CRANIOMAXILLOFACIAL DEFORMITIES/COSMETIC SURGERY The Impact of Orthognathic Surgery on Facial Expressions Ali Al-Hiyali, BDS, MSc, * Ashraf Ayoub, BDS, MDS, PhD,y Xiangyang Ju, PhD, BENG, MENG,z Mohammad Almuzian, BDS, MSc,x and Thamer Al-Anezi, BMS, BM BCh, BDS, MSck Purpose: The aim of this study was to evaluate the impact of orthognathic surgical correction of facial asymmetry and maxillary hypoplasia on the magnitude and pattern of facial expressions. Patients and Methods: This study was carried out on 2 cohorts of patients: in group 1, 10 patients had surgical correction of facial asymmetry; in group 2, 13 patients had Le Fort I osteotomy to correct maxillary hypoplasia. The patients were asked to perform 3 facial expressions (maximal smile, lip purse, and cheek puff) that were recorded using the Di4D image-capture system before and after surgery. The capture of each expression generated 180 3-dimensional (3D) facial images. Twenty-seven facial soft tissue landmarks were digitized on the first frame of the 3D image of each expression and a mathematical generic mesh was applied on the 3D model to clone each patient’s face. The cloned mesh was superimposed automatically on each sequence of the 3D images to evaluate the pattern of facial expressions. The digitization of facial landmarks was satisfactorily accurate and reproducible. Results: In group 1, the asymmetry of facial expressions was significantly decreased after surgical correction (P = .0458). In group 2, Le Fort I osteotomy decreased the magnitude of facial expressions (P = .0267). Conclusion: This study confirmed that orthognathic surgery affects the dynamics of facial expressions; this should be considered when planning the surgery and informing patients about the surgical correction of dentofacial deformities. Ó 2015 American Association of Oral and Maxillofacial Surgeons J Oral Maxillofac Surg -:1-11, 2015 Facial expressions are the most common means of communication among humans, with 55% of daily social interactions being nonverbal and dependent on facial expressions. 1 In addition, dentofacial deformities are associated with compromised facial expressions. 2 In living creatures, flawless bilateral facial and body symmetry is a hypothetical concept that rarely exists. Minor asymmetry exists in pleasing-looking faces and does not require treatment. For minor facial asymme- try, the right half of the face is frequently wider than the left, with the chin deviated to the left. 3 Maxillary hypoplasia combined with relative mandibular excess results in skeletal Class III skeletal deformity; this deformity esthetically affects the attrac- tiveness of the affected individuals. Most patients with Class III skeletal deformity have the appearance of an angry person and they look older than their actual *Master’s Student of Oral and Maxillofacial Surgery, College of Medicine, College of Medical, Veterinary and Life Sciences, Glasgow University Dental Hospital and School, Glasgow, UK. yProfessor, Oral and Maxillofacial Surgery, College of Medical, Veterinary and Life Sciences, University of Glasgow Medical School, Glasgow, UK. zSenior Software Engineer, Medical Devices Unit, NHS Greater Glasgow and Clyde; Honorary Research Fellow, Faculty of Medicine, College of Medical, Veterinary and Life Sciences, Glasgow University Dental Hospital and School, Glasgow, UK. xMaster’s Student, College of Medical, Veterinary and Life Sciences, Glasgow University Dental Hospital and School, Glasgow, UK. kMaster’s Student in Oral and Maxillofacial Surgery, Faculty of Medicine, College of Medical, Veterinary and Life Sciences, Glasgow University Dental Hospital and School, Glasgow, UK. Address correspondence and reprint requests to Prof Ashraf: Department of Oral and Maxillofacial Surgery, University of Glasgow, Dental School, 378 Sauchiehall Street, Glasgow G2 3JZ, UK; e-mail: [email protected] Received March 11 2015 Accepted May 13 2015 Ó 2015 American Association of Oral and Maxillofacial Surgeons 0278-2391/15/00592-3 http://dx.doi.org/10.1016/j.joms.2015.05.008 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CRANIOMAXILLOFACIAL DEFORMITIES/COSMETIC SURGERY
Me
Gla
Vet
Sch
Gla
Me
Gla
Sci
Gla
The Impact of Orthognathic Surgeryon Facial Expressions
*Master
dicine,
sgow U
yProfeserinary
ool, Gl
zSeniorsgow
dicine,
sgow U
xMaster
ences,
sgow, U
Ali Al-Hiyali, BDS, MSc,* Ashraf Ayoub, BDS, MDS, PhD,yXiangyang Ju, PhD, BENG, MENG,z Mohammad Almuzian, BDS, MSc,x
and Thamer Al-Anezi, BMS, BM BCh, BDS, MSck
Purpose: The aim of this study was to evaluate the impact of orthognathic surgical correction of facialasymmetry and maxillary hypoplasia on the magnitude and pattern of facial expressions.
Patients andMethods: This study was carried out on 2 cohorts of patients: in group 1, 10 patients had
surgical correction of facial asymmetry; in group 2, 13 patients had Le Fort I osteotomy to correct maxillary
hypoplasia. The patients were asked to perform 3 facial expressions (maximal smile, lip purse, and cheek
puff) that were recorded using the Di4D image-capture system before and after surgery. The capture of
each expression generated 180 3-dimensional (3D) facial images. Twenty-seven facial soft tissue landmarks
were digitized on the first frame of the 3D image of each expression and a mathematical generic mesh wasapplied on the 3D model to clone each patient’s face. The cloned mesh was superimposed automatically
on each sequence of the 3D images to evaluate the pattern of facial expressions. The digitization of facial
landmarks was satisfactorily accurate and reproducible.
Results: In group 1, the asymmetry of facial expressions was significantly decreased after surgical
correction (P = .0458). In group 2, Le Fort I osteotomy decreased the magnitude of facial expressions
(P = .0267).
Conclusion: This study confirmed that orthognathic surgery affects the dynamics of facial expressions;
this should be considered when planning the surgery and informing patients about the surgical correction
of dentofacial deformities.
� 2015 American Association of Oral and Maxillofacial Surgeons
J Oral Maxillofac Surg -:1-11, 2015
Facial expressions are the most common means of
communication among humans, with 55% of daily
social interactions being nonverbal and dependenton facial expressions.1 In addition, dentofacial
deformities are associated with compromised facial
expressions.2
In living creatures, flawless bilateral facial and body
symmetry is a hypothetical concept that rarely exists.
