e Integrated Health Systems Strengthening Project (IHSSP) Newsletter August - October 2013 Volume 1 Issue 2 IHSSP Office in Rwanda is located at: Kicukiro, KK 21 Avenue (Niboye Road), Plot No. 41 P.O. Box 371 Kigali PHONE: +250-788-308081 www.msh.org The Integrated Health Systems Strengthening Project (IHSSP) improves the health of Rwandans through its five components: Health Information, Health Finance, Human Resources for Health, Quality Improvement and Decentralization. Photo: Todd SHAPERA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1A u g u s t - O c t o b e r 2 0 1 3T h e I n t e g r a t e d H e a l t h S y s t e m s S t r e n g t h e n i n g P ro j e c t ( I H S S P ) N ew s l e t t e r
The Integrated Health Systems Strengthening Project (IHSSP)
NewsletterAugust - October 2013
Volume 1
Issue 2
IHSSP Office in Rwanda is located at: Kicukiro, KK 21 Avenue (Niboye Road), Plot No. 41 P.O. Box 371 KigaliPHONE: +250-788-308081 www.msh.org
The Integrated Health Systems Strengthening Project (IHSSP) improves the health of Rwandans through its five components:
Health Information, Health Finance, Human Resources for Health, Quality Improvement
and Decentralization.
Phot
o: T
odd
SHA
PER
A

A u g u s t - O c t o b e r 2 0 1 32 T h e I n t e g r a t e d H e a l t h S y s t e m s S t r e n g t h e n i n g P ro j e c t ( I H S S P ) N ew s l e t t e r
2 Editorial
3 IHSSP 2014 Planning Workshop August 28th, 2013
4 - 6 IHSSP: Most Recent Results
7 Improving Human Resources for Health Management through the New Integrated Human Resources Information System (iHRIS)in Rwanda
8 Improving Quality Service Delivery through the Development of National Clinical Protocols and Guidelines
9 Visit of Mr. Paul Auxila: MSH Executive Vice President and Chief Operations Officer
10 IHSSP Rwanda: Going to the People
11 IHSSP Presence in the East, Central, and Southern African (ECSA) Health Community Forum in Arusha, Tanzania: August, 2013
Inside this issue:
Chief Editor : Dr. Apolline UWAYITU
Redactors : Philbert RUGUMIRE, Candide TRAN NGOC
Designer : Emmanuel NTAKIRUTIMANA
Credits
This newsletter is made possible by the generous support of the American people through the US Agency for International Development (USAID), under the contract no. GHS-I-00-07-00006-00. The contents are the responsibility of the Integrated Health Systems Strengthening Project and do not necessarily reflect the views of
USAID or the US Government.
Dr. Apol l ine Uwayitu
Pho
to:
Tod
d S
hap
era
Dear Reader,
With about one year remaining in the project, sharing the
final year’s work plan with the main IHSSP partners
is crucial. This was done on August 28th, 2013 through
a workshop where we shared, finalized, and achieved consensus on the
remaining activities and discussed how the Ministry of Health (MOH) is
ready to take over.
The teams from each of the five project components, working in close
collaboration with the MOH, have achieved notable results. One of our
biggest achievements in partnership with the MOH, Ministry of Local
Administration (MINALOC), and others partners is that more than 10
million Rwandans representing 2,202,358 households (99 percent) have
been recorded in the Ubudehe stratification database. As a result, 23
percent of the population, the poorest cadre, is now benefiting from
subsidized health insurance.
In IHSSP’s final year, we will focus on institutionalization, capacity transfer,
sustainability, consolidation, and fine-tuning of previously introduced
systems strengthening initiatives. As the project provides mainly
technical assistance, the sustainability of innovations and improvements
that it helped to introduce to the Rwandan system is of the highest
priority and importance.
This second bulletin will provide information on the 2014 planning
workshop and our most recent results, activities, and achievements.
Dr. Apolline Uwayitu,Country Representative MSH-Rwanda, Project Director, IHSSP
Editorial

3A u g u s t - O c t o b e r 2 0 1 3T h e I n t e g r a t e d H e a l t h S y s t e m s S t r e n g t h e n i n g P ro j e c t ( I H S S P ) N ew s l e t t e r
IHSSP 2014 Planning Workshop August 28th, 2013
Ensure that government can continue the work and assess how the MOH is moving toward ownership!
