The High 5s Project Interim Report

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The High 5s Project Interim Report

The High 5s Project Interim Report
December 2013

2The High 5s Project Interim Report
WHO Library Cataloguing-in-Publication Data
The high 5s project: interim report.
1. Patient Safety – standards. 2. Hospital Administration. 3. Medical Errors – prevention
and control. 4. Delivery of Health Care. 5. Safety Management – standards. 6.Hospitals.
7. Data Collection. 8. Program Evaluation. I.World Health Organization.
ISBN 978 92 4 150725 7 (NLM classification: WX 167)
© World Health Organization 2014
All rights reserved. Publications of the World Health Organization are available on the WHO
website (www.who.int) or can be purchased from WHO Press, World Health Organization,
20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857;
e-mail: [email protected]).
Requests for permission to reproduce or translate WHO publications –whether for sale or for
non-commercial distribution– should be addressed to WHO Press through the WHO website
(www.who.int/about/licensing/copyright_form/en/index.html).
The designations employed and the presentation of the material in this publication do not imply
the expression of any opinion whatsoever on the part of the World Health Organization
concerning the legal status of any country, territory, city or area or of its authorities,
or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent
approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply
that they are endorsed or recommended by the World Health Organization in preference
to others of a similar nature that are not mentioned. Errors and omissions excepted, the names
of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify
the information contained in this publication. However, the published material is being
distributed without warranty of any kind, either expressed or implied. The responsibility for
the interpretation and use of the material lies with the reader. In no event shall the World Health
Organization be liable for damages arising from its use.
Design by CommonSense, Greece

3 Acknowledgements
This Interim Report was carried out as part of
the High 5s Project set up by the World Health
Organization in 2007 and coordinated globally by
the WHO Collaborating Centre for Patient Safety,
The Joint Commission in the United States of
America, with the participation of the following
Lead Technical Agencies including: Australian
Commission on Safety and Quality in Health Care,
Australia; Canadian Patient Safety Institute, Canada
and the Institute for Safe Medication Practices
Canada, Canada; National Authority for Health-
HAS, France, with CEPPRAL (Coordination pour
L’ Evaluation des pratiques professionnelles en
santé en Rhône-Alpes), France, OMEDIT Aquitaine
(Observatoire du Medicament, Dispositifs medicaux
et Innovation Therapeutique), France (from 2012-
2015) and EVALOR (EVAluation LORraine), France
(from 2009-2011); German Agency for Quality
in Medicine, Germany and the German Coalition
for Patient Safety, Germany; CBO Dutch Institute
for Healthcare Improvement, the Netherlands;
Singapore Ministry of Health, Singapore; Trinidad
and Tobago Ministry of Health, Trinidad & Tobago;
Former National Patient Safety Agency, United
Kingdom of Great Britain and Northern Ireland;
and the Agency for Healthcare Research and
Quality, USA.
This work is a part of the High 5s Project which
has been supported by the Agency for Healthcare
Research and Quality, USA, WHO, and the
Commonwealth Fund, USA.
Acknowledgements

This report is dedicated in memoriam to Jerod M. Loeb, PhD, friend,
colleague, master of performance measurement and quality improvement.
The unique feature of the work presented here is its multidimensional
system of evaluation, for which Jerod was the guiding force. His intellect,
integrity and joie de vivre brought out the best in each of us.
5

Executive Summary ...................................................................................................................... 9
1. The purpose and objectives of the High 5s Project ........................................................................14
2. The history, concepts, and overall strategy of the High 5s Project ................................................16
1. Historical background ............................................................................................................16
2. Scope of the High 5s Project....................................................................................................17
3. Unique features of the High 5s Project ....................................................................................18
3.1. Standardization ............................................................................................................18
3.2. Evaluation....................................................................................................................19
3. The High 5s Project governance, structures, participating LTAs and hospitals, description
of the work of the Steering Group and its several committees ......................................................22
1. Overall governance ................................................................................................................ 22
2. Lead Technical Agency governance ........................................................................................ 22
3. Lead Technical Agency structure ............................................................................................ 23
4. Participating hospitals ............................................................................................................ 25
5. High 5s Steering Group .......................................................................................................... 30
6. High 5s Project Committees .................................................................................................. 30
4. The design of the Project and its protocols and evaluation framework, including an overview
of methodologies, instruments and processes ............................................................................ 34
1. Design of the Project.............................................................................................................. 34
2. Standard Operating Protocols (SOPs)...................................................................................... 34
3. High 5s evaluation framework ................................................................................................ 34
3.1. SOP implementation experience .................................................................................. 35
3.2. SOP-specific performance measures.............................................................................. 35
3.3. Event analysis .............................................................................................................. 38
3.4. Patient safety culture survey ........................................................................................ 40
6The High 5s Project Interim Report
Contents

5. Qualitative and quantitative interim findings................................................................................ 44
1. Summary of culture survey findings ........................................................................................ 44
1.1. Culture surveys in participating Member States ............................................................ 45
2. Context survey of Medication Reconciliation .......................................................................... 48
2.1. Medication Reconciliation context survey findings in Member States ............................ 49
3. Context survey of Correct Site Surgery.................................................................................... 50
4. Interim findings ...................................................................................................................... 51
4.1. Summary of qualitative findings .................................................................................. 51
4.2. Member State implementation experiences and qualitative findings .............................. 56
4.3 Summary of event analysis findings .............................................................................. 65
4.4. Summary of quantitative findings ................................................................................ 67
4.5. Member State quantitative and event analysis findings .................................................. 80
6. Interim outcomes ...................................................................................................................... 90
1. Feasibility .............................................................................................................................. 90
1.1. Overall issues .............................................................................................................. 90
1.2. Summary of in-country experiences .............................................................................. 92
2. Impact .................................................................................................................................. 99
2.1. Overall issues .............................................................................................................. 99
2.2. Summary of Member State experiences ...................................................................... 101
7. Developing networks and awareness raising for the High 5s Project ............................................110
1. Developing global networks and awareness raising ................................................................110
2. National networks and awareness raising................................................................................112
8. High 5s Steering Group meetings and international hospital meeting ..........................................116
1. Steering Group meetings........................................................................................................116
2. International hospital meeting ..............................................................................................116
9. Next steps ................................................................................................................................118
1. Overview ..............................................................................................................................118
2. The cross High 5s Medication Reconciliation map ..................................................................118
3. Next steps by LTAs ................................................................................................................118
Annexes ............................................................................................................................................125
7 Contents

ACS American College of Surgeons
ADE Adverse Drug Event
ACSQHC Australian Commission on Safety and Quality in Health Care
AHRQ Agency for Healthcare Research & Quality
APS German Coalition for Patient Safety
AZQ / AQuMed German Agency for Quality in Medicine
CBO Dutch Institute for healthcare Improvement (a TNO company)
CC WHO Collaborating Centre for Patient Safety
CEPPRAL Qualité et Sécurité en santé, France
CI Concentrated Injectables
CPSI Canadian Patient Safety Institute
CI Concentrated Injectables
CSHP Canadian Society of Hospital Pharmacists
CSS Correct Site Surgery
BPMH Best Possible Medication History
EA Event Analysis
ED Emergency Department
EHR Electronic Health Record
EMGO Institute for Health and Care Research, The Netherlands
EMR Electronical Medical Record
EVALOR French EVAluation en LORraine
FMEA Failure Mode and Effects Analysis
HAS French National Authority for Health
HCO Healthcare Organization
HRO High Reliability Organization
IfPS Institute for Patient Safety
IMS Information Management System
ISMP Canada Institute for Safe Medication Practices Canada
JCI Joint Commission International USA
LTA Lead Technical Agency
MDS Event Analysis – Minimum Data Set
Med Rec Medication Reconciliation
MoH Ministry of Health
MMP Medication Management Plan
MMS Medicare & Medicaid Services
NIAZ The Netherlands Institute for Accreditation in Healthcare
NIVEL The Netherlands Institute for Health Services Research
OR/OT Operating Room/ Operating Theatre
PCEHR Personally Controlled Electronic Health Record
RHAs Trinidad & Tobago Regional Health Authorities
ROP Required Organizational Practices
SOP Standard Operating Protocol
WHO World Health Organization
8The High 5s Project Interim Report
Acronyms

Experience with standardization in non-health care
industries clearly shows that standardized processes
lead to improved safety and service excellence.
In health care, the standardization of hospital
processes may enable trained health-care providers
to perform more consistently and reduce latent
tendencies for processes to fail, that is, to reduce
errors.
The High 5s Project (the Project) was launched
in 2007 to examine the concept of standardization
in clinical processes by implementing targeted
patient safety improvement strategies. The High 5s
name derives from the Project’s original intent to
significantly reduce the frequency of 5 challenging
patient safety problems in 5 countries over 5 years.
A key objective was to develop and assess Standard
Operating Protocols (SOPs) in a range of health-
care systems and cultures, and to provide evidence
of the benefits of standardization in health care
as one of the means to effect safety and excellence
in performance. To this end, the Project initiated
the development of SOPs for certain priority
patient safety problems, undertook a
comprehensive evaluation, and then refined the
SOPs and its measurement strategies for later use
by interested countries around the world.
The specific goals of the Project were to determine
the feasibility of implementing SOPs in hospitals
in multiple countries, and to measure the impact
on patient safety. Standardization on such a large
scale is challenging, and to be globally relevant,
it needs to be applicable in different cultures and
health-care environments. If this goal proves to be
feasible, it will create leverage to spread both the
concept of standardization and the SOPs themselves
across the broader health care community.
To achieve these goals, a group of WHO Member
States – Australia, Canada, France, Germany, the
Netherlands, Singapore, Trinidad & Tobago,
and the USA–the World Health Organization
(WHO) Patient Safety Programme and the WHO
Patient Safety Collaborating Centre (The Joint
Commission), have joined forces to develop and
implement SOPs that address recognized patient
safety challenges.
Two unique features of the High 5s Project were
the use of standardization across multi-country
settings, and a carefully-designed, multi-pronged
approach to evaluation. The major components
of the High 5s Project work included:
ñ developing and implementing Standard Operating
Protocols;
ñ developing an Impact Evaluation Strategy;
ñ collecting, analyzing and reporting data;
ñ learning from data through a Collaborative
Learning Community;
ñ disseminating knowledge globally.
Five SOPs were initially drafted but due to resource
constraints, only two were fully developed
and implemented. These were the ‘Medication
Accuracy at Transitions in Care’ (Med Rec) and
‘Correct Procedure at the Correct Body Site’
(Correct Site Surgery) SOPs. Concurrent
performance measurement of these SOPs started
in 2010 and will continue until 2014.
Governance and Lead Technical Agencies
The Project’s activities were planned and
implemented by a Steering Group and five
technical subcommittees, composed of
representatives from the participating institutions
and countries. Each Member State nominated
a Lead Technical Agency (LTA) to coordinate
and support the implementation of the SOPs
in hospitals, and to monitor their impact using
evaluation tools developed by the technical
9
Executive Summary

