The HIV positive Child handout Heidelberg October 2017 Dr. Charlotte Adamczick

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
TheHIVpositiveChildhandout
HeidelbergOctober2017Dr. CharlotteAdamczick

Outlineofthepresentation
1. Somefacts2. Theinfectedpatient:earlyandlate
presentation3. TreatmentoftheHIVrelatedconditionsand
ARTregime4. TheAdolescent5. PMTCT6. Iris

Successesbut…(WHO2017)
• 36.7Miopeople livingwithHIV– Only19.5MioareonART(5.5.Mio in2015)– Theseare53%(39-65%)– (Withnewcut-off350CD4,15MioqualifyforARTin2015)
• 2.6Miokids<15yrs (90%infectedperinatally,living inSSA)– 150.000newlyinfectedin2015(>50%lessthan2001)– 110.000diedofAIDS(210.000in2012;320.000in2005)– only43%ofthoseinneedareontreatment
and13.3MioHIV/AIDSorphans
Special Group adolescents:

ClinicalclassificationforperinatalHIVinfectedchildren
• Withouttreatment,(fast“progressors”)• 30%diebefore1yr,• 60%before2yrs,• 80%beforetheyturn5yrs;
• Slowprogressors:symptomsinthefirstyearsoflife,AIDSwith6-9yrs• Rest:longtermsurvivor(5-10%)beyond8yrs• Survivalwithearlytreatment92%• NeedsearlyandaccuratediagnosisofHIVinfection• Establishexposure• Confirmationofinfection

Diagnostics
Serologicaltesting:
– DetectionofIgG-AB(cavewindowperiod,age<18months)– RapidABassay(recommendedbyWHOforlowresourcecountries)
• <18monthsofage:screeningassaytodetermineHIVexposure• >18monthsofage:diagnosticassaytoconfirm HIVinfection• IdentificationofnotHIV-infectedamonginfants&children<18
monthsofageneverbreastfedorstoppedbreastfeeding>6weeks
Diagnostics
Virologicaltesting:
– HIVRNA,DNA&p24AGdetectionwithPCR
• Confirmation ofHIVinfectionatallages,esp.children<18monthsofage(cave:lowsensitivityinthefirstweeksoflife)
• ExclusionofHIVinfectionininfants(>4-6weeksofage!)neverbreastfedorstoppedbreastfeedingonthepast6weeks

Diagnostics
• Confirmexposure aroundbirthoratleastat4-6weeks.
• ConfirmHIVinfection– Ifserologicaltestpositive:virologicaltestby4-6weeksofage
– Ifnovirologicaltestavailablefor<18monthsofage:• StartARTbasedonpositiveserologicaltestandaclinicalalgorithm(presumptivediagnose:Sepsis,oralthrush,severepneumonia)
• Confirmstatuswithserologicaltest>18months
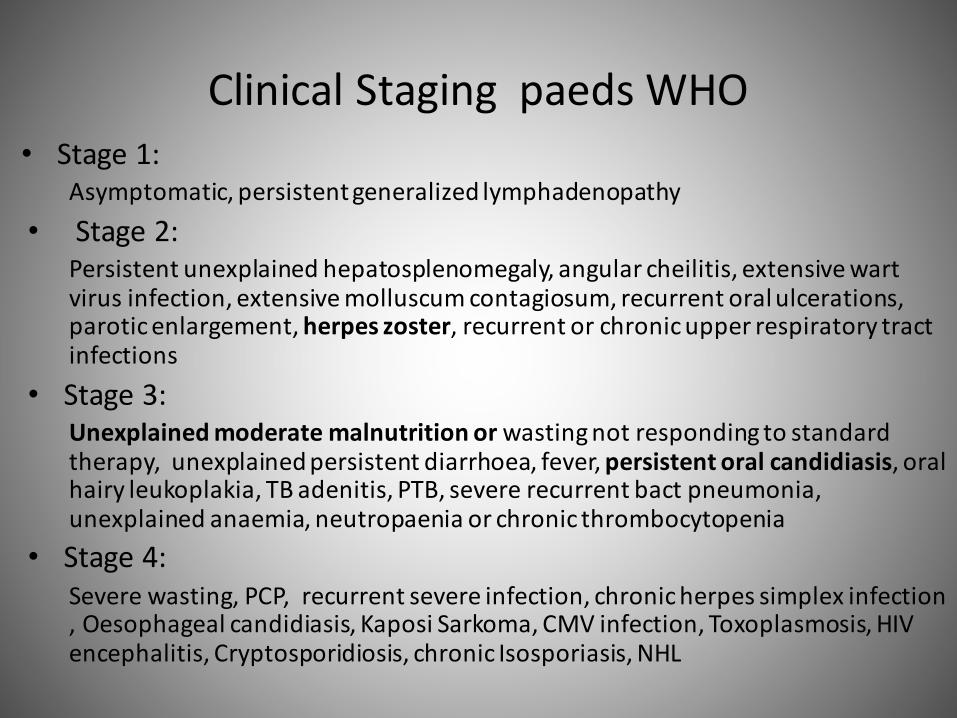
ClinicalStagingpaedsWHO• Stage1:
Asymptomatic,persistentgeneralizedlymphadenopathy• Stage2:
Persistentunexplainedhepatosplenomegaly,angularcheilitis,extensivewartvirusinfection,extensivemolluscumcontagiosum,recurrentoralulcerations,paroticenlargement,herpeszoster,recurrentorchronicupperrespiratorytractinfections
• Stage3:Unexplainedmoderatemalnutritionorwastingnotrespondingtostandardtherapy,unexplainedpersistentdiarrhoea,fever,persistentoralcandidiasis,oralhairyleukoplakia,TBadenitis,PTB,severerecurrentbact pneumonia,unexplainedanaemia,neutropaenia orchronicthrombocytopenia
• Stage4:Severewasting,PCP,recurrentsevereinfection,chronicherpessimplexinfection,Oesophagealcandidiasis,KaposiSarkoma,CMVinfection,Toxoplasmosis,HIVencephalitis,Cryptosporidiosis,chronicIsosporiasis,NHL

