Global Research Journal of Public Health and Epidemiology: ISSN-2360-7920 Vol. 2(3): pp xxx-xxx, March, 2014. Copyright © 2014 Spring Journals Review The impact of complementary Therapies in Ghanaian Men diagnosed with Prostate Cancer: A critical review of the impact of complementary therapies in Ghanaian men diagnosed with Prostate cancer as part of the Psychology of cancer care. Raphael Obu Sheffield Hallam University, Post Graduate Office, Faculty of Health and Well being, UK Men’s Health Foundation Ghana Accepted 19 th February, 2014 To examine the impact of complementary Therapies in Ghanaian Men diagnosed with Prostate cancer. To examine the literature in violation to the impact of complementary Therapies in Ghanaian Men diagnosed with Prostate cancer , looking at the complementary therapies in Cancer Care, Classification by mode of action, models of use in cancer care, Responses of orthodox medical bodies, it use in general , used by cancer patients, the complementary therapies-evidence , safety and applications, diets and dietary supplements, Top supplements for prostate cancer management and the prospect of croton membranaceus for prostate Health in Ghanaian men –Herbal Practitioners headache with the used of this plant for Benign Prostatic Hypertrophy and Prostate cancer management in Ghana. The impact of complementary Therapies in Ghanaian men diagnosed with prostate cancer appears as good form of patient’s psychology of cancer care and also it improves the quality of life of the patient, patient’s survival in general if used with conventional therapies and monitored by expert in both complementary medicine practice and conventional practice. From the result I hypothesize that complementary therapies will have a great impact on Ghanaian men diagnosed with prostate cancer and Patient’s must also be told the truth about side effects of these therapies and the practitioner in Ghana must not promise cure and must also not say complementary therapies are natural hence it has no side effect. Complementary Therapies have a major role to play and have high impact on Ghanaian men diagnosed with prostate cancer in Ghana, but however, it should not be used as the only management option for Ghanaian menand black men diagnosed with prostate cancer as it can be a calculated gamble for patient’s survival rate and quality of life. It should be used in conjunction with the traditional cancer treatment to save life and improve patient’s quality of life. This literature highlights the potentially significant impact complementary Therapies in Ghanaian men diagnosed with prostate cancer as part of psychology of cancer care. Keywords: Prostate cancer, complementary therapies, quality of life, Ghanaian men, croton membranaceus INTRODUCTION Complementary and alternative medicine,” “complementary medicine,” “alternative medicine,” integrative medicine”—are terms on the Internet and in marketing, but what do they really mean and do they actually have a role to play in Prostate Cancer Management? While the terms are often used to mean the array of health care approaches with a history of use or origins outside of mainstream medicine, they are actually hard to define and may mean different things to different people. These literatures critically look into these terms to help you understand them better, and give you a brief picture and role in this area of research. Many Ghanaians, nearly 70 percent, use health care approaches developed outside of mainstream Western, or conventional, medicine for specific conditions or overall well-being. When describing health approaches with non-mainstream roots, people often use the words “alternative” and “complementary” interchangeably, but

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Global Research Journal of Public Health and Epidemiology: ISSN-2360-7920 Vol. 2(3): pp xxx-xxx, March, 2014. Copyright © 2014 Spring Journals
Review
The impact of complementary Therapies in Ghanaian Men diagnosed with Prostate Cancer: A critical review of the
impact of complementary therapies in Ghanaian men diagnosed with Prostate cancer as part of the Psychology of
cancer care.
Raphael Obu
Sheffield Hallam University, Post Graduate Office, Faculty of Health and Well being, UK Men’s Health Foundation Ghana
Accepted 19
th February, 2014
To examine the impact of complementary Therapies in Ghanaian Men diagnosed with Prostate cancer. To examine the literature in violation to the impact of complementary Therapies in Ghanaian Men diagnosed with Prostate cancer , looking at the complementary therapies in Cancer Care, Classification by mode of action, models of use in cancer care, Responses of orthodox medical bodies, it use in general , used by cancer patients, the complementary therapies-evidence , safety and applications, diets and dietary supplements, Top supplements for prostate cancer management and the prospect of croton membranaceus for prostate Health in Ghanaian men –Herbal Practitioners headache with the used of this plant for Benign Prostatic Hypertrophy and Prostate cancer management in Ghana. The impact of complementary Therapies in Ghanaian men diagnosed with prostate cancer appears as good form of patient’s psychology of cancer care and also it improves the quality of life of the patient, patient’s survival in general if used with conventional therapies and monitored by expert in both complementary medicine practice and conventional practice. From the result I hypothesize that complementary therapies will have a great impact on Ghanaian men diagnosed with prostate cancer and Patient’s must also be told the truth about side effects of these therapies and the practitioner in Ghana must not promise cure and must also not say complementary therapies are natural hence it has no side effect. Complementary Therapies have a major role to play and have high impact on Ghanaian men diagnosed with prostate cancer in Ghana, but however, it should not be used as the only management option for Ghanaian menand black men diagnosed with prostate cancer as it can be a calculated gamble for patient’s survival rate and quality of life. It should be used in conjunction with the traditional cancer treatment to save life and improve patient’s quality of life. This literature highlights the potentially significant impact complementary Therapies in Ghanaian men diagnosed with prostate cancer as part of psychology of cancer care. Keywords: Prostate cancer, complementary therapies, quality of life, Ghanaian men, croton membranaceus
INTRODUCTION Complementary and alternative medicine,” “complementary medicine,” “alternative medicine,” integrative medicine”—are terms on the Internet and in marketing, but what do they really mean and do they actually have a role to play in Prostate Cancer Management? While the terms are often used to mean the array of health care approaches with a history of use or origins outside of mainstream medicine, they are actually hard to define and may mean different things to
different people. These literatures critically look into these terms to help you understand them better, and give you a brief picture and role in this area of research. Many Ghanaians, nearly 70 percent, use health care approaches developed outside of mainstream Western, or conventional, medicine for specific conditions or overall well-being. When describing health approaches with non-mainstream roots, people often use the words “alternative” and “complementary” interchangeably, but

the two terms refer to different concepts:“Complementary” generally refers to using a non-mainstream approach together with conventional medicine.“Alternative” refers to using a non-mainstream approach in place of conventional medicine. True alternative medicine is not common. Most people use non-mainstream approaches along with conventional treatments. And the boundaries between complementary and conventional medicine overlap and change with time. For example, guided imagery and massage, both once considered complementary or alternative, are used regularly in some hospitals to help with pain management. Non-mainstream health care approaches may also be considered part of integrative medicine or integrative health care.
For example, cancer treatment centers with integrative health care programs may offer services such as acupuncture and meditation to help manage symptoms and side effects for patients who are receiving conventional cancer treatments such as chemotherapy. There are various definitions for “integrative health
care,” but several facts about this growing health trend are clear:
It’s happening now. Many individuals, health care providers, and health care systems are integrating various practices with origins outside of mainstream medicine into treatment and health promotion.
The integrative trend is growing among providers and health care systems. Driving factors include marketing of integrative care by health care providers to consumers who perceive benefits to health or well-being, and emerging evidence that some of the perceived benefits are real or meaningful.
The scientific evidence is limited. In many instances, a lack of reliable data makes it difficult for people to make informed decisions about using integrative health care. Alternative cancer treatments are alternative or complementary treatments for cancer that have not been approved by the government agencies responsible for the regulation of therapeutic goods. They include diet and exercise, chemicals, herbs, devices, and manual procedures. The treatments may be untested or unsupported by evidence, either because no proper testing has been conducted, or because testing did not demonstrate statistically significant efficacy. Concerns have been raised about the safety of some of them. Some treatments that have been proposed in the past have been found in clinical trials to be useless or unsafe. Some of these obsolete or disproven treatments continue to be promoted, sold, and used. Alternative cancer treatments are typically contrasted with experimental cancer treatments – which are treatments for which experimental testing is currently underway – and with complementary treatments, which are non-invasive practices used alongside other
treatment. All currently approved chemotherapeutic cancer treatments were considered experimental cancer treatments before their safety and efficacy testing was completed.
A large-scale survey examining trends in the use of alternative medicine in the United States from 1990 to 1997 reported that the use of alternative medicine had increased from 34% to 42% in that time.More visits to alternative health practitioners are reported today than total visits to all primary care physicians.
Managed care organizations and insurance companies have started to increase coverage of some specific alternative therapies, such as acupuncture and massage therapy.Most U.S. medical schools have also begun to offer courses in this discipline.Other countries around the world have also reported a large increase in the use of alternative treatments. For example, separate studies suggest that one third of the Finnish and approximately 50% of the Australian population have used some type of alternative medicine.
One of the fastest growing areas of alternative or “complementary” medicine is the use of dietary changes and dietary supplements or herbal therapies. Herbal treatment sales exceeded $2.5 billion in 1996 and have been projected to increase by 25% every year. One of the largest surveys conducted on the attitudes of individuals using supplements found that most people do not discuss their usage with their physician, because they do not believe physicians know much about them and that they may be biased against their use.In addition, individuals were unexpectedly supportive of some type of regulation. Supplement use
during clinical trials may also be an area of concern. A recent report found that many of the participants from a colon cancer trial were using supplements.The authors believe that such large-scale use may result in investigators having to monitor supplement use more closely or increase participant numbers, because utilization could change the results of various cancer clinical trials.
Numerous complementary therapies could be discussed in this manuscript; however, few have gained more attention than fat consumption or soy and soy supplements. The reason for such attention to these two interventions has to do with the large geographical variation in the ageadjusted incidence of prostate
cancer. Autopsy series demonstrate that the incidence of latent prostate cancer is approximately equal in men from Asia and the United States.Nevertheless, African American men have the highest incidence of prostate cancer, which is roughly 30 times greater than Japanese men, and about 120 times greater than that observed in men from Shanghai, China.Japanese immigrants in the U.S. experience increases in incidence to about half that of the indigenous population within one or two generations.This rather fast epidemiological change and international comparisons in diet demonstrate that dietary differences, such as fat and soy consumption,

