The Internist’s Approach to the The Internist’s Approach to the Non Healing Wound Non Healing Wound Non Healing Wound Non Healing Wound Narayan Kulkarni, DO Narayan Kulkarni, DO Medical Director Medical Director FMH Center for Advanced Wound Care FMH Center for Advanced Wound Care and Hyperbaric Medicine and Hyperbaric Medicine Frederick Memorial Health System Frederick Memorial Health System Frederick MD Frederick MD Frederick, MD Frederick, MD

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The Internist’s Approach to theThe Internist’s Approach to theNon Healing WoundNon Healing WoundNon Healing WoundNon Healing Wound
Narayan Kulkarni, DONarayan Kulkarni, DOMedical DirectorMedical Director
FMH Center for Advanced Wound Care FMH Center for Advanced Wound Care and Hyperbaric Medicineand Hyperbaric Medicine
Frederick Memorial Health SystemFrederick Memorial Health SystemFrederick MDFrederick MDFrederick, MDFrederick, MD

Conflict of Interest Disclos reConflict of Interest Disclos reConflict of Interest DisclosureConflict of Interest Disclosure
The presenter does not have any The presenter does not have any relationship, financial or otherwise, with relationship, financial or otherwise, with ppany commercial interests.any commercial interests.

ObjectivesObjectivesObjectivesObjectives
Learn how to do to a basic wound assessment Learn how to do to a basic wound assessment Learn to recognize the presentations of the most
common types of woundscommon types of wounds Identify common barriers to wound healing Be aware of different types of therapies used in
wound healing Dressings, hyperbaric oxygen, debridement, negative
pressure therapy, skin substitutes
Chronic WoundsChronic WoundsChronic WoundsChronic Wounds
Affect 5.7 million patients annuallyAffect 5.7 million patients annuallyp yp y Account for $20Account for $20--25 billion in healthcare costs annually25 billion in healthcare costs annually Patients often have other significant comorbiditiesPatients often have other significant comorbidities Quality of life issuesQuality of life issues
AppearanceAppearance OdorOdorOdorOdor Social stigmaSocial stigma Financial costsFinancial costs Em ti l d ph i l tr /p iEm ti l d ph i l tr /p i Emotional and physical stress/painEmotional and physical stress/pain Disability for patient and lost productivity for patients and Disability for patient and lost productivity for patients and
caregiverscaregivers

The Wound Care/Hyperbaric The Wound Care/Hyperbaric Medicine subspecialtyMedicine subspecialty
Wound Healing and Hyperbaric Medicine has evolved Wound Healing and Hyperbaric Medicine has evolved g ypg ypinto a subspecialtyinto a subspecialty
“Wet to Dry” dressings are practically a thing of the “Wet to Dry” dressings are practically a thing of the pastpast
New modalities have transformed the careNew modalities have transformed the careH b iH b i Hyperbaric oxygenHyperbaric oxygen
Skin substitutesSkin substitutes Negative Pressure therapyNegative Pressure therapyg pyg py Enzymatic debridementEnzymatic debridement Effective dressings tailored to address needs of the woundEffective dressings tailored to address needs of the wound
Wound Care/Hyperbaric MedicineWound Care/Hyperbaric MedicineWound Care/Hyperbaric MedicineWound Care/Hyperbaric Medicine
900 HBO facilities nationwide and ?? Wound900 HBO facilities nationwide and ?? Wound900 HBO facilities nationwide and ?? Wound 900 HBO facilities nationwide and ?? Wound clinicsclinics
Multidisciplinary team of physicians andMultidisciplinary team of physicians andMultidisciplinary team of physicians and Multidisciplinary team of physicians and cliniciansclinicians
“CWS” certification“CWS” certificationCWS certificationCWS certification Streamlined patient flow to promoteStreamlined patient flow to promote
EvaluationEvaluation EvaluationEvaluation TreatmentTreatment “One stop shop”“One stop shop”One stop shopOne stop shop

