The impacts of pre-surgery wait for total knee replacement on pain, function and health-related quality of life six months after surgeryFrançois Desmeules PT PhD, 1 Clermont E Dionne OT PhD, 2 Étienne L Belzile MD FRCSC, 3 Renée Bourbonnais PhD 4 and Pierre Frémont MD PhD 5 1 Graduate Student, Population Health Research Unit, Research Centre of the Laval University Affiliated Hospital, Quebec, QC, Canada and Graduate Student, Department of Social and Preventive Medicine, Faculty of Medicine, Laval University, Quebec, QC, Canada 2 Director, Population Health Research Unit, Research Centre of the Laval University Affiliated Hospital, Quebec, QC, Canada and Professor, Department of Rehabilitation, Faculty of Medicine, Laval University, Quebec, QC, Canada 3 Orthopaedic Surgeon, Laval University Hospital (CHUQ), Quebec, QC, Canada 4 Professor, Department of Rehabilitation, Faculty of Medicine, Laval University, Quebec, QC, Canada and Researcher, Community Health Care Centre (CSSS) de la Vieille-Capitale, Quebec, QC, Canada 5 Professor, Department of Rehabilitation, Faculty of Medicine, Laval University, Quebec, QC, Canada and Researcher, Laval University Hospital (CHUQ), Quebec, QC, Canada Keywords function, health organization, health-related quality of life, knee replacement, pain, waiting lists Correspondence Assistant Professor François Desmeules École de Réadaptation Université de Montréal CP 6128 Succursale Centre-Ville Montréal, Québec Canada H3C 3J7 E-mail: [email protected] Accepted for publication: 16 July 2010 doi:10.1111/j.1365-2753.2010.01541.x Abstract Objective The purpose of the current study was to assess, in patients scheduled for primary total knee replacement (TKR), the effects of pre-surgery waiting time on pain and func- tional limitations related to the knee joint undergoing surgery, on health-related quality of life (HRQoL) and on contralateral knee pain 6 months after surgery. Method A total of 141 patients scheduled for TKR were recruited from three hospitals in Quebec City, Canada, and followed up until 6 months after surgery. Pre-surgery wait, defined as the time between enrolment on the pre-surgery waiting list and surgery, was considered in four categories (3, >3–6, >6–9, >9 months). Pain and functional limitations were measured with the Western Ontario and McMaster Osteoarthritis Index (WOMAC). HRQoL was measured with the SF-36. Results Mean pre-surgery waiting time was 184 (SD: 120.8) days. Six months after TKR, a significant difference was seen between the four groups of pre-surgery wait in terms of HRQoL SF-36 role physical [F(3, 136) = 2.74, P = 0.046] and contralateral knee WOMAC pain [F(3, 136) = 5.78, P = 0.0009] scores. Participants with the longest pre-surgery wait (>9 months) showed the worst scores 6 months after TKR. Conclusions Longer pre-surgery waiting time had a negative clinically important impact on HRQoL and contralateral knee pain 6 months after surgery. Introduction Total knee replacement (TKR) surgery is a common surgical pro- cedure that allows for an effective reduction of pain and adequate restoration of function for the vast majority of patients suffering from advanced knee osteoarthritis or other forms of arthritis [1]. Patients endure increasing pain, functional limitations and loss of health-related quality of life (HRQoL) for many years before ulti- mately undergoing TKR. In the last decades, the growing needs of the population have made this procedure, along with hip replace- ment, the second most popular orthopaedic surgery and future estimates indicate that demands will increase in years to come [2,3]. In Organisation for Economic Co-operation and Development countries, access to TKR surgery is limited by lengthy waiting lists where mean waiting time may range from 85 to 281 days [4]. In Canada, with the development of new government policies, more patients are being operated but waiting times remain a problem and recent data show that across the country, the median pre- surgery waiting time is 169 days [5]. Therefore, once TKR has been identified as a necessary treatment, patients have to wait for several months with important pain, functional limitations and impaired HRQoL. These potentially avoidable delays represent an important burden for patients [6]. Moreover, some authors have suggested that long delays for surgery could result in patient’s deterioration in terms of pain, functional limitations and HRQoL Journal of Evaluation in Clinical Practice ISSN 1356-1294 © 2010 Blackwell Publishing Ltd, Journal of Evaluation in Clinical Practice 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The impacts of pre-surgery wait for total knee replacementon pain, function and health-related quality of life sixmonths after surgeryjep_1541 1..10
François Desmeules PT PhD,1 Clermont E Dionne OT PhD,2 Étienne L Belzile MD FRCSC,3
Renée Bourbonnais PhD4 and Pierre Frémont MD PhD5
1Graduate Student, Population Health Research Unit, Research Centre of the Laval University Affiliated Hospital, Quebec, QC, Canada andGraduate Student, Department of Social and Preventive Medicine, Faculty of Medicine, Laval University, Quebec, QC, Canada2Director, Population Health Research Unit, Research Centre of the Laval University Affiliated Hospital, Quebec, QC, Canada and Professor,Department of Rehabilitation, Faculty of Medicine, Laval University, Quebec, QC, Canada3Orthopaedic Surgeon, Laval University Hospital (CHUQ), Quebec, QC, Canada4Professor, Department of Rehabilitation, Faculty of Medicine, Laval University, Quebec, QC, Canada and Researcher, Community Health CareCentre (CSSS) de la Vieille-Capitale, Quebec, QC, Canada5Professor, Department of Rehabilitation, Faculty of Medicine, Laval University, Quebec, QC, Canada and Researcher, Laval University Hospital(CHUQ), Quebec, QC, Canada
Keywords
function, health organization, health-relatedquality of life, knee replacement, pain,waiting lists
Correspondence
Assistant Professor François DesmeulesÉcole de RéadaptationUniversité de MontréalCP 6128 Succursale Centre-VilleMontréal, QuébecCanada H3C 3J7E-mail: [email protected]
Accepted for publication: 16 July 2010
doi:10.1111/j.1365-2753.2010.01541.x
AbstractObjective The purpose of the current study was to assess, in patients scheduled for primarytotal knee replacement (TKR), the effects of pre-surgery waiting time on pain and func-tional limitations related to the knee joint undergoing surgery, on health-related quality oflife (HRQoL) and on contralateral knee pain 6 months after surgery.Method A total of 141 patients scheduled for TKR were recruited from three hospitals inQuebec City, Canada, and followed up until 6 months after surgery. Pre-surgery wait,defined as the time between enrolment on the pre-surgery waiting list and surgery, wasconsidered in four categories (�3, >3–6, >6–9, >9 months). Pain and functional limitationswere measured with the Western Ontario and McMaster Osteoarthritis Index (WOMAC).HRQoL was measured with the SF-36.Results Mean pre-surgery waiting time was 184 (SD: 120.8) days. Six months after TKR,a significant difference was seen between the four groups of pre-surgery wait in terms ofHRQoL SF-36 role physical [F(3, 136) = 2.74, P = 0.046] and contralateral knee WOMACpain [F(3, 136) = 5.78, P = 0.0009] scores. Participants with the longest pre-surgery wait(>9 months) showed the worst scores 6 months after TKR.Conclusions Longer pre-surgery waiting time had a negative clinically important impacton HRQoL and contralateral knee pain 6 months after surgery.
