used her free arm to wave me off, demanding that her card be returned to her from the chartrack, as the wait was intolerable. It was clearly an outrage. Her soliloquy continued but faded as she walkeddown the ER hall and turned right to the waiting room exit. She was gone, and as she had assured us, wouldnot be back soon. A pause of bewilderment and self-doubt ensued, interrupted only by disbelief andbitterness. Surely she had heard the same ruckus, witnessed the same fray, and felt the same storm I had.After all, wasn’t the ER Treatment One area just one big room? Or was the thin curtain enclosing TraumaRoom D an adequate barrier to the atmosphere of urgency surrounding it? The chaotic winds stirred by thesick and injured seemingly spared Trauma Room D. It was like a bunker in the storm.
Next time, maybe we ought to send a bulletin to the bunker to update its occupants regarding the dangeroutside, and advise them to please wait for a calm. ❖
A Bunker in the StormAnonymous*
* Emergency Department, Baldwin Park Medical Center, Baldwin Park, California

85The Permanente Journal / Spring 2000 / Volume 4 No. 2
a w
ord
from
the m
ed
ical d
ir ecto
rs
Perhaps the older physicians among you will re-call the thirteenth and last law proclaimed in thenovel, The House of God1: “The delivery of medicalcare is to do as much nothing as possible.” Writtenwith tongue firmly in cheek in the late 1970s, thisnovel reminds physicians that a less aggressive ap-proach is sometimes the most reasonable. Perhapsthe more sage among you will even be reminded ofthat part of the Hippocratic Oath that warns againsterrors of commission. (Recent studies suggest thatsuch errors may be a major problem for Americanmedicine.) Today, the advice proposed by The Thir-teenth Law is sometimes greeted with suspicion atbest and with accusations of denial of care andthreats of lawsuit at worst. What has caused thischange of thinking?
In the past ten years, the managed care industryhas used “new” methods of physician compensation(capitation rates, “withholds,” etc) that require phy-sicians to share economic risk with the institutionsthat organize and pay for medical services. The man-aged care industry has also examined the wide varia-tion in clinical approaches to common problems andhas sought “best practices” in an attempt to stan-dardize perceived quality and cost-effectiveness.
PMG physicians have had a different experiencethan our private-practice peers, many of whom havefelt a loss of control and frustration with a systemthat “denies their patients the care they require.” Thesephysicians firmly believe—and I concur—that thephysician/patient relationship is the cornerstone ofmedicine as we know it. Many PMG physicians be-lieve that managed care as conducted by our for-profit competitors intrudes on that relationship.
Why has this change occurred? I believe that theseissues are only symptoms of the real problem: Inmost cases, neither participant in the physician/pa-tient relationship is placed at great financial risk bythe decisions made. In most cases, the employer isthe party responsible for making most payments to ahealth care insurer, and the insurance company is atrisk for any medical costs that exceed the sums paid.Unfortunately, as we know, this arrangement ofmultiple payors (patient, employer, insurance com-pany, and, yes, in many instances, the government)often leads to cost-shifting.
The real question is thus, “Should the employerand/or health insurance company at financial risk
for medical decisions have a right to ‘intrude’ intothe traditionally sacrosanct physician/patient rela-tionship?” I believe the answer should be no, butonly if the physician/patient relationship meetscertain conditions.
The first of these conditions is that both partici-pants in the physician/patient relationship be will-ing to base their medical decisions on evidence-based medicine.
Increasingly, as large volumes of medical informa-tion become available to patients “at the click of amouse,” patients are discovering what most doctorshave known for years: Medical literature can be foundthat will support almost any approach to treating al-most any illness. The physician must know the mostappropriate one or two approaches for that patient(not an easy task with today’s information explo-sion). Perhaps an even more difficult task is for thephysician to be willing and able to help the patientunderstand why these evidence-based approachesare the appropriate care for that patient. As requestsfor medical services increasingly diverge from whatwould be considered the appropriate “evidence-based” approach, patients should bear an increasingamount of the cost for services they request. Other-wise, Adam Smith’s concept of the Invisible Hand(ie, purchaser paying more for an item in short sup-ply) will not come into play, and the affordability ofhealth care will decline. For those who suggest thatthis approach constitutes “rationing of medical care,”I would suggest that many of the 47 million peoplein America today who cannot afford medical insur-ance would say that medical care in America is al-ready rationed.
Both the physician and the patient need help toidentify evidence-based approaches to diagnosis andtreatment. Certainly the state and federal governmentcould have some role in this arena, as have the Stateof Oregon and the US Centers for Disease Controland Prevention (CDC). More help is required, how-ever—and medical specialty societies could assumea greater role. Traditionally, their role has not beenemphasized; instead, the physician/patient relation-ship has been the cornerstone of health care. Thiscornerstone now needs help to bear the additionalweight of today’s medical decisions. I believe that byhelping to define evidence-based medical approaches(especially when a better approach is available or
A Word from the Medical Directors:Can Managing Cost Be Part of Managing Care?
By Donald L. McGuirk, MD
DONALD L. MCGUIRK, MD joined the Colorado Permanente Medical Group in June of 1980. Previous to that, he workedin private practice, and as a pediatrician in the United States Air Force. Doctor McGuirk moved to Kansas City and joined
the Permanente Medical Group of Mid-America five years ago. He has been the Executive Medical Director for three years.E-mail: [email protected]
Many PMGphysicians believethat managed careas conducted by
our for-profitcompetitors
intrudes on thatrelationship.

86 The Permanente Journal / Fall 1999 / Volume 3 No. 3
a w
ord
fro
m t
he m
ed
ical
dir
ect
ors
when several approaches have equal effectivenessbut one approach costs substantially less), medicalspecialty societies could help physician members toregain the control they so desperately seek.
Some contend that the second condition requiredto forestall giving employees and/or health insur-ance companies a right to intrude into the physi-cian/patient relationship is that the physician/pa-tient team be willing to make cofiduciary decisions.I strongly recommend the controversial and pro-vocative paper written by Laurence B. McCulloughon this issue.2 By “cofiduciary,” McCullough meansthat ethically clinical decisions must not only bebest for the individual patient but must also be popu-lation-based. “The regulation of clinical judgment,decision making, and behavior should be developedand implemented on the basis of rigorous scientificevaluation of processes of care, to identify thosethat can be reliably expected to produce a greaterbalance of goods over harms for patients as thesegoods and harms are identified and balanced in arigorous clinical perspective that will define themedically necessary”.2:94
McCullough suggests that without the physicianand patient being willing to at least consider theirdecision in the light of all patients as well as the
one patient involved, the financial decisions paidfor by others cannot be put into perspective. Thisidea is indeed controversial. Some will say that thisscenario will never take place. Trust and confidenceare mandatory for the patient/physician relationshipto work. For the participants in this relationship toconsider others during deliberations will be a sig-nificant challenge.
Without this “reality check,” however, some willsuggest that the system will eventually collapse un-der its own economic weight. If these commentatorsare right, this collapse cannot be allowed to occur; itwill be stopped by seizure of the financial controls—if not by employers or the insurance companies, thenpresumably by the government in some form—andthe control desired by physicians and patients willundoubtedly erode. ❖
This editorial reflects the personal opinion of the author, and not
necessarily that of PMG of MA or Kaiser Foundation Health Plan.
References1. Shem S. The House of God: a novel. Chapter III, p. 420 (NewYork: R. Marek Publishers, 1978).2. McCullough LB. A basic concept in the clinical ethics ofmanaged care: physicians and institutions as economicallydisciplined moral co-fiduciaries of populations of patients. JMed Philos 1999;24:77-97.
My DoctorNever stay in treatment with a doctor who thinks that you can’t get better.
Andrew Weil, MD, “Spontaneous Healing”
Trust andconfidence are
mandatory for thepatient/physician
relationship towork.

87The Permanente Journal /Spring 2000 / Volume 4 No. 2
health
syste
msAdapted from material previously published in: Group Practice
Journal 2000 May:49(5):37-8,40,40-2,44-6.
IntroductionTo fully capture the increased efficiency, multiple
patient care benefits, and economic advantageswhich group visit programs can provide, it is im-portant that these programs be set up in a grouppractice or managed care organization so as to bewell designed, adequately supported, and properlyrun. A carefully thought-out group visit program canmaximize benefits to patients, physicians, purchas-ers, insurers, and health care organizations alike;however, it is very important that any potentials forabuse also be thoroughly examined and scrupulouslyprevented if the benefits of the program are to befully realized.
In another article,1 we described three differentmodels of group medical visits: the CooperativeHealth Clinic of Colorado (CHCC),2,3 SpecialtyCHCC,2,3 and Drop-In Group Medical Appointment(DIGMA)4-18 models. These models are designed toserve different patient groups, and the effectivenessof these models depends upon meeting the needsof these patients at any given time as they try to livewell despite one or more medical problems. Thesemodels are not mutually exclusive and work best ifcombined as patients’ needs change over time. Forexample, geriatric patients with multiple medicalproblems including diabetes and hypertensionwould do well in a CHCC setting, might benefit froma specialty diabetic or hypertension group, and coulduse their own physician’s DIGMA for continuity ofcare and for convenient routine blood glucose andblood pressure monitoring.
By definition, group visits (ie, group medical visitsor group appointments) include delivery of medicalcare in a group setting with other patients—in fact, itis the delivery of medical care in a group setting thatis the core characteristic of a group visit. However,because DIGMAs, CHCCs, and Specialty CHCCs dif-fer in structure and function, each model suggeststhe need for different precautions to be taken duringplanning and implementation. This article outlinespotential pitfalls inherent in implementing eachmodel. These pitfalls can involve administrators, phy-sicians, or patients.
Emergence of Group Visits inMainstream Medical Care
Group visit programs are rapidly proliferating ingroup practice and managed care organizationsthroughout the United States in an effort to leverageexisting resources and to provide high-value, high-quality health care in this era of increasing purchaserand patient demands for enhanced services at reducedcost. Substantial economic pressures are at work intoday’s rapidly changing, highly competitive healthcare environment. Despite working long hours and ashard and efficiently as possible, many physicians arenonetheless finding that their patient panels are be-coming larger, that access problems are emerging, andthat the increasing size of their practices is makingthem difficult to manage. Others are striving to moveto same-day access but are finding that they need atool such as group visits to help them achieve andthen maintain this level of accessibility.
Health care organizations must address the fact thatinsufficient financial resources exist in the system tosolve problems of workload, access, utilization, ser-vice, and quality of care solely through traditionalmeans (ie, simply by hiring more physicians to giveindividual patient care). Despite organizational inertiaand physician resistance to change, innovative groupvisit programs are gradually but steadily emerging inan effort to increase efficiency, leverage physician time,improve service and quality of care, and better man-age high-risk patient populations. Various types ofproven group visit programs will be used increasinglyin the delivery of health care because of their abilityto provide better, more efficient care at reduced costand to create high levels of both patient and providerprofessional satisfaction. Therefore, it is important tosafeguard against any potential for abuse and to be-gin planning for this possibility now.
Major Group Visit ModelsMost group visits and programs for managing high-
risk patient populations use one of two major groupvisit models which have emerged in recent years.1
The Kaiser Permanente Cooperative Health CareClinic in Colorado focuses on patient populationseither by utilization behavior (eg, the CHCC modelfor high-utilizing geriatric patients) or by disease
Potential Abuses of Group Visits
By Edward B. Noffsinger, PhDJohn C. Scott, MD
EDWARD B. NOFFSINGER, PhD (left), worked as a psychologist for The Permanente Medical Group for more than 26years, before retiring a year ago. Prior to TPMG, he worked as a physicist at Xerox Corporation and Bell and Howell
Company. Dr Noffsinger now consults in the area of DIGMAs and group visits.He can be reached at (831) 427-1011 or (831) 458-3388.
JOHN C. SCOTT, MD (right), practices in the Primary Care Department of Kaiser Permanente Hidden LakeMedical Offices, Colorado Permanente Medical Group, Westminster, Colorado; and is a clinical faculty member
in the Department of Geriatrics, University of Colorado Health Sciences Center, Denver, Colorado.E-mail: [email protected]
... it is the deliveryof medical care in
a group setting thatis the core
characteristic of agroup visit.

88 The Permanente Journal / Spring 2000 / Volume 4 No. 2
healt
h s
yst
em
s
state (eg, the Specialty CHCC model), which is thefoundation for programs which manage high-risk pa-tient populations such as those with diabetes, asthma,hypertension, hyperlipidemia, congestive heart failure,depression, and irritable bowel syndrome.2,3
The other major group visit model, the Drop-InGroup Medical Appointment (DIGMA) model, wasoriginated by Dr Noffsinger in 1996 at the KaiserPermanente San Jose Medical Center. The DIGMAmodel focuses not on patient populations by eitherdisease state or utilization behavior, but instead on
A carefully thought-out group visit program can maximize benefits topatients, physicians, purchasers, insurers, and health care organizationsalike; however, it is very important that any potential for abuse also bethoroughly examined and scrupulously prevented if these benefits are tobe fully realized.
Simply stated, health care organizations can “shoot themselves in the foot”if they fail to minimize the risk for abuse while maximizing the benefits ofwell-run group visit programs. Minimizing this risk will ensure continuedsupport from patients, physicians, purchasers, and insurers.
In today’s challenging, competitive health care environment, group visitscan be abused in two basic ways: 1) by putting fewer resources into groupvisits than adequately supported, properly run programs require, or 2) byattempting to extract more from group visits than is commensurate withgood care.
If we wait until some abuse of group visits actually occurs and receivesnegative publicity, we could incur a public relations “black eye,” whichcould seriously undermine the credibility of all such programs in the fu-ture—a predictable, preventable, and completely unnecessary injury to theimage of group visit programs.
Should third-party insurers, upon recognizing the multiple economic andpatient care benefits which group visits can offer, overincentivize them rela-tive to individual visits, abuse could result which would reduce the volun-tary nature of group visits for physicians and patients alike.
An interesting observation is that group and individual visits work welltogether and complement each other: the strengths of one model are oftenthe weaknesses of the other, and vice versa.
Despite all of these concerns surrounding potential abuses, group visitswill undoubtedly continue to grow in importance and be ever more fre-quently used during the coming years. Without question, group visits havean important role to play in the future of health care.
Well-designed, adequately supported, and properly-run group visit pro-grams (such as DIGMAs, CHCCs, and high-risk patient population manage-ment programs—Specialty CHCCs) not only offer the benefits of greaterefficiency and reduced costs through economies of scale but also offer theadditional benefits of improved access, comprehensive mind-body care,better follow-up monitoring, and increased patient and physician profes-sional satisfaction.
the entire patient panel of each individual physician.4-19
The DIGMA is an extended medical appointment withthe patient’s own physician, held in a supportivegroup setting. Open only to the physician’s own pa-tients, each DIGMA is custom-designed around thespecific needs, goals, practice style, and patient panelconstituency of the individual physician. Specificallyfocused on improving accessibility and enabling phy-sicians to both leverage their time and better man-age their entire patient panel, DIGMAs have beenshown to dramatically increase physician productiv-ity in a way which enhances patient and physicianprofessional satisfaction while improving service,access, and quality of care.9,10
As is true of traditional office visits, DIGMAs ad-dress whatever medical needs patients bring to themedical visit as well as routine health maintenanceissues. However, due to the greater amount of timeavailable and the presence of both the behavioralhealth professional and the group itself, the needs ofboth mind and body can be comprehensively at-tended to. DIGMAs give patients what they most want:prompt access, high-quality health care, and moretime with their own doctor.
In addition to other successful models that might bedeveloped in the future, the CHCC, Specialty CHCC,and DIGMA group visit models can be expected toplay an increasingly important role in tomorrow’s healthcare environment. These models work well not onlyas stand-alone programs but also when combined;indeed, combining these models can provide evengreater efficiency than either model alone.
The Need for Safeguards Against AbuseNot only must the group practice or managed
care organization implementing a group visit pro-gram ensure that the program is properly designed,adequately supported, and well run; potentialabuses must also be considered, and proper safe-guards put in place. These new and innovativegroup visit models carry a real potential for beingabused, and such abuse could both undermine thecredibility of the entire program and severely re-duce the economic, patient care, and productivityadvantages that they offer.
Simply stated, health care organizations can “shootthemselves in the foot” if they fail to minimize therisk for abuse while maximizing the benefits of well-run group visit programs. Minimizing this risk willensure continued support from patients, physicians,purchasers, and insurers.

89The Permanente Journal /Spring 2000 / Volume 4 No. 2
health
syste
msThe group visit experience must be professional
and of high quality. This is achieved through thespecific advantages which group visits offer: addi-tional time available, a more relaxed pace of care,increased efficiency and productivity, closer follow-up care, a focus on the needs of mind as well asbody, and the information and support provided byothers. Group visits integrate all these advantagesinto each patient’s health care experience.
In today’s challenging, competitive health care en-vironment, group visits can be abused in two basicways: 1) by putting fewer resources into group visitsthan adequately supported, properly run programsrequire, or 2) by attempting to extract more fromgroup visits than is commensurate with good care.Problems in both of these areas can be reasonablyanticipated as group visit programs continue to pro-liferate. Abuse must therefore be vigilantly and con-tinuously guarded against if group medical visits areto retain credibility in the eyes of patients, purchas-ers, physicians, insurers, and health care organiza-tions. From the outset, professional and ethical con-straints, as well as “checks and balances,” will berequired as group visit programs continue to emerge.
The Importance of Addressing PotentialAbuses Now
As the originators of the CHCC and DIGMA mod-els, the authors are staunch advocates of well-de-signed, properly run group visit programs becausethey offer increased efficiency and multiple economicand patient care benefits—a “win-win-win” situationfor consumers, providers, and insurers. Even at thisearly stage in the development of group visit pro-grams, one is able to glimpse into the future, wherefull-scale implementation of group visits is likely toplay a substantial role in health care delivery. Groupvisits represent an important tool for achieving im-proved access and optimal value, both in the medi-cal services currently being delivered and in the cost-effective delivery of high-quality health care in theincreasingly integrated systems of the 21st century.
However, the authors already have concerns re-garding the potential for abuse of group visits. Safe-guards against this abuse must be built in from theoutset. Organizational self-interest demands that theseconcerns be addressed—even at this early stage inthe development of various group visit programs—before fee-for-service billing codes are developed forgroup visits and before these programs become wide-spread and begin to play a major role in the delivery
of health care. If group visit programs are to achievetheir full potential (which would include buy-in bycorporate purchasers, patients, physicians, health careorganizations, and insurers), abuse must be avoidedat all cost.
If we wait until some abuse of group visits actu-ally occurs and receives negative publicity, we couldincur a public relations “black eye” which couldseriously undermine the credibility of all such pro-grams in the future—a predictable, preventable, andcompletely unnecessary injury to the image of groupvisit programs.
Because group visit programs such as DIGMAs,CHCCs, and high-risk patient population managementprograms (ie, Specialty CHCCs) offer a “win-win-win-win” situation for patients, physicians, health careorganizations, and insurers, everyone has much togain from well-run group visit programs. Therefore,we must be careful to avoid jeopardizing these ben-efits by succumbing to any temptation for abuse, theultimate consequence of which could be rejection ofall group visit models.
This paper examines potential abuses of group vis-its from the perspectives of patients, physicians, healthcare organizations, and insurers.
Preventing Patient Abuses of Group VisitsAbuses can be either intentional or unintentional.
Along with the physician who is providing medicalcare, patients are in fact primary caregivers in chronicdisease management because they have the most first-hand experience in coping with illness and in devel-oping the requisite coping skills. Patients are alsothe key ingredient in the interactive educational pro-cess which occurs in the group medical visit milieu;and patients must be reminded of this as well asvalued for it.
Although no one is required to comment at anyspecific time during the group visit, relationshipsbetween patients as well as healthy group dynamicsare key to building self-efficacy skills and enablingpatients to help one another. Conversely,nonparticipation adversely affects both the groupdynamic and the benefit to each patient. Therefore,patients need to be encouraged to speak up openlyand candidly.
The entire group visit environment must be de-signed to foster feelings of safety, trust, and comfortso that patients will be willing to speak up. Whenone person has a question, it is a virtual certaintythat three or four other people have either the same
The entire groupvisit environmentmust be designed
to foster feelings ofsafety, trust, andcomfort so thatpatients will be
willing to speak up.

90 The Permanente Journal / Spring 2000 / Volume 4 No. 2
healt
h s
yst
em
s
question or another facet of that question which needsto be addressed. However, for this participation tooccur, patients must trust the group visit experience—and this trust cannot grow unless patient abuses arescrupulously guarded against.
Do Not Restrict Access to Individual VisitsRestricting access to traditional individual office visits
could precipitate unintended consequences and beperceived by patients as an abuse of group visits. Allpatients attending group visit programs such asDIGMAs, CHCCs, or Specialty CHCCs must be fullyinformed both that participation in these programs iscompletely voluntary and that patients who attendthem are always entitled to still have individual ap-pointments as needed. Using group visits to largelyor completely replace individual office visits wouldviolate this important condition and would restrictpatient access to the appropriate use of individualoffice visits. Everyone should remember that groupvisits are tools for providing better care, for helpingphysicians to more efficiently manage their largepatient panels, and for improving access to medicalcare; group visits are not meant to completely re-place individual appointments or to give health careorganizations an excuse to drastically reduce spe-cialty and primary care staffing.
Group visit programs are designed to offer the ad-vantages of increased efficiency, cost reduction, im-proved service, and more comprehensive attentionto the needs of mind and body. Nonetheless, judi-cious use of individual appointments will always playan important role in health care delivery: Throughproper use of group visits, patients best treated bygroup visits will be appropriately seen in group ap-pointments, whereas patients who require individualappointments can still be seen individually.
Group visits excel in treating the relatively stablechronically ill, the “worried well,” patients who arelonely or who have extensive emotional and psy-chosocial needs, patients who need more physiciancontact and professional “hand holding,” and patientswho require closer follow-up monitoring, surveillance,and care. Individual visits are usually superior forinitial evaluations, one-time consultations, lengthy in-dividual examinations, care of rapidly evolvingmedical conditions, acute infectious illnesses, mostmedical procedures, and for patients who refusegroup visits.
Despite the almost certain rapid future growth ofefficient and cost-effective group visit programs, pa-
tients will always have a need for individual care inthe fully integrated health care delivery systems oftomorrow. Using group visits to largely or completelyreplace individual visits would cause purchasers,patients, and physicians to lose confidence in groupvisit programs.
Make Group Visits Voluntary, Not MandatoryThe authors’ group visit models were designed to
be completely voluntary for patients as well as forstaff and to give patients both freedom of choice andimproved care. To insist that patients attend a groupvisit program despite their reluctance to do so wouldnot only probably prove unsuccessful but would alsobe an abuse of the group visit concept. Patients whorefuse group visits should never be forced to attend,and traditional office visits should always be madeavailable to such patients.
However, when an individual appointment is re-quired, two points are worth noting: 1) becausegroup visit programs are designed to convert nu-merous individual visits into group visits, individualvisits are eventually made more accessible to pa-tients who want or need them; and 2) as patientsbecome more familiar with the group visit programand hear positive comments about it from otherpatients (for example, in the physician’s lobby byhearing favorable remarks from other patients dis-cussing their recent group visit experience whilewaiting for an individual office visit), the number ofpatients who refuse group visits has been observedto decline over time. An important component towinning patients over to group visits is to have phy-sicians use 15 to 30 seconds during every routineoffice visit to personally invite suitable patients tohave their next visit be a group visit.
Always Address Confidentiality and Privacy Concerns
Group visit programs must address any concernsthat patients might have regarding privacy and con-fidentiality. Time must be allocated during each groupvisit session for patients to be able to have a briefprivate discussion or a brief individual examinationwith their physician as needed.
Confidentiality issues have seldom, if ever, beenbrought up by patients in DIGMA and CHCC visits.The rarity of these concerns is due in part to thesegroup visit models being designed and conductedwith sensitivity to patients’ confidentiality and pri-vacy needs. For example, in the DIGMA model, pa-tients are told at the beginning of each group session
Patients who refusegroup visits shouldnever be forced to
attend, andtraditional office
visits should alwaysbe made availableto such patients.

91The Permanente Journal /Spring 2000 / Volume 4 No. 2
health
syste
ms(as well as in fliers describing the group visit pro-
gram and by the physician and staff when invitingpatients to join the program) that any patient whowants to speak to the doctor in private or who wantsor needs a brief private examination will be giventhat opportunity toward the end of the group ses-sion. In the CHCC model, one-to-one time with thehealth care team is available both during the breakand at the end of the group session.
In addition, physicians who have concerns aboutconfidentiality in their group visit program can giveall attendees a brief informed consent/full disclosuredocument describing the limits of confidentialitywhich requires the patient’s signature. This documentcan be distributed at the beginning of each groupsession and can fully explain the limits of confidenti-ality in the group visit format, the availability of someone-to-one time with their physician during the groupsession, and that all patients attending a group visitprogram are still welcome to schedule individualappointments as needed.
Provide Adequate Facilities
Adequate facilities must be provided for all groupvisit programs. These facilities include convenientlylocated group rooms which are sufficiently large,adequately ventilated, and wheelchair-accessible withbathrooms nearby. The group room should be com-fortable, well-lighted, clean, and equipped withenough chairs to accommodate all participating pa-tients, support persons, and staff. A well-stockedexamination room should be located nearby andcontain all appropriate equipment and referral forms.
If no appropriate group room is available, creativ-ity is required: Consider using conference rooms,unused space which could be converted to grouprooms, or even the lobby during off-hours. If nosuch space is available for use as a group room,then consider taking the group visit program offcampus to a nearby building or even into the com-munity. Although health care organizations mayneed to make do with whatever facilities are avail-able during the pilot phase of evaluating group visitprograms, the obvious long-term solution (as theymove toward full-scale, organizationwide implemen-tation to fully capture the increased economic andpatient care benefits that group visits can provide),is to reinvest a portion of the savings which groupvisits provide into retooling the physical plant inorder to provide enough appropriate group andexamination room space.
If no examination room is located in the vicinity ofthe group room, consider converting nearby space(such as a staff break room) to an examination roomfor the group. If all else fails, consider improvisingan examination room by curtaining off one corner ofthe group room. In any case, always be careful toensure that patients’ privacy needs are attended toand that they are kept comfortable throughout thegroup visit session by use of adequate group andexamination room facilities.
Provide Marketing Materials Which Have aProfessional Appearance
Some group practices, HMOs, and managed careorganizations might be tempted to consider savingmoney by not using professional-appearing market-ing materials to make patients aware of the program.Instead of using carefully designed text and coordi-nated graphics for both the framed wall posters (ie,mounted in the physician’s lobby and examinationrooms) and program description fliers (ie, containedin a clear plastic dispenser mounted next to theposter), the organization might be tempted to tapeto the wall a cheap announcement hurriedly pro-duced on somebody’s copier or personal computer.Worse yet, the organization might be tempted to omitthese materials entirely.
Because patients have come to expect individualoffice visits with their physician, posters and fliersdescribing new group visit programs must be dis-played prominently in appropriate places through-out the medical center if we want to adequately in-form patients about new group visit programs andexpect them to attend. In addition, informationalmaterials must have a professional appearance toaccurately represent the high quality of medical carewhich properly run group visit programs provide.The graphic design of the wall posters can be usedas a template to establish a particular look for allmarketing materials for all such group visit programsdeveloped at that facility.
Excessive attempts to save money in this area willcause patients to be inadequately informed aboutnew group visit programs and the many patient carebenefits they provide. This result would not onlyundermine the success of the entire program butwould also be unfair to patients who would want toattend if they knew about the new program and un-derstood its benefits.
The appropriate way to save money in the area ofmarketing materials is to use the same high-quality
... physicians whohave concerns
aboutconfidentiality intheir group visit
program can giveall attendees abrief informedconsent/fulldisclosuredocument
describing thelimits of
confidentialitywhich requires thepatient’s signature.