Minor asymmetry exists in pleasing-looking faces and
’s Student of Oral and Maxillofacial Surgery, College of
College of Medical, Veterinary and Life Sciences,
niversity Dental Hospital and School, Glasgow, UK.
sor, Oral and Maxillofacial Surgery, College of Medical,
and Life Sciences, University of Glasgow Medical
asgow, UK.
Software Engineer, Medical Devices Unit, NHS Greater
and Clyde; Honorary Research Fellow, Faculty of
College of Medical, Veterinary and Life Sciences,
niversity Dental Hospital and School, Glasgow, UK.
’s Student, College of Medical, Veterinary and Life
Glasgow University Dental Hospital and School,
K.
1
does not require treatment. For minor facial asymme-
try, the right half of the face is frequently wider than
the left, with the chin deviated to the left.3
Maxillary hypoplasia combined with relative
mandibular excess results in skeletal Class III skeletal
deformity; this deformity esthetically affects the attrac-
tiveness of the affected individuals. Most patients with
Class III skeletal deformity have the appearance of an
angry person and they look older than their actual
kMaster’s Student in Oral and Maxillofacial Surgery, Faculty of
Medicine, College of Medical, Veterinary and Life Sciences,
Glasgow University Dental Hospital and School, Glasgow, UK.
Address correspondence and reprint requests to Prof Ashraf:
Department of Oral and Maxillofacial Surgery, University of Glasgow,
Dental School, 378 Sauchiehall Street, Glasgow G2 3JZ, UK; e-mail:
Received March 11 2015
Accepted May 13 2015
� 2015 American Association of Oral and Maxillofacial Surgeons
0278-2391/15/00592-3
http://dx.doi.org/10.1016/j.joms.2015.05.008
2 ORTHOGNATHIC SURGERY AND FACIAL EXPRESSIONS
age; therefore, they seek treatment to improve their
facial esthetics.4 Maxillary hypoplasia and facial asym-
metry are among the common facial deformities that
are readily correctable with orthognathic surgery.5-8
However, the impact of orthognathic surgery on
facial expressions has not been fully investigated.
The most common concerns of patients who seek
orthognathic surgery are the dysmorphology of facialappearance at rest and with facial expressions. Expres-
sions are dependent on the movement of facial
muscles and their relation to underlying bones. There-
fore, it is logical to assume that orthognathic surgery
will alter the orientation of facial muscles. It also has
been suggested that postsurgical stability is dependent
on muscle balance and that relapse is more likely if the
functional impairments of facial expressions persistafter orthognathic surgery.9
Several studies have assessed the impact of orthog-
nathic surgery on the bony structures and the covering
soft tissue10-14; however, the impact of orthognathic
surgery on the dynamics of facial expressions is rarely
investigated.9,15-17 The published studies on this topic
have limitations. The direct placement of multiple
markers on a patient’s face before image captures canvary between imaging sessions, which introduces
inaccuracies into the assessment. Direct application of
facial markers also is time consuming for the
clinician and requires a high level of cooperation
from the patient. Moreover, the application of markers
onto the face could prevent the achievement of a
natural facial expression.18,19 The small number of
landmarks to describe facial movements limits thecomprehensiveness of the analysis and the
interpretation of the results.17
Variousmethods have been developed to assess facial
expressions,19-21 some of them are 2-dimensional,
including photography and videotaping. However,
these methods underestimate the magnitude of facial
expressions by 43%.22 Facial expressions also have
been assessed using 3-dimensional (3D) statisticimaging-based systems.23 However, these methods do
not record or analyze the dynamic of facial expressions.
The objective assessment of facial muscle move-
ments requires the recording of the associated expres-
sions in a dynamic state. Static capture of maximum
facial expressions does not record the direction,
speed, and pattern of facial movements, which limits
the robustness of the analysis.6 Various 3D dynamicmotion-capture systems have been developed recently
that are based on active stereophotogrammetry, in
which a textured pattern is projected onto the face
to aid the 3D build of the facial model,24 or passive ster-
eophotogrammetry, which depends on skin texture to
build the 3D facial models.25 The dynamic imaging sys-
tem captures 60 3D images of the face per second; the
capture of each expressions takes approximately 3 sec-
onds, which generates approximately 180 3D facial
images for analysis. Facial landmarks are digitized on
the first 3D facial image, and their locations are auto-
matically tracked throughout the sequence of the
images of the captured facial expression. The accuracy
of the software in tracking the digitized facial land-
marks across the sequence of the 3D images of each
facial expression captured by a passive stereophotog-rammetry imaging system has been validated26 and
the clinical application of the method has
been tested.27
The purpose of this study was to investigate the
impact of orthognathic surgical correction of maxil-
lary hypoplasia and facial asymmetry on facial
expressions.
Patients and Methods
This study was carried out on 2 cohorts of patients:
10 patients (5 male and 5 female; 17 to 29 yr old) whohad surgical correction of facial asymmetry (group 1)
and 13 patients (8 female and 5 male; 18 to 50 yr
old) who had had Le Fort I osteotomy to address maxil-
lary hypoplasia (group 2). All patients were treated by
the same surgeon and followed a standard protocol of
data recording and analysis before and after surgery.
Preoperative facial expressions were captured
1 week before surgery and 6 to 18 months after sur-gery (Table 1) using the Di4D capture system (Dimen-
sional Imaging Ltd, Hilington Park, Glasgow, UK). The
system consisted of 2 gray-scale cameras (Model avA
1600-65km/kc; resolution, 1,600 � 1,200 pixels;
sensor model KAI-02050; Kodak, Basler, Germany), 1
color camera that captured 60 frames per second,
and a lighting system (Model DIV-401-DIVALITE;
Kino Flo Corporation, Burbank, CA). The system wasconnected to a personal computer (Win 8.1 profes-
sional; Intel Core i7; CPU, 3.40 GHz; RAM, 32.0 GB).
The Di4D system was calibrated before each capture
session to synchronize the intrinsic camera parame-
ters. The image recording and building of the dynamic
3D imagines were based on passive stereophotogram-
metry, which allowed the automatic tracking of facial
landmarks throughout the sequence of the capturedimages of each facial expression.
