θωερτψυιοπασδφγηϕκλζξχϖβνμθωερτψυι οπασδφγηϕκλζξχϖβνμθωερτψυιοπασδφγη ϕκλζξχϖβνμθωερτψυιοπασδφγηϕκλζξχϖβ νμθωερτψυιοπασδφγηϕκλζξχϖβνμθωερτψ υιοπασδφγηϕκλζξχϖβνθωερτψυιοπασδφ γηϕκτψυιοπασδφγηϕκλζξχϖβνθωερτψυι οπασδφγηϕκλζξχϖβνθωερτψυιοπασδφγη ϕκλζξχϖβνμθωερτψυιοπασδφγηϕκλζξχϖβ νμθωερτψυιοπασδφγηϕκλζξχϖβνμθωερτψ υιοπασδφγηϕκλζξχϖβνμθωερτψυιοπασδφ γηϕκλζξχϖβνμθωερτψυιοπασδφγηϕκλζξχ ϖβνμθωερτψυιοπασδφγηϕκλζξχϖβνμθωε ρτψυιοπασδφγηϕκλζξχϖβνμρτψυιοπασδφ γηϕκλζξχϖβνμθωερτψυιοπασδφγηϕκλζξχ ϖβνμθωερτψυιοπασδφγηϕκλζξχϖβνμθωε ρτψυιοπασδφγηϕκλζξχϖβνμθωερτψυιοπα σδφγηϕκλζξχϖβνμθωερτψυιοπασδφγηϕκλ ζξχϖβνμθωερτψυιοπασδφγηϕκλζξχϖβνμθ ωερτψυιοπασδφγηϕκλζξχϖβνμθωερτψ222 2υιοπασδφγηϕκλζξχϖβνμθωερτψυιοπασδ φγηϕκλζξχϖβνμθωερτψυιοπασδφγηϕκλζξ χϖβνμθωερτψυιοπασδφγηϕκλζξχϖβνμθω ερτψυιοπασδφγηϕκλζξχϖβνμρτψυιοπασδ The Impact of the 1918 Spanish Influenza Pandemic on Greater Syria MA Dissertation School of Oriental and African Studies Kjell Jostein Langfeldt Lind 2012

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
θωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµρτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψ2222υιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµθωερτψυιοπασδφγηϕκλζξχϖβνµρτψυιοπασδ
The Impact of the 1918 Spanish Influenza Pandemic on Greater Syria
MA Dissertation
School of Oriental and African Studies
Kjell Jostein Langfeldt Lind
2012
Title of dissertation: The Impact of the 1918 Spanish Influenza Pandemic on Greater Syria Name of student: Kjell Jostein Langfeldt Lind Student ID: 246272 Degree: MA Israeli Studies – School of Oriental and African Studies Date of submission: September 17 2012 Word count: 9.991

Abstract The 1918 Spanish influenza pandemic was the single worst demographic disaster of the 20th century. The attack by non-‐human agents came at a crucial time of historic transition with the military surrender and subsequent collapse of the Ottoman Empire. Yet, astonishingly little research exists on this demographic disaster on the Middle East. This dissertation zooms in on the area of Greater Syria at the time of the lethal second wave of the pandemic at the end of the First World War. It follows the geographic course of the virus into the area and presents evidence for mortality among combatants and civilians. Despite the paucity of textual references to the pandemic, mortality in the civilian population could have been substantial but obscured by the composite crisis of war and ignored by historiography as a discrete event.
Table of Contents
INTRODUCTION 2
THE GEOGRAPHIC COURSE OF THE SECOND WAVE OF SPANISH INFLUENZA INTO GREATER SYRIA 5
THE IMPACT ON COMBATANTS 11
THE IMPACT ON CIVILIANS 17
The silence of the sources 22
The question of mortality 26
THE INTERACTION OF PATHOGENS: INFLUENZA AND MALARIA 29
CONCLUSION 32
APPENDIX 34
The prevalence of malaria in Greater Syria 34
The question of acquired immunity and the uneven distribution of death 35
WORKS CITED 38 Map Figure 1:The geography of the second influenza wave in Greater Syria 10
2
Introduction Global mortality estimates for the 1918 Spanish influenza pandemic vary widely, from
30 million to 100 million. Regardless of the actual figure, it “was the single worst
demographic disaster of the 20th century” (Killingray & Phillips, 2003:3-‐4). In terms of
absolute numbers, it may have been the greatest single demographic shock that the
human species has ever received (Crosby, 1993:810). Bearing in mind this global havoc,
this dissertation poses a question rarely asked before: what was the impact of the 1918
Spanish influenza pandemic, in terms of mortality, on Greater Syria?1 The Middle East is
a region of the world where the absence of studies on the pandemic is very noticeable
(Killingray & Phillips, 2003:24)2. In the spirit of William McNeill´s Plagues and Peoples,
which sought to bring “the role of infectious disease in shaping human history into a
juster perspective” (McNeill, 1979:205), this study will attempt to cover some of this gap
in historical knowledge.
1 In terms of contemporary political units the name Greater Syria comprises all of four states – Syria, Jordan, Israel and Lebanon – as well as the Palestinian territories of the West Bank, the Gaza Strip as well as portions of southeastern Turkey (Pipes, 1990:14). 2 Only three academic articles exist on the subject of Spanish influenza in the Middle East. Amir Afkhami (2003), a medical doctor with a PhD in history, writes about the impact of Spanish flu in Iran. His article, based on his PhD thesis, was published in the Bulletin of the History of Medicine. Guido Steinberg, a German Arabist, has written two very similar articles on the impact and collective memory of the Spanish influenza in Syria and the Arabian Peninsula. The first (2002) is available to readers of German, the second in English. The latter article, more academically tweaked, was published as a chapter in the book The First World War as Remembered in the Countries of the Eastern Mediterranean (2006). Steinberg gives little textual evidence for the impact on Greater Syria but provides ample evidence for high mortality in the Arabian Peninsula. Professor G Dennis Shanks, a retired US Army Medical Corps Officer and an expert on malaria and pandemic influenza in military populations, has written an article (2009) on the interaction between influenza and malaria in the Australian Army in Palestine in 1918. I engage with all the mentioned articles in this dissertation. For books on the burden of infectious diseases and the medical response by the EEF and the Yildirim, see Dolev (2007) and Özdemir (2008). For general literature on the 1918 influenza pandemic there is more to choose from. A standard work for any self-‐respecting student of Spanish flu is Alfred W. Crosby´s America´s Forgotten Pandemic: The Influenza of 1918 (2003) – originally published in 1976. The layman reader who wishes to gain more epidemiological understanding with respect to the etiology of influenza and the dynamic life of the virus, a subject which is beyond the scope of this 10.000 word dissertation, Tom Quinn´s first chapter in Flu: A Social History of Influenza (2008) will be a good read. For a general and comprehensive overview of the global pandemic, the introductory chapter in The Spanish Influenza Pandemic of 1918-‐1919: New Perspectives (2003), written by the editors David Killingray and Howard Phillips, is highly recommended.
3
Humans are not the only agents that shape human history. In all the major wars of the
18th and 19th centuries, disease claimed far more lives than injuries in battle: the First
World War was the first major conflict in which this ratio was reversed and in which
deaths from battle injuries exceeded those from disease (Harrison, 2004:146). Yet, the
protagonists of the history of the nation and modernity are all human: human beings are
the agents around whose actions and intentions the story is written (Mitchell, 2002:29).
The anthropocentric omission of non-‐human agents of history fails to capture the
historical narrative in all its dimensions. Before humans are Arab nationalists,
Palestinians or Zionists, they are biological entities interconnected in a biological world
in which humans are predators as well as prey. Demographic disasters have numerous
implications for societies. As a demographic phenomenon, an epidemic is about more
than the people who die. It is also about the people left behind. The death of a
breadwinner will have direct consequences for survivors. On an individual and
collective social level, epidemics can have a profound psychological and economic
impact. The study of infectious diseases, therefore, goes beyond the history of medicine3.
An epidemic can be an earth shattering historical event. Studying a society´s response to
it offers the historian an illuminating window of insight into other aspects of society
which otherwise may be less evident. Faced with an existential situation in extremis,
every layer of society is mobilized looking for explanations and frequently for
scapegoats. Epidemics stress test the social fabric of a society, the quality and efficiency
of the state apparatus and its medical response. The success or failure of a collective
response offers valuable lessons for posterity and contemporary policy-‐makers. Here
the historian can help cast light on errors made in the past. Epidemics of disease can
have far-‐reaching and profound political, intellectual and cultural effects. An epidemic 3 For perceptions and responses to plague and pestilence and how epidemics of infectious diseases affect social and political change, see The Burdens of Disease (Hays, 1998).
4
may on occasion set its stamp on the “optimism” and “pessimism” of an entire age (Hays,
1998:2). The focus of this dissertation, however, is bound to be a narrow one. The
imposed limitation on its extent combined with the fact that there is no beaten track to
follow, command this study to direct its attention to the narrow question of mortality,
the most obvious of impacts.
The first chapter will track the geographic course of the second wave of the pandemic
into the Middle East and its assumed route through Palestine and Syria4. The second
chapter will present textual evidence for high morbidity and mortality among
combatants, from Medina to Aleppo. The third chapter explores the impact of the
influenza pandemic on the civilian population of Greater Syria. I will offer an explanation
for the paucity of anecdotal references to it. The silence of the sources, I argue, could be
deceptive. The fourth and final chapter will explain why mortality in the civilian
population could have been substantial. Here I lean on the shoulders of Dennis Shanks
(2009) and Amir Afkhami (2003), both medically trained historians, who point out the
interaction between malaria and influenza. As an epidemiologically informed student of
Spanish influenza I will apply their conclusions to my subject of investigation5.
4 The Spanish influenza pandemic came in 3-‐4 waves during 1918 to 1920. The second wave in the fall of 1918, the focus of this dissertation, was by far the most virulent. "Spanish influenza" is a misnomer. The influenza pandemic did not originate in Spain, but as a non-‐belligerent in the war with no censorship, reported extensively on the influenza and the name stuck. (Noymer, 2010:140). 5 The epidemiologically curious reader is also encouraged to read the section included in the appendix. In addition to providing evidence for the prevalence of endemic malaria in Greater Syria, it contemplates the possibility of an unequal distribution of mortality among the various communities.