may be partially responsible for the phenomena.
Complementary medicine has become an increasing area of interest for patients and researchers around the world. The utilization of some of these therapies by many individuals makes it imperative to understand if they have a role in cancer or other disease treatment. Soy products have generated a large interest because a variety of laboratory and epidemiologic research suggests these items may play a role in the prevention of prostate cancer. Clinical trials are addressing this issue and whether or not these products could also improve prognosis of prostate cancer.
Since the 1940s, medical science has developed chemotherapy, radiation therapy, adjuvant therapy and the newer targeted therapies, as well as refining surgical techniques for removing cancer. Before the development of these modern, evidence-based treatments, 90% of cancer patients died within five years. With modern mainstream treatments, only 34% of cancer patients die within five years. However, while mainstream forms of cancer treatment generally prolong life or permanently cure cancer, most treatments also have side effects ranging from unpleasant to fatal, such as pain, blood clots, fatigue, and infection.
These side effects and the lack of a guarantee that treatment will be successful create appeal for alternative treatments for cancer, which purport to cause fewer side effects or to increase survival rates.
Alternative cancer treatments have typically not undergone properly conducted, well-designed clinical trials, or the results have not been published due to publication bias (a refusal to publish results showing a treatment does not work).
Among those that have been published, the methodology is often poor. A 2006 systematic review of 214 articles covering 198 clinical trials of alternative cancer treatments concluded that almost none conducted dose-ranging studies, which are necessary to ensure that the patients are being given a useful amount of the treatment. These kinds of treatments appear and vanish frequently, and have throughout history. Complementary therapies in Prostate cancer care Macmillan Cancer Relief has commissioned a study in recognition of the value which patientsplace on complementary therapies, of the need of Macmillan post holders (healthcare professionals) for guidance on how to inform their patients, and of the high profile public andmedia attention given to complementary approaches in recent years.
The remit of Macmillan is to care for and support patients in a variety of ways from thetime of first diagnosis. The stated aims of Macmillan are: to help to improve the qualityand availability of care for patients and their families; to address the needs of patients, theirfamilies and their careers; to plan and develop new
services. Addressing psychosocial needs incancer patients – as detailed in the Calman-Hine report (1995) – is a great priority for Macmillan.
However, the impulse to satisfy these needs must be balanced by evidence in support ofcomplementary therapies and the actions of their practitioners. Thisreport confirms that a significant minority of people in the UK use complementary therapies,including up to one third of cancer patients.
Already, many oncology units and hospices offer at least one to patients. There is evidence from focus groups that complementary therapy provision is enthusiastically received by patients, especially for emotional and psychological support. Moreover, interest in these therapies isexpressed by GPs, oncologists, palliative care physicians and Macmillan nurse and medical post holders. Responding to the demand for guidance about these therapies, the orthodox medical bodies are formulating a response. The position statements have been addressed in this report. The therapies shown by surveys to be the most widely used by cancer patients are the touch therapies (aromatherapy, reflexology and massage) and psychological interventions (visualization, meditation and relaxation). Recent studies highlighted in this report suggest that at present cancer patients see these therapies –collectively termed though diverse – mainly as an adjunct to conventional therapy.
Although the evidence base for complementary therapies is still small, that does not imply thatthey are ineffective. Rather, it reflects the fact that only limited resources have been put intotheir research in the past and that many clinical trials have been of poor methodological quality. The two therapies for which the ‘best’ scientific
evidence exists – as far as cancer care isconcerned – are acupuncture for nausea and visualization/meditation for improved quality oflife. For aromatherapy, massage, reflexology and homoeopathy, few formal clinical trials havebeen conducted. Other therapies, presently considered to be outside the mainstream butdiscussed in this report, include healing and naturopathy. However, no therapy has in its favour the kind of evidence that would satisfy a proponent of evidence-based medicine. This report describes some government-funded and locally-funded initiatives that aim to improve thissituation. It should be pointed out that formal ‘evidence’ is important if complementarytherapies are to be considered as ‘treatments’. Research can give some indication of theirsupportive effects through such means as quality of life assessments, but the more intangiblebenefits may prove more difficult to assess. The issues surrounding the provision of thesetherapies are complex. Regulation and organization into professional bodies with anagreed corpus of knowledge and skills is still fairly rudimentary, especially for the therapies most used in cancer care. The recent initiatives taken by the British Medical Association, the
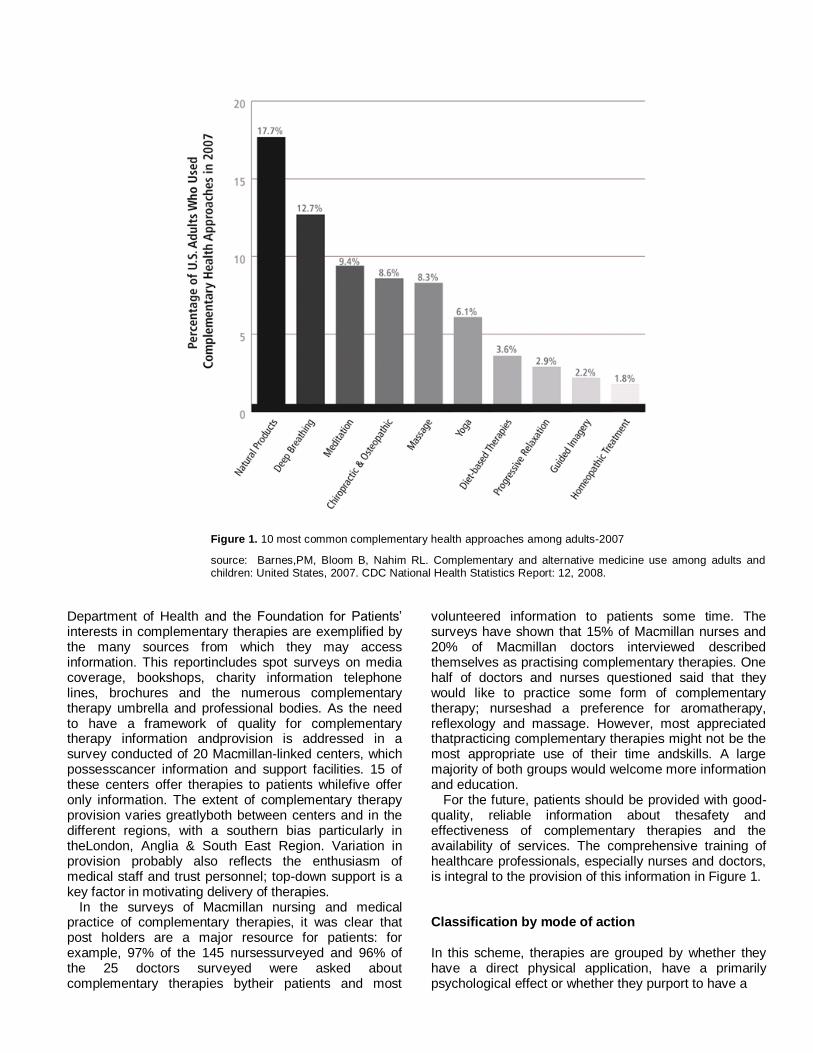
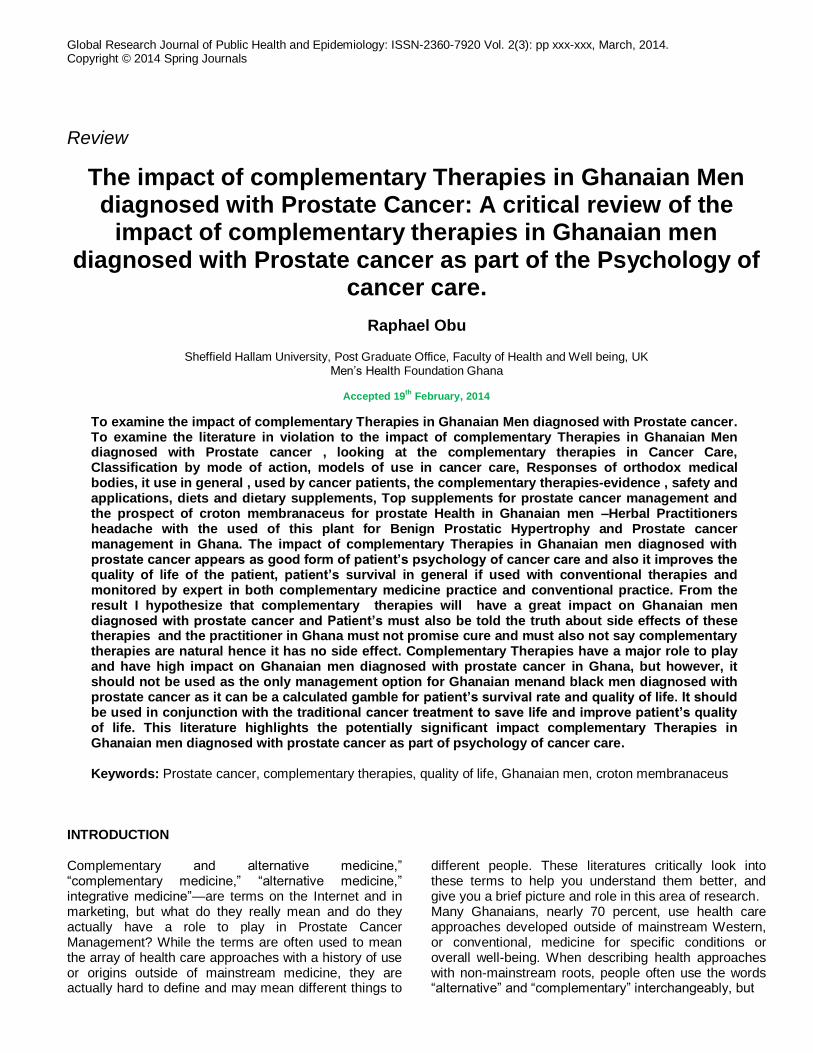
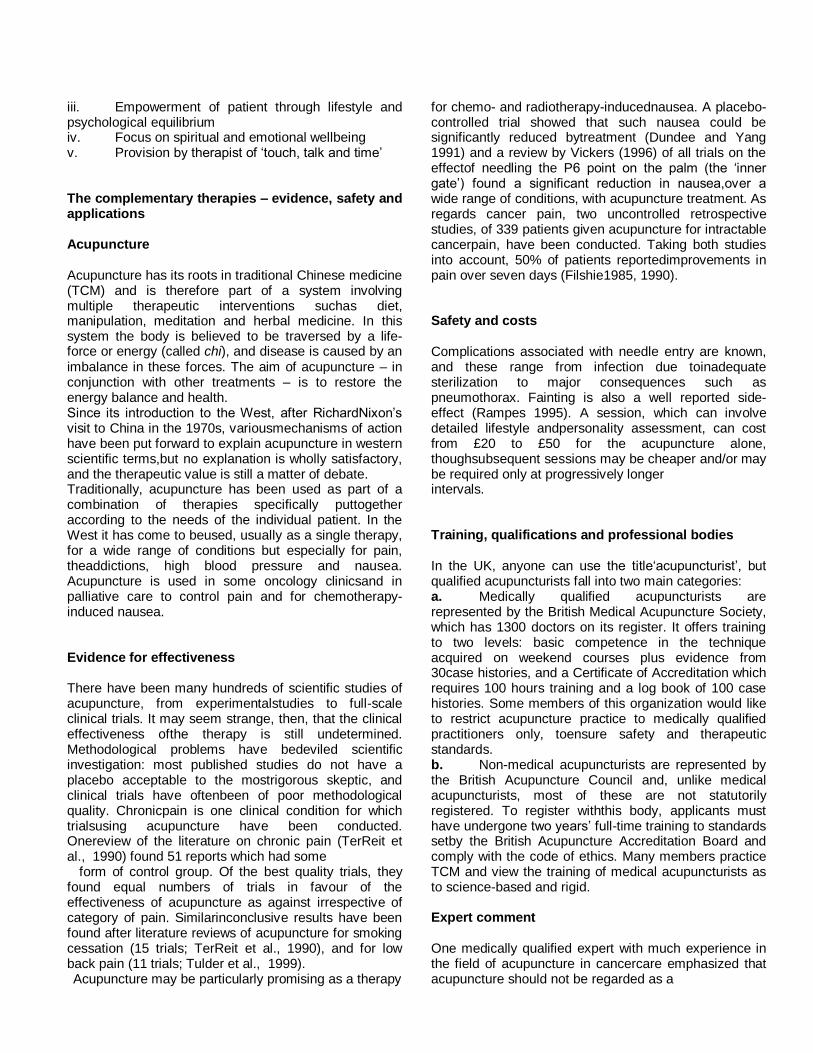
Figure 1. 10 most common complementary health approaches among adults-2007
source: Barnes,PM, Bloom B, Nahim RL. Complementary and alternative medicine use among adults and children: United States, 2007. CDC National Health Statistics Report: 12, 2008.
Department of Health and the Foundation for Patients’ interests in complementary therapies are exemplified by the many sources from which they may access information. This reportincludes spot surveys on media coverage, bookshops, charity information telephone lines, brochures and the numerous complementary therapy umbrella and professional bodies. As the need to have a framework of quality for complementary therapy information andprovision is addressed in a survey conducted of 20 Macmillan-linked centers, which possesscancer information and support facilities. 15 of these centers offer therapies to patients whilefive offer only information. The extent of complementary therapy provision varies greatlyboth between centers and in the different regions, with a southern bias particularly in theLondon, Anglia & South East Region. Variation in provision probably also reflects the enthusiasm of medical staff and trust personnel; top-down support is a key factor in motivating delivery of therapies.
In the surveys of Macmillan nursing and medical practice of complementary therapies, it was clear that post holders are a major resource for patients: for example, 97% of the 145 nursessurveyed and 96% of the 25 doctors surveyed were asked about complementary therapies bytheir patients and most
volunteered information to patients some time. The surveys have shown that 15% of Macmillan nurses and 20% of Macmillan doctors interviewed described themselves as practising complementary therapies. One half of doctors and nurses questioned said that they would like to practice some form of complementary therapy; nurseshad a preference for aromatherapy, reflexology and massage. However, most appreciated thatpracticing complementary therapies might not be the most appropriate use of their time andskills. A large majority of both groups would welcome more information and education.
For the future, patients should be provided with good-quality, reliable information about thesafety and effectiveness of complementary therapies and the availability of services. The comprehensive training of healthcare professionals, especially nurses and doctors, is integral to the provision of this information in Figure 1. Classification by mode of action In this scheme, therapies are grouped by whether they have a direct physical application, have a primarily psychological effect or whether they purport to have a
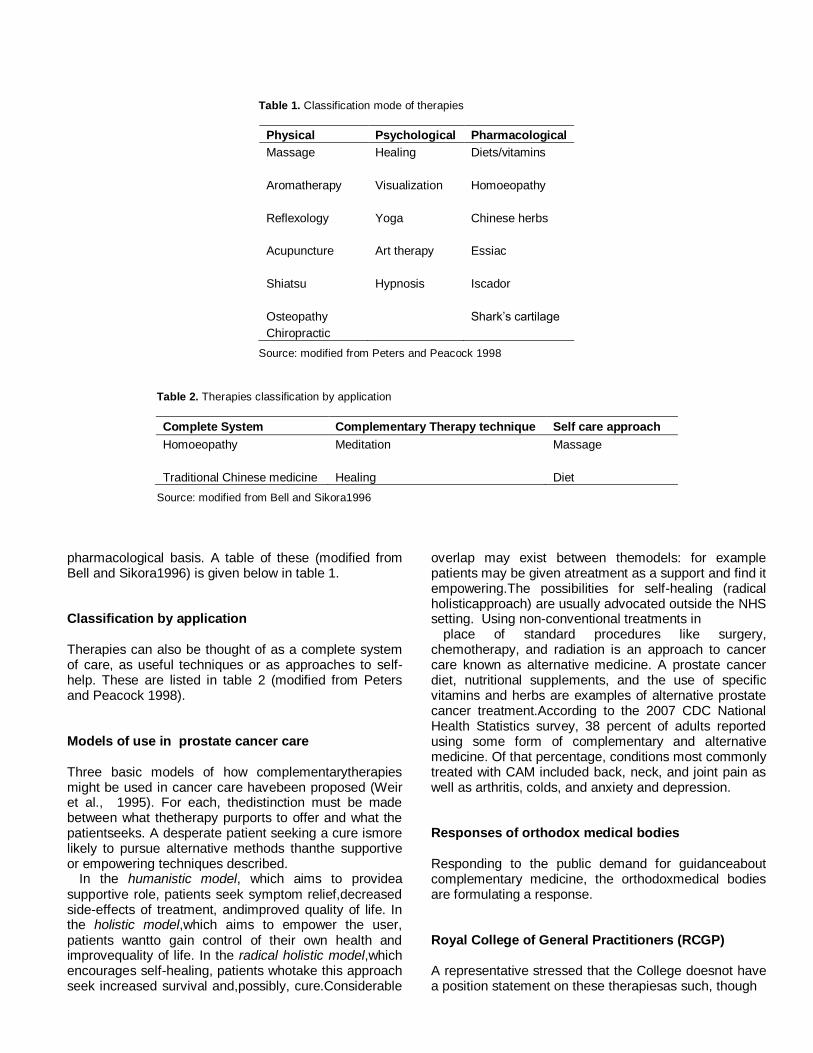
Table 1. Classification mode of therapies
Physical Psychological Pharmacological
Massage Healing Diets/vitamins
Aromatherapy Visualization Homoeopathy
Reflexology Yoga Chinese herbs
Acupuncture Art therapy Essiac
Shiatsu Hypnosis Iscador
Osteopathy Shark’s cartilage
Chiropractic
Source: modified from Peters and Peacock 1998
Table 2. Therapies classification by application
Complete System Complementary Therapy technique Self care approach
Homoeopathy
Meditation Massage
Traditional Chinese medicine Healing Diet
Source: modified from Bell and Sikora1996
pharmacological basis. A table of these (modified from Bell and Sikora1996) is given below in table 1. Classification by application Therapies can also be thought of as a complete system of care, as useful techniques or as approaches to self-help. These are listed in table 2 (modified from Peters and Peacock 1998). Models of use in prostate cancer care Three basic models of how complementarytherapies might be used in cancer care havebeen proposed (Weir et al., 1995). For each, thedistinction must be made between what thetherapy purports to offer and what the patientseeks. A desperate patient seeking a cure ismore likely to pursue alternative methods thanthe supportive or empowering techniques described.
In the humanistic model, which aims to providea supportive role, patients seek symptom relief,decreased side-effects of treatment, andimproved quality of life. In the holistic model,which aims to empower the user, patients wantto gain control of their own health and improvequality of life. In the radical holistic model,which encourages self-healing, patients whotake this approach seek increased survival and,possibly, cure.Considerable
overlap may exist between themodels: for example patients may be given atreatment as a support and find it empowering.The possibilities for self-healing (radical holisticapproach) are usually advocated outside the NHS setting. Using non-conventional treatments in
place of standard procedures like surgery, chemotherapy, and radiation is an approach to cancer care known as alternative medicine. A prostate cancer diet, nutritional supplements, and the use of specific vitamins and herbs are examples of alternative prostate cancer treatment.According to the 2007 CDC National Health Statistics survey, 38 percent of adults reported using some form of complementary and alternative medicine. Of that percentage, conditions most commonly treated with CAM included back, neck, and joint pain as well as arthritis, colds, and anxiety and depression. Responses of orthodox medical bodies Responding to the public demand for guidanceabout complementary medicine, the orthodoxmedical bodies are formulating a response. Royal College of General Practitioners (RCGP) A representative stressed that the College doesnot have a position statement on these therapiesas such, though
it acknowledges that they areused by an increasing number of GPs.
The College emphasized the need for research tovalidate their use, especially for vulnerablecancer patients. Royal College of Nursing (RCN) The RCN has set up its Complementary Therapies in Nursing Forum, established in response to demand from nurses interested incomplementary medicine. It now has some10 000 members. However, as an adviser for cancer care stated,
‘Nurses must not be pressurized into practising complementary therapies as part of the package of care – they must do it only if they are interested, and they must undertake appropriate training.’
The Forum provides educational guidelinesleading use of CAM, alternative, complementary and integrative applications of non-conventional treatment were found to be high among patients with serious illness, like cancer. Smaller studies conducted on cancer patients included the February 2000 statistic issued in the journal Cancer, reporting 37 percent of 46 patients with prostate cancer used one
or more CAM therapies as part of their cancer treatment regime. These treatments included vitamins, prostate cancer diets, and herbal remedies
.
CAM, alternative, complementary and integrative applications of non-conventional treatment were found to be high among patients with serious illness, like cancer. Smaller studies conducted on cancer patients included the February 2000 statistic issued in the journal Cancer, reporting 37 percent of 46 patients with prostate cancer used one or more CAM therapies as part of their cancer treatment regime.
These treatments included vitamins, prostate cancer diets, and herbal remedies
.
The Forum provides educational guidelines andadvises on setting up facilities. It has formulateda business strategy, and has a position statement/statement of beliefs, organizes seminars and meetings and produces anewsletter, In Touch, which promotesnetworking and information aboutcomplementary therapies. As regards theComplementary therapies in cancer care Knowledge baseintroduction of these therapies, a spokespersonsaid,‘We need to be evolutionary, not revolutionary.’ Royal College of Physicians (RCP) Stimulated by the discussion documentproduced by the Foundation for Integrated Medicine (FIM 1997), the RCP has set up acommittee and has circulated a questionnai- re to its fellows to ascertain their attitudes to comple-
mentary medicine.
The RCP has recently published Science-BasedComplementary Medicine (Meade 1998), whichprovides reviews on how to obtain evidence, discussions of any evidence already available,and ways in which evidence is being sought. As the lead spokesperson said,‘Disbelief amongst conventional practitioners has at least been replaced by a healthy scepticism and a clear wish to examine the evidence sensibly and logically.’One member of the committee, focusing on the education and training of medical students, said,‘Doctors need training to have the knowledge and confidence to discusscomplementary therapies with their patients.’ Royal college of surgeons (RCS) A spokesperson agreed that anything that wouldreduce stress would be advantageous, but thatthe RCS would be very much opposed to certainalternative therapies, such as fad diets, whichcan harm patients. For complementary therapies,the importance of evidence of effectiveness fromclinical trials was emphasized,‘At the present time, we are so stretched that without evidence we could not justifyspending money on unproven treatments.’ British medical association (BMA) In recent years the BMA has accepted thatpatients seem to want complementary therapies, and recognized that it must therefore contribute.Some specialists would, however, be prepared togive higher priority to complementary therapies.‘Maybe oncologists would reconsider giving last-ditch chemotherapy to desperately sick patients if they had something else to offer. It may save money from the drug budget.’ Palliative care physician Integration of complementary therapies into orthodox care There is a demand from complementarytherapists for integration into mainstream medicine. However, many treatments are already‘integrated’ in the sense that some NHSprofessionals have also received training incomplementary therapies. Also surveys of GPshave shown that 21% offer a service by amember of the existing primary care team (Wearn and Greenfield 1998). Thus integration, when it occurs, tends to happen in an existingprimary care set-up or a specialist center. Theposition of an independent therapist may appearinsecure in the longer term.Therefore, for successful integration (and delivery to the patient), complementary therapists should acquire biomedical

