ORIGINAL PAPER The national DBS brain tissue network pilot study: need for more tissue and more standardization V. Vedam-Mai • N. Krock • M. Ullman • K. D. Foote • W. Shain • K. Smith • A. T. Yachnis • D. Steindler • B. Reynolds • S. Merritt • F. Pagan • J. Marjama-Lyons • P. Hogarth • A. S. Resnick • P. Zeilman • M. S. Okun Received: 26 January 2010 / Accepted: 11 June 2010 / Published online: 30 June 2010 Ó Springer Science+Business Media B.V. 2010 Abstract Over 70,000 DBS devices have been implanted worldwide; however, there remains a pau- city of well-characterized post-mortem DBS brains available to researchers. We propose that the overall understanding of DBS can be improved through the establishment of a Deep Brain Stimulation-Brain Tissue Network (DBS-BTN), which will further our understanding of DBS and brain function. The objec- tives of the tissue bank are twofold: (a) to provide a complete (clinical, imaging and pathological) database for DBS brain tissue samples, and (b) to make available DBS tissue samples to researchers, which will help our understanding of disease and underlying brain cir- cuitry. Standard operating procedures for processing DBS brains were developed as part of the pilot project. Complete data files were created for individual patients and included demographic information, clinical infor- mation, imaging data, pathology, and DBS lead locations/settings. 19 DBS brains were collected from 11 geographically dispersed centers from across the U.S. The average age at the time of death was 69.3 years (51–92, with a standard deviation or SD of 10.13). The male:female ratio was almost 3:1. Average post-mortem interval from death to brain collection was 10.6 h (SD of 7.17). The DBS targets included: subthalamic nucleus, globus pallidus interna, and ventralis intermedius nucleus of the thalamus. In 16.7% of cases the clinical diagnosis failed to match the pathological diagnosis. We provide neuropatho- logical findings from the cohort, and perilead responses to DBS. One of the most important observations made V. Vedam-Mai Á K. D. Foote Á B. Reynolds Á M. S. Okun (&) Department of Neurosurgery, University of Florida, 100 S. Newell Drive, Room L3-100, P.O Box 100236, Gainesville, FL 32610, USA e-mail: [email protected]fl.edu N. Krock Á M. Ullman Á S. Merritt Á A. S. Resnick Á P. Zeilman Á M. S. Okun Department of Neurology, University of Florida, Gainesville, FL, USA W. Shain Á K. Smith Wadsworth Center, Albany, NY, USA D. Steindler Department of Neuroscience, University of Florida, Gainesville, FL, USA A. T. Yachnis Department of Pathology, University of Florida, Gainesville, FL, USA F. Pagan Georgetown University, Washington, DC, USA J. Marjama-Lyons Department of Neurology, University of New Mexico, Albuquerque, NM, USA P. Hogarth Department of Molecular and Medical Genetics, University of Oregon, Eugene, OR, USA 123 Cell Tissue Bank (2011) 12:219–231 DOI 10.1007/s10561-010-9189-1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ORIGINAL PAPER
The national DBS brain tissue network pilot study: needfor more tissue and more standardization
V. Vedam-Mai • N. Krock • M. Ullman • K. D. Foote • W. Shain •
K. Smith • A. T. Yachnis • D. Steindler • B. Reynolds • S. Merritt •
F. Pagan • J. Marjama-Lyons • P. Hogarth • A. S. Resnick • P. Zeilman •
M. S. Okun
Received: 26 January 2010 / Accepted: 11 June 2010 / Published online: 30 June 2010
� Springer Science+Business Media B.V. 2010
Abstract Over 70,000 DBS devices have been
implanted worldwide; however, there remains a pau-
city of well-characterized post-mortem DBS brains
available to researchers. We propose that the overall
understanding of DBS can be improved through the
establishment of a Deep Brain Stimulation-Brain
Tissue Network (DBS-BTN), which will further our
understanding of DBS and brain function. The objec-
tives of the tissue bank are twofold: (a) to provide a
complete (clinical, imaging and pathological) database
for DBS brain tissue samples, and (b) to make available
DBS tissue samples to researchers, which will help our
understanding of disease and underlying brain cir-
cuitry. Standard operating procedures for processing
DBS brains were developed as part of the pilot project.
Complete data files were created for individual patients
and included demographic information, clinical infor-
mation, imaging data, pathology, and DBS lead
locations/settings. 19 DBS brains were collected from
11 geographically dispersed centers from across the
U.S. The average age at the time of death was
69.3 years (51–92, with a standard deviation or SD of
10.13). The male:female ratio was almost 3:1. Average
post-mortem interval from death to brain collection
was 10.6 h (SD of 7.17). The DBS targets included:
subthalamic nucleus, globus pallidus interna, and
ventralis intermedius nucleus of the thalamus. In
16.7% of cases the clinical diagnosis failed to match
the pathological diagnosis. We provide neuropatho-
logical findings from the cohort, and perilead responses
to DBS. One of the most important observations made
V. Vedam-Mai � K. D. Foote � B. Reynolds �M. S. Okun (&)
Department of Neurosurgery, University of Florida,
100 S. Newell Drive, Room L3-100, P.O Box 100236,
Gainesville, FL 32610, USA
e-mail: [email protected]
N. Krock � M. Ullman � S. Merritt � A. S. Resnick �P. Zeilman � M. S. Okun
Department of Neurology, University of Florida,
Gainesville, FL, USA
W. Shain � K. Smith
Wadsworth Center, Albany, NY, USA
D. Steindler
Department of Neuroscience, University of Florida,
Gainesville, FL, USA
A. T. Yachnis
Department of Pathology, University of Florida,
Gainesville, FL, USA
F. Pagan
Georgetown University, Washington,
DC, USA
J. Marjama-Lyons
Department of Neurology, University of New Mexico,
Albuquerque, NM, USA
P. Hogarth
Department of Molecular and Medical Genetics,
University of Oregon, Eugene, OR, USA
123
Cell Tissue Bank (2011) 12:219–231
DOI 10.1007/s10561-010-9189-1

in this pilot study was the missing data, which was
approximately 25% of all available data fields.
Preliminary results demonstrated the feasibility and
utility of creating a National DBS-BTN resource for
the scientific community. We plan to improve our
techniques to remedy omitted clinical/research data,
and expand the Network to include a larger donor pool.
We will enhance sample preparation to facilitate
advanced molecular studies and progenitor cell
retrieval.
