The Leprosy Asylum in India: 1886 – 1947 JO ROBERTSON* ABSTRACT . Writing against a historical practice that situates the leprosy asylum exclusively within prison-like institutions, this article seeks to show the variation in leprosy asylums, the contingencies of their evo- lution, and the complexity of their designs, by devoting attention to the characteristics of the leprosy asylum in India from 1886 to 1947, in par- ticular to the model agricultural colony. Drawing upon the travel narra- tives of Wellesley Bailey, the founder of the Mission to Lepers in India, for three separate periods in 1886, 1890 – 91, and 1895 – 96, it argues that leprosy asylums were formed in response to a complex conjunction of impulses: missionary, medical, and political. At the center of these endea- vors was the provision of shelter for persons with leprosy that accorded with principles of good stewardship and took the form of judicious use of donations provided by benefactors. As the Mission to Lepers began to bring about improvements and restructuring to asylums, pleasant sur- roundings, shady trees, sound accommodation, and good ventilation became desirable conditions that would confer physical and psychological benefits on those living there. At the same time, the architecture of the asylum responded to economic imperatives, in addition to religious and medical aspirations, and asylums moved towards the regeneration of a labor force. Leprosy-affected people were increasinglyemployed in occu- pations that contributed to their sustenance and self-sufficiency, symboli- cally reincorporating the body damaged by leprosy into the economic world of productive relations. KEYWORDS: leprosy asylum, India, agricul- tural colony, built environment, Mission to Lepers, economy, labor. * Institut d’Histoire de la Me ´decine et de la Sante ´, Centre Me ´dicale Universitaire (CMU), Case postale, CH – 1211 Gene `ve 4, Switzerland and 3 Ovendean St., Yeronga, Brisbane, Queensland, Australia 4104. Email: [email protected]. This research was conducted using funding from both the Nippon Foundation and the Sasakawa Memorial Health Foundation, through WHO and the International Leprosy Association, while I was based at the Wellcome Unit for the History of Medicine at Oxford from 2001 to 2007. JOURNAL OF THE HISTORY OF MEDICINE AND ALLIED SCIENCES, Volume 64, Number 4 # The Author 2009. Published by Oxford University Press. All rights reserved. For permissions, please e-mail: [email protected] Advance Access publication on June 16, 2009 doi:10.1093/jhmas/jrp014 [ 474 ] at UQ Library on August 10, 2015 http://jhmas.oxfordjournals.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The Leprosy Asylum in India: 1886–1947
JO ROBERTSON*
ABSTRACT. Writing against a historical practice that situates the leprosyasylum exclusively within prison-like institutions, this article seeks toshow the variation in leprosy asylums, the contingencies of their evo-lution, and the complexity of their designs, by devoting attention to thecharacteristics of the leprosy asylum in India from 1886 to 1947, in par-ticular to the model agricultural colony. Drawing upon the travel narra-tives of Wellesley Bailey, the founder of the Mission to Lepers in India,for three separate periods in 1886, 1890–91, and 1895–96, it argues thatleprosy asylums were formed in response to a complex conjunction ofimpulses: missionary, medical, and political. At the center of these endea-vors was the provision of shelter for persons with leprosy that accordedwith principles of good stewardship and took the form of judicious use ofdonations provided by benefactors. As the Mission to Lepers began tobring about improvements and restructuring to asylums, pleasant sur-roundings, shady trees, sound accommodation, and good ventilationbecame desirable conditions that would confer physical and psychologicalbenefits on those living there. At the same time, the architecture of theasylum responded to economic imperatives, in addition to religious andmedical aspirations, and asylums moved towards the regeneration of alabor force. Leprosy-affected people were increasingly employed in occu-pations that contributed to their sustenance and self-sufficiency, symboli-cally reincorporating the body damaged by leprosy into the economicworld of productive relations. KEYWORDS: leprosy asylum, India, agricul-tural colony, built environment, Mission to Lepers, economy, labor.
* Institut d’Histoire de la Medecine et de la Sante, Centre Medicale Universitaire(CMU), Case postale, CH – 1211 Geneve 4, Switzerland and 3 Ovendean St., Yeronga,Brisbane, Queensland, Australia 4104. Email: [email protected].
This research was conducted using funding from both the Nippon Foundation and theSasakawa Memorial Health Foundation, through WHO and the International LeprosyAssociation, while I was based at the Wellcome Unit for the History of Medicine atOxford from 2001 to 2007.
JOURNAL OF THE HISTORY OF MEDICINE AND ALLIED SCIENCES, Volume 64, Number 4
# The Author 2009. Published by Oxford University Press. All rights reserved.For permissions, please e-mail: [email protected] Access publication on June 16, 2009 doi:10.1093/jhmas/jrp014
[ 474 ]
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

Before us is a wide stretch of tall green trees with little buildings, red andbuff and white, peeping through, and the little steeple of a church risingabove all. This is the first glimpse of the asylum, splendidly situated, withopen, wind-swept country all around. There are no walls to give it an airof confinement, and if one had no knowledge of the nature of the placeand of the suffering that is so patiently endured within its boundaries, onemight exclaim: “What a fortunate little community!”1
In contrast to this 1922 description of the leprosy asylum atPurulia, in Western Bengal, leprosy asylums in other places havegarnered an impressive reputation as sites of isolation and suffer-
ing. As part of his study of insanity in the Age of Reason, MichelFoucault famously described these places of seclusion in Europe: “Inthe margins of the community, at the gates of cities, there stretchedwastelands which sickness had ceased to haunt but had left sterile andlong uninhabitable. For centuries, these reaches would belong to thenon-human. . . . Leprosy withdrew, leaving derelict these low places.”2
These two descriptions, the one, reminiscent of an Englishvillage, the other, conjuring the echoing spaces of a gothic wilder-ness, use the economics of “space” in order to describe the placeswhere people with leprosy lived. The Indian one presents a pano-rama that balances the built environment with “open, windsweptcountry” so as to demonstrate the success of the work done by theMission to Lepers in India; Foucault evokes the emptiness of unin-habitable wastelands in order to describe the space vacated byleprosy in the medieval period.
More recently, in his analysis of institutions of “enclosure” incolonial and imperial settings, Rod Edmond has described theleprosy asylum as a “brutally literal form” of detention established
1. Mission to Lepers, The Forty-Eighth Annual Report of the Mission to Lepers. “A FruitfulField” (London: Botolph Printing, 1922), 12. The term “leper” carries demeaning anddehumanizing connotations that have a devastating impact on people affected by leprosy. Ihave attempted to avoid the use of this word in all instances except when directly quotingan historical document, the title of an organization, or the name of an asylum.
2. Michel Foucault, Madness and Civilization: A History of Insanity in the Age of Reason(New York: Random House, 1988), 3–6. Arguing metaphorically as well as literally,Foucault suggests that once the medieval lazaretto was vacated by leprosy, the space wasgiven over to “unreason.” In spite of this argument, the disease persisted in pockets, inEurope, over the next three hundred years. Carole Rawcliffe successfully contests the his-torical accuracy and persistence of the nineteenth-century orthodoxies of the disappear-ance of medieval leprosy. At that time it was argued that the disappearance of the diseasecame about as a result of segregation. See Rawcliffe, Leprosy in Medieval England (London:Boydell and Brewer, 2006).
Robertson : The Leprosy Asylum in India 475
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

in an attempt to protect the metropolis and the colonizer “from theworld they were colonizing.”3 As places of detention, he believes,leprosy asylums were subsequently adapted and applied to the colo-nized and then, in turn, to members of the imperial population.4
Edmond bases his analysis on Molokai, in Hawaii (established in1866), Robben Island (1846), South Africa, and the islands ofdetention in Australia (1889, 1891, 1907) and New Zealand (1903).5
In assessing Edmond’s claim, it is important to realize that the siteson which his case is based were representative of the earliest phaseof the establishment of many hundreds of leprosy asylums through-out the world. The asylums he refers to are, in fact, at one end of ahistorical continuum stretching into the mid-twentieth century.6
In addition, leprosy asylums that were established in any onedecade, such as those built after the first international leprosy con-ference in Berlin in 1897, or even those after the first internationalleprosy congress in Cairo in 1938, were not uniform in style andcharacter. As the Leprosy Commission of the League of Nationsconcluded, after an extensive world-wide survey in 1931, asylumsreflected the character of the society and culture in which theywere established.7
The leprosy asylum in the nineteenth and the twentieth centuriesneeds to be differentiated as a site, both historically and geographi-cally. The variation in asylums, the contingencies of their evolution,
3. Rod Edmond, Leprosy and Empire: Medical and Cultural History (New York:Cambridge University Press, 2006), 20–21.
4. Ibid., 20–22.5. In Hawaii, legislation was introduced on 3 January 1865 to prevent the spread of the
disease. Land on the island of Molokai was purchased for the first contingent ofleprosy-affected people, who were shipped there on 6 January 1866. Legislation for thecompulsory institutionalization of all people with leprosy was introduced into the CapeColony in 1891. For a discussion of this see Harriet Deacon, “Racial Segregation andMedical Discourse in Nineteenth-Century Cape Town,” J. Southern Afr. Stud., 1996, 22,287–308. There were also sites of detention at Little Bay in Sydney, New South Wales,and Derby in Western Australia. Edmond, Leprosy and Empire, 143–77.
6. See database search for “Leprosarium” at http://www.leprosyhistory.org. Withoutquestion, there were hellholes. For example, the Chinese who were, without benefit ofthe law, exiled to Dayman Island, in the Torres Straits, in 1889, almost certainly died ofexposure or starvation.
7. League of Nations: Health Organization, The Principles of the Prophylaxis of Leprosy:First General Report of the Leprosy Commission (Geneva: Publications Department of theLeague of Nations, 1931). “The isolation of lepers should be carried out in accordancewith the circumstances prevailing in the countries involved,” 6. As a result, leprosy asylumsnow provide eloquent indices of the specific socio-economic and cultural circumstances inwhich they were built.
Journal of the History of Medicine : Vol. 64, October 2009476
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

and the complexity of their designs remain to be explored. Between1856, when the hospital asylums of Norway were established, andthe first decade of the twentieth century, when the model leprosycolony of Culion, in the Philippines, was built, important changestook place in the idea of what a leprosy asylum should be. By thetime of the Cairo Congress in 1938, it was clear that the focus ofexpertise had shifted from the imperial centers to the colonies.
While this article emphasizes the geographical specificity ofleprosy asylums, it will do so within an understanding of the inter-national circulation of information about leprosy control andasylum creation. Medical and governmental authorities who wereinterested in leprosy shared information so that connections weremade across national borders and colonial empires. For example,questionnaires on leprosy were sent to the colonies by the RoyalCollege of Physicians of London in order to gauge the characterand progress of the disease following on a request in 1862 by theGovernor-in-Chief of the Windward Isles, James Walker.8
Responses were gathered from the West Indies, China, Japan, India,Africa, the Middle East, and European and Mediterranean countriesand these were published in its 1867 Report on Leprosy by the RoyalCollege of Physicians.9 This publication was then circulated through-out the British colonies. The first international leprosy conferencein Berlin in 1897 drew 150 attendees, with 44 delegates representing22 governments; the second conference in Bergen, Norway, in1909 attracted 168 attendees from 27 countries.10
8. Correspondence of James Walker to the Duke of Newcastle, 19 February 1862, inthe Report on Leprosy by the Royal College of Physicians, Prepared for, and Published by HerMajesty’s Secretary of State for the Colonies with an Appendix (London: Eyre and Spottiswood,1867), 2.
9. The Report on Leprosy by the Royal College of Physicians contained forty responses fromthe following: New Brunswick, Bermuda, Bahamas, Jamaica, Tortola, St. Kitts, Nevis,Montserrat, Antigua, Dominica, St. Lucia, St. Vincent, Barbados, Grenada, Tobago,Trinidad, British Guiana, Cape of Good Hope, Sierra Leone, Tangiers (Tunis, Tripoli,Bengazi, Cairo), Jerusalem (Caiffa), Beyrout (Cyprus), Damascus, Aleppo, Rhodes,Smyrna (Scio, Mytellene, Samos), Crete, Ionian Islands (Corfu), Salonica, Monastir(Bosnia Serai, Bucharest, Varna), Dardanelles (Brussa, Samsoun), Constantinople, Tarbreez,Japan, China (Hong Kong, Canton, Shanghai, New Chwang, Kin-Kiang, Kana Gawa,Formosa) Australia (Victoria, New South Wales), Mauritius, Ceylon, Madras Presidency,Bombay Presidency, Bengal Presidency.
10. This period, between the 1867 Report on Leprosy by the Royal College of Physiciansand the Berlin Conference, was a time of intense debate about the danger that leprosy rep-resented to the metropolitan centers of Britain and Europe.
Robertson : The Leprosy Asylum in India 477
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