5
The geographic course of the second wave of Spanish influenza into Greater Syria Following its appearance in the United States in early 19186, the first wave of Spanish
influenza rounded the globe in four months (Crosby, 2003:28). In the latter part of
August 1918, the virus mutated, possibly in France (Harrison, 2004:150), and initiated
the second wave of the global pandemic with unprecedented virulence. This firestorm of
influenza, which would kill millions, swept throughout the countries of the
Mediterranean in early September 1918. This mutated and virulent virus presumably
embarked on a ship in France or Britain and disembarked in the Egyptian port of
Alexandria primo September. The massive movement of troops in a world at war
assisted the rapid spread of the infection. The Suez Canal was a strategic point of transit
for the diffusion of the virus eastwards to India and Mesopotamia. Throughout the war,
troop ships from Port Said and Alexandria were shuttling between Egypt and India.
Between 1914 and 1919, India sent over 1.8 million combatants and non-‐combatants
overseas to serve imperial Britain in various theatres. Over 95.000 combatants and
350.000 non-‐combatants served in Egypt and Palestine (Kitchen, 2011:165)7. These
numbers give some indication of the intense maritime traffic through the Suez Canal and
the easy transmission of a highly contagious disease. The spring wave of the influenza
pandemic reached Bombay on May 29 while the second wave hit Bombay “as the
principal port of entry for military and passenger traffic” around September 10
(Phipson, 1920). Non-‐stop voyage time between Suez and Bombay (a distance of 2.960
6 Epidemiological evidence suggests that the new influenza virus originated in Haskell County, Kansas, early in 1918 (Barry, 2009:92). 7 By the time the campaign ended in Palestine in October 1918, the majority of the Egyptian Expeditionary Force (EEF), was made up of units drawn from the Indian Army. Of its eleven divisions, only two, the 54th (East Anglia) and the Australian and New Zealand Mounted Divisions (ANZAC), contained no Indian troops (Kitchen, 2011:165).
6
nautical miles) would be about 9 days for a passenger ship and 12 days for a cargo ship8.
Given that the second wave was reported in Bombay around September 10, it can be
inferred that the approximate date of debarkation of the influenza virus in Egypt was
early September. The seaport of Jaffa was the port of entry for British ships at the time of
the second offensive launched on September 19 1918. Jaffa was in all likelihood the first
point of entry for the virus on the Levantine coast, carried by British ships from
Alexandria or Port Said. The earliest textual evidence for Spanish influenza in the Levant
is from Jerusalem. On September 15 the diary of the Spanish consul of Jerusalem, Conde
de Ballobar, notes the appearance of the (“badly named”) Spanish influenza (Ballobar,
2011:210).
Colonel Cathcart Garner (Garner, 1921:75-‐83) provides us with a detailed account of the
itinerary of the influenza virus and its dissemination in Egypt9. He is, unfortunately,
silent on its course and impact in the Levant10. According to Garner, Spanish influenza
was introduced by sea from Europe. The fact that the first cases occurred among
military personnel “was only natural, as the communication between Europe and Egypt
at the time was practically entirely in the nature of military movement”. It was prevalent
“to a considerable extent in the Egyptian Expeditionary Force both in Egypt and
Palestine, before it manifested itself to any extent in the civilian population in Egypt”.
8 Personal communication with author Gordon Smith, an authority on naval history and operator of the online site "naval-‐history.net". According to Smith, voyage time between Suez and Aden would be about 4 days (minimum 12 hours at maximum speed of 7.5 knots through the Suez canal). The voyage between Aden and Bombay would take about 6 days. Cargo ships would travel at the approximate speed of 10 knots and passenger ships could do 18 knots. 9 Colonel Cathcart Garner, who in the memoirs of Sir Ronald Storrs is described as an “insistent Irishman” (Storrs, 1972:300), was the Principal Medical Officer of the Occupied Enemy Territory Administration (OETA). Colonel Garner was also the Director-‐General of the Public Health Administration in Egypt. 10 According to another medical report, On the Influenza Epidemic in Egypt (McWalter, 1919), “the amazing thing about the epidemic of influenza – as it appeared in troops who had been through Palestine – as well as in native Egyptians – was that it seemed to have the same clinical course, and the same results, as influenza at home, or in any other part of the world”.
7
Communication between military personnel and the native population of Egypt was
rendered very free by the existence of a Labour Corps of Egyptian fellaḥīn, “of
considerable strength recruited on a six months’ basis”11. Garner points out the two
distinct waves of influenza. The first reports were from Alexandria in May 1918. The
second and considerably more lethal wave of influenza came in September. From
September, and still continuing at the end of December, the disease showed a rising rate
of pulmonary complications and death. In October the influenza epidemic spread quickly
over the whole of Egypt and the frequency of pulmonary complication and the death
rate increased rapidly. By November 1918, influenza had “penetrated into every nook
and corner of the country”. It reached its zenith in the first week of December before it
declined.
Improved lines of communication facilitated the dissemination of the influenza virus.
From Egypt the virus traveled overland across the Sinai Peninsula. The virus also
traveled by sea. By mid and late October 1918, British ships were shuttling between
Alexandria, Port Said, Haifa, Beirut and Tripoli. The speed of the military operation and
the consequent problem of the rapid lengthening of the line of evacuation was reduced
by the capture of Haifa and the opening of a casualty clearing station from which
medical cases could be dispatched by hospital ships directly to Alexandria (Kay,
1919:104). The opening of new channels of supply through the port cities of the
Levantine coast simplified logistical operations and drastically cut down the travel time
of transport of goods and personnel. Indeed, ordnance stores, which had previously
been collected in Palestine, were sent all the way down again across the Sinai Peninsula
to Qantara for reshipment to the port cities (Kay, 1919:103). Furthermore, by October 11 According to A Brief Record of the Advance of the Egyptian Expeditionary Force (1919), by November 1918 the Egyptian Labour Corps numbered 100.002 men and 504 officers (Kay, 1919:108).
8
1918 overland lines of communication had been improved by a broad gauge, double-‐
track railway built by the Egyptian Labour Corps. This railway stretched across the Sinai
Peninsula running from the Egyptian town of Qantara on the Suez to Rafah on the
Palestine border through Gaza. From thereon a single-‐track railway proceeded to
Beersheba, Lydda and Jerusalem. A single-‐track, narrow gauge railway track connected
Jaffa, Nablus and Haifa12.
This study has failed to find textual evidence for the impact of the first wave of Spanish
influenza. It can merely be presumed that the Egyptian Expeditionary Corps (EEF)
would have disseminated this more mellow viral strain into its occupied area. The
northern boundary between the Occupied Enemy Territory Administration (OETA
South) and the Ottoman Yildirim zone ran from a little north of Jaffa through Ramallah
to Jericho (Storrs, 1937:342). Ottoman troops may have carried the virus into the
Yildirim zone. It cannot be ruled out that Ottoman troops and their German allies were
complicit in the spread of Spanish influenza also in its second wave. If so, the population
of Greater Syria may have been caught in the midst of a contagious wildfire from two
directions. During both the spring and fall waves, German reinforcements from Central
Europe as well as Ottoman troops could be brought from Constantinople by train to
Anatolia. However, uncompleted gaps in railroad interconnectability at Pozanti through
the Taurus Mountains and at Osmaniye through the Manus Mountains particularly
affected transportation going to Mesopotamia and Syria, since all cargo had to be
transloaded through the mountains. These choke points afflicted the entire Ottoman war
effort until the very last days of the war and greatly impeded military operations in both
Palestine and Mesopotamia (Erickson, 2000:18-‐19). “The grim condition of the 12 Source: Map: “Lines of Communications October 1918”, Survey of Egypt, Dec 1918, in Allenby´s Military Medicine (Dolev, 2007:171).
9
transportation facilities available to the wartime Ottoman army” meant that soldiers had
to pass through the Gülek Pass in the Taurus Mountains on foot in order to reach Syrian
territories (Özdemir, 2008:29). From Aleppo a continuation of the railway connected
Hama, Homs, Tripoli as well as Damascus. The failure to complete the railway
connection between Anatolia, Greater Syria and Mesopotamia, meant that Ottoman
soldiers had to walk on foot through challenging topography between the gaps in
railway lines. All Ottoman troops deployed to the Mesopotamian front could reach that
region only after a two-‐month walk (Özdemir, 2008:30). The slow movement of the
Ottoman Army contrasts with the efficient logistical infrastructure constructed by the
Egyptian Labour Corps. The British naval blockade of the Levantine coast ensured that
neither goods nor personnel could be brought into the Yildirim zone by Ottoman or
German ships. Bearing in mind the established maritime lines connecting Egypt with the
Levantine coast, it seems fairly safe to assume, supported by Colonel Garner´s medical
report, that the culprits in the transmission of the mutated virus were the men of the
EEF.
After General Allenby marched through Jaffa Gate in Jerusalem on December 11 191713
military operations came more or less to a halt and remained so for almost a year. On
September 19 1918, Allenby, who had assumed command of the EEF at the end of June
1917 (Mortlock, 2010:101), moved northwards once more in a final offensive. By this
time the new and significantly more virulent strain of the influenza A virus in this
second wave of the pandemic had taken a firm hold on the men of the EEF. The influenza
13 A recurrent theme in the literature on this event is the story of the multiple surrender of Jerusalem starring its mayor Hussein Al-‐Husseini who supposedly died from pneumonia ”early in 1918” (Storrs, 1972:337). Whatever he died from, the Spanish influenza virus can safely be exculpated. The first wave of the pandemic arrived no earlier than May-‐June in Palestine, too late to kill the Arab mayor.
