The optimized anti-CD20 monoclonal antibody ublituximab bypasses natural killer phenotypic features in Waldenström macroglobulinemia by Magali Le Garff-Tavernier, Linda Herbi, Christophe De Romeuf, Nabih Azar, Damien Roos-Weil, Patrick Bonnemye, Rémi Urbain, Véronique Leblond, Hélène Merle-Beral, and Vincent Vieillard Haematologica 2014 [Epub ahead of print] Citation: Le Garff-Tavernier M, Herbi L, De Romeuf C, Azar N, Roos-Weil D, Bonnemye O, Urbain R, Leblond V, Merle-Beral H, and Vieillard V. The optimized anti-CD20 monoclonal antibody ublituximab bypasses natural killer phenotypic features in Waldenström macroglobulinemia. Haematologica. 2014; 99:xxx doi:10.3324/haematol.2014.118083 Publisher's Disclaimer.0 E-publishing ahead of print is increasingly important for the rapid dissemination of science. Haematologica is, therefore, E-publishing PDF files of an early version of manuscripts that have completed a regular peer review and have been accepted for publication. E-publishing of this PDF file has been approved by the authors. After having E-published Ahead of Print, manuscripts will then undergo technical and English editing, typesetting, proof correction and be presented for the authors' final approval; the final version of the manuscript will then appear in print on a regular issue of the journal. All legal disclaimers that apply to the journal also pertain to this production process. Copyright 2014 Ferrata Storti Foundation. Published Ahead of Print on December 31, 2014, as doi:10.3324/haematol.2014.118083.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The optimized anti-CD20 monoclonal antibody ublituximab bypasses natural killer phenotypic features in Waldenström macroglobulinemia
by Magali Le Garff-Tavernier, Linda Herbi, Christophe De Romeuf, Nabih Azar, DamienRoos-Weil, Patrick Bonnemye, Rémi Urbain, Véronique Leblond, Hélène Merle-Beral, and Vincent Vieillard
Haematologica 2014 [Epub ahead of print]
Citation: Le Garff-Tavernier M, Herbi L, De Romeuf C, Azar N, Roos-Weil D, Bonnemye O, Urbain R, Leblond V, Merle-Beral H, and Vieillard V. The optimized anti-CD20 monoclonal antibody ublituximab bypasses natural killer phenotypic features in Waldenström macroglobulinemia. Haematologica. 2014; 99:xxxdoi:10.3324/haematol.2014.118083
Publisher's Disclaimer.0E-publishing ahead of print is increasingly important for the rapid dissemination of science.Haematologica is, therefore, E-publishing PDF files of an early version of manuscripts thathave completed a regular peer review and have been accepted for publication. E-publishingof this PDF file has been approved by the authors. After having E-published Ahead of Print,manuscripts will then undergo technical and English editing, typesetting, proof correction andbe presented for the authors' final approval; the final version of the manuscript will thenappear in print on a regular issue of the journal. All legal disclaimers that apply to thejournal also pertain to this production process.
Copyright 2014 Ferrata Storti Foundation.Published Ahead of Print on December 31, 2014, as doi:10.3324/haematol.2014.118083.

1
Letter to the Editor
The optimized anti-CD20 monoclonal antibody ublituximab bypasses natural killer
phenotypic features in Waldenström macroglobulinemia
Magali Le Garff-Tavernier1,2,3, Linda Herbi1,2,4, Christophe de Romeuf4, Nabih Azar5,
Damien Roos-Weil1,5, Patrick Bonnemye3, Rémi Urbain4, Véronique Leblond1,5, Hélène
Merle-Beral1,3,6,* and Vincent Vieillard1,2,7,*
1Sorbonne Universités, UPMC, Univ Paris 06, Paris, France; 2INSERM U1135, CIMI-Paris, Paris, France; 3AP-HP, Hôpital Pitié-Salpêtrière, Service d’Hématologie Biologique, Paris, France; 4Laboratoire Français de Fractionnement et des Biotechnologies (LFB), Les Ulis, France; 5AP-HP, Hôpital Pitié-Salpêtrière, Service d’Hématologie Clinique, Paris, France; 6INSERM U1138, Programmed cell death and physiopathology of tumor cells, team 19,
Centre de Recherche des Cordeliers, Paris, France and 7CNRS, ERL8255, CIMI-Paris, Paris, France * HMB and VV contributed equally to this manuscript.
Running heads: Ublituximab bypasses NK features in WM
Correspondence:
Dr Magali Le Garff-Tavernier, Service d’Hématologie Biologique, Groupe Hospitalier Pitié-
Salpêtrière Charles-Foix, Bâtiment de la Pharmacie, 47-83 bd de l’Hôpital, 75651 Paris
Cedex 13, France.
E-mail: [email protected]
Acknowledgments
The authors would like to thank the patients for providing the research samples used in this
study. We also thank C. Blanc and B. Hoareau from the Flow Cytometry Core CyPS (Pierre
et Marie Curie University, Paris, France) for the cell sorting. J. Decocq, M. Brissard, S.