Keywords Pathology � Neuromodulation �Devices � Safety � Adverse events �Deep brain stimulation � Parkinson’s disease �Essential tremor � Dystonia
Introduction
A dedicated brain repository with a defined mission for
providing deep brain stimulation (DBS) tissue does not
currently exist. The main objective of such a brain
tissue banking resource would be to facilitate the
availability of high quality samples and data for
research purposes (Alafuzoff and Winblad 1993).
Brain tissue studies provide the important framework
for understanding neurological diseases, as well as for
providing a platform and infrastructure for develop-
ment of interventions (Haroutunian 2007). Presently,
there are only a handful of brain banks that harvest
Parkinson’s disease (PD) tissue, and none have a
specific focus on DBS (e.g. the AZ brain consor-
tium (http://www.azpd.org/), the ‘‘Penn Brain Bank’’;
(http://www.med.upenn.edu/cndr/donatingbrain.shtml),
and the Netherlands Brain Bank to name a few
(http://www.brainbank.nl/)). This critical limitation has
narrowed the scope as well as the overall number of
DBS tissue studies that could potentially address the
question of what determines success and failure in this
procedure.
DBS is a neurosurgical procedure where a small
wire with four lead contacts is inserted into one or two
sides of the brain to address various neurological and
neuropsychiatric disorders (e.g. PD, essential tremor,
dystonia, Tourette syndrome, obsessive compulsive
disease, depression, etc.) that may prove refractory to
standard treatments. DBS acts as a neuromodulatory
therapy, however, its exact mechanisms of action
remain unknown. DBS is a symptomatic treatment,
and its positive and negative effects are com-
pletely reversible (e.g. leads can be removed) and
programmable.
A very important aspect of any tissue resource is
the collection of detailed clinical information. This
information must be paired with high quality neuro-
pathological samples. In the case of DBS, the tissue
samples must also be accompanied by detailed
imaging, and even potentially by intra-operative
neurophysiological data. Additionally, examination
of the tissue studies available on PD-DBS has
revealed major discrepancies between the clinical
and pathological diagnoses (Aalten et al. 2006;
Roulson et al. 2005; Hughes et al. 1992). These
mismatches in clinical versus pathological diagnosis
will be important to better understand, especially
when attempting to evaluate DBS outcome and
mechanism of action.
DBS has largely supplanted lesion therapy (e.g.
pallidotomy, thalamotomy) in most regions of the
world, and has over the last two decades been shown to
be highly effective for addressing medication refrac-
tory movement disorders. DBS in the setting of PD for
example, has proven to be a powerful treatment for
addressing disabling motor fluctuations, and also for
increasing the number of daily hours of quality ‘‘on’’
time for individual sufferers (Weaver et al. 2005).
The most common diagnostic indication for DBS
has been PD, and thus it naturally was the focus of
our pilot DBS brain tissue repository. Although the
cause of PD is poorly understood, it is likely that a
combination of genetic and environmental factors is
involved (Weiner 2008; Hughes et al. 1992). Addi-
tionally, PD is thought not to be a single disease, with
most experts now subscribing to the view that PD is a
syndrome, which in most cases has a largely favor-
able response to dopaminergic therapy. In many
cases, it is believed that an abnormal protein aggre-
gation (e.g. the Lewy Body) feeds a degenerative
cascade which may result in cell dysfunction, and
ultimately cell death within very specific neuronal
populations (e.g. dopaminergic neurons of the sub-
stantia nigra, or a family of parallel segregated basal
ganglia circuits; Delong et al. 1984; Chu et al. 2009).
The diagnosis of PD remains a clinical bedside
endeavor, and it rests largely on the presence
of characteristic features including bradykinesia,
rigidity, gait/postural abnormalities, and a resting
220 Cell Tissue Bank (2011) 12:219–231
123

tremor, although in 20% of cases tremor may be
absent. Post-mortem studies have consistently
revealed that up to a quarter of patients clinically
diagnosed with PD actually had an alternative
pathology (Davie 2008; Zijlmans et al. 2004).
Although over 70,000 DBS devices have been
implanted worldwide (http://www.medtronic.com/
our-therapies/neurostimulators-movement-disorders/
index.htm), there remains a paucity of reports on the
associated pathology. An example of the limited
amount of available data is demonstrated in Table 1.
Mild and non-specific gliosis seem to be the cardinal
themes of all available publications, and most reports
have a common shortcoming—missing detailed clin-
ical information (e.g. standardized scales, pre-opera-
tive and post-operative imaging, and detailed
microscopic analysis). Moreover, there is an over-
riding assumption that DBS leads are well placed, and
that there is only one ‘‘ideal’’ place in each target that
may result in clinical benefit(s).
We are establishing the first comprehensive DBS-
Brain Tissue Network (DBS-BTN), which will make
two essential contributions to the field. First, the
DBS-BTN will provide a database to include critical
clinical, imaging, physiological, and pathological
information. The acquired information will include
basic imaging (which also has the benefit of revealing
any underlying gross brain pathology) as well as a
clear description of the DBS lead track (Fig. 1).
Second, the DBS-BTN will create a catalogue and
storage system to provide opportunities for research-
ers to describe tissue responses (peri-lead, up/down-
stream), in order to more accurately assess
pathological changes associated with the DBS lead(s)
(Fig. 2). The availability of these tissues should allow
the researcher to investigate in greater detail than the
currently available conventional histopathology. Use
of DBS-BTN tissue samples will enable detailed
neuroanatomical studies using various imaging meth-
ods (e.g. MRI, light/confocal microscopy, and elec-
tron microscopy), as well as new investigations of
genomics, proteomics, and progenitor cells from
brain samples (at DBS lead sites as well as in other
brain regions). Thus, the DBS-BTN will enable many
new research initiatives. The DBS-BTN database will
include these ‘‘research data’’ and thus provide a
unique infrastructure to investigate correlations
within a comprehensive clinical database. The pur-
pose of the DBS-BTN was to (1) identify gaps in
information available on DBS brains, (2) establish
standard operating procedures for collection/storage,
and (3) establish a resource for high quality material
in order to facilitate availability of tissue for a clinical
and research network interested in studying DBS. We
present the results from the first 19 brains acquired in
the pilot DBS-BTN, and we highlight lessons learned,
as well as the areas of improvement/cooperation that
will be necessary to make this a higher quality
resource (e.g. a fully functioning DBS-BTN) for the
DBS research community.