Wound HealingWound Healing

A Quick Review of Wound HealingA Quick Review of Wound Healing
Inflammatory Phase• 0 to 3 days
h i ( C lik h hil i b i d d i )•Phagocystosis (WBC like macrophages, neutrophils ingest bacteria, dead tissue)•Vasodilation (WBC release inflammatory markers to cause swelling, redness)
Proliferative Phase•3 to 21 days•Fibroblasts produce collagen new blood vessel growth rich vascular network in collagenFibroblasts produce collagen, new blood vessel growth, rich vascular network in collagen matrix•Contraction and epithelialization, wound edges move toward the center to close the wound
Maturation/Remodeling•Scar develops tensile strength•Scar develops tensile strength•80% strong as original skin
Compromised Wound HealingCompromised Wound Healing
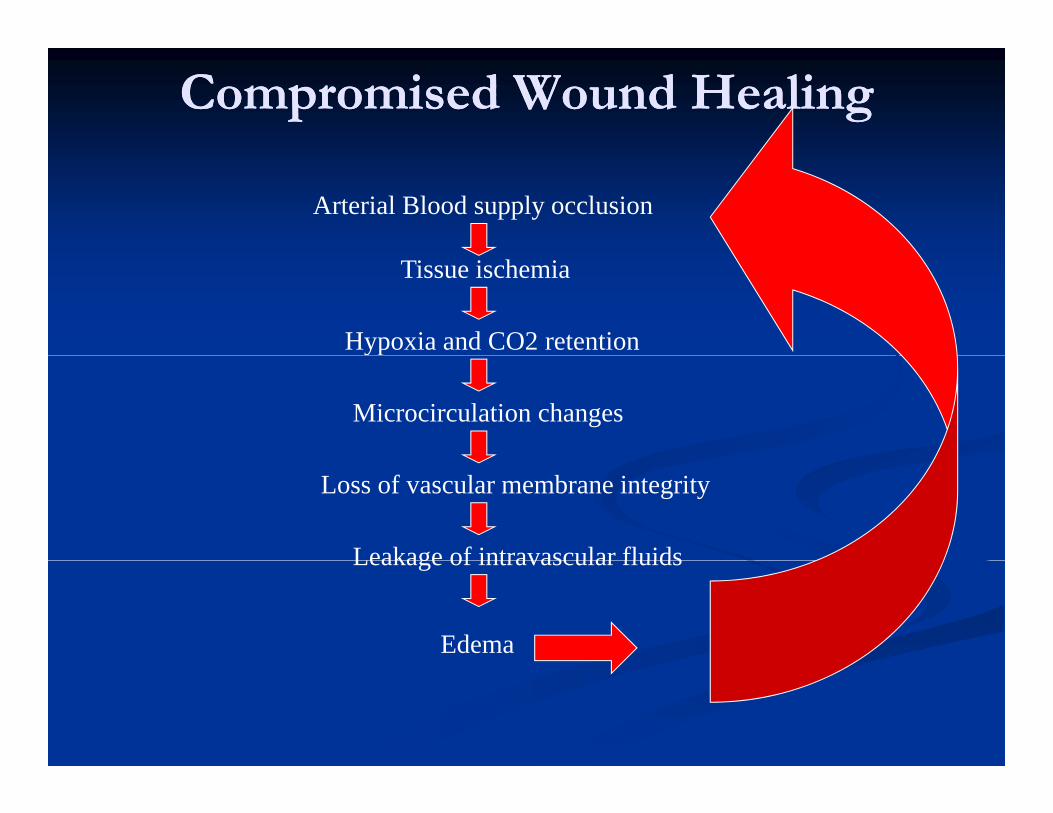
Arterial Blood supply occlusion
Tissue ischemia
Hypoxia and CO2 retention
Microcirculation changes
Loss of vascular membrane integrity
Leakage of intravascular fluidsLeakage of intravascular fluids
Edema

Assessment of Chronic WoundsAssessment of Chronic Wounds

Types of Chronic WoundsTypes of Chronic WoundsTypes of Chronic WoundsTypes of Chronic Wounds
Vascular ulcersVascular ulcers AtypicalAtypical ArterialArterial VenousVenous
ypyp Bullous pemphigoidBullous pemphigoid VasculitidesVasculitides
LymphedemaLymphedema Neuropathic/diabetic Neuropathic/diabetic
VasculopathyVasculopathy MalignancyMalignancy
foot ulcersfoot ulcers Pressure or decubitusPressure or decubitus
“Internal” wounds“Internal” wounds Radiation injuryRadiation injury
TraumaticTraumatic SurgicalSurgical
j yj y