training atleast at a basic level. They also need otherqualities, such as willingness to compromise and to learn from experience. On theorganizational side, accommodation within a center or unit must be made available andexplicit contracts or service agreements offered.
At the moment provision is based on top-downsupport from physicians or a supportive trust, and guidelines for hiring therapists are locallyimplemented. In an ideal world, provision would not be ‘personality driven’ as at present, andsecure financial agreements would be offered.
The practical issues involved in integratingcomplementary therapies into the NHS havebeen addressed in several recent reports. Overall, use by the public Use in general In 1989 the BMJ reported that 12% of thepopulation had used or were using complementary therapies. The most commonlyused were herbals, manipulation, homoeopathy, acupuncture, hypnotherapy and spiritual healing (Aldridge 1989). In the USA a 1997 surveyrevealed that over 40% of respondents had useda complementary therapy in the preceding 12months, compared with 34% in 1991 (Eisenberg et al., 1998). In Europe, surveys suggest that onethird of people have used complementarymedicine in the previous year and that the number is growing: for example, the use ofhomoeopathy – the most popular of complementary therapies in France – rose from16% of the population in 1982 to 36% in 1992(Fisher and Ward 1994). Use by prostate cancer patients In a study at the Hammersmith Hospital inLondon in 1993 (Burke and Sikora 1993), two-thirds of cancer patients questioned said theywould accept some form of complementarytherapy if it was offered in the hospital: userstended to be younger, of higher social class andfemale.A recent systematic review of the publishedliterature on complementary therapy use byoncology patients to 1998 (Ernst and Cassileth1998) found that rates in the UK varied from16% (Downer et al., 1994) to 32% (Burke and Sikora 1993). In the USA, rates varied between 7% (Eidinger and Schapira 1994) and 54%(Cassilethet al., 1984, 1996). In 1992 a largersurvey in the USA suggested that 9% of patientshad used these approaches (Lerner and Kennedy1992). Comparing UK patterns of use to thoseof the USA reveals an interesting contrast.
Metabolic treatments, diets and megavitaminsare more likely to be taken in the USA (Cassilethet al., 1984).In 1998 the NHS executive for the South Thamesregion commissioned a survey of the use ofthese therapies by women with breast cancer.Early
findings suggest that, of the 1023 womensurveyed, one third of women diagnosed withbreast cancer had visited complementarytherapists since diagnosis, and over one fifth hadused such therapies in the previous 12 months.Costs of treatment were quite modest sincemuch was provided free, and treatment itselfwas more for side-effects of cancer treatment orfor symptoms of cancer than in any hope of acure (Rees et al., 1999). Similarly in the USA arecent study of 480 breast cancer patients hasrevealed that 28% of newly diagnosed breastcancer patients began to use complementarymedicine as an adjunct to conventional therapy(Burstein et al., 1999). Importance of the patients’ views In order to provide optimum patient care, patients’ views are increasingly being taken intoconsideration. The Calman–Hine report recognized the importance of consideringpatients’ and their families’ views on therapeuticprovision in order to address psychosocial needs (Calman and Hine 1995). Patients increasinglyhave a voice through patient and healthprofessional alliances, such as Cancer BACUP, Cancer link and the National Cancer Alliance.
Focus groups and qualitative research studies are ‘In a way I don’t really see how you can compare the two. They have the same effect on you – but one is being done to you and one you are doing yourself.’ Reasons why Prostate cancer patients seek complementary therapies Knowing the reasons why patients seektherapies is fundamental in evaluating their use– that is, distinguishing where possible the factors ‘pushing’ patients away from orthodoxmedicine and those factors ‘pulling’ patients towards complementary therapies. Orthodox medicine Ghana:‘push’ factors i. Failure to produce curative treatments ii. Adverse effects of orthodox medicine, e.g. chemotherapy side-effects iii. Lack of time with practitioner, loss of iv. Bedside skills v. Dissatisfaction with the technical approach vi. Fragmentation of care due to specialization Complementary therapies Ghana: ‘pull’ factors i. Media reports of dramatic improvements produced by complementary therapies ii. Belief that these therapies are natural
iii. Empowerment of patient through lifestyle and psychological equilibrium iv. Focus on spiritual and emotional wellbeing v. Provision by therapist of ‘touch, talk and time’ The complementary therapies – evidence, safety and applications Acupuncture Acupuncture has its roots in traditional Chinese medicine (TCM) and is therefore part of a system involving multiple therapeutic interventions suchas diet, manipulation, meditation and herbal medicine. In this system the body is believed to be traversed by a life-force or energy (called chi), and disease is caused by an imbalance in these forces. The aim of acupuncture – in conjunction with other treatments – is to restore the energy balance and health. Since its introduction to the West, after RichardNixon’s visit to China in the 1970s, variousmechanisms of action have been put forward to explain acupuncture in western scientific terms,but no explanation is wholly satisfactory, and the therapeutic value is still a matter of debate. Traditionally, acupuncture has been used as part of a combination of therapies specifically puttogether according to the needs of the individual patient. In the West it has come to beused, usually as a single therapy, for a wide range of conditions but especially for pain, theaddictions, high blood pressure and nausea. Acupuncture is used in some oncology clinicsand in palliative care to control pain and for chemotherapy-induced nausea. Evidence for effectiveness There have been many hundreds of scientific studies of acupuncture, from experimentalstudies to full-scale clinical trials. It may seem strange, then, that the clinical effectiveness ofthe therapy is still undetermined. Methodological problems have bedeviled scientific investigation: most published studies do not have a placebo acceptable to the mostrigorous skeptic, and clinical trials have oftenbeen of poor methodological quality. Chronicpain is one clinical condition for which trialsusing acupuncture have been conducted. Onereview of the literature on chronic pain (TerReit et al., 1990) found 51 reports which had some
form of control group. Of the best quality trials, they found equal numbers of trials in favour of the effectiveness of acupuncture as against irrespective of category of pain. Similarinconclusive results have been found after literature reviews of acupuncture for smoking cessation (15 trials; TerReit et al., 1990), and for low back pain (11 trials; Tulder et al., 1999). Acupuncture may be particularly promising as a therapy
for chemo- and radiotherapy-inducednausea. A placebo-controlled trial showed that such nausea could be significantly reduced bytreatment (Dundee and Yang 1991) and a review by Vickers (1996) of all trials on the effectof needling the P6 point on the palm (the ‘inner gate’) found a significant reduction in nausea,over a wide range of conditions, with acupuncture treatment. As regards cancer pain, two uncontrolled retrospective studies, of 339 patients given acupuncture for intractable cancerpain, have been conducted. Taking both studies into account, 50% of patients reportedimprovements in pain over seven days (Filshie1985, 1990). Safety and costs Complications associated with needle entry are known, and these range from infection due toinadequate sterilization to major consequences such as pneumothorax. Fainting is also a well reported side-effect (Rampes 1995). A session, which can involve detailed lifestyle andpersonality assessment, can cost from £20 to £50 for the acupuncture alone, thoughsubsequent sessions may be cheaper and/or may be required only at progressively longer intervals. Training, qualifications and professional bodies In the UK, anyone can use the title‘acupuncturist’, but qualified acupuncturists fall into two main categories: a. Medically qualified acupuncturists are represented by the British Medical Acupuncture Society, which has 1300 doctors on its register. It offers training to two levels: basic competence in the technique acquired on weekend courses plus evidence from 30case histories, and a Certificate of Accreditation which requires 100 hours training and a log book of 100 case histories. Some members of this organization would like to restrict acupuncture practice to medically qualified practitioners only, toensure safety and therapeutic standards. b. Non-medical acupuncturists are represented by the British Acupuncture Council and, unlike medical acupuncturists, most of these are not statutorily registered. To register withthis body, applicants must have undergone two years’ full-time training to standards setby the British Acupuncture Accreditation Board and comply with the code of ethics. Many members practice TCM and view the training of medical acupuncturists as to science-based and rigid. Expert comment One medically qualified expert with much experience in the field of acupuncture in cancercare emphasized that acupuncture should not be regarded as a
complementary therapy since it is practiced by mainstream doctors and has‘scientific basis’ in the form of recent neuropharmacological and neurophysiological advances. In relation to cancer care, it was emphasized that its main use is for pain relief and chemotherapy-induced nausea (Thompsonand Filshie 1993). For cancer pain, both TENS (transelectrical nerve stimulation) and acupuncture are used to ‘improve pain control’ sufficiently to allow reduced dosage ofanalgesics and, therefore, reduce side-effects. The expert uses acupuncture for both pain andnausea in patients and feels that there is much scope for its use in cancer care. However, since acupuncture is not without complications, its use should be medically led in cancer patients, and performed by anaesthetists, palliative care physicians and general practitioners. Aromatherapy Many plant species contain essential oils, which give them their distinctive smell. The oils can be condensed from any plant parts by a distillation process to create a very concentrated aromaticsolution. These oils have been associated with healing properties. Practitioners believe that each essential oil can have a particular physiological or psychological effect. The chemical constituents of the oils, in a vegetable carrier, are quickly absorbed through the skin into the bloodstream, and anytherapeutic effect probably results from a combination of a physiological effect of the oils, the relaxation of the massage procedure and the specific effect of the massage on the body. Asoils also excite the sense of smell and thereby elicit certain emotions, the limbic system of themidbrain, concerned with emotional as well as visceral function, may also be involved in theeffect of aromatherapy, including the release of hormones or chemicals in the brain. However,some proponents claim a more ethereal, mysticalrationale for the therapy.
Aromatherapy is said to be useful for stress, since it is said to aid relaxation and sootheemotions, for example by the use of lavender and eucalyptus. It is also used for menstrual anddigestive problems and bacterial infections, and for skin conditions such as acne, eczema andburns. In cancer care, aromatherapy is used for stress management and relaxation, and is oftenprovided by nurses and paramedical staff. Evidence for effectiveness One controlled trial of cardiac surgery patients in intensive care found that the group that received active aromatherapy had significantly less anxiety after five days, but other physiological variables were largely unchanged (Stevensen 1994). Similarly, in one of the few randomized controlled trials of aromatherapy, the
effect of lavender oil for perineal discomfort after childbirth was investigated in 635 women but there was no difference between groups in terms of discomfort at the end of the study (Dale and Cornwall 1994).
As regards cancer care, one uncontrolled study(Kite 1998) investigated the aromatherapyservice at Mount Vernon Centre for Cancer Treatment. Six sessions of aromatherapy weregiven to 58 patients, who at the end of the study showed significant improvements inanxiety and depression. Also, during a trial in 1995, 51 cancer patients had three massagesover three weeks with or without the essential oil roman chamomile. Anxiety was reduced andquality of life improved in the group treated with the oil (Wilkinson 1995, 1996). The small-scale
nature of studies to date makes it difficult to draw conclusions. A CRC-funded multi-centeredrandomized controlled trial – 504 patients in four centers – is currently underway to evaluatethe use of aromatherapy massage and relaxation therapy in improving quality of life in patients with advanced cancer. Safety and costs Undiluted oils can harm skin and should certainly not be taken into the body. There isalso a chance of allergic skin reaction in sensitive people. Some oils can induce a reaction whencombined with sunlight. Costs can range from £30 to £55 per session. Training, qualifications and professional bodies Aromatherapy, like most complementary interventions, is unregulated. However, mostpractitioners belong to the Aromatherapy Organizations Council, which is an umbrellabody for at least 14 aromatherapy organizations and more than 80 colleges involving almost7000 therapists. It runs a range of short- or long-term courses (180 hours in class is astipulated minimum) and national standards are being developed. Expert comment The expert consulted stated that patients are often satisfied with their treatments, but isaware of the need to formally evaluate theeffects of aromatherapy and massage in cancercare. Short-term benefits, in terms of reduced anxiety have been demonstrated but researchhas usually been observational, non-controlled or on small samples. It was emphasized thatcomplementary therapies must be regarded as ‘packages of care’, and this should be borne inmind when designing trials. The importance of the particular qualities of the therapist and thetherapeutic relationship was acknowledged: this is not a failing of the treatment but rather complicates its assessment.
Healing Healing, also known as ‘therapeutic touch’ in the USA, can be defined as the channelling of‘energy’ from a source through a healer to the patient for therapeutic purposes. The source ofthis energy is unknown – it may be God or a natural reservoir in the universe – but the claimis that it can help to stimulate self-healing mechanisms in the patient, promoting alleviationor cure of disease. Conceptually, healing can be divided into two main forms: faith healing,
which is generally carried out in a religious setting and may require faith on the part of thehealer or patient; and spiritual healing, which does not necessarily have a religious basis and isthe modality practiced in the UK. It can occur either during face-to-face sessions betweenhealer and patient, or distantly in the form of ‘absent healing’.The exact mechanism of action is unknown. Onesuggestion is that the human body is anelectromagnet, producing a radiating energy field (which may involve an ‘aura’) that can beaffected by the incoming energy channeled through the healer. Another possibilityadvocated is that the power of love can encourage the spirit body of the patient toreverse disease progression in the physical plane. Healers claim that there are no conditions thatcannot benefit from healing. It can be used to speed up recovery after illnesses treated byorthodox means, to alleviate symptoms and, atleast in principle, to affect a complete cure.
Spiritual healers are allowed to practice in GP surgeries, under the clinical supervision of the GP.A number of surveys have attempted to determine its use by cancer patients. One of these, by Cassileth et al., (1984), found that healing was used though less frequently thandiets or vitamins. Downer et al., (1994) foundthat 16% of cancer patients in the UK usedsome kind of complementary medicine and that healing was one of the most popular. A recentsurvey from Norway found that 74% of cancer patients who used complementary medicinewere using healing either alone or in combination with another therapy (Risberg et al., 1996, 1998). Evidence for effectiveness There is some evidence that visiting a healer can be beneficial. Dixon et al., (1998) showed theclear benefits to chronically ill patients of visiting a healer on the recommendation of a GP.Though this study was not placebo controlled, it indicates that for long-term patients in thecommunity, consulting a healer can have some benefit, for whatever reason. As regards clinical trials, Benor (1992) found a large number of studies on plants, animals and human beings which on balance favoured healing, though many of these were of very poor quality. Of fivegood-quality studies on human physical problems,
three reported a significant effect ofhealing over placebo and two did not. A pilot study recently reported the use of Reiki healingas an aid to pain management in 24 people, some of them with cancer pain, and stated thatthere was a highly significant decrease in pain following healing (Olson and Hanson 1997).
However, there have been no large-scale trials of healing as an adjunctive cancer treatment toallow assessment of its therapeutic effectiveness. Safety and costs There are no reports of adverse effects of healing, beyond disillusion if the treatment failsto have a beneficial effect. Some healers charge nothing at all or merely ask for a contribution, but most ask for £20 (or upwards for arenowned healer) for an hour-long session whichcomprises counseling and healing. Training, qualifications and professional bodies The Confederation of Healing Organizations (CHO) is an umbrella body created to representthe interests of a large number of healing organizations, the largest of which is theNational Federation of Spiritual Healers (NFSH), representing 6500 members. Members of theNFSH conform to very strict ethical guidelines and must complete a two-year probationaryperiod which involves vocational training and case reports of five cases. However, there are nohealing qualifications, and anyone can call themselves a healer. All members of CHO andallied organizations have professional indemnity and public health liability insurance. Expert comment The expert consulted, also a practicing GP, described the ‘healing’ process as the channelling of energy from the healer to the patient. The healer has the intention that thepatient should benefit, not unlike most healthcare professionals. In response to thequestion of using healing for physical healing, the expert stated that extraordinary things canhappen. For cancer patients, outcomes might be feeling better, having more energy, or reevaluating their purpose in life. The expert stated, ‘Spiritual issues are often paramount in answering the questions, Why me? Why cancer?’ It was emphasized that although palliative care teams and hospices are often excellent atproviding psychological support, they do not focus on spiritual support and care. Healing isabout encouraging self-healing – emotional, mental, spiritual and perhaps physical – through care and compassion. Though a supporter of evidence-based medicine, the expert pointed to difficulties in measuring outcomes when a
range of variables is involved. The exaggerated claimsmade by certain healers were acknowledged. Charismatic healers are the worst things about spiritual healing. They give spiritualhealing a bad name.’ Homoeopathy The German physician Samuel Hahnemann claimed to rediscover the ancient principle that‘like can treat like’, a concept known to the ancient Greeks. In his law of minimal dose hecodified the belief that ‘ultradilution’ of a substance can increase its potential to curedisease. Accordingly, homoeopathic remedies areprepared from a ‘mother tincture’ – the originalsolution of the substance – which is diluted down in successive steps. At each step, thesolution is given a vigorous shake (‘successed’), and homoeopaths believe that the power of the
diluted solution to heal is conferred (‘potentization’ occurs) during these successiveshakes. There is great debate about how this might occur, or indeed whether it is occurring atall. The most prevalent view is that the ‘power’ generated during ‘potentization’ is stored in chemical form, perhaps through a lasting alteration to the structure of the water (the‘memory of water’ theory) presently undetectable by science. The therapeutic effectmight be transferred to the patient via an unknown mechanism. Homoeopathy claims to treat the ‘whole person’– not
just the local symptoms of the disease – by boosting a dysfunctional ‘self-healing mechanism’. Homoeopaths therefore prescribe aremedy that is specific to a particular patient at a particular time. According to home theory, there is no disease that cannot in principle be treated. Like other complementary therapies, homoeopathic remedies tend to be most used by patients for the chronic conditionsfor which orthodoxy has no cure, such as asthma, chronic pain and emotional problems. Ina survey of cancer patients in the UK, 16% reported using some form of complementary oeopathic medicine: homoeopathy was one of the mostfrequently used therapies (Downer et al., 1994). Evidence for effectiveness The most rigorous overview of clinical trials was conducted by Kleinjenet al., (1991) after areview of all the scientific literature. This group found a total of 107 controlled trials over a largenumber of different conditions, from respiratory diseases to psychological problems. Though thequality of trials was very variable, overall 81 reported positive results for homoeopathy and24 found no benefit of homoeopathy over placebo. Of the 22 best-quality trials, 15 showeda benefit of homoeopathy and 7 showed no benefit. An extension and re-analysis of this review in the Lancet (Linde et al., 1997) arrived at essentially the same conclusions.
One trial,comparing the effects of a homoeopathy preparation of grass seed pollen and placebo in144 hay-fever sufferers (Reilly 1986) found a significant reduction in symptoms in thetreatment group. As regards cancer care, a pilot study from theGlasgow Homoeopathic Hospital in 1995 found a significant reduction in stress in 21 out of 50patients with breast cancer who survived to six month follow-up. There have also been someclaims, published in Health Which? in 1997, that homoeopathy can reduce the hot flushessometimes caused by chemotherapy. Theconventional view, however, is that homoeopathy is not appropriate as a single cure for life-threatening conditions. To 1999, there have been no good quality trials of homoeopathic remedies for cancer. Safety and costs As most true homoeopathic remedies have either no molecules of the original solution left,or so few as to be negligible, there is usually little chance of direct harm. However, there have been some reports of contaminated products. Homoeopaths report that ‘aggravations’ ofsymptoms can occur shortly after start of treatment, but claim these are minor andtransient.First consultation can cost between £30 and£100, with cheaper follow-up appointments. Inaddition, GPs can prescribe remedies and canrefer patients to one of the homoeopathic hospitals. Training, qualifications and professional bodies Homoeopathy is the only complementary therapy to have a Faculty of Homoeopathy totrain medical doctors, and five NHS-funded hospitals. Anyone can use the title‘homoeopath’, but there are two categories of professional training available: a. Medical homoeopaths, who take a six-monthexamined postgraduate course at the Facultyof Homoeopathy, become registered and abide by the code of conduct: there arepresently over 400 of these. b. Non-medical homoeopaths, who take a three-year full-time course organized by theSociety of Homoeopaths, after which they become members, abide by the code ofconduct and use the letters RSHom. Currently, there are over 1100 members Expert comment The expert consulted, who has had many years’ experience in treating cancer patients and whoworks in an acute NHS Trust Hospital, stressed the importance of auditing practice todemonstrate patient satisfaction and effectiveness. The expert’s philosophy is that since cancer is a multifactorial and enigmatic disease, a multifactorial approach should be adopted in its
treatment. Usually, the advice given extends beyond prescribing a homoeopathic remedy. Since diet, stress, genetics, environmental and other factors maybe implicated in the origin of the disease, these areas are addressed as part of the holisticapproach. The suggestion that patients influence their disease, rather than expect cure,is key to the contribution from this expert. It was emphasized that medically trained
Homoeopaths are to be preferred, since they understand theydisease process and know when the patients require other interventions.
Another medical homoeopath reinforced theimportance of being guided by the patient,‘The approach is narrative-based. It is observational.’ Massage therapy Massage is a generic term for a variety of techniques which involve touching, pressing orkneading the surfaces of the body to promote mental and physical relaxation. Types range fromtraditional Thai massage to the Ayurvedicmarma. The precise tissues and points that are stimulated, and how the massage therapist connects with them, depend on the culture fromwhich the technique has originated and the philosophy on which it is based. Westernmassage, such as the kind used by sports therapists, concentrates on the structures andphysiology of the body as recognized by orthodox western science. By direct stimulationof skin and underlying tissues, massage can relieve tension and stimulate circulation,indirectly promoting relaxation and the benefits that accrue from it.
Massage is used primarily for musculo-skeletal pain, since part of the pain experienced is oftencaused by the tension caused in guarding the body against pain. Massage can relieve thisadditional pain by helping the body to relax. Similarly, it is also used for stress-relatedproblems such as tension headaches, sleeplessness, sciatica and migraine. Somepractitioners claim that it can help conditions such as asthma and irritable bowel syndrome. Evidence for effectiveness Despite many anecdotal claims for the effectiveness of massage to relieve anxiety anddepression, and for the relief of pain, when Vickers (1996) reviewed the literature on theeffectiveness of massage the results were disappointing. Good-quality conclusive studieswere few, and overall there was no goodevidence that massage relieved pain. Thisfinding, however, is counterintuitive and probably says more about the paucity of goodresearch than the effectiveness of massage. In a research paper in 1994 from the MacmillanPractice Development Unit at the Institute of Cancer Research, London, 52 cancer
Patients undergoing an eight-week course of massage reported significantly reduced anxiety and decreased physical and emotional symptoms (Corner, 1994). In another study of massage forcancer pain, 60% of patients said their pain was reduced after a 30-minute massage, and thiswas confirmed by physiological tests (Ferrel-Tory and Glick 1993). In another report, post mastectomylymphoedema was reduced by massage (Becker 1990), while a study at theLiverpool Marie Curie Centre followed 87 patients who had been referred for massage andhad completed the course; 71 of these completed a postal questionnaire, and mostfound the experience of massage beneficial (Wilkinson 1995, 1996).
While these results are intriguing, massage urgently requires further evaluation if it is toprove its worth as a specific therapy. It is nevertheless widely used in the NHS cancer careunits, and anecdotal benefits are claimed. Safety and costs As eastern types of massage can be quite vigorous, there may be some pain and discomfort after a massage session. Patients should be relatively safe in the hands of atrained therapist, though anyone with underlying disease of the bones, varicose veins, blood clots or severe back pain should seek medical advice first. Indeed it is always wise toseek medical advice. A one-hour session can cost upwards of £25. Training, qualifications and professional bodies Massage therapists are unregulated, and there are several hundred training colleges in the UKwith over 60 kinds of massage qualifications. British Massage Therapy Council is preparing alist oforganizations and drawing up a registration procedure for practitioners and a training programme. There is also the Massage Therapy Institute of Great Britain. The ShiatsuSociety has a register of practitioners, and members conform to a code of practice andethics. Massage is widely available inside the NHS, and is provided by trained therapists, suchas nurses/paramedical staff (dual training) and trained volunteers. Expert comment The expert consulted was a research practitioner who had published a critique of themethodology of research studies evaluating massage. She concluded that, after analysis, the methods employed varied so greatly between studies that it was difficult to make any firmconclusion about the effectiveness of massage.
‘We need to replicate existing studies rather than
constantly changing the methodology.We need to draw on the knowledge gainedfrom earlier studies.’ Naturopathy, diets and herbals This section outlines the use of these therapiesand is not intended as a detailed critique. Naturopathy The term ‘naturopathy’ actually covers a range of therapies, and within it patients might finddiets and various physical techniques. The philosophy is that ‘natural cures’ can give thebody the maximum opportunity to heal itself without interference. In the UK, the term is usedto describe a core of ‘therapies’ arranged around the principles of dietary advice (includingfasting), hydrotherapy and exercise. Training, qualifications and professional bodies In the UK, naturopathy has traditionally beenassociated with osteopathy and some naturopaths today are also osteopaths. It is represented by the General Council and Registerof Naturopaths (with 180 members in 1997) and the Register of Nutritional Therapists Ltd (with95 members in 1997). Expert comment The view of the expert consulted was that the aim of naturopathy is to help the individualrestore his/her normal function to as near its healthy level as possible.‘A naturopath is creating health, not treatingdisease.’
It uses a careful nutritional approach combined with controlled exercise and positive thinking: foods should preferably be organic, though the diet should not be too restrictive. Patients should eat things with high nutritional value. The basic idea is that the therapy ‘will initially releaseenergy’ within the patient. The mistake made bydieticians, in the view of this expert, is to pushfood on to patients when they cannot ‘use it’ optimally. In cancer patients naturopathy might ‘stimulate the immune system, prevent blocks in energy, and contain the cancer’. Diets and dietary supplements Diet and supplements are extensively used by the general population, but are also proposedfor certain conditions. The following are three examples with relevance to cancer care.
The Gerson diet Developed in Germany, this diet consists of mainly fresh organic fruit and vegetableswith emphasis on those parts with a high potassium content. Sodium is restricted.
There are other additional ingredients, such as vitamin B12 and royal jelly. Gerson himselfmade great claims for the use of the diet in cancer (Gerson 1978), but further evidence from randomised clinical trials is needed to support its use as a therapy. Some cancer patients have used this diet, but it is rigorous and requires commitment to see it through. Prostate diet for prostate cancer and prostate health Cancer experts and nutrition and diet studies estimate that our food choices account for up to 90 percent of cancers of the prostate, breast, pancreas, and colon. Even lung cancer is believed to have a dietary link. If you’re skeptical, consider the rates of prostate cancer in China compared with those in North America. In 2002, there were 1.6 cases of prostate cancer for every 100,000
males in China, compared with 120 cases per 100,000 in North America. That’s 75 times the rate in China! (Parkin 2005)
Experts believe that a major part of the reason for the difference prostate cancer rates is diet. According to the World Health Organization (WHO)“diets high in red meat, dairy products, and animal fat have frequently been implicated in the development of prostate cancer”.The traditional Chinese diet consists of vegetables, fish, sea vegetables, fiber-rich foods, and a small amount of soy, a fare that is typically low in saturated fat and sugar. The SAD—Standard American Diet—is true to its name: high in saturated fat and sugar, low in fruits, vegetables, fish, and fiber. When you combine SAD with our notoriously couch-potato lifestyle, you have the formula for the alarming rise in lifestyle-related diseases, especially obesity, that we are surrounded with today in Western countries.
SAD is a disaster as are many of the fad and gimmick diets on the market. The Prostate Diet for Prostate Cancer is a sensible eating plan designed to promote and maintain prostate health by safeguarding against inflammation and cancer, as well as maximizing overall wellness. Vitamin supplements Vitamin supplements are seen by some as complementary therapies. Much research isbeing undertaken within orthodox science to assess the effectiveness of vitaminsupplementation. In cancer care,
Figure 2. Cayenne Pepper Prostate Benefits
there is limited evidence for the recommendation ofvitamins A, C and E as supplements for patients, though it is essentially inconclusiveand falls short of indubitable scientific proof of efficacy (Canadian Breast Cancer ResearchInitiative, Vitamin A, C and E supplements, 1996). As vitamins can interact with eachother and with other medications, the use of supplementation by cancer patients should be done under the care of a physician. Shark’s cartilage Shark’s cartilage is thought to contain a factor that inhibits the development of the blood supply to a tumour, preventing angiogenesis. As a result, supporters argue that the tumour can be starved of its necessary nutrients. They claim that it worksbeston solid tumours, as these need substantial new blood vessels to grow. The scientific basis for the use of shark’s cartilage is the finding that sharks infrequently getcancer. No clinical controlled studies of the effectiveness of shark’s cartilage have beenpublished, despite the thousands of cancer patients who have bought and used it (Markman 1996). This suggests that, despite extensive commercial publicity, the productoffers unsubstantiated benefit to cancer patients. Cayenne pepper prostate benefits Hot and spicy, the cayenne pepper (Capsicum annuum) figure 2 is a member of the Capsicum family of vegetables, which you may know better as chili peppers. The pepper got its name because it was cultivated in a town named Cayenne in French Guiana in South America.
Cayenne pepper, which is also known as African pepper, capsicum fruit, grains of paradise, and Zanzibar pepper, is hot and spicy largely because it has a high
concentration of a substance called capsaicin. In scientific circles capsaicin is largely recognized for its pain-reducing abilities. It has also, however, demonstrated a talent for helping kill cancer cells, including prostate cancer cells. Cayenne and prostate cancer What has research shown us about cayenne (capsaicin) and prostate health?
In a laboratory study published in 2007, scientists found that capsaicin slowed growth of prostate cancer cells and encouraged them to “commit suicide” (apoptosis). (Sanchez 2007)
In a more recent study (April 2009), Italian researchers reported that capsaicin can induce apoptosis (cell destruction) in prostate cancer cells. (Ziglioli 2009)
A study performed at the University of California, Los Angeles, showed capsaicin tohave what the researchers called a “profound antiproliferatgive effect on prostate cancer cells,” inducing cell suicide and leading them to note that capsaicin “may have a role in the management of prostate cancer.” (Mori 2006)Researchers who conducted a study at Nottingham University and published it in 2007 reported that they found how and why capsaicin kills cancer cells: it attacks the mitochondria, the energy-generating portion of cells. The family of molecules to which capsaicin belongs, called the vanilloids, attach to proteins in the cancer cell mitochondria and trigger apoptosis without harming the surrounding healthy cells. (Athanasiou, 2007). Genistein Figure 3: Genistein, an antioxidant and is of lav one found primarily in soybeans and soybean products, has