10
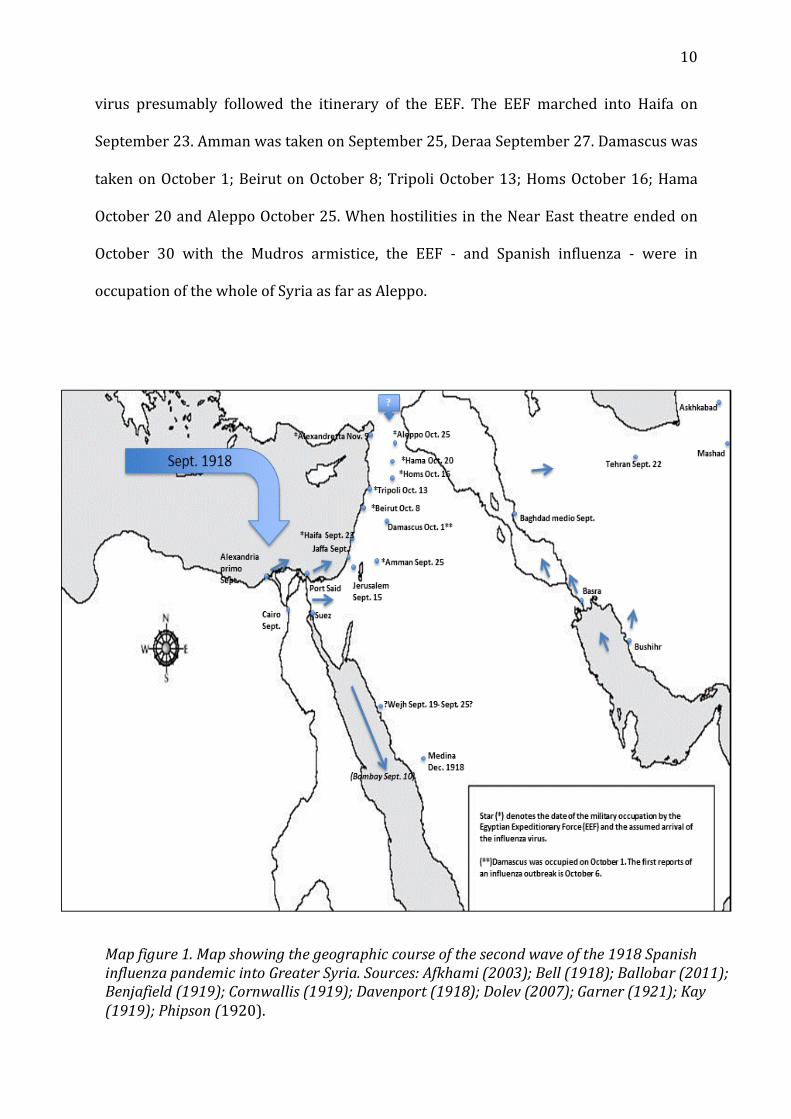
virus presumably followed the itinerary of the EEF. The EEF marched into Haifa on
September 23. Amman was taken on September 25, Deraa September 27. Damascus was
taken on October 1; Beirut on October 8; Tripoli October 13; Homs October 16; Hama
October 20 and Aleppo October 25. When hostilities in the Near East theatre ended on
October 30 with the Mudros armistice, the EEF -‐ and Spanish influenza -‐ were in
occupation of the whole of Syria as far as Aleppo.
Map figure 1. Map showing the geographic course of the second wave of the 1918 Spanish influenza pandemic into Greater Syria. Sources: Afkhami (2003); Bell (1918); Ballobar (2011); Benjafield (1919); Cornwallis (1919); Davenport (1918); Dolev (2007); Garner (1921); Kay (1919); Phipson (1920).
11
The impact on combatants I have established that Spanish influenza was present in Palestine no later than by
medio September 1918. By early October influenza was raging in Syria. A Sergeant-‐
Major of the 3rd Battalion of the Australian Infantry Brigade retrospectively made the
following observation on his participation in Allenby´s dash to Damascus: “Where the
divisions had been spared the ravages of shell and machine gun fire during the advance,
they were destined to have their ranks decimated by the influenza epidemic that swept
over the whole of Syria early in October. Men died like flies. In some of the Australian
regiments there were three and four horses to every trooper" (Goldenstedt, 1931). The
EEF marched into the Syrian capital on October 1. Spanish flu arrived in Damascus on
October 6 (Dolev, 2007:167). The Australian military historian Henry Gullet (1941:773-‐
775) describes the impact on the Syrian capital from a lethal cocktail of infectious
diseases, among which influenza was a primary ingredient. As the operations about the
town ceased, the sickness spread with ominous rapidity; within a few days more than
half the men of many regiments were on their backs. “The scourge of pneumonic
influenza, which was raging in many parts of the world, was at that time sweeping
through the Near East, and assailed the spent troops in a virulent form”. Already all the
buildings in the city were overflowing with sick Turks; British medical supplies were
slow in reaching Damascus and the nearest casualty clearing station was at Kuneitra, 65
kilometers away. “The Turks in the main hospital died at the rate of 70 or 80 a day, and
were buried by their fellow countrymen in a great continuous trench. Of about 20.000
Turkish prisoners of war, 3.000-‐4.000 died from diseases”. Ottoman soldiers were not
the only to suffer. Spanish influenza in Damascus, accompanied by malaria, put nearly
half the Desert Mounted Corps of the Australian and New Zealand Army Corps (ANZAC)
out of action. From the week ending on October 5 to the end of the following week,
12
admissions to hospital from the Desert Mounted Corps more than doubled, from 1.246
to 3.109. Nearly four times the number of horsemen died in the cramped, unhealthy
dormitories of Damascus as had been killed on the advance. Sanitation was lacking in
the hospitals and “rats gorged on corpses putrefying alongside the living” (Hamilton,
2002:139). In the next stage, after the fall of Damascus and the advance towards Aleppo
(taken on October 25), soldiers of the EEF continued to suffer from simultaneous
outbreaks of malaria and influenza. The 5th Cavalry Division commanded by Major
General MacAndrew, himself "much reduced by sickness" had to make the advance to
Aleppo unsupported (except for by an Arab force) as "malaria and influenza had by now
quite immobilized the 5th Cavalry Division” (Wavell, 1941:231).
ANZAC also suffered in the southern area of operations. During October and November,
the 13.000 men under Brig. General Chaytor´s command, who included the 38th and
39th Royal Fusiliers battalions of Jewish volunteers, lost 8.352 to malignant malaria -‐
“and maybe also to Spanish flu” (Dolev, 2007:170). After its swift raid from the Jordan
valley to Amman, Chaytor´s force was withdrawn to Jerusalem and Bethlehem. Like the
divisions in the north, they suffered severely from disease. "The fighting around Amman
was scarcely over before malaria, pneumonic influenza, and other maladies ran like fire
through the ranks. Indians, British West Indians, and Jews shared in the suffering which
followed” (Gullet, 1941:780). As in Damascus, Chaytor´s Force may very well have
experienced simultaneous epidemics of falciparum malaria and influenza.
13
Combatants of the Jewish Legions almost certainly fell victims to Spanish influenza14.
The Jewish soldiers that saw action in the Palestinian theatre suffered
disproportionately to their modest contribution on the battlefield. Their casualties are
usually reported as due to malaria. It is highly likely that the flu virus interacted with the
malaria parasite. The 38th Battalion spent the summer of 1918 in the sweltering heat of
the highly malarious Jordan Valley. It finished its participation in the war with a minor
reconnaissance mission within the framework of the Battle of Armageddon on
September 20, in which four of its soldiers were killed in action (Neumann, 1993:296).
Thereafter, the battalion was tasked to march prisoners of war to Jerusalem during
which 80% of its troops fell ill and the number who died from it vastly outnumbered
those killed by enemy fire (Neumann, 1993:297). In early October, the 39th battalion,
tasked with a similar escort mission of Ottoman and German prisoners of war, also lost
most of its people to “malaria” (Neumann, 1993:299)15.
In Beirut Ottoman troops as well as soldiers of the EEF were sick and dying with
influenza. Lt. Wilson, a British officer with the Desert Mounted Corps, collapsed in early
October in Baalbeck during the pursuit to Aleppo and was subsequently hospitalized in
Beirut. On October 18, while waiting for a hospital ship to Alexandria, he wrote to his
mother that he was down “with a touch of Spanish flu” (Wilson, 1987:151). The young
British lieutenant sweated it out and survived, like most people did. But many did not.
14 The Jewish Legions consisted of four battalions and 7.000 men. Three battalions were formed as part of the Royal Fusiliers: the 38th Battalion composed of English Jews, the 39th Battalion, composed mainly of Jews from North America and Argentina and the 40th Battalion, recruited in the summer of 1918 from the Palestinian Yishuv. An additional 42nd Battalion was a battalion stationed in Plymouth, UK (Keren & Keren, 2010:5) 15 The Jewish Legions suffered casualties from Spanish flu also in Europe while waiting to be dispatched to the front in Palestine. On November 3 1918 an unknown Jewish recruit to the 38th Battalion of the Royal Fusiliers waiting to be shipped to the front in Palestine, noted in his diary from London that a fellow soldier had died of Spanish flu in the hospital and expressed his hope that "before we go to war an armistice will be signed, because the newspapers are full of this" (Keren & Keren, 2010:37).
14
More than half of the 17 soldiers of the German Asia Corps buried in the Protestant
cemetery in Beirut, died during the period between December 1918 and January 1919,
when the war was over but influenza still raging (Steinberg, 2006:160). Soldiers of the
German Asia Corps of the Yildirim Army Groups may have been sick and dying of
influenza also after their evacuation from Greater Syria. Otto Liman von Sanders´ Fünf
Jahre Türkei (1919) makes no explicit mention of influenza. However, he does briefly
mention that around mid November 1918 German troops upon their defeat in Palestine
and their arrival in Constantinople, suffered 80 deaths in four weeks due to what he
thought to be Erkältungskrankheiten -‐ common cold16. The large German staging
hospital in the Haidar Pasha neighborhood of the city was severely overcrowded with
1.200 sick men (Von Sanders, 1919:409)17.
By December 1918 Spanish flu had penetrated the interior of the Arab Peninsula18. On
January 9 1919 commander Fakhri Pasha, who had refused to surrender his Medina
garrison even after the Mudros armistice on October 30, finally capitulated (Murphy,
2008:81). But it was not human agency that forced the Ottoman soldiers to lay down
their arms. It was Spanish influenza. An intelligence report by Kinahan Cornwallis,
deputy director of the Arab Bureau and Gilbert Clayton´s next in command (Cornwallis,
1919), describes the impact of Spanish flu on the Ottoman Hejaz Expeditionary Force
16 Von Sanders himself had been recalled to Constantinople after the Mudros armistice on October 30 (Erickson, 2002:201). General von Sanders had replaced Erich von Falkenhayn as the commander of the Ottoman Empire´s Yildirim´s Army Group in wake of the military conquests of General Allenby in late 1917. 17 Little is known about the course and impact of Spanish flu on Constantinople, but according to one source, the spread was controlled very effectively. Cases of influenza occasionally appeared in Constantinople but was spared the terrible impact suffered by many other world cities (Criss, 1999:156). 18 An intelligence report sent to the Arab Bureau by Major Davenport, a British officer attached to the Arab Army and who commanded a detachment of troops in the Hejaz, might be evidence for an outbreak of Spanish influenza in the Arab Army and the Arabian Peninsula already in late September 1918. Major Davenport, writing from Wejh, a port on the Red Sea, writes: "Owing to the plague which most unhappily has fallen like a scourge on the town of Wejh…I am not allowed to move for fear of spreading the infection” (Davenport, 1918). That infection may have been Spanish influenza.