The main journal in the field, Lepra Bibliotheca Internationalis, aninitiative of the Berlin conference, which was published up untilthe beginning of World War I, demonstrates an even wider circula-tion of information.11 Although the editorial committee was predo-minantly European, it also included Americans and committeemembers based in Jamaica and Havana. In addition, contributionscame from more exotic locales such as Cambodia, Anglo-EgyptianSudan, Arabia, South Africa, the Marquesas, Hawaii, the DutchAntilles, British Guiana, Madagascar, Laos, New Zealand,Reunion, the Loyalty Islands, Guadeloupe, Indochina, Algeria, thehighlands of West Central Africa, and British India. The journalcarried reports of leprosy asylums and of differing legislation con-cerning people with leprosy in various countries, as well as articlesof scientific and medical interest.
At the time of the 1897 Berlin and also the 1909 Bergen leprosyconferences, when European medical influences were strongest, theasylums and medical practices that were considered most worthy ofemulation were Norwegian, but American measures against leprosyalso increasingly commanded attention.12 In Hawaii, the leprosysettlement of Kalaupapa, on the island of Molokai, admitted 5,800
people with leprosy between 1866 and 1905, with the year 1888
marking the peak in numbers of people segregated there. By 1906,the Americans had established the very modern leprosy colony ofCulion in the Philippines, which had patients’ dormitories andquarters for 400 employees. This colony resembled a small townshipwith streets and alleys, a theater, a town hall, a school, a pipedwater supply and reservoirs, a sewer line, docks, warehouses, dining
11. The journal was published in London, Leipzig, and Paris (and later New York).12. Leprosy control in Norway, where the disease was endemic, focused on a system of
medical registration, legislation, hospitalization, and research. Surveys were conducted in1836, 1845, and 1852, and a medical superintendent for leprosy, Ove Guldberg Høegh(1814–1863), was appointed to be responsible for a national leprosy register, established in1856. St. Jørgen’s Hospital, three additional hospitals, and a research hospital were dedi-cated to leprosy. Knowledge of the disease of leprosy entered a new era through the workof Daniel Cornelius Danielssen (1815–1894), Carl Wilhelm Boeck (1808–1875), andGerhard Henrik Armauer Hansen (1841–1912). Although nineteenth century debatesabout leprosy argued that the disease had disappeared from Europe because of segregationand isolation practices in the Middle Ages, views about the actual presence of the diseasein Europe right up until the 1950s need to be revised. Carole Rawcliffe has begun thistask. See Rawcliffe, Leprosy in Medieval England (Suffolk, UK and New York: BoydellPress, 2006).
Journal of the History of Medicine : Vol. 64, October 2009478
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

halls, a post office, a store, and a garbage disposal plant, a church,public bath-latrines and a cemetery.13 The transition from theNorwegian model of the 1850s to the American model that beganin 1906 is paralleled by international exchanges of expertise thatwere grounded in local experience, as can be seen from paperspresented at the international conferences.
I have chosen India as the focus of my study because this is wherein the nineteenth century the earliest extensive program of construc-tion of asylums took place, and while there were never enoughasylums in India to care for all those affected by leprosy, there weremore asylums there than in any other country. From the 1870sonwards, the leprosy asylum in India incrementally changed, so that bythe 1940s, it could be described as existing in three distinct forms: thewell organized sanatorium for active and infective cases, with properstaff, buildings, and equipment; the asylum for crippled, deformed,and disabled cases; and the agricultural colony in which patients couldmaintain themselves.14 This study will focus on the emergence of thelast of these forms and the rationale that sustained it.
Both Sanjiv Kakar and Jane Buckingham have independentlyprovided studies of the leprosy asylum in India. Kakar argues that inthe light of medical uncertainties about transmission and causationof the disease, asylums were shaped by religious and medical inten-tions.15 Buckingham, as part of a larger study of leprosy in colonial
13. Secretary of the Interior, Dean C. Worcester, member of the American Cabinet inthe civilian government of the American occupied Philippines, cited in Cristina VerzolaRodriguez, ed. Culion Island: A Leper Colony’s 100-Year Journey toward Healing (Philippines:Culion Foundation, Inc. and Fundacion A Nuestros Enfermos Servimos Viendo A Dios,2003), 60. For critical articles on Culion, see Warwick Anderson, “Leprosy andCitizenship,” Positions: East Asia Cultures Critique, 1998, 6, 707–30; and Jo Robertson,“Culion, the ‘Island of the Living Dead’: Or Another Look at Leprosy and Citizenship,”in Politics of Prevention, Health Propaganda, and the Organisation of Hospitals, 1800–2000, ed.Astri Andresen, Kari Tove Elvakken, and Tore Gronlie (Bergen: Rokkansenteret, 2005).
14. Government of India, Committee Appointed by the Central Advisory Board ofHealth (1941), Report on Leprosy and Its Control in India (New Delhi: Government of IndiaPress, 1942), 28.
15. Sanjiv Kakar, “Medical Developments and Patient Unrest in the Leprosy Asylum,1860 to 1940,” Soc. Sci., 1996, 24, 62–80; and Kakar, “Leprosy in British India, 1860–1940: Colonial Politics and Missionary Medicine,” Med. Hist., 1996, 40, 215–30. Kakarexamines “various forms of protest adopted by patients within asylums” and identifiesflashpoints between patients and asylum authorities around issues of religious teaching,medical treatment, and sexual segregation. He argues that medical advances in the 1920sand 1930s provided a platform for greater militancy on the part of the leprosy affected forthe improvement of asylum conditions. See Kakar, “Medical Developments,” 73.
Robertson : The Leprosy Asylum in India 479
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

south India in the period before missionary anti-leprosy activity,describes the emergence, function, and design of the leprosy hospi-tal in Madras.16 Neither of these authors devotes an extended analy-sis to the regimes of value, especially the economic ones, out ofwhich Indian asylums emerged and for which the allocation ofspace and the construction of the built environment were an index.
In order to reconstruct a sense of the material and physical spaceof the leprosy asylum in India as it changed from being a refuge anda haven for the few, this article will describe how the missionaryorganization dedicated to supporting leprosy work in India, theMission to Lepers, invested the unrelenting stream of donations thatit received from British and Indian benefactors into land and thebuilt environment. It will describe the extent, location, and struc-tures of leprosy asylums in India that preceded many of the activitiesof the Mission, and then it will delineate the process of acquisition,improvement, and renovation that took place under the Mission. Atthe same time, the article will explain the rationales that governedthe acquisition of new asylums and lay bare an archaeology of thespaces that governed life in these places describing the buildings,the walls, courtyards, and separations within the compounds. Itthereby aims to describe the gradual processes of change out ofwhich emerged a new form of asylum: the agricultural colony, typi-fied by Purulia in Western Bengal.
This article will do this by using the descriptions of leprosyasylums furnished in reports by Wellesley Bailey, the founder of theMission to Lepers, on his travels on behalf of the Mission over threeseparate periods in 1886, 1890–91, and 1895–96.17 It will draw onthe Mission to Lepers’ reports that were produced after meetings ofleprosy asylum superintendents in Wardha in 1902, Purulia in 1908,Chandkhuri in 1911, and Calcutta in 1920.18 It will also draw upon
16. Jane Buckingham, Leprosy in Colonial South India: Medicine and Confinement(Basingstoke: Palgrave, 2002), 45–51.
17. Wellesley Bailey, A Glimpse at the Indian Mission-Field and Leper Asylums in 1886–87(London: John F. Shaw, 1887); The Lepers of Our Indian Empire: A Visit to Them in 1890–91(London: John F. Shaw, 1891); A Visit to Leper Asylums in India and Burma, 1895–96(Edinburgh: Darien Press, 1896).
18. Anon., Report of the Conference of Superintendents of Leper Asylums: The CentralProvinces and the Bombay Presidency, Wardha, CP, February 1902 (Bombay: Bombay GuardianMission Press, 1902); Anon., Report of a Conference of Leper Asylum Superintendents Held atPurulia, Bengal, from 18th to 21st February 1908 (Edinburgh: Darien Press, Bristo [sic] Place,1908); Anon., Report of a Local Conference of Superintendents of Leper Asylums, Held at
Journal of the History of Medicine : Vol. 64, October 2009480
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

the unpublished Minutes of the Mission to Lepers and the IndianAuxiliary of the Mission to Lepers, as well as photographs, plans,and official government reports.
WELLESLEY BAILEY, INDIA, AND THE MISSION TO LEPERS
Wellesley Bailey, the founding father of the Mission to Lepers, wasan Irishman, who after attempting to make his fortune in Australiaand New Zealand, set out to India where his brother was in theIndian police force. Bailey joined the American PresbyterianMission at Ambala, in the Punjab, and it was there that he firstbecame aware of people with leprosy. Bailey was filled with horror,fascination, pity, and an immediate sense of purpose: “If ever therewas a Christ-like work,” this was it.19 On his return to Dublin in1874, Charlotte Pim, a friend of his wife, Alice Grahame, heard hisstory and began to organize small meetings in her drawing room inDublin in order to tell others of “the terrible condition of India’slepers, physically, mentally, spiritually, and of what we were tryingto do, for just a few of them, at Ambala, in the Punjab.”20
Against all expectations, the small group found that many peoplewere responsive to their appeal for help. They had tapped into anincremental but consistent source of funding that still supports whatis today known as the Leprosy Mission International. Charlotte Pimhad hoped to raise about £30 a year, but by the end of the secondyear, had succeeded in raising £809.21 As can be seen from theMinutes of the Meetings, the group took a keen responsibility inaccounting for these donations. They apportioned small amounts ofmoney to Protestant missionary organizations in India assistingleprosy-affected people. In turn these organizations would accountfor their expenditure. Every gift of money was meticulously tracked
Chandkuri, Central Provinces, November 29th and 30th, 1911 (Chandkuri: W. H. P. Andersonfor the Mission to Lepers, 1911); Mission to Lepers, Report of a Conference of Leper AsylumSuperintendents and Others on the Leper Problem in India, Held in the Town Hall, Calcutta, from3rd to 6th Feb 1920 (Cuttack: Orissa Mission Press, 1920).
19. Cited by John Jackson, Lepers, Thirty-Six Years Work Among Them: Being the Historyof the Mission to Lepers in India and the East 1874–1910 (London: The Mission to Lepers,1910), 12.
20. Wellesley C. Bailey, Fifty Years Work for Lepers, 1874–1924 (London: Mission toLepers, 1924), 10.
21. A. Donald Miller, An Inn Called Welcome: The Story of the Mission to Lepers, 1874–1917 (London: Mission to Lepers, 1965), 13.
Robertson : The Leprosy Asylum in India 481
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from
and in the early years much of it went into purchasing lands andconstructing and maintaining leprosy asylums in India.22 WhileBailey’s awakening to the needs of the leprosy affected was expressedas concern for their spiritual well being, the work of the Missionalso took material form through judicious financial investment inland and buildings.
Ordinary people in Britain enthusiastically supported the work ofthe Mission to Lepers. Donations were given in the tradition ofsubscriptions for infirmaries and dispensaries that was usual inBritain in the nineteenth century.23 At public meetings held in theUnited Kingdom, donations of £250, £100, £50, and £30 weremade towards the asylums.24 Demonstrating a keen interest and aclose sense of connection with the work taking place in India,donors would sometimes specify where and on what the moneywas to be spent. For example, a legacy was received for the exclu-sive use of the Raniganj Asylum, in Bengal, “to be spent on itsimprovement, over and above our ordinary expenditure on thatasylum.”25
In addition to British support, there was also strong Indian finan-cial support, both from the British in India and from the Indianelite. In 1920, at the conference of leprosy asylum superintendentsin Calcutta, the Reverend Frank Oldrieve announced that he hadreceived 186,000 rupees in donations, mostly from Indians.26
Sometimes the support of inmates would be shared between theMission to Lepers and the relevant municipality.27 When thisdonated money was allocated to various asylums, the Minutes ofthe Mission to Lepers’ meetings reveal how these small amounts of
22. Gussow, Leprosy, 206. Gussow argues that missionaries restigmatized leprosy at theend of the nineteenth century, and he refers specifically to the Mission to Lepers. Adebate about stigmatization is for another article, except to note that stigmatization isalways a by-product of a loss of economic status.
23. Keir Waddington, Charity and the London Hospitals, 1850–1898 (Suffolk, UK andRochester, NY: Royal Historical Society, Boydell Press, 2000).
24. Minutes of the Mission to Lepers, June 1890, Minute Book, 139–140, 308,Leprosy Mission International Archives, Brentford, London.
25. Ibid.26. Frank Oldrieve, “Survey of Present Work among Lepers in India,” Report of a
Conference of Leper Asylum Superintendents, 80–88. Buckingham has already drawn attentionto the role of the Indian elite in supporting the legislation that would detainleprosy-affected paupers.
27. Minutes of the Mission to Lepers, 10 June 1890, 115, Leprosy Mission InternationalArchives, Brentford, London.
Journal of the History of Medicine : Vol. 64, October 2009482
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