Figure 3. Genistein
demonstrated an ability to fight prostate cancer in a number of studies. In test tube and animal studies, researchers have shown that genistein can interfere with the growth of prostate cancer cells and help prevent the spread of prostate cancer (metastasis). A study conducted at Northwestern University was the first to show that genistein could prevent the spread of prostate cancer in living organisms (mice). In a University of Alabama, Birmingham, study, scientists found that genistein induced apoptosis in prostate cancer cells, while the combination of genistein and resveratrol successfully decreased proliferation of prostate cancer cells in rats. The preferred way to get genistein is in soybeans and soy foods, such as tofu, miso, and soy beverages. Genistein and prostate cancer Genistein health benefits include possible help in lowering prostate cancer risk. Studies have shown that when men ate more foods rich in genistein (e.g., tofu, soybeans), there was a lower incidence of prostate cancer, while lower intake of genistein was associated with higher rates of cancer. (Moline 2009)
Genstein is an isoflavone and a phytoestrogen, a substance found in plants that has estrogen-like properties. The antioxidant abilities of genistein may make it helpful in fighting prostate disease.In test tube studies, scientists have also shown that genistein hinders the growth of prostate cancer cells. (Raffoul 2006; Kazi 2003) A research team at Northwestern University went a step beyond and found that genistein fights human prostate cancers that have been implanted in mice.
Although the genistein health benefits did not include elimination of the cancer or tumor shrinkage, the cancer cells were prevented from spreading. It was also the first
study to show that one of genistein health benefits could be the prevention of the spread of prostate cancer in a living organism. (Lakshman 2008)
Another study from Northwestern University reported on how genistein could help fight prostate cancer. The scientists identified MEK4 as a pro-invasion protein and the target for genistein in prostate cancer cells. The authors concluded they had found a possible link between high dietary consumption of foods that contain genistein and a lower rate of prostate cancer metastasis and death. (Xu 2009)More recently, researchers at the University of Alabama, Birmingham, reported on the effects of genistein or resveratrol alone and in combination in rats with induced prostate cancer. They found that a high-dose combination decreased proliferation of prostate cancer cells and that genistein as a single agent induced cell suicide. (Harper 2009). Green tea Figure 4. Green tea and green tea supplements contain potent antioxidants known as catechins. Research shows that catechins, including the most powerful one discovered thus far—epigallocatechingallate (EGCG)—have an ability to fight prostate cancer, as well as boost the immune system. In a recent Cancer Prevention Research article, experts noted that EGCG and other polyphenols significantly reduced the levels of PSA and two indicators for prostate cancer in men who had the disease. Results of several large studies show that men who drink green tea regularly are less likely to develop prostate cancer than men who avoid the beverage. The more green tea men drink, the more they protect their prostate against cancer. Green tea catechins also benefit men who have pre-cancerous prostate lesions, a condition known as prostate intraepithelial neoplasia(PIN),which indicates a high risk of developing prostate cancer. Three or more cups of green tea daily

Figure 4. Green tea and green tea supplements
are often recommended, or consider a green tea extract supplement. Green tea catechins (EGCG) The medicinal powers attributed to green tea come from catechins, potent antioxidants that boast an array of health-promoting properties. For starters, they can destroy certain bacteria and viruses, enhance the immune system, and combat several forms of cancer, including prostate cancer. Although there are several different kinds of catechins, the most powerful is epigallocatechingallate, EGCG.The amount of catechin in green tea varies depending on where the tea is cultivated, the diversity of plants used, the harvest season, and how it is processed. Generally, Japanese green tea has a greater EGCG content than does Chinese tea, but within these two categories there are
differences as well. According to an analysis of EGCG content in different types of green tea conducted by the authors of Foods to Fight Cancer, Senchauchiyama (a Japanese green tea) is superior to a dozen other Japanese and Chinese green tea varieties. (Beliveau 2007)Other Japanese green teas that rank high in EGCG content include Gyokuro, Sencha, and Matcha. The most nutrient rich green tea is Matcha, which contains 10 times the amount of EGCG than other green teas. When choosing Matcha green tea, select one from Japan that has been steamed, not roasted or pan-fried, and that has been stone ground into a fine powder. These processing details are what make Matcha green tea nutritionally superior to other green teas.
Although Matcha green tea takes a little longer to prepare, the extra time (and higher cost) are well worth the health benefits. Chinese green tea that is roughly equivalent to Matcha is pitochun emperor; other Chinese
green teas that have a lesser amount of EGCG than Matcha and Pilochun emperor are YHunnan, Yuzan, Paimutan, Meng ding, Lung chin, Dong ding, Pouchong, and Tikuan yin. Regardless of which green tea you buy, choose organic. Types of tea The four main types of tea are white, green, oolong, and black, yet they all come from the same plant, Camellia sinensis. Processing is what determines the “color” and the qualities of each types of tea.
White tea is the least processed. The leaves are picked before they even open up, and at that point they are covered with fuzzy white hairs, which gives the tea its name. The leaves are simply steamed and dried. Studies indicate that white tea offers more antioxidant properties than the other teas, but it is much more difficult to find in stores.
Oolong tea (or wu long) is a combination of green and black leaves, which are partly fermented, which makes it stronger than green tea but more delicate than black teas, which are fully fermented. Black tea, the type most commonly consumed around the world, undergoes the most processing before it makes its way into teabags. To make black tea, the leaves are oxidized, which means they are exposed to the air for a specific amount of time to allow natural chemical
reactions to occur. These reactions change the leaves’ color from green to copper and intensify their flavor until it is rich.
Green teas are not oxidized; instead the leaves are allowed to wither and dry without processing. The lack of oxidation allows the leaves to retain the essential substances that give green tea its potent properties. Green tea and prostate cancer The ability of green tea to impact prostate cancer is impressive. Studies of large populations of men have shown that those who consume green tea regularly are less likely to develop prostate cancer than men who do not drink the beverage. (Heilbrun 1986; Jain 1998) In other studies, researchers found that the risk of prostate cancer decreases proportionally as the amount, frequency, and duration of green tea consumption increases. (Jian 2004)In terms of amount of tea consumed, men who drank more than three cups of green tea daily showed a reduced risk of prostate cancer. In a large study that evaluated the green tea drinking habits of 49,920 men aged 40 to 69 who were followed for at least 10 years, the investigators found that men who consumed five or more cups of green tea daily had a reduced risk of advanced prostate cancer when compared with men who drank less than one cup daily. (Kurahashi 2008)
Seven prostate cancer benefits of green tea
It interferes with the activity of an enzyme called ortnithine decarboxylase, which plays a role in the “birth” of prostate cancer (Gupta 1999)
It slows the growth of human prostate cancer cells and prompts them to “commit suicide” (apoptosis) (Gupta, Ahmad 2000)
It encourages the repair of damaged DNA that might otherwise promote cancer growth (Butt 2009)
It inhibits the activity of an enzyme called COX-2, which accumulates in prostate cancer tissue and is involved in the prostate cancer process. (Hussein, Gupta 2005). Research shows that prescription medications called COX-2 inhibitors, such as celecoxib (Celebrex) have the ability to slow the growth of prostate cancer in animal models. However, a recent study published in Clinical Cancer Research shows that the EGCG found in green tea was nearly as effective as COX-2 inhibitors in slowing the growth of prostate cancer. (Adhami 2007)
It stimulates the activity of certain immune system cells that fight cancer tumors. (Butt 2009)
In a study published in the journal Cancer Prevention Research in June 2009, researchers reported that green tea polyphenols, primarily EGCG, significantly reduced the levels of PSA. The study included 26 men who had prostate cancer and who were scheduled for radical prostatectomy. (McLarty 2009)
It also appears that catechins may benefit men who have pre-cancerous prostate lesions (prostate intraepithelial neoplasia, or PIN), a condition that indicates a high risk of developing prostate cancer. Studies indicate that 30 percent of men who have a high-grade PIN go on to develop prostate cancer within one year after repeated biopsy. In a 2006 study published in Cancer Research, 60 men who had high-grade PIN participated in the double-blind, placebo-controlled study. (Bettuzzi 2006) Men in the treatment group received three 200-mg capsules of catechins daily. After one year, only one tumor was diagnosed among the 30 treated men, compared with nine cancers found among the 30 controls. As a “bonus,” the researchers also noticed that the men who took the catechins had reduced lower urinary tract symptoms, which suggests catechins may be helpful in treating symptoms of BPH. Lycopene Figure 5. Lycopene, a plant pigment found in high concentrations in tomatoes, guava, watermelon, and several other foods, has demonstrated the ability to help prevent and fight prostate cancer. Most studies of the impact of lycopene on prostate health have involved tomatoes and tomato products, and the results have been impressive. In one long-term study of about 14,000 participants, investigators found that men who ate five or