15
(HEF). During questioning a medical officer of the HEF revealed that in June 1918 “fever
was unusually violent”. This statement possibly refers to the spring wave of the
influenza pandemic. In December 1918 Spanish flu suddenly broke out “in a virulent
form”. Out of 11.000 men, 850 died in December 1918. Nearly 450 men died in January
1919. No unit was free from influenza and Fakhri himself had a sharp attack. A Turkish
officer by the name of Emin Bey “gave the total daily loss from it as 150, and computed
that the whole HEF would be decimated by it in two months”. After the surrender and
the subsequent evacuation of 8.000 men to Egypt by the EEF, “another 100 succumbed
while en route for the coast, while 300 have remained in hospital in Medina” including
“many Syrians and Baghdadis”19. Captain Herbert Garland reported that in the first
batch of Ottoman soldiers who reached Bir Derwish (a transit point en route to the coast
located 40 kilometers south-‐west of Medina), “many could hardly walk”.
As we have seen, Spanish influenza struck combatants on both sides in the theatre, from
Medina in the south, to Aleppo in the north. In Europe General Ludendorff blamed the
failure of the German military offensive in the spring of 1918 on influenza (Storey,
2010:147). Was the influenza virus the most formidable general on the battlefield in
Greater Syria and the ally of the EEF? With the exception of the battle of the Medina
garrison, the Spanish influenza was possibly irrelevant to the final outcome of the battle.
From the perspective of the EEF, it was fortunate that victory was swift, as twin
epidemics of falciparum malaria and pandemic influenza ended most military
19 For more insight into the role of Arabs in the Ottoman Army, see Salim Tamari (2007). The majority of Arabs did in fact remain faithful to the Ottoman Empire and did not fight under the banner of the Arab Revolt. Lloyd George retrospectively commented that the Balfour Declaration did not seem to give the Arabs “much anxiety” and added: “We could not get in touch with the Palestinian Arabs as they were fighting against us” (Cited in Fromkin, 2009:297). Lloyd George´s caustic remark was perhaps not entirely off the tangent. Adding a further ironic dimension to the ethnic composition of the warring armies, 29 % of Allenby´s new infantry in the September 1918 offensive were actually Muslim Indians (Kitchen, 2011:175).

16
operations (Shanks, 2009:654). Allenby´s blitzkrieg was in effect over before the full
impact of the epidemic descended upon the combatants20.
20 See the appendix for a discussion of the possibility of an uneven distribution of mortality.
17
The impact on civilians
I have established that Spanish influenza killed combatants in the Syrian and Palestinian
theatre. Textual evidence for mortality in the civilian population is much sparser. The
diary of the Spanish consul of Jerusalem, Conde de Ballobar, the only diary produced by
a western resident of Jerusalem during the First World War (Ballobar, 2011:23),
confirms that influenza was raging in Jerusalem by mid September 1918. In an entry
dated September 15 the Spanish consul writes: "Here we have returned to the heat, and
what is worse to the illnesses, since beside the flu, badly named ´Spanish´, we now have
no less than the pernicious malaria. Because of this disease a poor Christian girl, whom I
met in the bank, has died, and she lasted no more than six hours” (Ballobar, 2011:210).
The “badly-‐named” influenza was taking lives in Jerusalem also in early November. In an
entry dated November 6 Ballobar again briefly mentions the influenza pandemic: “There
are so many cases of pneumonia lately. The sadly famous flu transforms into pneumonia,
and in three days one is making the trip to the next world. Mrs. Bandakech died of it and,
yesterday, a girl only 20 years old. They say the latter got a temperature of 43 ℃. She
died, so to say, all burned up” (Ballobar, 2011:227).
What was the situation elsewhere in Greater Syria at the time of the dissemination of
Spanish influenza into the civilian population? On October 14 General Clayton21
reported that the general situation in the newly occupied territory was “satisfactory”,
and that 13.000 refugees had returned to Gaza, and over 4.000 to Jaffa (Ormsby-‐Gore,
1918). However, I cannot but conclude that the situational understanding of his
intelligence service must have been poor. According to Dr. Fritz Grobba of the Weimar
21 Major-‐General Clayton was the Chief political Officer of the OETA (Storrs, 1937:342). He also created the Arab Intelligence Bureau in Cairo (Jacobson, 2006:200).
18
Foreign Ministry, the winter and famine of 1917-‐1918 had been very severe in Beirut
and Lebanon. The scenes in the streets were heartbreaking. In March 1918 the German
consulate in Aleppo estimated the daily number of dead from hunger to be 100, mostly
Armenian refugees. The Christian communities and the "Israelites" [sic] were able to
protect their poor from the worst of the hunger (Grobba, 1923:82-‐83). In Damascus,
after the entry of the EEF and the Arab Army, the condition is described as “deplorable”;
only the highly dangerous cases of disease could be admitted, and the crowded wards
were lamentably short of doctors, trained orderlies and rugs: “The hopeless Arab
Administration was indifferent to human suffering” (Gullet, 1941, 773-‐775). In Tiberias
children who had got separated from their parents or were orphaned roamed the streets
hungry (Baratz, 1954:87-‐88). The population of Lebanon, “where the Turkish
authorities had followed a policy of discrimination in the distribution of food as a
reprisal for the sympathies of the population with the Allies” (Hourani, 1968:49), may
have been particularly vulnerable to influenza. Along the route of the advancing EEF,
“inhabitants of tiny villages in Lebanon gathered by the roadside to beg for food” (Bluett,
1919:279). “You could ride through village after village without seeing a soul” (Bluett,
1919:283)22.
According to Adolf Böhm, the population of the British occupied territories of Palestine
was by the fall of 1918 sufficiently provisioned, whereas the situation in the Yildirim-‐
zone was getting worse by everyday. In Tiberias and Safed “hunger, typhus und andere
Seuchen [and other epidemics] raged among the population and refugees, and took
many lives” (Böhm 1935:682). During the spring of 1917 Jamal Pasha had ordered the
immediate evacuation of the entire population of Jaffa and Tel Aviv. According to Arthur 22 For a disturbing account of the sufferings of the Lebanese people prior to the onslaught of Spanish influenza, see Fawaz (1917).
19
Ruppin (1971:164), who himself remained exiled in Constantinople23, their population
was then 40.000, of whom about 9.000 were Jews. The number of refugees grew when
the British occupied southern Palestine in the fall of 1917 (up to about 20 kilometers
north of Tel Aviv). “All the Jewish inhabitants of Judea who happened to be outside the
occupied territory at the time of the conquest were unable to return to their homes and
had to find emergency accommodation in the unoccupied regions, especially in Haifa,
Tiberias and the settlement in the Galilee”. When the refugees were dispersed, some,
“including Meir Dizengoff, [the first mayor of Tel Aviv], went as far as Damascus”.
In October 1918 the Spanish consul made a tour in northern Palestine, now occupied by
the EEF. Ballobar makes no mention of Spanish flu but briefly mentions cholera in
Tiberias. He passed through the city but "stopped only to put some gas in the car, and I
was not sorry for it, because there have been some cases of cholera in the town"
(Ballobar, 2011:219). The men of the EEF occupied Tiberias on September 25. Cholera
was present there prior to their arrival. The source of the outbreak was the
contaminated drinking water of the Lake of Galilee (Dolev, 2007:157). According to
military historian Cyril Falls, "the biggest killers of all were malaria and influenza",
whereas cholera was a minor problem. "Nearly all diseases known to man were
prevalent, with the happy exception of the worst of all, cholera, […] only a single British
soldier caught it and Tiberias was the only town where a few civilians were affected"
(Falls, 1979:131-‐132). Spanish flu may have been present in Tiberias but obscured by
the cholera epidemic. A simultaneous outbreak of cholera interacting with the influenza
pathogen could have been a deadly combination. Also Saffed, taken by the EEF on
September 26, may have been hit hard. According to Uziel Schmelz, mortality in Saffed 23 Arthur Ruppin, the director of the Zionist Office in Jaffa, had been exiled to Constantinople in September 1916 (Jacobson, 2006:49).
20
was extremely high during the war. A 1919 census found that 2.688 Jews remained in
Saffed, out of which 1.858 were Ashkenazim. Citing a source that quantifies the pre-‐war
Ashkenazi population of Saffed to 5.540, Schmelz remarks that a mortality rate of about
3.200 people is indeed “a scary number" (Schmelz, 1991:42). Certainly, many of these
deaths occurred prior to the arrival of Spanish influenza. Nevertheless, its impact may
have been significantly underreported. There is some circumstantial evidence that the
population of both Tiberias as well as Saffed may have been suffering particularly hard
in early October, well synchronized with the advance of the EEF and the march of
Spanish influenza. On October 8 1918, when, as we have seen, influenza was killing
combatants as far north as Damascus, Nahum Sokolow and Chaim Weizmann dispatched
a telegram to the Jacob de Haas, the leader of the American Zionist organization:
“Further report from Palestine moral and material situation good in Galileean colonies
6.000 expatriated still in north stop Much distress in Tiberias and Saffed stop” (Barzilay &
Litvinoff, 1977:276).
As pointed out by Arthur Ruppin, information was poor on the fate of the Yishuv in the
north at the time of Allenby´s advance starting on September 19. The division of
Palestine between a British occupied southern area and a northern territory still
controlled by the Ottomans had cut off communication between the Yishuv population
of the north and the Zionist Palestine office in Jerusalem (Ruppin, 1971:164). It seems
likely that both Jewish and Arab observers would have had little understanding and
ability to report on the influenza attack in Greater Syria during the fall and winter of
1918. Moreover, in the fog of war and lack of situational awareness that follows any
advancing military force, it is no surprise that military records are silent on the fate of
the civilian population. As it advanced northwards into the Yildirim-‐zone, the EEF was
21
busy saving itself24. Civilians would have been ill prepared to respond effectively to the
onslaught of influenza. Only complete physical isolation could have saved a settlement
from infection. Penicillin, or any of its antibiotic derivatives, could have remedied a
secondary bacterial infection of the lungs, but no such heroic “magic bullet” medicine
was available to humanity until the mid 1940s. Within the tiny geographic space of Syria
and Palestine there would be little escape from the virus. It would easily penetrate into
every nook and corner, spread by thousands of refugees on the move and a rural
population flocking to urban areas in search of food. The only therapy for influenza is
supportive and symptomatic. In a already hungry, malarious and war-‐fatigued
population with many relatives already dead, rest and nursing care would not be
available to all.