92 The Permanente Journal / Spring 2000 / Volume 4 No. 2
healt
h s
yst
em
s
graphics on all wall posters and fliers so that thematerials look expensive even though they are not.By developing a graphic design template for all groupvisit programs, DIGMA organizers can generate anyfuture posters and fliers from the template at mini-mal cost while preserving the professional appear-ance of the original; only the names of both the groupand the physician will need to be changed. Addi-tional savings can be realized by using inexpensive,premanufactured frames to complement the graphicdesign of the poster at minimal expense.
Use of inappropriate, cheap-appearing, or sloppymarketing materials is likely to result in poor atten-dance, lack of patient buy-in, reduced efficiency andproductivity, and lack of success for the group visitprogram. Omission of all marketing materials—wallposters, program description fliers, announcements,and follow-up letters—could even more seriouslyundermine the success of the program.
Schedule Adequate Time for the Number of PatientsAttending
To fully realize the benefits which well-runDIGMAs, CHCCs, and Specialty CHCCs can offer topatients, group visit sessions must be long enoughfor all attendees to receive a high level of care. There-fore, 90-minute DIGMAs should include not morethan 15 to 20 patients (not counting caregivers orfamily members), even though larger groups haveon several occasions been successful. One-hourDIGMAs should not include more than 13 patients,and two-hour DIGMAs should not include more than25 patients. Similarly, 2.5-hour CHCC visits shouldnot include more than 25 patients. We have ob-served that, when group visit census exceeds thesenumbers, patients begin to feel rushed, personal-ized care is diminished, and patients bond less withone another. In addition, if insufficient time is avail-able to adequately attend to each patient ’smind-body medical needs, then patients might be-gin to view the group visit program as a class or asupport group instead of a medical appointment ina group setting.
Sessions which include too many patients and toolittle time constitute an abuse of group visits be-cause such sessions sacrifice the high levels of qualityof care, service, patient satisfaction, and physicianprofessional satisfaction which group visits are in-tended to deliver. Carefully designed and properlyrun group visit programs offer substantial cost sav-ings by increasing physician productivity and effi-
ciency while providing a myriad of patient and phy-sician benefits. Group visit organizers should notbecome greedy by driving the time available perpatient below acceptable limits in a misguided ef-fort to achieve even more productivity and evenlower costs; this effort is likely to result only in re-duced quality of care and decreased patient andphysician professional satisfaction.
Avoid Holding Group Visits Too Infrequently
If group visits are to be successful, they must beheld with adequate frequency. DIGMAs are typicallyheld weekly and occasionally held biweekly, althoughthey could be held daily if the demand is high enough.CHCCs designed to accommodate high-utilizing ge-riatric patients are typically held monthly. SpecialtyCHCCs are held at more variable time intervals, de-pending on the particular needs of each patient popu-lation (ie, populations selected by diagnosis).
Consider, for example, the CHCC model—whereadequate frequency of visits appears to be critical tosuccess. In this model, increased contact with pa-tients in the group format is not only clinically ben-eficial but also facilitates identification of problemsbefore they become crises. A recent two-year studyof a quarterly group intervention held every threemonths in a frail elderly population failed to showany effect on utilization, falls, incontinence, etc.20
Experience at the Cooperative Health Care Clinicin Colorado has shown that if a monthly CHCC ses-sion is canceled for any reason, a large percentageof its patients will make an individual appointmentduring the weeks after the scheduled meeting.Whether this occurrence is psychologically motivated(eg, by a need to “touch base” with the physician) ormedically necessary has not yet been studied. In ei-ther case, infrequent meetings seem to result in in-creased utilization of individual visits. Therefore, al-though other explanations might also account forthese data, one possible interpretation is that monthlyCHCC meetings are sufficient to meet high-utilizinggeriatric patients’ needs whereas quarterly CHCCmeetings are not.
Preventing Physician AbusesAvoid issuing “top-down” demands for all physi-
cians to provide group visitsFrom their inception, DIGMAs, CHCCs, and Spe-
cialty CHCCs were intended for use by interestedphysicians on a voluntary basis to provide better andmore cost-effective care, to increase productivity and
... if a monthlyCHCC session iscanceled for anyreason, a large
percentage of itspatients will make
an individualappointment
during the weeksafter the scheduled
meeting.

93The Permanente Journal /Spring 2000 / Volume 4 No. 2
health
syste
msefficiency, and to enable physicians to better man-
age their large medical practices. The authors alwaysenvisioned that physician participation would beentirely voluntary and achieved out of self-interest atthe grassroots level—ie, achieved “from the bottomup” instead of being imposed upon physicians “fromthe top down” by administration. “Top-down” impo-sition of group visits is likely to engender resent-ment, distrust, and passive-aggressive resistanceamong physicians.
Group visits must not be mandated for patients,physicians, nurses, medical assistants, schedulers,or nurses. All staff, including any guest speakers,must share in the positive perspective and enthu-siasm which are required if the group visit programis to succeed. Reluctant participants communicatetheir resistance—if only through their body lan-guage—and inhibit the beneficial effect of thegroup process.
We strongly encourage that group medical prac-tices, managed care organizations, and HMOs inter-ested in establishing group visit programs implementthem initially at a pilot site and then, if successful,eventually disseminate them throughout the organi-zation. This gradual approach allows physician buy-in to develop on a voluntary basis at the grassrootslevel. To insist that physicians participate in groupvisit programs, regardless of whether they want to ornot, would not only be self-defeating but would alsoconstitute physician abuse of group visits as they wereoriginally conceived (ie, as a way to help physiciansinstead of burdening them).
Do Not Create Large Increases in Patient Panel Size
In an earlier article, Dr Noffsinger cautioned againststripping away most or all of the benefits which groupvisits provide for physicians (eg, increased produc-tivity and efficiency) through a corresponding largeincrease in the physician’s patient panel size.5 Physi-cians express this concern by asking, “Why should Istart a group visit program when the net long-termeffect will be 1000 more patients added to my panel?”Physicians in capitated systems are concerned thatparticipation in a group visit program (which theyotherwise might consider implementing to increaseproductivity and better manage a large practice)would only result in a corresponding large, long-term net increase in patient panel size. From thephysician’s perspective, this result would completelynullify any net gain in efficiency that the group visitprogram might provide.
To create a “win-win-win” situation for patients,physicians, and health care organizations, physicianstoo must derive a substantial long-term net benefitfrom the increased productivity and efficiency pro-vided by their DIGMAs or CHCCs. Physicians viewthis matter as one of fairness and trust.
A health care organization seeking to realize themany patient, physician, and organizational benefitsoffered by group visits must adopt long-term busi-ness policies which build physicians’ trust and whichprovide benefits to physicians as well as to patientsand to the organization. Physicians in capitated andfee-for-service practices need reassurance from ad-ministrators that implementation of a DIGMA, CHCC,or Specialty CHCC for their practices will producesome meaningful long-term net benefit to them-selves. Physicians in capitated systems must be as-sured that any future increase in panel size result-ing from the increased efficiency that the group visitprogram provides will be reasonable, so that theywill nonetheless be left with a substantial net gainfor their efforts.
Avoid Excessively Large Group Sizes
Because increased physician professional satis-faction is a primary objective of the DIGMA andCHCC models and because physician buy-in is criti-cal to success of these models, insistence on overlylarge group census (ie, imposed to extract evengreater physician productivity) would be self-de-feating and would constitute an abuse of thesegroup visit models. It is important that all aspectsof the group visit program stay within thephysician’s zone of comfort—professionally, ethi-cally, and in terms of productivity.
The limiting factor for maximum group censusappears to be physician professional satisfaction.For 90-minute DIGMAs, physicians seldom likegroup census to exceed 22 members, even thoughpatients have been satisfied with considerably largergroup sizes. For example, after the conclusion ofone particularly large DIGMA session of 28 attend-ees, the group gave the physician a standingovation; nonetheless, the physician felt that thelarge size of the group created excessive workloaddemands. Therefore, because physician profes-sional satisfaction remains a priority, the groupcensus for 90-minute DIGMAs should not gener-ally exceed 22 members. Of course, the DIGMAmodel cannot completely prevent occasions whenthis number is exceeded; no organizer can com-
Therefore, becausephysician
professionalsatisfaction
remains a priority,the group census
for 90-minuteDIGMAs should
not generallyexceed 22members.

94 The Permanente Journal / Spring 2000 / Volume 4 No. 2
healt
h s
yst
em
s
pletely control for the number of patients who willdrop into any given session.
An interesting observation is that, in actual practice,the greatest census-related problem is not frequentexcesses in group census; this problem happens oc-casionally, but not often. Instead, the greatest prob-lem appears to be establishing (on the basis of medi-cal economics) and then consistently maintaining aminimum group census for each group visit program.
An exception to this recommended maximum groupcensus can be made for DIGMAs conducted bysubspecialists whose patient panels have substantialemotional and psychosocial needs. This exceptionwould thus apply to nephrology, oncology, and rheu-matology DIGMAs; for these DIGMAs, experiencehas shown that the group census can occasionallybe set slightly higher.
Reward Physicians by Giving Them Time
In the effort to increase access to care, administra-tors might be tempted to allow physicians just enoughtime to conduct the group visit for 15 to 25 patients,often high-intensity patients, and then expect thephysicians to rush back to the clinic to see a largenumber of “routine” patients (ie, those who haveacute minor illnesses or who come to the clinic on awalk-in basis) immediately after the group is over. Ina fee-for-service practice, physicians may choose todo this to maximize productivity and revenue; how-ever, in a capitated health care environment, this prac-tice provides little incentive for physicians to be moreefficient and is even a disincentive.
To ask physicians to be doubly efficient by seeingsubstantially more patients but reward them withnothing but more work will not help in the effort torecruit physicians to care for the burgeoning chroni-cally ill population. Instead, consider providing phy-sicians participating in group visit programs a mean-ingful reward such as additional time for “desktopmedicine”—ie, phone calls and paperwork.
Provide Adequate Preparation and Training
If a group visit program is to be successful, suffi-cient staff preparation time and training must be pro-vided. For example, the DIGMA model not only re-quires that the physician be prepared for his or herrole in the DIGMA and know how to refer patientsinto it but also requires that training be provided forthe other members of the DIGMA team (ie, the cham-pion, behavioral health professional, nurse or medi-cal assistant, scheduler, and reception staff).
When starting out with the CHCC model, the tradi-tional, minimal-preparation method (ie, “see one, doone, teach one”) works reasonably well; however, ifmore than five or six groups are implemented, andespecially if they are in different facilities, formal ori-entation and coaching of providers and patients be-comes more important, as does subsequent monitor-ing of both quality and effectiveness of the groups.Our experience has shown that, ideally, these trainingand monitoring functions are done by a nurse-admin-istrator, who can maintain as many as 40 or 50 CHCCgroups with the help of a monitoring checklist.
Evaluate the Effectiveness of the Group Visit Program
Physicians’ professional satisfaction can be enhancedby showing the physicians that the group visit pro-gram is achieving its intended objectives in terms ofcost savings, improved access, reduced utilization, le-veraging of physician time, and increased levels ofpatient satisfaction, service, and quality of care.
This assurance is reasonable because group visitsrequire physicians to deliver medical care in a waydramatically different from the individual office visitmodel, in which physicians have traditionally beentrained and have become comfortable. If physiciansare to be satisfied with the expenditure of time andeffort necessary to adapt to the DIGMA or CHCCmodels, then they must receive a demonstrable ben-efit for this time and effort. The same is true for ad-ministrators in the health care organization.
The importance of the evaluation process needs tobe emphasized. If use of group visits is to continueto grow and if they are to eventually be assigned aCPT code, ongoing documentation must show theeffectiveness, efficiency, and consistency of thesemodels in achieving their desired objectives.
Do Not Require Physicians to ConductGroup Visits Alone
Demanding that physicians run group visit pro-grams alone (ie, without the assistance of importantsupport personnel such as behavioral health profes-sionals, nurses, medical assistants, schedulers, andreception staff) to further reduce costs would consti-tute an abuse of group visits. Physicians would dislikethis demand, and professional satisfaction woulddecrease. In addition, such an arrangement wouldbe unlikely to succeed because those support per-sonnel play critical roles in the CHCC and DIGMAmodels. Further, it is the use of the less costly sup-port personnel associated with the DIGMA, CHCC,
Instead, considerprovidingphysicians
participating ingroup visitprograms a
meaningful rewardsuch as additionaltime for “desktopmedicine”—ie,phone calls and
paperwork.

95The Permanente Journal /Spring 2000 / Volume 4 No. 2
health
syste
msand Specialty CHCC group visit models that enables
expensive physician time to be so highly leveraged.For example, consider the DIGMA group medical visit
model, which was designed to be led jointly by a phy-sician and a behavioral health professional (eg, healthpsychologist, social worker, marriage and family thera-pist, nurse, or health educator) who possesses special,complementary skills for addressing group dynamic,emotional, and psychosocial issues. The behavioralhealth professional starts the group on time—even ifthe physician is late; handles group dynamic and psy-chosocial issues; keeps the group running smoothlyand on time; takes primary responsibility for maintain-ing group census; conducts the group alone when thephysician is called out on an emergency or leaves thegroup to conduct brief private examinations; and doeseverything possible to enable the physician to focus ondelivering high-quality medical care.
Presence of a carefully selected behavioral healthprofessional who is experienced in running groups,handling group dynamics, and in addressingpsyochosocial needs (and who is trained to assistthe physician in running the DIGMA and is wellmatched to both the physician and the patients) iscritical to success of the DIGMA. Enjoyable camara-derie and occasional bantering also occur betweenthe physician and the behavioral health professional—which has been found to enhance physician profes-sional satisfaction. Some physicians might be able torun the DIGMA alone, but not even one physicianhas indicated any interest in doing so—even thoughmore than 9000 DIGMA patient visits have beenlogged in 22 different DIGMAs to date.
Prevent Physician Abuse of Group VisitsIn addition to being misused by the organization,
group visits can also be misused by physicians. Forexample, consistent lateness of physicians in arriv-ing at their group sessions is likely to leave insuffi-cient time to adequately attend to all patient needs.Similarly, although support personnel are trained toaddress most of the details in designing, implement-ing, conducting, and evaluating the group visit pro-gram, some physician involvement is nonethelessrequired during each phase.
Physicians cannot realistically expect a group visitprogram to be designed for them solely throughthe efforts of others without investing any personaltime and effort. In addition, physicians must playan active role in achieving and maintaining the de-sired level of group census. This participation can
be achieved if physicians take 15 to 30 secondsduring every routine office visit to personally invitesuitable patients to have their next visit be a DIGMAvisit. Similarly, physicians must continually adviseall personnel associated with the program regard-ing which activities are being done satisfactorily orunsatisfactorily, what improvements still need to bemade, and what suggestions the physician wouldmake as to how to achieve the desired results.
Avoiding Organizational andInsurance AbusesDo Not “Overincentivize” Group Visits
Clearly if insurers and health care organizationsunderincentivize group visits through inadequatereimbursement and support, there would be no rea-son or incentive for physicians to substantially altertheir style of practice from traditional one-on-one careto include the offering of group visits. Clearly,underincentivizing group visits would undermine theentire program and preclude its widespread use.
However, there is another concern as well, andone that is less obvious: Once insurers and healthcare organizations become aware of the substantialeconomic and patient care advantages that group visitsoffer, they could overincentivize them relative to in-dividual office visits.
The authors have concerns regarding the long-term potential for abuse of group visits byoverincentivizing them at the expense of individualvisits. These excessive incentives would reduce free-dom of choice for patients as well as for physicians.In addition, an effective, fair billing system must bedeveloped with appropriate billing codes for thedifferent types of group visits; however, after sucha billing system has been developed, it must befollowed honestly and scrupulously by physiciansand health care organizations alike.
At present, the authors are aware of no fee-for-service or Medicare billing codes specifically designedfor group medical visits. Should third-party insurers,upon recognizing the multiple economic and patientcare benefits that group visits can offer,overincentivize them relative to individual visits, abusecould result that would reduce the voluntary natureof group visits for physicians and patients alike.
Similarly, if health care administrators overincentivizegroup visits in terms of physicians’ future salaries withinthe organization, physicians who would otherwise bereluctant or not be ready to start a group visit programmight feel compelled to do so. The authors strongly
The authors haveconcerns regarding
the long-termpotential for abuseof group visits byoverincentivizing
them at theexpense of
individual visits.

96 The Permanente Journal / Spring 2000 / Volume 4 No. 2
healt
h s
yst
em
s
recommend against this practice because we have al-ways intended that physicians participate in group visitprograms strictly on a voluntary basis. To do otherwisewould create physician resistance to the entire program.
Both Group and Individual Visits Are Important
Group visits are intended to work in conjunctionwith the judicious use of individual visits and not tocompletely replace them. In this way, patients whocan appropriately be efficiently and cost-effectivelyseen in group medical visits will be seen in that venuewhenever possible. By off-loading numerous indi-vidual visits appropriately onto group visits, individualappointments will be made more accessible for pa-tients who need or want them. Both group and indi-vidual visits will be important for the future deliveryof high-quality, cost-effective care. Nowhere will thisimportance be more evident than in the high-valuecare provided by the progressive, fully integratedhealth care delivery systems of the future.
As group visits begin to play an increasingly im-portant role in the delivery of quality medical care,individual visits will nonetheless be expected to con-tinue to play a key role in the delivery of health care.Therefore, it is important that the incentives for bothgroup and individual visits be carefully thought out,appropriate, and fair.
An interesting observation is that group and indi-vidual visits work well together and complement eachother: the strengths of one model are often the weak-nesses of the other, and vice versa. For example,individual appointments are most appropriate foracute infectious illnesses, lengthy individual exami-nations, initial evaluations, one-time consultations,most medical procedures, and care of patients whorefuse group visits. In contrast, group visits are mostappropriate for relatively stable chronically ill patients,patients who are anxious or depressed, the “worriedwell,” patients who are difficult or demanding, pa-tients who have excessive psychosocial and emo-tional needs, and patients who require more timewith their doctor or who require more professional“hand holding.”
Miscellaneous Tips for Group VisitsFacilitate, Do Not Dominate!
In group visits, physicians should be interactiveinstead of giving lectures. The primary benefits ofgroup visits, other than the excellent access andcomprehensive medical care provided, include acombination of shared information, mutual support,
and an enhanced sense of self-efficacy for eachmember of the group. A world of difference existsbetween delivering a lecture on angina and askingthe group: “Has anyone here ever had heart pain?”;“What was it like?” and “What did you do?” In aninteractive group process, several people will re-spond to these questions and relate their own spe-cial stories. The physician acts as a facilitator, addsinformation, emphasizes key points, and elaboratesas necessary.
This interactive model validates participants in theeyes of the other group members. The interactionshows that patients are legitimate sources of infor-mation for coping with particular health problems.Patients’ skills are reinforced by the physician as wellas by the behaviorist or nurse, and everyone benefitsfrom the therapeutic process of the group. Like phy-sicians, patients enjoy being of value to others. Infact, patients often have more “hands-on” experiencein coping with illness and aging than do the provid-ers of care. It is important to validate the patients’role in being their own caregivers.
In addition, physicians providing group visits shouldfeel free to be themselves. Patients choose their phy-sicians on the basis of the way the physicians nor-mally interact with their patients. Physicians neednot try to be either professorial or entertaining in thegroup visit. Patients simply want quality medical careand more time with their physician.
The “bottom line” is that the most important thingis what patients take home with them from the groupvisit session: What they have learned about bettermanaging and coping with their illness. Patients willhave learned much from the physician, from thesupport personnel (behaviorist, nurse, medical as-sistant), and in large part from interacting with otherpatients. Physicians should think of patients as “pri-mary caregivers” who are learning to help them-selves and each other to better manage their healthproblems. A critical aspect of achieving this is tofoster interaction among patients and between pa-tients and staff.
To undermine this sharing of information, mutualsupport, and dynamic interaction would be a mis-take which could easily happen. Group visits canprovoke anxiety in physicians because they have notbeen trained in conducting group visits during medi-cal school and often have had little or no experiencein running groups. Group visits can also be intimi-dating to physicians, as shown by statements suchas: “What if I lose control of the group?,” “What if
Group visits areintended to work
in conjunctionwith the judicioususe of individualvisits and not to
completely replacethem.

97The Permanente Journal /Spring 2000 / Volume 4 No. 2
health
syste
msnegative emotions spiral out of control?,” and “What
if I say something stupid and embarrass myself infront of 15 or 20 of my patients at once?”
Physicians may try to cope with this anxiety bybecoming professorial and turning the group into aclass instead of conducting it as an interactive group.This approach is ultimately self-defeating, however,because it disrupts the normal social interaction andemotional support which group visits can provide. Ifthe professorial approach is adopted—thereby re-ducing the healthy interaction both among patientsand between patients and staff—the group visit can-not be nearly as helpful to patients, which can con-sequently reduce physician professional satisfaction.
Instead, physicians should remain aware of thistendency to adopt a professorial role and shouldguard against it so that the group maintains a healthy,lively, interactive nature whereby much informationand support is exchanged and medical care is deliv-ered. This type of group will not only prove to bemaximally beneficial to patients but will also be muchmore professionally satisfying for the physician con-ducting the group visit program.
Focus on Patients Who Want to Attend Group Visits
Since CHCC groups began in 1991, experience hasconsistently shown that roughly 40% of older patientsrespond enthusiastically to the invitation to join a CHCCgroup. Twenty percent say they might be interested,and 40% decline to participate. The greatest economicbenefit to the organization is clearly to be found inpatients who respond with unqualified willingness toparticipate. These patients are the most likely to par-ticipate and thus to benefit; therefore, the focus shouldbe placed on this patient population.
A related finding is that experience with DIGMAshas shown that with the passage of time, patientsgradually become more familiar with, and acceptingof, the group visit program. Eventually, the popula-tion of patients refusing to attend a DIGMA programgrows smaller and smaller.
Remember: Support Is Required for Success
In another article published in this journal, we stateda point which cannot be overemphasized:
“A major hurdle for the CHCC model is the factthat the benefits are invisible to the staff in the clinicproviding the care. Nursing staffs are stretched tothe breaking point providing same-day access for amyriad of minor complaints that must be addressedin the service-quality imperatives of managed care.
Frontline nursing supervisors are faced with the hereand now issues of same-day access, unscheduledwalk-in patients, and emergency care. Althoughaware of the long-term favorable results of CHCC,staff is frequently diverted to more visible demands.High-level administrative support for CHCC, evenwhen present, is not enough. Dedicated nurse sup-port is a necessity.”1:50
This issue of invisibility is not a concern for the DIGMAmodel because it focuses on the entire patient panel ofthe individual physician and its benefits are highly vis-ible to the physician conducting a DIGMA. Therefore,the physician then becomes a strong advocate for main-taining the DIGMA. However, the issue of necessarystaff being diverted to more pressing demands of themoment is as real for DIGMAs as for CHCCs, whereimportant scheduling or medical assistant support canbe pulled from the group on any given week—the re-sult of which is often a substantial reduction in thatweek’s census from what it otherwise could have been(in the case of the scheduler) or not having patients’vital signs taken and other important duties performed(in the case of the medical assistant).
Speak Frankly about the Program
Physicians should not be afraid to state the goals ofthe group visit program. In focus group interviews,patients tell us that they are well aware of the over-burdened state of most providers and actually sym-pathize with their physicians. For their part, patientsoften cut their question list short or decide that aparticular symptom need not be mentioned during a“routine” visit for a different problem. They oftenmake another appointment not only to deal with theirissues but also to reduce the stress on their physi-cian. All too often, the pejorative label of “high uti-lizer” is then applied to these patients.
When implementing a group visit program, physi-cians may find it helpful to openly acknowledge thesefacts and then explain that plenty of time is availableto address everyone’s issues today; to respond fully toall questions; and then to follow-up on all issues, ei-ther individually or in the next group session. Physi-cians should explain that if the group visit programsucceeds, it will result not only in multiple benefits tothe patients attending, but also in cost savings for theorganization, which will allow continuation of the pro-gram. Follow-up visits for routine care are always al-lowed but are encouraged, whenever possible, to oc-cur within the group visit setting. Physicians can alsoincrease patients’ awareness of critical symptoms (short-
Although aware ofthe long-term
favorable results ofCHCC, staff is
frequently divertedto more visible
demands.