Methods
Patient recruitment and the brain donor program
The DBS-BTN pilot project was launched in 2006 by
an interdisciplinary team with the stated intention to
collect post-mortem brains of DBS patients from
within the University of Florida Shands Hospital
System (UF/Shands), as well as from outside DBS
implantation sites. Subjects/donors were prospec-
tively enrolled (IRB approved study) when still
living if possible, but in most cases (particularly
tissue collected outside of the UF/Shands system)
consent was obtained post-mortem.
Tissue acquisition
The first step in tissue acquisition was the notification
of death of a donor. This notification was documented
by several potential sources: family members, doc-
tors, allied health professionals, funeral home direc-
tors, tissue coordinators, hospice, etc. Upon arrival to
the pilot DBS-BTN, each brain received an accession
number, and a general information page was gener-
ated. This information was linked to the accession
number after removal of all personal information to
comply with HIPPA regulations, and this information
was later linked to a database. The post mortem
interval (PMI) for brain tissue removal depended
primarily on the donor’s location (within-town, or
out-of-town), but an attempt was made to keep brain
removal to within 24 h. Appropriate paperwork for
removal had to be verified and signed by family
members/next of kin (similar to the protocol of the
donor program established by Waldvogel et al., at the
University of Auckland, NZ; Waldvogel et al. 2008).
Cell Tissue Bank (2011) 12:219–231 221
123

Table 1 Studies reporting pathological response to DBS electrode
Author Year na Diagnosis Target Laterality Pathology
Boockvar 2000 1 ETb VIMc Bilateral Both stimulators terminated in Vim
Minor reactive changes noted from chronic DBS confined
to electrode tracks
Haberler 2000 8 PDd VIM(6),
STN(2)eBilateral Well-preserved neural parenchyma
Mild gliosis around lead track
Conclusion: Chronic DBS does not cause damage to adjacent brain tissue
Burbaud 2003 1 Chorea VIM Bilateral Minimal tissue damage near electrode tip
Conclusion: DBS has small impact on surrounding tissues
Chou 2004 1 MSAf STN Bilateral Neuron loss in SN and and basal ganglia
Numerous a-synuclein-positive glial cytoplasmic inclusions
in subcortical nuclei, cerebellum, and brainstem
Atypical and robust inflammatory reaction, numerous
glial cytoplasmic inclusions surrounding electrode termination sites
Lezcano 2004 1 MSA STN Bilateral Data not available on PubMed
Talmant 2006 1 MSA STN Bilateral Severe neuronal depletion in SN, but no Lewy bodies
Argyrophilic glial cytoplasmic inclusions positive for a-synuclein and
ubiquitin in the STN, putamen, globus pallidus, pontine nuclei and
cerebellar white matter, significant of MSA
Conclusions: DBS is not recommended for MSA as improvement
is time limited
Sun 2008 1 PD STN/ZIg Bilateral The neural tissue surrounding active and nonactive contacts responds
similarly, with a thin glial capsule and foreign-body giant cell reaction
surrounding the leads as well as piloid gliosis, hemosiderin-laden
macrophages, scattered lymphocytes, and Rosenthal fibers; Separate
tracts in adjacent tissue for intraoperative microelectrode and
semimacroelectrode passes together with reactive gliosis, microcystic
degeneration, and scattered hemosiderin deposition;
Active bilateral contacts used effectively for 6 years lie in the ZI
Guehl 2008 1 PD STN/ZI Bilateral Position of the right electrode track more posterior and less deep
than the left electrode track
Glial reaction due to electrode track visible slightly lateral to the
anterior part of the STN within the ZI & reached external part of the SN
No trace was found through the STN on the preceding or subsequent
histologic sections
The left electrode track passed along the dorsal border of the STN,
continued more medially within the ZI, and stopped in the SN
No trace was found through the STN
Pilitsis 2008 1 Epilepsy Anterior
nucleus
Bilateral Minimal tissue damage, mild astrocytosis, and mild inflammation
surrounding the electrode termination site
Compared to control tissue, no significant difference other than mild
inflammation along the lead track
a Numberb Essential tremorc Ncl ventralis intermedius thalamid Parkinson’s diseasee Subthalamic nucleusf Multiple system’s atrophyg Zona Incerta
222 Cell Tissue Bank (2011) 12:219–231
123

Pathological methods
Fixation and blocking
A Standard Operating Procedure (SOP) was devel-
oped for the DBS-BTN pilot study to standardize the
harvest, collection, and processing of tissue. Per this
SOP, the brain harvest procedure was performed in
the autopsy suite at UF/Shands and the McKnight
Brain Institute if the death occurred in town, or
nearby. If death of a subject occurred out of town, the
brains were removed by outside neuropathologists
following the DBS-BTN protocol. Prior to removal of
the subject’s brain, the DBS lead wires were cut
enabling the DBS leads to be left in the brains with
minimal disruption. Each brain was weighed, and
gross examination was performed by a Board certi-
fied neuropathologist (ATY). Each brain was placed
in a 10% Zn-buffered formalin fixative solution.
After the tissue was completely fixed, usually in
1–2 weeks, the brain was prepared for dissection.
The cerebellum and brainstem were separated at
the level of the caudal brainstem, and the brain was
sectioned in the coronal plane into 3-cm slabs. The
goal of the initial blocking was to obtain a 3 9 3 cm
column of CNS tissue surrounding the lead track.
This ensured that adequate tissue was collected to
study changes in cell and tissue morphology and the
organization around the lead. This procedure allowed
for a clear description of brain tissue changes as a
function of the distance from the lead. We used
available MRIs or CTs to identify the DBS target
(lead tip) and to describe the device trajectory. As
part of the pilot study we obtained post-mortem
imaging information on four brains to identify the
general pathology, and the location/trajectory of the
DBS lead (Fig. 1). The information from imaging in
these cases demonstrated the potential utility of using
these data for planning the brain cutting and obtain-
ing useful samples. Once the tissue columns were
dissected, a series of 1 cm thick tissue blocks were
collected from the surface of the brain until the end of
the lead cavity. All steps of the dissection process
were photographed to ensure accurate tissue block
identification.
Fig. 1 Panel a MRI imaging showing the right DBS lead
terminates in thalamus superior to the intended target of the
STN. Panel b MRI imaging showing that the left sided lead
terminates deeper in the STN/brainstem region. The two slices
reveal that the trajectories were different, and that the antero-
posterior difference in lead placement could not be captured in
the same coronal sections without using multiple MRI slices.
