THE INTRODUCTION OF UMBILICAL ARTERY LACTATE SAMPLING AS A TOOL TO IMPROVE INTRAPARTUM CARE IN SOUTH AFRICA Dr Emma Rose Allanson MBBS (Hons) MPHTM FRANZCOG A thesis submitted in total fulfilment of the requirements of the degree of Doctor of Philosophy Division of Obstetrics and Gynaecology, Faculty of Health and Medical Sciences The University of Western Australia 2019

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

THEINTRODUCTIONOFUMBILICALARTERYLACTATESAMPLINGASA
TOOLTOIMPROVEINTRAPARTUMCAREINSOUTHAFRICA
DrEmmaRoseAllanson
MBBS(Hons)
MPHTM
FRANZCOG
Athesissubmittedintotalfulfilmentofthe
requirementsofthedegreeof
DoctorofPhilosophy
DivisionofObstetricsandGynaecology,FacultyofHealthandMedicalSciences
TheUniversityofWesternAustralia
2019

ii
DEDICATION
ForBenjaminandTheodore,whoareeverything.

iii
INMEMORIAM
TeresaIka
1967-2010
Aboveall,forteachingmetoalwaysfightwithequalmeasuresofstrengthandgrace.

iv
ABSTRACT
Perinatal mortality remains one of the most pressing global health problems, and
improvementsinthequalityofcarearoundthetimeofchildbirthhavethepotentialto
save millions ofwomen’sand newborn lives, particularly in low and middle-income
countries (LMIC).One of the major contributors to perinatal mortality in LMIC is
intrapartum hypoxia and its sequelae, for which the lack of consistently available
qualityintrapartumcareisasignificantcontributor.
The ability to identify andmanage acute intrapartumhypoxia is a significant clinical
challenge,andthecapacitytoachievethisinaLMICformsthebasisofthisthesis.The
specific focus of this thesiswas a comprehensive series of clinical trial and data set
analysesbasedinoneLMIC,SouthAfrica,wheretheperinatalmortalityrate(PNMR)is
33 per 1000 births,with 5 deaths per 1000 births being attributable to intrapartum
asphyxia. Thus, the principle aim of this research was to use the concept of a
commonlyusedtoolinhigh-incomecountries(measurementoffetallactatetoassess
acidosis at birth from an umbilical cord sample), and apply it in a resource limited
settinginordertoimproveintrapartumcare.
Wehypothesisedthatintroducingumbilicalartery(UA)lactatesamplingasaqualityof
care feedback tool would modify clinicians’ behaviours and improve maternal and
neonataloutcomesovertime.Inordertotestthishypothesis,itwasnecessarytofirst

v
develop an understanding of perinatal mortality in South Africa, secondly to be
assuredofthediagnosticaccuracyofUAacidosistestingwithlactate,thirdlytoexplore
theimpactofqualityofcareaudit,andfinallytoimplementUAlactatetesting,assess
itsimpact,anditsfeasibilityoutsideofaresearchsetting.Theconceptsexploredand
analysesusedareoutlinedbelow:
1. Tounderstand the causesofperinataldeath in SouthAfricausingpopulation
baseddata. Frequency distributionswere performed for outcome summaries
and Fisher’s exact test was used to interrogate the relationship between
maternalconditionsandperinatalmortality,andthetimingofperinataldeath.
2. To synthesise the existing evidence on the diagnostic test accuracy of UA
lactate inmeasuring fetal acidosis and predicting poor neonatal outcome by
comparing lactate with other assessments of acidosis in the immediate
newborn and by assessing the capability of lactate to predict neonatal
outcomes. A meta-analysis of correlations was performed applying the
hierarchical summary receiveroperatingcharacteristicsmodelandabivariate
model.
3. Todeterminetheimpactofqualityofcareauditonperinatalmortality in163
facilities inSouthAfricawithat leastfiveyearsofcontinuousaudit.Temporal
trends in perinatal mortality rates were tested using the extended Mantel-
HaenszelM2statisticwithonedegreeoffreedom.
4. To investigate the utility of UA lactate measurements in a South African
hospital for assessing intrapartum care and predicting neonatal outcomes.

vi
Using receiver operator curve (ROC) analysis, the optimal lactate cut-off for
discriminatingbetweentherequirementforneonatal resuscitation,admission
tonurseryandApgar<7at5minuteswasdetermined.
5. To ascertain the clinical impact of introducing UA lactate sampling, in
conjunctionwitheducationoncardiotocograph (CTG) interpretationand fetal
andlactatephysiology.Usinglinearandlogisticregressionanalysis,theimpact
of introducing UA lactate sampling onmaternal and neonatal outcomeswas
determined.
6. To assess theUA lactate results, and intrapartum and neonatal outcomes of
mothers with and without human immunodeficiency virus (HIV) infection.
Univariate comparisonsweremade using independent t-tests for continuous
outcomesandChi-squareorFisherexacttestsforcategoricalcomparisons.
7. ToassesstheattitudesandbarriersofclinicalstafftotheimplementationofUA
lactate in South Africa. In addition to descriptive statistics, the relationship
between various attitudes and barriers before and after a training program
wereanalysedusingFisher’sexacttest,andordinalregressionmodelsusedto
interrogate the role of various factors (e.g. age) on the identification of
individualbarriers.
There are several original contributions arising from this thesis, including the first
systematicreviewandmeta-analysisofthediagnostictestaccuracyofumbilicallactate
formeasuringacidosisandpredictingneonataloutcome,acomprehensiveanalysisof
theimpactofqualityofcareaudit,andthelargestassessmentofaninterventionusing

vii
UA lactate measurement and its impact in a LMIC on intrapartum obstetric
management.Specifically,thekeyfindingsareasfollows:
• In a comprehensive data set representative of a total obstetric population in
South Africa, 49.5% and 74.2% of women having a late stillbirth or early
neonataldeath, respectively,werehealthy (nocomplicationsofpregnancyor
labour)andaquarteroftheperinataldeathsfollowedintrapartumasphyxia.
• Inthefirstsystematicreviewofthediagnostictestaccuracyofumbilicallactate
for measuring acidosis and predicting neonatal outcome, including 38,284
women, lactate was shown to correlate with pH (pooled ES -0.650 95% CI -
0.663to-0.637,p<0.01),BE(pooledES-0.71095%CI -0.721—0.699,p<0.01),
andApgarscoreat5minutes(pooledES0.395%CI0.193-0.407p<0.01).Using
thecommonthresholdoutcomeofHIE,lactatehasasensitivityof69.7%anda
specificityof93%.
• In the largest analysis of the impact of QoC audit on perinatalmortality,we
interrogatedthechangesinPNMRin163SouthAfricanfacilitieswithatleast5
yearsofcontinuousQoCauditdata.3,406,347birthsand85,728deathswere
included and 29% of facilities had a decrease in their PNMRwith 5 years of
continuousQoCaudit.Facilitieswithincreasingmortalityappearedlesslikelyto
haveacomprehensiveQoCauditprocess.
• Ina largecohortof946babieswithaUAlactatesample,wedeterminedthat
theoptimal cut-off for lactate for theoutcomeofneonatal resuscitationwas
5.46mmol/L (sensitivity 68%, specificity 72%). For neonatal admission the
optimal lactate cut-offwas 4.95mmol/L (sensitivity 61%, specificity 59%) and

viii
for an Apgar score of <7 at five minutes the optimal lactate cut-off was
5.65mmol/L(sensitivity64%,specificity69%).
• In a before and after trial assessing the impact of introducing UA lactate
sampling,wefoundnodifferenceinmeanlactate(4.6mmol/L{95%CI4.4-4.8}
comparedwith4.9mmol/L{95%CI4.7-5.1},p=0.089).Howeversuspectedfetal
compromisewasreducedinthepost-interventionperiod:30·2%vs.22·1%,aOR
0·71, 95% CI 0·52-0·96, p=0·027 without worsening neonatal outcomes.
Caesarean section rateswere significantly reduced in the univariate analysis:
pre- 40·3% vs. post-intervention 31·6% (p=0·007). This reduction remained
significantwhenadjustedforpreviouscaesareansection,primiparity,maternal
HIV infection and preterm birth (aOR 0·72, 95%CI 0·54-0·98, p=0·035).
Moreover,emergency caesareandeliveries in theunit asawhole (not just in
women recruited to the trial) decreased from692/2436 (28·4%) to399/2232
(17·0%,P<0·001), andneonatalnurseryadmissionsdecreased from450/2436
(18·5%)to349/2232(15·6%,P=0·010).
• In the 21.6% of women in our before and after trial that were HIV positive,
therewasnoimpactofeithertheirdiseaseortheuseofHAARTonthepreterm
delivery rate, mode of delivery, neonatal resuscitation rate, 1 or 5 minute
Apgarscorebelow7,ortherateofhavingaUAlactatelevel>5.45mmol/L.
• InthefinalstudyassessingtheattitudesandbarrierstointroducingUAlactate
sampling,themajorityofmidwivesanddoctorsprovidingintrapartumcareina
SouthAfricandistricthospitalwerepositiveaboutboththeroleofUAlactate
analysis as well as the potential benefits it provides. Training aided in

ix
overcoming some of the perceived barriers to implementing UA lactate
sampling.
Thethesisoutlinedbelowdemonstratesthattheuseofumbilicalarterylactateisboth
feasible andeffective in SouthAfrica, and can contribute to improvedmaternal and
perinataloutcomes.
SCHOLARSHIPACKNOWLEDGEMENTS
ThisresearchwassupportedbyanAustralianGovernmentResearchTrainingProgram
(RTP)Scholarship.ThisresearchwassupportedbyanAustralianPostGraduateAward,
anAthelstanandAmySawMedicalScholarship,andaWomenandInfants’Research
FoundationGordonKingDoctorofPhilosophyScholarship.

x
DECLARATION
I,EmmaRoseAllanson,certifythat:
Thisthesishasbeensubstantiallyaccomplishedduringenrolmentinthedegree.
This thesis does not containmaterial that has been accepted for the award of any
otherdegreeordiplomainmyname,inanyuniversityorothertertiaryinstitution.
Nopartofthisworkwill, inthefuture,beused inasubmission inmyname,forany
otherdegreeordiplomainanyuniversityorothertertiaryinstitutionwithouttheprior
approval of The University of Western Australia and where applicable, any partner
institutionresponsibleforthejoint-awardofthisdegree.
This thesisdoesnotcontainanymaterialpreviouslypublishedorwrittenbyanother
person,exceptwhereduereferencehasbeenmadeinthetext.
Thework(s)arenotinanywayaviolationorinfringementofanycopyright,trademark,
patent,orotherrightswhatsoeverofanyperson.
Theresearchinvolvinghumandatareportedinthisthesiswasassessedandapproved
by The University of Western Australia Human Research Ethics Committee on the

xi
26/02/2014 (Reference number RA/4/1/6581), the University of Pretoria, Pretoria,
SouthAfricaonthe10/02/2014(Referencenumber7/2014).
Writtenpatientconsenthasbeenreceivedandarchivedfortheresearch involving
patientdatareportedinthisthesis.
Thisthesiscontainspublishedworkand/orworkpreparedforpublication,someof
whichhasbeenco-authored.
Signature:
Date:6thMarch,2019

xii
AUTHORSHIPDECLARATION:CO-AUTHOREDPUBLICATIONS
In accordance with the University of Western Australia’s regulations regarding
Research Higher Degrees, this thesis is presented as a series of journal papers. The
contributionofthecandidateandco-author(s)forthepaperscomprisingchapters3,4,
5,6,7,8and9areherebysetforth.
Detailsofthework:
ThepaperpresentedinChapter4isfirstauthoredbythecandidateandco-authoredbyMariMullerandRobertCPattinsonandispublishedas:
Allanson ER,MullerM, Pattinson RC. Causes of perinatalmortality and associatedmaternal complications in a South African province: challenges in predicting pooroutcomes.BMCPregnancyChildbirth.2015;15(1):37.
Locationinthesis:
Chapter4
Studentcontributiontowork:
EA reviewed the perinatalmortality data from the PPIP database, analysed the dataandwrote thedraftandrevisionsandapproved the finalmanuscript.RPcontributedsignificantlytothestudydesign,reviewedthedraftandapprovedthefinalmanuscript.MMcoordinated all of thedata collection andquality controlled thedata collection,reviewedthedraftandapprovedthefinalmanuscript.
Co-authorsignaturesanddates:
MariMuller
RobertCPattinson

xiii
Detailsofthework:
ThepaperpresentedinChapter5isfirstauthoredbythecandidateandco-authoredby Talal Waqar, Christopher R H White, Ozge Tuncalp and Jan E Dickinson and ispublishedas:
Allanson ER, Waqar T, White CR, Tunçalp Ö, Dickinson JE. Umbilical lactate as ameasure of acidosis and predictor of neonatal risk: a systematic review. BJOG.2017;124(4):584-94.
Locationinthesis:
Chapter5
Studentcontributiontowork:
EAandJDdevelopedthereviewprotocol.EAandCWexecutedthesearchstrategy.EA,CW, TW, and OT completed data extraction and quality assessment. EA and OTundertook the meta-analyses. EA drafted the manuscript. All authors revised themanuscriptandapprovedthefinalversion.
Co-authorsignaturesanddates:
TalalWaqar
HWhite
OzgeTuncalp
JanEDickinson

xiv
Detailsofthework:
ThepaperpresentedinChapter65isfirstauthoredbythecandidateandco-authoredbyRobertCPattinsonandispublishedas:
Allanson ER, Pattinson RC. Quality-of-care audits and perinatal mortality in SouthAfrica.BullWorldHealthOrgan.2015;93(6):424-8.
Locationinthesis:
Chapter6
Studentcontributiontowork:
EAreviewedtheperinatalmortalitydatafromthePPIPdatabase,analysedthedataandwrotethedraftandrevisionsandapprovedthefinalmanuscript.RPcontributedsignificantly to the study design, reviewed the draft and approved the finalmanuscript.
Co-authorsignaturesanddates:
RobertCPattinson
Detailsofthework:
ThepaperpresentedinChapter7isfirstauthoredbythecandidateandco-authoredbyRobertCPattinson,ElizabethANathanandJanEDickinsonandispublishedas:
Allanson ER, Pattinson RC, Nathan EA, Dickinson JE. The introduction of umbilicalcord lactate measurement and associated neonatal outcomes in a South Africantertiaryhospitallaborward.JMaternFetalNeonatalMed.2018;31(10):1272-8.
Locationinthesis:
Chapter7
Studentcontributiontowork:
ERAdesignedthestudy,supervisedtheconductofthestudy,collectedthedata,wrotethe initial manuscript, and approved the final manuscript. EAN contributed to thedesignofthestudy,analysedthedata,andapprovedthefinalmanuscript.RCPandJEDcontributed to the design of the study, supported the conduct of the study, andapprovedthefinalmanuscript.

xv
Co-authorsignaturesanddates:
RobertCPattinson
ElizabethANathan
JanEDickinson
Detailsofthework:
ThepaperpresentedinChapter8isfirstauthoredbythecandidateandco-authoredbyRobertCPattinson,ElizabethANathanandJanEDickinsonandunderreviewwithBMC Pregnancy Childbirth as:Allanson ER, Pattinson RC, Nathan EA, Dickinson JE Abeforeandafterstudyoftheimpactonobstetricandperinataloutcomesfollowingtheintroduction of an educational package of fetal heart rate monitoring educationcoupledwithumbilicalarterylactatesamplinginalowresourcesettinglabourwardinsouthafrica
Locationinthesis:
Chapter8
Studentcontributiontowork:
ERAdesignedthestudy,supervisedtheconductofthestudy,collectedthedata,wrotethe initial manuscript, and approved the final manuscript. EAN contributed to thedesignofthestudy,analysedthedata,andapprovedthefinalmanuscript.RCPandJEDcontributed to the design of the study, supported the conduct of the study, andapprovedthefinalmanuscript.

xvi
Co-authorsignaturesanddates:
RobertCPattinson
ElizabethANathan
JanEDickinson
Detailsofthework:
ThepaperpresentedinChapter9isfirstauthoredbythecandidateandco-authoredbyRobertCPattinson,ElizabethANathanandJanEDickinsonandispublishedas:
Allanson ER, Pattinson RC, Nathan EA, Dickinson JE. Impact of maternal HIV onumbilical cord lactate measurement at delivery in a South African labor ward. Int JGynaecolObstet.2018;141(3):366-70.
Locationinthesis:
Chapter9
Studentcontributiontowork:
ERAdesignedthestudy,supervisedtheconductofthestudy,collectedthedata,wrotethe initial manuscript, and approved the final manuscript. EAN contributed to thedesignofthestudy,analysedthedata,andapprovedthefinalmanuscript.RCPandJEDcontributed to the design of the study, supported the conduct of the study, andapprovedthefinalmanuscript.

xvii
Co-authorsignaturesanddates:
RobertCPattinson
ElizabethANathan
JanEDickinson
Detailsofthework:
ThepaperpresentedinChapter10isfirstauthoredbythecandidateandco-authoredbyKateGrobicki,RobertCPattinsonandJanEDickinsonandispublishedas:
Allanson ER, Grobicki K, Pattinson RC, Dickinson JE. Attitudes towards theimplementationofuniversalumbilicalarterylactateanalysisinaSouthAfricandistricthospital.BMCPregnancyChildbirth.2016;16(1):166.
Locationinthesis:
Chapter10
Studentcontributiontowork:
EAdesignedthestudy,supervisedtheconductofthestudy,analysedtheresultsandwrotetheinitialmanuscript.KGcontributedtothedesignofthestudy,conductedthetrainingand surveysandapproved the finalmanuscript.RCPand JEDcontributed tothedesignofthestudyandapprovedthefinalmanuscript.
xviii
Co-authorsignaturesanddates:
KateGrobicki
RobertCPattinson

xix
Studentsignature:
Date:6thMarch,2019
I, Professor Jan Dickinson, certify that the student statements regarding theircontributiontoeachoftheworkslistedabovearecorrect
Coordinatingsupervisorsignature:
Date:6thMarch,2019

xx
ACKNOWLEDGEMENTS
ItisasomewhatoverwhelmingprocesstositandreflectupontheprocessofaPhDas
the end draws near, and to wonder where on earth one is to begin with
acknowledgements.TherearemanypeopleIhavebeenprivilegedtohavebymyside
throughoutthisentireprocess,andmanymorewhohavecontributedatstepsalong
theway.Iwillinnowaydojusticetotheprocessofthankingallofthemintheseshort
words;pleasejustknowthatmygratitudeisdeepandlong-lasting.
Firstly, to thewomenofKalafongandZithulelehospitals inSouthAfrica - this thesis
wouldneverhavecome to fruitionwithoutyou.Youareall strength inmotherhood
embodiedandtheimpressionyouleftisdeep.Tothemidwives,doctorsandresearch
staffatKalafong,thankyouforyourdedicationtothisprojectfromtheverybeginning,
andformakingmeawelcomepartofyourfamily.
ProfessorRobertPattinsonandDrJennyMakin,myloveforyoubothisgreat.In2014I
packedupmythingsandarrivedaloneinSouthAfrica,completelyunsureofwhatwas
tocome.Thatyearturnedouttobelifechanging,andlaunchedmanyofthepathsthat
I now find my career winds along. You are two extraordinary people whose
commitmenttoglobalhealthandrespectofandadvocacyforwomen issomething I
aspiretoeveryday.

xxi
I am very grateful to Dr Özge Tunçalp, who took on the role of supervisor when I
headeduptoSwitzerlandin2015.Thankyouforguidingandsupportingmethrough
the second year ofmy PhD, spendingmany hours reading papers, advisingme, and
becoming one of my fondest friends. To Metin Gulmezoglu, thank you for the
opportunity to join your group, for teaching me much about the world of global
maternalhealth,andshowingmethetruevalueofcreatingateamintheworkplace.
I am so lucky to have had extraordinary researcher Professor John Newnham as a
constant inmyentiremedical andPhD life as a supervisor,mentor, andgeneral life
guide. Many of my fondest memories of the PhD process are sitting in your office
debatingthemeaningoflife,thevalueofoverseasfellowshipsandthelessonslearnt
fromPhDs. Thank you for givingme the finalpush I needed to geton thatplane to
South Africa - for that I will be forever grateful. To Talal, Chris, Kate, Mari, and
Elizabethwhoallco-authoredpaperswithmethroughthisprocess;thankyouforyour
hardwork,adviceandsupport.AlsotothethirdmemberofmyPhDadvisoryboard,
ProfessorYeeLeung– thankyou for themanyyearsofmentorship,and forenticing
meovertothedarksideofsub-specialtytraining.
To Professor JanDickinson,what can I say? There is noway inwhichwords cando
justicetohowyouhaveshapedmylife.Isuspectitisveryraretofindsomeonewhois
truly amentor in theway youare.Anextraordinary clinician and researcher, I have
beenveryprivilegedtohaveyouasasupervisor.Youhavehadmybackeverystepof

xxii
my careerandhaveguidedme through thisPhDwithmorewisdom than I canever
hope tohave.Thankyou forbeingamentor, colleagueandwonderful friend tome,
andIwouldbethrilledifinmycareer,Icanbeafractionofthewomanyouare.
TomyfamilywhomIlovedearly-Joel,Tess,Dylan,WilliamandAlexandra,thankyou
forallofyoursupport,andsorryfortheimportanteventsImissedbeingaway.ToGina
andAndrew,mywonderfulparents;youcreatedaworldwhereIbelievedIcoulddo
anything and knew that youwould always be bymy side. Your support ofmy long-
windedcareerpathhasbeenunwavering.IthankyouandIloveyou.
TomybeautifulhusbandBen.Youareanextraordinaryman,andIamsoluckytobe
yourwife.Ithasbeenajoytonavigatelifewithyouthelast14years,andmygoodness
I am looking forward to the next many years of adventures. Thank you for the
immeasurable support youhavegivenmeduring thisPhD. I loveyou. Finally, tomy
son, Theodore. You have bought me nothing but happiness since the day you so
casually arrived in to this world. May you continue to be the life loving, sweet,
inquisitive littleman that youarenow forevermore. Iwill always loveyouand Iwill
alwayshaveyourback.

xxiii
PRESENTATIONSANDARTICLESARISINGFROMTHISTHESIS
PRESENTATIONS
South African Society of Obstetricians and Gynaecologists National Congress. May
19th, 2014. Cape Town, South Africa. “The role of audit in changing perinatal
mortality”
South African Society of Obstetricians and Gynaecologists Mini Symposium. August
23rd,2014.Pretoria,SouthAfrica.“Perinatalmortality:currentandfuturefocus.”
Priorities in Perinatal Care. March 17th, 2015. Drakensberg, South Africa. “Causes
ofperinatalmortality and associated maternal complications in a South African
province:Challengesinpredictingpooroutcomes”
Women and Infants Research Foundation Rising Stars Event. September 15th, 2016.
Perth,Western Australia. “Introducing umbilical artery lactate sampling as a tool to
improveintrapartumcareinamiddleincomecountrysetting”

xxiv
RoyalAustralianandNewZealandCollegeofObstetriciansandGynaecologistsAnnual
ScientificMeeting.October17th,2016.Perth,WesternAustralia.“FromAlpstoZebras
andEverythinginBetween”
ARTICLES
Allanson ER, Muller M, Pattinson RC. Causes of perinatal mortality and associated
maternal complications in a South African province: challenges in predicting poor
outcomes.BMCPregnancyChildbirth.2015;15:37.
Allanson ER, Pattinson RC. Quality-of-care audits and perinatal mortality in South
Africa.BullWorldHealthOrgan.2015;93(6):424-428.
Allanson ER, Waqar T, White CR, Tunçalp Ö, Dickinson JE. Umbilical lactate as a
measure of acidosis and predictor of neonatal risk: a systematic review. BJOG.
2017;124(4):584-594.
Allanson ER, Pattinson RC, Nathan EA, Dickinson JE. The benefit of introducing
umbilicalarterylactatesamplingintoalowresourcesettinglabourward:abeforeand
aftertrialinSouthAfrica.(UnderconsiderationbyBMCPregnancyChildbirth,2019)

xxv
Allanson ER, Grobicki K, Pattinson RC, Dickinson JE. Attitudes towards the
implementationofuniversalumbilicalarterylactateanalysisinaSouthAfricandistrict
hospital.BMCPregnancyChildbirth.2016;16(1):166.
AllansonER,PattinsonRC,NathanEA,DickinsonJE.Theintroductionofumbilicalcord
lactate measurement and associated neonatal outcomes in a South African tertiary
hospitallaborward.JMaternFetalNeonatalMed.2018;31(10):1272-1278.
Allanson ER, Pattinson RC, Nathan EA, Dickinson JE. Impact of maternal HIV on
umbilical cord lactatemeasurement at delivery in a South African labor ward. Int J
GynaecolObstet.2018;141(3):366-70.
BerghAM,AllansonE, PattinsonRC.What is needed for taking emergencyobstetric
and neonatal programmes to scale? Best Pract Res Clin Obstet Gynaecol.
2015;29(8):1017-1027.
Allanson ER, Tunçalp Ö, Vogel JP, Khan DN, Oladapo OT, Long Q, Gülmezoglu AM.
Implementationofeffectivepracticesinhealthfacilities:asystematicreviewofcluster
randomisedtrials.BMJGlobHealth.2017;2(2):e000266.

xxvi
AllansonE,TunçalpÖ,GardosiJ,PattinsonRC,ErwichJJ,FlenadyVJ,FrøenJF,Neilson
J,ChouD,MathaiM,SayL,GülmezogluM.Classifyingthecausesofperinataldeath.
BullWorldHealthOrgan.2016;94(2):79-79A.
AllansonER,TuncalpÖ,GardosiJ,PattinsonRC,VogelJP,ErwichJ,FlenadyVJ,Froen
JF,NeilsonJ,QuachA,FrancisA,ChouD,MathaiM,SayL,GülmezogluAM.Givinga
voice to millions: developing the WHO application of ICD-10 to deaths during the
perinatalperiod:ICD-PM.BJOG.2016;123(12):1986-1899.
AllansonER,TunçalpÖ,GardosiJ,PattinsonRC,FrancisA,VogelJP,ErwichJJ,Flenady
VJ,FrøenJF,NeilsonJ,QuachA,ChouD,MathaiM,SayL,GülmezogluAM.TheWHO
applicationofICD-10todeathsduringtheperinatalperiod(ICD-PM):resultsfrompilot
databasetestinginSouthAfricaandUnitedKingdom.BJOG.2016;123(12):2019-2028.
AllansonER,VogelJP,TunçalpӦ,GardosiJ,PattinsonRC,FrancisA,ErwichJJ,Flenady
VJ, Frøen JF,Neilson J,QuachA. Application of ICD-PM to preterm-relatedneonatal
deathsinSouthAfricaandUnitedKingdom.BJOG.2016;123(12):2029-2036.

xxvii
AllansonER,TunçalpӦ,GardosiJ,PattinsonRC,FrancisA,VogelJP,ErwichJJ,Flenady
VJ,FrøenJF,NeilsonJ,QuachA.OptimisingtheInternationalClassificationofDiseases
to identify the maternal condition in the case of perinatal death. BJOG.
2016;123(12):2037-2046.
LeisherSH,TeohZ,ReinebrantH,AllansonE,BlencoweH,ErwichJJ,FrøenJF,Gardosi
J,GordijnS,GülmezogluAM,HeazellAE,KortewegF,LawnJ,McClureEM,PattinsonR,
SmithGC,TunçalpÖ,WojcieszekAM,FlenadyV.Classification systems for causesof
stillbirth and neonatal death, 2009–2014: an assessment of alignment with
characteristicsforaneffectiveglobalsystem.BMCPregnancyChildbirth.2016;16:269.
LeisherSH,TeohZ,ReinebrantH,AllansonE,BlencoweH,ErwichJJ,FrøenJF,Gardosi
J,GordijnS,GülmezogluAM,HeazellAE,KortewegF,LawnJ,McClureEM,PattinsonR,
Smith GC, Tunçalp Ö, Wojcieszek AM, Flenady V. Seeking order amidst chaos: a
systematicreviewofclassificationsystemsforcausesofstillbirthandneonataldeath,
2009–2014.BMCPregnancyChildbirth.2016;16(1):295.
FrøenJF,FribergIK,LawnJE,BhuttaZA,PattinsonRC,AllansonER,FlenadyV,McClure
EM,FrancoL,GoldenbergRL,KinneyMV,LeisherSH,PittC,IslamM,KheraA,Dhaliwal
L, AggarwalN, PainaN, TemmermanM, Lancet Ending Preventable Stillbirths Series
study group. Stillbirths: progress and unfinished business. Lancet.
2016;387(10018):574-586.

xxviii
WojcieszekAM,ReinebrantHE, LeisherSH,AllansonE,CooryM,Erwich JJ, Frøen JF,
GardosiJ,GordijnS,GulmezogluM,HeazellAE,KortewegFJ,McClureE,PattinsonR,
Silver RM, Smith GC, Teoh Z, Tunçalp Ö, Flenady V. Characteristics of a global
classification system for perinatal deaths: aDelphi consensus study.BMCPregnancy
Childbirth.2016;16(1):223.

xxix
CONTENTS
Dedication.............................................................................................................................ii
InMemoriam........................................................................................................................iii
Abstract................................................................................................................................iv
Scholarshipacknowledgements............................................................................................ix
Declaration............................................................................................................................x
Authorshipdeclaration:Co-authoredpublications...............................................................xii
Acknowledgements.............................................................................................................xx
Presentationsandarticlesarisingfromthisthesis.............................................................xxiii
Presentations...............................................................................................................xxiii
Articles.........................................................................................................................xxiv
Abbreviations........................................................................................................................1
Tableoffigures......................................................................................................................6
Tableoftables.......................................................................................................................9
Tableofimages....................................................................................................................13
CHAPTERONE:THESISAIMANDOUTLINE............................................................................15
Thesisaim........................................................................................................................16
Thesisoutline..................................................................................................................19
References.......................................................................................................................27
CHAPTERTWO:LITERATUREREVIEW...................................................................................29
Chapteroutline................................................................................................................30
Introduction....................................................................................................................31
Definitionsofperinatalmortality.....................................................................................32
Perinatalmortalityinmiddleincomesettings..................................................................36
Perinatalmortalityinthemiddle-incomecountryliterature:areview.............................39
Perinatalmortalityinroutineobstetriccare....................................................................40
Facilitybaseddeliveryandperinatalmortalityinmiddle-incomecountries.....................42

xxx
Qualityofcare................................................................................................................44
Caesareansectioninmiddleincomecountries................................................................46
PerinatalmortalityinSouthAfrica..................................................................................48
CausesofperinatalmortalityinSouthafrica...................................................................49
PerinatalmortalityinSouthAfrica:areview...................................................................53
Theglobalclassificationofperinatalmortality.................................................................54
Fetalphysiologyandtheimpactofhypoxia.....................................................................58
Acidbasebalanceinthefetus.........................................................................................58
Intrapartumhypoxia.......................................................................................................59
Thefetalresponsetohypoxia.........................................................................................60
Thepretermfetalresponsetohypoxiaandasphyxia......................................................64
Lactateasameasurementofmetabolicacidosis..............................................................65
Theclinicalconsequencesofhypoxiaandacidaemia.......................................................66
Theconceptofasphyxia..................................................................................................66
Causesofacutehypoxiaandasphyxiaintheintrapartumperiod....................................67
Optionsformeasuringhypoxiaanditssequelae..............................................................70
pH...................................................................................................................................70
Baseexcess(BE)..............................................................................................................71
Apgarscore.....................................................................................................................71
Lactate............................................................................................................................72
Measuringumbilicallactate.............................................................................................73
Timingoflactatesampling..............................................................................................74
Methodofsampling........................................................................................................76
Cordarteriallactatelevels..............................................................................................78
Fetalheartratemonitoring..............................................................................................80
TheCTGandacidosis:areview.......................................................................................85
Theneonatewithacidosis...............................................................................................93

xxxi
Neonatalacidosisandadverseoutcomes........................................................................94
Thewellnewbornwithacidosis......................................................................................95
Qualityofcareaudits.......................................................................................................97
Definingqualityofcareandqualityofcareaudit............................................................97
Qualityofcareauditinmaternalandnewbornhealth....................................................99
Qualityofcareauditandnearmisscases......................................................................102
MaternalHIVInfection..................................................................................................103
Conclusion.....................................................................................................................104
References.....................................................................................................................105
CHAPTER THREE: THESIS OUTLINE AND METHODOLOGY OF THE RESEARCH…………………………………….....................................................................................................134
Thesisoutline................................................................................................................135
Outlineoftheresearchinchapterfour..........................................................................137
Aim................................................................................................................................137
Methodology.................................................................................................................138
Inclusioncriteria............................................................................................................138
Dataextracted...............................................................................................................138
Ethics.............................................................................................................................139
Outlineoftheresearchinchapterfive...........................................................................140
Objectivesofthereview................................................................................................140
Criteriaforconsideringstudiesinthereview.................................................................140
Generalinclusion/exclusioncriteria.............................................................................140
Typesofstudydesignsfordiagnostictestaccuracy........................................................141
Typesofparticipants.....................................................................................................141
Typesofoutcomes.........................................................................................................141
Searchstrategyforidentificationofstudies...................................................................142
Customisedsearchstrategy...........................................................................................143
Methodsofthereview..................................................................................................158

xxxii
Analysisplan..................................................................................................................164
Outlineoftheresearchinchaptersix.............................................................................166
Aim................................................................................................................................166
Methodology.................................................................................................................166
Ethics.............................................................................................................................167
Analysis.........................................................................................................................167
Outlineoftheresearchinchaptersseven,eightandnine..............................................168
Background...................................................................................................................168
Studyobjective.............................................................................................................168
Primary aims................................................................................................................169
Secondary aims............................................................................................................170
Methodology................................................................................................................170
Phase1..........................................................................................................................171
Studydesignandstudysetting......................................................................................171
Studypopulation..........................................................................................................171
Studyproceduresanddatacollected............................................................................172
Datacollected...............................................................................................................173
Samplesizecalculation.................................................................................................175
Phase two.....................................................................................................................176
Studydesignandstudysetting......................................................................................176
Studypopulation..........................................................................................................176
Studyproceduresanddatacollected............................................................................177
Teachingintervention...................................................................................................177
Datacollected...............................................................................................................180
Ethics............................................................................................................................181
Outlineoftheresearchinchapterten...........................................................................182
Background...................................................................................................................182

xxxiii
Studyobjective.............................................................................................................183
Primaryaims.................................................................................................................183
Methodology................................................................................................................183
Studydesignandstudysetting......................................................................................184
Informedconsent..........................................................................................................184
Pre-intervention...........................................................................................................184
Intervention..................................................................................................................185
Postintervention..........................................................................................................186
CHAPTER FOUR: CAUSES OF PERINATAL MORTALITY AND ASSOCIATED MATERNALCOMPLICATIONS IN A SOUTH AFRICAN PROVINCE: CHALLENGES IN PREDICTING POOROUTCOMES........................................................................................................................187
Chapteroverview..........................................................................................................188
Abstract........................................................................................................................189
Background...................................................................................................................189
Methods.......................................................................................................................190
Results..........................................................................................................................191
Discussion.....................................................................................................................191
Conclusion....................................................................................................................194
References....................................................................................................................195
CHAPTER FIVE: UMBILICAL LACTATE AS A MEASURE OF ACIDOSIS AND PREDICTOR OFNEONATALRISK:ASYSTEMATICREVIEW...........................................................................196
Chapteroverview..........................................................................................................197
Abstract........................................................................................................................198
Introduction..................................................................................................................198
Methods.......................................................................................................................199
Results..........................................................................................................................200
Discussion.....................................................................................................................203
Conclusion....................................................................................................................205
References....................................................................................................................206

xxxiv
Referencesforchapterintroduction..............................................................................209
CHAPTERSIX:QUALITYOFCAREAUDITSANDPERINATALMORTALITYINSOUTHAFRICA..211
Chapteroverview..........................................................................................................212
Abstract........................................................................................................................213
Introduction..................................................................................................................213
Approach......................................................................................................................213
Relevantchanges..........................................................................................................214
Lessonslearnt...............................................................................................................215
References....................................................................................................................217
CHAPTER SEVEN: THE INTRODUCTIONOFUMBILICAL CORD LACTATEMEASUREMENTANDASSOCIATED NEONATAL OUTCOMES IN A SOUTH AFRICAN TERTIARY HOSPITAL LABOURWARD................................................................................................................................218
Chapteroverview..........................................................................................................219
Abstract........................................................................................................................220
Introduction..................................................................................................................220
Materialsandmethods.................................................................................................221
Results..........................................................................................................................221
Discussion.....................................................................................................................224
Conclusion....................................................................................................................225
References....................................................................................................................225
CHAPTER EIGHT: PREVENTING THE FIRST CAESAREAN: A BEFORE AND AFTER TRIALDEMONSTRATINGTHEBENEFITOFINTRODUCINGUMBILICALARTERYLACTATESAMPLINGINTOALOWRESOURCESETTINGLABOURWARD..................................................................227
Chapteroverview..........................................................................................................228
Referenceforchapterintroduction................................................................................231
Abstract.........................................................................................................................235
Introduction..................................................................................................................238
Materialsandmethods..................................................................................................239
Statisticsandanalysis....................................................................................................241

xxxv
Ethics.............................................................................................................................243
Results...........................................................................................................................244
Maternalcharacteristics................................................................................................244
Pregnancyandlabour...................................................................................................245
Lactateresults...............................................................................................................247
Birthcharacteristics......................................................................................................247
Neonatalcharacteristics................................................................................................248
Modeofdeliveryandneonataloutcomesforalldeliveries...........................................251
Discussion......................................................................................................................251
Conclusion.....................................................................................................................256
References.....................................................................................................................260
CHAPTERNINE: IMPACTOFMATERNALHIVONUMBILICALCORDLACTATEMEASUREMENTATDELIVERYINASOUTHAFRICANLABOURWARD...........................................................263
Chapteroverview..........................................................................................................264
Abstract........................................................................................................................265
Introduction..................................................................................................................265
Materialsandmethods.................................................................................................266
Results..........................................................................................................................266
Discussion.....................................................................................................................267
References....................................................................................................................269
CHAPTER TEN: ATTITUDES TOWARDS THE IMPLEMENTATION OF UNIVERSAL UMBILICALARTERYLACTATEANALYSISINASOUTHAFRICANDISTRICTHOSPITAL...............................270
Chapteroverview..........................................................................................................271
Abstract........................................................................................................................272
Background...................................................................................................................272
Methods.......................................................................................................................273
Results..........................................................................................................................273
Discussion.....................................................................................................................275

xxxvi
Conclusion....................................................................................................................276
References....................................................................................................................277
CHAPTERELEVEN:DISCUSSION..........................................................................................278
Overview.......................................................................................................................279
Applicabilityoftheresearch..........................................................................................281
Themanagementofintrapartumasphyxia....................................................................281
TheuseandbenefitsofUAlactatesampling.................................................................282
Translatingresearchintoclinicalpractice......................................................................285
TheimplementationofQOCaudit.................................................................................286
Strengthsoftheresearch...............................................................................................288
Limitationsoftheresearch............................................................................................289
Futuredirectionsforresearch........................................................................................291
Conclusion.....................................................................................................................291
References.....................................................................................................................292
APPENDICES.......................................................................................................................295
AppendicesforChapter2...............................................................................................296
Appendix2.1:PapersbythethesisauthoronthedevelopmentoftheICD-PM.............296
AppendicesforChapter3...............................................................................................329
Appendix 3.1: Patient information and consent form for the “introduction of universalcordlactatesamplingandcorrelationwithneonataloutcomes”...................................330
Appendix3.2:Datacollectionsheet..............................................................................334
Appendix3.3:PretrainingCTGtestfordoctors(questions)...........................................336
Appendix3.4:PretrainingCTGtestfordoctors(answers).............................................350
Appendix3.5:PosttrainingCTGtestfordoctors...........................................................351
Appendix3.6:PosttrainingCTGtestfordoctors(answers)...........................................371
Appendix3.7:PretrainingCTGtestformidwives(questions).......................................373
Appendix3.8:PretrainingCTGtestformidwives(answers)..........................................380
Appendix3.9:PosttrainingCTGtestformidwives........................................................381

xxxvii
Appendix3.10:PosttrainingCTGtestformidwives(answers)......................................391
AppendicesforChapter5...............................................................................................392
Appendix5.1:Searchstrategy.......................................................................................393
Appendix5.2:Datafromeachincludedstudy,includingthethresholdsforeachoutcome.....................................................................................................................................394
Appendix5.3Characteristicsofincludedstudies(n=12)................................................398
AppendicesforChapter10.............................................................................................403
Appendix10.1Questionnaire:attitudesandbarrierstowardsimplementationofuniversalcordlactatesampling....................................................................................................404
Appendix10.2Patient/participant’sinformationleaflet&informedconsentform.....410

1
ABBREVIATIONS
ABE actualbaseexcess
aOR adjustedoddsratio
ACTH adrenocorticotropichormone
AFA advancedfetalassessment
ANS autonomicnervoussystem
APH antepartumhaemorrhage
ART anti-retroviraltherapy
ATP adenosinetriphosphate
AUC areaunderthecurve
AVD assistedvaginaldelivery
AVP argininevasopressin
BG bloodgas
BE baseexcess
BPM beatsperminute
CI confidenceintervals
CO2 carbondioxide

2
CRH corticotropin-releasinghormone
CS caesareansection
CTG cardiotocograph
CV coefficientofvariation
DHIS DistrictHealthInformationSystem
ENND earlyneonataldeath
ESMOE EssentialStepsintheManagementofObstetricEmergencies
FDIU fetaldeathinutero
FIGO InternationalFederationofGynecologyandObstetrics
FSB freshstillbirth
GR grams
HAART highlyactiveanti-retroviraltherapy
HIE hypoxicischaemicencephalopathy
HIV humanimmunodeficiencyvirus
HMD hyalinemembranedisease
HPA hypothalamic-pituitary-adrenal
HR heartrate

3
ICD-10 International Statistical Classification of Diseases and Related Health
Problems10thRevision
ICD-PM The WHO application of ICD-10 to perinatal deaths: ICD-perinatal
mortality
IQ interquartilerange
IUGR intrauterinegrowthrestriction
KEMH KingEdwardMemorialHospital
LBW lowbirthweight
LFD latefetaldeath
LMIC lowandmiddle-incomecountries
LND lateneonataldeath
MAP meanarterialpressure
MAS meconiumaspirationsyndrome
MeSH medicalsubjectheadings
MDG millenniumdevelopmentgoals
MIC middle-incomecountries
MMR maternalmortalityrate
MSB maceratedstillbirth

4
NEC necrotisingenterocolitis
NND neonataldeath
NNJ neonataljaundice
OR oddsratio
PCI perinatalcareindicators
PMTCT preventionofmothertochildtransmission
PNMR perinatalmortalityrate
POC pointofcare
PPIP PerinatalProblemsIdentificationprogram
PT provincialtertiaryhospital
QoC qualityofcare
QUADAS2 Qualityassessmentofdiagnostictestaccuracystudies2
RCT randomisedcontrolledtrial
RDS respiratorydistresssyndrome
ROC receiveroperatorcurve
SBE standardbaseexcess
SD standarddeviation
SDG sustainabledevelopmentgoals

5
TTN transienttachypnoeaofthenewborn
UA umbilicalartery
UV umbilicalvein
VBAC vaginalbirthaftercaesarean
WHO WorldHealthOrganization
WHOMCS WorldHealthOrganizationmulti-countrysurvey

6
TABLEOFFIGURES
Chapter2
Figure2.1 Thecalculationofperinatalmortality
Figure2.2: Distribution of perinatalmortality across three time periods in
SouthAfrica
Figure2.3 Aerobicandanaerobicmetabolism.
Figure2.4 Anexampleof thecolorimetric reactionusedbytheAccutrend
monitor
Figure2.5 CTG with the normal fetal baseline HR lying within the 110-
160bpmareadefinedbythegreyline
Figure2.6: CTGsshowingdecreased,normalandincreasedvariability
Figure2.7: CTGshowingaccelerationsabovethebaseline
Figure2.8: CTGshowingearlydecelerations
Figure2.9: CTGshowinglatedecelerations
Figure2.10: CTGshowingvariabledecelerations
Figure2.11: CTGshowingprolongeddecelerations

7
Chapter5
Figure1: PRISMAflowchart
Figure2: Forestplotofumbilicalarteriallactatesensitivityandspecificity
foracidosisdefinedbypH<7.2
Figure3: Forestplotofumbilicalarteriallactatesensitivityandspecificity
foracidosisdefinedbyBE(>8)
Figure4: Forestplotofumbilicalarteriallactatesensitivityandspecificity
forneonatalpoorneurologicaloutcomeincludingHIE
Figure5: Plotof fittedmodel formeta-analysis sensitivity and specificity
ofumbilicallactateforpoorneurologicaloutcomeincludingHIE
Figure6: Risk of bias and applicability concerns graph: review authors’
judgementsabouteachdomainpresentedaspercentagesacross
includedstudies
Figure7: Riskofbiasandapplicabilityconcernssummary:reviewauthors’
judgementabouteachdomainforeachincludedstudy

8
Chapter6
Figure1: Trendsinperinatalmortalityforthefirstfiveyearsofquality-of-
careauditsinhealth-carefacilities,SouthAfrica
Chapter7
Figure1: Receiver operating characteristics curves for UA lactate for
neonatal resuscitation in all babies (black solid line), preterm
babies (light grey solid line), and term babies (dark grey solid
line).Thedashedlineindicatesthediagonalreferenceline
Figure2: Receiver operating characteristics curves for UA lactate for
neonataladmissiontothenurseryinallbabies(blacksolidline),
pretermbabies(lightgreysolidline),andtermbabies(darkgrey
solidline).Thedashedlineindicatesthediagonalreferenceline
Figure3: ReceiveroperatingcharacteristicscurvesforApgarscore<7at5
minutesinallbabies(blacksolidline),pretermbabies(lightgrey
solidline),andtermbabies(darkgreysolidline).Thedashedline
indicatesthediagonalreferenceline

9
TABLEOFTABLES
Chapter2
Table2.1 Perinatalmortalityratesinmiddleincomecountries
Table2.2 PerinatalcareindicatorsatKalafongHospital,2013
Table2.3 Causes and frequency of clinical events that result in
intrapartumhypoxiaandasphyxiainLMIC
Table2.4: Cut-offvaluesforcohortsassessingacidosisusinglactatelevels
Table2.5: ComponentsoftheCTG.
Chapter4
Table1: Fetal/neonatal and maternal characteristics of macerated and
freshstillbirthsandearlyneonataldeaths
Table2: Comparisonofmaternalconditioninthelatestillbirthandearly
neonataldeaths
Table3: Obstetric causes of death in late stillbirth and early neonatal
death

10
Table4: Causesofneonataldeath
Chapter5
Table1: Meta-analysisofcorrelationcoefficientsof lactatecomparedto
threeothermeasuresofacidosis(pH,SBEandApgarscoreat5
minutes)
Chapter6
Table1: Obstetric causes of death in quality-of-care audits for health-
carefacilitieswithincreasinganddecreasingperinatalmortality,
SouthAfrica
Chapter7
Table1: Maternalandpregnancycharacteristics

11
Chapter8
Table8.1: Preandposttestscoresfordoctors
Table8.2: Preandposttestscoresformidwives
Table1: Maternalcharacteristicsinpre-andpost-interventiongroups
Table2: Intrapartumcomplicationsinpre-andpost-interventiongroups
Table3: Neonatalcharacteristicspre-andpost-interventiongroups
Table4: Neonatal outcomes stratified by birth weight <2500gr and ≥
2500gr
Chapter9
Table1: Maternalcharacteristics
Table2: Deliverycharacteristics

12
Chapter10
Table1: Characteristicsofrespondents
Table2: Perceived barriers to introduction of universal umbilical artery
lactateanalysispreandposttraining
Table3: Identification of barriers to implementing universal umbilical
artery lactate analysis pre and post training (the influence of
clinicalrole)
Chapter11
Table11.1 PerinatalcareindicatorsforKalafongHospital,2014

13
TABLEOFIMAGES
Chapter1
Image1.1 WomenintheantenatalwardatKalafonghospital
Image1.2 AnelephantatKrugerNationalPark,Mpumalanga
Image1.3 BedsoutforwashingatKalafongHospital
Image1.4 IntrapartumCTGatKalafongHospital
Image1.5 CTGpriortointrapartumdeathatKalafongHospital
Chapter2
Image2.1: Saving Babies. The most recent report from the Perinatal
ProblemsIdentificationProgram
Image2.2a
and2.2b: AccutrendPlusTM©hand-heldlactatemeter
Image2.3: Asegmentofumbilicalcordwiththelargerveinclearlyvisible
Image2.4: Acrosssectionofumbilicalcordshowing2arteriesand1vein
Image2.5: A1mlnon-heparinisedsyringeand26-gaugeneedle

14
Chapter3
Image3.1: KalafongHospitalbynight,2014
Image3.2: AKalafonghospitalobstetricsregistrartestingaUAsample
Chapter11
Image11.1 CrowdedantenatalwardatKalafongHospital
Image11.2 The primary author of this thesis and SisterMaria, Matron of
KalafongHospitallabourward

15
CHAPTERONE:THESISAIMANDOUTLINE

16
THESISAIM
Millionsofwomenandtheirbabiesdieeveryyeararoundthetimeofchildbirthand
improving this statistic remains a priority of the Sustainable Development Goals
(SDGs)(1). Thus, the basis of this dissertation centres on the concept of perinatal
mortalityinlowandmiddle-incomecountries(LMIC)andparticularlythecontribution
of intrapartum care to this. Lack of quality of intrapartum care around the time of
childbirth leads to adverse outcomes, frequently as a result of hypoxia and its
sequelae, which in LMIC is a significant contributor to both stillbirths and early
neonatal deaths(2). Intrapartum hypoxaemia can be considered the intermittent or
permanent fall in fetal blood oxygen levels during labour, which may lead to
intrapartum hypoxia, or a fall in oxygen levels in organs(3). With the influence of
maternal,fetal,andcarefactors,thiscanleadtoacidosis(increaseofhydrogenionsin
thetissues(4)),andfinallytointrapartumasphyxia,aconglomerateofclinicalfeatures
includinganeurologicallydepressedneonateatbirth,aswellas intrapartumorearly
neonataldeath(5).
Themiddle-incomecountryofSouthAfricahasaperinatalmortalityrate(PNMR)of33
per 1000 births, with only small improvement in this statistic in since 2000(6).
Intrapartum asphyxia causes at least 10% of all stillbirths in South Africa(7) and
additionally,at leastaquarterofearlyneonataldeathsareattributedtointrapartum
asphyxia(8),withanuntoldnumberofsurvivorssufferinglongtermdisability(9).

17
ReducingthePNMRinLMICrequiresinterventionsthatmeetthecontextualneedsof
the relevant populations. That is, any intervention needs to be easily applied,
inexpensive, easily taught and sustainable. Reducing intrapartum hypoxia requires
accurate recognition of the condition, followed by an appropriate clinical response.
Interventions toachieve this includeelectronic fetalheart ratemonitoring,access to
instrumental deliveries and caesarean section facilities, and effective neonatal
resuscitation, in addition to adequate staffing with access to teaching and case
reflection(9-11).
WhileelectronicfetalheartratemonitoringisfrequentlyusedinSouthAfricawiththe
aim of detecting fetal hypoxia and compromise(12), there are several limitations to
CTGusethatmaylimititsimpactonintrapartumoutcomes.Dependingonthesystem
usedforinterpretation,specificityforCTGandfetalacidosiscanbeaslowas18%,with
positivepredictivevaluesaround35%(13).However,thesensitivityofelectronicfetal
heartratemonitoringmaybeimprovedwithumbilicalcordbloodsamplingtoassess
acid-basebalanceimmediatelyafterdelivery.Umbilicalcordsamplingsupplementsthe
clinical picture provided by fetal heart rate patterns, as it objectively reflects fetal
tissue hypoxia and acidosis, which have morbid and mortal sequelae(14). Sampling
allows immediate case reflection with positive or negative reinforcement of
management decisions for eachdelivery to occur(15).Although this clearly does not
change the intrapartum management for the sampled case, doing so has several
potentialbenefits.Firstly,inthecaseofanormalresult, intrapartumasphyxiacanbe

18
excludedandhealthcareprovidersreassuredabouttheirclinicaldecisionmaking(14).
In the case of an abnormal result, staff can both reflect on intrapartum care and
potentiallytakestepstochangemanagementstrategies inthefuture(15). Itwasthis
latterconceptthatformedthebasisofthisthesis.
UAbloodgasmeasurementallowsanobjectiveassessmentofthemetabolicstateof
thefetuspriortodeliveryandprovidesabiochemicalrepresentationoffetalacid-base
statusintheintrapartumperiod.Itisconventionallyperformedusingameasurement
ofpH(14).WhilstUApHisthegoldstandardformeasurementoffetalhypoxiathathas
resulted inacidosis, thecostandmaintenanceof therequiredequipment (bloodgas
analyser)renderthisnotfeasibleforresourcepoorsettings,includingmostfacilitiesin
South Africa. An alternate way to measure acidosis is with UA cord blood lactate;
whichcanbereadilytestedonahandhelddeviceandcorrelateswellwithpHvaluesin
theassessmentoffetalhypoxia(16).Thus,theaimofthisresearchwastointroduceUA
lactatesamplinginaresourcelimitedsetting,asaqualityofcarefeedbacktool,which
it was hypothesised, would alter clinicians’ behaviours and improve maternal and
neonatal outcomes over time. This research was performed at Kalafong Hospital,
Pretoria,SouthAfrica(Image1.1),withapproximately6500deliveriesperyearina16
bedlabourward,usuallystaffedwith3midwivesand3doctorsatanyonetime.

19
THESISOUTLINE
In this thesis I have explored the causes of perinatal mortality in South Africa,
undertakena systematic reviewandmeta-analysisof thediagnostic test accuracyof
lactate,completedacomprehensiveanalysisoftheimpactofqualityofcareauditon
perinatal mortality, implemented UA lactate testing to ascertain its capacity in this
setting topredict short-termneonataloutcomes,assessed the impactof introducing
UA lactate sampling, investigated the role maternal HIV infection may play in the
resultsofthetest,aswellasitsfeasibilityoutsideofaresearchsetting.Chaptertwo
reviews the literature to provide anunderstandingof perinatalmortality in lowand
middleincomesettings(andinSouthAfricaspecifically),normalfetalphysiology,fetal
lactate,qualityofcareaudit,nearmisscases,andotherfactorsrelatedtointrapartum
care,includingmaternalHIVinfectionandcaesareansectionrates.