98 The Permanente Journal / Spring 2000 / Volume 4 No. 2
healt
h s
yst
em
s
ness of breath, chest pressure, etc.) during group visitsessions and can educate patients as to the appropri-ate use of same-day appointments and emergency care.
In the CHCC model, regular attendance is encour-aged, both because of its economic impact and be-cause of the effective group dynamic which it cre-ates. Nonattendees should be replaced by patientswho are more committed to the program. In theDIGMA model, patients attend only on an as-neededbasis so that different patients are typically presentduring each week’s session.
ConclusionDespite all of these concerns surrounding poten-
tial abuses, group visits will undoubtedly continueto grow in importance and be ever more frequentlyused during the coming years. Although physiciansare already working as hard and as efficiently as pos-sible using traditional office visits, they are findingthat this is often still not enough. What is needednow is an additional tool which will leverage physi-cian time and increase productivity, improve accessand quality of care, enhance patient and physicianprofessional satisfaction, and do all this without re-quiring physicians to put more hours in at the officeor to increase their fatigue due to workload demands.Group visits provide such a tool.
Without question, group visits have an importantrole to play in the future of health care. Well-de-signed, adequately supported, and properly run groupvisit programs (such as DIGMAs, CHCCs, and high-risk patient population management programs—Spe-cialty CHCCs) not only offer the benefits of greaterefficiency and reduced costs through economies ofscale but also offer the additional benefits of improvedaccess, comprehensive mind-body care, better fol-low-up monitoring, and increased patient and physi-cian professional satisfaction.
Nonetheless, the potential for abuse of group visitsis real and must therefore be carefully thought out inadvance and scrupulously safeguarded against. Thiswill preserve the credibility of group visit programsand protect the multiple economic and patient carebenefits which they can provide. ❖
The views expressed in this article are those of the authors and do
not necessarily represent those of The Permanente Medical Group.
References1. Noffsinger EB, Scott JC. Understanding today’s group visitmodels. Group Pract J 2000 Feb;49(2):46-8,50.52-4,56-8.2. Scott JC, Robertson BJ. Kaiser Colorado’s Cooperative HealthCare Clinic: a group approach to patient care. In: Fox PD, FamaT, editors. Managed care and chronic illness: challenges andopportunities. Gaithersburg, Maryland: Aspen; 1996. p 125-32.3. Beck A, Gade G, Scott JC, et al. Cooperative health care clinics:results from a 2-yr randomized trial. In preparation, 2000.4. Noffsinger EB. Increasing quality of care and access whilereducing costs through Drop-In Group Medical Appointments(DIGMAs). Group Pract J 1999 Jan;48(1):12-8.5. Noffsinger EB. Answering physician concerns about Drop-InGroup Medical Appointments (DIGMAs). Group Practice J 1999Feb;48(2):14-21.6. Noffsinger EB. Benefits of Drop-In Group Medical Appoint-ments (DIGMAs) to physicians and patients. Group Pract J 1999Mar;48(3):21-8.7. Noffsinger EB. Establishing successful primary care andsubspecialty Drop-In Group Medical Appointments (DIGMAs) inyour group practice. Group Pract J 1999 Apr;48(4):20-8.8. Noffsinger EB, Mason JE, Culberson CG, Abel T, Dowdell LA,Peters W, et al. Physicians evaluate the impact of Drop-InGroup Medical Appointments (DIGMAs) on their practices.Group Pract J 1999 Jun;48(6):22-33.9. Noffsinger EB. How to develop successful Drop-In GroupMedical Appointments (DIGMAs) in the primary care setting. [inprocess, 2000].10. Noffsinger EB. Increasing efficiency, accessibility, andquality of care through Drop-In Group Medical Appointments(DIGMAs). Submitted for publication, 1999.11. Noffsinger EB. Keys to success when establishing a Drop-InGroup Medical Appointment (DIGMA) program. Submitted forpublication, Medical Economics, 1999.12. Noffsinger EB. Pitfalls to avoid when developing a Drop-InGroup Medical Appointment (DIGMA) program. Submitted forpublication, 1999.13. Noffsinger EB. Will Drop-In Group Medical Appointments(DIGMAs) work in practice? Permanente J 1999 Fall; 3(3):58-67.14. Noffsinger EB. Providing “Dr Welby care” in a managed caresetting through Drop-In Group Medical Appointments(DIGMAs). Presented on 6/19/99 at the annual meeting of theAmerican Medical Group Association on physician-directedhealth care.15. Morrison I. The 1 percent problem. The organization ofmedicine has changed little in the century. Health Forum J 1999Jul-Aug;42(4):42-6.16. Walpert B. A novel approach for capitation: group visits.ACP-ASIM Observer 1999 Oct;19(9):5.17. Brunk D. Group appointments may enhance physician-patient relationship. Fam Pract News 2000 March 15;30(6):70.18. Brunk D. Group medical appointments aid communication.Intern Med News 2000 March 1;33(5):50.19. Noffsinger EB, Scott JC. Winning in your market: increasingphysician productivity and patient satisfaction through groupvisit models. Presented at the Annual Meeting, AmericanMedical Group Association, Las Vegas, NV, March 7-8, 2000.20. Coleman EA, Grothaus LC, Sandhu N, Wagner EH. Chronic careclinics: a randomized controlled trial of a new model of primarycare for frail older adults. J Am Geriatr Soc 1999;47:775-83.
Without question,group visits havean important role
to play in thefuture of
health care.

99The Permanente Journal /Spring 2000 / Volume 4 No. 2
health
syste
msAdapted from material previously published in: Group Practice
Journal 2000 Feb;48(2):46-8,50,52-4,56-8.
IntroductionWith its increasing patient demands for expanded
services at reduced rates, today’s rapidly changing andhighly competitive health care environment requireshealth care organizations to look for innovative waysto improve level of service and quality of care whilereducing costs. Group visit models have been devel-oped to achieve these complex objectives effectivelyand simultaneously through use of existing resources.As developers of today’s group visit models, the au-thors realize that much confusion unfortunately existsas to what defines these group visit models, how theydiffer, and how they can work together. Nonetheless,experience with group visits to date has been excitingand encouraging. This article discusses the features,advantages, and disadvantages of the basic models ofgroup medical visits, what their future looks like, andhow they might best work together to produce evengreater efficiencies than any one model alone or indi-vidual office visits could provide.
We invite physicians, administrators, and health careorganizations to take a closer look at using groupmedical visits for their own practices. Many physi-cians and administrators are concluding that the cur-rent paradigm—individual office visits only—is eco-nomically unsustainable. There simply isn’t enoughmoney in the system to allocate enough physiciansto solve current access, service, and quality-of-careproblems through traditional means. We need a toolfor leveraging physician time and for increasing bothefficiency and production while improving serviceand quality of care. The authors feel strongly thatproperly run and adequately supported group medi-cal visits can provide this much-needed tool.
The Need for New Models of Delivering CareThe physician-patient relationship, widely believed
to be the bedrock of medical care, is being eroded tothe detriment not only of both those parties but also tothe detriment of those who would manage that care.The glue that cements the physician-patient relation-ship and that ought to cement the physician-manage-ment relationship is trust; indeed, erosion of trust is thekey issue. It is pointless to try to assign blame for thiserosion, which is a product of complex changes in theworld—everything from the business imperatives of aglobal economy to the impact of technology on bothpatient and provider in the information age.
Physicians must master a huge and growing bodyof scientific and technical information. This learningprocess often requires a decade of formal trainingand must be ongoing. Discussing the applicablepieces of this technical knowledge and translating itinto meaningful, individualized decisions requiresspending more time with patients than in the erawhen there were only a half dozen antibiotics andonly two imaging techniques available (ie, x-ray filmsand laparotomy). The emerging guidelines and check-lists of evidence-based medicine compete with timeavailable for seeing patients. The medical record hasbecome an instrument of reimbursement instead ofa record of medical decision-making. Data entry fur-ther competes with time available for seeing patients.
Patients, too, are overwhelmed with informationand with expectations of accountability. Some areable to extract the information they need for theirmedical care directly from the Internet, but most areswayed by the mass media urging them to “ask yourdoctor about ....” Sound bytes on advertisements rarelydiscuss the complexities of false-positive and false-negative test results and risk-benefit analyses. Thus,patients often bring a great deal of information, butfrequently much less knowledge, along with manysets of questions and expectations that also must beaddressed in the limited time allotted for the doctoroffice visit. The general movement toward more pa-tient empowerment lends validity to these questionsand expectations.
Managers of the time allotted for doctor office vis-its are not unaware of the above issues and are acutelyaware that patient satisfaction is the key to success.Nonetheless, these managers must focus on accessand cost as primary issues. The almost universal re-sponse to these twin pressures is to see more patients.Because clinicians’ capacity for late hours and week-end clinics has already been stretched to maximumtolerance, the result is generally less time for thedoctor office visit—less time for the patient to com-municate fears, expectations, and even criticalsymptoms. The physician has less time to discussdiagnostic or treatment options along with their risksand benefits and has virtually no time to address thepsychosocial issues which often drive medical visitsand which result in different outcomes from the sameprocess of care. Unanswered questions and inad-equate explanations generate more anxiety and thusmore utilization—and the spiral continues.
Eventually, patients feel that the physician is notlistening or doesn’t have the needed answers. Trust
Understanding Today’s Group Visit Models
By Edward B. Noffsinger, PhDJohn C. Scott, MD
This articlediscusses the
features,advantages, anddisadvantages of
the basic models ofgroup medical
visits ...

100 The Permanente Journal / Spring 2000 / Volume 4 No. 2
healt
h s
yst
em
s
is eroded. Physicians begin to categorize their pa-tients’ concerns as either appropriate or inappropri-ate and to communicate the verdict through bodylanguage. Effective communication is difficult, andadministrators bemoan declining patient satisfaction.For their part, patients frequently turn to alternativemedicine, which emphasizes the humanistic insteadof the scientific and technical aspects of medical care.
What is the answer? Better communication, address-ing fears and anxieties, focusing more on psychoso-cial issues, active listening, increasing access to care,and lowering costs are some obvious answers whichwould satisfy everyone concerned. Unfortunately,these answers are impossible to achieve within bud-get through the current physician-patient dyad, theindividual doctor office visit.
Advantages of Group VisitsMany physicians feel that the traditional individual
office-visit model for which they have been trainedand with which they have been practicing is thebest form of care; they would therefore like to main-tain the status quo. Unfortunately, patient panel sizesare now so large that schedules are backlogged,waiting lists are common, patients have difficultyobtaining timely appointments, and the level of ac-cessibility is not commensurate with good care. Atool is needed to enable physicians to leverage theirtime and to “work smarter, not harder.” Group vis-its can be such a tool.
We invite the reader to consider the benefits thatgroup visits offer. For example, by integrating intomedical care the encouragement and support of otherpatients, group visits reduce the sense of isolationthat medical patients often feel. Not only do patientsno longer feel alone, but they also gain a more bal-anced perspective because they leave group visitsrealizing that many others are much worse off. Pa-tients often comment that attending group sessionsrelieved them of the “woe is me” type of thinkingand caused them to realize three things: that theirsituation could be worse, that they can still do muchwhich others cannot do, and that they can build ontheir strengths without merely perseverating on theirillness and disability.
Unlike individual office visits, where physiciansmust do everything themselves, group visits providethe help of other patients and support staff (eg, thebehavioral health professional in the DIGMA modeland the nurse, pharmacist, and health educator inthe CHCC model). In group visits, patients teach pa-
tients by discussing successful coping strategies, bysharing personal experiences, and by providing help-ful information. Unlike rushed individual visits, thepace of group visits is generally more relaxed be-cause of the greater amount of time available.
For many patients, group visits reduce the stigma ofillness through the emotional support of others, in-cluding those who are similarly afflicted. Often, patientsstate how much they have been wanting to talk tosomeone else experiencing the same health problemsbut that they never knew such a person until theyattended the group. After attending a group visit, theycomment upon how much they appreciated the op-portunity to finally meet and talk to such a person.
Group visits are meant to work in conjunction withthe judicious use of individual office visits—not tocompletely replace them. Group and individual ap-pointments both have their own advantages anddisadvantages, and neither is best for all situationsand circumstances. In this article, we discuss the ad-vantages and disadvantages of major group visitmodels and how they can work together with indi-vidual office visits to provide optimal value throughboth reduced cost and improved, integrated care.
Types of Group-Visit ModelsTwo major group visit models have been devel-
oped—one that is patient-focused and another thatis physician-focused. The first—the result of pioneer-ing work begun in 1990 in the Cooperative HealthCare Clinic (CHCC) at The Permanente Medical Groupin Colorado1-4 (Beck A, PhD, unpublished data)a—focuses on patient populations. Although the CHCCmodel initially focused on specific patient popula-tions categorized by their utilization behavior (ie, high-utilizing geriatric patients), the model was later ex-tended to focus on various specific patient popula-tions categorized by their diagnosis (ie, SpecialtyCHCC groups). The Specialty CHCC model serves asthe foundation on which high-risk patient popula-tion management programs can be based (eg, formanagement of diabetes, asthma, hypertension, hy-perlipidemia, congestive heart failure, depression,anxiety, irritable bowel syndrome, chronic fatiguesyndrome, fibromyalgia, and headache). The CHCCmodel was designed to provide adequate time todeliver the quality of care that all physicians knowthey should deliver. The therapeutic benefit of thegroup dynamic; enhanced physician and patient sat-isfaction; better patient outcomes with reduced utili-zation of the hospital, emergency department, and
Group visits aremeant to work inconjunction with
the judicious use ofindividual office
visits—not tocompletely replace
them.

101The Permanente Journal /Spring 2000 / Volume 4 No. 2
health
syste
msnursing facilities; and lower costs were positive con-
sequences of well-trained physicians having adequatetime to practice their art.
The second major group visit model, the Drop-inGroup Medical Appointment (or DIGMA) model, wasoriginated by Dr Noffsinger in 1996 at the KaiserPermanente San Jose Medical Center.5-15 The DIGMAmodel has an entirely different focus than that of theCHCC model. Instead of focusing on patient popula-tions categorized either by utilization behavior or bydiagnosis, the DIGMA model focuses on the entirepatient panel of an individual physician and includesonly patients from the physician’s own panel. TheDIGMA model has been effectively achieving all thegoals for which it was originally designed: to im-prove access for patients on the physician’s panel; toleverage the physician’s time and increase produc-tivity so that the physician is better able to managean increasingly large patient panel; to improve qual-ity of care, both by providing closer follow-up careand by better attending to the mind as well as bodyneeds that patients bring to the medical visit; and tosimultaneously increase patient satisfaction and phy-sician professional satisfaction.
In this article, we propose alternative delivery mod-els that use group office visits of various types forspecific patient populations as well as for thephysician’s entire patient panel. Evidence shows notonly that these models work but that they actuallywork better for a large percentage of patients thanthe current dyad paradigm. We will present threegroup visit models of care that have been shown toincrease patient and physician satisfaction, enhancequality of care, improve access, and cost less thanthe current individual office visit model. These mod-els include the CHCC (Cooperative Health Care Clinic)model, the Specialty CHCC model, and the DIGMA(Drop-in Group Medical Appointment) model.
Although each model is directly concerned withpatient care, each has a slightly different philosophi-cal basis. The CHCC model is designed primarily forthe benefit of the patient, whereas the DIGMA’s pri-mary goal is to improve access and to help physi-cians better manage their large patient panels. TheSpecialty CHCC model is designed primarily for thebenefit of the organization as a whole.
Description of the CHCC ModelThis model is designed to serve high-utilizing se-
niors who have contact with the system twice a monthor more. They are over age 65 years and therefore
usually have multiple medical conditions. Patients areidentified by administrative data and are grouped bytheir physician. If the physician is willing to imple-ment the CHCC model, invitations explaining the CHCCconcept and process are sent to the target population.
Nine years of consistent experience has taught usthat 40% of these patients accept the invitation en-thusiastically, 20% equivocate, and 40% decline toparticipate. A recent two-year, randomized, controlledclinical trial sponsored by the Robert Wood JohnsonFoundation clearly showed that the target popula-tion consists of the 40% who unequivocally acceptthe invitation.1-4 Optimal group size is set at 20 to 25participants. Participating physicians were surveyedon the issue of group size, and their consensus opin-ion was that groups with more than 25 people losethe group dynamic and personal interaction whichare key to their success; and that groups with fewerthan 15 people require too much energy from thephysician and nurse to keep discussions lively. Inaddition, groups with fewer than 15 people start tolose the up-front cost benefit to the organization.
Groups should meet once a month on a regularbasis at the same time and in the same place. Thesame patients are invited to attend each month, al-though new patients are added as group membersmove, change health plans, or die. Daylight hoursare essential for geriatric patients because most haveproblems with driving in the dark. Two-and-one-halfhours are set aside for each CHCC model session: a90-minute period of group time is followed by onehour for one-to-one patient-physician visits, asneeded. On average, six or seven patients are seenafter each group session in this model.
In the CHCC model, each group session has fivekey components: socialization time, education time,the break, question-and-answer time, and one-to-onephysician-patient time.
Socialization Time
Each session begins with 10-15 minutes of eitherorganized or spontaneous socialization. In the firstfew sessions, reminiscence therapy techniques areused to help build the cohesiveness of the groups.Questions like “What was Christmas Day like whenyou were ten years old?” or “What was your mostmemorable trip?” are passed around the U-shapedseating arrangement for optional responses. The com-monality of experiences that this process elicits helpsbuild the foundation for communication about spe-cific diseases and coping skills, as well as the
Groups shouldmeet once a monthon a regular basisat the same time
and in thesame place.

102 The Permanente Journal / Spring 2000 / Volume 4 No. 2
healt
h s
yst
em
s
emotional support that evolves quickly in every group.As time goes on, the socialization time becomes moreinformal, eg, vacation stories or even jokes are told.Formal or informal, the focused group interviewsdone after seven years of CHCC experience showhow important this process really is. Patients describethe group as a stronger support system than eventheir own families.
Education Time
The next half hour of group time is allotted foreducation. During the first year, certain core topicsare delivered in every group. These topics includeadvance directives, health maintenance requirements,use of the emergency system, Medicare coverage,and long-term care. Later, topics are selected by thegroup and range from safety at home to cardiovas-cular signs and symptoms among the elderly. Educa-tional sessions are interactive and not didactic. Forexample, the physician might ask, “Has anyone inthe group ever had a heart pain?” Usually three orfour hands are raised and those folks are asked, “Whatwas it like?” or “What did you do?” After several de-scriptions, the physician elaborates on key points orfills in the blanks. Not only is information conveyed,but also the patients are validated as reliable sourcesof information for each other.
The Break
Next comes the most active and most essential partof the group session, inappropriately referred to as“the break.” During this 15-20 minute segment, thephysician and nurse position themselves at oppositesides of the U-shaped seating arrangement and ad-dress multiple issues presented by members of thegroup. Blood pressure levels are monitored, prescrip-tions are refilled, forms are filled out for everythingfrom durable medical equipment to parking stickers,immunizations are given as needed, and “Oh, by theway, doc” issues are addressed. Everyone gets anopportunity for one-to-one contact with both thephysician and the nurse. Patients who are not ac-tively engaged with the provider interact with eachother while enjoying the snacks that designated groupmembers provide for each session.
Question-and-Answer Time
The working break is followed by a question-and-answer period that is also highly interactive and thatmay range from topics presented on that day to thelatest media medical stories. Often one question trig-
gers a series of questions and leads to discussion ofmultiple facets of complex medical issues.
One-to-One Physician-Patient Time
It is critical in describing the CHCC model to in-clude the one-to-one physician-patient time that fol-lows the group visit time. Six or seven patients areseen after each session—about half for interveningillness or flares in chronic conditions and about halffor health maintenance (eg, physical examinations,routine checks for diabetes or heart disease). Onaverage, each patient is seen about four times a yearin this individualized setting.
Advantages of the CHCC Model
CHCC is a health care delivery system that is en-tirely voluntary for both patients and staff. It effi-ciently and effectively enhances quality of care andthe satisfaction of the professional staff and patientswho participate. In focus group interviews, patientstell us that this format improves the doctor-patientrelationship, is far superior to the usual patient edu-cation formats, gives them an opportunity to get alltheir questions and issues addressed, and helps themto feel capable of coping with their various medicalissues. Confidentiality, although available in theone-to-one time, is a “nonissue” because patients feelthat the support group function of CHCC is “strongerthan family.”
This patient satisfaction and commitment to CHCCtranslates into membership retention that is more thandouble that of seniors who do not attend CHCC ses-sions. This format is not only good medicine—it isgood business.
Perhaps the greatest strength of the CHCC model isthat it is evidence-based. The outcomes—improvedindependence and functional ability, improved per-ception of quality of life, fewer hospital days, andless need to use ambulance and emergency depart-ment facilities—are important1-3 and reproducible4
(Beck A, PhD, unpublished data).a In these days ofcost-conscious medical care, the cost-effectivenessof CHCC cannot be overemphasized.
Disadvantages of the CHCC Model
Despite its strengths, the CHCC model has fourmajor disadvantages.
First, the financial success of the CHCC model de-pends upon major savings in “big-ticket” items suchas hospitalization and emergency department use.The model is dramatically economically successful
Confidentiality,although availablein the one-to-one
time, is a“nonissue”
because patientsfeel that the
support groupfunction of CHCCis “stronger than
family.”

103The Permanente Journal /Spring 2000 / Volume 4 No. 2
health
syste
msonly in an integrated system of care—at least in the
world of medicine as it is currently constituted.Second, the CHCC model requires constant moni-
toring and coaching to be sure that it remains aninteractive care delivery process and does not become“a class,” ie, purely educational. We have found thateven well-intentioned physicians left to their own de-vices often slip into the role of authority figure andprofessor—roles that can be much more comfortablethan the role of facilitator in an interactive process.
Third, to use the CHCC model most effectively mayrequire more up-front skill building in the group pro-cess than we have been able to provide. As men-tioned above, the model requires coaching and moni-toring. One person could provide these services fora minimum of 40 groups (our experience) and per-haps for as many as 100 groups.
A fourth—and major—hurdle for CHCC is the factthat the benefits are invisible to the staff in the clinicproviding the care. Nursing staffs are stretched to thebreaking point as they provide same-day access fora myriad of minor complaints that must be addressedin the service quality imperatives of managed care.Frontline nursing supervisors are faced with issuesof same-day access, unscheduled walk-in patients,and emergency care. Although aware of the long-term favorable results of the CHCC model, staff arefrequently diverted to more visible demands. High-level administrative support for the CHCC model, evenwhen present, is not enough; dedicated nurse sup-port is a necessity.
Future of the CHCC Model
The future for the CHCC model looks bright. Re-flect at first only on the geriatric population. Thispopulation, currently about 12% of the whole, willdouble in the next two or three decades. It does andwill control the majority of wealth in the country andthus, for better or worse, will influence federal healthcare policy. Medicare will not be allowed to languish,and 7 1/2-minute doctor office visits—(long predicted,currently not uncommon, and surely the scourge ofthe future) will not be tolerated, even under the ru-bric of “computer-assisted quality time” or “institu-tional memory.” People want to talk to doctors aboutaging, death, and dying. WWW.DEATH.com will notsuffice—not for today’s elderly population nor fortheir children and grandchildren.
The same is true for virtually every chronic disease inevery age group. People’s thoughts, beliefs, fears, andexpectations about their medical issues cannot be
bundled into simple guidelines and checklists. Humanreactions to illness are often the major determinants ofoutcomes, regardless of prescribed interventions. It takestime to address these issues, and the CHCC model pro-vides both the time and the environment to do this.The current one-to-one doctor-patient paradigm is notonly economically unsustainable as a sole delivery sys-tem but lacks the power and the therapeutic benefit ofthe group dynamic.16
Two challenges loom for the CHCC model. Thefirst is data entry and retrieval in the computer age.The current CHCC model features patients sitting withtheir medical chart in front of them. Notations aremade in the chart both during and after the groupsession. Transition to a fully computerized medicalrecord will require new formats for transfer of infor-mation. The second challenge for the CHCC modelis to secure a CPT code—a process which can belong and arduous and which must include safeguardsagainst abuse.
Description of the Specialty CHCC ModelThe CHCC model of care is adaptable to a large
number of diseases and patient populations. In someinstances, the emotional support provided is lessimportant than the education component. Thus, hy-pertension groups for working-age adults meet onlytwice a year, whereas diabetic groups might meet forfour to six intense educational sessions followed bytwo to three meetings a year for routine maintenancecare. Although the frequency, content, and durationmay vary considerably (ie, from the original geriatricmodel to pediatric groups for attention deficit disor-der and well-baby care), the basic elements remainthe same: sufficient time for interactive care deliverywith multidisciplinary assistance as needed. Thus, theCHCC model can be used as a foundation for allpopulation management programs designed for high-risk patient populations.
Specialists find the CHCC model useful for address-ing diseases associated with significant psychosocialissues. The list of such diseases is long, but success-ful pilot groups have been done for rheumatology(fibromyalgia), gastroenterology (functional boweldisorder), cardiology (congestive heart failure), andpulmonary medicine (chronic obstructive pulmonarydisease). Specialists emphasize efficiency in caringfor time-consuming patients who do not require anymedical procedures. This same focus has recentlybeen brought to orthopedics where group preopera-tive and postoperative visits are viewed as poten-
Specialists find theCHCC model
useful foraddressing diseases
associated withsignificant
psychosocialissues.

