American Family Physician® Return to Previous Page May 15, 2000 Table of Contents (http://www.aafp.org/afp/2000/0515/) The Painful Shoulder: Part I. Clinical Evaluation THOMAS W. WOODWARD, M.D., and THOMAS M. BEST, M.D., PH.D., University of Wisconsin Medical School, Madison, Wisconsin Am Fam Physician. 2000 May 15;61(10):3079-3088. This is Part I of a two-part article on clinical evaluation of the painful shoulder. Part II, “Acute and Chronic Injuries,” (http://w w w .aaf p.org/af p/2000/0601/p3291) will appear in the next issue of AFP. Family physicians need to understand diagnostic and treatment strategies for common causes of shoulder pain. We review key elements of the history and physical examination and describe maneuvers that can be used to reach an appropriate diagnosis. Examination of the shoulder should include inspection, palpation, evaluation of range of motion and provocative testing. In addition, a thorough sensorimotor examination of the upper extremity should be performed, and the neck and elbow should be evaluated. Shoulder pain is a common complaint in family practice patients. The unique anatomy and range of motion of the glenohumeral joint can present a diagnostic challenge, but a proper clinical evaluation usually discloses the cause of the pain. Anatomy The shoulder is composed of the humerus, glenoid, scapula, acromion, clavicle and surrounding soft tissue structures. The shoulder region includes the glenohumeral joint, the acromioclavicular joint, the sternoclavicular joint and the scapulothoracic articulation (Figure 1a). The glenohumeral joint capsule consists of a fibrous capsule, ligaments and the glenoid labrum. Because of its lack of bony stability,

The Painful Shoulder_ Part I. Clinical Evaluation.pdf
Oct 25, 2015
Painful Shoulder Clinical evaluation guidelines physical exam
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

American Family Physician®Return to Previous Page
May 15, 2000 Table of Contents (http://www.aafp.org/afp/2000/0515/)
The Painful Shoulder: Part I. Clinical Evaluation
THOMAS W. WOODWARD, M.D., and THOMAS M. BEST, M.D., PH.D., University of Wisconsin Medical School, Madison, Wisconsin
Am Fam Physician. 2000 May 15;61(10):3079-3088.
This is Part I of a two-part article on clinical evaluation of the painful shoulder. Part II, “Acute and Chronic Injuries,”
(http://w w w .aafp.org/afp/2000/0601/p3291) will appear in the next issue of AFP.
Family physicians need to understand diagnostic and treatment strategies for common causes of shoulder pain. We
review key elements of the history and physical examination and describe maneuvers that can be used to reach an
appropriate diagnosis. Examination of the shoulder should include inspection, palpation, evaluation of range of motion
and provocative testing. In addition, a thorough sensorimotor examination of the upper extremity should be performed,
and the neck and elbow should be evaluated.
Shoulder pain is a common complaint in family practice patients. The unique anatomy and range of motion of the glenohumeral joint can
present a diagnostic challenge, but a proper clinical evaluation usually discloses the cause of the pain.
Anatomy
The shoulder is composed of the humerus, glenoid, scapula, acromion, clavicle and surrounding soft tissue structures. The shoulder
region includes the glenohumeral joint, the acromioclavicular joint, the sternoclavicular joint and the scapulothoracic articulation (Figure
1a). The glenohumeral joint capsule consists of a fibrous capsule, ligaments and the glenoid labrum. Because of its lack of bony stability,

the glenohumeral joint is the most commonly dislocated major joint in the body. Glenohumeral stability is due to a combination of
ligamentous and capsular constraints, surrounding musculature and the glenoid labrum. Static joint stability is provided by the joint
surfaces and the capsulolabral complex, and dynamic stability by the rotator cuff muscles and the scapular rotators (trapezius, serratus
anterior, rhomboids and levator scapulae).
The rotator cuff is composed of four muscles: the supraspinatus, infraspinatus, teres minor and subscapularis (Figure 1b). The
subscapularis facilitates internal rotation, and the infraspinatus and teres minor muscles assist in external rotation. The rotator cuff
muscles depress the humeral head against the glenoid. With a poorly functioning (torn) rotator cuff, the humeral head can migrate
FIGURE 1A.
Anatomy of the shoulder girdle.