Three nonverbal, reproducible facial expressions
were captured in this study, which included maximal
smile, lip purse, and cheek puff, according to a previ-
ously published protocol.18,20,21 Patients sat in an
upright and comfortable position at a 95-cm distance
from the cameras. Patients were asked to keep their
eyes open and remain relatively still during imagecapturing. The system’s illumination lights were
adjusted by the operator to avoid excessive brightness
that could affect the patient’s facial expressions. Three
facial expressions were recorded: maximum smile, lip

Table 1. DEMOGRAPHIC DISTRIBUTION OF CASES IN THE 2 GROUPS
Patient Number Age (yr) Gender Performed Surgical Procedure Follow-Up (mo)
Group 1
P1 20 M Le Fort I osteotomy + genioplasty 5
P2 20 M BSSO 8
P3 21 M Bimaxillary osteotomy, Le Fort I + BSSO 6
P4 20 F Bimaxillary osteotomy, Le Fort I + BSSO 6
P5 29 F Bimaxillary osteotomy, Le Fort I + BSSO 6
P6 17 M bimaxillary osteotomy, Le Fort I + BSSO 6
P7 19 M Bimaxillary osteotomy, Le Fort I + BSSO 5
P8 20 F Bimaxillary osteotomy, Le Fort I + BSSO 8
P9 18 F BSSO 18
P10 18 F BSSO + genioplasty 18
Group 2
P1 41 M Le Fort I osteotomy 6
P2 20 F Le Fort I osteotomy 6
P3 20 F Le Fort I osteotomy 6
P4 19 M Le Fort I osteotomy 6
P5 41 M Le Fort I osteotomy 6
P6 19 F Le Fort I osteotomy 6
P7 45 M Le Fort I osteotomy 6
P8 20 M Le Fort I osteotomy 6
P9 49 F Le Fort I osteotomy 6
P10 27 F Le Fort I osteotomy 6
P11 50 F Le Fort I osteotomy 6
P12 18 F Le Fort I osteotomy 6
P13 20 F Le Fort I osteotomy 6
Abbreviations: BSSO, bilateral sagittal split osteotomy; F, female; M, male.
Al-Hiyali et al. Orthognathic Surgery and Facial Expressions. J Oral Maxillofac Surg 2015.
AL-HIYALI ET AL 3
purse, and cheek puff (Fig 1). Ethics approval was
granted to conduct this study under the IntegratedResearch Application System GN12DN441 (protocol
1 18) and sponsored by the UK NHS Greater Glasgow
and Clyde health board.
DATA PROCESSING
A set of facial landmarks (Table 2) was digitized on
the first 3D facial model of each of the 3D sequence
of images for each facial expression. The position of
these landmarks was tracked automatically acrossthe set of 180 3D sequences of facial images for each
expression. To assess the errors of the method, facial
soft tissue landmarks of 10 cases were digitized twice,
1 week apart, by the same operator for each of the
3 captured expressions.
A novel method was applied to assess the impact of
orthognathic surgery on facial expressions using a
generic mesh (Fig 2). The generic mesh consists of1,982 points andwas adapted to themorphologic char-
acteristic of the face to generate a confirmedmesh that
was specific to each case. The first frame of each 3D
sequence for each expression and its related generic
mesh were selected for manual digitization of 27
anthropometric facial landmarks (Table 2).28-30 Thelandmarks on the first 3D frame were used to clone
(transform) a generic mesh to the 3D model in the
first frame (Fig 3). The cloned (transformed) mesh
was automatically tracked throughout the sequence
of the 3D imagining of each expression. The coordi-
nated tracked facial landmarkswere saved for statistical
analysis.
STATISTICAL ANALYSIS
The analysis of variance (ANOVA) linear mixed-
effects (LME) model was applied to test the impact
of the orthognathic surgery on the 3 facial expressions
at a chosen level of significance (P < .05). The LME
model represents a model of a response variable
with fixed and random effects. For each fixed-effects
term, ANOVA performs a t test to determine whether
all coefficients representing the fixed-effects termare equal to 0. Facial asymmetry score and maximal
distance changes of facial expressions were analyzed
in this study. To investigate the dissimilarity in the
shape of lips, cheeks, and chin regions, each 3D facial

FIGURE1. Three-dimensional image sequence of the captured maximum smile before surgical correction. All expressions were captured fromrest to maximum positions.
Al-Hiyali et al. Orthognathic Surgery and Facial Expressions. J Oral Maxillofac Surg 2015.
4 ORTHOGNATHIC SURGERY AND FACIAL EXPRESSIONS
image was mirror imaged; the reflected image was
superimposed on its own original configuration
(shape) using partial Procrustes analysis (PPA). Theprocess of mirror reflection of each 3D image was
based on the equation x = x��x(�1), which allowed
the entire set of 3D images to be ‘‘mirrored’’ around the
x axis to obtain a mirror-like reflection. PPA allowed
the maximum superimposition of corresponding
shapes by transformation (rotation without scaling).
PPA was applied in this study to maintain the original
sizes of the tested regions (lips, cheeks, and chin).PPA allowed the values of the differences between
the original and mirror-reflected 3D images to be
measured as the sum of squared distances of the corre-
sponding vertices, which represented the asymmetry
score in each 3D facial image. The average scores
from at rest tomaximal expressionmeasured the asym-
metry of the facial movements. An ANOVA LME model
was applied to test the impact of surgery on the asym-metry scores of facial expressions as a fixed effect and
the types of facial expression and gender as random
effects. The 3 recorded facial expressions were amal-
gamated together and analyzed collectively to evaluate
the impact of orthognathic surgery on these facial
movements. The scores obtained from the PPA were
tested using the ANOVA LME model to generate the
facial asymmetry score. This protocol was appliedfor each sequence of facial expressions that were
recorded before and after surgery for each case in
the 2 groups. The method also was applied to measure
the differences of the vertices in the lips, cheeks, and
chin regions.
Differences in the magnitude of maximal expres-
sions were investigated in this study. The tracked
coordinates of facial landmarks were used to assessthe magnitude of maximal movement for each of the
recorded facial expressions before and after surgery.
The change from the rest position (first 3D frame of
facial expression) to maximal expression (peak 3D
frame of the same facial expression) was tracked and
calculated using correspondence analysis (CA). CA is
a statistical method based on mapping the difference
between 2 facial confirmed meshes. The obtainedCA scores were analyzed by the ANOVA LME model
to assess the impact of orthognathic surgery on the
magnitude of facial expressions.
Results
ERRORS OF THE METHOD
Themean differences among the repeated landmark
procedures of the 3D facial images were 0.1, 0.2, and
0.6 mm in the x, y, and z directions, which confirmed
that the landmark technique was accurate and
reproducible.