20
Image1.1WomenintheantenatalwardatKalafonghospital
Chapter four explores the causes of perinatal mortality and associated maternal
conditionsinSouthAfrica.ItusesdatafromMpumalanga,aprovinceineasternSouth
Africa bordering Swaziland and Mozambique (and well known for the presence of
KrugerPark),wheremorethan90%ofwomengivebirthinahealthcarefacilityandall
facilitiescaptureperinatalmortalityqualityofcareauditdatausingtheSouthAfrican
Perinatal Problems Identification Program (PPIP) database. A secondary analysis of
PPIP data for the Provincewas undertaken for the period October 2013 to January
2014, inclusive. Data for each individual late perinatal death were reviewed. The
frequencies of maternal and perinatal characteristics for late fetal deaths were

21
examined and the relationships between the maternal condition and perinatal
outcomesanalysed.
Image1.2AnelephantatKrugerNationalPark,Mpumalanga
Chapter five is a systematic review and diagnostic test accuracy of umbilical cord
lactatetomeasureacidosisandpredictneonataloutcome.Tosynthesisetheevidence
for the diagnostic test accuracy of umbilical cord lactate in measuring acidosis and
predictingpoorneonataloutcome,publishedandunpublishedstudiesbetween1990
and 2014 from PubMed/Medline, EMBASE, Cochrane Central Register of Controlled
Trials, and clinicaltrials.gov, extracting cross-sectional and randomised studies that
assessedfetalacidosis(usinglactateastheindextest)withorwithoutanassessment
of neonatal outcome, were reviewed. Correlations between index and reference
test(s) were recorded, as were the raw data, to classify the predictive ability of

22
umbilical lactateforneonataloutcomes.Meta-analysisofcorrelationwasperformed.
Estimatesofthestudies'observedsensitivitiesandspecificitieswereplottedonForest
plots with 95% confidence intervals (CI). Where possible, we combined data using
meta-analysis, applying the hierarchical summary receiver operating characteristics
modelandabivariatemodel.
Chaptersixexplores the impactsofqualityofcareauditonPNMR inSouthAfrica.A
review of several small studies showed a reduction in perinatal mortality after the
introductionofperinatal auditsbutno large scale researchexists(17). Therefore,we
analysedthechangesinPNMRin163facilitiesinSouthAfricawithatleastfiveyearsof
continuous quality of care audit.We tested for temporal trends in PNMR using the
extendedMantel-HaenszelM2statisticwithonedegreeoffreedom.
Chapters seven to nine originate from research undertaken at Kalafong Hospital in
2014.(Image1.3)ChapterseveninvestigatestheutilityofUAlactatemeasurementsat
Kalafong Hospital to assess intrapartum care and predict neonatal outcomes. From
March 3rd to 12th of November 2014, a prospective cohort study of UA lactatewas
conducted.Usingreceiveroperatorcurve (ROC)analysis,wedeterminedtheoptimal
lactatecut-offfordiscriminatingbetweentherequirementforneonatalresuscitation,
admissiontotheneonatalnurseryandApgarscorelessthansevenatfiveminutes.

23
Image1.3BedsoutforwashingatKalafongHospital
ChaptereightcentresontheconceptthattheintroductionofUAlactatesamplinginall
deliveries inotherunitsproducesprogressive improvements inneonatalbiochemical
markersand reducedadmission tohigh care facilitiesover time, independentof the
rate of obstetric intervention(15). Thus, from 3rdMarch - 12th November 2014, we
undertook a before and after trial to determine the impact of introducing UA cord
lactate sampling, using a hand-held lactatemeter, in conjunctionwith education on
CTGinterpretationandfetalandlactatephysiology.(Images1.4&1.5)Usinglinearand
logistic regression analysis, we determined the impact of introducing UA lactate
samplingonmaternalandneonataloutcomes.

24
\
Image1.4IntrapartumCTGatKalafongHospital
InChapternine,theUAlactatelevelsandperinataloutcomesamongwomenwithand
withoutHIV infectionwereassessed. InacohortofwomenwithUAlactatesamples,
maternalandneonataldatawerecollected, includingHIVstatusandCD4counts.UA
lactate levels and neonatal outcomes were compared between women with and
without HIV infection. The potential confounding impact of HIV treatment on
outcomeswasstudiedusingmaternalCD4counts.Univariatecomparisonsweremade
using independent t-tests for continuous outcomes and Chi-square or Fisher exact
testsforcategoricalcomparisons.

25
Image1.5CTGpriortointrapartumdeathatKalafongHospital
Itiscriticalthatinterventionscanbeimplementedbeyondaresearchsetting,andare
acceptable to clinicians and patients in daily clinical practice. Thus, Chapter ten
assesses the acceptability and barriers to implementing universal umbilical artery
lactate testing inadistricthospital in Zithulele,on theeastern capeof SouthAfrica.
During the period 16/11/2014 - 13/01/2015, we conducted a training course in
cardiotocograph(CTG)interpretation,fetalphysiology,andthesamplingandanalysing
of UA lactate, with a pre- and post-training questionnaire aimed at assessing the
barriers and facilitators to the introduction of universal UA lactate sampling. In
addition to descriptive statistics, the relationship between various attitudes and
barriersbeforeandafterthetrainingprogramwereanalysedusingFisher’sexacttest.
Theroleofgender,age,position,andlengthoftimepractisingontheidentificationof
individual barriers to the implementation of the intervention pre- and post-training
wereexploredusingordinalregressionmodels.

26
Chapterelevensummarisesthefindingsofthisthesis,thestrengthsandlimitationsof
theresearchandfuturedirectionsforimplementationandongoingresearch.

27
REFERENCES
1. Scott H, Danel I. Accountability for improvingmaternal and newborn health.BestPractResClinObstetGynaecol.2016;36:45-56.2. Lawn J, Shibuya K, Stein C. No cry at birth: global estimates of intrapartumstillbirths and intrapartum-related neonatal deaths. Bull World Health Organ.2005;83(6):409-17.3. Nordstrom L, Arulkumaran S. Intrapartum fetal hypoxia and biochemicalmarkers:areview.ObstetGynecolSurv.1998;53(10):645-57.4. Ayres-de-Campos D. Introduction: Why is intrapartum foetal monitoringnecessary - Impact on outcomes and interventions. Best Pract Res Clin ObstetGynaecol.2016;30:3-8.5. GrahamEM,RuisKA,HartmanAL,NorthingtonFJ,FoxHE.Asystematicreviewof the role of intrapartum hypoxia-ischemia in the causation of neonatalencephalopathy.AmJObstetGynecol.2008;199(6):587-95.6. Pattinson R. Saving Babies: A Perinatal Care Survey of South Africa 2000.Pretoria,SouthAfrica;2000.7. PattinsonR,Rhoda,N.Savingbabies2012-2013:NinthreportonperinatalcareinSouthAfrica.TshepesaPress,Pretoria,SouthAfrica;2014.8. LloydLG,DeWittT.NeonatalmortalityinSouthAfrica:Howarewedoingandcanwedobetter?SAMJ:SouthAfricanMedicalJournal.2013;103(8):518-9.9. Hofmeyr GJ, Haws RA, Bergström S, Lee AC, Okong P, Darmstadt GL, et al.Obstetriccareinlow‐resourcesettings:what,who,andhowtoovercomechallengesto scale up? International Journal of Gynecology & Obstetrics.2009;107(Supplement):S21-S45.10. BuchmannE, PattinsonR,NyathikaziN. Intrapartum-relatedbirth asphyxia inSouth Africa lessons From the first national perinatal care survey. S Afr Med J.2002;92(11):897-901.11. Wall SN, Lee AC, CarloW, Goldenberg R, Niermeyer S, Darmstadt GL, et al.,editors. Reducing intrapartum-related neonatal deaths in low-and middle-incomecountries—whatworks?SeminPerinatol;2010:Elsevier.12. van Bogaert LJ, Misra A. Neonatal outcome after caesarean birth for fetaldistressand/ormeconiumstaininginaSouthAfricanruralsetting.JObstetGynaecol.2008;28(1):56-9.13. Di Tommaso M, Seravalli V, Cordisco A, Consorti G, Mecacci F, Rizzello F.Comparisonoffiveclassificationsystemsforinterpretingelectronicfetalmonitoringinpredictingneonatalstatusatbirth.TheJournalofMaternal-Fetal&NeonatalMedicine.2013;26(5):487-90.14. Thorp JA, Rushing RS. Umbilical cord blood gas analysis.Obstet Gynecol ClinNorthAm.1999;26(4):695-709.15. White CR, Doherty DA, Henderson JJ, Kohan R, Newnham JP, Pennell CE.Benefitsof introducinguniversalumbilicalcordbloodgasandlactateanalysis intoanobstetricunit.AustNZJObstetGynaecol.2010;50(4):318-28.16. HamedHO.Intrapartumfetalasphyxia:studyofumbilicalcordbloodlactateinrelationtofetalheartratepatterns.ArchGynecolObstet.2013;287(6):1067-73.17. PattinsonR,KerberK,WaiswaP,DayLT,MussellF,AsiruddinS,etal.Perinatalmortality audit: counting, accountability, and overcoming challenges in scaling up in

28
low‐ and middle‐ income countries. International Journal of Gynecology &Obstetrics.2009;107(Supplement).

29
CHAPTERTWO:LITERATUREREVIEW

30
CHAPTEROUTLINE
Chaptertwoexplorestheexistingliteraturefortheconceptsthatformthebasisofthis
thesis. It commences with the definitions of perinatal mortality, an overview of
perinataloutcomesinmiddleincomecountries(MIC)andtheclassificationofperinatal
deathsinSouthAfrica.Thenormalphysiologyofthefetusandtheimpactofhypoxia
onthis,themeasurementofacidosisincludingwithlactate,theinterplaybetweenCTG
andacidosisisthendiscussed.Finally,qualityofcare(QoC)auditsarereviewed.

31
INTRODUCTION
Perinatal death is both a global public health concern and an individual tragedy for
millions ofwomen, their partners, and their families around theworld. The time of
childbirthposes thegreatest risk towomenandtheirbabies,andthere is significant
overlapintheaetiologyofthecausesofdeathofboth(1).AsdiscussedinChapterone,
hypoxiaduringthefirstandsecondstageoflabourplacesthefetusatriskofsignificant
morbidity andmortality(2). Intrapartum hypoxia contributes tomore than amillion
perinataldeathsgloballyeachyear(3)andthemajorityofthesedeathsoccurinLMIC,
where the lack of consistent availability of quality intrapartum care is a significant
contributing factor(4). Thus, quality of care (QoC) around the time of childbirth is
imperative to thesurvivalmothersandbabies(5).Moreover, issueswith intrapartum
carethatdonotresultinperinataldeath,havethepotentialtoresultinnearmissesor
perinatalmorbidity.
While it is clear that the causesof perinatalmortality aremultifactorial,QoC in low
resourcesettingsareasignificantcontributoryfactor.SouthAfrica,forexample,hasa
perinatalmortalityrate(PNMR)of33per1000births.Australia’sPNMRbycomparison
is6per1000.InSouthAfrica,5deathsper1000birthsareattributedtobirthasphyxia,
and more than a third of these asphyxia perinatal deaths are secondary to either
inadequate fetal heart rate monitoring or failure to recognise intrapartum fetal
compromise(6).

32
The ability to identify and manage intrapartum hypoxia is a significant clinical
challenge,particularlygiventhatmostcaseswillhavenoantepartumriskfactors,and
morethanathirdwillhavenoobviousintrapartumriskfactors(7).Intrapartumhypoxia
oftenmanifestsinlabourwithabnormalitiesinthefetalheartrate,howeverthefetal
cardiotocograph (CTG) has a limited positive predictive value of only 30% for the
outcomeofacidosis(8). There is great variability in theuseofobjectivemeasuresof
intrapartum compromise such as fetal scalp sampling and assessment of acidosis
during labour (using pH or lactate) internationally(8-10). While improving the
sensitivityoftheCTGwith intrapartumfetalscalpsamplinghasbeendescribedsince
the1960’s(withvariableresultsonitsabilitytoreduceintrapartumasphyxia)(10),its
use in LMIC is limited(11).Reasons for thisutilisation include the resources required
for fetal scalp sampling, and the contraindications to scalp sampling, including
maternalHIVinfectionandotherbloodborneviruses.
DEFINITIONSOFPERINATALMORTALITY
GLOBALPERINATALMORTALITY
Theburdenofperinatal (andmaternal)mortality isalmostexclusivelywithLMIC(12).
The most recent estimates indicate more than 2.5 million stillbirths and a similar
number of neonatal deaths annually(13-16). Additionally, there were 303,000
maternaldeathsglobally in2015(17).Bothmothersandbabiesaremost likelytodie

33
onthedayofdelivery(18,19).Therefore,anyinterventionfocusedaroundthetimeof
childbirth has the potential to impact the outcomes of both mother and baby.
Perinatalmortalityiscalculatedper1000totalbirths,usingtheformulainFigure2.1.
Thedefinition of perinatalmortality varies between countries as to the gestation at
whichafetalorneonataldeathisincludedinperinatalmortalitystatistics.Stillbirthis
definedas“deathpriortothecompleteexpulsionorextractionfromitsmother”and
earlyneonataldeathisdeathwithinthefirst7daysoflife(20).Whilethedefinitionof
the perinatal period is generally defined as any death from 22 weeks gestation
onwards,globalreportingandcomparisonsaregenerallydoneusingthedefinitionof
28weeksgestationorabirthweightof1000grams(gr)ormore(21),withbirthweight
asthepreferentialdenominator(22).ThePNMRforSouthAfricaisgenerallyquotedas
that for babies with a birth weight of 1000gr or more, although PNMR for smaller
babiesarealsorecorded(23).Conversely,perinatalmortalityinAustraliaisdefinedby
deathofatleast20weeksgestationordeathofababywithabirthweightofatleast
400grams(24).
Figure 2.1 The calculation of perinatal mortality, where early neonatal deaths are
withinthefirst7daysoflife(20).

34
Perinatal mortality can be separated in to three largely distinct time periods:
antepartum, intrapartumandneonataldeaths.The latter canbeconsideredasearly
(inthefirst7daysoflife)orlate(7-28daysoflife)neonataldeaths.Whenconsidering
theroleintrapartumcareplaysinneonataldeaths,itisthepredominantlyearlydeaths
thatareofinterest.
ANTEPARTUMMORTALITY
Antepartummortality isgenerallydefinedas“deathbeforetheonsetof labour”(25),
althoughthereisvariationbetweencountriesastowhichdeathsareincludedwithin
thisdefinition.Forexample,Australiadefinesstillbirthas“ababybornofat least20
weeksgestationor400grbirthweightwhodidnot,atanytimeafterdelivery,breathe,
orshowanyevidenceoflifesuchasaheartbeat”(26),whereasinSouthAfrica,babies
weighing500grormoreareincludedinthisdefinition(23),andICD-10definesafetal
deathasthatoccurringinababyweighingmorethan500grorbeinggreaterthan22
completed weeks gestation(22). Antepartum deaths are sometimes separated into
early(≥500grand<1000gr)orlate(≥1000gr)fetaldeaths(25).Estimatesofglobalrates
of antepartum deaths (stillbirths) are difficult given the lack of recording and
registrationofmoststillbirthsaroundtheworld(18).

35
INTRAPARTUMMORTALITY
Anintrapartumdeathisthatoccurringafterthecommencementoflabour,butbefore
completeexpulsionofthefetus(25),withmanycountriesaroundtheworldidentifying
a“freshstillbirth”asasurrogateforanintrapartumdeathintheabsenceoffetalheart
ratemonitoringthatdefinitively identifies thetimeofdeath(27,28).Theeventsthat
can lead to intrapartummortality are the focus for this research. This is particularly
pertinentasintrapartumstillbirthsinLMICrepresentthemajorityoftheglobalburden
ofthesetypesofdeathsandconsideredlargelypreventable(29,30).Upto70%ofall
stillbirths in LMIC are likely to be intrapartum deaths(19). Moreover, given that in
some LMIC attendance for antenatal care is uncommon (for example in Bangladesh
whereanyantenatalattendanceforcareoccurs in<2/3ofwomen(31)),contactwith
health care professionals in the intrapartum period may be the first medical
interaction, severely hampering the potential for obstetric care provision and risk
reduction(32).
EARLYNEONATALMORTALITY
Early neonatal deaths are those that occur before day 7 of neonatal life (25), and,
especiallyinlowresourcesettings,mayoccurasadirectconsequenceofintrapartum
careandevents(29,33,34). Indeed,mostearlyneonataldeaths inLMICoccur inthe
firstdayafterbirth,andmorethanhalfofthesefollowintrapartumasphyxia(35).Early
neonataldeathsareofparticularly importanceastheycontributeapproximately75%

36
of all post-natal deaths(36), and are responsible for 50% of the under five year
mortalityratesinLMIC(35,37-40).
PERINATALMORTALITYINMIDDLEINCOMESETTINGS
There exists a substantial body of literature on global perinatal mortality. Our trial
aimedtoconsideraninterventionthatwouldbeapplicableinmiddle-incomecountries
(MIC) where it is critical to consider the distribution of resources, such that any
interventiondoesnotcompromiseotheraspectsofcare.Perinatalmortality inthese
settings is disproportionately represented around the time of childbirth, and
interventions at this point are critical(41), however theuseof one interventionmay
resultinlessaccesstoanotherbecauseoffiniteresources.Thus,wearebeholdento
consider the scope of the problem of perinatal mortality in MIC in order to affect
changethatismeaningful,contextuallyappropriate,andpragmatic(42).
EstimatesofperinatalmortalityinMICarepresentedinTable2.1.Whileestimatescan
beinfluencedbyvaryingdefinitionsofdeaths,particularlystillbirths(43),itisclearthat
rates varywidely, from 7/1000 births inMalaysia to 111/1000 births inMauritania.
South Africa’s reported PNMR is 33/1000 births, which, it is worth noting, is 500%
higher than that in Australia(20). The impact of any intervention is related to the
frequencyofthecausativeproblem. It isevidentfromTable2.1thattherearemany

37
MICwheremortalityratescouldpotentiallybeimpactedbyaninterventionsuchasUA
lactatesampling.
Table 2.1 Perinatal mortality rates in middle income countries (Adapted from the
WorldHealthOrganization(20),exceptwhereadditionalreferencesindicated)
Country Perinatalmortalityrate (per1000births)
Country Perinatalmortalityrate (per1000births)
Country Perinatalmortality rate(per 1000births)
Albania 20 Grenada 21 Panama 15
Algeria 47 Guatemala 23 Papua NewGuinea
51
AmericanSamoa
5(44)* Guyana 40 Paraguay 20
Angola 86 Honduras 28 Peru 20
Argentina 14 India 70 Philippines 23
Armenia 29 Indonesia 30 Romania 12
Azerbaijan 58 Iran, IslamicRep.
35 RussianFederation
25
Bangladesh 50 Iraq 76 Samoa 21
Belarus 9 Jamaica 17 Sao TomeandPrincipe
61
Belize 33 Jordan 26 Serbia andMontenegro
13
Bhutan 40 Kazakhstan 57 SolomonIslands
20
Bolivia 31 Kenya 53 SouthAfrica 33
Bosnia andHerzegovina
20 Kiribati 44 SriLanka 20
Botswana 79 Kosovo 19(45) St.Lucia 20

38
Brazil 20 KyrgyzRepublic
57 St. Vincentand theGrenadines
19
Bulgaria 13 LaoPDR 57 Sudan 44
CaboVerde 30 Lebanon 34 Suriname 30
Cambodia 66 Lesotho 46 Swaziland 61
Cameroon 70 Libya 19 Syrian ArabRepublic
16
China 35 Macedonia,FYR
16(20) Tajikistan 62
Colombia 23 Malaysia 7 Thailand 20
Congo,Rep. 76 Maldives 54 Timor-Leste 65
CostaRica 13 MarshallIslands
43 Tonga 18
Coted'Ivoire 96 Mauritania 111 Tunisia 20
Cuba 14 Mauritius 17 Turkey 36
Djibouti 62 Mexico 22 Turkmenistan
39
Dominica 12 Micronesia,Fed.Sts.
20 Tuvalu 36
DominicanRepublic
28 Moldova 31 Ukraine 37
Ecuador 20 Mongolia 46 Uzbekistan 46
Egypt, ArabRepublic.
27 Morocco 31 Vanuatu 31
ElSalvador 20 Myanmar 65 Venezuela,RB
18
EquatorialGuinea
65 Namibia 46 Vietnam 37
Fiji 16 Nicaragua 23 West BankandGaza
21(46)
Gabon 59 Nigeria 86 Yemen,Rep. 44

39
Georgia 42 Pakistan 59 Zambia 56
Ghana 45 Palau 23
*Dataonlyavailableforneonataldeaths
PERINATALMORTALITYINTHEMIDDLE-INCOMECOUNTRYLITERATURE:AREVIEW
A literature review on perinatal mortality in MIC was conducted. PubMed was
searched,usingacombinationof theMeSHterms forpoverty,developingcountries,
perinatal death and perinatal mortality. (((("Poverty"{Mesh}) OR "Developing
Countries"{Mesh})AND"PerinatalDeath"{Mesh})OR("PerinatalMortality"{Mesh}OR
"Fetal Mortality"{Mesh})). Middle income countries were defined usingWorld Bank
criteria(47), and are outlined in Table 2.1. 1299 studies were identified since 2000.
Titlesandabstractsweresearchedandfulltextarticlesrelevanttoperinataloutcomes
inMICareexploredbelow.
MICmayhaveahighbaselinePNMR,andthenwithincountryhaveregionswitheven
higher PNMR and therefore face greater resource challenges in addressing these
regionaldisparities(48-54).Moreover,analysesofperinataldeathsinMICoftenshow,
in addition to a high PNMR, significant numbers of these deaths are preventable,
althoughprogressonthisisoftenlimitedbyhumanandphysicalresources(55,56).Itis
this large group of preventable perinatal deaths where efforts to improve global
perinatalmortalityshouldbetargetedandwheretheconceptofthisthesisstemmed
from.

40
PERINATALMORTALITYINROUTINEOBSTETRICCARE
One of the challenges for obstetric care in MIC is the mortality associated with
commoneventsorclinicalproblemsthatwouldbeconsideredlargelystraightforward
tomanageinhigh-incomesettings.Oneofthecontributorstothismaybetheconcept
of “fragile states” – that is, that thismortality occurs in countrieswhere theoverall
physical and human infrastructure deficits lead to worse outcomes in vulnerable
groups,includingwomenandtheirnewborns(57).
Many clinical pregnancy and intrapartum scenarios in high-income countries are
recognised as potential situations for complications, and resources formanagement
directedasappropriate.ThesameisnottrueforMIC,anditisevidentfromreviewing
theliteraturethattheprevalence,aetiology,treatmentandconsequencesofmaternal
andperinatalclinicalissuesordiseasebecomefarmorecomplexthanthesameissue
inhigh-incomesettings.
Maternal conditions in pregnancy are potentially more complex to manage inMIC,
with consequent worse maternal and perinatal outcomes. Several examples are
outlinedbelow.

41
• Hypertensive disorders, which are among the commonest maternal
complicationofpregnancy,are frequentlyassociatedwithworseoutcomes in
MIC(58).
• Non-pregnancymedical conditions complexifymanagement inMIC.Maternal
anaemia, for example, has been shown in a large systematic review to be
associatedwithadverseperinataloutcomes(59).
• Even common pregnancy occurrences, such asmultifetal gestations, perform
poorly in lowresourcesettings,AGlobalNetworkStudy insixmiddle income
countries (Kenya, Zambia, Pakistan, India, Guatemala and Argentina)
demonstrated a significant contribution of multifetal gestations to adverse
outcomes in these settings,withamaternalmortalityof 0.5%andanoverall
perinatalmortalityofaround20%(60).Similarfindingsarereportedfromother
studiesofmiddleincomecountries(61,62).
• Even common labour management issues increase in complexity in MIC. A
retrospectivereviewinDakarofvaginalbirthaftercaesareansectionrevealed
a perinatal mortality of 26.4%, largely due to abruption and uterine
rupture(63).
Suchmorbidity andmortalityof so-called routineevents is repeated throughout the
literature formortality inMIC, and not often seen in high-income countries(64-68).
This is highlighted in the rates of intrapartum asphyxia in LMIC, which is markedly
differenttohigh-incomecountries.InoneprospectivecohortstudyinPakistan,119of
the1103deliverieswereperinataldeaths,andnearlyhalfofthesewereattributedto

42
birth asphyxia(69). Audit in a tertiary unit in Nigeria showed that when macerated
stillbirths were removed from consideration, asphyxia caused the overwhelming
majorityoftheremainingperinataldeaths(70).
FACILITYBASEDDELIVERYANDPERINATALMORTALITYINMIDDLE-INCOMECOUNTRIES
Itisworthnotingthattheaimofthisresearchistoimproveintrapartumcareusinga
tool that by definition necessitates facility-based delivery, which is not universal in
MIC.Thus,theinterventionneedstobeconsideredwithinthecontextoftheproblem,
andthepotentialscopeoftheresearchisclearlyrelatedtotheissueoffacility-based
delivery,aswellasthequalityofcaredeliveredinthosefacilities.TherearemanyMIC
wherefacility-baseddeliveryisstilluncommon,andthismodelofcare,particularlyin
the absence of training of community birth attendants, increases perinatal
mortality(71-81). Nigeria, for example, has a facility-based delivery rate of only
35%(82),Ghana of up to 75%(83), Kenya of only 50%(84, 85), but countries such as
China and India nearly 100%. However, while facility-based delivery will generally
result in improved perinatal outcomes(86), the referral bias of shifting high-risk
deliveriesfromthecommunitytofacilitiesmayresultinlessimprovementbeingseen
than expected(87). In LMIC, complex cases often require transfer to higher acuity
units,increasingthelikelihoodofasphyxiaanditsconsequences.InonestudyinIndia,
the rate of intrapartum perinatal mortality secondary to asphyxia among cases
referredemergentlyinlabourwas80/1000births(79).

43
Women inMICwill often, but not always, have improved perinatal outcomeswhen
antenatalandintrapartumcareisshiftedtofacilities(88),howevertheimprovementin
perinatal mortality is often not commensurate with the increase in facility-based
delivery(89). In Bangladesh the rate of facility delivery is reported as 16%, while
perinatal mortality is up to 64.7/1000 births, with up to one in five women having
intrapartum complications(90). Hence, translocating these women to facility-based
delivery shifts the acuity of cases in those centres too. Higher acuity does not
necessarilyresultinadverseoutcomesinallMIC;Chinaforexamplehasahighfacility
birthrate(91,92)butaperinatalmortalityrateofonly7.2/1000births(93).
It is clear that the occurrence of facility-based delivery does not guarantee human
resourcestodeliverintrapartumcare(94),orifdelivered,thereisnoguaranteeofthe
qualityof intrapartumcare (18, 34, 87, 95),which is necessary to improveperinatal
outcomes(96). This concept is borne out in the literature repeatedly. There are still
unacceptablyhighratesof intrapartumstillbirthreported in institutionaldeliveries in
middle income countries; for example, Ghana reports a rate of 1% frommore than
400,000institutionalbirths(42).RegionsofIndia,whichhavenearlyuniversalcoverage
of facility-based birth, have seen the shift to facility birth impact stillbirth but not
neonatalmortalityrates(97).Similarly,astudyinTurkeycomparingratesandcausesof
perinatalmortalityfrom1998to2009showedareductioninantenatalstillbirthbutan
increaseinperinatalasphyxiarelateddeathswhenbirthswereshiftedtofacilities(98).
Onewouldpresumethatantenatalinterventionstoimprovestillbirthrates(e.g.blood
pressureandurinechecksatantenatalvisitstoidentifycasesofpre-eclampsia)areless

44
complextoimplementthanwidescaleimprovedqualityofcareinfacilities,whichmay
explain the discordance between increased facility-based births and persistent
perinatalmortality.
QUALITYOFCARE
Suboptimalqualityofcarearoundthetimeofchildbirthcontributestotheburdenof
perinatalmortalityinMIC.ThereisextensivereportingintheMICliteratureregarding
the contribution of intrapartum care (and issues with the quality of that care) to
perinatal mortality. The concept of quality of care around the time of childbirth
possiblyexplains large in-countryvariations inperinatalmortalityrates.Forexample,
Turkey has a PNMR reported as 36/1000(20), but regional studies report rates of
nearly 50/1000(99). The prevention of asphyxia and the early treatment of the
asphyxiated neonate has the potential to save millions of women’s and babies
lives(100,101),howeveraccesstocarealoneisnotnecessarilyenoughforprevention,
ifthereareissueswiththequalityofthatcare(102).Examplesofthisconceptcanbe
seenthroughouttheliteratureinanalysesofthetypeofcaregivenandtheoutcomes
ofperinatalaudit.
• TheDemocraticRepublicofCongohasaveryhighPNMR,andlowQoCinthe
maternal and newborn health services that do exist(32) and Pakistan has a
neonatalmortality rate of 55/1000 births, with the lack of access to “good”

45
newborncarebeingidentifiedtoattributingtothishighrate(103).Theconcept
ofQoC(orlackthereof)islikelysynonymouswithpreventableperinataldeath.
• An analysis of perinatal deaths in Salvador, Brazil, reported a perinatal
mortalityrateof25.8/1000butmorethan90%ofthesewerepreventable,and
moreover, nearly half of the deaths would have been prevented with QoC
aroundthetimeofchildbirth(104).
• The linkbetweenQoCandperinataldeath isseen intheratesof intrapartum
asphyxia,whichaswehavealreadysaid,usuallyoccurs intheabsenceofrisk
factors (i.e. otherwise healthy mothers and fetuses). In a large population
based study inChina, a quarterof theneonatal deathswere causedbybirth
asphyxia(105). Similarly comprehensive audit of deaths in Guatemala, the
Democratic Republic of Congo, Zambia, and Pakistan resulted in a quarter of
neonataldeathsbeingattributed tobirthasphyxia(106).Tertiary level care in
NigeriahasaPNMRofupto81/1000births,withperinatalasphyxiabeingthe
greatest contributor to this(107). InGhanabothasphyxiaandbirth injuryare
thegreatestcontributorstoearlyneonataldeaths(108),andinTanzania,athird
ofneonataldeathsareattributedtoasphyxia,despiteatleasthalfofallbirths
occurringinhealthfacilities(101,109).
The critical role of QoC can be seen if one considers the outcomes of nulliparous
comparedwithmultiparouswomeninthesameinstitutions.Nulliparouswomenoften
bear the burden of obstetric complications, particularly in MIC(66, 110-115), with
multiparity often protective against adverse obstetric outcomes(116). Hence, the

46
impactofQoCmaybemorepronouncedinnulliparouswomen.Inonecomparisonof
parity-basedmaternalandperinataloutcomesinwomenhaving institutionaldelivery
in the Democratic Republic of the Congo, nulliparous women had higher rates of
obstetricinterventionandperinataldeath(4.93%comparedwith2.8%)(117).
It is evident from the above data that persisting poor quality of intrapartum care
continues to drive high perinatal mortality rates in MIC by its contribution to
preventabledeaths(118).
CAESAREANSECTIONINMIDDLEINCOMECOUNTRIES
WhileintrapartummortalityisunacceptablyhighinMIC,itisclearthatashifttowards
caesareansection(CS)toaddressthisissueisnottheentiretyoftheanswer,andtodo
sowouldpotentiallyincreaseperinatalandmaternalmorbidityandmortalityinsome
settings(3,119-122).Thatsaid,itcanbedifficulttoanalysewhethertheindicationfor
theCSortheprocedureitselfcontributesmosttothemortalitystatistics(123).Access
toCS inMICneeds tobeapartof comprehensiveemergencyobstetric servicesand
well-functioninghealthsystems(101).Moreover, inMICsettingswheretheCSrate is
alreadyhigh, forexampleBrazil, a reduction in the ratehasbeenshown to improve
maternal and perinatal outcomes(124). In a quality audit study in Nigeria,
paradoxically, fetal mortality increased with increased CS rates(125), which may
representinfrastructureissuesintimelydeliveryorintheuseofCSformaternalrather
thanfetalindications.WhileaccesstoCSisnecessaryforsafeobstetricoutcomes(126),

47
theQoCaroundCS inMICmay result inhighperinatal andmaternalmortality(127).
This isparticularlytrue inpoorlyresourcedsettings,wherethe“decisiontodelivery”
time once an emergency caesarean section is indicated may be delayed (due to
staffingandphysicalresources)suchthatperinataloutcomesareworsened(128).
48
PERINATALMORTALITYINSOUTHAFRICA
PerinatalmortalityinSouthAfricaisapproximately33/1000births(23),withstillbirths
contributing around two thirds of this rate, and neonatal deaths comprising the
remainder. This rate is highlighted as particularly unacceptable given that neonatal
deaths (deathsprior to28daysof life)account fornearlya thirdof themortalityof
childrenunderfiveinSouthAfrica,andalargeproportionofthesefollowintrapartum
hypoxia(129-131).Moreover,individualunitorregionalstillbirthratesarereportedas
fargreater,at30-40/1000births(132,133).However,therateofperinatalmortalityis
consistentlyreportedasimprovingoverthelasttwotothreedecades(130,134,135),
although some individual facilities have not followed this trend(136). One of the
challenges in perinatalmortality reporting in someprovinces is the largenumber of
women that deliver at home, oftenwithout a skilled birth attendant(135), although
thisnumberisprogressivelydeclining(130,137).
Reporting of perinatal mortality in South Africa is predominantly derived from two
sources; the District Health Information System (DHIS) and the Perinatal Problems
IdentificationProgram(PPIP)(130).SecondarytothePerinatalProblemsIdentification
Program(PPIP)(23),SouthAfricaisuniqueamongstLMICinbothitsperinatalmortality
data collection and ability for within country comparison. PPIP is a quality of care,
facility based audit system,which captures data around perinatal deaths, aswell as
identifypotentiallymodifiablefactors inthosedeaths.Since2012 it ismandatoryfor
allpublichealthfacilitiesinSouthAfricatousethePPIPsystem(129).PPIPreportson

49
PNMRforallbabieswithabirthweightmorethan500gr,aswellasratesfordifferent
weight categories. PPIP specifically reports onbirthweight rather than gestation, as
this is commonly not definitively known at the time of delivery. This represents a
limitationofthedata(commontolowandmiddleincomecountries),wherebyoutliers
of fetal weight for gestation (for example in the case of unidentified intrauterine
growthrestriction)maybeerroneouslyincludedorexcludedinthedata.
CAUSESOFPERINATALMORTALITYINSOUTHAFRICA
In themost recent PPIP report, which is a summary of the 24months prior to the
commencementoftheauthor’sthesisresearchinSouthAfrica,datawerecollectedon
76%ofallbirthsinSouthAfrica.Inthattimeperiod,therewere1,412,355birthswith
32,662stillbirthsand14,576earlyneonataldeaths(23).

50
Image 2.1: Saving babies. The most recent report from the perinatal problems
identificationprogram
The PPIP data reports on all levels of obstetric care in South Africa, including
community health centres and district hospitals. The research for this thesis was
conductedinaProvincialTertiary(PT)Hospital.Thehospitalwheretheresearchwas
conductedis intheTshwanedistrictwithintheGautengprovinceofSouthAfricaand
additionaldataforthisregion isoutlinedbelow.Thedata inthefollowingparagraph
areextractedfromthe2012-2013SavingBabiesReport(23).

51
ThePNMRforPThospitalsinSouthAfricais55.3/1000births,presumablyareflection
ofhigheracuitycasesandreferralfromother,lowerlevelsofcare.ThePNMRinthese
unitsforbabieswithabirthweightgreaterthan1000grams,aweightatwhichthereis
a significant increase in survival (compared with lower birth weight babies)(138), is
36.16/1000 births. The primary obstetric causes of death for all perinatal mortality
cases in PT hospitals are, in order of frequency, unexplained stillbirth, hypertensive
disorders, spontaneous preterm labour, antepartum haemorrhage, and intrapartum
asphyxia. For babies greater than 1000gr at birth, spontaneous preterm labour is
removedfromthislistandtheorderoffrequencyremainsotherwiseunchanged.The
PNMR in theTshwanedistrict is23.74/1000births,and16.09/1000births forbabies
weighinggreaterthan1000gr.
Whilst this research should be widely applicable in South Africa, it is important to
consider themortality data specific to the study location prior to commencing this
thesis.KalafongHospitalisa1000bedmulti-servicehospitalinPretoriaintheprovince
ofGauteng,withmore than 6000 deliveries per year. Table 2.2 shows the perinatal
careindicators(PCI)forKalafonghospitalin2013,theyearpriortocommencementof
the research contained in this thesis. The total PNMR was 14.8/1000 births, with
substantially higher rates in certain birthweight categories, for example a PNMRof
24.9/1000forbabiesweighing2000-2499gr.

52
Table2.2:PerinatalcareindicatorsatKalafongHospital,2013

53
PERINATALMORTALITYINSOUTHAFRICA:AREVIEW
A literature review was performed to explore the reporting of causes of perinatal
mortalityinSouthAfrica,inadditiontoPPIP,relevanttothisthesisandtoconsiderthe
applicability of our intervention. PubMed was searched, using the following search
strategy, restricted to articles published since 2000; (((South Africa) AND perinatal
mortality(MeSHTerms))ORfetalmortality(MeSHTerms)),aswellasanon-Meshterm
search for South Africa AND perinatal mortality. 788 articles were identified, with
relevantstudiesexploredbelow.Additionally, theSouthAfricanJournalofObstetrics
andGynaecologywashand-searchedfrom2006onwards.Themainpointsidentifiedin
thelimitedliteratureavailableareoutlinedbelow.
• Intrapartumasphyxiaisfrequentlyreportedintheliteratureasoneofthemain
contributors to perinatal mortality in South Africa, due to both (late or no)
access to hospital-based care and access to quality care once in the hospital
system,particularlyconcerningtheuseof fetalmonitoringandrecognitionof
fetalheartrateanomalies(1,131,132,134-136,139-146).
• Inananalysisof stillbirthsavertedbycarepractises,Michalowetal reported
that nearly three quarters of those averted were done so with intrapartum
interventions,includingaccesstocomprehensiveemergencycare(130).Infants
inSouthAfricaareatsignificantriskofdeathinthefirstweekoflifefollowing
clearly preventable intrapartum hypoxia(147) and this sentiment is echoed
repeatedlyintheliterature(137,140,144).

54
• There are large in-country variations in PNMR and intrapartum care; in one
retrospective audit using the PPIP data, the contribution of intrapartum
hypoxiawasfoundtobefargreaterinoneunit intheEasternCapethanthat
reportedinthenationalstatistics(148).
• The most common causes of perinatal mortality in South Africa are usually
(with slight variations in order of frequency, often depending on the level of
care) intrapartum asphyxia, unexplained intrauterine death, spontaneous
preterm labour, antepartumhaemorrhage,hypertension, fetal anomalies and
infection(130,133-135,144,149-151).Alackofqualityorcareorappropriate
responses when these situations arise contributes to both perinatal and
maternalmortalityinSouthAfrica(152,153).
THEGLOBALCLASSIFICATIONOFPERINATALMORTALITY
While themain trial in this thesiswasbased inKalafongHospital, itwasanticipated
thattheresultswouldpotentiallybeapplicabletootherLMICsettingsinternationally.
Thus,followingonfromidentifyingthecausesofperinatalmortalitybothatKalafong
hospital and in South Africa, onemust consider classifying them, such as is done in
PPIP,inordertobeabletoidentifyareaswhereinterventiononalargerscaleislikely
toimpactthePNMR.PPIP,however,isuniquetoSouthAfricaandthuscomparisonsof
theimpactofinterventionsindifferentsettingsoutsideofSouthAfricaarepotentially
difficult. The question arises: is all globally reported perinatal mortality the same?
Estimating and comparing global perinatal mortality is particularly challenging,

55
secondaryto largevariations inregistrationdataandinterpretationsofdefinitionsof
mortality,particularlyatthelimitsofviability(154).Thisisoneofthemainreasonsthat
the WHO uses the definition of 1000gr birth weight or 28 weeks gestation for
internationalcomparisons(22).
Including PPIP, there aremore than 80 perinatal death classification systems in use
around the world(155), making comparisons between countries particularly
challenging. To that end, based on experienceswith the PPIP system,we sought to
developa global classification system forperinatal deaths.Over2014and2015, the
World Health Organization, in collaboration with partners, developed The WHO
applicationof ICD-10toperinataldeaths: ICD-perinatalmortality (ICD-PM)(156,157).
Wewere thenable to further analysis the causesofdeath in SouthAfricausing the
ICD-PM. The author of this thesis co-lead the work (with Dr Ozge Tuncalp) on
developing the ICD-PM and undertook the initially field testing of the classification
system.ThepaperspublishedaboutICD-PMbytheauthorofthisthesisareoutlinedin
Appendix2.1.AfterthedevelopmentoftheICD-PM,Ifield-testedthesystemonnearly
10,000perinataldeathsfromtheUKandSouthAfrica.
The ICD-PM classifies perinatal death according to the time period of the death
(antepartum,intrapartum,orneonatal),andlinkstheperinataldeathtothematernal
conditionatthetimeofdeath(158).AnanalysisofSouthAfricandatausingtheICD-PM
provides insights in to the timings and causes of death in one large region in South

56
Africa.Halfofalldeathsinthisanalysis(344/689)occurredintheantepartumperiod,
with74(11%)occurring intrapartum,andtheremainder (271/689,39%)occurring in
theearlyneonatalperiod(21)(Figure2.2).
The major cause of death in the antepartum period was a fetal hypoxic event,
associatedmostcommonlywiththematernalconditionsofhypertensionorplacental
abruption.Intrapartumdeathswerelargelyacutehypoxicoccurrences,inthecontext
ofotherwisehealthymothers; the implicationsof thisbeing that thesedeathsarea
consequence of intrapartum care. Early neonatal deaths are distributed among
respiratorydisorders(largelyrespiratorydistressandmeconiumaspiration),lowbirth
weightandprematurity,andhypoxicischaemicencephalopathyfollowingintrapartum
asphyxia(21).

57
Figure2.2:DistributionofperinatalmortalityacrossthreetimeperiodsinSouthAfrica.
Adapted fromAllansonetal 2016(21). “Distributionn (%)ofperinatal deaths across
the antepartum, intrapartum, and neonatal time periods in South Africa (n=689,
October2013–January2014)”
GiventhisanalysisandthePPIPdata,itappearsalargeproportionoftheintrapartum
andearlyneonataldeaths inSouthAfricaareaconsequenceof thecareprovided in
theintrapartumperiod.This isaperiodduringpregnancywherecarewithinfacilities
occurs and therefore ispotentially amenable toalterations inpractice. Thus, for the
purpose of this thesis, we focused on this period and an intervention that would
potentiallyimpacttheseoutcomes.
n=344
n=74
n=271
0
10
20
30
40
50
60
Antepartum Intrapartum Neonatal
%
Timingofperinataldeath
SouthAfrica
SouthAfrica

58
FETALPHYSIOLOGYANDTHEIMPACTOFHYPOXIA
ACIDBASEBALANCEINTHEFETUS
In order to consider the impact of hypoxaemia, hypoxia, and acidosis in the
intrapartumperiod,anunderstandingofthenormalphysiologicalstateofthefetusis
necessary.
In its normal state, the fetus metabolises glucose to energy using aerobic
processes(159).Theendproductofthisprocessistheformationofpyruvateandthen
adenosinetriphosphate(ATP)(159).Maintenanceofacid-basehomeostasisinthefetus
islargelycontrolledbytheplacenta,andtheby-productofaerobicmetabolisminthe
fetus (CO2) is transferred to, and eliminated by, the placenta(160). The placenta
thereforefunctionstoresultinawell-oxygenatedfetuswithwell-oxygenatedtissues.
Tomaintain a homeostatic state, a fetus at termor near-term gestationwill have a
cardiacoutputbetween300and480ml/min/kilogramof fetalweight,with supply to
themyocardiumandthebrain(161,162).Whenhypoxaemiaandhypoxiaoccurs,the
fetus loses the capacity to efficiently convert pyruvate toATP, and thus switches to
anaerobic metabolism. This process results in rapid consumption of glucose and
accumulationoflactatewithasubsequentfallinpH.(Figure2.3)Thisultimatelyleads
toacidosis,tissuedamage,andtheclinicalmanifestationsofintrapartumasphyxia.

59
Figure 2.3 Aerobic and anaerobic metabolism. Adapted from Yli and Kjellmer,
2016(159)
INTRAPARTUMHYPOXIA
As previously described, intrapartumhypoxia canbe considered a “deficiency in the
amount of oxygen reaching the tissues(163)” during the first and second stage of
labour. Any period of hypoxaemia (interruption in fetal oxygen supply) has the

60
potentialtoresultinhypoxia(2),dependentonavarietyoffactors,whichareoutlined
laterinthischapter.Sustainedsignificanthypoxiawilleventuallyresultinacidosis,by
themechanismsdescribedabove,whichplacethefetusatriskofsignificantmorbidity,
includingneurologicalmorbidity,anddeath(2).
THEFETALRESPONSETOHYPOXIA
While the fetus is relatively hypoxic (compared to a neonate)(101), further limiting
oxygen supply to the fetus will result in one of three sequential steps occurring;
hypoxaemia, hypoxia, asphyxia(159). Hypoxaemia is defined a reduction in arterial
oxygen levels, hypoxia a reduction in oxygen supply to tissues, and asphyxia is the
consequence of acidosis (increased tissue levels of hydrogen ions) and acidaemia
(increased blood levels of hydrogen ions) (164, 165). If both acidosis and acidaemia
prolonged,thesewillleadtoadisruptioninthenormalacidbasebalance,withafallin
pH and an accumulation of PCO2 and lactic acid ions(160). As such, acidosis and
acidaemia (frequentlyused interchangeably in the literature)arehenceforthused to
reflecttheacidoticconsequenceofhypoxia.
Disruptions in oxygen supply to the fetus are more likely to occur at the time of
labour(159),howeverthefetusisdesignedtoadapttoadegreeofhypoxiapriortothe
manifestationofanyclinicalconsequence.Duringhypoxaemia,thefetuswill increase
the flow of blood through the ductus venosus in order to maintain adequate

61
oxygenation(161).Thefetuswillalsorespondtohypoxaemiabyreducingitsheartrate,
andincreasingbloodflowtobrain,myocardium,andadrenalglands(162).Theamount
ofhypoxia a fetus canendurebefore it switches tomaladaptivemechanisms varies.
Oncethefetusreachesitsself-definedlimitofprolongedhypoxia,itwillthenmoveto
thefarlessefficientformofenergyproductionofanaerobicmetabolism(159,164).
PRODUCTIONOFLACTATEANDFETALORGANSYSTEMRESPONSETOHYPOXIAANDACIDAEMIA
The fall in p02 following a hypoxic inducing event activates an acute fetal stress
response, mediated by the hypothalamic-pituitary-adrenal (HPA) axis, whereby the
production of corticotropin-releasing hormone (CRH), arginine vasopressin (AVP),
adrenocorticotropic hormone (ACTH), and glucocorticoids all increase (166). The
responsetoacutehypoxicevents includesarise infetalcortisol,whichwillgenerally
resolvewith the resolutionof theprecipitatingevent, andwitha consequent rise in
fetal lactate(167). Animal studies show complete cord occlusion results in a
progressive andmarked rise in fetal lactate,with variable recovery tobaseline after
resolutionofthe insult(168-171).Moreover,thegrowthrestrictedfetuscanmounta
similar lactateresponsetohypoxicstress,whencomparedtoitsappropriatelygrown
counterparts(172).

62
Thecomplexinterplayofanaerobicmetabolism,lactateproductionandindividualfetal
organresponsetoperiodsofhypoxianeedstobeconsideredastheresultantpotential
forclinicalconsequencesstemsfromthisinteraction.
CARDIACSYSTEM
The autonomic nervous system (ANS) regulates the fetal heart rate(159),whichwill
lower in response to hypoxia, largely vagally mediated, with the aim of reducing
overall fetaloxygenconsumptionandconservingenergy(173,174). It is importantto
notethatthefetalcardiacoutputwillremainstableinthepresenceofhypoxiawithout
acidaemia(162),whichisclearlyanadaptivemechanismforthefetusduringlabour.
Theinitialresponsetohypoxia(showninanimalstudieswithcompletecordocclusion)
isariseinmeanarterialpressure(MAP),withacorrespondingfall inheartrate(HR).
Blood flow will be redistributed to central organs and cerebral perfusion will be
maintained.TheMAPwillfallwithcontinuedhypoxia,howeverboththeMAPandthe
HRwillhaveareboundriseafterresolutionoftheinsult(168-170,174-177).Inavery
sophisticatedadaptivemechanism, the increase in lactate levelsand theconsequent
acidaemia is a further technique for the fetus to survive a hypoxic insult, as the
acidaemia aids the transfer of oxygen from haemoglobin to tissue(173). The aim of
thesecomplexcoordinatedresponsestohypoxia is to limit the impactof“threats to
fetalhomeostasis”(174).
63
RENALSYSTEM
Thefetalkidneywillgenerallymetaboliselactate,howeverwhenexposedtohypoxia,
thekidneywill insteadmetaboliseglucoseandexcretelactate(161).Bothrenalblood
flowandurineoutputwillfallduringhypoxia,andsimilartotheotherorgansystems
thereisaperiodofrenalhypoperfusionfollowingresolutionoftheinsult(170).
CEREBRALSYSTEM
Thecerebralsystemrepresentsthemainclinicalmanifestationofintrapartumhypoxia
resultingintissuedamage,withnearlyalldefinitionsofintrapartumasphyxiaincluding
somementionofalteredneonatalneurological state(178).Thecerebralvascularbed
undergoes vasodilation during hypoxia, promoting neurological protection.(173)
However, cerebral blood flowwill decrease during cord occlusion(171), and cortical
oedemawill occur during prolonged hypoxia(175). Animal studies show evidence of
decreased neurological activity (measured via EEG) during hypoxic insults(168, 179).
Thepost-insultperiodisnotwithoutriskeither,withre-perfusionandre-oxygenation
ofcerebraltissuesanatriskperiodfordamage.

64
GASTROINTESTINALSYSTEM
Cardiac output during a hypoxic insult is preferentially shunted away from the
gastrointestinal system and redistributed to the cardiac and cerebral systems. In
animal studies, there isevidence that thehypoperfusion to thegutduringahypoxic
episode is sustained after resolution of the insult, with cardiovascular collapse
followingthe insultresulting inafailureof immediatenormalredistributionofblood
flow(168,180).This furthersupports theconcept thatevenshortperiodsofhypoxia
significant enough to cause fetal circulation redistribution may have consequences,
evenintheinstanceofapparentfetal/neonatalrecovery.
THEPRETERMFETALRESPONSETOHYPOXIAANDASPHYXIA
Attheoutset,theresearchthatformedthebasisforthisthesisaimedtoincludeboth
preterm and term gestational age births. It is therefore pertinent to consider the
response that the preterm infant has to hypoxia, particularly in the intrapartum
period.Pretermfetusesareclearlyalsoatriskofintrapartummortality(181),however
thethresholdforthepretermfetustorespondtohypoxiaappearsgreaterthanthatof
its term counterpart, which is possibly a reflection of its immature autonomic
system(174).Preterm fetusesappear tobeable to survive longerperiodsofhypoxia
thantermfetuses,howevertheimmaturityoftheirphysiologicalsystemputsthemat
greater risk of more severe clinical consequences(174), and therefore potentially
contributesignificantlytohypoxiarelatedperinataldeathsinLMIC(182).

65
LACTATEASAMEASUREMENTOFMETABOLICACIDOSIS
As outlined earlier, lactate can be expected as an end product of glucosemediated
anaerobicmetabolism(159,183-185),whichoccursinthefetusinresponsetohypoxic
stress(166, 186, 187). The metabolism of pyruvate in this cycle results in the
productionoflactate(188-190),whichbyvirtueofbeingtheendproductinthecycle,
may give the most objective measure of metabolic acidosis in the fetus(191). UA
lactateisalmostentirelyfetalinorigin(189,192,193),makingitanidealmeasurement
forassessingthe impactof intrapartumcareonthefetusandnewborn.Additionally,
UA lactate is likely to reflect metabolic acidosis(191), which is more likely than
respiratory acidosis to result in poor neonatal outcome andpermanent neurological
damage(194, 195). Practically, UA lactate is simple to measure (as outlined in
subsequentsectionsofthischapter).
The most common precipitating event for lactate production in labour is transient
umbilical cord occlusion. Fraschet al demonstrated in animal studies an increase in
fetalarteriallactateof0.56mmol/Lperminuteofcordocclusion(196).Hypoxicinsults
beyond“normal”cordocclusioncouldresult ingreaterdegreesof lactateproduction
andacidoticconsequences.