ClassiPcation of HIV disease in childrenThere are two diherent classidcation systems in use internationally: the Centres for Disease Control(CDC) and the World Health Organisation (WHO).
These classidcation systems are used for:
• Assessing need for treatment prioritisation• Describing individuals and populations• Surveillance purposes• Research studies (e.g. disease presentation, progression and ehectiveness of treatment)
Both provide valuable prognostic information and aid clinical decision making, including how quickly tostart ART. Both classidcations have several clinical categories/stages and the last one is describing AIDS-dedning conditions (Table 2). Until recently, both had separate classidcations of HIV-related symptomsand conditions for (i) children and (ii) adults and adolescents. In 2014 CDC revised case dednitions andcombined AIDS-dedning conditions for persons of all ages into one.
Table 2. Two classidcations of HIV disease in children
CDC WHO
Clinical categories: Clinical stages:
N: no symptomsA: mild symptomsB: moderateC: severe symptoms / AIDS / HIV infection stage 3
1: no symptoms2: mild symptoms3: advanced symptoms4: severe symptoms / AIDS
Immunological stages: Immunological stages:
1: no/mild impairment2: intermediate3: severe / AIDS
1: no impairment2: mild3: advanced4: severe / AIDS
Paediatric CDC classidcation was drst introduced in 1994. It is widely used in well-resourced countries,where diagnostic tools are readily available. CDC 1994 classidcation subdivided HIV-related clinicalconditions into N, A, B and C categories. CDC C category included severe symptoms and illnesessassociated with late stage of HIV infection (AIDS). CDC now uses a stage system to describe HIV infection:stage 0 is based on a sequence of negative and positive HIV test results indicative of early (primary) HIVinfection (it is an additional stage introduced in 2014), stages 1–3 are categorized on the basis of theCD4+ T-lymphocyte count (Tables 2 and 3). If a person has an AIDS–dedning opportunistic illness, it isconsidered stage 3 regardless of CD4 counts.
WHO has last updated its classidcation in 2007 when in addition to clinical categories immunologicalstages were included. It is widely used in resource-constrained settings (with or without access todiagnostic and laboratory testing).
Table 3. CDC 2014 and WHO 2007 immunological classidcation
CDC 2014* WHO 2007
Module 2: Diagnosis and staging of HIV in children, and role of co-infectionsand malignancy: ClassiPcation of HIV disease in children
Copyright © 2016 PENTA.
Mother and child image© UNICEF/CAR/2007/Pierre Holtz
Tr@inforPedHIV 2016Page 15 of 92

3. HIV related conditions:Kaposi Sarkoma
• NamedafterHungarianDermatologistMoritzKaposi• 1994ChangandMoorediscoveredanadditionalHerpesVirus,Humanherpesvirus8(HHV8),(closelyrelatedtoEBV).
• identifiedasbeingtheaetiologicalagentforKS.• Virustransformsepithelialcells oflymphaticsorbloodvesselsandcausestheirproliferation
• Affectedsitesaremainlyskin,lymphenodes,lungandgastrointestinaltract
• SinceART,incidencedecreasedand“aggressiveness”
Treatmentoptions
• BestareARVs
• Vincristine (sideeffects:peripheralneuropathy,myelo-suppression,constipation)– Childdosing:1.4mg/m²,0.05mg/kgif<10kgweeklyfor6weeks,
than2weeklyfor6weeks– Adults:2mg
• Bleomycin (sideeffects:allergicreaction,myelo-suppression,pulmonaryfibrosis,pneumonitis)– Indicatedwithrapiddiseaseprogression,relapseconsideringVincristin
failure– Childdosing:15units/m²i.m.weeklyfor2weeks,thanonceevery
twoweeks(notexceeding250mg/m²)– Adultdosing:15mgi.m.
• Thalidomide• Doxorubicin20mg/m2(cavecardioandmyelotoxic)• Interferon