How do you Assess a Wound?How do you Assess a Wound?
AppearanceAppearance DrainageDrainage
How do you Assess a Wound?How do you Assess a Wound?
AppearanceAppearance Irregular or uniform?Irregular or uniform? Draining heavily or dry?Draining heavily or dry?
gg Degree, color, consistencyDegree, color, consistency
“Bioburden” and “Bioburden” and Eschar Eschar Granulation tissueGranulation tissue
SiSi
necrotic tissuenecrotic tissue PainPain
T hT h SizeSize Area, Depth, UnderminingArea, Depth, Undermining Sinus tracts, fistulaeSinus tracts, fistulae
Temperature, erythemaTemperature, erythema Surrounding skinSurrounding skin
Maceration eczemato sMaceration eczemato sSinus tracts, fistulaeSinus tracts, fistulae LocationLocation
Leg, ankle, toes, trunkLeg, ankle, toes, trunk
Maceration, eczematous, Maceration, eczematous, indurationinduration
Barriers to Wound HealingBarriers to Wound HealingBarriers to Wound HealingBarriers to Wound Healing
Vascular dysfunction (arterial or venous)Vascular dysfunction (arterial or venous)Vascular dysfunction (arterial or venous)Vascular dysfunction (arterial or venous) Bioburden and infectionBioburden and infection Scarring and fibrosisScarring and fibrosis Scarring and fibrosisScarring and fibrosis EdemaEdema PressurePressure PressurePressure Necrotic tissueNecrotic tissue H t f t rH t f t r Host factorsHost factors
Nutrition, comorbidities, social history Nutrition, comorbidities, social history Medications: steroids antirheumatic agents chemotherapyMedications: steroids antirheumatic agents chemotherapy Medications: steroids, antirheumatic agents, chemotherapyMedications: steroids, antirheumatic agents, chemotherapy

How are those barriers treated?How are those barriers treated?How are those barriers treated?How are those barriers treated?
Vascular correction Vascular correction –– angioplasty or venous interventionangioplasty or venous intervention Bioburden and infection Bioburden and infection –– routine debridement, antibiotics, routine debridement, antibiotics,
drainage controldrainage control Scarring and fibrosis Scarring and fibrosis –– medications, surgery, negative pressure medications, surgery, negative pressure gg , g y, g p, g y, g p
therapytherapy Edema Edema –– compression therapycompression therapy Pressure Pressure -- offloadingoffloadingess eess e o oad go oad g Necrotic tissue Necrotic tissue –– routine debridement, bedside or ORroutine debridement, bedside or OR Host factorsHost factors
NutritionNutrition dietary evaluation lean body mass monitoringdietary evaluation lean body mass monitoring Nutrition Nutrition –– dietary evaluation, lean body mass monitoringdietary evaluation, lean body mass monitoring Comorbidities Comorbidities –– control control Social history Social history –– smoking cessation, assistance at homesmoking cessation, assistance at home MedicationsMedications –– drug holidays if possibledrug holidays if possibleMedications Medications drug holidays if possibledrug holidays if possible