66
THECLINICALCONSEQUENCESOFHYPOXIAANDACIDAEMIA
There is a complex interplay between the pre-exposure state of the fetus, and the
extent,frequencyandintensityofexposuretohypoxiaandacidaemiathatdetermines
the clinical consequences, if any, a fetus and neonatemaymanifest(166, 197). The
fetus, even in the preterm period, has the capacity to survive prolonged periods of
acutehypoxia,withanimalstudiesexploringtheconsequencesofupto30minutesof
complete cord occlusion(168, 169, 171, 179). More chronic hypoxia is seen in the
antenatal period with conditions such as fetal growth restriction and, whilst these
fetuses have the potential to have an uncomplicated antenatal intrapartum course,
this is not always the case, and they are at significant risk for both stillbirth and
intrapartum asphyxia(198). It is the sequence of events from hypoxia to the
developmentofasphyxiathatisofparticularinteresttothisthesisproject,giventhat
intrapartumasphyxialeadstothedeathsofmillionsofbabiesinLMICannually(199).
THECONCEPTOFASPHYXIA
Intrauterine hypoxia and intrauterine asphyxia are frequently used
interchangeably(200),howevertechnically,thetwoshouldbeseparated.Hypoxiaisan
(invivo)objectiveprocess,whileasphyxia isa farmorebroad term,encompassinga
conglomerationofclinicalmeasures(201).TheICD-10groupsintrauterinehypoxiaand
birth asphyxia together, but with varied definitions. Intrauterine hypoxia includes

67
“fetal or intrauterine acidosis, anoxia, asphyxia, distress or hypoxia”. Intrapartum
asphyxia is however defined with clinical terms including “pulse less than 100 per
minuteatbirthandfallingorsteady,respirationabsentorgasping,colourpoor,tone
absent”.(22)Anobjectivemeasurementofacidosis,suchaswithcordpH,baseexcess
or lactate level, can be used where available tomake the diagnosis of intrapartum
asphyxia(200),whichisappropriatewhensustainedhypoxialeadstoacidosis,thebasis
fortheclinicalsequelae(2).
CAUSESOFACUTEHYPOXIAANDASPHYXIAINTHEINTRAPARTUMPERIOD
Inordertofurtherinterrogateintrapartumhypoxiaandasphyxia,eventsthatcanlead
to the previously described physiological changes and consequent clinical outcomes
shouldbeconsidered.Normaluterineactivitywilltemporarilydiminishumbilicalblood
supply(164), however the degree of hypoxia and clinical response to that hypoxia is
likelyminimalinanotherwisewellfetus.
Thecausesofacutehypoxiathathavethepotentialtoresultinadverseoutcomesfor
the fetus are outlined in Table 2.3, with the causes, published rates for LMIC, and
consequences shown. These are particularly important to consider given the
contributionof intrapartumevents in LMIC to acutehypoxia, asphyxia andperinatal
deaths(90, 108, 202-204), and that the babies who do not die as a result of
intrapartum events are at significant risk of adverse neonatal outcomes such as
68
hypoxic ischaemicencephalopathy(205).Furthermore, thecomplications that lead to
intrapartumperinatal(andpotentiallymaternal)mortality,areoftenmoreprevalentin
LMIC(101). Once facility-based delivery is achieved, one of the next steps is the
collection of comprehensive data so prevalence can be clarified and areas where
interventions to improve PNMR can be identified and targeted. The scarcity of
prevalence and outcome data for obstetric complications in LMIC contributes to
ongoingissueswithresourceallocation(206).
Asphyxia in high income countries is of low prevalence and as such intrapartum
intervention programs may have no or minimal impact on the rate of cases(201).
HoweverthesameisnottrueinLMIC(36),wheretheoccurrenceofperinatalhypoxia
andasphyxia isassociatedwithasignificant incidenceofobstetriccomplicationsand
resultantadversematernaloutcomes(114).Obstetriccomplications inLMIC including
haemorrhage, severe pre-eclampsia/eclampsia, sepsis, prolonged/obstructed labour,
severe abortion complications, ruptureduterus, andectopic pregnancy are reported
byBaileyetalinupto30%ofwomen(42).
As outlined previously, intrauterine hypoxic injury commences with a reduction in
cerebral blood flow following a precipitating event (whichmay be acute or chronic,
andmaternal,placentalorfetalinorigin(207)),whichinturncausesthefetustoswitch
to anaerobic metabolism(159, 208), leading to asphyxia(165, 209, 210). It is
reasonable,toadegree,toexpectthataprecipitatingeventcanbeidentifiedtowhich

69
the outcomeof acidosis can be linked.We appreciate that predicting the degree of
responseafetushastoaparticulareventispotentiallymoredifficult(160).Regardless,
givenboththeratesofasphyxiainLMICandtheobstetriccomplicationratesreported
byBaileyetal,weconsideredtheratesandconsequencesofthecommonintrapartum
eventsthatmayresultinhypoxiaandasphyxiainLMIC(Table2.3).
Table2.3.Causesand frequencyof clinicalevents that result in intrapartumhypoxia
andasphyxiainLMIC.
Cause Frequencyreported inLMIC
Consequence
Normaluterineactivity(164,165,211)
N/A TransienthypoxiawithfallsinpHinnormallabour.
Suspectedfetaldistressandperinatalmortalityinthecaseofnuchalcord(78).
Excessiveuterineactivity(tachysystole)(212,213)
Not reported,data fromhigh incomecountries
Reported at a rate of approximately 10% in aretrospectivecohortofmorethan50,000cases.2/3hadnocorrespondingfetalheartratechanges.CaseswithtachysystoleweremorelikelytohavelowApgarscoresoradmissiontothenursery
Cordprolapse(214-230)
0.3-2.3% Caesarean section is themost likely consequenceofcordprolapse,withaPNMR21.7%-47.9%.
Survivaloutsideofhospitalisrare;thelengthoftimebetweenprolapseanddeliverynegatively correlateswith adverse fetal and neonatal outcome, as theacute situation results in total asphyxia – leading tolackofbloodflowandcellularinsulttobrainstem
Placentalabruption(28,67,69,231-234)
0.08-1.4% MayresultintheneedforCS,perinatalmortality(upto65%),neonatalneurological injury,hysterectomy,maternalsepsis,andmaternalmortality(upto2%)
Uterinerupture(28,42,235-238)
0.1-1% Commonly occurs after obstructed labour.Maternalmortalityupto20%,perinatalmortalityinupto95%,peripartumhysterectomy

70
OPTIONSFORMEASURINGHYPOXIAANDITSSEQUELAE
Regardlessofidentificationoftheprecipitatingevent,hypoxia,atathresholdofboth
length and levelwhich appears to vary for individual fetuses,will eventually lead to
acidosis, and possibly ischaemia, altered neurological function, and ultimately poor
clinicaloutcome(260-262).Theacidosis in thispathwaycanbeobjectivelyquantified
usingvariousmeasurements,includingumbilicalcordlactate,pH,andbaseexcess.In
LMICsettings,theApgarscore(whenlow,althoughwithheterogeneouslydefinedcut
offs)maybeusedasaproxyforacidosis,givenitsassociatedwithclinicalasphyxiaand
poorperinataloutcomes(263,264).
PH
MeasurementofumbilicalcordpHatbirth isgenerallyconsideredthegoldstandard
formeasurementofperinatalacidosis(165,207,265-268),anda lowarterialcordpH
Pre-eclampsia/Eclampsia(28,54,58,239-259)
1.02%-11.3% Maternal (up to 18%) and perinatal death (up to81%),neonatalmorbidity (RDS,NEC, IVH, Sepsis)upto55%
Intrapartumhaemorrhage(49,90)
1.9%-4.3%
Fetalgrowthrestriction(198)
5-10% of allbirths
Responsibleforuptoathirdofallstillbirthsandthemostcommoncauseinsomesettingsofintrapartumasphyxia.

71
(defined often as less than 7.2-7.0) may be associated with adverse neonatal
outcomes(269).
BASEEXCESS(BE)
Baseexcess isa calculatedvalue, requiringmeasuredvaluesofpHandpCO2,and is
themmolofbaseneededtocorrectthemeasuredpHto7.4,assumingapCO2of40
mmHg(270).Baseexcessinthecontextofacidosisisexpressedasanegativenumber
(and isa termthat isused interchangeablywithbasedeficit),andgivesanobjective
measureofmetabolicacidosisinthefetus(271)giventhattheconsumptionofbuffers
occurswith theproductionof fetalacids followingmetabolic rather than respiratory
acidosis.Theconsumptionofbuffersandanabnormalnegativebaseexcesspotentially
occursbeforeanymeasureablechangeinpH(272).
APGARSCORE
TheApgar scorewas first proposed in 1953 by the anaesthesiologist Virginia Apgar,
andassessesfetalconditionwithascoreoutof10,derivedfrom5parameters;heart
rate, respiratory effort, reflex irritability,muscle tone, and colour(273). A lowApgar
score has also been found to correlate with suboptimal intrapartum care(274) and
with poor neonatal outcomes(275-277), and may be used as a proxy for a more
objective measurement for acidosis and birth asphyxia, particularly in low resource

72
settings(278). There are obvious limitations to using Apgar score as a measure of
acidosis,which are addressed indetail in thediscussion sectionof Chapter 5. These
include,butarenotlimitedto,thesubjectivenatureofthescore,thelackofsensitivity
of the score for adverse neurological outcome and the potential for poor intra-
observerreliabilityofthescore.However,itisamarkerforacidosisfrequentlyusedin
LMIC and thereforewarrants inclusion in the options formeasuring acidosis and its
sequelae.
LACTATE
Oneobjectivemeasurementthatthecliniciancanusetogaugetheimpactofhypoxia
andthedevelopment,ifany,ofacidaemia,istomeasurethelactatelevelofthefetus
and neonate(279). Fetal lactate is increasingly used to measure fetal acidosis and
predicting risk inboth the intrapartum setting (from the fetal scalp)(185) and in the
immediatepost-partumperiod(fromtheumbilicalcord)(280).Benefitstothisinclude
thatcomparedwithothermeasurementsofacidosis(e.g.pH),itispotentiallyeasierto
implement as a clinical tool, with a higher rate of success, due to the need for a
significantlysmallersampleofblood(11,185,281).Moreover,lactatecanbemeasured
onahandheldmeter,makingitpotentiallymoreuseableinawiderrangeofresourced
challenged settings, than other measures of acidosis, which require a blood-gas
analyser(282).IthasalsobeenshowntobecomparabletopHinmeasuringacidaemia
(192,283,284),andisthemeasurementofinterestinthisthesis.

73
MEASURINGUMBILICALLACTATE
Thebenefitofusinglactatetoassessacidosisisthatitcanbeperformedasapointof
care(POC)test;thatisonahandheldbedsidemachineasasimpletestrequiringvery
fewresources.UnlikemeasuringpH,whichgenerallyrequiresaminimumof30-90uL
ofblood(285),lactatecanbemeasuredonaPOCdeviceusingaslittleas0.5uL-15uLof
blood(286,287).
The lactate cut-off levels for fetalornewbornacidaemiameasuredonaPOCdevice
varybetweendevices(286,288).Thelactatelevelinthisthesisresearchwasmeasured
on a Roche Accutrend PlusTM© hand-held lactate meter (Rotkreuz, Switzerland),
whichmeasures lactate in a range of 0.8-22mmol/L in 60 seconds onwhole blood,
requiringasampleof15-50uL(Figures2.2aand2.2b).
Image2.2aand2.2b:AccutrendPlusTM©hand-heldlactatemeter

74
The device has been shown to be accurate in themeasurement of lactate from the
umbilical artery (as planned for our research study) at results between 1 and
20mmol/L.Ithasalsobeendemonstratedasaccurateinmeasuringfetalscalplactate,
further adding to our reasoning to use this machine in our research(289). The
Accutrend has a a coefficient of variation (CV) of 1.8-5%(287, 290) and ismeasured
using reflectancephotometry, after a lactateoxidase-mediated colorimetric reaction
occurs(291)(Figure2.4).
Figure2.4:AnexampleofthecolorimetricreactionusedbytheAccutrendmonitor,as
describedbyEmmert(292).
TIMINGOFLACTATESAMPLING
UsualpracticeatKalafonghospital is theclampingof theumbilical cordwithinone
minuteofbirth.This is important,giventhat lactatelevelshavebeendemonstrated
tochangewithdelaysinbothcordclampingandsampling.Followingvariablereports
of outcomes of delays in sampling, recommended practice included early cord

75
clamping (ideallywithinoneminute)andsamplingofthecordwithin20minutesto
benecessary[23],whereasothers findnodifference inbloodgasparameterswhen
cords are immediately clamped or delayed for greater than one to two
mintues[Tang, 2019 #632]. Dessolle and colleagues collected cord arterial lactate
samplesatdeliveryandataperiodof5-30minuteslaterandfoundacorresponding
linear rise in lactate levels in the second sample, with a rise of 0.062mmol/L per
minute(293).DePacoet alhavereportednosignificantdifferenceinumbilicalartery
pHlevelsinumbilicalcords(termand healthy)clampedimmediatelyafterbirthandin
thosewheretherewasadelayofuptotwo minutes[24].
Whiteet al describe an increase in lactate levels after 15minuteswhenbloodwas
bothstoredinasyringe,orleftinsitu(inthecord)(294).

76
METHODOFSAMPLING
Theequipmentnecessarytosample:Thenormalumbilicalcordcontainsoneveinand
two arteries, with a surrounding layer of Wharton’s Jelly, connective tissue and
amnion(295). Either artery can be sampled for the assessment of UA lactate. The
arteries are usually smaller and firmer (due to their muscular structure) than the
tortuousvein(Images2.3and2.4).
Image2.3:Asegmentofumbilicalcordwiththelargerveinclearlyvisible.

77
Image2.4:Acrosssectionofumbilicalcordshowing2arteriesand1vein.
Onceidentified,asmallcalibreneedlecanbeinsertedintoeitherartery,andasmall
amount of blood drawn with relative ease. The syringe used is often heparinised,
however as a long as the sample is measured shortly after it is drawn, a non-
heparinisedsyringecanbeused,makingtheprocesscheaper(296,297)(Image2.5).

78
Image2.5:A1mlnon-heparinisedsyringeand26-gaugeneedle.
CORDARTERIALLACTATELEVELS
Cord UA lactate is used in many settings to assess acidosis (or lack thereof) in the
immediatenewbornperiod.Cut-offvaluesusedincohortstudiesareoutlinedinTable
2.4.

79
Author Numberof included
samples
Lactateresults(mmol/L)
Chilindaetal(298) 391 Median 3.4 (IQ range 2.6-4.9), with a
cut-off of 5 for admission to the
nursery
Dessolleetal(293) 149 Mean 3.76 (SD + 1.53, range=1.1-9.8).
90thpercentile=5.72
Gjerris(192) 2554 Mean 4.63 (SD + 2.33),with amedian
of 4.30 and a cut-off for neonatal
acidosisof8
Labrecque(285) 52 Median3.7(range1.7-8.8)andacutoff
4.9 for the outcome of acidosis (as
definedbypH)
Linet(299) 200 Median 3.2, and a cut off 4.9 for the
outcomeofacidosis(asdefinedbypH)
Martin(300) 763 Mean3.71(SD+1.81),97thpercentile
oflactatewas7.54
Racinetetal(301) 867 Mean3.4(SD+0.05)
Tuuli(183) 4910 Theoptimalcutoffvalue forpredicting
neonatalmorbiditywas3.90

80
Westgren 4045 90th centile 3.21 with a sensitivity of
57% forneonatal death and specificity
of90%
Whiteetal(302) 21182 OptimalcutoffforHIE=5.68
Wibergetal(303) 13735 Optimalcutoff6.0 for5minuteApgar
<7
Table2.4:Cut-offvaluesforcohortsassessingacidosisusinglactatelevels.
FETALHEARTRATEMONITORING
Identification of the hypoxic fetus such that the consequence of acidosis can be
avoidediscentraltothisthesis.Inlabour,thesuspicionoffetalhypoxiaisoftenbased
onabnormalfetalheartratemonitoring.Inmanysettings,includingKalafonghospital
wherethemainstudyofthisthesiswasconducted,thisisdonewithacardiotocograph
(CTG),aformofelectronicfetalheartratemonitoring.
TheCTGisperformedwithtwotransducersplacedonthepregnantabdomen.Oneisa
pressure transducer that assesses contractions, such that the relationship between
fetal heart rate changes and contractions can be determined. The other transducer
measuresfetalheartrate.TheInternationalFederationofGynecologyandObstetrics
(FIGO) developed the first international consensus on fetal heart ratemonitoring in

81
1987, and thesewere still in place at the time of the clinical trial conducted in this
thesis(theywereupdatedin2015)(304).TheFIGOguidelinesforCTGcomponentsand
interpretationareoutlinedbelow(305). Itshouldbenotedthatsomecomponentsof
theCTGarenotdefinedbyFIGO,butaredefinedbytheRoyalCollegeofObstetricians
and Gynaecologists, and the research outlined in this thesis used these additional
definitions.

82
FEATURE DEFINITION
Baselinerate Baselinefetalheartrateisthemeanlevelofthefetalheartratewhenthis is stable, accelerations and decelerations being absent. It isdeterminedoveratimeperiodof5or10minandexpressedinbeatsperminute(bpm)
• Normal=110-160bpm• Tachycardia = not defined in FIGO, defined by RCOG as
>180bpm• Bradycardia<80bpm
Figure2.5CTGwiththenormalfetalbaselineHRlyingwithinthe110-160bpmareadefinedbythegreyline
Variability Oscillations of fetal heart rate around its mean level (long-termvariability). This is usually only quantitated by description of theamplitude of the oscillations around the baseline heart rate. Underphysiologicalconditionsthefetalbeat-to-beatintervalsareconstantlysubjecttosmallchanges.
• Normal=5-25bpm• Reduced<5bpmformorethan40minutes• Increased>25bpm
Figure 2.6: CTGs showing decreased, normal and increasedvariability

83
Accelerations Transient increase in heart rate of 15 bpm or more and lasting 15secondsormore
Figure2.7:CTGshowingaccelerationsabovethebaseline
Decelerations Transientepisodesof slowingof fetalheart ratebelow thebaselinelevel of more than 15 bpm and lasting 10 seconds or more.DecelerationsarenotdefinedinFIGO,butaredefinedbyRCOG
• Earlydecelerations=Uniform, repetitive, periodic slowingofFHRwithonsetearlyinthecontractionandreturntobaselineattheendofthecontraction
Figure2.8:CTGshowingearlydecelerations
• Late decelerations = Uniform, repetitive, periodic slowing ofFHRwithonsetmidtoendofthecontractionandnadirmorethan20secondsafterthepeakofthecontractionandendingafter the contraction. In the presence of a non-accelerativetracewithbaselinevariability less than5bpm, thedefinitionwouldincludedecelerationslessthan15bpm

84
Figure2.9:CTGshowinglatedecelerations
• Variable decelerations = Variable, intermittent periodicslowing of FHR with rapid onset and recovery. Timerelationshipswithcontractioncyclearevariableandtheymayoccurinisolation.
Figure2.10:CTGshowingvariabledecelerations
• Prolongeddecelerations=anabruptdecreaseinFHRtolevelsbelow the baseline that lasts at least 60–90 seconds. Thesedecelerationsbecomepathologicaliftheycross2contractions(i.e.greaterthan3minutes)

85
Figure2.11:CTGshowingprolongeddecelerations
Table 2.5: Components of the CTG. Adapted from Ayres-de-Campos and Bernades,
2010(305),andtheKEMHAdvancedFetalAssessmentprogram.
Oncethecomponentsof theCTGareassessed,onemustdetermine ifabnormalities
seenaresuspiciousorpathological,anddecideontheappropriateintervention.Thisis
wheremanydisagreementsintheliteratureandbetweencliniciansarise(306).
THECTGANDACIDOSIS:AREVIEW
Theultimateaimoffetalmonitoringinlabouristopreventacidosis,whichisthebasis
of the abnormal sequelae that follow hypoxia. The occurrence of hypoxia itself, as
outlinedpreviously,willnotresultinclinicalconsequenceandsooneneedstobeable
to intervene such that the potential complications of the intervention are balanced
againsttherisksofadverseneonataloutcomewithprogressivehypoxia. Inthestudy
relatedtothisthesis, intrapartumassessmentofacidosisthroughscalpsamplingwas
not feasible, so the focusof this reviewwasonacidosisdiagnosed fromasampleof

86
blood from the umbilical cord after birth. The concept being that taking a
measurementof acidosis on all births functions as an audit of intrapartumcare and
allows clinicians receive real-time quality of care feedback on their practice,
particularly their interpretation of and response to the fetal heart rate changes in
labour(307). Thus, in order to interrogate the interaction between fetal heart rate
monitoring and consequent acidosis, a literature review was undertaken using the
following search (((((cardiotocography) OR cardiotocogram(MeSH Terms)) OR fetal
monitoring(MeSH Terms)))) AND ((acidosis) OR (acidosis(MeSH Terms)) OR (fetal
distress(MeSH Terms)OR (neonatal outcome)OR (neonatal acidosis))). 1021 articles
were identified from2000onwards.After title and abstract review, relevant articles
areexploredbelow.
WhiletheCTGremainsstandardofcareinlabourformanywomenaroundtheworld,
there is a plethora of evidence, including randomised evidence, that, while its
specificityisat least90%(308), ithasapoorsensitivityforacidosis.Thereareseveral
issuesthatfollowonfromthis.
• SensitivityoftheCTGforpredictingacidosisandadversefetaloutcomemaybe
aslowas15%(309-313).
• Therateofintervention(oftencaesareansection)withoutpotentialbenefitto
mother or fetus is high(271, 314-319), although it is clearly sometimes both
necessaryandhelpful(320).

87
• ThePPVof theCTG foracidosis (evenwhenmeasuredusingcomputerbased
algorithms) is reportedbetween27.4%and50%(314,321-324). In fact, in the
large randomised INFANT trial of more than 47,000 cases, there was no
difference in the rate of acidosis when the interpretation of the CTG by
clinicians was aided by the addition of computer based decision support
software(325), supporting the concept that the poor sensitivity of the CTG is
notonlyaconsequenceofvariationsinclinicalinterpretationbutisalsoaresult
ofvaryingfetalcapacitytocopewithhypoxicstress.
• ThereislittletonoevidencethatinterveninginabnormalCTGwithcaesarean
delivery reduces the rate of acidosis(326, 327), although in many situations,
women more often than not are delivered by caesarean section when fetal
compromiseissuspected(328).
RespondingtotheCTGduringlabourrequiresthecliniciantoconsidereachaspectof
the heart rate (as outlined in Table 2.5) and diagnose the fetal heart rate as being
somewhereonthespectrumbetweenreassuringandpotentiallypathological.Various
interpretationtoolsforCTGsexist,howeverinterandintra-observerreliabilityofthose
tools is often poor, resulting inmarkedly differing sensitivity for predicting acidosis,
whichmakesthetaskforcliniciansdifficult(329-334).Cliniciansarefrequently,butnot
universally, able to agreewhen CTG traces are reassuring or normal, but frequently
unabletoagreewhenCTGtracesareconcerningorominous(317,335).Inareviewof
inter-observervariability,clinicianswereunabletoagreeonwhichofthenearly50%
ofsuspiciousCTGtracingswouldbeindicatedforemergencydelivery,ortopredictin

88
which2%ofcasesacidosiswasevidentondelivery(336).Kunduetaldemonstratethe
challengesofCTGinterpretationverysuccinctlywiththeirretrospectivereviewof300
cases.Thecasesweregivento7variablyexperiencedclinicianswithboththeobjective
acidosisresults(UAgasanalysis)andthedeliveryoutcomes(mode,Apgarscores,etc.)
blinded.ClinicianswereverypooratpredictingthepHbasedontheCTGappearances,
and therewasmarked inter-observer variability of CTG interpretation(337). Overall,
clinicianshavedifferentthresholdsforinterventionfortheconceptofsuspectedfetal
distress,whichmakestheinterpretationoftheCTGachallengingclinicalissue.
The individual components of the CTG (Table 2.5) are variably related to neonatal
acidosisandoutcome.Cliniciansareoftenreassuredbythepresenceofnormal fetal
heartratevariabilityandfetalheartrateaccelerations,whichlikelyexplainswhymost
can agree when CTGs are considered normal. The presence of normal variability is
associatedwithahigh likelihood (at least>85%)ofanormalpH(338,339), although
conversely in their large retrospective cohort Milson et al found a sensitivity of
reduced fetal heart rate variability for the outcome of asphyxia of only 19%(340).
Thereissomeevidencethataccelerationsinlabourareunlikelytobeassociatedwith
acidosis,althoughthereisadescribedfalsenegativerateofatleast6%(341).
TheCTGchangesthatconcernaclinicianneedtobetakenwithinthecontextof the
entireCTGandclinical scenario(342);achangesuchasprolongedbradycardia is less
likely to result inacidosisandadverseneonataloutcome if theperiodpreceding the

89
bradycardiawassuggestiveofanormalfetalphysiologicalstate(343-345).Herein lies
the challenge – even ominous CTG patterns are not likely to result in an adverse
outcome.Chuangetalshowedsensitivityforadverseneonataloutcomeforprolonged
bradycardia of only 29%(346). The frequency of occurrence of decelerations or the
lengthofaprolongedbradycardiaaremorelikelythannormalCTGstobeassociated
withneonatalacidosis,butmanycaseswillhaveneitheracidosisnoradverseclinical
outcome(347). Even when the fetus that has both decreased variability and late
decelerations,bothconsideredominouspatterns,WilliamsandGalemeaufoundarate
ofacidosisinthisscenarioof44%(339).
Even a common pregnancy occurrence such as a nuchal cord, which the clinician is
unabletomodify,canresult inCTGabnormalities,particularlyvariabledecelerations.
Again,withanotherwisenormalCTG,theseareunlikelytobeassociatedwithadverse
outcomes,howeverthecontinuoustransienthypoxiathatmaybeassociatedwiththis
clinicalscenariomayleavethefetuswithlessreservetocopewithother insults(346,
348,349).ThefrequencyordurationofabnormalCTGpatternsmaybemorelikelyto
beassociatedwithadverseneonataloutcomes(350),butthetimeofabnormalities is
clearlyacontinuum,andagaincliniciansareinthedifficultpositionofdecidingwhen
tointervene.
There is no doubt thatwomenwith adverse fetal andneonatal outcomeswill often
haveabnormalCTGs,howeverthereverseisoftennottrue(351,352).Thefetushasan

90
extraordinary capacity to cope with hypoxia and acidosis before there are clinical
manifestations(317),andasfewasaquarterofthemostpathologicaltraceswillhave
consequent neonatal encephalopathy(353). Cahill et al undertook a retrospective
studyof951womenwith“terminaldecelerations” (prolongeddecelerationswithout
recoveryofatleast120seconds)andfoundthatmorethan98%didnothaveacidosis
onUAsampling(354).Furthermore,notallcasesofneonatalencephalopathywillhave
a pre-delivery pathological CTG(355), making interpretation of CTGs to prevent
acidosisallthemoredifficult.Onreviewingcaseswithacidosisdetectedonumbilical
cord sampling, Olofsson et al found that one third of CTGs showed both normal
baselineandnormalvariability(329).
Decelerationsareofteninterpretedwithconcernbyclinicians,howeverthepresence
of decelerations may be just as common in fetuses without acidosis as in those
with(321, 356, 357). There is a clear relationship between the length of time of
decelerations and consequent acidosis, however this is a continuum that requires
clinician discretion to choose themoment for intervention(306, 358-362).Moreover
there remain issueswith the interpretationofdecelerations; the conceptof atypical
features of decelerations being associatedwithworse outcomes is not borne out in
large cohort studies(363). Even variability, which is often regarded as the most
important feature of the CTG(340, 364), has a PPV for acidaemia of, at most, 17-
67%(365-369).

91
FetaldistressisacommonindicationforcaesareansectioninbothhighandLMIC(370),
including South Africa(371, 372). The diagnosis however (often based on fetal heart
ratetracing)isnotnecessarilyborneoutintermsofadverseneonataloutcomes(319,
373, 374), with no apparent association between CS for fetal distress in one South
African study and adverse perinatal outcome(375). Indeed, a Cochrane Systematic
review comparing operative intervention with conservative management for fetal
distress includes only one RCT from 1959, with no difference in perinatal
mortality(376). Despite the absence of contemporary RCTs, there is no lack of non-
randomised evidence regarding the limited role of the CTG to improve perinatal
outcomes.
InLMIC,therearesimilardatatothosedescribedaboveonthepoorpredictabilityof
CTG. In one prospective Indian study, while the CTG abnormality correlated with
adverse outcomes, the correlation was not impacted by decision to delivery time,
further cementing the poor PPV of CTG interpretation(377). Similar findings are
replicatedinmanyLMIC(378).
• ANigerianreviewof300casesofsuspectedfetaldistressshowedthatnotonly
was the time from suspicion to caesarean section (the planned intervention)
greater than 2 hours in the majority of women, less than a quarter had
diagnosedbirthasphyxia(379).

92
• Of a 146 women having a CS for suspected fetal distress in one Indian
prospectivecohort,only2%of caseshad that suspicionborneout inacidosis
andsubsequentpooroutcome(380),and inanothercase-control study,more
thanathirdofcaseswithsuspectedfetaldistressandUAprovenacidosishada
normal clinical outcome(381). That said, the aim of intervening for hypoxia
beforeacidosisoccursisimportant(382).
• In one study in Pakistan for a trace that was defined as suspicious or
pathological(FIGO),thePPVforhypoxiawas18%andacidosis26%,inanother
similarretrospectivecohort,thesensitivityofCTGtopredictacidosisbasedon
BEwas15%(383). This canbe improvedwithpathologicalonly traces to50%
(228,384).
Asinhighincomecountrybasedstudies,thepresenceofabnormalitiesonCTGismore
likelytobeassociatedwithabnormalneonataloutcomes(367),andmoreover,onecan
findevidence inbothhigh incomeandLMIC for the introductionofCTG resulting in
improvedperinataloutcomes,includingimprovedmortality,howeverthismaybeasa
resultof trainingandawarenessaroundhypoxiaratherthanthe introductionofCTG
itself(109,385,386).
FetaldistressisfrequentlycitedintheliteratureexploringperinatalmortalityinLMIC.
Itisclearlyacomponentofintrapartumcarewhereattentioncanbefocused,however
increasingcaesareansectionratesinLMICinresponsetosuspectedfetalcompromise
doesnotnecessarilyhaveany impactonPNMR(387).Moyeretal reportan8%fetal

93
distressrateinnearly5000deliveries,withanoverallperinatalmortalityof10%(388).
While the crossover between these twodiagnoses is not clear in this study,what is
clearisthatinterventionstoaddressfetaldistressareofvalueinLMIC,acceptingthe
obviouslimitationsoffetalheartratemonitoringoutlinedabove.Therearetwomajor
issues with this concept. Firstly, the availability of CTG in LMIC is often scarce to
absent(389), however it isworthnoting thatmonitoringwithout aCTG, and instead
withahandhelddevice,maybeaseffective(orineffective)ascontinuousmonitoring,
particularlyinLMIC(101,390,391).Secondly,eveninthescenariowherefetaldistress
issuspectedbasedonheartratetracing,thecapacityto intervene(forexamplewith
instrumentaldeliveryorcaesareansection)islimitedbytheavailabilityofresourcesto
doso,and therefore thepotentialbenefitsof interventionarenotnecessarilyborne
outinneonataloutcomes(392).Thatsaid,thepoorperformancecharacteristicsofthe
CTGmeansthatprolongeddecisiontodeliveryintervalsmaynotnecessarilyresult in
adverseneonataloutcome(393).
THENEONATEWITHACIDOSIS
Acidosis,asoutlinedearlierinthischapter,isdefinedvariablyinpractice,whichresults
inheterogeneousreportingofratesofacidosis.WhileoftendeterminedusingpH,the
cut-off for this is reported ranging between7.0 and7.2.We therefore rely on large
cohortstudiestobestestimatetherateofacidosis,asdeterminedwithauthordefined
cutoffs,andacceptingthelimitationsofreporting.Whiteetalintheircohortof19646
births,reportedarateofacidosis(pH<7.0)oflessthanonepercent(394),withsimilar

94
findingsrepeatedinotherlargecohortstudies(395-397).Itisclearthatnotallacidotic
neonates have adverse clinical sequelae, and equally not all unwell neonates are
acidotic.Itshouldbenotedthatneonatalacidosisinthiscontextisconsideredacidosis
diagnosedimmediatelyafterbirthfromtheumbilicalcord,andis largelyreflectiveof
intrapartumevents.Itisimportantinintroducingatooltoobjectivelymeasureacidosis
atthetimeofbirththatoneconsiderstheadverseoutcomesofacidosisaswellashow
tomanagethe“well”newbornwithacidosis.
NEONATALACIDOSISANDADVERSEOUTCOMES
Worsening levels of acidosis are associated with increasing likelihood of neonatal
resuscitation, low Apgar scores, admission to the neonatal nursery, and hypoxic
ischaemic encephalopathy(268, 398). Acidosis can result in seizures (Williams and
Singh found a sensitivity of 73% for acidosis at birth (defined as pH<7.0) for the
outcome of neonatal seizures(399)), and long term neurological complications
includingcerebralpalsy(2).
Itisclearthattheclinicalpictureguidesthemanagementofthenewborn,ratherthan
the presence or absence of acidosis. While babies born with low Apgar scores are
often acidaemic(400), there are a host of reasons for why neonates may have low
Apgarscores.Intheircohortofnearly28,000patients,Locatellietalfoundthatonlya
thirdofneonateswith lowApgarscoresalsohadumbilicalacidaemia(401).Likewise,

95
Lavrijsenet al found in their case control study that seizuresonly occurred in up to
20% of neonateswith umbilical acidaemia at birth, with no clear difference in long
termoutcomesbetweenacidaemicandnon-acidaemiccases(402).
THEWELLNEWBORNWITHACIDOSIS
The presence of acidosis at the timeof birthwithout apparent clinical consequence
presentsachallengeforclinicians.Whileitmaybepossibletodismissthisscenario,we
couldequallyconsiderthatwhenacidosisisidentifiedonumbilicalcordsamplingand
the newborn is otherwisewell, a neonatal nearmiss has occurred. That is, that the
event that leadtoacidosishasnot resulted inadverseoutcomebutcouldhave,and
reviewof thecasesmay revealanareaofpotential improvement to reduceacidosis
ratesanditspotentialmorbidandmortalconsequences.
AsdescribedbyBonnaerensetal,theconceptofneonatalnearmissisnotwidelyused
in audits of intrapartum care, but has the potential to value-add to perinatal care,
particularlywhencasesofnearmissare frequently inwomenandneonateswithno
identifiable pre-labour risk factors(403). In undertaking universal screening for
acidosis, Bonnaerens and colleagues found amore than doubling in the number of
cases where audit was warranted and improvement of perinatal care was
possible(404).Thiswasfurtherconfirmedwhentheinitialstudygroupwasexpanded
across threeyears(405). Jonssonandcolleaguescollecteddataonmore than28,000

96
deliveries,withametabolicacidosisrateof0.68%.Whilemostneonatesdidwellinthe
postdeliveryperiod,theyestimated,basedonauditofacidosiscases,thattheacidosis
couldhavebeenavoidedinnearlyhalfofallcases(406).Itisimportanttoconsiderthat
metabolicacidosiscanbeboththecauseandconsequenceofadverseintrapartumand
neonataloutcomes.Ifallacidoticcaseshaveanidentifiablepotentialprecipitant,then
itstandstoreasonthatreviewofthesecasesmaystimulateachangeinpractice,even
where the ultimate outcome for the neonate is positive (407). The identification of
acidosisatbirth,whileuncommon,maybeasignofadditionalriskofneonataladverse
events, including respiratory distress syndrome and NICU admission, and universal
testingand reviewof casesmay stimulatealternatemanagementof suchcases(268,
408).
Inthecaseofthewellnewbornwithacidosis,isthereapotentiallong-termimpactof
the acidosis? Dani et al studied 53 infants with an unexpected cord arterial pH
between 7.0 and 7.1, and more than half were asymptomatic with no short-term
consequences (409).However, there is someevidence to suggest that the long-term
developmental outcomes, although clinically minor, of these neonates may be
differenttotheirequallyclinicallywellbuteucapniccounterpartsatvariousstagesof
childhood(159, 410). Themeasurement of acidosis (or lack thereof) on all deliveries
therefore provides the clinician with the opportunity to review the “near miss”
intrapartum events, with the aim of reducing the rates of acidosis and potentially
impactinglongtermoutcomes.

97
QUALITYOFCAREAUDITS
DEFININGQUALITYOFCAREANDQUALITYOFCAREAUDIT
QualityofCare(QoC)isdifficulttodefineasitisoftencontextual(411,412),howeverit
generallyencompassescomponentscontributingtomorethanonelevelofcare(413),
and is care far beyond the basic provision of essential and emergency medicine.
Tuncalp et al define QoC in maternal and newborn health as that reflecting the
“physical infrastructure, supplies, management, and human resources with the
knowledge,skillsandcapacitytodealwithpregnancyandchildbirth”(5).Moreover,it
is consistently repeated in recentmaternal andnewborn literature thatQoCaround
the time of childbirth has the capacity to save millions of women and newborn
lives(414-419).
Audit is defined as “a systematic review or assessment”(163), a process integral to
healthserviceprovision,andhasseveralroles:
• It allows comparisons of care within a system against an agreed
standardofcare(420).
• Itmaybeusedasanassessmentofspecificandobjectivemarkersofa
desiredoutcome (e.g.perinatalmortality as a functionof intrapartum
care)(421).

98
• It canbe amotivator for adequatedata collection,which is critical to
theusefulnessofaudit(422).
Thus, clinical audit is critical to the identification of potential problems and focused
facility auditswithin awider system can identify contextually specific health service
deficienciesandprovidetheimpetusforchange(411,422-425).
Furthermore,havingauditthatdetectsproblemsinthestepstoaparticularoutcome
(quality of care audit) is more likely to be sensitive for identifying areas that need
improvement(125, 426-428). Indeed, rather than assessing an endpoint as the sole
goal,auditcan(andonewouldargueshould)beextendedtoqualityofcareaudit in
whichmarkersoftheprocessthatleadtoanendpointcanreflecttheappropriateness
and quality of the care given(429). Merali et al undertook a systematic review of
identified avoidable factors in maternal and perinatal audit in LMIC. In addition to
identifying42avoidablefactorsindeathaudits,theyestimatednearlyathirdofdeaths
werespecificallyrelatedto“substandardhealthworkerpractice”(430).Thisconceptof
specificcriteriabasedauditallowscliniciansandresearcherstohighlightdefinedgaps
wherebyresourcescanbetargeted(431).Tothatend,thestepstoimprovingqualityof
care, includingauditasapartofthatprocess,havebecomeaglobalfocusinwomen
andnewbornhealth(417).

99
QUALITYOFCAREAUDITINMATERNALANDNEWBORNHEALTH
Comprehensive data registries in LMIC are critical in order to facilitate audit that
identifies specific clinical and systempractises,whichmustbeaddressed inorder to
affectanychangeonPNMR(432-436).ThisisofparticularimportanceinLMIC,where
datacapturearoundperinatalmortalityisfrequentlypoor(437,438),andthemajority
of avoidable perinatal mortality is attributed to the poor quality or absence of
intrapartumcare(430,439).There is someevidence thatauditalone (asan inherent
intervention)mayimproveclinicaloutcomesandmortalityrateswithameta-analysis
ofsevennonRCTtrialsshowingthattheprocessofintroducingauditwithinaspecific
systemreducesmortalitybyupto30%(440).Audithasbeenshowntoattheveryleast
improveclinicalpractice,andvariablytoimprovemortalityoutcomes,althoughthere
isaclearlackofrandomiseddataonaudit,whichisinandofitselfaninterventionthat
wouldwarrantaRCT(441,442).
At itsmostbasic level,simpledatacollectionover6years inruralNigeriaresultedin
improvedmortality statistics(242) and the registrationofwomen in ruralGuatemala
onapregnancydatabase(communitylevelaudit)resultedinareducinginallmaternal
andperinatalmortality statistics, presumably secondarily to theprocessof engaging
pregnantwomenandincreasingtheirfacility-basedbirth(51).Pragmaticaddressingof
systemproblemsidentifiedbyaudithasbeenshowntoimprovemortalityinaKenyan
study(413),althoughdesignflaws(withonlya1/3ofperinataldeathsincluded)make
theevidencedifficulttointerpret.MovingfromsimpledatacollectioninaunitinFijito

100
standardisedperinatalmortalityauditresulted identificationofhealthsystemfactors
that could be addressed to reduce preventable deaths(443). Similar findings were
showninaTanzanianstudy,whereashifttocriteriabasedauditresultedinimproved
recognitionandmanagementofsuspectedfetaldistress(109).Furthermore,thelarge
multi-countryMaternalNewbornHealthRegistry studyclearly showscomprehensive
datacollectionfeedsandauditprocessthatclearlyresults in improvedmaternaland
newbornoutcomes(434).
Theimpactofauditonresultingchangesinpracticehasthepotentialtobesignificant,
aswasthecaseintheHlabisaHealthDistrictofKwaZulu/Natal,SouthAfricain1991-
1995. Rigorous classification of avoidable perinatal deaths and audit resulting in
changestohealthservicedeliverysawareductioninperinataldeathfrom18%to0%
overafouryearperiod(444).Similarly,theuseofthePPIPsysteminanEasternCape
hospitalinSouthAfricawasassociatedwithareductioninintrapartumhypoxicrelated
deaths, attributed to both the awareness generated by audit and the addressing of
specificsystemissuesthatauditidentified(148).Theintroductionofacomprehensive
training program in audit andperinatal death classification inMoldova resulted in a
reduction inperinatalmortalityandan improvement inqualityof care(445). Further
examples includeabeforeandafterstudyexaminingthe introductionofacombined
emergency obstetric care andmonitoring and evaluation program (the Advances in
LabourandRiskManagementInternationalProgram)inKenya,whichresultedinclear
improvementsinbothmaternalandperinataloutcomes(446).

101
Itisclearthatasystemthatisbothsupportiveoftherequirementsforauditandhas
the capacity to implement changes once issues are identified is central to improved
outcomes.AnauditofvillagebasedregistriesinruralIndonesiashowedastillbirthrate
fourtimesthereportedratefromthenationalvitalstatisticsprogram(447)andsitesin
Pakistan in the Maternal Newborn Health Registry study had worsening mortality
statisticswiththeintroductionofaudit,bothapparentlysecondarytopoorqualityof
care(448).Thereismoretotheprocessofauditthansimpleregistrationandpresumed
inherent clinical response to adverse outcomes, including having the resources to
executeanyclinicalresponse.Theremustalsobeinternalinfrastructuretorunaudit,
clinicalandmanagerialstaffsupport,afeelingofresponsibilityandownershipamongst
thestaff,andtheprocessofauditmustnotbeseenaspunitive(449,450).
QoC in low resource settings is likely to contribute to poor perinatal outcomes and
QoC audit in these settings repeatedly identifies poor care around the time of
childbirthasapreventablefactorinsignificantnumbersofperinataldeaths(451).
However,itisnotentirelyclearthatQoCauditbyitselfimproveslongtermoutcomes;
is it audit alone or is there a deeper process thatmust be undertaken for it to be
effective? If thisprocess is feedback (passiveoractive),which is identifiedascritical
foraudit,doesit infacthaveasustainablelongtermeffectonmortality?(423)Other
quality improvement programs aimed at improvement care around the time of
childbirthhavebeen shown to reduceperinatal andmaternal deaths(452).However

102
the inherent flaws in theseprogramsare the lackofeffectivecontroland the issues
with reproducibility. PPIP is frequently cited in the literature as the foundation on
which improvement in perinatal care and perinatal mortality has been made in
individual units and larger districts(131, 135, 453). Belizanet al identified fourmain
drivers in the successful implementation of PPIP; drivers and teams, outreach and
supervision,perinatalreviewmeetings,andcommunicationandnetworking(454).
QUALITYOFCAREAUDITANDNEARMISSCASES
Withsubstandard intrapartumand immediatenewborncarebeing linkedtonearlya
million neonatal deaths annually(4), it is evident that there is a significant group of
survivingneonatesthatcomprisethenearmissgroup.Theconceptofusingnearmiss
cases to assess quality of care is well described in maternal and newborn health
literature(427). Defining and identifying neonatal near miss allows identification of
deficiencies inobstetricandneonatal care toguide improvement in clinicalpractice.
Moreover,thecliniciancompliancewiththismaybe improvedbythe“positiveentry
point(455)” to the process; that is the survival of the babymay encourage in depth
analysis in thequalityofcareauditprocesswhentheoutcomeofanyconcernswith
careisalreadyknowntobepositive.Thetermneonatalnearmissisbeingincreasingly
used in the literature in an attempt to identify those babies who would have
potentially died from a severe obstetric complication and thus may represent a
consequenceofdeficienciesinperinatalcare(456-458).

103
MATERNALHIVINFECTION
MaternalHIVinfectionaffectsmorethan17millionwomenovertheageof15around
theworld,withtheburdenoftheseconcentratedinlowandmiddle-incomecountries.
There is a clear crossover between women with HIV and women with adverse
pregnancy outcomes, from both HIV related and non-related causes(459). It was
important to consider the role of maternal HIV infection in any study investigating
labouroutcomes,giventhatinSouthAfrica30%ofthepopulationisinfectedwithHIV
andmorethan600,000birthsoccurtowomenwithHIVeveryyear(460).MaternalHIV
infectioninpregnancy,particularlyinwomennotreceivingantiretroviralmedication,is
associatedwithadverseperinataloutcomes,includingpretermbirthandstillbirth(461).
ThereisevidenceinSouthAfricathatwhilepregnancyisoftenprotectiveagainstnew
acquisitionofHIV, youngerwomenwithhigherparitymaybeatgreater riskofnew
infections in pregnancy(462). Thereforewe need evidence of the potential effect of
HIVonintrapartumcare.This isparticularly importantgivensomeretrospectivedata
fromthesameregionasthelocationofthiscurrentresearchsuggestingwomenwith
HIVinfectionhaveahigherrateofbirthasphyxiarelatedperinatalmortalitythantheir
HIV negative counterparts(463). The small numbers and retrospective nature of the
datameansone should interpret thiswith caution, however the concept formedan
importantconsiderationinourresearch.

104
CONCLUSION
Perinatalmortalityinlowandmiddleincomecountriesisacomplexandmultifaceted
entity. Intrapartum hypoxia contributes significantly to perinatal mortality in these
settings.Inordertounderstandthis,thephysiologyofthefetus,theunderlyingcauses
and clinical consequences of hypoxia and the capacity to measure and respond to
hypoxia must be considered. The thesis interrogates these issues and attempts to
addressthemwithaspecificfocusonSouthAfrica.

105
REFERENCES
1. Allanson ER, Muller M, Pattinson RC. Causes of perinatal mortality andassociatedmaternalcomplicationsinaSouthAfricanprovince:challengesinpredictingpooroutcomes.BMCPregnancyChildbirth.2015;15(1):37.2. Rei M, Ayres-de-Campos D, Bernardes J. Neurological damage arising fromintrapartumhypoxia/acidosis.BestPractResClinObstetGynaecol.2016;30:79-86.3. BuchmannEJ, StonesW,ThomasN.Preventingdeaths fromcomplicationsoflabouranddelivery.BestPractResClinObstetGynaecol.2016;36:103-15.4. Bhutta ZA, Das JK, Bahl R, Lawn JE, Salam RA, Paul VK, et al. Can availableinterventionsendpreventabledeathsinmothers,newbornbabies,andstillbirths,andatwhatcost?Lancet.2014;384(9940):347-70.5. Tunçalp Ӧ,WereW,MacLennan C, Oladapo O, Gülmezoglu A, Bahl R, et al.Quality of care for pregnant women and newborns—the WHO vision. BJOG.2015;122(8):1045-9.6. BuchmannE, PattinsonR,NyathikaziN. Intrapartum-relatedbirth asphyxia inSouth Africa lessons From the first national perinatal care survey. S Afr Med J.2002;92(11):897-901.7. Low JA, Pickersgill H, Killen H, Derrick EJ. The prediction and prevention ofintrapartumfetalasphyxiaintermpregnancies.AmJObstetGynecol.2001;184(4):724-30.8. PinasA,ChandraharanE.Continuouscardiotocographyduringlabour:Analysis,classificationandmanagement.BestPractResClinObstetGynaecol.2016;30:33-47.9. Prior T, Kumar S. Expert review--identification of intra-partum fetalcompromise.EurJObstetGynecolReprodBiol.2015;190:1-6.10. Jorgensen JS, Weber T. Fetal scalp blood sampling in labor--a review. ActaObstetGynecolScand.2014;93(6):548-55.11. EastCE,LeaderLR,SheehanP,HenshallNE,ColditzPB,LauR.Intrapartumfetalscalp lactate sampling for fetal assessment in thepresenceof anon-reassuring fetalheartratetrace.CochraneDatabaseSystRev.2015(5):Cd006174.12. LassiZS,MiddletonPF,BhuttaZA,CrowtherC.Strategiesforimprovinghealthcareseekingformaternalandnewbornillnessesinlow-andmiddle-incomecountries:asystematicreviewandmeta-analysis.GlobHealthAction.2016;9(1):31408.13. UNInter-agencyGroupforChildMortalityEstimation(IGME).Levelsandtrendsinchildmortality:Report2013.NewYork:UNICEF;2013.14. Akseer N, Lawn JE, KeenanW, Konstantopoulos A, Cooper P, Ismail Z, et al.Endingpreventablenewborndeaths inageneration. IntJGynaecolObstet.2015;131Suppl1:S43-8.15. Froen JF, Friberg IK, Lawn JE, Bhutta ZA, Pattinson RC, Allanson ER, et al.Stillbirths:progressandunfinishedbusiness.Lancet.2016;387(10018):574-86.16. Blencowe H, Cousens S, Jassir FB, Say L, Chou D,Mathers C, et al. National,regional,andworldwideestimatesofstillbirthratesin2015,withtrendsfrom2000:asystematicanalysis.LancetGlobHealth.2016;4(2):e98-e108.17. Alkema L, Chou D, Hogan D, Zhang S, Moller AB, Gemmill A, et al. Global,regional,andnationallevelsandtrendsinmaternalmortalitybetween1990and2015,

106
with scenario-based projections to 2030: a systematic analysis by the UNMaternalMortalityEstimationInter-AgencyGroup.Lancet.2016;387(10017):462-74.18. RoosN, vonXylander SR.Whydomaternal andnewborndeaths continue tooccur?BestPractResClinObstetGynaecol.2016;36:30-44.19. Saleem S, McClure EM, Goudar SS, Patel A, Esamai F, Garces A, et al. Aprospective studyofmaternal, fetal andneonataldeaths in low-andmiddle-incomecountries.BullWorldHealthOrgan.2014;92(8):605-12.20. WorldHealthOrganization.Neonatalandperinatalmortality:country,regionalandglobalestimates.2006.21. AllansonE,TunçalpÖ,GardosiJ,PattinsonR,FrancisA,VogelJ,etal.TheWHOapplicationof ICD‐10todeathsduringtheperinatalperiod(ICD‐PM):resultsfrompilotdatabasetestinginSouthAfricaandUnitedKingdom.BJOG.2016;123(12):2019-28.22. World Health Organization. ICD-10: international statistical classification ofdiseasesandrelatedhealthproblems:tenthrevision.2004.23. PattinsonR,Rhoda,N.Savingbabies2012-2013:NinthreportonperinatalcareinSouthAfrica.TshepesaPress,Pretoria,SouthAfrica;2014.24. Australian Institute of Health andWelfare. National PerinatalMortality DataCollection (NPMDC) 2019 [updated 16/04/2019 v9.0. Available from:https://www.aihw.gov.au/about-our-data/our-data-collections/national-perinatal-mortality-data-collection-npmdc.25. Blencowe H, Calvert Ph DC, Lawn JE, Cousens S, Campbell OM. Measuringmaternal,foetalandneonatalmortality:Challengesandsolutions.BestPractResClinObstetGynaecol.2016;36:14-29.26. GordonA, Raynes-GreenowC,McGeechanK,Morris J, JefferyH. Risk factorsfor antepartum stillbirth and the influence of maternal age in New South WalesAustralia:apopulationbasedstudy.BMCPregnancyChildbirth.2013;13(1):12.27. Allanson ER, Muller M, Pattinson RC. Causes of perinatal mortality andassociatedmaternalcomplicationsinaSouthAfricanprovince:challengesinpredictingpooroutcomes.BMCPregnancyChildbirth.2015;15:37.28. Vogel J, Souza J, Mori R, Morisaki N, Lumbiganon P, Laopaiboon M, et al.Maternal complications and perinatal mortality: findings of the World HealthOrganization Multicountry Survey on Maternal and Newborn Health. BJOG.2014;121:76-88.29. Ariff S, LeeAC, Lawn J, Bhutta ZA.Global Burden, Epidemiologic Trends, andPrevention of Intrapartum-Related Deaths in Low-Resource Settings. Clin Perinatol.2016;43(3):593-608.30. Kamath-RayneBD,Griffin JB,MoranK, JonesB,DownsA,McClureEM,etal.ResuscitationandObstetricalCaretoReduceIntrapartum-RelatedNeonatalDeaths:AMANDATEStudy.MaternChildHealthJ.2015;19(8):1853-63.31. AkterT,DawsonA,SibbrittD.Whatimpactdoesantenatalandpostnatalcarehave on neonatal deaths in low-and lower-middle-income countries? Evidence fromBangladesh.HealthCareWomenInt.2017;38(8):848-60.32. Ntambue AM,Malonga FK, Dramaix-WilmetM, Ngatu RN, Donnen P. Betterthan nothing?maternal, newborn, and child health services and perinatalmortality,Lubumbashi, democratic republic of the Congo: a cohort study. BMC PregnancyChildbirth.2016;16:89.