Pulmonary manifestations
• Pneumocystiscarinii/jirovecipneumonia (PCP)• Lymphocyticinterstitialpneumonia(LIP)• PulmonaryTB• KarposiSarkoma
Pneumocystis carinii/jiroveci pneumonia
SomeFacts:• Yeastlikefungus• Theagentiswidespreadworldwide;75%sero-positivitybytheageof4yrs.
• ReductionofsevereinfectionthroughCo-Trimoxazole(!Prophylaxis rightafterdiagnosis!)
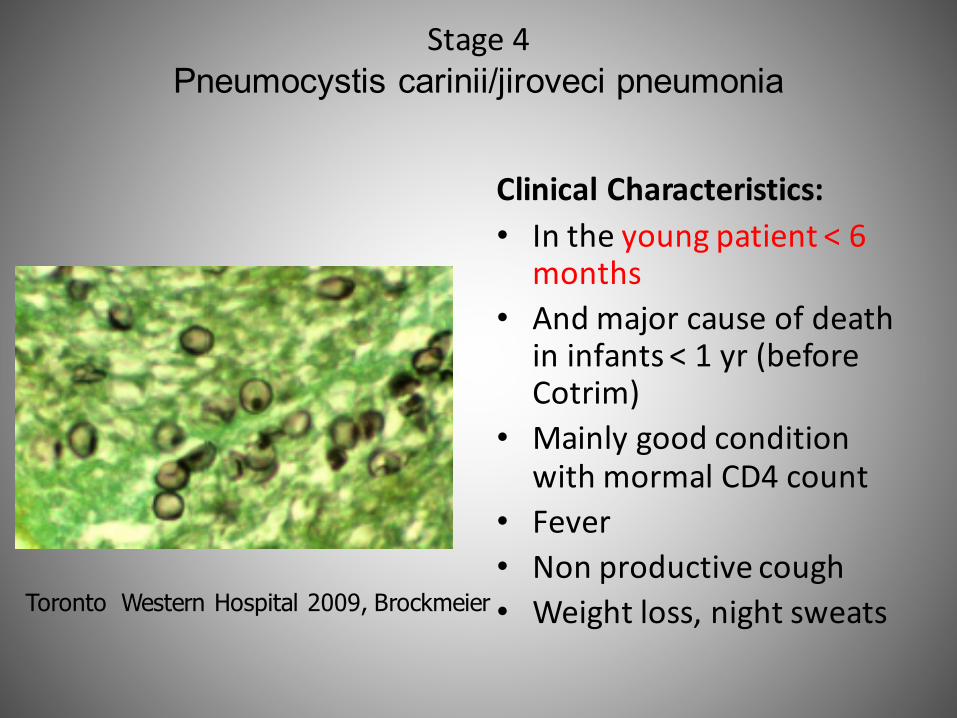
Stage4Pneumocystis carinii/jiroveci pneumonia
ClinicalCharacteristics:• Intheyoungpatient<6
months• Andmajorcauseofdeath
ininfants<1yr(beforeCotrim)
• MainlygoodconditionwithmormalCD4count
• Fever• Nonproductivecough• Weightloss,nightsweatsToronto Western Hospital 2009, Brockmeier

Pneumocystis carinii/jiroveci pneumonia
• veryfewsymptomsinitially,laterwithincreasingwheezeandSOB(respiratorydistress)
• Invasionofvisceralorgans
• Biopsy: thickenedalveolarseptawitheosinophilic exudateinthealveoli
CxR:No pleural effusionLess hili enlargement than in PTB„milky“ glas appearance

Pneumocystis carinii/jiroveci pneumonia
Therapy:1. Steroids2. Co-Trimoxazole
Alternatives:Pentamidine,Dapsone,Atovaquone,Primaquine,Clindamycin
CavePentamidine:Pancreatitis,renalfailure,Hepatotoxicity,Leucopenia,Rash,
Hypoglycaemia

Lymphocytic interstitial pneumonitis (LIP)
NotuncommenlythefirstpresentationofverticalHIVtransmisssion
• Aethiology:Infiltrationofalveolarseptabyplasma
cellscontainingEBVDNA
• Clinic: >2yrs– AsymptomaticorwithSOB,
wheezing– Recurrentinfections– Clubbing– Lymphadenopathy– Hepatosplenomegaly– EnlargedSalivaglands
• DD miliaryTB
• Therapy:BronchodilatorARVs
CXR:Bilateral, symmetircal, reticular, nodular shadowing
Hilar lymphadenopathy