IHSSP held a workshop with the
MOH management technical
teams in August, in which they
shared, finalized, and achieved
consensus on the remaining activities.
This was also a review of the major
achievements gained by the Ministry
of Health with USAID support
provided through IHSSP.
During a group working session, staff from the
ministry and IHSSP revised and finalized the work
plan activities. The group members also agreed
onplans for institutionalization, capacity transfer,
sustainability, consolidation, and fine-tuning of
previously introduced system strengthening
initiatives.
At the end of these working sessions, MOH
representatives provided feedback. This workshop
resulted on the agreed draft work plan, which
was submitted to USAID for approval before
proceeding to implementation.
The Ministry of Health feels that the project is great, and that all components are in the vision of the Government of Rwanda.”
-Ms. Mukakigeri Daphy, MOH Rwanda
“
IHSSP 2014 Planning Workshop
Phot
o: C
andi
de T
ran
Ngo
c

A u g u s t - O c t o b e r 2 0 1 34 T h e I n t e g r a t e d H e a l t h S y s t e m s S t r e n g t h e n i n g P ro j e c t ( I H S S P ) N ew s l e t t e r
IHSSP: Most Recent ResultsCommunity-Based Health Insurance (CBHI)
IHSSP supported the development of the community health data quality assessment (DQA) tool, which will provide a quantitative comparison
of recounted to reported data, and a review of the accuracy, completeness, reliability, precision and integrity. The project conducted a field test of the tool prior to its institutionalization within different levels of care. The above figure, confirms that the main source of funds to the CBHI is the premium contributions collected from the population (66% of total funding). The 14% contribution from government covers the contributions for impoverished citizens, the payment of referral hospital bills, and the remaining support to cover
the running costs of CBHI.
As planned by the CBHI Law, the CBHI funds are mainly sourced from the population contributions, the co-payments, the Government, and other health insurance contributions.
Rwanda Health Management Information System (R-HMIS):
The HMIS team rolled out a new version of the DHIS-2 (version 2.13), which adds new dashboard features. Users can add charts, maps, pivot tables, and links to standard reports on their dashboards. Dashboards can be pre-populated with charts and maps and shared among groups of users. The Ministry’s Planning Directorate has already used this functionality to develop a District Monitoring & Evaluation Dashboard (pictured below) that displays a key set of about 25 indicators. When district M&E officers log into the
system they see each of the charts displaying the data for their own districts; national level staff see the data aggregated across the entire country.
C B H I S O U R C E O F F U N D
GLOBAL FUND 10%
OTHERREVENUES
3%PUBLIC AND PRIVATE HEALTH INSURANCE
1%
CO-PAYMENT6%
GOVERNEMENT14%
POPULATIONCONTRIBUTION
66%

5A u g u s t - O c t o b e r 2 0 1 3T h e I n t e g r a t e d H e a l t h S y s t e m s S t r e n g t h e n i n g P ro j e c t ( I H S S P ) N ew s l e t t e r
These analyses feed into a quarterly monitoring and evaluation report that is produced in each of the districts. In the past, it was very difficult to compare performance between districts, since they often calculated indicators differently or did not report on the same set of indicators. Now each district reports on the same
set of indicators and the new tools save them time producing analyses, so that they can spend more time thinking about what the numbers mean and what they can do to improve their performance.
District Key Indicator Set Pivot Table from DHIS-2
The development of the strategic plan for the pharmacists’ council was finalized this quarter. IHSSP supported the whole development process, including the hiring of consultants, organization of work sessions, working with council members to provide inputs into the document, and the final validation,
which included other council members and stakeholders. The council is now using this plan to mobilize resources from different sources so as to be able to implement its activities.
Thirty-one percent of the 137 public sector pharmacists operate in Kigali, 69 percent in the countryside. In the private sector, 77 percent of the 239 pharmacists practice in Kigali.
A pharmacist attends to a cl ient
Development and Validation of the Pharmacists’ Council’s Strategic Plan
Phot
o: P
hilb
ert
RUG
UM
IRE

A u g u s t - O c t o b e r 2 0 1 36 T h e I n t e g r a t e d H e a l t h S y s t e m s S t r e n g t h e n i n g P ro j e c t ( I H S S P ) N ew s l e t t e r
National Clinical Protocols and Guidelines
This quarter IHSSP organized two workshops to disseminate guidelines and protocols on pain management and internal medicine adopted in late 2012. Those workshops brought together about 90 medical practitioners from both public and private health institutions operating across the country.