Figure 5. Lycopene
more servings of tomatoes or tomato products each week had a significantly lower risk of developing prostate cancer than men who consumed less than one serving per week. A report in the Journal of the National Cancer Institute reveals that men who consumed lots of tomatoes and tomato products had a 35 percent reduced risk of developing prostate cancer and a 53 percent lower risk of getting an aggressive form of the disease. The most beneficial way to get lycopene is through diet, not supplements, and processed tomato foods are the best food sources. Most lycopene supplements are oil-based and available as soft gels. A recommended dose is 10 mg daily. Lycopene and prostate cancer Study after study has shown that lycopene has properties that enhance prostate health. For example:
One of the first studies to suggest that tomatoes might help prevent prostate cancer was conducted in the late 1970s in a group of approximately 14,000 Seventh-day Adventists (this religious group is largely vegetarian). All the participants completed a food-frequency questionnaire. After six years of follow-up, 180 men were diagnosed with prostate cancer. When food consumption was analyzed along with the incidence of prostate cancer, the investigators found that the risk of developing prostate cancer was significantly lower in men who consumed five or more servings of tomatoes or tomato products each week compared with men who consumed less than one serving per week. They also noted that the men who were at reduced risk of prostate cancer also consumed greater amounts of beans, lentils, peas, and dried fruit. (Mills 1989)
Lycopene may help prevent the worsening of prostate enlargement that occurs in BPH. Researchers
from Germany’s University of Hohenheim studied 40 elderly men with BPH who were randomly assigned to take either 15 mg lycopene or a placebo daily for six months. (Schwarz et al 2008) The results were encouraging: among the men who took the lycopene, PSA levels fell and the prostate did not grow larger. In the placebo group, however, the PSA did not decline and the prostate grew larger.
A Brazilian study was designed to evaluate the impact of lycopene on prostate biology. (Edinger 2006) Men with BPH who consumed 50 grams of tomato paste daily for 10 weeks had a decline in their PSA levels by an average of 10.77 percent when compared with levels before starting the study.
In a Yale University study, researchers looked at the role of lycopene in prostate cancer among blacks and whites. They found that men who had lower levels of the antioxidant in their blood or prostate tissue were more likely to develop the disease than those who had higher levels, and that blacks tended to have lower levels of lycopene. (Vogt 2002)
A large study (about 48,000 men), published in the Journal of the National Cancer Institute found that eating lots of tomatoes, tomato sauce, tomato juice, and pizza was associated with a 35 percent reduced risk of developing prostate cancer and a 53 percent lower risk of getting aggressive prostate cancer. (Giovannuci 1995)
The authors of a 2009 paper that evaluated the relationship between diet and prostate cancer noted that “There is accumulating evidence to support the consumption of lycopene, in particular tomato and tomato-based products, as protective factors against prostate cancer.” (Chan 2009) Just how many tomatoes should you eat? Researchers from Germany’s University of Bonn state that just one serving of tomatoes or a tomato product every day could protect against the DNA

Figure 6. Magnolia Bark tree
Figure 7. Mushrooms
damage that may set the stage for prostate cancer. (Ellinger 2006)
A Canadian study that used a mouse model reported that lycopene combined with selenium and vitamin E was effective in inhibiting prostate cancer, while selenium and vitamin E without lycopene was not. Thus the researchers concluded that lycopene is an essential component of the selenium/vitamin E combination in helping to prevent prostate cancer. (Venkateswaran 2009)Not every study has praised the ability of lycopene and tomatoes to fight prostate cancer and protect the prostate, however, while some have reported a mixed results.
Experts at the University of Bonn, Germany, reviewed the studies that have explored the value of tomatoes/lycopene in the prevention and treatment of prostate cancer and/or benign prostate hyperplasia. They found that although studies on BPH and tomatoes/tomato products did not show any evidence that these foods helped prevent BPH, most of the interventional trials showed that consumption of tomatoes and tomato products may probably protect against prostate cancer, at least low-grade cancer. They also reported that tomato products might be used in the treatment of BPH and prostate cancer, but that consuming lycopene alone does not protect from the development of prostate cancer. (Ellinger 2009)
In the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial, investigators found no association between lycopene or other carotenoids and prostate cancer, but they did see an association between increased risk for aggressive, clinically relevant prostate cancer and intake of beta-carotene. Magnolia Bark Figure 6. Bark of the magnolia tree contains several active ingredients, including magnolol, which some scientists have identified as having anticancer properties. Preliminary laboratory study results indicate that magnolol can prompt human prostate cancer cells to commit suicide (apoptosis). Subsequent lab studies have also shown that magnolol can stop the development, invasion, growth, and metastasis (spread) of prostate cancer cells. Anyone wanting to take magnolia bark supplements should consult their healthcare provider before beginning treatment. Mushrooms Figure 7. Extracts of Asian mushrooms, including cordyceps, maitake, oyster, reishi, and shiitake, contain components that are valued for their ability to fight cancer, including prostate cancer. One of those

components is ergosterol peroxide, which research indicates has an impact on human prostate cancer cells by triggering cell suicide (apoptosis) and inhibiting cell growth. Extracts from reishi mushrooms demonstrated both antitumor and immune-stimulating properties in one study, while other research shows that shiitake and cordyceps mushrooms contain anticancer and immune-boosting compounds as well. Asian mushrooms also contain the antioxidant L-ergothioneine, which appears to protect cells from substances that could damage them and result in cancer. AHCC mushroom prostate health benefits Mushrooms offer great benefits for overall health, including their ability to help fight cancer. Asian mushrooms in particular have been used for their medicinal powers by the Chinese for more than 6,000 years.
Asian mushrooms come in dozens of varieties, and some of the ones most recognized in the United States include shiitake, maitake, reishi, oyster, and cordyceps. Although you can benefit from eating Asian mushrooms, supplements that contain mushroom extracts also provide healing components. Anticancer properties of mushrooms One of those components is ergosterol peroxide, which researchers found to be effective against human prostate cancer cells. (Russo 2010) Specifically, they found that ergosterol peroxide inhibited cancer cell growth and triggered cell suicide (apoptosis), which prompted the researchers to say their findings “confirm the use of mushrooms as origin of compounds to be used as novel therapeutic agents for prostate cancer treatment.”
Cancer Research UK, the leading funder of cancer research in the United Kingdom, reports that medicinal mushrooms have the ability to restrict tumor spread (metastasis) and antitumor activity. Research shows that shiitake and cordyceps, for example, contain several active compounds that have anticancer activity and can enhance the immune system rather than attack cancer cells directly. These compounds are used to help support immune function in cancer patients during chemotherapy and radiation and can prolong survival times in some types of cancer. (Cancer Research UK)
Extracts from another Asian fungus, reishi mushrooms, are used to stimulate the immune system in cancer patients. The active substances in reishi mushrooms have both antitumor and immune stimulating properties. (Mao 1999)
A mushroom compound called polysaccharopeptide (PSP), which can be extracted from the turkey tail mushroom, demonstrated an ability to target prostate
cancer stem cells and suppress the formation of prostate tumors in a mouse study. According to the senior research fellow Dr. Patrick Ling at Queensland University of Technology, “In the past, other inhibitors tested in research trials have been shown to be up to 70 percent effective, but we’re seeing 100 percent of this tumour prevented from developing with PSP.” While conventional therapies are effective in targeting certain cancer cells, PSP was shown to focus on cancer stem cells, which initiate cancer and cause its progression. Ling noted, however, that although turkey tail mushrooms possess health benefits, individuals cannot reap the same benefits found in his research from eating the mushrooms. (Ling 2011)
A review article in the journal Clinical and Experimental Metastasis recently identified and reported on the specific mechanisms responsible for reishi mushroom extract’s ability to suppress cancer invasion and metastasis. The authors noted that more in vitro and in vivo tests as well as clinical trials are necessary to better understand these effects. (Weng 2010)
Shiitake, maitake, oyster and reishi mushrooms also contain a powerful antioxidant called L-ergothioneine. Scientists at Johns Hopkins University School of Medicine reported that ergothioneine has a role in protecting cells from damage from toxins and other substances that could result in the development of cancer. (Paul 2009). Mushrooms and BPH Reishi also seem to have another benefit. In the Journal of Ethnopharmacology, researchers reported that extracts of reishi may be useful for the treatment of benign prostatic hypertrophy. (Fujita 2005) In the study, the mushroom extract significantly inhibited hormone-driven growth of the prostate in lab animals.
In a randomized, double-blind, placebo-controlled study using reishi mushroom extract, 88 men who had lower urinary tract symptoms, characteristic of BPH, were assigned to take either 6 mg of mushroom extract or placebo daily for 12 weeks. Men in the treatment group had a significant improvement in the International Prostate Symptom Score and variables of uroflowmetry. (Nogushi 2008)
In a recent study published in Chemistry and Biodiversity, treatment with reishi extract significantly inhibited the testosterone-induced growth of the prostate in rats. This finding indicated that reishi mushroom extract may be helpful in the treatment of benign prostatic hyperplasia or prostate cancer. (Liu, 2009). AHCC: A promising natural therapy for prostate cancer What is AHCC? AHCC, short for active hexose correlated compound, is
a hybridized extract of medicinal mushrooms — specifically the mycelia (or underground portion) of shiitake mushrooms. The subject of 30 PubMed-listed published studies confirming its immuno-modulating capabilities, AHCC is used in over 700 clinics worldwide. Unlike conventional cancer treatments, AHCC has a strong safety profile, with no side effects. This is not surprising, as mushroom mycelia have been consumed as food since antiquity and have a long tradition of medicinal use in Japan.
AHCC is unique in that while most mushrooms contain primarily betaglucans, AHCC is very rich in alpha-glucans, a different type of polysaccharide with very potent immunomodulating properties. Due to a patented manufacturing process, AHCC has a low molecular weight (under 5,000 daltons, as compared to 200,000 daltons for most medical mushrooms). The small size of AHCC molecules translates to increased absorption and increased efficacy compared to traditional shiitake, maitake, and reishi extracts. AHCC and immune function The job of the immune system is to protect the body from foreign organisms such as bacteria, viruses, fungi, and cancer cells. Therefore, cancer is ultimately a failure of the immune system. AHCC enhances immune function by increasing numbers of several key types of cells and molecules.
Cytokines are messengers that allow the immune system to organize a response to an infection or another threat to the body, such as cancer. A study in healthy elderly people demonstrated that AHCC increases the production of cytokines, such as INF-γ and TNF-α.
Natural killer (NK) cells are white blood cells that serve as the body’s first line of defense. They recognize and destroy infected or cancerous cells by injecting material into them that causes them to swell and explode. Human studies have shown that AHCC can increase the activity of NK cells by 200-300 percent. Specifically, AHCC makes NK cells more effective by increasing their ability to bind to tumor cells. Macrophages engulf and destroy bacteria. AHCC has been demonstrated to increase populations of these cells by up to 100 percent.
Dendritic cells are white blood cells that present foreign substances to B and T cells, which then destroy them. AHCC significantly increases numbers of dendritic cells. AHCC and cancer treatment AHCC has been used worldwide to treat many kinds of cancer. Although there have not been numerous large-scale randomized controlled trials yet conducted, many
human studies have pointed its efficacy in treating cancer.
A cohort trial of liver cancer patients who had undergone hepatectomy (partial removal of the liver) found that among patients who received AHCC, only 39 out of 113 suffered a recurrence of their cancer (34.5 percent), while 72 out 109 patients in the control group did (66 percent) — nearly twice as many. Moreover, survival rates in the AHCC group were significantly better than those in the control group.
AHCC also helps patients with gastric and colon cancers. When used in combination with chemotherapy, AHCC improved five-year survival rates of early-stage gastric cancer patients and late-stage colon cancer patients.
Another clinical study of late-stage liver cancer patients found that subjects who took AHCC survived for an average of 3.5 months, while those in the control group survived just 1.5 months. In fact, after 3.5 months, the entire control group had passed away, while 61.5 percent of the AHCC group was still alive. AHCC and Quality of Life AHCC has no side effects and can even help ameliorate the side effects of cancer treatments. Using both physical and mental criteria after three months of AHCC treatment, researchers found that the quality of life of liver cancer patients was significantly improved. Another study found AHCC helped ease the debilitating side effects of chemotherapy for patients with late-stage head and neck cancers. The subjects had better appetites, felt stronger, and reported less nausea and vomiting when they took AHCC. Their white blood cell counts also improved and they suffered less constipation. AHCC and Prostate Cancer Prostate-specific antigen (PSA) is a protein secreted by the prostate that is found in the blood of healthy men. However, elevated or rising PSA levels can signal prostate cancer.
Some clinical evidence indicates that AHCC lowers PSA levels while other research has shown that AHCC stabilizes PSA but without causing a reduction. Even in the case of the latter findings, the ability to stabilize PSA levels with a very safe natural compound provides a significant benefit for the patient.
A study of 11 advanced cancer patients (three with prostate cancer) found that the PSA levels of the prostate cancer patients began dropping significantly after 1-2 months of treatment and had fallen to normal levels by 4 months.
Published case reports have come to similar conclusions. One such report described the case of a prostate cancer patient whose cancer had metastasized

Figure 8. AHCC Mushroom
Figure 9. Omega-3 Fatty Acids
to his bones and who had not responded to androgen deprivation therapy. On treatment with AHCC, his PSA levels dropped from 69.3 ng/ml to just 1.5 ng/ml. His bone cancer became stable and his pain and ability to walk were improved.
One human clinical trial found that 39 of 62 prostate cancer patients treated with AHCC for six months either had stable or falling PSA levels. Moreover, when the data was further analyzed, it was found that older patients and those whose cancer had metastasized had the most stable PSA levels, although the trend was not statistically significant.
Another study of 74 patients showed that while AHCC did not lower PSA levels, the patients’ PSA levels remained stable. This was an interesting finding, considering that PSA levels would be expected to rise in the normal progression of the disease. Therefore, AHCC may be a good treatment option for late-stage prostate cancer patients.
While large-scale, randomized double-blind studies are needed to reach decisive conclusions, the evidence thus far indicates that AHCC is a safe, natural compound with no known side effects that holds promise in the treatment of prostate cancer by helping reduce or stabilize PSA levels while improving patients’ quality of life (Figure 8. AHCC Mushroom below). AHCC Mushroom Omega-3 Fatty Acids Figure 9 is Omega-3 Fatty Acids, of the three types of omega-3s—EPA (eicosapentaenoic acid), DHA (docosahexaenoic acid), and ALA (alpha-linolenic acid), EPA and DHA provide the most health benefits. Specifically, these polyunsaturated fats help prevent
prostate cancer cell growth. In a large Swedish study, experts found that men who consumed the most EPA and DHA had a 30 percent less risk of developing prostate cancer than men who consumed the least amount. A Harvard study of more than 20,000 men found that among men diagnosed with prostate cancer, those who ate fish at least five times a week had a 48 percent lower risk of dying from the disease than men who ate fish less than once a week. Men may want to follow the recommendations of the American Heart Association and take 0.5 to 1.8 grams of EPA and DHA daily either as supplements or eat omega-3 rich fish (e.g., salmon, halibut, sardines, tuna). Omega 3 fatty acid and prostate cancer Omega 3 and prostate cancer are making the news again. Omega 3 is considered an essential fatty acid for a number of reasons, not the least of which may be its benefit in promoting prostate health and in reducing the risk of prostate cancer. There are several reputable studies on the health benefits for Omega 3 and prostate cancer. Here is what we know so far from the studies: University of California, San Francisco One of the most promising studies about the benefits of omega-3s and prostate health was conducted by researchers from the University of California, San Francisco, and published in 2009. The investigators evaluated 466 men who had aggressive prostate cancer and 478 healthy men. All the men were asked to complete questionnaires about the foods they ate daily. They also were screened for a variant of the COX-2 gene that is known to increase a man’s risk for developing prostate cancer.
When the researchers analyzed all the collected data, they discovered that the men who ate dark, fatty fish rich in EPA/DHA (e.g., salmon) at least once a week had a 63 percent reduced risk of developing prostate cancer. The men who consumed little or no EPA/DHA and who also had the COX-2 variant were five times more likely to develop advanced prostate cancer. (Fradet, 2009). Harvard school of public health At the Harvard School of Public Health, researchers followed more than 20,000 men to determine the relationship between prostate cancer and fish consumption. A total of 20,167 men who were part of the Physician’s Health Study were evaluated. Although the investigators did not find an association between how much fish the men ate and prostate cancer, they did find that eating fish had an impact on cancer survival rates. In fact, of the men in the study who were diagnosed with
prostate cancer, those who ate fish at least five times a week had a 48 percent lower risk of dying from the disease than the men who ate fish less than once a week. (Chavarro 2008) CAPS study (cancer prostate in Sweden) A large Swedish study also evaluated the relationship between intake of fatty fish and prostate cancer. A total of 1,499 men who had prostate cancer who were already part of the CAPS study (Cancer Prostate in Sweden) were monitored along with 1,130 men who were cancer-free at the beginning of the study. The researchers determined that the risk of prostate cancer was 43 percent lower in men who consumed “salmon-like fish” one or more times per week when compared with men who never ate that type of fatty fish. The investigators also analyzed the men’s intake of
EPA and DHA and found that the men who consumed the highest amount of marine fatty acids (both EPA and DHA) had a 30 percent less risk than men who consumed the least amount of EPA and DHA. Another finding was that men who possessed a variant of the COX-2 gene and who ate the most salmon-like fish has a 72 percent lower risk for prostate cancer when compared with men who had the COX-2 gene variant and ate the least amount of salmon-type fish. And one more thing: the researchers also determined that a high intake of linoleic acid (an omega-6 fatty acid) increased the risk of prostate cancer. (Hedelin 2007) Harvard school of public health Researchers from the Harvard School of Public Health followed 47,866 men who had participated in the Health Professional Follow Up Study from 1986 until 2000. (Leitzmann 2004) The men were asked to complete food-frequency questionnaires and to include specific details about their use of cooking oil, the amount of dark-meat fish they ate, and if they used fish oil supplements. In the final analysis, the researchers found that consumption of ALA from meats, plants, and dairy sources increase the risk of advanced prostate cancer, while a high intake of EPA and DHA was associated with a decreased risk of total and advanced prostate cancer.
Plasma Phospholipid Fatty Acids and Prostate Cancer Risk in the SELECT Trial
This flawed study from 2013, which stated that Omega 3 might actually cause prostate cancer, made all the headlines and made men taking these supplements safely for years panic. The study was a retrospective study that was called “scientifically weak” by prostate cancer expert, Dr. Anthony Victor D’Amico. It did not show cause and effect, and this study did not account for well-known risk factors such as age, race, BMI, PSA, or DRE. It made a weak association between omega 3 and