Vascular UlcersVascular Ulcers

Venous UlcersVenous UlcersVenous UlcersVenous Ulcers EtiologyEtiology
Typically from long standing venous hypertensionTypically from long standing venous hypertension Typically from long standing venous hypertensionTypically from long standing venous hypertension Distension damages vein walls leading to exudation of fluidDistension damages vein walls leading to exudation of fluid Valvular incompetenceValvular incompetence Chronic inflammation and ischemia from high interstitial fluidChronic inflammation and ischemia from high interstitial fluid Chronic inflammation and ischemia from high interstitial fluid Chronic inflammation and ischemia from high interstitial fluid
pressurepressure LocationLocation
“Gaiter” (medial aspect of leg from calf to below ankle)“Gaiter” (medial aspect of leg from calf to below ankle) Gaiter (medial aspect of leg from calf to below ankle) Gaiter (medial aspect of leg from calf to below ankle) distribution of both legsdistribution of both legs
Ulcer AppearanceUlcer Appearance Shallow with irregular bordersShallow with irregular borders Shallow with irregular bordersShallow with irregular borders Increased drainageIncreased drainage Fibrotic scar tissueFibrotic scar tissue BioburdenBioburden BioburdenBioburden
Venous UlcersVenous Ulcers
Skin examSkin exam
Venous UlcersVenous Ulcers
EdematousEdematous Stasis changes, pitting, lipodermatosclerosis, atrophie blancheStasis changes, pitting, lipodermatosclerosis, atrophie blanche Hemosiderin stainingHemosiderin staininggg Palpable pulsesPalpable pulses
SymptomsSymptoms Painful, especially when debridedPainful, especially when debrideda , espec a y w e deb deda , espec a y w e deb ded Recurrent cellulitisRecurrent cellulitis
Medical HistoryMedical History Family History of “vein problems” personal history of DVTs/phlebitisFamily History of “vein problems” personal history of DVTs/phlebitis Family History of vein problems , personal history of DVTs/phlebitisFamily History of vein problems , personal history of DVTs/phlebitis “Standing” Occupations“Standing” Occupations Multigravid femalesMultigravid females

Venous UlcersVenous UlcersVenous UlcersVenous Ulcers
DiagnosisDiagnosisgg PresentationPresentation Confirm by Venous Studies, test for insufficiency/refluxConfirm by Venous Studies, test for insufficiency/reflux
TreatmentTreatment TreatmentTreatment Venous intervention (eg. closure)Venous intervention (eg. closure) Compression therapyCompression therapy
Multilayer bandaging systemsMultilayer bandaging systems Local wound care: debridement, dressing selectionLocal wound care: debridement, dressing selection Pain controlPain control Medications, eg. pentoxifyllineMedications, eg. pentoxifylline Negative pressureNegative pressure Skin substitutes and/or graftingSkin substitutes and/or grafting Skin substitutes and/or graftingSkin substitutes and/or grafting

Compression TherapyCompression TherapyCompression TherapyCompression Therapy
• Application of “4 layer” compression wraps
Lymphedema UlcersLymphedema UlcersLymphedema UlcersLymphedema Ulcers EtiologyEtiology
Develop from lymphedema and “phlebolymphedema”Develop from lymphedema and “phlebolymphedema”v p y p d d p b y p dv p y p d d p b y p d Excessive accumulation of interstitial fluid and poor lymph flowExcessive accumulation of interstitial fluid and poor lymph flow Any disruption of lymph channelsAny disruption of lymph channels
Primary (congenital) or Secondary classificationPrimary (congenital) or Secondary classification Secondary lymphedema often from obstructive or inflammatory Secondary lymphedema often from obstructive or inflammatory
processesprocesses Tumor, surgery, infectious, venous insufficiencyTumor, surgery, infectious, venous insufficiency
L iL i LocationLocation Usually in the extremities, can move into trunkUsually in the extremities, can move into trunk
Ulcer AppearanceUlcer Appearance Ulcers are irregular, heavy drainageUlcers are irregular, heavy drainage No specific predeliction to locationNo specific predeliction to location
Lymphedema UlcersLymphedema UlcersLymphedema UlcersLymphedema Ulcers
Skin ExamSkin Exam Stasis changesStasis changes Edematous and fibroticEdematous and fibrotic
P ill i di li i h b b kiP ill i di li i h b b ki Papillamatosis, dimpling causing smooth but bumpy skinPapillamatosis, dimpling causing smooth but bumpy skin “Stemmer’s sign”“Stemmer’s sign”
SymptomsSymptomsy py p May or may not be painfulMay or may not be painful Recurrent cellulitisRecurrent cellulitis
Medical HistoryMedical History Multiple comorbiditiesMultiple comorbidities Morbid obesity is commonMorbid obesity is common Morbid obesity is commonMorbid obesity is common

Lymphedema UlcersLymphedema Ulcers
DiagnosisDiagnosis
Lymphedema UlcersLymphedema Ulcers
gg Clinical Clinical Important to rule out other causes of edema, eg. Important to rule out other causes of edema, eg. p gp g
CHF, RICHF, RI TreatmentTreatment
Compression therapyCompression therapyManual lymphatic decongestive therapyManual lymphatic decongestive therapyLymphedema pumpsLymphedema pumpsAvoid diuretics!Avoid diuretics!