DDTbandLIP
MiliaryTBLIP(nodular)noteclinicalsigns:notacutelysick,clubbing

It took along wayAge WHO clinical
stagingand/orCD4 value
<2 All Independent
>2-5 WHO III-IV CD4 < 750 cells/mm³
>5 WHO III-IV CD4 < 350 cells/mm³
all TB or Hepatitis B
HIV Treatment
Optimal timing of antiretroviral treatmentinitiation in HIV-positive children andadolescents: a multiregional analysis fromSouthern Africa, West Africa and Europe
Michael Schomaker,1* Valeriane Leroy,2 Tom Wolfs,3
Karl-Gunter Technau,4,5 Lorna Renner,6 Ali Judd,7 Shobna Sawry,8
Madeleine Amorissani-Folquet,9 Antoni Noguera-Julian,10
Frank Tanser,11,12,13 Francois Eboua,14 Maria Luisa Navarro,15
Cleophas Chimbetete,16 Clarisse Amani-Bosse,17 Josiane Warszawski,18
Sam Phiri,19 Sylvie N’Gbeche,20 Vivian Cox,21 Fla Koueta,22
Janet Giddy,23 Haby Sygnate-Sy,24 Dorthe Raben,25 GenevieveChene26,27,28 and Mary-Ann Davies;1 on behalf of the IeDEA West andSouthern Africa regional collaborations and COHERE in EuroCoord
1Centre for Infectious Disease Epidemiology and Research, University of Cape Town, Cape Town, SouthAfrica, 2Inserm, U1027, Universite Paul Sabatier Toulouse 3 Toulouse, France, 3Children’s Hospital/UMCU, Department of Infectious Diseases, Utrecht, The Netherlands, 4Department of Paediatrics &Child Health, Rahima Moosa Mother and Child Hospital and University of the Witwatersrand,Johannesburg, South Africa, 5Empilweni Services and Research Unit, Department of Paediatrics & ChildHealth, Rahima Moosa Mother and Child Hospital and University of the Witwatersrand, Johannesburg,South Africa, 6University of Ghana Medical School, Accra, Ghana, 7MRC Clinical Trials Unit, UniversityCollege London, London, UK, 8University of the Witwatersrand, Wits Reproductive Health and HIVInstitute, Chris Hani Baragwanath Academic Hospital, Soweto, South Africa, 9Felix Houphou€et BoignyUniversity Hospital, Abidjan, Cote d’Ivoire, 10Pediatrics Department, Hospital Sant Joan de Deu,Universitat de Barcelona, Barcelona, Spain, 11Africa Centre for Health and Population Studies,University of KwaZulu-Natal, Somkhele, South Africa, 12School of Nursing and Public Health, Universityof KwaZulu-Natal, Durban, South Africa, 13Centre for the AIDS Programme of Research in South Africa– CAPRISA, University of KwaZulu-Natal, Congella, South Africa, 14Yopougon University Hospital,Abidjan, Cote d’Ivoire, 15Hospital Gregorio Mara~n"on, Madrid, Spain, 16Newlands Clinic, Harare,Zimbabwe, 17MTCT-Plus Center, Abidjan, Cote d’Ivoire, 18Centre de recherche en epidemiologie et santedes populations, 1018 Inserm, France, 19Lighthouse Trust Clinic, Kamuzu Central Hospital, Lilongwe,Malawi, 20Centre de Prise en Charge de Recherche et de Formation Enfants, Abidjan, Cote d’Ivoire,21Medecins Sans Frontieres South Africa, Cape Town, South Africa, 22Charles de Gaulle UniversityHospital, Ouagadougou, Burkina Faso, 23Sinikithemba Clinic, McCord Hospital, Durban, South Africa,24Albert Royer Hospital, Dakar, Senegal, 25Department of Infectious Diseases, Rigshospitalet, Universityof Copenhagen, Copenhagen, Denmark, 26University of Bordeaux Bordeaux, ISPED, Centre INSERMU1219-Bordeaux Population Health, F-33000 Bordeaux, France, 27INSERM, ISPED, Centre INSERM
VC The Author 2016; all rights reserved. Published by Oxford University Press on behalf of the International Epidemiological Association 453
International Journal of Epidemiology, 2017, 453–465
doi: 10.1093/ije/dyw097
Advance Access Publication Date: 22 June 2016
Original article