Gueguen and A. Grelier are acknowledged for their technical assistance. This study was
supported in part by funds from the Laboratoire Français de Fractionnement et des
Biotechnologies (LFB, Les Ulis, France), the association la Ligue contre le cancer (RS08/75-
2
4) and INSERM. V. Vieillard is recipient of a Contrat Hospitalier de Recherche
Translationnelle (CHRT).
3
Waldenström macroglobulinemia (WM) is a rare form of lymphoma characterized by
an infiltration of lymphoplasmacytic cells in bone marrow and immunoglobulin M
monoclonal gammopathy.1 Despite the introduction of several therapies, WM remains
incurable.2 Therefore, novel strategies await a better understanding of the mechanisms
underlying the immune surveillance around this pathology. Natural killer (NK) cells were
initially identified through their ability to lyse tumor cells. They express an array of inhibitory,
activating, adhesion and cytokine receptors that enable them to kill targets while sparing
normal cells.3 NK cells also express the low-affinity Fc receptor (FcγRIIIA/CD16), enabling
them to detect antibody-coated target cells and to exert antibody-dependent cell cytotoxicity
(ADCC).3 In this study, we focused our attention on NK cells relative to the presence of a
circulating B-cell clone in WM patients.
The 47 WM patients were diagnosed at the WM French Reference Center Pitié-
Salpêtrière Hospital (Paris, France) according to classical biological criteria.1 This study was
approved by the institutional ethic committee at the Pitié-Salpêtrière Hospital (CPPIDF6) and
all patients provided informed consent prior to participation.
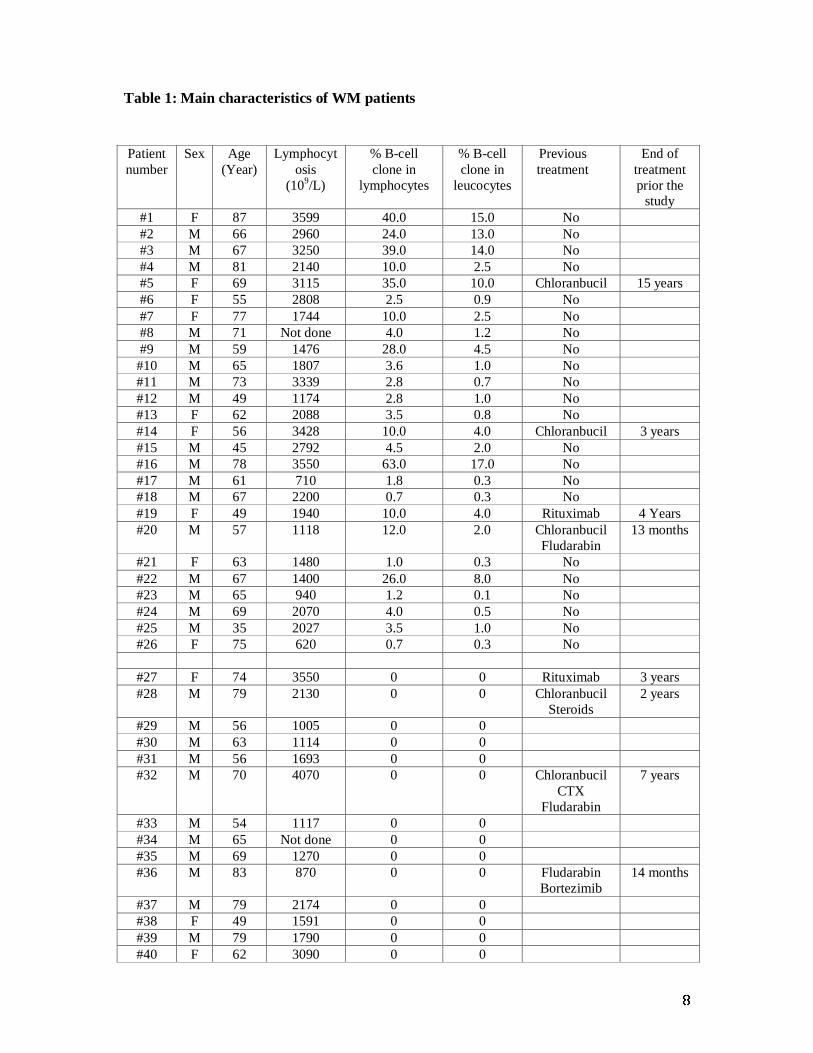
The characteristics of WM patients are summarized in Table 1. They were untreated or
received no treatment during the two years prior to the study, and compared to 20 healthy
blood donors from the Etablissement Français du Sang. In 26/47 patients, circulating B-cell
clone was detected with a frequency ranging from 0.7 to 63.0 % of lymphocytes,
corresponding to 0.1 to 17.0% of leukocytes. NK cells, B- and T-lymphocytes from freshly
harvested whole blood samples were analyzed on the CD45+ lymphocytic gate after staining
with an appropriate antibody cocktail (Supplemental data 1), as previously described.4,5 At
least 100,000 leucocytes were analyzed on a FACSCanto II (BD Biosciences) to assess the
distribution of NK cells, B and T lymphocytes from WM patients, relative to the presence of
circulating B-cells (as defined in Supplemental data 2), and compared with healthy controls.