upward within the joint because of an opposed action of the deltoid muscle.
Scapular stability collectively involves the trapezius, serratus anterior and rhomboid muscles. The levator scapular and upper trapezius
muscles support posture; the trapezius and the serratus anterior muscles help rotate the scapula upward, and the trapezius and the
rhomboids aid scapular retraction.
History
A complete history begins with the patient's age, dominant hand and sport or work activity. It is important to assess whether the injury
prevents or hampers normal work activities, hobbies and sports. The patient should be asked about shoulder pain, instability, stiffness,
locking, catching and swelling. Stiffness or loss of motion may be the major symptom in patients with adhesive capsulitis (frozen
shoulder), dislocation or glenohumeral joint arthritis. Pain with throwing (such as pitching a baseball) suggests anterior glenohumeral
instability. Patients who complain of generalized joint laxity often have multidirectional glenohumeral instability.
Distinguishing between an acute and a chronic problem is diagnostically helpful (Table 1). For example, a history of acute trauma to the
shoulder with the arm abducted and externally rotated strongly suggests shoulder subluxation or dislocation and possible glenoid labral
injury. In contrast, chronic pain and loss of passive range of motion suggest frozen shoulder or tears of the rotator cuff.
FIGURE 1B.
The muscles of the rotator cuff.

Once the location, quality, radiation, and aggravating and relieving factors of the shoulder pain have been established, the possibility of
referred pain should be excluded. Neck pain and pain that radiates below the elbow are often subtle signs of a cervical spine disorder
that is mistaken for a shoulder problem.
The patient should be asked about paresthesias and muscle weakness. Pneumonia, cardiac ischemia and peptic ulcer disease can
present with shoulder pain. A history of malignancy raises the possibility of metastatic disease. The patient should be asked about
previous corticosteroid injections, particularly in the setting of osteopenia or rotator cuff tendon atrophy.
Physical Examination
TABLE 1
Key Findings in the History and Physical Examination
FINDING PROBABLE DIAGNOSIS
Scapular winging, trauma, recent viral illness Serratus anterior or trapezius dysfunction
Seizure and inability to passively or actively rotate affected arm externally Posterior shoulder dislocation
Supraspinatus/infraspinatus wasting Rotator cuff tear; suprascapular nerveentrapment
Pain radiating below elbow; decreased cervical range of motion Cervical disc disease
Shoulder pain in throwing athletes; anterior glenohumeral joint pain andimpingement
Glenohumeral joint instability
Pain or “clunking” sound with overhead motion Labral disorder
Nighttime shoulder pain Impingement
Generalized ligamentous laxity Multidirectional instability

A complete physical examination includes inspection and palpation, assessment of range of motion and strength, and provocative
shoulder testing for possible impingement syndrome and glenohumeral instability. The neck and the elbow should also be examined to
exclude the possibility that the shoulder pain is referred from a pathologic condition in either of these regions.
INSPECTION
The physical examination includes observing the way the patient moves and carries the shoulder. The patient should be properly
disrobed to permit complete inspection of both shoulders. Swelling, asymmetry, muscle atrophy, scars, ecchymosis and any venous
distention should be noted. Deformity, such as squaring of the shoulder that occurs with anterior dislocation, can immediately suggest a
diagnosis. Scapular “winging,” which can be associated with shoulder instability and serratus anterior or trapezius dysfunction, should be
noted. Atrophy of the supraspinatus or infraspinatus should prompt a further work-up for such conditions as rotator cuff tear,
suprascapular nerve entrapment or neuropathy.
PALPATION
Palpation should include examination of the acromioclavicular and sternoclavicular joints, the cervical spine and the biceps tendon. The
anterior glenohumeral joint, coracoid process, acromion and scapula should also be palpated for any tenderness and deformity.
RANGE-OF-MOTION TESTING
Because the complex series of articulations of the shoulder allows a wide range of motion, the affected extremity should be compared
with the unaffected side to determine the patient's normal range. Active and passive ranges should be assessed. For example, a patient
with loss of active motion alone is more likely to have weakness of the affected muscles than joint disease.
Shoulder abduction involves the glenohumeral joint and the scapulothoracic articulation. Glenohumeral motion can be isolated by
holding the patient's scapula with one hand while the patient abducts the arm. The first 20 to 30 degrees of abduction should not require
scapulothoracic motion. With the arm internally rotated (palm down), abduction continues to 120 degrees. Beyond 120 degrees, full
abduction is possible only when the humerus is externally rotated (palm up).
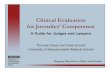
The Apley scratch test is another useful maneuver to assess shoulder range of motion (Figure 2). In this test, abduction and external
rotation are measured by having the patient reach behind the head and touch the superior aspect of the opposite scapula. Conversely,
internal rotation and adduction of the shoulder are tested by having the patient reach behind the back and touch the inferior aspect of
the opposite scapula. External rotation should be measured with the patient's arms at the side and elbows flexed to 90 degrees.