GROUP 1 (SKELETAL FACIAL ASYMMETRY)
There was a significant difference in facial expres-
sion asymmetry scores as a result of the surgicalcorrection (P = .0458; Fig 4). The improvement in
the symmetry of facial expressions for this group of pa-
tients is illustrated in the color mapping of Figure 5,
which shows the degree of difference between the
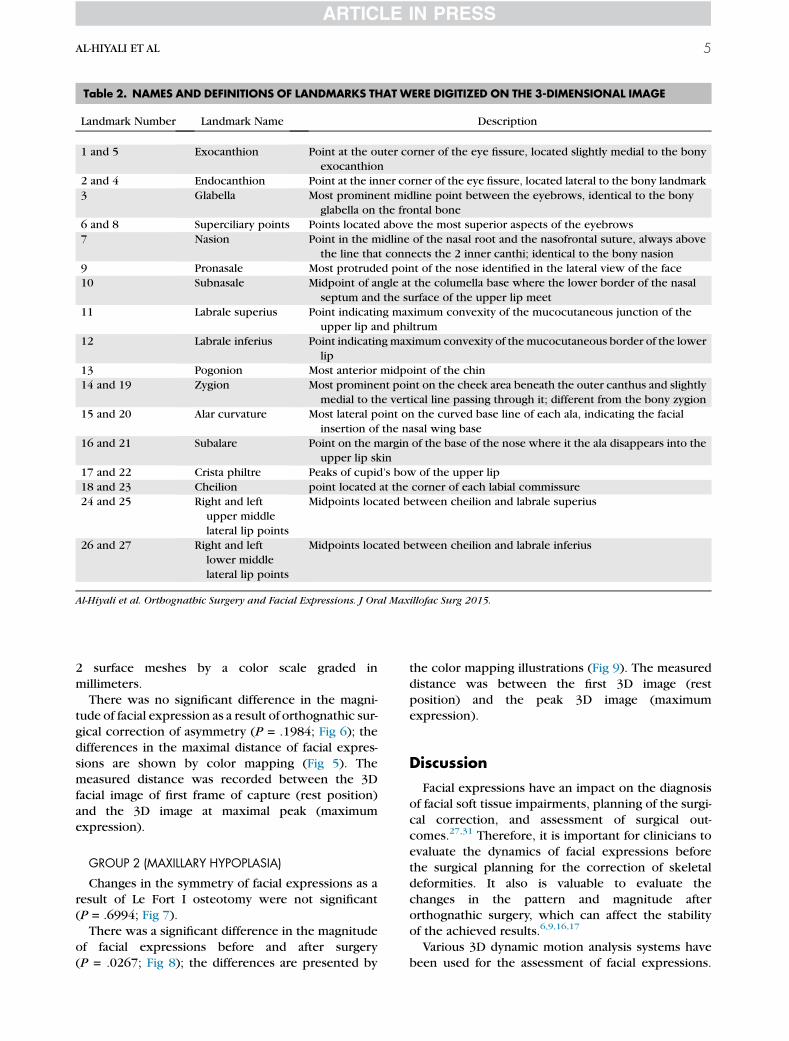
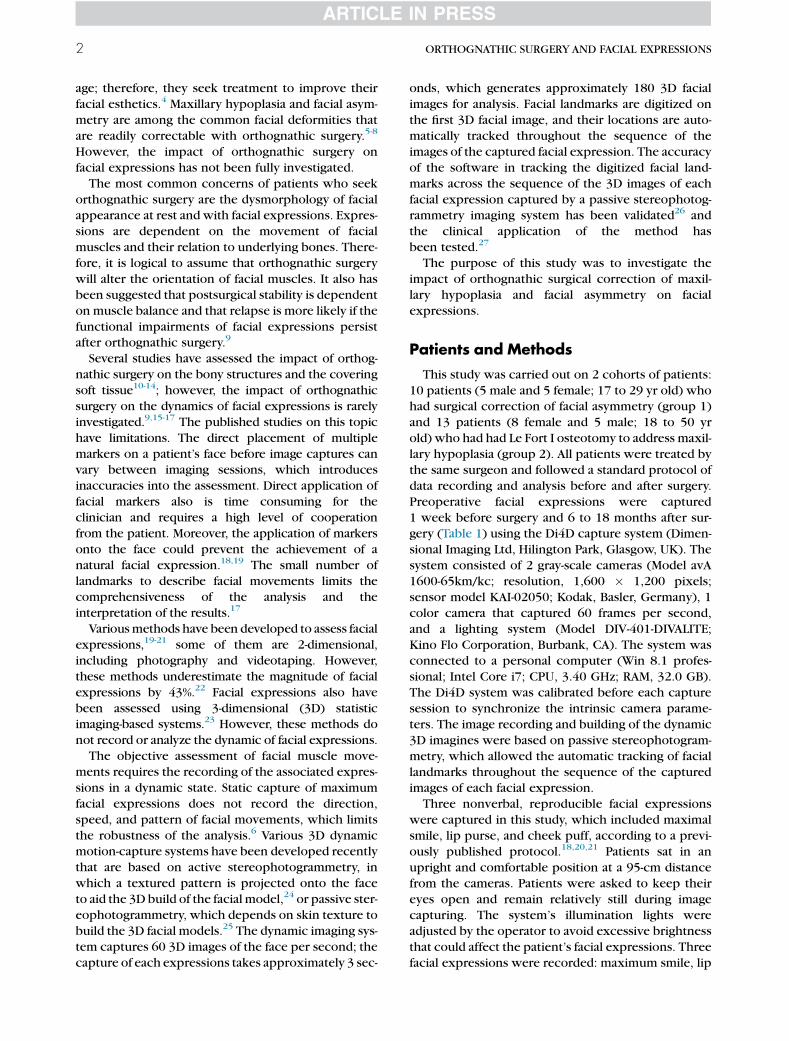
Table 2. NAMES AND DEFINITIONS OF LANDMARKS THAT WERE DIGITIZED ON THE 3-DIMENSIONAL IMAGE
Landmark Number Landmark Name Description
1 and 5 Exocanthion Point at the outer corner of the eye fissure, located slightly medial to the bony
exocanthion
2 and 4 Endocanthion Point at the inner corner of the eye fissure, located lateral to the bony landmark
3 Glabella Most prominent midline point between the eyebrows, identical to the bony
glabella on the frontal bone
6 and 8 Superciliary points Points located above the most superior aspects of the eyebrows
7 Nasion Point in the midline of the nasal root and the nasofrontal suture, always above
the line that connects the 2 inner canthi; identical to the bony nasion
9 Pronasale Most protruded point of the nose identified in the lateral view of the face
10 Subnasale Midpoint of angle at the columella base where the lower border of the nasal
septum and the surface of the upper lip meet
11 Labrale superius Point indicating maximum convexity of the mucocutaneous junction of the
upper lip and philtrum
12 Labrale inferius Point indicating maximum convexity of the mucocutaneous border of the lower
lip
13 Pogonion Most anterior midpoint of the chin
14 and 19 Zygion Most prominent point on the cheek area beneath the outer canthus and slightly
medial to the vertical line passing through it; different from the bony zygion
15 and 20 Alar curvature Most lateral point on the curved base line of each ala, indicating the facial
insertion of the nasal wing base
16 and 21 Subalare Point on the margin of the base of the nose where it the ala disappears into the
upper lip skin
17 and 22 Crista philtre Peaks of cupid’s bow of the upper lip
18 and 23 Cheilion point located at the corner of each labial commissure
24 and 25 Right and left
upper middle
lateral lip points
Midpoints located between cheilion and labrale superius
26 and 27 Right and left
lower middle
lateral lip points
Midpoints located between cheilion and labrale inferius
Al-Hiyali et al. Orthognathic Surgery and Facial Expressions. J Oral Maxillofac Surg 2015.