subcommittees. Each LTA was responsible for
coordinating the Project in its country, including
hospital training, support for evaluation and event
analysis and hospital data submission into a secure
web-based Information Management system (IMS)
developed by the Collaborating Centre to be used
for data collection, analysis and reporting.
Design of the High 5s Project
An early challenge for the Project was to apply
established best practices and evidence based
interventions in quality improvement and patient
safety to the development of standardized
processes and tools. Steering Group members
and other experts provided input to the process
designs, which included development of a
comprehensive system of evaluation that made
possible the production of comparative results
locally, nationally and internationally.
Each SOP summarizes a safety problem, proposes
a solution, presents the evidence for the solution,
identifies potential barriers to adoption, and
delineates potential unintended consequences
of the solution. Through step-by-step instructions
and tools for implementing a defined patient care
process, each SOP can be used by multiple users
in a consistent and measurable way. The SOPs are
intended to achieve systems change and health
care professionals’ behavioral change by applying
standardized, evidence-based quality improvement
methods.
With regard to evaluation, the High 5s Project set
out to answer two key questions.
1. Is it feasible to implement standardized
processes in health care within individual hospitals,
among multiple hospitals within individual Member
States, and across country boundaries?
2. What is the impact of standardization on the
safety problems that the project targets?
The basis for answering these questions was the
‘Impact Evaluation Strategy’ designed to assess
the feasibility and impact of implementing the SOPs
using both quantitative and qualitative approaches.
This strategy applied evaluation approaches that
allowed impact of the interventions to be measured
from different perspectives, including:
1. qualitative evaluation of the SOP
implementation experiences;
2. SOP-specific performance measures;
3. event analysis to identify and investigate
occurrences that may represent SOP failures;
and
4. hospital culture surveys.
An SOP implementation evaluation process
was used to determine if the SOPs could be
implemented as designed in diverse hospital
settings, to identify barriers to implementation,
and to identify ways to overcome these barriers.
Self-reported narrative and interview data were
(and continue to be) collected from the hospitals
for a deeper understanding of the feasibility and
impact of SOP implementation in multi-country
settings and environments.
The second component of the evaluation strategy
was performance measurement. Data, normally
collected on a monthly basis, were used to assess
the degree to which the SOPs were followed
by the participating hospitals.
The third component employed event analysis.
Each participating hospital was directed to
actively seek and investigate a pre-determined set
of patient safety problems (events) that should
have been prevented by the SOP. A systematic
analysis of the facts and contributing factors
of a patient safety incident, and whether it was
linked to the design and/or implementation
of the SOP took place.
The fourth and complementary area of action
was the voluntary administration of a patient safety
culture survey in hospitals. These surveys were
done to provide insight into the patient safety
culture of hospitals participating in the High 5s
Project and to sensitize frontline staff and hospital
management about staff members’ perception
of the hospital’s patient safety culture.
Interim Findings
All country-specific sections in this report reflect
the status of 2nd quarter 2013.
Patient safety culture surveys
Overall, culture survey results showed the
highest scores on teamwork issues within units
(70% positive), and the lowest scores on handoffs
and transitions (34% positive). The percentage
of respondents giving the hospital’s work area/unit
a patient safety grade of an ‘A-Excellent’ or
‘B-Very Good’ ranged from 70% to 21%. Percent
of hospitals, by country, reporting one or more
10The High 5s Project Interim Report

events ranged from 78% to 37%. Culture survey
results were limited by inconsistent statistical
selection of samples of hospitals, variation in
number of respondents per country, variable
administration of the surveys, and variable quality
of submitted data.
Context surveys
It was considered that the ‘context surveys’
would be useful to understand what external
factors were influencing the uptake of the SOPs
in the different Member States.
Qualitative findings
Hospitals shared their implementation experiences
through quarterly and then six-monthly reports.
For purposes of analyzing and reporting evaluation
data, the hospitals were asked to determine
whether implementation of a SOP was ‘full’–
when all required components of the SOP were
in place across all eligible locations and patient
populations within the hospital– or ‘partial’.
For the Correct Site Surgery SOP implementation,
challenges related to assembling a representative
group to oversee implementation, lack of resources,
resistance to change, poor communication or lack
of leadership were identified. Identification of areas
of potential breakdown through a risk- assessment
allowed them to implement controls, warnings or
protections to minimize identified problem areas.
Much was learned about SOP implementation from
the initial pilot testing which most hospitals did
before starting full SOP implementation. During
piloting, the hospitals were able to identify barriers
and correct them prior to full implementation
through increased communication, enlisting staff
and leadership support, and providing additional
training. Further, many hospitals reported that they
were not using the prescribed High 5s data quality
methodology. However, most hospitals were
performing some form of data quality monitoring,
conducting audits, soliciting information from staff,
engaging in project oversight meetings and
identifying opportunities for improvement.
Hospitals’ implementation experiences for the
Medication Reconciliation SOP emphasized lack of
resources and challenges in assembling an oversight
group. Most hospitals did not complete a formal
risk assessment because of lack of resources or
because it was considered a low priority. Those that
did conduct risk assessment reported that it was
beneficial in helping to identify potential areas
for process breakdown. Although some hospitals
reported that the SOP implementation was an
extension of their existing medication reconciliation
process, many barriers to implementation were
reported including limited resources, data
collection burden, insufficient communication, and
resistance to change. Most responding hospitals
indicated technical challenges and technical issues
with the SOP performance measures.
A detailed description of implementation
experiences for both SOPs in Member States is
presented in the main body of the Interim Report.
Overall, they point to leadership and stakeholder
commitment and support as well as an
organizational culture of safety, adequate
resources, team cohesion, and ongoing training
to be among the key factors for successful SOP
implementation. The principle barrier was the
burden of data collection, although hospitals
themselves appreciated the value of measurement
as a means to successful improvement. Another
major challenge to implementation was resistance
to change by providers and leaders.
Quantitative findings
Hospital performance measurement data were
collected to provide a profile of each SOP
implementation in Member States. Details
are presented in section 5.4 of this report.
Interim Conclusions
Feasibility
In this context, feasibility refers to the degree
to which an SOP can be implemented as it was
originally defined, in a standardized way across
hospitals within a country and in multiple countries.
Over the course of the High 5s Project it became
clear that some aspects of the SOPs were easier
to implement than others. When participants
encountered issues with the implementation of
an SOP, they were invited to submit requests to
adapt or revise components of the SOP. Overall,
relatively few adaptations and revisions were required,
suggesting that a high degree of standardization
of health care processes was seen as feasible.
Impact
The SOPs had a significant impact in hospitals in
all participating Member States. As a result of
implementation of the SOP, certain process steps
were introduced or improved in the Member States
which were not part of everyday care previously.
For example, site-marking was introduced in French
11 Executive summary

hospitals. In Singapore, the improvement in clinical
practice and staff cooperation was reflected in
the performance measure data, which showed 98%
compliance with complete preoperative verification
and Time Outs, and improvement in surgical
site-marking from 40% to 97%. Safety components
are now built into surgical work flows and a culture
of shared ideas and learning among hospitals has
been promoted.
In the case of the Med Rec SOP, the results were
encouraging in that some hospitals managed
to reduce medication inaccuracies substantially.
Implementation of the SOP had an impact in
improving the quality of the medication histories
obtained, resolving discrepancies, and other
related patient care activities.
In the case of the Correct Site Surgery SOP,
the qualitative evaluation showed positive effects
in stimulating organizational safety cultures,
improving communication and teamwork in the OR
and beyond, optimizing surgical care, improving
the quality of patient records and demonstrating
that hospital processes can be re-designed to
provide better patient care. Because of the
infrequency of incorrect surgeries, it is not possible
at this point to demonstrate a measureable
decline in the number of these events. However,
implementing this SOP has resulted in an increase
in the number of identified and resolved
discrepancies in the surgical preparation process,
each of which carries a risk of incorrect surgery.
Developing networks
A major goal of the High 5s Project was to build
national and global networks. The initiative’s early
focus concentrated on building government and
ministerial support for implementing standardised
patient safety solutions by encouraging Member
States’ expert institutions to participate in the
Project. In later stages, the design of all steps in
the SOP development and the implementation
and evaluation plan included engagement of
networks of hospitals. The networks and the
learning communities they comprised have been
successful in raising awareness of the SOPs and
the benefits they bring to institutions and patients.
A good networking achievement was the
participation of 31 hospitals at the ‘International
Hospital Meeting’ at WHO Headquarters in
October 2012, to exchange knowledge and
implementation experiences and further strengthen
and motivate hospitals’ commitment.
Another example of an effective networking tool
is the interactive online map developed by the
Institute for Safe Medication Practices (ISMP)
Canada, the Med Rec SOP lead, to profile High 5s
Project achievements in the participating Member
States which have implemented the Med Rec
SOP. The map includes Med Rec implementation
site information and highlights High 5s Med Rec
implementation publications and national supports
such as accreditation standards. The anticipated
spread of the Med Rec SOP will be reflected in
this map.
Next steps
There is growing consensus that implementation
and evaluation of the SOPs is progressing
successfully in participating hospitals. Next steps
for the LTAs involve the active spread of the SOPs
and implementation experiences to more hospitals
within each Member State and beyond. Plans to
disseminate the SOPs and share the evaluation
methodologies with more WHO Member States
are also being developed. It is expected that
at the last Steering Group meetings in 2014,
discussions will focus on how to expand
the networks to the developing world.
12The High 5s Project Interim Report

1The purpose and objectivesof the High 5sProject

The High 5s Project is a collaboration among
a group of WHO Member States, the World
Health Organization (WHO) Patient Safety
Programme and the WHO Patient Safety
Collaborating Centre - The Joint Commission
to achieve measurable and sustainable reductions
in challenging patient safety problems through
the implementation of standardized operating
protocols.
The basic assumption being tested in the High 5s
Project is that process standardization, with
minimal variation, can improve patient safety
across national boundaries. This is being evaluated
by assessing the feasibility and impact of
implementing standardized approaches to specific
patient safety problems across multiple WHO
Member States and cultures.
Achieving process consistency, while retaining
the ability to recognize and accommodate variation
in the input (for example, the patient’s severity
of illness, co-morbidities), is one of the major
challenges to standardization in health care.
Process variation to meet individual patient needs
is essential in care delivery. But variation to meet
the preferences of health-care organizations or
individual practitioners need not be. Standardization
supersedes “best practice” when it comes to safety.
To test this, the High 5s Project has taken this
thesis to another level by standardizing certain
processes within multiple organizations in different
WHO Member States around the world.
14The High 5s Project Interim Report
The purpose and objectives of the High 5s Project