This type of preliminary data has been critical in guiding the
brain cutting procedures. This scan was obtained using a 3T
magnet with overnight imaging (12 h). We can now obtain
similar information using a 1 h inverted MRI T1 sequence for
1 h or less of scan time
Fig. 2 An example of a traditional histopathology section,
showing the DBS lead track within the subthalamic nucleus in
a brain from the UF DBS-BTN pilot
Cell Tissue Bank (2011) 12:219–231 223
123

The tissue block containing the terminal ends of
the lead including the distal most lead contact was
processed by conventional histopathological tech-
niques (Fig. 2). Associated astrocytic gliosis was
assessed by immunohistochemical study for glial
fibrillary acidic protein (GFAP) and in occasional
cases a Masson’s Trichrome stain was performed to
evaluate collagen accumulation near the lead tip.
Representative areas of the brain were sampled, and
embedded in paraffin blocks for pathological analy-
ses. The remaining tissue was stored in the fixative
solution in a covered plastic storage box. The fixative
solution was replaced at least every 6 months.
Immunohistochemistry and pathological methods
Data were recorded for each donor and included the
date, time, and cause of death, age, sex, PMI and DBS
characteristics. For standard pathological examina-
tion, brains received by the DBS-BTN were routinely
dissected from select and standard regions of the brain,
as described previously by the Columbia Brain Bank
Protocol (Vonsattel et al. 2008). These tissue regions
were subject to standard tissue processing, and paraffin
embedding. Paraffin blocks were sectioned at 5 lm,
and were stained with the standard hematoxylin-eosin
(H&E) tissue staining method. For neuropathological
confirmation of neurodegenerative disease diagnosis,
standard immunohistochemistry was performed on
select tissue sections, using antibodies against all, or a
subset of the following proteins: b-amyloid peptide
(1:15 dilution, DAKO M0872), phosphorylated tau
(1:2000 dilution, DAKO A0024), a-synuclein (1:100,
Novocastra NCL-ASYN), and ubiquitin (1:100 dilu-
tion DAKO Z0458) (others employed on a case by case
basis; Spillantini et al. 1997; Schubert et al. 1991;
Perry et al. 1987). Briefly, antigen retrieval was
performed for only a-synuclein by incubating slides
in Trilogy solution (Cell Marque) at 92�C for 25 min.
The histopathological findings were described by a
neuropathologist (ATY) and were based on the
standard, widely accepted criteria for neurodegenera-
tive diseases (Waldvogel et al. 2008; Braak et al. 2001,
2004; McKeith et al. 1996; Schiesling et al. 2008;
Beach et al. 2009). Any additional tissue regions that
were required for the specific diagnosis of a neurode-
generative disorder were by protocol sampled at the
discretion of the trained neuropathologist (Waldvogel
et al. 2006). Tissue samples can be processed for
additional immunohistochemistry (eg: GFAP, Iba1)
and confocal imaging to further our knowledge on
the cellular reactivity produced by lead-tissue
interactions.
Database
Two standardized reports were generated and stored
for each patient based on the results of the gross/
microscopic examinations and other available out-
come data. All medical records were requested for
each patient, and pre-defined fields were populated in
a database. A designated clinical study coordina-
tor collected clinical data. The specific fields were
defined by a group of expert movement disorders
neurologists who examined the plethora of informa-
tion collected on DBS brains, and narrowed the fields
to the most critical for research purposes.
Results
General characteristics of the DBS-BTN pilot
study
Between 2006 and 2009, 19 subjects were enrolled
into the pilot study. Ten of the brains were from
outside the UF system. Brains were logged into the
system and institutional identity was protected during
the data processing procedures. The UF site was the
only site prospectively enrolling potential donors for
this pilot study (other sites retrospectively consented
subjects). Over 60 months, 19 DBS brains were
collected from eleven total sites (including the UF
system).
The age range for the collected brains was 51–
92 years, and the mean age was 69. The average age
for females was 70.5 years (SD = 12.2), and for
males it was 68.9 (SD = 9.9). Males were more
represented (14 vs. 5).
Identification of missing data points
The overarching goal of the pilot DBS-BTN was to
assess needs for a larger DBS-BTN and to specifically
and objectively assess all missing data points (clinical
and pathological) that may have been important for
quantifying outcome. Table 2 summarizes all of the
clinical, imaging, and pathological data points that
224 Cell Tissue Bank (2011) 12:219–231
123

were collected. The table reveals the number of points
available, the number of points missing, and the
percentage of completed items. Strikingly, the data
missing was that from the recording of objective scale
based scores. Predominantly, mini-mental status
examination (MMSE) post-op scores for almost 68%
and MMSE pre-op scores for 27% of the patients were
not recorded. Also Mattis Dementia Rating Scale
(DRS) pre-op scores for 48% and DRS post-op scores
for 74% of the subjects enrolled were unknown.
Further, early and late cognitive and mood related
issues were not known for 16 and 48% of these
patients, respectively. The lack of available clinical
information was significant, and appeared in multiple
domains (see Table 2). Other potentially important
information that was missing included specific details
of lead location and stimulation parameters (almost
45% of this data section was not available), the angle
of the intended lead trajectory, microelectrode and
macroelectrode intraoperative physiology data, and
actual measurements of lead location.
DBS characteristics
The brain areas targeted included the subthalamic
nucleus or STN (n = 19 leads in 12 patients), the
Globus pallidus internus or GPi (n = 9 leads in 6
patients), and the ncl ventralis intermedius thalami or
Vim thalamus (n = 2 leads in 2 patients). Two
patients had two different brain targets implanted
(n = 2 STN, n = 1 Vim thalamus, n = 1 GPi). The
number of months of stimulation varied from 1 to
102, with the average being 35.4 months for the left
side (SD = 22.5), and 41.5 months for the right side
(SD = 29.0).
The lead placement based on available information
was grossly judged (from the combination of avail-
able imaging, clinical response, and pathology) to be
likely accurate in 64.7% of subjects, possibly accu-
rate in 23.5% of the subjects, and inaccurate in 11.8%
of subjects. This determination was made based a
gross determination that the lead reasonably reached
the intended target and also from available clinical
data. Though the exact determination of x, y, z
imaging and pathological correlation of lead loca-
tions was not precisely available on all cases, enough
information was available to make preliminary and
very general determinations of lead locations in all
cases.