AL-HIYALI ET AL 5
2 surface meshes by a color scale graded in
millimeters.
There was no significant difference in the magni-
tude of facial expression as a result of orthognathic sur-
gical correction of asymmetry (P = .1984; Fig 6); the
differences in the maximal distance of facial expres-
sions are shown by color mapping (Fig 5). Themeasured distance was recorded between the 3D
facial image of first frame of capture (rest position)
and the 3D image at maximal peak (maximum
expression).
GROUP 2 (MAXILLARY HYPOPLASIA)
Changes in the symmetry of facial expressions as a
result of Le Fort I osteotomy were not significant(P = .6994; Fig 7).
There was a significant difference in the magnitude
of facial expressions before and after surgery
(P = .0267; Fig 8); the differences are presented by
the color mapping illustrations (Fig 9). The measured
distance was between the first 3D image (rest
position) and the peak 3D image (maximum
expression).
Discussion
Facial expressions have an impact on the diagnosis
of facial soft tissue impairments, planning of the surgi-
cal correction, and assessment of surgical out-
comes.27,31 Therefore, it is important for clinicians to
evaluate the dynamics of facial expressions before
the surgical planning for the correction of skeletal
deformities. It also is valuable to evaluate the
changes in the pattern and magnitude afterorthognathic surgery, which can affect the stability
of the achieved results.6,9,16,17
Various 3D dynamic motion analysis systems have
been used for the assessment of facial expressions.

FIGURE2. Generic mesh used to evaluate the dynamic changes offacial expressions.
Al-Hiyali et al. Orthognathic Surgery and Facial Expressions. J Oral
Maxillofac Surg 2015.
6 ORTHOGNATHIC SURGERY AND FACIAL EXPRESSIONS
These systems track markers on the face or trackpixels of the facial images. These systems have been
used to assess facial expressions,2,30-36 after non-
orthognathic surgical procedures, and to quantify
the symmetry of normal facial movements.23,28,37-40
FIGURE 3. Transformed mesh (generic mesh) to track the changes of anaduring facial expressions (patient from facial asymmetry group).
Al-Hiyali et al. Orthognathic Surgery and Facial Expressions. J Oral Max
The first video-based study to investigate the impact
of orthognathic surgery on facial expressions was
conducted on 19 patients.9 Eleven patients had skel-
etal Class II mandibular retrognathia, 5 patients had
anterior open bite, and the other 3 patients had skel-
etal Class III maxillomandibular relation. A set of 34
spherical, retroreflective markers, 2 mm in diameter,
were attached by eyelash adhesive to specific anthro-pologic landmarks on the patients’ faces, and facial
expressions were recorded by a video-based tracking
system (Motion Analysis; Motion Analysis Corporation,
Santa Rosa, CA). Seven facial animations were per-
formed by each patient, including the instructed
maximal smile, lip purse, mouth opening, cheek
puff, eye opening, eye closure, grimace, and a natural
smile animation. The aim was to measure the relativechange or percentage of change in distance from rest
to maximal animation between corresponding pairs
of landmarks. There was a statistical difference in
the magnitude of animations after surgery, with the
most important changes detected in the lip purse
animation. These findings suggested that facial
movements are affected by skeletal malocclusion and
orthognathic surgical procedures. The results showedthat all changes were related to the direction of the
facial expressions and these varied for each patient
group in the study. However, the symmetry and magni-
tude of facial expressions were not assessed.
A 3D laser scanner was used to assess the effect of
orthognathic surgery on facial expressions16 in 11
cases that required orthognathic surgery. Only 13
landmarks were directly placed on the patients’ facesbefore capturing 5 basic facial expressions (frowning,
tomic landmarks throughout the sequence of 3-dimensional capture
illofac Surg 2015.

FIGURE 4. Boxplot showing changes in the asymmetry score offacial expressions after surgery (group 1).
Al-Hiyali et al. Orthognathic Surgery and Facial Expressions. J Oral
Maxillofac Surg 2015.
AL-HIYALI ET AL 7
eye closure, grimace, smile, and lip purse). The facial
images were captured at 1 week before surgery and
at 3, 6, and 12 months postoperatively. The displace-
ment of every landmark at specific intervals was inves-tigated. A change in the symmetry of facial expressions
as a result of surgery was detected. At 1-year follow-up,
FIGURE 5. Illustration of the change of symmetry of the maximum smile amasks (group 1).