104 The Permanente Journal / Spring 2000 / Volume 4 No. 2
healt
h s
yst
em
s
tially freeing up more operating suite time. From theadministration’s point of view, the cost-benefit of thisavailability is obvious; and, of course, working in theoperating suite is essential for the surgeons.
Quality assurance is another mandatory consider-ation for health plan administrators. Guidelines formanaging specific diseases and patient populationsare proliferating faster than providers can read them,let alone implement the details. Reporting require-ments are likewise proliferating, with HEDIS beingthe most prominent of these to date. The SpecialtyCHCC model, either run by or including specialistsas guest speakers, is the ideal forum for implement-ing guidelines and enlisting patients in monitoringtheir own compliance.
Description of the DIGMA ModelThis section discusses the DIGMA model: what it
is; how it looks; what it can achieve; how it is differ-ent from other group medical appointment models;what its strengths and weaknesses are; and howDIGMAs can positively impact service, quality of care,and the bottom line.
The DIGMA model was created in 1996 to improveaccess to care and to enable physicians to bettermanage their large patient panels by seeing dramati-cally more patients in the same amount of time whileincreasing patient and physician professional satis-faction as well as improving access to care, level ofservice, and quality of care.5-15 DIGMAs enable phy-sicians to “work smarter, not harder” andsimultaneously provide patients with more integrated,holistic care that addresses not only physical medi-cal needs but also their psychological and behavioralhealth needs—needs that typically cannot be ad-equately addressed during the brief timespan of anindividual office visit.
DIGMAs are customized to the needs, goals, prac-tice style, and patient panel constituency of the indi-vidual physician. Open only to the physician’s ownpatients (ie, they are not drawn from elsewhere inthe medical center), DIGMAs are designed to en-compass most or all of the physician’s own patientpanel. DIGMAs combine an extended medical ap-pointment with the patient’s own physician and aneffective support group consisting of the physician,a behavioral health professional, and other patientsfrom the physician’s panel. Surveys have consistentlyshown that patients are highly satisfied with DIGMAsbecause DIGMAs provide what patients most want:better access, high-quality health care in which both
mind and body needs are addressed, and more timewith their own doctor.
Co-led by the physician and a behavioral healthprofessional (such as a health psychologist, socialworker, marriage and family therapist, nurse, orhealth educator), both of whom are present through-out each DIGMA session, DIGMAs are typically heldfor 60, 90 or 120 minutes weekly or biweekly. Mostcurrent DIGMAs are 90 minutes long, are heldweekly, and are supported by a medical assistantand a scheduler. DIGMAs are typically attended by10 to 16 patients plus two to six support persons(most frequently the spouse, family members,friends, or the caregiver), bringing the total DIGMAgroup size to between 12 and 22 group members.Different patients attend each week, typically when-ever they have a question or medical need. Patientshelp other patients in the group by sharing infor-mation, encouragement, support, effective copingstrategies, and disease management skills.
The behavioral health provider plays a very activerole throughout each DIGMA session by introducingthe DIGMA group concept and discussing proceduralitems at the beginning of each session; by handlinggroup dynamic issues; by keeping the group run-ning smoothly and on time; by addressing emotionaland psychosocial issues; by dealing with psychiatricemergencies; by providing behavioral health evalua-tions and interventions; by seeing that each patient’smind and body needs are met during each session;by doing whatever is necessary both during and out-side of the group to assist the physician in runningthe DIGMA; and by conducting the group alone whenthe physician is late or leaves the room to deliverbrief private examinations near the end of the groupsession. The behavioral health professional then fo-cuses on psychosocial issues of common interestwhich have been brought up by patients attendingthe DIGMA session. Fulfillment of this role of behav-ioral health professional frees the physician to focuson delivering high-quality, high-value medical carein the warm, supportive DIGMA group setting en-joyed by patients and physicians alike.
Patients often remark that the increased time withtheir own doctor, the warm and comfortable atmosphere,and the relaxed pace of DIGMAs is like “Dr Welby care”and that it puts the “care” back into health care.
Patients enter DIGMAs either by being directlybooked into the DIGMA in lieu of an individual ap-pointment (which provides much of their economicbenefit) or by simply attending whenever they have
Patients oftenremark that theincreased timewith their own
doctor, the warmand comfortableatmosphere, and
the relaxed pace ofDIGMAs is like “Dr
Welby care” andthat it puts the
“care” back intohealth care.

105The Permanente Journal /Spring 2000 / Volume 4 No. 2
health
syste
msa question or medical need. Allowing patients to drop
in often avoids the need to schedule an individualvisit, improves accessibility, increases efficiency, addscontinuity to the DIGMA, and provides a warm andcompassionate side to medical care. Patients can bedirectly booked into DIGMAs in two ways: 1) byphysician invitation during routine office visits, whenthe physician invites appropriate patients to have theirnext visit be a DIGMA group visit in lieu of an indi-vidual appointment; or 2) by a scheduler who tele-phones patients approved by the physician from theirpanel or waiting list who are either due or past duefor a return visit, inviting them through a scriptedmessage and follow-up letter to have their next visitbe a DIGMA visit.
More than 9000 DIGMA patient visits have beenrecorded to date for the 32 DIGMAs co-led by theauthor with 31 specialty and primary care physiciansat the Kaiser Permanente San Jose Medical Centerand elsewhere around the nation. DIGMAs in oncol-ogy, nephrology, endocrinology (one endocrinolo-gist had two DIGMAs), rheumatology, neurology,physiatry, obstetrics, gynecology (women’s health),pediatrics, cardiology, family practice, and internalmedicine have consistently worked well in actualpractice during the past four years. The results haveshown that DIGMAs work equally well in both pri-mary and specialty care settings.
Because a DIGMA is primarily an extended medi-cal appointment with one’s own doctor held in awarm and supportive group setting, extensive medi-cal care is provided during every DIGMA session:charts are reviewed; visits are documented througha progress note on each patient (which is largelypreprinted and partially in check-off form so as tominimize charting time); vital signs are monitored;prescriptions are changed or refilled; medications andside effects are discussed; tests and procedures areordered, and the results are discussed; referrals aremade; medical questions are answered; treatmentoptions are explained; routine health maintenanceissues are addressed, and, when appropriate, briefprivate examinations and discussions are providedby the physician toward the end of the group ses-sion. Medical care is the central focus of DIGMA vis-its, and the physician plays an active role throughoutthe session.
DIGMAs are not meant to completely replace indi-vidual appointments, but instead to complement thejudicious use of traditional office visits in order toachieve maximum value. In this way, patients such
as the relatively stable, chronically ill and the “wor-ried well,” all of whom can be appropriately seen ina group visit, will be seen in a cost-effective andhighly accessible DIGMA group visit. Conversely,patients needing individual visits can be seen indi-vidually, which should now be more accessible as aresult of off-loading numerous individual office vis-its onto more efficient and cost-effective DIGMAgroup visits. Patients should always be reminded thatparticipation in DIGMAs is completely voluntary andthat it is meant to offer them freedom of choice. Pa-tients are always welcome to have individualappointments, as before, even after they have at-tended a DIGMA session.
Profile of a Typical Digma Session
If you were to first walk into a typical CHCC groupvisit and then into a typical DIGMA session, youwould immediately notice substantial differences.Although a DIGMA session usually begins with briefintroductory comments by the behavioral health pro-fessional about the purpose of the group, its intendedbenefits to patients, and the importance of telephon-ing and preregistering a day or two before droppinginto the group session, the focus then immediatelyshifts to the delivery of medical care—a focus whichis maintained throughout the remainder of the groupsession. Initial socialization or education componentscan be present but typically aren’t.
Because DIGMAs typically meet weekly and areonly 90 minutes (including a few minutes for intro-ductions and 10 to 15 minutes at the end of eachgroup session for individual examinations), most ofthe group session is used for delivery of comprehen-sive mind-body medical care to all patients present.For this reason and because the physician and be-havioral health provider are typically present through-out each DIGMA session, DIGMAs far more closelyresemble a traditional individual office visit than ahealth education class, behavioral medicine program,or psychiatry group. Patients never confuse a DIGMAwith a class or psychotherapy group.
Upon entering a representative DIGMA session, anobserver would see a group of 12 to 22 membersseated in a circular arrangement, along with the phy-sician and the behavioral health professional, whotypically sit together with a small table between themupon which medical charts, forms, and any hand-outs are stacked. The medical assistant or nurse, whoarrives 15 minutes early, would be calling patientsout of the group one at a time at the beginning of
Patients shouldalways be
reminded thatparticipation in
DIGMAs iscompletely
voluntary and thatit is meant to offerthem freedom of
choice.

106 The Permanente Journal / Spring 2000 / Volume 4 No. 2
healt
h s
yst
em
s
the session in order to take vital signs and performother important duties—such as pulling and partiallycompleting the patient information section of lab slipsand referral forms for preventive tests and medicalservices which are due or past due (this tactic mini-mizes the amount of physician time required duringgroup to complete the forms and make these refer-rals). Although DIGMAs can be designed asheterogeneous, mixed, or homogeneous models,2
they are typically attended by a heterogeneous mixof patients in terms of age, sex, diagnosis, maritalstatus, race, utilization behavior, etc. (although theywould be relatively homogeneous as to diagnosis inthe mixed and homogeneous DIGMA models).
Introductory comments about the group are fol-lowed by a request for patients to introduce them-selves one at a time with each saying whatever theywould like by way of introducing themselves, start-ing with patients who have to leave early. However,everyone is asked to state what their medical con-dition is and what specific information or assistance,if any, they hope to obtain from their doctor today.They are assured that their doctor will answer allmedical questions and will deliver most of the medi-cal services normally provided during routine of-fice visits, only at a more relaxed pace because moretime is available in the group setting, where all canlisten and learn. All present are invited to activelyparticipate in this highly interactive format. A pa-tient who volunteers to speak first starts the group,and the focus shifts sequentially from one patientto another in either a clockwise or counterclock-wise direction. The physician might prefer to ad-dress patients in clusters according to diagnoses (eg,a neurologist might ask Parkinson’s disease patientsto speak first, followed in turn by patients with head-ache, seizure disorder, and stroke). When every pa-tient in the room has spoken, a process which typi-cally uses all but the last 10 to 15 minutes of grouptime, the physician leaves to provide brief privateexaminations while the behaviorist takes over nurs-ing the group.
The DIGMA group consistently provides a highlyinteractive experience so that the physician, behav-ioral health professional, and others present in thegroup all actively help the patient being focused onat any given moment. The physician spends much ofthe time in group answering patients’ medical ques-tions, occasionally walking over to give a prescrip-tion refill to a patient, to provide a referral (ie, for alaboratory test, procedure, or medical service), or to
perform a brief examination which can be appropri-ately conducted in group (eg, examination of thy-roid, arthritic hand or wrist, swollen ankle, growthon the face, tennis elbow, skin rash on the arm orleg, or sore on the foot). Meanwhile, other patientsoffer encouragement and support, provide gentleconfrontation when needed for noncompliant pa-tients, and share relevant information and personalexperiences—all of which can be helpful to the pa-tient being focused upon.
This high degree of interaction between each pa-tient and the physician, behavioral health professional,and other group members, combined with deliveryof comprehensive mind-body health care, is a char-acteristic feature of the DIGMA model. Activities whichcan be appropriately conducted in the group settingare conducted during the DIGMA so that all patientscan listen, learn, and respond. Issues of confidential-ity are rarely, if ever, mentioned by patients, but anyphysician concerned about confidentiality could con-sider having patients sign at the beginning of eachDIGMA session a full-disclosure consent form en-compassing confidentiality.
Patients and staff alike consistently report that theyfind DIGMA sessions lively, interesting, helpful, anda wonderful learning opportunity. Physicians reportlearning things about their patients that they neverknew, despite often having seen them previously foryears during individual office visits. Patients learnfrom the physician, the behavioral health professional,and other patients—often stating that they evenlearned answers to relevant questions that they didnot know to ask because somebody else did ask.
The number of patients actually requiring an indi-vidual examination at the end of group is surprisinglysmall—typically one or two, and occasionally threeor four. This finding supports the claim of variousauthors that most medical visits are driven by psy-chosocial and behavioral health issues rather thanby medical need.13-15 The reason that only a smallpercentage of patients require an individual exami-nation at the end of group is that after their questionsare answered and their various mind and body needswhich can appropriately be attended to during thegroup setting are addressed, very few patients areleft who actually need an individual examination.
Occasionally during the DIGMA session the physi-cian spots a medical condition requiring a traditionalindividual office visit, which is then scheduled. Whenthis referral occurs, the good news is that the officevisit should be readily accessible because DIGMAs
Patients and staffalike consistentlyreport that they
find DIGMAsessions lively,
interesting, helpful,and a wonderful
learningopportunity.

107The Permanente Journal /Spring 2000 / Volume 4 No. 2
health
syste
mspermit many appropriate individual visits to be
off-loaded onto DIGMA group visits, so that indi-vidual office visits eventually become more acces-sible to those who need them.
A goal of every DIGMA session is to end on timewith all of the physician’s duties completed. This in-cludes writing a progress note for each patient presentin the group, which is typically done in group aseach patient is being focused upon. Accomplishingthis end requires discipline, coordination betweenthe physician and the behavioral health provider, anda certain amount of experience in running the DIGMA.In so doing, the physician leaves the DIGMA sessionback on schedule, even if the physician entered thegroup late—which is but one of the many physicianbenefits that a well-run DIGMA can offer.7
How DIGMAs Provide Cost Savings
The CHCC and DIGMA group visit models havebeen shown to provide substantial cost savings. Be-cause of the different focuses of these two groupvisit models, their financial benefits to the health careorganization have been correspondingly evaluatedin different ways.
Some of the financial benefits provided by theDIGMA model can be measured directly by evaluat-ing the degree to which the model leverages existingstaffing resources, a strategy which can solve accessproblems without hiring additional staff. The DIGMAmodel has been shown to dramatically leverage phy-sicians’ time,12,13 and its implementation can be con-verted to cost savings based upon the lower staffinglevels required to provide good service and care. Inaddition to off-loading many individual appointmentsonto more cost-effective group visits, DIGMAs alsoexcel in addressing the behavioral health and psy-chosocial issues which drive such a large percentageof all medical visits.17-19 Addressing mind as well asbody needs during a medical visit decreases utiliza-tion of medical resources.
Because DIGMAs are readily accessible, patientsoften drop into a DIGMA any week that they have aquestion or medical need instead of scheduling anindividual office visit, demanding an urgent work-inappointment, complaining about poor access, or tele-phoning with a question. This practice saves moneythrough both reduced individual office visits anddecreased phone call volume. In addition, patientscan be taught during DIGMAs by the physician, thebehavioral health professional, and other patients tomore appropriately use the emergency department
and other inpatient and outpatient services. BecauseDIGMAs are specifically designed to handle many ofthe most difficult, time-consuming, psychosociallyneedy, and inappropriately high-utilizing patients inthe physician’s practice, such patients can often bebetter treated and with less cost in the more effectiveformat of a DIGMA group visit, where mind as wellas body needs can be met.
DIGMAs represent best use of staff and budget.They increase physician productivity and efficiency,provide many economic and patient care benefits,offer the competitive advantage of a new servicewhich is much appreciated by patient-customers, andreduce costs by leveraging existing staffing. A prop-erly run and adequately supported DIGMA programcan substantially and positively impact a health careorganization’s bottom line while simultaneously cre-ating happier patients and physicians. Happier pa-tients and physicians translates into better retentionof both patients and staff—an additional cost sav-ings. DIGMAs increase value by providinghigh-quality medical care with excellent access andservice at reasonable cost in a warm, supportive groupatmosphere which is enjoyed by patients and physi-cians alike. Because they optimally balance the needsof patients, physicians, and health care organizations,DIGMAs provide a “win-win-win” situation and, as aresult, are expected to play an increasingly impor-tant role in the future of health care delivery.
Advantages of the DIGMA Model
DIGMAs are specifically focused upon improvingprimary and specialty care access through the use ofexisting resources and upon enabling physicians tobetter manage their large patient panels. Access hasbecome a national problem. Physicians are alreadyworking as hard and efficiently as is possible, so thatthis access problem cannot be solved by simply hav-ing physicians work longer or harder—any “fat” whichmay have existed here has long since been removed.What is needed is a tool which will enable physi-cians to substantially leverage their time so that theycan see dramatically more patients in the same amountof time while also providing excellent service andhigh-quality medical care which is satisfying to pa-tients and physicians alike. The DIGMA model pro-vides precisely the right tool for this purpose. DIGMAshave been shown to use existing resources to im-prove access by rapidly reducing return appointmentbacklogs at both the individual physician10 and thedepartmental11 levels.
The DIGMA modelhas been shown to
dramaticallyleverage
physicians’ time ...

108 The Permanente Journal / Spring 2000 / Volume 4 No. 2
healt
h s
yst
em
s
Because they provide patients with the prompt ac-cess, quality health care, and increased time they wantwith their own doctor, DIGMAs increase both patientsatisfaction and patients’ perception of quality of care.Patients appreciate the fact that DIGMAs comprehen-sively address the totality of mind-body needs theybring to the medical visit. This view contrasts withthat engendered by individual office visits, which of-ten make patients feel rushed and which might notprovide enough time to address a patient’s physicalmedical needs, let alone psychosocial needs. One in-dication of the degree to which DIGMAs have beenmeeting patients’ needs occurred shortly after bothrheumatologists at the Kaiser Permanente San JoseMedical Center started their Rheumatology DIGMAs,when a previously successful fibromyalgia and chronicfatigue syndrome program in the Division of Behav-ioral Medicine failed due to a complete loss of census.The reason given was that these patients preferredattending their rheumatologist’s DIGMA whenever theyhad a question or medical need.
Consider the noncompliant patient, whose needsare often poorly addressed during traditional, indi-vidual office visits. The information, encouragement,support, and gentle confrontation provided by othermembers in the group and by the behavioral healthprofessional increases patient compliance with rec-ommended treatment regimens. It is amazing howinfluential another patient who has already benefitedfrom the recommended treatment or lifestyle change(dietary compliance, initiating insulin, undergoingchemotherapy, starting dialysis, smoking cessation,etc) can be in relieving the noncompliant patient’sanxiety about the treatment and in persuading theresistant patient to comply with recommended treat-ment by confronting them with the long-term conse-quences of noncompliance.
Individual appointments need no longer be largelyoccupied by either worried well or relatively stable,chronically ill medical patients requiring much pro-fessional hand-holding and contact with the physician.Such patients can be more efficiently andcost-effectively handled through DIGMA group visitsand with better care because both mind and bodyissues are effectively addressed and closer follow-upcare is made available. Because of the added helpfrom the behavioral health professional and the groupitself, DIGMAs provide an efficient and effective meansof dealing with many of the physician’s most prob-lematic patients, all of whom the physician isencouraged to invite to the DIGMA. This includes
patients who are difficult and time-consuming;noncompliant; inappropriately high utilizers of healthcare services; angry, depressed, or anxious; demand-ing or distrusting of their health care; experiencingextensive psychosocial needs; lonely or lacking socialsupport; or having excessive needs for information,reassurance, or contact with their physician.
DIGMAs represent a biopsychosocial model20,21 fortreating both mind and body needs, including anxi-ety and depression, which are known to beunderdiagnosed in medical settings.22 DIGMAs excelin treating the behavioral health and psychosocialissues known to drive such a large percentage of allmedical visits (with estimates running as high as 60%and more).17-19 DIGMAs also treat caregiver and fam-ily issues: Family members and caregivers are invitedto accompany patients to DIGMA visits because ill-ness impacts loved ones as well as patients.
Improved access as well as increased patient andphysician professional satisfaction are certainly amongthe great strengths of the DIGMA model which havebeen consistently demonstrated in actual practice.DIGMAs which are carefully designed, properly run,and adequately supported result not only in high levelsof patient satisfaction but also in increased physicianprofessional satisfaction as each DIGMA is customizedto the particular needs, goals, practice style, and patientpanel constituency of the individual physician.
Physicians appreciate being able to better managetheir burgeoning panel sizes and to regain controlover their practices while delivering a more satisfy-ing level of care and enjoying improved relationshipswith their patients. They like the more relaxed paceof DIGMAs, the reduction in repetition of informa-tion, the opportunity to try something interesting anddifferent, and the collegial interaction with the be-havioral health professional. Physicians also appre-ciate the ability to respond effectively in DIGMAs toangry or demanding patients and to have more com-pliant patients. Because of the many benefits DIGMAsoffer, they are already beginning to gain acceptanceand recognition for the role that they can play indelivering health care.23-26
The physician and his or her panel of patients di-rectly benefit from the increased efficiency and qual-ity of care that DIGMAs offer. Because DIGMAs en-able physicians to better manage their large patientpanels and offer many other physician benefits,8
DIGMAs are “owned” by the physicians running them.DIGMAs ensure that no invisible or orphan programexists without strong physician ownership and sup-
Improved access aswell as increased
patient andphysician
professionalsatisfaction arecertainly among
the great strengthsof the DIGMA
model which havebeen consistentlydemonstrated inactual practice.

109The Permanente Journal /Spring 2000 / Volume 4 No. 2
health
syste
msport, as could be the case for some group programs
(such as for hypertension, diabetes, asthma, irritablebowel, etc), where only a comparatively small per-centage of the physician’s panel is covered (oftentheir easier patients, whom physicians may prefer tosee individually for that very reason).
Additional strengths of DIGMAs include the following:• Instead of repeating the same information
with different patients as is done inindividual office visits, the physician canaddress the entire group at once (and ingreater detail because of the greater timeavailable). They all can listen and learn,focusing on such issues of commoninterest as the information and misinfor-mation which patients glean from themedia, the Internet, friends, and directadvertising by pharmaceutical companies.
• DIGMAs improve not only patient andphysician professional satisfaction but alsophysician-patient relationships. Patientscan see their physician be more relaxed—they even joke and laugh together—andphysicians get to know their patientsbetter as people and not just as patients.
The prompt access without barriers which DIGMAsprovide, when coupled with the relaxed pace andsupport of other group members (which makes thegroup feel safe to patients), sometimes results in pa-tients opening up more in group than in office visits.The result is that physicians occasionally detect veryserious and even life-threatening conditions whichwould otherwise have gone unnoticed. This detec-tion often happens because the patient is minimiz-ing or denying their symptoms. Consider the patientwho dropped into an endocrinology DIGMA request-ing a prescription for glasses, almost apologizing forbeing there and stating that he would not have both-ered to come in if it were not for the fact that he wasable to simply drop in without an appointment. Be-cause fingerstick blood glucose levels were routinelymeasured for all diabetics attending the endocrinol-ogy DIGMA, his blood glucose level was discoveredto be extremely high (49.9 mmol/L), and he wasimmediately given emergency care. Another patient,who had been quiet throughout most of the session,spoke up in another DIGMA when other patientswere complaining about the fatigue they were expe-riencing, stating that he needed a pep pill. Whenasked why, he explained that he became extremelyfatigued with even minor exertion and that when he
lay down to rest, he felt like an elephant was step-ping on his chest. What he received was an urgentcardiac evaluation, not a pep pill!
Disadvantages of the DIGMA Model
One weakness of DIGMAs is that they have somesupport needs which, while modest, must be met ifthe DIGMA model is to be successful. Most impor-tant is the fact that for larger group practices andmanaged care organizations, a highly skilled cham-pion who is very knowledgeable of the DIGMA modelis needed to move the entire DIGMA program for-ward throughout the facility. Second, a behavioralhealth professional trained by the champion is neededto take over each of the DIGMAs the champion hasestablished. In each case, the behavioral health pro-fessional must be well matched to both the physi-cian and the patients attending the DIGMA.
Most DIGMAs also require a nurse or medical as-sistant and a scheduler. The primary requirement forthe medical assistant or nurse is willingness to workhard, both in terms of seeing the larger volume ofpatients which DIGMAs entail and in terms of theexpanded responsibilities which need to be assumed.Similarly, a scheduler trained by the champion mustbe provided for most DIGMAs with adequate dedi-cated time each week (as much as four hours) tomaintain the desired census level by telephoningenough patients selected by the physician with ascripted message and then sending them follow-upletters containing all important details on the DIGMA.
Clearly, any innovative health care delivery pro-gram which differs as much as the DIGMA modeldoes from the format of traditional office visits re-quires a high level of administrative commitmentand support. As is the case for all group programs,there are also certain facilities requirements. In par-ticular, DIGMAs require a comfortable group roomof sufficient size with an examination room locatednearby. In addition, the DIGMA model requires thateach physician running a DIGMA for his or her prac-tice take approximately 15 to 30 seconds duringroutine office visits to invite all their appropriatepatients to have their next visit be a DIGMA visit. Asmall one-time expense must also be budgeted forat the beginning of each DIGMA to provide the pro-fessional-appearing framed wall posters and pro-gram description flier holders to be mounted onthe walls of the physician’s lobby and examinationrooms. Because DIGMAs differ dramatically fromthe traditional one-on-one office visits patients have
In each case, thebehavioral healthprofessional must
be well matched toboth the physicianand the patients
attending theDIGMA.