IntroductionTotal knee replacement (TKR) surgery is a common surgical pro-cedure that allows for an effective reduction of pain and adequaterestoration of function for the vast majority of patients sufferingfrom advanced knee osteoarthritis or other forms of arthritis [1].Patients endure increasing pain, functional limitations and loss ofhealth-related quality of life (HRQoL) for many years before ulti-mately undergoing TKR. In the last decades, the growing needs ofthe population have made this procedure, along with hip replace-ment, the second most popular orthopaedic surgery and futureestimates indicate that demands will increase in years to come[2,3].
In Organisation for Economic Co-operation and Developmentcountries, access to TKR surgery is limited by lengthy waiting listswhere mean waiting time may range from 85 to 281 days [4]. InCanada, with the development of new government policies, morepatients are being operated but waiting times remain a problemand recent data show that across the country, the median pre-surgery waiting time is 169 days [5]. Therefore, once TKR hasbeen identified as a necessary treatment, patients have to wait forseveral months with important pain, functional limitations andimpaired HRQoL. These potentially avoidable delays represent animportant burden for patients [6]. Moreover, some authors havesuggested that long delays for surgery could result in patient’sdeterioration in terms of pain, functional limitations and HRQoL
Journal of Evaluation in Clinical Practice ISSN 1356-1294
© 2010 Blackwell Publishing Ltd, Journal of Evaluation in Clinical Practice 1

and could ultimately affect post-surgery outcomes [7–10]. Fewstudies have looked at the effects of pre-surgery waiting time inpatients undergoing TKR, and those that have done so haveyielded conflicting evidence. Six studies found a significant,although clinically small to moderate, deterioration of patientswhile on pre-surgery waiting lists in terms of pain and functionallimitations [9,11–15], four other studies found no significantchanges [16–19]. However, as outlined by a recent systematicreview, the majority of these studies were underpowered, of poormethodological quality or had relatively short pre-surgery waitingtimes [10]. Only two of these studies looked at the effects ofpre-surgery wait on the TKR post-surgery outcomes and none ofthese studies found a significant deleterious effect of pre-surgerywaiting time on post-surgery pain, function or HRQoL [16,19,20].But again, short pre-surgery waiting times or low methodologicalquality could have biased their conclusions.
We have previously reported results from a cohort of Canadianpatients waiting for TKR (mean waiting time: 183 days), demon-strating a significant deterioration of their condition in terms ofpain and functional limitations related to the knee scheduled forsurgery, in HRQoL and in contralateral knee pain while waiting forsurgery [15]. Following on these results, the purpose of the currentstudy was to assess, in patients scheduled for primary TKR, theeffects of pre-surgery waiting time on pain and functional limita-tions related to the knee joint undergoing surgery, on HRQoL andon contralateral knee pain 6 months after surgery.
Methods
Study design
This study was a longitudinal prospective epidemiological studywith repeated measures.
Settings
From February 2006 to September 2007, patients were recruitedfrom the waiting lists of the departments of orthopaedic surgery ofthree university hospitals in Quebec City, Canada (CHUL, HSFAand HDQ). All seven surgeons performing TKR in these hospitalsparticipated in the study.
Participants
Every week, patients newly enrolled on the waiting lists of thethree hospitals were contacted by a research nurse. Eligible sub-jects had to meet the following inclusion criteria: (1) aged 40 yearsor more; (2) newly enrolled on the orthopaedic waiting lists forprimary unilateral TKR; (3) resident of the province of Quebec,with provincial universal health insurance coverage; (4) under-stands and speaks French. Patients were excluded if they weresuffering from a severe cardiac condition, any severe degenerativedisease or a severe mental disorder. Patients with a previous jointreplacement (hip or knee) were also excluded. Those who suffereda major trauma to the knee in the previous year or underwentsurgery urgently within 30 days of being put on the waiting listwere further excluded.
Data collection
Data were collected through review of the subjects’ medical filesand structured telephone interviews, lasting about 45 minutes,conducted by three trained interviewers. The interviews were con-ducted a few days after enrolment on the pre-surgery waiting list(mean � SD: 12.6 � 4.7 days) and 6 months after the TKR(mean � SD: 188.7 � 5.4 days). This paper focuses on the effectsof waiting time 6 months after surgery. The results of anotherinterview that took place before surgery, regarding change in pain,functional limitations and HRQoL prior to TKR have beenreported previously [15].
The main independent variable was pre-surgery waiting timedefined as the period (in days) between the date the patient was puton the waiting list and the actual date of surgery. These dates wereextracted from the surgical waiting list database of each hospital.Pre-surgery wait was considered in categories because of the non-linear association with the dependent variables [15,21]. Four cat-egories of waiting time were used (�3, >3–6, >6–9 and >9months) for analyses, because these categories are used as thresh-olds of established maximum acceptable waiting times (MAWT)[22,23]. At the 6-month follow up interview, patients were alsoasked if they had postponed their surgery for personal reasons.
The first dependent variable was the Western Ontario andMcMaster Osteoarthritis Index (WOMAC), which measures pain,stiffness and functional limitations related to the knee [24]. TheWOMAC scores were transformed in order to obtain a range from0 to 100, where a score of 100 indicated no pain or any functionallimitations. The WOMAC has been found to have very goodreliability, convergent construct validity and responsiveness, andhas been used extensively with similar populations [25–27].
The second dependent variable addressed HRQoL and was mea-sured with the Medical Outcomes Study 36-Item Short FormHealth Survey (SF-36), a generic questionnaire on health statusand HRQoL related to eight dimensions of health [28]. It allowsfor the calculation of a specific scale for each of the eight healthdimensions. The score ranges from 0 to 100, where 100 indicatesoptimal HRQoL. Use of the SF-36 has been extensive in thispopulation [19,20,28–32]. The reliability and validity of this ques-tionnaire have been well established [33–35].
The third dependent variable addressed contralateral knee painand was assessed with the WOMAC pain scale. The WOMACfunction scale was not used to measure functional limitations ofthe contralateral knee because of time constraint. The use of thepain scale without the function scale is possible as the WOMACscales’ results are commonly presented separately [36].
Initial diagnosis, anthropometric data and comorbiditieswere collected through review of the subjects’ medical files. TheCumulative Illness Rating Scale was used to assess the burden ofcomorbidities [37].
Marital status, household living status and clinical variablessuch as duration of disease symptoms and use of a walking aidwere documented during the first interview. Formal education,employment status, household income and social support werealso measured at the first interview with questions drawn from thequestionnaire of the 1998 Quebec Health Survey [38]. Psychologi-cal distress was documented with a modified version of the Psy-chological Symptom Index, which measures depression andanxiety during the last week (range 0–42) [39].
The impacts of pre-surgery wait on TKR F. Desmeules et al.
