The Importance of Beta- Blockers in Patients with Heart Failure: A Resynchronization- Defibrillation for Ambulatory Heart Failure Trial (RAFT) Analysis. L. Brent Mitchell, Jean L. Rouleau, Gary E. Newton, Jonathon Howlett, Elizabeth Yetisir, George A. Wells, Anthony S.L. Tang

The Importance of Beta-Blockers in Patients with Heart Failure: A Resynchronization-Defibrillation for Ambulatory Heart Failure Trial (RAFT) Analysis.
Dec 14, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The Importance of Beta-Blockers in Patients with Heart Failure:
A Resynchronization-Defibrillation for Ambulatory Heart Failure Trial (RAFT)
Analysis.
L. Brent Mitchell, Jean L. Rouleau, Gary E. Newton, Jonathon Howlett, Elizabeth Yetisir, George A. Wells, Anthony S.L. Tang

DECLARATION - 1
Beta-Blockers
ACE-I / ARB
Aldo Block
CRT
Declaration of Potential Conflict of Interest
• I have nothing to declare

BACKGROUND - 1
Beta-Blockers
ACE-I / ARB
Aldo Block
ICD
CRT
CHF - Proven Effective Therapies on All-Cause Mortality

• multicenter, randomized, two parallel-group, clinical trial
• 1798 patients with NYHA II/III congestive heart failure
• receiving optimal medical therapy
• with LVEF ≤ 0.30 and QRSd ≥ 120ms (≥ 200ms if V-paced)
• and with an independent indication for an ICD
• were randomized 1:1 to receive an ICD or a CRT-ICD
Resynchronization-defibrillation for Ambulatory heart Failure Trial (RAFT)
BACKGROUND - 2

RAFT Results: Death or CHF Hospitalization
BACKGROUND - 3
0
10
20
40
50
30
Cu
mu
lati
ve In
cid
ence
1 2 3 4 60
Years of Follow-up
5
60ICD
CRT-ICD
HR = 0.7595% CI: 0.64 – 0.87p < 0.001
Tang AS et al. N Engl J Med 363:2385-95, 2010

BACKGROUND - 4
CHF - Proven Effective Therapies on All-Cause Mortality
Beta-Blockers
ACE-I / ARB
Aldo Block
ICD
CRT

PURPOSE
To assess the contemporary importance,
independence, and dose-dependence of
beta-blocker therapy in the congestive
heart failure patients studied in RAFT.

METHODS
PATIENT POPULATION: RAFT patients that were treatedwith one of bisoprolol, carvedilol, or metoprolol.
BETA-BLOCKER TARGET DOSAGES: were as defined byESC guidelines1 - bisoprolol 10 mg/d, carvedilol 50 mg/d,metoprolol 200 mg/d.
PRIMARY OUTCOME: death or CHF hospitalization.
STATISTICS: Times to outcome displayed as KM curves.Sixteen variables were included in stepwise proportionalhazards analyses.
1. McMurray JJV et al. Eur Heart J 33:1787-847, 2012

RESULTS - 1
The RAFT Patient Population:
• N = 1798, mean age 66 yrs, 83% male, 67% ischemic• 80% NYHA Class II, mean LVEF 0.23• 90% beta-blocker use, 97% ACE-I / ARB use• 42% spironolactone use
This Substudy Patient Population (82%):
• N = 1474, mean age 66 yrs, 83% male, 66% ischemic• 82% NYHA Class II, mean LVEF 0.23• 100% beta-blocker use, 97% ACE-I / ARB use• 42% spironolactone use

RESULTS - 2
Beta-Blocker Use Distributions
< 50% target
≥ 50% target
bisoprolol carvedilol metoprolol0
100
200
300
400
500
600
700
nu
mb
er
489
356
629
(39%) (34%)(67%)
p < 0.001