110 The Permanente Journal / Spring 2000 / Volume 4 No. 2
healt
h s
yst
em
s
come to expect, in order to obtain patient buy-in,all marketing materials must be of high quality soas to accurately reflect the quality of care whichDIGMAs do in fact provide.
Finally, it is important to note that DIGMAs workbest for routine return appointments with the wor-ried well, patients with extensive informational andpsychosocial needs, and patients experiencing rela-tively stable chronic health problems who requiremind-body care, more time with their physician, pe-riodic surveillance and monitoring, or closer follow-upcare. DIGMAs are not meant for initial evaluations,one-time consultations, inpatients, most medical pro-cedures (although the rheumatologists are consider-ing offering some of their simpler injections towardthe end of their Rheumatology DIGMA sessions),highly contagious illnesses, medical emergencies,rapidly evolving medical conditions, lengthy indi-vidual examinations, many acute illnesses, or patientsrefusing to attend group visits.
With regard to patients refusing to attend DIGMAs,an interesting observation has been repeatedly made.As time passes, patients who initially refuse theDIGMA will often later be persuaded to attend afterhearing other patients in the physician’s waiting roomdiscuss how much they enjoyed and got out of theirrecent DIGMA visit. Sometimes patients who initiallyrefuse the invitation to participate will eventuallyconsider attending a DIGMA after being invited sev-eral times by their physician during routine officevisits. On rare occasion, patients have mistakenlycome to a DIGMA session with the misunderstand-ing that it will be an individual appointment. In thiscase, they are given the option of staying for thegroup or being seen immediately by the physician inprivate in the adjacent examination room. Such pa-tients will often choose to stay out of curiosity to seewhat the DIGMA is all about. In any case, after apatient does attend a DIGMA session, he or she al-most invariably is won over to this new approachand is then open to returning whenever there is amedical need. Many patients report that they actu-ally prefer and get more out of their DIGMA visitsthan from traditional individual office visits.
How Group-Visit Models Can Work TogetherAlthough the CHCC, Specialty CHCC, and DIGMA
models individually offer their own distinct advan-tages in terms of reduced costs and increased effi-ciency, productivity, service, quality of care, and bothpatient and physician professional satisfaction, these
models can operate together to provide even greaterbenefits than they could alone. The authors feel thatoptimal value can only be achieved in the futuredelivery of health care when the best possible mix ofefficient group visits (using group-visit models whichhave been demonstrated to be effective in actual prac-tice) and traditional individual visits is offered. Thenpatients who can appropriately be treatedcost-effectively in group visits can be efficiently seenin group while individual visits can be used judi-ciously for patients truly needing them.
To fully capture the potential economic and pa-tient care benefits which group visits can provide, allgroup visit programs must be carefully designed,properly run, and adequately supported. If, in therush to roll out a group visit program, group prac-tices and managed care organizations hurriedly launchpoorly planned, inadequately supported DIGMAs orCHCC groups with flawed implementation strategies,their multiple potential benefits will never be com-pletely realized.
As a means of fully achieving the many benefitsthat the DIGMA, CHCC, and Specialty CHCC modelscan conjointly offer, consider the following illustra-tive example of fully integrated care. First of all, everyprimary and specialty care provider at the group prac-tice or managed care organization who wants aDIGMA would have one for their practice as a meansof better managing their patient panel, leveragingtheir time, solving their access problem, providingcomprehensive mind-body care, and increasing bothpatient and physician professional satisfaction. Inaddition, the facility would have numerous CHCCand Specialty CHCC group visit programs for man-aging high-risk patient populations both in terms ofutilization behavior (eg, CHCC programs for high-utilizing geriatric patients) and by diagnosis(population management programs based upon theSpecialty CHCC model for diabetes, hypertension,asthma, hyperlipidemia, depression, anxiety,fibromyalgia, irritable bowel, congestive heart fail-ure, etc). Then any patient seen in a physician’sDIGMA who needed further help for their particularhealth problem could be efficiently referred to theappropriate CHCC or Specialty CHCC group or to anindividual office visit, when appropriate. Conversely,when appropriate, patients seen in CHCC and Spe-cialty CHCC groups could be encouraged to havetheir next medical visit with their doctor be a DIGMAvisit. In this way, all patients who could best be seenin a group visit would be—thus, capturing the in-
Many patientsreport that they
actually prefer andget more out of
their DIGMA visitsthan fromtraditional
individual officevisits.

111The Permanente Journal /Spring 2000 / Volume 4 No. 2
health
syste
mscreased efficiency, improved service and quality of
care, and reduced cost which group visits can offer.In this schema, individual office visits would be re-served for those patients who need them.
This vision for optimizing value in health caredelivery through the integration of the variousgroup-visit models with individual office visitswould involve substantial alteration in: the long-range business plan; allocation of funding; staff-ing resources; facilities planning; and the way inwhich future mainstream medical care will be de-livered. Nonetheless, what is being proposed isachievable and can result not only in improvedaccess, dramatic cost savings, and more efficientutilization of existing staffing resources but also insubstantially improved service, quality of care, andpatient and physician satisfaction.
Concluding CommentsContinuity of care is a recurring theme for most man-
aged care organizations.27 Its benefits need no elabora-tion. Continuity presupposes physician retention as wellas member retention. Primary care physicians as a wholeare not a happy group, and turnover rates in someorganizations are alarming. The professional satisfac-tion derived from a job well done is a major part ofphysician satisfaction with the CHCC and DIGMA mod-els, yet control issues loom large for physicians in man-aged care. DIGMAs provide some degree of control inthe management of large patient panels, and such in-creased control in and of itself is a positive develop-ment for the physicians. In addition, both group mod-els provide some variety in an often tedious workday.This is especially true in an environment where hospi-tal and emergency department duties have been as-sumed by dedicated teams of hospitalists andemergentologists. Satisfied physicians create satisfiedpatients either in the group model or in the traditionaldyad. Satisfied physicians and their patients stay in theorganization. Continuity is enhanced.
Next, consider panel management. About half of apanel of patients could be candidates for group visitsof some type, and this percentage is expected to growin the future as patients become more familiar withthe benefits of group visits. Experience shows that theother half prefers the traditional physician-patient dyad,at least at this time, even though satisfaction with thatmodel is in decline. This situation presents the indi-vidual physician with some potentially wonderfuloptions for better managing their panels through groupvisits. However, in a fully capitated system, a
physician’s panel size must be fixed for any physicianto even consider the benefits of group visits. If thereward for efficiency is a correspondingly larger paneland no commensurate increase in reimbursement (ei-ther in time or dollars), then innovation is improbablefrom the outset. If, however, group visits are appro-priately recorded and everyone in the organizationparticipates in some way, then group appointmentswill increase access and efficiency, improve serviceand quality of care, enhance patient and physiciansatisfaction, more efficiently utilize existing resources,and reduce the cost of health care delivery—and allthis while providing more time for effective and ful-filling physician-patient relationships.
An effectively integrated system of CHCCs, SpecialtyCHCCs, DIGMAs, and traditional individual office visitscan provide a “win-win-win” for patients, physicians,and managers of health care. CHCCs and DIGMAs pro-vide useful tools in helping to manage the ever-increas-ing demand for specialty and primary care servicesthrough the use of existing resources. We offer themfor consideration to group practices and managed careorganizations as exceptionally helpful tools for confront-ing the access, service, quality of care, and economicchallenges facing them in today’s rapidly evolving andhighly competitive health care environment. ❖
aDepartment of Research and Development, Colorado Permanen-
te Medical Care Program, Denver, Colorado.
The views expressed in this article are those of the authors and do
not necessarily represent those of The Permanente Medical Group.
Acknowledgments: I acknowledge the many hours spent by my wife,
Janet M. Noffsinger, BA; son, Michael E. Noffsinger, and daughter,
Angela M. Noffsinger, in word processing and proofreading this
article.
Most especially, I would like to give heartfelt thanks to the physicians
who have run DIGMAs for their practices at the Kaiser Permanente-
San Jose Medical Center with the assistance of the author (EN).
Without their commitment and cooperation, this entire effort would
not have been possible.
Oncology: Joseph Mason, Jr, MD; Joseph Ramek, MD
Neurology: Rajan Bhandari, MD; Jai Cho, MD; C. Gregory
Culberson, MD
Endocrinology: Lynn Dowdell, MD; Patricia Kan, MD
Rheumatology: Thomas Abel, MD; David Granovetter, MD
Primary Care: Monica Donovan, MD (Family Practice)
I would also like to thank Administration at the Kaiser Permanen-
te-San Jose Medical Center for their support and encouragement.
... groupappointments will
increase access andefficiency, improveservice and qualityof care, enhance
patient andphysician
satisfaction, moreefficiently utilize
existing resources,and reduce the cost
of health caredelivery ...

112 The Permanente Journal / Spring 2000 / Volume 4 No. 2
healt
h s
yst
em
s
References1. Scott JC, Robertson BJ. Kaiser Colorado’s Cooperative HealthCare Clinic: a group approach to patient care. Manag Care Q1996 Summer;4(3):41-5.2. Beck A, Scott J, Williams P, Robertson B, Jackson D, Gade G,et al. A randomized trial of group outpatient visits forchronically ill older HMO members: the Cooperative HealthCare Clinic. J Am Geriatr Soc 1997;45:543-9.3. Scott J, Gade G, McKenzie M, Venohr I. Cooperative healthcare clinics: a group approach to clinical care. Geriatrics1998;53:68-70, 76-8, 81; quiz 82.4. Beck A, Kramer A, Scott J, Gade G, et al. Cooperative HealthCare Clinics: results from a 2 yr randomized trial. In prepara-tion:2000.5. Noffsinger EB. Increasing quality of care and access whilereducing costs through Drop-In Group Medical Appointments(DIGMAs). Group Pract J 1999 Jan;48(1):12-8.6. Noffsinger EB. Answering physician concerns about Drop-InGroup Medical Appointments (DIGMAs). Group Pract J 1999Feb;48(2):14, 16-21.7. Noffsinger EB. Benefits of Drop-In Group Medical Appoint-ments (DIGMAs) to physicians and patients. Group Pract J 1999Mar;48(3):21-4, 26-8.8. Noffsinger EB. Establishing successful primary care andsubspecialty Drop-in Group Medical Appointments (DIGMAs) inyour group practice. Group Pract J 1999 Apr;48(4):20-2,25-8.9. Noffsinger EB, Mason JE Jr, Culberson CG, Abel T, DowdellLA, Peters W, et al. Physicians evaluate the impact of Drop-InGroup Medical Appointments (DIGMAs) on their practices.Group Pract J 1999 Jun;48(6):22-3, 25-33.10. Noffsinger EB. How to develop successful Drop-In GroupMedical Appointments (DIGMAs) in the primary care setting. [inprocess,2000]11. Noffsinger EB. Increasing efficiency, accessibility, andquality of care through Drop-In Group Medical Appointments(DIGMAs). 1999. Submitted for publication.12. Noffsinger EB. Keys to success when establishing a Drop-InGroup Medical Appointment (DIGMA) Program. 1999.Submitted for publication.13. Noffsinger EB. Pitfalls to avoid when establishing a
successful Drop-In Group Medical Appointment (DIGMA)program. 1999. Submitted for publication.14. Noffsinger EB. Will Drop-In Group Medical Appointments(DIGMAs) Work In Practice? Permanente J 1999 Fall;3(3):58-67.15. Noffsinger EB. “Providing ‘Dr Welby care’ through Drop-InGroup Medical Appointments (DIGMAs),” presented at the:American Medical Group Association meeting, San Francisco,California, on June 19, 1999.16. Pratt JH. The class method of treating consumption in thehomes of the poor. J Am Med Assoc 1907 Aug;49(9):755-9.17. Cummings NA. Behavioral health in primary care: dollarsand sense. In: Cummings NA, Cummings JL, Johnson JN,editors. Behavioral health in primary care: a guide for clinicalintegration. Madison, CT: Psychosocial Press; 1997. p. 3-21.18. Mechanic D. Response factors in illness: the study of illnessbehavior. Soc Psychiatry 1966;1:11-20.19. Mechanic D. Strategies for integrating public mental healthservices. Hosp Community Psychiatry 1991;42:797-801.20. Green SA. Mind and body: the psychology of physicalillness. Washington, DC: American Psychiatric Press; 1985.21. Cohen-Cole SA, Levinson RM. The biopsychosocial model inmedical practice. In: Stoudemire A, editor. Human behavior: anintroduction for medical students. Philadelphia, PA: Lippincott;1994. p. 22-63.22. Derogatis LR, Wise TN. Anxiety and depressive disorders inthe medical patient. Washington, DC: American PsychiatricPress; 1989.23. Morrison I. The 1 percent problem: the organization ofmedicine has changed little in a century. Health Forum J 1999Jul-Aug;42(4):42-6.24. Brunk D. Group medical appointments aid communication.Intern Med News 2000 March 1;33(5):50.25. Brunk D. Group appointments may enhance physician-patient relationship. Fam Prac News 2000 March 15;30(6):70.26. Walpert B. Patients tired of waiting? Try these strategies ... Anovel approach for capitation: group visits. ACP-ASIM Observer1999 Oct;19(9):5.27. Weyrauch KF. Does continuity of care increase HMOpatients’ satisfaction with physician performance? J Am BoardFam Pract 1996;9:31-6.
On Being IllThere is, let us confess it (and illness is the great
confessional), a childish outspokenness in illness; things aresaid, truths blurted out, which the cautious respectability
of health conceals.Virginia Woolf,
On Being Ill, The Moment (1947)

113The Permanente Journal /Spring 2000 / Volume 4 No. 2
health
syste
msAlthough the STAR (Satisfaction Track-
ing and Reporting) survey has been used for sev-eral years by Kaiser Permanente (KP), I’mamazed how little working knowledge many Per-manente clinicians have about this tool. All suc-cessful organizations listen to their customers—and we are no exception. Therefore, David Glassfrom Program Offices provides us with insighton just what the STAR survey is and how it canprovide useful information to our medical groups.
– Lee Jacobs, MD, Section EditorDr Jacobs: To get us started, David, why don’t
you tell our readers when the STAR survey was firstimplemented, and why?
Mr David Glass: The STAR survey was started inthe summer of 1988 as an attempt to col-lect member information in a uniformmanner and on a regular basis across theProgram. Prior to 1988, KP Regions occa-
sionally conducted their own surveys but not on anannual basis. The nonmember component of the STARsurvey was not begun until 1995.
Dr Jacobs: You mentioned that several Regionshad used their own periodic member surveys priorto 1988. I thought that surveying members in healthcare was more of a recent business phenomenon.
Mr Glass: There is clearly a much stronger focus onmember and patient attitudes now than in the past. How-ever, the importance of those attitudes still shined through,even in our distant past. For example, we have a mem-ber and terminated-member survey from our SouthernCalifornia Region from 1958 that was spurred by a largeloss of membership to Blue Cross in that year.
Dr Jacobs: Could you describe for our readers howthe STAR survey is actually accomplished?
Mr Glass: The survey is conducted on an ongoingbasis by telephone with a random sample of ourmembership, and since 1995, a random sample ofnonmembers in each Region.
Dr Jacobs: You mentioned that in 1995 the STARsurvey was expanded to include nonmembers as wellas members. Why was that?
Mr Glass: The addition of nonmembers to the sur-vey really was a reflection of the evolution of the healthcare marketplace. The STAR was started in the late 1980sat a time when Kaiser Permanente still occupied a fairlycomfortable niche and was somewhat internally focused.We wanted to hear from our members about ourstrengths and weaknesses. By the mid-1990s, however,Kaiser Permanente began to confront stiff competition,and we had a need to better understand our potentialin the local market. As a result, we started asking non-members for their evaluation of their own health planas well as their perceptions of Kaiser Permanente.
Dr Jacobs: David, I’m certain that through the yearsour organization has collected a lot of informationfrom the STAR survey. However, I think there is someconfusion in the Permanente community as to howthis information might benefit Kaiser Permanente.Could you give our readers an idea how the resultsof the STAR survey might be used?
Mr Glass: A good question. I think that there are atleast six main uses of the STAR survey (Table 1). First, itgives us a chance to determine what is most importantto our members. Second, it helps us track how we aredoing on those important attributes. Third, it provides us
What does the STAR Survey mean to a Permanente Physician?Interview with David Glass, National Director of Market Research
Table 1. Largest KP Regional increases on satisfaction in the 1990s (1999 score minus 1991score). Georgia has made significant improvement on these key drivers
Attribute Region 1999 Scorea 1991 Scorea Difference
Overall satisfaction GA 66 52 +14
Care index GA 68 50 +18
Phone wait GA 65 30 +35
Appointment waitHIGA
6459
4944
+15+15
Have MD OH 83 59 +24
See MD GA 74 55 +19
MD Interest/Attention Southern CA 70 66 +4
a These scores represent the percent of members giving a rating of 8, 9, or 10 on a 10-point scale.
We wanted to hearfrom our membersabout our strengths
and weaknesses.
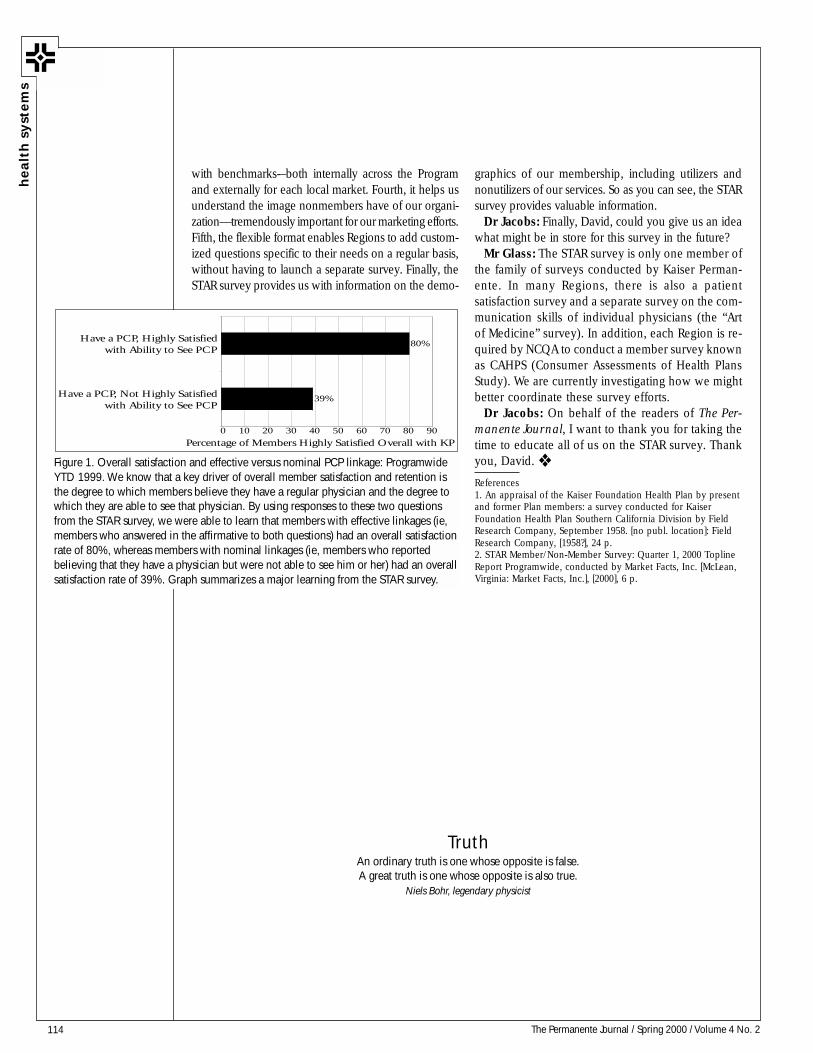
114 The Permanente Journal / Spring 2000 / Volume 4 No. 2
healt
h s
yst
em
s
with benchmarks-–both internally across the Programand externally for each local market. Fourth, it helps usunderstand the image nonmembers have of our organi-zation—tremendously important for our marketing efforts.Fifth, the flexible format enables Regions to add custom-ized questions specific to their needs on a regular basis,without having to launch a separate survey. Finally, theSTAR survey provides us with information on the demo-
graphics of our membership, including utilizers andnonutilizers of our services. So as you can see, the STARsurvey provides valuable information.
Dr Jacobs: Finally, David, could you give us an ideawhat might be in store for this survey in the future?
Mr Glass: The STAR survey is only one member ofthe family of surveys conducted by Kaiser Perman-ente. In many Regions, there is also a patientsatisfaction survey and a separate survey on the com-munication skills of individual physicians (the “Artof Medicine” survey). In addition, each Region is re-quired by NCQA to conduct a member survey knownas CAHPS (Consumer Assessments of Health PlansStudy). We are currently investigating how we mightbetter coordinate these survey efforts.
Dr Jacobs: On behalf of the readers of The Per-manente Journal, I want to thank you for taking thetime to educate all of us on the STAR survey. Thankyou, David. ❖
References1. An appraisal of the Kaiser Foundation Health Plan by presentand former Plan members: a survey conducted for KaiserFoundation Health Plan Southern California Division by FieldResearch Company, September 1958. [no publ. location]: FieldResearch Company, [1958?], 24 p.2. STAR Member/Non-Member Survey: Quarter 1, 2000 ToplineReport Programwide, conducted by Market Facts, Inc. [McLean,Virginia: Market Facts, Inc.], [2000], 6 p.
39%
80%
0 10 20 30 40 50 60 70 80 90
Have a PCP, Not Highly Satisfiedwith Ability to See PCP
Have a PCP, Highly Satisfiedwith Ability to See PCP
Percentage of Members Highly Satisfied Overall with KP
Figure 1. Overall satisfaction and effective versus nominal PCP linkage: ProgramwideYTD 1999. We know that a key driver of overall member satisfaction and retention isthe degree to which members believe they have a regular physician and the degree towhich they are able to see that physician. By using responses to these two questionsfrom the STAR survey, we were able to learn that members with effective linkages (ie,members who answered in the affirmative to both questions) had an overall satisfactionrate of 80%, whereas members with nominal linkages (ie, members who reportedbelieving that they have a physician but were not able to see him or her) had an overallsatisfaction rate of 39%. Graph summarizes a major learning from the STAR survey.
TruthAn ordinary truth is one whose opposite is false.A great truth is one whose opposite is also true.
Niels Bohr, legendary physicist

115The Permanente Journal / Spring 2000 / Volume 4 No. 2
DONALD W. PARSONS, MD, is the Permanente Federation’s Associate Executive Director for Health Policy Development.E-mail: [email protected]
Patient safety has emerged as a major health policy issue. Fortu-nately, several years ago, Kaiser Permanente’s Health Policy Com-mittee peered into the crystal ball and made a modest investmentin founding the National Patient Safety Foundation (NPSF). Thisinvestment was an important first step in taking ownership of anew wave of consumer concern about health care. That wave hasnow crested with publication of the Institute of Medicine’s (IOM)To Err is Human: Building a Safer Health System, an effort con-tributed to substantially by the NPSF and its members.1
Authored by a prestigious committee, which included DavidLawrence, MD, KFHP CEO, the report2 summarizes what is knownabout the toll taken on American life by preventable error in hospi-tals. The report concludes that most problems are not due to mali-cious intent or even to individual failure but can be ascribed tofailure of systems and processes. Two large, retrospective medicalrecord review studies (one based on 1992 experience in Utah andColorado3 and another based on 1985 experience in New York4)indicated that, nationwide, as many as 98,000 patients each yearlose their lives, most commonly because of medication error orcomplications of infection. Although these estimates are based onold data, direct observations have suggested that these estimatesmay be low. Given also that no published studies have describedexperience in nonhospital settings, the aggregate loss of life may bemuch higher. We do know that as many as 10% of hospital admis-sions are occasioned by adverse drug events,1 suggesting a large-magnitude problem in nonhospital settings. And no solid estimate—only speculation—has been presented to quantify the secondarycontribution of medications to fatal car crashes and falls. For ex-ample, the sedating antihistamine diphenhydramine may cause driverimpairment as severe as that caused by alcohol.
Errors of commission are more easily measured than errors ofomission. Among the most vulnerable of our citizens, the frailelderly, noncompliance with medication prescriptions may be highand may account for preventable failure to control acute exacer-bation of chronic illness—and this failure can result in fatal com-plications. In addition, the failure to prescribe or take medicationsof known efficacy (eg, beta blockers for patients who have had amyocardial infarction) is thought to contribute to many cases ofpreventable fatal illness.
The magnitude of the patient safety problem is poorly under-stood. Physicians and other health care professionals are trained—and are expected—to deliver error-free care. When regarded asindicating professional shortcomings, error causes professional blameand shame. Errors can lead to sanctions imposed by regulatory bod-ies, public embarrassment, and malpractice litigation. The pervasivefear of discovering grounds for lawsuit drives underground the in-terest of health practitioners and institutions to report errors, even(and especially) those that cause patients no harm.
During a tumultuous election year in which there is consider-able restlessness on several fronts about America’s flawed healthcare system, the IOM report’s recommendations for mandatory aswell as voluntary reporting systems have captured the imaginationof both the American public and its Congressional representatives.Consumers are demanding information about specific hospitalsand practitioners. Congressional hearings have generated enthusi-asm about establishing new federally prescribed mandatory re-porting systems for the most severe errors, such as death, perma-nent disability, and wrong-site surgery. Only the provider tradegroups (specifically, the American Medical Association and theAmerican Hospital Association) have voiced strong opposition topublic disclosure of specific information, cautioning that this dis-closure would invite trial attorneys to file a deluge of lawsuits.Currently, few instances of true negligence result in medical mal-practice lawsuits. Many entities, including KP, think that strongfederal peer review protections and tort reform must accompanymandatory reporting if such reporting is to be legislated, or elsereporting will not occur—a situation experienced in several statesthat have enacted mandatory error reporting statutes. For example,Pennsylvania has implemented such a system but elicited only asingle report from among all Philadelphia hospitals during themost recent reporting cycle. All health care providers and practi-tioners fear malpractice suits, loss of professional reputation, andmedia exposure.
A voluntary reporting system in which close calls and “nearhits” would be aggregated and analyzed is a more acceptableapproach, particularly if reports are stripped of patient and pro-vider identifiers. Congress has heard from the Aviation SafetyReporting System (ASRS), based in NASA, about its 25-year-oldsystem, which elicits up to 30,000 reports annually—all madeanonymous after initial verification. Because no plaintiff discov-ery of that information has ever succeeded, great credibility andtrust have been conferred in the ASRS by pilots and by otherairline employees. Vastly improved aviation safety over the pasttwo decades is a result of this system; why can’t the same thinghappen in medicine? After all, the anesthesiologists in this coun-try have shown that concerted action can mitigate damage in ahigh-risk environment. Operating suites are 90% safer now thanthey were just ten years ago because of improved patient moni-toring, application of professional guidelines, and sharing of in-formation through the Anesthesia Patient Safety Foundation.
Individual members of Congress have staked out turf in thisdebate already. Rep Bill Thomas (R-CA), Chairman of the HouseWays and Means Committee’s Health Subcommittee, has indi-cated that there can be no greater protection of patients thansafe medical care. Therefore, the subject of patient safety canlogically be introduced into the ongoing debate on managed
By Donald W. Parsons, MD
Primum Non Nocere:Safety, Medical Errors and Congressional Intent
exte
rnal a
ffairs