Some of the medical practit ioners del iberate during the seminar
Performance-Based Financing (PBF)
This quarter the health financing component focused on revising performance measurement and processes for PBF and drafting a concept note that describes the process of PBF integration to the accreditation of facilities. The intent is to use the results of accreditation to inform performance-based financing payments, as a means of recognizing facilities that progress toward meeting the quality standards and ultimately achieving accreditation. IHSSP organized a training workshop with teams from the Belgian Development Agency (CTB), the Rwanda Family Health Project (RFHP, and five hospitals. Fifty-five participants attended the workshop. The integration of existing PBF incentives and accreditation process was explained to the participants. Consequently, the standards are clear and the process for measuring these standards is rigorous, reliable, unbiased, and duplication of effort is decreased.
Quality Improvement in Health Services 2012 - B120
100
80
60
40
20
0
2008 2009 2010 2011 2012
Laboratory
Qu
alit
y av
erag
e in
hea
lth
fac
iliti
es (
%)
HIV controlGeneral OrganizationFamily Planning
Phot
o: P
hilb
ert
RUG
UM
IRE
A u g u s t - O c t o b e r 2 0 1 3T h e I n t e g r a t e d H e a l t h S y s t e m s S t r e n g t h e n i n g P ro j e c t ( I H S S P ) N ew s l e t t e r
Improving Human Resources for Health Management through the New Integrated Human
Resources Information System (iHRIS)in Rwanda
7
The health workforce is the core of every health system. In Rwanda,
qualified clinical staff are in short supply. The country has just one nurse for every 1,500 inhabitants and one doctor per 15,306 citizens, 1therefore efficiently allocating human resources is crucial to the provision of quality services.
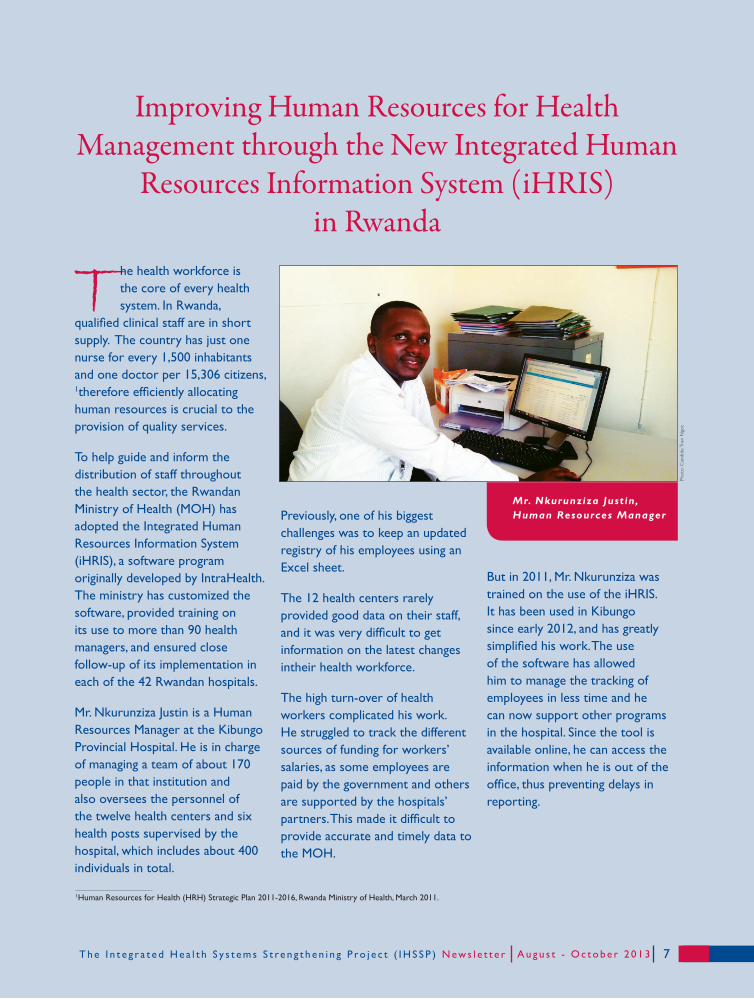
To help guide and inform the distribution of staff throughout the health sector, the Rwandan Ministry of Health (MOH) has adopted the Integrated Human Resources Information System (iHRIS), a software program originally developed by IntraHealth.The ministry has customized the software, provided training on its use to more than 90 health managers, and ensured close follow-up of its implementation in each of the 42 Rwandan hospitals.