A similar absolute number of whole CD3+ T and CD19+ B cells in healthy controls and WM
samples are observed (Figure 1a). The absolute value of B cells correlated significantly with
the percentage of a circulating B-cell clone (Figure 1b). The distribution of CD3-CD56+ NK
cells and both CD56dim and CD56bright subsets did not differ between the study groups (Figures
1c-1d), indicating that WM does not disturb this immune subset, compared with other
hematological diseases.5-8
The phenotypic frequency of the CD3-CD56dim cytotoxic NK cell subset was further
investigated on a Gallios (Beckman-Coulter) flow cytometer, while gating out CD3-CD56bright
cell. The frequency of CD56dim NK cells from WM patients was indistinguishable from those

4
of controls in terms of the cell-surface expression of NK receptors (FcγRIIIA/CD16, NKG2A,
NKG2D, NKG2C, ILT-2, LAIR1, DNAM-1, NKp80, and 2B4) (Figure 1e and data not
shown). However, it is important to note that mean of fluorescence intensity (MFI) values for
CD16 are significantly increased in WM patients, whatever the presence of circulating B-cell
clone, as compared to controls (Figures 1e). Additionally, the early activation marker CD69 is
increased in WM, both in absolute value and percentage (Figure 1f), whereas it is decreased in
chronic lymphocytic leukemia (CLL).5 Notably, the expression of each tested receptor
seemed remarkably stable over a 1-year period (Supplemental data 3). More importantly,
CD57, a marker associated with terminal NK differentiation,9 was profoundly increased in the
WM patients, both in percentage and absolute value, and particularly in those with a
circulating B-cell clone (Figure 1g). These data are consistent with those reported by Li et al10
showing that CD57+ cytotoxic T cells are increased in patients with WM. CD57 was also
frequently reported in the association with several cancers, strongly linked to a less severe
disease and a better outcome, in sharp contrast to what was observed for CD8+ T cells.11 We
also observed a weaker expression of the activating NK receptors NKp30 in WM patients,
compared with controls (Figures 1h). In addition, Figure 1h shows an inverse correlation
between CD57 and NKp30 expressions, which is highly more significant in WM patients
(Spearman test: r=-0.91, p<0.0001), than in healthy controls (Spearman test: r=-0.49, p=0.01),
previously reported in the relationship with differentiation of NK cells. Taken together, these
data suggest that CD56dim NK cells in WM are more differentiated in patients with a
circulating B-cell clone. Similar modulations of the NK-cell repertoire was previously
described in the elderly individuals,4 and in patients with acute leukemia,12 but not with CLL.5
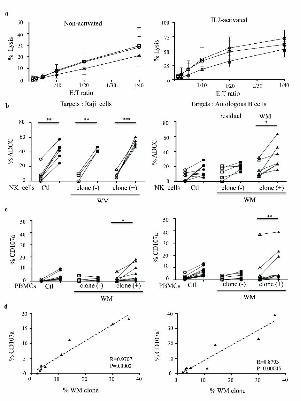
We further assessed the overall cytolytic activity of NK cells from WM patients.
Direct cytotoxicity was performed against K562 target cells. NK cells were purified from
fresh peripheral blood mononuclear cells (PBMCs) at the Flow Cytometry Core CyPS (Pitie-
Salpetriere hospital) with a cell-sorting BD FACSAria II flow cytometer. The purification of
CD3-CD56+ NK cells was >98%. Direct cytotoxicity was assessed on purified NK cells
before or after IL-2 stimulation (1,000 U/ml, Proleukin, Chiron) for 48 hours with a standard 51Cr-release assay against the K562 cell line, at a different effector/target (E:T) cell ratio.5,6 A
slight but non-significant decrease of the cytotoxicity mediated by non- or IL2-activated NK
cells was observed in the group of WM patients with a circulating B-cell clone compared with
two other groups (Figure 2a). Of note, granzyme-B and perforin were expressed at equivalent
levels in all samples (Supplemental data 3).