Arterial UlcersArterial UlcersArterial UlcersArterial Ulcers EtiologyEtiology
PressurePressure shoewear bracesshoewear braces Pressure Pressure –– shoewear, bracesshoewear, braces Trauma Trauma Embolus Embolus –– acute eventacute event I h iI h i i PADi PAD Ischemia Ischemia –– progressive PADprogressive PAD InfectionInfection Poor healing due to compromised arterial blood flowPoor healing due to compromised arterial blood flow
L iL i LocationLocation Usually lower extremities, often shin, feet or toesUsually lower extremities, often shin, feet or toes
Ulcer AppearanceUlcer Appearance Punched out, dry appearingPunched out, dry appearing Little drainage unless infectedLittle drainage unless infected Yellow slough or exudate, maybe escharYellow slough or exudate, maybe eschargg Wet or dry gangreneWet or dry gangrene

Arterial UlcersArterial Ulcers
Skin examSkin exam
Arterial UlcersArterial Ulcers
Nonpalpable or diminshed DP and PT pulsesNonpalpable or diminshed DP and PT pulses Cool skin, loss of hair on toesCool skin, loss of hair on toes Periwound skin is “blue”, taut, shiny or show reactive hyperemiaPeriwound skin is “blue”, taut, shiny or show reactive hyperemia, , y yp, , y yp Legs may be skinny, nails dystrophicLegs may be skinny, nails dystrophic “Monophasic” pulse sounds by hand held doppler“Monophasic” pulse sounds by hand held doppler
SymptomsSymptoms SymptomsSymptoms Rest pain or night painRest pain or night pain Claudication, dependency improvesClaudication, dependency improves
M di l HiM di l Hi Medical HistoryMedical History Multiple comorbidities: DM2, CAD, CVAMultiple comorbidities: DM2, CAD, CVA “ABCDEs”:A1C, BP, Cholesterol, Diet/Obesity, Exercise, Smoking“ABCDEs”:A1C, BP, Cholesterol, Diet/Obesity, Exercise, Smoking

Arterial ulcersArterial ulcersArterial ulcersArterial ulcers
DiagnosisDiagnosisgg Arterial evaluationArterial evaluation
ABI studiesABI studies Arterial dopplersArterial dopplers MRAMRA Vascular referralVascular referral Vascular referralVascular referral
TreatmentTreatment Vascular evaluation and intervention imperativeVascular evaluation and intervention imperativepp Conservative approach until interventionConservative approach until intervention After intervention: debridement, moisture balance, skin After intervention: debridement, moisture balance, skin
substitutessubstitutessubstitutessubstitutes
Diabetic Foot UlcersDiabetic Foot Ulcers
Diabetic Foot UlcersDiabetic Foot UlcersDiabetic Foot UlcersDiabetic Foot Ulcers EtiologyEtiology
Diabetic neuropathy and its sequelaeDiabetic neuropathy and its sequelae Diabetic neuropathy and its sequelaeDiabetic neuropathy and its sequelae Arterial and “small vessel” diseaseArterial and “small vessel” disease PressurePressure Deformity/Charcot footDeformity/Charcot foot Deformity/Charcot footDeformity/Charcot foot
LocationLocation By definition, anywhere on dorsal or plantar aspect of footBy definition, anywhere on dorsal or plantar aspect of foot
Ul r App rUl r App r Ulcer AppearanceUlcer Appearance Often full thickness, may probe to bone or tendonOften full thickness, may probe to bone or tendon Sometimes communicate from surface to surfaceSometimes communicate from surface to surface
D i b hD i b h Drainage can be heavyDrainage can be heavy Initial appearance is often necrotic Initial appearance is often necrotic If on plantar aspect, callus is very commonIf on plantar aspect, callus is very common