Clinical features
Primary clinical diagnosis
The brains were collected from 11 geographically
dispersed centers from across the United States. The
average post-mortem interval for brain removal was
10.8 h. The primary clinical diagnosis was PD
(n = 16; 88.8%), but other diagnoses included multi-
ple system atrophy (n = 1; 5.5%), and essential
tremor (n = 1; 5.5%). The mean disease duration of
the cohort was 18.1 years (SD = 13.5).
Post-operative clinical symptoms
Post DBS surgery, there was a reported improvement
of PD symptoms as perceived by the clinician and by
the patients regardless of diagnosis, or lead place-
ment. This improvement was reported both early
(within the first 6 months) as well as late (chronic). It
is interesting to note that although there was much
clinical discrepancy with the lead placement (12%
inaccurate, and 23.5% possibly accurate), both the
patient and the clinician perceived a significant
improvement following DBS in all cases. Some of
the early (within the first 6 months) cognitive, mood
and behavioral issues encountered in patients
included hallucinations (n = 5), dementia (n = 5),
and impulsivity/compulsions (n = 3). Such early, as
well as late cognitive issues (after the first 6 months)
were poorly documented (47% of data was unavail-
able). These data raise important questions as to the
validity of clinician and patient derived general
outcomes.
Objective scale based scores
A mini-mental status examination (Folstein et al.
1975) is commonly used as a test to screen for
dementia. Usually, a score of greater than or equal to
25 points (Folstein et al. 1975) is considered accept-
able, and anything below may be indicative of
developing or possibly even frank dementia (how-
ever, these cut-offs frequently are oversimplified). In
our pilot study, the pre-operative MMSE data was
available for 74% of patients, however, the post-op
MMSE data was only available for 32%. The DRS
(Mattis dementia rating scale), another test designed
to screen and track the mental state of adults was
Cell Tissue Bank (2011) 12:219–231 225
123
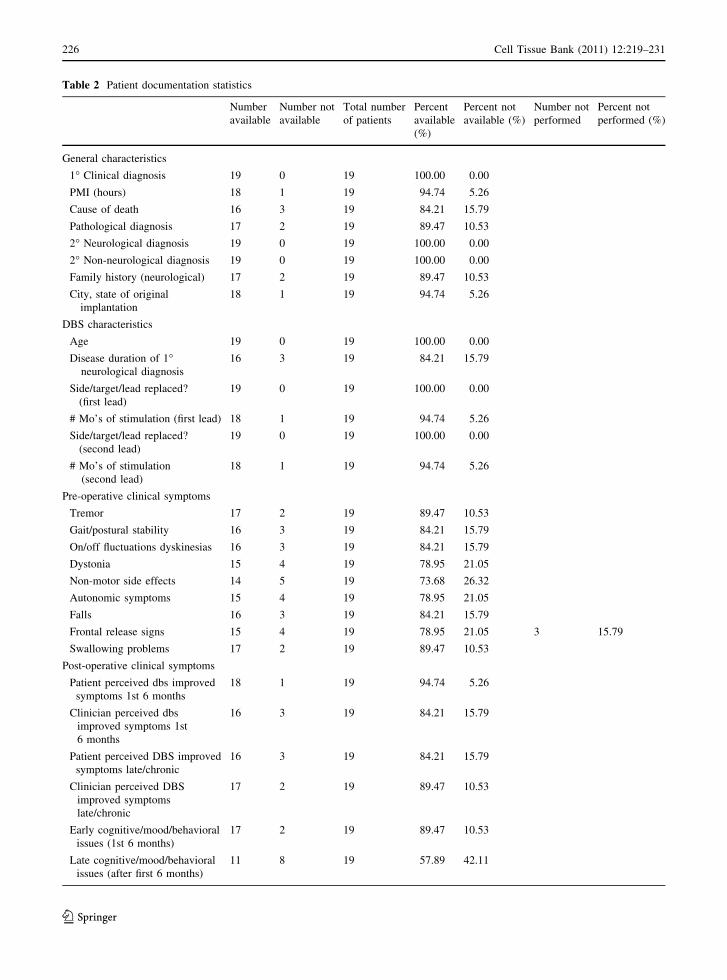
Table 2 Patient documentation statistics
Number
available
Number not
available
Total number
of patients
Percent
available
(%)
Percent not
available (%)
Number not
performed
Percent not
performed (%)
General characteristics
1� Clinical diagnosis 19 0 19 100.00 0.00
PMI (hours) 18 1 19 94.74 5.26
Cause of death 16 3 19 84.21 15.79
Pathological diagnosis 17 2 19 89.47 10.53
2� Neurological diagnosis 19 0 19 100.00 0.00
2� Non-neurological diagnosis 19 0 19 100.00 0.00
Family history (neurological) 17 2 19 89.47 10.53
City, state of original
implantation
18 1 19 94.74 5.26
DBS characteristics
Age 19 0 19 100.00 0.00
Disease duration of 1�neurological diagnosis
16 3 19 84.21 15.79
Side/target/lead replaced?
(first lead)
19 0 19 100.00 0.00
# Mo’s of stimulation (first lead) 18 1 19 94.74 5.26
Side/target/lead replaced?