116 The Permanente Journal / Spring 2000 / Volume 4 No. 2
care reform and patient protection. Others have called for newlycommissioned demonstration projects to test the concepts ofmandatory and voluntary reporting. Sen Arlen Specter (R-PA),who chairs the Senate Health and Human Services (HHS) LaborAppropriations Subcommittee, wants to make new money avail-able to the FDA for more intense oversight of medication er-rors. Sen Bill Frist (R-TN), the Senate’s lone physician—wholed the push to redefine the newly named Agency for HealthResearch and Quality (AHRQ) in last year’s Congressional ses-sion—would like to establish a new center for patient safetywithin that agency. This recommendation has also been es-poused by the Administration; indeed, the President has calledon all federal agencies responsible for health care programs tobuild patient safety expectations into all systems (the VeteransAdministration and the Department of Defense) and into allcontracts administered by the Health Care Financing Adminis-tration (HCFA) and the Federal Employees Health Benefit Pro-gram (FEHBP). Senators Lieberman, Grassley, and Bryan haveintroduced legislation to set up a national center for patientsafety and a national mandatory reporting system for all Medi-care and Medicaid contracting providers. Patient safety is a“motherhood-and-apple-pie” issue that no legislator standingfor reelection will oppose. Tom Bliley (R-VA), who chairs theHouse Commerce Committee, has taken the argument one stepfurther by supporting Sen Ron Wyden’s (D-OR) call for publicdisclosure of malpractice and disciplinary reports on physicianscontained in the National Practitioner Data Bank.
The private sector is jumping in front of the parade. The largestis the “Leapfrog Group,” which includes leaders from several largepurchasers of health care, including General Motors, General Elec-tric, GTE, the Pacific Business Group on Health, the federal Officeof Personnel Management, and others. This group has developedand disseminated three standards for patient safety that have beenconsidered by General Motors and by some large purchasers, in-cluding the “V-8” group of eight purchasing coalitions, in forminghealth plan contractual performance expectations for the year 2000and beyond (Pat Salber, MD, personal communication). First, thegroup wants health plans to influence their contracted hospitals toadopt computerized physician order entry for medications, a tech-nique available in only a small percentage of hospitals now butwhich has reduced medication errors by two thirds in the VA hos-pital system. Second, the group is calling for improved trainingand staffing for intensive care units. Third, the group is setting
volume standards for hospitals where highly technical procedures,such as open-heart surgery, are done. All these new standards areevidence-based and are tied to improved patient outcomes throughreduction of preventable complications, according to the LeapfrogGroup’s Executive Director, Suzanne del Banco (who can bereached at (202) 973-2953 or e-mail [email protected]).
As the IOM has cautioned, medical errors and patient safety arenot problems of managed care. Instead, these problems pervadeAmerican medicine.1 The good news for Kaiser Permanente istwofold: First, we have an enviable track record and have beenexamining our own data for some time; second, as David Lawrenceis eager to point out, correcting such systemic problems requiresan integrated medical care delivery system based on patient focus,professional and administrative collaboration, and excellent infor-mation technology.2 In the area of patient safety, the private sectoris likely to develop innovations before Congress can act. We at KPare moving ahead with our own efforts to promote patient safetyand report errors.5,6
Our new Health Policy Institute, directed by Senior Vice Presi-dent Bob Crane, has convened national experts who have devel-oped policy suggestions to guide legislative activity. We are call-ing for a nationwide, voluntary reporting system modeled on theAviation Safety Reporting System and including additional protec-tions to safeguard the information from discovery intended solelyto encourage civil legal action. We also recommend State-man-dated reporting of near-miss events, postmarketing drug and de-vice surveillance, and funding for a new national center for pa-tient safety.
With the high current level of public interest in patient safety,we can be sure Congress will take action soon. ❖
References1. Kohn LT, Corrigan J, Donaldson MS, editors; Committee on Quality of HealthCare in America, Institute of Medicine. To err is human: building a safer healthsystem. Washington DC: National Academy Press; Mar 2000, 312 p.2. Lawrence D. Is Medical Care Obsolete? Speech for National Press Club,Washington DC, July 14, 1999.3. Thomas EJ, Studdert DM, Newhouse JP, Zbar BI, Howard KM, Williams EJ, et al.Costs of medical injuries in Utah and Colorado. Inquiry 1999 Fall;36(3):255-64.4. Brennan TA, Leape LL, Laird NM, Hebert L, Localio AR, Lawthers AG, et al.Incidence of adverse events and negligence in hospitalized patients: results ofthe Harvard Medical Practice Study I. N Engl J Med 1991 Feb 7;324(6):370-6.5. Tolbert LD. The risk management approach at Kaiser Permanente Los AngelesMedical Center. Permanente J 1998 Summer; 2(3):69-72.6. Stajer R, Pate B. Kaiser Permanente’s response to JCAHO’s Sentinel EventStandards: Our Significant Event Root-Cause Analysis Program Leads ToPreventing Medical Errors (this issue, The Permanente Journal).
exte
rnal
aff
air
s

117The Permanente Journal / Spring 2000 / Volume 4 No. 2
exte
rnal a
ffairsThis article explains Kaiser
Permanente’s Programwide policy regardingSignificant Events and how this policy meetsJCAHO standards regarding Sentinel Events. TheRoot-Cause Analysis Program developed in theCalifornia Division-Southern California Regionto support this policy is described in detail withparticular emphasis illustrating our focus onpatient safety and risk reduction in our healthcare delivery systems. Since the policy went intoeffect in April 1998, our work has led us to con-clude that blaming individuals solely when anadverse event occurs hinders our ability to findthe true root cause, whose correction will pre-vent the adverse event from recurring. Similarfindings are noted in relevant literature.
IntroductionThe prevalence of medical errors has galvanized
health care leaders, regulators, politicians, andaccreditors around the issue of improving patientsafety. Proposals for mandatory reporting of medicalerrors are currently being studied by the US Con-gress; at the same time, the Joint Commission for theAccreditation of Health Care Organizations (JCAHO)has heightened its requirements for analyzing rootcauses of Sentinel Events.
Health care is an inherently risky business that isalso extremely complex—and becoming increasinglyso. Hospital care is more complicated, patients aresicker, choices among medications are more numer-ous, and technology is more sophisticated than everbefore. Paradoxically, the technologic advances thathelp achieve medical miracles also increase thechances that something will go wrong.
Although some medical errors are inevitable, manyare preventable. Most medical errors are not the resultof negligence or incompetence but of faulty systemsand poorly designed processes that increase the likeli-hood of mistakes. We believe that frank, open discus-sion about the vulnerabilities in our health care systemscan help reduce errors and create safer environments;however, this type of discussion requires a fundamen-tal shift in attitude. With this requirement in mind, Kai-ser Permanente (KP) developed a process designed tochange the culture of reporting medical errors. Our in-tent is threefold: to move away from defensiveness andpointing fingers, to identify flaws in the system, and todesign ways to create a safer patient environment.
Root-Cause Analysis: the Push from JCAHOPatient safety has always been a priority of our
organization. Our policies and procedures providestrict internal quality control measures that far ex-ceed those mandated by federal, state, local, and in-dependent oversight groups. Quality and risk man-agement committees routinely examine unexpecteddeaths and errors and monitor patient safety issues.
Although not a new concept for those familiar withquality improvement, root-cause analysis has at-tracted a resurgence of interest as a result of theJoint Commission on Accreditation of Healthcare Or-ganizations (JCAHO) policy for identifying and man-aging medical errors. The process is designed tofoster a blame-free environment that encouragesseveral activities: systematic reporting of SignificantEvents; in-depth analyses done to identify the “root”or ultimate systemic cause of errors; implementa-tion of barriers or safeguards to reduce the likeli-hood of similar errors occurring in the future; anddissemination of lessons learned.
To improve its processes of event analysis, theKP California Division incorporated theories andconcepts taught by, among others, Drs LucianLeape, Richard Cook, and James Reason as well asorganizations such as the National Patient SafetyFoundation and the Institute for Healthcare Im-provement. Input of KP physicians, directors ofquality assurance programs, risk managers, seniorleaders, committee chairpersons, nursing represen-tatives, and other internal resources are also re-flected in these processes.
Defining JCAHO’s “Sentinel” andKP’s “Significant” Events
All would agree that a medical mistake that makesthe headlines is a Significant Event. The wrong legamputated, for example, or a chemotherapy over-dose are definitely Significant Events. Most errors don’tmake the headlines, however, and are considerablyless dramatic.
The KP definition of a Significant Event is consis-tent with JCAHO’s definition of a Sentinel Event1
(any unexpected occurrence involving death or se-rious physical or psychological injury or risk thereof),but we take this definition a step further: Our defi-nition of a Significant Event is any unexpected clini-cal or nonclinical occurrence that results in loss oflife or bodily harm, disrupts operations, or threat-
Kaiser Permanente’s Response to JCAHO’s SentinelEvent Standards: Our Significant Event Root-CauseAnalysis Program Leads to Preventing Medical Errors
By Ricki Stajer, RN, MA, CPHQBud Pate, BA, REHS
RICKI STAJER, RN, MA, CPHQ (left), is a Senior Consultant in the California Division, Southern California officeof Accreditation and Licensing. She has worked for Kaiser Permanente since 1989. E-mail: [email protected]
BUD PATE, BA, REHS (right), is the Director of Accreditation and Licensing in Southern California. He receivedhis Bachelor of Arts degree from the University of California at Los Angeles. E-mail: [email protected]
Most medicalerrors are not the
result ofnegligence or
incompetence butof faulty systems
and poorlydesigned processesthat increase the
likelihood ofmistakes.

118 The Permanente Journal / Spring 2000 / Volume 4 No. 2
exte
rnal
aff
air
s
ens the organization’s assets and reputation. Thedefinition also includes “near misses”—any break-down in process that carries the risk of a seriousadverse outcome.2
Significant Events range from unanticipated deathof a patient to outbreaks of nosocomial infectionto fires and accidental release of hazardous mate-rials. Kaiser Permanente classifies Significant Eventsinto three levels, with Level 1 the most serious(see sidebar).
Fostering Blame-Free ReportingFear of blame and its consequences tends to drive
mistakes “underground.” Not all mistakes are hid-den, however; obviously, the more egregious errorsare impossible to hide. Nonetheless, for every ad-verse event that sets the rumor mills abuzz, manymore such events occur that we would rather ig-nore: mishaps where the error was caught beforeharm was done. Yes, our policy is to report them,but the natural inclination is not to do so.
Because health care still relies primarily on train-ing and standards to prevent errors and enforcesstandards by imposing punishment for lapses,health care workers have a strong incentive not toreport mistakes. This incentive robs clinicians andothers of two more beneficial incentives: to inves-tigate underlying causes that may have contributedto the error and to make the necessary changes toprevent recurrence.
Complex systems fail because of the combinationof multiple small failures, each individually insuffi-cient to cause an accident.3 Numerous steps existalong the way to completing even a simple process,and numerous steps lead to numerous opportunitiesfor error; and any unreported error—even a “nearmiss”—is a lost opportunity for improvement.
The KP Significant Event policy requires regionalreporting and root-cause analysis of Level 1 and 2events, but because reporting even minor errors canhelp us to pinpoint flaws in the system, we encour-age staff to report all errors. We emphasize that weare looking for ways in which systems fail; we arenot seeking to pinpoint blame. The more we learnwhy things go wrong, the more safeguards can beput in place to prevent error recurrence.
An example of this is the problem of the missingidentification bands for infants. When we noticed acluster of minor (Level 3) events, our analysis re-vealed that the bands are very difficult to keep onsmall wrists. The bands slip off, and rebanding the
babies is a cumbersome, time-consuming task. Post-partum obstetric units tend to be hectic places wheremistakes can occur when information is transferredonto new bands. Underlying the problem was thetype of bands being used: The design required nursesto slip their fingers inside the bands, thereby auto-matically widening them. When (as typically hap-pens) babies lose weight, the bands become too bigand fall off. The solution was a new banding systemwith a pull-through lock that can be tightened as thebaby loses weight.
A blame-and-punishment culture would have calledfor discipline of the nurse who put the wrong infor-mation on the wristband. This approach would haveignored other factors that enabled the error to bemade and would thus have done little to ensure thatthe error did not happen again. In short, nothingwould have been learned.
Significant Event DefinedLevel One
• Infant abduction or discharge to thewrong family
• Rape of a patient• Hemolytic transfusion reaction• Any invasive procedure—wrong
patient; wrong side, organ, or part• Suicide of a patient in a 24-hour care
facility• Unexpected death or loss of function
not related to the natural course ofillness
• Significant deviation from the usualprocesses of care
• Adverse media attention
Level Two
• Nosocomial outbreak or foodborneillness
• Reportable incident to the State Boardof Medical Examiners or NationalPractitioners’ Data Bank
• Internal or external disaster• Regulatory sanctions• Release of toxic substance• Suicide within the KP Program• Cluster of Level 3 events
Level Three
• Unusual occurrences
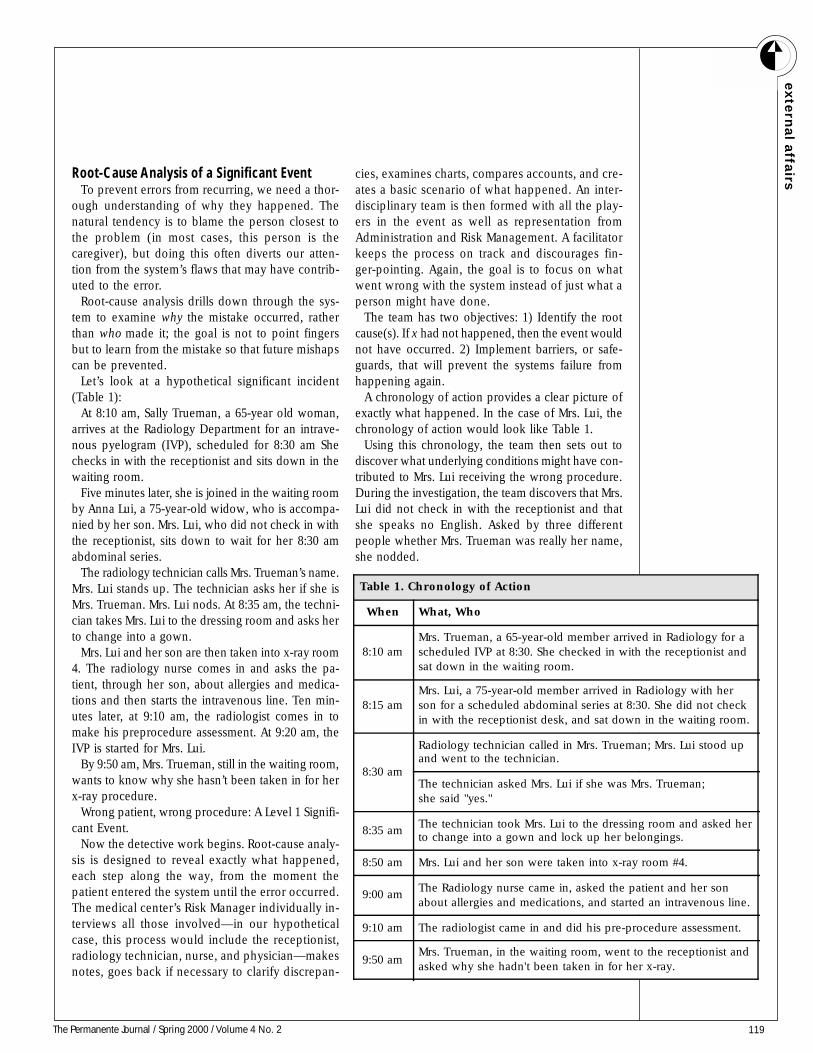
119The Permanente Journal / Spring 2000 / Volume 4 No. 2
exte
rnal a
ffairsRoot-Cause Analysis of a Significant Event
To prevent errors from recurring, we need a thor-ough understanding of why they happened. Thenatural tendency is to blame the person closest tothe problem (in most cases, this person is thecaregiver), but doing this often diverts our atten-tion from the system’s flaws that may have contrib-uted to the error.
Root-cause analysis drills down through the sys-tem to examine why the mistake occurred, ratherthan who made it; the goal is not to point fingersbut to learn from the mistake so that future mishapscan be prevented.
Let’s look at a hypothetical significant incident(Table 1):
At 8:10 am, Sally Trueman, a 65-year old woman,arrives at the Radiology Department for an intrave-nous pyelogram (IVP), scheduled for 8:30 am Shechecks in with the receptionist and sits down in thewaiting room.
Five minutes later, she is joined in the waiting roomby Anna Lui, a 75-year-old widow, who is accompa-nied by her son. Mrs. Lui, who did not check in withthe receptionist, sits down to wait for her 8:30 amabdominal series.
The radiology technician calls Mrs. Trueman’s name.Mrs. Lui stands up. The technician asks her if she isMrs. Trueman. Mrs. Lui nods. At 8:35 am, the techni-cian takes Mrs. Lui to the dressing room and asks herto change into a gown.
Mrs. Lui and her son are then taken into x-ray room4. The radiology nurse comes in and asks the pa-tient, through her son, about allergies and medica-tions and then starts the intravenous line. Ten min-utes later, at 9:10 am, the radiologist comes in tomake his preprocedure assessment. At 9:20 am, theIVP is started for Mrs. Lui.
By 9:50 am, Mrs. Trueman, still in the waiting room,wants to know why she hasn’t been taken in for herx-ray procedure.
Wrong patient, wrong procedure: A Level 1 Signifi-cant Event.
Now the detective work begins. Root-cause analy-sis is designed to reveal exactly what happened,each step along the way, from the moment thepatient entered the system until the error occurred.The medical center’s Risk Manager individually in-terviews all those involved—in our hypotheticalcase, this process would include the receptionist,radiology technician, nurse, and physician—makesnotes, goes back if necessary to clarify discrepan-
cies, examines charts, compares accounts, and cre-ates a basic scenario of what happened. An inter-disciplinary team is then formed with all the play-ers in the event as well as representation fromAdministration and Risk Management. A facilitatorkeeps the process on track and discourages fin-ger-pointing. Again, the goal is to focus on whatwent wrong with the system instead of just what aperson might have done.
The team has two objectives: 1) Identify the rootcause(s). If x had not happened, then the event wouldnot have occurred. 2) Implement barriers, or safe-guards, that will prevent the systems failure fromhappening again.
A chronology of action provides a clear picture ofexactly what happened. In the case of Mrs. Lui, thechronology of action would look like Table 1.
Using this chronology, the team then sets out todiscover what underlying conditions might have con-tributed to Mrs. Lui receiving the wrong procedure.During the investigation, the team discovers that Mrs.Lui did not check in with the receptionist and thatshe speaks no English. Asked by three differentpeople whether Mrs. Trueman was really her name,she nodded.
Table 1. Chronology of Action
When What, Who
8:10 amMrs. Trueman, a 65-year-old member arrived in Radiology for ascheduled IVP at 8:30. She checked in with the receptionist andsat down in the waiting room.
8:15 amMrs. Lui, a 75-year-old member arrived in Radiology with herson for a scheduled abdominal series at 8:30. She did not checkin with the receptionist desk, and sat down in the waiting room.
8:30 am
Radiology technician called in Mrs. Trueman; Mrs. Lui stood upand went to the technician.
The technician asked Mrs. Lui if she was Mrs. Trueman;she said "yes."
8:35 amThe technician took Mrs. Lui to the dressing room and asked herto change into a gown and lock up her belongings.
8:50 am Mrs. Lui and her son were taken into x-ray room #4.
9:00 amThe Radiology nurse came in, asked the patient and her sonabout allergies and medications, and started an intravenous line.
9:10 am The radiologist came in and did his pre-procedure assessment.
9:50 amMrs. Trueman, in the waiting room, went to the receptionist andasked why she hadn't been taken in for her x-ray.
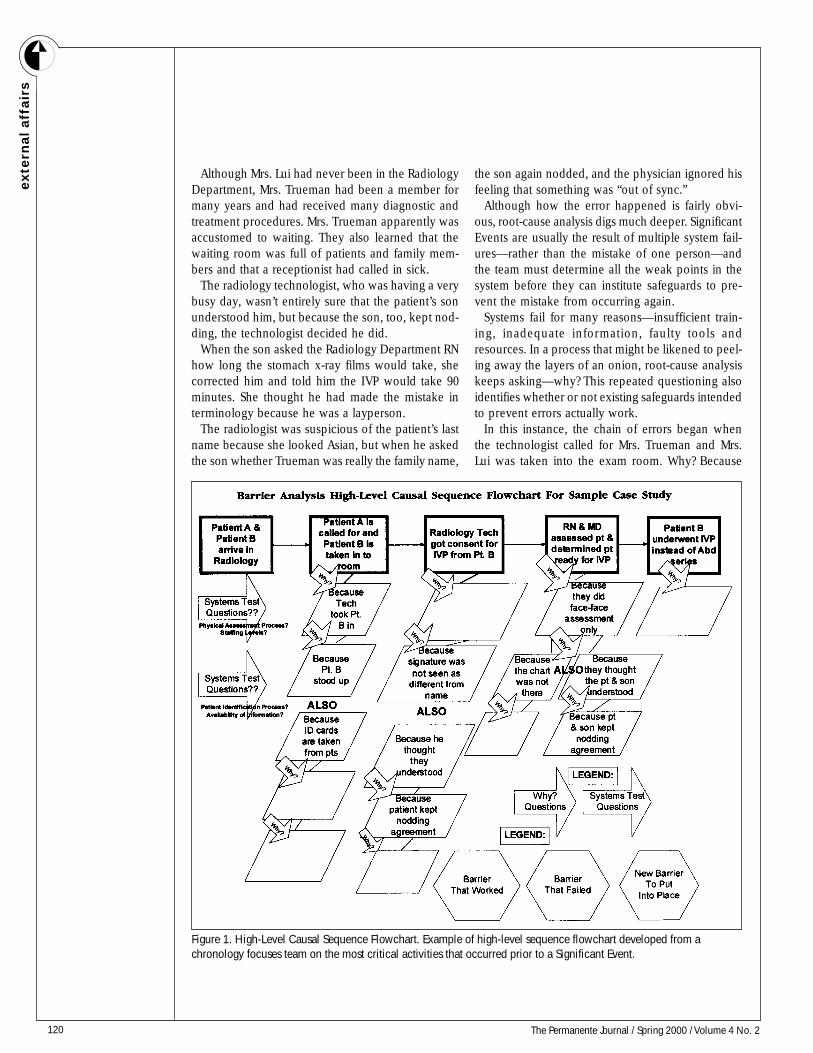
120 The Permanente Journal / Spring 2000 / Volume 4 No. 2
exte
rnal
aff
air
s
Although Mrs. Lui had never been in the RadiologyDepartment, Mrs. Trueman had been a member formany years and had received many diagnostic andtreatment procedures. Mrs. Trueman apparently wasaccustomed to waiting. They also learned that thewaiting room was full of patients and family mem-bers and that a receptionist had called in sick.
The radiology technologist, who was having a verybusy day, wasn’t entirely sure that the patient’s sonunderstood him, but because the son, too, kept nod-ding, the technologist decided he did.
When the son asked the Radiology Department RNhow long the stomach x-ray films would take, shecorrected him and told him the IVP would take 90minutes. She thought he had made the mistake interminology because he was a layperson.
The radiologist was suspicious of the patient’s lastname because she looked Asian, but when he askedthe son whether Trueman was really the family name,
the son again nodded, and the physician ignored hisfeeling that something was “out of sync.”
Although how the error happened is fairly obvi-ous, root-cause analysis digs much deeper. SignificantEvents are usually the result of multiple system fail-ures—rather than the mistake of one person—andthe team must determine all the weak points in thesystem before they can institute safeguards to pre-vent the mistake from occurring again.
Systems fail for many reasons—insufficient train-ing, inadequate information, faulty tools andresources. In a process that might be likened to peel-ing away the layers of an onion, root-cause analysiskeeps asking—why? This repeated questioning alsoidentifies whether or not existing safeguards intendedto prevent errors actually work.
In this instance, the chain of errors began whenthe technologist called for Mrs. Trueman and Mrs.Lui was taken into the exam room. Why? Because
Figure 1. High-Level Causal Sequence Flowchart. Example of high-level sequence flowchart developed from achronology focuses team on the most critical activities that occurred prior to a Significant Event.