© 2010 Blackwell Publishing Ltd2

Surgical variables, such as type of implant, bearing type,implant fixation, patella resurfacing and the number and type ofin-hospital complications (wound infection, dislocation, kneeankylosis and manipulation, cardiovascular/pulmonary/circulatorycomplications, peripheral/central nervous system involvement,urinary infection, acute confusion, tendon and ligament rupture,blood transfusion) following TKR, were documented through thereview of the subjects’ medical files. Hospital length of stay anddischarge to a rehabilitation or recovery facility were also docu-mented through review of the subjects’ medical files.
Six months after surgery, patients were asked about their currentuse of a walking aid and the number of community physiotherapytreatment hours they received following discharge from thehospital.
Analyses
Descriptive statistics were used to summarize waiting time, sub-jects’ characteristics as well as WOMAC and SF-36 scores. PairedStudent’s t-tests and 95% confidence intervals (95% CI) were usedto assess overall change in the mean WOMAC and SF-36 scoresbetween the baseline and 6 months after TKR interviews. Usingwaiting time in four categories, an analysis of covariance wasconducted to compare mean WOMAC and SF-36 scores 6 monthsafter surgery by groups of waiting time. For the SF-36, only thethree more responsive health domain scores related to physicalhealth – physical functioning, role-physical and bodily pain – arepresented in this paper [40]. All regression models were adjustedfor initial WOMAC or SF-36 scores at enrolment on pre-surgerylists. Confounding was defined as a change of at least 10% on thewaiting time effect (regression coefficient), and independent vari-ables (demographic, clinical, socio-economic and psychosocial)meeting this definition were included in final adjusted models [41].Data were initially checked for normal distribution. Because of thesmall number of subjects in some categories of waiting time,values of the dependent variables were also transformed into ranksand the resulting models were compared with initial models toassess their robustness [42]. Residual plots, outliers and multicol-linearity of final models were also assessed. Significance level wasset at 0.05. All statistical analyses were performed with the SASsoftware version 9.1 for Windows (SAS Institute Inc, Cary, NC,USA).
Ethics
All participants signed an informed consent form. The study wasapproved annually by the Research Ethics Boards of all threehospitals.
Results
Participants
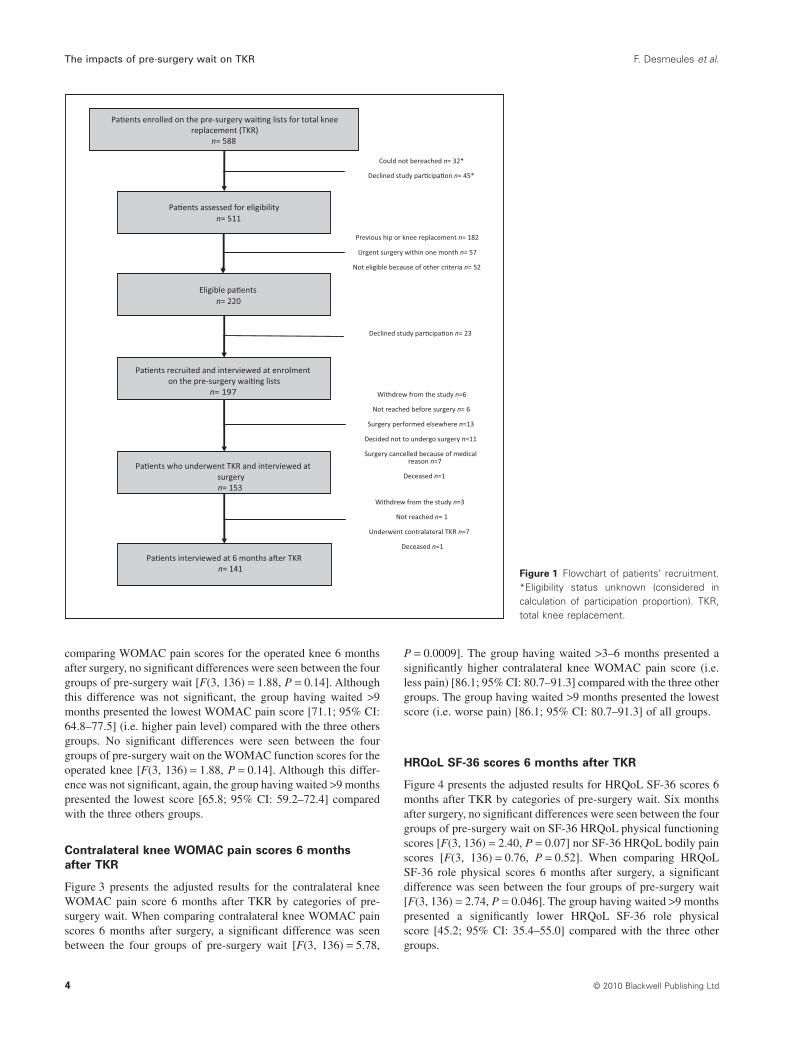
Figure 1 presents the flow of patients considered and recruited forthis study. Overall, 588 consecutive new patients were enrolled onthe pre-surgery waiting lists for knee replacement during therecruitment period. A total of 220 patients were found eligible, ofwhom 197 accepted to participate. Forty-five patients refused toparticipate before eligibility was assessed and 32 could not be
contacted within 3 weeks. These patients were included in thecalculation of the overall eligibility proportion, (220 + 32)/(588 –45) = 0.464 and in the calculation of the participation proportion,
197/(220 + (45 ¥ 0.464)) = 81.8%. A total of 141 subjects com-pleted the interview conducted 6 months after surgery (72% of theinitial cohort). Thirteen had surgery performed outside the threestudy hospitals. Eleven decided not to undergo surgery for per-sonal reasons. Seven had the surgery cancelled for medicalreasons. One subject died during wait and one after surgery (notrelated to TKR). Seven subjects underwent contralateral kneereplacement in the 6 months following the first knee replacement.Nine subjects withdrew from the study and seven could notbe reached at follow-up interviews (follow-up proportion:(197 - 9- 7)/197 = 92%).