Mr. Nkurunziza Justin is a Human Resources Manager at the Kibungo Provincial Hospital. He is in charge of managing a team of about 170 people in that institution and also oversees the personnel of the twelve health centers and six health posts supervised by the hospital, which includes about 400 individuals in total.
Previously, one of his biggest challenges was to keep an updated registry of his employees using an Excel sheet.
The 12 health centers rarely provided good data on their staff, and it was very difficult to get information on the latest changes intheir health workforce.
The high turn-over of health workers complicated his work. He struggled to track the different sources of funding for workers’ salaries, as some employees are paid by the government and others are supported by the hospitals’ partners. This made it difficult to provide accurate and timely data to the MOH.
But in 2011, Mr. Nkurunziza was trained on the use of the iHRIS. It has been used in Kibungo since early 2012, and has greatly simplified his work. The use of the software has allowed him to manage the tracking of employees in less time and he can now support other programs in the hospital. Since the tool is available online, he can access the information when he is out of the office, thus preventing delays in reporting.
Mr. Nkurunziza Just in, Human Resources Manager
1Human Resources for Health (HRH) Strategic Plan 2011-2016, Rwanda Ministry of Health, March 2011.
Phot
o: C
andi
de T
ran
Ngo
c
A u g u s t - O c t o b e r 2 0 1 3T h e I n t e g r a t e d H e a l t h S y s t e m s S t r e n g t h e n i n g P ro j e c t ( I H S S P ) N ew s l e t t e r

Improving Quality Service Delivery through the Development of National Clinical
Protocols and Guidelines
8
Until recently in Rwanda, few clinical conditions had protocols and guidelines for treatment, and the existing protocols had not been reviewed since 2007.
IHSSP filled this gap through collaboration with professional councils to develop the first edition of the National Clinical Protocols and Treatment
Guidelines, which details protocols and guidelines that are designed to provide a useful resource for healthcare professionals involved in clinical case management in Rwanda. These new clinical protocols and treatment guidelines will:
- Improve the management of common high risk clinical conditions, resulting in consistent and appropriate treatment;
- Help ensure efficient use of resources and
encourage standardized rational use of drugs;
- Provide quality care by standardizing treatment, promotinginterventions of proven benefit, and discouraging in effective interventions;
- Harmonize the supply chain system; and
- Contribute to the streamlining of referral systems and inform the next review of the essential drug list and drug formulary.
Through extensive working sessions and consultations, clinicians developed clinical protocols for high risk and high volume clinical conditions. The document details protocols and treatment guidelines designed to provide a useful resource for healthcare professionals in Rwanda.IHSSP held a workshop to disseminate the document, elaborate on its use, and explain its usefulness to clinicians.
Airway &Breathing
1. Obstructed breathing2. Central Cyanosis3. Severe respiratory distress4. Weak / absent breathing
Cold Hands with any of:5. Capillary refill > 23 seconds6. Weak + fast pulse7. Slow (<60bpm) or absent pulse
Immediate transfer to emergency area:1. Start Life support procedures2. Give oxygen3. Weigh if possible
Circulation
Coma / convulsing / confusion: AVPU = ‘P or U’ or Convulsions
- Tiny – sick infant aged < 2 months- Temperature - very high > 39.50C- Trauma - major trauma- Pain – child in severe pain- Poisoning – mother reports poisoning- Pallor - severe palmar pallor- Restless/Irritable/Floppy- Respiratory distress- Referral – has an urgent referral letter- Malnutrition – Visible severe wasting
Front in the queue – Clinical review as soon as possible:- Weigh- Baseline Observations
Priority signs
Phot
o: P
hilb
ert
RUG
UM
IRE
Example of Flow chart for Triage in pediatric emergencies protocol
A u g u s t - O c t o b e r 2 0 1 3 T h e I n t e g r a t e d H e a l t h S y s t e m s S t r e n g t h e n i n g P ro j e c t ( I H S S P ) N ew s l e t t e r

9A u g u s t - O c t o b e r 2 0 1 3T h e I n t e g r a t e d H e a l t h S y s t e m s S t r e n g t h e n i n g P ro j e c t ( I H S S P ) N ew s l e t t e r
Visit of Mr. Paul Auxila: MSH Executive Vice President and Chief Operations Officer
Mr. Paul Auxila, MSH’s Executive Vice President and Chief
Operations Officer visited IHSSP in October. He congratulated the
IHSSP staff, saying that their work was very effective.