Al-Hiyali et al. Orthognathic Surgery and Facial Expressions. J Oral Max
the magnitude of facial movements was statistically
similar to that recorded before surgery. The path of
movement of facial landmarks was not tracked and
the results were based only on the positional differ-
ences between rest and maximum expression. The
landmarks-based analysis has limitations, and the
anatomic areas between the landmarks were not
considered in this study.The direct placement of multiple markers on the
face before image capture is a major obstacle for the
assessment of facial expressions. This can vary be-
tween sessions and among operators, which contrib-
utes to the errors of the method and affects the
reliability of the assessment. Direct marker placement
also is time consuming for the patient and the clinician
and could prevent the patient from producing a natu-ral facial expression.18,19
The applied generic mesh in the present study was
an innovation in assessing the impact of orthognathic
surgery on facial expressions. The confirmed mesh is
considered a fingerprint that captures facial patterns
and morphologic characteristics of each patient’s
face. The 27 landmarks that were digitized on the 3D
facial model in this study were used only to guidethe cloning of the facial mesh for the transformation
fter surgery shown on photorealistic images and color-coded facial
illofac Surg 2015.
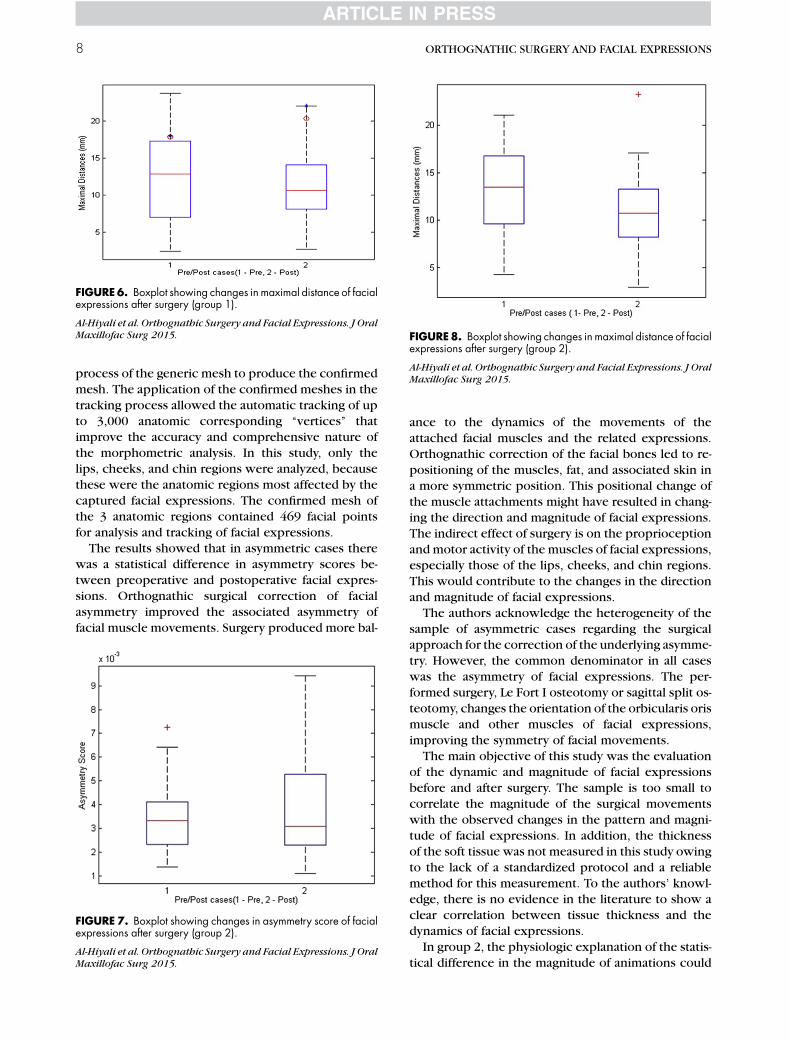
FIGURE6. Boxplot showing changes in maximal distance of facialexpressions after surgery (group 1).
Al-Hiyali et al. Orthognathic Surgery and Facial Expressions. J Oral
Maxillofac Surg 2015. FIGURE8. Boxplot showing changes in maximal distance of facialexpressions after surgery (group 2).
Al-Hiyali et al. Orthognathic Surgery and Facial Expressions. J Oral
Maxillofac Surg 2015.
8 ORTHOGNATHIC SURGERY AND FACIAL EXPRESSIONS
process of the generic mesh to produce the confirmed
mesh. The application of the confirmed meshes in the
tracking process allowed the automatic tracking of up
to 3,000 anatomic corresponding ‘‘vertices’’ thatimprove the accuracy and comprehensive nature of
the morphometric analysis. In this study, only the
lips, cheeks, and chin regions were analyzed, because
these were the anatomic regions most affected by the
captured facial expressions. The confirmed mesh of
the 3 anatomic regions contained 469 facial points
for analysis and tracking of facial expressions.
The results showed that in asymmetric cases therewas a statistical difference in asymmetry scores be-
tween preoperative and postoperative facial expres-
sions. Orthognathic surgical correction of facial
asymmetry improved the associated asymmetry of
facial muscle movements. Surgery produced more bal-
FIGURE 7. Boxplot showing changes in asymmetry score of facialexpressions after surgery (group 2).
Al-Hiyali et al. Orthognathic Surgery and Facial Expressions. J Oral
Maxillofac Surg 2015.
ance to the dynamics of the movements of the
attached facial muscles and the related expressions.
Orthognathic correction of the facial bones led to re-
positioning of the muscles, fat, and associated skin in
a more symmetric position. This positional change of
the muscle attachments might have resulted in chang-ing the direction and magnitude of facial expressions.
The indirect effect of surgery is on the proprioception
and motor activity of the muscles of facial expressions,
especially those of the lips, cheeks, and chin regions.
This would contribute to the changes in the direction
and magnitude of facial expressions.
The authors acknowledge the heterogeneity of the
sample of asymmetric cases regarding the surgicalapproach for the correction of the underlying asymme-
try. However, the common denominator in all cases
was the asymmetry of facial expressions. The per-
formed surgery, Le Fort I osteotomy or sagittal split os-
teotomy, changes the orientation of the orbicularis oris
muscle and other muscles of facial expressions,
improving the symmetry of facial movements.
The main objective of this study was the evaluationof the dynamic and magnitude of facial expressions
before and after surgery. The sample is too small to
correlate the magnitude of the surgical movements
with the observed changes in the pattern and magni-
tude of facial expressions. In addition, the thickness
of the soft tissue was not measured in this study owing
to the lack of a standardized protocol and a reliable
method for this measurement. To the authors’ knowl-edge, there is no evidence in the literature to show a
clear correlation between tissue thickness and the
dynamics of facial expressions.