EVALUATING THE ROTATOR CUFF
In evaluating the rotator cuff, the patient's affected extremity should always be compared with the unaffected side to detect subtle
differences in strength and motion. A key finding, particularly with rotator cuff problems, is pain accompanied by weakness. True
weakness should be distinguished from weakness that is due to pain. A patient with subacromial bursitis with a tear of the rotator cuff
often has objective rotator cuff weakness caused by pain when the arm is positioned in the arc of impingement. Conversely, the patient
will have normal strength if the arm is not tested in abduction.1
The supraspinatus can be tested by having the patient abduct the shoulders to 90 degrees in forward flexion with the thumbs pointing
downward. The patient then attempts to elevate the arms against examiner resistance (Figure 3). This is often referred to as the “empty
can” test.
FIGURE 2.
Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. (Left) Testing abduction andexternal rotation. (Right) Testing adduction and internal rotation.

Next, with the patient's arms at the sides, the patient flexes both elbows to 90 degrees while the examiner provides resistance against
external rotation (Figure 4). This maneuver is used to evaluate the function of the infraspinatus and teres minor muscles, which are
mainly responsible for external rotation.
FIGURE 3.
Supraspinatus examination (“empty can” test). The patient attempts to elevate the arms against resistance while the elbows are extended, thearms are abducted and the thumbs are pointing downward.
FIGURE 4.
Infraspinatus/teres minor examination. The patient attempts to externally rotate the arms against resistance while the arms are at the sides andthe elbows are flexed to 90 degrees.

Subscapularis function is assessed with the lift-off test. The patient rests the dorsum of the hand on the back in the lumbar area. Inability
to move the hand off the back by further internal rotation of the arm suggests injury to the subscapularis muscle.2 In one study, the
investigators noted that only a few of the patients with confirmed subscapularis ruptures actually demonstrated a positive result on the
lift-off test; the remainder could not complete the test because of pain.3
A modified version of the lift-off test is useful in a patient who cannot place the hand behind the back. In this version, the patient places
the hand of the affected arm on the abdomen and resists the examiner's attempts to externally rotate the arm.
Provocative TestingProvocative tests provide a more focused evaluation for specific problems and are typically performed after the history and general
examination have been completed (Table 2).
TABLE 2
Tests Used in Shoulder Evaluation and Significance of Positive Findings
TEST MANEUVERDIAGNOSIS SUGGESTED BY POSITIVERESULT
Apley scratchtest
Patient touches superior and inferior aspects of opposite scapula Loss of range of motion: rotator cuffproblem
Neer's sign Arm in full flexion Subacromial impingement
Hawkins' test Forward flexion of the shoulder to 90 degrees and internal rotation Supraspinatus tendon impingement
Drop-arm test Arm lowered slowly to waist Rotator cuff tear
Cross-arm test Forward elevation to 90 degrees and active adduction Acromioclavicular joint arthritis
Spurling's test Spine extended with head rotated to affected shoulder while axially
loaded
Cervical nerve root disorder
Apprehensiontest
Anterior pressure on the humerus with external rotation Anterior glenohumeral instability

NEER'S TEST
Neer's impingement sign is elicited when the patient's rotator cuff tendons are pinched under the coracoacromial arch. The test4 is
performed by placing the arm in forced flexion with the arm fully pronated (Figure 5). The scapula should be stabilized during the
maneuver to prevent scapulothoracic motion. Pain with this maneuver is a sign of subacromial impingement.
Relocation test Posterior force on humerus while externally rotating the arm Anterior glenohumeral instability
Sulcus sign Pulling downward on elbow or wrist Inferior glenohumeral instability
Yergason test Elbow flexed to 90 degrees with forearm pronated Biceps tendon instability or tendonitis
Speed's
maneuver
Elbow flexed 20 to 30 degrees and forearm supinated Biceps tendon instability or tendonitis
“Clunk” sign Rotation of loaded shoulder from extension to forward flexion Labral disorder
FIGURE 5.
Neer's test for impingement of the rotator cuff tendons under the coracoacromial arch. The arm is fully pronated and placed in forced flexion.