2The history,concepts and overallstrategy of the High 5sProject

The Project is a global health sector collaboration
reflecting the efforts of stakeholders in patient
safety from the government agencies of Australia,
Canada, France, Germany, the Netherlands, Singapore,
Trinidad & Tobago and the USA, as well as research
and patient safety organizations from these Member
States, and other international organizations.
Working together, the High 5s partners achieve
objectives that no single organization or patient
safety agency could achieve individually. These
include:
ñ accelerating the development and
implementation of standardized patient safety
solutions and addressing risk areas having
a high burden of morbidity and mortality;
ñ testing them across different settings and
country cultures;
ñ introducing robust tools for implementing
and evaluating the solutions; and
ñ generating learning and sharing knowledge
globally.
In action, the High 5s Project draws on the specific
strengths of its current and former partners. Since
the Project’s initiation the following types of
organizations have contributed to its activities:
ñ Lead Technical Agencies and technical institutes
from participating Member States;
ñ WHO Collaborating Centre for Patient Safety
designated as The Joint Commission and the Joint
Commission International;
ñ WHO.
The Member States involved in the initiation of the
High 5s Project were Australia, Canada, Germany,
the Netherlands, New Zealand, the United Kingdom
of Great Britain and Northern Ireland, and the
United States of America. France and Singapore
joined the High 5s Project in 2008 and 2009
respectively. In 2010, Trinidad and Tobago joined
as well. Several technical institutes/agencies from
these countries have contributed to the work of
the High 5s Project. These include:
ñ The Canadian Patient Safety Institute (CPSI);
ñ The Institute for Safe Medication Practices
Canada, Canada (ISMP Canada);
ñ The former National Patient Safety Agency, UK.
The Project has been supported by the Agency
for Healthcare Research and Quality, WHO, and
the Commonwealth Fund. It is being coordinated
by the WHO Collaborating Centre for Patient
Safety- The Joint Commission and JCI (hereafter
the Collaborating Centre).
1. Historical background
In 2002, the World Health Assembly recognized
the need to promote patient safety as a fundamental
principle of all health systems and called on the
World Health Organization (WHO) to develop
global norms and standards; promote the framing
of evidence-based policies and mechanisms to
recognize excellence in patient safety globally;
encourage research on patient safety; and support
efforts by Member States to improve the safety
of care. Subsequently, WHO initiated efforts to
address patient safety and established the World
Alliance for Patient Safety in 2004, renamed as
the Patient Safety Programme in 2009.
At the 2005 annual Commonwealth Fund
International Symposium on Health Care Policy,
the need for developing and implementing
standardized patient safety processes to reduce
the magnitude of adverse events was discussed.
The High 5s Project emerged as a result of:
ñ a shift in priorities to address the growing
problems of unsafe care;
16The High 5s Project Interim Report
The history, concepts and overall strategy of the High 5s Project

ñ an increasing recognition of the importance
of patient safety process improvement as the
means to safer care;
ñ a desire to see if standardized approaches might
be the key to improving and maintaining safety
across different settings and cultures;
ñ a growing interest among WHO, The Joint
Commission, and the Ministers of Health of
Australia, Canada, Germany, the Netherlands,
the United Kingdom and the United States of
America to develop, implement and evaluate
standardized approaches for making care safer.
The High 5s name derives from the Project’s
original intent to significantly reduce the frequency
of 5 challenging patient safety problems in 5
Member States over 5 years.
At the 2006 annual Commonwealth Fund
Symposium, Ministers of Health of Canada,
Germany, the Netherlands, New Zealand,
the United Kingdom and the United States of
America signed formal letters of commitment
to participate in and support the High 5s Project
together with WHO, the Commonwealth Fund,
and the Collaborating Centre. The Project began
to take shape in late 2006 with the nomination
of representatives from the Lead Technical
Agencies (LTAs) of participating Member States
who subsequently constituted the nucleus of
the High 5s Steering Group.
Lead Technical Agencies
Each participating Member State nominated
a LTA which subsequently coordinated and
supported the implementation of Standard
Operating Protocols (SOPs) at hospitals and
monitored their impact through applying evaluation
tools developed by the High 5s Project Steering
Group members. LTAs underwent intense initial
training and were given high visibility and
recognition for their willingness to implement
and evaluate the SOPs and for their leadership
in working to standardize patient care processes
in their country’s health-care system.
Each LTA was responsible for identifying at least
10 hospitals per SOP it decided to implement;
providing hospital training in the use of the SOPs
and Project evaluation process and tools; and
collecting data from participating hospitals and
submitting it to the Collaborating Centre (CC)
for analysis and tracking. Following completion
of LTA and hospital training, the SOPs began to be
implemented in some participating hospitals
in the autumn of 2009. Data collection began
in 2010 and will finish by September of 2014.
2. Scope of the High 5s Project
The mission of the High 5s Project is to facilitate
implementation and evaluation of standardized
patient safety solutions within a global learning
community to achieve measurable, significant,
and sustainable reductions in challenging patient
safety problems.
The major components of the High 5s work
included:
ñ developing and implementing SOPs;
ñ developing an Impact Evaluation Strategy;
ñ collecting, reporting, and analyzing data;
ñ developing a Collaborative Learning Community;
ñ disseminating knowledge learned globally.
The Project was designed to generate learning
that would permit the continuous refinement
and improvement of the SOPs within selected
hospitals of participating Member States, as well
as assessment of the feasibility and impact of
implementing standardized approaches to specific
patient safety problems across multiple Member
States and cultures. The Project has built on
existing structures in the participating Member
States. SOP implementation was expected
to provide valuable lessons and knowledge
to support the advancement of patient safety
around the world.
Five SOPs and associated evaluation instruments
were developed between 2007 and 2009 to address
the following challenges:
1. Medication Accuracy at Transitions in Care;
2. Correct Procedure at the Correct Body Site;
3. Use of Concentrated Injectable Medicines;
4. Communication During Patient Care Handovers;
5. Health Care-Associated Infections.
The first two SOPs, ‘Medication Accuracy at
Transitions in Care (Medication Reconciliation)’
and ‘Correct Procedure at the Correct Body Site
(Correct Site Surgery)’ have been implemented by
the participating Member States. Implementation
of the third SOP ‘Use of Concentrated Injectable
Medicines’ was initiated in the UK, but testing
ceased in 2010 when this Member State disengaged
from the High 5s Project. Planning towards
17 The history, concepts and overall strategy of the High 5s Project

implementation of this SOP has been re-initiated
in 2013 by the Dutch Lead Technical Agency.
Extensive investigation of the potential to
implement a standardized approach to
‘Communication During Patient Care Handovers’
found that this SOP was heavily influenced by
cultural and environmental issues that were not
measurable and easy to standardize.
Therefore, work on this SOP was abandoned
in 2010. The ‘Health care-associated infections’
SOP was withdrawn from further development
and testing because parallel work towards
standardizing procedures to address health
care-associated infections was taking place
independently by WHO and other global
organizations.
18The High 5s Project Interim Report
Table 1: SOP implementation by WHO Member States between 2009-2014
Member State CSS SOP Med Rec SOP Conc. Inject. SOP
Australia �
Germany � �
France � �
The Netherlands � � (initiated in 2013)
Singapore �
Trinidad & Tobago �
U.K. � (stopped in 2010)
U.S.A. � � (initiated in 2013)
3. Unique features of the High 5s Project
Two unique features of the High 5s Project are
the use of standardization across multi-country
settings, and a carefully-designed, multi-pronged
approach to evaluation.
3.1. Standardization
Standardization is the process of developing,
agreeing upon, and implementing technical or
uniform specifications, criteria, methods, processes,
designs or practices that can increase compatibility,
interoperability, safety, repeatability, and quality.
Process standardization is the specification and
communication of a process at a level of detail
sufficient to permit consistent and verifiable
implementation by different users at different
times and in different settings. Standardization
reduces variation: ‘The tendency for a process to
fail is also diminished in relation to the consistency
with which it is carried out; that is, the degree
to which it is standardized.’1 This enables shared
learning, facilitates multi-disciplinary teamwork
and improves efficiency in interactions by
establishing optimum conditions. It also allows
for consistency during changes in scale and the
transfer of processes between people or
organizations – attributes which are essential
for global interactions.
Standardization in health care
The most commonly referenced examples of
standardization are by high reliability organizations
(HROs) in industries such as nuclear energy or
aviation which have well ingrained organizational
safety cultures and standardized management
approaches toward risk. These HROs serve as
an example for improving safety by focusing
on standardizing the systems involved.
Experience with standardization in these industries
is decades ahead of health care. Their standardized
safety approaches acknowledge the prospect
of failure from the start of the process,
and efforts are made to build in safety from
the beginning to the end. This contrasts with
health care, where successful outcomes
are often assumed to be the baseline. Recent
efforts to standardize health-care processes
have been slow to demonstrate their impact on
the delivery of care processes.
Standardization in patient safety
There are examples of standardization in the
area of patient safety informatics2, classification
and definitions3,4,5, and some recent development
in standardizing interventions6, protocols7,8,
outcome measurement9, data collection10,

patient handovers11, medication use12, and patient
monitoring13.
The key to optimizing patient safety is to design
systems that prevent the inevitability of human
error from actually reaching and harming the
patient14. Standardization takes the sharing
of success stories and best practices to a new
level – allowing sharing of new approaches
among health-care workers. Health-care providers
themselves have underscored the need for
standardization in patient safety.
The benefits of implementing standardized patient
safety processes and evaluating that implementation
and its impact are outlined in Box 1.
19 The history, concepts and overall strategy of the High 5s Project
Box 1: Benefits of implementing and evaluating standardized protocols
ñ Standardization provides policy and decision-makers, and health-care workers a means to compare
actions and outcomes implemented within or between groups.
ñ Standardization better enables investigators to compare data and to interpret the relevance and
efficacy of an intervention.
ñ Through standardization, more health-care workers will be able to relate to one another in
meaningful ways (including the standardization of terms used).
ñ As more and more hospitals begin to use the same protocols with the same data fields, the ability
to analyze risk will be enhanced.
ñ Health-care workers who become proficient with SOPs will be constantly building on a solid
foundation, rather than struggling to grasp the range of safety concepts that might otherwise arise
in an unstructured environment.
ñ Standardization will allow health-care workers to learn from each other’s experiences (i.e., new ideas
on how to address problems – what has worked, what has not and why).
3.2. Evaluation
The second unique feature of the High 5s Project
relates to its integrated, multi-pronged approach
to evaluation. The triangulated impact evaluation
approach being used in this Project was necessary
because of the difficulties in assessing the impact
of preventive patient safety interventions,
particularly where the targeted adverse event can
occur relatively infrequently, such as in the case of
wrong- site surgery. The High 5s Project evaluation
approach addresses the impact measurement
challenge from different perspectives, including
qualitative data collection regarding the SOP
implementation experiences, quantitative
performance measurement results, event analysis,
and organization culture assessment. These methods
were used to assess the feasibility and impact of
implementing standardized patient safety protocols.
A secure web-based Information Management
System (IMS) was developed to facilitate the
storage, analysis, dissemination and exchange
of data. The system was designed around a secure
web-based application called TWiki (version
TWiki-4.2.4, Plugin API version 1.2). Several levels
of security were incorporated into the IMS
to protect data submitted. Three types of data
were gathered through the IMS:
1) narrative descriptions of the implementation
experience;
2) aggregate counts of hospital-level data used
to calculate performance measure results; and
3) de-identified and aggregated data from event
analyses conducted by participating hospitals.
This design permits participants to come together
on a global electronic learning platform.
Participating hospitals and LTAs were also asked
to use a standardized approach - the High 5s Data
Quality Management Programme - to assess
and ensure the quality of their data. To manage
data quality, hospitals, LTAs and the CC assumed
the following responsibilities:
ñ the hospitals were responsible for re-collecting
data through independent observation or
‘re-abstraction’ to determine the “data element
agreement rate” or to identify inconsistencies
among the different components of the
evaluation process;