107
33. Chaudhury S, Arlington L, Brenan S, Kairuki AK,Meda AR, Isangula KG, et al.Cost analysisof large-scale implementationof the 'HelpingBabiesBreathe'newbornresuscitation-trainingprograminTanzania.BMCHealthServRes.2016;16(1):681.34. YegoF,D'EsteC,BylesJ,NyongesaP,WilliamsJS.Acase-controlstudyofriskfactors for fetal and early neonatal deaths in a tertiary hospital in Kenya. BMCPregnancyChildbirth.2014;14:389.35. SankarMJ,NatarajanCK,DasRR,AgarwalR,ChandrasekaranA,PaulVK.Whendonewbornsdie?Asystematicreviewoftimingofoverallandcause-specificneonataldeathsindevelopingcountries.JPerinatol.2016;36Suppl1:S1-s11.36. LehtonenL,GimenoA,Parra-LlorcaA,VentoM,editors.Earlyneonataldeath:Achallengeworldwide.SeminarsinFetalandNeonatalMedicine;2017:Elsevier.37. Engmann CM, Hodgson A, Aborigo R, Adongo PL,Moyer CA. Addressing thecontinuum of maternal and newborn care in Ghana: implications for policy andpractice.HealthPolicyPlan.2016;31(10):1355-63.38. SinhaS,AggarwalAR,OsmondC,FallCH,BhargavaSK,SachdevHS.MaternalAgeatChildbirthandPerinatalandUnderfiveMortalityinaProspectiveBirthCohortfromDelhi.IndianPediatr.2016;53(10):871-7.39. SemrauKEA,HerlihyJ,GroganC,MusokotwaneK,Yeboah-AntwiK,MbeweR,et al. Effectiveness of 4% chlorhexidine umbilical cord care on neonatalmortality inSouthern Province, Zambia (ZamCAT): a cluster-randomised controlled trial. LancetGlobHealth.2016;4(11):e827-e36.40. Sazawal S, Dhingra U, Ali SM, Dutta A, Deb S, Ame SM, et al. Efficacy ofchlorhexidineapplicationtoumbilicalcordonneonatalmortalityinPemba,Tanzania:acommunity-based randomised controlled trial. Lancet Glob Health. 2016;4(11):e837-e44.41. Engmann C, Garces A, Jehan I, Ditekemena J, Phiri M, Mazariegos M, et al.Causes of community stillbirths and early neonatal deaths in low-income countriesusingverbalautopsy:anInternational,MulticenterStudy.JPerinatol.2012;32(8):585.42. Bailey PE, AndualemW, BrunM, Freedman L, Gbangbade S, KanteM, et al.Institutional maternal and perinatal deaths: a review of 40 low andmiddle incomecountries.BMCPregnancyChildbirth.2017;17(1):295.43. Woods R. Long-term trends in fetal mortality: implications for developingcountries.BullWorldHealthOrgan.2008;86:460-6.44. TuiletaE.AmericanSamoaVitalStatisticsReport2010-2012,AmericanSamoaGovernment.2015.45. Moore JE, Uka S, Vogel JP, Timmings C, Rashid S, Gülmezoglu AM, et al.Navigating barriers: two-year follow up on recommendations to improve the use ofmaternalhealthguidelinesinKosovo.BMCPublicHealth.2016;16(1):987.46. KalterHD,KhazenRR,BarghouthiM,OdehM.Prospectivecommunity‐basedclustercensusandcase‐controlstudyofstillbirthsandneonataldeaths intheWestBankandGazaStrip.PaediatrPerinatEpidemiol.2008;22(4):321-33.47. WorldBankGroup. TheWorldBankData [Internet] 2018 [5thAugust, 2018].Availablefrom:https://data.worldbank.org/income-level/low-and-middle-income.48. AnastasiE,EkanemE,HillO,AdebayoOluwakemiA,AbayomiO,BernasconiA.Unmasking inequalities: Sub-national maternal and child mortality data from twourbanslumsinLagos,Nigeriatellsthestory.PLoSOne.2017;12(5):e0177190.

108
49. AnggondowatiT,El-MohandesAA,QomariyahSN,KielyM,RyonJJ,GipsonRF,etal.MaternalcharacteristicsandobstetricalcomplicationsimpactneonataloutcomesinIndonesia:aprospectivestudy.BMCPregnancyChildbirth.2017;17(1):100.50. Banda M, Kazembe L, Lewycka S, King C, Phiri T, Masache G, et al. Spatialmodelling of perinatal mortality inMchinji, Malawi. Spat Spatiotemporal Epidemiol.2016;16:50-8.51. Garces A, McClure EM, Hambidge K, Krebs NF, Figueroa L, Aguilar M, et al.Trends inperinataldeathsfrom2010to2013 intheGuatemalanWesternHighlands.ReprodHealth.2015;12Suppl2:S14.52. Memon ZA, Khan GN, Soofi SB, Baig IY, Bhutta ZA. Impact of a community-based perinatal and newborn preventive care package on perinatal and neonatalmortality in a remote mountainous district in Northern Pakistan. BMC PregnancyChildbirth.2015;15:106.53. Groppi L, SomiglianaE, PisaniV, IkaM,Mabor JL,AkecHN,et al.Ahospital-centeredapproachtoimproveemergencyobstetriccareinSouthSudan.IntJGynaecolObstet.2015;128(1):58-61.54. Ugwa EA, Ashimi A. An assessment of stillbirths in a tertiary hospital innorthernNigeria.JMaternFetalNeonatalMed.2015;28(13):1585-8.55. Nascimento RCS, Costa M, Braga JU, Natividade MSD. Spatial patterns ofpreventable perinatal mortality in Salvador, Bahia, Brazil. Rev Saude Publica.2017;51:73.56. Okonofua F, Randawa A, Ogu R, Agholor K, Okike O, Abdus-Salam RA, et al.Views of senior health personnel about quality of emergency obstetric care: AqualitativestudyinNigeria.PLoSOne.2017;12(3):e0173414.57. LawnJE,BlencoweH,KinneyMV,BianchiF,GrahamWJ.Evidencetoinformthefutureformaternalandnewbornhealth.Bestpractice&researchClinicalobstetrics&gynaecology.2016;36:169-83.58. BrowneJL,VissersKM,AntwiE,SrofenyohEK,VanderLindenEL,AgyepongIA,etal.Perinataloutcomesafterhypertensivedisordersinpregnancyinalowresourcesetting.TropMedIntHealth.2015;20(12):1778-86.59. RahmanMM,AbeSK,RahmanMS,KandaM,NaritaS,BilanoV,etal.Maternalanemia and risk of adverse birth and health outcomes in low- and middle-incomecountries:systematicreviewandmeta-analysis.AmJClinNutr.2016;103(2):495-504.60. Marete I, Tenge C, Pasha O, Goudar S, Chomba E, Patel A, et al. PerinatalOutcomes of Multiple Gestation Pregnancies in Kenya, Zambia, Pakistan, India,GuatemalaandArgentina:AGlobalNetworkStudy.AmJPerinatol.2014;31(2):125.61. FajoluI,EzeakaV,AdeniyiO,IrohaE,Egri-OkwajiM.PrevalenceandoutcomeofhigherordermultiplepregnanciesinLagos,Nigeria.TheJournalofMaternal-Fetal&NeonatalMedicine.2013;26(13):1342-5.62. Olamijulo J, Olaleye O. Perinatal mortality in Lagos University TeachingHospital:afiveyearreview.NigQJHospMed.2011;21(4):255-61.63. Koulimaya-Gombet CE, Diouf AA, Diallo M, Dia A, Sene C, Moreau JC, et al.[Pregnancy and delivery in patients with a personal history of cesarean section inDakar: epidemiological, clinical, therapeutic and prognostic aspects].Pan AfrMed J.2017;27:135.
109
64. Kalisa R, Rulisa S, vanRoosmalen J, van denAkker T.Maternal andperinataloutcomeafterpreviouscaesareansectioninruralRwanda.BMCPregnancyChildbirth.2017;17(1):272.65. Boatin AA, Adu-Bonsaffoh K, Wylie BJ, Obed SA. Evaluating Facility-BasedDecision-Making in Women with a Prior Cesarean Delivery and Association withMaternalandPerinatalOutcomes.MaternChildHealthJ.2017;21(9):1845-52.66. Yirgu R, Molla M, Sibley L, Gebremariam A. Perinatal Mortality Magnitude,Determinants and Causes in West Gojam: Population-Based Nested Case-ControlStudy.PLoSOne.2016;11(7):e0159390.67. Macheku GS, Philemon RN, Oneko O, Mlay PS, Masenga G, Obure J, et al.Frequency,riskfactorsandfeto-maternaloutcomesofabruptioplacentaeinNorthernTanzania: a registry-based retrospective cohort study. BMC Pregnancy Childbirth.2015;15:242.68. KaboreC,ChailletN,KouandaS,BujoldE,TraoreM,DumontA.Maternalandperinataloutcomesassociatedwithatrialoflabourafterpreviouscaesareansectioninsub-Saharancountries.BJOG.2016;123(13):2147-55.69. PerveenF,TayyabS,ZuberiBF.Risk factors forperinataldeaths inPakistan. JObstetGynaecolRes.2011;37(10):1359-64.70. Ekure E, Ezeaka V, Iroha E, Egri-Okwaji M. Prospective audit of perinatalmortalityamonginbornbabiesinatertiaryhealthcenterinLagos,Nigeria.NigerJClinPract.2011;14(1).71. Harrison MS, Goldenberg RL. Global burden of prematurity. Semin FetalNeonatalMed.2016;21(2):74-9.72. ChinkhumbaJ,DeAllegriM,MuulaAS,RobberstadB.Maternalandperinatalmortality by place of delivery in sub-Saharan Africa: a meta-analysis of population-basedcohortstudies.BMCPublicHealth.2014;14:1014.73. Ali AAA, Elgessim ME, Taha E, Adam GK. Factors associated with perinatalmortality in Kassala, Eastern Sudan: a community-based study 2010–2011. J TropPediatr.2013;60(1):79-82.74. Turab A, Ariff S, Habib MA, Ahmed I, Hussain M, Rashid A, et al. Improvedaccessibilityofemergencyobstetricsandnewborncare(EmONC)servicesformaternaland newborn health: a community based project. BMC Pregnancy Childbirth.2013;13(1):136.75. More NS, Bapat U, Das S, Alcock G, Patil S, Porel M, et al. Communitymobilization in Mumbai slums to improve perinatal care and outcomes: a clusterrandomizedcontrolledtrial.PLoSMed.2012;9(7):e1001257.76. WilsonA,GallosID,PlanaN,LissauerD,KhanKS,ZamoraJ,etal.Effectivenessof strategies incorporating training and support of traditional birth attendants onperinatalandmaternalmortality:meta-analysis.BMJ.2011;343:d7102.77. Matendo R, Engmann C, Ditekemena J, Gado J, Tshefu A, Kinoshita R, et al.Reduced perinatal mortality following enhanced training of birth attendants in theDemocraticRepublicofCongo:atime-dependenteffect.BMCMed.2011;9(1):93.78. GoudarSS,DhadedSM,McClureEM,DermanRJ,PatilVD,MahantshettiNS,etal. ENC training reduces perinatal mortality in Karnataka, India. The Journal ofMaternal-Fetal&NeonatalMedicine.2012;25(6):568-74.

110
79. Rani S, Chawla D, Huria A, Jain S. Risk factors for perinatalmortality due toasphyxia among emergency obstetric referrals in a tertiary hospital. Indian Pediatr.2012;49(3):191-4.80. YakoobMY, AliMA, AliMU, Imdad A, Lawn JE, Van Den BroekN, et al. Theeffectofprovidingskilledbirthattendanceandemergencyobstetriccareinpreventingstillbirths.BMCPublicHealth.2011;11(3):S7.81. EllisM, Azad K, Banerjee B, Shaha SK, Prost A, Rego AR, et al. Intrapartum-relatedstillbirthsandneonataldeathsinruralBangladesh:aprospective,community-basedcohortstudy.Pediatrics.2011:peds.2010-0842.82. Anastasi E, Ekanem E, Hill O, Oluwakemi AA, Abayomi O, Bernasconi A.Unmasking inequalities: Sub-national maternal and child mortality data from twourbanslumsinLagos,Nigeriatellsthestory.PLoSOne.2017;12(5):e0177190.83. EnuamehYA,OkawaS,AsanteKP,KikuchiK,MahamaE,AnsahE,etal.FactorsInfluencing Health Facility Delivery in Predominantly Rural Communities across theThree Ecological Zones in Ghana: A Cross-Sectional Study. PLoS One.2016;11(3):e0152235.84. BelladRM,BangA,CarloWA,McClureEM,MelethS,GocoN,etal.Apre-poststudyofamulti-countryscaleupofresuscitationtrainingof facilitybirthattendants:does Helping Babies Breathe training save lives? BMC Pregnancy Childbirth.2016;16(1):222.85. BucherS,KonanaO,LiechtyE,GarcesA,GisoreP,MareteI,etal.Self-reportedpracticesamongtraditionalbirthattendantssurveyedinwesternKenya:adescriptivestudy.BMCPregnancyChildbirth.2016;16(1):219.86. Berhan Y, Berhan A. Skilled health personnel attended delivery as a proxyindicatorformaternalandperinatalmortality:asystematicreview.EthiopJHealthSci.2014;24Suppl:69-80.87. NkwoPO,LawaniLO,EzugwuEC,IyokeCA,UbesieAC,OnohRC.Correlatesofpoorperinataloutcomesinnon-hospitalbirths inthecontextofweakhealthsystem:theNigerianexperience.BMCPregnancyChildbirth.2014;14:341.88. Pervin J, Moran A, Rahman M, Razzaque A, Sibley L, Streatfield PK, et al.Associationofantenatalcarewithfacilitydeliveryandperinatalsurvival–apopulation-basedstudyinBangladesh.BMCPregnancyChildbirth.2012;12(1):111.89. SinghSK,KaurR,GuptaM,KumarR.ImpactofnationalruralhealthmissiononperinatalmortalityinruralIndia.IndianPediatr.2012;49(2):136-8.90. KhanamR,BaquiAH,SyedMIM,HarrisonM,BegumN,QuaiyumA,etal.Canfacility delivery reduce the risk of intrapartum complications-related perinatalmortality?Findingsfromacohortstudy.Journalofglobalhealth.2018;8(1).91. FengXL,GuoS,HipgraveD,ZhuJ,ZhangL,SongL,etal.China'sfacility-basedbirth strategy and neonatal mortality: a population-based epidemiological study.Lancet.2011;378(9801):1493-500.92. FengXL,XuL,GuoY,RonsmansC.SocioeconomicinequalitiesinhospitalbirthsinChinabetween1988and2008.BullWorldHealthOrgan.2011;89(6):432-41.93. Liang J,MuY, Li X, TangW,WangY, Liu Z, et al. Relaxationof theone childpolicy and trends in caesarean section rates and birth outcomes in China between2012and2016:observationalstudyofnearlysevenmillionhealthfacilitybirths.BMJ.2018;360:k817.

111
94. Lori JR, Stalls S, Rominski SD. Strengthening Midwifery to End PreventableMaternal,Child,andNewbornDeaths.JMidwiferyWomensHealth.2015;60(4):343-7.95. KrukME,LeslieHH,VerguetS,MbarukuGM,AdanuRMK,LangerA.QualityofbasicmaternalcarefunctionsinhealthfacilitiesoffiveAfricancountries:ananalysisofnationalhealthsystemsurveys.LancetGlobHealth.2016;4(11):e845-e55.96. SemrauKE,HirschhornLR,MarxDelaneyM,SinghVP,SaurastriR,SharmaN,etal.OutcomesofaCoaching-BasedWHOSafeChildbirthChecklistProgramin India.NEnglJMed.2017;377(24):2313-24.97. GoudarSS,GocoN,SomannavarMS,VernekarSS,MallapurAA,MooreJL,etal.Institutional deliveries and perinatal and neonatalmortality in Southern andCentralIndia.ReprodHealth.2015;12Suppl2:S13.98. Ecevit A, Oguz SS, Tarcan A, Yazici C, Dilmen U. The changing pattern ofperinatal mortality and causes of death in central Anatolian region of Turkey. TheJournalofMaternal-Fetal&NeonatalMedicine.2012;25(9):1738-41.99. Kültürsay N, Aşkar N, Terek D, Yeniel AÖ, Köroğlu ÖA, Yalaz M, et al. TheChangeofPerinatalMortalityOverThreeDecadesinaReferenceCentreintheAegeanRegion:NeonatalMortality has decreased but FoetalMortality RemainsUnchanged.Balkanmedicaljournal.2017;34(6).100. Goldenberg RL, McClure EM, Kamath BD. Intrapartum perinatal mortality.IndianPediatr.2012;49(3):187-90.101. Wall SN, Lee AC, CarloW, Goldenberg R, Niermeyer S, Darmstadt GL, et al.,editors. Reducing intrapartum-related neonatal deaths in low-and middle-incomecountries—whatworks?SeminPerinatol;2010:Elsevier.102. RonsmansC,ChowdhuryME,KoblinskyM,AhmedA.Care seekingat timeofchildbirth, and maternal and perinatal mortality in Matlab, Bangladesh. Bull WorldHealthOrgan.2010;88:289-96.103. AhmedM,WonY.Cross-NationalSystematicReviewofNeonatalMortalityandPostnatal Newborn Care: Special Focus on Pakistan. Int J Environ Res Public Health.2017;14(12):1442.104. NascimentoRdCdS,CostaMdCN,BragaJU,NatividadeMSd.SpatialpatternsofpreventableperinatalmortalityinSalvador,Bahia,Brazil.RevSaudePublica.2017;51.105. SunL,YueH,SunB,HanL,QiM,TianZ,etal.Estimationofbirthpopulation-basedperinatal-neonatalmortalityandpretermrateinChinafromaregionalsurveyin2010.TheJournalofMaternal-Fetal&NeonatalMedicine.2013;26(16):1641-8.106. EngmannC,JehanI,DitekemenaJ,GarcesA,PhiriM,MazariegosM,etal.Analternativestrategyforperinatalverbalautopsycoding:singleversusmultiplecoders.TropMedIntHealth.2011;16(1):18-29.107. SuleimanB,MokuoluO,AdesiyunO,AdeniyiA.PatternofperinatalmortalityinbabiesdeliveredattheUniversityofIlorinTeachingHospital,Ilorin,Nigeria.WestAfrJMed.2012;31(2):102-8.108. Engmann C, Walega P, Aborigo RA, Adongo P, Moyer CA, Lavasani L, et al.StillbirthsandearlyneonatalmortalityinruralNorthernGhana.TropMedIntHealth.2012;17(3):272-82.109. Mgaya AH, Litorp H, Kidanto HL, Nyström L, Essén B. Criteria-based audit toimprove quality of care of foetal distress: standardising obstetric care at a nationalreferral hospital in a low resource setting, Tanzania. BMC Pregnancy Childbirth.2016;16(1):343.

112
110. Esike COU, Chukwuemeka UI, Anozie OB, Eze JN, Aluka OC, Twomey DE.EclampsiainruralNigeria:Theunmitigatingcatastrophe.AnnAfrMed.2017;16(4):175.111. Niang MM. [Unmet obstetrical needs for major obstetric interventions inDakar].MedSanteTrop.2015;25(3):276-9.112. BerhanY,BerhanA.Ameta-analysisofselectedmaternalandfetalfactorsforperinatalmortality.EthiopJHealthSci.2014;24Suppl:55-68.113. MouraPMSS,MaestáI,RugoloLMSS,AngulskiLFRB,CaldeiraAP,PeraçoliJC,etal.Riskfactorsforperinataldeathintwodifferentlevelsofcare:acase–controlstudy.Reproductivehealth.2014;11(1):11.114. Oliveira LC, CostaAARd. Fetal and neonatal deaths among cases ofmaternalnearmiss.RevAssocMedBras.2013;59(5):487-94.115. NankabirwaV,TumwineJK,TylleskärT,NankundaJ,SommerfeltH,ConsortiumPER. Perinatal mortality in eastern Uganda: a community based prospective cohortstudy.PLoSOne.2011;6(5):e19674.116. Bai J,WongFW,BaumanA,MohsinM.Parityandpregnancyoutcomes.AmJObstetGynecol.2002;186(2):274-8.117. Munan R, Kakudji Y, Nsambi J, Mukuku O, Maleya A, Kinenkinda X, et al.[Childbirth among primiparous women in Lubumbashi: maternal and perinatalprognosis].PanAfrMedJ.2017;28:77.118. Jacinto E, Aquino EM, Mota EL. [Perinatal mortality in the municipality ofSalvador, Northeastern Brazil: evolution from 2000 to 2009]. Rev Saude Publica.2013;47(5):846-53.119. MohammadiS,EssenB,FallahianM,TaheripanahR,SalehGargariS,KallestalC.Maternal near-miss at university hospitals with cesarean overuse: an incident case-controlstudy.ActaObstetGynecolScand.2016;95(7):777-86.120. WilsonA,LissauerD,ThangaratinamS,KhanKS,MacArthurC,CoomarasamyA.A comparison of clinical officers with medical doctors on outcomes of caesareansection in the developing world: meta-analysis of controlled studies. BMJ.2011;342:d2600.121. Chongsuvivatwong V, Bachtiar H, Chowdhury ME, Fernando S, Suwanrath C,Kor‐anantakul O, et al. Maternal and fetal mortality and complications associatedwith cesarean sectiondeliveries in teachinghospitals inAsia. JObstetGynaecolRes.2010;36(1):45-51.122. MaswimeS,BuchmannE.Causesandavoidablefactorsinmaternaldeathduetocesarean‐relatedhemorrhageinSouthAfrica.InternationalJournalofGynecology&Obstetrics.2016;134(3):320-3.123. Lumbiganon P, LaopaiboonM,Gülmezoglu AM, Souza JP, Taneepanichskul S,RuyanP,etal.Methodofdeliveryandpregnancyoutcomes inAsia: theWHOglobalsurveyonmaternalandperinatalhealth2007–08.TheLancet.2010;375(9713):490-9.124. RudgeMV,MaestáI,MouraPM,RudgeCV,MorceliG,CostaRA,etal.Thesafemotherhood referral system to reduce cesarean sections and perinatal mortality-across-sectionalstudy[1995-2006].Reproductivehealth.2011;8(1):34.125. GaladanciH,KünzelW,ShittuO,ZinserR,GruhlM,AdamsS.ObstetricqualityassurancetoreducematernalandfetalmortalityinKanoandKadunaStatehospitalsinNigeria.InternationalJournalofGynecology&Obstetrics.2011;114(1):23-8.

113
126. Chu K, Maine R, Trelles M. Cesarean section surgical site infections in sub-Saharan Africa: amulti-country study fromMedecins Sans Frontieres.World J Surg.2015;39(2):350-5.127. KinenkindaX,MukukuO,ChengeF,KakudjiP,BanzuluP,KakomaJB,etal.[Riskfactors for maternal and perinatal mortality among women undergoing cesareansectioninLubumbashi,DemocraticRepublicofCongoII].PanAfrMedJ.2017;26:208.128. OppongSA,TuuliMG,Seffah JD,AdanuRM. Is therea safe limitofdelay foremergencycaesareansectioninGhana?Resultsofanalysisofearlyperinataloutcome.GhanaMedJ.2014;48(1):24-30.129. Rhoda N, Greenfield D, Muller M, Prinsloo R, Pattinson R, Kauchali S, et al.Experiences with perinatal death reviews in South Africa—the Perinatal ProblemIdentificationProgramme: scalingup fromprogrammetoprovince tocountry.BJOG.2014;121(s4):160-6.130. MichalowJ,CholaL,McGeeS,TugendhaftA,PattinsonR,KerberK,etal.Triplereturn on investment: the cost and impact of 13 interventions that could preventstillbirths and save the lives ofmothers and babies in South Africa.BMC PregnancyChildbirth.2015;15(1):39.131. Baleta A. South Africa takes steps to reduce perinatal mortality. The Lancet.2011;377(9774):1303-4.132. NtuliST,MalanguN.An investigationof thestillbirthsata tertiaryhospital inLimpopoProvinceofSouthAfrica.Globaljournalofhealthscience.2012;4(6):141.133. PattinsonR.Whybabiesdie-aperinatalcaresurveyofSouthAfrica,2000-2002.SAfrMedJ.2003;93(6):445-50.134. TalipQ,TheronG,SteynW,HallD.TotalperinatallyrelatedlossesatTygerbergHospital–acomparisonbetween1986,1993and2006.SAfrMedJ.2010;100(4).135. Gaunt CB. Are we winning? Improving perinatal outcomes at a deeply ruraldistricthospitalinSouthAfrica.SAMJ:SouthAfricanMedicalJournal.2010;100(2):101-4.136. Allanson ER, Pattinson RC. Quality-of-care audits and perinatal mortality inSouthAfrica.BullWorldHealthOrgan.2015;93(6):424-8.137. McGeeS-A,CholaL,TugendhaftA,MubaiwaV,MoranN,McKerrowN,etal.Strategic planning for saving the lives of mothers, newborns and children andpreventingstillbirthsinKwaZulu-NatalprovinceSouthAfrica:modellingusingtheLivesSavedTool(LiST).BMCPublicHealth.2015;16(1):49.138. BallotDE,ChirwaT,RamdinT,ChirwaL,MareI,DaviesVA,etal.Comparisonofmorbidity and mortality of very low birth weight infants in a Central Hospital inJohannesburgbetween2006/2007and2013.BMCPediatr.2015;15(1):20.139. BothmaM,BuchmannEJ.Astudyoffreshstillbirthsweighing2500gormoreatthree academic hospitals in South Africa. International Journal of Gynecology &Obstetrics.2016;134(2):186-9.140. Bateman C. Stillbirths: an invisible earthquake. SAMJ: South African MedicalJournal.2011;101(6):364-6.141. Buchmann E, Pattinson R. Babies who die from labour-related intrapartumhypoxia: a confidential enquiry in South African public hospitals. Trop Doct.2006;36(1):8-10.142. Hofmeyr GJ, Mancotywa T, Silwana-Kwadjo N, Mgudlwa B, Lawrie TA,Gülmezoglu AM. Audit of a new model of birth care for women with low risk

114
pregnancies in SouthAfrica: the primary care onsitemidwife-led birth unit (OMBU).BMCPregnancyChildbirth.2014;14(1):417.143. PattinsonR.Reduction inperinatalmortality feasiblewithout incurringmajorcosts.SAfrJObstetGynaecol.2003;9(3):54-5.144. Ebrahim S, Daponte A, Guidozzi F. The impact of free antenatal care onperinatalmortality. InternationalJournalofGynecology&Obstetrics.2000;71(3):205-7.145. Woods D. Appropriate technology and education for improved intrapartumcareinunderresourcedcountries.SAfrJObstetGynaecol.2009;15(3).146. Velaphi S,PattinsonR.Avoidable factorsandcausesofneonataldeaths fromperinatal asphyxia-hypoxia in South Africa: national perinatal survey. Ann TropPaediatr.2007;27(2):99-106.147. Pattinson R, Woods D, Greenfield D, Velaphi S. Improving survival rates ofnewborninfantsinSouthAfrica.Reproductivehealth.2005;2(1):4.148. PatrickM.PerinatalmortalityatFrontierHospital,Queenstown-a6-yearauditusingthePerinatalProblemIdentificationProgramme(PPIP).SAfrJObstetGynaecol.2007;13(1):10-4.149. NgocNTN,MerialdiM,Abdel-AleemH,CarroliG,PurwarM,ZavaletaN,etal.Causes of stillbirths and early neonatal deaths: data from 7993 pregnancies in sixdevelopingcountries.BullWorldHealthOrgan.2006;84(9):699-705.150. OdendaalHJ,GebhardtGS,TheronGB.Stillbirthratesinsingletonpregnanciesin a stable population at Karl Bremer and Tygerberg hospitals over 50 years.SAfr JObstetGynaecol.2013;19(3):67-70.151. Lavin T, Preen DB, Pattinson R. Timing and cause of perinatal mortality forsmall-for-gestational-age babies in South Africa: critical periods and challenges withdetection.Maternalhealth,neonatologyandperinatology.2016;2(1):11.152. FrankK,LombaardH,PattinsonRC.Doescompletionof theEssentialSteps inManaging Obstetric Emergencies (ESMOE) training package result in improvedknowledge and skills in managing obstetric emergencies? S Afr J Obstet Gynaecol.2009;15(3).153. Pattinson R. Challenges in saving babies-Avoidable factors, missedopportunities and substandard care in perinatal deaths in SouthAfrica.SAfrMed J.2003;93(6):450-5.154. Joseph KS, Razaz N, Muraca GM, Lisonkova S. Methodological Challenges inInternationalComparisonsofPerinatalMortality.CurrEpidemiolRep.2017;4(2):73-82.155. Leisher SH, Teoh Z, Reinebrant H, Allanson E, Blencowe H, Erwich JJ, et al.Seekingorderamidstchaos:Asystematicreviewofclassificationsystemsforcausesofstillbirthandneonataldeath,2009–2014.BMCPregnancyChildbirth.2016;16(1):295.156. Allanson E, TunçalpÖ, Gardosi J, Pattinson RC, Erwich JJH, Flenady VJ, et al.Classifyingthecausesofperinataldeath.BullWorldHealthOrgan.2016;94(2):79.157. Organization WH. The WHO application of ICD-10 to perinatal deaths: ICD-perinatalmortality(ICD-PM).Geneva:WHO.2015.158. AllansonE,TunçalpӦ,Gardosi J,PattinsonR,Vogel J,ErwichJ,etal.Givingavoice tomillions: developing theWHO application of ICD‐10 to deaths during theperinatalperiod:ICD‐PM.BJOG.2016;123(12):1896-9.159. Yli BM, Kjellmer I. Pathophysiology of foetal oxygenation and cell damageduringlabour.BestPractResClinObstetGynaecol.2016;30:9-21.

115
160. AssaliNS,AssaliNS.FetalandNeonatalDisorders.SaintLouis:ElsevierScience;2013.161. Jensen A, Garnier Y, Berger R. Dynamics of fetal circulatory responses tohypoxiaandasphyxia.EurJObstetGynecolReprodBiol.1999;84(2):155-72.162. Martin CB, Jr. Normal fetal physiology and behavior, and adaptive responseswithhypoxemia.SeminPerinatol.2008;32(4):239-42.163. StevensonA.OxforddictionaryofEnglish:OxfordUniversityPress,USA;2010.164. Ayres-de-Campos D. Introduction: Why is intrapartum foetal monitoringnecessary - Impact on outcomes and interventions. Best Pract Res Clin ObstetGynaecol.2016;30:3-8.165. Fahey J, King TL. Intrauterine asphyxia: clinical implications for providers ofintrapartumcare.JMidwiferyWomensHealth.2005;50(6):498-506.166. NewbyEA,MyersDA,DucsayCA.Fetalendocrineandmetabolicadaptationstohypoxia: the role of the hypothalamic-pituitary-adrenal axis.Am J Physiol EndocrinolMetab.2015;309(5):E429-39.167. VaughanOR,DeBlasioMJ, FowdenAL.OVINEUTEROPLACENTALAND FETALMETABOLISM DURING AND AFTER FETAL CORTISOL OVEREXPOSURE IN LATEGESTATION.American JournalofPhysiology-Regulatory, IntegrativeandComparativePhysiology.2018.168. Bennet L, Rossenrode S, Gunning MI, Gluckman PD, Gunn AJ. Thecardiovascular and cerebrovascular responses of the immature fetal sheep to acuteumbilicalcordocclusion.JPhysiol.1999;517(Pt1):247-57.169. Yan EB, Baburamani AA,Walker AM,Walker DW. Changes in cerebral bloodflow, cerebral metabolites, and breathing movements in the sheep fetus followingasphyxiaproducedbyocclusionoftheumbilicalcord.AmJPhysiolRegulIntegrCompPhysiol.2009;297(1):R60-9.170. Quaedackers JS, Roelfsema V, Hunter CJ, Heineman E, Gunn AJ, Bennet L.Polyuria and impaired renal blood flow after asphyxia in preterm fetal sheep.Am JPhysiolRegulIntegrCompPhysiol.2004;286(3):R576-83.171. LotgeringFK,BishaiJM,StruijkPC,BloodAB,HunterCJ,PowerGG,etal.Ten-minute umbilical cord occlusion markedly reduces cerebral blood flow and heatproductioninfetalsheep.AmJObstetGynecol.2003;189(1):233-8.172. HolzmannM,CnattingiusS,NordströmL.Lactateproductionasaresponsetointrapartumhypoxiainthegrowth‐restrictedfetus.BJOG.2012;119(10):1265-9.173. Giussani DA. The fetal brain sparing response to hypoxia: physiologicalmechanisms.JPhysiol.2016;594(5):1215-30.174. BennetL.Sex,drugsandrockandroll:talesfrompretermfetallife.TheJournalofphysiology.2017;595(6):1865-81.175. MallardEC,WilliamsCE,JohnstonBM,GluckmanPD.Increasedvulnerabilitytoneuronal damage after umbilical cord occlusion in fetal sheep with advancinggestation.AmJObstetGynecol.1994;170(1Pt1):206-14.176. Hernandez-Andrade E, Hellstrom-Westas L, Thorngren-Jerneck K, Jansson T,LiubaK,LingmanG,etal.Perinataladaptiveresponseoftheadrenalandcarotidbloodflowinsheepfetusessubjectedtototalcordocclusion.JMaternFetalNeonatalMed.2005;17(2):101-9.

116
177. vanDijk AJ, van Loon JP, TaverneMA, Jonker FH.Umbilical cord clamping interm piglets: a useful model to study perinatal asphyxia? Theriogenology.2008;70(4):662-74.178. GrahamEM,RuisKA,HartmanAL,NorthingtonFJ,FoxHE.Asystematicreviewof the role of intrapartum hypoxia-ischemia in the causation of neonatalencephalopathy.AmJObstetGynecol.2008;199(6):587-95.179. GeorgeS,GunnAJ,WestgateJA,BrabynC,GuanJ,BennetL.Fetalheart ratevariability and brain stem injury after asphyxia in preterm fetal sheep.Am J PhysiolRegulIntegrCompPhysiol.2004;287(4):R925-33.180. Bennet L,Quaedackers JS,GunnAJ,RossenrodeS,HeinemanE.Theeffectofasphyxia on superior mesenteric artery blood flow in the premature sheep fetus. JPediatrSurg.2000;35(1):34-40.181. SarratoSZ,CastroSV,NavarroCR,SarratoGZ,LunaMS.Risksfactorsassociatedwith intra-partum foetal mortality in pre-term infants. Anales de Pediatría (EnglishEdition).2017;86(3):127-34.182. deAlmeidaMF,MoreiraLM,VazdosSantosRM,KawakamiMD,AnchietaLM,Guinsburg R. Early neonatal deathswith perinatal asphyxia in very low birthweightBrazilianinfants.JPerinatol.2015;35(11):954-7.183. TuuliMG,StoutMJ,ShanksA,OdiboAO,MaconesGA,CahillAG.Umbilicalcordarterial lactate comparedwith pH for predicting neonatalmorbidity at term.ObstetGynecol.2014;124(4):756-61.184. Morales P, Bustamante D, Espina-Marchant P, Neira-Pena T, Gutierrez-HernandezMA,Allende-CastroC,etal.Pathophysiologyofperinatalasphyxia:canwepredictandimproveindividualoutcomes?Epmaj.2011;2(2):211-30.185. EastCE,LeaderLR,SheehanP,HenshallNE,ColditzPB.Intrapartumfetalscalplactate sampling for fetalassessment in thepresenceofanon-reassuring fetalheartrate trace.CochraneDatabase of Systematic Reviews. 2010;2010(3):CD006174-1-CD-30.186. ZanardoV,MariG,deLucaF,ScambiaG,GuerriniP,StrafaceG.Lactateincordbloodand its relation to fetal gluconeogenesis in at termdeliveries.EarlyHumDev.2015;91(3):165-8.187. RossMG.Laborand fetalheart ratedecelerations: relation to fetalmetabolicacidosis.ClinObstetGynecol.2011;54(1):74-82.188. HamedHO.Intrapartumfetalasphyxia:studyofumbilicalcordbloodlactateinrelationtofetalheartratepatterns.ArchGynecolObstet.2013;287(6):1067-73.189. Nordstrom L, Arulkumaran S. Intrapartum fetal hypoxia and biochemicalmarkers:areview.ObstetGynecolSurv.1998;53(10):645-57.190. Nordstrom L, Ingemarsson I, Westgren M. Fetal monitoring with lactate.BaillieresClinObstetGynaecol.1996;10(2):225-42.191. HeinisAM,SpaandermanME,GunnewiekJM,LotgeringFK.Scalpbloodlactatefor intra-partum assessment of fetalmetabolic acidosis.ActaObstet Gynecol Scand.2011;90(10):1107-14.192. GjerrisAC,Staer-JensenJ,JorgensenJS,BergholtT,NickelsenC.Umbilicalcordbloodlactate:avaluabletoolintheassessmentoffetalmetabolicacidosis.EurJObstetGynecolReprodBiol.2008;139(1):16-20.193. Nordstrom L, Achanna S, Naka K, Arulkumaran S. Fetal andmaternal lactateincreaseduringactivesecondstageoflabour.BJOG.2001;108(3):263-8.

117
194. Low JA, Panagiotopoulos C, Derrick EJ. Newborn complications afterintrapartum asphyxia with metabolic acidosis in the preterm fetus. Am J ObstetGynecol.1995;172(3):805-10.195. Low JA, Panagiotopoulos C, Derrick EJ. Newborn complications afterintrapartumasphyxiawithmetabolicacidosis inthetermfetus.AmJObstetGynecol.1994;170(4):1081-7.196. Frasch MG, Mansano RZ, Gagnon R, Richardson BS, Ross MG. Measures ofacidosiswithrepetitiveumbilicalcordocclusionsleadingtofetalasphyxiainthenear-termovinefetus.AmJObstetGynecol.2009;200(2):200.e1-.e7.197. Low JA.Metabolic acidosis and fetal reserve.Baillieres Clin Obstet Gynaecol.1996;10(2):211-24.198. NardozzaLMM,CaetanoACR,ZamarianACP,MazzolaJB,SilvaCP,MarçalVMG,etal.Fetalgrowthrestriction:currentknowledge.ArchGynecolObstet.2017:1-17.199. Sousa S, Mielke JG. Does Resuscitation Training Reduce Neonatal Deaths inLow-ResourceCommunities?ASystematicReviewof theLiterature.AsiaPac JPublicHealth.2015;27(7):690-704.200. Endrich O, Rimle C, Zwahlen M, Triep K, Raio L, Nelle M. Asphyxia in theNewborn: Evaluating the Accuracy of ICD Coding, Clinical Diagnosis andReimbursement: Observational Study at a Swiss Tertiary Care Center on RoutinelyCollectedHealthDatafrom2012-2015.PLoSOne.2017;12(1):e0170691.201. Ensing S, Abu-Hanna A, Schaaf JM, Mol BWJ, Ravelli AC. Trends in birthasphyxia, obstetric interventions and perinatal mortality among term singletons: anationwide cohort study. The Journal of Maternal-Fetal & Neonatal Medicine.2015;28(6):632-7.202. Manandhar SR, Manandhar DS, Adhikari D, Shrestha J, Rai C, Rana H, et al.AnalysisofHealthFacilityBasedPerinatalVerbalAutopsyofElectoralConstituency2ofArghakhanchiDistrict,Nepal.JNepalHealthResCounc.2015;13(29):73-7.203. ViswanathK,PsR,ChakrabortyA,Prasad JH,MinzS,GeorgeK.AcommunitybasedcasecontrolstudyondeterminantsofperinatalmortalityinatribalpopulationofsouthernIndia.RuralRemoteHealth.2015;15(3):3388.204. NouailiEBH,ChaouachiS,Ayadi I,SaidAB,ZouariB,MarrakchiZ.Risk factorsforperinatalmortalityinaTunisianpopulation.InternationalJournalofGynecology&Obstetrics.2010;111(3):265-6.205. Kali GTJ,Martinez‐BiargeM, Van Zyl J, Smith J, RutherfordM. Therapeutichypothermia for neonatal hypoxic‐ ischaemic encephalopathy had favourableoutcomes at a referral hospital in a middle‐ income country. Acta Paediatr.2016;105(7):806-15.206. Phoa KY, Chedraui P, Perez-Lopez FR,Wendte JF, Ghiabi S, Vrijkotte T, et al.Perinatal outcome in singleton pregnancies complicated with preeclampsia andeclampsiainEcuador.JObstetGynaecol.2016;36(5):581-4.207. BobrowCS, Soothill PW. Causes and consequences of fetal acidosis.ArchDisChildFetalNeonatalEd.1999;80(3):F246-9.208. Perlman JM. Intervention strategies for neonatal hypoxic-ischemic cerebralinjury.ClinTher.2006;28(9):1353-65.209. Pin TW, Eldridge B, GaleaMP. A review of developmental outcomes of terminfants with post-asphyxia neonatal encephalopathy. Eur J Paediatr Neurol.2009;13(3):224-34.
118
210. Perlman JM. Intrapartum asphyxia and cerebral palsy: is there a link? ClinPerinatol.2006;33(2):335-53.211. Westgate JA, Wibbens B, Bennet L, Wassink G, Parer JT, Gunn AJ. Theintrapartumdecelerationincenterstage:aphysiologicapproachtotheinterpretationoffetalheartratechangesinlabor.AmJObstetGynecol.2007;197(3):236.e1-11.212. Heuser CC, Knight S, Esplin MS, Eller AG, Holmgren CM, Richards D, et al.Tachysystoleintermlabor:incidence,riskfactors,outcomes,andeffectonfetalhearttracings.AmJObstetGynecol.2013;209(1):32.e1-.e6.213. BakkerPC,KurverPH,KuikDJ,VanGeijnHP.Elevateduterineactivityincreasestheriskoffetalacidosisatbirth.AmJObstetGynecol.2007;196(4):313.e1-6.214. GibbonsC,O'HerlihyC,MurphyJ.Umbilicalcordprolapse–changingpatternsandimprovedoutcomes:aretrospectivecohortstudy.BJOG.2014;121(13):1705-8.215. Huang J-P, Chen C-P, Chen C-P, Wang K-G, Wang K-L. Term pregnancy withumbilicalcordprolapse.TaiwanJObstetGynecol.2012;51(3):375-80.216. NorwitzER,BelfortMA,SaadeGR,MillerH.CordProlapse.Oxford,UK:Wiley‐Blackwell;2010.156-7p.217. Holbrook BD, Phelan ST. Umbilical Cord Prolapse.Obstet Gynecol Clin NorthAm.2012.218. Kahana B, Sheiner E, Levy A, Lazer S,MazorM. Umbilical cord prolapse andperinataloutcomes.IntJGynaecolObstet.2004;84(2):127-32.219. Gabbay-Benziv R, MamanM,Wiznitzer A, Linder N, Yogev Y. Umbilical cordprolapse during delivery - risk factors and pregnancy outcome: a single centerexperience.Thejournalofmaternal-fetal&neonatalmedicine:theofficial journalofthe European Association of PerinatalMedicine, the Federation of Asia andOceaniaPerinatalSocieties,theInternationalSocietyofPerinatalObstetricians.2014;27(1):14.220. Wasswa EW, Nakubulwa S, Mutyaba T. Fetal demise and associated factorsfollowingumbilical cord prolapse inMulagohospital,Uganda: a retrospective study.ReproductiveHealth.2014;11:12.221. UmarU,GayaS.OutcomeofumbilicalcordprolapseatAminuKanoTeachingHospital,Kano,North-WesternNigeria.NigerianJournalofBasicandClinicalSciences.2015;12(1):20-4.222. BehbehaniS,PatenaudeV,AbenhaimHA.MaternalRiskFactorsandOutcomesof Umbilical Cord Prolapse: A Population-Based Study. Journal of Obstetrics andGynaecologyCanada.2016;38(1):23-8.223. Hasegawa J, SekizawaA, IkedaT,KoresawaM, Ishiwata I,KawabataM,etal.Clinicalriskfactorsforpoorneonataloutcomesinumbilicalcordprolapse.Thejournalofmaternal-fetal&neonatalmedicine:theofficialjournaloftheEuropeanAssociationof Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, theInternationalSocietyofPerinatalObstetricians.2016;29(10):1652.224. EsikeCOU,AlukaOC,UkanwokoC,EzeJN,TowmeyDE.O044CORDPROLAPSEIN A RURAL SOUTH EASTHERN NIGERIA HOSPITAL: A TEN‐ YEAR EXPERIENCE.InternationalJournalofGynecology&Obstetrics.2012;119:S276-S.225. ObeidatN,ZayedF,AlchalabiH,ObeidatB,El-JalladMF,ObeidatM.Umbilicalcord prolapse: A 10-year retrospective study in two civil hospitals, North Jordan. JObstetGynaecol.2010;30(3):257-60.226. EnakpeneCA,OdukogbeA-TO,Morhason-BelloIO,OmigbodunAO,ArowojoluAO.Theinfluenceofhealth-seekingbehaviorontheincidenceandperinataloutcome

119
of umbilical cord prolapse in Nigeria. International Journal of Women's Health.2010;2:177-82.227. FazilA,ZafarF,AsifaA,AkmalN,KarimA.Prevalenceandperinatalmortalityofcordprolapseandpresentation.AnnalsofKingEdwardMedicalUniversity.2016;11(3).228. KamoshitaE,AmanoK,KanaiY,MochizukiJ,IkedaY,KikuchiS,etal.Effectofthe interval between onset of sustained fetal bradycardia and cesarean delivery onlong‐term neonatal neurologic prognosis. International Journal of Gynecology &Obstetrics.2010;111(1):23-7.229. Kalu C, Umeora O. Risk factors and perinatal outcome of umbilical cordprolapse in Ebonyi StateUniversity TeachingHospital, Abakaliki,Nigeria.Niger J ClinPract.2011;14(4):413-7.230. Lamina M, Adefuye P, Akinsanya A, Odubena O. Risk factors and perinataloutcome of umbilical cord prolapse in Sagamu, Nigeria. Annals of Health Research.2016;2(2):98-.231. Downes KL, Grantz KL, Shenassa ED.Maternal, Labor, Delivery, and PerinatalOutcomesAssociatedwithPlacentalAbruption:ASystematicReview.AmJPerinatol.2017;34(10):935-57.232. Nkwabong E, Tiomela Goula G. Placenta abruption surface and perinataloutcome.JMaternFetalNeonatalMed.2017;30(12):1456-9.233. ColemanJ,SrofenyoEK,OforiEK,BrakohiapaEK,AntwiWK.Maternalandfetalprognosis in abruptio placentae at Korle-Bu Teaching Hospital, Ghana.Afr J ReprodHealth.2014;18(4):115-22.234. BerhanY.Predictorsofperinatalmortalityassociatedwithplacentapreviaandplacentalabruption:anexperiencefromalowincomecountry.Journalofpregnancy.2014;2014.235. Akintayo AA, Olagbuji BN, Aderoba AK, Akadiri O, Olofinbiyi BA, Bakare B.Emergency Peripartum Hysterectomy: A Multicenter Study of Incidence, IndicationsandOutcomesinSouthwesternNigeria.MaternChildHealthJ.2016;20(6):1230-6.236. AbasiattaiAM,UmoiyohoAJ,UtukNM,Inyang-EtohEC,AsuquoE.Emergencyperipartum hysterectomy in a tertiary hospital in southern Nigeria. Pan Afr Med J.2013;15(1).237. Rizwan N, Abbasi RM, Uddin SF. Uterine rupture, frequency of cases andfetomaternal outcome. JPMA-Journal of the Pakistan Medical Association.2011;61(4):322.238. Gupta A, Nanda S. Uterine rupture in pregnancy: a five-year study. ArchGynecolObstet.2011;283(3):437-41.239. Rezende KB, Bornia RG, Esteves AP, Cunha AJ, Amim Junior J. Preeclampsia:PrevalenceandperinatalrepercussionsinaUniversityHospitalinRiodeJaneiro,Brazil.PregnancyHypertens.2016;6(4):253-5.240. Mooij R, Lugumila J, Mwashambwa MY, Mwampagatwa IH, van Dillen J,Stekelenburg J. Characteristics and outcomes of patientswith eclampsia and severepre-eclampsia inaruralhospital inWesternTanzania:aretrospectivemedicalrecordstudy.BMCPregnancyChildbirth.2015;15:213.241. DasR,BiswasS.Eclapmsia:TheMajorCauseofMaternalMortality inEasternIndia.EthiopJHealthSci.2015;25(2):111-6.

120
242. GaladanciH,KunzelW,ZinserR,ShittuO,AdamsS,GruhlM.Experiencesof6years quality assurance in obstetrics in Nigeria - a critical review of results andobstacles.JPerinatMed.2016;44(3):301-8.243. Vigil-DeGraciaP,Rojas-SuarezJ,RamosE,ReyesO,CollantesJ,QuinteroA,etal. Incidence of eclampsia with HELLP syndrome and associated mortality in LatinAmerica.IntJGynaecolObstet.2015;129(3):219-22.244. Perveen S. Frequency and impact of hypertensive disorders of pregnancy. JAyubMedCollAbbottabad.2014;26(4):518-21.245. Kumari A, ChakrawartyA, SinghA, SinghR.Maternofoetal complications andtheir associationwithproteinuria in a tertiary carehospital of adeveloping country.Journalofpregnancy.2014;2014.246. AsıcıogluO,ŞahbazA,GüngördükK,YildirimG,AsıcıogluBB,ÜlkerV.Maternaland perinatal outcomes in women with placenta praevia and accreta in teachinghospitalsinWesternTurkey.JObstetGynaecol.2014;34(6):462-6.247. Kiondo P, Tumwesigye NM, Wandabwa J, Wamuyu-Maina G, Bimenya GS,Okong P. Adverse neonatal outcomes in women with pre-eclampsia in MulagoHospital, Kampala,Uganda: a cross-sectional study.ThePanAfricanmedical journal.2014;17(Suppl1).248. Sadaf N, Haq G, Shukar-ud-Din S. Maternal and foetal outcome in HELLPsyndromeattertiarycarehospital.JPakMedAssoc.2013;63(12):1500-3.249. ParnaF, LatifT,SultanaN,AliM,ChowdhuryS.Maternal& fetaloutcomeofeclampticpatientsadmittedinobstetrics&gynaecologydepartmentofsecondarycarehospitalinBangladesh.Mymensinghmedicaljournal:MMJ.2013;22(3):522-6.250. Vigil-DeGraciaP,Montufar-RuedaC,RuizJ.Expectantmanagementofseverepreeclampsia and preeclampsia superimposed on chronic hypertension between 24and 34 weeks’ gestation. European Journal of Obstetrics & Gynecology andReproductiveBiology.2003;107(1):24-7.251. AdamuA,EkeleB,AhmedY,MohammedB,IsezuoS,AbdullahpiA.PregnancyoutcomeinwomenwitheclampsiaatatertiarycentreinnorthernNigeria.AfrJMedMedSci.2012;41(2):211-9.252. JidoTA.Ecalmpsia:maternalandfetaloutcome.AfrHealthSci.2012;12(2):148-52.253. TukurJ,AhonsiB,IshakuSM,AraoyinboI,OkerekeE,BabatundeAO.Maternaland fetal outcomes after introduction of magnesium sulphate for treatment ofpreeclampsia and eclampsia in selected secondary facilities: a low-cost intervention.Maternalandchildhealthjournal.2013;17(7):1191-8.254. UgwuE,DimC,OkonkwoC,NwankwoT.Maternalandperinataloutcomeofseverepre-eclampsiainEnugu,NigeriaafterintroductionofMagnesiumsulfate.NigerJClinPract.2011;14(4):418-21.255. Abd El Aal DE, Shahin AY. Management of eclampsia at Assiut UniversityHospital,Egypt.IntJGynaecolObstet.2012;116(3):232-6.256. Kumar M, Meena J, Gupta U, Singh A, Jain N. Management of early onsetseverepreeclampsia inatertiaryhospital in india:doesexpectantmanagementalterperinataloutcome?IndianJMedSci.2011;65(12).257. AgidaE,AdekaB,JibrilK.PregnancyoutcomeineclampticsattheUniversityofAbuja Teaching Hospital, Gwagwalada, Abuja: a 3 year review. Niger J Clin Pract.2010;13(4).

121
258. YildirimG,GungordukK,GulA,AsiciogluO,SudolmusS,GungordukOC,etal.HELLP Syndrome: 8 years of experience from a tertiary referral center in WesternTurkey.HypertensPregnancy.2012;31(3):316-26.259. Tukur J,Muhammad Z.Management of eclampsia at AKTH: before and aftermagnesiumsulphate.NigerJMed.2010;19(1).260. Low JA. Cerebral perfusion, metabolism, and outcome. Curr Opin Pediatr.1995;7(2):132-9.261. DeppR.Perinatalasphyxia:assessing itscausalroleandtiming.SeminPediatrNeurol.1995;2(1):3-36.262. Blackstone J, Young BK. Umbilical cord blood acid-base values and otherdescriptorsoffetalcondition.ClinObstetGynecol.1993;36(1):33-46.263. OliveiraTGd,FreirePV,MoreiraFT,Moraes JdSBd,ArrelaroRC,RossiS,etal.Apgarscoreandneonatalmortality inahospital located in thesouthernareaofSãoPauloCity,Brazil.Einstein(SãoPaulo).2012;10(1):22-8.264. SabiriN,KabiriM,KarboubiL,BouzianeA,BarkatA.Risk factors forperinatalmortality at Souissi Maternity Hospital, Rabat, Morocco. International Journal ofGynecology&Obstetrics.2012;119(3):285-6.265. Thorp JA, Rushing RS. Umbilical cord blood gas analysis.Obstet Gynecol ClinNorthAm.1999;26(4):695-709.266. BlicksteinI,GreenT.Umbilicalcordbloodgases.ClinPerinatol.2007;34(3):451-9.267. YehP,EmaryK, ImpeyL. The relationshipbetweenumbilical cordarterialpHand serious adverse neonatal outcome: analysis of 51,519 consecutive validatedsamples.BJOG.2012;119(7):824-31.268. VictoryR,PenavaD,DaSilvaO,NataleR,RichardsonB.UmbilicalcordpHandbaseexcessvaluesinrelationtoadverseoutcomeeventsforinfantsdeliveringatterm.AmJObstetGynecol.2004;191(6):2021-8.269. MalinGL,MorrisRK,KhanKS.StrengthofassociationbetweenumbilicalcordpHandperinatalandlongtermoutcomes:systematicreviewandmeta-analysis.BMJ.2010;340:c1471.270. Olofsson P. Determination of base excess in umbilical cord blood at birth:accessoryorexcess?AmJObstetGynecol.2015;213(3):259-61.271. UccellaS,CromiA,ColomboG,AgostiM,BoganiG,CasarinJ,etal.Predictionof fetal base excess values at birth using an algorithm to interpret fetal heart ratetracings:aretrospectivevalidation.BJOG.2012;119(13):1657-64.272. Blechner JN. Maternal-fetal acid-base physiology. Clin Obstet Gynecol.1993;36(1):3-12.273. Apgar V. A proposal for a newmethod of evaluation of the newborn infant.CurrResAnesthAnalg.1953;32(4):260-7.274. BerglundS,PetterssonH,CnattingiusS,GrunewaldC.HowoftenisalowApgarscoretheresultofsubstandardcareduringlabour?BJOG.2010;117(8):968-78.275. Thorngren-JerneckK,HerbstA.Low5-minuteApgarscore:apopulation-basedregisterstudyof1milliontermbirths.ObstetGynecol.2001;98(1):65-70.276. Ehrenstein V, Pedersen L, Grijota M, Nielsen GL, Rothman KJ, Sorensen HT.Association of Apgar score at five minutes with long-term neurologic disability andcognitive function in a prevalence study of Danish conscripts. BMC PregnancyChildbirth.2009;9:14.