(second lead)
19 0 19 100.00 0.00
# Mo’s of stimulation
(second lead)
18 1 19 94.74 5.26
Pre-operative clinical symptoms
Tremor 17 2 19 89.47 10.53
Gait/postural stability 16 3 19 84.21 15.79
On/off fluctuations dyskinesias 16 3 19 84.21 15.79
Dystonia 15 4 19 78.95 21.05
Non-motor side effects 14 5 19 73.68 26.32
Autonomic symptoms 15 4 19 78.95 21.05
Falls 16 3 19 84.21 15.79
Frontal release signs 15 4 19 78.95 21.05 3 15.79
Swallowing problems 17 2 19 89.47 10.53
Post-operative clinical symptoms
Patient perceived dbs improved
symptoms 1st 6 months
18 1 19 94.74 5.26
Clinician perceived dbs
improved symptoms 1st
6 months
16 3 19 84.21 15.79
Patient perceived DBS improved
symptoms late/chronic
16 3 19 84.21 15.79
Clinician perceived DBS
improved symptoms
late/chronic
17 2 19 89.47 10.53
Early cognitive/mood/behavioral
issues (1st 6 months)
17 2 19 89.47 10.53
Late cognitive/mood/behavioral
issues (after first 6 months)
11 8 19 57.89 42.11
226 Cell Tissue Bank (2011) 12:219–231
123

Table 2 continued
Number
available
Number not
available
Total number
of patients
Percent
available
(%)
Percent not
available (%)
Number not
performed
Percent not
performed (%)
Objective scale based scores
Pre-Op DRS 10 9 19 52.63 47.37 1 5.26
Post-Op DRS 5 14 19 26.32 73.68 2 10.53
Pre-Op MMSE 14 5 19 73.68 26.32 1 5.26
Post-Op MMSE 6 13 19 31.58 68.42 1 5.26
Pre-Op DSM IV 4 15 19 21.05 78.95 9 47.37
Post-Op DSM IV 4 15 19 21.05 78.95 9 47.37
UPDRS baseline OFF 15 4 19 78.95 21.05
UPDRS baseline ON 13 6 19 68.42 31.58
UPDRS baseline off/on med
improvement
12 7 19 63.16 36.84
UPDRS baseline off/longest
follow-up off meds/On DBS
13 6 19 68.42 31.58
UPDRS baseline off/longest
follow-up on med/On DBS
13 6 19 68.42 31.58
TRS baseline 1 1 2 50.00 50.00 1 50.00
TRS baseline/longest follow-up
off DBS
1 1 2 50.00 50.00 1 50.00
TRS baseline/longest follow-up
on DBS
1 1 2 50.00 50.00 1 50.00
Lead location and stimulation parameters #1
Side-target 19 0 19 100.00 0.00
Stimulation parameters 19 0 19 100.00 0.00
AC-PC angle 13 6 19 68.42 31.58
Microelectrode passes 10 9 19 52.63 47.37
Macroelectrode passes 10 9 19 52.63 47.37
Measured lead tip location 12 7 19 63.16 36.84
0 Contact location 14 5 19 73.68 26.32
1 Contact location 13 6 19 68.42 31.58
2 Contact location 13 6 19 68.42 31.58
3 Contact location 13 6 19 68.42 31.58
Lead location and stimulation parameters #2
Side-target 12 0 12 100.00 0.00
Stimulation parameters 12 0 12 100.00 0.00
AC-PC angle 6 6 12 50.00 50.00
Microelectrode passes 2 10 12 16.67 83.33
Macroelectrode passes 3 9 12 25.00 75.00
Measured lead tip location 7 5 12 58.33 41.67
0 Contact location 8 4 12 66.67 33.33
1 Contact location 6 6 12 50.00 50.00
2 Contact location 6 6 12 50.00 50.00
3 Contact location 6 6 12 50.00 50.00
Cell Tissue Bank (2011) 12:219–231 227
123

available for only part of the cohort. A score below
130 is noteworthy. The DRS scores were available
for only 53%/73% of the subjects with respect to pre-
and post-operative screenings.
Pathological features
Pathological assessment (clinical and pathological
mismatches)
The majority of the patients were diagnosed clinically
with idiopathic PD (Braak et al. 2003). The patho-
logical diagnosis failed to correlate with the clinical
diagnosis in 3/19 cases (15.78%). The clinical
diagnosis for one of the patients was determined to
be multiple system atrophy, however, upon patho-
logical examination it was shown that the subject
actually had idiopathic PD with diffuse Lewy body
deposition (McKeith et al. 1996). Of the other two
subjects, both had multiple system atrophy at post-
mortem examination.
One patient had a severe loss of nigral cells, but
did not exhibit any Lewy Bodies or neurofibrillary
pathology. This patient had a family history of PD
and we suspect carried one of the PD genes (e.g.
Parkin, or a LRRK2 variant; Schiesling et al. 2008).
This was a significant observation as the patient was
clinically diagnosed with PD, and had a tremendous
response to levodopa and to DBS therapy.
The primary cause of death of the subjects enrolled
in our pilot study was variable: myocardial infarction
(n = 4, 21%), respiratory arrest (n = 3, 15.8%), organ
failure (n = 2, 10.5%), cancer (n = 2, 10.5%), anoxic
brain injury (n = 1, 5.2%), drowning (n = 1, 5.2%),
car accident (n = 1, 5.2%), and stroke (n = 1, 5.2%).
Forty-two percent lacked a family history of any
neurological disorder. The most common ailment for
those with a positive family history was PD (26.3%).
Other neurological comorbidities included essential
tremor (10.5%), depression (5.2%), stroke (5.2%), and
dementia (5.2%).
Pathological and peri-lead responses
Neuropathologically the cohort of brains revealed the
following: cortical Lewy Bodies (n = 5), changes
indictative of Alzheimer’s (n = 1), changes indica-
tive of hypoxic-ischemic encephalopathy (n = 2),
Fig. 3 A representative sample of the cellular reactive
responses seen at a DBS lead site. A confocal image taken
from a 100 lm thick tissue section. The image is from the STN
containing the DBS lead site (DBS SITE). Immunohistochem-
istry shows astrocytes (GFAP = magenta), microglia (Iba-
1 = cyan), and all cell nuclei (CyQuant = yellow). The
microglia (white arrows) seen throughout the image are in an
amoeboid reactive state. The astrocytes (white arrow heads)
are also reactive with extended and enlarged processes.
The astrocytes and microglia can be seen in layers around
the DBS site. The field denoted by asterisks shows a large
blood vessel coursing into the area near the lead site.
Calibration bar = 100 lm
Table 2 continued
Number
available
Number not
available
Total number
of patients
Percent
available
(%)
Percent not
available (%)
Number not
performed
Percent not
performed (%)
Pathological response around DBS lead
Pathological response around
DBS lead
17 2 19 89.47 10.53
Lead location clinical 13 6 19 68.42 31.58
228 Cell Tissue Bank (2011) 12:219–231
123

nigrostriatal degeneration with oligodendroglial
inclusions (2), and one PD brain with nigral degen-
eration but no Lewy Bodies (n = 1). An example of
the results of the techniques employed can be seen in
Fig. 3, showing both reactive astrocytes and reactive
microglia relative to the DBS lead site. These data
reveal that the reactive gliosis (astrocytes and microg-
lia) is oriented in layers surrounding the DBS lead
site. Post-mortem histological analysis revealed that
in all the subjects except for one, the peri-lead
pathological response was minimal, and was primarily
gliosis. This tissue specimen showed the most
dramatic response to the DBS lead. A thick fibro-
collagenous wall was discovered around the DBS
lead, which was associated with chronic inflamma-
tion. This observation can be further confirmed by
techniques such as Masson’s trichrome staining. The
peri-lead pathological response was also evaluated
and the following characteristics were uncovered:
gliotic cuffing (n = 3), an organized cavity with a
mild astrocytic response (mainly microglia; n = 8;
Fig. 3), mild hemorrhage at the lead site (n = 3), peri-
lead stroke (n = 1), organizing cortical necrosis at the
lead insertion site (probable prior hemorrhage;
n = 3), and the formation of a fibrocollagenous wall
of chronic inflammation (as confirmed by Masson’s
trichrome stain; n = 1).