ñ the LTAs were responsible for overseeing
the hospitals’ implementation of data quality
activities, identifying and evaluating results
from and among their participating hospitals,
and reporting to the CC “the extent and nature
of unresolved discrepancies and any identified
data collection problems”;
ñ the CC was responsible for overseeing the LTAs’
data quality activities. Assessing the data quality
information received from the LTAs, reporting
the reliability and completeness of submitted
data to the Evaluation Committee and presenting
its views on the implications of the findings
on achieving data quality goals of the High 5s
initiative.
Assessment of data quality focuses on the
completeness and reliability of the data for each
component of the High 5s Impact Evaluation
Strategy, including narrative data, performance
measurement data, and event analysis data.
The standardization of data collection and
reporting contributes to the following objectives:
ñ ensure comparability of performance and quality
measures across health-care systems;
ñ improve health-care quality15;
ñ share information/data across health care
systems and increase the usefulness, integration
and exchange of data16;
ñ improve efficiency of performance measurement
over time; and
ñ facilitate coordination and cooperation among
all parties in performance measurement and
health care quality improvement17.
20The High 5s Project Interim Report
1 Croteau RJ, Schyve PM, Chapter 8, “Proactively Error-Proofing Health Care Processes” Error Reduction in Health
Care, 2nd Edition Patrice Spath, editor Jossey-Bass Publishers San Francisco, 2010
2 Bakken S, Cimino J, Hripcsak G. Promoting patient safety and enabling evidence-based practice through informatics
Medical Care, 2004. 42(2):49-56, (sup, Feb 2004).
3 Odwazny R, Hasler S, Abrams R, McNutt R. Organizational and cultural changes for providing safe patient care.
Quality Management in Health Care, 2005, 14/3:132-143.
4 Hellings J, Vleugels A. Patient safety in hospitals: Context and concepts Tijdschriftvoor Geneeskunde, 2007;
63(16):743-750.
5 Chang A, Schyve PM et al. The JCAHO patient safety event taxonomy: a standardised terminology and classification
scheme for near misses and adverse events. Int J for Qual in Health Care 2005.
6 The Health Roundtable Ltd. Australia. SAFE Patient Care Program 2009 – Standardising Actions for Excellent Patient
Care.
7 O’Connor, EJ, Fiol, CM. Resistance to Patient Safety Initiatives. Physician Executive, 01 November 2005; 31(6):64-67.
8 Rozich JD, Howard Ramona J et al. Standardization as a Mechanism to Improve Safety in Health Care. Joint
Commission Journal on Quality and Patient Safety. 2004; 30(1): 5-14.
9 Weiser TG, Makary MA et al; Standardised metrics for global surgical surveillance The Lancet 2009; 374: 1113–17.
10 Runciman, WB, Baker GR, Michel P, Larizgoitia I, Lilford, RJ, Andermann A, Flin, R, Weeks WB. The epistemology
of patient safety research. International Journal of Evidence-Based Healthcare. 2008; 6(4):476-486.
11 Patterson ES. Structuring flexibility: the potential good, bad and ugly in standardisation of handovers. QualSaf
Health Care. 2008;17(1):4-5.
12 Kazandjian VA, Ogunbo S, Wicker KG, Vaida AJ, Pipesh F. Enhancing medication use safety: benefits of learning
from your peers.QualSaf Health Care. 2009;18(5):331-5.
13 Davies M, Tales H. Enhancing Patient Safety Through a Standardized Model of Physiologic Monitoring Healthcare
Quarterly, 8(Sp) 2005: 49-52.
14 O’Leary DS. Patient safety: the search for global solutions. World Hosp Health Serv. 2008;44(1):19-21.29.
Franklin, B.D., Standardization is key to improving patient safety. Pharmaceutical Journal, 2003; 271.
15 O’Leary DS. Patient safety: the search for global solutions. World Hosp Health Serv. 2008;44(1):19-21.
16 Standardization for Health Care Quality Improvement. http://www.ahrq.gov/research/iomracereport/reldata5.htm
17 AHRQ Conference on Health Care Data Collection and Reporting, AHRQ Publication No. 07-0033-EF, March 2007.

3The High 5sProjectgovernance,structures andparticipatingorganizatons

1. Overall governance
The High 5s Project is a collaborative whose
participants include representatives from the LTAs
of the participating Member States, WHO, and
the Collaborating Centre, and experts from
associated national institutions or agencies
which are not LTAs. In addition to the development
of the SOPs and associated implementation and
evaluation instruments, collaborative actions
include participation in strategy setting, advocacy,
fund-raising, Member State and hospital
mobilization, Project implementation, data
collection, evaluation and knowledge dissemination.
The Project’s plans and activities are governed
by a Steering Group composed of representatives
from the WHO Patient Safety Programme,
the Collaborating Centre, the LTAs and associated
experts. The Steering Group meets twice a year
to review progress achieved; set future direction
for the Project; approve technical plans, activities
and products; review data; and review and act
on committee recommendations.
The websites of the High 5s Project organizations,
agencies, institutions and LTAs are presented in
Annex 1.
2. Lead Technical Agency (LTA)governance
The Australian LTA: The Australian Commission on
Safety and Quality in Health Care (the Commission)
is a government agency which was established to
lead and coordinate national improvements in
safety and quality in health care across Australia.
It provides a number of programmes, publications
and resources to support health-care professionals,
health-care organizations and health-care policy
makers, and works with patients and care- givers
to deliver safe, high quality health care across
Australia. The Commission is responsible for the
conduct and governance of the High 5s Project
in Australia. The SOP selected for implementation
in Australian hospitals was ‘Assuring medication
accuracy at transitions of care’.
The French LTA: The French National Authority
for Health (Haute Autorité de Santé, HAS), is an
independent public authority, located near Paris.
HAS contributes to the regulation of health system
quality. Its mission is in the field of evaluation of
health products, professional practices, organization
of care and in public health. With the commitment
of the French Ministry of Health HAS joined the
Project in 2008 as the French Lead Technical Agency
The SOPs selected for implementation were the
‘Assuring medication accuracy at transitions of care’
(Med Rec) and the Correct Site Surgery (CSS) SOPs.
HAS is responsible for the overall management
and has partnered with two regional organizations.
These receive funding from HAS for supporting
participant, hospitals and monitoring
implementation and evaluation of the two SOPs:
ñ CEPPRAL, a regional quality and security of care
organization, has been responsible for follow-up
and evaluation of the CSS SOP implementation;
ñ EVALOR (EVAluation en LORraine) was
responsible for the first two years of the Med Rec
SOP implementation. In 2012, this task was
turned over to OMEDIT (Observatory of Drugs,
Medical Devices and Therapeutic Innovations
of Aquitaine) whose mission addresses the quality
and safety of medication throughout the care
pathway.
The German LTAs: The German Federal Ministry
of Health has been funding the High 5s Project in
Germany since the end of 2007. Two organizations
were appointed to share the tasks in implementing
the High 5s Project on a national level:
22The High 5s Project Interim Report
The High 5s Project governance, structures,participating LTAs and hospitals, descriptionof the work of the Steering Group and itsseveral committees

ñ The German Agency for Quality in Medicine
(AQuMed, ÄZQ): Located in Berlin, AQuMed
is a non-profit organization owned by the
German Medical Association and the National
Association of Statutory Health Insurance
Physicians. AQuMed coordinates health-care
quality programmes with a special focus on
evidence-based medicine, clinical practice
guidelines, patient empowerment, patient safety
programmes, and quality management;
ñ The German Coalition for Patient Safety (APS):
The German Coalition for Patient Safety is
a non-profit association of health-care
professionals, institutions and patient organizations
whose mission is to improve patient safety
in Germany. The German Coalition for Patient
Safety has appointed the Institute for Patient
Safety (IfPS) of the University of Bonn to carry
out its tasks in the High 5s Project.
The SOPs selected to be implemented by German
LTAs were ‘Assuring medication accuracy at
transitions of care’ and Correct Site Surgery (CSS).
The Dutch (Netherlands) LTA: With the support
of the Dutch Ministry of Health, CBO Dutch
Institute for Healthcare Improvement (a TNO
company) located in Utrecht, assumed responsibility
as the LTA in 2009. The purpose of Dutch
participation in this international collaboration
was primarily to introduce and put into practice
international expertise in Dutch hospitals
and provide technical support to national and
international development of patient safety
solutions. The SOP selected for implementation in
Dutch hospitals was ‘Assuring medication accuracy
at transitions of care’ (Med Rec). In 2013, the LTA
started the ‘Concentrated Injectable Medicines’
SOP for implementation in Dutch hospitals.
The Singaporean LTA was formed to support
the High 5s Project following the expression
of interest to participate in the High 5s project
by Singapore’s Minister of Health in May 2009.
The LTA comprises representatives from the
Standards and Quality Improvement Division in
the Singapore Ministry of Health. The SOP
selected to be implemented by Singapore’s LTA
was Correct Site Surgery (CSS).
The Trinidad & Tobago LTA: In May 2011,
Trinidad & Tobago participated at the High 5s
Steering Group Meeting in Berlin to obtain first
hand experiences from Member States on
implementation of the SOPs. The Collaborative
Action Statement was signed by the Minister
of Health in August 2011, signaling the Ministry’s
support to the Project, and confirming the Ministry
of Health as the LTA for Trinidad and Tobago.
The SOP selected to be implemented by the Trinidad
& Tobago LTA was Correct Site Surgery (CSS).
The United States of America (U.S.A.) LTA:
The Agency for Healthcare Research and Quality
(AHRQ) serves as the official U.S.A. LTA. Since it
has no formal health care delivery responsibilities,
AHRQ has delegated SOP implementation
responsibilities to private sector groups. The first
of these is the American College of Surgeons
(ACS). The ACS is a scientific and educational
association of surgeons that was founded in 1913
to improve the quality of care for the surgical
patient by setting high standards for surgical
education and practice. The ACS is headquartered
in Chicago, Illinois. AHRQ is located in Rockville,
Maryland, is committed to improving care safety
and quality by developing successful partnerships
and generating the knowledge and tools required
for long-term improvement. AHRQ has been
a financial supporter for the High 5s Project.
Thus the ACS has assumed some of the LTA
responsibilities.
The initial SOP selected to be implemented by
the U.S.A. LTA was Correct Site Surgery (CSS).
At the beginning of 2013, The Wheaton Franciscan
system of hospitals volunteered to assume
responsibility for implementing the Med Rec SOP.
3. Lead Technical Agency structure
The Australian LTA: The High 5s Project sits
within the Commission’s Medication Safety Program
and is overseen by an expert advisory group,
The Medication Continuity Expert Advisory Group,
which comprises representatives from medical,
pharmacy, nursing and consumer organizations,
state and territory departments of health, academia
and individual experts from hospital, residential
aged care and community health-care sectors.
The group advises on the conduct of the Project
and reports through the Commission’s Medication
Reference Group to the Commission Board.
The High 5s Project is supported by a senior
project officer and a project manager who are
responsible for the day-to-day management
of the project activities.
23 The High 5s Project governance, structures and participating organizations