money were used judiciously, making it possible for the Mission toembark on a building program that would bring about progressivechanges to the leprosy asylum in India.28
Wellesley Bailey went to India on three occasions between 1886
and 1896 in order to ascertain the needs of those affected withleprosy and of those of the Christian missions that were eitheralready assisting leprosy-affected people or desired to do so.29 Oncompletion of each of these tours, Bailey reported back to a com-mittee set up by the Mission to Lepers. At the same time, hisreports were published as three books that would have foundreaders among benefactors and those interested in joining thatgrowing group.30 Bailey’s descriptions were filtered through hisagenda, which sought to demonstrate to an audience of actual andpotential benefactors the difference that the Mission to Leperscould make and was, in his view, in the process of making in thelives and to the souls of those affected with leprosy in India, inorder to generate further funding. But the detailed descriptions ofthe leprosy asylums that he discovered in his travels and the changesthat he envisaged also reveal what asylums were like between 1886
and 1896, as well as how the Mission to Lepers changed the leprosyasylum in India, by incrementally altering its built environment, atthe turn of the nineteenth century.
Carolyn Strange and Alison Bashford argue that places of iso-lation in the nineteenth century were legitimated by discourses ofliberty and modernity so that their architecture reflects a paradoxicalneed to demonstrate humane values, while depriving individuals oftheir rights, in the name of public health.31 I will argue for themore determining role played by contingency in the shaping ofleprosy asylums in India, one element of which was the pressingdemand from those who wished to gain admittance.
28. This is evident from the painstaking details taken to account for and record expen-ditures. See Minutes of the Mission to Lepers, Leprosy Mission International Archives,Brentford, London.
29. For a discussion of Bailey’s using the travel literature genre to raise funds, seeD. George Joseph, “‘Essentially Christian, Eminently Philanthropic’: The Mission toLepers in British India,” Historia, Ciencias, Saude-Manguinhos, 2003, 10, Suppl. 1, 263–66.
30. Bailey, A Glimpse at the Indian Mission-Field; The Lepers of Our Indian Empire; A Visitto Leper Asylums in India and Burma.
31. Carolyn Strange and Alison Bashford, eds., Isolation: Places and Practices of Exclusion(London: Routledge, 2003).
Robertson : The Leprosy Asylum in India 483
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

Leprosy reduced its victims to pauper status, irrespective of theirpre-leprosy lives. In addition to leprosy altering the physical body,especially the face and hands, thereby compromising individuality, adiagnosis of the disease brought about a traumatic alteration in aperson’s social status and social identity. A. T. W. Simeons’s novel, TheMask of a Lion, vividly describes these changes, both physical andsocial, in the life of a village tailor, Govind, who is forced by leprosyto give up his livelihood and take to the roads with a band of fellowbeggars.32 Therefore a distinction must be made between those whovoluntarily sought entrance to Indian leprosy asylums and those whowere placed in asylums under the Lepers Act of 1898.33 Voluntaryadmissions were in the majority as is demonstrated in the case of thePurulia Asylum, Bengal, which in the twenty years from its inceptionin 1884 admitted 2,358 leprosy sufferers. Very few of these wereplaced in the asylum by order of the law. Although Purulia was placedunder the Act in 1902, by 1908 it had only received seven peoplewith leprosy who had been sent there under compulsion.34 Of these,one had escaped, four had died, and two were still at Purulia.35 Theleprosy-affected people in institutions in India therefore were mostlyvoluntary admissions and as such were separately housed from thosefew who had been detained under the law.
In addition, there were always more people in need of asylum thanthere was accommodation available. In Bengal, e.g., there were twoleprosy mission asylums at Raniganj and Bankura, and there was oneinstitution in Calcutta that was associated with the Mission toLepers. By 1921, in a population of 47 million in Bengal, there were15,550 people affected with leprosy and only 440 of these were in
32. A. T. W. Simeons, The Mask of a Lion (New York: Alfred A. Knopf, 1952).33. The Lepers Act of 1898 (Act no. III of 1898) was passed by the Governor-General
of India in Council. It was described as “An Act to provide for the segregation andmedical treatment of pauper lepers and the control of lepers following certain callings.” Init a “leper” was “any person suffering from any variety of leprosy in whom the process ofulceration has commenced.” The Act is published in an Appendix in Conference Purulia,79–87. For a discussion of the Act, its implementation, and its weakness, see Buckingham,Leprosy in South Colonial India.
34. The Lepers Act empowered local governments “to appoint places to be leperasylums for the purposes of the Act and specify the local areas from which lepers may besent to such asylums.” It was only implemented locally and not uniformly in forcethroughout India. Conference Purulia, 79–87.
35. Conference Purulia, 75. At the conference in 1908, the superintendent of Puruliacomplained that too few pauper lepers had been sent under the Act.
Journal of the History of Medicine : Vol. 64, October 2009484
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

asylums.36 In 1941, the government Report on Leprosy and its Control inIndia stated that “In India we are in the peculiar position that practi-cally every leprosy institution in the country is full, and thousands ofapplicants have to be refused each year for lack of accommodation.”37
Even in the late nineteenth century, the demand for admission was sohigh that the Mission to Lepers had to issue a notice to the missionsit supported that from June 1898, asylums were forbidden to take onmore leprosy-affected people or children or construct more buildingsor incur expenses on behalf of the Mission without the sanction of itsCommittee.38 Consequently, the changes that took place in leprosyasylums in India were incremental, continuously shaped by a balancebetween the values and ideals of their founders and managers whowere operating with scarce financial resources that were apportionedpiecemeal and by demand from those who waited “outside” in thehope of gaining entry.39
LEPROSY LEGISLATION AND THE GOVERNMENT OF INDIA
The tours of Wellesley Bailey were conducted against an inter-national backdrop of growing interest in leprosy in India, as well asan intense debate within India in the ten years leading up tothe Lepers Act in 1898.40 In London, the National Leprosy
36. “Map of India: Showing Leper Institutions,” in Robert G. Cochrane, Leprosy:Symptoms, Diagnosis, Treatment and Prevention, 2nd ed. (London: British Empire LeprosyRelief Association, 1927), 22.
37. Government of India, Report on Leprosy and its Control in India, 40.38. Minutes of the Mission to Lepers, June 1898, 148, Leprosy Mission International
Archives, Brentford, London.39. Minutes of Meetings of the Mission, Leprosy Mission International Archives,
Brentford, London, UK. I argue that, in India, these institutions were overwhelmed byapplicants for admission. See annual reports of the Mission to Lepers, e.g., The Mission toLepers, A Report of the Sixty-Third Year’s Work in India and Burma: September 1936-August1937, issued by the Indian Auxiliary in India, 16, accessed in Leprosy Mission InternationalArchives, Brentford, London, UK. This report records the need to turn away applicantsfor lack of space. Rev. G. C. Mackintosh is quoted as saying that “When the PuruliaLeprosy Relief Association opened their new Leper Home in May we were for a timerelieved of the pressure of applicants for admission. However since then they have enrolled200 and can take no more, and once again we are having to turn people away for lack ofspace.”
40. In India, in the decade of the seventies, when Hansen was attempting to replicatethe causative agent of leprosy, Mycobacterium leprae, in Norway, and just after Bailey saw hisfirst leprosy-affected people, an intense exchange of information on leprosy was takingplace. See Jo Robertson, “In Search of M. Leprae: Medicine, Public Debate, Politics andthe Leprosy Commission to India,” in Economies of Representation, 1790–2000: Colonialismand Commerce, ed. Leigh Dale and Helen Gilbert (Aldershot, UK and Burlington, VT:
Robertson : The Leprosy Asylum in India 485
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

Fund appointed an Indian Leprosy Commission which was sentto India on 23 October 1890.41 Its investigation coincided withBailey’s second tour, and the commission and Bailey crossed pathsin Purulia, in Western Bengal. The commissioners found that“neither compulsory nor voluntary segregation would at presenteffectually stamp out the disease, or even markedly diminish theleper population, under the existing conditions of life in India.”42
Their commissioning body, the National Leprosy Fund, “enter-tain[ed] a precisely opposite opinion” and appended recommen-dations for segregation to the commissioners’ report.43 Studies ofleprosy in India have independently analyzed the web of intercon-nected interests by which leprosy legislation was introducedincrementally at the end of the nineteenth century. They reveal thereluctance of the colonial government to implement legislation, thepublic pressure from European and Indian elites to detain andisolate beggars with leprosy, as well as the international climate thatsought to determine the threat that leprosy represented to theEmpire.44
As Buckingham shows in her study of leprosy in colonial SouthIndia, the application of legislation in India was subject to nego-tiation at every level of government. The Lepers Act was only
Ashgate, 2007); and Michael Worboys, “Was There a Bacteriological Revolution in LateNineteenth-Century Medicine?” Stud. Hist. Phil. Biol. & Biomed. Sci., 2007, 38, 20–42.
41. The National Leprosy Fund, began as the Committee for the Father DamienMemorial Fund, was established to pay tribute to the life and personal sacrifice of FatherDamien de Veuster, who had died in April 1889 after spending sixteen years on Molokai,in Hawaii, caring for people with leprosy. The Fund assembled a cast of luminaries—members included the Archbishop of Canterbury, the Duke of Norfolk, Lord RandolphChurchill, Baron Ferdinand de Rothschild, the Bishop of London, Sir William Jenner,and the Hon. G. Curzon, as well as prominent members of the medical fraternity—andwas presided over by the Prince of Wales. By the end of June, the executive committeehad decided that Damien’s memory should be perpetuated in four ways: a memorialwould be erected to him at Molokai; a fund would be established for lepers in the UnitedKingdom; two Studentships would be endowed for doctors to study the disease; and anIndian Leprosy Commission was to be appointed.
42. National Leprosy Fund, President HRH The Prince of Wales, Report of the LeprosyCommission in India (Executive Committee: William Clowes and Sons, 1893), 389.
43. Ibid., 456. See William Tebb, The Recrudescence of Leprosy and Its Causation (London:Swan Sonnenschein, 1893), 302, for a discussion of the timing of the publication of thereport and the response of the National Leprosy Fund to the findings of the Commission.
44. Kakar, “Leprosy in British India”; Buckingham, Leprosy in Colonial South India;Worboys, “Was There a Bacteriological Revolution”; and Robertson, “In Search ofM. Leprae.”
Journal of the History of Medicine : Vol. 64, October 2009486
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