5
ADCC assays were performed with purified non-activated NK cells in the presence of 51Cr-labeled Raji target cells or purified autologous peripheral blood B cells, at an effector
ratio of 1:10 in the presence of anti-CD20 rituximab (Roche Ltd) or ublituximab (LFB
Biotech), an optimized anti-CD20 mAb characterized by a low fucose content in its Fc region
that improves FcγRIIIA (CD16) binding and consequently increases ADCC activity.13 ADCC
against Raji cells was significantly increased in the presence of 1 ng/ml of ublituximab,
compared with rituximab, in all groups (Figure 2b, left panel). However, ADCC against
autologous B cells was significantly increased in WM patients with a circulating B-cell clone
only in the presence of ublituximab, and not of rituximab (Figure 2b, right panel). The
comparison of ADCC mediated in the presence of Raji cells and autologous B-cells revealed
that ADCC efficacy is mainly more dependent of the intrinsic resistance to the tumor target
cells, than on the NK functionality. An additional support for ADCC findings provided from
the degranulation capacities of NK cells, which are highlighted by CD107a cell-surface
expression by flow cytometry, in the presence of these two anti-CD20 mAbs, as described.6
Indeed, regardless of the concentration, ublituximab triggered better effector functions to clear
WM cells in patients with a circulating B-cell clone compared with rituximab (Figure 2c),
which is consistent with findings in CLL patients.5,6 Importantly, the percentage of CD107a+
NK cells significantly correlated with the frequency of circulating B-cell clones only in the
presence of ublituximab (Figure 2d).
Taken together, these data show that the efficacy of NK cells against B-cell clones is
greater with ublituximab than with rituximab, allowing the NK phenotypic features observed
in WM to be bypassed.
Finally, our findings provide additional insights into the cellular mechanisms
underlying the clinical activity of optimized anti-CD20 mAbs. An ongoing phase I/II study of
ublituximab (NCT01647971) to evaluate monotherapy in rituximab-relapse and refractory B-
cell lymphoid malignancies, including WM shows promising early results.14 However, it
should be important to perform side-by-side in vivo experiments in human testing both
ublituximab and rituximab efficacy in WM. In parallel, further combination of optimized anti-
CD20 mAbs with novel chemo-free drugs that target B-cell receptor signaling such as bruton
tyrosine kinase (BTK) inhibitor (ibrutinib) and phosphatidylinositol-3-kinase delta (PI3Kδ)
inhibitor (idelalisib) may achieve complete remission in WM patients.15
6
Authorship
MLT, HMB and VV were the principal investigators and take primary responsibility for the
paper; CdR and RU provided anti-CD20 mAb reagents and participated to the design of the
study; NA, DR, and VL recruited the patients; MLT, LH and PB performed the laboratory
work for this study; MLT, HMB and VV wrote the paper. CdR, NA, DR, RU and VL
critically read and approved the manuscript.
Disclosures
CdR and RU are employed by LFB. Ublituximab was designed, manufactured and provided
by LFB Biotechnologies (Les Ulis, France). CdR has filed patent application
(PCT/FR2005/003123) owned by LFB Biotechnologies covering the use of ublituximab in B-
cell lymphoma. In January 2012, LFB Biotechnologies licensed the exclusive rights to
develop and commercialize ublituximab to TG Therapeutics, Inc. (New York, NY, USA).
MLT, LH, NA, DRW, PB, HMB, and VV have no relevant conflicts of interest to disclose.
References
1. Campo E, Swerdlow SH, Harris NL, Pileri S, Stein H, Jaffe ES. The 2008 WHO
classification of lymphoid neoplasms and beyond: evolving concepts and practical
applications. Blood. 2011;117(19):5019-32.
2. Leblond V, Johnson S, Chevret S, et al. Results of a randomized trial of chlorambucil
versus fludarabine for patients with untreated Waldenstrom macroglobulinemia, marginal
zone lymphoma, or lymphoplasmacytic lymphoma. J Clin Oncol. 2013;31(3):301-317.
3. Vivier E, Ugolini S, Blaise D, Chabannon C, Brossay L. Targeting natural killer cells and
natural killer T cells in cancer. Nat Rev Immunol. 2012;12(4):239-252.
4. Le Garff-Tavernier M, Beziat V, Decocq J, et al. Human NK cells display major
phenotypic and functional changes over the life span. Aging Cell. 2010; 9(4):527-535.
5. Le Garff-Tavernier M, Decocq J, de Romeuf C, et al. Analysis of CD16+CD56dim NK
cells from CLL patients: evidence supporting a therapeutic strategy with optimized anti-
CD20 monoclonal antibodies. Leukemia. 2011; 25(1):101-109.
6. Le Garff-Tavernier M, Herbi L, de Romeuf C, et al. Antibody-dependent cellular
cytotoxicity of the optimized anti-CD20 monoclonal antibody ublituximab on chronic
lymphocytic leukemia cells with the 17p deletion. Leukemia. 2014;28(1):230–233.
7
7. Farnault L, Sanchez C, Baier C, Le Treut T, Costello RT. Hematological malignancies
escape from NK cell innate immune surveillance: mechanisms and therapeutic
implications. Clin Dev Immunol. 2012;2012:421702.
8. Lion E, Willemen Y, Berneman ZN, Van Tendeloo VF, Smits EL. Natural killer cell
immune escape in acute myeloid leukemia. Leukemia. 2012;26(9):2019-2026.