Downloaded from https://academic.oup.com/ije/article-abstract/46/2/453/2622841/Optimal-timing-of-antiretroviral-treatmentby Bodleian Law Library useron 10 October 2017
U1219-Bordeaux Population Health, F-33000 Bordeaux, France, 28CHU de Bordeaux, Pole de sante publi-que, Service d information medicale, F-33000 Bordeaux, France
*Corresponding author. Michael Schomaker, University of Cape Town, School of Public Health and Family Medicine,
Centre for Infectious Disease Epidemiology and Research, Falmouth Building, Anzio Road, Observatory, 7925, Cape Town,
South Africa. E-Mail: [email protected]
Accepted 31 March 2016
Abstract
Background: There is limited knowledge about the optimal timing of antiretroviral treat-ment initiation in older children and adolescents.Methods: A total of 20 576 antiretroviral treatment (ART)-naıve patients, aged 1-16 yearsat enrolment, from 19 cohorts in Europe, Southern Africa and West Africa, were included.We compared mortality and growth outcomes for different ART initiation criteria, alignedwith previous and recent World Health Organization criteria, for 5 years of follow-up, ad-justing for all measured baseline and time-dependent confounders using the g-formula.Results: Median (1st;3rd percentile) CD4 count at baseline was 676 cells/mm3 (394; 1037)(children aged ! 1 and < 5 years), 373 (172; 630) (! 5 and < 10 years) and 238 (88; 425)(! 10 and < 16 years). There was a general trend towards lower mortality and bettergrowth with earlier treatment initiation. In children < 10 years old at enrolment, by 5years of follow-up there was lower mortality and a higher mean height-for-age z-scorewith immediate ART initiation versus delaying until CD4 count < 350 cells/mm3 (or CD4%< 15% or weight-for-age z-score < -2) with absolute differences in mortality and height-for-age z-score of 0.3% (95% confidence interval: 0.1%; 0.6%) and -0.08 (-0.09; -0.06) (! 1and < 5 years), and 0.3% (0.04%; 0.5%) and -0.07 (-0.08; -0.05) (! 5 and < 10 years). Inthose aged > 10 years at enrolment we did not find any difference in mortality or growthwith immediate ART initiation, with estimated differences of -0.1% (-0.2%; 0.6%) and -0.03 (-0.05; 0.00), respectively. Growth differences in children aged < 10 years persistedfor treatment thresholds using higher CD4 values. Regular follow-up led to better heightand mortality outcomes.Conclusions: Immediate ART is associated with lower mortality and better growth for upto 5 years in children < 10 years old. Our results on adolescents were inconclusive.
Key words: Antiretroviral treatment, paediatrics, g-formula, causal inference
Key Messages
• We found lower mortality and better growth with immediate versus delayed antiretroviral treatment initiation in chil-
dren < 10 years of age after 5 years of follow-up.
• We showed neither benefits nor harms with immediate treatment initiation in adolescents aged 10-16.
• The best outcomes were observed in European children who attained growth outcomes comparable to HIV-negative
children. The effects for the different ART initiation criteria were similar in Southern Africa, West Africa and Europe.
• Irregular clinic visits led to worse outcomes than with regular follow-up, but the comparative effectiveness of different
ART initiation criteria were not affected.
454 International Journal of Epidemiology, 2017, Vol. 46, No. 2
Downloaded from https://academic.oup.com/ije/article-abstract/46/2/453/2622841/Optimal-timing-of-antiretroviral-treatmentby Bodleian Law Library useron 10 October 2017