Pre-surgery waiting time andsubjects’ characteristics
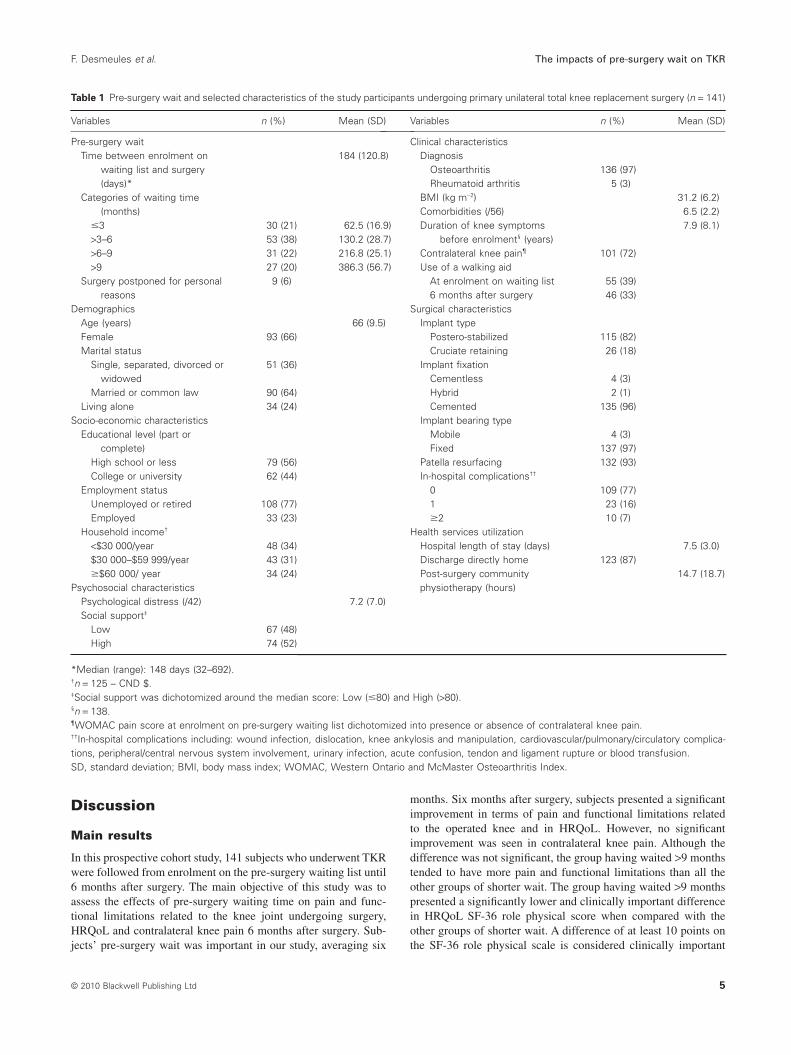
Table 1 presents pre-surgery waiting time and selected character-istics of the participants of this study. Mean waiting time was 184(SD: �120.8) days and median waiting time was 148 days (range32–692). Subjects had a mean age of 66 (SD: �9.5) years. Themajority of patients were women (66%) and suffered from con-tralateral knee pain (72%). The majority of implants were postero-stabilized (82%) and cemented (96%). Mean hospital length ofstay was 7.5 days (SD: �3.0) and only 18 subjects (13%) were notdischarged directly at home. 33 subjects (23%) sufferedin-hospital complications; the most common complication waspost-surgery anaemia requiring a blood transfusion.
Overall changes in WOMAC and SF-36 scoresbetween enrolment on pre-surgery waiting listsand 6 months after TKR
Participants showed significant improvement 6 months aftersurgery on the WOMAC pain [30.6; 95% CI: 26.9–34.2] andfunction [25.4; 95% CI: 22.0–28.8] scores related to the operatedknee. No significant improvements were observed on the con-tralateral knee WOMAC pain score [1.1; 95% CI: –2.6 to 4.8]. Interms of HRQoL, subjects showed a significant improvement 6months after surgery in the HRQoL SF-36 physical functioning[17.8; 95% CI: 14.1–21.5], role physical [18.4; 95% CI: 12.8–24.0] and bodily pain [9.4; 95% CI: 6.7–12.1] scores (Table 2).
Effects of pre-surgery waiting time 6 monthsafter TKR
Because no important differences were found between the initialregression models and those in which values of the dependentvariables were transformed into ranks, the final models were builtwith untransformed scores. All models were adjusted for initialWOMAC or SF-36 baseline scores at enrolment on pre-surgerywaiting lists. The only independent variable to have a confoundingeffect was age for the HRQoL role-physical model; it was there-fore kept in that final model.
WOMAC pain and function scores for the operated
knee 6 months after TKR
Figure 2 presents results for WOMAC pain and function scores6 months after TKR by categories of pre-surgery wait. When
F. Desmeules et al. The impacts of pre-surgery wait on TKR
© 2010 Blackwell Publishing Ltd 3
comparing WOMAC pain scores for the operated knee 6 monthsafter surgery, no significant differences were seen between the fourgroups of pre-surgery wait [F(3, 136) = 1.88, P = 0.14]. Althoughthis difference was not significant, the group having waited >9months presented the lowest WOMAC pain score [71.1; 95% CI:64.8–77.5] (i.e. higher pain level) compared with the three othersgroups. No significant differences were seen between the fourgroups of pre-surgery wait on the WOMAC function scores for theoperated knee [F(3, 136) = 1.88, P = 0.14]. Although this differ-ence was not significant, again, the group having waited >9 monthspresented the lowest score [65.8; 95% CI: 59.2–72.4] comparedwith the three others groups.
Contralateral knee WOMAC pain scores 6 months
after TKR
Figure 3 presents the adjusted results for the contralateral kneeWOMAC pain score 6 months after TKR by categories of pre-surgery wait. When comparing contralateral knee WOMAC painscores 6 months after surgery, a significant difference was seenbetween the four groups of pre-surgery wait [F(3, 136) = 5.78,
P = 0.0009]. The group having waited >3–6 months presented asignificantly higher contralateral knee WOMAC pain score (i.e.less pain) [86.1; 95% CI: 80.7–91.3] compared with the three othergroups. The group having waited >9 months presented the lowestscore (i.e. worse pain) [86.1; 95% CI: 80.7–91.3] of all groups.
HRQoL SF-36 scores 6 months after TKR
Figure 4 presents the adjusted results for HRQoL SF-36 scores 6months after TKR by categories of pre-surgery wait. Six monthsafter surgery, no significant differences were seen between the fourgroups of pre-surgery wait on SF-36 HRQoL physical functioningscores [F(3, 136) = 2.40, P = 0.07] nor SF-36 HRQoL bodily painscores [F(3, 136) = 0.76, P = 0.52]. When comparing HRQoLSF-36 role physical scores 6 months after surgery, a significantdifference was seen between the four groups of pre-surgery wait[F(3, 136) = 2.74, P = 0.046]. The group having waited >9 monthspresented a significantly lower HRQoL SF-36 role physicalscore [45.2; 95% CI: 35.4–55.0] compared with the three othergroups.
Figure 1 Flowchart of patients’ recruitment.*Eligibility status unknown (considered incalculation of participation proportion). TKR,total knee replacement.
The impacts of pre-surgery wait on TKR F. Desmeules et al.