The French LTAs: The National Authority
for Health (Haute Autorité de Santé, HAS) and
the EVALOR/OMEDIT and CEPPRAL teams provide
support and assistance to participating hospitals
with respect to training, SOP implementation,
and data collection, analysis and evaluation.
A national pilot committee, led by HAS, was set up
in 2010 and includes representatives from the
Ministry of Health, sanitary agencies, the patient
community, hospital federations, and scientific
societies. This group met annually during the two
first years of the Project. Two committees (one
for each of the SOPs) – co- chaired by the LTA
and including participating hospital representatives
and scientific experts – have been set up and
convene workshops every six months.
The German LTA: The two LTA partner
organizations in Germany share the tasks and
work closely together in implementing the High 5s
Project on a national level:
ñ AQuMed is responsible for overall project
management, recruiting hospitals,
implementation of the SOPs, supporting the
hospitals, and representing the German LTA on
the international level of the High 5s Project;
ñ on behalf of the German Coalition for Patient
Safety, the Institute for Patient Safety (IfPS)
of the University of Bonn carries out its tasks
in the High 5s Project. The IfPS is responsible
for the evaluation tasks which encompass data
management, analysis and feedback to hospitals.
The Ministry of Health convened an expert advisory
committee consisting of leading national experts
on the SOP topics. The expert advisory committee,
representatives from the Federal Ministry of Health
and the project teams from AQuMed and IfPS meet
yearly to discuss strategic aspects of their
involvement in the High 5s Project.
The Dutch (The Netherlands) LTA: The Dutch
Institute for Healthcare Improvement (CBO)
nominated a project leader and an advisor to
oversee the tasks and work of the High 5s project
in the Netherlands. National implementation
networks for ‘Assuring medication accuracy at
transitions of care’ and for Concentrated Injectable
Medicines SOPs was then established. The
implementation strategy for the SOPs was based
on the ‘Breakthrough Series’ developed by the
Institute for Healthcare Improvement in 1994.
The objective of participating hospitals was to
strengthen both the implementation of the national
guidelines for Medication Accuracy at Transitions
in Care (2008) and High Risk Medication (preparing
for administration) (2009) the Medication
Reconciliation and High Risk themes of the national
patient safety programme (2008-2012).
The Singaporean LTA set up three key structures
that aided the facilitation of the High 5s Project.
First, it engaged two leading anaesthetists from
two of the largest public hospitals in the country as
part-time consultants to help in workflow redesign
of operating theatres. Second, it set up a local High
5s Network comprising surgeons, anaesthetists,
and OT nurse managers from all public hospitals.
Each public hospital has two representatives
participating in this Network. The Network was
co-chaired by the LTA’s two part time consultants.
Third, with regard to implementation of the
Correct Site Surgery (CSS) SOP, the LTA funded
each hospital with an operational executive to
adapt the SOP checklists, collect data, conduct
staff education and address identified gaps.
The Trinidad & Tobago LTA: Letters of invitation
to participate in the High 5s Project were sent from
the Ministry of Health to all five Regional Health
Authorities (RHAs) to participate in the
implementation of the Correct Site Surgery SOP in
October 2011. All five RHAs indicated willingness
to implement this SOP in the surgical units of their
secondary care hospitals. The Health Care Protocol
Officer of the Directorate of Quality Management
of the Ministry of Health is the focal Project person
and liaison with the project teams at the RHAs.
Each project team is headed by a designated Project
Team Leader whose responsibility is to ensure
implementation of the SOP at the surgical units of
the respective hospitals. The Quality Improvement
Units at the RHAs and the Quality Directorate
at the Ministry of Health provide technical and
logistical support.
The U.S.A. LTA: AHRQ has supported the High 5s
Project through an expert consultant, in-house
technical contributions and funding of the global
and technical activities of the Project over a period
of four years. The American College of Surgeons
provides support to the High 5s Project through
two of its staff members who serve as consultants
and provide technical expertise on the Correct Site
Surgery SOP.
24The High 5s Project Interim Report

4. Participating hospitals
Table 2: Participating hospitals in each Member State
25 The High 5s Project governance, structures and participating organizations
Hospital /health service Description
The Alfred Hospital Acute care, 400 bed public tertiary referral hospital in Victoria
Armadale Health Service Acute care, 250 bed public hospital in Western Australia
Epworth HealthCare Acute care, 550 bed private hospital in Victoria
Greater Southern Area Health 9 rural public hospitals in southern New South Wales
Service (9 hospitals) (total of 810 beds across 9 sites)
Logan Hospital* Acute care 390 bed public hospital in Queensland
Mater Health Services (3 hospitals) Tertiary hospital with public and private beds
(in total approximately 1000 beds) consisting of
Mater Adult Hospital (Public)
Mater Children’s Hospital (Public and Private)
Mater Mothers’ Hospital (Public and Private)
Mater Private Hospital in Queensland
Noosa Hospital Acute care, 92 bed private hospital in Queensland
North West Regional Hospital Acute care, 120 bed public hospital in Tasmania
Prince of Wales Hospital Acute care, 550 bed public tertiary referral hospital in New
South Wales
Redland Hospital Acute care, 150 bed public hospital in Queensland
Rockingham Peel Group Acute care, 180 bed public hospital in Western Australia
Royal North Shore Hospital Acute care, 560 bed public tertiary referral hospital in New
South Wales
The Wesley Hospital Acute care, 530 bed private hospital in Queensland
Australia
The Australian collaborative commenced in January
2010 with 18 health services comprising 28 hospitals
recruited through an expression of interest process.
Five health services have since withdrawn from the
project. Reasons given for withdrawal included
changes in priorities, loss of project champions, lack
of resources, and the need to prioritize work to
direct patient care. Participants comprise a mix of
public and private hospitals of differing sizes and
complexity from regional centres and capital cities
in five states. See table 1 for list and description of
the participating hospitals.
(Withdrew from project in October 2012.)

France
A total of 18 health-care organizations (HCO)
were selected (November 2009) and entered
the Project in 2010. The LTA defined selection
criteria* and developed a questionnaire which
was followed-up by an interview conducted
with each potential hospital project coordinator.
Altogether, nine hospitals were recruited for
26The High 5s Project Interim Report
each SOP. In 2011, one hospital withdrew
from the CSS project following the retirement
of the initial surgical lead. Likewise, one hospital
withdrew from Med Rec SOP implementation
because of competing priorities, lack of leadership,
and lack of resources. Currently, eight hospitals
are participating in the implementation and
evaluation of the two SOPs.
CSS hospitals and health facilities Description
St Joseph St Luc Hospital in Lyon Urban, private, non-profit hospital with 344 beds;
multi specialties surgery, medicine and gynecology/obstetrics
Joseph Ducuing Hospital in Toulouse Urban, private, non-profit hospital with 146 beds;
multi specialties surgery, medicine and gynecology/obstetrics
Clinique du Cambresis in Cambrai Private for profit surgical clinic with 50 beds; surgical specialties:
orthopaedic, vascular, ophthalmology, visceral surgery
Centre Léon Bérard Cancer center Urban private non-profit center with 250 beds;
in Lyon multi-specialties surgery including reconstructive surgery
Centre hospitalier de Cornouaille Urban public hospital with 1 044 beds; multi specialties surgery,
in Quimper medicine and gynecology/obstetrics
Centre hospitalier de Chambéry Urban public hospital with 1643 beds; multi specialties surgery,
in Chambéry medicine and gynecology/obstetrics
Centre hospitalier de Bourg en Bresse Urban, public hospital with 584 beds;
Fleyriat in Bourg en Bresse multi specialties surgery, medicine, gynecology/obstetrics
Pasteur hospital, a subdivision of the Urban, public, academic, affiliated hospital with one surgical
Nice University Hospital in Nice specialty (neurosurgery) and 49 beds
Med Rec hospitals Description
Association clinique la Croix Blanche Private health care facilities specialized in surgery;
Moutier Rozeille acute care: 48 beds
Centre Hospitalier Universitaire Nîmes University hospital. acute care: 722 beds; Long Term Care,
Complex Continuing Care: 295 beds; Psychiatry: 265 beds
Centre Hospitalier Saint Marcellin General hospital; acute care: 30 beds; Long Term Care,
Complex Continuing Care: 38; Home Care/Ambulatory: 30/132
Hôpitaux Universitaire Paris Nord Val University hospital Bichat Claude Bernard; acute care: 1 718 beds.
de Seine Beaujon - Bichat-Claude Long Term Care, Complex Continuing Care: 596 beds.
Bernard - Bretonneau - Louis Mourier Psychiatry: 85 beds.
Centre Hospitalier Universitaire University hospital; acute care: 1 388 beds; Long Term Care,
Grenoble Complex Continuing Care: 419; Psychiatry: 54
Centre Hospitalier Compiègne General hospital acute care; acute care: 418 beds; Long Term
Care, Complex Continuing Care: 142 beds; Home Care /
Ambulatory: 37 beds
Hôpitaux Universitaires de Strasbourg University hospital; acute care: 1 854 beds; Long Term Care,
Complex Continuing Care: 287 beds; Psychiatry: 92 beds
Centre Hospitalier de Lunéville General hospital; acute care: 162 beds; Long Term Care,
Complex Continuing Care: 30 beds; Home Care/Ambulatory:
30 beds /132 beds