121The Permanente Journal / Spring 2000 / Volume 4 No. 2
exte
rnal a
ffairsMrs. Lui stood up. Why? Because neither she nor her
son understood English. Why wasn’t this recognized?Because they both kept nodding as though they un-derstood. This scenario raises a number of systemsprocess questions about existing safeguards—patientidentification (ID) cards, charts and consent form sig-natures—that should have prevented the error. Thescenario also brings up issues of patient and staffattitudes and communication.
Because teams often uncover contributing factors aswell as root causes, improvement activities must beprioritized. The Barrier Analysis High-Level Casual Se-quence Flowchart was developed to assist in the iden-tification of key points on the chronology. They aremoved to the flowchart for more intensive analysis (seeFigure 1). To help teams identify what are truly rootcauses—causes most fundamentally linked to theevent—and those that must be corrected in order toreduce risk to the next patient, participants are asked tocomplete a phrase: “If x had not occurred, then thisSignificant Event would not have happened.” The teamcontinues to ask questions until the answers are obvi-ously beyond its realm of capability to change—bud-get constraints, staffing shortages, for example.
Blame is integral to human nature and, in a caselike this, it is easy to see how the analysis processcould lapse into finger-pointing. Why didn’t the tech-nician make sure he had the right patient? Why didn’tthe physician go with his hunch that something waswrong? Why didn’t Mrs. Trueman stand up when hername was called? If she had, the whole thing wouldn’thave happened...this time.
In performing root-cause analysis, the team mustovercome blame and defensiveness so that the sys-tem can be opened up for review. To do this, par-ticipants are taught to focus on the system and awayfrom the individual. The issue under review is notthe clinical outcome but the event—the point in thesystem where the error occurred. In this case, theoutcome was Mrs. Lui receiving the wrong proce-dure begun when Mrs. Lui answered to the wrongname and complicated by repeated missed clues.The Significant Event was the mix-up of the pa-tients. The root cause was an inadequate patientidentification system.
Outcomes are all about the previous patient. Root-cause analysis is designed to protect the next pa-tient. What safeguards can be put into place to en-sure that the error doesn’t happen again? The idea isto create a safer patient environment by eliminatingfuture risk instead of defending past practices.
Moving Beyond Blame and PunishmentThe belief that human error is the most common
cause of accidents is a comfortable one because itprovides satisfying closure to an accident. The culpritis identified, removed from practice, or put throughremedial training. Blame is emotionally satisfying; theproblem is that it doesn’t fix the problem.
In fact, blame is like a huge boulder on the roadto progress. Until you can move beyond it, pro-ceeding with the more constructive work of fixingwhat is wrong with the system is difficult. But al-though we understand how destructive blaming eachother is to systems improvement, we continue toparticipate in it.
Through the root-cause analysis process, we havediscovered that although blame is difficult to avoidentirely, it can be managed. One way to move be-yond blame is simply to acknowledge its existence.Someone (in most cases, the caregiver) was to blamefor the error. Mistakes happen. We can’t prevent allof them or entirely eliminate the possibility that theywill occur. When blame becomes an obstacle, ac-tively recognize its presence and move on.
All this is not to say that we should not hold our-selves accountable for our performance. Patient caremust be entrusted to those who can competently carryit out. If discipline is warranted, the decision must bemade early in the review process, preferably rightafter the initial investigation and determination of theprobable cause but before actual root-cause analy-sis. To expect much candor from anyone hoveringunder the cloud of possible discipline is unrealistic.
Ultimately, the opportunity to learn from the eventmay be more valuable than stifling participation withthe threat of discipline. Remember, root-cause analy-sis expects that the people who are part of the pro-cess will make errors. By anticipating variation in hu-man performance and designing our processes to ac-count for them, we can go on to build safer systems.
Communicating Significant Event FindingsIn Southern California, findings from each KP medi-
cal center’s Significant Event analysis are reviewed atthe Risk Managers’ monthly meetings.
As a multidisciplinary clearinghouse, the SignificantEvent Review Committee (SERC) reviews all Signifi-cant Events occurring in KP Southern California facilitieswith the ultimate goal of ensuring patient safety. Thecommittee works closely with similar structures inNorthern California to coordinate and compare find-ings and to plan risk-reduction strategies. The
... blame is like ahuge boulder on
the road toprogress.
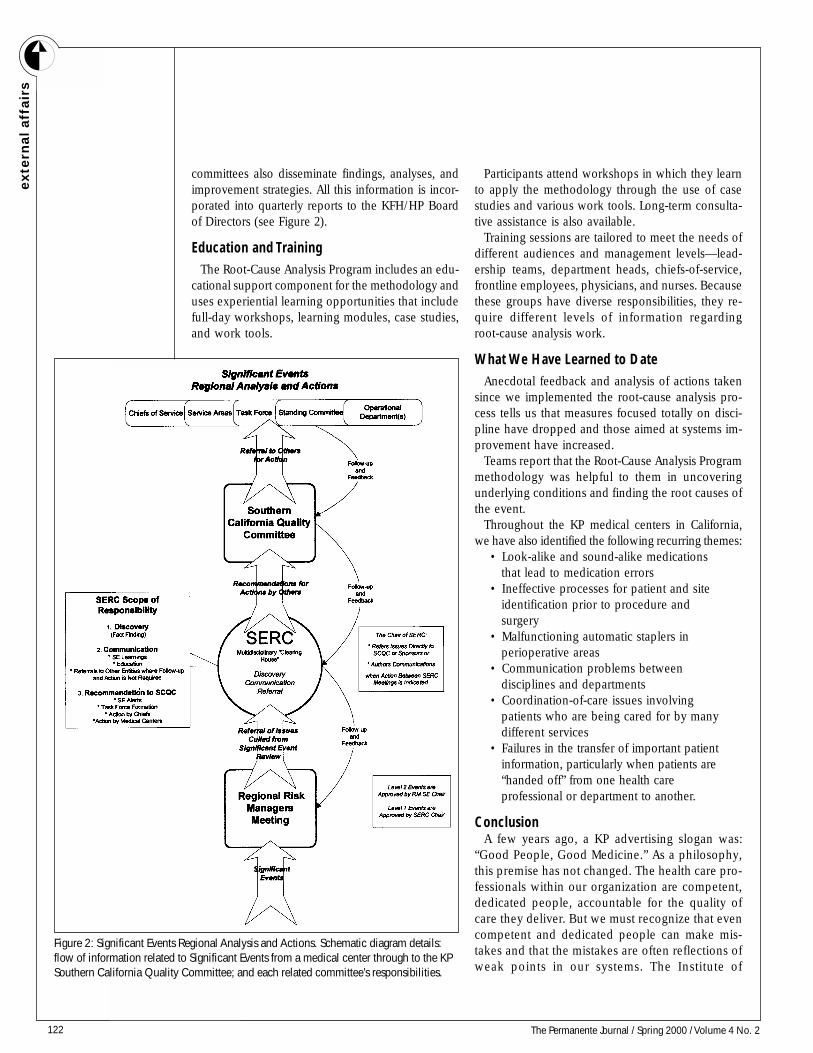
122 The Permanente Journal / Spring 2000 / Volume 4 No. 2
exte
rnal
aff
air
s
committees also disseminate findings, analyses, andimprovement strategies. All this information is incor-porated into quarterly reports to the KFH/HP Boardof Directors (see Figure 2).
Education and TrainingThe Root-Cause Analysis Program includes an edu-
cational support component for the methodology anduses experiential learning opportunities that includefull-day workshops, learning modules, case studies,and work tools.
Participants attend workshops in which they learnto apply the methodology through the use of casestudies and various work tools. Long-term consulta-tive assistance is also available.
Training sessions are tailored to meet the needs ofdifferent audiences and management levels—lead-ership teams, department heads, chiefs-of-service,frontline employees, physicians, and nurses. Becausethese groups have diverse responsibilities, they re-quire different levels of information regardingroot-cause analysis work.
What We Have Learned to DateAnecdotal feedback and analysis of actions taken
since we implemented the root-cause analysis pro-cess tells us that measures focused totally on disci-pline have dropped and those aimed at systems im-provement have increased.
Teams report that the Root-Cause Analysis Programmethodology was helpful to them in uncoveringunderlying conditions and finding the root causes ofthe event.
Throughout the KP medical centers in California,we have also identified the following recurring themes:
• Look-alike and sound-alike medicationsthat lead to medication errors
• Ineffective processes for patient and siteidentification prior to procedure andsurgery
• Malfunctioning automatic staplers inperioperative areas
• Communication problems betweendisciplines and departments
• Coordination-of-care issues involvingpatients who are being cared for by manydifferent services
• Failures in the transfer of important patientinformation, particularly when patients are“handed off” from one health careprofessional or department to another.
ConclusionA few years ago, a KP advertising slogan was:
“Good People, Good Medicine.” As a philosophy,this premise has not changed. The health care pro-fessionals within our organization are competent,dedicated people, accountable for the quality ofcare they deliver. But we must recognize that evencompetent and dedicated people can make mis-takes and that the mistakes are often reflections ofweak points in our systems. The Institute of
Figure 2: Significant Events Regional Analysis and Actions. Schematic diagram details:flow of information related to Significant Events from a medical center through to the KPSouthern California Quality Committee; and each related committee’s responsibilities.

123The Permanente Journal / Spring 2000 / Volume 4 No. 2
exte
rnal a
ffairsMedicine’s recent report “To Err is Human” states:
“Building safety into processes of care is a moreeffective way to reduce errors than blaming indi-viduals.”4:4 The report also emphasizes that the “fo-cus must shift from blaming individuals for pasterrors to a focus on preventing future errors bydesigning safety into the system.”4:5 In accordancewith JCAHO requirements, KP has established aroot-cause analysis process to better understandthe underlying causes of system errors and to re-duce the probability of recurrence. Although thisprocess has already proved valuable, if we are tomake significant improvement, we must move be-yond the entrenched blame and punishment cul-ture toward one of greater honesty and openness.Only in this way can we truly create a safer healthcare environment. ❖
References1. Sentinel Events. In: Joint Commission on Accreditation ofHealthcare Organizations Department of Publications.
Comprehensive Accreditation Manual for Hospitals 2000.Oakbrook Terrace, Illinois: JCAHO Department of Publications,2000, p. SE-1-SE-8.2. Tolbert LD. The risk management approach at KaiserPermanente Los Angeles Medical Center. Permanente J 1998Summer;2(3):69-72.3. Modified from Reason JT. Human error. Cambridge [England];New York: Cambridge University Press, 1990.4. Kohn LT, Corrigan JM, Donaldson MS, editors. Committee onQuality of Health Care. Institute of Medicine. To err is human:building a safer health system. Washington, DC: NationalAcademy Press; 2000.
Related ArticlesBlaming not point in sentinel event. OR Manager 1998Dec;14(12):11.Leape LL. A systems analysis approach to medical error. J EvalClin Pract 1997;3:213-22.Leape LL, Woods DD, Hatlie MJ, Kizer KW, Schroeder SA,Lundberg GD. Promoting patient safety by preventing medicalerror. JAMA 1998;280:1444-7.Reason J. The contribution of latent human failures to thebreakdown of complex systems. Philos Trans R Soc Lond B BiolSci 1990;327:475-84.Reason J. Understanding adverse events: human factors. QualHealth Care 1995 Jun;4(2):80-9.
What A Human Being IsThe last third of the 20th century has inserted, with blatantcynicism, quotation marks around most of our cherishednotions of social, political, historical, and psychological
existence. Indeed, the whole notion of what a human being isin the age of cloning, cyberspace, and public opinion polls has
undergone a radical transformation.Andrei Codrescu, “Messiah”
“Building safetyinto processes of
care is a moreeffective way to
reduce errors thanblaming
individuals.”

124 The Permanente Journal / Spring 2000 / Volume 4 No. 2
bo
ok r
evie
w
“The Back Pain Revolution” by GordonWaddell, Alf L. Nachemson (Introduc-tion), Reed B. Phillips (Introduction).Review by Gary Stein, MD
This book is a “must read” for all clinicians seeingpatients who have back pain. The Back Pain Revo-lution covers most of the pertinent areas of interestto the student of back pain: medical history andphysical examination, epidemiology, risk factors,natural history, the differences between physical im-pairment and disability, and psychological distress.The chapter discussing patient beliefs about backpain is an excellent summary of the many unspo-ken ideas patients bring with them to the examina-tion room and how these ideas vary enormouslyamong different cultures.
The Back Pain Revolution has changed treatmentmethods dramatically. We now encourage patientsto remain active and to resume usual activities assoon as possible. Narcotics are used much less fre-quently and usually only for severe and acute pain.We have learned the power of the medical historyand physical examination for making the diagnosis,and we appreciate the appropriate and more limitedrole of plain radiographs and advanced imaging tech-niques. We have a better understanding of pain asaffecting and being affected by the central nervoussystem with insight into the diverse influences pro-ducing and sustaining pain. Dr Waddell and othershave used the phrase “back pain as a biopsychosocialphenomenon” to summarize the diverse factors in-fluencing pain perception. Above all, our inclinationto cure by wielding a blade has been inhibited: Achance to cut is not necessarily a chance to cure.Indeed, the suffering that accompanies the patientwith back pain is best treated with sincere concernand wise counsel. The tricyclic and tetracyclic anti-depressant agents work well to improve sleep and
pain tolerance. The selective serotonin reuptake in-hibitors (SSRIs) and the newer antidepressants helppatients when depression is prominent.
The last third of this book contains the clinicalpractice guidelines developed for governmentalbodies in the United States, the United Kingdom,and New Zealand. These guidelines have served asmodels for the guidelines established by most Per-manente Medical Groups.
In addition, the book contains “Information forPatients” that can be reproduced and given to themto help them understand that back pain is both mus-culoskeletal and neurological. This may be of helpespecially to patients who insist on knowing the pre-cise anatomic location of the pain. These patientsfrequently request magnetic resonance imaging (MRI)to help find the pain even when MRI is not neededfor diagnostic or therapeutic purposes. A request ofthis sort is based on long-outdated thinking; we musthelp our patients and, when need be, our colleagues,to understand the newer concepts of back pain. Thiswell-written, easy-to-read, informative book does justthat. Our patients with back pain will get well withthe least possible pain and suffering if we appropri-ately obtain the medical history and conduct thephysical examination, rule out dreaded disease, rec-ognize those few conditions that surgery can pre-dictably improve, and explain the problem to thepatient in the way Dr Waddell explains it to us. Thisbook is an interesting and important contributionabout a very common problem. ❖
Churchill Livingstone, $60; Edinburgh, New York;1999: ISBN:
0443060398.
Gary Stein, MD
Dr Stein is an internist with The Permanente Medical Group in
San Jose, California, where he is head of the Spine Clinic.
Book Reviews

125The Permanente Journal / Spring 2000 / Volume 4 No. 2
bo
ok re
vie
w
“God Unmasked; the Full Life Revealed,”by Ernest Lane, MDReview by Albert Ray, MD
Dr Ernest Lane practiced medicine with the North-west Permanente Medical Group for 17 years. Afterspending his lifetime as a healer of humans, Dr Lanehas written God Unmasked; the Full Life Revealed, atreatise on the value of bridging the schism betweenscience and religion. Dr Lane offers a series of com-pelling and logical arguments concerning 1) the ex-istence of the spiritual self and 2) the importance ofrecognizing the bond between the physical, measur-able realm of science and the intangible, incalcu-lable world of the spirit. Skeptics as well as religiousbelievers with a somewhat questioning outlook willachieve reconciliation by reading this book, which,contrary to my expectations, actually embraces “open-ness to doubt” as the cornerstone of spiritual devel-opment. And for unwavering believers, reading thisbook presents an opportunity to more fully contem-plate—and thereby appreciate—the gift of faith.
As educated individuals, we are taught from an earlyage to be critical thinkers. The scientific and spiritualrealms grow apart and seem to be at odds. Dr Laneportrays an existence where these entities are broughttogether under a central canopy that results in a morefulfilling life. Through exploration of the psychologyof human behavior, the book asserts, a person canbecome aware of God’s presence in the world. Thisawareness results in a change in mental outlook forthe individual, who is rewarded with a more whole-some existence.
Dr Lane asserts that people must be committed tointegrity, defined by its open door to doubt; indeed,acceptance of uncertainty is what allows a person tofeel God’s presence. In this way, not only is Godunmasked but each of us comes to understand whatwe are really all about. Ultimately, this process al-lows us to comprehend what constitutes the essenceof a fuller life for ourselves and for all the world.
With great creativity and sensitivity, Dr Lane un-veils a compelling saga for those who seek a deeperunderstanding of human existence. A person mustlook beyond personal needs to find the key to deepercomprehension of the meaning of life and must learnthe fine balance between detachment and engage-ment in order to navigate existence successfully.
This book was not written in a vacuum. Dr Lane hasdrawn from the rugged circumstances of his own per-sonal history, combining it with more than 30 years ofexperience working in general medical practice. If youwant to be challenged, read this book. The famouswords, “God, reveal yourself; hide no more” do be-come a reality, and, within that reality, you will beable to experience greater understanding of self. ❖
High Ground Publishing, $24.95. Montpelier, VT; 1998; ISBN O-
9654915-2-8
Albert Ray, MD
Albert Ray, MD, is Assistant Chief in the Department of Family
Practice at Kaiser Permanente in San Diego and an elected Direc-
tor of the Southern California Permanente Medical Group.
Doctor’s PlantsNever go to a doctor whose office plants have died.
Erma Bombeck
126 The Permanente Journal /Spring 2000 / Volume 4 No. 2
an
no
un
cem
en
ts
❑ ❑ 00KPNC-P1A&B Keynote: The Future of Healthcare: Delivering Service& the KP Promise (2 Tape Set)
❑ ❑ 00KPNC-P2A&B Disease Management and The Care ManagementInstitute (2 Tape Set)
❑ 00KPNC-P3 Current Concepts in the Management of Diabetes
❑ 00KPNC-P4 Common Pediatric Infectious Diseases: Management of theFebrile Infant
❑ 00KPNC-P5 Managing Osteoarthritis: Making Your Patients and YourselfMore Comfortable
❑ ❑ 00KPNC-P6A&B The Patient, the Clinitian, and the Microbe: An Updatein Infectious Diseases (2 Tape Set)
❑ ❑ 00KPNC-P7A&B End of Life Care: Patient Concerns and ProviderChallenges (2 Tape Set)
❑ ❑ 00KPNC-P8A&B Integrative Care For Congestive Heart Failure(2 Tape Set)
❑ ❑ 00KPNC-P9A&B Improving Disability Management in Primary CarePractice (2 Tape Set)
❑ ❑ 00KPNC-P10A&B Depression in Primary Care (2 Tape Set)
❑ ❑ 00KPNC-P11A&B New Asthma Concepts (2 Tape Set)
❑ ❑ 00KPNC-P12A&B Pediatric Preventative Services (2 Tape Set)
BY PHONE: With your creditcard; please call Toll-Free:800-369-5718.Monday thru Friday:7:00 a.m. to 5:00 p.m. PST
BY MAIL: Please check tapesdesired, complete this form, andmail to Mobiltape at the addressbelow.
BY FAX: 24 hrs/day. PleaseFAX a copy of order form withcredit card info to:(661) 295-8474
ByWEB:www.mobiltape.com
❑ ❑ 00KPNC-W1A&B Keynote: The Future of Healthcare: Delivering Serviceand the KP Promise (2 Tape Set)
❑ ❑ 00KPNC-W2A&B What Women Want in Health Care (2 Tape Set)
❑ ❑ 00KPNC-W3A&B Providing Evidence-Based, Cost-Effective ClinicalPreventive Services For Adult Women (2 Tape Set)
❑ 00KPNC-W4 Abnormal Vaginal Bleeding: From Menarche toMenopause
❑ ❑ 00KPNC-W5A&B Menopause and Libido; The Psychological Aspects ofPMS and Menopause (2 Tape Set)
❑ ❑ 00KPNC-W6A&B Update on Osteoporosis: Diagnosis, Prevention andTreatment Alternatives to Standard HRT: Low Dosage Estrogen, SERMs andPhytoestrogens (2 Tape Set)
❑ ❑ 00KPNC-W7A&B Gender Specific Aspects of Health Promotion(2 Tape Set)
❑ ❑ 00KPNC-W8A&B Common Gyn Disorders Plus STDs (2 Tape Set)
❑ ❑ 00KPNC-W9A&B Gender Specific Medicine: Cardiovascular Disease andWomen’s Health (2 Tape Set)
❑ 00KPNC-W10 Reproductive Health and Family Planning
❑ ❑ 00KPNC-W11A&B Sociological Aspects of Women’s Health(2 Tape Set)
❑ ❑ 00KPNC-W12A&B Women’s Work and Health: Interactions andApproaches (2 Tape Set)
SESSION A: Practical Primary Care Skills SESSION B: Women's Health
DOMESTIC SHIPPING CHARGES
Audio:$2.00 per audio tape; $8.00 max
Syllabus:$5.00 per syllabus
PLEASE ALLOW 3 WEEKS FOR SHIPPING.
• PRICES AND DISCOUNTS •
❏ Entire A or B Session Set Special: All audiotapes listed in A or B Session Track, in albums for only $115.00
❏ Any 12 audiotapes for the price of 10, including storage album only $80.00
❏ Any 6 audiotapes for the price of 5, only $40.00
❏ Matching syllabus for A or B Sessions, only $18.00
Individual audiotapes are $8.00 each
National Primary Care ConferenceAUDIO TAPE ORDER FORMApril 23-28, 2000Kauai Marriott Resort and Beach Club
ORDERING INFORMATION
Mobiltape Co. Inc., • 24730 Avenue Tibbitts, Suite 170, Valencia, CA 91355 • (661) 295-0504
Name_______________________________________
Company____________________________________
Address_____________________________________
City, State,Zip________________________________
Telephone___________________________________
Amount for Audio Tapes / Handouts
Calif. orders 8.25% sales tax
Domestic Shipping: See Charges To Left
Total of Order
Payment methodMake checks payable to MOBILTAPE COMPANY, INC.U.S. Currency only❏ Cash ❏ Check ❏ Charge Card Number Exp. Date___
VISAMasterCardAMERICAN
EXPRESS
Entire Set SpecialsSession A: $115.00Session B: $115.00
Free sample videotape and bookleton Hereditary Hemochromatosis!
Easy-to-understand format is an excellent way to educateyour patients and staff about this common genetic disorder.Significant discount for large orders. Please contactNaomi Howard with your request at [email protected].
Announcements