Population Differences by Beta-Blocker Dosage
RESULTS - 3
VARIABLE BB < 50% Target BB ≥ 50% Target P-value
Age (years ± SD) 67.5 ± 9.0 64.6 ± 9.6 <0.0001
Ischemic HD n(%) 541 (73.2%) 436 (59.3%) <0.0001
NYHA Class II n(%) 568 (76.9%) 621 (84.5%) 0.0002
Weight (kg ± SD) 79.6 ± 16.5 85.3 ± 18.1 <0.0001
BMI (± SD) 27.1 ± 5.1 28.6 ± 5.4 <0.0001
Prior CABG n(%) 288 (39.0%) 214 (29.1%) <0.0001
PVD n(%) 88 (11.9%) 61 (8.3%) 0.0216
CHF Hosp < 6mo n(%) 211 (28.6%) 166 (22.6%) 0.0087
Beta-blocker use at baseline n(%) 643 (87.0%) 709 (96.3%) <0.0001
ASA use n(%) 517 (70.0%) 477 (64.9%) 0.0381
Warfarin use n(%) 231 (31.3%) 266 (36.2%) 0.0452
Clopidogrel use n(%) 130 (17.6 %) 96 (13.1%) 0.0158
Amiodarone use n(%) 114 (15.4%) 78 (10.6%) 0.0060
eGFR (ml/min/1.73m2 ± SD) 58.7 ± 21.9 61.8 ± 19.1 0.0039
6 MWT distance (m ± SD) 346 ± 111 367 ± 107 0.0010

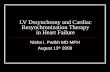
Death / CHF Hospitalization by Beta-Blocker Dosage
RESULTS - 4
0
10
20
40
50
30
Cu
mu
lati
ve In
cid
ence
1 2 3 4 60
Years of Follow-up
5
60< 50%
≥ 50%
HR = 1.5095% CI = 1.24 – 1.81p < 0.001

Independent Predictors of Primary Outcome
RESULTS - 5
PARAMETER HR (95% CI) P-value
previous CABG 1.63 (1.32-2.02) <0.0001
beta-blocker < 50% target 1.50 (1.24-1.81) <0.0001
ICD without CRT 1.50 (1.25-1.80) <0.0001
ischemic heart disease 1.39 (1.07-1.80) 0.01
peripheral vascular disease 1.36 (1.04-1.76) 0.02
lower estimated GFR (per 5 units) 1.10 (1.01-1.16) 0.0002

0
20
40
1 2 3 4 60 5
60
0
20
40
1 2 3 4 60 5
60
0
20
40
1 2 3 4 60 5
60
RESULTS - 6
Death / CHF Hospitalization by Beta-Blocker Dosage
Years of Follow-up
< 50%
≥ 50%Inc
ide
nc
e
0
20
40
1 2 3 4 60 5
60
Inc
ide
nc
e
by beta-blocker dosage (N=1474)
Years of Follow-up
< 50%
< 50%
< 50%
≥ 50%
≥ 50%
≥ 50%
by carvedilol dosage (N=629)
by bisoprolol dosage (N=489)
by metoprolol dosage (N=356)
p < 0.0001 p < 0.0001
p < 0.0001 p = 0.006

0
20
40
1 2 3 4 60 5
60
0
20
40
1 2 3 4 60 5
60
RESULTS - 7C
um
ula
tive
Inci
den
ce
Years of Follow-up
Death / CHF Hospitalization by RAFT Randomisation
Randomised to CRT-ICD (N=740)
Years of Follow-up
p < 0.001 p = 0.07
Randomised to ICD (N=734)
< 50%
≥ 50%
< 50%
≥ 50%

• independent predictors of death / CHF hospitalization were:
• beta-blockers use at < 50% (not ≥ 50%) of target dosage• use of an ICD (not a CRT-ICD)• ischemic heart disease and previous CABG• peripheral vascular disease or impaired renal function
• with lower dosage these outcome were 50% more likely
• there were no efficacy differences among the beta-blockers•
• carvedilol is more often used at ≥ 50% of target dosages
• the superiority of higher beta-blocker dosages are less evident in CRT-ICD patients than in ICD patients
INFERENCES
In this subgroup analysis of CHF patients studied in RAFT:

The Importance of Beta-Blockers in Patients with Heart Failure:
A Resynchronization-Defibrillation for Ambulatory Heart Failure Trial (RAFT)
Analysis.
L. Brent Mitchell, Jean L. Rouleau, Gary E. Newton, Jonathon Howlett, Elizabeth Yetisir, George A. Wells, Anthony S.L. Tang
Related Documents