applied selectively by district and was specifically directed at remov-ing leprosy-affected beggars from sight.45 She indicates that, by1898, the government was happy to hand over responsibility forleprosy institutions to, and would increasingly provide financialsupport for, societies or missionary groups to maintain asylums46:
Since most private institutions for leprosy care existing in India by 1898
were run under the auspices of the Mission to Lepers, the passing of theLepers Act began the process of delineating the new relationship betweenthe Mission and the government. The Mission insisted on retainingautonomy while receiving government funding linked to their provisionof accommodation under the Act. Thus, from the early twentiethcentury, care and treatment of leprosy sufferers substantially became theresponsibility of the Mission to Lepers.47
I differ from Buckingham with respect to the timing of this shift inresponsibility. Buckingham argues that “From being almost entirelya government matter, leprosy care became a missionary concern.”48
I agree with this, but I argue that activities of the Mission and thechanges to asylums preceded and, in some instances, provided amodel for the government institutions. Although the transition wasaccomplished by 1898, the process can be seen to have commencedby the time of Bailey’s first tour in 1886. It is true that the MadrasLeper Hospital was established and operational when Bailey visitedin 1886, but the other Presidencies had nothing comparable at thistime. Acworth, which was then known as the Matunga LeprosyAsylum and was financed by subscriptions and by the Municipalityof Bombay, was opened in 1890.49 This unevenness in timing ismost evident in the Bengal Presidency. In 1906 the governmentconsidered which districts in the province should be brought underthe Lepers Act. This was after it had spent years prevaricating about
45. Buckingham, Leprosy in South Colonial India, 191.46. Ibid., 188.47. Ibid., 187.48. Ibid.49. Government of Bengal, “Bill to Provide for the Segregation of Pauper Lepers,” 15
September 1893, File 3-L/4 1, nos. 10–11, 7, Municipal Department, Medical, 5/12139,Orissa State Archives, Bhubaneshwar, Orissa, includes “A Resume of the Steps Taken toEstablish a Leper Asylum in Bombay and to Remove Lepers from the Public Streets;” andGovernment of Bengal, “Report of the Leprosy Commission – What Effect to be Givento Its Conclusions,” July 1895, File M 3-L/4, nos. 10–29, Municipal Department,Medical, 22/12134, Orissa State Archives, Bhubaneshwar, Orissa.
Robertson : The Leprosy Asylum in India 487
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

the transfer of the government funded asylum in Calcutta fromAmherst Street to the new Albert Victor Asylum, only to decidethat “By assisting the Mission Asylums, Government will be able toaccomplish much more than it could by establishing asylums of itsown.”50 It did this after it received a report on the Purulia LeprosyAsylum, which had been operating since 1888.
The beginnings of this arrangement between the Mission toLepers and the government of India started after Bailey’s 1886 tour,and negotiations probably began when he was in India in 1891–92.Minutes of the Mission to Lepers committee note that “theGovernment of India have expressed their readiness to make grantsin aid of leper asylums maintained by voluntary efforts” and thefinance committee is instructed “to make a formal application forGovernment assistance for the asylums belonging to this committee. . . .”51 This would indicate that Bailey’s survey tours and reports onasylums were carried out in a climate of negotiation that wouldeventually lead to an arrangement agreeable to both the govern-ment and the Mission, and the changes in responsibility would havebeen accomplished by the time of the introduction of the LepersAct in 1898.52 The nature of the process is demonstrated by thesupport provided for the Purulia asylum. It was first provided bythe district and later by the provincial government, once it wasdecided to bring the asylum under the Lepers Act.53 Nonetheless,as a result of a measure of financial independence, with increasingsupport from members of the public, the Mission to Lepers tookthe opportunity to form asylums in a way that suited its own senseof purpose.
50. Government of Bengal, “Report of the Leprosy Commission – What Effect to BeGiven to Its Conclusions”; and Government of Bengal, “Grants to Leper Asylums,” 10
March 1906, File M 3-L/8, no. 6, 2, Municipal Department, Medical, Orissa StateArchives, Bhubaneshwar, Orissa.
51. Minutes of the Mission to Lepers, 13 February 1889, 112–13, Leprosy MissionInternational Archives, Brentford, London.
52. Communication between the Mission and the various Presidencies was more devel-oped in some instances than others, as is clear from Bailey’s correspondence with theBengal government, which inquired about other provinces that were assisting the Mission.Government of Bengal (1907) Municipal Department, Medical, December, nos. 57–64,“Grant to the Leper Asylums Maintained by the Mission to Lepers in India and the East,”Orissa State Archives, Bhubaneshwar, Orissa.
53. Government of Bengal, “Leper Asylum at Purulia and Lohardaga,” December1895, File 3-L/5, nos. 40–49, Municipal Department, Medical File, 6/12152, Orissa StateArchives, Bhubaneshwar, Orissa.
Journal of the History of Medicine : Vol. 64, October 2009488
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

These negotiations about Indian asylums would not have beenindependent of the deliberations at international leprosy conferencesin this period, which recommended the isolation and segregation ofleprosy-affected people, especially those belonging to the lowerclasses.54 The Berlin Conference in 1897 resolved that “Every leperis a danger to his surroundings, the danger varying with the natureand extent of his relations therewith, and also with the sanitary con-ditions under which he lives. Among the lower classes every leperis especially dangerous to his family and fellow workers, but cases ofleprosy frequently appear in the higher social circles.”55 The BergenConference in 1907 would affirm the resolutions of the Berlin oneand recommend the regular examination of contacts of people withleprosy, a prohibition on certain trades and occupations, and thestrict isolation of leprosy-affected beggars and vagabonds.56 Countryspecific legislation, along with new leprosy institutions, was sub-sequently introduced following conferences and congresses inStrasbourg, in 1923, and in Cairo, in 1938.57
THE EXTENT OF LEPROSY ASYLUMS IN INDIA
The descriptions that Bailey made during his three tours of Indianleprosy asylums offer an insight into the number of places in whichpeople with the disease lived. On the first tour (1886–87), he foundeleven centers where leprosy work was supported by the Mission toLepers, three of which the Mission owned. Four years later in 1890–91, there were twenty-one centers, six of which were outrightMission to Lepers homes, and by the 1895–96 tour, there were thirty-seven centers, fourteen of which the Mission owned (see Figure 1).
The later extent of the development of asylums in India can beseen from a map produced in 1927, by Robert Cochrane, themedical director for the Mission, as a result of his own tour ofinspection. This shows the institutions owned by the Mission to
54. Bailey attended the Bergen Conference and all subsequent congresses were attendedby a member from the Mission to Lepers.
55. Isadore Dyer, “The Berlin Leprosy Conference,” New Orleans Med. Surg. J., 1897,50, 361.
56. D. H. Currie, “The Second International Conference on Leprosy, Held in Bergen,Norway, August 1 to 19, 1909,” Pub. Health Rep., 1909, 24, 1357–61.
57. Anon., “Reports of the International Congress of Leprosy Held in Cairo, March,1938,” reprinted for the Leonard Wood Memorial from the Int. J. Leprosy, 1938, 6, 389–417, first published in the J. Egyptian Med. Assoc., 1938, 21, 149–74.
Robertson : The Leprosy Asylum in India 489
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

Fig.1. Map of Wellesley Bailey’s tour in 1886–87, found in Wellesley Bailey, AGlimpse at the Indian Mission-Field and Leper Asylums in 1886–87 (London: JohnF. Shaw, 1887), frontpiece to page 5.
Journal of the History of Medicine : Vol. 64, October 2009490
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

Lepers, those for which the Mission provided support, and thosethat were independent. This map also shows the population in eachstate of India, the estimated numbers of people affected withleprosy (according to the 1921 census returns), and the numbers ofthose who were segregated. In Bengal, e.g., there were two leprosymission asylums at Raniganj and Bankura and one institution inCalcutta that was associated with the Mission. At the 1920 Calcuttaconference of asylum superintendents, it was claimed that therewere 150,000 leprosy-affected people in India and of those 5.8%were in asylums (see Figure 2).
By 1886, different sorts of asylums existed simultaneously inIndia. One was the traditional indigenous charity shelter, or dhar-mashala, which accommodated leprosy-affected people amongother indigents. Others were those that were managed by districts,municipalities, or provinces, as well as those run by missionary,charitable, or benevolent organizations.
Traditionally, those affected with leprosy were treated in the sameway as other recipients of charity who found shelter and sustenancein locally established and administered poor houses:
Dharmashalas were generally situated near temples, holy places or in thelarger town and cities. Such institutions therefore, traditionally accommo-dated all variety of needy and handicapped persons, there being no facili-ties, or even intention, to regard lepers as a special class of indigentrequiring isolation. Dharmashalas were used as temporary or permanentabiding places or night shelters for those who might spend their daysbegging for alms.58
Some of these institutions had come into existence by royal decree,such as the King’s Poor House in Lucknow, which was establishedin 1831 by King Naseer-ood-deen Hyder. This asylum held elevenpeople affected by leprosy, among other recipients of charity, andwas managed by a committee of European officers and Indians.59 Ina remarkable contrast to this benign environment, in Bhopal State,people with leprosy were forced into the asylum founded by theBegum, at Sehore, and guarded there as prisoners.60 Princely
58. Shubhada S. Pandya, “Leprosy in the Bombay Presidency, 1840–1897: Perceptionsand Approaches to its Control” (PhD diss., University of Bombay, 2001).
59. Bailey, Glimpse, 104–5.60. Bailey, Visit, 11.
Robertson : The Leprosy Asylum in India 491
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

Fig. 2. “Map of India: Showing Leper Institutions,” in Robert G. Cochrane,Leprosy: Symptoms, Diagnosis, Treatment and Prevention, 2nd ed. (London: BritishEmpire Leprosy Relief Association, 1927), fronts on page 22.
Journal of the History of Medicine : Vol. 64, October 2009492
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

benevolence could also be inconsistent. At Chamba, Bailey foundthat the local prince was intent on reclaiming houses that he hadoriginally granted as part of the asylum.61
District benevolent institutions included shelter for smallnumbers of leprosy sufferers. In Benares, the District BenevolentInstitution housed six leprosy-affected men and two women.62
Local societies were also responsible for asylums such as that estab-lished by the Agra Local Relief Society in 1861, which in 1886
housed twenty leprosy-affected people.63
There were also asylums that were managed by the municipality,which in some instances, would appoint a board (of managers).64
Tarn Taran, in the Punjab, e.g., was a large government institutionthat was supported by different municipalities. These dispatchedtheir leprosy-affected to the asylum and then contributed fourrupees a month for every person sent.65 Municipal support couldbe a mixed blessing, as a municipality could be parsimonious orneglectful. Rawalpindi was supported by a Municipal and DistrictCommittee, but the native doctor told Bailey that no money wasnow being spent upon the place, as the Committee was waiting tosee what the government would decide to do about an asylum.66
In addition to institutions established as a result of municipal orindividual support, there were informal clusters of people affectedby leprosy dwelling independently. On his first trip, Bailey discov-ered a group in huts by the wayside at Saharanpore, in the divisionof Meerut, in the North West Provinces.67 On later trips he would
61. Bailey, Glimpse, 149.62. Ibid., 100.63. Ibid., 170. The Dharmsala in Byculla, Bombay; the Dharmsala in Ahmedabad and
the poor house at Poona, in the Bombay Presidency; the various District CharitableAssociation asylums at Allahabad; Benares; Amherst St., Calcutta; and Rawalpindi were allinspected by Bailey.
64. Bailey, Visit, 64. The two institutions at Saharanpore, one for men on one side ofthe city, and the other for women on the other side, were both supported and managed inthis way.
65. Bailey, Glimpse, 153. Matunga or Acworth, in Bombay, was supported by twomonthly grants of 1,000 rupees per month each from the Bombay Government and theMunicipal Corporation.
66. Bailey, Lepers of Our Indian Empire, 9. This indecision in 1891 indicates the generaluncertainty about who would take responsibility for the future of leprosy asylums and alsoprevarication that used the impending report of the Leprosy Commission as justificationfor indecision.
67. Bailey, Glimpse, 130.
Robertson : The Leprosy Asylum in India 493
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

seek out other groups in huts (at Neyoor, in the south, nearTrivandrum; or Muzaffarnagar, in Derajat, Punjab), or in small vil-lages (e.g., in Lodiana/Ludhiana, in Jullunder Commissionership,Punjab).68
In the Presidencies, larger hospitals, such as the JJ Hospital inBombay, had a ward for leprosy-affected patients.69 In the MadrasPresidency, the Monegar Choultry or Government Leper Hospital,in Madras was purpose built and considered a model of its kind.70
Separate asylums also existed in both British and Native States. Theasylum in Bangalore belonged to the Mysore Government, and theCochin Lazarus Hospital at Pallypuram belonged to the British gov-ernment, even though it was situated in a Native State.71
Individual British benevolence could also be responsible for theestablishment of an asylum such as that at Almora, in theNorth-West provinces, which was founded in 1840 and maintainedby Sir Henry Ramsay when he was a Civil Officer in the district.72
Many establishments resulted from a combination of British andIndian local benevolence. As an example, the asylum at Bhagulpore,in Bihar and Orissa, was reconstructed in cooperation with thechairman of the municipality, Shib Chandar Banerji, Rai Bahadur.In addition, 1,000 rupees had been contributed by an Englishmanwho lived in the district during the winter months, and theMission to Lepers also donated 500 rupees. As a result, a combinedsum of 10,000 rupees was available for this asylum.73
68. Bailey, Lepers of Our Indian Empire, 160, 210; Bailey, Visit, 63.69. Pandya, “Leprosy in the Bombay Presidency, 1840–1897,” 220–24.70. As discussed by Buckingham, Leprosy in South Colonial India.71. Ibid., 38. The Calicut Leper Asylum was a government institution, as was Baba
Lakhan, near Sialkot, in the Punjab.72. Mission to Lepers, Fifty Years Work for Lepers, 1874–1924: An Account of the Funding
and Growth of the Mission to Lepers (London: Mission to Lepers, 1924), 42. Similarly, theAsansol Asylum, in Bengal, was a gift to the Mission to Lepers from Georgiana, Countessof Seafield, who was inspired by the memory of a leprosy-affected Indian convert toChristianity. A note on Asansol appears in the minutes of the Mission to Lepers, whichmentions plans for an asylum and requests of financial support. Minutes of the Mission toLepers 1890, 136, The Leprosy Mission International Archives, Brentford, London; Bailey,Lepers of Our Indian Empire, 145.
73. Bailey, Lepers of Our Indian Empire, 148. The joint local project for the new LeperAsylum at Matunga, in Bombay, in 1890 would show the culmination of this form of civiccooperation: in response to Acworth’s and the city’s growing concern about leprousbeggars, buildings were subscribed to by the public, and this enabled a sum of 73,000
rupees to be spent on the asylum.
Journal of the History of Medicine : Vol. 64, October 2009494
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