Diabetic Foot UlcersDiabetic Foot Ulcers
Skin examSkin exam
Diabetic Foot UlcersDiabetic Foot Ulcers
Skin examSkin exam NeuropathyNeuropathy Concurrent arterial disease commonConcurrent arterial disease common
RuborRubor EczematousEczematous
SymptomsSymptoms Neuropathy makes wound insensateNeuropathy makes wound insensate
Medical HistoryMedical History DM2, PAD, HTN, hyperlipidemia are commonDM2, PAD, HTN, hyperlipidemia are common

Diabetic Foot UlcersDiabetic Foot Ulcers
DiagnosisDiagnosis
Diabetic Foot UlcersDiabetic Foot Ulcers
gg Clinical historyClinical history
TreatmentTreatment Arterial assessment (pulses, ABIs with TBIs)Arterial assessment (pulses, ABIs with TBIs) Topical agents (eg. PDGF)Topical agents (eg. PDGF) DM2 controlDM2 control DM2 controlDM2 control OffloadingOffloading Serial debridementsSerial debridements Appropriate dressingsAppropriate dressings Hyperbaric oxygenHyperbaric oxygen

Pressure UlcersPressure Ulcers

Pressure UlcersPressure UlcersPressure UlcersPressure Ulcers EtiologyEtiology
Localized ischemia from prolonged pressure over a bony prominenceLocalized ischemia from prolonged pressure over a bony prominencep g p y pp g p y p Damage at superficial and deeper layers Damage at superficial and deeper layers
LocationLocation Mid body: Sacrum, buttocks, coccyx, ischiumMid body: Sacrum, buttocks, coccyx, ischium Foot: Heel, lateral and medial ankles, toesFoot: Heel, lateral and medial ankles, toes Upper body: Elbows, scapula, shoulderUpper body: Elbows, scapula, shoulder Head: Occiput, earsHead: Occiput, ears
Ulcer AppearanceUlcer Appearance Staged from I to IV according to NPUAPStaged from I to IV according to NPUAP I I –– Intact skin with non blanching rednessIntact skin with non blanching redness
IIII P i l hi k d bli d d b dP i l hi k d bli d d b d II II –– Partial thickness wound or blister, red wound bedPartial thickness wound or blister, red wound bed III III –– Full thickness with slough, no bone/muscle/tendonFull thickness with slough, no bone/muscle/tendon IV IV –– Full thickness with exposed bone, muscle or tendonFull thickness with exposed bone, muscle or tendon UnstageableUnstageable full thickness tissue loss with base covered byfull thickness tissue loss with base covered by Unstageable Unstageable –– full thickness tissue loss with base covered by full thickness tissue loss with base covered by
eschar/slougheschar/slough

Pressure UlcersPressure Ulcers
Skin examSkin exam
Pressure UlcersPressure Ulcers
Poor turgor, inelasticPoor turgor, inelastic May be wet from incontinenceMay be wet from incontinence Localized skin dermatosesLocalized skin dermatoses
SymptomsSymptoms Painless to painfulPainless to painful
Medical HistoryMedical HistoryN l i l i j hN l i l i j h Neurological injury, neuropathyNeurological injury, neuropathy
Cachexia, malnutritionCachexia, malnutrition ImmobilityImmobility ImmobilityImmobility
Pressure UlcersPressure Ulcers
DiagnosisDiagnosis
Pressure UlcersPressure Ulcers
gg Clinical Clinical
TreatmentTreatment Offloading!Offloading! Offloading!Offloading!
Severity of ulcer will dictate offloading surfaceSeverity of ulcer will dictate offloading surface Offloading devices and practices need to be routinely evaluatedOffloading devices and practices need to be routinely evaluated
Minimize moisture, friction, shearing forcesMinimize moisture, friction, shearing forces Nutritional assessment and interventionNutritional assessment and intervention Local wound care including serial debridementsLocal wound care including serial debridementsgg Reconstructive surgery in severe casesReconstructive surgery in severe cases Prevention and Braden Scale Prevention and Braden Scale
R mm nd f mili rizin n lf ith th Br d n l f rR mm nd f mili rizin n lf ith th Br d n l f r Recommend familiarizing oneself with the Braden scale for Recommend familiarizing oneself with the Braden scale for predicting pressure ulcer riskpredicting pressure ulcer risk