Figure 10. Pectin
Figure 11. modified citrus pectin
prostate cancer despite numerous studies stating the opposite. Pectin Pectin (figure 10) is a complex carbohydrate found in between the cell walls of some plants. Several laboratory studies have shown that pectin may promote cell suicide (apoptosis) and inhibit the spread of human prostate cancer cells. In human subjects, the use of modified citrus pectin in men who had prostate cancer showed that pectin may extend the PSA doubling time in men who have recurrent prostate cancer. At this time, no definitive dose of citrus pectin has been determined, and anyone interested in taking pectin supplements should consult their healthcare provider.
Modified Citrus Pectin – Natural Treatment for Prostate Cancer? “Along with diet, exercise and lifestyle changes, Modified Citrus Pectin helps my patients keep the cancer at bay and slows its growth, thereby reducing its negative impact on their life,” says Dr. Geo Espinosa, Director of the Integrative Urology Center at NYU.(Figure 11) What is Modified Citrus Pectin? Modified citrus pectin (MCP) is a form of pectin, a complex polysaccharide (a type of carbohydrate) that is composed of thousands of sugar molecules chemically bound together.

Pectin is present in most plant cell walls and also in the region between plant cells where the cells bind together.
The pulp and peels of citrus fruits have especially concentrated amounts of pectin. Apples, guava, quince, and plums also contain pectin. Pectin is widely used as a gelling ingredient in canned foods and jellies, and in the production of food, cosmetics, and some anti-diarrhea medications. Modified citrus pectin and prostate cancer Numerous animal and human studies have found that modified citrus pectin may inhibit the spread of prostate cancer.
In a recent study published in Integrative Cancer Studies, scientists from Columbia University Medical Center analyzed and tested two forms of a brand of modified citrus pectin, 1.0% PectaSoland 1.0% PectaSol-C, to determine their impact on prostate cancer in the lab. The investigators used both androgen-dependent and androgen-independent human prostate cancer cell lines, two similar prostate cancer cell lines from mice, and a noncancerous human benign prostate hyperplasia cell line in their analyses.
Testing revealed that both PectaSol and PectaSol-C performed similarly against both human prostate cancer cell lines and BPH cells, while PectaSol-C performed slightly better than PectaSolagainst mouse prostate cancer cell lines. The study’s authors concluded that both PectaSoland PectaSol-C inhibited cell proliferation and apoptosis in human and mouse prostate cancer cell lines, and that 1.0% PectaSol-C should be used in additional chemopreventive and chemotherapy evaluation in animal and human studies. (Yan 2010)
At an International Conference on Diet and Prevention of Cancer held in Finland in 1999, Dr. Stephen Strum, an oncologist specializing in prostate cancer, and his team reported that five of seven men who had advanced prostate cancer and who had not responded to conventional therapy experienced a positive response after taking modified citrus pectin daily for three months or longer. The positive response was in the form of an increase in PSA doubling time. One of the five men had no increase in PSA level at all. (Strum, 1999)
In subsequent research that also involved Dr. Strum, investigators conducted a phase II pilot study and evaluated the efficacy and tolerability of modified citrus pectin (Pecta-Sol) in 13 men who had prostate cancer and prostate-specific antigen (PSA) failure after they underwent radiation, cryosurgery, or radical prostatectomy. Ten men were evaluated for efficacy and 13 for tolerability. After taking modified citrus pectin for 12 months, the PSA doubling time increased in 7 (70%) of 10 men compared with before taking the supplement. Even though this study lacked a control group, the results suggest that modified citrus pectin may increase
PSA doubling time in men who have recurrent prostate cancer. (Guess 2003)
In an earlier rat study, researchers explored the ability of modified citrus pectin to inhibit the binding of rat prostate cancer cells to endothelial cells. Rats were injected with prostate cancer cells and then divided into groups that received 0.0%, 0.01%, 0.1%, or 1.0% modified citrus pectin continuously in their water from day 4 after the injection until day 30, when the researchers counted the number of tumor colonies in the lungs.
By day 30, compared with the rats in the 0.0% and 0.01% groups, half of the 14 rats in the 0.1% group and nine of 16 in the 1.0% group had significant reductions in cancer that spread to the lungs (lung metastases). The lungs of the rats treated with 1.0% modified citrus pectin had significantly fewer colonies of lung metastases than did the rats in the two control groups. Modified citrus pectin did not have an effect on the growth of the primary tumors, however. In a petri dish, modified citrus pectin inhibited binding of the rat prostate cancer cells to rat endothelial cells. (Pienta 1995)
The results of the studies performed thus far suggest modified citrus pectin is helpful in reducing the growth and spread of prostate cancer. Large, randomized controlled trials are needed to support and verify these findings.
“Along with diet, exercise and lifestyle changes, Modified Citrus Pectin helps my patients keep the cancer at bay and slows its growth, thereby reducing its negative impact on their life,” says Dr. Geo Espinosa, Director of the Integrative Urology Center at NYU. Pomegranate A growing number of studies are demonstrating the anticancer abilities of pomegranate (figure 12a) extracts in the fight against prostate cancer. In test-tube and animal studies, researchers have shown that pomegranate extracts can slow the reproduction of prostate cancer cells, promote apoptosis (cell suicide), and hinder the growth of new blood vessels, which tumors need for nourishment and to survive. A University of Quebec study reported that four compounds present in pomegranates—delphinidin chloride, epigallocatechingallate, kaempferol, and punicic acid, and especially the latter—inhibited prostate cell growth. In another study, pomegranate juice significantly extended the time for PSA levels to double in men who had undergone treatment for prostate cancer, while University of California, Riverside, investigators note they have identified the components of pomegranate that are responsible for the fruit’s beneficial effects. Men interested in including pomegranate in their lifestyle can choose between pomegranate juice and supplements.

Figure 12a. Pomegranate
Figure 12b. Pomegranate
Pomegranates and prostate cancer The pomegranate is a round shrub or small tree native to the Middle East and Asia that produces a pomegranate fruit (figure 12b) characterized by a distinctive leathery outer rind and juicy seeds surrounded by white, spongy tissue. Pomegranates are rich in antioxidants, and in particular a prostate-friendly phytonutrient called ellagitannin.
Test-tube studies have shown that pomegranate extracts can slow the reproduction of prostate cancer cells and encourage the cells to commit suicide, a process called apoptosis. (Seeram 2005) Other test-tube and animal studies have indicated that pomegranate extracts called ellagitannins can hinder the growth of new blood vessels, which are necessary to nourish prostate tumors. (Sartippour 2008)
A University of California, Los Angeles study evaluated the effects of pomegranate in men who had had surgery or radiation for prostate cancer but whose PSA levels had risen, which indicated that the cancer may be
returning. When the study began the men’s average PSA level doubled every 15 months. The men were then given 8 ounces of pomegranate juice to drink daily. By the end of the study, it was taking 54 months for the average PSA level to double, cancer cell apoptosis had increased by 17 percent, and proliferation of cancer cells had declined by 12 percent. These findings suggested that the disease progression had slowed, and that pomegranate was involved. (Pantuck 2006)
In a 2010 study from the University of Quebec, researchers exposed human prostate cancer cells to 13 compounds present in pomegranates and found that four—epigallocatechingallate, delphinidin chloride, kaempferol, and punicic acid–inhibited cell growth stimulated by dihydrotestosterone (DHT). In particular, punicic acid, the main constituent of pomegranate seed, inhibited cell growth. (Gasmi 2010)
As a side benefit, several studies provide evidence that pomegranate may have a role in treating erectile dysfunction. In one animal study, investigators compared pomegranate juice, red wine, green tea, and several

Figure 13. Quercetin
berry juices and found that pomegranate juice showed the most antioxidant capacity. Long-term intake of pomegranate juice improved erectile function and prevented erectile tissue fibrosis. (Azadozoi) A study of men with mild to moderate erectile dysfunction found that pomegranate juice intake resulted in some improvement in erectile function, although the improvement was not significant. (Forest)
Fresh pomegranate is the best way to get all the nutrients from this fruit. Quercetin Quercetin health benefits can be gotten from in many plants and foods, most notably red grapes, red wine, apples, tea, berries, and onions. For more than a decade, quercetin has been recognized as a potent antioxidant that has strong anti-inflammatory and anti-allergy effects. It is inhibiting the production and release of histamine and other inflammatory factors (figure 13). Quercetin for BPH, Prostatitis and Prostate Cancer Quercetin is also used to relieve symptoms for men with BPH, prostatitis and prostate cancer. It has been identified as being especially beneficial for BPH and in cases of prostatitis in numerous clinical studies, usually at a dose of 500 mg daily. Chronic nonbacterial prostatitis/chronic pelvic pain In a randomized, double-blind study published in Urology, 28 men who had chronic nonbacterial
prostatitis/chronic pelvic pain syndrome took either placebo or500 mg of quercetin twice a day for one month. The authors also conducted a follow-up unblind, open-label study that involved an additional 17 men who received a supplement that contained quercetin, as well as saw palmetto, bromelain, cranberry, and papain.
At the end of the month, the International Prostate Symptom Score (IPSS) fell from 21.0 to 13.1 in the quercetin group and from 20.2 to 18.8 in the placebo group. An improvement in symptoms of at least 25 percent was reported by 20 percent of patient taking placebo and 67 percent of patients taking quercetin. In the 17 patients who took the Quercetin supplement, 82 percent had at least a 25 percent improvement in their symptom score. Overall, the authors noted that quercetin“provides significant symptomatic improvement” in men who have chronic nonbacterial prostatitis/chronic pelvic pain syndrome. (Shoskes, 1999). Quercetin health benefits for bacterial prostatitis A prospective, randomized study was conducted to determine the therapeutic effect of quercetin and curcumin and saw palmetto and stinging nettle extracts compared with the antibiotic prulifloxacin in men who had chronic bacterial prostatitis. A total of 143 patients were enrolled, and they were split into two groups: Group A (106 patients) received both prulifloxacin (600 mg daily) plus ProstaMEV and FlogMEV for 14 days; Group B (37 men) received the antibiotic only. After one month, 89.6 percent of men who received the herbal formulas had no symptoms of prostatitis compared with only 27 percent of the men in the antibiotic-only group.