States were increasingly happy to hand over management of anasylum for a term to a willing and competent Western missionary.For example, the asylum at Srinagar had originally been intendedto be a state concern and was to be managed by state officials, but itwas subsequently offered for five years to Dr. Neve, a medical mis-sionary.74 In 1891, he constructed buildings to accommodate thirtypatients, and received 5,000 rupees from the state for the buildingsand an additional 2,000 rupees a year to run the asylum.
The Mission to Lepers increasingly provided support to manyasylums by sharing responsibility for costs with either a District or aMunicipal Association and/or another missionary group, therebygaining more say in the new constructions. By the end of 1896,fourteen missionary organizations received funds for buildings and,in some instances, funds for the upkeep of an asylum, while thecooperating missionary organization would provide staff.75 InAllahabad, a small asylum on the Nynee road, over the Jumnabridge, had mostly been supported by the Allahabad DistrictCharitable Association and superintended by the AmericanPresbyterian Missionaries. In 1891, it also received an annual grantfrom the Mission to Lepers in India, as well as the costs of buildingone row of houses.76 An asylum such as that at Rurki in the Punjabcame to be almost entirely supported by the Mission to Lepers inIndia by 1891, although it still received a small grant from theMunicipality. New accommodation for this asylum was to costabout £10, and when the houses of the asylum were full tocapacity, maintenance was estimated to cost about £150 perannum.77 Sometimes support was provided for a specific purpose sothat the cost of the asylum was divided between benefactors. InDehra, e.g., the support of the institution came from interestearned on trust funds, as well as from voluntary subscriptions anddonations from Dehra residents, but the cost of the religious work,specifically the support of a native pastor and a subordinate Indian
74. Bailey, Lepers of Our Indian Empire, 16.75. Bailey, Visit, 92. Almora was managed by the London Missionary Society. Bailey,
Glimpse, 111; Subathu in the Punjab was established by John Newton and supported bythe Mission to Lepers, Bailey, Glimpse, 137; and Chumba, which had been built by Baileyas a missionary for the Church of Scotland, Bailey, Glimpse, 148.
76. Bailey, Glimpse, 119; and Bailey, Visit 59.77. Bailey, Glimpse, 70.
Robertson : The Leprosy Asylum in India 495
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

leprosy-affected Christian, was met by the Mission to Lepers inIndia.78
On his later trips, Bailey would return to many sites he hadvisited previously and report on their condition and development,especially if the Mission to Lepers had provided support. The twolater trips were notable for reports of new establishments, includingthe purchase of land and the progress of construction, as well as thecost of upkeep. These new asylums were either wholly owned bythe Mission to Lepers and run by a missionary organization or theywere the initiative of another missionary organization and sup-ported by the Mission to Lepers.
LOCATIONS OF EXISTING ASYLUMS
In a country as diverse as India, the locations of asylums could beexpected to be mixed; nonetheless, some commonalities doemerge. The practice seems to have been to locate the asylum somedistance from the city and beside a thoroughfare. The asylum inAgra, e.g., was situated two miles past the fort, on the river road.79
Proximity to a road enabled the inhabitants of the asylum to maketheir living by begging. In Rurki, Patiala, in the Punjab, a few hutswere placed by the roadside, outside the township, and inSaharanpore, seven men found shelter in a long row of houses situ-ated on an open plain outside the city.80 These huts appear to havebeen haphazardly grouped and life there proceeded with minimalor only cursory attention from outsiders.
Some of these sites were quite large and very well organized. AtLodiana, e.g., a community of forty men, women, and childrendwelt in a village that was well supplied with ponies, cattle, andfour goats. The ponies were used for travel to locations for begging.This village was also strategically located close to the campingground used by the British troops as they marched throughLodiana.81 In some instances, a site may have accidentally or purpo-sefully served a therapeutic purpose; for example, the asylum atCalicut was located on the beach, close to a fishing village.82 Other
78. Bailey, Glimpse, 132–3; and Visit, 65–71.79. Bailey, Glimpse, 170
80. Bailey, Visit, 66–67; and Bailey, Glimpse, 130.81. Bailey, Lepers of Our Indian Empire, 160–61.82. Ibid., 219.
Journal of the History of Medicine : Vol. 64, October 2009496
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from
situations were less appealing. Prisoners affected by leprosy in theNagpur jail were not only imprisoned, but also isolated from otherinternees.83
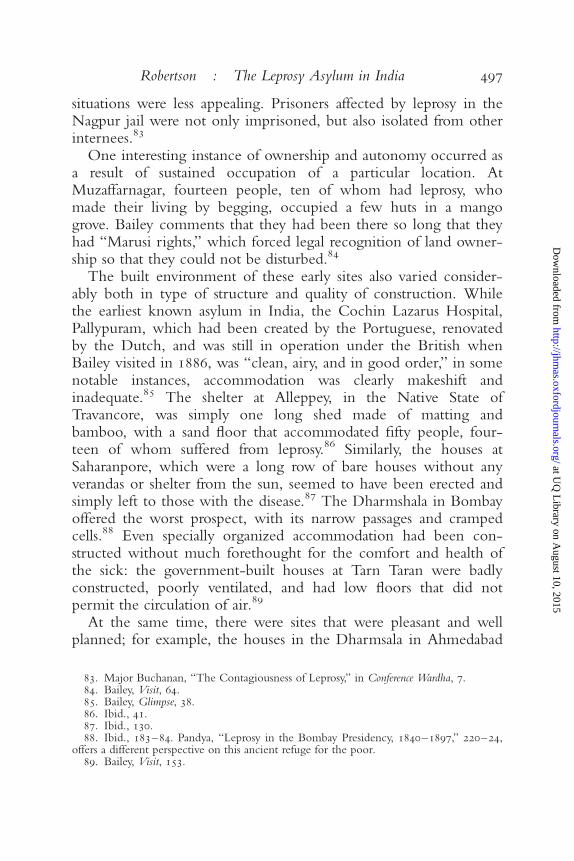
One interesting instance of ownership and autonomy occurred asa result of sustained occupation of a particular location. AtMuzaffarnagar, fourteen people, ten of whom had leprosy, whomade their living by begging, occupied a few huts in a mangogrove. Bailey comments that they had been there so long that theyhad “Marusi rights,” which forced legal recognition of land owner-ship so that they could not be disturbed.84
The built environment of these early sites also varied consider-ably both in type of structure and quality of construction. Whilethe earliest known asylum in India, the Cochin Lazarus Hospital,Pallypuram, which had been created by the Portuguese, renovatedby the Dutch, and was still in operation under the British whenBailey visited in 1886, was “clean, airy, and in good order,” in somenotable instances, accommodation was clearly makeshift andinadequate.85 The shelter at Alleppey, in the Native State ofTravancore, was simply one long shed made of matting andbamboo, with a sand floor that accommodated fifty people, four-teen of whom suffered from leprosy.86 Similarly, the houses atSaharanpore, which were a long row of bare houses without anyverandas or shelter from the sun, seemed to have been erected andsimply left to those with the disease.87 The Dharmshala in Bombayoffered the worst prospect, with its narrow passages and crampedcells.88 Even specially organized accommodation had been con-structed without much forethought for the comfort and health ofthe sick: the government-built houses at Tarn Taran were badlyconstructed, poorly ventilated, and had low floors that did notpermit the circulation of air.89
At the same time, there were sites that were pleasant and wellplanned; for example, the houses in the Dharmsala in Ahmedabad
83. Major Buchanan, “The Contagiousness of Leprosy,” in Conference Wardha, 7.84. Bailey, Visit, 64.85. Bailey, Glimpse, 38.86. Ibid., 41.87. Ibid., 130.88. Ibid., 183–84. Pandya, “Leprosy in the Bombay Presidency, 1840–1897,” 220–24,
offers a different perspective on this ancient refuge for the poor.89. Bailey, Visit, 153.
Robertson : The Leprosy Asylum in India 497
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

were large and airy, and the Native Leper Asylum in Bengal was“on a nice site” and had several well-built wards.90 Bailey oftenremarked on the unused capacity of several asylums, particularly theasylum at Wazirabad, in northern Punjab: “The Leper Asylum wasa nice little building of four rooms, capable of housing twelvelepers comfortably; but there were no lepers.”91
ACQUIRING NEW SITES AND IMPROVING EXISTING ASYLUMS
Increasingly, the Mission to Lepers established new sites for leprosyasylums, in addition to improving existing sites. Land acquisitionoccurred incrementally as the need arose and in response to thelocal conditions of purchase. In the period of Bailey’s three trips,new sites were established at Srinagar, Moradabad, Purulia, Asansol,Bhagulpore, Burdwan, Ranigunj, Jubbulpore, Wardha, Ratnagiri,and Alleppey.92 When there was no other way of securing the land,a perpetual lease was taken, as for the site for Asansol Asylum.93
Building and development progress was reported in subsequenttrips by Bailey and in annual reports to the public.
Improvements to existing sites took the form of providing betteraccommodation in more regulated spaces that catered to the physicaland spiritual wellbeing of the residents and were dictated by com-monly held assumptions that sound accommodation, ventilation,shade, and pleasant surroundings would benefit the health and well-being of the sick. As an example, the people at Rurki who were dis-covered living in wretched huts by the roadside were provided withan enlarged space that accorded more closely with the idea of anasylum, including new accommodations, a prayer room, and treesfor shade.94 Similarly, new accommodation was provided for thepeople living in old huts at Neyoor, Chandag, and at Srinagar.95
90. Bailey, Glimpse, 177–78; and Bailey, Visit, 59–60.91. Bailey, Lepers of Our Indian Empire, 37.92. Srinagar (Bailey, Lepers of Our Indian Empire, 16); Moradabad (Bailey, Lepers of Our
Indian Empire, 69); Purulia (Bailey, Visit, 15–23; and Bailey, Lepers of Our Indian Empire,122–23); Asansol (Bailey, Visit, 26; and Bailey, Lepers of Our Indian Empire, 145–47);Bhagulpore (Bailey, Visit, 55; and Bailey, Lepers of Our Indian Empire, 148); Burdwan(Bailey, Lepers of Our Indian Empire, 174); Ranigunj (Bailey, Visit, 28); Jubbulpore (Bailey,Visit, 13); Wardha (Bailey, Visit,14); Ratnagiri (Bailey, Visit, 87); Alleppey (Bailey, Lepers ofOur Indian Empire, 216).
93. Bailey, Lepers of Our Indian Empire, 177.94. Bailey, Lepers of Our Indian Empire, 66; and Bailey, Visit, 66.95. Bailey, Lepers of Our Indian Empire, 17, 201–7; and Bailey, Glimpse, 121.
Journal of the History of Medicine : Vol. 64, October 2009498
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