122
277. IliodromitiS,MackayDF,SmithGC,PellJP,NelsonSM.Apgarscoreandtheriskof cause-specific infant mortality: a population-based cohort study. Lancet.2014;384(9956):1749-55.278. Lawn J, Shibuya K, Stein C. No cry at birth: global estimates of intrapartumstillbirths and intrapartum-related neonatal deaths. Bull World Health Organ.2005;83(6):409-17.279. Allanson E,Waqar T,White C, Tunçalp Ö, Dickinson J. Umbilical lactate as ameasureofacidosisandpredictorofneonatalrisk:asystematicreview.BJOG.2016.280. BorrutoF,ComparettoC,WegherE,TreisserA.Screeningoffoetaldistressbyassessmentofumbilicalcordlactate.ClinExpObstetGynecol.2006;33(4):219-22.281. ParisA,Maurice-Tison S, Coatleven F,Vandenbossche F,DallayD,Horovitz J.[Interestoflactatemicro-dosageinscalpandumbilicalcordincasesofabnormalfetalheart rate during labor. Prospective study on 162 patients]. J Gynecol Obstet BiolReprod(Paris).2012;41(4):324-32.282. ReifP,LakovschekI,TappaufC,HaasJ,LangU,SchollW.Validationofapoint-of-care(POC)lactatetestingdeviceforfetalscalpbloodsamplingduringlabor:clinicalconsiderations,practicalitiesandrealities.ClinChemLabMed.2014;52(6):825-33.283. Wiberg-ItzelE,LipponerC,NormanM,HerbstA,PrebensenD,HanssonA,etal.DeterminationofpHorlactateinfetalscalpbloodinmanagementofintrapartumfetaldistress:randomisedcontrolledmulticentretrial.BMJ.2008;336(7656):1284-7.284. RamanahR,MartinA,ClementM-C,MailletR,RiethmullerD.Fetalscalplactatemicrosamplingfornon-reassuringfetalstatusduringlabor:aprospectiveobservationalstudy.FetalDiagnTher.2010;27(1):14-9.285. Labrecque L, Provencal M, Caqueret A, Wo BL, Bujold E, Lariviere F, et al.CorrelationofcordbloodpH,baseexcess,andlactateconcentrationmeasuredwithaportabledevice for identifying fetal acidosis. JObstetGynaecolCan. 2014;36(7):598-604.286. IorizzoL,KlausenT,Wiberg-ItzelE,OvinF,WibergN.UseofLactateProTM2formeasurement of fetal scalp blood lactate during labor–proposing new cutoffs fornormality,preacidemiaandacidemia:across-sectionalstudy.TheJournalofMaternal-Fetal&NeonatalMedicine.2018:1-7.287. PennellCE,TracyMB.Anewmethodforrapidmeasurementoflactateinfetalandneonatalblood.AustNZJObstetGynaecol.1999;39(2):227-33.288. WangM,ChuaSC,BouhadirL,TreadwellEL,GibbsE,McGeeTM.Point‐of‐caremeasurementoffetalbloodlactate–Timetotrustanewdevice.AustNZJObstetGynaecol.2018;58(1):72-8.289. AllenRM,BowlingFG, Jeremy J.Determining the fetal scalp lactate level thatindicates the need for intervention in labour. Aust N Z J Obstet Gynaecol.2004;44(6):549-52.290. Baldari C, Bonavolonta V, Emerenziani GP, Gallotta MC, Silva AJ, Guidetti L.Accuracy,reliability, linearityofAccutrendandLactateProversusEBIOplusanalyzer.EurJApplPhysiol.2009;107(1):105-11.291. Karagiannis MH, Reniker AN, Kerl ME, Mann F. Lactate measurement as anindicatorofperfusion.Compendium.2006;28(4):287-98.292. Emmert J, editor Analytical requirements for the measurement of lactate.WorkshopreportAccusportMannheim,Germany:BoehringerMannheimGmbH;1995.

123
293. DessolleL,LebrecJ,DaraïE.Impactofdelayedarterialcordbloodsamplingforlactateassay.Neonatology.2009;95(3):224-9.294. White CR, Mok T, Doherty DA, Henderson JJ, Newnham JP, Pennell CE. Theeffectoftime,temperatureandstoragedeviceonumbilicalcordbloodgasandlactatemeasurement:arandomizedcontrolledtrial.TheJournalofMaternal-Fetal&NeonatalMedicine.2012;25(6):587-94.295. Ferguson VL, Dodson RB. Bioengineering aspects of the umbilical cord.European Journal of Obstetrics & Gynecology and Reproductive Biology.2009;144:S108-S13.296. DuerbeckNB,ChaffinDG,SeedsJW.ApracticalapproachtoumbilicalarterypHandbloodgasdeterminations.ObstetGynecol.1992;79(6):959-62.297. Westgate J, Garibaldi JM, Greene KR. Umbilical cord blood gas analysis atdelivery:atimeforqualitydata.BJOG.1994;101(12):1054-63.298. ChilindaGK,GadamaLA,StonesW.Point-of-careumbilicalarteriallactateandnewborn outcomes in a low resource setting: cohort study. BMC Res Notes.2018;11(1):477.299. Linet T, Laporte J, GueyeH, BoogG. [Microvolume dosage of lactate in cordblood for the evaluation of the neonatal well-being]. J Gynecol Obstet Biol Reprod(Paris).2002;31(4):352-7.300. MartinA,GaillardM,MiotS,RiethmullerD,SchaalJP.[Lactatemeasurementsandacid-basebalance incordblood].JGynecolObstetBiolReprod(Paris).2003;32(8Pt1):713-9.301. Racinet C, Richalet G, Corne C, Faure P, Peresse J, Leverve X. Diagnosis ofneonatal metabolic acidosis by eucapnic pH determination. Gynecol Obstet Fertil.2013;41(9):485-92.302. White CR, Doherty DA, Henderson JJ, Kohan R, Newnham JP, Pennell CE.Accuratepredictionofhypoxic-ischaemicencephalopathyatdelivery:acohortstudy.TheJournalofMaternal-Fetal&NeonatalMedicine.2012;25(9):1653-9.303. Wiberg N, Källén K, Herbst A, Olofsson P. Relation between umbilical cordblood pH, base deficit, lactate, 5‐minute Apgar score and development of hypoxicischemicencephalopathy.ActaObstetGynecolScand.2010;89(10):1263-9.304. Ayres-de-CamposD,SpongCY,ChandraharanE.FIGOconsensusguidelinesonintrapartum fetal monitoring: Cardiotocography. Int J Gynaecol Obstet.2015;131(1):13-24.305. Ayres-de-CamposD, Bernardes J. Twenty-five years after the FIGO guidelinesfortheuseoffetalmonitoring:timeforasimplifiedapproach?IntJGynaecolObstet.2010;110(1):1-6.306. Makino S, Hirai C, Takeda J, Itakura A, Takeda S. Relationship between fetalheart rate patterns and a time course for evaluation of fetal well-being:“the 30minutesrule”fordecisionofmechanicaldelivery.TaiwaneseJournalofObstetricsandGynecology.2017;56(6):788-92.307. BulkmansN,LyrenasS,HallbergG,NiklassonF.Umbilicalcordbloodsampling--atoolfordeliveryqualitycontrol?ActaObstetGynecolScand.1997;76(5):419-22.308. CrovettoF,FumagalliM,DeCarliA,BafferoGM,NozzaS,DessimoneF,etal.Obstetric risk factors forpoorneonataladaptationatbirth.The JournalofMaternal-Fetal&NeonatalMedicine.2018;31(18):2429-35.

124
309. SantoS,Ayres‐de‐CamposD,Costa‐SantosC,SchnettlerW,UgwumaduA,Da Graça LM. Agreement and accuracy using the FIGO, ACOG and NICEcardiotocography interpretation guidelines. Acta Obstet Gynecol Scand.2017;96(2):166-75.310. Gamboa SM, Giménez OR, Mancho JP, Moros ML, Sada JR, Mateo SC.DiagnosticaccuracyoftheFIGOandthe5-tierfetalheartrateclassificationsystemsinthedetectionofneonatalacidemia.AmJPerinatol.2017;34(05):508-14.311. GrahamEM,AdamiRR,McKenneySL,JenningsJM,BurdI,WitterFR.Diagnosticaccuracy of fetal heart rate monitoring in the identification of neonatalencephalopathy.ObstetGynecol.2014;124(3):507.312. CostantineMM, SaadeGR, editors. The first cesarean: roleof “fetal distress”diagnosis.SeminPerinatol;2012:Elsevier.313. HadarA,SheinerE,HallakM,KatzM,MazorM,Shoham-VardiI.Abnormalfetalheartratetracingpatternsduringthefirststageoflabor:effectonperinataloutcome.AmJObstetGynecol.2001;185(4):863-8.314. Chandraharan E, Arulkumaran S. Prevention of birth asphyxia: respondingappropriately to cardiotocograph (CTG) traces. Best Pract Res Clin Obstet Gynaecol.2007;21(4):609-24.315. Grivell RM, Alfirevic Z, Gyte GM, Devane D. Antenatal cardiotocography forfetalassessment.CochraneDatabaseSystRev.2015(9):Cd007863.316. Impey L, Reynolds M, MacQuillan K, Gates S, Murphy J, Sheil O. Admissioncardiotocography:arandomisedcontrolledtrial.Lancet.2003;361(9356):465-70.317. Freeman RK. Problems with intrapartum fetal heart rate monitoringinterpretationandpatientmanagement.ObstetGynecol.2002;100(4):813-26.318. MiresG,WilliamsF,HowieP.RandomisedcontrolledtrialofcardiotocographyversusDopplerauscultationof fetalheartatadmission in labour in lowriskobstetricpopulation.BMJ.2001;322(7300):1457-60;discussion60-2.319. Dellinger EH, Boehm FH, Crane MM. Electronic fetal heart rate monitoring:earlyneonataloutcomesassociatedwithnormal rate, fetal stress,and fetaldistress.AmJObstetGynecol.2000;182(1Pt1):214-20.320. Ribak R, Harlev A, Ohel I, Sergienko R, Wiznitzer A, Sheiner E. Refusal ofemergency caesarean delivery in cases of non-reassuring fetal heart rate is anindependent risk factor for perinatal mortality. European Journal of Obstetrics &GynecologyandReproductiveBiology.2011;158(1):33-6.321. Larma JD, Silva AM, Holcroft CJ, Thompson RE, Donohue PK, Graham EM.Intrapartumelectronicfetalheartratemonitoringandtheidentificationofmetabolicacidosis and hypoxic-ischemic encephalopathy. Am J Obstet Gynecol.2007;197(3):301.e1-8.322. Vintzileos AM, Nochimson DJ, Antsaklis A, Varvarigos I, Guzman ER, KnuppelRA. Comparison of intrapartum electronic fetal heart rate monitoring versusintermittent auscultation in detecting fetal acidemia at birth. Am J Obstet Gynecol.1995;173(4):1021-4.323. Georgieva A, Redman CW, Papageorghiou AT. Computerized data‐driveninterpretationoftheintrapartumcardiotocogram:acohortstudy.ActaObstetGynecolScand.2017;96(7):883-91.

125
324. NunesI,Ayres-de-CamposD,UgwumaduA,AminP,BanfieldP,NicollA,etal.Central Fetal Monitoring With and Without Computer Analysis. Obstet Gynecol.2017;129(1):83-90.325. Brocklehurst P, Field D, Greene K, Juszczak E, Keith R, Kenyon S, et al.Computerisedinterpretationoffetalheartrateduringlabour(INFANT):arandomisedcontrolledtrial.TheLancet.2017;389(10080):1719-29.326. HendrixNW,ChauhanSP.Cesareandeliveryfornonreassuringfetalheartratetracing.ObstetGynecolClinNorthAm.2005;32(2):273-86,ix.327. KuhnertM,SchmidtS. Intrapartummanagementofnonreassuring fetalheartrate patterns: a randomized controlled trial of fetal pulse oximetry. Am J ObstetGynecol.2004;191(6):1989-95.328. Elimian A, Lawlor P, Figueroa R, Wiencek V, Garry D, Quirk JG. Intrapartumassessment of fetal well-being: any role for a fetal admission test? J Matern FetalNeonatalMed.2003;13(6):408-13.329. OlofssonP,NorénH,CarlssonA,RosénKG.IdentifyingnewbornswithumbilicalcordbloodmetabolicacidosisbyintrapartumcardiotographycombinedwithfetalECGST analysis (STAN): comparison of the new and old FIGO systems to classifycardiotocograms. The Journal of Maternal-Fetal & Neonatal Medicine. 2018(just-accepted):1-11.330. GarabedianC,ButruilleL,DrumezE,SchreiberES,BartoloS,BleuG,etal.Inter-observerreliabilityof4fetalheartrateclassifications.Journalofgynecologyobstetricsandhumanreproduction.2017;46(2):131-5.331. RhöseS,HeinisAM,VandenbusscheF,DrongelenJ,DillenJ.Inter‐andintra‐observer agreement of non‐reassuring cardiotocography analysis and subsequentclinicalmanagement.ActaObstetGynecolScand.2014;93(6):596-602.332. BlixE,OianP.Interobserveragreementsinassessing549laboradmissiontestsafterastandardizedtrainingprogram.ActaObstetGynecolScand.2005;84(11):1087-92.333. FiguerasF,AlbelaS,BoninoS,PalacioM,BarrauE,HernandezS,etal.Visualanalysisofantepartum fetalheart rate tracings: inter-and intra-observeragreementandimpactofknowledgeofneonataloutcome.JPerinatMed.2005;33(3):241-5.334. HolcroftCJ,GrahamEM,Aina-MumuneyA,RaiKK,HendersonJL,PenningDH.Cordgasanalysis,decision-to-deliveryinterval,andthe30-minuteruleforemergencycesareans.JPerinatol.2005;25(4):229-35.335. BlixE,SviggumO,KossKS,OianP.Inter-observervariationinassessmentof845labouradmissiontests:comparisonbetweenmidwivesandobstetriciansintheclinicalsettingandtwoexperts.BJOG.2003;110(1):1-5.336. ChauhanSP,KlauserCK,WoodringTC,SandersonM,MagannEF,MorrisonJC.Intrapartum nonreassuring fetal heart rate tracing and prediction of adverseoutcomes:interobservervariability.AmJObstetGynecol.2008;199(6):623.e1-5.337. Kundu S, Kuehnle E, Schippert C, von Ehr J, Hillemanns P, Staboulidou I.EstimationofneonataloutcomearterypHvalueaccordingtoCTGinterpretationofthelast 60 min before delivery: a retrospective study. Can the outcome pH value bepredicted?ArchGynecolObstet.2017;296(5):897-905.338. Parer J, King T, Flanders S, FoxM, Kilpatrick S. Fetal acidemia and electronicfetalheartratepatterns:isthereevidenceofanassociation?TheJournalofMaternal-Fetal&NeonatalMedicine.2006;19(5):289-94.

126
339. Williams KP, Galerneau F. Intrapartum fetal heart rate patterns in thepredictionofneonatalacidemia.AmJObstetGynecol.2003;188(3):820-3.340. MilsomI,LadforsL,ThiringerK,NiklassonA,OdebackA,ThornbergE.Influenceofmaternal,obstetricandfetalriskfactorsontheprevalenceofbirthasphyxiaatterminaSwedishurbanpopulation.ActaObstetGynecolScand.2002;81(10):909-17.341. Trochez RD, Sibanda T, Sharma R, Draycott T. Fetal monitoring in labor: areaccelerationsgoodenough?JMaternFetalNeonatalMed.2005;18(5):349-52.342. TharmaratnamS.Fetaldistress.BaillieresBestPractResClinObstetGynaecol.2000;14(1):155-72.343. Schifrin BS. The CTG and the timing and mechanism of fetal neurologicalinjuries.BestPractResClinObstetGynaecol.2004;18(3):437-56.344. Williams KP, Galerneau F. Fetal heart rate parameters predictive of neonataloutcomeinthepresenceofaprolongeddeceleration.ObstetGynecol.2002;100(5Pt1):951-4.345. Han JY, Nava-Ocampo AA. Fetal heart rate response to cordocentesis andpregnancy outcome: a prospective cohort. J Matern Fetal Neonatal Med.2005;17(3):207-11.346. ChuangJ,ChouCT,ChengWC,HuangLW,HwangJL,TsaiYL.Spontaneousfetalheart rate deceleration: an ominous sign for fetal outcome. Arch Gynecol Obstet.2004;269(4):254-8.347. Strachan BK, Sahota DS, van Wijngaarden WJ, James DK, Chang AM.Computerised analysis of the fetal heart rate and relation to acidaemia at delivery.BJOG.2001;108(8):848-52.348. Agrawal SK, Doucette F, Gratton R, Richardson B, Gagnon R. Intrapartumcomputerized fetal heart rate parameters and metabolic acidosis at birth. ObstetGynecol.2003;102(4):731-8.349. Kazandi M, Sendag F, Akercan F, Terek MC, Gundem G. Different types ofvariable decelerations and their effects to neonatal outcome. Singapore Med J.2003;44(5):243-7.350. WilliamsKP,GalerneauF.Comparisonof intrapartumfetalheartratetracingsinpatientswithneonatalseizuresvs.noseizures:whatarethedifferences?JPerinatMed.2004;32(5):422-5.351. BorrutoF,ComparettoC,TreisserA.Preventionofcerebralpalsyduringlabour:roleoffoetallactate.ArchGynecolObstet.2008;278(1):17-22.352. Amer-WahlinI,IngemarssonI,MarsalK,HerbstA.FetalheartratepatternsandECG ST segment changes preceding metabolic acidaemia at birth. BJOG.2005;112(2):160-5.353. SonciniE,PaganelliS,VezzaniC,GarganoG,GiovanniBattistaLS. Intrapartumfetalheartratemonitoring:evaluationofastandardizedsystemof interpretationforpredictionofmetabolicacidosisatdeliveryandneonatalneurologicalmorbidity.TheJournalofMaternal-Fetal&NeonatalMedicine.2014;27(14):1465-9.354. CahillAG,CaugheyAB,RoehlKA,OdiboAO,MaconesGA.Terminalfetalheartdecelerationsandneonataloutcomes.ObstetGynecol.2013;122(5):1070-6.355. Jonsson M, Ågren J, Nordén-Lindeberg S, Ohlin A, Hanson U. Neonatalencephalopathy and the association to asphyxia in labor. Am J Obstet Gynecol.2014;211(6):667.e1-.e8.

127
356. Galazios G, Tripsianis G, Tsikouras P, Koutlaki N, Liberis V. Fetal distressevaluation using and analyzing the variables of antepartum computerizedcardiotocography.ArchGynecolObstet.2010;281(2):229-33.357. Ghi T, Morganelli G, Bellussi F, Rucci P, Giorgetta F, Rizzo N, et al.Cardiotocographicfindingsinthesecondstageoflaboramongfetusesdeliveredwithacidemia:acomparisonoftwoclassificationsystems.EuropeanJournalofObstetrics&GynecologyandReproductiveBiology.2016;203:297-302.358. Martí Gamboa S, Lapresta Moros M, Pascual Mancho J, Lapresta Moros C,CastánMateoS.Decelerationareaandfetalacidemia.TheJournalofMaternal-Fetal&NeonatalMedicine.2017;30(21):2578-84.359. TriebwasserJE,ColvinR,MaconesGA,CahillAG.Nonreassuringfetalstatusinthe second stage of labor: fetal monitoring features and association with neonataloutcomes.AmJPerinatol.2016;33(07):665-70.360. TranquilliAL,BiaginiA,GrecoP,DiTommasoM,GiannubiloSR.Thecorrelationbetweenfetalbradycardiaareainthesecondstageoflaborandacidemiaatbirth.TheJournalofMaternal-Fetal&NeonatalMedicine.2013;26(14):1425-9.361. Cahill AG, Roehl KA, Odibo AO, Macones GA. Association and prediction ofneonatalacidemia.AmJObstetGynecol.2012;207(3):206.e1-.e8.362. GiannubiloSR,BuscicchioG,Gentilucci L,PallaGP,TranquilliAL.Decelerationarea of fetal heart rate trace and fetal acidemia at delivery: a case-control study. JMaternFetalNeonatalMed.2007;20(2):141-4.363. Cahill AG, Roehl KA, Odibo AO, Macones GA. Association of atypicaldecelerationswithacidemia.ObstetGynecol.2012;120(6):1387-93.364. Ugwumadu A. Understanding cardiotocographic patterns associated withintrapartum fetal hypoxia and neurologic injury. Best practice & research Clinicalobstetrics&gynaecology.2013;27(4):509-36.365. GarciaGS,MarianiNetoC,AraujoJuniorE,GarciaRL,NardozzaLM,MoronAF.Fetal acidemia prediction through short-term variation assessed by antepartumcomputerized cardiotocography in pregnant women with hypertension syndrome.ArchGynecolObstet.2008;278(2):125-8.366. LowJA,VictoryR,DerrickEJ.Predictivevalueofelectronicfetalmonitoringforintrapartumfetalasphyxiawithmetabolicacidosis.ObstetGynecol.1999;93(2):285-91.367. AmsumangS,WuttikonsammakitP,ChamnanP,ChuenwattanaP,PhaophanA,Mongkolchat N, et al. Association Between Intrapartum Cardiotocogram and EarlyNeonatal Outcomes in a Tertiary Hospital in Thailand. Journal of the MedicalAssociationofThailand=Chotmaihetthangphaet.2017;100(4):365-73.368. KapayaH,JacquesR,RahaimN,AnumbaD.“Doesshort-termvariationinfetalheart rate predict fetal acidaemia?” A systematic review and meta-analysis. TheJournalofMaternal-Fetal&NeonatalMedicine.2016;29(24):4070-7.369. HolzmannM,WretlerS,CnattingiusS,NordströmL.Cardiotocographypatternsandriskofintrapartumfetalacidemia.JPerinatMed.2015;43(4):473-9.370. De Los Santos-GarateA,Villa-GuillenM,Villanueva-GarciaD,Vallejos-RuizM,Murguia-Peniche M. Perinatal morbidity and mortality in late-term and post-termpregnancy. NEOSANO perinatal network's experience in Mexico. J Perinatol.2011;31(12):789.

128
371. AdamY,MwinyogleeJ,MasukuB,NicolaouE.Anevaluationoftheindicationsfor caesarean sections at Chris Hani Baragwanath Academic Hospital. S Afr J ObstetGynaecol.2018;24(1):8-11.372. Makhanya V, Govender L, Moodley J. Utility of the Robson Ten GroupClassification System to determine appropriateness of caesarean section at a ruralregionalhospitalinKwaZulu-Natal,SouthAfrica.SAfrMedJ.2015;105(4):292-5.373. BenzouinaS,BoubkraouiMelM,MrabetM,ChahidN,KharbachA,El-HassaniA, et al. Fetal outcome in emergency versus elective cesarean sections at SouissiMaternityHospital,Rabat,Morocco.PanAfrMedJ.2016;23:197.374. OettleCA,OdendaalHJ.Umbilicalarterybloodgases innewbornsofhigh-riskmothers delivered within 6 hours of antenatal fetal heart monitoring. S Afr Med J.2000;90(7):705-6.375. van Bogaert LJ, Misra A. Neonatal outcome after caesarean birth for fetaldistressand/ormeconiumstaininginaSouthAfricanruralsetting.JObstetGynaecol.2008;28(1):56-9.376. Hofmeyr GJ, Kulier R. Operative versus conservative management for'fetaldistress' in labour.TheCochranedatabaseof systematic reviews.2012(6):CD001065-CD.377. Roy KK, Baruah J, Kumar S, Deorari AK, Sharma JB, Karmakar D. Cesareansectionforsuspectedfetaldistress,continuousfetalheartmonitoringanddecisiontodeliverytime.IndianJPediatr.2008;75(12):1249-52.378. ShiekhSM,KamruddinA,SetnaF,RiazT.Roleofpathologicalcardiotocographyinevaluatingfetalwell-being.JCollPhysiciansSurgPak.2006;16(6):404-7.379. Adanikin AI, Awoleke JO. Clinical suspicion, management and outcome ofintrapartum foetal distress in a public hospital with limited advanced foetalsurveillance.TheJournalofMaternal-Fetal&NeonatalMedicine.2017;30(4):424-9.380. GangwarR,ChaudharyS.CaesareanSectionforFoetalDistressandCorrelationwith Perinatal Outcome. The Journal of Obstetrics and Gynecology of India.2016;66(1):177-80.381. Perveen F, Khan A, Ali T, Rabia S. Umbilical Cord Blood pH in IntrapartumHypoxia.JCollPhysiciansSurgPak.2015;25(9):667-70.382. Ayres-de-Campos D. Introduction: why is intrapartum foetal monitoringnecessary–impact on outcomes and interventions. Best Practice & Research ClinicalObstetrics&Gynaecology.2016;30:3-8.383. ParveenS.Umbilicalcordarterialbloodbaseexcessasgoldstandardforfoetalwell being screening test validity at termdelivery. JPMAThe Journal of thePakistanMedicalAssociation.2010;60(5):347.384. Tasnim N, Mahmud G, Akram S. Predictive accuracy of intrapartumcardiotocographyintermsoffetalacidbasestatusatbirth.JCollPhysiciansSurgPak.2009;19(10):632-5.385. LawrenceER,QuarshieEL,LewisKF,PeltzmanT,AndersonFJ. IntroductionofcardiotocographmonitoringimprovesbirthoutcomesinwomenwithpreeclampsiainGhana.InternationalJournalofGynecology&Obstetrics.2016;132(1):103-4.386. Katsuragi S, Parer JT, Noda S, Onishi J, Kikuchi H, Ikeda T. Mechanism ofreduction of newborn metabolic acidemia following application of a rule-based 5-category color-coded fetal heart rate management framework. The Journal ofMaternal-Fetal&NeonatalMedicine.2015;28(13):1608-13.

129
387. GeidamAD,AuduBM, KawuwaBM,Obed JY. Rising trend and indications ofcaesarean section at the university ofMaiduguri teaching hospital, Nigeria.Ann AfrMed.2009;8(2).388. Moyer CA, Kolars CK, Oppong SA, Bakari A, Bell A, Busingye P. Predictors ofstillbirths and neonatal deaths in rural western Uganda. Int J Gynaecol Obstet.2016;134(2):190-3.389. LawrenceER,QuarshieEL,LewisKF,PeltzmanT,AndersonFJ. IntroductionofcardiotocographmonitoringimprovesbirthoutcomesinwomenwithpreeclampsiainGhana. International journal of gynaecology and obstetrics: the official organ of theInternationalFederationofGynaecologyandObstetrics.2016;132(1):103-4.390. MartisR,EmiliaO,NurdiatiDS,BrownJ.Intermittentauscultation(IA)offetalheartrateinlabourforfetalwell‐being.TheCochraneLibrary.2017.391. ErsdalHL,MdumaE,SvensenE,SundbyJ,PerlmanJ.Intermittentdetectionoffetalheartrateabnormalitiesidentifyinfantsatgreatestriskforfreshstillbirths,birthasphyxia, neonatal resuscitation, and early neonatal deaths in a limited-resourcesetting: a prospective descriptive observational study at Haydom Lutheran Hospital.Neonatology.2012;102(3):235-42.392. Adanikin AI, Awoleke JO. Clinical suspicion, management and outcome ofintrapartum foetal distress in a public hospital with limited advanced foetalsurveillance.Thejournalofmaternal-fetal&neonatalmedicine:theofficialjournalofthe European Association of PerinatalMedicine, the Federation of Asia andOceaniaPerinatalSocieties,theInternationalSocietyofPerinatalObstet.2017;30(4):424-9.393. Tomlinson J, LucasD.Decision-to-delivery interval: Is30min themagic time?Whatistheevidence?Doesitwork?BestPractice&ResearchClinicalAnaesthesiology.2017;31(1):49-56.394. White CR, Doherty DA, Henderson JJ, Kohan R, Newnham JP, Pennell CE.Benefitsof introducinguniversalumbilicalcordbloodgasandlactateanalysis intoanobstetricunit.AustNZJObstetGynaecol.2010;50(4):318-28.395. Norén H, Carlsson A. Reduced prevalence of metabolic acidosis at birth: ananalysisof establishedSTANusage in the total populationofdeliveries in a Swedishdistricthospital.AmJObstetGynecol.2010;202(6):546.e1-.e7.396. Maisonneuve E, Audibert F, Guilbaud L, Lathelize J, JousseM, Pierre F, et al.Riskfactorsforsevereneonatalacidosis.ObstetGynecol.2011;118(4):818-23.397. RacinetC,PeresseJF,RichaletG,CorneC,OuelletP.[NeonataleucapnicpHatbirth:Applicationinacohortof5392neonates].GynecolObstetFertil.2016;44(9):468-74.398. JonssonM,Agren J,Norden-LindebergS,OhlinA,HansonU.Suboptimalcareand metabolic acidemia is associated with neonatal encephalopathy but not withneonatalseizuresalone:apopulation-basedclinicalaudit.ActaObstetGynecolScand.2014;93(5):477-82.399. Williams KP, Singh A. The correlation of seizures in newborn infants withsignificant acidosis at birth with umbilical artery cord gas values. Obstet Gynecol.2002;100(3):557-60.400. HoganL, IngemarssonI,Thorngren-JerneckK,HerbstA.Howoftenisa low5-minApgarscoreintermnewbornsduetoasphyxia?EuropeanJournalofObstetrics&GynecologyandReproductiveBiology.2007;130(2):169-75.

130
401. LocatelliA,IncertiM,GhidiniA,GrecoM,VillaE,PaterliniG.Factorsassociatedwithumbilical artery acidemia in term infantswith lowApgar scores at 5min.Eur JObstetGynecolReprodBiol.2008;139(2):146-50.402. LavrijsenSW,UiterwaalCS,StigterRH,deVriesLS,VisserGH,GroenendaalF.Severe umbilical cord acidemia and neurological outcome in preterm and full-termneonates.BiolNeonate.2005;88(1):27-34.403. Ronsmans C, Cresswell JA, Goufodji S, Agbla S, Ganaba R, Assarag B, et al.CharacteristicsofneonatalnearmissinhospitalsinBenin,BurkinaFasoandMoroccoin2012-2013.TropMedIntHealth.2016;21(4):535-45.404. BonnaerensA,ThaensA,MesensT,VanHolsbekeC,DeJongeE,GyselaersW.Identificationofneonatalnearmissbysystematicscreeningformetabolicacidosisatbirth.Facts,views&visioninObGyn.2011;3(4):281.405. KerkhofsC,DeBruynC,MesensT,TheyskensC,VanhoestenbergheM,BruneelE, et al. Identification of peripartum near-miss for perinatal audit. Facts Views VisObgyn.2014;6(4):177-83.406. Jonsson M, Norden-Lindeberg S, Ostlund I, Hanson U. Metabolic acidosis atbirth and suboptimal care--illustration of the gap between knowledge and clinicalpractice.BJOG.2009;116(11):1453-60.407. MorganJL,CaseyBM,BloomSL,McIntireDD,LevenoKJ.MetabolicAcidemiainLiveBirthsat35WeeksofGestationorGreater.ObstetGynecol.2015;126(2):279-83.408. SabolBA,CaugheyAB.Acidemiainneonateswitha5-minuteApgarscoreof7orgreater-Whataretheoutcomes?AmJObstetGynecol.2016;215(4):486.e1-6.409. DaniC,BresciC,BertiE,LoriS,DiTommasoMR,PratesiS.Shorttermoutcomeof term newborns with unexpected umbilical cord arterial pH between 7.000 and7.100.EarlyHumDev.2013;89(12):1037-40.410. WibergN,KlausenTW,TyrbergT,NordströmL,Wiberg-ItzelE.Infantoutcomeat four years of age after intrapartum sampling of scalp blood lactate for fetalassessment.Acohortstudy.PLoSOne.2018;13(3):e0193887.411. NyamtemaAS,deJongAB,UrassaDP,vanRoosmalenJ.Usingaudittoenhancequality of maternity care in resource limited countries: lessons learnt from ruralTanzania.BMCPregnancyChildbirth.2011;11(1):94.412. BohrenMA,TitiloyeMA,KyaddondoD,HunterEC,OladapoOT,TunçalpÖ,etal. Defining quality of care during childbirth from the perspectives of Nigerian andUgandanwomen:Aqualitativestudy.InternationalJournalofGynecology&Obstetrics.2017;139(S1):4-16.413. VandenBroekN,GrahamW.Qualityofcareformaternalandnewbornhealth:theneglectedagenda.BJOG.2009;116(s1):18-21.414. OladapoOT,SouzaJP,BohrenMA,TunçalpÖ,VogelJP,FawoleB,etal.WHOBetterOutcomesinLabourDifficulty(BOLD)project: innovatingtoimprovequalityofcarearoundthetimeofchildbirth.Reproductivehealth.2015;12(1):48.415. LawnJE,BlencoweH,OzaS,YouD,LeeAC,WaiswaP,etal.EveryNewborn:progress, priorities, and potential beyond survival. The Lancet. 2014;384(9938):189-205.416. BohrenMA,OladapoOT,TunçalpÖ,WendlandM,VogelJP,TikkanenM,etal.Formative research and development of innovative tools for “Better Outcomes inLabourDifficulty”(BOLD):studyprotocol.Reproductivehealth.2015;12(1):50.

131
417. Adeniran A, Likaka A, Knutsson A, Costello A, Daelmans B, Maliqi B, et al.Leadership, action, learning and accountability to deliver quality care for women,newbornsandchildren.BullWorldHealthOrgan.2018;96(3):222.418. WilundaC,PutotoG,DallaRivaD,ManentiF,AtzoriA,CaliaF,etal.Assessingcoverage,equityandqualitygapsinmaternalandneonatalcareinsub-saharanAfrica:anintegratedapproach.PLoSOne.2015;10(5):e0127827.419. TraversCP,CarloWA.HowtoSave1MillionLivesinaYearinLow-andMiddle-IncomeCountries.Neonatology.2017;111(4):431-6.420. Group SAEDCW. Every death counts: use ofmortality audit data for decisionmakingtosavethelivesofmothers,babies,andchildreninSouthAfrica.TheLancet.2008;371(9620):1294-304.421. Pirkle CM, Dumont A, Traore M, Zunzunegui M-V. Validity and reliability ofcriterionbasedclinicalaudit toassessobstetricalqualityofcare inWestAfrica.BMCPregnancyChildbirth.2012;12(1):118.422. LindmarkG,Langhoff-RoosJ,editors.Regionalqualityassessment inperinatalcare.SeminNeonatol;2004:Elsevier.423. Mancey-Jones M, Brugha RF. Using perinatal audit to promote change: areview.HealthPolicyPlan.1997;12(3):183-92.424. Nakibuuka V, Okong P,Waiswa P, Byaruhanga R. Perinatal death audits in aperi-urbanhospitalinKampala,Uganda.AfrHealthSci.2012;12(4):435-42.425. YoungP,HamiltonR,HodgettS,MossM,RigbyC,JonesP,etal.Reducingriskbyimprovingstandardsofintrapartumfetalcare.JRSocMed.2001;94(5):226-31.426. Mant J. Process versus outcome indicators in the assessment of quality ofhealthcare.IntJQualHealthCare.2001;13(6):475-80.427. TunçalpÖ,HindinMJ,Adu‐BonsaffohK,AdanuRM.Assessmentofmaternalnear‐miss and quality of care in a hospital‐ based study in Accra, Ghana.InternationalJournalofGynecology&Obstetrics.2013;123(1):58-63.428. BuchmannE.Towardsgreatereffectivenessofperinataldeathaudit in low‐andmiddle‐incomecountries.BJOG.2014;121:134-6.429. DonabedianA.Evaluating thequalityofmedical care.TheMilbankQuarterly.2005;83(4):691-729.430. Merali HS, Lipsitz S, HeveloneN, Gawande AA, Lashoher A, Agrawal P, et al.Audit-identified avoidable factors in maternal and perinatal deaths in low resourcesettings:asystematicreview.BMCPregnancyChildbirth.2014;14(1):280.431. Browne JL, vanNievelt SW, Srofenyoh EK,GrobbeeDE, Klipstein-GrobuschK.Criteria-based audit of quality of care to women with severe pre-eclampsia andeclampsiainareferralhospitalinAccra,Ghana.PLoSOne.2015;10(4):e0125749.432. ElAminS,Langhoff-Roos J,BödkerB,BakrAA,AshmeigAL, IbrahimSA,etal.Introducing qualitative perinatal audit in a tertiary hospital in Sudan. Health PolicyPlan.2002;17(3):296-303.433. KodkanyBS,DermanRJ,HonnungarNV,TyagiNK,GoudarSS,MastiholiSC,etal. Establishment of aMaternal Newborn Health Registry in the BelgaumDistrict ofKarnataka,India.ReprodHealth.2015;12Suppl2:S3.434. GoudarSS,StolkaKB,Koso-ThomasM,HonnungarNV,MastiholiSC,RamadurgUY, et al. Data quality monitoring and performance metrics of a prospective,population-basedobservationalstudyofmaternalandnewbornhealthinlowresourcesettings.ReprodHealth.2015;12Suppl2:S2.

132
435. ShresthaS,SharmaA,UpadhyayS,RijalP.Perinatalmortalityaudit.NepalMedCollJ.2010;12(4):257-9.436. Barbuscia DM, Rodrigues-Júnior AL. Completeness of data on live birthcertificatesanddeath certificates forearlyneonatal and fetaldeaths in theRibeirãoPretoRegion,SãoPauloState,Brazil,2000-2007.CadSaudePublica.2011;27(6):1192-200.437. Almeida MFd, Alencar GP, Schoeps D, Minuci EG, Silva ZPd, Ortiz LP, et al.Quality of information registered on fetal deaths certificates in São Paulo,SoutheasternBrazil.RevSaudePublica.2011;45(5):845-53.438. PhillipsJ,MillumJ.Valuingstillbirths.Bioethics.2015;29(6):413-23.439. KidantoHL,MogrenI,vanRoosmalenJ,ThomasAN,MassaweSN,NystromL,etal. IntroductionofaqualitativeperinatalauditatMuhimbiliNationalHospital,DaresSalaam,Tanzania.BMCPregnancyChildbirth.2009;9(1):45.440. PattinsonRC,SayL,MakinJ,BastosMH.Criticalincidentauditandfeedbacktoimproveperinatalandmaternalmortalityandmorbidity.TheCochraneLibrary.2005.441. Kerber KJ,MathaiM, Lewis G, Flenady V, Erwich JJ, Segun T, et al. Countingeverystillbirthandneonataldeaththroughmortalityaudittoimprovequalityofcarefor every pregnantwoman and her baby.BMC Pregnancy Childbirth. 2015;15 Suppl2:S9.442. PattinsonRC,SayL,MakinJ,BastosMH.Criticalincidentauditandfeedbacktoimprove perinatal andmaternalmortality andmorbidity. The Cochrane database ofsystematicreviews.2005(4):CD002961.443. Raman S, Iljadica A, Gyaneshwar R, Taito R, Fong J. Improvingmaternal andchildhealthsystems inFiji throughaperinatalmortalityaudit. Int JGynaecolObstet.2015;129(2):165-8.444. WilkinsonD.Reducingperinatalmortalityindevelopingcountries.HealthPolicyPlan.1997;12(2):161-5.445. Stratulat P, CurteanuA, Caraus T, PetrovV,Gardosi J. The experience of theimplementationofperinatalauditinMoldova.BJOG.2014;121Suppl4:167-71.446. SpitzerRF,SteeleSJ,CaloiaD,ThorneJ,BockingAD,Christoffersen‐DebA,etal.One‐yearevaluationof the impactofanemergencyobstetricandneonatalcaretrainingprograminWesternKenya. InternationalJournalofGynecology&Obstetrics.2014;127(2):189-93.447. BurkeL,SuswardanyDL,MichenerK,MazurkiS,AdairT,ElmiyatiC,etal.Utilityof local health registers in measuring perinatal mortality: a case study in ruralIndonesia.BMCPregnancyChildbirth.2011;11(1):20.448. PashaO, SaleemS,Ali S,Goudar SS,GarcesA, Esamai F, et al.Maternal andnewbornoutcomesinPakistancomparedtootherlowandmiddleincomecountriesintheGlobalNetwork'sMaternalNewbornHealthRegistry:anactive,community-based,pregnancysurveillancemechanism.ReprodHealth.2015;12Suppl2:S15.449. Drife JO,editorPerinatalaudit in low-andhigh-incomecountries.Seminars inFetalandNeonatalMedicine;2006:Elsevier.450. NyamtemaAS,UrassaDP,PembeAB,KisangaF,vanRoosmalenJ.Factors forchange inmaternalandperinatalauditsystems inDaresSalaamhospitals,Tanzania.BMCPregnancyChildbirth.2010;10(1):29.

133
451. MusafiliA,PerssonLA,BaribwiraC,PafsJ,MulindwaPA,EssenB.CasereviewofperinataldeathsathospitalsinKigali,Rwanda:perinatalauditwithapplicationofathree-delaysanalysis.BMCPregnancyChildbirth.2017;17(1):85.452. Goodman DM, Ramaswamy R, Jeuland M, Srofenyoh EK, Engmann CM,OlufolabiAJ,etal.ThecosteffectivenessofaqualityimprovementprogramtoreducematernalandfetalmortalityinaregionalreferralhospitalinAccra,Ghana.PLoSOne.2017;12(7):e0180929.453. FlenadyV,WojcieszekAM,EllwoodD,LeisherSH,ErwichJJH,DraperES,etal.,editors.Classificationof causesandassociatedconditions for stillbirthsandneonataldeaths.SeminarsinFetalandNeonatalMedicine;2017:Elsevier.454. Belizán M, Bergh A-M, Cilliers C, Pattinson RC, Voce A. Stages of change: Aqualitative study on the implementation of a perinatal audit programme in SouthAfrica.BMCHealthServRes.2011;11(1):243.455. Tunçalp Ö, Souza J. Maternal near‐miss audits to improve quality of care.BJOG.2014;121(s4):102-4.456. Say L. Neonatal nearmiss: a potentially useful approach to assess quality ofnewborncare.JPediatr(RioJ).2010;86(1):1-2.457. Pileggi-Castro C, Camelo JS, Jr., Perdona GC, Mussi-Pinhata MM, Cecatti JG,MoriR,etal.Developmentofcriteriaforidentifyingneonatalnear-misscases:analysisoftwoWHOmulticountrycross-sectionalstudies.BJOG.2014;121Suppl1:110-8.458. NardelloDM,GuimaraesAM,BarretoID,GurgelRQ,RibeiroER,GoisCF.Fetalandneonataldeathsof childrenofpatientsclassifiedasnearmiss.RevBrasEnferm.2017;70(1):104-11.459. Chevalier MS, King CC, Ellington S, Wiener J, Kayira D, Chasela CS, et al.MaternalandneonataloutcomesamongwomenwithHIVinfectionandtheirinfantsinMalawi.IntJGynaecolObstet.2017;137(3):282-9.460. ChweneyagaeD,Delis-JarrosayN,FarinaZ,FawcusS,GodiN,KhaoleN,etal.The impact of HIV infection on maternal deaths in South Africa. S Afr J ObstetGynaecol.2012;18(3):70-6.461. WediCO,KirtleyS,HopewellS,CorriganR,KennedySH,HemelaarJ.Perinataloutcomes associated with maternal HIV infection: a systematic review and meta-analysis.LancetHIV.2016;3(1):e33-48.462. ChettyT,VandormaelA,ThorneC,CoutsoudisA.IncidentHIVduringpregnancyand early postpartum period: a population-based cohort study in a rural area inKwaZulu-Natal,SouthAfrica.BMCPregnancyChildbirth.2017;17(1):248.463. PattinsonR,HulsbergenM,VanHoorickL.TheeffectofmaternalHIVinfectiononmaternal conditions and perinatal deaths in southwest Tshwane. Facts, views &visioninObGyn.2010;2(4):227.

134
CHAPTERTHREE:THESISOUTLINEANDMETHODOLOGYOFTHE
RESEARCH

135
THESISOUTLINE
This thesis is centredon twodata set analyses, a systematic reviewand two clinical
trials.
Bothclinicaltrialswereconductedin2014.Thefirstofwhichwasabeforeandafter
trial, conducted at KalafongHospital, Pretoria, South Africa (Image 3.1). The second
was an implementation research trial, conducted at Zithulele Hospital, South Africa.
Thedesignofeachofthesestudiesisoutlinedbelow.Themethodsforthebeforeand
afterstudyarerelevantforthemanuscriptsinChapters7-9,andthemethodsforthe
implementationtrialarerelevantforChapter10.
Image3.1:KalafongHospitalbynight,2014

136
Thedataforthesetrialsweresupportedbyalargescaleretrospectivecohortstudyof
thecausesofperinatalmortalityinSouthAfrica(Chapter4),asystematicreviewand
meta-analysisofthediagnostictestaccuracyoflactate(Chapter5),andtheimpactof
largescaleperinatalaudit(Chapter6).

137
OUTLINEOFTHERESEARCHINCHAPTERFOUR
The research relevant to this thesis was predominantly based in South Africa. As
outlined below, the clinical trials conducted were specific to two South African
hospitals.Thepotentialapplicabilityoftheresearchinthelongtermwasanimportant
consideration from thebeginningof this thesis. Therefore, itwas critical to consider
thecausesofperinatalmortalityinSouthAfricaasawhole.Themostaccuratemethod
ofexecutingthiswaswithananalysisofdatafromonespecificprovince,Mpumalanga.
Mpumalanga is the second smallest province in South Africa, covering an area of
76,495squarekilometres,withapopulationof4,039,939asatthelastcensus(2011).
Mpumalangaisuniqueinthatallpublicobstetricfacilitiesintheprovincecollectdata
on every birth and death using the Perinatal Problems Identification Program (PPIP)
(version3)asoutlinedinChapter2.
AIM
TodeterminethecausesofperinatalmortalityinSouthAfrica

138
METHODOLOGY
A retrospective analysis of the PPIP database from 1st October 2013 to 31st January
2014,inclusive,wasundertaken
INCLUSIONCRITERIA
- Late fetaldeaths (babiesweighing1000gror≥28weeksgestation)andearly
neonataldeaths(deathsupto7daysofneonatallife).
DATAEXTRACTED
- Foreachindividualdeath,thefollowingdatawereextracted:
o Maternalage
o Parity
o SyphilisandHIVstatus
o Gestationalage
o BirthweightforgestationusingcountryspecificTheroncharts
o Certaintyoruncertaintyofgestation
o Conditionofthenew-born(bornaliveandearlyneonataldeath(ENND),
freshstillborn,maceratedstillborn)
o Primaryobstetriccauseofdeath(allcases)
o Primaryneonatalcauseofdeath(ENNDs).
o Maternalconditionspresentatthetimeofdeath

139
o Avoidablefactorsidentifiedineachdeath
Weexaminedthefrequenciesofmaternalandfetalorneonatalcharacteristicsinlate
fetal deaths and analysed the relationship betweenmaternal condition and fetal or
neonatal outcomes. IBM SPSS Statistics 22.0 was used for data analysis. Frequency
distributionswereperformedforoutcomesummaries.Fisher’sexacttestonbivariate
correlationwasusedtointerrogatetherelationshipbetweenmaternalconditionsand
obstetriccausesofdeathandthetimingoflateperinataldeath.Analysisoutcomesare
summarisedusing risk ratios and95%confidence intervals.All testswere two tailed
andp-values<0.05wereconsideredsignificant.
ETHICS
ThePPIPprogramhasethical approval from theUniversityofPretoria. Thedataare
collected with permission from the South African Department of Health. All public
obstetricfacilitiesinSouthAfricahavebeenmandatedtousethePPIPprogramsince
2012.All data is deidentifiedprior to entry in thePPIPdatabase. ThePPIP technical
task teamapproved this secondaryanalysis.TheMpumalangaDepartmentofHealth
grantedpermissionforanalysisandpublicationoftheProvince’sPPIPdata.

140
OUTLINEOFTHERESEARCHINCHAPTERFIVE
Chapterfiveisasystematicreviewofthediagnostictestaccuracyofumbilicallactate
in the setting of acidosis and neonatal outcomes. The protocol for this review is
outlinedbelow.
OBJECTIVESOFTHEREVIEW
1. Tocompareumbilicallactatewithotherassessmentsofacidosis(pH,base
excess,pO2,pCO2)throughcorrelationforthemeasuringtheoutcomeof
acidosis
2. Tocomparethesensitivityandspecificityofumbilicalarterylactatewithother
assessmentsofacidosisinpredictingneonataloutcomes
CRITERIAFORCONSIDERINGSTUDIESINTHEREVIEW
GENERALINCLUSION/EXCLUSIONCRITERIA
All identified studies, irrespective of language, published orwritten from1990-2013
willbeassessed.
Exclusioncriteria:

141
- Studiesoutsidetheinclusiondates
- Studieswithnodataavailable
TYPEOFSTUDYDESIGNSFORDIAGNOSTICTESTACCURACY
Theidealstudydesignfordiagnostictestperformanceiscross-sectionalwherethetest
isperformedonconsecutivelyassessedpatientsiscross-classifiedwithdiseasestatus
andareferencetest.Althoughlessideal,randomisedcontroltrialsthatusepreviously
independentlyassessedtestswillalsobeconsidered.
TYPEOFPARTICIPANTS
Women delivering in a facility with the ability to undertake an assessment of fetal
acidosisandneonatalriskandneonatesintheimmediatepost-deliveryperiod
TYPEOFOUTCOMES
Acidosis (defined by the study being assessed); typically pH <7.2 or <7.15, BE <15,
p02<10,pCO2>70(1)
Neonatal risk / outcome (defined by the study); potentially APGAR scores <7 at 5
minutes, admission to the neonatal intensive care nursery, need for neonatal
resuscitation,diagnosisofhypoxicischaemicencephalopathy

142
SEARCHSTRATEGYFORIDENTIFICATIONOFSTUDIES
Thereviewwillhaveno languagerestrictions.ReviewerswillbeabletoreadEnglish,
IndonesianandFrench.AnassociatedresearcherwillreadreviewsinTurkish.Reports
inotherlanguageswillbetranslatedintoEnglish.Thereviewwillcoverpublishedand
unpublishedstudiesfrom1990-2013
Electronic databases that will be search are: PubMed/Medline, CINAHL, EMBASE.
Search strategieswill be customised to the subject heading and search structure of
individualdatabases.
Otherelectronicsearching:Aninternetsearchusing“GoogleScholar”searchingengine
withtheterms“lactate”,“fetalacidosis”,“predict*neonatalrisk”
Handsearching:Referencelistsfromreviewarticleswillbesearched.
Initially a comprehensive search to identify existing systematic reviews was
undertakenusingtheHuntandMcKibbonmethod
1. Meta-analysis(pt)
2. Meta-anal:(tw)
3. Metaanal:(tw)
4. Quantitative:review:ORquantitative:overview:(tw)
5. Systematic:review:ORsystematic:overview:(tw)
6. Methodological:review:ORmethodologic:overview:(tw)
7. Review(pt)ANDmedline(tw)
8. 1OR2OR3OR4OR5OR6OR7

143
Contenttermswerethenaddedwithmedlineexplosion
TW: fetal; neonatal; risk; lactate; intrapartum; umbilical; acidosis; asphyxia; labour;
fetal;cord;lacticacid;outcome
Contentterms:fetal;neonatal;risk;lactate;intrapartum;umbilical;acidosis;asphyxia;
outcomes
Usingthismethod,therewerenorelevantexistingsystematicreviewsidentified
CUSTOMISEDSEARCHSTRATEGY:
PubMed/Medlinesearchstrategy:
The lists the MeSH Terms (Medline Subject Headings) and keywords for the three
concepts:UmbilicalArtery;Lactate;NeonatalRisk/Outcome
Notes:
Removing“FetalBlood”anditsvariantsremovesmanyresultsrelatingto“fetalscalp
blood”.Although“FetalBlood”isthepreferredMESHtermforCordBloodorUmbilical
CordBlood
AddingthefollowingsearchstringwithinPubMedremovesreferencesthatarereferto
animalsandnothumans.
NOT(“animals”[MESHTerms]NOT“humans”[MESHTerms])
ConceptswithMESHTermsandKeywords

144
UmbilicalArteryConcept
"umbilicalarteries"[MeSHTerms]
“umbilicalartery”
“umbilicalarteries”
"umbilicalcord"[MeSHTerms]
"umbilicalcordblood"
“umbilicalcordartery”
“cordblood”
"fetalblood"[MeSHTerms]
"fetalblood"
“foetalblood”
("umbilical arteries"[MeSH Terms] OR “umbilical artery” OR “umbilical arteries” OR
"umbilicalcord"[MeSHTerms]OR"umbilicalcordblood"OR“umbilicalcordartery”OR
“cordblood”OR"fetalblood"[MeSHTerms]OR"fetalblood"OR“foetalblood”)
WithoutFetalBlood
("umbilical arteries"[MeSH Terms] OR “umbilical artery” OR “umbilical arteries” OR
"umbilicalcord"[MeSHTerms]OR"umbilicalcordblood"OR“umbilicalcordartery”OR
“cordblood”)

145
LactateConcept
"lacticacid"[MeSHTerms]
"lacticacid"
"lactates"[MeSHTerms]
lactate
lactates
"acidosis,lactic"[MESHTerms]
“lacticacidosis”
("lacticacid"[MeSHTerms]OR"lacticacid"OR"lactates"[MeSHTerms]ORlactateOR
lactatesOR"acidosis,lactic"[MESHTerms]OR“lacticacidosis”)
NeonatalRisk/OutcomeConcept
"neonataloutcome"
"neonataloutcomes”
(("infant,newborn"[MESHTerms]ORneonat*)AND"riskfactors"[MESHTerms])
“FetalHypoxia”[MESH]
“fetalhypoxia”

146
“foetalhypoxia”
AsphyxiaNeonatorum[MESH]
“birthasphyxia”
"fetalasphyxia"
"foetalasphyxia"
“intrapartumhypoxia”
"intrapartumfetalasphyxia"
“intrapartumstillbirths”
“intrapartum-linkedneonataldeaths”
"PerinatalMortality"[MeSHTerms](2008+)
“perinatalmortality”
“perinatalmorbidity”
“Neonatalnearmiss”
“InfantMortality[MESH]”(UsedforPerinatalMortality1990-2007)
“Neonatalmortality”
"APGARscore"[MeSHTerms]
“APGARscore”
"fetaldistress"[MeSHTerms]

147
“fetaldistress”
“foetaldistress”
"Infant,newborn,diseases/mortality"[MeshTerms]
"RespiratoryDistressSyndrome,Newborn"[MeSHTerms]
("neonatal outcome"OR "neonatal outcomes"OR (("infant, newborn"[MESH Terms]
OR neonat*) AND "risk factors"[MESH Terms]) OR “Fetal Hypoxia”[MESH Terms]OR
“fetal hypoxia” OR “foetal hypoxia” OR “Asphyxia Neonatorum”[MESH Terms] OR
“birthasphyxia”OR"fetalasphyxia"OR"foetalasphyxia"OR“intrapartumhypoxia”OR
"intrapartum fetal asphyxia" OR “intrapartum stillbirths” OR “intrapartum-linked
neonataldeaths”OR"PerinatalMortality"[MeSHTerms]OR“perinatalmortality”OR
“perinatalmorbidity”OR“Neonatalnearmiss”OR“InfantMortality”[MESHTerms]OR
“Neonatal mortality” OR "APGAR score"[MeSH Terms] OR “APGAR score” OR "fetal
distress"[MeSH Terms]OR “fetal distress”OR “foetal distress”OR "Infant, newborn,
diseases/mortality"[Mesh Terms] OR "Respiratory Distress Syndrome,
Newborn"[MeSHTerms])
DescriptionsofMeSHTerms
MeSHHEADING:UMBILICALARTERIES
SCOPE: Specialized arterial vessels in the umbilical cord. They carry waste and
deoxygenated blood from the FETUS to the mother via the PLACENTA. In humans,
thereareusuallytwoumbilicalarteriesbutsometimesone.