Discussion
DBS is becoming an increasingly important therapy
for a wide variety of movement disorders. This report
presents the initial pilot findings from 19 brain
samples utilized to establish a National Pilot DBS-
BTN. The preliminary results demonstrated the fea-
sibility of such a tissue bank for the preparation, and
storage of DBS brain specimens, but also revealed
shortcomings particularly in obtaining complete clin-
ical datasets. The data revealed the post-mortem
cohort on average was close to age 70, and there was a
larger than expected preponderance of men (2:1 is the
usual male to female disease ratio, and in our study it
was almost 3:1. The most common clinical diagnosis
was PD (89%), and post-mortem examination
revealed (similar to non-DBS studies) diagnostic
mismatch in three cases (18%). The primary brain
target utilized was STN (n = 19 leads) and lead
placement was grossly inaccurate in 12% of the
cohort, despite patient and clinician reports of signif-
icant benefit. In general, our data supports the results
of previous post-mortem studies, which have shown
that a glial response (e.g. mild inflammation) is
consistently generated to DBS leads (Sun et al. 2008;
Nielsen et al. 2007; Haberler et al. 2000; Henderson
et al. 2002). Interestingly we were able to observe a
few cases of peri-lead inflammatory cuffing, as well as
cortical and peri-lead hemorrhage/stroke.
This pilot study revealed some important suc-
cesses and failures that will need to be addressed in
the future. Perhaps the most important observation
was the missing data rate which of almost 25% of all
data fields sought by investigators (Table 2). In total,
the relatively small dataset sought by the pilot
investigators proved extremely hard to obtain across
11 centers. The future success of the DBS-BTN will
therefore be highly dependent on limiting the lack of
missing data, and also by introducing standardization
of collection instruments and techniques.
There were several important successes derived
from this project. There was an establishment of a DBS
SOP for the preparation of brain tissue. Establishing
such a standardized protocol enabled the generation of
high quality tissue, which was essential for the
maintenance of a systematic histological review of
brain regions. In order to ensure that our samples were
suitable for further use, the collection, dissection, and
processing of samples were carried out only by an
experienced and qualified multidisciplinary team.
Additionally, we developed a clinico-pathological-
imaging post-mortem DBS database, a protocol to
preserve tissue for proteomics/genomics, and a proto-
col to preserve and grow post-mortem cells from
various brain regions (both cells and progenitor/stem
cells). The pilot DBS-BTN was also successful in the
collection of 19 post-mortem DBS brains from 11
different geographical locations/implanting centers
throughout the United States. The study defined a
SOP for brain fixation, and generation of basic
histological profiles, and it developed a quick and
simple 3T MRI sequence to examine post-mortem
DBS brains. The imaging development was important
for describing the lead trajectory, as well as for
describing the position of the DBS lead tips prior to the
brain cutting sessions. This information allowed us to
refine our brain cutting technique and facilitated the
availability of a larger amount of useful tissue. To our
knowledge there have been no post mortem MRI
Cell Tissue Bank (2011) 12:219–231 229
123

studies of human brain confirming lead position. These
studies can be hampered by artifacts and by fixation
issues once the brain has been removed from the skull.
Usually histological sectioning approaches are utilized
for localization, however, these techniques in isolation
often fail to provide an accurate picture of lead
location. Although we had some CT and MRI images
pre-mortem, post-mortem imaging, histology, and
information on clinical outcome, it is not clear that
this was enough to justify the classification of lead
placement/misplacement we used for this paper. This
component of the repository will need to be addressed
in the future in lieu of establishing a correlation
between lead placement and patient’s/clinician’s per-
ception of the DBS procedure.
There were several important failures that can be
improved upon. One failure was in systematically
keeping the PMI’s as short as possible. Some
biomarkers have relatively short half-lives, and
specific antigenicity that can be lost over time.
Typically, advanced studies requiring fresh tissue
involve RNA (such as gene expression studies), and it
is crucial that the PMI be as short as possible
(typically \ 24 h). The range of studies that a
specific tissue donation can support differs from
one sample to another (Haroutunian and Pickett
2007), and we need to attempt to maximize this
range. The DBS BTN utilizes a system where we
attempt to pre-morbidly consent subjects, although
when not possible or feasible we utilize post-mortem
consenting.
Forming a more integrated network and adopting
common institutional protocols/procedures as well as
collecting a common dataset will be critical for the
future of the DBS-BTN. New molecular research
techniques for gene and protein expression studies
will require the use of snap-frozen tissue, and we will
need to begin to routinely collect this material. Even
though the use of frozen tissue has limitations (such
as the need for a shorter PMI, proper freezing
techniques and appropriate storage and handling), the
studies of gene and corresponding protein expression
can best be performed with appropriately frozen
specimens (Schmitt et al. 2007). Immunohistochem-
ical methods using specific antibodies usually work
best on tissue that has been formalin-fixed/paraffin
embedded material. For our future tissue collections
and SOPs, we plan to broaden our procedures to
include both fixed as well as frozen materials.
It is our hope that in the future we will be able to
offer other researchers our tissue resources as well as
clinical databases in a collaborative manner, in order
to further the understanding of DBS, PD and other
diseases potentially addressed by neuromodulation.
Acknowledgments This work was supported by the Adelaide
Lackner Professorship to MSO, The University of Florida
Foundation Funds, The Eric and Jennifer Scott Fund, the
National Parkinson Foundation Center of Excellence, and NIH
(R01-NS044287 to WS). We would also like to thank the
members of the NPF DBS Working Group for their contributions
and the Wadsworth Center Advanced Microscopy and Image
Analysis Core facility for their contributions. This study has
Institutional Review Board (UF-IRB) approval for use and the
IRB# is: 130-2008.