HAWKINS' TEST
The Hawkins' test is another commonly performed assessment of impingement.5 It is performed by elevating the patient's arm forward to
90 degrees while forcibly internally rotating the shoulder (Figure 6). Pain with this maneuver suggests subacromial impingement or
rotator cuff tendonitis. One study6 found Hawkins' test more sensitive for impingement than Neer's test.
DROP-ARM TEST
A possible rotator cuff tear can be evaluated with the drop-arm test. This test is performed by passively abducting the patient's shoulder,
then observing as the patient slowly lowers the arm to the waist. Often, the arm will drop to the side if the patient has a rotator cuff tear or
supraspinatus dysfunction. The patient may be able to lower the arm slowly to 90 degrees (because this is a function mostly of the
deltoid muscle) but will be unable to continue the maneuver as far as the waist.
CROSS-ARM TEST
Patients with acromioclavicular joint dysfunction often have shoulder pain that is mistaken for impingement syndrome. The cross-arm test
isolates the acromioclavicular joint. The patient raises the affected arm to 90 degrees. Active adduction of the arm forces the acromion
into the distal end of the clavicle (Figure 7). Pain in the area of the acromioclavicular joint suggests a disorder in this region.
FIGURE 6.
Hawkins' test for subacromial impingement or rotator cuff tendonitis. The arm is forward elevated to 90 degrees, then forcibly internally rotated.

Instability Testing
The tests described in this section are useful in evaluating for glenohumeral joint stability. Because the shoulder is normally the most
unstable joint in the body, it can demonstrate significant glenohumeral translation (motion). Again, the uninvolved extremity should be
examined for comparison with the affected side.7,8
APPREHENSION TEST
The anterior apprehension test is performed with the patient supine or seated and the shoulder in a neutral position at 90 degrees of
abduction. The examiner applies slight anterior pressure to the humerus (too much force can dislocate the humerus) and externally
rotates the arm (Figure 8). Pain or apprehension about the feeling of impending subluxation or dislocation indicates anterior
glenohumeral instability.
FIGURE 7.
Cross-arm test for acromioclavicular joint disorder. The patient elevates the affected arm to 90 degrees, then actively adducts it.

RELOCATION TEST
The relocation test is performed immediately after a positive result on the anterior apprehension test. With the patient supine, the
examiner applies posterior force on the proximal humerus while externally rotating the patient's arm. A decrease in pain or apprehension
suggests anterior glenohumeral instability.
YERGASON TEST
Patients with rotator cuff tendonitis frequently have concomitant inflammation of the biceps tendon. The Yergason test is used to
evaluate the biceps tendon.9 In this test, the patient's elbow is flexed to 90 degrees with the thumb up. The examiner grasps the wrist,
resisting attempts by the patient to actively supinate the arm and flex the elbow (Figure 9). Pain with this maneuver indicates biceps
tendonitis.
FIGURE 8.
Apprehension test for anterior instability. The patient's arm is abducted to 90 degrees while the examiner externally rotates the arm and appliesanterior pressure to the humerus.

SPEED'S MANEUVER
Speed's maneuver is used to examine the proximal tendon of the long head of the biceps. The patient's elbow is flexed 20 to 30 degrees
with the forearm in supination and the arm in about 60 degrees of flexion. The examiner resists forward flexion of the arm while palpating
the patient's biceps tendon over the anterior aspect of the shoulder.
SULCUS SIGN
With the patient's arm in a neutral position, the examiner pulls downward on the elbow or wrist while observing the shoulder area for a
sulcus or depression lateral or inferior to the acromion. The presence of a depression indicates inferior translation of the humerus and
suggests inferior glenohumeral instability (Figure 10). The examiner should remember that many asymptomatic patients, especially
adolescents, normally have some degree of instability.10
FIGURE 9.
Yergason test for biceps tendon instability or tendonitis. The patient's elbow is flexed to 90 degrees, and the examiner resists the patient's activeattempts to supinate the arm and flex the elbow.

POSTERIOR APPREHENSION AND INSTABILITY
Posterior instability of the shoulder can be assessed by using a simple test.11 With the patient supine or sitting, the examiner pushes
posteriorly on the humeral head with the patient's arm in 90 degrees of abduction and the elbow in 90 degrees of flexion.
‘CLUNK’ SIGN
Glenoid labral tears are assessed with the patient supine. The patient's arm is rotated and loaded (force applied) from extension through
to forward flexion. A “clunk” sound or clicking sensation can indicate a labral tear even without instability.12
Cervical Disc Disease
FIGURE 10.
Sulcus test for glenohumeral instability. Downward traction is applied to the humerus, and the examiner watches for a depression lateral or
inferior to the acromion.