Germany
Germany currently has 16 hospitals implementing CSS and seven hospitals implemnting the Med Rec SOP.
CSS hospitals Description
Allgemeines Krankenhaus An urban, non-profit, general hospital with 698 beds and nine
Celle Operating Rooms (ORs) in Celle, a town in the northern part of Germany
Altmark Klinikum Gardelegen A small rural, non-profit, general hospital with with 200 beds and three
ORs in Gardelegen, a small town in the north eastern part of Germany
Altmark Klinikum Salzwedel A small rural, non-profit, general hospital with 218 beds, and three ORs.
It is closely linked with the other Altmark Klinikum mentioned above
Evangelische Elisabeth Klinik A small urban, non-profit, general hospital with 160 beds in the center
Berlin of Berlin
Evangelisches Krankenhaus A small urban, non-profit, general hospital with 210 beds and two ORs
Hubertus on the outskirts of Berlin
Evangelische Lungenklinik A small urban, non-profit hospital with 164 beds, two ORs, with
Berlin a specialized thoracic centre on the outskirts of Berlin
Evangelisches Krankenhaus Paul An urban, non-profit, general hospital with 412 beds and eight ORs in
Gerhardt Stift Lutherstadt Wittenberg, a town in the eastern part of Saxony-Anhalt
Evangelisches Waldkrankenhaus An urban, non-profit, general hospital with 474 beds and eight ORs
Spandau on the outskirts of Berlin
Herzogin Elisabeth Hospital A small urban non-profit hospital with 215 beds, six ORs and
an orthopaedic focus in Braunschweig, a town in Lower Saxony
Klinikum Chemnitz An urban, non-profit, general hospital with more 1720 beds and 23 ORs
in Chemnitz, a town in Saxony
Klinikum Coburg An urban, non-profit, general hospital with 522 beds and six ORs
in Coburg, a town in Bavaria
GRN-Klinik Sinsheim A rural, non-profit, general hospital with 225 beds and four ORs
in Sinsheim, a small town in Baden-Württemberg
Martin-Luther-Krankenhaus An urban, non-profit, general hospital with 285 beds and six ORs
in Berlin
Städtisches Klinikum Solingen An urban, non-profit, general hospital with 716 beds and eight
ORs in Solingen, a town in North Rhine-Westphalia
University Hospital Aachen A large university medical center with 1 282 beds and 30 ORs
in Aachen, a town at the border to the Netherlands and Belgium
University Hospital Freiburg A large university medical center with 1 484 beds and 27 ORs
in Freiburg, a town at the border to Switzerland and France
Med Rec hospitals Description
Diakoniekrankenhaus An urban, non-profit, general hospital with 444 beds in Hannover,
Friederikenstift a town in Lower Saxony
Klinikum Lüneburg An urban, non-profit, general hospital with 472 beds in Lüneburg,
a town in Lower Saxony
Klinikum Coburg An urban, non-profit, general hospital with 522 beds in Coburg,
a town in Bavaria. (Note: This is also a CSS hospital)
Städtische Kliniken- An urban, non-profit, general hospital with 577 beds in
Mönchengladbach Elisabeth Mönchengladbach, a town in North Rhine-Westphalia
Krankenhaus
University Hospital Aachen A large university medical center with 1 282 beds and 30 ORs
in Aachen, a town at the border to the Netherlands and Belgium.
(Note: This is also a CSS hospital)
University Medical Center A large university medical center with 1 484 beds and 27 ORs in Freiburg,
Freiburg a town at the border to Switzerland and France.
(Note: This is also a CSS hospital)
University Medical Center A large university medical center with 1 250 beds in Hamburg
Hamburg-Eppendorf
27 The High 5s Project governance, structures and participating organizations

The Netherlands
The Netherlands currently has 15 hospitals
implementing the Med Rec SOP. A total
of 16 hospitals, of which five are also
28The High 5s Project Interim Report
Med Rec hospitals, are implementing the SOP
for Safe Management of Concentrated Injectable
Medicines.
Med Rec hospitals - group 1/2011 Description
Antonius Hospital, Sneek General hospital
Diakonessenhuis, Utrecht, Zeist, Doorn General hospital
Fransiscus Hospital, Roosendaal General hospital
HAGA Teaching Hospital, The Hague Large teaching hospital
Medical Center Alkmaar, Alkmaar Large teaching hospital
Rivas Beatrix Hospital, Gorinchem General hospital
Sint Fransiscus Gasthuis, Rotterdam Large teaching hospital
Tergooi, Hilversum, Blaricum General hospital
Radboud University Nijmegen Medical Centre, Nijmegen Academic hospital
VU University Medical Centre, Amsterdam Academic hospital
Rivierenland Hospital, Tiel General hospital
Med Rec hospitals -group 2/ 2011 Description
Hospital Group Twente (ZGT), Almelo, Hengelo General hospital
Elkerliek Hospital, Helmond Non-teaching hospital
Med Rec hospitals -group 3/ 2012 Description
Gelderse Vallei, Ede Teaching hospital
University Medical Centre, Groningen Academic hospital
Med Rec experts involved in group 1 support Description
Erasmus Medical Centre, hospital pharmacist, Rotterdam Academic hospital
Medical Centre Haaglanden, location Westeinde, Large teaching hospital
ED Nurse Practitioner, The Hague
TweeSteden Hospital, hospital pharmacy technician, Tilburg General hospital
Wilhelmina Hospital, ED doctor, Assen General hospital
CIM hospitals involved in group 1 support Description
Albert Schweitzer Hospital Dordrecht General hospital
Antonius Hospital, Sneek General hospital
Elkerliek Hospital, Helmond Non-teaching hospital
Erasmus Medical Centre, Rotterdam Academic hospital
Flevo Hospital, Almere General hospital
HAGA Teaching Hospital, The Hague Large teaching hospital
Maasstad Hospital, Rotterdam General hospital
Martini Hospital, Groningen Large teaching hospital
Meander Medical Centre, Amersfoort Large teaching hospital
Medical Center Alkmaar, Alkmaar Large teaching hospital
Tergooi, Hilversum, Blaricum General hospital
Rijnland Ziekenhuis Leiderdorp Large teaching hospital
Reinier de Graaf Hospital, Delft Large teaching hospital
St. Jansdal Hospital, Harderwijk General hospital
Van Weel Bethesda Hospital, Dirksland General hospital
Westfries Gasthuis, Hoorn General hospital

29 The High 5s Project governance, structures and participating organizations
Singapore
The following list provides a snapshot of the hospital sizes in Singapore. The smallest is Jurong Health
Services with 400 beds; this hospital will be relocating in a few years’ time to a bigger establishment that will
house 700 beds. The largest hospital is Singapore General Hospital at close to 1 500 beds.
CSS hospitals Description
Changi General Hospital 753 beds www.cgh.com.sg
KK Women’s and Children’s Hospital 739 beds www.kkh.com.sg
National University Hospital 1 007 beds www.nuh.com.sg
Singapore General Hospital 1 449 beds www.sgh.com.sg
Tan Tock Seng Hospital 1 293 beds www.ttsh.com.sg
Khoo Teck Puat Hospital 550 beds www.ktph.com.sg
Jurong Health Services -operating at former 400 beds
Alexandra Hospital site
Trinidad & Tobago
The five public hospitals provide 24-hour general, specialized surgical and medical services to the population.
The patient populations vary among the RHAs. Currently, only four of the five hospitals have piloted the CSS
SOP in their respective surgical units.
CSS hospitals / facilities Description
San Fernando General Hospital An urban hospital of more than 300 beds, with12 in-patient operating
rooms, and 12 344 surgical cases performed in the latest calendar year
Port of Spain General Hospital A regional governmental hospital of more than 300 beds, with six
in-patients operating rooms, and 5 561 surgical cases performed
in the latest calendar year
Sangre Grande Hospital A suburban hospital of 100-299 beds, with three in-patient operating
rooms, and 2 694 surgical cases performed in the latest calendar year
Scarborough General Hospital A regional governmental hospital of 100-299 beds, with two in-patient
operating rooms, and 2 342 surgical cases performed in the latest
calendar year
Eric Williams Medical Sciences An urban academic hospital of more than 300 beds, with 8 in-patient
Complex operating rooms and 4 908 surgical cases performed in the latest
calendar year
United States of America
The following list provides a snapshot of the hospitals participating in the High 5s Project in the U.S.A.
CSS hospitals / facilities Description
Baylor University Medical Center Large Teaching and Research Hospital
Washington University School of Medicine Large Teaching and Research Hospital
Med Rec hospitals / facilities Description
Wheaton Fransiscan Elmbrook Small hospital; part of the Wheaton Fransciscan System
Wheaton Fransiscan Healthcare Franklin Small hospital; part of the Wheaton Fransciscan System
Hospital
Wheaton Fransciscan Healthcare St. Francis Small hospital; part of the Wheaton Fransciscan System
Hospital
Wheaton Fransiscan St. Joseph Hospital Small hospital; part of the Wheaton Fransciscan System
Wheaton Fransiacan Wisconsin Heart Hospital Small hospital; part of the Wheaton Fransciscan System