Sometimes the cost of these improvements was shared. In orderto replace the “charity shed” at Alleppey, in which Bailey had dis-covered fifty people in benighted conditions, the new asylum therebecame a joint affair between the Mission to Lepers in India, whichprovided 750 rupees, and the Rajah of Travancore, who donated500 rupees. In addition to this, “a few friends in India” promisedother sums.96 The Mission to Lepers also contributed financialsupport for the expansion of existing and successfully run ventures,such as that at Almora. In 1890, the Mission’s committee increasedtheir grant from 1,800 rupees to 2,400 rupees for increasednumbers. They also provided 200 rupees towards repairs and contin-ued to provide annual grants.97
When a new site for an asylum was chosen, in addition to theavailability of the land, its suitability was judged on the balancebetween remoteness and accessibility. The site for the new asylumat Srinagar was considered to be suitable because it stood on apeninsula that extended into the lagoons, and at one point touchedthe Great Lake. It fulfilled the conditions both of remoteness andaccessibility, for while those affected with leprosy would be wellaway from other people, they would be within easy reach of thetown, either by land or by water. The land for the Asansol asylumwas situated on a long narrow strip of land, with some risingground that had fields for cultivation. It was located beyond therailway lines and on the opposite side of the railway station, awayfrom other dwellings, but still within easy access.98 At Raniganj,in Bengal, a new asylum was built two miles outside the town,on a high, dry site.99 Sometimes the choice of remoteness wasconsidered to be in the interests of those affected by leprosy. Theasylum at Sabathu, in the Punjab, was at one time considered to bea suitable site for Europeans with the disease because it was inthe hills.100
The suitability of a site was enhanced if there were already build-ings on the property that could be adapted to asylum use. Thehouse and property at Bhaugulpore, in West Bengal, already had a
96. Bailey, Glimpse, 42.97. Bailey, Lepers of Our Indian Empire, 136.98. Ibid., 177.99. Bailey, Visit, 29.
100. Ibid., 73–74.
Robertson : The Leprosy Asylum in India 499
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

good pucca house and some out-offices that were ready for use.101
Similarly, the site at Wardha, in the Central Provinces, had severalgood buildings and also others in need of repairs.102 At Ratnagiri,Konkan, in the Bombay Presidency, a piece of ground of about twoand a quarter acres by the river recommended itself because italready had one small hut on it and the site seemed suitable forfurther permanent buildings.103
Often negotiations for suitable land had to take into accountcompetition with other interests. At Ranigunj, it was necessary tonegotiate with the General Manager of the Bengal Coal Companyto ask if he would try to secure a site for an asylum.104 There weresometimes difficulties in finding a site. At Bhandara, near Nagpore,the search for a site was a prolonged affair. Bailey described theprocess:
In the evening I drove out with Drs Revie and Sandilands, and MrRango Harri, Secretary to the Municipal Committee, and a pleader.Sandilands was interested in an asylum, and the Mission to Lepers hadpromised him a grant for building and an annual grant for maintenance,but a site had to be found first. One possibility was located on the otherside of the river, which Mr Harri had offered as a gift to the LeperMission, but it was decided that during the rainy season it would becomeflooded.105
The next day another site was inspected and was considered favor-ably because it had a mango grove, a small tank, and a few goodfields, but it belonged to some local people, and they would haveto be persuaded to sell it. Two days later, the group was still lookingand had not found anything suitable.106 Similarly, at Jubbulpore, asite that was suitable was not for sale, and although some nativeChristians offered a site on their own property, it was not con-sidered suitable.”107
101. Pucca housing referred to permanent solidly-built constructions made of kiln-burnt brick, stone, or mortar. Bailey, Lepers of Our Indian Empire, 148.
102. Bailey, Visit, 14–15.103. Ibid., 87.104. Bailey, Lepers of Our Indian Empire, 175.105. Ibid., 180–81.106. Ibid., 183.107. Bailey, Visit, 13–14.
Journal of the History of Medicine : Vol. 64, October 2009500
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

THE IDEAL ASYLUM: WALLS AND COURTYARDS
In most instances, before the Mission to Lepers began constructingasylums, dwellings for people with leprosy were enclosed by a wall.Walls did not necessarily make the shelters prison-like, and theymay have served to provide seclusion just as walls did in privatedwellings in India at that time. Thomas Metcalf points out that theBritish in India also built themselves bungalows that were situatedin courtyards.108 The already-existing asylums usually had some sortof central area, in which huts, small houses, or a building, contain-ing several small rooms, provided shelter for men and women. In1886, the Cochin Lazarus Hospital was in a large enclosed com-pound, as was the Native Leper Asylum at Baidyanath, Bengal, andin Agra, the asylum, albeit laid out in a large quadrangle, wasenclosed by a high wall.109 The asylum at Dehra and the Dharmsalain Ahmedabad were surrounded by high walls, and the CalicutLeper Asylum was enclosed by a wooden fence on the front partthat faced the sea.110
Missionary-built asylums that pre-existed the Mission to Lepersvaried in character. One of the most remarkable asylums at Almora,which was constructed by Sir Henry Ramsay in 1849 and run bythe London Missionary Society, was built on terraces.111 AtChumba, the asylum, which Bailey himself had built, was dividedinto two parts; the first set of buildings, forming two sides of asquare, consisted of low huts; and the second set of buildings was ofa single row of huts, about 400 yards further down the river.112 Thesite does not seem to have been enclosed in any way.
Buckingham traces the history of the politics of contestation thatwas brought about by the walls of the Madras Leper Asylum. Therethe walls around the asylum highlighted the ambiguous status of theleprosy-affected person: “Many leprosy sufferers were not entirelyconvinced of their status as patients in the Madras Leper Hospitaland feared that once they had entered the asylum they would be
108. Thomas R. Metcalf, “Architecture and the Representation of Empire: India,1860–1910,” Representations, 1984, 6, 37–65, 38.
109. Bailey, Visit, 59–60; and Bailey, Glimpse, 170.110. Bailey, Glimpse, 312–13; Bailey, Visit, 79; Bailey, Lepers of Our Indian Empire, 219.111. Bailey, Visit, 32.112. Bailey, Glimpse, 149; and Bailey, Lepers of Our Indian Empire, 41–42.
Robertson : The Leprosy Asylum in India 501
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

prevented from leaving. . . . Rumours had already gone abroad thatthe hospital was indeed a prison for incarceration of the leprosy suf-ferers in Madras.”113 Additionally, the contest between medicalauthorities and the government over the height of the wall“reflected the complexity and incoherence of British notions ofconfinement and charitable care for leprosy sufferers in Madras.”114
Surrounding walls seemed to become increasingly necessary forthe construction of new asylums. But, if the example of the asylumat Pui can be relied upon, the nature of the wall could vary. Whenthe Collector of the District wanted this asylum fenced, the Missionto Lepers planned to plant a prickly pear hedge around it at a costof about ten rupees an acre.115 At the Chandag asylum, which wasacquired by the Mission to Lepers, a row of nine houses was built alittle down the hill and to the north of the main bungalow.116
Once again, there seems to have been no attempt at enclosing thesite. Nonetheless, it seems that the general practice was to erect asurrounding wall, and when the Mission to Lepers constructed thenew asylum at Alleppey, they built a surrounding brick and mortarwall, and the new shelters for the people at Rurki were enclosed ina courtyard.117 While the inmates of Purulia were strictly prohibitedfrom going to the town, there were no guards or walls or fences ofany kind. Reverend Hahn, the Superintendent of Purulia, reportedthat the aim was to manage the asylum by attracting people ratherthan by using “forcible detention.”118
Courtyards were also remarked upon as offering a pleasant spaceand as forming a focal point for an asylum. Early sites that pre-existed the Mission to Lepers were described by Bailey as havingpleasant courtyards. The courtyard to the Agra Asylum wasdescribed as cool and shaded by several fine trees.119 TheDharmsala Leper Asylum in Ahmedabad was a large open place
113. Buckingham, Leprosy in Colonial South India, 54.114. Ibid., 59.115. Bailey, Visit, 85.116. Bailey, Glimpse, 121–22.117. Bailey, Lepers of Our Indian Empire, 216; and Bailey, Visit, 66.118. Conference Purulia, 71. Independently of the Mission to Lepers, the new Acworth
asylum at Matunga, in Bombay, constructed by the Municipality, was surrounded by abarbed-wire fence. (Bailey, Lepers of Our Indian Empire, 222; Pandya, “Leprosy in theBombay Presidency,” chap. 9.)
119. Bailey, Glimpse, 170.
Journal of the History of Medicine : Vol. 64, October 2009502
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

with large trees and surrounded by a wall.120 The compound atBhagulpore was considered to be very beautiful and suitable as anasylum.121 A line of graceful plantain trees grew between the tworows of huts in the middle of the Cochin enclosure.122 Underthe direction of the Mission to Lepers, courtyards became increas-ingly structured. The modest huts by the wayside at Rurki becamepart of a larger establishment with a courtyard and a large shadytree.123 On Bailey’s third trip, it is described as being an enclosedspace with a large shady tree, seven houses, a church, andgardens.124 When the Mission rebuilt Alleppey, they constructed acourtyard one hundred yards square with coconut trees in thecenter.125
SEPARATIONS WITHIN THE COMPOUND
In 1889, the British government required that asylums separate menand women stating that:
His Excellency in Council expressed the opinion that in such institutionsthe necessity of strictly segregating the sexes should invariably be kept inview, and desired that this condition should be enforced in the case ofevery institution for the relief of lepers receiving aid from public funds,and that every effort should be made to induce the supporters of insti-tutions of the kind maintained by voluntary contributions to adopt asimilar rule.126
The reason for this requirement was expressed by Gavin Milroy in1874 in response to Carter’s report on Norwegian measures to dealwith leprosy. Speaking for the Royal College of Physicians ofLondon, he stated:
The fact that Leprosy is transmitted by parent to child is indisputable, andas Leprosy by descent is often through a natural error (mistaken forLeprosy by contagion, the members of one family being naturally in
120. Ibid., 177–78.121. Bailey, Visit, 55–56.122. Bailey, Glimpse, 37.123. Bailey, Lepers of Our Indian Empire, 66.124. Bailey, Visit, 66.125. Bailey, Lepers of Our Indian Empire, 216.126. The original opinion of 1889 is reproduced in Government of Bengal,
“Segregation of Pauper Lepers,” 1895, File 3-L/4 16, no. 30, 1, Municipal Department,Medical, 1/12135, Orissa State Archives, Bhubaneshwar, Orissa.
Robertson : The Leprosy Asylum in India 503
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

contact, it is important that this fact should be borne in mind. It is a factwhich points also to the expediency of placing asylums for females at adistance from asylums for males when circumstances permit, and whenthe numbers are such to justify separate establishments.127
Nevertheless, in structures that existed before the changes broughtabout by the Mission to Lepers, there were inconsistencies in theapplication of these policies. In the Agra asylum, men and womenoccupied different sides of the courtyard, but the Dharmsala inBombay, which was roundly condemned by Bailey, made no suchdistinction.128 At Dehra and Sehore, Bhopal State, there were separ-ate large courtyards for men and women, and at Moradabad, themen were in one yard and the women were in another, with a lineof houses back to back acting as a division and a barrier.129 On alarger scale and breaking with the courtyard enclosure structure, inthe asylum run by the London Missionary Society at Almora, thewomen’s terraces were separated from the others by a wall runningthe whole length of the terrace.130
Kakar states that many features of the medieval European leprosyasylum were reproduced in India and, as a result, practices such assexual segregation and sexual abstinence were implemented withoutquestion, but there were other pressures that reinforced this impera-tive.131 Benefactors of the Mission to Lepers were adamant that menand women be kept apart: first, there was no intention of supportingleprosy-infected men and women in dubious moral conditions, butthe possibility of births and the chance of infecting children withleprosy became an equally strong reason for separation. Increasingly,the Mission constructed asylums that would keep men and womenseparate. By 1895, at Alleppey, a wall was added down the middle ofthe enclosure, and at Asansol, at the same time, the length of thenew site was considered advantageous because it would be possibleto have men’s quarters at one end and women’s at the other.132
127. Gavin Milroy to the Honourable R. H. Meade, 8 September 1874, vol. 35, 1875,191–99, General Department, Maharashtra State Archives, Mumbai, India.
128. Bailey, Visit, 170; and Bailey, Glimpse, 10.129. Bailey, Glimpse, 312–13; Bailey, Visit, 11; and Bailey, Lepers of Our Indian Empire
69–70.130. Bailey, Glimpse, 111.131. Kakar, “Medical Developments,” 65–66.132. Bailey, Lepers of Our Indian Empire, 177, 217–18.
Journal of the History of Medicine : Vol. 64, October 2009504
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