9. Bjorkstrom NK, Riese P, Heuts F, et al. Expression patterns of NKG2A, KIR, and CD57
define a process of CD56dim NK-cell differentiation uncoupled from NK-cell education.
Blood. 2010;116(19):3853-3864.
10. Li J, Sze DM, Brown RD, et al. Clonal expansions of cytotoxic T cells exist in the blood
of patients with Waldenström macroglobulinemia but exhibit anergic properties and are
eliminated by nucleoside analog therapy. Blood. 2010;115(17):3580-3588.
11. Nielsen CM, White MJ, Goodier MR, Riley EM. Functional Significance of CD57
Expression on Human NK Cells and Relevance to Disease. Front Immunol. 2013;4:422.
12. Fauriat C, Just-Landi S, Mallet F, et al. Deficient expression of NCR in NK cells from
acute myeloid leukemia: Evolution during leukemia treatment and impact of leukemia
cells in NCRdull phenotype induction. Blood. 2007;109(1):323-330.
13. de Romeuf C, Dutertre CA, Le Garff-Tavernier M, et al. Chronic lymphocytic leukaemia
cells are efficiently killed by an anti-CD20 monoclonal antibody selected for improved
engagement of FcgammaRIIIA/CD16. Br J Haematol. 2008;140(6):635-643.
14. Deng C, Effie Amengual J, Schreeder MT, et al. A phase I dose-escalation trial of
ublituximab (TG-1101), a novel anti-CD20 monoclonal antibody (mAb), for rituximab
relapsed/refractory B-cell lymphoma patients. J Clin Oncol. 2013;31(15):8575.
15. Ghobrial IM. Choice of therapy for patients with Waldenstrom macroglobulinemia. J
Clin Oncol. 2013;31(3):291-293.
8
Table 1: Main characteristics of WM patients
Patient number
Sex Age (Year)
Lymphocytosis
(109/L)
% B-cell clone in
lymphocytes
% B-cell clone in
leucocytes
Previous treatment
End of treatment prior the
study #1 F 87 3599 40.0 15.0 No #2 M 66 2960 24.0 13.0 No #3 M 67 3250 39.0 14.0 No #4 M 81 2140 10.0 2.5 No #5 F 69 3115 35.0 10.0 Chloranbucil 15 years #6 F 55 2808 2.5 0.9 No #7 F 77 1744 10.0 2.5 No #8 M 71 Not done 4.0 1.2 No #9 M 59 1476 28.0 4.5 No #10 M 65 1807 3.6 1.0 No #11 M 73 3339 2.8 0.7 No #12 M 49 1174 2.8 1.0 No #13 F 62 2088 3.5 0.8 No #14 F 56 3428 10.0 4.0 Chloranbucil 3 years #15 M 45 2792 4.5 2.0 No #16 M 78 3550 63.0 17.0 No #17 M 61 710 1.8 0.3 No #18 M 67 2200 0.7 0.3 No #19 F 49 1940 10.0 4.0 Rituximab 4 Years #20 M 57 1118 12.0 2.0 Chloranbucil
Fludarabin 13 months
#21 F 63 1480 1.0 0.3 No #22 M 67 1400 26.0 8.0 No #23 M 65 940 1.2 0.1 No #24 M 69 2070 4.0 0.5 No #25 M 35 2027 3.5 1.0 No #26 F 75 620 0.7 0.3 No
#27 F 74 3550 0 0 Rituximab 3 years #28 M 79 2130 0 0 Chloranbucil
Steroids 2 years
#29 M 56 1005 0 0 #30 M 63 1114 0 0 #31 M 56 1693 0 0 #32 M 70 4070 0 0 Chloranbucil
CTX Fludarabin
7 years
#33 M 54 1117 0 0 #34 M 65 Not done 0 0 #35 M 69 1270 0 0 #36 M 83 870 0 0 Fludarabin
Bortezimib 14 months
#37 M 79 2174 0 0 #38 F 49 1591 0 0 #39 M 79 1790 0 0 #40 F 62 3090 0 0

9
#41 M 79 690 0 0 #42 M 67 1540 0 0 #43 F 65 3964 0 0 #44 M 73 1495 0 0 #45 M 47 1609 0 0 #46 F 73 2243 0 0 #47 F 65 1565 0 0 Chloranbucil 3 years
F: Female ; M: Male ; CTX: Cyclophosphamide

10
Figure Legends
Figure 1. Distribution of lymphocyte subsets and characteristics of NK cells from WM
patients with or without circulating B-cell clones. (a) Absolute values of CD3+ T and CD19+
B cells from peripheral blood. (b) Linear regression between absolute value of CD19+ B cells
and the percentage of circulating B-cell clones (WM clone). (c) Absolute value and frequency
of CD3-CD56+ NK cells from peripheral blood. (d) Expression of CD56bright gated on CD3-
CD56+ NK cells. (e) Frequency and mean fluorescence intensity (MFI) of CD16 on CD3-
CD56dim NK cells. (f) Frequency and absolute value of CD69 on CD3-CD56dim NK cells. (g)
Frequency and absolute value of CD57 on CD3-CD56dim NK cells. (h) Frequency of NKp30
on CD3-CD56dim NK cells. Cells were collected from healthy donors (Ctl; circles) and WM
patients without (clone (-); squares) or with (clone (+); triangles) circulating B-cell clones
(WM clone). Horizontal bars represent the median values. Intergroup comparisons were
assessed with the Kruskal Wallis test and Dunn post-test; *P<0.05, **P<0.001, ***P<0.0001.