148
YEARofENTRY:68(64)
PREVIOUSINDEXING:UmbilicalCord/BS(1966-1967)
UsedFor:
umbilicalartery
arteryumbilical
umbilicalarteries
arteriesumbilical
MeSHHEADING:UMBILICALCORD
SCOPE: The flexible rope-like structure that connects a developing FETUS to the
PLACENTA in mammals. The cord contains blood vessels, which carry oxygen and
nutrientsfromthemothertothefetusandwasteproductsawayfromthefetus.
NOTE:CORDBLOODseeFETALBLOODisavailable
UsedFor:
cordumbilical
umbilicalcords
umbilicalcord
cordsumbilical
MeSHHEADING:FETALBLOOD
SCOPE: Blood of the fetus. Exchange of nutrients andwaste between the fetal and
maternal blood occurs via the PLACENTA. The cord blood is blood contained in the
umbilicalvessels(UMBILICALCORD)atthetimeofdelivery.

149
YEARofENTRY:75
PREVIOUSINDEXING:UmbilicalCord(1966-1974)
UsedFor:
bloodsfetal
cordblood
bloodfetal
cordbloodumbilical
bloodscord
fetalbloods
bloodcord
umbilicalcordbloods
umbilicalcordblood
cordbloodsumbilical
cordbloods
bloodsumbilicalcord
bloodumbilicalcord
fetalblood
MeSHHEADING:LACTATES
SCOPE:SaltsorestersofLACTICACIDcontainingthegeneralformulaCH3CHOHCOOR.
NOTE:donotconfusewithLACTATEseeLACTICACID
UsedFor:
lactates

150
MeSHHEADING:LACTICACID
SCOPE:Anormal intermediate in the fermentation (oxidation,metabolism)of sugar.
The concentrated form is used internally to prevent gastrointestinal fermentation.
(FromStedman,26thed)
NOTE:donotconfuseXrefLACTATEwithLACTATES
YEARofENTRY:97;wasLACTICACID(NM)1981-96
SEARCHNOTE:useLACTICACID(NM)tosearchLACTICACID1981-96
PREVIOUSINDEXING:Lactates(1981-1996)
MeSHHEADING:ACIDOSIS,LACTIC
SCOPE: Acidosis caused by accumulation of lactic acid more rapidly than it can be
metabolized. It may occur spontaneously or in association with diseases such as
diabetesmellitus,leukemia,orliverfailure.
NOTE:accumulationoflacticacid
YEARofENTRY:87
PREVIOUSINDEXING:Acidosis(1966-1986);Lactates(1966-1986)
UsedFor:
acidosislactic
lacticacidosis
MeSHHEADING:ASPHYXIANEONATORUM
SCOPE:Respiratoryfailureinthenewborn.(Dorland,27thed)

151
NOTE: do not use /congen & do not coord with INFANT, NEWBORN, DISEASES; tag
INFANT,NEWBORN
REFERENCES:
UsedFor:
asphyxianeonatorum
MeSHHEADING:FETALHYPOXIA
SCOPE:DeficientoxygenationofFETALBLOOD.
NOTE:donotconfusewithASPHYXIANEONATORUM
YEARofENTRY:2006(1975)
PREVIOUSINDEXING:FetalDiseases(1966-1974)
UsedFor:
hypoxiafetal
fetalanoxia
anoxiafetal
fetalhypoxia
MeSHHEADING:INFANTMORTALITY
SCOPE: Postnatal deaths from BIRTH to 365 days after birth in a given population.
Postneonatalmortalityrepresentsdeathsbetween28daysand365daysafterbirth(as
definedbyNationalCenterforHealthStatistics).Neonatalmortalityrepresentsdeaths
frombirthto27daysafterbirth.
UsedFor:

152
infantmortality
mortalitiesinfant
neonatalmortalities
infantmortalities
neonatalmortality
mortalityneonatal
postneonatalmortality
mortalityinfant
mortalitiesneonatal
MeSH HEADING: PERINATAL MORTALITY (Note: Used from 2008+; Infant Mortality
usedpriortothis)
SCOPE:Deathsoccurringfromthe28thweekofGESTATIONtothe7thdayafterbirth.
NOTE: a statistical concept and not a substitute for /mortal with FETAL DISEASES;
INFANT,NEWBORN,DISEASESorspecificdisease;specifygeographyifpertinent
YEARofENTRY:2008;useINFANTMORTALITY1990-2007
PREVIOUSINDEXING:InfantMortality(1965-2007)
REFERENCES:
SeeRelated:
INFANTMORTALITY
UsedFor:
mortalitiesperinatal
perinatalmortality

153
perinatalmortalities
mortalityperinatal
MeSHHEADING:FETALDISTRESS
SCOPE:Anonreassuringfetalstatus(NRFS) indicatingthattheFETUSiscompromised
(American College of Obstetricians and Gynecologists 1988). It can be identified by
sub-optimal values in FETAL HEART RATE; oxygenation of FETAL BLOOD; and other
parameters.
NOTE:donotconfusewithRESPIRATORYDISTRESSSYNDROME,NEWBORN(postnatal)
MeSHHEADING:RESPIRATORYDISTRESSSYNDROME,NEWBORN
SCOPE:AconditionofthenewbornmarkedbyDYSPNEAwithCYANOSIS,heraldedby
suchprodromalsignsasdilatationofthealaenasi,expiratorygrunt,andretractionof
the suprasternal notch or costal margins, mostly frequently occurring in premature
infants, childrenof diabeticmothers, and infants deliveredby cesarean section, and
sometimeswithnoapparentpredisposingcause.
Customisedsearchstrategy:
Embasesearchstrategy:
SubjectHeadings
ThefollowingareSubjectTermsusedwithinEmbase:
MAINTERM:umbilicalartery

154
UsedFor:
allantoicartery
arteriaumbilicalis
springleumbilicalartery
umbilicalarteries
umbilicalartery,persisting
umbilicalcordartery
umbilicusartery
MAINTERM:umbilicalcordblood
UsedFor:
blood,umbilical
cordblood
cordblood,umbilical
umbilicalblood
umbilicalcordfluid
umbilicalcordplasma
MAINTERM:LacticAcid
MAINTERM:lactatebloodlevel
UsedFor:
bloodlactate
bloodlacticacid

155
lactateplasmalevel
lactateserumlevel
lacticacidbloodlevel
lacticacidserumlevel
plasmalactate
plasmalacticacid
serumlactate
serumlacticacid
MAINTERM:lacticacidosis
UsedFor:
acidosis,lactic
acidosis,lacticacid
congenitallacticacidosis
lactacidosis
lactateacidosis
lacticacidacidosis
lacticacidosis,congenital
MAINTERM:fetusoutcome
UsedFor:
fetaloutcome
outcome,fetus
MAINTERM:perinatalmortality

156
UsedFor:
mortality,perinatal
perinataldeathrate
MAINTERM:newbornmortality
UsedFor:
mortality,neonatal
neonatalmortality
neonatalsurvival
neonatusmortality
newbornsurvival
postneonatalmortality
survival,newborn
MAINTERM:perinatalmorbidity
UsedFor:
morbidity,perinatal
perinataldisease
MAINTERM:fetusdistress
UsedFor:
distress,fetal
fetaldistress
foetaldistress

157
foetusdistress
intrauterinedistress
MAINTERM:perinatalasphyxia
UsedFor:
asphyxia,perinatal
birthasphyxia
MAINTERM:fetushypoxia
UsedFor:
fetalanoxia
fetalasphyxia
fetalhypoxemia
fetalhypoxia
fetusanoxia
fetusasphyxia
fetusasphyxiation
foetalhypoxia
foetushypoxia
hypoxia,fetus
intrauterineasphyxia
intrauterinehypoxia
MAINTERM:neonatalrespiratorydistresssyndrome
UsedFor:

158
neonatalrds
neonatalrespiratorydistress
newbornrespiratorydistress
newbornrespiratorydistresssyndrome
respiratorydistresssyndrome,newborn
respiratorydistress,newborn
METHODSOFTHEREVIEW
SCREENINGANDDATAEXTRACTIONFORMS
SCREENINGQUESTIONSFORABSTRACTANALYSIS:
SCREENINGQUESTIONS
No Yes
1 Does the report include data on umbilical artery lactate and another
methodofassessingfetalacidosis?⃝ □
2 Does the report compare the tests in either their ability to predict
acidosisortheirabilitytopredictpotentialneonatalrisk?⃝ □
3 Isthestudyacross-sectionaldesignorrandomisedcontroltrial? ⃝ □

159
4 Areacidosisand/orneonataloutcomedefined? ⃝ □
Note:Ifanyanswerfallsintoacirclethenthestudywillbeexcluded
DATAEXTRACTIONFORM:
DATAEXTRACTIONFORM
1 Studyidentificationnumber #
2 Nameofdataextractor
3 Dateofextraction __/__/__
4 Lastnameoffirstauthor
5 Countryoforigin
6 Published
7 Yearofpublication ____
8 Languageofpaper
9 Studyperiod __/__/__-__/__/__
10 Studydesign
11 Methodofsampling

160
12 Whattestsarebeingevaluated?
12 Numberofeligiblesubjects
13 Samplesizestudied
14 Whatisthestudysetting?
15 Description of the characteristics of the study
population
16 Description of the health characteristics of the
women
17 Description of the health characteristics of the
fetus
18 Is there information regarding the number of
non-validsamples
Yes/No
19 Is the incremental value of the test being
comparedtootherroutinetests?
Yes/No
20 Isthedecisiontoperformthereferencestandard
independentofthetestresult?
Yes/No
21 Ifnot,whatpercentwerenotverified __%
22 Wasthereavalidreferencestandard? Yes/No
23 Arethetestsandreferencesstandardsmeasured Yes/No

161
independently?
24 Are tests measured independently of other
clinicalandtestinformation?
Yes/No
25 If tests are being compared, have they been
assessed independently in the same patients or
doneinrandomlyallocatedpatients?
Yes/No
26 Whatistheprimaryoutcome?
27 Whattest(s)islactatecomparedto?
28 Whatistherbetweenlactateandthetest(s)?
29 What is the sensitivity and specificity of lactate
fortheoutcome?
30 What is the sensitivity and specificity of the
comparisonfortheprimaryoutcome?
MANAGEMENTOFSTUDIESANDDATAEXTRACTION
Endnote bibliographic software will be used to store the citations identified in the
search, keep track of them and delete duplicates. Electronic searches can be
downloadeddirectly in toEndnote.Reports fromothersourcescanbeentered in to
Endnote manually. Duplicates will be deleted and each study will be assigned an
identificationnumberforreview.

162
All citations identified fromtheelectronicsearchstrategieswillbeevaluated initially
withthescreeningformonthebasisoftitlesandabstracts,whereavailable.Records
notmeetingthescreeningcriteriawillbediscarded.Fulltextarticlesoftheremaining
citationswillbeobtained.Fulltextarticleswillalsobeobtainedforcitationswherethe
initial screeningcouldnotbecompletedbecauseof lackof information in the title /
abstract.Alistoftheirrelevantrecordswillbeavailableuponrequest.
The full text articleswill be evaluatedusing the screening form. Studies excludedat
thispoint in the reviewwillbe listed separately,with the reason for theirexclusion.
Data from the remaining studies will be extracted by reviewer EA using the data
extraction form.A secondand third reviewerwill be availablewhendata cannotbe
extracted from the first review and where there are queries about a manuscript.
Attempts will be made to contact authors where data is missing or requiring
clarification. Datawill bemanually entered in a database and processedwith SPSS
software.
CRITICALAPPRAISALOFSTUDIES
Includedstudieswillbe interrogated todeterminedifference in studycharacteristics
usingthedataextractionform.Therewill thenbeaqualityassessmentofstudiesby
threereviewersusingthefollowingcriteria:
- Highqualityifall4criteriaaremet
- Mediumqualityif2or3criteriaaremet

163
- Lowqualityif1ornocriteriaaremet
ADEQUATE INADEQUATE
Sampling Consecutive,random Selectgroups
Population Type and characteristic of
populationspecified
Notspecified
Followup Reportedand<20%loss Notreportedor>20%loss
Definitionofoutcome Definition of acidosis and
neonatal outcome
reported
Definition of acidosis and
neonatal outcome not
reported
Assessmentofbias:
- Hasselectionbiasbeenminimised?
o Haveconsecutivepatientsbeenenrolled?
o Studiesthatonlyincludedcaseswithconfirmedneonataloutcome(e.g.
HIE)arelikelytooverestimatesensitivityandspecificity
- Wasfollowupforprimaryoutcomesadequate?
o Wereallthoseenrolledshouldbeverifiedbythereferencestandard
(e.g.pH)
o Wereallthoseenrolledincludedintheanalysis?
o Wasthereferencestandardapplieddifferentlytothetestpositivesand
thetestnegatives?

164
- Applicability
o Howtestswereperformede.g.kitsfromdifferentmanufacturers?What
thresholdwasusedtodifferentiatepositivefromnegativetests?
- Hasmeasurementormisclassificationbiasbeenminimised?
o Wasavalidatedreferencestandardused?
o Iftestsarebeingcompared,havetheybeenassessedindependently?
o Werebothtestsdoneonthesameindividual?
ANALYSISPLAN
Twomethods of analysis are anticipated as there are likely twomodes of reported
data; those that compare lactate and other measures of acidosis (e.g. pH) using a
correlationcoefficient(r)andthosethatreportthesensitivityandspecificityoflactate
topredictneonataloutcomecomparedtoothermeasuresofacidosis.
Analysisofstudieswithcorrelationcoefficients
- Meta-analysisusingfixedandrandomeffectmodels(MonteCarlosimulation)
Analysisofstudieswithsensitivityandspecificity
- InitialsimpleplotofsensitivityandspecificitywithCI
- Thenasynthesisofstudyresultsforsensitivityandspecificitywillbedoneby
fittingasummaryROC(SROC)
o Truepositiverate(sensitivity)andthefalsepositiverate(1-specificity)
arefirsttransformedthroughthelogarithmoftheirodds
165
o Theregressionanalysisisdone
§ D=a+bS
§ D=(logitTPR)-(logitFPR)=log(oddsratio)
§ S=(logitTPR)+(logitFPR)=log(oddsproduct),whichisaproxyfor
thethreshold
§ a=estimatedlinearintercept
§ b=estimatedregressioncoefficient(slope)
§ RelationshipcanbeplottedwithDontheverticalaccessandS
onthehorizontal
o Theresultsareback-transformedandplottedinthestandardROC
format
Themanuscript of the reviewwill bewritten by EA. JanDickinson, CW and TWwill
reviewthedraftsandapprovethefinalmanuscript.
DESCRIPTIONOFSTUDIES
Atablewiththecharacteristicsoftheincludedstudieswillbepreparedcontainingthe
methods, participants, and outcomes studied. This tablewill show the studies listed
chronologicallybyyearofpublication,listedalphabeticallybythesurnameofthefirst
author.

166
OUTLINEOFTHERESEARCHINCHAPTERSIX
The South African PPIP database is a nationally supported program, which was
voluntaryfromthe1990s–2012andcompulsorythereafter,thatallowsprovidersof
perinatalcaretoenterandanalyseperinatalbirthsanddeathsandmaternaldeathsin
detail.Asof2014,94%ofhospitalcontributedatatoPPIPandmorethan73%ofbirths
inallinstitutionsarecaptured.
AIM
ToassesstheimpactoncontinuousauditusingPPIPonperinatalmortalityinallSouth
Africanobstetricunitswithatleastfiveyearsofcontinuousauditdata.
METHODOLOGY
- IdentifysitesfromthePPIPdatabasewithatleastfiveyearsofcontinuousaudit
(morethan80%compliancewithmonthlysubmissionofdata) fromthepoint
offirstusingthePPIPprogram.
- Undertake an analysis of trend in PNMR (defined as fetal deaths and early
neonatal deathsper1000births) forbirthswithweights greater than1000gr
overthefirstfiveyearsofauditinthesesites.

167
- AlldatawasanalysedusingEpiinfoversion7andSPSSversion22.Themonthly
perinatalmortalityrateforeachsiteforthefirstfiveyearswasobtained.The
datawassmoothedbyusingtwelvemonthmovingaverages.Achi-squaretest
forlineartrend(extendedMantel-Haenszel)wasundertakenoneachsite.AM2
statistic for each sitewas calculatedwith one degree of freedomwith linear
trend(eitherincreasingordecreasing)beingrelatedtothefirstPNMRratefor
eachsite (thebeginningofaudit)withtheconstraintbeingthat theratesare
monotonic.Ap-valueof<0.05wasconsideredsignificant.
- TofurtherinterrogatethereasonsforthedifferencesinPNMR,asubgroupof
siteswhoonlybeganauditingafter2006wasformedfromtheinitial163sites.
ETHICS
The PPIP program has ethical approval from the University of Pretoria. The data is
collected with permission from the South African Department of Health. The PPIP
technicaltaskteamapprovedthissecondaryanalysis.
ANALYSIS
All datawas analysedusing Epiinfo version 7 and SPSS version 22. The trendof the
PNMRusing themonthlyPNMR (defined forPPIPas fetaldeathsandearlyneonatal
deathsper1000births)overfiveyearswasanalysedbyperformingaChisquaretest
fortrendonthe12monthmovingaverages.

168
OUTLINEOFTHERESEARCHINCHAPTERSSEVEN,EIGHTANDNINE
BACKGROUND
ResearchintoUAlactatesamplinghasshownthatintroductionoftheproceduretoall
deliveries in a unit produces progressive improvement in neonatal biochemical
markersand reducedadmission tohigh care facilitiesover time, independentof the
rate of obstetric intervention(1). However, previous studies into implementation of
universal UA lactate sampling and its effect on neonatal outcomes have been
performed in resource-rich environments, usually in developed countries and
particularlyintertiaryandteachingfacilities(2).Thismainaimofthisprojectseeksto
identify the impact of implementation of cord lactate sampling into a SouthAfrican
hospital,withcomparativelylimitedresourcesandaPNMRof14.8/1000births.
STUDYOBJECTIVE
This study aimed to investigate whether UA cord lactate sampling correlates with
neonatal outcome at Kalafong Hospital, Pretoria, South Africa, and to determine
whether the use of lactate sampling and cardiotocograph (CTG) interpretation
training combinedwith education in lactate physiology as a functionof intrapartum
careresultsinachangeinclinicalpracticeand/orneonataloutcomes.

169
PRIMARY AIMS
1. To determine whether UA cord lactate sampling correlates with neonatal
outcomeatKalafongHospital.
2. To determine whether the introduction of UA cord lactate sampling at
KalafongHospital , with concomitant staff education inCTGinterpretation
and lactate physiologyresults inachange inclinicalpractice, including
a. Achange in instrumentaldeliveryrates
b. Achangeincaesareansectionrates
3. To determine whether the introduction of UA cord lactate sampling with
concomitant staff education in CTG interpretation and lactate physiology
resultsinanimprovementinlactatelevelsovertimeatKalafonghospital.
4. To determine whether the introduction of UA cord lactate levels with
concomitant staff education in CTG interpretation and lactate physiology
results in a change in the rate of neonatal admission tohighdependencyor
intensivecareat Kalafonghospital.
5. To determine whether the introduction of UA cord lactate levels with
concomitant staff education in CTG interpretation and lactate physiology
resultsinachangeintherateofneonatalmortalityatKalafong Hospital.

170
SECONDARY AIMS
1. To compare UA lactate levels in neonates of HIV positive and negative
womenat KalafongHospital.
2. To compare UA lactate levels in preterm and term neonates at Kalafong
hospital.
METHODOLOGY
This studywas conducted in two phases. Initially a cohort studywas undertaken to
determine whether UA cord lactate sampling correlates with neonatal outcome at
KalafongHospital. The results from this cohortwere servedas the control group for
thesecondphaseofthestudy,whichtestedtheinterventionofUAlactatesamplingin
combination with staff education in lactate physiology and CTG interpretation on
neonataloutcomes.

171
PHASE1
STUDYDESIGNANDSTUDYSETTING
During the period 3rd March 2014 to the 12th November 2014, we conducted a
prospectivecohortstudyofUAlactatelevelsinthelabourwardatKalafongHospital.
Kalafong Hospital is a tertiary hospital in Pretoria, South Africa, affiliated with the
UniversityofPretoria.In2014,therewere6,499deliveriesintheunit.
The study group consisted of prospectively collected samples of umbilical artery
lactateobtainedbytheprimaryresearcher(EA),oradoctorintheunittrainedbythe
primaryresearcher.TheUAwas identifiedbysite,andknowledgeoftheanatomyof
theumbilicalcord.AsUAsamplinghadnotbeenperformedintheunitbefore,theaim
of this cohort studywas to determine the optimal cut-off of lactate level for a pre-
definedsetofoutcomesintheunit.Theoutcomeschosenweretheneedforneonatal
resuscitation,neonataladmissiontothenursery,andApgarscoresat1and5minutes.
STUDYPOPULATION
Allwomenaimingtohaveavaginaldeliverywereeligibletobeconsentedforthetrial,
regardlessoftheirultimatemodeofdelivery.Womenofanygestationwhereaviable

172
outcomewasexpectedwereeligibletobeincludedinthestudy.AtKalafonghospital
thisincludesexpectedbirthweightsof600grormore.
STUDYPROCEDURESANDDATACOLLECTED
Aftermaternalconsentwasobtained(Appendix2.2),theumbilicalcordwasclamped
andcutwithinoneminuteofbirth.Asmallarterialbloodsample(upto1ml)wasthen
taken from a double clamped segment of the remaining umbilical cord, prior to
deliveryoftheplacenta.Thecordbloodsamplewastakenwithin15minutesofbirth,
regardlessofmodeofdelivery.The lactate levelwasmeasured(mmol/L)onaRoche
Accutrend PlusTM© hand-held lactate meter (Rotkreuz, Switzerland). The handheld
lactatemachinewasavailablewithinthebirthunitandthepatient’sdetailsandcord
lactateresultwasrecorded.Casereviewthenoccurredtocorrelatethepatientdetails
andcordlactateresultwiththeprimaryendpoints.
Introductionofanewprocessintoalowresourcesettingmandatesbotheaseofuse
andfinancialefficiency.Heparinisedsyringesareusedinmanysettingstoallowfora
lapseoftimebetweenobtainingandtestingthesample.Non-heparinisedsyringesare
howevermorefinanciallysoundandcanbeusedforUAsampleswithoutanychange
inthebiochemicalmeasurements,providedthesampleistestedshortlyaftertaking(3,
4).

173
Thecordlactateresultwaskeptblindtoclinicians(midwives,obstetricregistrarsand
obstetricconsultants)managing intrapartumcare,allowingtheentirestudygroupto
serveasthecontrolgroupforthesecondstageoftheproject.
Adatasheetwascompletedforeachcaseusingthebirthregistry,thepatient’scase
file,andtheneonatalnurseryadmissiondata (Appendix2.3).Thefollowingvariables
wererecorded:
DATACOLLECTED
The variables collected were defined by the clinicians in the unit. For example
gestation was taken as recorded (regardless of the method) or if a case was
documentedtohavepre-eclampsiathanthiswastakenasread.
1. Maternaldata
a. Maternalage
b. Gravidity, parity
c. Gestation
d. HIVstatus
e. HIVtreatment

174
f. Lengthoffirststage
g. Lengthofsecondstage
h. Complications of pregnancy
• Including:Abruption,adolescentpregnancy,advancedmaternalage,
anaemia, antepartum haemorrhage, breech presentation, cervical
incompetence, decreased fetal movements, eclampsia, gestational
diabetes mellitus, HELLP syndrome, hypertension (not pre-
eclampsia), intrauterine growth restriction, fetal macrosomia,
maternalmedicalconditionsnotrelatedtopregnancy,noantenatal
care, oligohydramnios, pre-eclampsia, placenta praevia, prelabour
and / or preterm rupture of membranes, syphilis, thyrotoxicosis,
tuberculosis, urinary tract infection, uterine anomaly, venous
thromboembolicevent
i. Complications of labour
j. Modeofbirth
k. Dateandtimeofbirth
l. Decisiontodeliverytime
2. Neonataldata
a. Birthweight

175
b. Cordlactateresult
c. Dateandtimeofcordlactatesample
d. Needforneonatalresuscitation
e. Apgarscore
f. Neonataloutcome
• Admissiontothenursery
• Diagnosisforadmission
• Hypoxic IschaemicEncephalopathy
• Deathbeforedischarge
SAMPLESIZECALCULATION
A sample size calculation was performed for both phase one and two. The
estimationof sample sizewasperformedusing standardisednormal lactatemean
and standard deviation. A sample size of 265 in each of the pre and post
intervention groups would achieve an 80% power to detect a difference of 0.25
standard deviations (approximately 8% difference in means) in lactate
measurementsbetweengroupsusinga two-sided sample t-test at5%significance
level.Thissamplesizewouldalsoachieveatleast80%powertodetectanR-squared
of 0.05 attributed to one or more independent variable/s while simultaneously

176
adjusting for multiple other relevant covariates with an R-squared of 0.2 in a
multiple linear regression analysis. Assuming a 15% attrition rate, the sample size
wasincreasedto305ineachgroupforatotalsamplesizeof610(PowerandSample
Size(PASS2008)).
PHASE TWO
The aim of this arm was to determine whether the introduction of the
interventions of sampling of UA lactate in addition to education in CTG
interpretation,fetalphysiology,andacidbasebalanceresultedinachangein
clinicalpracticeand/orneonataloutcomes.
STUDYDESIGNANDSTUDYSETTING
Thisisthesameasforphaseone
STUDYPOPULATION
AllmidwivesanddoctorsinvolvedinintrapartumcareatKalafongHospital.

177
Allwomenaimingtohaveavaginaldeliverywereeligibletobeconsentedforthetrial,
regardlessoftheirultimatemodeofdelivery.Womenofanygestationwhereaviable
outcomewasexpectedwereeligibletobeincludedinthestudy.AtKalafonghospital
thisincludesexpectedbirthweightsof600grormore.
STUDYPROCEDURESANDDATACOLLECTED
Beforethecompletionofthecohortoutlinedinphaseone,allmidwivesandregistrars
in the unit underwent a training course in fetal physiology, lactate physiology and
cardiotocograph(CTG)interpretation,conductedbytheprimaryresearcher(EA).
TEACHINGINTERVENTION
All staff members involved in CTG interpretation and intrapartum care
participated in the study and the teaching intervention. The teaching coursewas
adapted from the King Edward Memorial Hospital (KEMH) Advanced Fetal
Assessment(AFA) course resources (with permission).
Therewere18midwivesintheunit,managingnearly6500deliveriesperyear.Staffing
ratios and resources were therefore stretched and so the teaching intervention
needed to be delivered in one session to minimise the time away from work and

178
ensure allmidwiveswere trained.As such, the threepart teaching interventionwas
modified for themidwives to fit in toone90-minutesession.Conversely,47doctors
across the study period participated in the course, with the staff resource capacity
allowingfortheteachinginterventiontobedeliveredacrossthree90-minutesessions.
Theteachinginterventionwasdividedintofivecomponents
1.Baselinestaffdemographicsandpre-test
• Demographicsincluded
o Clinicalrole(Midwiferyornursingstudent,midwife,professionalnurse,
communityservicenurse)or(Intern,registrar)
o Previoustraining inCTGinterpretation(none,medicalschoolteaching,
ESMOEcourse)
Thedoctorscompleteda19questionandthemidwivescompleteda10questionpre-
teachingtesttoassessbaselineknowledge.
• Thepre-teachingtestassessed:
o Baseline confidence in CTG interpretation
o Baselineconfidenceinunderstandingfetalphysiology
o Baselineconfidenceininterpretationofcordlactatevalues

179
2.Fetalphysiology
The fetal physiology lecture outlined the history of fetal heart ratemonitoring, the
physiological control of the fetal heart, and the physiological mechanisms behind
specificfetalheartratepatterns.
3.Fetalacidbasestatus
The fetal acid base lecture outlined the fetal response to labour, fetal acid base
physiologyandnormal ranges forcomponentsofacidbase, thecomponentsofcord
acidbaseassessment,andtheroleoflactateinintrapartummonitoringandcare.
4.CTGpatternrecognition
TheCTGpattern recognition lecturegaveanoverviewofelectronic fetalmonitoring,
explained the differences between antenatal and intrapartum monitoring, outlined
CTG pattern recognition, and explored different clinical responses for the CTG
patterns.
5.Post-test
Thedoctorscompleteda33questionandthemidwivescompleteda14questionpost-
teaching test to assess acquisition of knowledge. Pre and post test scores were
comparedandanalysisofchangeinmedianswithstudentst-testperformed.
180
Atcompletionof theteachingintervention,eligiblewomenwhogaveconsenthadUA
lactatesamplestaken,withthesameprocessasdescribedforphaseone.From21stJuly
2014 to 12th November 2014, lactate sampling occurred, with the results made
immediatelyavailabletothecliniciansmanagingtheintrapartumcareofwomeninthe
labourward.Daily reviewof lactate results occurred everyweekdaymorning at the
department team meeting, involving all medical staff (interns, registrars, and
consultants).Alllactatesamplesobtainedintheprevious24hourswerereviewedand
cases with abnormal lactate levels were discussed, the CTG reviewed and the case
outcomes (including need for NICU admission and adverse neonatal outcome)
discussed. Clinical practice components of the cases where changes could be
considered were explored briefly. In addition, an in-depth review of interesting or
challenging cases occurred twice weekly, facilitated by the primary researcher (EA).
Casereflection,education,andoptionsforchanges infuturepracticewerediscussed
indetailatthesesessions.
DATACOLLECTED
Thisisthesameasforphaseone.

181
Image3.2AKalafonghospitalobstetricsregistrartestingaUAsample.
ETHICS
ThisstudywasapprovedbytheHumanEthicsResearchCommitteeofTheUniversity
ofWesternAustralia,Perth,WesternAustraliaonthe09/10/2014(Referencenumber
RA/4/1/6581),andtheUniversityofPretoria,Pretoria,SouthAfricaonthe01/10/2014
(Referencenumber7/2014).

182
OUTLINEOFTHERESEARCHINCHAPTERTEN
BACKGROUND
The hypothesis of the first trialwas thatUA lactate sampling as a clinical audit tool
wouldresultinanimprovementinseveralaspectsofintrapartumcare.Ifthisproved
to be the case, the tool needed to be applicable outside the research setting in an
LMICunit.Thusweaimedtoaddress the feasibilityof introducingthetool inclinical
practiceatZithuleleHospitalontheeasterncapeinSouthAfrica.
Implementingumbilicalcordsamplingintonon-teachingfacilitiesinSouthAfricasuch
asZithuleleHospitalispotentiallybeneficialbutlikelytoposeanumberofchallenges
whenconsideringthelimitedresourceswithinthesesettings.Whiteetalinterviewed
midwives and other professionals involved inmaternity care in a resource rich high
income country setting, and found that more than 50% considered universal cord
blood gas or lactate analysis to be difficult to introduce due to insufficient time
following delivery to perform the sample, increasedworkload and encroachment of
technology onto birth(5). Overall the majority of participants (67.3%) agreed that
umbilical cord blood gas/lactate analysis was beneficial to maternity care with
proposedbenefits beingobjectivemeasurementof neonatal status to assist in care,
objectiveprotectionformedico-legalissuesandimprovedopportunitiesforauditand
teaching.

183
STUDYOBJECTIVE
Todeterminefeasibilityofintroducinguniversalumbilicalarterycordlactatesampling
intoadistrictlevel,ruralhospitalinSouthAfrica.
PRIMARYAIMS
1. To Identify attitudes and barriers towards implementation of universal cord
lactatesampling.
2. ToimplementatrainingmodulecombiningCTGinterpretationandcordlactate
sampling to assess pre and post training confidence and competence of
midwiferyandmedicalstaff.
METHODOLOGY
Thisstudywasabeforeandafterimplementationstudy,consistingofabaselinestaff
survey, a training program in CTG interpretation, fetal physiology, and the practical
stepsandinterpretationofUAlactatesampling,andfinallyaposttrainingsurvey.The
studywasconductedfromNovember2014toJanuary2015.
184
STUDYSETTING
ZithuleleHospitalisaruraldistricthospitalintheEasternCapeofSouthAfrica.Despite
itsresourcepoorenvironmentitperformsbetterthanmostfacilitiesinitscategoryin
theareaofneonataloutcomes. Theperinatalmortality rate in2013was25.2/1000
births,ofwhich25.4%wasdueto intrapartumasphyxia.Monthlyperinatalmortality
meetings with case reflection are attended by midwives, doctors and hospital
managers.
INFORMEDCONSENT
Midwivesanddoctorsweregivenwritteninformationbeforetakingpartinthestudy.
Participationwas voluntary.Written informationwas also provided towomen from
whocordbloodwasextractedforthepurposeoftrainingandwrittenconsentwasbe
obtained(Appendix9.2).
PRE-INTERVENTION
Allmidwives and doctors were invited to consent to participate in a survey, as the
baselineforthestudy.

185
• Demographics
• PreviousexperiencewithCTG
• Previousexperiencewithcasereflection/qualityofcareaudit
• Attitudes towards perinatal audit, CTG monitoring and cord lactate blood
sampling
• Confidenceintheattainmentofcordlactateblood
• ConfidenceinthepotentialbenefitsofknowingUAlactatelevels
• Perceived barriers to implementation of CTG/lactate training and universal
measurementofcordlactatevalues
Questionnairesincluded20statementswithresponseoptionsofstronglyagree,agree,
neutral, disagree and strongly disagree. Baseline demographics were taken. See
proposedquestionnaireincluded,adaptedfromWhiteetal.,‘Attitudesandbarriersto
the introduction of umbilical cord blood gas and lactate analysis at birth’ (with
permission)(5).
INTERVENTION
We then performed a modified CTG training program, which explained lactate
physiologyandthebenefitsofmeasuringit,adaptedfromtheKingEdwardMemorial
HospitalAdvancedFetalAssessmentcourseresources(withpermission).Thisincluded
lecturesonfetalphysiology,fetalacidbasestatus,andCTGpatternrecognition(asper
themethodologyfor“Abeforeandafterstudyoftheimpactonobstetricandperinatal

186
outcomes following the introduction of an educational package of fetal heart rate
monitoringeducationcoupledwithumbilicalarterylactatesamplinginalowresource
settinglaborwardinSouthAfrica”).
A teaching session on the steps to sample the umbilical artery and test the lactate
formed the second componentof the intervention. Thiswasdoneonumbilical cord
post-delivery with patient consent for its use as a training tool. Teaching was
undertaken by an obstetric clinician who was trained in cord sampling in Western
Australiainaunitwherealldeliveriesundergopairedcordsamplingatbirth.Segments
of cord (usedwithmaternal permission)was used to demonstrate cord anatomy as
well as samplingof theartery.All participantswere taught and supervised sampling
theumbilicalartery.
POSTINTERVENTION
After the training program, an identical survey as in the pre-interventionphasewas
presented to midwifery and medical staff and pre and post intervention responses
compared.

187
CHAPTERFOUR:CAUSESOFPERINATALMORTALITYANDASSOCIATED
MATERNALCOMPLICATIONSINASOUTHAFRICANPROVINCE:
CHALLENGESINPREDICTINGPOOROUTCOMES

188
CHAPTEROVERVIEW
Asoutlined inChapter two, theburdenofglobalperinatalmortality liesheavilywith
the LMICs. Itwas important thatweascertained the causesofperinatalmortality in
SouthAfricainordertobeginconsideringthepotentialroleourinterventionmayplay.
Oneofthemajorchallenges inLMICisthepaucityofcomprehensivedatacollection,
whichcanbeusedto identifyareaswhereresourcescanbetargeted.SouthAfrica is
unique in its comprehensiveuseof thePPIPauditprogram,whichallows systematic
dataanalysisrelatedtoperinatalmortality.TheProvinceofMpumalangaisparticularly
notable in that facility-based delivery is almost universal, and every facility
comprehensively participates in QoC audit using PPIP. Furthermore, the units also
record thematernal condition associatedwith every perinatal death, allowing an in
depthanalysisofallaspectsofthecontributorstoperinatalmortalityintheProvince.

189

190

191

192

193

194

195

196
CHAPTERFIVE:UMBILICALLACTATEASAMEASUREOFACIDOSISAND
PREDICTOROFNEONATALRISK:ASYSTEMATICREVIEW

197
CHAPTEROVERVIEW
HavingascertainedinChapter3thatintrapartumasphyxiacontributesto25%oflate
stillbirthsandearlyneonataldeathsinSouthAfrica,itwasthenimportanttoconsider
the accuracy of the planned intervention. The gold standard assessment of acidosis
fromtheumbilicalarteryatbirthispH.However,pHassessmenttypicallynecessitates
abloodgasanalyser,whichusuallyrequiresupto90uLofblood.Thisisnotfeasiblein
low resources settings for the following reasons. Firstly the cost of obtaining and
maintainingabloodgasanalyser isprohibitive inmanyLMIC.Secondly,given lactate
can bemeasured using a hand-heldmeter with as little as 5uL of blood, there is a
markeddifference inconsumablecosts intermsofsyringes(6,7).Finally, theeaseof
collection in terms of human resources (training and time) renders lactate
measurementmorefeasibleinresourcesstretchedareas,suchasSouthAfrica.
That said, the decision to assess acidosis at delivery with lactate rather than pH
necessitatesconfidenceinthediagnosticaccuracyoflactateintheassessmentofthe
targetoutcome. Lactatehas repeatedlybeen shown to correlatewithumbilical cord
pH (the gold standard assessment of acidosis) and to have reasonable accuracy in
predictingpoorneonataloutcome(7-18).Therefore,thenextstepinthisthesiswasto
synthesise the evidence on the diagnostic test accuracy of umbilical cord lactate by
comparing it with other assessments of acidosis in the immediate newborn and by
assessingtheabilityofumbilicalcordlactatetopredictneonataloutcomes.

198

199

200

201

202

203

204

205

206

207

208

209
REFERENCESFORCHAPTERINTRODUCTION
1. White CR, Doherty DA, Henderson JJ, Kohan R, Newnham JP, Pennell CE.Benefitsof introducinguniversalumbilicalcordbloodgasandlactateanalysis intoanobstetricunit.AustNZJObstetGynaecol.2010;50(4):318-28.2. Allanson E,Waqar T,White C, Tunçalp Ö, Dickinson J. Umbilical lactate as ameasureofacidosisandpredictorofneonatalrisk:asystematicreview.BJOG.2016.3. DuerbeckNB,ChaffinDG,SeedsJW.ApracticalapproachtoumbilicalarterypHandbloodgasdeterminations.ObstetGynecol.1992;79(6):959-62.4. Westgate J, Garibaldi JM, Greene KR. Umbilical cord blood gas analysis atdelivery:atimeforqualitydata.BJOG.1994;101(12):1054-63.5. White CR, Kohan R, Doherty DA, Newnham JP, Pennell CE. Attitudes andbarriers to the introductionofumbilical cordbloodgasand lactateanalysis atbirth.AustNZJObstetGynaecol.2013;53(3):271-6.6. WestgrenM,KrugerK,EkS,GrunevaldC,KublickasM,NakaK,etal. Lactatecomparedwith pH analysis at fetal scalp blood sampling: a prospective randomisedstudy.BrJObstetGynaecol.1998;105(1):29-33.7. Labrecque L, Provencal M, Caqueret A, Wo BL, Bujold E, Lariviere F, et al.CorrelationofcordbloodpH,baseexcess,andlactateconcentrationmeasuredwithaportabledevice for identifying fetal acidosis. JObstetGynaecolCan. 2014;36(7):598-604.8. SuTY,ReeceM,ChuaSC.Lactatestudyusingumbilicalcordblood:agreementbetween Lactate Pro hand-held devices with blood gas analyser and evaluation oflactatestabilityovertime.AustNZJObstetGynaecol.2013;53(4):375-80.9. GjerrisAC,Staer-JensenJ,JorgensenJS,BergholtT,NickelsenC.Umbilicalcordbloodlactate:avaluabletoolintheassessmentoffetalmetabolicacidosis.EurJObstetGynecolReprodBiol.2008;139(1):16-20.10. Linet T, Laporte J, GueyeH, BoogG. [Microvolume dosage of lactate in cordblood for the evaluation of the neonatal well-being]. J Gynecol Obstet Biol Reprod(Paris).2002;31(4):352-7.11. MartinA,GaillardM,MiotS,RiethmullerD,SchaalJP.[Lactatemeasurementsandacid-basebalance incordblood].JGynecolObstetBiolReprod(Paris).2003;32(8Pt1):713-9.12. Racinet C, Richalet G, Corne C, Faure P, Peresse JF, Leverve X. [Diagnosis ofneonatal metabolic acidosis by eucapnic pH determination]. Gynecol Obstet Fertil.2013;41(9):485-92.13. TuuliMG,StoutMJ,ShanksA,OdiboAO,MaconesGA,CahillAG.Umbilicalcordarterial lactate comparedwith pH for predicting neonatalmorbidity at term.ObstetGynecol.2014;124(4):756-61.14. WestgrenM,DivonM,HoralM,IngemarssonI,KublickasM,ShimojoN,etal.Routinemeasurementsofumbilicalarterylactatelevels inthepredictionofperinataloutcome.AmJObstetGynecol.1995;173(5):1416-22.15. White CR, Doherty DA, Henderson JJ, Kohan R, Newnham JP, Pennell CE.Accuratepredictionofhypoxic-ischaemicencephalopathyatdelivery:acohortstudy.JMaternFetalNeonatalMed.2012;25(9):1653-9.

210
16. Wiberg N, Kallen K, Herbst A, Olofsson P. Relation between umbilical cordblood pH, base deficit, lactate, 5-minute Apgar score and development of hypoxicischemicencephalopathy.ActaObstetGynecolScand.2010;89(10):1263-9.17. WattWF,TanKH,YeoGSH.Umbilicalcord lactate:apreliminarystudyof130termbabies.SingaporeJournalofObstetricsandGynaecology.2002;33(2):42-8.18. HamedHO.Intrapartumfetalasphyxia:studyofumbilicalcordbloodlactateinrelationtofetalheartratepatterns.ArchGynecolObstet.2013;287(6):1067-73.

211
CHAPTERSIX:QUALITYOFCAREAUDITSANDPERINATALMORTALITY
INSOUTHAFRICA

212
CHAPTEROVERVIEW
Theaimofthisthesiswastoconsidertheroleof introducingumbilicalartery lactate
samplinginanLMIC.AsoutlinedinChapters1-3,theintentionwasforthesamplingto
serveasfeedbacktocliniciansprovidingcare,suchthatcasereflectioncanoccurand
ideallypracticealtered,ultimatelywiththegoalofimprovingclinicaloutcomes.Thus,
the intervention is essentially a quality of care audit intervention. Once we had
determined that it was possible to use UA lactate as a measure of acidosis, it was
importanttoconsidertherolethatQoCauditcanplay, ifany,onperinatalmortality.
Therefore, the following study was set up to retrospectively analyse the impact of
qualityofcareperinataldeathauditontheratesofperinatalmortalityinSouthAfrica,
andthisisreportedinthemanuscriptthatfollows.

213

214

215

216

217
218
CHAPTERSEVEN:THEINTRODUCTIONOFUMBILICALCORDLACTATE
MEASUREMENTANDASSOCIATEDNEONATALOUTCOMESINASOUTH
AFRICANTERTIARYHOSPITALLABOURWARD

219
CHAPTEROVERVIEW
Having established the contribution of intrapartumhypoxia to perinatalmortality in
South Africa, the diagnostic accuracy of umbilical artery lactate, and the potential
benefitofQoCauditinSouthAfrica,itwasthenimportanttoassesstheutilityofUA
lactatesamplinginoursetting.AstherearelittledataontheuseoflactateinLMIC,we
neededtoestablish itsutility inmeasuring intrapartumhypoxia inoursetting,rather
thanrelyingonthepublishedcut-offsforlactatelevelsfromhighincomesettings.

220

221

222

223

224

225

226

227
CHAPTEREIGHT:ABEFOREANDAFTERSTUDYOFTHEIMPACTON
OBSTETRICANDPERINATALOUTCOMESFOLLOWINGTHE
INTRODUCTIONOFANEDUCATIONALPACKAGEOFFETALHEARTRATE
MONITORINGEDUCATIONCOUPLEDWITHUMBILICALARTERYLACTATE
SAMPLINGINALOWRESOURCESETTINGLABOURWARDINSOUTH
AFRICA.

228
CHAPTEROVERVIEW
ItisevidentfromChapter7thattheoptimalcut-offforumbilicalarterylactateinour
setting is similar to that inhigh-income settings. We thenaimed to assesswhether
training of doctors and midwives in fetal physiology, acid-base balance and CTG
interpretation in addition to umbilical artery lactate sampling improved intrapartum
outcomes.
AsoutlinedinChapter3,thesecondphaseoftheumbilicalarterylactatesamplingtrial
involvedaneducationalinterventionwherebytheauthorofthisthesistraineddoctors
andmidwivesprovidingintrapartumcareinfetalphysiology,fetalandneonatallactate
andacidbasebalance, and interpretationofCTGsand their relationship to acidosis.
Participants completed a pre-and post-training test to demonstrate acquisition of
knowledge. Fifty-three doctors participated in training,with 47 (89%) completing all
three sessions and the pre-and post-tests. Mean test scores significantly improved
from43%to70%,p<0.001.(Table8.1)All18midwivesintheunitcompletedtraining
aswellaspreandpost-tests,withanimprovementinmeanscoresfrom38%to59%,
p<0.001.(Table8.2)

229
Table8.1:Preandposttestscoresfordoctors

230
Table8.2:Preandposttestscoresformidwives
There is a plethora of evidence that training such as we conducted increases
knowledge(1), however, while the improvement in test scores is reassuring, the
ultimate aim of the research is a change in clinical practice and improvement in
intrapartumoutcomes.Theremainderofthischapterexploresthisphenomenon,and
hasbeensubmittedandisunderreviewbyBMCPregnancyChildbirthandisformatted
forthisjournal’sspecifications.

231
REFERENCEFORCHAPTERINTRODUCTION
1. CalvertKL,McGurganPM,DebenhamEM,GratwickFJ,MaourisP.Emergencyobstetricsimulationtraining:howdoweknowwherewearegoing,ifwedon'tknowwherewehavebeen?AustNZJObstetGynaecol.2013;53(6):509-16.

232
ABEFOREANDAFTERSTUDYOFTHEIMPACTONOBSTETRICANDPERINATALOUTCOMES
FOLLOWINGTHEINTRODUCTIONOFANEDUCATIONALPACKAGEOFFETALHEARTRATE
MONITORINGEDUCATIONCOUPLEDWITHUMBILICALARTERYLACTATESAMPLINGINALOW
RESOURCESETTINGLABOURWARDINSOUTHAFRICA.
AllansonER1,2,PattinsonRC2,NathanEA1,DickinsonJE1
1. Division of Obstetrics and Gynaecology, Faculty of Health and Medical Sciences,
UniversityofWesternAustralia,Crawley,WA,Australia.
2. SAMRC/UP Maternal and Infant Health Care Strategies Unit, Department of
ObstetricsandGynaecology,UniversityofPretoria,Pretoria,SouthAfrica.
EmmaRAllanson
Division of Obstetrics and Gynaecology, Faculty of Health and Medical Sciences,
UniversityofWesternAustralia,Crawley,WA,Australia.
(M550)TheUniversityofWesternAustralia
35StirlingHwyCRAWLEYWA6009
+61432199297

233
RobertCPattinson
UniversityofPretoria,KalafongCampus
SAMRC/UPMaternalandInfantHealthCareStrategies,UnitPrivateBagX323Arcadia,
SouthAfrica,0007
ElizabethANathan
DivisionofObstetricsandGynaecology,FacultyofHealthandMedicalSciences,
(M550)TheUniversityofWesternAustralia
35StirlingHwyCRAWLEYWA6009
JanEDickinson
DivisionofObstetricsandGynaecology,FacultyofHealthandMedicalSciences,
(M550)TheUniversityofWesternAustralia
35StirlingHwyCRAWLEYWA6009

234
Correspondingauthor:ERAllanson
DivisionofObstetricsandGynaecology,FacultyofHealthandMedicalSciences,
(M550)TheUniversityofWesternAustralia
35StirlingHwyCRAWLEYWA6009
+61432199297
Wordcount:3242
CONFLICTSOFINTEREST
Theauthorsdeclarenoconflictsofinterest

235
ABSTRACT
INTRODUCTION
Rates of caesarean section (CS) are increasing and abnormal fetal heart rate tracing
andconcernaboutconsequentacidosis remainoneof themostcommon indications
forprimaryCS.Umbilicalartery(UA)lactatesamplingprovidesclinicianswithpointof
care feedbackonCTG interpretationand intrapartumcareandmay result inaltered
futurepractice.
MATERIALSANDMETHODS
From 3rd March - 12th November 2014 we undertook a before and after study in
Pretoria, South Africa, to determine the impact of introducing a clinical package of
fetal heart rate monitoring education and prompt feedback with UA cord lactate
sampling,usingahand-heldmeter,onmaternalandperinataloutcomes.
RESULTS
936 consecutive sampleswere analyzed (pre n=374 and post n=562). Therewas no
difference in mean lactate (4.6 mmol/L [95%CI 4.4-4.8] compared with 4.9 mmol/L
[95%CI 4.7-5.1], p=0.089). Suspected fetal compromise was reduced in the post-
interventionperiod:30·2%vs22·1%,aOR0·71,95%CI0·52-0·96,p=0·027.Cesarean

236
sectionratesweresignificantlyreducedintheunivariateanalysis:pre-40·3%vspost-
intervention31·6% (p=0·007). This reduction remained significantwhenadjusted for
previouscaesareansection,primiparity,maternalHIVinfectionandpretermbirth(aOR
0·72,95%CI0·54-0·98,p=0·035).Neonataloutcomesdidnotdifferbetween the two
groups.
CONCLUSION
Theintroductionofaclinicalpracticepackageoffetalheartratemonitoringeducation
combined with routine UA cord lactate sampling has the potential to reduce the
caesarean section rate without increasing adverse neonatal outcomes in a low-
resourcesetting.
KEYWORDS
Lactate;caesarean;SouthAfrica;maternal;neonatal
KEYMESSAGE
Both rising caesarean section rates and high perinatalmortality are issues of global
concern.We have demonstrated, using a simplemethod of testing umbilical artery

237
lactateatbirth,thatitispossibletoreducecaesareansectionrateswithoutworsening
neonatalmorbidityinalowresourcesetting.

238
INTRODUCTION
Theratesofcaesareansection(CS)areincreasingglobally(1),althoughboththetotal
rates and the rate of rise vary considerably between low,middle, and high income
countries(2). While there is little agreement about the optimal rate of CS, there is
some evidence that increasing rates above a certain threshold may not result in a
corresponding improvement in maternal and perinatal mortality(3). Moreover, CS,
while a life-saving procedure that allwomenmust have access towhen required, is
alsoassociatedwithpotentialadversematernaloutcomesinboththeindexandfuture
pregnancies(4). Balancing the indication for CS with its potential risks is a critical
clinicalandpublichealthchallenge.
Abnormal fetal heart rate tracing or suspected fetal distress with concern for
consequenthypoxiaandacidaemiaremainsoneof themostcommon indications for
thefirstCS(withratescitedbetween10-32%)(5-8).However,theratesofpathological
acidaemia in neonates generally is far lower than this level, and although there are
documentedbenefits, theuseofelectronic fetalheart ratemonitoring in labourhas
not been shown to improve neonatal mortality(9). It is important to consider fetal
physiologyintheintrapartumperiodandcardiotocograph(CTG)interpretationingreat
detail given the need to balance the role that intrapartum hypoxia plays in global
perinatal deaths, with the role that potentially unnecessary CS play in maternal
morbidityandmortality.