© 2010 Blackwell Publishing Ltd4
Discussion
Main results
In this prospective cohort study, 141 subjects who underwent TKRwere followed from enrolment on the pre-surgery waiting list until6 months after surgery. The main objective of this study was toassess the effects of pre-surgery waiting time on pain and func-tional limitations related to the knee joint undergoing surgery,HRQoL and contralateral knee pain 6 months after surgery. Sub-jects’ pre-surgery wait was important in our study, averaging six
months. Six months after surgery, subjects presented a significantimprovement in terms of pain and functional limitations relatedto the operated knee and in HRQoL. However, no significantimprovement was seen in contralateral knee pain. Although thedifference was not significant, the group having waited >9 monthstended to have more pain and functional limitations than all theother groups of shorter wait. The group having waited >9 monthspresented a significantly lower and clinically important differencein HRQoL SF-36 role physical score when compared with theother groups of shorter wait. A difference of at least 10 points onthe SF-36 role physical scale is considered clinically important
Table 1 Pre-surgery wait and selected characteristics of the study participants undergoing primary unilateral total knee replacement surgery (n = 141)
Variables n (%) Mean (SD)
Pre-surgery waitTime between enrolment on
waiting list and surgery(days)*
184 (120.8)
Categories of waiting time(months)
�3 30 (21) 62.5 (16.9)>3–6 53 (38) 130.2 (28.7)>6–9 31 (22) 216.8 (25.1)>9 27 (20) 386.3 (56.7)
Surgery postponed for personalreasons
9 (6)
DemographicsAge (years) 66 (9.5)Female 93 (66)Marital status
Single, separated, divorced orwidowed
51 (36)
Married or common law 90 (64)Living alone 34 (24)
Socio-economic characteristicsEducational level (part or
complete)High school or less 79 (56)College or university 62 (44)
Employment statusUnemployed or retired 108 (77)Employed 33 (23)
Household income†
<$30 000/year 48 (34)$30 000–$59 999/year 43 (31)�$60 000/ year 34 (24)
Psychosocial characteristicsPsychological distress (/42) 7.2 (7.0)Social support‡
Low 67 (48)High 74 (52)
Variables n (%) Mean (SD)
Clinical characteristicsDiagnosis
Osteoarthritis 136 (97)Rheumatoid arthritis 5 (3)
BMI (kg m-2) 31.2 (6.2)Comorbidities (/56) 6.5 (2.2)Duration of knee symptoms
before enrolment§ (years)7.9 (8.1)
Contralateral knee pain¶ 101 (72)Use of a walking aid
At enrolment on waiting list 55 (39)6 months after surgery 46 (33)
Surgical characteristicsImplant type
Postero-stabilized 115 (82)Cruciate retaining 26 (18)
Implant fixationCementless 4 (3)Hybrid 2 (1)Cemented 135 (96)
Implant bearing typeMobile 4 (3)Fixed 137 (97)
Patella resurfacing 132 (93)In-hospital complications††
0 109 (77)1 23 (16)�2 10 (7)
Health services utilizationHospital length of stay (days) 7.5 (3.0)Discharge directly home 123 (87)Post-surgery communityphysiotherapy (hours)
14.7 (18.7)
*Median (range): 148 days (32–692).†n = 125 – CND $.‡Social support was dichotomized around the median score: Low (�80) and High (>80).§n = 138.¶WOMAC pain score at enrolment on pre-surgery waiting list dichotomized into presence or absence of contralateral knee pain.††In-hospital complications including: wound infection, dislocation, knee ankylosis and manipulation, cardiovascular/pulmonary/circulatory complica-tions, peripheral/central nervous system involvement, urinary infection, acute confusion, tendon and ligament rupture or blood transfusion.SD, standard deviation; BMI, body mass index; WOMAC, Western Ontario and McMaster Osteoarthritis Index.
F. Desmeules et al. The impacts of pre-surgery wait on TKR
© 2010 Blackwell Publishing Ltd 5

[43]. In terms of contralateral knee pain, the longer waiting timegroup (>9 months) tended to have higher pain levels than all theother groups. When compared with the group having waited >3–6months, the difference was statistically significant and clinicallyimportant. A difference of at least 10 points is considered clinicallyimportant for the WOMAC pain scale [44,45]. The group havingwaited >3–6 months also presented significantly less pain (i.e.higher WOMAC score) when compared with the groups havingwaited �3 or >6–9 months.
Comparison with the literature
This study is, to our knowledge, the first to report a deleteriouseffect of pre-surgery wait on post-surgery outcomes for TKR. One
0
Categories of pre-surgery waiting time≤3 months >3−6 months >6−9 months >9 months
10
20
30
WO
MA
C p
ain
scor
e at
6 m
onth
s po
st-s
urge
ry
40
50
60
70
80
90
100
0
Categories of pre-surgery waiting time≤3 months >3−6 months >6−9 months >9 months
10
20
30
WO
MA
C fu
nctio
n sc
ore
at 6
mon
ths
post
-sur
gery
40
50
60
70
80
90
100
Figure 2 WOMAC pain and function adjusted scores for the operatedknee 6 months after total knee replacement by categories of pre-surgery waiting time. Scores presented as %. Higher scores sign abetter condition. Results are adjusted for initial WOMAC baselinescores at enrolment on the pre-surgery waiting lists. Error barsrepresent 95% confidence intervals. WOMAC, Western Ontario andMcMaster Osteoarthritis Index.
Table 2 Overall changes in WOMAC and SF-36 scores of the study participants between enrolment on the pre-surgery waiting lists and 6 monthsafter TKR (n = 141)
Mean score atenrolment† (SD)
Mean score 6 monthsafter TKR† (SD)
Change inscore‡ (SD) 95% CI
Comparison betweentime points (P-value)
WOMACPain 46.9 (17.9) 77.5 (17.1) 30.6 (21.8) 26.9–34.2 <0.001*Function 46.5 (14.3) 71.9 (17.9) 25.4 (20.5) 22.0–28.8 <0.001*Contralateral knee pain 76.4 (21.2) 77.5 (24.2) 1.1 (22.1) –2.6–4.8 0.56
SF-36Physical functioning 23.4 (17.6) 41.2 (21.7) 17.8 (22.2) 14.1–21.5 <0.001*Role physical 38.7 (25.8) 57.1 (26.1) 18.4 (33.6) 12.8–24.0 <0.001*Bodily pain 27.0 (11.6) 36.4 (11.2) 9.4 (16.1) 6.7–12.1 <0.001*
*P < 0.05.†Scores presented as %. Higher scores sign a better condition.‡Positive changes in score sign an improvement of the condition.TKR, total knee replacement; SD, standard deviation; CI, confidence interval; WOMAC, Western Ontario and McMaster Osteoarthritis Index; SF-36,Medical Outcomes Study 36-Item Short Form Health Survey.
0
P = 0.006∗
P < 0.001∗
P = 0.008∗
≤3 months >3−6 months >6−9 months >9 months
10
Categories of pre-surgery waiting time
20
30
40
50
60
70
Con
tral
ater
al k
nee
WO
MA
C p
ain
scor
e at
6 m
onth
s po
st-s
urge
ry 80
90
100
Figure 3 Contralateral knee WOMAC pain adjusted scores 6 monthsafter total knee replacement by categories of pre-surgery waiting time.Scores presented as %. Higher scores sign a better condition. Resultsare adjusted for initial contralateral knee WOMAC baseline score atenrolment on the pre-surgery waiting lists. Error bars represent 95%confidence intervals. *Significant difference between categories(P < 0.05). WOMAC, Western Ontario and McMaster OsteoarthritisIndex.
The impacts of pre-surgery wait on TKR F. Desmeules et al.