127The Permanente Journal / Spring 2000 / Volume 4 No. 2
an
no
un
cem
en
ts
San Diego Physician Chairs California’s Young Physician GroupSan Diego, CA, April 22, 2000—Jeffrey Krebs, MD, FACP, an Internal Medicine specialist with Kaiser
Permanente, was recently elected chair of the Young Physician Section of the California Medical Association(CMA). Young physicians are those who are under age 40 years or in their first five years of medical practice.
“My role as chair is to oversee the entire Young Physician Section, to plan seminars of interest to youngphysicians in the state, to chair the Executive Committee, and respond to media questions or comment onissues affecting young physicians,” says Dr Krebs.
Young physicians are concerned about legislative issues such as malpractice premiums, according to DrKrebs, as well as getting credentialed for hospital staffs and HMOs, financial planning, and more.
Dr Krebs was elected to his new role at the annual Assembly for Young Physicians (March 10, 2000), whichis held in conjunction with the CMA House of Delegates meeting.
“This year I will be planning two professional development meetings for young physicians—one inNorthern California and one in Southern California,” says Dr Krebs. “I will have representatives from theAmerican Medical Association, CMA, and other organizations give presentations on how to interface withthe media. This is an increasingly important role for physicians as we try to communicate our positionsand strategic messages on a variety of medical and political issues.”
Other planned activities include increasing membership in the CMA Young Physician section and conduct-ing seminars on financial planning, legal issues, and time management.
Dr Krebs is actively involved in the San Diego County Medical Society (SDCMS). He is the past chair ofYoung Physician Section, the current Vice-chair of the Professional Conduct Committee, the Co-Chair of theMembership Committee, and is serving his third year on the Council of the SDCMS.
Dr Krebs has been with Kaiser Permanente since 1989, and his practice is at Kaiser Permanente’s La MesaMedical Offices. ❖
In MemoriamNaomi Elizabeth Torrez
1939 – 2000
In 1979, Naomi Elizabeth Torrez joined the Northern California Kaiser Permanente family as alibrarian as the KP Vallejo Medical Librarian. The daughter of a pastor and professor of Classical Greekand Latin, Mrs. Torrez followed in his footsteps of community involvement and scholarship. In 1953,she earned a Championship at the US National Spelling Bee. She was a graduate of the University ofArizona, the University of California, Berkeley, and Golden State School of Theology. At Kaiser Per-manente, Mrs. Torrez was a member of numerous committees, including the Latino Association,Affirmative Action, Health Education, and the Librarians group. In 1988, Golden State School ofTheology published a “Research Manual” by Mrs. Torrez, in which she stated, in the Introduction:
“… never be afraid of information … Almost daily, claims are made about newmanuscripts, new fossils, or new revelations, but Christians do not need to be concernedabout such claims. True knowledge is always in harmony with true religion.”
Mrs. Torrez was an extended member of The Permanente Journal team, working on bibliographicdetails as Copyright Review Editor in the Medical Editing Department. We will all miss her scholarshipand expertise.
Mrs. Torrez is survived by her husband, Reverend Lupe Torrez, and her children, Sterling, Linda, and Stan.
128 The Permanente Journal / Spring 2000 / Volume 4 No. 2
Send all manuscripts to:Merry Parker, Managing EditorThe Permanente Journal500 NE Multnomah St, Suite 100Portland, OR 97232(503) 813-2659
Editorial PoliciesManuscripts are received with the understanding that they have
not been published or submitted for publication in whole or inpart elsewhere, except for a scientific abstract, unless otherwisespecified. Manuscripts will be reviewed by the Editor, AssociateEditors, members of the Review Board, and appropriate special-ists internally and externally as deemed necessary. Acceptance ofa paper for publication is based on the relevance, quality of workdescribed, clarity of the presentation, and especially applicabilityto daily clinical practice. If the article is accepted for publication,editorial revision may be made to aid clarity and understandingwithout altering the meaning (see Proofreading). Authors are re-minded that they assume full responsibility for final wording andform of all materials submitted for publication. The contact au-thor will be required to complete coauthor and acknowledgmentconsent forms before publication.
Articles, editorials, letters to the editor, and other text materialin the Journal represent the opinion of the authors and do notnecessarily reflect the opinion of Kaiser Permanente.
Authors submitting a manuscript do so with the understandingthat if it is accepted for publication, copyright of the article, in-cluding the right to reproduce the article in all forms and media,shall be assigned exclusively to the publisher. The publisher willgrant any reasonable request by the author for permission toreproduce any part of his/her contribution to the Journal.
Types of PapersThere is no required length, although concise, readable, and
practical articles within the ranges listed are preferred. Empha-size information that clinicians can use in their practice, that givesthem regional and national perspective, and that integrates “Per-manente Medicine” into the largest scope of health care delivery.
Notes About Specific Sections• Clinical Contributions
Clinical articles on the practice of medicine within ThePermanente Medical Groups and their affiliates. Articletopics may include reviews of “successful” practices, pro-grams and policies, and analyses of new technologies.
(word count range is 725-5000)• Original Research
Articles on Kaiser Permanente’s research contributionsthrough original, empirically-based research in areas of greatclinical importance. This includes outcomes research, stud-ies that use Kaiser Permanente databases, and rigorousevaluations of best practices and innovations in clinical care.
(word count range is 725-5000)• Health Systems
Articles from a “systems” perspective, recognizing that medi-cine is practiced in the larger context of health care, includingambulatory care delivery, hospital strategy, program expan-sion, and network development and is supported byinformation technology and the Internet. Growth in this sys-tem occurs through the leadership, education, anddevelopment of clinicians.
(word count range is 725-3000)
• External AffairsNonclinical articles on external issues related to the prac-
tice and perception of Permanente Medicine. These mayinclude articles by customers and consumer groups, as wellas internally generated articles on health policy, the media,the marketplace, and our social mission.
(word count range is 725-3000)• Medical Legal Update
Articles educating clinicians about medical-legal issues, in-cluding risk management, claims review, loss prevention,and ethical issues. Improved clinician communication withpatients, families, and the health care team is the goal.
(word count range is 725-1400)• Soul of the Healer
Poetry, stories, musings, and nonfiction articles written byPermanente clinicians as an expression of the soul of thehealer. This is a forum to appreciate each other personallythrough creativity in the humanities.
(word count range is 725-2200)• A Moment in Time
A look back at milestones in the history of the PermanenteMedical Groups.
(word count range is 700-740)• Abstracts
Abstracts from articles published in other journals, prefer-entially featuring the work of Permanente physicians.
• AnnouncementsSignificant achievements related to the practice or man-
agement of medicine by Permanente physicians orPermanente Medical Groups. Also posted will be upcomingcourses, meetings, and conferences sponsored by the Per-manente Medical Groups or Kaiser Permanente.
• The Lighter Side of Permanente MedicineJokes, stories, and humorous encounters tied to the practice
of Permanente medicine, managed care, or health care in gen-eral.
Cover LetterIn a cover letter, please give a concise statement of the authors’
view of the importance and uniqueness of the article. Also provideseveral names and addresses of non-Kaiser Permanente experts whocould provide informed, objective reviews of the work. The namesof any persons considered unlikely by the authors to supplynonbiased reviews may also be submitted; this request will be hon-ored. It is important that the cover letter also include the names,addresses, phone numbers, and fax numbers of all coauthors.
Manuscript Preparation and ProcessingA 3-1/2” disk containing the article and one complete paper
copy of the manuscript must be submitted, along with a photo-graph of the author(s) labeled with name and a 2-3 sentenceauthor profile. (Please, no photos smaller than 2”×3” or largerthan 5”×7”.) If more than four authors, submit the authors’ pro-files only—no photographs.
Manuscripts must be typewritten in a word-processing program(identify program and platform used), double-spaced, with mar-gins of at least 1 inch. All parts of the manuscript must be includedin a single file on the disk, and the disk file must match the print-out. Tables and illustrations are also to be included in separateelectronic files. The 3-1/2” disk must be labeled with the first author’sname, an abbreviated article title, the file name(s), the disk format(eg, Mac), and the software used (eg, Microsoft Word 6.0, MicrosoftPowerPoint, Microsoft Excel).
Instructions to Authors?
inst
ruct
ion
s fo
r au
tho
rs
129The Permanente Journal / Spring 2000 / Volume 4 No. 2
Checklist for Authors___ 3.5” disk labeled with author name, article title, file
name(s), word count, disk format, and word-processingsoftware used
___ Cover letter
___ One copy of manuscript
___ Title page___ Author profile (2-3 sentences)
___ Author photo (no smaller than 2”×3”, no larger
than 5”×7”)
___ Structured Abstract (limit: 250 words): include key words
___ References (double-spaced on a separate sheet)
___ Illustrations, properly labeled (one original set, electronicand hard copy)
___ Figure legends (double-spaced)
___ Tables (provide a brief title)
___ Permission to reproduce previously published material;
photographic consent
___ IRB Documentation
?The first page of the manuscript should contain the following
information: 1) title of paper; 2) authors’ names; 3) name(s) ofKaiser Permanente Division and medical office in which workwas done; 4) name and address of author to whom communica-tions regarding the manuscript should be directed; 5) telephoneand fax number of the communicating author; 6) word count.
The second page of an Article (Clinical or Nonclinical) shouldcontain an Abstract (limit: 250 words). The abstract for NonclinicalArticles should use these headings: Context, Objective, Design,Main Outcome Measure(s), Results, and Conclusion(s). Also listkey words and terms, in alphabetical order, under which you be-lieve the article should be indexed.
Begin the text on a new page. Define all abbreviations exceptthose that have been approved by the International System of Unitsfor length, mass, time, electric current, temperature, luminous in-tensity, and amount of substance. Provide a footnote or box at thebeginning of the article to define abbreviations when great num-bers of abbreviations are used. Do not create abbreviations for drugs,procedures, or substrates. Use generic drug names. If a brand nameis used, insert it in parentheses after the generic name.
Institutional Review Board (IRB) ReviewDocumentation of IRB approval or exemption must be appended
to the manuscript being submitted for publication in The Perman-ente Journal. If there has been no IRB review of the project, pleaseso indicate. In this case, the article will be reviewed by KaiserFoundation Research Institute to determine if IRB review shouldhave been conducted. The result of this review may determinewhether or not the article will be considered for publication.
Preparing Illustrations and TablesIllustrations and tables are desirable and highly encouraged be-
cause they expand the value of the article. Tables and illustrationsmust be cited in order in the text using Arabic numerals. Submitone complete set as glossy prints or high-quality laser prints, andinclude electronic files on disk for each illustration and/or table.Do not staple, clip, or write heavily on the back. Paste a label onthe back of each illustration indicating its number in order of ap-pearance, author’s name, and the top edge of the picture.
Legends for illustrations should be typewritten, double-spaced,on a separate sheet, and included at the end of the manuscript. Alegend must accompany each illustration.
Figures, especially charts, graphs, and line drawings, are gener-ally reduced in size for publication. To maintain legibility, allnumbers, letters, and symbols should be large enough originallyso that when reduced they will remain at least 2 mm high.
Each table should be typed on a separate sheet and appropri-ately numbered. Abbreviations used in the table should be definedin the legend to the table; legends should be typed on the samesheets as the tables.
Any figure, table, or long portions of text that have been previ-ously published must be accompanied by a letter of permission toreprint, signed by the publisher, at the time of submittal. It is theresponsibility of the author to obtain such permission.
Legal and Ethical ConsiderationsAvoid use of patients’ names, initials, and medical record num-
bers. A patient must not be recognizable in photographs or casedescriptions unless written consent of the subject has been obtained.
ReferencesReferences must be numbered with Arabic numerals and cited in
the text in numeric order. The reference list at the end of the article
must also be in numeric order (do not list references in alphabeticalorder). The list should be double-spaced under the heading REFER-ENCES. Abbreviations for title of medical periodicals should conformto those used in the latest edition of Index Medicus.
Examples.Journal article, one to six authors1. Beutler E. The effect of methemoglobin formation on sickle
cell disease. J Clin Invest 1961;40:1856-1858.2. Karpatkin S, Charmatz A. Heterogeneity of human platelets.
III. Glycogen metabolism in platelets of different sizes. Br JHaematol 1970;19:135-143.
Journal article, more than six authors3. Golomb HM, Vardiman J, Sweet DL Jr, et al. Hairy cell leuke-
mia: Evidence for the existence of a spectrum of functionalcharacteristics. Br J Haematol 1978;38:161-2.
Journal article in press4. O’Malley JE, Eisenberg L. The hyperkinetic syndrome. Semin
Psychiatry (in press)(Note: A copy of the manuscript must be included.)
Complete book5. Lillie RD. Histopathologic Technique and Practical Histochem-
istry (ed 3). New York, NY: McGraw Hill: 1965.Chapter of book6. Moore G, Minowada J. Human hemopoietic cell lines: A
progress report. In: Farnes P. Hemic Cells in Vitro, vol. 4.Baltimore, MD: Williams & Wilkins; 1969. 100-105.
Editing AssistanceYou can obtain help with preparing your manuscript from the
Medical Editing Department, which is a resource available to manyresearchers throughout the Program. The department’s professionaleditors can help you organize your paper, edit your text, and verifyreferences before publication in The Permanente Journal. CallMedical Editing at 510-987-3573 for further information.
ProofreadingContributors are provided with galley proofs and are asked to
proofread them for typesetting errors. Important changes in dataare allowed, but authors are requested to not make excessive al-terations. Galley proofs should be returned within 48 hours.
instru
ction
s for a
uth
ors
130 The Permanente Journal / Spring 2000 / Volume 4 No. 2
?in
stru
ctio
ns
for
au
tho
rs
Copyright TransferThe Permanente Journal (TPJ) is owned, published, and copyrighted by The Permanente Federation. In the event that TPJ publishes
my work and in consideration of the editing and publication of my work, I transfer to TPJ all rights, title, and interest to all parts of thewritten work named below. TPJ shall own the work, including 1) copyright; 2) the right to grant permission to republish the article inwhole or in part; 3) the right to produce reprints for distribution; and 4) the right to republish the work in a collection of articles in anyother mechanical or electronic format. In addition, I affirm that the work has not been previously published, is not subject to copyrightor other rights except my own to be transferred to TPJ, and has not otherwise been submitted for publication, except under circum-stances communicated to TPJ in writing at the time the work was submitted. (All authors must sign below. Photocopy form if necessary.)
Manuscript Title ____________________________________________________________________________________________________________________________
__________________________________________________________________________________________________________________________________________
__________________________________ __________________________________ ________________________________Principal Author Signature & Date Coauthor Signature & Date Coauthor Signature & Date
__________________________________ __________________________________ ________________________________Print Name Print Name Print Name__________________________________ __________________________________ ________________________________Address Address Address
Coauthor Agreement• I certify that the author(s) listed below is/are coauthor(s) of the above manuscript.
Principal author signature: _______________________________________ Print Name: ________________________________________________
Address: _______________________________________ Phone : ________________________________________________
• I agree to be named as a coauthor of the above manuscript.• I have reviewed the final version of the above manuscript and approve it for publication.• To the best of my knowledge and belief, the above manuscript has not been published and is not being considered for publication
except as described in an attachment hereto.• Except as described in an attachment hereto, to the best of my knowledge and belief, all intellectual contributions, technical help,
financial or material support, and financial or other relationships that may constitute or lead to a conflict of interest, have beenacknowledged or disclosed in the manuscript.
__________________________________ __________________________________ ________________________________Coauthor Signature & Date Coauthor Signature & Date Coauthor Signature & Date__________________________________ __________________________________ ________________________________Print Name Print Name Print Name__________________________________ __________________________________ ________________________________Address Address Address
Consent to Acknowledgment• I agree that I have made a substantive contribution to the above manuscript.• I have reviewed and approved the language in the manuscript acknowledging my contribution.• I consent to the acknowledgment in the manuscript and understand that readers may infer my endorsement of the data or
conclusions reported in the manuscript.
__________________________________ __________________________________ ________________________________Acknowledgee Signature & Date Acknowledgee Signature & Date Acknowledgee Signature & Date__________________________________ __________________________________ ________________________________Print Name Print Name Print Name__________________________________ __________________________________ ________________________________Address Address Address
The Permanente Journal Author’s Form
131The Permanente Journal / Spring 2000 / Volume 4 No. 2
CME Evaluation Form
All PMG physicians and those clinicians eligible to do so may earn up to two hours of Category 1 credit forreading and analyzing the four designated CME articles, by selecting the most appropriate answer to the questionsbelow, and by successfully completing the evaluation form. This form must be returned (fax or mail to the addresslisted on the back of this form) to The Permanente Journal by July 31, 2000 in order to receive credit. You will receivean acknowledgment by August 31, 2000. You must complete all sections to receive credit.
The Kaiser Permanente National Continuing Medical Education Program (KPNCMEP) is accredited by the Accredita-tion Council for Continuing Medical Education to provide continuing medical education for physicians. The KPNCMEPtakes responsibility for the content, quality, and scientific integrity of this CME activity. The KPNCMEP designates thiseducational activity for up to two hours of Category 1 CME credit for each TPJ issue applicable to the AMA PhysicianRecognition award and/or state award. Each physician should claim credit for only those hours that were actually spent inthis educational activity. Author disclaimer forms are on file with no conflicts listed or necessary disclaimers.
Section A.Article 1. Bright Systems®: A Total Quality Management Project to Improve Children’s Health (page 24)
Bright Systems® demonstrated improvements in::a. Physician injury prevention counselingb. Physician tobacco counselingc. Parent safety behaviorsd. Parent tobacco usee. A, B, and Cf. All of the above
Adaptation of the office system through combined use of parent safety behavior data and physician consensus hadwhat outcomes?
a. It improved acceptance of the office system by physicians and nonphysician staff, which facilitated programdissemination
b. Physicians learned more about health supervision and quality improvement by participating in the adaptation of theoffice system
c. The system had a greater effect at improving parent safety behaviorsd. The office system tools were continuously improved, and new tools were developede. All of the above
Article 2. Emergency Contraception Research and Demonstration Project (page 57)
Which of the following progestogens has not been shown to be effective as emergency contraception (EC)?a. Levonorgestrelb. Norgestrelc. Norethindrone
Two high doses of estrogen/progestogen oral contraceptives given within 72 hours of intercourse are highly effectivein preventing pregnancy. Which of the following statements describes the effectiveness of ECP numerically?
a. 100 women who have unprotected intercourse would become pregnant without EC; none of them would becomepregnant with it
b. 100 women who have unprotected intercourse would become pregnant without EC, two of them would becomepregnant with it
c. Of 100 women who have unprotected intercourse, 8 would become pregnant without EC; 2 would becomepregnant with it
Article 3. Asthma Disease Management Program (page 48)
Nationally, what is the percentage of patients with known heart disease who have LDL cholesterol levels < 100 mg/dL?a. 10-15%b. 20-25%c. 40-45%d. 60-65%
con
tinu
ing
med
ical e
du
catio
n
132 The Permanente Journal / Spring 2000 / Volume 4 No. 2
Section D. (Please print)
Name: E-mail Address:
Address:
Signature: Date:
The Permanente Journal500 NE Multnomah Street, Suite 100, Portland, OR 97232
Phone: (503) 813-2623 Fax: (503) 813-2348
Section C.What change(s) (if any) do you plan to make in your practice as a result of reading these articles?
Section B. Referring to the CME articles and the stated objectives, please check the box next to each statement as appropriate
Article 1 Article 2 Article 3 Article 4
The article covered the stated objectives
I learned something new that was important
I plan to use this information as appropriate
I plan to seek more information on this topic
I understood what the author was trying to say
Strongly
Agree
Strongly
Disagree
5 4 3 2 1
Strongly
Agree
Strongly
Disagree
5 4 3 2 1
Strongly
Agree
Strongly
Disagree
5 4 3 2 1
Strongly
Agree
Strongly
Disagree
5 4 3 2 1
Physician reminders at the moment of carea. Improve cholesterol screening in coronary artery disease patientsb. Improve cholesterol control in coronary artery disease patientsc. Improve prescribing of aspirin in CAD patientsd. All of the above
Article 4. Achieving Positive Outcomes through Collaborative Pharmaceutical Care: The KPNW MedicationManagement Program (page 37)
Which of the following is not an objective of the KPNW Medication Management Program?a. Provide evidence-based care and improve health care outcomes of populationsb. Improve support to those medical offices which have clinical pharmacy resourcesc. Focus clinical pharmacy resources to support KPNW Regional Clinical and Pharmacy Department prioritiesd. Improve consistency and reduce service variation in providing clinical pharmacy care
The KPNW Medication Management Program (MMP) has achieved all but the following:a. Positioned KPNW as the Programwide leader in LDL managementb. Clinician survey results that describe MMP as providing high-quality care and an important part of the local health
care teamc. Decreased the number of patients cared for by existing personneld. Patient satisfaction results that define members as extremely or very satisfied with the care provided by MMP
con
tin
uin
g m
ed
ical
ed
uca
tio
n

Advisory Board
Review BoardColorado Permanente Medical Group, PC (CPMG): Paul Barrett Jr, MD; Pat Connor, PA; Wayne DuBois, PA; Richard Erickson, MD; Spencer Erman, MD; Timothy Garling, PA; Mark
Groshek, MD; Bob Lederer, MD; David Price, MD; Richard Spurlock, MD; Andrew Wiesenthal, MDHawaii Permanente Medical Group, Inc. (HPMG): Dorothy Chu, MD; Robert Decker, MD; Randy Jensen, MSN; John Payne Jr, MD; Raymond Tam, MDMid-Atlantic Permanente Medical Group, PC (MAPMG): Barbara Boardman, MD; Nooshin Farr, MD, FACP; Kirk Huang, MD; John Hurley, MD; Ann Komelasky, NP; Robert Kritzler,
MD; Jonathan Rosenthal, MD; Surender Vaswani, MD, FACP; Bradley Winston, MDNorthwest Permanente, PC, Physicians and Surgeons (NWP): Mike Barrett, MD; Jan Bellis-Squires; Ben Brown, MD; Homer Chin, MD; Colleen Chun, MD; Maurice Comeau, MD;
John Gale, MD; Stephen Gancher, MD; Jim Gersbach; Vern Harpole, MD; A. Hayward, MD; Carolyn Hokanson, MD; Roderick Hooker, PA; Peter Jacky, PhD, FACMG; Kathleen Kennedy,MD; Mike Kositch, MD; John Lasater, MD; Reed Paulson, MD; Jacob Reiss, MD; Eric Schuman, PA; David Scott, MD; Michael Stine, MS, LPC; Paul Wallace, MD; Don Wissusik, MA, MS, LPC
Ohio Permanente Medical Group, Inc. (OPMG): Joseph Armao, MD; Nuzhat Ashai, MD; Ronald Copeland, MD; Charles Duncan, MD; Aiyappan Menon, MD; Roland Philip, MD;Christopher Spevak, MD
The Permanente Medical Group, Inc. (TPMG): David Baer, MD; Kenneth Berniker, MD; Gilbert Carroll, MD; Andrew Chan, MD; Calvin Chao, MD; Francis Chui, MD FACP; CharlesClemons, MD; Linda Copeland, MD; David Cornish, MD; Sakti Das, MD; Anne Delaney, MD; Ward Flad, MD; Robin Fross, MD; Jay Gehrig, MD; Lisa Hake, MD; Helen Hammer, MD; PatHardy, MD; Aquia Heath, MD; Kathleen Hering, RNC, FNP/GNP; Raymond Hilsinger Jr, MD; Robert Hosang, MD; Thomas Kidwell, MD; Susan Kutner, MD; Irene Landaw, MD; RichardLeahy, MD, JD, FCLM; John Loftus, MD; Joseph Mason, MD; Barry Jay Miller, MD; Dana Miller-Blair, MD; Jerome Minkoff, MD; Conrad Pappas, MD PhD; Barbi Phelps-Sanda, MD; MaryPiper, NP; S. Ramachandra, MD; Jack Rozance, MD; James Ruben, MD; Edgar Schoen, MD; William Sheridan, MD; Stanford Shoor, MD; Lee Shratter, MD; Shelley Spiro, NP; Gary Stein,MD; John Stienstra, DPM; KM Tan, MD; B. Rao Tripuraneni, MD; David Williams, MD
Permanente Medical Group of Mid-America, PA (PMGofMA): Ellen Averett, PhD; Steven Hull, MDThe Southeast Permanente Medical Group, Inc. (TSPMG): Jeffrey Hoffman, MD; Adrienne Mims, MD; Fred Reifsteck, MDSouthern California Permanente Medical Group (SCPMG): Donna Beard, NP; Allen Bredt, MD; Dale Daniel, MD; James Delaney, PA; Richard Drucker, MD; Raed Fahmy, MD; F.
Ronald Feinstein, DMD; Vincent Felitti, MD; Woldemariam Gebreselassie, MD; Todd Goldenberg, MD; Jimmy Hara, MD; Joel Hyatt, MD; A. Robert Kagan, MD; Michael Kanter, MD;Charles Koo, MD; Barbara Kotlik, NP; Sok Lee, MD; Jenifer Lipman, NP; George Longstreth, MD; Bryan Maltby, MD; S. Michael Marcy, MD; Gholam Pezeshkpour, MD; Ronald Rosengart,MD; Robert Schechter, MD; Jerry Schilz, MD; Patricia Schmidt, MD; Michael Schwartz, MD; Ira Jeffry Strumpf, MD; Reva Winkler, MD; Frederick Ziel, MD
Kaiser Foundation Health Plan (KFHP), Program Offices: Ann Evans, MS; Patricia Lynch; Julia Shepard; Nancy VaughanGuest Reviewers (Group Health): Tim Gilmore, MD; Deborah Hammond, MD; Frank Marre, DO, MS; Steven Shaffer, MD; Jeff Shornick, MD; Lester Sloan, PA
Administrative Team
EditorsTom Janisse, MD
Editor-In-Chief & PublisherMary Durham, PhDResearch & Abstracts
Vincent J. Felitti, MDBook Reviews
Lee Jacobs, MDHealth Systems
Arthur Klatsky, MDClinical ContributionsScott Rasgon, MD
External Affairs & Medical LegalJon Stewart
CommunicationsKM Tan, MD
Continuing Medical Education
ProductionMerry Parker
Production EditorJim Cook
Print & Web DesignerAmy Eakin
Operations CoordinatorMax McMillen
Editorial Assistant
The Permanente Journal
Linda Fahey, NP; Regional Coordinator of Advanced Practice ........................................................................ SCPMGCarol Havens, MD; Director, Department of Continuing Medical Education .................................................... TPMGArthur Hayward, MD; Internist and Geriatrician, Continuing Care Services ....................................................... NWPTom Janisse, MD; Chairperson, Assistant Regional Medical Director, Health Plan Liaison ................................ NWPIrene Landaw, MD; Staff Pediatrician ................................................................................................................... TPMGChristopher Lang, MD; Clinical Cardiologist ....................................................................................................... CPMGSally Ling, MD; Internist; Member, Board of Directors ................................................................................. PMGofMALaura Marshall; Public Affairs and Communications, Program Offices ............................................................... KFHPMichael Mustille, MD; Director of Employer Relations ........................................................................................... TPFRobert McDuffie, MD; Chief, Perinatology .......................................................................................................... CPMGRichard Popiel, MD, MBA; Vice President and Senior Medical Director ........................................................ PermCoBruce Sabin, MD; Internist, Health Care Team Leader ..................................................................................... TSPMGBarbara Scherokman, MD; Assistant Chief of Neurology ................................................................................ MAPMGEric Schuman, PA; Family Practice Clinician, Northwest Division ...................................................................... KFHPJoe Selby, MD, MPH; Assistant Director for Health Services Research, California Division .............................. KFHPDavid Waters, MD; Department of Ophthalmology ............................................................................................HPMGWinkler Weinberg, MD; Section Chief of Infectious Disease Services ............................................................. TSPMGLes Zendle, MD; Associate Medical Director, Clinical Services ........................................................................ SCPMG
* KFHP - Kaiser Foundation Health Plan; TPMG - The Permanente Medical Group, Inc.; NWP - Northwest Permanente, Physicians andSurgeons; CPMG - Colorado Permanente Medical Group, PC; PMGofMA - Permanente Medical Group of Mid-America, PA; TPF - ThePermanente Federation; PermCo - The Permanente Company; OPMG - Ohio Permanente Medical Group, Inc.; TSPMG - TheSoutheast Permanente Medical Group, Inc.; MAPMG - Mid-Atlantic Permanente Medical Group; HPMG - Hawaii Permanente MedicalGroup, Inc.; SCPMG - Southern California Permanente Medical Group
tab
le o
f co
nte
nts
Spring 2000/Volume 4. No. 2
If you would liketo submit art for
consideration for the
cover ofThe Permanente Journal,please use the following
guidelines…
Send us a high-qualitycolor photograph of your
art no smaller than 4”Χ5”and no larger than
8”Χ10”. Portraitorientation is preferred.
Editor’s Comments3 Healing Physicians: Physicians Healing. Tom Janisse, MD
Permanente Abstracts9 Evaluating Hypertension Control in a Managed Care Setting ◆ Diabetes Management in a Health
Maintenance Organization. Efficacy of Care Management Using Cluster Visits ◆ Lack of Correlation ofSymptoms with Specialist-Assessed, Long-Term Asthma Severity ◆ Effect of a Pediatric Self-CareBook on Utilization of Services in a Group-Model HMO ◆ Exploring Indicators of TelephoneNursing Quality ◆ HMO Physicians’ Use of Referrals ◆ Cost of Care for Patients in Cancer ClinicalTrials ◆ Spousal Concordance for Cancer Incidence: a Cohort Study ◆ Changing Paternity and theRisk of Preeclampsia/Eclampsia in the Subsequent Pregnancy ◆ Second-Trimester Serum ChorionicGonadotropin Concentrations and Complications and Outcome of Pregnancy ◆ Effect of Age onReasons for Initiation and Discontinuation of Hormone Replacement Therapy ◆ PsychosocialTreatments for Adolescent Depression ◆ Cigarette Smoking, Alcohol Consumption, and Risk ofARDS: a 15-Year Cohort Study in a Managed Care Setting ◆ Warfarin Use among AmbulatoryPatients with Nonvalvular Atrial Fibrillation: the Anticoagulation and Risk Factors in Atrial Fibrillation(ATRIA) Study
Clinical Contributions15 The James A. Vohs Award for Quality.
17 Bright Systems® Sheds Light and Lightens the Load at Pediatric Health Supervision Visits.Diane Fraser
This article complements the outline by Dr Gee et al of the 2000 Vohs award-winning project. It describesthe actual workings of the system and personalizes some of the details with anecdotal examples. There isdiscussion of the underlying personal motivations for development of the system and historical aspects. Thespecific tools used are described, and examples of the project in action are given.
24 Bright Systems®: A Total Quality Management Project to Improve Children’s Health.Northern California Region
This project targets the preventive health needs of almost 50% of Health Plan members, when children andtheir families are included. This article outlines the project in detail. The system emphasizes comprehensive-ness and anticipation of needed counseling. Injury prevention and healthy behaviors are among the majorfoci of the effort. Results showed substantial improvements in quality of care as well as high patient andphysician satisfaction. Potential cost savings are also discussed.
32 The Childhood/Adolescent Immunization Program. Colorado Region
This program assesses immunization status at every visit, operates tracking and audit systems, improvesavailability of protocols, and provides education to patients and staff. An “Immunization Tool Kit” is akey feature. Outcome data show that this low-cost program has been highly successful in achieving itsgoals. It achieved a first-place award from The American Association of Health Plans for “InnovativeQuality Improvement.”
37 Achieving Positive Outcomes through Collaborative Pharmaceutical Care:The KPNW Medication Management Program. Northwest Region
Emphasizing lipid management and diabetic glucose control, this centralized program integrates manage-ment into the care delivery system. Tools include development of a list of those at risk, streamlining testordering, group appointments, educational efforts, and nurse care management. Measured results includeimproved percentages of coronary disease patients with LDL cholesterol levels below 130 mg/dL, andimproved glycemic control in diabetics. Substantial reductions in acute myocardial infarction rates andcoronary disease mortality are predicted.
On the Cover“Half Dome from the
Yosemite Falls Trail,” byJ. Richard Gaskill, MD, a
physician with ThePermanente Medical
Group since 1990.His interests include
biking, skiing, hiking,climbing, photography,and travel. More of his
photography can be seenon pages 8 and 16.
Related Documents