ARTs
• NRTI(Nucleosidereversetranscriptaseinhibitor)– approvedforchildren(e.g.Lamivudine3TC,ZidovudineAZT)– 2NRTIsrecommendedforallregimesas“backbone”– Fewsideeffects,welltoleratedandfewdruginteractions
• NNRTI(Nonnucleosidereversetranscriptaseinhibitor)– approvedforchildren(Nevirapine NVP,Efavirenz EFV)– Rapidemergeofresistance– Sideeffects:commonlycutaneousreactions

ART
• PI(Proteaseinhibitor)– 7approvedforchildren(e.g.Lopinavirritonavir-boostedLPV/r,
AtazanavirATV/r)– Mortalityreduction65%
• Entryinhibitors(fusioninhibitors)– 2approvedforchildren
• IntegraseInhibitors

Principlescont.ARTsinspecialsituations:
•InfantandchildwithpreviousNNRTIexposure:startonPI+2NRTIs
•Childrenwithsevereanaemiaorneutropenia:avoidAZT
•Adolescents>12yrswithHepB:starton:TDF(Tenofovir)+FTC(Emtricitabine)or3TC(Lamivudine)+NNRTI.

Monitoring
• CD4monitoring:– Atdiagnosis– Every6monthsthereafter– MorefrequentwhendecreasingtowardsthethresholdofARTstart(giventhechildis>24month,hasnoTBornoHepB)
– PriortoARTinitiation– Every6monthsafterinitiation– Incaseofanyclinicalchange(delayingrowth,neuro-
development)

ClinicalsignificanceofVLandCD4count
Monitoringcont.
• VL– Notessentialbeforeinitiation– Assessmentisdesirabletoassessanddiagnoseimmunologicalfailure
• Clinicalandlaboratory– BaselineHBandWBCatinitiation– Every8weeksHBinAZTregimes– Growthandnutritionalstatus(doseadjustment)– LFT,SerumLipids
Interruptedtreatment
• Significantdrugtoxicity• Acutegastrointestinalillness• Surgery• STI(structruedtreatmentinterruptions)poordata.KnowninPMTCT
NeurodevelopmentinHIV
PRE– ARTarea• SevereCNSmanifestationsin50-90%children• GreatestriskforHIV– encephalopathywithinthefirstyearof
lifeanddependantonviralload• ProgressiveHIVencephalopathy(PHE):usuallydeathin2yrs
POST– ART• SevereCNSmanifestationssuchasPHE<2% (Chiriboga,2005)
NeurodevelopmentinHIV
Clinicalrelevance
• EarlyARTisprotectingthedevelopingbrain(betterlearning!)
• Inadolescentsdecreaseofthehighprevalenceofpsychiatricandbehaviouralillness
4.disclosuretoadolescents(LizLowenthal,Baylor)
Disclosure:• Ageisveryindividual• It’saprocess• Youngptisfocalperson,nottheguardian,but“disclosure
plan”shouldbedonewiththecaringperson
• Overallaim:1. Betterunderstanding2. Psychologicaladjustmentandself-esteem3. “nomoresecrets”4. Eachvisitpositivereinforcementandmessages5. Advise,whatandhowtotellothers6. Encouragetodailyroutines
Disclosure• Withappropriatematerials
andterms,evensmallchildrencangetanunderstanding oftheircondition.
Eg.Goodsoldiersneedgoodnutrition,medicine, tokeepthemstrong.
Laterintroduce thetermsofCD4,viralloadetc.

• Avoidassigningblame• NOT:“yourmothergaveittoyou”• INSTEAD:“somechildrenarebornwiththevirus,wethinkthatiswhathappenedtoyou”
Supportmaterials:• Paediatricadherencesupportcurriculumonwww.bayloraids.org
• Southtosouth




“youthclub”• Specialclinicdaysforadolescents• Adherenceoftenonly30%• Sideeffectsduetolongtreatment• “buddy”• Educationonprotection• Familyplanning• Papillomavaccination• Otherprofessionals:socialworker,psychhologist
6.PMTCT(preventionofmothertochildtransmission)
• ImportanceofPMTCT• 3.3millionchildrenwithHIVinfection• 90%acquiredMTCT• High2yearmortality
• Riskoftransmissionapproximately35%• 25%in-utero,60%intra-partum,15%breastfeeding
– Decreasedto10%• withthe3-stepAZTPACTGregimen(1994)
– Decreasedto<1%• withHAART,formulafeedingandelectiveC/Sasappropriate
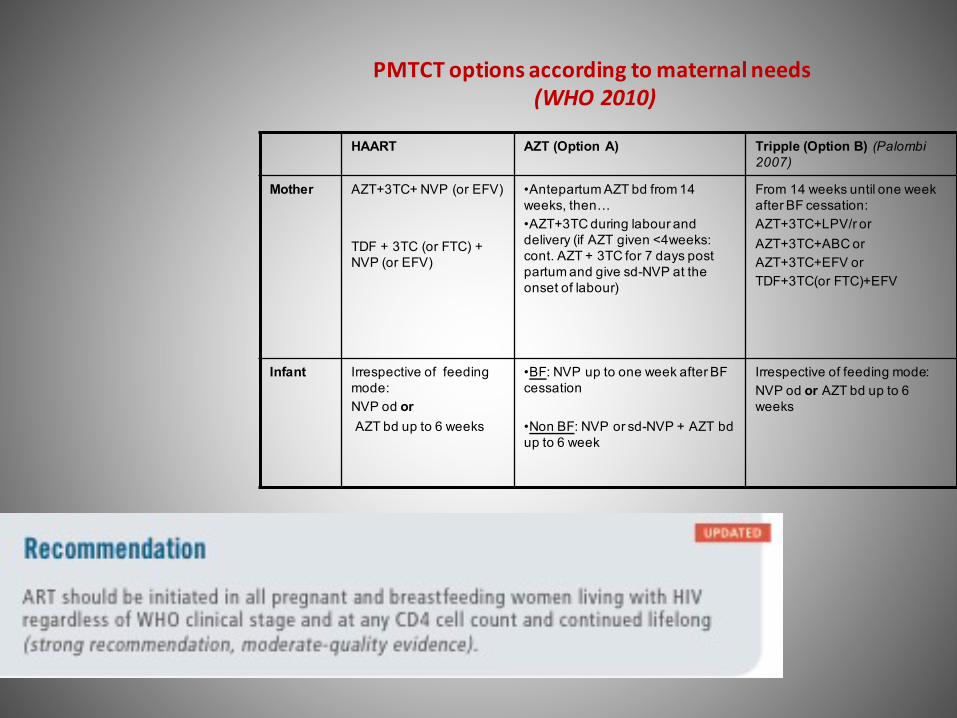
PMTCToptions according tomaternal needs(WHO2010)
HAART AZT (Option A) Tripple (Option B) (Palombi 2007)
Mother AZT+3TC+ NVP (or EFV)
TDF + 3TC (or FTC) + NVP (or EFV)
•Antepartum AZT bd from 14 weeks, then…•AZT+3TC during labour anddelivery (if AZT given <4weeks: cont. AZT + 3TC for 7 days postpartum and give sd-NVP at theonset of labour)
From 14 weeks until one weekafter BF cessation:AZT+3TC+LPV/r orAZT+3TC+ABC orAZT+3TC+EFV orTDF+3TC(or FTC)+EFV
Infant Irrespective of feeding mode:NVP od orAZT bd up to 6 weeks
•BF: NVP up to one week after BF cessation
•Non BF: NVP or sd-NVP + AZT bd up to 6 week
Irrespective of feeding mode:NVP od or AZT bd up to 6 weeks