© 2010 Blackwell Publishing Ltd6

Canadian study found a negative non-significant trend, betweenlonger pre-surgery waiting time and worse WOMAC and SF-36scores, one year after total joint replacement (hip or knee).However, in this study, baseline WOMAC and SF-36 were notcollected precisely at enrolment on the pre-surgery list but duringpre-surgery wait, which could have resulted in underestimating the
effects of pre-surgery waiting time [19]. Another Canadian studydid not find any significant association between pre-surgerywaiting times and function at 6 months, but waiting time was quiteshort in this study (mean = 4.5 months) [16,20]. Our results aresimilar in some aspects to the results of these studies, as we didonly see marginal differences between groups of waiting time interms of WOMAC pain and function scores and no significantdifferences in terms HRQoL SF-36 physical functioning andbodily pain scores. A significant difference was, however,observed between groups of waiting time in terms of HRQoLSF-36 role physical, where the group having waited >9 monthspresented the worst score at 6 months when compared with theother groups. Contrary to the WOMAC scales and the SF-36physical functioning scale that focus on pain and function for basicactivities of daily living, the role physical scale relates to difficul-ties (type of activities possible and amount accomplished) withwork or daily activities [28]. This may explain the significantdifference observed for this scale.
In terms of contralateral knee pain, we previously reported astatistically significant and clinically important deterioration whilewaiting for surgery in subjects scheduled for TKR [15]. One veryinteresting finding of this study is that 6 months after surgery, westill observe a significant deleterious effect of pre-surgery wait oncontralateral knee pain and the differences seen here is clinicallyimportant [36,45]. We did not specifically measure functional limi-tations of the contralateral knee because of time constraint, andclearly further research is needed to fully evaluate the effects ofpre-surgery wait on contralateral knee status. But delays forsurgery could have consequences on the outcomes of a subsequentcontralateral TKR, as pre-surgery pain is a strong predictor of painafter surgery [46]. Bilateral involvement is common in osteoarthri-tis and in this cohort, within one year of the initial TKR, as manyas 35 subjects received a contralateral TKR (Desmeules F., unpub-lished results). These results also have important clinical implica-tions regarding the prioritization of patients on waiting lists or foroptimization of conservative treatment while patients wait forsurgery (often called prehabilitation programs), because suchtherapeutic interventions could realistically target both knees tomaximize patients’ status.
Strengths of the study
Strengths of this prospective cohort study include a high partici-pation (81.8%) and follow-up (92%) proportions. There is noindication of a selection bias, as there were no significant differ-ences between participants and eligible non-participants on ageand gender and no significant differences in terms of pain, func-tional limitations and HRQoL at enrolment on the pre-surgerywaiting lists between subjects lost to follow-up, subjects who didnot undergo surgery and participants who completed the interview6 months after surgery (data not shown). Baseline measurementsof the dependent variables were made as soon as the patients wereenrolled on the pre-surgery waiting list (mean � SD: 12.6 � 4.7days) contrary to other studies on waiting times that used face-to-face interviews or postal survey [10]. The study took place in threehospitals of the Quebec city area, where more than half of kneereplacements for this region takes place, and waiting times foundin this study are comparable to pre-surgery waiting times pub-lished for the region [47]. All comparisons were adjusted for
P = 0.006∗
P = 0.06P = 0.03∗
≤3 months >3−6 months >6−9 months >9 months
Categories of pre-surgery waiting time
0
0
0
5
10
15
20
25
30
35
40
45
10
20
30
40
50
60
70
80
HR
QoL
SF-
36 p
hysi
cal f
unct
ionn
ing
scor
eat
6 m
onth
s po
st-s
urge
ryH
RQ
oL S
F-36
rol
e-ph
ysic
al s
core
at 6
mon
ths
post
-sur
gery
HR
QoL
SF-
36 b
odily
pai
n sc
ore
at 6
mon
ths
post
-sur
gery
10
20
30
40
50
60
≤3 months >3−6 months >6−9 months >9 monthsCategories of pre-surgery waiting time
≤3 months >3−6 months >6−9 months >9 months
Categories of pre-surgery waiting time
Figure 4 HRQoL SF-36 physical functioning, role physical and bodilypain adjusted scores 6 months after total knee replacement by catego-ries of pre-surgery waiting time. Scores presented as %. Higher scoressign a better condition. Results are adjusted for initial SF-36 baselinescores at enrolment on the pre-surgery waiting lists. The HRQoL SF-36role physical model scores are also adjusted for age. Error bars repre-sent 95% confidence intervals. *Significant difference between cate-gories (P < 0.05). HRQoL, health-related quality of life; SF-36, MedicalOutcomes Study 36-Item Short Form Health Survey.
F. Desmeules et al. The impacts of pre-surgery wait on TKR
© 2010 Blackwell Publishing Ltd 7

baseline WOMAC and SF-36 scores at enrolment on the pre-surgery waiting lists and further adjustments with other potentialconfounding factors only marginally changed the strength of thepre-surgery waiting time effects and were consequently not kept inthe final models (except for the HRQoL SF-36 role-physicalmodel, which was adjusted for baseline score and age).
Study limitations
The precision of some estimates was low, as shown by the largeconfidence intervals found in the analyses by categories of waitingtime. The use of these categories was based on thresholds oftencited for MAWT, even though it resulted in small count categoriesin our study [23]. Also, although we did find significant differenceson the WOMAC contralateral knee pain and HRQoL role physicalscores, the actual statistical power was not optimal, as final samplesizes of 205 and 325 subjects would have been necessary to obtaina statistical power (1 - b) of 0.80 to detect a minimal clinicallyimportant difference of 10%, assuming a type I error (a) of 0.05,and standard deviations of 23.5 (%) for the WOMAC contralateralknee score and of 25.7 (%) for the SF-36 role physical score,respectively [43–45]. However, other categorizations of waitingtime yielded similar results and did not change our conclusions(data not shown), as was non-parametric modelling (with ranktransformation of the dependent variables).
We did not take into account the wait between the doctor’sreference and the initial orthopaedic consult, because of method-ological difficulties in recruiting patients at that point in time. Wedid, however, retrospectively find that the mean waiting timebetween the doctor’s reference and the initial orthopaedic consultwas 90 days (data not shown). Therefore, we believe the totalcombined waiting time could result in a worse effect on outcomes6 months after TKR. Another limitation of our study was that themain outcome measures were self-reported and we did not includeperformance-based measures. The WOMAC and the SF-36 havebeen found to be valid instruments; still, it has been reported thatperformance-based measures complement self-reported measures[48]. Therefore, the pre-surgery waiting time effect or the strengthof this effect on performance-based measures could be differentfrom the effects observed in our study.
Participants of our study waited for several months with impor-tant pain, functional limitations and impaired HRQoL before TKR.Pre-surgery waiting time had a negative impact on HRQoL andcontralateral knee pain, 6 months after surgery, and this deleteriouseffect could also potentially impact direct and indirect costs. Moreresearch is needed to assess the effects of pre-surgery wait on thesecosts. Actions should be taken to alleviate patient’s burden and tominimize potential deterioration of patients waiting for TKR. Webelieve such actions should include a reduction in waiting time andprioritization of patients. Better conservative management andimplementation of prehabilitation should also be considered.More research is needed to evaluate the full impact of contralateralknee pain in patients waiting for TKR.