References
Aalten CM, Samson MM, Jansen PA (2006) Diagnostic errors;
the need to have autopsies. Neth J Med 64(6):186–190
Alafuzoff I, Winblad B (1993) How to run a brain bank: poten-
tials and pitfalls in the use of human post-mortem brain
material in research. J Neural Transm Suppl 39:235–243
Beach TG, Adler CH, Lue L, Sue LI, Bachalakuri J, Henry-
Watson J, Sasse J, Boyer S, Shirohi S, Brooks R, Esc-
hbacher J, White CL 3rd, Akiyama H, Caviness J, Shill
HA, Connor DJ, Sabbagh MN, Walker DG (2009) Unified
staging system for Lewy body disorders: correlation with
nigrostriatal degeneration, cognitive impairment and
motor dysfunction. Acta Neuropathol 117:613–634
Braak E, Sandmann-Keil D, Rub U, Gai WP, de Vos RA, Steur
EN, Arai K, Braak H (2001) Alpha-synuclein immuno-
positive Parkinson’s disease-related inclusion bodies in
lower brain stem nuclei. Acta Neuropathol 101(3):195–201
Braak H, Del Tredici K, Rub U, de Vos RA, Jansen Steur EN,
Braak E (2003) Staging of brain pathology related to
sporadic Parkinson’s disease. Neurobiol Aging 24:197–
211
Braak H, Ghebremedhin E, Rub U, Bratzke H, Del Tredici K
(2004) Stages in the development of Parkinson’s disease-
related pathology. Cell Tissue Res 318(1):121–134
Chu Y, Dodiya H, Aebischer P, Olanow CW, Kordower JH
(2009) Alterations in lysosomal and proteasomal markers
in Parkinson’s disease: relationship to alpha-synuclein
inclusions. Neurobiol Dis 35:385–398
Davie CA (2008) A review of Parkinson’s disease. Br Med
Bull 86:109–127
Delong MR, Georgopoulos AP, Crutcher MD, Mitchell SJ,
Richardson RT, Alexander GE (1984) Functional orga-
nization of the basal ganglia: contributions of single-cell
recording studies. Ciba Found Symp 107:64–82
Folstein MF, Folstein SE, McHugh PR (1975) Mini-mental
state. A practical method for grading the cognitive state of
patients for the clinician. J Psychiatr Res 12:189–198
Haberler C, Alesch F, Mazal PR, Pilz P, Jellinger K, Pinter
MM, Hainfellner JA, Budka H (2000) No tissue damage
230 Cell Tissue Bank (2011) 12:219–231
123

by chronic deep brain stimulation in Parkinson’s disease.
Ann Neurol 48:372–376
Haroutunian V, Pickett J (2007) Autism brain tissue banking.
Brain Pathol 17:412–421
Henderson JM, Pell M, O’Sullivan DJ, McCusker EA, Fung
VS, Hedges P, Halliday GM (2002) Postmortem analysis
of bilateral subthalamic electrode implants in Parkinson’s
disease. Mov Disord 17:133–137
Hughes AJ, Daniel SE, Kilford L, Lees AJ (1992) Accuracy of
clinical diagnosis of idiopathic Parkinson’s disease: a
clinico-pathological study of 100 cases. J Neurol Neuro-
surg Psychiatry 55:181–184
McKeith IG et al (1996) Consensus guidelines for the clinical
and pathologic diagnosis of dementia with Lewy bodies
(DLB): report of the consortium on DLB international
workshop. Neurology 47:1113–1124
Nielsen MS, Bjarkam CR, Sorensen JC, Bojsen-Moller M,
Sunde NA, Ostergaard K (2007) Chronic subthalamic
high-frequency deep brain stimulation in Parkinson’s
disease—a histopathological study. Eur J Neurol 14:
132–138
Perry G, Friedman R, Shaw G, Chau V (1987) Ubiquitin is
detected in neurofibrillary tangles and senile plaque neu-
rites of Alzheimer disease brains. Proc Natl Acad Sci
USA 84:3033–3036
Roulson J, Benbow EW, Hasleton PS (2005) Discrepancies
between clinical and autopsy diagnosis and the value of
post mortem histology; a meta-analysis and review. His-
topathology 47(6):551–559
Schiesling C, Kieper N, Seidel K, Kruger R (2008) Review:
familial Parkinson’s disease—genetics, clinical phenotype
and neuropathology in relation to the common sporadic
form of the disease. Neuropathol Appl Neurobiol 34:
255–271
Schmitt A et al (2007) How a neuropsychiatric brain bank
should be run: a consensus paper of Brainnet Europe II. J
Neural Transm 114:527–537
Schubert W, Prior R, Weidemann A, Dircksen H, Multhaup G,
Masters CL, Beyreuther K (1991) Localization of Alz-
heimer beta A4 amyloid precursor protein at central and
peripheral synaptic sites. Brain Res 563:184–194
Spillantini MG, Schmidt ML, Lee VM, Trojanowski JQ, Jakes
R, Goedert M (1997) Alpha-synuclein in Lewy bodies.
Nature 388:839–840
Sun DA, Yu H, Spooner J, Tatsas AD, Davis T, Abel TW, Kao
C, Konrad PE (2008) Postmortem analysis following
71 months of deep brain stimulation of the subthalamic
nucleus for Parkinson disease. J Neurosurg 109:325–329
Vonsattel JP, Amaya Mdel P, Cortes EP, Mancevska K, Keller
CE (2008) Twenty-first century brain banking: practical
prerequisites and lessons from the past: the experience of
New York Brain Bank, Taub Institute, Columbia Uni-
versity. Cell Tissue Bank 9:247–258
Waldvogel HJ, Curtis MA, Baer K, Rees MI, Faull RL (2006)
Immunohistochemical staining of post-mortem adult
human brain sections. Nat Protoc 1:2719–2732
Waldvogel HJ, Bullock JY, Synek BJ, Curtis MA, van Roon-
Mom WM, Faull RL (2008) The collection and processing
of human brain tissue for research. Cell Tissue Bank
9:169–179
Weaver F, Follett K, Hur K, Ippolito D, Stern M (2005) Deep
brain stimulation in Parkinson disease: a metaanalysis of
patient outcomes. J Neurosurg 103:956–967
Weiner WJ (2008) There is no Parkinson disease. Arch Neurol
65:705–708
Zijlmans JC, Daniel SE, Hughes AJ, Revesz T, Lees AJ (2004)
Clinicopathological investigation of vascular parkinson-
ism, including clinical criteria for diagnosis. Mov Disord
19:630–640
Cell Tissue Bank (2011) 12:219–231 231
123
Related Documents