In group 2, the physiologic explanation of the statis-
tical difference in the magnitude of animations could
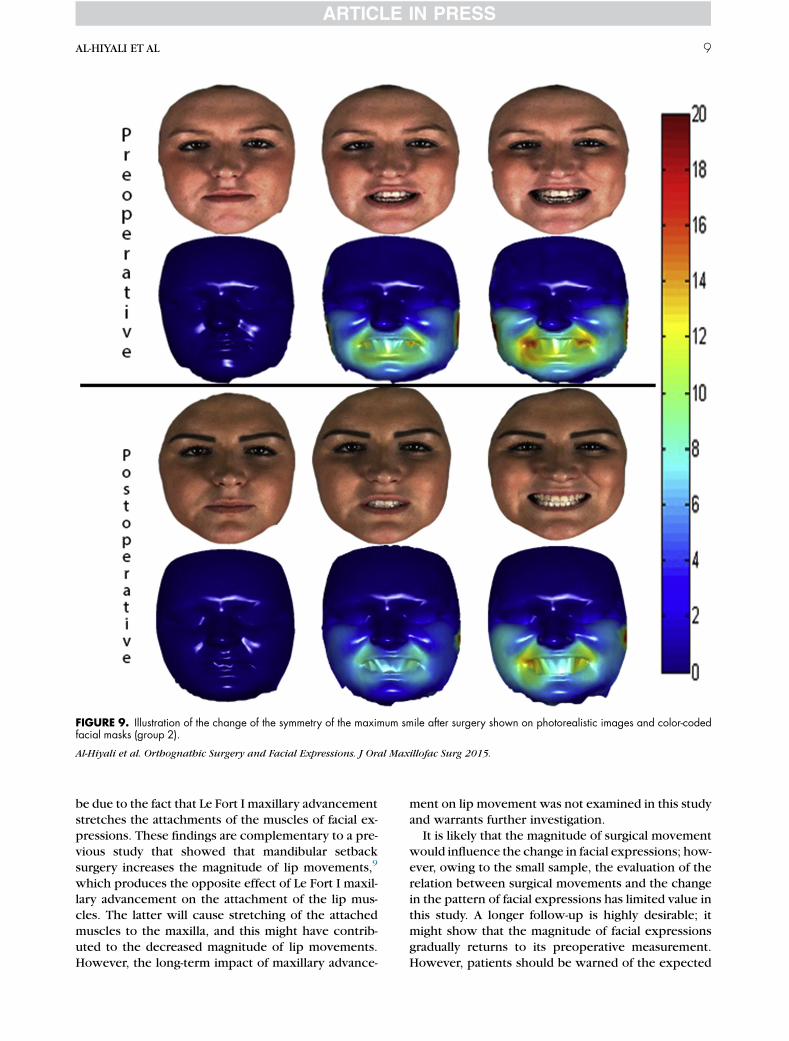
FIGURE 9. Illustration of the change of the symmetry of the maximum smile after surgery shown on photorealistic images and color-codedfacial masks (group 2).
Al-Hiyali et al. Orthognathic Surgery and Facial Expressions. J Oral Maxillofac Surg 2015.
AL-HIYALI ET AL 9
be due to the fact that Le Fort I maxillary advancement
stretches the attachments of the muscles of facial ex-
pressions. These findings are complementary to a pre-
vious study that showed that mandibular setback
surgery increases the magnitude of lip movements,9
which produces the opposite effect of Le Fort I maxil-lary advancement on the attachment of the lip mus-
cles. The latter will cause stretching of the attached
muscles to the maxilla, and this might have contrib-
uted to the decreased magnitude of lip movements.
However, the long-term impact of maxillary advance-
ment on lip movement was not examined in this study
and warrants further investigation.
It is likely that the magnitude of surgical movement
would influence the change in facial expressions; how-
ever, owing to the small sample, the evaluation of the
relation between surgical movements and the changein the pattern of facial expressions has limited value in
this study. A longer follow-up is highly desirable; it
might show that the magnitude of facial expressions
gradually returns to its preoperative measurement.
However, patients should be warned of the expected

10 ORTHOGNATHIC SURGERY AND FACIAL EXPRESSIONS
restriction in facial expressions during the first
6 months after surgery. A larger sample would lend it-
self to a more intensive analysis on the relation be-
tween skeletal jaw movements and the change in the
dynamic of facial expressions.
Another limitation of this study is the amalgamation
of the 3 facial expressions for the analysis of the impact
of orthognathic surgery on muscle movements. Onecould argue that the changes of one expression in
one direction cancel the changes of another expres-
sion in an opposite direction. A larger sample would
have allowed the study of the impact of orthognathic
surgery on each facial expression separately and a
more robust conclusion on understanding the relation
between the surgical movements of the osteotomy
segments and the attached muscles. This study didnot investigate the relation among the extent of sur-
gery, 1- or 2-jaw surgery, the magnitude and direction
of movements of the osteotomy segments (yaw, pitch,
and roll), and the recorded changes in facial expres-
sions. A larger sample would be required to answer
these questions. Nevertheless, the study shows clearly
the impact of orthognathic surgery on the magnitude
and overall symmetry of facial expressions.The authors hope this study inspires amore compre-
hensive investigation on a more homogenous group of
orthognathic cases. They study just the first step in
highlighting the importance of investigating the dy-
namics of facial expressions and evaluating the impact
of orthognathic surgery on the symmetry and magni-
tude of these movements.
Correction of asymmetry improved the symmetry offacial expressions. Themagnitude of facial expressions
was decreased after Le Fort I osteotomy. The asymme-
try score developed in this study is a novel and sensi-
tive tool in quantifying facial expressions that could
have a broad clinical application in the assessment of
facial muscle movements.