5. High 5s Steering Group
The Steering Group is responsible for overseeing
the High 5s Project planning, management,
coordination and technical direction as outlined
below:
1) Strategic planning
ñ Political and technical direction.
ñ Strategic planning.
ñ Global and country-level Project advocacy and
capacity building at ministerial levels.
ñ Coordination with associated national institutions
or agencies (not LTAs).
2) Management & coordination
ñ Global coordination of planning and activities;
provision of logistics support and services to
LTAs; and High 5s Project biannual meetings.
ñ Country-level coordination of planning and
activities.
ñ Global communications.
3) Technical functions
ñ Development of Standard Operating Protocols
(SOPs) and the Impact Evaluation Strategy and
related tools.
ñ Support and coordination of High 5s Project
national planning, implementation, data
collection, analysis, and training activities.
ñ Development of a global learning community
and associated tools and services as deemed
necessary for implementation, data collection
and analysis, evaluation and dissemination.
ñ Compilation and active dissemination of findings,
outcomes, improved practices and lessons
learned from the High 5s Project for worldwide
publication.
6. High 5s Project Committees
There are five committees composed of
representatives from the WHO, the CC, and LTAs.
The committees advise, plan, develop and execute
activities and are overseen by the Steering Group.
The committees are:
1. Collaborative Learning;
2. Communications;
3. Evaluation;
4. Event Analysis; and
5. Publications.
Participation within each committee varies
according to the task and activity to be achieved.
The Collaborative Learning Committee was
established to develop an implementation plan
for a High 5s Project core learning strategy
including consideration of target audiences and
levels and mechanisms of learning. Strategies
were collaboratively designed and scheduled
to prepare LTAs and hospitals for the
implementation and evaluation of the three SOPs.
They included in-person train-the-trainer workshops,
provision of online resources, and online posting
of Questions and Answers.
The Communications Committee was established to
develop and implement a High 5s communications
strategy that included consideration of target
audiences and creation of common messages/
themes for global use and for High 5s LTA members
to use within their own countries.
The committee’s objectives are to communicate
the concepts, strategies and actions of the High 5s
Project in an effective manner with particular
attention to:
ñ presenting the political profile of the High 5s
Project to external audiences;
ñ supporting LTA activities with in-country
communications and advocacy;
ñ meeting communication needs of the High 5s
Steering Committee members; and
ñ engaging new partners to participate as part
of the High 5s Project expansion strategy.
The Evaluation Committee has overseen the
development of a consistent, integrated approach
to the High 5s Project evaluation across the SOPs.
Specific activities have included:
ñ development of materials and tools necessary
to carry out the evaluation strategy;
ñ development of performance measures as well
as a method for evaluating the SOP
implementation experience;
ñ development of a process for maintaining
the confidentiality of data and comply with LTA
privacy requirements; and
ñ development and monitoring of the overall
evaluation plan.
The Event Analysis Committee is a subcommittee
of the Evaluation committee which was established
to develop the process by which each participating
hospital would actively identify and investigate
30The High 5s Project Interim Report

a pre-determined set of patient safety problems
(events) that are or could be related to the SOP.
These findings help to determine the effectiveness
of the SOP and are intended to guide future
revisions of the SOPs, as appropriate. Key activities
include:
ñ delineation of SOP-specific prompts for the
identification of SOP-related events for analysis;
ñ establishment of criteria for assessing the
thoroughness and credibility of event analysis;
ñ determination of a minimum data set for the
results of event analyses;
ñ develop a process for submission and review
of the event analyses by the LTA;
ñ creation of a process for submitting an event
analysis report to the Collaborating Center.
The Publications Committee was established to:
ñ identify a potential list of peer-reviewed High 5s
publications;
ñ establish procedures for publishing data under
the High 5s Project; and
ñ develop guidelines that govern publications,
copyright issues, and data ownership and sharing.
31 The High 5s Project governance, structures and participating organizations

4The design of the Project,its protocolsand evaluationframework

1. Design of the Project
The High 5s Project has applied established best
practices and interventions to support the
development of standardized processes and tools.
These processes have included input from all levels
of team members from management to individual
health-care workers. This has also permitted
development of a consistent system of monitoring
that makes the production of comparable results
possible locally, nationally and internationally.
2. Standard Operating Protocols (SOPs)
Each SOP summarizes the problem, proposes
a solution, presents the evidence for the solution,
identifies potential barriers to adoption, and
delineates potential unintended consequences
of the solution. It contains a set of instructions
for implementing a defined patient care process
by multiple users in a consistent and measurable
way. The SOPs were designed to be systematically
implemented using quality improvement methods
that include the following components:
1. oversight of the implementation;
2. project workplan;
3. risk assessment of the proposed process;
4. pilot testing;
5. spread methodology;
6. communication plan;
7. evaluation Strategy;
8. maintenance and Improvement strategy.
Institutions which led the development
of the SOP
In this multi-country collaboration, the Canadian
Patient Safety Institute and the Institute for Safe
Medication Practices in Canada led the
development of the Medication Accuracy at
Transitions in Care SOP. The former National
Patient Safety Agency in the United Kingdom led
the development of the Concentrated Injectable
Medicines SOP. The Joint Commission and the
Agency for Healthcare Research and Quality in
the USA led the development of the Correct Site
Surgery SOP. Participants from all of the LTAs,
the Collaborating Centre, and consultants
associated with Joint Commission International
and the Institute for Safe Medication Practices in
Canada provided technical expertise to support
development of the implementation and evaluation
frameworks that are integral to the SOPs.
3. High 5s evaluation framework
The High 5s Project aims to answer two main
questions:
1. Is it feasible to implement standardized
processes in health care within individual hospitals,
among multiple hospitals within individual
Member States, and across country boundaries?
2. What is the impact of standardization on
the safety problems that the project targets?
The High 5s Project combines process
standardization and intensive evaluation of
the feasibility and impact of implementing SOPs
on a global scale.
A standardized approach to evaluation, the ‘Impact
Evaluation Strategy’ was designed to assess the
feasibility and impact of implementing the SOPs.
Both quantitative and qualitative approaches were
used in this process. The Impact Evaluation Strategy
included structured qualitative and quantitative
evaluation of the SOP implementation experience,
on-site application of SOP-specific performance
measures, use of an event analysis framework to
identify occurrences that may represent SOP
failures, and a baseline hospital patient safety
culture survey. The evaluation strategy identifies
the factors underlying patient safety problems,
matches these problems against those that the
34The High 5s Project Interim Report
The design of the Project, its protocolsand evaluation framework, including anoverview of methodologies, instrumentsand processes

SOPs are trying to prevent, and tracks
improvements in patient safety in the participating
hospitals.
Following LTA and hospital training on SOP
implementation and use of the evaluation
instruments, the materials and tools necessary to
implement each SOP were pre-tested in individual
representative hospitals in participating Member
States for a two-month period. This was done
to permit revisions and adaptations of the SOPs
and their related evaluation processes prior
to full-scale implementation of the SOPs in 2010.
3.1. SOP implementation experience
The goals of the SOP implementation evaluation
process were to determine if one or more SOPs
could be implemented as designed in diverse
hospital settings, to identify barriers to
implementation, and to identify ways to overcome
said barriers. In order to evaluate the fidelity and
portability of SOP implementation in multi-country
settings and environments, self-reported narrative
data was collected at the beginning of the Project,
at six-monthly intervals throughout the project.
Related interview data is also being collected at
selected hospitals annually.
Methodologies, instruments and processes
employed
A narrative of real-world experiences from
individuals engaged in SOP-implementation
provides a deeper understanding of the feasibility
and impact of SOP implementation. On a biannual
(every six months) basis, participating hospitals
from each Member State were asked to complete
a 67-item questionnaire that was divided into
ten sections. These included implementation
status, oversight, work plan, risk assessment,
pilot test, spread methodology, communication
plan, evaluation strategy, events analysis and
maintenance. A summary of this data was compiled,
classified by specific SOP (either Correct Site
Surgery or Medication Reconciliation), and
reported. Hospitals that had already completed
the initial questionnaire were given the option
from the 4th quarter 2012 to complete a brief
implementation update form. This form included
five open-ended questions which were designed
to capture any new information regarding parts
of the implementation experience that had most
likely changed, such as implementation status,
communication strategies, new strategies or
barriers regarding maintenance, efforts to measure
the effectiveness of the SOP, and any experiences
of the hospital that might benefit other
organizations. This brief update form was designed
to reduce the reporting burden on hospitals
and allowed for participants to describe, in only
a few sentences, any significant changes over
a period of six months. Use of this brief update
form was optional; hospitals were given the
option of completing the questionnaire in full.
3.2. SOP-specific performance measures
Implementation of each SOP is evaluated using
performance measures that determine the extent
to which the protocol was followed during
implementation by the participating hospitals
in multiple Member States and enable national
and international comparability of data.
The standard performance measures include SOP
process measures and outcome measures.
Standardization of SOP performance measures
increases data reliability and comparability.
Performance measurement results are presented
in various formats within the High 5s Information
Management System to support LTA and hospital
needs and enable sites to benchmark and trend
their data over time.
35 The design of the Project, its protocols and evaluation framework

36The High 5s Project Interim Report
Performance measures for ‘Medication Reconciliation’
H5sMR-1 Percent of patients with medications reconciled within 24 hours of the decision to admit
the patient
H5sMR-2 The mean number of outstanding undocumented intentional medication discrepancies
per patient
H5sMR-3 The mean number of outstanding unintentional medication discrepancies per patient
H5sMR-4 Percent of patients with at least one outstanding unintentional discrepancy
Performance measures for ‘Correct Site Surgery’
H5sCS-0 Proportion of verification checklists for all eligible surgical cases
H5sCS-1 Proportion of eligible surgical cases with a complete preoperative verification process
(exclusive of site marking and Time Out)
H5sCS-2 Proportion of cases with properly marked surgical site
H5sCS-3 Proportion of cases with complete final Time Out
H5sCS-4 Proportion of cases with discrepancy noted at final Time Out
H5sCS-5 Proportion of cases undergoing surgery with unresolved Time Out
H5sCS-6 The proportion of surgical cases that are cancelled or postponed due to discrepancies
identified at any point in the conduct of the SOP
H5sCS-7 Proportion of cases with incorrect surgery (wrong site, procedure or person cases).
Performance measures for ‘Concentrated Injectables’
H5sCI-01 Time between concentrated injectable adverse events
H5sCI-02 Time between adverse drug events delay or omission of administration of injectable medicines
H5sCI-03 The number of adverse events for specified concentrated injectables per 1 000 patient days
H5sCI-P1 Concentrated injectable medicines stored in unauthorized clinical areas
H5sCI-P2 Concentrated injectable medicines supplied to unauthorized clinical areas
H5sCI-P3 Ready-to-administer and ready-to-use injectable medicines supplied to unauthorized clinical
area
H5sCI-P4 The number of clinical areas storing concentrated injectable medicines according to selected
SOP specifications
Although performance measures for the implementation of the ‘Concentrated Injectables’ SOP were
developed, implementation data were not collected.
Data quality
Data and information provided and collected
have to be accurate to ensure a credible evaluation.
The aim is to reach a level of data quality
consistent with the limits of precision that are
achievable with respect to the analytic tools
and sample sizes defined for use in the High 5s
Project. Only data that has been confirmed to
meet the data quality criteria by both the hospital
and the LTA is included in performance measure
calculations.
Methodologies, instruments and processes
employed
The performance measure data is normally
collected at monthly intervals in the secure
High 5s IMS and international evaluation reports
are generated at quarterly intervals. A list of the
performance measures for each SOP is provided
below.