Henry Near, the author of the History of the Kibbutz Movement has remarked that “in
purely human terms, the conquest of Palestine by the British was an act of physical
salvation” (Near, 1992:58). Similarly, George Antonius observed that on the entry of the
EEF in Damascus, "the Arabs were in a frenzy of joy and gave themselves over wholly to
their emotions" (Antonius, 1938:238). However, a brief encounter with the personnel of
the EEF, driving, riding or marching past an Arab village and Jewish Kibbutz, would
suffice to transmit the lethal virus. A brief handshake with the conquering “redeemers”
could be lethal and infect a whole community. Once the advancing men in uniform
disappeared into the horizon, the virus would stay behind to wreak havoc. Civilians,
24 It is beyond the scope of this dissertation to explore the medical response to the Spanish flu as Occidentals scrambled, in the spirit of a medical mission civilisatrice, to heal the "Holy Land". For a description of the activities of the American Red Cross, which began operations in Jerusalem on July 4 1918, see Davison, (1919:86-‐88). For an interesting report on the reopening of the Rothschild Hospital, where the Mufti of Jerusalem was present, see The Rothschild Hospital in Jerusalem (Ormsby-‐Gore, 1918). For details of the response of Zionists, eager to become a modern nation among other paternalistic nations of modern medicine, see Shvarts (1996:329-‐360).

22
already starved, malaria-‐ridden and lethargic, would be left to fend for themselves. The
administration of quinine would have alleviated the symptoms of malaria, but done
nothing to save someone from influenza complicated by pneumonia. Most would sweat
it out and survive, but since morbidity was so high, mortality would be proportionally
high. In a society where the average fellaḥ was expected to live only 35 years (Shepherd,
1999:126), an early death from infectious disease was no aberration. Still in the
miasmatic paradigm and with no understanding of contagionism, civilians would not
know what killed their relatives. No doubt this ignorance was to the benefit of the men
of the EEF who escaped being scapegoated for the spread of the disease. Consistent with
a widely accepted belief of the late 19th and early 20th centuries, that fevers constituted
one form of miasmatic disease, both Jewish and Arab doctors in Palestine commonly
diagnosed malaria for any ailment with symptoms of fever, including influenza and
typhus (Sufian, 2008:80). Influenza, or influenza interacting with other infectious
diseases such as malaria, would be obscured by the routinization of death by disease
and easily misdiagnosed, as most patients would die of a secondary infection. War is
hell, and in the numerous man-‐made and natural calamities that descended upon
Greater Syria during the war, the invasion of Spanish influenza was but one in a
composite demographic disaster. Spanish influenza was obscured by the dark horrors of
expulsion, locust infestation, hunger, disease, chaos and confusion.
The silence of the sources With few secondary sources to offer guidance, I have turned to primary sources in the
form of military records and personal diaries. Indeed, a lot can be said of the military
machinery of the British Empire, but it had one merit for which the historian must be
grateful: it did keep excellent records. Stored in London´s archives and libraries are
23
records that, as we have seen, have helped dispel some of the fog surrounding this
historic event. Military records have their limitation: medical reports are primarily
concerned with the health of their own combatants. On the other hand, military
documents can be classified thus escaping the policy of military censorship that
prevents bad news from leaking out to the public through newspapers. Also personal
diaries have their limitations. The absence of observations in diaries on the influenza
pandemic in the foggy times of war can be deceiving. Trees can fall in the forest without
the noise being recorded by the diarist. Moreover, in the case of Greater Syria there is
another dimension to diaries as a source of information that should be kept in mind.
Countless numbers of diaries and letters are available to us in numerous European
languages, written by private soldiers and their family members during the First World
War. Conversely, the majority of the population of Greater Syria was illiterate. Issa Al-‐
Issa, the editor of the Jaffa-‐based newspaper Filastīn, estimated the literacy rate among
Arabs in 1911 to be roughly 2% (Ayalon, 2004:16). The Jewish population, comprising
the Sephardic community and the European immigrants, was more literate and a
thorough reading of diaries in Hebrew (an undertaking beyond the capacity of this
author) may reveal more clues to the impact of the pandemic.
In History of Zionism (1972) Walter Laqueur describes the Zionists as “a talkative tribe"
(Laqueur, 1972:xxvii). But the Zionist protagonists did not talk much about influenza.
Hunting down anecdotal evidence by Zionist writers on Spanish influenza is a bit like
trying to spy a virus without an electron microscope. A full-‐text search through the 22
volumes and 21.000 entries of the eBook edition of the enormous Encyclopaedia Judaica
(2007) conjures up only a singular hit. According to the encyclopaedia, Israel Giladi, a
pioneer Zionist, member of the Poalei Zion and leader of the Ha-‐shomer, died from
24
Spanish influenza at the age of 32, probably in the kibbutz of Kefar Bag (renamed Kefar
Giladi), south of Metullah (Skolnik & Berenbaum, 2006:595). Likewise, Arabic sources
are silent on Spanish influenza, as if it never happened. In Greater Syria, where the virus
must have killed “tens of thousands”, historians discuss the famine of the war years with
no mention of influenza (Steinberg, 2002:3). The diaries of Khalil Al-‐Sakakini (1878-‐
1953), a Christian Arab whose written observations have otherwise been such a
valuable source of information to Arabic-‐reading social historians, are silent on the
influenza pandemic. Having been deported by Ottoman authorities in 1917 for a brief
period of incarceration in Damascus, he left the Syrian capital on August 8 1918
(Sakakini, 2004:365). British military authorities denied him entry into the British
occupied zone and he consequently spent the next two months in Egypt (ibid) when the
second wave of Spanish flu was traveling through the area. Zionist leaders outside
Palestine, anxiously waiting for the war to come to an end and the Balfour Declaration to
be implemented, were too busy with statecraft and politics to let themselves be
distracted by microscopic agents of history. Also ambitious Arab nationalists were
disinterested in Spanish flu. Zionists and Arabs could use atrocities, dearth and general
devastation to discredit Ottomanism. Microorganisms, in contrast, are poor scapegoats
and not well suited to mobilize popular support. Good and evil are human concepts and
not applicable to forces of nature which cannot speak and whose agency cannot be
reproached or applauded. As pointed out by Timothy Mitchell (2002), social scientists
are generally uncomfortable with non-‐human agents of change in historical processes.
This discomfort could partly explain the historiography’s silence on this non-‐human
historical agent at play in this period. Historical narratives have a limited number of
actors (Mitchell, 2002:50), and the virus arriving with the men of the EEF, was not one
of them.
25
Guido Steinberg (2006:161) offers further explanation for the silence of the sources.
First, he points out, this silence is not an aberration but rather conforms to the norm of
“global amnesia” which struck humanity after the catastrophe of the world war. Second,
death by disease and famine in Greater Syria during this period was routine and lost in
the background noise of the general horrors of war: “the Spanish flu´s impact was thus
hidden under a layer of other, seemingly more important events”. Conversely, in the
Arabian Peninsula, where the horrors of war and hunger were less omnipresent, the
devastation of Spanish influenza has been preserved in the collective memory.
Steinberg points out that the 1918 influenza year (1337 in the Hijrah lunar calendar) is
known in the Arabian Peninsula as sanat al-‐raḥmah and sanat al-‐sakhnah – a reference
to the disease´s high fever (Steinberg, 2006:154). Steinberg cites Harry Philby who
reported that about 25.000 people had perished from Spanish influenza in the Central
Arabian cities (Steinberg, 2006:155). Additional reasons should be added to Steinberg´s
explanation. First, in contrast to other so-‐called imperial or colonial diseases such as
cholera, influenza was initially “a non-‐notifiable disease” (Killingray, 2003:2). Only in
February 1919 was it made compulsory by law to notify British medical authorities on
cases of influenza (Garner, 1922:19). Second, the absence of printed news material in
circulation due to both Ottoman and British military censorship at the time of the
outbreak, contributed to creating an atmosphere of a deficient collective situational
awareness that has endured into the present. Even Amir Afkhami (2003) who writes
about the pandemic in Iran, where mortality from Spanish flu may have been close to
22%, bemoans the fact that none of the published Persian primary or secondary sources
on the war makes any mention of influenza (2003:371). Afkhami therefore has to rely on
primarily British military records in his research. The example of Iran suggests that it is
26
possible for Spanish influenza to have killed thousands of people in Greater Syria
without it being noticed and chronicled as a discrete event. The silence of the sources, I
believe, does not qualify as evidence for the virus being in a mellow mood during its
course through Greater Syria. The fact that mortality was high among combatants
suggests otherwise.
The question of mortality
The historiography on the fate of the civilian population of Greater Syria during the war
remains limited. It is better on the Yishuv for readers of Hebrew. The unknown variables
include demographic figures. Consequently, any attempt to quantify mortality from
influenza constitutes an undertaking reserved for the brave only. Population estimates
for Greater Syria in the period 1910-‐1915 “cluster around 3.5 million” (Issawi,
1993:179). According to Fritz Grobba, the population of Greater Syria for the year 1915
numbered in total 3.423.626 people. Estimating the number of non-‐registered persons
to constitute 25% (mostly bedouins), Grobba estimates the population to have been
around 4 million (Grobba, 1923:8). The population of Palestine on the eve of the First
World War is “roughly estimated at between 689.000-‐800.000, according to different
sources” (Jacobson, 2006:5). According to Zvi Shilony, 14.000 of the total population
died of diseases only in Jerusalem, and one out of every seven Jews (Shilony, 1991:82).
Howard M Sachar´s mortality estimate for the Jewish Yishuv is more conservative. From
its prewar figure of 85.000 the Yishuv emerged from the war reduced to 55.000: “of
those lost, between 8.000 and 10.000 had perished of hunger, illness or exposure”
(Sachar, 2007:113). According to James Gelvin, estimates for total Ottoman losses run
almost as high as 25% – approximately 5 million out of a population of 21 million. Four
out of every five Ottoman citizens who died were non-‐combatants (Gelvin, 2007:77).
27
According to Linda Schatkowski Schilcher (1992:229), “hundreds of thousands of people
died of starvation or starvation related diseases in Greater Syria during the second half
of the First World War” and “may have reached 500.000 by the end of 1918”. Schilcher
makes no mention of Spanish influenza. But as pointed out by Steinberg, these half a
million victims “probably contained a large number of influenza victims” (Steinberg,
2006:157).