Hyperbaric OxygenHyperbaric Oxygen

Hyperbaric OxygenHyperbaric OxygenHyperbaric OxygenHyperbaric Oxygen
Treatment where patient breathes 100% oxygen at pressure greater than Treatment where patient breathes 100% oxygen at pressure greater than h ih iatmosphericatmospheric
Oxygen dissolves into plasma and generates very high oxygen partial Oxygen dissolves into plasma and generates very high oxygen partial pressure gradientspressure gradients Up to 2000 mm Hg orUp to 2000 mm Hg or 20 times20 times PO2 from room airPO2 from room air Up to 2000 mm Hg, or Up to 2000 mm Hg, or 20 times20 times PO2 from room airPO2 from room air
Multiple different mechanisms through which hyperbaric oxygen effectiveMultiple different mechanisms through which hyperbaric oxygen effective Significantly increases activity of fibroblasts and neutrophilsSignificantly increases activity of fibroblasts and neutrophils Drives angiogenesisDrives angiogenesis Drives angiogenesisDrives angiogenesis Reduces local edemaReduces local edema Reduces reperfusion injuryReduces reperfusion injury
Wounds/injury must be ischemic for therapy to be effectiveWounds/injury must be ischemic for therapy to be effective Wounds/injury must be ischemic for therapy to be effectiveWounds/injury must be ischemic for therapy to be effective Arterial disease, edematous conditions, infectious, radiation injuryArterial disease, edematous conditions, infectious, radiation injury
Be aware of unusual symptoms with radiation historyBe aware of unusual symptoms with radiation history Pelvic pain, discharge, hematuria, hematocheziaPelvic pain, discharge, hematuria, hematocheziav p , d g , ,v p , d g , ,

Indications for HBOIndications for HBOIndications for HBOIndications for HBO Acutely compromised or failed skin Acutely compromised or failed skin
fl ftfl ft Carbon monoxide poisoningCarbon monoxide poisoning
D i illD i illflap or graftflap or graft Preparation for skin graftPreparation for skin graft Severe diabetic foot ulcersSevere diabetic foot ulcers
Decompression illnessDecompression illness Arterial Gas embolismArterial Gas embolism Brain abscessBrain abscess
Osteo and soft tissue radionecrosisOsteo and soft tissue radionecrosis Chronic Refractory OsteomyelitisChronic Refractory Osteomyelitis
Thermal BurnsThermal Burns Exceptional Blood Loss Exceptional Blood Loss
AnemiaAnemia
Clostridial Myonecrosis (Gas Clostridial Myonecrosis (Gas Gangrene)Gangrene)g )g )
Crush injury, Compartment Crush injury, Compartment syndromesyndrome
Acute arterial insufficiencyAcute arterial insufficiencyAcute arterial insufficiencyAcute arterial insufficiency Necrotizing FasciitisNecrotizing Fasciitis

Atypical UlcersAtypical Ulcers

Atypical UlcersAtypical UlcersAtypical UlcersAtypical Ulcers
Pyoderma GangrenosumPyoderma Gangrenosum Atrophie BlancheAtrophie Blanchey gy g Livedoid VasculopathyLivedoid Vasculopathy Bullous PemphigoidBullous Pemphigoid
pp Malignant melanomaMalignant melanoma Basal cell carcinomaBasal cell carcinomap gp g
PorphyriaPorphyria Necrobiosis Lipoidica Necrobiosis Lipoidica
Squamous cell carcinomaSquamous cell carcinoma Mycosis fungoidesMycosis fungoidespp
DiabeticorumDiabeticorum Leukocytoclastic VasculitisLeukocytoclastic Vasculitis
y gy g SclerodermaScleroderma Antiphospholipid syndromeAntiphospholipid syndrome
Mycobacterium marinum Mycobacterium marinum ulcerulcer
Factitious dermatitisFactitious dermatitis
• Biopsies are often needed to make the diagnosis