(i) Linear regression between CD57 and NKp30 frequencies on CD3-CD56dim NK cells in
healthy donors (Ctl, upper panel) and WM patients (lower panel).
Figure 2. Cytolytic activities of NK cells from WM patients with or without circulating B-
cell clones. (a) Direct lysis of non-activated (left panel) and IL2-activated (right panel) NK
cells from healthy donors (Ctl; circles; n=6) and WM patients without (clone (-); squares;
n=4) or with (clone (+); triangles; n=3) circulating B-cell clones. Cytotoxicity was measured
using standard 51Cr release-assays against K562 target cells at different effector:target cells
(E:T) ratio. The mean percentage values ± s.d. (vertical bars) are shown. (b) Comparison of
NK cell ADCC in the presence of rituximab (open symbols) or ublituximab (closed symbols)
against Raji cells at 1 ng/ml of anti-CD20 (left panel) or against purified peripheral blood
autologous B cells at 100 ng/ml of anti-CD20 (right panel). Assays were performed with
purified NK cells from healthy donors (Ctl; circles) and from WM patients without (clone (-);
squares) or with (clone (+); triangles) circulating B-cell clones (WM clone) (E:T ratio at 1:10).
(c) Degranulation response determined using CD107a expression on CD3-CD56+ NK cells in
the presence of 10 ng/ml (left panel) or 1,000 ng/ml (right panel) of rituximab (open symbols)
or ublituximab (closed symbols). Assays were performed on fresh PBMCs from healthy
donors (Ctl; circles) or WM patients without (clone (-); squares) or with (clone (+); triangles)
circulating B-cell clones (WM clone). P-values were calculated with the Wilcoxon rank-sum
test and refer to the comparison between rituximab and ublituximab; *P<0.05, **P<0.001,

11
***P<0.0001. (d) Linear regression between the percentage of CD107a expression on CD3-
CD56+ NK cells and the percentage of circulating B-cell clones (WM clone) after treatment
with 10 ng/ml (left panel) or 1,000 ng/ml (right panel) of ublituximab. All data relative to
ADCC and CD107a expression are presented after subtraction of the values obtained in the
absence of any antibody.


Antibodies Clone # Fluorochrome Compagny NK Cell-surface staining
Anti-CD3 UCHT1 ECD Beckman Coulter Anti-CD8 T8 FITC Beckman Coulter
Anti-CD16 3G8 FITC Beckman Coulter Anti-CD56 N901 PC7 Beckman Coulter Anti-CD69 TPI.55.3 PE Beckman Coulter
Anti-CD159a/NKG2A Z199 APC Beckman Coulter Anti-NKG2D ON72 APC Beckman Coulter
Anti-CD335/NKp46 BAB281 PE Beckman Coulter Anti-ILT‐2/CD85j GHI/75 PE Beckman Coulter
Anti-CD19 SJ25C1 PerCP Cy5.5 BD Biosciences Anti-DNAM‐1 DX11 FITC BD Biosciences Anti-LAIR1 DX26 FITC BD Biosciences
Anti-2B4 C1.7 PE BD Biosciences Anti-CD57 HNK‐1 FITC BD Biosciences
Anti-CD107a H4A3 FITC BD Biosciences Anti-NKG2C 134591 PE R&D systems
Anti-NKp80/KLFR1 239127 PE R&D systems Anti-CD337/NKp30 AF29‐4D12 APC Miltenyi Biotec
Intra-cellular staining Anti-Perforin δG9 FITC BD Biosciences
Anti-Granzyme-B GB11 FITC BD Biosciences B Cell-surface staining
Anti-CD19 J3‐119 PC5.5 Beckman Coulter Anti-CD20 B9H9 (HRC20) PB Beckman Coulter Anti-FMC7 FMC7 FITC Beckman Coulter Anti-CD10 ALB1 AF750 Beckman Coulter Anti-CD45 HI30 HV500 BD Biosciences Anti-CD5 L17F12 PE-Cy7 BD Biosciences
Anti-CD23 EBVCS‐5 APC BD Biosciences Anti-CD79b SN8 APC BD Biosciences Anti-CD38 HB7 PE BD Biosciences
Anti Kappa/Lambda polyclonal FITC/PE Dako
Supplemental data 1 : Antibodies used in this study
+
SSC
-A
SSC
-A
CD45-HV500 FSC-A CD19-PC5.5
SSC
-A
Lambda-PE CD79b-APC CD79b-APC CD5-PE.Cy7
Kap
pa-F
ITC
CD
19-P
C5.