239
Objectivemeasurementsof intrapartumfetalhypoxia(suchaspHor lactatesampled
from the fetal scalp) may improve upon the known limited specificity of CTG and
reducetherateofunnecessarycaesareansections(10,11).Thecostoftheequipment
to do this, alongside high rates of maternal HIV infection makes this prohibitive in
someunitsaroundtheworld.Universalumbilicalcord-gassamplingafterdeliveryhas
been suggested as amethod to improve the specificity of the CTG(12). Paired cord
arterial and venous gas sampling is both time and resource intensive however,
particularly outside of high-income country settings. To that end, it is possible to
introduceinexpensivebedsidepointofcareumbilicalartery(UA)lactatetesting,which
provides clinicians feedback on intrapartum care and potentially alters practice for
futurecases,whichmaypartlymitigatethepoorspecificityoftheCTG.Therefore,we
conductedabeforeandafterstudyinatertiarylabourwardinPretoria,SouthAfrica,
to determine the impact of introducing UA lactate sampling, in conjunction with
education on CTG interpretation and fetal and lactate physiology, on maternal and
perinataloutcomes.
MATERIALSANDMETHODS
Kalafong Hospital is a tertiary hospital in Pretoria, South Africa, affiliated with the
UniversityofPretoria. In2014,therewere6,499birthsintheunit.Duringtheperiod
3rd March to the 12th November 2014 we conducted a before and after study to
determine the impact of umbilical artery lactate sampling, combined with an

240
educational program on fetal heart rate monitoring, on maternal and neonatal
outcomes.
Thestudygroups includedprospectivelycollectedsamplesofumbilicalartery lactate
obtainedbytheprimaryresearcher(EA),oradoctorintheunittrainedbytheprimary
researcher.WehavepresentedthespecificsofUAsamplingintheunit,andthedata
points collected previously(13). Briefly, after maternal consent was obtained, the
umbilicalcordwasclampedandcutwithinoneminuteofbirth.Asmallarterialblood
sample (<0.5uL) was then taken from a double clamped segment of the remaining
umbilical cord, prior to delivery of the placenta. The lactate level was measured
(mmol/L) on a Roche Accutrend PlusTM© hand-held lactate meter (Rotkreuz,
Switzerland).Thecoefficientofvariation(CV)forthislactatemeteris1.8-3%(14).All
women aiming to have a vaginal birth were eligible to be consented for the trial,
regardlessoftheirultimatebirthmode.
Duringtheperiod3rdMarchto18thofJuly,2014,aprospectivecohortofwomenwere
consented to be enrolled in the study. As this was a blinded cohort, this was a
convenience sample, obtained within the capacity of a single researcher (EA). The
resultsofthelactatesamplinginthiscohortwereblindedtotheclinicians(midwives,
registrars, and consultants) managing the intrapartum care of women. This cohort
served as the baseline for the unit, the results of which have been published
previously(13).Beforethecompletionofthecohort,allmidwivesandregistrarsinthe

241
unit underwent a training course in fetal physiology, lactate physiology and
cardiotocograph(CTG)interpretation,conductedbytheprimaryresearcher(EA).The
courseconsistedofapre-test,a seriesofdidactic lectures, interactiveapplicationof
knowledgewith CTG examples, and a post-test. Subsequently, from21st July to 12th
November 2014, lactate sampling continued, with the results made immediately
availabletothecliniciansmanagingtheintrapartumcareofwomeninthelaborward.
Furthermore,all lactatesamplesobtainedintheprevious24hourswerereviewedat
the dailymorning labourwardmeetings of allmedical staff (interns, registrars, and
consultants),andtwiceweekly,anin-depthreviewofinterestingorchallengingcases
wasfacilitatedbytheprimaryresearcher(EA).DailyreviewsinvolvedcorrelatingCTG
interpretationpre-birthwithneonataloutcomes,includingtheUAlactate.Duringthe
two study periods, basic data on all births (regardless of recruitment to the study)
were collected, including number of births, mode of birth, and admissions to the
neonatalnursery(alllevels).
STATISTICSANDANALYSIS
The estimation of sample size was performed using standardised normal lactate
mean and standard deviation. A sample size of 265 in each of the pre and post
intervention groups would achieve an 80% power to detect a difference of 0.25
standard deviations (approximately 8% difference in means) in lactate
measurementsbetweengroupsusinga two-sided sample t-test at5%significance
level.Thissamplesizewouldalsoachieveatleast80%powertodetectanR-squared

242
of 0.05 attributed to one or more independent variable/s while simultaneously
adjusting for multiple other relevant covariates with an R-squared of 0.2 in a
multiple linear regression analysis. Assuming a 15% attrition rate, the sample size
was increased to 305 in each group for a total sample size of 610. ([Power and
SampleSize(PASS2008)].
Toassessthelactateresults,dataweretransformedtothenaturallogarithmtocorrect
normality and summarised as geometric means and 95% confidence intervals (CI).
Linear regression analysis was conducted on the log transformed lactate
measurementsandpresentedasestimatedmeaneffectsand95%CI’s.Amultivariate
analysis on lactate levels, adjusted for primiparity, HIV, fetal problems in pregnancy
and preterm birth, was done with lactate measurements log transformed for the
analysis. Summary values of estimated mean effects and 95% confidence intervals
were back transformed. Outcomes were summarised using means and standard
deviations or medians, interquartile ranges and ranges for continuous data and
frequencydistributionsforcategoricaldata.Basedonourpreviouslypublishedcohort
study, a cut-off for an abnormal lactate was assumed to be 5·45 mmol/L(13).
Univariate comparisons were made using independent t-tests for continuous
outcomes and Chi-square or Fisher exact tests for categorical comparisons.
Multivariable logistic regression analysis was performed on maternal and neonatal
outcomes including fetal distress, cesarean section, resuscitation, Apgar scores and
admissiontospecialcarenursery.Resultsweresummarisedwithunadjusted(OR)and
adjustedoddsratios(aOR)and95%CI’s.

243
Analyses of outcomes were adjusted for preterm birth, primiparity, HIV, previous
uterine surgery or maternal problems in pregnancy (maternal outcome), and fetal
problems during pregnancy (neonatal outcomes). Maternal problems in pregnancy
includedbeinganadolescent,havingadvancedmaternalage(>35),anaemia,cervical
incompetence, eclampsia, gestational diabetes mellitus, HELLP syndrome,
hypertensionwithoutpre-eclampsia,maternalmedicalconditions,noantenatalcare,
pre-eclampsia, preterm labour, syphilis, thyrotoxicosis, tuberculosis, urinary tract
infection,uterineanomaly,orvenousthromboembolicevent.Apre-plannedsubgroup
analysiswas conducted on infantswith birthweight <2500g comparedwith ≥2500g
and neonatal outcomes were assessed. A Bonferroni adjustment was applied such
that the significance level for each comparison of pre- and post-intervention groups
within birth weight strata was set to 0·025. All tests were two-sided and a p-value
<0·05was considered statistically significant for theoverall analysis. SPSS statistical
softwarewasusedindataanalysis(version22·0,Armonk,NY:IBMCorp).
Aprotocolwasdevelopedforthisstudy;itisnotpublishedbutavailableuponrequest.
ETHICS
This study was approved by the ethics committees of The University of Western
Australia Human Research Ethics Committee on the 26/02/2014 (Reference number

244
RA/4/1/6581), the University of Pretoria, Pretoria, South Africa on the 10/02/2014
(Referencenumber7/2014).
RESULTS
397sampleswerecollectedinthepre-interventionperiodfrom2196plannedvaginal
births and 2436 total births. 597 samples were collected in the post-intervention
period from1978plannedvaginalbirthsand2232 totalbirths.Afterexclusionof54
twinpregnancies,atotalof936sampleswereanalysed(pren=374andpostn=562).
MATERNALCHARACTERISTICS
Maternal characteristics did not differ between groups. (Table 1) Thematernal HIV
prevalenceinthepre-interventiongroupwas21·8%(n=79),withantiretroviraltherapy
(both prophylactic antiretroviral therapy and highly active antiretroviral treatment)
used in 96·2%·of women antenatally. The maternal HIV prevalence in the post-
interventiongroupwas23%(n=123),withantiretroviraltherapyin92·4%ofwomen.A
comparison of the maternal and neonatal outcomes between the HIV and non-HIV
infectedmothershasbeenpublishedelsewhere(15).

245
Datasummariesaremean(±SD),median(IQR,R)orN(%),asappropriate
PREGNANCYANDLABOUR
The pre-intervention group had a higher rate of maternal-related pregnancy
complications (41·8% vs 22·4%, p<0·001) and were also more likely to have
intrapartumcomplications (55·6%vs45·9%,p=0·004), fetaldistress (30·2%vs22·1%,
p=0·005), other labor complications (3·5% vs 1·4%, p=0·038) and be transferred
intrapartum from a referral unit (19·5% vs 7·3%, p<0·001). The intrapartum
complications are outlined in Table 2. Other labor complications included were
infrequent in both groups and included twin pregnancy diagnosed intrapartum, the
development of isolated intrapartum hypertension, acute twin to twin transfusion
syndromeand singleunusual occurrences such as “patient foundon antenatalward
Table1:Maternalcharacteristicsinpre-andpost-interventiongroups
Pre-intervention(N=374) Post–intervention
(N=562)
p-value
Maternalage(y) 27·4(±6·1) 27·4(±6·6) 0·897
Gestation(w) 38·8(±3·1)(n=345) 38·8(±3·2)(n=504) 0·963
Gravidity 2(1-3;1-7) 2)1-3;1-8) 0·672
Parity 1(0-2;0-5) 1(0-2;0-7) 0·820
Nulliparous 136(36·7%) 195(36·2%) 0·899
Previousuterinesurgery 53(14·7%) 56(10·6%) 0·072
HIVstatus 79(21·8%) 123(23·0%) 0·655
HIVtreatment 75(96·2%) 109(92·4%) 0·369

246
withfetalheaddelivered”,“patientpushingfromfourcentimetres”,maternalcollapse
atfulldilatation,andfailedinstrumentaldeliveryatlocalclinicpriortotransfer.
Table2:Intrapartumcomplicationsinpre-andpost-interventiongroups
Pre-intervention
N=374
N(%)
Post–intervention
N=562
N(%)
p-value
Any 208(55·6%) 258(45·9%) 0·004
Abruption 7(1·9%) 7(1·2%) 0·440
Chorioamnionitis 0 4(0·7%) 0·155
Delayedprogress1ststage 40(10·7%) 85(15·1%) 0·051
Delayedprogress2ndstage 15(4·0%) 23(4·1%) 0·950
Intrapartumhaemorrhage 7(1·9%) 12(2·1%) 0·779
Malpresentation 8(2·1%) 14(2·5%) 0·728
Meconiumstainedamnioticfluid 27(7·2%) 40(7·1%) 0·953
Augmentationoflabour 13(3·5%) 25(4·4%) 0·460
Shoulderdystocia 9(2·4%) 7(1·2%) 0·180
Fetaldistress 113(30·2%) 124(22·1%) 0·005
Other* 13(3·5%) 8(1·4%) 0·038
Intrapartumtransfer 73(19·5%) 41(7·3%) <0·001
*Other=seenoteinmainbodyoftext.

247
LACTATERESULTS
Alactateresultwasrecordedfor351(94%)ofwomenrecruitedinthepre-intervention
groupand542(96%)ofwomenrecruitedpost-intervention.Therewasnodifferencein
themeanlactateresult(4.6mmol/L[95%CI4.4-4.8]comparedwith4.9mmol/L[95%CI
4.7-5.1], p=0.089) or in babies born with a lactate greater than 5.45 mmol/L (122
(34.8%) compared with 210 (38.7%), p=0.228). There was no difference in mean
lactate levels between the two groupswhen adjusted for primiparity, HIV infection,
fetalproblemsinpregnancyandpretermbirth(unadjustedOR1.05[95%CI0.99-1.13],
comparedwithanadjustedOR1.06[95%CI0.99-1.13],p=0.108).
BIRTHCHARACTERISTICS
Pre-intervention women were more likely to have a caesarean section due to
suspected fetal distress (21·4% vs14·9%, p=0.011) and vaginal birth after caesarean
(VBAC) in labour (8·0% vs 2·5%, p<0·001). Other indications for caesarean delivery
were similar between the two groups. Suspected fetal distress during labor was
reduced in thepost-interventionperiod:pre-30·2%vspost-intervention22·1%,aOR
0·71,95%CI0·52-0·96,p=0·027.Caesareansectionratesweresignificantlyreducedin
the univariate analysis: pre- 40·3% vs post-intervention 31·6% (p=0·007). This
reduction remained significant when adjusted for previous caesarean section,
primiparity, maternal HIV infection and preterm birth (aOR 0·72, 95%CI 0·54-0·98,
p=0·035).

248
NEONATALCHARACTERISTICS
Theneonatalcharacteristics in thetwogroupsareoutlined inTable3.Therewasno
difference in neonatal outcomes when adjusted for primiparity, HIV infection, fetal
problems in pregnancy and pretermbirth. When stratified by birthweight (<2500g
and≥2500g),therewasnodifferenceinanyoutcomes, includinglactateresults.(See
Table4)

249
Table3:Neonatalcharacteristicspre-andpost-interventiongroups
N*
Pre-intervention
N*
Post–intervention
p-value
Preterm(<37w) 345 64(18·6%) 504 99(19·6%) 0·691
Birthweight(g) 363 3033·9(±623·5)
520 3006·4(±641·2)
0·527
Lactate>5·45 122(34·8%) 210(38·7%) 0·228
Resuscitation 344 71(20·6%) 532 129(24·2%) 0·214
Apgar<7at1min 365 45(12·3%) 526 83(15·8%) 0·149
Apgar<7at5min 366 20(5·5%) 526 35(6·7%) 0·468
Special care nurseryadmission
374 56(15·0%) 562 80(14·2%) 0·754
Admissiontype 367 558
None 318(86·6%) 480(86·0%)
Highdependencyunit 8(2·2%) 22(3·9%) 0·387
Intensivecareunit 14(3·8%) 15(2·7%)
Neonatalward 27(7·4%) 41(7·3%)
Datasummariesaremean(±sd)orN(%),asappropriate*Nreflectscasesforwhichdatawereavailable
forthevariable

250
Table4:Neonataloutcomesstratifiedbybirthweight<2500gand≥2500g.
Birthweight<2500g Birthweight≥2500g
Pre-intervention
Post–intervention
p-value
Pre-intervention
Post-intervention
p-value
n=52 n=78 n=311 n=442
Birth weight(g)
1937.48(±556.1)
1836.35(±534.2)
0.300 3217.2(±409.6) 3212.9(±386.3)
0.884
n=46 n=68 n=291 n=417
Gestation(w) 35.4(±4.7) 34.6(±4.4) 0.372 39.3(±2.4) 39.5(±2.3) 0.454
Preterm(<37w)
25(54.3%) 47(69.1%) 0.109 38(13.1%) 47(11.3%) 0.472
N=52 N=75
Lactate1 4.4(3.8-5.2) 4.9(4.4-5.4) 0.263 4.7(4.4-4.9) 4.8(4.6-5.1) 0.333
Lactate>5.45 19(36.5%) 27(36.0%) 0.950 99(34.3%) 165(38.8%) 0.215
Resuscitation 22(43.1%) 34(44.2%) 0.909 47(16.5%) 90(20.5%) 0.181
Apgar<7 at 1min
14(27.5%) 24(32.0%) 0.585 30(9.8%) 56(12.8%) 0.209
Apgar <7 at 5min
7(13.7%) 16(21.3%) 0.278 12(3.9%) 19(4.3%) 0.771
Special carenurseryadmission
25(48.1%) 41(52.6%) 0.616 30(9.6%) 38(8.6%) 0.621
Admissiontype
None 27(55.1%) 37(48.7%) 0.687 281(91.5%) 402(91.2%) 0.664
Ward 15(30.6%) 24(31.6%) 6(2.0%) 13(2.9%)
Highdependencyunit /Intensive careunit
7(14.3%) 15(19.7%) 20(6.5%) 26(5.9%)
Data summaries are mean (±SD) or N (%), as appropriate. P-values less than 0.025 consideredstatisticallysignificantwithaBonferronicorrection.1Dataaresummarisedasgeometricmeanand95%confidenceintervals.

251
MODEOFDELIVERYANDNEONATALOUTCOMESFORALLDELIVERIES
Therewere 2,436births during the entire pre-interventionperiod, and 2,232during
thepost-interventionperiod.Duringthepre-interventionperiodtherewere932/2436
cesarean deliveries (38·3%), which decreased in the post-intervention period to
653/2232 (29·3%, P<0·001). There was no change in rate of elective caesarean
sections; 240/2436 (9.9%) to 254/2232 (11.4%, P=0.09). There was no difference in
instrumental births 73/2436 (3%) to 81/2232 (3.6%, P=0.227). Emergency caesarean
deliveries decreased from 692/2436 (28·4%) to 399/2232 (17·0%, P<0·001), and
neonataladmissionsdecreasedfrom450/2436(18·5%)to349/2232(15·6%,P=0·010).
Adiagnosiswasrecordedfor360(80%)admissionsinthepre-interventionperiodand
278 (80%) of admissions in the post-operative period. The commonest reasons for
admission in the pre-intervention period were respiratory distress syndrome (RDS)
(19.7%), neonatal jaundice (NNJ) (13.1%), congenital infections (8.6%), hypoglycemia
(7.5%),hypoxicischaemicencephalopathy(HIE)(7.2%),andprematurity(7.2%).Inthe
post intervention period the commonest reasons were RDS (19.1%), NNJ (12.2%),
hyalinemembranedisease(HMD)(10.1%),transienttachypneaofthenewborn(TTN)
(10.1%),lowbirthweight(LBW)(8.6%)andHIE(7.9%).
DISCUSSION
This study explored the impact of an educational program coupled with the
introduction of UA lactate sampling in a low-resource setting on intrapartum

252
outcomes. Previous studies have been based in high-income settings(16) and itwas
notclearwhetherthepreviouslyobservedbenefitsinearlierstudieswouldtranslateto
alowerresourcecentre.Whiletherewasnosignificantdifferenceinthecordlactate
results between the two groups, we found a reduction in the CS rate without
worseninganyofneonataloutcomes.Thelargestcontributortothisreductionwasin
CS for suspected fetal compromise. A significant reduction post-intervention was
observed inCS,emergencyCS, andneonatal admissions forallwomen regardlessof
whethertheywererecruitedtothestudyforlactatemeasurementornot.Whilethese
overallresultsarenotadjustedforconfoundingfactors,theyarereassuring;thefalling
CSratehasnotworsenedfetalandneonataloutcomes,and,basedonthereductionin
overall neonatal unit admission rate, may have improved them. The impact of an
educational program on fetal physiology and intrapartum heart rate monitoring
demonstratedbenefitsthatweretranslatedtoallwomeninthelabourwardandwe
speculate this should be sustainedwhen coupledwith the introduction of universal
cordlactatesamplingforongoingclinicianoutcomefeedback.
There is evidence that the lack of appropriate interpretation of fetal monitoring in
South Africa contributes to the unacceptably high intrapartum and early neonatal
mortality rates(17, 18). Equally, there is evidence that theprocessofqualityof care
audit and the feedback to cliniciansof theUA lactate resultsmay improvematernal
and neonatal outcomes(12, 19). Given the reduction in suspected fetal compromise
without an increase in adverse neonatal outcomes that occurred following our
intervention,wehypothesise that theobjective feedbackavailable to clinicians from

253
the UA lactate result highlighted recognition on CTG interpretation of the “true”
acidemic cases. This theorymaybe supportedby the trend to lessneonatalnursery
admissionsinthestudygroupandthesignificantlylessadmissionsoverallinthepost-
intervention study period, regardless of trial recruitment status. In addition, we
observed an increase in delayed labour progress in the post-intervention group
without worse neonatal outcomes; it may be that less early interventions for
suspectedfetaldistressallowedotherpotentialcomplicationsoflongerlabourslabor
tobecomeapparent.
Interestingly,therewerelessmaternalproblemsinthepostinterventionperiod,which
plausibly could have resulted in fewer fetuses at risk of compromise. There were,
however, significantly less intrapartum transfers from referral facilities in the post-
interventionperiod. Thenatureof an intrapartum transfer indicates thewomenare
morelikelytohavematernalrelatedpregnancyproblems,necessitatingup-referralto
a tertiary unit(20, 21), and this may have accounted for some of the reduction in
maternalcomplicationsinthepost-interventionperiod.
TherewasnosignificantchangeintheelectiveCSrate,withthereductioninourstudy
almost exclusively intrapartum non-elective CS, which remained significant when
adjustedforprimiparity.Thisiswherewebelievethestrengthofthisinterventionlies
–inpreventingthefirstCS,particularconsideringevidencesuchasthatofVillaretal,
demonstrating that intrapartum caesarean section in a sample of nearly 100000

254
deliveries in 8 Latin American countries was associated with an increased risk in
severalmaternalandneonatalmorbidityandmortality(22).TheRobsonclassification
for caesarean section is widely used tomonitor CS rates internationally(23), with a
particularfocusonreducingcaesareansectioninnulliparouswomen(group1and2in
theRobsonclassification)andthosewithapreviouscaesareansection,(group5),with
thelatteraclearconsequenceoftheformer(1).Althoughheterogeneousinthequality
ofincludedstudies,arecentmeta-analysishasdemonstratedthatqualityofcareaudit
usingtheRobsonclassificationsystemtomonitorcesareansectionratescanresultina
reduction in CS(24). In our studywe introduced a quality of care audit process and
providedinstantfeedbacktothecliniciansintheunit,withareductioninCSinwomen
ingroups1and2oftheRobsonclassification.
Reduction inCS isofparticular importance inSouthAfrica,aswomeninthiscountry
are more likely to die following a CS compared with a vaginal birth(25). This is
particularly concerning as 22·6% of deliveries in South Africa are by CS, and in
provincialtertiaryhospitals,asistheunitinthisstudy,therateis35·2%(26).Moreover,
maternaldeathsrelatedtoCShavebeenincreasing,anddisturbingly,largenumbersof
theseareduetoperioperativehaemorrhage(27),withsurgical traumabeingoneof, if
notthemostcommon,reasonfordeath(28,29).ThereductioninCSinourstudy(bothin
theincludedcasesandoverallduringthestudyperiod)hasthepotentialforimmediate
and downstream effects for future pregnancies, as well as long-term outcomes for
womenandtheirfamilies.

255
Finally, testing forpotential fetal acidemiawith lactateonahandheld,pointof care
devicehasseveraladvantages.Firstly;itmaybemorefeasible(botheconomicallyand
in ease of use) than other measures (such as paired arterial and venous cord gas
sampling), especially in the limited resource setting. Secondly, the hand-held device
correlateswellwithlaboratoryanalysers,addingvaliditytotheprocessofpointofcare
testing(30,31).
STRENGTHS
To our knowledge this is the largest assessment of an intervention using umbilical
lactatemeasurementanditsimpactinalowormiddleincomecountryonintrapartum
obstetric management(16), and is likely representative of the unit as a whole. The
presenceofasingleresearcheronthelaborward(EA)tooverseethetrainingofhealth
care providers in sample collection and ensure complete data collection throughout
thestudyperiodaddstotheinternalvalidityoftheresults.
LIMITATIONS
It is difficult to separate the impact of the fetal physiology and CTG interpretation
trainingwiththelactatesamplingonthechangeinpracticefollowingtheintervention,
and indeed it is likely the combination of both that has created a management
package. All staffwho cared forwomen inour studyhadpreviously completed the
essential steps in themanagement of obstetric emergencies (esmoe) course, which

256
includes a module on ctg interpretation. this suggests that the addition of the ua
lactateandthequalityofcareauditprocessaroundthiswasthemainfactorinpractice
change. however, ongoing revision of ctg interpretation is an essential element in
labourwardpracticeandwerecommendregularcasereviewandeducationprograms.
Aspartof this study,we introducedpointof care testing,andalthough trainingwas
undertaken for all involved in the collection, we do not have paired samples (both
arterial and venous) to provide confirmation of arterial sampling.We are, however,
reassured by the fact that venous lactate is shown to be predictive of arterial lactic
acidaemia,andthat thepreviousoptimalcut-off for lactateweobtainedusing these
sampleswasverysimilartoalargecohortincludingpairedsamples(13).
CONCLUSION
The introduction of UA lactate has the ability to significantly reduce the CS rate
without increasing adverse neonatal outcomes in a low-resource setting. Further
researchtoexpandthebodyofevidenceontheuseofUAlactatesamplinginlowand
middle-incomecountriesisneeded.

257
ABBREVIATIONS
aOR Adjustedoddsratio
AVD Assistedvaginaldelivery
CI Confidenceintervals
CS Caesareansections
CTG Cardiotocograph
CV Coefficientofvariation
HIE Hypoxicischaemicencephalopathy
HIV Humanimmunodeficiencyvirus
HMD Hyalinemembranedisease
LBW Lowbirthweight
NNJ Neonataljaundice
OR Oddsratio
RDS Respiratorydistresssyndrome
TTN Transienttachypnoeaofthenewborn
UA Umbilicalartery
VBAC Vaginalbirthaftercaesarean

258
DECLARATIONS
ETHICSAPPROVALANDCONSENTTOPARTICIPATE
This study was approved by the ethics committees of The University of Western
Australia Human Research Ethics Committee on the 26/02/2014 (Reference number
RA/4/1/6581), the University of Pretoria, Pretoria, South Africa on the 10/02/2014
(Referencenumber7/2014).
Allparticipantsconsentedtothestudy.
Availabilityofdataandmaterials:
The datasets used and/or analysed during the current study are available from the
correspondingauthoronreasonablerequest.
COMPETINGINTERESTS
Theauthorsreportnoconflictsofinterest

259
FUNDING
EAisaPhDcandidatefundedbytheUniversityofWesternAustraliawithanAustralian
PostgraduateAward,andanAthelstanandAmySawMedicaltop-upscholarship,and
by the Women and Infants Research Foundation with a Gordon King Doctor of
Philosophyscholarship.
AUTHORS'CONTRIBUTIONS
ERAdesignedthestudy,supervisedtheconductofthestudy,collectedthedata,wrote
the initial manuscript, and approved the final manuscript. EAN contributed to the
designofthestudy,analysedthedata,andapprovedthefinalmanuscript.RCPandJED
contributed to the design of the study, supported the conduct of the study, and
approvedthefinalmanuscript.
ACKNOWLEDGEMENTS
The authors would like to thank the midwives, doctors, and women of Kalafong
Hospitalfortheirsupportinrunningthisstudy.

260
REFERENCES
1. VogelJP,BetránAP,VindevoghelN,SouzaJP,TorloniMR,ZhangJ,etal.Useofthe Robson classification to assess caesarean section trends in 21 countries: asecondary analysis of two WHO multicountry surveys. The Lancet Global health.2015;3(5):e260-e70.2. Betrán AP, Ye J, Moller A-B, Zhang J, Gülmezoglu AM, Torloni MR. Theincreasing trend in caesarean section rates: global, regional and national estimates:1990-2014.PLoSOne.2016;11(2):e0148343.3. BetranAP,TorloniMR,Zhang J, Ye J,MikolajczykR,Deneux-TharauxC,et al.Whatistheoptimalrateofcaesareansectionatpopulationlevel?Asystematicreviewofecologicstudies.Reproductivehealth.2015;12(1):57.4. Lumbiganon P, LaopaiboonM,Gülmezoglu AM, Souza JP, Taneepanichskul S,RuyanP,etal.Methodofdeliveryandpregnancyoutcomes inAsia: theWHOglobalsurveyonmaternalandperinatalhealth2007–08.TheLancet.2010;375(9713):490-9.5. CaugheyAB,CahillAG,GuiseJ-M,RouseDJ,ObstetriciansACo,Gynecologists.Safe prevention of the primary cesarean delivery. Am J Obstet Gynecol.2014;210(3):179-93.6. Spong CY, Berghella V,Wenstrom KD,Mercer BM, SaadeGR. Preventing thefirstcesareandelivery:summaryofajointEuniceKennedyShrivernationalinstituteofchild health and human development, society for maternal-fetal medicine, andAmerican college of obstetricians and gynecologists workshop. Obstet Gynecol.2012;120(5):1181.7. BarberEL,LundsbergL,BelangerK,PettkerCM,FunaiEF,IlluzziJL.Contributingindicationstotherisingcesareandeliveryrate.ObstetGynecol.2011;118(1):29.8. Chauhan S, Beydoun H, Hammad I, Babbar S, Hill J, Mlynarczyk M, et al.Indications for caesarean sections at≥ 34 weeks among nulliparous women anddifferential composite maternal and neonatal morbidity. BJOG. 2014;121(11):1395-402.9. AlfirevicZ,DevaneD,GyteGM.Continuouscardiotocography(CTG)asaformofelectronicfetalmonitoring(EFM)forfetalassessmentduringlabour.TheCochraneLibrary.2013.10. Wiberg-ItzelE,LipponerC,NormanM,HerbstA,PrebensenD,HanssonA,etal.DeterminationofpHorlactateinfetalscalpbloodinmanagementofintrapartumfetaldistress:randomisedcontrolledmulticentretrial.BMJ.2008;336(7656):1284-7.11. MorinC,ChartierM,BounanS,HatemG,GoffinetF,LeRayC.FetalscalppHduring labor:Which threshold for intervention? Journalofgynecologyobstetricsandhumanreproduction.2017;46(2):183.12. White CR, Doherty DA, Newnham JP, Pennell CE. The impact of introducinguniversalumbilicalcordbloodgasanalysisandlactatemeasurementatdelivery.AustNZJObstetGynaecol.2014;54(1):71-8.13. Allanson E, Pattinson R, Nathan E, Dickinson J. The introduction of umbilicalcord lactate measurement and associated neonatal outcomes in a South Africantertiary hospital labor ward. The Journal of Maternal-Fetal & Neonatal Medicine.2017:1-7.

261
14. Baldari C, Bonavolonta V, Emerenziani GP, Gallotta MC, Silva AJ, Guidetti L.Accuracy,reliability, linearityofAccutrendandLactateProversusEBIOplusanalyzer.EurJApplPhysiol.2009;107(1):105-11.15. AllansonE, R, Pattinson,RC,Nathan, EA,Dickinson, JE. The impactofHIVonperinataloutcomesinaSouthAfricanlabourward.2017.16. Allanson E,Waqar T,White C, Tunçalp Ö, Dickinson J. Umbilical lactate as ameasureofacidosisandpredictorofneonatalrisk:asystematicreview.BJOG.2016.17. Buchmann EJ, Pattinson RC. Babieswho die from labour-related intrapartumhypoxia: a confidential enquiry in South African public hospitals. Trop Doct.2006;36(1):8-10.18. BothmaM,BuchmannEJ.Astudyoffreshstillbirthsweighing2500gormoreatthree academic hospitals in South Africa. International journal of gynaecology andobstetrics: the official organ of the International Federation of Gynaecology andObstetrics.2016;134(2):186-9.19. Allanson ER, Pattinson RC. Quality-of-care audits and perinatal mortality inSouthAfrica.BullWorldHealthOrgan.2015;93(6):424-8.20. GandhiM,WelzT,RonsmansC.SevereacutematernalmorbidityinruralSouthAfrica.InternationalJournalofGynecology&Obstetrics.2004;87(2):180-7.21. SchoonMG.Impactofinter-facilitytransportonmaternalmortalityintheFreeStateProvince.SAMJ:SouthAfricanMedicalJournal.2013;103(8):534-6.22. VillarJ,CarroliG,ZavaletaN,DonnerA,WojdylaD,FaundesA,etal.Maternaland neonatal individual risks and benefits associated with caesarean delivery:multicentreprospectivestudy.BMJ.2007;335(7628):1025.23. BetranAP,VindevoghelN,SouzaJP,GulmezogluAM,TorloniMR.Asystematicreviewof the Robson classification for caesarean section:whatworks, doesn'tworkandhowtoimproveit.PLoSOne.2014;9(6):e97769.24. Boatin AA, Cullinane F, TorloniMR, BetranAP. Audit and feedback using theRobson classification to reduce caesarean section rates: a systematic review. BJOG.2017.25. Gebhardt S, editor Preparing for caesarean delivery: review. Obstetrics andGynaecologyForum;2015:InHousePublications.26. PattinsonR,Rhoda,N.Savingbabies2012-2013:NinthreportonperinatalcareinSouthAfrica.TshepesaPress,Pretoria,SouthAfrica;2014.27. FawcusS,PattinsonRC,MoodleyJ,MoranNF,SchoonMG,MhlangaRE,etal.Maternal deaths from bleeding associated with caesarean delivery: A nationalemergency.SAfrMedJ.2016;106(5):53-7.28. MaswimeS,BuchmannE.Causesandavoidablefactorsinmaternaldeathdueto cesarean-related hemorrhage in South Africa. Int J Gynaecol Obstet.2016;134(3):320-3.29. Gebhardt GS, Fawcus S,Moodley J, Farina Z.Maternal death and caesareansection in South Africa: results from the 2011-2013 saving mothers report of thenational committee for confidential enquiries into maternal deaths. SAMJ: SouthAfricanMedicalJournal.2015;105(4):287-91.30. Labrecque L, Provencal M, Caqueret A, Wo BL, Bujold E, Lariviere F, et al.CorrelationofcordbloodpH,baseexcess,andlactateconcentrationmeasuredwithaportabledevice for identifying fetal acidosis. JObstetGynaecolCan. 2014;36(7):598-604.

262
31. Karon BS, Scott R, Burritt MF, Santrach PJ. Comparison of lactate valuesbetween point-of-care and central laboratory analyzers. Am J Clin Pathol.2007;128(1):168-71.

263
CHAPTERNINE:IMPACTOFMATERNALHIVONUMBILICALCORD
LACTATEMEASUREMENTATDELIVERYINASOUTHAFRICANLABOUR
WARD

264
CHAPTEROVERVIEW
Asoutlined inChapter8,21%of thewomen included inour trialwereHIVpositive.
ThereareconflictingdataontheroleofHIVinfectioninintrapartumoutcomes.Itwas
thereforeimportanttoconsideriftheperinataloutcomesinourstudywereimpacted
bymaternalHIVstatus.

265

266

267

268

269

270
CHAPTERTEN:ATTITUDESTOWARDSTHEIMPLEMENTATIONOF
UNIVERSALUMBILICALARTERYLACTATEANALYSISINASOUTH
AFRICANDISTRICTHOSPITAL

271
CHAPTEROVERVIEW
The capacity to translate research into practice is potentially difficult in all areas of
medicine,nonemoresothanmaternalandnewbornhealthinLMIC,wherehighrates
of mortality persist despite clear evidence on the steps to prevention(1). Having
establishedtheutilityandeffectivenessofintroducingumbilicalarterylactate(withina
packageof interventionsincludingCTGeducation) inaresearchsettinginanLMIC, it
wasnextpertinent to consider the implementationof the tool inpractice. It is clear
thatoneofthepotentialchallengestoanynewtool inLMICsettings isthepotential
forburdenonalready limitedresources.Asoutlined inchapter3, thiscomponentof
theresearchwasconductedatZithuleleHospital intheeasterncapeofSouthAfrica,
whereweassessedstaffattitudestowardstheintroductionofUAlactatesampling.

272

273

274

275

276

277

278
CHAPTERELEVEN:DISCUSSION
279
OVERVIEW
Thisthesisconsistsofcomprehensiveseriesofclinicaltrialsanddatasetanalysesthat
demonstratethatthe introductionofumbilicalcordartery lactatesampling isuseful,
feasibleandacceptableinaresourcepoorMICsetting.Ihavesystematicallyexplored
the causes of perinatalmortality in South Africa, the diagnostic test accuracy ofUA
lactate,theroleofQoCauditinperinatalmortalityinSouthAfrica,andtheeffectsof
the implementation on UA lactate sampling. The key findings are summarised as
follows:
• In a comprehensive data set representative of a total obstetric population in
South Africa, 49.5% and 74.2% of women having a late stillbirth or early
neonataldeathwerehealthy(nocomplicationsofpregnancyor labour)anda
quarteroftheperinataldeathsfollowedintrapartumasphyxia.
• Inthefirstsystematicreviewofthediagnostictestaccuracyofumbilicallactate
for measuring acidosis and predicting neonatal outcome, including 38,284
patients, lactatewas shown to correlatewith pH (pooled ES -0.650 95% CI -
0.663to-0.637,p<0.01),BE(pooledES-0.71095%CI -0.721—0.699,p<0.01),
andApgarscoreat5minutes(pooledES0.395%CI0.193-0.407p<0.01).Using
thecommonthresholdoutcomeofHIE,lactatehasasensitivityof69.7%anda
specificityof93%.
• In the largest analysis of the impact of QoC audit on perinatalmortality,we
interrogatedthechangesinPNMRin163SouthAfricanfacilitieswithatleast5

280
yearsofcontinuousQoCauditdata.3,406,347birthsand85,728deathswere
included and 29% of facilities had a decrease in their PNMRwith 5 years of
continuousQoCaudit.Facilitieswithincreasingmortalityappearedlesslikelyto
haveacomprehensiveQoCauditprocess.
• Ina largecohortof946babieswithaUAlactatesample,wedeterminedthat
theoptimal cut-off for lactate for theoutcomeofneonatal resuscitationwas
5.46mmol/L (sensitivity 68%, specificity 72%), for neonatal admission was
4.95mmol/L (sensitivity61%,specificity59%),andforanApgarscoreof<7at
fiveminuteswas5.65mmol/L(sensitivity64%,specificity69%).
• In a before and after trial assessing the impact of introducing UA lactate
sampling,wefoundnodifferenceinmeanlactate(4.6mmol/L{95%CI4.4-4.8}
comparedwith4.9mmol/L{95%CI4.7-5.1},p=0.089).Howeversuspectedfetal
compromisewasreducedinthepost-interventionperiod:30·2%vs.22·1%,aOR
0·71, 95% CI 0·52-0·96, p=0·027 without worsening neonatal outcomes.
Caesarean section rateswere significantly reduced in the univariate analysis:
pre- 40·3% vs. post-intervention 31·6% (p=0·007). This reduction remained
significantwhenadjustedforpreviouscaesareansection,primiparity,maternal
HIV infection and preterm birth (aOR 0·72, 95%CI 0·54-0·98, p=0·035).
Moreover,emergency caesareandeliveries in theunit asawhole (not just in
patients recruitedtothetrial)decreasedfrom692/2436(28·4%)to399/2232
(17·0%,P<0·001), andneonatal admissionsdecreased from450/2436 (18·5%)
to349/2232(15·6%,P=0·010).
• Inthe21.6%ofwomeninourbeforeandaftertrialthatareHIVpositive,there
was no impact of either their disease or the use of HAART on the preterm

281
delivery rate, mode of delivery, neonatal resuscitation rate, 1 or 5 minute
Apgar score below 7, or the rate of having a UA lactate level greater than
5.45mmol/L.
• InthefinalstudyassessingtheattitudesandbarrierstointroducingUAlactate
sampling,themajorityofmidwivesanddoctorsprovidingintrapartumcareina
SouthAfricandistricthospitalwerepositiveaboutboththeroleofUAlactate
analysis as well as the potential benefits it provides. Training aided in
overcoming some of the perceived barriers to implementing UA lactate
sampling.
APPLICABILITYOFTHERESEARCH
THEMANAGEMENTOFINTRAPARTUMASPHYXIA
MostperinataldeathsinLMICarepreventable(2)anditisreiteratedrepeatedlyinthe
literature that the use of QoC measures is associated with improved maternal and
neonataloutcomes.Thisisparticularlytrueofintrapartumstillbirthsandintrapartum
relatedneonataldeaths(3,4),as is the focusof the research in this thesis. It is clear
that intrapartum hypoxia and asphyxia need to remain a focus of global efforts to
reduce perinatal mortality, as we have demonstrated in the analysis of causes of
perinataldeathinSouthAfrica(Chapter3)aswellasintheapplicationoftheICD-PM
to perinatal deaths (Appendix 2.1). It isworth noting that in high-income countries,

282
intrapartumasphyxiaisalsooftenassociatedwithstaff-relatedqualityofcareissues(5-
9),andsothereispotentialapplicabilityofthisthesisoutsideofanLMIC.
THEUSEANDBENEFITSOFUALACTATESAMPLING
Theuseof umbilical artery lactate in LMIC is only applicable to facility-basedbirths,
which remain uncommon in many LMIC(10). However, there are many places
internationallywithsimilarratesoffacility-basedbirthandintrapartumissuesasSouth
Africa. InBrazil, forexample,more thana thirdofperinataldeathsaresecondary to
asphyxia,andfacility-basedbirthisusual(11).Wewouldthereforeanticipatethatthis
trial could be replicated in other resource-limited settings. Equally, umbilical cord
assessmentofacidosis isusedfrequently inhigh-incomecountriesandwewereable
to conduct a large meta-analysis showing that this can conducted using lactate
measurementonasimplehandheldmachine,expandingtheapplicabilityofthisthesis.
While there is need for complex multifactorial approaches to improve perinatal
mortality inLMIC(12,13),theprocessofUAlactatesamplingcanformapartofthis.
However, itwasimportantthatweconsiderthebalanceof impactonresourceswith
thepotential for improvedoutcomeswhen implementingour trial. Simplemeasures
suchasuseofthepartograminlabour,orbasicneonatalresuscitationarecomponents
ofQoCthatarepositivelyassociatedwithmaternalandperinatalsurvival,andthese
basicmeasuresarecriticalbeforeconsiderationofcomplex technologicalanswers to
perinatalmortality(14-19).Thefeasibilityof introducingUA lactatesamplingoutlined

283
inChaptersixinadditiontothepositiveattitudesofstaffseeninthestudyinChapter
ninemakesitpossiblethatthisinterventioncouldbeintroducedalongsideotherQoC
measures. However, oversaturation of existing resources in combination with
deficiencies in QoC contributes to adverse maternal and perinatal outcomes in
LMIC(20)(Figure10.1).
Image11.1CrowdedantenatalwardatKalafongHospital
WhileIsawsomebenefitwiththeintroductionofUAlactatesampling(lower
caesareandeliveriesandreducedadmissions to thenursery), therewasno
apparent change in neonatal acidosis or mortality. It was important to
consider that the benefits of introduction were greater than any risks. In

284
Chapter2IshowedthePerinatalCareIndicators(PCI)forKalafongfor2013,
prior to the intervention and outlined below are the same PCI for 2014,
duringwhichourtrialwasconducted(Table11.1).Itwasreassuringtonote
that PNMR was lower in 2014 than in 2013, so while there was not a
significant result in our trial for this outcome, the introduction of the
samplingdidnotworsenKalafong’soutcomes.
Table11.1PerinatalcareindicatorsforKalafongHospital,2014
ItisalsoreassuringtoobservethattheUAlactatelevelsinwomenwithHIVinfection
in this thesiswere no differentwhen comparedwithwomenwithout HIV, and that
their neonatal outcomes were similarly comparable. The burden of HIV distribution

285
overlapswiththeglobalburdenofadverseperinataloutcomes,andUAsamplingcan
beconfidentlyimplementedinthesesettings.
TRANSLATINGRESEARCHINTOCLINICALPRACTICE
Itwas clear during the implementationof this quality of care intervention that staff
ownershipoftheprocesscontributedtothesuccessof thetrial.Bothmidwiferyand
medicalstaffbecameinvestedintheprocess,andcouldseethefruitsoftheir labour
on a daily basis (Image 11.2). A quality improvement program in India similarly
described health care training and ownership of a maternal and newborn quality
improvementprogramthat resulted insignificant results(21).The introductionofUA
lactatesampling inothersettingswillclearlyrequirestaffbuy-inandcommitmentto
eachpartoftheQoCauditprocess,ratherthanjustthesamplingitself.

286
Image 11.2 The primary author of this thesis and SisterMaria, Matron of Kalafong
Hospitallabourward
THEIMPLEMENTATIONOFQOCAUDIT
Audit can objectively identify areas where QoC interventions can be targeted.
However, our analysis demonstrated that audit alone does not necessarily improve
mortalitygiven thevariation indirectionof trends inmortalityof163 siteswith five
years of continuous audit. Thus, the assumption is false that once a problem is
identified health care providers will make an automatic correction and solve the
problem.TheintroductionoftheUAlactatesamplingandthedailyandweeklyreview
of cases in this thesis was a QoC audit process, which appeared to have some
beneficialoutcomes, includingareduction intherateofCS.Moreover, thereal-time
qualityofcarefeedbackmayhaveotherbenefits;immediatepostnatalcareimproves
probability of neonatal survival in sub-Saharan Africa(22) and so the process of

287
obtaining a lactate sample may identify an additional safety net for clinicians to
recognisetheat-riskneonate.
Thereremainseveralchallengestoimplementingaudits.Inorderforaudittohaveany
effectonperinatalcare,itmustbeimplementedinasystemthatissupportiveofthe
requirements for audit. An assessment in Dar es Salaam hospitals (with a hospital
basedMMRof1602/100000livebirthsandaPNMRof123/1000livebirths)showeda
lack of internal infrastructure for audit as well as clinical staff support and
responsibility.This resulted inanessentially ineffectiveprocess–withvery fewstaff
surveyedbeingabletonameasingleoutcome/changeasaresultofaudit(23).Audit
must leadintodatareportingtoappropriatehealthcareprofessionalsfollowedbya
processofimplementingchangetomakeitarelevanttool.QualitativeanalysisofPPIP
showsthattheabilitytosustainauditandimplementchangesrequiresmotivatedstaff
(amulti-levelandmulti-disciplinaryapproach) toconductandbe responsible for the
program(24). This is one of the potential challenges of audit as a tool to improve
perinatalmortality–ifitisonlyintroducedasapointintimecapturetoolratherthan
asanagentofprogresstochange,thenanyeffectshavethepotentialtobeveryshort
lived.

288
STRENGTHSOFTHERESEARCH
Thestrengthsofthisresearchlieinthelargeclinicaltrialssupportedbycomprehensive
dataanalysesoftherelatedevidence.Theassessmentofcausesofperinatalmortality
was from largepopulationbaseddata, truly reflectiveof theusual stateofobstetric
outcomesinSouthAfrica.Themeta-analysisofthediagnostictestaccuracyoflactate
samplingincludeabroadsearchtermsystematicreview,withmorethan40,000titles
andabstractsscreenedtoensureanycohortassessinglactateasameasureofacidosis
was captured. More than 38,000 women were included in the analysis in the first
comprehensivesystematic reviewofusing lactateasameasureofacidosis.TheQoC
auditdata focusedon facilitieswithat least fiveyearsof continuousaudit,andwith
morethanthreemillionbirthsandnearly100,000deathsincluded,thelargenumbers
likelyreducedtheimpactofanyindividualfacilityconfoundersontheimpactofQoC
audit.AssessingtheuseandimpactofUAlactateinoursettingwas,toourknowledge,
the largest cohort ofUA lactate samples in an LMIC,with cut-off findings similar to
high-incomecountries.TheintroductionofUAsamplingwaspartofacomprehensive
QoC audit program, including focused educations and daily and weekly review
meetings, which was known to be important in the successful implementation of
qualityofcareauditprogramsinSouthAfrica(24).Equallyourlargecohortmakesthe
assessmentof the impactofHIV infectiononUA lactateresultsmorerobust.Finally,
wehaveconsideredthechallengesoftranslatingresearchintopracticeinLMIC

289
LIMITATIONSOFTHERESEARCH
Much of our supporting data (causes of perinatal mortality and the impact of QoC
audit) was retrospective and therefore subject to confounders that we could not
control for. Thiswas particularly true for the analysis of the impact of audit,where
there were no overt differences in the data between the facilities with increasing
comparedtodecreasingmortality.Clearlythereissomethingdifferentoccurringhere,
butwehadnocapacitytointerrogatethisissue.
TheuseofUA lactatemeasuringrequiresbothphysicalandhumanresources.While
onthesurfacetheseseeminsignificant,inlowresourcesettingsthisislesslikelytobe
thecase.Asurveyof53deliveryunitsintheDemocraticRepublicofCongofoundthat
notonehadthealloftheequipmentnecessarytoexecutebasicemergencyobstetric
andneonatalcare(25).Moreover, theavailabilityofCTG in thesesettings is far from
universal(26). These deficiencies are replicated innumerable times in the literature
acrossAfrica(27,28).Wethereforerecognisethat inLMICthebasicstepsneededto
reduce the high perinatalmortality burdenwould and should take priority over the
introduction of umbilical artery sampling. However there is great variability in units
withinLMICandwehaveshownbothfeasibilityandeffectivenessof introducingthis
tool.

290
Therewerepragmaticcomponentstomain lactatestudy,whichcouldbeconsidered
limitations.Onlyumbilicalartery lactatesweremeasured,and theabsenceofpaired
arterial and venous sampling may have resulted in inadvertent venous sampling in
somecases.Whileoursystematicreviewshowedthatvenouslactatecorrelatedwith
neonatal acidosis, this limitation potentially altered the lactate results in the study.
Furthermore, the sampling of lactateswas essentially a convenience sample, within
thelimitationsofboththemainresearcheraswellasthelimitedhumanresourcesof
the Kalafong obstetric unit. The resultsmust be interpretedwithin the potential for
sampling error given only a proportion of deliveries during the study period had an
umbilicalartery lactatesampling.Thatsaid,therewasevidencethattheintervention
potentially impacted the care in theunit as awhole (reduction in caesarean section
ratesinalldeliveries)andsothesamplingandoutcomesmaybereflectiveoftheunit
overallduringthestudyperiod.
It isalsoclear thatwecannotseparate theCTGtrainingcomponentof thetrialwith
thelactatesamplingintermsoftheimpactonmaternalandneonataloutcomes.We
know that training in fetal monitoring in large cohort studies is associated with
improvedneonataloutcomes(29).However the lactatesamplingcanonlyadd to the
understanding of the fetalmonitoring,which is critical if themonitoring is to be of
benefitwithcorrectclinicalmanagementwhereappropriate(30,31).

291
FUTUREDIRECTIONSFORRESEARCH
Sincetheconductofourclinicaltrial,weareawareofasimilarcohortstudyinMalawi
being commenced to review umbilical arterial lactate and neonatal outcomes(32).
There is large variance in the levels of intrapartum resources, care andoutcomes in
LMIC and ongoing large cohort studies looking at the role of UA lactate to improve
intrapartumcarewouldbeappropriate.Weinitiallyhypothesisedthattheintroduction
of UA lactate sampling would result in an improvement in lactate levels over time,
however this was not borne out. It may be because our sample size was relatively
small compared to other large cohorts that have proved that hypothesis(33), and
further testing in larger LMICcohortswouldbeappropriate. Equallyweaccept that
thecomplexfacetsofbothantenatalandintrapartumcareinoursettingmaylimitthe
impactofthissingleintervention.
CONCLUSION
The initial concept for this thesis stemmed from the overwhelming burden of
intrapartumhypoxiaandasphyxiatoperinatalmortalityinLMIC.Aquarterofperinatal
deathsinSouthAfricafollowintrapartumasphyxiaandit ispossibleinthesesettings
to introduce quality of care audit that decrease perinatal mortality. The use of
umbilical artery lactate is both feasible and effective in South Africa, and can
contributetoimprovedmaternalandperinataloutcomes.

292
REFERENCES
1. Allanson ER, Tunçalp Ö, Vogel JP, Khan DN, Oladapo OT, Long Q, et al.Implementation of s in health facilities: a systematic review of cluster randomisedtrials.BMJglobalhealth.2017;2(2):e000266.2. TheL.Yemen'ssilentkillers.Lancet.2017;389(10070):672.3. Ariff S, LeeAC, Lawn J, Bhutta ZA.Global Burden, Epidemiologic Trends, andPrevention of Intrapartum-Related Deaths in Low-Resource Settings. Clin Perinatol.2016;43(3):593-608.4. CarloWA,McClureEM,ChombaE,ChakrabortyH,HartwellT,HarrisH,etal.Newborn care training of midwives and neonatal and perinatal mortality rates in adevelopingcountry.Pediatrics.2010:peds.2009-3464.5. Sadler LC, Farquhar CM, Masson VL, Battin MR. Contributory factors andpotentiallyavoidableneonatalencephalopathyassociatedwithperinatalasphyxia.AmJObstetGynecol.2016;214(6):747.e1-.e8.6. Eggermont M. Intrapartum care and substandard care: juridicalrecommendationstoreducetheriskofliability.ArchGynecolObstet.2015;292(1):87-95.7. Andreasen S, Backe B, Øian P. Claims for compensation after alleged birthasphyxia: a nationwide study covering 15 years. Acta Obstet Gynecol Scand.2014;93(2):152-8.8. Evers AC, Brouwers HA, Nikkels PG, Boon J, VAN EGMOND‐ LINDEN A,Groenendaal F, et al. Substandard care in delivery‐related asphyxia among terminfants:prospectivecohortstudy.ActaObstetGynecolScand.2013;92(1):85-93.9. BerglundS,GrunewaldC,PetterssonH,CnattingiusS.Riskfactorsforasphyxiaassociated with substandard care during labor. Acta Obstet Gynecol Scand.2010;89(1):39-48.10. Khanam R, Ahmed S, Creanga AA, Begum N, Koffi AK, Mahmud A, et al.AntepartumcomplicationsandperinatalmortalityinruralBangladesh.BMCPregnancyChildbirth.2017;17(1):81.11. AlmeidaMFB,KawakamiMD,MoreiraLMO,SantosR,AnchietaLM,GuinsburgR. Early neonatal deaths associated with perinatal asphyxia in infants >/=2500g inBrazil.JPediatr(RioJ).2017;93(6):576-84.12. Pasha O, McClure EM, Wright LL, Saleem S, Goudar SS, Chomba E, et al. Acombinedcommunity-andfacility-basedapproachtoimprovepregnancyoutcomesinlow-resource settings: a Global Network cluster randomized trial. BMC Med.2013;11(1):215.13. OsrinD,ProstA.Perinatalinterventionsandsurvivalinresource-poorsettings:whichwork,whichdon't,whichhavethejuryout?:BMJPublishingGroupLtd;2010.14. GetiyeY,FantahunM.Factorsassociatedwithperinatalmortalityamongpublichealth deliveries in Addis Ababa, Ethiopia, an unmatched case control study. BMCPregnancyChildbirth.2017;17(1):245.15. Kamath-RayneBD,Griffin JB,MoranK, JonesB,DownsA,McClureEM,etal.ResuscitationandObstetricalCaretoReduceIntrapartum-RelatedNeonatalDeaths:AMANDATEStudy.MaternChildHealthJ.2015;19(8):1853-63.