AcknowledgementsWe gratefully acknowledge the help of the study participants, thecollaborating orthopaedic departments, Marie-Ève Laflamme andJulie Lapointe, interviewers and Ann Wright, research nurse.
Authors’ contributionsThis paper reports part of the doctoral dissertation in Epidemiol-ogy of FD, realized under the supervision of CED and theco-supervision of RB. FD participated in the design, coordinationand collection of data. He performed the statistical analyses, ledthe interpretation of results and drafted the manuscript. CED par-ticipated in the design, coordination, and interpretation of resultsand writing of the manuscript. EB participated in the design,coordination and writing of the manuscript. RB participated in thedesign and writing of the manuscript. PF participated in the col-lection of data and the writing of the manuscript. All authors readand approved the final version of the paper.
Role of the funding sourceF. Desmeules is supported by a training fellowship from the Cana-dian Institutes of Health Research (CIHR). C.E. Dionne is a seniorQuebec Health Research Fund (FRSQ) scholar. The URESPresearch unit is funded by FRSQ through an infrastructure grant.
Competing interest statementThe authors declare that they have no competing interests.
References1. Forrest, G., Fuchs, M., Gutierrez, A. & Girardy, J. (1998) Factors
affecting length of stay and need for rehabilitation after hip and kneearthroplasty. Journal of Arthroplasty, 13 (2), 186–190.
2. Brady, O. H., Masri, B. A., Garbuz, D. S. & Duncan, C. P. (2000)Rheumatology: 10. Joint replacement of the hip and knee – when torefer and what to expect. Canadian Medical Association Journal, 163(10), 1285–1291.
3. Kurtz, S., Ong, K., Lau, E., Mowat, F. & Halpern, M. (2007) Projec-tions of primary and revision hip and knee arthroplasty in the UnitedStates from 2005 to 2030. Journal of Bone and Joint Surgery. Ameri-can Volume, 89 (4), 780–785.
4. Siciliani, L. & Hurst, J. (2003) Explaining Waiting Times Variationsfor Elective Surgery across OECD Countries. Paris: Organisation forEconomic Co-operation and Development.
5. The Canadian Institute for Health Information (2009) Hip and KneeReplacements in Canada – Canadian Joint Replacement Registry(CJRR) 2008–2009 Annual Report. Ottawa: Canadian Institute forHealth Information.
6. Ackerman, I. N., Graves, S. E., Wicks, I. P., Bennell, K. L. & Osborne,R. H. (2005) Severely compromised quality of life in women and thoseof lower socioeconomic status waiting for joint replacement surgery.Arthritis and Rheumatism, 53 (5), 653–658.
7. Fortin, P. R., Clarke, A. E., Joseph, L., et al. (1999) Outcomes of totalhip and knee replacement: preoperative functional status predicts out-comes at six months after surgery. Arthritis and Rheumatism, 42 (8),1722–1728.
8. Fortin, P. R., Penrod, J. R., Clarke, A. E., et al. (2002) Timing of totaljoint replacement affects clinical outcomes among patients withosteoarthritis of the hip or knee. Arthritis and Rheumatism, 46 (12),3327–3330.
9. Ashworth, A., Brulé, C., Day, A., Harrison, M., Hopman, W. &Rudan, J. (2002) The Development of An Orthopedic Waiting ListAlgorithm for Elective Total Hip and Total Knee ReplacementSurgery. Ottawa: Canadian Health Services Research Foundation. p.44.
The impacts of pre-surgery wait on TKR F. Desmeules et al.
© 2010 Blackwell Publishing Ltd8
10. Hoogeboom, T. J., van den Ende, C. H., van der Sluis, G., et al. (2009)The impact of waiting for total joint replacement on pain and func-tional status: a systematic review. Osteoarthritis and Cartilage, 17(11), 1420–1427.
11. Pace, A., Orpen, N., Doll, H. & Crawfurd, E. J. (2006) Outcomescoring system evaluation of knee osteoarthritis in patients awaitingTKA. Journal of Knee Surgery, 19 (2), 85–88.
12. Ahmad, I. & Konduru, S. (2007) Change in functional status ofpatients whilst awaiting prinmary total knee arthroplasty. Surgeon, 5(5), 266–267.
13. Kapstad, H., Rustoen, T., Hanestad, B. R., Moum, T., Langeland, N. &Stavem, K. (2007) Changes in pain, stiffness and physical function inpatients with osteoarthritis waiting for hip or knee joint replacementsurgery. Osteoarthritis and Cartilage, 15 (7), 837–843.
14. McHugh, G. A., Luker, K. A., Campbell, M., Kay, P. R. & Silman, A.J. (2008) Pain, physical functioning and quality of life of individualsawaiting total joint replacement: a longitudinal study. Journal ofEvaluation in Clinical Practice, 14 (1), 19–26.
15. Desmeules, F., Dionne, C. E., Belzile, E., Bourbonnais, R. & Fremont,P. (2010) The burden of wait for knee replacement surgery: effects onpain, function and health-related quality of life at the time of surgery.Rheumatology, 49 (5), 945–954.
16. Kelly, K. D., Voaklander, D. C., Johnston, D. W., Newman, S. C. &Suarez-Almazor, M. E. (2001) Change in pain and function whilewaiting for major joint arthroplasty. Journal of Arthroplasty, 16 (3),351–359.
17. Hirvonen, J., Blom, M., Tuominen, U., Seitsalo, S., Lehto, M.,Paavolainen, P., Hietaniemi, K., Rissanen, P. & Sintonen, H. (2007)Evaluating waiting time effect on health outcomes at admission: aprospective randomized study on patients with osteoarthritis of theknee joint. Journal of Evaluation in Clinical Practice, 13 (5), 728–733.
18. Vuorenmaa, M., Ylinen, J., Kiviranta, I., Intke, A., Kautiainen, H. J.,Malkia, E. & Hakkinen, A. (2008) Changes in pain and physicalfunction during waiting time and 3 months after knee joint arthro-plasty. Journal of Rehabilitation Medicine, 40 (7), 570–575.
19. Williams, J. I., Llewellyn Thomas, H., Arshinoff, R., Young, N. &Naylor, C. D. (1997) The burden of waiting for hip and knee replace-ments in Ontario. Ontario Hip and Knee Replacement Project Team.Journal of Evaluation in Clinical Practice, 3 (1), 59–68.
20. Jones, C. A., Voaklander, D. C. & Suarez-Alma, M. E. (2003) Deter-minants of function after total knee arthroplasty. Physical Therapy, 83(8), 696–706.
21. Kleinbaum, D. G., Kupper, L. L. & Muller, K. E. (1998) AppliedRegression Analysis and Other Multivariable Methods, 3rd edn,Belmont, CA: Duxbury Press.