Although Bailey was troubled by the separation of elderlymarried couples in particular and married couples in generalbecause it went against Christian principles, it is without doubt oneof the features of asylums that he never fails to remark on. Heapproved of the situations in which the sexes were separated, andstrongly disapproved of the instances where men and women werefree to mix with each other. Debates about segregation were on theagenda of meetings of superintendents of the asylums well into theearly twentieth century.
In 1908, superintendents still debated whether to separateleprosy-affected people, who were already married, from eachother, and the Conference at Purulia was reminded by Bailey, theChairman of the Conference, that “many subscribers at homerefused to assist the Mission unless assured that all lepers were care-fully segregated,” but practices in asylums still varied.133 In thePunjab, married couples were allowed to live together. In theUnited Provinces, segregation was still in the process of being intro-duced in 1908, and couples who had been in residence for sometime were permitted to live together.134 Further south, segregationwas strictly enforced. When Bailey visited Purulia in 1891, themen’s quarters and women’s quarters were separated by a high wall,with a door that was locked at night.135 In the same year, Dr.Hilson, the Surgeon-General and Inspector-General of CivilHospitals, from Bengal, visited Purulia and reported that he waspleased with arrangements for the segregation of the sexes. He alsonoted that children were housed in separate buildings “and whileallowed to see their parents occasionally, do not have any close orintimate connection with them.”136 This process of segregationcontinued unevenly, but irrevocably, with the 1908 conference ofleprosy asylum superintendents recommending the segregation ofthe sexes, except in exceptional circumstances.137 Even in 1941, thegovernment of India’s report stated that it was desirable for married
133. Conference Purulia, 20.134. Ibid.135. Bailey, Lepers of Our Indian Empire, 122–23; Rev. K. W. Nottrott, “Segregation of
the Sexes; and of Untainted Children,” Conference Wardha, 26. Discussion of the segre-gation of children is outside the scope of this article.
136. Hilson cited in Bailey, Lepers of Our Indian Empire, 128.137. Conference Purulia, 21.
Robertson : The Leprosy Asylum in India 505
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

life in leprosy institutions to be forbidden unless the woman wasbeyond child-bearing age.138
STRUCTURES WITHIN THE COMPOUND
The constructions within the asylum compound were oftenarranged in rows and barracks, and their placement was governedeither by the terrain upon which they were built or the availabilityof local building materials. Under the supervision of the Mission toLepers, these constructions became more standardized. The inten-tion of the overall design was to provide shared accommodation forliving, rather than to create a hospital, although something of thecharacter of a monastic retreat is retained by having small rooms. In1886, the Cochin Lazarus Hospital was in a large compound, withtwo sets of fourteen houses arranged in two rows of seven: one rowfor men and the other for women. These were placed back to backand parallel with each other, and each row was enclosed with arailing and a gate. The structures at the government institution atTarn Taran were also arranged in two long rows of double housesthat were placed back to back.139 At Sehore in Bhopal State, a longrow of houses opened into each of the two separate courtyards.140
Some asylums such as the asylum at Almora were designed as bar-racks, with three barracks of five houses each, on each of the threecentral terraces.141 At Baba Lakhan, too, there were three barracksparallel to each other containing twenty-four rooms each (twelveon either side, back to back), and providing accommodation forseventy-two inmates.142 Eventually barracks gave way to cottageaccommodations that were described in the Central Provinces(Champa) as a preferred example in 1920 to the attendees at theCalcutta conference, when the Superintendants from the variousasylums gathered to confer with each other, pool their experiences,and standardize their practices.143 These cottages were 48 feet longand 31 feet wide, with walls 14 feet high and one and a half feetthick. Each had three 12 by 14 feet living rooms and corresponding
138. Government of India, Report on Leprosy and its Control in India, 43.139. Bailey, Glimpse, 154.140. Bailey, Visit, 11.141. Bailey, Glimpse, 111.142. Bailey, Visit, 82–83.143. Conference Calcutta, 91–94.
Journal of the History of Medicine : Vol. 64, October 2009506
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

7 by 14 feet veranda rooms. Each of the three main rooms couldaccommodate four people, and the veranda rooms were for cookingor for sleeping. Ventilation was provided by transoms, two endwindows, and also by low partition walls that did not reach to theroof of the building.
Local materials and local building practices had a determininginfluence over the built environment of the leprosy asylums in India.The structures within the new courtyard at Rurki consisted of sevensmall mud houses with tiled roofs and a church made of the samematerial.144 The asylum at Pui in the Kolaba district of the BombayPresidency consisted of a pucca building, made of stone and lime,with a roof of Mangalore tiles. It had two rows of five rooms that wereplaced back to back, with a verandah in front of each set of rooms.The partitions between the rooms were of rods covered in plaster.145
New structures were invariably grafted onto what was already stand-ing. At Bhagulpore, e.g., in addition to the already-existing old bun-galow, five wards were added so that each ward had three large roomseach and each room accommodated four people.146
By 1920, superintendents of the asylums were directed by theMission that accommodation be constructed from substantial materialssuch as bricks that were either pointed or plastered. All wood workwas to be of sawn timber and the doors and windows were to bemade of seasoned timber. The roof had to be built out of materialsthat would be rainproof. Floors could vary with location. In Calicut,floors were of glazed tiles, in Cuttack, floors were of cement, and inthe Central Provinces, mud floors were preferred because they werenot so cold and could be cleaned daily with disinfectant.147
The surroundings of asylums were often described by Bailey, andmany asylums were considered to be situated in particularly beauti-ful settings. The emphasis on gardens and trees served to soften theimpression of the asylum and to create a sense of a gardenretreat.148 Before improvements by the Mission to Lepers, the
144. Bailey, Lepers of Our Indian Empire, 66.145. Bailey, Visit, 74.146. Ibid., 55–56.147. P. A. Penner, “The Best Type of Ward,” Conference Calcutta, 88.148. The effect of settings for the leprosy asylum on Robben Island, in South Africa, is
discussed in Harriet Deacon, “Landscapes of Exile and Healing: Climate and Gardens onRobben Island,” South Afr. Archaeol. Bull., 2000, 55, 147–54.
Robertson : The Leprosy Asylum in India 507
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

asylum at Ahmedabad was described as being beautifully situated ina grove of fir trees and next to a tea garden, and the women’s hutsat Saharanpore were near some old gardens and close to a mangogrove.149 The asylum at Dehra also stood in the middle of a greenplain, with groves of mango trees, and it was approached by a longroad lined with trees.150 Bailey described the asylum at Chumba,which he built himself in 1875, as being beautifully situated on oneside of the Ravi river, about two miles from the city. This asylumwas to be found down “a lovely road” that followed “the rightbank of the river.”151 The area around the asylum at Chandag,which had originally belonged to a European settler and then tothe Mission to Lepers, was also described by Bailey as spectacular:
In front of the houses and to the east, there was a fine row of blue gumtrees, and this was expected to provide shade in the warm weather. Therewas a well-cut path from the main road up to the house, lined withyoung cedar trees; and on the left on the approach, a piece of ground waslaid out for a garden, and some hundreds of English fruit trees of differentsorts were growing. The whole stands on the top of a ridge, with a beau-tifully fertile valley sloping away to the west . . . in the midst of a greatamphitheatre of hills, stands Pithoragarh. There are high hills all round,while to the north are to be seen several peaks of the “Snows.” On thenorth end of the ridge on which Chandag stands, and on a tableland, is atemple, at which a great mela [explain] is held every August. Altogether,this place is beautifully situated.152
If the surroundings of the asylum were unappealing, every effortwas made to improve them, especially by planting trees to provideshade. While the new Moradabad asylum was situated away fromthe city and close to the lake, it was not wholeheartedly endorsedby Bailey because it was situated on a bare stretch of groundwithout shade and he thought that one of the few disadvantages ofthe site chosen for the new asylum at Asansol was a lack of trees,but there were plans to plant some immediately.153 Generally, thenew establishments took the need for having surrounding trees intoaccount so that, e.g., the new asylum at Neyoor was built on
149. Bailey, Glimpse, 131, 177–78; and Bailey, Lepers of Our Indian Empire, 64–65.150. See quotation from Bailey, Glimpse, 312–13.151. Bailey, Lepers of Our Indian Empire, 41–42.152. Bailey, Glimpse, 121–22.153. Ibid., 69, 177.
Journal of the History of Medicine : Vol. 64, October 2009508
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

elevated ground which ran down towards a large piece of water,fringed by Palmyra palms and other trees, and the new asylum atSrinagar was built near a magnificent crimson flowering chunartree.
This emphasis on aesthetic surroundings cannot be disregarded.It was obviously important to demonstrate that the new asylumswere well situated in ways that would soothe the inmates.Additionally, the beauty of the physical landscape was often anoccasion for a meditation on the contrast between the beauty of thesurroundings and the condition of the people affected with leprosy.
AGRICULTURAL COLONIES
By degrees the asylums sponsored or owned by the Mission focusedupon providing garden plots needing to be tended in order tooccupy the inhabitants, and also to allow the asylum to becomeincreasingly self-sufficient. The courtyard of the newly enlargedasylum at Rurki included some small gardens with shrubs and treesin the center, and adjoining land with shady trees.154 Bailey notedthe blossoming peach and apricot trees in front of the houses atSubathu Leper Asylum. At this asylum, the inmates also cultivatedtheir own gardens.155 At Tarn Taran, one of the improvementsinfluenced by the Mission to Lepers was the laying out of smallplots for those who were able to use them:
The surroundings of the asylum are much improved; nice little plots ofground having been laid out, and given to the inmates capable of cultivat-ing them. There is an abundant supply of water, so that the plots areeasily worked, and the lepers take great pleasure in them, besides whichthe work is very good for them. 156
The Leprosy Investigation Commission of the British NationalLeprosy Fund initially suggested the idea of “experimental lepercolonies or farms in rural districts” for people affected by leprosy, inits report of 1891, and this idea was reiterated by the government ofIndia in 1895:
154. Bailey, Lepers of Our Indian Empire, 96–98; and Bailey, Visit, 66.155. Bailey, Glimpse, 138.156. Bailey, Visit, 76.
Robertson : The Leprosy Asylum in India 509
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

it may, it appears to His Excellency in Council, be found desirable toestablish lepers asylums or farms in remote places outside municipal areasand within the jurisdiction of a Local Board. The Bill might provide forthe sending of pauper lepers to such asylums or farms without bringinginto operation the powers of arresting pauper vagrants within the areasfrom which lepers may be permitted to be sent to them.157
Influenced by this and developing what had already begun, sites forasylums with the potential for farming and gardening were increas-ingly sought out. The Mission to Lepers’ acquisition of Chandagwas considered favorably by Bailey because it had extensivegrounds, some of which were laid out in terraced fields of wheatand rice.158 There were also plans at Subathu for larger agriculturalprojects.159 At Asansol, fields suitable for cultivation were includedin the site, and at Rawalpindi, little plots of ground were laid outfor cultivation. By 1934, the asylum at Raniganj, in Bengal, wasreferred to as a “model garden-town.”160
In concert with attempts to persuade the government of India toamend the 1898 Lepers Act by widening the definition of “theleper” from applying to those “in the process of ulceration” toinclude “any person suffering from any variety of leprosy,” the ideaof large leprosy settlements or agricultural colonies was devel-oped.161 The practicality of this idea was canvassed at the 1920
Conference of Superintendents in Calcutta. The Reverend FrankOldrieve, the Secretary for India for the Mission to Lepers,expressed the aspirations of the conference when he stated that“The compulsory segregation of all lepers in India is not, in myopinion, a practical question, but the segregation of even 20,000 or30,000 pauper lepers, if there should be so many, is certainly a thingthat can be attempted, and if it can, then the attempt should most
157. National Leprosy Fund, Report of the Leprosy Commission in India (ExecutiveCommittee: William Clowes and Sons, 1893), 389; and Government of Bengal, “Bill toProvide for the Segregation of Pauper Lepers: From J. P. Hewett, Offg. Sec. to theGovernment of India to the Secretary to the Gov. of Bengal, Municipal Government,” 7
February 1895, 12/132, File 3-L/4 14, no. 28, Municipal Department, Orissa StateArchives, Bhubaneshwar, Orissa.
158. Bailey, Glimpse, 121–22.159. Bailey, Visit, 74.160. Bailey, Lepers of Our Indian Empire, 7–8, 177; Mission to Lepers, Sixty Years of
Service, 1874–1934, on Behalf of the Lepers and Their Children (London: Mission to Lepers,1934), 31.
161. Mission to Lepers, Conference Calcutta, ii, 141.
Journal of the History of Medicine : Vol. 64, October 2009510
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