ArgumentsforHAARTineverypregnantwoman
• KEEPTHEMOTHERALIVE
• HIVpos pregnantwomenhave:
1. Increasedriskofprematurity,PROM,IUGR
2. Morevulnerableforsevereinfection
3. Worseoutcomeplacentalmalaria
4. Infanthashigheroverallmortalityrisk,evenwhenremainingHIVneg.
• MotheronHAART(since2012:OptionB+):
1. Overallbetterimmunestatusofmother
2. loverviralloadduringpregnancywithdecreasedriskoftransmissiontothechild
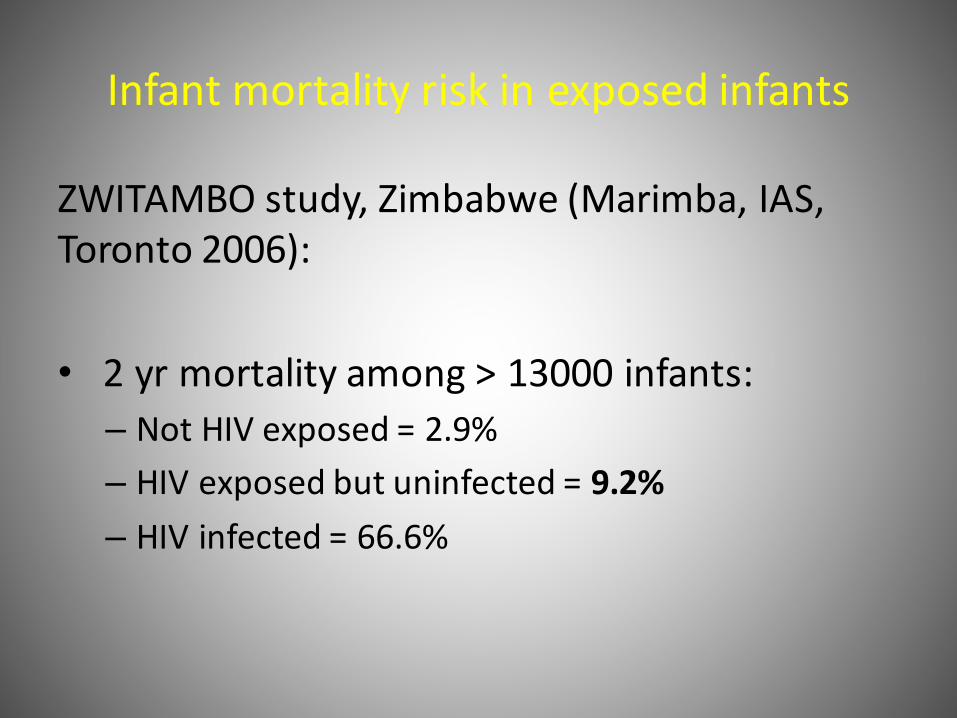
Infantmortalityriskinexposedinfants
ZWITAMBOstudy,Zimbabwe(Marimba,IAS,Toronto2006):
• 2yr mortalityamong>13000infants:– NotHIVexposed=2.9%– HIVexposedbutuninfected=9.2%– HIVinfected=66.6%
PMTCT• MotherHIVpos,testedduringsecondPregnancyandqualifiedforART
• Firstbornpresentedwithseveremalnutrition,extensiveoralthrush,posstatus
• Sibling,8months,PCRneg.andclinicallywell.BFstoppedwith6months(WHOrecommendation:exclusiveBF6months,BFupto12monthswithfood)