Met with IHSSP, USAID, and Ministry of Health Representatives
“ You don’t need to be perfect, but do the best you can in strategic and innovative ways, according to the country’s context, to improve the health of Rwandans, which should be your main objective,” he said.
Mr. Paul Auxi la, MSH Executive Vice President and Chief Operations Off icer (COO)
“You have had a wonderful journey so far, which
has not always been without difficulties.”
Mr. Auxila also met with USAID and Ministry of
Health Representatives.
S O M E A C H I E V E M E N T S :The Rwandan Ministry of Health, in collaboration with MSH/ISSP and other partners, has achieved
the following results:
• 45,000 community health workers have been trained;
• More than 90% of the population has access to health services;
• Nearly 100% of pregnant women receive antenatal care;
• Death of children under the age of five has dropped by over half (2005 to 2010 DHS);
• Health facilities now maintain adequate stocks of medicines;
• Use of modern contraception has increased from 10% in 2005 to 45% in 2010.
MSH Rwanda and IHSSP would like to acknowledge support from the Rwanda Ministry of Health, the Rwanda Biomedical Center, and other national and international partners who have worked closely with us.
Photo: Philbert RUGUMIRE
A u g u s t - O c t o b e r 2 0 1 310 T h e I n t e g r a t e d H e a l t h S y s t e m s S t r e n g t h e n i n g P ro j e c t ( I H S S P ) N ew s l e t t e r
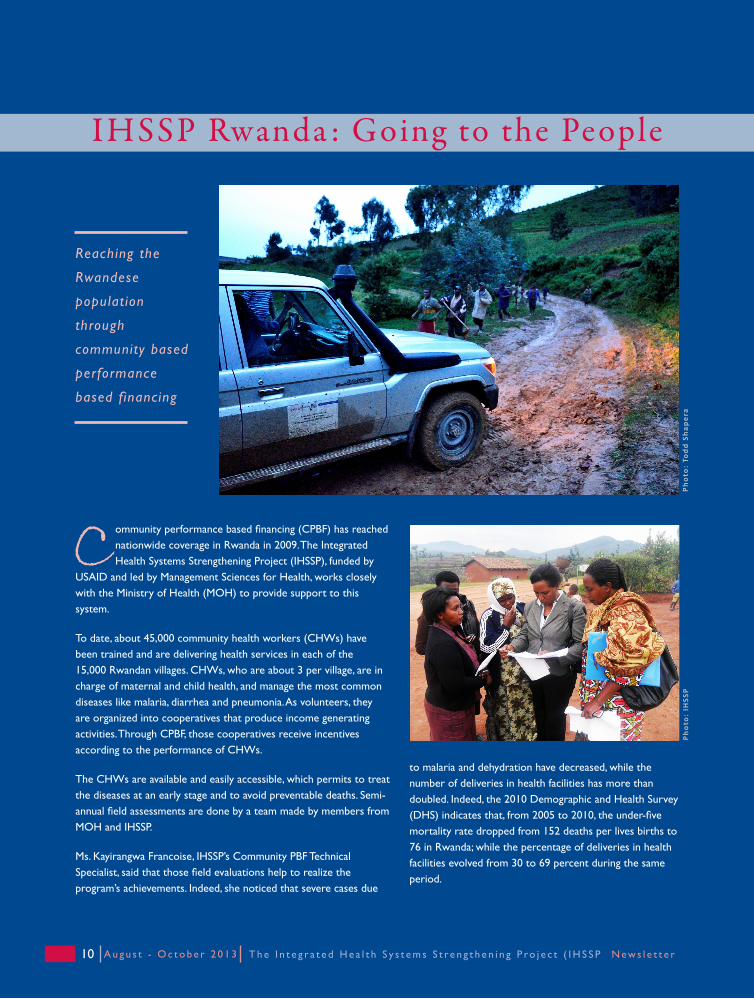
Community performance based financing (CPBF) has reached nationwide coverage in Rwanda in 2009. The Integrated Health Systems Strengthening Project (IHSSP), funded by
USAID and led by Management Sciences for Health, works closely with the Ministry of Health (MOH) to provide support to this system.