5
CD
5-PE
-Cy7
CD
20-P
B
All events Leucocytes Leucocytes
CD19+ Lymphocytes CD19+ Lymphocytes CD19+ Lymphocytes CD19+ Lymphocytes
b
a C
D16
-FIT
C
0 102
103
104
105
0
102
103
104
105
280934.fcs!<PE-Cy7-A>, <APC-A> subset
<APC-A>: CD56
<F
ITC
-A>
: C
D57
0 102
103
104
105
0
102
103
104
105
280936.fcs!<FITC-A>, <APC-A> subset
<APC-A>: CD56
<P
E-A
>: C
D69
0 102
103
104
105
0
102
103
104
105
280952.fcs!<FITC-A>, <APC-A> subset
<APC-A>: CD56
<P
E-A
>: C
D16
0 102
103
104
105
0
102
103
104
105
280934.fcs!FSC-H, SSC-A subset
<PE-Cy7-A>: CD3
<A
PC
-A>
: C
D56
0 50K 100K 150K 200K 250K
0
50K
100K
150K
200K
250K
280952.fcs
FSC-H
SSC-A
0
50
100
150
200
250
150 200 250 100 50 0
FSC-A
SSC
-A
All events Leucocytes
0
CD
56-A
PC
102
103
104
105
0 102 103 104 105
CD3-PE-Cy7
0 102 103 104 105 0 102 103 104 105 0 102 103 104 105
0
102
103
104
105
0
102
103
104
105
0
102
103
104
105
CD56-APC
CD
69-P
E
CD56-APC CD56-APC
CD
57-F
ITC
CD3-CD56dim CD3-CD56dim CD3-CD56dim

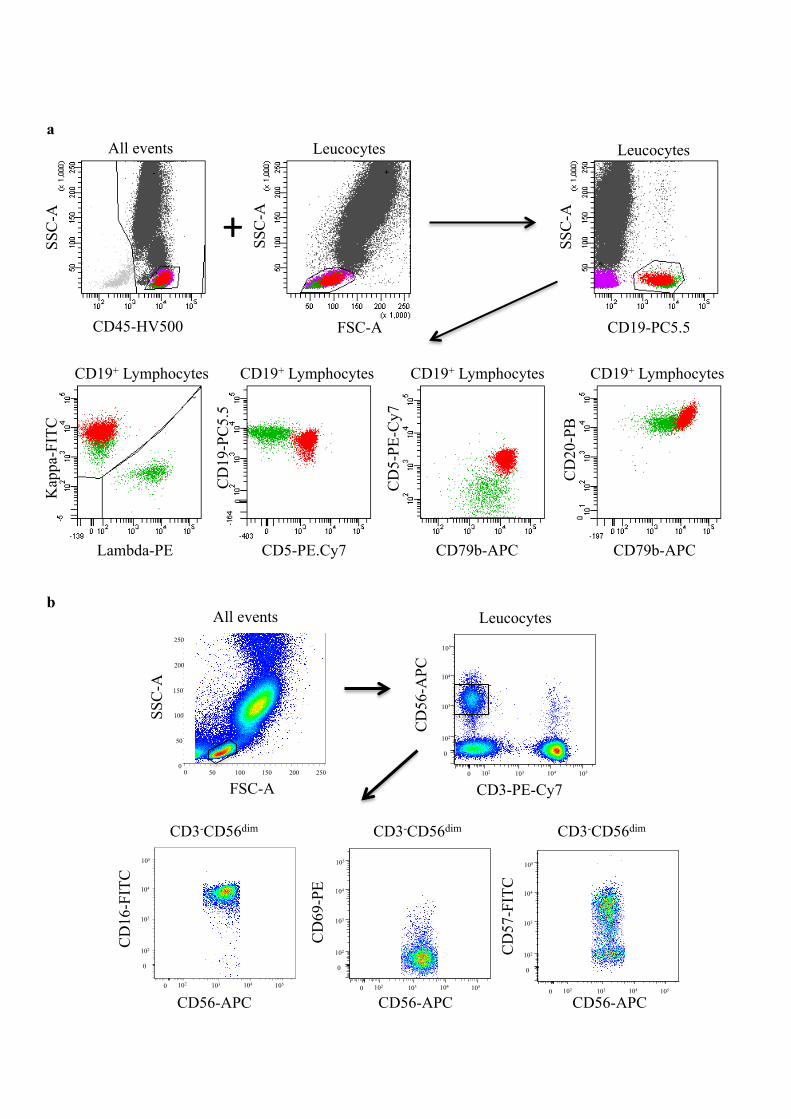
Supplemental data 2. Determina,on of a B‐cell circula,ng clone in WM. Lymphocytes were isolated from peripheral blood samples by ga,ng on the forward (FSC)/side (SSC) scaEers and CD45/SSC. (a) The CD19+ B‐lymphocytes were evaluated for the B‐cell surface markers (Supplemental data 1) for the determina,on of the Matutes/Moreau score, which was less than or equal to 3 for all pa,ents. In this representa,ve case (pa,ent #7, Table 1), the B‐cell circula,ng clone, shown in red, was Kappa+CD5+CD79b+CD20+. This B‐cell clone corresponded to 50% of the peripheral B‐lymphocytes and to 10% of the total lymphocytes. Residual normal B lymphocytes are shown in green. (b). The NK cells were evaluated on the CD3‐CD56+ lymphocy,c gate for the determina,on of a panel of NK‐cell markers (Supplemental data 1), like CD16, CD69 and CD57.