The question of how many deaths can be attributed to Spanish influenza will
presumably remain a mystery. Given the lack of diagnostic evidence and considerable
discrepancies even in pre-‐war census data, this mystery will plague not only this
dissertation but also the research of those who follow. The reader who still doubts that
mortality from Spanish flu has been understated is encouraged to ponder the statistics
of areas of relative geographical proximity, such as the Arabian Peninsula, Cyprus, Egypt
and Iran. Guido Steinberg has given ample evidence for the massive impact on the
Arabian Peninsula. Little is known about the impact on Cyprus but death rates in 1918
“rose dramatically” (Killingray, 2003:34). The published death toll from Spanish flu in
Egypt is 138.600. However, a recalculated and updated estimate, at the order of a global
mortality of 50 million, has put the death rate to be around 10.7% of a population of
about 12.9 million (Johnson & Mueller, 2002:110). Colonel Garner writes in his medical
report on Egypt that “in the village outbreaks in which it was possible to study the
death-‐rate it was found from September to December 1918 to be about 25%” (Garner,
1921:83). Due to the high mortality from Spanish flu, deaths in Egypt outnumbered
births for the only time in at least a quarter of a century (Goldberg, 1992:267). Afkhami
(2003), whose work will be discussed in the next chapter, has given a mortality figure
for Iran at up to 21.7%. This dissertation can offer no evidence for a high mortality rate
28
in Greater Syria beyond reference to neighboring areas, which are in themselves open to
question. We have seen that in contrast to military sources, which show beyond doubt
that mortality among combatants was high, sources reveal few clues as to the impact on
the civilian population. In the Medina garrison, 1.300 men out of 11.000 died from
influenza over the course of two months, a mortality rate of 11.8 percent. This well-‐
documented and isolated case gives us an idea of the potentially devastating impact of
the virus. The following chapter will explain why mortality could have been substantial
also in the civilian population due to the phenomenon of influenza interacting with
malaria25.
25 Another dimension to the question of mortality should be mentioned. As previously pointed out, I have been unable to find any textual references to the first wave of Spanish influenza. Populations unaffected by the less virulent first wave of the 1918 pandemic, suffered higher mortality rates in the second wave. The question of acquired immunity is given more attention in the appendix.
29
The interaction of pathogens: influenza and malaria
According to A Brief Record of the Advance of the Egyptian Expeditionary Force, “from a
medical point of view, the most important problem of this campaign – as of all previous
campaigns in this country – has been that of malaria” (Kay, 1919:105). In 1946 a medical
consultant on malaria to the British War office, with no mention of influenza, observed
that during the advance in Palestine a severe epidemic of malaria began on October 5
1918, and that 20.000 cases were reported before the end of that year (Sinton, 1946:7).
But Spanish flu was also present. During Allenby´s final offensive, lasting from
September 19 to October 30, combatants of both sides as well as civilians probably
experienced simultaneous and overlapping epidemics of falciparum malaria and
influenza. William T. Massey, a correspondent embedded with the Egyptian
Expeditionary Force, made the following observation: “There can be no question that the
influenza epidemic which was killing hundreds of thousands of people throughout the
world swept over General Allenby's Army, but a considerable proportion of the cases of
sickness was due to malaria, which in September and the beginning of October is always
bad in this country” (Massey, 1920:271). Victims of Spanish flu came with an
extraordinary array of symptoms, previously unknown in influenza and with unknown
intensity. Influenza was, even by good European and American doctors far removed
from the battlefield, routinely misdiagnosed and confused with dengue fever, yellow
fever, cholera, dysentery, tuberculosis, typhoid and malaria (Barry, 2009:234-‐245). The
possibility that medical personnel of the EEF in the heat of battle confused influenza
with malaria, or other diseases, seems likely. Significantly, as the malariologist Dennis
Shanks (2009) explains, reality is messy. Infectious diseases are not necessarily caused
by a single pathogen but rather by an interaction of multiple causative agents whose
30
symptoms overlap. It was initially not understood that two epidemics of febrile disease
were present in Palestine in late 1918 (Shanks, 2009:656). In the EEF (of about 315.000
soldiers), a total of 773 deaths from malaria infection were recorded during the last
three months of the campaign and another 934 deaths from influenza-‐pneumonia
during the same period (ibid). J.D. Benjafield, a captain in the Royal Army Medical
Corps, in his Notes on the Influenza Epidemic in the Egyptian Expeditionary Force (1919),
similarly observed that in patients of the EEF “already debilitated by malignant tertian
malaria, influenza proved much more serious, many developed bronchopneumonia, and
considerably over 50% of such cased ended fatally” (Benjafield, 1919).
According to Afkhami (2003), Iran was hit hard by the 1918 Spanish influenza
pandemic. His mortality estimates are frightful. Spanish influenza in Iran may have
killed between 8.0%-‐21.7% of the population, between 910.400 and 2.431.000 people
(Afkhami, 2003:383). Afkhami attributes this high mortality rate to a lethal cocktail of
“famine, opium consumption, malaria and anemia26” (Afkhami, 2003:367). With the
exception of opium, the cofactors mentioned by Afkhami are relevant to this study.
Malaria was a cursed commonality both of the Persian as well as Syrian and Palestinian
populations. Malaria was endemic in Greater Syria. It was the most common health
problem caused by infectious disease27. Afkhami postulates a synergism between the
two pathogens of the influenza virus and the parasite of malignant malaria in causing
drastically increased fatalities (Afkhami, 2003:388). People who had malarial fevers had
a substantially worse prognosis when they contracted influenza; this included refugees
in northern India as well as Indians of the British Expeditionary Force (Afkhami,
26 According to Afkhami, anemia was rampant among Iranians on account of malaria and hookworm (Afkhami, 2003:391) 27 For evidence of the prevalence of malaria in Greater Syria, see the appendix of this dissertation.
31
2003:388). As we have seen, Shanks (2009) and Benjafield (1919) support Afkhami´s
hypothesis of malaria significantly exacerbating mortality rates among patients infected
with Spanish flu. If the hypothesis is correct, that malaria interacted with influenza and
significantly increased death rates in malarious populations, I must conclude that
mortality in Greater Syria could have been substantial.
32
Conclusion Initially introduced into the Middle East by sea in early September, the deadly second
wave of the 1918 influenza pandemic was diffused into Greater Syria by the Egyptian
Expeditionary Force. As General Allenby´s force dashed northwards with the second
offensive on September 19, the virus spread into the civilian population of the Yildirim
zone. This dissertation has shown that Spanish influenza took a heavy toll on
combatants of both sides. On the other hand, evidence for the physical impact on the
civilian population remains sparse and inconclusive. This study has failed to quantify
mortality but has suggested it may have been substantial based on comparative
references to neighboring areas, the high mortality among combatants and the
epidemiological phenomenon of influenza being particularly virulent in malarious
populations. I have attempted to identify the reasons for the paucity of textual
references to Spanish influenza. The silence of the sources, I have argued, does not
qualify as evidence for its pathological insignificance. The composite crisis of the war
eclipsed the impact of the 1918 Spanish influenza pandemic.
The course and impact of the 1918 global influenza pandemic in Greater Syria is to a
great extent virgin soil historiographic territory. The geographic diffusion of the virus
into the area has remained unchartered and its impact uncharted. For the student of
Spanish influenza, this attempt to identify a historiographic blind spot, break the ground
and map its course and impact in a hitherto academic terra incognita constitutes in its
own right a raison d'être for this dissertation. It is the hope that future research will be
able to provide more textual evidence for the impact of Spanish flu. Such evidence may
exist in records of the International Red Cross or in private diaries. Further research will
hopefully be able to give a more educated mortality estimate for the civilian population.
33
For historians of the Middle East, it will hopefully inspire more research that go beyond
the narrow focus on mortality in the second wave of the pandemic and explore the
political, economic, social, psychological and medical dimensions of the wider historical
impact. Globally the single worst demographic disaster of the 20th century, the
pandemic struck at a crucial period of historical transition with the collapse of the
Ottoman Empire. The impact of the 1918 Spanish influenza pandemic on the Middle East
has yet to receive its due attention.
34
Appendix
The prevalence of malaria in Greater Syria How malarious was Greater Syria? We know that even during World War II, Allied
troops experienced a high incidence of malaria in the Syrian theatre. "With many rivers
and numerous swamps lying between the Lebanon and Ante-‐Lebanon ranges"
"inhabitants of many villages were observed with high spleen rates" (Stout, 1954:522).
With regard to the Jews of Palestine it can safely be asserted that malaria was an
inescapable part of life and death. Dr. Puchovsky, chairman of the Hebrew Medical
Society of Jaffa from 1912 to 1913, and who treated malaria in the late Ottoman era and
Mandate Palestine, observed that prior to the British Mandate period, malaria incidence
was so high that it was hard to find a single person who had not suffered from it at least
once. Contracting malaria amounted to a "certificate of citizenship", and constituted
nothing less than a rite of passage and initiation rite into residence in the Yishuv (Cited
in Sufian, 2008:79). In cities like Jerusalem, 60% of the Jewish population was said to
have contracted malaria during the First World War and between 1918 and 1919, 50%
of children in Jewish settlements suffered from chronic malaria (Sufian, 2008:84).
But it would be a mistake to believe that malaria affliction was an eccentricity of
Occidental immigrants. Orientals suffered as well28. According to Dr. Ernest W. G.
Masterman (1918) “a large proportion of the bedouins of Palestine are constantly
suffering from malarial fever and even from pulmonary tuberculosis” (Masterman,
28 It should here be pointed out that the sickle-‐cell and beta-‐thalassemia genes, which bestows resistance to severe attacks of malaria are today present among the populations in the eastern Mediterranean (Crosby, 2004:65). This could confer on the indigenous population of Greater Syria a certain resistance to malaria attacks but not from infection.
35
1918:15)29. Another report gives us some indication of the prevalence and distribution
of malaria in Jerusalem: “The greatest scourge of Jerusalem is malaria, which in the
autumn months is almost universal. On examination of some 4.626 children attending
school in Jerusalem, 27.3% had malarial parasites in the blood, and of 7.771 persons of
all classes and conditions 26.7% had the parasites. Among poor Jews the percentage was
40.5%; among Mohammedans [sic] 31.1%; among native Christians 16.4%, and among
Europeans 7.2%” (Hall, 1918:76). In short, malaria was endemic throughout Greater
Syria. To make things worse, the annual outbreak of plasmodium falciparum, the
malignant form of malaria, was well synchronized with the advance of Allenby´s military
offensive launched on September 19. According to data from 1912-‐13, collected by
German scientists of the International Hygiene Bureau, and cited in Eran Dolev´s
Allenby´s Military Medicine (2007), “an annual epidemic of malignant malaria hit
Palestine during the autumn months, its peak being mid-‐October, while the benign
malaria [plasmodium vivax] was at its height during the summer” (Dolev, 2007:133)30.