Dressings and Wound CareDressings and Wound Care

Advanced Wound DressingsAdvanced Wound DressingsAdvanced Wound DressingsAdvanced Wound Dressings
4 Basic Functions of Advanced Wound dressings4 Basic Functions of Advanced Wound dressings Protect the wound from contamination or infectionProtect the wound from contamination or infection Promote wound cleansing and debridement of unhealthy tissuesPromote wound cleansing and debridement of unhealthy tissues Absorb excess tissue fluid and wound exudates/debrisAbsorb excess tissue fluid and wound exudates/debris Absorb excess tissue fluid and wound exudates/debrisAbsorb excess tissue fluid and wound exudates/debris Maintain a moist environment for healingMaintain a moist environment for healing
Hydrating Hydrating -- hydrogelshydrogelsAb iAb i f l if l i Absorptive Absorptive –– foams, alginatesfoams, alginates
CollagenCollagen AntimicrobialAntimicrobial Skin SubstitutesSkin Substitutes
Extracellular matrix productsExtracellular matrix products Living cell therapy productsLiving cell therapy products Living cell therapy productsLiving cell therapy products
Growth factors and living keratinocytesGrowth factors and living keratinocytes

How do I start to workup the How do I start to workup the chronic wound?chronic wound?
Do a good wound assessmentDo a good wound assessmentgg Size, appearance, drainage, painSize, appearance, drainage, pain Choose a dressing to address immediate needs of Choose a dressing to address immediate needs of
ddwound wound Assess the patient’s vascular statusAssess the patient’s vascular status
Palpable pulses Arterial studiesPalpable pulses Arterial studies Palpable pulses, Arterial studiesPalpable pulses, Arterial studies Venous studies (order “reflux” evaluation)Venous studies (order “reflux” evaluation) Edema control (be cautious if arterial compromise)Edema control (be cautious if arterial compromise)
Surgical (vascular or plastics) referralSurgical (vascular or plastics) referral Based on history and appearance, classify the wound Based on history and appearance, classify the wound
typetypetypetype

How do I start to workup the How do I start to workup the
Evaluate for presence of infectionEvaluate for presence of infection
chronic wound?chronic wound?pp
Avoid swab cultures or antibiotics if not neededAvoid swab cultures or antibiotics if not needed Imaging studiesImaging studiesg gg g
If needed, determine patient’s offloading requirementsIf needed, determine patient’s offloading requirements Appliances and surfacesAppliances and surfaces Assess risk for ulcer development and healingAssess risk for ulcer development and healing
Examine the patient’s host factorsExamine the patient’s host factors Nutrition, comorbidities, social history, medicationsNutrition, comorbidities, social history, medications Anemia, renal insufficiency, liver dysfunctionAnemia, renal insufficiency, liver dysfunction Discuss likelihood of wound healing with your Discuss likelihood of wound healing with your
patientpatient

How do I start to workup the How do I start to workup the
Wound Center referralWound Center referral
chronic wound?chronic wound? Wound Center referralWound Center referral When patient comes back to youWhen patient comes back to you
E l i di i h l i dE l i di i h l i dExplain conditions that may result in wounds Explain conditions that may result in wounds or delay wound healing (eg. edema)or delay wound healing (eg. edema)
Educate on therapy to reinforce compliance Educate on therapy to reinforce compliance with recommendations with recommendations
Routinely discuss skin care and ulcer Routinely discuss skin care and ulcer preventionpreventionpp

SummarySummarySummarySummary
Wound Care and Hyperbaric Medicine has really Wound Care and Hyperbaric Medicine has really yp yyp ybecome its own subspecialtybecome its own subspecialty
Wounds can be a result of multifactorial etiologiesWounds can be a result of multifactorial etiologies Most chronic wounds fall into 6 categories but atypical Most chronic wounds fall into 6 categories but atypical
wounds should always be in the differentialwounds should always be in the differentialM l idi i li h i f d d hM l idi i li h i f d d h Multidisciplinary approach is often needed to treat the Multidisciplinary approach is often needed to treat the chronic or complex wound/limb salvagechronic or complex wound/limb salvage
Primary care providers can initiate a good workupPrimary care providers can initiate a good workup Primary care providers can initiate a good workupPrimary care providers can initiate a good workup Patient education can help tremendously to heal and Patient education can help tremendously to heal and
keep healedkeep healedpp
Related Documents