0
25
50
75
100
0
20
40
60
80
% C
D57
+ 0
10 20
40 50
% C
D69
+
30
% C
D16
+
0
25
50
75
100
% P
erfo
rin+
0
25
50
75
100
% G
ranz
yme
B+
b
a
clone (+) clone (-)
T0 T1 T0 T1 clone (+) clone (-)
T0 T1 T0 T1 clone (+) clone (-)
T0 T1 T0 T1
Ctl clone (-) clone (+)
WM
Ctl clone (-) clone (+)
WM
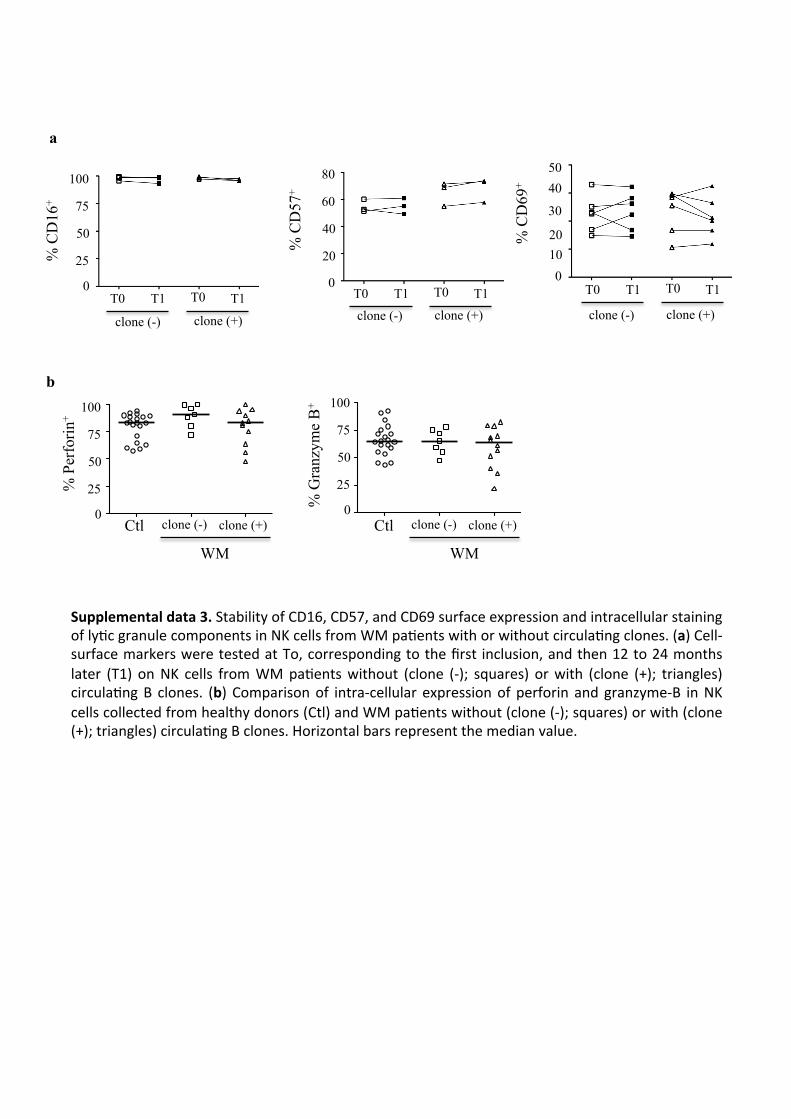
Supplemental data 3. Stability of CD16, CD57, and CD69 surface expression and intracellular staining of ly,c granule components in NK cells from WM pa,ents with or without circula,ng clones. (a) Cell‐surface markers were tested at To, corresponding to the first inclusion, and then 12 to 24 months later (T1) on NK cells from WM pa,ents without (clone (‐); squares) or with (clone (+); triangles) circula,ng B clones. (b) Comparison of intra‐cellular expression of perforin and granzyme‐B in NK cells collected from healthy donors (Ctl) and WM pa,ents without (clone (‐); squares) or with (clone (+); triangles) circula,ng B clones. Horizontal bars represent the median value.
Related Documents