293
16. YismaE,DessalegnB,AstatkieA,FessehaN.CompletionofthemodifiedWorldHealthOrganization (WHO) partograph during labour in public health institutions ofAddisAbaba,Ethiopia.Reproductivehealth.2013;10(1):23.17. OdendaalHJ,GebhardtGS,TheronGB.Stillbirthratesinsingletonpregnanciesin a stable population at Karl Bremer and Tygerberg hospitals over 50 years.SAfr JObstetGynaecol.2013;19(3):67-70.18. Gans-Lartey F, O'Brien BA, Gyekye FO, Schopflocher D. The relationshipbetweentheuseofthepartographandbirthoutcomesatKorle-Buteachinghospital.Midwifery.2013;29(5):461-7.19. Alfirevic Z, Edwards G, Platt MJ. The impact of delivery suite guidelines onintrapartum care in 'standard primigravida'. Eur J Obstet Gynecol Reprod Biol.2004;115(1):28-31.20. MgayaA,Hinju J, KidantoH. Is timeof birth a predictor of adverseperinataloutcome?Ahospital-basedcross-sectional study ina low-resource setting, Tanzania.BMCPregnancyChildbirth.2017;17(1):184.21. SarinE,Kole SK,PatelR, SoodenA,Kharwal S, SinghR, et al. Evaluationof aquality improvement intervention for obstetric and neonatal care in selected publichealthfacilitiesacrosssixstatesofIndia.BMCPregnancyChildbirth.2017;17(1):134.22. SinghK,BrodishP,HaneyE.Postnatalcarebyprovidertypeandneonataldeathinsub-SaharanAfrica:amultilevelanalysis.BMCPublicHealth.2014;14:941.23. NyamtemaAS,UrassaDP,PembeAB,KisangaF,vanRoosmalenJ.Factors forchange inmaternalandperinatalauditsystems inDaresSalaamhospitals,Tanzania.BMCPregnancyChildbirth.2010;10(1):29.24. Belizán M, Bergh A-M, Cilliers C, Pattinson RC, Voce A. Stages of change: Aqualitative study on the implementation of a perinatal audit programme in SouthAfrica.BMCHealthServRes.2011;11(1):243.25. Ntambue AM, Malonga FK, Cowgill KD, Dramaix-Wilmet M, Donnen P.Emergencyobstetricandneonatalcareavailability,use,andquality:across-sectionalstudy in the city of Lubumbashi, Democratic Republic of the Congo, 2011. BMCPregnancyChildbirth.2017;17(1):40.26. LawrenceER,QuarshieEL,LewisKF,PeltzmanT,AndersonFJ. IntroductionofcardiotocographmonitoringimprovesbirthoutcomesinwomenwithpreeclampsiainGhana. International journal of gynaecology and obstetrics: the official organ of theInternationalFederationofGynaecologyandObstetrics.2016;132(1):103-4.27. KrukME,LeslieHH,VerguetS,MbarukuGM,AdanuRMK,LangerA.QualityofbasicmaternalcarefunctionsinhealthfacilitiesoffiveAfricancountries:ananalysisofnationalhealthsystemsurveys.LancetGlobHealth.2016;4(11):e845-e55.28. Lawani LO, Iyoke CA, Onoh RC, Nkwo PO, Ibrahim IA, Ekwedigwe KC, et al.Obstetricbenefitsofhealthinsurance:Acomparativeanalysisofobstetricindicesandoutcome of enrollees and non-enrollees in southeast Nigeria. J Obstet Gynaecol.2016;36(7):946-9.29. Brown L, Permezel M, Holberton J, Whitehead C. Neonatal outcomes afterintroduction of a national intrapartum fetal surveillance education program: aretrospective cohort study. The Journal of Maternal-Fetal & Neonatal Medicine.2017;30(15):1777-81.30. Woods D. Appropriate technology and education for improved intrapartumcareinunderresourcedcountries.SAfrJObstetGynaecol.2009;15(3).

294
31. Williams KP, Galerneau F. Intrapartum fetal heart rate patterns in thepredictionofneonatalacidemia.AmJObstetGynecol.2003;188(3):820-3.32. ChilindaGK,GadamaLA,StonesW.Point-of-careumbilicalarteriallactateandnewborn outcomes in a low resource setting: cohort study. BMC Res Notes.2018;11(1):477.33. White CR, Doherty DA, Henderson JJ, Kohan R, Newnham JP, Pennell CE.Benefitsof introducinguniversalumbilicalcordbloodgasandlactateanalysis intoanobstetricunit.AustNZJObstetGynaecol.2010;50(4):318-28.

295
APPENDICES

296
APPENDICESFORCHAPTER2
APPENDIX2.1:PAPERSBYTHETHESISAUTHORONTHEDEVELOPMENTOFTHEICD-PM

297

298

299

300

301

302

303

304

305

306

307

308

309

310

311

312

313

314

315

316

317

318

319

320

321

322

323

324

325

326

327

328

329
APPENDICESFORCHAPTER3

330
APPENDIX3.1:PATIENTINFORMATIONANDCONSENTFORMFORTHE“INTRODUCTIONOF
UNIVERSALCORDLACTATESAMPLINGANDCORRELATIONWITHNEONATALOUTCOMES”

331
332

333

334
APPENDIX3.2:DATACOLLECTIONSHEET

335

336
APPENDIX3.3:PRETRAININGCTGTESTFORDOCTORS(QUESTIONS)
PretrainingCTGtest
KalafongHospital
Name:______________________________________
Demographics(pleasecircle)
Male/female
Traininglevel:
Internyear1
Internyear2
Registraryear1/2/3/4/5
Other__________________
PreviousCTGtraining:

337
Noformaltraining
ESMOElecture
Other__________________
1) Earlydecelerationsare:
a) Duetoinhibitionofthesympatheticnervoussystem
b) Usuallybelow100beats/min
c) Alwaysphysiological
d) Reproducedbypressureovertheposteriorfontanelle
2) Latedecelerationsduetoreflexvagalstimulationusuallyareassociatedwith:
a) Fetaltachycardia
b) Fetalbradycardia
c) Increasedbaselinevariability
d) Normalbaselinevariability
e) Decreasedbaselinevariability
3) Themostimportantfeatureoflatedecelerationsis:

338
a) Thefrequencyoftheiroccurrence
b) Thedepthofthedecelerations
c) Durationofthedecelerations
d) Thetimefromonsetofcontractiontoonsetofdeceleration
e) Thetimefromcessationofthecontractiontocessationofthedeceleration
4) Theaccelerationswhich frequentlyprecedeandfollowvariabledecelerationsare
saidtoresultfrom:
a) Adrenalinerelease
b) Atropinerelease
c) Umbilicalarteryocclusion
d) Umbilicalveinocclusion
e) Totalcordocclusion
5) WhichofthefollowingisNOTimportantintheinterpretationofthe
significanceofvariabledecelerations:
a) Baselinevariability
b) Thedepthofthedecelerations

339
c) Thedurationofthedecelerations
d) Anincreasingbaselinerate
e) Thedurationfromonsetofthecontractionstoonsetofthedecelerations
6) Which of the following tests for the assessment of fetal wellbeing has been
validated through rigorous scientific investigation, and found to reduce perinatal
mortality?
a) Antenatalelectronicfetalmonitoring
b) Intrapartumelectronicfetalmonitoring
c) Amnioticfluidvolumeassessment
d) FetalumbilicalarteryDopplerassessmentinlowriskpregnancies
e) FetalumbilicalarteryDopplerassessmentinhighriskpregnancies

340
7) Thefollowingcordbloodgasresultsuggests:
UmbilicalArtery UmbilicalVein
pH 6.983 6.999
pO2 10.5 24.5
pCo2 100.6 92.8
BaseExcess -11.2 -10.8
a) Acuterespiratoryacidosis
b) Acutemetabolicacidosis
c) Chronicrespiratoryacidosis
d) Chronicmetabolicacidosis
e) Chronicmixedrespiratoryandmetabolicacidosis
8) Intermittent fetal heart rate monitoring has the same outcomes as continuous
monitoringif:
a) 1:1dedicatedmidwife
b) Allwomenhaverupturedmembranes(SROM,ARM)
c) Allbabieswithmeconiumhavecontinuousmonitoring

341
d) All suspected abnormalities on intermittent monitoring are confirmed by
continuousfetalmonitoring
e) Alloftheabove
9) WhichofthefollowingassociationswithasinusoidalFHRtraceisNOTtrue:
a) Vasapraevia
b) Feto-maternalhaemorrhage
c) Normalbaselinevariability
d) Rhisoimmunisation
e) Normalbaselinerate
10) Inanaerobicmetabolism
a) ThetissuepHrises
b) TheFHRpatternisalwaysunchanged
c) 29timesmoreenergyisproducedduringthedegradationofeachglucose
molecule
d) Lacticacidaccumulates
e) ThetissuepHdoesnotchange

342
11) Thefrequencyofepisodesof fetalbreathingmovements (chestwallmovements)
onultrasoundexaminationisdecreasedinallthefollowingconditionsEXCEPT:
a) Labour
b) Normalfetaloxygenation
c) Hypoglycaemia
d) CNSdepressantdrugs
e) Fetalacidosis
12) Followingdeliveryanumbilicalarterialbloodgasanalysisisreportedas:
Umbilicalartery Umbilicalvein
pH 7.08 7.34
pO2 14.6 20.4
pCO2 76.7 38.6
BaseExcess -9.1 -4.8
a) Acuterespiratoryacidosis
b) Acutemetabolicacidosis

343
c) Chronicrespiratoryacidosis
d) Acutemixedrespiratoryandmetabolicacidosis
e) Chronicmixedrespiratoryandmetabolicacidosis
13) TheInternationalCerebralPalsyTaskforceconsensusstatementoutlinesessential
criteriathatmustbepresenttoconsiderthatacute Intrapartumhypoxiawasthe
causeofcerebralpalsy.Whicharethecorrectstatements?
1) Evidenceofametabolicacidosisinintrapartumfetal,umbilicalarterialcordor
earlyneonatalblood(pH<7.00andbasedeficit>=12mmol/L)
2) Earlyonsetofsevereormoderateneonatalencephalopathyininfantsof>=34
weeksgestation
3) Cerebralpalsyofthespasticquadriplegicordyskinetictype
4) Evidenceofametabolicacidosisinintrapartumfetal,umbilicalarterialcordor
earlyneonatalblood(pH<7.20andbasedeficit>=6mmol/L)
(a) 1,2,3
(b) 2,3,4
(c) 2and4
(d) 1and3
(e) Alloftheabove

344
14) Followingdeliveryanumbilicalarterybloodgasanalysisisreportedas:
pH7.04
pO210
pCO250
BaseExcess–18
Thisdataisconsistentwith
a) Respiratoryacidosis
b) Mixedrespiratoryandmetabolicacidosis
c) Metabolicacidosis
d) Normalacidbasebalance

345
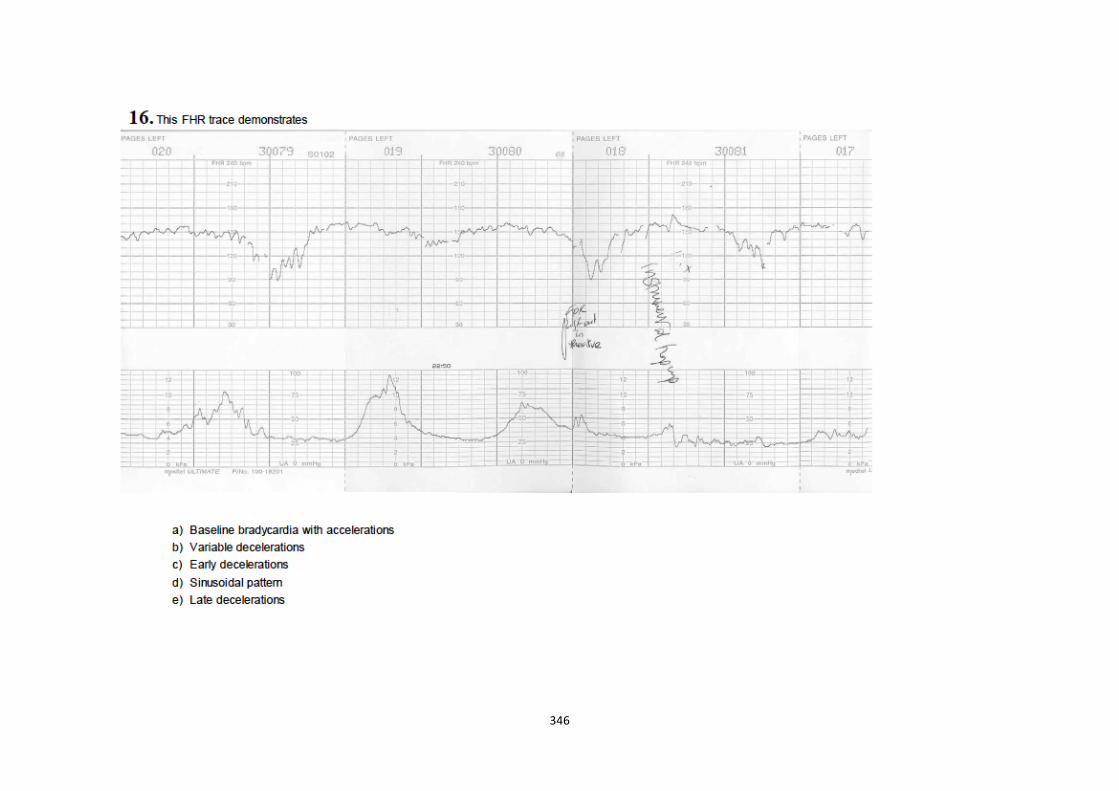
346

347

348

349

350
APPENDIX3.4:PRETRAININGCTGTESTFORDOCTORS(ANSWERS)
1. C
2. D
3. A
4. D
5. E
6. E
7. E
8. E
9. C
10. D
11. B
12. A
13. A
14. C
15. C
16. E
17. B
18. C
19. E

351
APPENDIX3.5:POSTTRAININGCTGTESTFORDOCTORS
PosttrainingCTGtest
KalafongHospital
1. FetalsleepstatesmaybeassociatedwithanyorallofthefollowingEXCEPT
a. AbsentVariability
b. NormalFHRvariability
c. Absentfetalbreathingmovements
d. Latedecelerations
e. Reducedfetalmovements
2. Earlydecelerationsare
a. Duetoinhibitionofthesympatheticnervoussystem
b. Usuallybelow100beats/min
c. Alwaysphysiological
d. Reproducedbypressureovertheposteriorfontanelle
e. Common

352
3. Whichofthefollowingisnotarecognisedcauseoflatedecelerations
a. Fetalheadcompression
b. Uterinehypertonia
c. Maternalhypotension
d. Uterinerupture
e. Placentalfailure
4. Latedecelerationsduetoreflexvagalstimulationusuallyareassociatedwith
a. Fetaltachycardia
b. Fetalbradycardia
c. Increasedbaselinevariability
d. Normalbaselinevariability
e. Decreasedbaselinevariability
5. Themostimportantfeatureoflatedecelerationsare
a. Thefrequencyoftheiroccurrence
b. Thedepthofthedecelerations

353
c. Durationofthedecelerations
d. Thetimefromonsetofcontractiontoonsetofdeceleration
e. Thetimefromcessationofthecontractiontocessationofthedeceleration
6. Theaccelerationswhichfrequentlyprecedeandfollowvariabledecelerationsare
saidtoresultfrom
a. Adrenalinerelease
b. Atropinerelease
c. Umbilicalarteryocclusion
d. Umbilicalveinocclusion
e. Totalcordocclusion
7. Regardingphysiologicalfetalheartratemechanismswhichoneofthefollowing
associationsisFALSE:
a. Earlydecelerationsareduetoheadcompression
b. Variabledecelerationsareduetocordcompression
c. Variabledecelerationsareduetofetalhypoxia
d. Latedecelerationsmaybeduetoareflexreceptorresponse

354
e.Latedecelerationsarealwaysduetomyocardialischaemia
8. WhenperforminganantenatalCTGafter10-20minutesnon-reactivitythemost
appropriateactionisto
a. Recommenddelivery
b. Informthemedicalofficer
c. Manuallypalpatethefetus(ifnotcontraindicated)andadministeradrink
tothemother
d. Repeatthetestthefollowingday
e. Performavaginalexamination
9. Which of the following tests for the assessment of fetal wellbeing has been
validated through rigorous scientific investigation, and found to reduce perinatal
mortality?
a. Antenatalelectronicfetalmonitoring
b. Intrapartumelectronicfetalmonitoring
c. Amnioticfluidvolumeassessment
d. FetalumbilicalarteryDopplerassessmentinlowriskpregnancies
e. FetalumbilicalarteryDopplerassessmentinhighriskpregnancies

355
10. Thefollowingcordbloodgasresultsuggests:
A V
pH 6.983 6.999
pO2 10.5 20.4
pCO2 100.6 92.8
BE -10.8 -11.2
a. Acuterespiratoryacidosis
b. Acutemetabolicacidosis
c. Chronicrespiratoryacidosis
d. Chronicmetabolicacidosis
e. Chronicmixedrespiratoryandmetabolicacidosis
11.Indicationsforcontinuousfetalmonitoringincludeallthefollowingexcept
a) Maternalautoimmunecondition(SLE)
b) Pregnancyinducedhypertension
c) Oligohydramnios

356
d) Allwomeninlabourat40weeksgestation
e) labourinduction
12. Intermittent fetal heart ratemonitoring has the same outcomes as continuous
monitoringif
a) 1:1dedicatedmidwife
b) Allwomenhaverupturedmembranes(SROM,ARM)
c) Allbabieswithmeconiumhavecontinuousmonitoring
d) All suspected abnormalities on intermittentmonitoring are confirmed by
continuousfetalmonitoring.
e) Alloftheabove
13.WhichofthefollowingassociationswithasinusoidalFHRtraceisNOTtrue
a) Vasapraevia
b) Feto-maternalhaemorrhage
c) Normalbaselinevariability
d) Rhisoimmunisation
e) Normalbaselinerate
14.Inanaerobicmetabolism
a. ThetissuepHrises

357
b. TheFHRpatternisalwaysunchanged
c. 29 timesmoreenergy isproducedduring thedegradationofeachglucose
molecule
d. Lacticacidaccumulates
e. ThetissuepHdoesnotchange
15. Followingdeliveryanumbilicalarterialbloodgasanalysisisreportedas
A V
pH 6.76 6.87
pO2 8.2 15.2
pCO2 50.2 58.4
BE -21.7 -20.1
Thesedataareconsistentwith
a. Respiratoryalkalosis
b. Acuterespiratoryacidosis
c. MixedRespiratory&Metabolicacidosis
d. Metabolicalkalosis
e. ChronicMetabolicacidosis

358
16. The frequency of episodes of fetal breathing movements (chest wall
movements)onultrasoundexaminationisdecreasedinallthefollowingconditions
EXCEPT
a. Labour
b. Normalfetaloxygenation
c. Hypoglycaemia
d. CNSdepressantdrugs
e. Fetalacidosis
17.WhichoneofthefollowingisNOTincludedintheBiophysicalprofile?
a. Fetalbreathingmovements
b. ReactiveCTG
c. FetalRapidEyeMovements
d. Fetalmovements
e. Fetaltone

359
18.Followingdeliveryanumbilicalarterialbloodgasanalysisisreportedas
A V
pH 7.08 7.34
pO2 14.6 20.4
pCO2 76.7 38.6
BE -9.1 -4.8
a. Acuterespiratoryacidosis
b. Acutemetabolicacidosis
c. Chronicrespiratoryacidosis
d. Acutemixedrespiratoryandmetabolicacidosis
e. Chronicmixedrespiratoryandmetabolicacidosis
19.Currentlythemostsensitivereflectionofbirthasphyxiais
a. umbilicalarterypH
b. Apgarscore
c. Neonataladmission
d. FirstneonatalpH

360
e. Fetalheartratepatterninlast60minutesoflabour
20.TheInternationalCerebralPalsyTaskforceconsensusstatementoutlinesessential
criteriathatmustbepresenttoconsiderthatacuteIntrapartumhypoxiawasthecause
ofcerebralpalsy.
Whicharethecorrectstatements?
1. Evidenceofametabolicacidosisinintrapartumfetal,umbilicalarterialcordor
earlyneonatalblood(pH<7.00andbasedeficit>=12mmol/L)
2. Earlyonsetofsevereormoderateneonatalencephalopathyininfantsof>=34
weeksgestation
3. Cerebralpalsyofthespasticquadriplegicordyskinetictype
4. Evidenceofametabolicacidosisinintrapartumfetal,umbilicalarterialcordor
earlyneonatalblood(pH<7.20andbasedeficit>=6mmol/L)
a. 1,2,3
b. 2,3,4
c. 2and4
d. 1and3
e. Alloftheabove

361
21.Regardingumbilicalarterylactate
a. Samplingshouldonlybeperformedoncordfromfulltermfetuses
b. Ismostlymaternalinorigin
c. IscomparabletopHinpredictingtheneonateatrisk
d. Indicateswhichneonatesneedresuscitation
22.Thisdataisconsistentwith
A V
pH 7.08 7.34
pO2 14.6 20.4
pCO2 76.7 38.6
BE -12.1 -11.8
a. AcuteRespiratoryacidosis
b. AcuteMetabolicacidosis
c. Normalacidbasebalance
d. ChronicMetabolicacidosis
e. Mixedrespiratoryandmetabolicacidosis
362
23.Inlabour,thepresenceofafetalheartaccelerationduringavaginalexamination
indicates:
a. Anacidoticfetus
b. Labourisprogressingnormally
c. Acaesareansectionshouldbeperformed
d. Normalfetaloxygenationin99%ofcases
e. Uterinehyper-stimulation

363
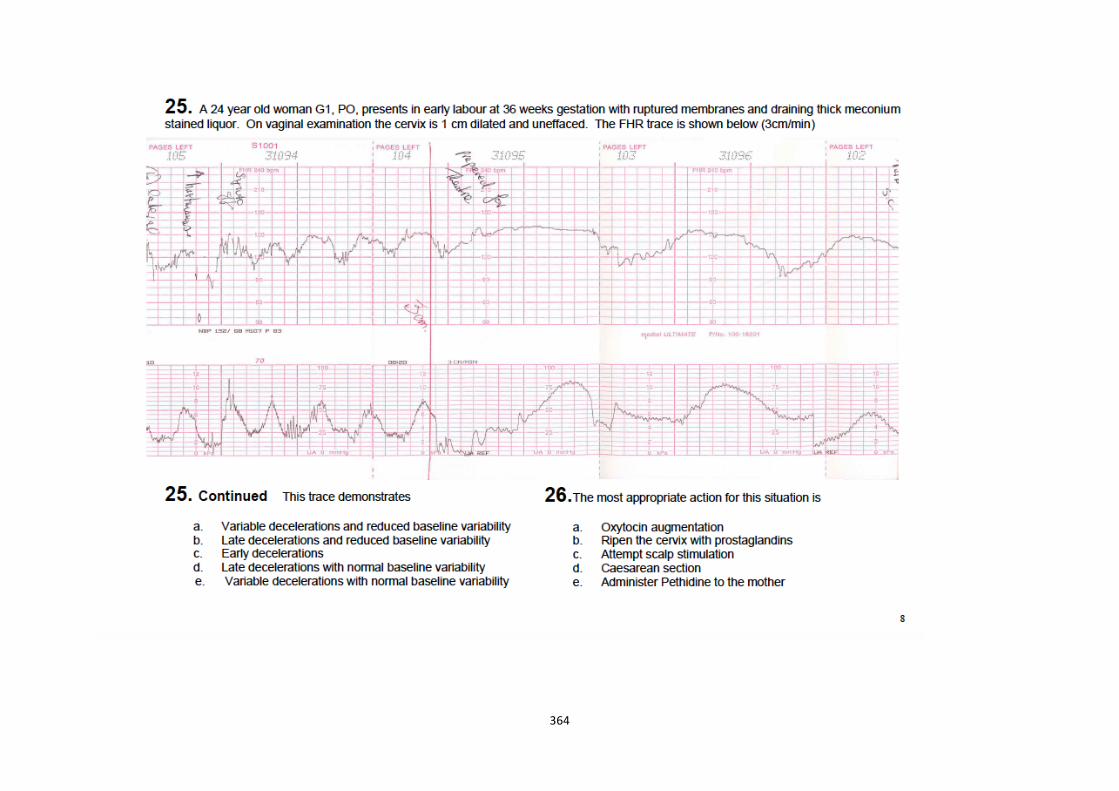
364

365

366

367

368

369

370

371
APPENDIX3.6:POSTTRAININGCTGTESTFORDOCTORS(ANSWERS)
1. D
2. C
3. A
4. D
5. A
6. D
7. E
8. C
9. E
10. E
11. D
12. E
13. C
14. D
15. E
16. B
17. C
18. A
19. A
20. A
21. C

372
22. E
23. D
24. C
25. B
26. D
27. E
28. E
29. C
30. B
31. E
32. C
33. E

373
APPENDIX3.7:PRETRAININGCTGTESTFORMIDWIVES(QUESTIONS)
KalafongHospital
PretrainingCTGtest
Demographics(pleasecircle)
Male/female
Traininglevel:
Student
Midwife
Professionalnurse
Communityservice
Other___________________
PreviousCTGtraining
Noformaltraining
ESMOElecture

374
Other__________________
1. Earlydecelerationsare:
a. Duetoinhibitionofthesympatheticnervoussystem
b. Usuallybelow100beats/min
c. Alwaysphysiological
d. Reproducedbypressureovertheposteriorfontanelle
2. Themostimportantfeatureoflatedecelerationsis:
a. Thefrequencyoftheiroccurrence
b. Thedepthofthedecelerations
c. Durationofthedecelerations
d. Thetimefromonsetofcontractiontoonsetofdeceleration
e. The time from cessation of the contraction to cessation of the
deceleration
3. Theaccelerationswhich frequentlyprecedeand followvariabledecelerations
aresaidtoresultfrom:
a. Adrenalinerelease
b. Atropinerelease
c. Umbilicalarteryocclusion
d. Umbilicalveinocclusion
e. Totalcordocclusion

375
4. Which of the following is NOT important in the interpretation of the
significanceofvariabledecelerations:
a. Baselinevariability
b. Thedepthofthedecelerations
c. Thedurationofthedecelerations
d. Anincreasingbaselinerate
e. The duration from onset of the contractions to onset of the
decelerations
5. Intermittentfetalheartratemonitoringhasthesameoutcomesascontinuous
monitoringif:
a. 1:1dedicatedmidwife
b. Allwomenhaverupturedmembranes(SROM,ARM)
c. Allbabieswithmeconiumhavecontinuousmonitoring
d. All suspected abnormalities on intermittentmonitoring are confirmed
bycontinuousfetalmonitoring
e. Alloftheabove
6. Regardingumbilicalarterylactate
a. Samplingshouldonlybeperformedoncordfromfulltermfetuses
b. Ismostlymaternalinorigin
c. IscomparabletopHinpredictingtheneonateatrisk
d. Indicateswhichneonatesneedresuscitation

376

377

378

379

380
APPENDIX3.8:PRETRAININGCTGTESTFORMIDWIVES(ANSWERS)
1. C
2. A
3. D
4. E
5. E
6. C
7. C
8. E
9. C
10. E

381
APPENDIX3.9:POSTTRAININGCTGTESTFORMIDWIVES
PosttrainingCTGtest
KalafongHospital
1. FetalsleepstatesmaybeassociatedwithanyorallofthefollowingEXCEPT
a. AbsentVariability
b. NormalFHRvariability
c. Absentfetalbreathingmovements
d. Latedecelerations
e. Reducedfetalmovements
2. Whichofthefollowingisnotarecognisedcauseoflatedecelerations
a. Fetalheadcompression
b. Uterinehypertonia
c. Maternalhypotension
d. Uterinerupture
f. Placentalfailure

382
3. Themostimportantfeatureoflatedecelerationsare
a. Thefrequencyoftheiroccurrence
b. Thedepthofthedecelerations
c. Durationofthedecelerations
d. Thetimefromonsetofcontractiontoonsetofdeceleration
f. Thetimefromcessationofthecontractiontocessationofthedeceleration
4. Intermittent fetal heart rate monitoring has the same outcomes as continuous
monitoringif
a. 1:1dedicatedmidwife
b. Allwomenhaverupturedmembranes(SROM,ARM)
c. Allbabieswithmeconiumhavecontinuesmonitoring
d. All suspected abnormalities on intermittent monitoring are confirmed by
continuousfetalmonitoring.
e. Alloftheabove
5.Currentlythemostsensitivereflectionofbirthasphyxiais
a. umbilicalarterypH
b. Apgarscore
c. Neonataladmission

383
d. FirstneonatalpH
e. Fetalheartratepatterninlast60minutesoflabour
6.Regardingumbilicalarterylactate
a. Samplingshouldonlybeperformedoncordfromfulltermfetuses
b. Ismostlymaternalinorigin
c. IscomparabletopHinpredictingtheneonateatrisk
d. Indicateswhichneonatesneedresuscitation
7. In labour, thepresenceofa fetalheartaccelerationduringavaginalexamination
indicates:
a. Anacidoticfetus
b. Labourisprogressingnormally
c. Acaesareansectionshouldbeperformed
d. Normalfetaloxygenationin99%ofcases
e. Uterinehyper-stimulation

384

385

386

387
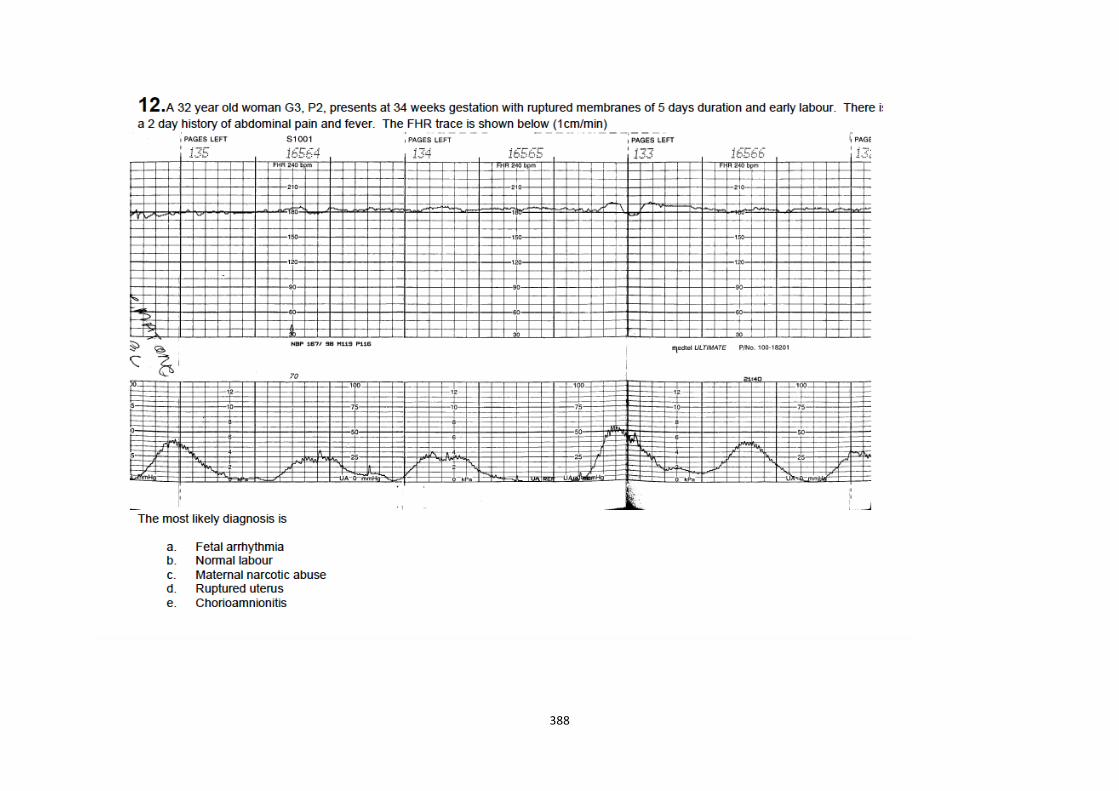
388

389

390

391
APPENDIX3.10:POSTTRAININGCTGTESTFORMIDWIVES(ANSWERS)
1. D
2. A
3. A
4. E
5. A
6. C
7. D
8. C
9. B
10. E
11. E
12. E
13. C
14. E

392
APPENDICESFORCHAPTER5

393
APPENDIX5.1:SEARCHSTRATEGY
PUBMED 1 ("umbilical arteries"{MeSH Terms} OR “umbilical artery” OR “umbilical
arteries” OR "umbilical cord"{MeSH Terms} OR "umbilical cord blood" OR“umbilicalcordartery”OR“cordblood”)NOT(“animals”{MESHTerms}NOT“humans”{MESHTerms})
36795
2 ("lactic acid"{MeSHTerms}OR "lactic acid"OR "lactates"{MeSHTerms}ORlactateOR lactates OR "acidosis, lactic"{MESH Terms} OR “lactic acidosis”)NOT(“animals”{MESHTerms}NOT“humans”{MESHTerms})
70437
3 ("neonataloutcome"OR"neonataloutcomes"OR(("infant,newborn"{MESHTerms} OR neonat*) AND "risk factors"{MESH Terms}) OR “FetalHypoxia”{MESHTerms}OR“fetalhypoxia”OR“foetalhypoxia”OR“AsphyxiaNeonatorum”{MESH Terms} OR “birth asphyxia” OR "fetal asphyxia" OR"foetalasphyxia"OR“intrapartumhypoxia”OR"intrapartumfetalasphyxia"OR “intrapartum stillbirths” OR “intrapartum-linked neonatal deaths” OR"Perinatal Mortality"{MeSH Terms} OR “perinatal mortality” OR “perinatalmorbidity”OR“Neonatalnearmiss”OR“InfantMortality”{MESHTerms}OR“Neonatalmortality”OR"APGARscore"{MeSHTerms}OR“APGARscore”OR"fetal distress"{MeSH Terms} OR “fetal distress” OR “foetal distress” OR"Infant,newborn,diseases/mortality"{MeshTerms}OR"RespiratoryDistressSyndrome, Newborn"{MeSH Terms}) NOT (“animals”{MESH Terms} NOT“humans”{MESHTerms})
81649
4 1OR2OR3 1847545 1AND3 33576 2AND3 4947 1AND2 4098 1OR6 48039 EMBASE 1 Umbilicalartery,umbilicalcordblood,lacticacid,lacticacidosis 12 Lacticacidandfetusoutcome 153 Lacticacid,perinatalasphyxia,fetushypoxia 64 Lacticacid,perinatalasphyxia 875 Lacticacid,fetushypoxia 916 Umbilicalartery,umbilicalcordblood,lacticacid 247 Umbilicalcordbloodandfetusoutcome 1618 Umbilicalarteryandfetusoutcome 2609 1OR2OR3OR4OR5OR6OR7OR8 651 COCHRANE 1 Lactate 53262 Neonat* 88663 Umbilical 90614 2OR3 99765 1AND4 1872 CLINICALTRIALS.GOV 1 "umbilical arteries” OR “umbilical artery” OR “umbilical arteries” OR
"umbilical cord" OR "umbilical cord blood" OR “umbilical cord artery” OR“cordblood”OR“lactate”
1247

394
APPENDIX5.2:DATAFROMEACHINCLUDEDSTUDY,INCLUDINGTHETHRESHOLDSFOREACH
OUTCOME

395
Abessolo Chou Gjerris Labrecque Linet Martin Racinet Westgren White Wiberg Tuuli
Lactate foracidosispH
Sample size52tp9fp4tn 37 fn 2lactate>4.9pH<7.2
Samplesize200tp8 fp 15 tn169 fn 8lactate >6pH>7.15
Lactate foracidosisusingBE
Sample size52tp5fp0fn3tn44
Samplesize 44 tp4 fp 2 tn35 fn 4lactate >6,BE>-8
Lactate forHIE (studydefinedreference)
Sample size58. tp 15, fp10,tn33,fn0.high lactatedefined as4500-5100 - 2SDabove this.sens100,spec77
See studyfordef. forlactate>3.21 tp 1fp 404 tn3635 fn 5sample4045
Lactate>5.68samplesize21182tp 30 fp2497 tn18644fn12
Lactate>10tp3fp 314tn12609fn3
Lactate forpoorAPGAR
<7 at5/60 tp24 fp304 tn13293

396
fn95
Lactate forany poorneonataloutcome(studieddefinedreference)
Compositeneonataloutcome tp45 fp 4258tn 3598 fn9 forlactate>3.90
CorrelationRandR2forlactate andpH
Samplesize2554,r=-0.73;p<0.001
Sample size52 r=-0.678;p<0.001;r2=0.52
Samplesize 200r=-0.693;p<0.001;r2=0.48
Samplesize 410r=0.538p<0.001
Samplesize 867r=-0.75,sig
Samplesize 4045r2=0.20;p<0.001
CorrelationRandR2forlactate andAPGAR at5/60
Samplesize81.r=-.258;p=0.0010
Samplesize 200r2=0.1
CorrelationRandR2forlactate andSBE
Samplesize2554,r=-0.76;p<0.001
Sample size52 r=-0.719;p<0.001;r2=0.46
Samplesize 44 atrisk r=-0.837;p<0.0001
Samplesize 410r=-0.586p<0.001
Samplesize 867r=-0.79,sig
Samplesize 4045r2=0.29;r=-0.53p=0.001
CorrelationRandR2for
Samplesize

397
lactate andABE
2554,r=-0.83;p<0.001

398
APPENDIX5.3CHARACTERISTICSOFINCLUDEDSTUDIES(N=12)
Studycharacteristics
Countryandsetting
Patientsampling &#ofpatients
Patientcharacteristics Indextests Target condition andreferencesstandards
Flowandtiming
Abessolo2009
Gabon.Tertiaryhospital
Consecutive.81
Low risk, non-anomalouslivebirths
Umbilical venouslactate
Neonatal Apgar at 5minutes. Umbilicalvenous superoxidasedismutase andglutamateperoxidase
Consecutivedeliveries,samplestaken immediatelypost-delivery fromclamped cord. Alltestsperformedatthe same time.Allsamples takenfrom umbilicalvein.
Chou1998
Taiwan.Tertiaryhospital.
Consecutive.128
Consecutive patientsincluded, but classified byrisk. Low risk: no maternalmedical or obstetricproblems with a non-anomalousneonate,withnoevidence of prenatal orperinatal insult, at an
Umbilical arteriallactate, pyruvate,andlactate/pyruvate(LP)ratio
Neonatalencephalopathy(classified according toSarnat and Sarnat(1))UmbilicalarterialpH
Consecutivepatients with anarterial blood gas,samples takenfrom a clampedcord, using aheparinisedsyringe stored on

399
appropriate weight forgestation. High risk:maternal complication (atleast one of placentapraevia,placentalabruption,breech, APH, pre-eclampsia/eclampsia, IUGR,diabetes, cephalopelvicdisproportion, or ROM > 48hours)with a neonatalwithat least one of history ofabnormal fetal heart rate,meconiumaspiration,orlowApgar.
ice. Arterial bloodgasdonewithin5-10 minutes ordelivery, serumstored -20 andlactate andpyruvate donewithin 6-12 hoursofdelivery
Gjerris2008
Denmark.Universityhospital
Consecutive.2554
Allwomenregardlessofriskwithasingletonpregnancy
Umbilical arteriallactate
Umbilical arterial pH,ABE,SBE
Consecutivepatients had asampletakenafterdelivery from adouble clampedsegment ofarterialcord,usingheparinisedsyringes. Samplesweremeasuredonaverage6minutesafterobtaining.
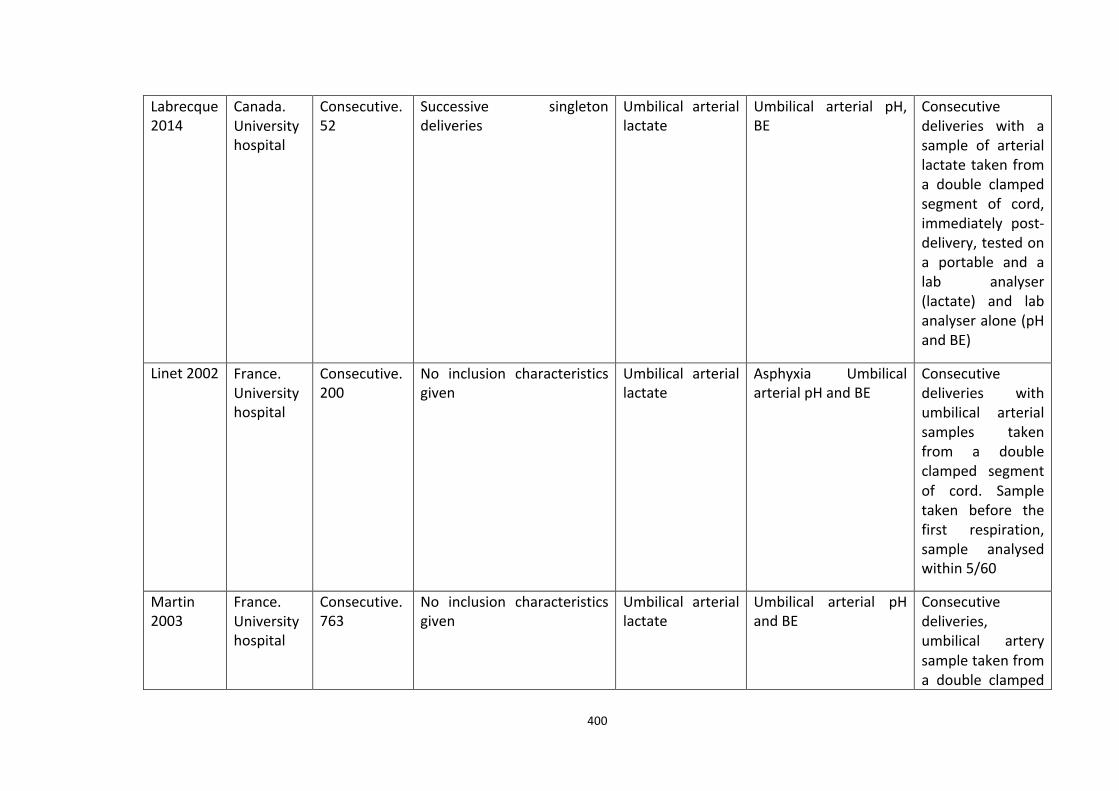
400
Labrecque2014
Canada.Universityhospital
Consecutive.52
Successive singletondeliveries
Umbilical arteriallactate
Umbilical arterial pH,BE
Consecutivedeliveries with asample of arteriallactatetakenfroma double clampedsegment of cord,immediately post-delivery,testedona portable and alab analyser(lactate) and labanalyseralone(pHandBE)
Linet2002 France.Universityhospital
Consecutive.200
No inclusion characteristicsgiven
Umbilical arteriallactate
Asphyxia UmbilicalarterialpHandBE
Consecutivedeliveries withumbilical arterialsamples takenfrom a doubleclamped segmentof cord. Sampletaken before thefirst respiration,sample analysedwithin5/60
Martin2003
France.Universityhospital
Consecutive.763
No inclusion characteristicsgiven
Umbilical arteriallactate
Umbilical arterial pHandBE
Consecutivedeliveries,umbilical arterysampletakenfroma double clamped

401
segment of cordbeforethefirstcry
Racinet2013
France.Privateclinic
Consecutive.867
Low risk deliveries, >34weeksgestation
Umbilical arteriallactate
Umbilical arterial pH,BE,CO2
Consecutivedeliveries, withsampletakenfromclamped segmentof umbilical arteryafterdelivery
Tuuli2014 USA.Universityhospital
Consecutive.4910
Women who laboured atdelivery with a term, non-anomaloussingletonfetus
Umbilical arteriallactate
Composite neonataloutcome: Neonataldeath, intubation,mechanical ventilation,MAS, HIE, need forhypothermictreatmentUmbilicalarterialpH
Consecutivedeliveries, with asample collectedimmediately afterdelivery, beforeknowledge ofneonataloutcome. Sampleanalysed in thelaboratory
Watt
2002
Singapore.Tertiaryhospital
Unclear.130
Deliveriesattermgestation Umbilical arterialand venouslactate
Fetal distress on CTGUmbilical arterial andvenouspHandBE
Samples collectedpost-delivery inheparinisedsyringes,measured withinonehour

402
Westgren1995
Sweden.Universityhospitals
Consecutive.4045
Alldeliverieseligible Umbilical arteriallactate
NICU admission, MAS,IRDS, assistedventilation,neurologicalabnormality, neonataldeaths UmbilicalarterialpH,pCO2,pO2,HCO3,BE
Consecutive,samples takenimmediately afterdelivery from adouble clampedsegment of cord,all analysisperformed within5minutes
White2012
Australia.Tertiaryhospital
Consecutive.21182
All modes of delivery, allmaternal ages, andconditions,withdeliveryofafetus(s)>36weeksgestation
Umbilical arterialand venouslactate
Hypoxic ischemicencephalopathy(classified according toSarnat andSarnat(56))Umbilicalarterial and venous pHandBE
Consecutivedeliveries, with asampletakenfroma double clampedsegment of cord,straight afterbirth, using aheparinisedsyringe, stored onice
Wiberg2010
Sweden.Universityhospitals
Consecutive.13753
All planned vaginaldeliveries, with accuratedatingof gestationage, andasingletonfetus
Umbilical arterialand venouslactate
5/60 Apgar <7 or <4;HIEstage2-3Umbilicalarterial and venous pHandBE
Consecutivedeliveries, with asample from adouble clampedsegments of cord,taken immediatelyafter delivery andbefore newbornsfirstbreath

403
APPENDICESFORCHAPTER10

404
APPENDIX10.1QUESTIONNAIRE:ATTITUDESANDBARRIERSTOWARDSIMPLEMENTATIONOF
UNIVERSALCORDLACTATESAMPLING
Thisquestionnaireisanonymousandallyourresponseswillbetreatedconfidentially.
For thedemographic questionplease circle the corresponding answerwhilst for the
remainderofquestionsplease tick theanswer thatbestagreeswithyouropinionor
situation.
Demographics(pleasecircle)
1. Currentpositioninwhichyouprovidematernitycare:
Midwife Doctor
Nurse
2. Age
20to29years 30to39years
40to49years ≥50years

405
3. Gender
Male Female
4. Lengthoftimepracticinginmaternitycare:
<1year 1-5years
6-10years >10years
PreviousexperienceofCTGuse(pleasecircle)
1. WhatisyourpreviousCTGtrainingexperience:
None
Atworkonly
Aspartofmedicalormidwiferydegree
Specifictrainingcourse

406
2. Ticktheresponsewhichbestagreeswithyouropinion
Strongly
Agree
Agree
Neu
tral
Disagree
Strongly
Disagree
I feel confident to identify the
normalfeaturesofaCTG
I feel confident to identify the
abnormalfeaturesofaCTG
PreviousExperienceofCaseReflection:
1.Ticktheresponsewhichbestagreeswithyouropinion
Strongly
Agree
Agree
Neu
tral
Disagree
Strongly
Disagree
I regularly attend monthly
perinatalmortalitymeetings
Perinatal mortality meetings are
effective in reducing adverse
neonataloutcomes
In attending perinatal mortality
meetings,Ihavelearntnewthings
In attending perinatal mortality
meetings I have changed my

407
practice
I feel thatmore couldbedone to
reducebadoutcomesduetobirth
asphyxia
PreviousExperienceofUmbilicalCordBloodGas/LactateAnalysis
1. Have you previously had experience in undertaking umbilical cord lactate
analysis?
Yes No
2. Ifyouhavehadpreviousexperienceinutilisingumbilicalcordlactateanalysisin
whichmannerwasitutilised:
Universal(e.g.alldeliverieshaveumbilicalcordbloodsamplesanalysed)
Selective(e.g.cordbloodsamplesareonlyanalysedonsomedeliveries)
Notapplicable
3. Ticktheresponsewhichbestagreeswithyouropinion
StronglyAgree
Agree
Neu
tral
Disagree
StronglyDisa
gree
I feel confident to take blood from the

408
umbilicalarteryofaplacenta
I feel confident to interpret the results of a
cordlactateresult
SpecificBenefitsofUmbilicalCordBloodGas/LactateAnalysis
Ticktheresponsethatbestagreeswithyouropinion
Anumberofpotentialbenefitsofumbilical
cordbloodgas/lactateanalysishavebeen
suggested:
StronglyAgree
Agree
Neu
tral
Disagree
StronglyDisa
gree
Objective measurement of status at birth
assistsinneonatalcare
An objective record of status at birth is
protective for staff in the event of medico-
legalissues
Umbilicalcordbloodgasorlactateanalysisis
cost-effective
Improved opportunities for audit and
teachingofmaternitycarepractice
BarrierstoImplementationofUniversalUmbilicalCordBloodGas/LactateAnalysis
Ticktheresponsethatbestagreeswithyouropinion

409
Anumberofpotentialimpediments
totheintroductionofuniversal
umbilicalcordbloodgas/lactate
analysishavebeensuggested: StronglyAgree
Agree
Neu
tral
Disagree
StronglyDisa
gree
Expense
Insufficienttimefollowingdelivery
Increased workload on
midwifery/medicalstaffmembers
Lackofnecessaryequipment
Lackofnecessaryexpertise
Encroachmentof technology into the
birth process (or ‘medicalisation’ of
birth)
Decreasedpatientcontacttime
FurtherComments
Doyouhaveanyfurthercommentsonumbilicalcordbloodgas/lactateanalysis?

410
APPENDIX10.2PATIENT/PARTICIPANT’SINFORMATIONLEAFLET&INFORMEDCONSENTFORM
PATIENT/PARTICIPANT’SINFORMATIONLEAFLET&INFORMED
CONSENTFORMFORCLINICALTRIAL/INTERVENTIONRESEARCH
TRIALTITLE:Feasibilityofumbilicallactatetestingasaclinicaltoolinalowandmiddle-
incomesetting
INTRODUCTION
Youareinvitedtovolunteerforaresearchstudy.Thisinformationleafletistohelpyou
todecide ifyouwould liketoparticipate.Beforeyouagreetotakepart inthisstudy
youshouldfullyunderstandwhatisinvolved.Ifyouhaveanyquestions,whicharenot
fullyexplained in this leaflet,donothesitate toask the investigator.Youshouldnot
agreetotakepartunlessyouarecompletelyhappyaboutalltheproceduresinvolved
WHATISTHEPURPOSEOFTHISSTUDY?
This studyaims to teachmidwiferyandmedical staffhow tomeasure the levelof a
substancecalled lactate in thebaby’sumbilicalcord,which isusedtodeterminethe
healthandwellbeingofnewbornbabies.
EXPLANATIONOFPROCEDURESTOBEFOLLOWED

411
The labouranddeliverywillproceedas itnormallywould.Afteryourbabyhasbeen
delivered theumbilical cord is clampedandcutand thebabywillbemanaged,as it
normallywouldbe.Theplacentawillthenbedelivered,as itnormallywouldbe.The
doctorwillthentakeasmallsamplefromaclampedsectionoftheumbilicalcordafter
itisdelivered.
HASTHESTUDYRECEIVEDETHICALAPPROVAL?
This clinical trial Protocolwas submitted to the Faculty of Health Sciences Research
Ethics Committee, University of Pretoria and written approval has been granted by
thatcommittee.ThestudyhasbeenstructuredinaccordancewiththeDeclarationof
Helsinki (lastupdate:October2008),whichdealswith the recommendationsguiding
doctors in biomedical research involving human/subjects. A copy of the Declaration
maybeobtainedfromtheinvestigatorshouldyouwishtoreviewit.
WHATAREYOURRIGHTSASAPARTICIPANTINTHISSTUDY?
Yourparticipation in this trial is entirely voluntary and you can refuse toparticipate
without stating any reason. Your withdrawal will not affect your access to other
medicalcare.
ISALTERNATIVETREATMENTAVAILABLE?
As this isnota study lookingat treatment,yourcarewillbeasnormalwhetheryou
choosetoparticipateornot.

412
MAY ANY OF THESE TRIAL PROCEDURES RESULT IN DISCOMFORT OR
INCONVENIENCE?
Theumbilicalcordwillhavealreadybeenremovedfromthebaby(asnormal)before
thesampleistakenandsonodiscomfortwillbefeltbyeitheryouoryourbaby.
WHATARETHERISKSINVOLVEDINTHISSTUDY?
Therearenomedicalriskstoyouoryourbaby.
ARETHEREANYWARNINGSORRESTRICTIONSCONCERNINGMYPARTICIPATIONIN
THISSTUDY?
No
INSURANCEANDFINANCIALARRANGEMENTS
N/A
SOURCEOFADDITIONALINFORMATION
Ifyouhaveanyquestionsregardingthetrial,youmaycontactDrKateGrobickiatany
time.Thetelephonenumberis0818062213
CONFIDENTIALITY
Allinformationobtainedduringthecourseofthisstudyisstrictlyconfidential.Asthe
sample of the umbilical cord will be used for training purposes only, no personal
informationwill begathered fromyouother than thatof your signedconsent form.
Theseformswillbeusedfornootherpurposesotherthanforconsent.Theumbilical

413
cordwillbedisposedwiththerestofyourplacenta immediatelyafterthetraining is
completed.
INFORMEDCONSENT
IherebyconfirmthatIhavebeeninformedbytheinvestigator,DrKateGrobickiabout
the nature, conduct, benefits and risks of the study “Feasibility of umbilical lactate
testingasaclinicaltoolinalowandmiddleincomesetting”.Ihavealsoreceived,read
and understood the above written information (Patient Information Leaflet and
InformedConsent)regardingthestudy.
Imay,atanystage,withoutprejudice,withdrawmyconsentandparticipation inthe
study. I have had sufficient opportunity to ask questions and (ofmy own free will)
declaremyselfpreparedtoparticipateinthestudy.
Patient'sname(Pleaseprint)
Patient'ssignature Date
I, Dr …………………………………. herewith confirm that the above patient has been
informedfullyaboutthenature,conductandrisksoftheabovestudy.

414
Investigator'sname(Pleaseprint)
Investigator'ssignature Date
Witness'sname*
Witness'ssignature Date
*Consentprocedureshouldbewitnessedwheneverpossible.
VERBAL PATIENT INFORMED CONSENT (applicable when patients cannot read or
write)
I,theundersigned,Dr……………………………………………,havereadandhaveexplainedfully
tothepatient,named……………………………………………………………..and/orherrelative,the
patientinformationleaflet,whichhasindicatedthenatureandpurposeofthestudyin
which I have asked the patient to participate. The patient indicated that she
understands that she will be free to withdraw from the study at any time for any
reason.

415
Iherebycertifythatthepatienthasagreedtoparticipateinthisstudy.
Patient'sName(Pleaseprint)
Investigator'sName(Pleaseprint)
Investigator'sSignature Date
Witness'sName(Pleaseprint)
Witness'sSignature Date

416
Related Documents