certainly be made.”162 This was to be achieved by establishing largesettlements throughout India.
The 1920 Conference of Superintendents in Calcutta was toldthat the new idea of “the settlement” was to be “a place wherethere is as much as possible the idea of community life.”163 It wasto be so attractive that the pauper would be willing to remain therewithout restraints, with the best wards that could be designed andthe best medical attention available. The buildings would include acentral hall, a hospital for advanced cases, a dispensary where treat-ment would be given, school buildings for the young people in theasylum, and recreation rooms where people could amuse them-selves. There would be work available, beside plantation work,which would receive remuneration: “in this way the inmates wouldbe kept from thinking too much about their miseries, while itwould help keep down the cost of maintenance if a good many oftheir needs were supplied by themselves.”164
In a study of model agricultural colonies in the Netherlands andIndonesia, Albert Schrauwers claims that such utopian spaces (inthe service of a form of socialist idealism) were designed “as ameans of eliminating pauperism in a wide variety of settings, inradically divergent forms, throughout the early nineteenthcentury.”165 They sprang from a common regime of value:
Whether through the colonies of the Benevolent Society in theNetherlands, Fourier’s phalanxes in France, Robert Owens’ NewHarmony, or a variety of religious sects such as the Shakers and theOneida perfectionists in America, the idiom of charity and pauper reliefinspired a spate of intentional communities marked by communal pro-duction for the market.166
162. Ibid., 70–71.163. Ibid., 70.164. Ibid. This movement was not only confined to India. In 1906, Colombia and
Venezuela developed their own agricultural colonies for leprosy-affected people, and thehospital and agricultural colony of Fontilles in Spain was established in1907. J. Bernabeu-Mestre and T. Ballester-Artigues, “Disease as a Metaphorical Resource:The Fontilles Philanthropic Initiative in the Fight against Leprosy, 1901–1932,” Soc. Hist.Med., 2004, 17, 409–21.
165. Albert Schrauwers, “The ‘Benevolent’ Colonies of Johannes van den Bosch:Continuities in the Administration of Poverty in the Netherlands and Indonesia,” Compar.Stud. Soc. Hist., 2001, 43, 298–328, 319.
166. Ibid., 319.
Robertson : The Leprosy Asylum in India 511
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

He argues that these colonies presented a solution to poverty at atime when global commodity markets were restructuring productiverelations around the world.167 In concert with this solution to pau-perism, as the asylums that were sponsored by the Mission toLepers changed their structure, provision for the leprosy-affectedinmates to engage in gardening and farming and other productiveactivities that would enable a degree of self-sufficiency emergedmore and more strongly, until the asylum that was set up as an agri-cultural colony became one of the preferred options.
Frank Oldrieve’s grand idea was never completely realized, as in atotal of ninety-five institutions in India, both Mission and State,only 13,676 people were institutionalized in 1941, but certainasylums developed into large settlements with many hundreds ofinmates.168 By 1941, the largest institutions (over 500) were Purulia,in what was then Bihar, with 805 people; Chandkhuri and Champain the Central Provinces, with 554 and 550, respectively;Chingleput, in the Madras Presidency with 800; Naini (Allahabad)in the United Provinces with 500; and Dichpali in Hyderabad (theNizam’s Dominions) with 800 (see Figures 3 and 4).
The idea of the agricultural colony for leprosy-affected peoplenever really died out. In 1937, rehabilitated inmates of an asylumhad begun to clear virgin forest land in the Central Provinces. Theywere referred to as “pioneers” and “settlers-to-be.” The intentionwas to give “ex-patients a stake in the land, a healthy occupationcarried on under sympathetic oversight, and such necessary supportas may be required until the settler has won for himself resourcesfor times of difficulty.”169 Again in 1942, colonies were rec-ommended as the center of anti-leprosy work for the districts inOrissa and Bihar, by the Indian Council of the British EmpireRelief Association, for infectious cases or for those who neededtreatment other than that provided by clinics. The colonies couldalso serve for the cultivation of Hydnocarpus wightiana trees as asource of income, and the Forest and Agricultural departmentswere to be consulted for suitable sites for colonies with 100 acres of
167. Schrauwers, “Benevolent Colonies,” 320.168. Government of India, Report on Leprosy and its Control in India, 60.169. The Mission to Lepers, A Report of the Sixty-Third Year’s Work in India and Burma:
September 1936-August 1937, issued by the Indian Auxiliary in India, 4–5, accessed inLeprosy Mission International Archives, Brentford, London, UK.
Journal of the History of Medicine : Vol. 64, October 2009512
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

Fig. 3. “Our Purulia Leper Asylum, Bihar (From a photograph of a model),” in Wellesley C. Bailey, Fifty Years Work forLepers, 1874–1924 (London: Mission to Lepers, 1924), 24.
Robertson
:T
heL
eprosyA
sylum
inIn
dia513
at UQ Library on August 10, 2015 http://jhmas.oxfordjournals.org/ Downloaded from

arable land each.170 The feudatory states of Orissa were consideredideal as they possessed “plenty of lands which can be spared for thecolonies.”171 The Dewan of Baudh State was instructed to set aside640 acres, five miles from Baudh. The patients were to produce atleast half of their food and to this end they were to be offered “afew acres of land.” They were also to be encouraged to bring theirown bullocks and agricultural implements. In this instance, families
Fig. 4. “Women at Work in the Rice Fields at Purulia Asylum,” in Rev. FrankOldrieve, The Mission to Lepers: A Statement of Its Work in India with Financial andother Information (Cuttack: Orissa Mission Press, 1921), opposite page 9.
170. See John Parascandola, “Chaulmoogra Oil and the Treatment of Leprosy,” Pharm.Hist., 2003, 45, 47–57; Shubha Pandya, “Ridding the Empire of Leprosy: Sir LeonardRogers FRS (1868–1962) and the Oil of Chaulmoogra,” unpublished paper presented at“Health and Medicine in History: East-West Exchange: Third Conference of the AsianSociety for History of Medicine,” Jawaharlal Nehru University, New Delhi, 2–4
November 2006, copy supplied by author; and G. Verghese, “Epidemiological Features ofLeprosy in Orissa,” Leprosy in India, 1942, 14, 4, 135.
171. Isaac Santra, Report to the Political Agent, Orissa States, 1105/1 BELRA, 9 April1946, Orissa State Archives.
Journal of the History of Medicine : Vol. 64, October 2009514
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

were to be welcomed into the colony. Doing this would also servemedical ends: “This is a good idea as it will make their life comfor-table and give us the opportunity to observe the contacts, especiallythe children. Those who bring their families may be given separatecottages and separate pieces of land.”172
At the 1934 Jubilee Celebrations of the Mission to Lepers in India,messages of gratitude from the residents of leprosy asylums in Indiawere included in the celebration booklet. The message from Purulia,Bihar, was written in Hindi by one of the elders called Bibhabati.Describing the leprosy asylum at Purulia as an ashram, he referred to“the beautiful hospital buildings and the good nursing and doctor’sarrangements” that had grown out of what had been established in1884.173 An ashram usually means “a place of religious retreat, sanctu-ary, or hermitage,” and it carries the connotation of spiritualhealing.174 Thinking of a leprosy asylum as an ashram complicates thismeaning by suggesting a tension between physical and spiritualhealing. At a time when a cure for leprosy was so uncertain, anashram provided a place that could, at the very least, soothe the spirit.When Bibhabati referred to the asylum as an ashram and in the samebreath commented on its medical arrangements, he linked both setsof aspirations expressed in the architecture of the leprosy asylum atPurulia: the aspiration both to soothe the spirit and to heal the body.What he does not express are the economic regimes of value whichmade these asylums possible and within which they developed andchanged their identity. The built environment of these asylums washighly structured and was as responsive to economic imperatives asmissionary and medical values. While these asylums functioned asshelters for bodies and also as places that would at the very leastsoothe sufferers, they also provided their inmates with useful occu-pations. As the architecture of the asylum was changed, the aim alsowas to provide work. In a manner that fitted perfectly with the valuesof a Protestant Missionary organization, people with leprosy were
172. Isaac Santra, “Isolation of Leprosy Cases in the Baudh State,” 1105/2, 9 April1946, Orissa State Archives.
173. Bibhabati, prachina (elder) “A Message from Purulia, Bihar,” trans. Rev. E. B.Sharpe, in Mission to Lepers, Sixty Years of Service 1874–1934 (London: Mission to Lepers,1934), 12.
174. See entry for “asylum” in Oxford English Dictionary, 2nd ed. (1989; Oxford,Oxford University Press, 2009), accessed online at http://www.oed.com (accessed 12 May2009).
Robertson : The Leprosy Asylum in India 515
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

increasingly offered productive occupations that contributed to thesustenance and self-sufficiency of their asylums. Their labor symbo-lized their economic and their psychological rehabilitation, andfound one form of expression, among others, in the self-sustaining,agriculturally based leprosy settlement.
CONCLUSION
In conclusion, in order to begin to differentiate the variety ofleprosy asylums built throughout the world, this article has devotedits attention to the characteristics of the leprosy asylum in India from1886 to 1947. There, leprosy asylums were restructured by theactivities of the Mission to Lepers in India, and the changes financedout of a tradition of subscription and benevolence that coincidedwith British and Indian practices. This response was incremental andpiecemeal and expressed in the appropriation of land and thedevelopment of the built environment. It was enabled by a politicalsituation that opened a space for missionary participation so thatspiritual, medical, and economic regimes of value coincided at atime when little could be done to alleviate the suffering of thosewith leprosy. Consequently, pleasant surroundings, shady trees,sound accommodation, and good ventilation became desirable com-ponents of an asylum that would confer physical and psychologicalbenefits for residents. In addition, while it was never necessaryforcibly to isolate inmates, men, women, and children were increas-ingly segregated in such institutions. Gradually, the spaces of theasylum became more highly structured: walls provided seclusion,courtyards were cool and shaded, and buildings were provided toensure a degree of self-sufficiency. Increasingly, emphasis was placedon the need to occupy the inhabitants so that larger colonies weredeveloped where inmates produced their own food and made theirown clothes, rather than sustaining themselves by begging. Oneform of the leprosy asylum in India found expression in the agricul-tural colony, which symbolically reincorporated the body damagedby leprosy into the economic world of productive relations.
EPILOGUE
This is not the place for an extended analysis of the ways in whichleprosy-affected people were both coerced and enabled by leprosy
Journal of the History of Medicine : Vol. 64, October 2009516
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from

asylums, but it is important to realize that the complexities of thisprocess of incorporation do not end in the asylum and cannot berelegated to the past. Today, in India, people whose lives were con-nected to these asylums, whether as past leprosy sufferers or as theadult offspring of leprosy-affected parents, seem to function as aself-enclosed “caste.” Many still dwell in a multitude of self-formedcommunities, in villages, clustered around the old colonies.175 Itseems to be impossible to disentangle the degree to which colonial-ism and missionary activity or leprosy, as a socially stigmatized andself-stigmatizing disease, is responsible for this complex process ofidentity formation. While the structures of colonialism seem lessapparent today and the changes wrought by Christianity are stillapparent, it is the taint of leprosy that seems to linger longest.
175. These views were formed from three field trips over three years to leprosy coloniesin order to meet people still living in or adjacent to colonies in Orissa, Chhattisgarh,Tamil Nadu, Madhya Pradesh, Uttar Pradesh, and Maharashtra.
Robertson : The Leprosy Asylum in India 517
at UQ
Library on A
ugust 10, 2015http://jhm
as.oxfordjournals.org/D
ownloaded from
Related Documents