Six months after the intervention portion of the study ended, no patients in Group A had recurrent of prostatitis compared with two patients in Group B. The authors concluded that the association of quercetin, curcumin, saw palmetto, and stinging nettle extracts can improve the clinical efficacy of prulifloxacin in men who have chronic bacterial prostatitis. (Cai, 2009) Quercetin health benefits for chronic prostatitis A more recent study was conducted at Cleveland Clinic and included 100 men who had chronic prostatitis/chronic pelvic pain syndrome. The study used a multimodel therapy based on the UPOINT phenotype (e.g., urinary: alpha blocker or antimuscarinic; organ-specific: quercetin; tenderness: physical therapy; psychosocial; infection; and neurologic/systemic). The men participated in the therapy for 26 weeks, and the main endpoint was a minimum 6-point decline in NIH-Chronic Prostatitis Symptom Index (CPSI). A median of 3 UPOINT domains were positive: organ-
specific (70%), tenderness (64%), and urinary (59%). At a median 50-week follow-up, 84 percent of the men had a least a 6-point decline in CPSI. The number of domains and initial CPSI were not predictors of a man’s response. Although no one domain predicted outcome, quercetin use was associated with a greater CPSI decrease. (Shoskes, 2010). Quercetin health benefits for prostate cancer Based on previous research that showed quercetin to possess antitumor activity, investigators at State University of New York at Buffalo studied the effect of quercetin on the ability of prostate cancer cell lines to form colonies. They observed that at concentrations of 25 and 50 micro M,quercetin significantly inhibited the growth of both moderately aggressive DU-145 prostate cancer and highly aggressive PC-3 prostate cancer cell lines, but had no affect on the poorly aggressive LNCaP prostate cancer cell line. Quercetin also significantly inhibited the expression of certain oncogenes and genes that control specific phases of the cell cycle and “reciprocally up-regulated the expression of several tumor suppressor genes.” The authors concluded that their results “provide a scientific basis for the potential use of flavonoids as nutraceuticals in the chemoprevention of cancer.” (Nair 2004)
Quercetin has also demonstrated the ability to interrupt the spread of prostate cancer (metastases) and to promote cell death. A study published in Molecular and Cellular Biochemistry reported that quercetin was able to decrease the activity of specific enzymes known to be involved in tumor invasion and metastases. This finding led the authors to note that quercetin could be developed as a chemopreventive agent for metastatic
prostate cancer. (Vijayababu 2006) The ability of quercetin to promote and enhance cell death in human prostate cancer cell lines has also been shown in several studies conducted at the University of Pittsburgh. (Kim 2007; Lee 2008) A more recent study from the University of Madras suggests that quercetin can decrease the survival of androgen-independent prostate cancer cells by changing the expression of insulin-like growth factor signaling and inducing apoptosis, which could make the supplement useful in cancer patients. (Senthilkumark, 2010). Quercetin health benefits for BPH In a study published in the Journal of Endocrinology, scientists reported on their evaluation of the effect of quercetin and the drug finasteride (Proscar) on the prostate gland in rats. Administration of quercetin (doses of 50, 100, or 150 mg quercetin per kg of body weight) along with finasteride resulted in a 31.8%, 40.0%, and 48.2% reduction, respectively, in prostate weight. The authors concluded that quercetin works with finasteride to reduce prostate weight through a cell cycle-related pathway that may function independent of androgens. (Ma 2004) Resveratrol Resveratrol health benefits include many healing properties as a phytonutrient and a potent antioxidant. But resveratrol also has other healing properties, as demonstrated in a recent study conducted by researchers from the US Department of Agriculture (figure 14). (Hudson 2008) The scientists found that resveratrol slowed the growth of prostate cancer cells, which led them to suggest that the phytonutrient may be helpful in preventing the growth of the cancer in its early stages. Resveratrol also can reduce the activity of substances that cause inflammation in the body. Although studies show that resveratrol can inhibit the proliferation of various cancer cell lines, it is not known whether high intakes of resveratrol can help prevent cancer in humans. The anti-inflammatory properties of resveratrol health benefits came into play in a study at Stanford University, in which researchers noted that up-regulation of MKP5 by resveratrol may contribute to its actions against prostate cancer by decreasing inflammation of the prostate. (Nonn 2007) A University of Missouri study looked at various botanical compounds, including resveratrol, and found that it was effective in inhibiting the growth of both human and mouse prostate cancer cell lines. (Slusarz 2010) At New York Medical College, scientists evaluated the impact of two resveratrol analogues in cultured human
Figure 14. Resveratrol
Figure 15. red wine
prostate cancer cells. They found that the analogues were active against different stages of the prostate cancer cells. (Hsieh 2010) A collaborative effort among researchers from three institutions in Virginia set out to identify the mechanisms behind resveratrol’s ability to inhibit cell growth and induce apoptosis. Their research indicated that certain transcription factors mediate the anti-proliferative and pro-apoptotic benefits of resveratrol, partly due to activation of a specific pathway. These findings help support claims regarding resveratrol’s anticancer properties. (Chen 2010) In a Japanese study, researchers explored how resveratrol inhibits the function of androgen receptors, which have a key role in the development of prostate cancer. In a laboratory experiment, they discovered that resveratrol inhibits DNA binding of androgen receptors, which furthers the understanding of how resveratrol health benefits may be helpful in fighting prostate cancer. (Harada, 2011). How Ghanaian men can get resveratrol health benefits Drinking red wine is one way to get resveratrol, but individuals would need to drink a great deal of wine to
get any possible medicinal benefits. Resveratrol supplements can serve as a logical alternative (figure 14). Most resveratrol supplements in the United States contain extracts of Polygonumcuspidatum, which is also known as Japanese knotweed, Hu Zhang, or kojo-kon. Others contain extracts of red wine and red grapes, although Japanese knotweed is a cheaper source of resveratrol. There is some debate about whether knotweed supplements are inferior to those made from red grapes or red wine extract, but so far no studies have come to a conclusion on either side of the question. However, we suggest you look for brands that use red grape and red wine extracts. Supplements typically contain 10 to 50 mg of resveratrol, but effective doses for humans are not known. Turmeric Turmeric/Curcumin and Prostate Cancer Turmeric (Curcuma longa) is a member of the ginger family (figure 15). The roots of the plant are ground into the spice that is the mainstay of curry, but it also responsible for making mustard yellow. The active ingredient in turmeric is curcumin, which
Figure 16. Turmeric
gives the spice its peppery, bitter taste. Turmeric has long been used as an anti-inflammatory
and in the treatment of colds and asthma in both Chinese and Indian medicine systems. Scientists have also found that turmeric/curcumin
appears to have cancer-fighting properties. Turmeric/curcumin and prostate cancer studies
Scientists at Rutgers, The State University of New Jersey, had noticed that in contrast to the high incidence of prostate cancer in the United States, disease incidence in India is very low. It has been suggested that this difference may be related to the fact that Indians consume large amounts of plant-based foods that are rich in phytochemicals, which have been shown to protect against disease. To see if this might be true, the researchers used mice that were injected with human prostate cancer cell lines to grow tumors so they could test certain compounds—namely turmeric and a nutrient found incruciferous vegetables (e.g., broccoli, cabbage, kale, cauliflower, turnips, and others). The scientists found that turmeric (curcumin) may be effective in the prevention and treatment of prostate cancer. (Khor 2006)
An Oregon Health and Science University study published in 2009 reported that curcumin has “potential anti-metastatic effects in bone-derived prostate cancer cells.” (Herman 2009)
A Columbia University report noted that turmeric “is a novel and potent inducer of apoptosis [cell death] in both androgen-dependent and androgen-independent prostate cancer cells.” and that “curcumin may provide an alternative, nontoxic modality by which the clinician may prevent the progression of prostate cancer…or to treat advanced prostate cancer by forcing them to
undergo apoptosis (cancer cell destruction).” (Dorai 2000). Vitamin D It is important for men to get enough vitamin D for prostate health (figure 16). That’s because the body converts vitamin D into several factors that help prevent the reproduction of prostate cancer cells as well as hinder their ability to spread throughout the body. Research also supports the idea that a vitamin D deficiency increases the risk of developing prostate cancer, including a 2009 report in the British Journal of Urology International in which investigators found that men with prostate cancer were more likely to have low levels of the vitamin compared to men without the disease. Experts vary on the amount of vitamin D men need for prostate health, but the Vitamin D Council is joined by other authorities in recommending taking enough vitamin D (about 5,000 IU daily) to maintain a blood level between 50 and 80 ng/mL. Your healthcare provider can arrange a blood test to identify your vitamin D needs. Vitamin D and prostate cancer Vitamin D and prostate cancer are connected (figure 17). Here is some of the latest research on vitamin D as it applies to prostate cancer and prostate health as well as heart disease, bone health, diabetes, and colon cancer. Vitamin D is a substance that functions like a vitamin
(as a fat-soluble vitamin it is stored in fat tissue in the body), but it is also a hormone. Its many activities include regulating bone health, muscle health, immune system response, insulin and blood sugar levels, and calcium and phosphorus metabolism.
Figure 17. Vitamin D
Figure 18. Vitamin D and Prostate Cancer
Vitamin D (in the form of D3) is manufactured by the body through exposure to sunlight and it can also be obtained from a limited number of foods, and through supplements. The body also needs co-factors in order to properly utilize vitamin D. These include magnesium, zinc, vitamin K, boron, and small amounts of vitamin A. Vitamin D and prostate health Although the connection of vitamin D and prostate cancer remains controversial, some researchers have found evidence that a vitamin D deficiency increases the risk of developing prostate cancer. In the British Journal of Urology International, investigators reported that men with prostate cancer were more likely to have low levels of vitamin D compared with men who did not have the disease. (Trump 2009) Figure18.
Also, in a smaller study published in BJU International in November 2009, 26 men who had prostate cancer were given a daily dose of vitamin D. The PSA levels in
five men declined: two by more than 50 percent, two by 25 to 50 percent, and in one by less than 25 percent. In the remaining patients, their PSA levels stabilized after treatment with vitamin D for up to 36 months. (Newsom-Davis 2009)
Vitamin D may also impact the prostate in another way. At least one study has reported that a low level of vitamin D circulating in the blood is linked to a greater risk of having an enlarged prostate. (Galic 2008). How to get Vitamin D Vitamin D can be gotten through sun exposure or diet but if sun is a source of vitamin D, then why do Ghanaian men have problem with prostate cancer? Most people have insufficient or deficient levels of vitamin D (figure 19). One reason for this deficiency is that the main and most efficient way to get enough vitamin D is through exposure to sunlight. According to the Vitamin D Council, the skin produces about 10,000 International Units (IUs) of vitamin D in response to 20 to 30 minutes
Figure 19. Vitamin D and Prostate Health
of summer sun exposure. That’s 50 times more than the US government’s (Institute of Medicine’s) recommendation of only 200 IU.
Unfortunately, modern lifestyles often are not conducive to regular sun exposure for a great number of people. Most people work and spend much of their time indoors, children do not play outside as much as they used to, and older adults are often homebound or have limited access to sunlight. Also, there is a widespread campaign to “cover up” when in the sun that may be another reason for the widespread deficiency.
Dietary sources of vitamin D are limited. The healthiest and richest food sources of vitamin D are salmon and sardines and, to a lesser extent, 2% cow’s milk. However, eating normal amounts of these foods will generally not provide sufficient amounts of vitamin D. Also, food is not the best way to meet the body’s requirements for this vitamin, which is why sunlight exposure and supplements are so important. How much do Ghanaians men needs The Food and Nutrition Board (FNB) at the Institute of Medicine (IOM) at the National Academies currently recommends 200 IU of vitamin D daily for adults younger than age 50, a dose of 400 IU for adults 50 to 70, and 600 IU for adults ages 71 and older. (These doses are currently under review by the FNB at the IOM, and a report is expected in September 2010, with an anticipated increase in vitamin D recommendations.) Among conventional American medical circles, 30 ng/mL is considered a “normal” blood level of vitamin D. However, many experts from different disciplines believe both these doses and the blood level are much too low and result in deficiency and associated health problems.
For example, a statement released by the International Osteoporosis Foundation on May 11, 2010, noted that adults age 65 and older need up to twice the amount of vitamin D that is generally recommended in the United
States, and recommends 800 to 1,000 mg for this age group. The International Osteoporosis Foundation also warned that people who are obese, have osteoporosis, have limited exposure to the sun, or have difficulty absorbing vitamin D should take 50 micrograms (2,000 IU) daily. Dr. Bess Dawson-Hughes of Tufts University, who was the lead author of the Foundation’s statement, noted that the “high prevalence of suboptimal levels [of vitamin D] raises the possibility that many falls and fractures can be prevented with vitamin D supplementation.”
Higher doses are also recommended by Harvard School of Public Health (HSPH). In a recent article, HSPH recommended that everyone older than one year of age take up to 2,000 IU of vitamin D daily, and that some people may need 3,000 to 4,000 IU to reach adequate blood levels, especially individuals who have darker skin, those who spend winters at higher latitudes, and anyone who gets little exposure to direct sunlight. (HSPH 2010)
According to the Vitamin D Council and other experts, the ideal blood level of vitamin D is between 50 and 80 ng/mL. Because the majority of people are deficient (at 30 ng/mL or lower), the Council recommends that people take 5,000 IU daily for 2 to 3 months, then ask their healthcare provider for a 25-hydroxyvitamin D (25[OH]D) test to check their levels. Home test kits are also available and may be a more economic choice if you don’t have health insurance or if your insurance does not cover the test. In either case, the test requires just a few drops of blood from a finger or heel, which is then sent to a lab for analysis. Once you know your body’s level of vitamin D, you can adjust your supplement intake until your blood levels are between 50 and 80 ng/mL year round.
Why is this level important? Research shows that the body does not begin to adequately store vitamin D until the nutrient reaches a level of 50 nanograms per milliliter (ng/mL). Below 50 ng/mL, the body uses up the vitamin as fast as it can produce it or take it in. Therefore,

Figure 20. How to get Vitamin D
people who have “normal” vitamin D levels by American standards are deficient. It can take many months of taking high doses of vitamin D to make up the deficiency. According to the Vitamin D Council, that amount may be 5,000 IU daily, although you should consult your healthcare provider to determine the best dose for your situation.
Results of a study around “super-dosing” of vitamin D were just published, and they serve as an example of “too much of a good thing”. Two scientists commented on the results of the study, in which a single dose of vitamin D (500,000 IU) given to older women increased rather than decreased their risk of falls and fractures. (Dawson-Hughes 2010) The two scientists noted that while this single dose did not provide the hoped-for response (i.e., less falls and related fractures), “there is no evidence that adverse effects of more frequent, lower-dose regimens, so daily, weekly, or monthly dosing with vitamin D3 appears to be the best option for clinicians at this time.” One reason for the increase in fractures was the possibility that the older women actually were feeling “too” good and may have increased their mobility too much as a result of the effects of the vitamin. I doubt whether the researchers had this potential effect in mind when they started their research! White Tea White tea has a higher concentration of the potent antioxidants called catechins than do green and black teas (figure 21). This finding was made in 2001 by researchers from Oregon State University, and it prompted scientists to investigate the anticancer properties of white tea. In one study, a comparison of green tea versus white tea showed that white tea was superior in its ability to inhibit mutations in DNA, which is
an early step in the development of cancer. Another study found white tea helped inhibit the proliferation of early lesions in models of colon cancer. Although studies using white tea in prostate cancer cells have not yet been published, results of other studies are promising. Consuming two to three cups daily is suggested. White tea health benefits White tea health benefits come from the same plant (Camellia sinensis) as do green, black, and other teas, but for white tea, producers use the buds and young leaves rather than the more mature leaves. The buds are covered with whitish hairs, which is where the tea gets its name. Once the white tea buds and young leaves are picked, they are steamed and dried rapidly, just enough to stop oxidation. The result is a tea that is barely processed, which allows it to hold onto high concentrations of its catechins.
Many claims have been made about white tea health benefits, but some of them lack scientific evidence to support them. One reason for the scarcity of information is that more studies have been conducted using the more readily available green and black teas. White tea is also more costly.
Advocates of white tea health benefits say it can lower blood pressure, reduce cholesterol levels, fight viruses and bacteria, build strong bones, and fight cancer. There are some studies to support several of these claims, including those for cancer.
At the 219th national meeting of the American Chemical Society about a decade ago, researchers from Oregon State University conducted an analysis and reported that white tea had more catechins than other teas. (Santana-Rios 2001) Armed with that information, they tested the cancer-fighting abilities of white tea using
Figure 21. White Tea
the Salmonella test, which identifies whether a substance can cause or prevent mutations in DNA, an early step in cancer. They discovered that white tea inhibited mutations more effectively than did green tea. The scientists attributed this superior result to the higher proportion of catechinsin white tea than in green.
In another study, researchers at Ohio University Southern looked at the impact of white tea, green tea, and caffeine in a colon cancer model and found that white tea helped inhibit proliferation of early lesions in the colon. (Carter 2007)
When shopping for white tea, choose loose-leaf, which is superior in flavor and quality than bagged teas. Brew 2 teaspoons of loose-leaf tea per 8-ounce cup of very hot, but not boiling, water. For average strength, steep for 3 to 5 minutes; if you like a stronger tea, go a few minutes longer. White tea contains somewhat less caffeine than other teas: approximately 15 mg per serving compared with 40 mg for black tea and 20 mg for green. Unlike the slightly grassy taste of green tea, white tea is lighter and sweeter. Zinc Because zinc is found in high concentrations in the prostate gland, it is believed to play a major role in prostate health. Studies have indicated that zinc supplements can reduce the risk of developing advanced prostate cancer, and that men who have prostate cancer often have low concentrations of zinc (figure 22). When researchers at the University of Maryland in Baltimore exposed human prostate cancer cells to zinc, the cells were prone to undergo apoptosis
(cell suicide). In another study, investigators found evidence that zinc plays a part in regulating cell growth and cell suicide in prostate cancer cells. The RDA for zinc is 11 mg for adult males. Zinc Health Benefits Zinc health benefits include several ways it is important for prostate health. This mineral is found in large concentrations in the prostate gland. In addition to its role in proper sexual development and reproduction, zinc helps keep the immune system strong, memory intact, cholesterol and blood sugar in line, and blood pressure and heart beat regulated.
It is believed that a deficiency of zinc may result in an increase in infections and prostatitis, or it may make a male susceptible to prostate cancer because the mineral is also a key player in the body’s DNA-damage repair process. Although zinc sulfate is the most frequently used zinc supplement (and also the most inexpensive), it is not easily absorbed. Therefore the preferred form is zinc citrate, which is more bioavailable, at a dose of 15 mg daily.
An agric officer once told me he said, the soil is supposed to be the powerhouse of the zinc which our crops pick and when we also consumed the crops we get our source of zinc for prostate health but unfortunately he said, we are using chemicals to grow our crops and this is depleting the zinc from the soil so our crops can’t get enough zinc hence we don’t have enough source of zinc from the crops when we consume them.
Figure 22. Zinc
Zinc health benefits for prostate cancer In a University of Washington Cancer Prevention Program study, researchers analyzed the relationship between dietary and supplemental zinc and prostate cancer using the VITamins and Lifestyle (VITAL) cohort. Of 35,242 men who completed the dietary and supplemental questionnaire, 832 men developed invasive prostate cancer over a four-year period. The investigators did not observe a reduced risk of prostate cancer associated with a ten-year average intake of supplemental zinc greater than 15 mg per day, but they did see a decreased risk of advanced prostate cancer with a greater intake of supplemental zinc (greater than 15 mg daily vs no zinc supplement). No association between dietary zinc and prostate cancer risk was seen. (Gonzalez 2009)
A study conducted in Venezuela set out to determine zinc concentrations in the prostatic fluid of men who had prostate problems (30 subjects) compared with healthy controls (10). The researchers found that zinc concentrations in men who had prostatitis and prostate cancer—but not BPH–were lower than those in the controls. This finding led them to “consider the possibility of recommending zinc supplements as a co adjuvant therapy in patients with prostatitis,” and to use zinc levels as a diagnostic tool to distinguish BPH from prostate cancer. (Gomez 2007). Laboratory studies on zinc health benefits Researchers at the University of Maryland (Baltimore) showed that exposing human prostate cancer and BPH cells to zinc induced cell suicide, and they identified the specific genes involved. Thus this study provided an
extensive database on zinc-related prostate cancer research, and the results suggested zinc regulation of gene expression is cell-type specific; that is, the genes Fos, Akt1, Jak3, and PI3K showed themselves to be highly regulated by zinc. (Lin 2009)
In a similar vein, Oregon State University was the setting for a study that evaluated the antiproliferative effects of zinc in both prostate cancer cells and benign prostatic hyperplasia cells. Based on the knowledge that zinc concentrations in the prostate are “uniquely high” but significantly low in the presence of prostate cancer, the study’s authors set out to evaluate the antiproliferative effects of zinc in prostate cancer cells and BPH cells, with the goal of identifying possible mechanisms. Both prostate cancer and BPH cells were treated with zinc for 24 and 48 hours, and cell viability and growth were observed. BPH cells were more sensitive than were prostate cancer cells to zinc’s antiproliferative effects. The authors concluded that the differential response to zinc in the prostate cancer and BPH cells “suggests that zinc may serve an important role in regulating cell growth and apoptosis in prostate cancer and hyperplasia cells.” (Yan 2010)
Foods that contain a good level of zinc include oysters (extremely high levels), beef, poultry, seafood, fortified cereals, calf’s liver, sesame seeds, pumpkin seeds, crimini mushrooms, and low-fat yogurt. The RDA for zinc is 11 mg for adult males. Herbal remedies Plant products have been used for centuries andmuch of western allopathic medicine, includingoncology drugs, is derived from plants. Each has a different mode of action. Between 1960 and1981 approximately 114,000 plant