No physical examination in a patient with shoulder pain is complete without excluding cervical spine disease. Referred or radicular pain
from disc disease should be considered in patients who have shoulder pain that does not respond to conservative treatment. The patient
should be questioned about neck pain and previous neck injury, and the examiner should note whether pain worsens with turning of the
neck, which suggests disc disease. Pain that originates from the neck or radiates past the elbow is often associated with a neck disorder.
Plain film is a useful screening tool for degenerative cervical disc disease. Further work-up and imaging studies depend on the
differential diagnosis and the treatment plan.
SPURLING'S TEST
In a patient with neck pain or pain that radiates below the elbow, a useful maneuver to further evaluate the cervical spine is Spurling's
test. The patient's cervical spine is placed in extension and the head rotated toward the affected shoulder. An axial load is then placed
on the spine (Figure 11). Reproduction of the patient's shoulder or arm pain indicates possible cervical nerve root compression and
warrants further evaluation of the bony and soft tissue structures of the cervical spine.
FIGURE 11.
Spurling's test for cervical root disorder. The neck is extended and rotated toward the affected shoulder while an axial load is placed on the spine.

The Authors
THOMAS W. WOODWARD, M.D., is a clinical assistant professor of family medicine at the University of Wisconsin Medical School,
Madison. A graduate of the University of Iowa College of Medicine, Iowa City, Dr. Woodward completed a family practice residency at the
University of Wisconsin Medical School.
THOMAS M. BEST, M.D., PH.D., is an assistant professor of family medicine and orthopedics at the University of Wisconsin Medical
School. He received his medical degree from the University of Western Ontario Faculty of Medicine and Dentistry, London, Ontario, and
served a family practice residency in Chapel Hill, N.C. After receiving a doctorate in biomedical engineering from Duke University,
Durham, N.C., Dr. Best completed sports medicine training at the University of Wisconsin Medical School.
Address correspondence to Thomas M. Best, M.D., Ph.D., University of Wisconsin Hospitals and Clinics, 621 Science Dr., Madison, WI
53711. Reprints are not available from the authors.
REFERENCES
1. Miniaci A, Salonen D. Rotator cuff evaluation imaging and diagnosis. Orthop Clin North Am. 1997;28:43–58.
2. Gerber C, Krushell RJ. Isolated rupture of the tendon of the subscapularis muscle: clinical features in 16 cases. J Bone Joint Surg [Br].
1991;73B:389–94.
3. Deutsch A, Altchek DW, Veltri DM, Potter HG, Warren RF. Traumatic tears of the subscapularis tendon: clinical diagnosis, magnetic
resonance imaging findings, and operative treatment. Am J Sports Med. 1997;25:13–22.
4. Neer CS. Impingement lesions. Clin Orthop. 1983;173:70–77.
5. Hawkins RJ, Kennedy JC. Impingement syndrome in athletes. Am J Sports Med. 1980;8:151–7.
6. Bak K, Fauno P. Clinical findings in competitive swimmers with shoulder pain. Am J Sports Med. 1997;25:254–60.
7. Harryman DT, Sidles JA, Clark JM, McQuade KJ, Gibb TD, Matsen FA. Translation of the humeral head on the glenoid with passive
glenohumeral motion. J Bone Joint Surg [Am]. 1990;72:1334–43.
8. Harryman DT, Sidles JA, Harris SL, Matsen FA. Laxity at the normal glenohumeral joint: a quantitative in-vivo assessment. J Shoulder
Elbow Surg. 1992;1:66–76.
9. Yergason RM. Supination sign. J Bone Joint Surg [Am]. 1931;13:160.

10. Emery RH, Mullaji AB. Glenohumeral joint instability in normal adolescents. J Bone Joint Surg [Br]. 1991;73B:406–8.
11. O'Driscoll SW. A reliable and simple test for posterior instability of the shoulder. J Bone Joint Surg [Br]. 1991;73B(suppl 1):50.
12. Glasgow SG, Bruce RA, Yacobucci GN, Torg JS. Arthroscopic resection of glenoid labral tears in the athlete: a report of 29 cases.
Arthroscopy. 1992;8:48–54.
Members of various family practice departments develop articles for “Problem-Oriented Diagnosis.” This article is one in a series
coordinated by the Department of Family Medicine at the University of Wisconsin Medical School, Madison. Guest editor of the series is
William E. Scheckler, M.D.
Related Documents