KEYMESSAGE:PMTCTBestresultsforreductioninHIVtransmissionismaternalHAART
duringearlypregnancy,regardlesstheCD4value
andneonate/infantonAZTregimeuntilcessationofbreastfeeding
IntegratePMTCTintoMCH,TB,FP,STIclinics
!Note:EliminationofpaediatricAIDSthroughmaternalHAART!
• Botswanaconference2008,2010• Cotton2009SAJHIVMED• Becquet2009• WHOrecommendations2010
Pitfalls
“slippingthroughthenet”
• Mothersgetinfectedlaterinpregnancy
• Mothersgetinfectedduringbreastfeeding
• Note: Recommendationformultipletestingarelacking
• Note: first3weeksofnewinfection► highviralload;high
transmissionriskduringbreastfeeding

PrEP

Futurechallenges
• Adolescence• Orphans• Nonadherence• Emergingresistances• Organfailure• Costs;reliabledonorswithlong-termcommitment
7.IRIS
(Immunereconstitutioninflammatorysyndrome)

IRISDef:unexpectedandparadoxclinicalaggravationafter
ARTstart
• Mostlyafter3month• CommonwithCD4<50/mm3• Seenin15-25%ofthepatients• Potentiallyunder-diagnosed
Differentforms:• LatentInfection;f.ex.TB,CryptococcalMeningitis• Knowninfection,alreadytreated,gettingworse

IRIScont.• Inchildrenupto21%(BCGadenitisininfancy,TBinolderchildren)
• MostcommonformofIRISisTB.
• InSSA:highTBincidenceinHIVinfectedchildren(1600in100.000) (Hesseling2009)
• EarlyARVsdecreasestheriskofIRISupto70%(Martinson2009)
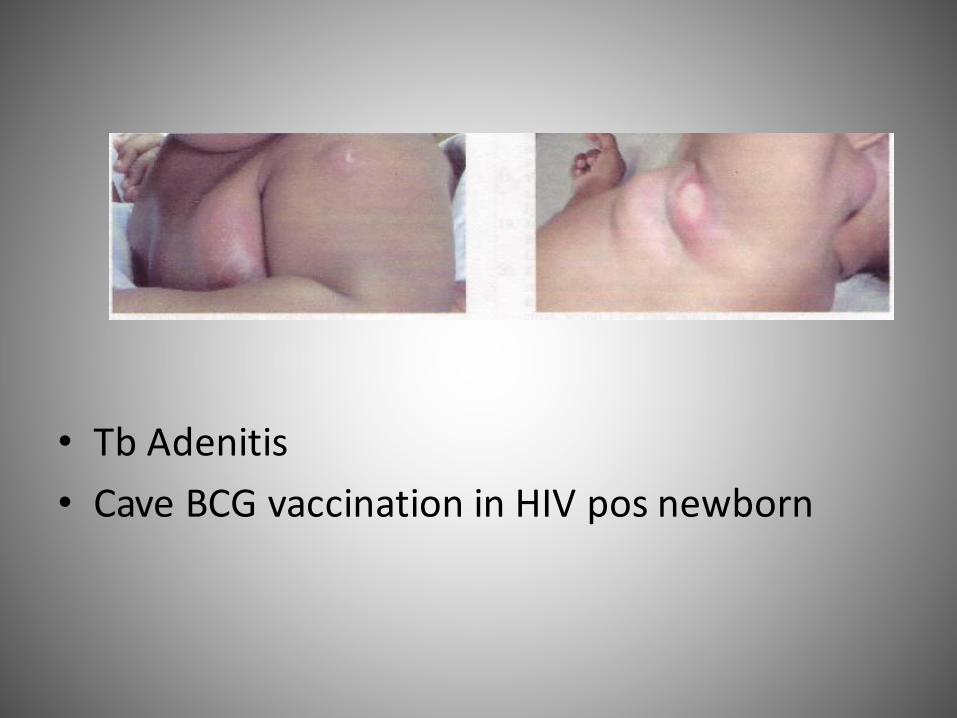
• TbAdenitis• CaveBCGvaccinationinHIVposnewborn

OtherformsofIRISSkin
• Moluscumcontagiosum• Tineacapitis• warts• Impetigo• HerpesZoster• Fungalinfections
others
• GuillainBarré• MyocardialeDilatation• Leukencephalopathie• Lepra• KarposiSarkoma• CMV• PCP• Opsoclonus– myoclonus• Toxoplasmosis

TreatmentoptionofIRIS
• 30%hospitalisation
• WithsevereTBIRIS,HAARTinterruption(cave:evolvingresistancewithEfavirenzandNevirapin,lesscommonwithPI)
• NSAIDwithmildclinic,steroidswithsevereIRIS
Related Documents