extracts from 35,000 species were screened for anticanceractivity. None proved effective in clinical trials during that time, and so interest diminished(Reynolds 1991). However, other countries, notably Japan, France and China continue to screen new plant materials. The problem withstudying plant products is the lack of standardization of dosage and formulation. Also, the plant contains many potentially effectivecompounds, and determining which are beneficial and which are harmful is a challenge.
Moreover, the constituents may work synergistically to provide the effect. Hundreds of herbal remedies purported to have anticancer benefits are available over thecounter, for example Chinese herbs, ginseng and garlic. Most of them have no such demonstrated benefit. The following are two examples of herbals for which many anecdotal claims are made in the popular literature available to cancer patients. Prospect of Cronton membranaceus for Prostate Health in Ghanaian men- Herbal Practitioners headache with the used of this plant for BPH/PCa In Ghanan ,one plant (figure 22) actually creating a lots of confusion regarding treatment option for prostate disorders is croton membranaceus.
Cancer is still responsible for many deaths worldwide. However, cancer prevention is almost impossible due to its numerous aetiological factors. Therefore, the best solution for cancers remains early detection and cure or treatment. Meanwhile, the current treatment options available for cancer including; surgery, radiation therapy, bone marrow transplant and chemotherapy are not only extremely expensive and unaffordable especially for third world countries such as Ghana, but are plagued with treatment failures due to toxic side effects, drug resistance and intolerance. As
such the need to search for new, potent, effective, relatively safer, reliable and affordable remedies for the treatment and management of cancer is still paramount. Research into plants has increased in recent years as they have been a
source of numerous bioactive compounds including very potent anticancer agents.
In Ghana, several plants are used by herbalists and traditional healers for the treatment and/or management of various cancers generally called "kokram" (Twi). However, the efficacies of these plant products as anticancer agents are often ill defined. Marcel Bayor research project therefore, sought to establish a scientific basis for the justification and validation or otherwise of the traditional uses of a selection of Ghanaian medicinal plants in the treatment and management of cancers, and to identify and select suitable candidate(s) for further anticancer investigations and other possible bioactivities including, antimalarial and antimicrobial effects.
The challenged with herbal practitioners in Ghana with the used of this plant As a clinical Sonographer I have worked in the major Herbal hospitals in Ghana for about (5)years diagnosing men with prostate problems using ultrasound . The challenged with Herbal practitioners is to differentiate between BPH and Prostate Cancer and refer those with prostate cancer to the specialists ,but however since there is a major competition between this Health sectors, herbal practitioners believe that they can solve all the patients problem leaving this patients with major problem later. Secondly, since Pca and BPH also present with the same urinary symptoms once this patients are giving cronton membranaceus, their urinary symptoms improve drastically and then they believed that the patient has been treated. One challenging situation in the herbal centers is when medical professional working there also suggest to them that the patient’s need a further medical attention you will be kick off your work so eventually medical professionals working in this centers cannot suggest further medical interventions. Cronton Membranaceus for BPH Management in Ghana Croton membranaceus is used by Ghanaian traditional medical practitioners in the treatment of benign prostatic hyperplasia (BPH). Preparations of the root of this plant have been observed to relieve symptoms of BPH and enhance urination without the accompanying difficulty. There are no observable adverse effects associated with the clinical use of preparations of C. membranaceus. While medicinal significance has generated scientific interest in the plant there is real concern relative to the longer term availability of this indigenous plant in its natural habitat. The objective of this review is to highlight the prospects of C. membranaceus for prostate health. As clinical sonographer I have seen patients with BPH and after a few weeks taking this c. membranaceustheir prostate gland shrink drastically in the Herbal Hospital, Their PSA level also fell drastically and they also present with enhanced libido. Hence, I believed there must be collaboration between the medical practitioners and herbal practitioners in this area to really save the lives of so many patients and croton membranaceus is a powerful local remedy for benign Prostatic Hypertrophy. Iscador Iscador is the brand name of an extract of the common species of European mistletoe,Viscum album. This plant was studied by Rudolph Steiner, who believed that cancerwas caused by an imbalance of forces on the body for growth and organization. He proposed the use of mistletoe extracts as a therapy for cancer since this
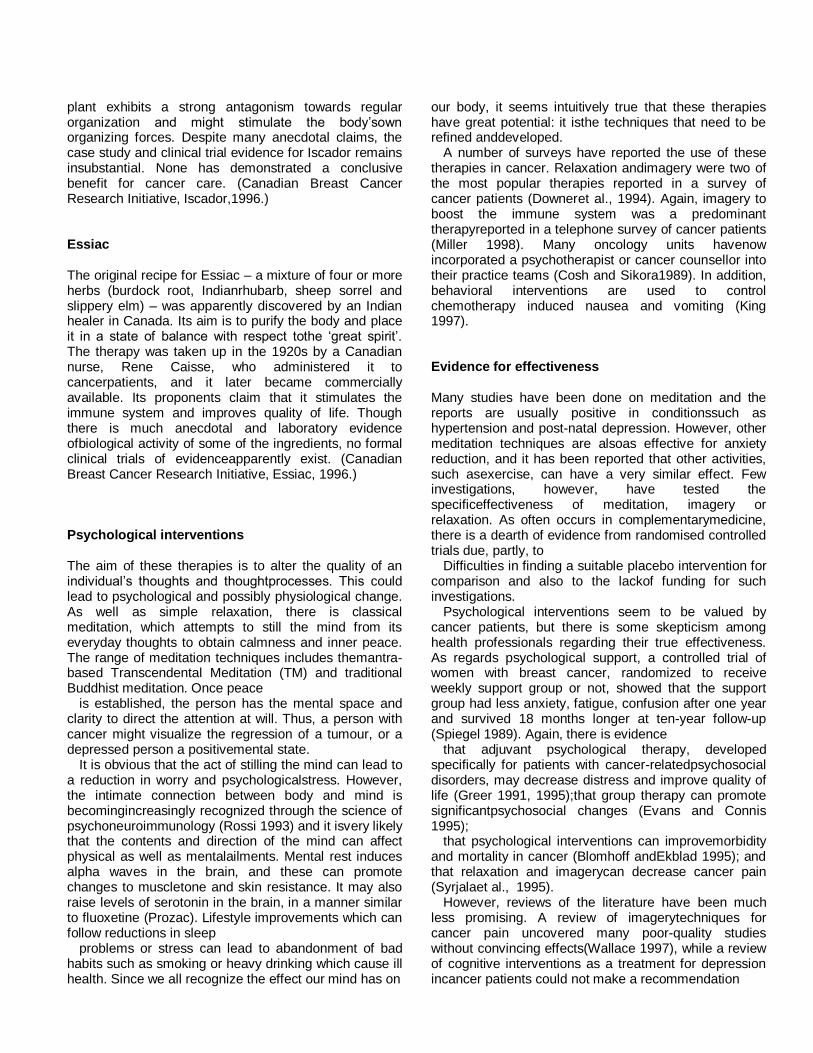
plant exhibits a strong antagonism towards regular organization and might stimulate the body’sown organizing forces. Despite many anecdotal claims, the case study and clinical trial evidence for Iscador remains insubstantial. None has demonstrated a conclusive benefit for cancer care. (Canadian Breast Cancer Research Initiative, Iscador,1996.) Essiac The original recipe for Essiac – a mixture of four or more herbs (burdock root, Indianrhubarb, sheep sorrel and slippery elm) – was apparently discovered by an Indian healer in Canada. Its aim is to purify the body and place it in a state of balance with respect tothe ‘great spirit’. The therapy was taken up in the 1920s by a Canadian nurse, Rene Caisse, who administered it to cancerpatients, and it later became commercially available. Its proponents claim that it stimulates the immune system and improves quality of life. Though there is much anecdotal and laboratory evidence ofbiological activity of some of the ingredients, no formal clinical trials of evidenceapparently exist. (Canadian Breast Cancer Research Initiative, Essiac, 1996.) Psychological interventions The aim of these therapies is to alter the quality of an individual’s thoughts and thoughtprocesses. This could lead to psychological and possibly physiological change. As well as simple relaxation, there is classical meditation, which attempts to still the mind from its everyday thoughts to obtain calmness and inner peace. The range of meditation techniques includes themantra-based Transcendental Meditation (TM) and traditional Buddhist meditation. Once peace
is established, the person has the mental space and clarity to direct the attention at will. Thus, a person with cancer might visualize the regression of a tumour, or a depressed person a positivemental state.
It is obvious that the act of stilling the mind can lead to a reduction in worry and psychologicalstress. However, the intimate connection between body and mind is becomingincreasingly recognized through the science of psychoneuroimmunology (Rossi 1993) and it isvery likely that the contents and direction of the mind can affect physical as well as mentalailments. Mental rest induces alpha waves in the brain, and these can promote changes to muscletone and skin resistance. It may also raise levels of serotonin in the brain, in a manner similar to fluoxetine (Prozac). Lifestyle improvements which can follow reductions in sleep
problems or stress can lead to abandonment of bad habits such as smoking or heavy drinking which cause ill health. Since we all recognize the effect our mind has on
our body, it seems intuitively true that these therapies have great potential: it isthe techniques that need to be refined anddeveloped.
A number of surveys have reported the use of these therapies in cancer. Relaxation andimagery were two of the most popular therapies reported in a survey of cancer patients (Downeret al., 1994). Again, imagery to boost the immune system was a predominant therapyreported in a telephone survey of cancer patients (Miller 1998). Many oncology units havenow incorporated a psychotherapist or cancer counsellor into their practice teams (Cosh and Sikora1989). In addition, behavioral interventions are used to control chemotherapy induced nausea and vomiting (King 1997). Evidence for effectiveness Many studies have been done on meditation and the reports are usually positive in conditionssuch as hypertension and post-natal depression. However, other meditation techniques are alsoas effective for anxiety reduction, and it has been reported that other activities, such asexercise, can have a very similar effect. Few investigations, however, have tested the specificeffectiveness of meditation, imagery or relaxation. As often occurs in complementarymedicine, there is a dearth of evidence from randomised controlled trials due, partly, to
Difficulties in finding a suitable placebo intervention for comparison and also to the lackof funding for such investigations.
Psychological interventions seem to be valued by cancer patients, but there is some skepticism among health professionals regarding their true effectiveness. As regards psychological support, a controlled trial of women with breast cancer, randomized to receive weekly support group or not, showed that the support group had less anxiety, fatigue, confusion after one year and survived 18 months longer at ten-year follow-up (Spiegel 1989). Again, there is evidence
that adjuvant psychological therapy, developed specifically for patients with cancer-relatedpsychosocial disorders, may decrease distress and improve quality of life (Greer 1991, 1995);that group therapy can promote significantpsychosocial changes (Evans and Connis 1995);
that psychological interventions can improvemorbidity and mortality in cancer (Blomhoff andEkblad 1995); and that relaxation and imagerycan decrease cancer pain (Syrjalaet al., 1995).
However, reviews of the literature have been much less promising. A review of imagerytechniques for cancer pain uncovered many poor-quality studies without convincing effects(Wallace 1997), while a review of cognitive interventions as a treatment for depression incancer patients could not make a recommendation
about effectiveness (Lovejoy 1997). In a review of psychological approaches to cancer (Loscalzo 1996) there was someevidence that these can reduce powerlessness and increase hope. In a review of the field, Walker (1992) found that hypnotherapy can be useful for all the above, apart from survival enhancement. A further review by the same author (1999) found evidence that psychologicalinterventions – including hypnosis – could also modulate the immune response in a waypossibly relevant to cancer. Safety and costs Meditation and other psychological interventionsmay unlock suppressed worries and fears, andfor that reason it is usually wise to undertake it under guidance. Some GPs prescribe psychological interventions under the NHS. Training, qualifications and professional bodies Anyone can call themselves a meditation teacher, though specialist courses are offered fortraining in conducting relaxation or guided imagery sessions. However, these therapies areoften acquired as part of general nursing communication skills and are practised by many nurses and paramedical staff after only a limited amount of formal training – often from tapes orbooks. However, in some units psychological interventions are taught by a clinical psychologistwho leads more formal programmes. Expert comment The expert consulted has been much involved in the practice and research of psychologicalinterventions in cancer care, and has come to believe that these therapies are undoubtedlyhere to stay. Relaxation and guided imagery are the therapies that have the most substantialevidence supporting their use in cancer care.
However, patients should be carefully assessed and the therapies only given to those foundsuitable. Nurses who may be trained to practice therapies should select patients accordingly.
Specialist backup from psychologists or psychiatrists would be preferred. Reflexology Reflexology has its roots in traditional Chinese medicine, and practitioners apply pressure tospecific zones on the soles and top of the feet to assess the disease state of the patient and alsoto improve health. Each zone on the foot is said to correspond to a zone of the body, and to
be connected to it in terms of energy flow along an energy pathway. Massaging these points isthought to unblock the energy pathway and restore normal energy flow. As regardsdiagnosis, some reflexologists claim to feel granular structures at specific points in the foot, indicative of disease in the corresponding organ, and it is hypothesized that these may be uric acid deposits from the diseased organ concerned. Similarly, unusual swellings at pointson the foot can also indicate a weakness of the corresponding body part.
Reflexology is used to restore energy levels and promote emotional well-being, and is used formost chronic conditions. It is used as a support during radio- or chemotherapy treatment forcancer in some oncology units. Evidencefor effectiveness Much has been written about reflexology, but there is a dearth of scientific investigation intothis therapy. Some studies have reported positive physiological effects, but they are small and ofpoor quality. In one controlled clinical trial in the USA, 35 women with pre-menstrual syndromewere randomized to receive either true or sham reflexology. The real treatment group showed an improvement in range of physical and mental symptoms compared with the control group(Oleson and Flocco 1993). This appears to be the only randomized controlled trial of reflexology. There are no good clinical trials of its effectiveness in cancer. Safety and costs No data exist to show ill effects, but some reflexologists will not treat certain conditions. Costs range from £20 upwards for a one-hour session, but up to eight treatment sessions arerecommended. Training, qualifications and professional bodies Reflexology is represented by six organizations, each of which issues a code of conduct for itsmembers. The two largest are the Association of Reflexologists, which has 70 accredited courses in the UK and over 2600 members, and which entitles graduates to use the letters MAR and has set standards for the profession; and the British Reflexology Association, linked with the Bayley School, which also issues qualifications that entitle the graduate to use the letters
MBRA. Accredited therapists of both organizations must have insurance. Expert comment A practicing reflexologist who treats cancer patients
explained that reflexology could helpwith cancer as part of a ‘holistic’ regime including diet and visualization to ‘rebalance’ the body. Most often, its role would be to enhance quality of life and combat side-effects oforthodox treatment. This expert would not recommend reflexology as a ‘cure’ in itself, butrather as part of a broader complementary approach. It was stated that no research intoreflexology and cancer is known, and that training standards of therapists need to beregulated. The future of Complementary Medicine in Ghana There should be collaboration between Herbal Practitioners and Medical Practitioners in Ghana.Treatment phase, i.e. during chemotherapy or radiotherapy, and in palliative care. There is aneed to reach consensus with oncologists, palliative care physicians, surgeons, GPs and nursing practitioners about which therapies should be provided at each stage of disease –and this, of course, depends on the existing evidence base as well as the views of the patients.
Since cancer treatment also depends upon the stage of the cancer it is best if both practitioners work hand in hand to save the lives of the patient. Herbal practitioners must also know their limitations and not promise patients of cure. Management of the disease must be language form the herbal practitioners.
At a national level there would appear to be a contradiction between the government’s wish toensure NHIS-wide equality of access to treatment through the implementation of frameworkstandards, and its general policy that purchasing is a ‘local decision’. In the absence of nationalguidelines on complementary therapy purchasing, the ‘lottery by postcode’ of NHIS
complementary therapy provision will continue. Until guidelines (themselves informed byresearch into effectiveness) are provided, there is evidence to suggest that complementarytherapies, while a relatively marginal element of NHIS purchasing, will be among the first services to be squeezed whenever lack of finance dictates cuts in provision. CONCLUSION Prostate cancer is affecting a large of Ghanaian men population and the used of complementary therapies has received a major boost.
However, complementary therapies have a role to play in the Psychology of cancer care to improve the patient’s survival rates and quality of life. However, complementary therapies should not be used as the only alternative in the management of Ghanaian men diagnosed with prostate cancer and it must be used in conjunction with traditional cancer treatment. Ghanaian men diagnosed with prostate cancer should not be promise cure suing these therapies and there
must be a good working environment between Herbal practitioners in Ghana and Medical Practitioners in Ghana. The plant Cronton Membranaceus must be taken seriously and more research must be done on this plant as it could give way to cancer breakthrough in Ghana and the world.
There should be a national guidelines on the cancer journey in Ghana as early as possible as the incidence of cancer appears high. The Ghana Federation OfTraditional Medicine Practitioners Association (GHAFTRAM) must also wake up and ensured Herbal Practitioners live up to and implement national guidelines for their members in the management of cancers and also let members know their boundaries in the Health sector in Ghana. REFERENCES Mark AM, Wael AS, Daisaku M, Gary JM (2001;2003).
Complementary Medicine for Prostate Cancer: Effects of Soy and Fat Consumption. Rev Uro.3(suppl 2):S20-S3
Living with hormonal therapies (accessed date updated may 2013 to be reviewed 2015. www:prostatecanceruk.org toolkits living-with-hormone-therapy
Saw P (Review: 11/28/2008Last Revised: 11/28/2008)–American cancer society www.cancer.org › ... › Herbs, Vitamins, and Minerals .
Hardiman MG (2010). Complementary and Alternative Prostate Cancer Therapy.CAM Therapeutic Approaches to Treat Prostate Cancer and Promote Healing. voices.yahoo.com/complementary-alternative-prostate-cancer-therapy-6, June, 26.
Complementary therapies in prostate cancer (nd). www.http//sixpartswater.org› Conditions › Prostate cancer
Complementary Therapies (August 02, 2011) www.http// hivinsite.ucsf.edu › ... › Daily Living › Complementary Therapies
Complementary, Alternative, or Integrative Health: What's In a Name ...( Date Created: October 2008 Last Updated: May 2013 ) www.http//nccam.nih.gov/health/whatiscam
Barrie RC (1999). Complementary and Alternative Cancer Medicine. JCO 17( suppl 1): 44-52, November.
Dr MK (1999). Complementary therapies in cancer care. Abridge report of a study produced for Macmillan cancer Relief. June 1999 PD
Prostate Cancer Treatment Choices(August 20,2009) www.articles.mercola.com sites ... 0 ... prostate-cancer-treatment-choices.aspx
Top 15 supplements for prostate cancer (February 3, 2011) .www.prostate.net › Articles › Lists (all) › Prostate Cancer Lists
Alternative cancer treatment (2014). .www;en.wikipedia.org wiki Alternative cancer treatments .Last modified 17 January 2014 at 04:16.
Marcel B (2011). The Bioactivity of Cronton membranaceus- A traditional Anticancer Herb. http://www.lap-publishing.com/../the-bioactivity-of -cronton-membranaceus.
Related Documents