22. Masri, B. A., Cochrane, N., Dumbar, M., et al. (2005) Priority Criteriafor Hip and Knee Replacement: Addressing Health Services WaitTimes. Vancouver. Available at: http://www.basmasri.com/ (lastaccessed 10 September 2010).
23. Noseworthy, T., Sanmartin, C., Bohm, E., Conner-Spady, B.,DeCoster, C., Dumbar, M., Lorenzetti, D., McLaren, L. & McGurran,J. (2005) Towards establishing evidence-based benchmarks for accept-able waiting times for joint replacement surgery-Report 2. Calgary:University of Calgary. Report No.: CIHR Request for Application76440.
24. Bellamy, N. & Buchanan, W. W. (1986) Apreliminary evaluation of thedimensionality and clinical importance of pain and disability in osteoar-thritis of the hip and knee. Clinical Rheumatology, 5 (2), 231–241.
25. Bellamy, N., Campbell, J., Hill, J. & Band, P. (2002) A comparativestudy of telephone versus onsite completion of the WOMAC 3.0osteoarthritis index. Journal of Rheumatology, 29 (4), 783–786.
26. McConnell, S., Kolopack, P. & Davis, A. M. (2001) The WesternOntario and McMaster Universities Osteoarthritis Index (WOMAC):
a review of its utility and measurement properties. Arthritis andRheumatism, 45 (5), 453–461.
27. Faucher, M., Poiraudeau, S., Lefevre-Colau, M. M., Rannou, F., Fer-manian, J. & Revel, M. (2004) Assessment of the test-retest reliabilityand construct validity of a modified WOMAC index in knee osteoar-thritis. Joint, Bone, Spine: Revue Du Rhumatisme, 71 (2), 121–127.
28. Ware, J. E. Jr & Sherbourne, C. D. (1992) The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selec-tion. Medical Care, 30 (6), 473–483.
29. Bombardier, C., Melfi, C. A., Paul, J., Green, R., Hawker, G.,Wright, J. & Coyte, P. (1995) Comparison of a generic and a disease-specific measure of pain and physical function after knee replacementsurgery. Medical Care, 33 (4 Suppl.), AS131–AS144.
30. Jones, C. A., Voaklander, D. C., Johnston, D. W. & Suarez-Almazor,M. E. (2000) Health related quality of life outcomes after total hip andknee arthroplasties in a community based population. Journal of Rheu-matology, 27 (7), 1745–1752.
31. Jones, C. A., Voaklander, D. C., Johnston, D. W. & Suarez-Almazor,M. E. (2001) The effect of age on pain, function, and quality of lifeafter total hip and knee arthroplasty. Archives of Internal Medicine,161 (3), 454–460.
32. Keller, S. D., Majkut, T. C., Kosinski, M. & Ware, J. E. Jr (1999)Monitoring health outcomes among patients with arthritis using theSF-36 Health Survey: overview. Medical Care, 37 (5 Suppl), MS1–MS9.
33. Brazier, J. E., Harper, R., Munro, J., Walters, S. J. & Snaith, M. L.(1999) Generic and condition-specific outcome measures for peoplewith osteoarthritis of the knee. Rheumatology, 38 (9), 870–877.
34. Lingard, E. A., Katz, J. N., Wright, E. A. & Sledge, C. B. (2004)Predicting the outcome of total knee arthroplasty. Journal of Bone andJoint Surgery. American Volume, 86-A (10), 2179–2186.
35. Leplege, A., Mesbah, M. & Marquis, P. (1995) [Preliminary analysisof the psychometric properties of the French version of an interna-tional questionnaire measuring the quality of life: the MOS SF-36(version 1.1)]. Revue d’Epidemiologie et de Sante Publique, 43 (4),371–379.
36. Bellamy, N. (2004) WOMAC Osteoarthritis Index, User Guide VII.Brisbane, NSW.
37. Miller, M. D., Paradis, C. F., Houck, P. R., Mazumdar, S., Stack, J. A.,Rifai, A. H., Mulsant, B. & Reynolds, C. F. (1992) Rating chronicmedical illness burden in geropsychiatric practice and research: appli-cation of the Cumulative Illness Rating Scale. Psychiatry Research, 41(3), 237–248.
38. Daveluy, C., Pica, L., Audet, N., Courtemanche, R. & Lapointe, F.(2001) Enquête Sociale Et De Santé 1998, 2e édition. Québec: Institutde la statistique du Québec.
39. Ilfeld, F. W. Jr (1976) Further validation of a psychiatric symptomindex in a normal population. Psychological Reports, 39, 1215–1228.
40. Ware, J. E. Jr, Kosinski, M. & Gandek, B. (2000) SF-36 HealthSurvey: Manual & Interpretation Guide. Lincoln, RI: Quality MetricIncorporated; 1993.
41. Rothman, K. & Greenland, S. (1998) Modern Epidemiology, 2nd edn.Philadelphia, PA: Lippincott Williams & Wilkins.
42. Conover, W. & Iman, R. (1981) Rank transformations as a bridgebetween parametric and nonparametric statistics. The AmericanStatistician, 35 (3), 124–130.
43. Escobar, A., Quintana, J. M., Bilbao, A., Arostegui, I., Lafuente, I. &Vidaurreta, I. (2007) Responsiveness and clinically important differ-ences for the WOMAC and SF-36 after total knee replacement.Osteoarthritis and Cartilage, 15 (3), 273–280.
44. Angst, F., Aeschlimann, A., Michel, B. A. & Stucki, G. (2002)Minimal clinically important rehabilitation effects in patients withosteoarthritis of the lower extremities. Journal of Rheumatology,29 (1), 131–138.
F. Desmeules et al. The impacts of pre-surgery wait on TKR
© 2010 Blackwell Publishing Ltd 9

45. Angst, F., Aeschlimann, A. & Stucki, G. (2001) Smallest detectableand minimal clinically important differences of rehabilitation inter-vention with their implications for required sample sizes usingWOMAC and SF-36 quality of life measurement instruments inpatients with osteoarthritis of the lower extremities. Arthritis andRheumatism, 45 (4), 384–391.
46. Escobar, A., Quintana, J. M., Bilbao, A., Azkarate, J., Guenaga,J. I., Arenaza, J. C. & Gutierrez, L. F. (2007) Effect of patient
characteristics on reported outcomes after total knee replacement.Rheumatology, 46 (1), 112–119.
47. Ministère de la Santé et des Services Sociaux (2006) ATLAS DE LASANTÉ ET DES SERVICES SOCIAUX DU QUÉBEC. Quebec, QC:Ministère de la Santé et des Services Sociaux.
48. Kennedy, D. M., Stratford, P. W., Hanna, S. E., Wessel, J. & Gollish,J. D. (2006) Modeling early recovery of physical function followinghip and knee arthroplasty. BMC Musculoskeletal Disorders, 7, 100.
The impacts of pre-surgery wait on TKR F. Desmeules et al.
© 2010 Blackwell Publishing Ltd10
Related Documents