References
1. Mehrabian A: Inference of attitudes from nonverbal communica-tion in two channels. J Consult Psychol 31:248, 1967
2. Weeden JC, Trotman CA, Faraway JJ, et al: Three dimensionalanalysis of facial movement in normal adults: Influence of sexand facial shape. Angle Orthod 71:132, 2001
3. Cheong YW, Lo LJ: Facial asymmetry: Etiology, evaluation, andmanagement. Chang Gung Med J 34:341, 2011
4. Posnick JC: Orthognathic Surgery: Principles and Practice. NewYork, NY, Elsevier, 2014, pp 686–757
5. Proffit WR, Turvey TA, Phillips C: Orthognathic surgery: A hierar-chyof stability. Int JAdultOrthodonOrthognath Surg11:191, 1996
6. Johns FR, Johnson PC, Buckley MJ, et al: Changes in facial move-ment after maxillary osteotomies. J Oral Maxillofac Surg 55:1044, 1997
7. Bauer RE, Ochs MW: Maxillary orthognathic surgery. Oral Max-illofac Surg Clin North Am 26:523, 2014
8. Severt TR, ProffitWR: The prevalence of facial asymmetry in thedentofacial deformities population at the University of NorthCarolina. Int J Adult Orthodon Orthognath Surg 12:171, 1996
9. Nooreyazdan M, Trotman CA, Faraway JJ: Modeling facial move-ment: II. A dynamic analysis of differences caused by orthog-nathic surgery. J Oral Maxillofac Surg 62:1380, 2004
10. Katsumata A, Fujishita M, Maeda M, et al: 3D-CT evaluation offacial asymmetry. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 99:212, 2005
11. Trpkova B, Prasad NG, Lam EW, et al: Assessment of facialasymmetries from posteroanterior cephalograms: Validity ofreference lines. Am J Orthod Dentofacial Orthop 123:512,2003
12. Yamamoto M, Takaki T, Shibahara T: Assessment of facialasymmetry based by subjective evaluation and cephalo-metric measurement. J Oral Maxillofac Surg Med Pathol24:11, 2012
13. Forsberg CT, Burstone CJ, Hanley KJ: Diagnosis and treatmentplanning of skeletal asymmetry with the submental-verticalradiograph. Am J Orthod 85:224, 1984
14. Bishara SE, Burkey PS, Kharouf JG: Dental and facial asymme-tries: A review. Angle Orthod 64:89, 1994
15. Wachtman GS, Cohn JF, VanSwearingen JM, et al: Automatedtracking of facial features in patients with facial neuromusculardysfunction. Plast Reconstr Surg 107:1124, 2001
16. Verz�e L, Bianchi FA, Dell’Acqua A, et al: Facial mobility afterbimaxillary surgery in Class III patients: A three-dimensionalstudy. J Craniofac Surg 22:2304, 2011
17. Popat H, Richmond S, Marshall D, et al: Three-dimensionalassessment of functional change following Class 3 orthognathiccorrection—A preliminary report. J Craniomaxillofac Surg 40:36, 2012
18. Sawyer AR, SeeM, Nduka C: Assessment of the reproducibility offacial expressions with 3-D stereophotogrammetry. OtolaryngolHead Neck Surg 140:76, 2009
19. Frey M, Giovanoli P, Gerber H, et al: Three-dimensional videoanalysis of facial movements: A new method to assess thequantity and quality of the smile. Plast Reconstr Surg 104:7, 1999
20. Johnston DJ, Millett DT, Ayoub AF, et al: Are facial expressionsreproducible? Cleft Palate Craniofac J 40:291, 2003
21. O’Leary E, Ju X, Khambay B, et al: Evaluation of the reproduc-ibility of non-verbal facial animations. Lecture Notes ComputSci 7378:184, 2012
22. Gross MM, Trotman CA, Moffatt KS: A comparison of three-dimensional and two-dimensional analyses of facial motion.Angle Orthod 66:189, 1996
23. Hajeer MY, Ayoub AF, Millett DT: Three-dimensional assessmentof facial soft-tissue asymmetry before and after orthognathic sur-gery. Br J Oral Maxillofac Surg 42:396, 2004
24. Popat H, Richmond S, Benedikt L, et al: Quantitative analysis offacial movement—A review of three-dimensional imaging tech-niques. Comput Med Imaging Graph 33:377, 2009
25. Mishima K: Analysis methods for facial motion. Jpn Dent Sci Rev45:4, 2009
26. Al-Anezi T, Khambay B, Peng MJ, et al: A new method for auto-matic tracking of facial landmarks in 3Dmotion captured images(4D). Int J Oral Maxillofac Surg 42:9, 2013
27. Shujaat S, Khambay BS, Ju X, et al: The clinical application ofthree-dimensional motion capture (4D): A novel approach toquantify the dynamics of facial animations. Int J Oral MaxillofacSurg 43:907, 2014
28. Farkas L: Anthropometry of the Head and Face (ed 2). NewYork,NY, Raven Press, 1994, pp 79–88
29. Sawyer AR, See M, Nduka C: Quantitative analysis of normalsmile with 3D stereophotogrammetry—An aid to facial reanima-tion. J Plast Reconstr Aesthet Surg 63:65, 2010
30. Hajeer MY, Ayoub AF, Millett DT, et al: Three-dimensional im-aging in orthognathic surgery: The clinical application of anew method. Int J Adult Orthodon Orthognath Surg 17:318, 2002
31. Trotman CA: Faces in 4 dimensions: Why do we care, and whythe fourth dimension? Am J Orthod Dentofacial Orthop 140:895, 2011
32. Popat H, Richmond S, Playle R, et al: Three-dimensional motionanalysis—An exploratory study. Part 1: Assessment of facialmovement. Orthod Craniofac Res 11:216, 2008

AL-HIYALI ET AL 11
33. Popat H, Richmond S, Zhurov AI, et al: A geometric morpho-metric approach to the analysis of lip shape during speech:Development of a clinical outcome measure. PLoS One 8:e57368, 2013
34. Mishima K, Yamada T, Matsumura T, et al: Analysis of lip motionusing principal component analyses. J Craniomaxillofac Surg 39:232, 2011
35. Trotman CA, Faraway JJ: Sensitivity of a method for the analysisof facial mobility. II. Interlandmark separation. Cleft PalateCraniofac J 35:142, 1998
36. Trotman CA, Faraway JJ: Modeling facial movement: I.A dynamic analysis of differences based on skeletal characteris-tics. J Oral Maxillofac Surg 62:1372, 2004
37. Trotman CA, Faraway JJ, Phillips C: Visual and statisticalmodeling of facial movement in patients with cleft lip and pal-ate. Cleft Palate Craniofac J 42:245, 2005
38. Hontanilla B, Aub�a C: Automatic three-dimensional quantitativeanalysis for evaluation of facial movement. J Plast Reconstr Aes-thet Surg 61:18, 2008
39. Tzou CH, Pona I, Placheta E, et al: Evolution of the3-dimensional video system for facial motion analysis: Tenyears’ experiences and recent developments. Ann PlastSurg 69:173, 2012
40. Coulson SE, Croxson GR, Gilleard WL: Three-dimensional quan-tification of the symmetry of normal facial movement. Otol Neu-rotol 23:999, 2002
Related Documents