The question of acquired immunity and the uneven distribution of death Another dimension to the impact of Spanish flu in Greater Syria is the question of
acquired historic immunity which may have increased survival for those previously
exposed to a similar strain of the 1918 influenza virus, thus having an uneven impact of
mortality on the various communities. It may be speculated that the presumably more
immunologically naïve rural population of Greater Syria, and in particular the nomadic
Arab bedouin, was more susceptible to death from the influenza pandemic than those in
29 Ernest W. G. Masterman, a British doctor, arrived in Palestine in 1892 and practiced medicine at the English Mission Hospital in Jerusalem until the outbreak of the war in 1914. He traveled extensively in the region and performed medical examinations on the local populations (Perry & Lev, 2007:87-‐101). 30 Malaria has a substantial secondary effect on other causes of mortality. Malaria associated mortality is probably three times greater than deaths due solely to malaria. See Shanks, Hay and Bradley (2008) for a medical explanation for this phenomenon. For an account of how malaria interacts with HIV, see Shah (2010:222).
36
urban communities. Although this is a controversial hypothesis, it is not unlikely that
previous exposure to outbreaks of influenza similar to that of the Spanish flu may have
conferred a degree of resistance, if not full immunity, in the pandemic of 1918. Previous
exposure to H1-‐like viruses (the subtype of the 1918 virus) would not prevent infection
but could save the patient´s life. We know that once the immune system has
encountered a pathogen, it will activate its immune cells and develop antibodies, thus
developing acquired (or adaptive) immunity (Lerner, 2007:432). In other words, the
immune system epitomizes the Nietzschean aphorism “what does not kill you, will make
you stronger” (Barry, 2009:109). Alfred Crosby (2003) dismisses the possibility that the
so-‐called Russian influenza of 1889-‐1890 conferred historic immunity to the
contemporaries of the 1918 pandemic. Crosby writes that “immunity to influenza is
measured in months, not decades; and anyway, if exposure to the earlier flu had meant
immunity to Spanish influenza, then the mortality rate of all over 30 would have been
low. The truth of the matter is that those in their thirties had a remarkable high death
rate in 1918-‐1919” (Crosby, 2003:215). However, Mamelund (2011) suggests that
peak-‐mortality around age 30 may not be as universal as previously thought and that
one explanation for the extremely high mortality level of remotely residing populations
may be lack of immunity (Mamelund, 2011:8). Mamelund supports the idea that
populations with no or little previous exposure to H1-‐like influenza viruses, due to
geographical remoteness and isolation, would be significantly more immunologically
naive and consequently considerably more vulnerable to death by influenza31.
31 Svenn-‐Erik Mamelund (2003) has documented that areas with high shares of an indigenous population, the Sami in Norway, had high Spanish influenza mortality and postulates a lack of acquired immunity to their relative geographic peripherality (Mamelund, 2003:99). Other "virgin soil" populations which rarely had been exposed to influenza viruses and in which the virus demonstrated extreme virulence, include Eskimo settlements of Alaska, Africans in jungle villages and on islands of the Pacific (Barry, 2009:232).
37
Mamelund´s idea appears to be supported by Steinberg´s conclusion on the devastating
impact on the population of the Arabian Peninsula. The fact that it was hit so hard could
be explained by immunological naiveté due to their relative geographical isolation and
lack of exposure to previous outbreaks of global influenza pandemics. Arabian society
did not enjoy splendid biological isolation, but it was considerably less exposed than the
inhabitants of Greater Syria. As Steinberg puts it, “Central Arabia was in no way isolated,
but was definitely a regional backwater compared to Syria” (Steinberg, 2006:160).
Steinberg suggests that the high mortality in the bedouin population probably holds true
also for bedouins of Syria and Iraq (Steinberg, 2006:155). If the sedentary and farming
populations of the Syrian and Palestinian countryside were less immunologically naïve
relative to the nomadic bedouins, they would still suffer a disadvantage relative to the
urban populations in cities like Jaffa and Jerusalem. The possibility of varying degrees of
immunological resistance to the 1918 influenza virus has some intriguing, although
admittedly speculative, implications. From a military perspective, Spanish influenza may
have been a contributing factor to the defeat of Ottoman troops. There is a possibility
that Ottoman soldiers, many of whom were conscripted from the rural countryside both
in Turkey and the Arab world, may have been immunologically more naïve than their
Western, if not Indian, counterparts. In terms of demographic consequences for Greater
Syria, European immigrants, including Ashkenazim from Eastern Europe of whom many
would be survivors of the Russian flu pandemic of 1889-‐90, would have had higher
survival rates than Sephardic Jews32. Arab urban residents in Jaffa and Jerusalem would
presumably be less immunologically naïve than Arabs in the countryside.
32 For an insight into how Jews from Eastern Europe were accused of bringing influenza to the U.K. in the 1889-‐1890 pandemic, see Smith (1995). For an account of the course of the 1889-‐90 influenza pandemic in North Africa and the Middle East, see Patterson (1986:62-‐65).
38
Works cited
Afkhami, A., 2003. “Compromised Constitutions: The Iranian Experience with the 1918 Influenza Pandemic” in Bulletin of the History of Medicine, 77, 367-392.
Antonius, G., 1938. The Arab Awakening: The Story of the Arab National Movement, London, Hamish Hamilton. Ayalon, A., 2004. Reading Palestine: Printing and Literacy, 1900-1948, Austin, University of Texas Press. Ballobar, A. de la C. L., 2011. Jerusalem in World War I: The Palestine Diary of a European Diplomat, Mazza, R.,
ed., London, I. B. Tauris. Baratz, J., 1954. A Village by the Jordan: The Story of Degania, London, Harvill Press.
Barry, J. M., 2009. The Great Influenza: The Story of the Deadliest Pandemic in History, revised edition., Penguin.
Barzilay D. & Litvinoff B., 1977. ”Letter 278, To Jacob de Haas, New York”, London, 8 October 1918, p.276 in The
Letters and Papers of Chaim Weizmann, series A Volume 8 November 1917 -‐ October 1918, Jerusalem, Israel Universities Press.
Bell, G., 1918. "Letter, October 25 1918", Gertrude Bell Archive. Digitized. Available at Newcastle University Library at: http://www.gerty.ncl.ac.uk/letter_details.php?letter_id=330 [Accessed June 20 2012].
Benjafield, J.D., 1919. ”Notes on the influenza epidemic in the Egyptian Expeditionary Force” in The British Medical
Journal, volume 2, issue 3058, pp. 167-169.
Bluett, A., 1919. With Our Army in Palestine, London, Melrose. Böhm, A., 1935. Die Zionistische Bewegung: Zwei Bände, Berlin, Jüdischer Verlag. [in German] Cornwallis, K. 1919. "The Siege of Medina: Sickness", in Arab Bulletin, intelligence report from the Director of the
Arab Bureau, No 110, April 30 1919, p 35-39, Public Records Office, Kew (PRO), FO/882/28. Criss, N.B., 1999. Istanbul Under Allied Occupation, 1918-1923, Brill. Crosby, A.W., 1993."Influenza", in The Cambridge World History of Human Disease, Kiple, K.F. ed, pp. 807- 811,
Cambridge University Press.
Crosby, A.W., 2003. America’s Forgotten Pandemic: The Influenza of 1918, 2nd ed., Cambridge University Press. Crosby, A.W., 2004. Ecological Imperialism: The Biological Expansion of Europe, 900-1900, 2nd ed., Cambridge
University Press Davenport, W. A., 1918. "Hedjaz operations", 19-25 September 1918 [Precise date is illegible but within the period
given], in Miscellaneous correspondence, 1916 May 03-1920 Apr 26, Public Records Office, Kew (PRO), FO 882/3.
Davison, H. P., 1919. The work of the American Red cross during the war: a statement of finances and
accomplishments for the period July 1, 1917, to February 28, 1919, American Red cross, 1919. Digitized. Available at: http://archive.org/details/cu31924027870777 [Accessed June 29 2012].
Dolev, E., 2007. Allenby’s Military Medicine: Life and Death in World War I Palestine, London, I. B. Tauris. Erickson, E.J., 2000. Ordered To Die, A History of the Ottoman Army in the First World War, London, Greenwood
Press. Falls, C., 1979. Armageddon, 1918 2nd ed., Annapolis, Md., Nautical & Aviation Pub. Co. of America.
39
Fawaz, J.M., 1917. ”Syrias Tragedy: Deportation, Starvation, and Execution”, in The Argus (Melbourne, Vic:1848-1956), 29 September, 1917, p. 6. Digitized. Available with the National Library of Australia at: http://nla.gov.au/nla.news-article1652636 [Accessed June 3 2012].
Fromkin, D., 2009. A Peace to End All Peace: The Fall of the Ottoman Empire and the Creation of the Modern Middle East, 2. reprint, New York, Second Holt.
Garner, C., 1921. “Annual report for the year 1918”, in Colonial Medical Reports No 126, Egypt, reprinted in The
Journal of Tropical Medicine and Hygiene 24, supplement, pp 75-88.
Garner, C., 1922. “Annual report of the Department of Public Health for the year 1919”, in Colonial Medical Reports No 133, Egypt”, reprinted in The Journal of Tropical Medicine and Hygiene 25, supplement, pp 17-25.
Gelvin, J.L., 2007. The Israel-Palestine Conflict: One Hundred Years of War, 2nd ed., New York, Cambridge
University Press. Goldberg, E., 1992. "Peasants in Revolt - Egypt 1919" in International Journal of Middle East Studies, Vol. 24, No. 2,
pp. 261-280, Cambridge University Press. Available at: http://www.jstor.org/stable/164298 [Accessed May 14 2012 ].
Goldenstedt, P., 1931. “Allenby´s Ride – Dash to Damascus”, in The Sydney Morning Herald (New South Wales,
Australia : 1842 - 1954) Saturday 19 September 1931, p 12. Digitized. Available with the National Library of Australia at: http://nla.gov.au/nla.news-article16828461 [Accessed June 3 2012].
Grobba, F., 1923. Die Getreidewirtschaft Syriens und Palästinas seit Beginn des Weltkrieges, Hannover, Orient
Buchhandlung Heinz Lafaire. [In German] Gullett, H.S., 1941. The Australian Imperial Force in Sinai and Palestine, volume 7, 10th edition, of Official History
of Australia in the War of 1914-1918, Angus and Robertson. Hall, W. H., ed., 1918. “Reconstruction in Turkey: a series of reports”, The American Committee for Armenian and
Syrian Relief, New York City. Hamilton, J. .D., 2002. First to Damascus: The Great Ride and Lawrence of Arabia, East Roseville, N.S.W, London,
Simon & Schuster. Harrison, M., 2004. Disease and the Modern World: 1500 to the Present Day, Cambridge, Polity Press. Hays, J.N., 1998. The Burdens of Disease: Epidemics and Human Response in Western History, New Jersey and
London, Rutgers University Press Hourani, A., 1968. Syria and Lebanon: A Political Essay, Beirut, Librairie du Liban. Issawi, C., 1993. "Middle East Economic Development, 1815-1914: the General and the Specific", in The Modern
Middle East: A Reader, Hourani, A.H., Khoury, P.S. & Wilson M.C. , eds, part II, pp. 177-194, University of California Press.