To date, about 45,000 community health workers (CHWs) have been trained and are delivering health services in each of the 15,000 Rwandan villages. CHWs, who are about 3 per village, are in charge of maternal and child health, and manage the most common diseases like malaria, diarrhea and pneumonia. As volunteers, they are organized into cooperatives that produce income generating activities. Through CPBF, those cooperatives receive incentives according to the performance of CHWs.
The CHWs are available and easily accessible, which permits to treat the diseases at an early stage and to avoid preventable deaths. Semi-annual field assessments are done by a team made by members from MOH and IHSSP.
Ms. Kayirangwa Francoise, IHSSP’s Community PBF Technical Specialist, said that those field evaluations help to realize the program’s achievements. Indeed, she noticed that severe cases due
Reaching the
Rwandese
populat ion
through
community based
performance
based financing
IHSSP Rwanda : Going to the People
to malaria and dehydration have decreased, while the number of deliveries in health facilities has more than doubled. Indeed, the 2010 Demographic and Health Survey (DHS) indicates that, from 2005 to 2010, the under-five mortality rate dropped from 152 deaths per lives births to 76 in Rwanda; while the percentage of deliveries in health facilities evolved from 30 to 69 percent during the same period.
Pho
to:
Tod
d S
hap
era
Pho
to:
IHSS
P

11A u g u s t - O c t o b e r 2 0 1 3T h e I n t e g r a t e d H e a l t h S y s t e m s S t r e n g t h e n i n g P ro j e c t ( I H S S P ) N ew s l e t t e r
World Health Organization, NCDs, such as cancers,
diabetes, and cardiovascular and respiratory diseases
account for nearly 25 percent of Rwanda’s burden of
disease. This represents a major financial burden for
the poorest, who would have to pay out of pocket for
their care if the services were not covered by CBHI.
In Rwanda, NCDs are already integrated into the
health service packages, and patients with chronic
diseases can benefit from specialized health treatment,
thanks to CBHI.
This forum permitted health specialists to share
experiences and make recommendations on health
policies in the ECSA region. The aim of these
recommendations is to help member states take the
lead in strategy development and planning, which will
allow better integration and management of NCDs.
IHSSP Presence in the East, Central, and Southern African (ECSA) Health Community
Forum in Arusha, Tanzania: August, 2013
Extending access to health care for non-communicable diseases in Rwanda through community-based health insurance
Thérèse Kunda,Technical Advisor, Community Based Health Insurance (CBHI), IHSSP (standing) and
Joseph SHEMA, Head of PBF (MoH), at the Forum
F rom August 10 to 14, 2013, Ms. Thérèse
Kunda, IHSSP’s community-based health
insurance (CBHI) Technical Advisor and
Mr. Joseph Shema, Head of the MOH’s Health
Financing Unit, attended the 7th East, Central, and
Southern African (ECSA) Best Practices Forum in in
Arusha, Tanzania.
This forum brought together senior officialsfrom
ministries of health, health researchers, heads of
health training institutions, and diverse collaborating
partners to identify key policy issues and make
recommendations to strengthen the response to
emerging and re-emerging health concerns in the
ECSA region.
Ms. Kunda presented a paper detailing how CBHI
has increased access to care for non-communicable
diseases (NCDs) in Rwanda. According to the
Par tic ipants at the ForumPhoto: ARUSHA Conference
Phot
o: A
RUSH
A C
onfe
renc
e

A u g u s t - O c t o b e r 2 0 1 312 T h e I n t e g r a t e d H e a l t h S y s t e m s S t r e n g t h e n i n g P ro j e c t ( I H S S P ) N ew s l e t t e r
“You don’t need to be perfect, but to do the best you can in strategic and innovative ways…
to improve the health of Rwandans.”- Mr. Paul Auxila, MSH Executive Vice President and Chief Operations Officer (COO)
I H S S P N e w s l e t t e r
Photo: Todd SHAPERA
MSH Rwanda/IHSSP Communications Team: [email protected] / [email protected]
Related Documents