Jacobson, A., 2006. From Empire to Empire: Jerusalem in the Transition Between Ottoman and British Rule, 1912-1920, Chicago. PhD thesis edition.
Johnson, N. P., & Mueller, J., 2002. “Updating the accounts: global mortality of the 1918-1920 Spanish influenza
pandemic” in Bulletin of the History of Medicine, volume 76, pp. 105-15. Kay, W.R., ed., 1919. A Brief Record of the Advance of the Egyptian Expeditionary Force Under the Command of General Sir Edmund H. H. Allenby: July 1917 to October 1918, Cairo, The Government Press and Survey of Egypt. Keren, M. & Keren, S., 2010. We are Coming, Unafraid: The Jewish Legions and the Promised Land in the First
World War, New York, Rowman & Littlefield.
40
Killingray, D., 2003. "A New Imperial Disease: The Influenza Pandemic of 1918-9 and its Impact on the British Empire" in Caribbean Quarterly, Vol. 49, No. 4, Colonialism and Health in the Tropics, University of the West Indies and Caribbean Quarterly. Available at: http://www.jstor.org/stable/40654422 [Accessed May 30 2012].
Killingray, D. & Phillips, H. eds., 2003. ”Introduction”, in The Spanish Influenza Pandemic of 1918-1919: New Perspectives, pp. 1-25, 1st ed., London, Routledge.
Kitchen, J. 2011. ”The Indianization of the Egyptian Expeditionary Force: Palestine 1918” in The Indian Army in the Two World Wars, Kaushik, R, ed, chapter 5, pp. 165-190, Brill Academic Publishers.
Laqueur, W., 1972. A History of Zionism Walter Laqueur 1st ed., New York Holt, Rinehart And Winston. Lerner, B.W., 2007. Infectious Diseases in Context, 1st ed., Cengage Gale. Mamelund, S-E., 2003. "Spanish Influenza Mortality of Ethnic Minorities in Norway 1918-1919" in Journal of
Population, Vol. 19, No. 1, pp.83-102. Available at http://www.jstor.org/stable/20164214. [Accessed July 1 2012].
Mamelund, S-E., 2011. Geography May Explain Adult Mortality from the 1918–20 Influenza Pandemic. Epidemics, 3(1), pp.46–60. Available at: http://www.sciencedirect.com/science/article/pii/S1755436511000053 [Accessed July 1 2012].
Massey, W.T., 1920. Allenby’s Final Triumph, London, Constable. Masterman, E., 1918. "Hygiene and Disease in Palestine in Modern and in Biblical Times” in Palestine Exploration
Quarterly 50, chapter 1 pp. 13-20, chapter 2 pp. 56-71, chapter 3 pp.12-19. Public Domain. Digitally prepared by T. Hildebrandt (2004). Available at: http://ebookbrowse.com/ma/masterman [Accessed June 4 2012].
McNeill, W. H., 1979. Plagues and Peoples, Harmondsworth, Penguin Books.
McWalter, J. C.,1919. “On the influenza epidemic in Egypt”, in The Medical Press, London, new series, volume 107, no. 4,157, pp. 24-25.
Mitchell, T., 2002. ”Can the Mosquito Speak?” in Rule of Experts: Egypt, Techno-Politics, Modernity, chapter 1 pp.
19-53, Los Angeles, University of California Press. Mortlock, M.J., 2010. The Egyptian Expeditionary Force in World War I: A History of the British-led Campaigns in
Egypt, Palestine and Syria, Jefferson, McFarland & Co Inc.
Murphy, D., 2008. The Arab Revolt 1916-18: Lawrence Sets Arabia Ablaze, 1st ed., Oxford, Osprey.
Near, H., 1992. The Kibbutz Movement: A History, Vol. 1, Origins and growth, 1909-1939, Oxford, Oxford U.P. for Littman Library.
Neumann, O., 1993. A Battle for Survival: The Struggle of the Jewish Yishuv for Existence in Palestine During World
War I, 1914-1918, PhD thesis, Los Angeles, University of California.
Noymer, A., 2010. ”Epidemics and Time: Influenza and Tuberculosis during and after the 1918-1919 Pandemic”, in Plagues and Epidemics: Infected Spaces Past and Present, Herring, D.A. & Swedlung, A.C. eds., Oxford, New York, Berg.
Ormsby-Gore, W, 1918. “The Rothschild Hospital in Jerusalem” in Eastern Report, No 94, November 14 1918, p. 4,
Public Records Office, Kew (PRO), CAB/24/145. Ormsby-Gore, W, 1918. “Palestine – General Situation” in Eastern Report, No 90, October 17 1918, p. 7, Public
Records Office, Kew (PRO), CAB/24/145. Patterson, K.D., 1986. Pandemic Influenza, 1700-1900: A Study in Historical Epidemiology illustrated ed., New
Jersey, Rowman & Littlefield.
41
Perry, Y & Lev E., 2007. Modern Medicine in the Holy Land: Pioneering British Medical Services in Late Ottoman Palestine, London, Tauris Academic Studies.
Phipson, E.S., 1920. Observations on the outbreak of influenza in India in the year 1918: With special reference to the
city of Bombay, MD thesis, University of London. Pipes, D., 1990. Greater Syria: The History of an Ambition, Oxford, Oxford University Press. Quinn, T., 2008. Flu: A Social History of Influenza, London, New Holland Publishers Ltd.
Ruppin, A., 1971. Arthur Ruppin: Memoirs, Diaries, Letters / Edited with an introduction by Alex Bein; translated
from the German by Karen Gershon; afterword by Moshe Dayan, 1st ed., New York, Herzl Press. Sachar, H.M., 2007. History of Israel: From the Rise of Zionism to Our Time 3rd ed., New York, Random House Inc. Sakakini, K. 2004. The Diaries of Khalil Sakakini. Volume Two: Orthodox Renaissance, World War I, Exile to
Damascus, Mousallam A. (ed.), first edition, Khalil Sakakini Cultural Centre, Ramallah, and The Institute of Jerusalem Studies. [In Arabic]
Schatkowski Schilcher, L., 1992. “The famine of 1915-1918 in Greater Syria”, in Problems of the Modern Middle East
in Historical Perspective: Essays in Honour of Albert Hourani, J P. Spagnolo (ed.), chapter 13, pp. 229-258, Reading, Ithaca Press.
Schmelz, U. O., 1991. “The Decline in the Population of Palestine during World War I”, in Siege and Distress, Eretz
Israel During the First World War. Mordechai E. (ed.), pp. 17-47, Jerusalem, Yad Yizhak Ben Zvi. [In Hebrew] Shah, S., 2010. The Fever: How Malaria Has Ruled Humankind for 500,000 Years 1st ed., New York, Sarah Crichton
Books. Shanks G. D., Hay S. I., Bradley D. J., 2008. "Malaria's indirect contribution to all-cause mortality in the Andaman
Islands during the colonial era" in Lancet Infectious Diseases, volume 8, no. 9, pp. 564-570. Shanks, G. D., 2009. ”Simultaneous epidemics of influenza and malaria in the Australian Army in Palestine in 1918”,
in The Medical Journal of Australia, Volume 191, number 11/12. Available at: https://www.mja.com.au/journal/2009/191/11/simultaneous-epidemics-influenza-and-malaria-australian-army-palestine-1918 [Accessed May 30 2012].
Shepherd, N., 1999. Ploughing Sand: British Rule in Palestine, 1917-1948, London, John Murray. Shilony, Z., 1991. “Health services in Jerusalem”, in Siege and Distress, Eretz Israel During the First World War,
Mordechai E. (ed.), pp.61-83, Jerusalem, Yad Yizhak Ben Zvi. [In Hebrew] Shvarts, S., 1996. "Kupat Holim and Jewish Health Services during the Mandate", in Health and Disease in the Holy
Land: Studies in the History and Sociology of Medicine from Ancient Times to the Present, Waserman, M. & Kottek, S. (eds.), chapter 14, pp. 329- 360, Lewiston, N.Y, Lampeter, Edwin Mellen Press.
Sinton, B.J.A., 1946. “Malaria in War”, in The Ulster Medical Journal, 15(1), pp. 3-28. Available at:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2479199/ [Accessed June 19 2012]. Skolnik, F. & Berenbaum, M. eds., 2006. "Giladi, Israel" in Encyclopaedia Judaica, second edition, volume 7, p. 596,
Jerusalem, Thompson and Gale. Smith, F.B., 1995. ”The Russian Influenza in the United Kingdom, 1889–1894” in Social History of Medicine, 8(1),
pp.55–73. Available at: http://shm.oxfordjournals.org/content/8/1/55 [Accessed June 6 2012]. Steinberg, G., 2002. Die Spanische Grippe von 1918/19 in Deutschland. Syrien und Saudia, Freie Universität Berlin.
Available at: http://www.fu-berlin.de/presse/publikationen/fundiert/archiv/2002_01/02_01_steinberg/index.html [Accessed May 31 2012]. [In German]
42
Steinberg, G., 2006. “The Commemoration of the ”Spanish Flu“ of 1918–1919 in the Arab East”, in The First World War as Remembered in the Countries of the Eastern Mediterranean, O. Farschid, M. Kropp, S. Dähne (eds.), pp. 151-162, Beiruter Texte und Studien 99, Orient Institut Beirut.
Storey, W.K., 2010. The First World War: A Concise Global History, Plymouth, Rowman & Littlefield Publishers. Storrs, R., 1937. Orientations, London, I. Nicholson & Watson. Storrs, R., 1972. The Memoirs of Sir Ronald Storrs, New York, Arno Press. Stout, T.D. 1954. War Surgery and Medicine, Historical Publications Branch, Wellington. Sufian, S.M., 2008. Healing the Land and the Nation: Malaria and the Zionist Project in Palestine, 1920-1947,
Chicago and London, University of Chicago Press. Tamari, S., 2007. “The Short Life of Private Ihsan: Jerusalem 1915”, in Jerusalem Quarterly, Vol. 8, no. 1, pp. 26-58. Von Sanders, L., 1919. Fünf Jahre Türkei, Berlin, Verlag von August Scherl. [In German]
Wavell, A.P.W., 1941. The Palestine Campaigns, 3rd ed., London, Constable. Wilson, R.H., 1987. Palestine 1917, edited by Millgate, H.D, Tunbridge Wells, Costello. Özdemir, H., 2008. The Ottoman Army, 1914-1918: Disease & Death on the Battlefield, Salt Lake City, University of
Utah Press.
Related Documents