National and international comparison
data calculations
a) Country-level data (national comparison)
Country-level data points are calculated using
a similar approach to the one employed for
calculating an individual hospital’s performance
on a specific measure. The major difference is
that for rate and ratio measures, all the hospital
numerator cases (from within a specific Member
State) are summed, and all of the hospital
denominator cases (from within a specific Member
State) are summed before calculating the measure
rate or ratio. The measure is calculated in the
aggregate for all hospitals in a Member State
during the specific time period. This calculation
creates a weighted mean (weighted by the number
of cases contributed by each hospital) rather than
a grand mean (simply taking the average of the
calculated hospital rates). The approach is slightly
different for continuous variable measures (used
for the Concentrated Injectables SOP). For these
measures, the comparison group value is:
b) International-level data (international
comparison groups)
International-level data points are calculated
using a similar approach to the one employed
for calculating an individual hospital’s performance
on a specific measure. The major difference is
that for rate and ratio measures, all the hospital
numerator cases (from all Member States) are
summed and all of the hospital denominator cases
(from all Member States) are summed before
calculating the measure rate or ratio. The measure
is then calculated in the aggregate for all hospitals
contributing data during the specific time period.
This calculation creates a weighted mean (weighted
by the number of cases contributed by each
hospital) rather than a grand mean (simply taking
the average of the calculated hospital rates or
the average of the national rates). The approach
is slightly different for continuous variable
measures (used for the Concentrated Injectables
SOP). For these measures, the comparison group
value is:
c) Requests for measure revisions
Over the course of the Project, a number of
requests to revise the measures were submitted.
The Evaluation Committee considered each request
and made recommendations to accept or reject
the modification based upon the nature of the
request and the degree to which it would impact
longitudinal analyses. To date, there have been
nine requests for measure revision: four were for
measures related to Medication Reconciliation,
three were for Correct Site Surgery, and two were
for Concentrated Injectables.
In order to reduce data collection burden, Australia
requested to reduce the frequency of data
collection for measures MR 2, 3 and 4 for hospitals
that had met an established performance threshold.
The request was approved and hospitals that
had consistently met a defined threshold were
permitted to submit data quarterly. If a hospital
later failed to meet the threshold, it would then
return to monthly submissions until it could meet
the expected benchmark for three consecutive
months.
Canada requested a 24-hour time boundary for
measures MR 2, 3 and 4. This request was approved
because it allows for standardization and ease
of data collection across all participating Member
States.
Australia also requested changes to measures
MR 2, 3 and 4. Specifically, they requested a tighter
definition of what are to be included as documented
intentional discrepancies and unintentional
discrepancies. They further asked for specific
examples of inclusions/exclusions. Finally, they
requested additional language that would state
that “medications prescribed for the first time
on admission are intentional discrepancies and
shouldn’t be included.” These requested changes
were approved.
A request was made by the United Kingdom,
and approved, to revise the measure statements
for measures CI-02 and CI-03 to include the
intended patient populations. In order to increase
understanding of the SOP and to be consistent
with measure CI-P1, that measure statement
was changed to indicate that measure events
are restricted to only those that caused harm
to patients.
The United Kingdom also made a request to
change the value statement for measure P1
37 The design of the Project, its protocols and evaluation framework
Σ (each hospital value* the number of cases upon
which that value was based)
Σ of hospital cases
Σ (each hospital value* the number of cases upon
which that value was based)
Σ of hospital cases

to read “It is important to monitor whether
concentrated products are held in stock in
unauthorized clinical areas.” Because measure
P1 is not intended to measure the number of
concentrated products held in stock, but instead
measures the number of unauthorized clinical
areas storing concentrated products, this change
was approved and the language was amended
in the performance measure value statement.
The U.S.A. requested that a new measure, CS-0,
be created. This measure would capture the percent
of eligible cases having a pre-operative verification
checklist (total number of checklists/total number
of eligible cases). This measure was created based
on the assumption that it will help ensure that the
correct data are used in the performance measure
calculations.
Because of ambiguity in the labeling of the
numerator data element for CS-1, Germany
requested that the name of the numerator
data element be changed from “Completed
Pre-Operative Verification Checklist” to “Number
of Eligible Surgical Cases with a Completed
Pre-Operative Verification Process”. Because
this change clarified the intent of the measure
to ensure standardized data collection, this change
to the data element was approved.
3.3. Event analysis
An ‘event’ is defined as an occurrence that happens
to or involves a patient and which could have
resulted, or did result, in unnecessary harm to the
patient.
The evaluation framework includes an Event
Analysis (EA) component that directs each
participating hospital to actively seek and
investigate a pre-determined set of patient safety
problems (events) that should have been prevented
in the clinical setting by the SOP. Hospitals
are then asked to report specific de-identified
information regarding the case to their LTA for
review and submission to the High 5s Collaborating
Centre.
Event analysis is undertaken after a patient safety
incident takes place and aims to determine
whether there is a link to the SOP implementation
and, if so, whether factors in the design and/or
implementation of the SOP contributed to
the occurrence of that incident. The event analysis
process yields important information as to
the functioning of the SOP, as well as how
to improve the SOP and its implementation.
In order to effectively identify events for analysis
beyond those that are independently reported,
participating hospitals have been expected to use
the specifically designed methods, including chart
audits and checklist reviews (where applicable).
Minimum Data Set (MDS) forms and checklists
were also developed to ensure thorough and
credible event analysis and methodical de-identified
reporting of specific SOP-related events. Where
appropriate, aggregate or cluster event analysis
processes were applied where certain events
appeared to have common characteristics, in order
to identify patterns of performance.
There are four types of events:
1. Hazard: a circumstance, agent or action
with the potential to cause harm;
2. Near miss/Close Call/Good Catch: an event
which did not reach the patient;
3. No-harm: an event which reached a patient
but no discernible harm resulted;
4. Adverse: an event which resulted in harm
to a patient.
Event analysis is defined as a systematic process
whereby the facts, contributing factors and
resultant recommendations are identified and
reported as a means of investigating an event.
This aspect of the evaluation framework was
intended to go beyond fact-finding, and to help
understand the applicable contributing factors.
The EA process provided an unprecedented
opportunity to obtain and analyze findings
regarding the safety and effectiveness of the SOPs.
The complexity of developing and implementing
the SOPs delayed the High 5s Steering Group
in finalizing and implementing the EA evaluation
process. The Event Analysis Subcommittee
played a key role in formalizing the proposed EA
instructions for the participating hospitals.
After the approval by the Steering Group,
the instructions were posted on the High 5s
Information Management System (see Annex 4A
and 4B for the EA Overview for the Medication
Reconciliation and Correct Site Surgery SOPs).
Each LTA provided specific instructions to
participating hospitals regarding the methodology
to be used by their participating hospitals to
perform the event analysis. Where an LTA did not
38The High 5s Project Interim Report

have a preferred methodology, they could adopt
one of the established event methodologies
identified by the Event Analysis Subcommittee
and approved by the Evaluation Committee.
The sources of these methodologies were:
1. National Patient Safety Agency
http://www.nrls.npsa.nhs.uk/resources/?entryid45=5
9901
2. United States Department of Veterans Affairs
National Center for Patient Safety
hhttp://www.patientsafety.gov/CogAids/RCA/
3. Canadian Patient Safety Institute
http://www.patientsafetyinstitute.ca/English/toolsR
esources/IncidentAnalysis/Pages/default.aspx
4. The Joint Commission
http://www.jointcommission.org/Framework_for_Co
nducting_a_Root_Cause_Analysis_and_Action_Plan
The Collaborating Centre offered specific
training in any of the above methodologies
requested by an LTA. Most, but not all,
participating LTAs had in-country EA expertise
and a standardized tool for analyzing events after
they were identified. Some LTAs needed to first
invest time and resources in building this capability
before attempting to implement the High 5s EA
evaluation process.
The EA principles were specified to facilitate a
consistent, timely, thorough and credible approach.
The goals of EA were to determine:
1. what happened?
2. why did it happen?
3. how can the likelihood of recurrence of this
event be reduced?
Four types of ‘Event analysis’ were defined:
1. Concise
Event analysis of these occurrences is usually
conducted by someone who is aware of the details
of the event and is knowledgeable about
the involved process and effective solutions.
The EA process is often completed within hours
or days because of the less intensive approach.
Events without patient harm may receive Concise
Event Analysis or Cluster Analysis.
2. Comprehensive
Event analysis is undertaken by an inter-disciplinary
group of staff and physicians that is facilitated
by a person(s) who is knowledgeable about the
involved process(es), human factors and effective
solutions development. The process may take up
to 90 days because of the depth and breadth of
the analysis. Events resulting in patient harm
should receive ‘Comprehensive Event Analysis’.
3. Aggregate
This is the optional but recommended process
of analyzing data combined from the findings
of several completed event analyses (concise
or comprehensive) of similar event characteristics,
in order to identify patterns of causation
and enhance the effectiveness of actions for
improvement.
4. Cluster analysis
This is a process for analyzing three or more no-
harm events having similar event characteristics as
a group in order to identify patterns in causation
and enhance the effectiveness of actions for
improvement. Cluster analysis may be used instead
of concise analysis if there are three or more
no-harm SOP-related events of the same type
within a month.
Identification of events for analysis
Initial development of the EA evaluation involved
creation of a trigger tool for chart reviews in order
to identify wrong site surgeries or medication
reconciliation failures. The Australian LTA provided
key expertise and leadership in pilot testing this
strategy. Eventually an agreed upon strategy was
formalized and implemented for the identification
of events.
A. Medication Reconciliation events
Med Rec events are process issues or outcomes
that are possible SOP-related events. Examples
include:
ñ ‘Best Possible Medication History’ (BPMH) not
obtained and/or reconciled within 24 hours
of decision to admit;
ñ inaccurate or incomplete BPMH;
ñ inaccurate or incomplete resolution of any
discrepancies;
ñ all discrepancies not resolved within 48 hours
of decision to admit.
Two primary sources of SOP events for analysis are:
1. independently reported adverse events during
or after the SOP is implemented;
2. independent ‘Observer Chart Audits’.
39 The design of the Project, its protocols and evaluation framework

Chart audits are a defined independent double-
check strategy to assess the quality of the
Medication Reconciliation “process” that is
performed in hospitals as part of the evaluation
strategy to collect performance measures. During
audits by the independent observer to measure MR-
2 – MR-4, medication reconciliation process
events/issues identified are flagged for EA.
B. Correct Site Surgery events
CSS SOP events are process issues or
outcomes that are possible SOP-related events.
Examples include:
ñ wrong site surgery;
ñ wrong limb prepped for surgery but error
discovered before incision occurred.
Two primary sources of SOP events for analysis are:
1. independently reported adverse events during
or after the SOP is implemented;
2. retrospective SOP checklist review.
The SOP checklist is a defined requirement to
document steps in preparing each patient for
surgery and for recording the outcomes relevant
to the SOP. There are four outcomes requiring
analysis that may be identified by a member
of the health-care team concurrently and/or, a
reviewer of the checklists on a retrospective basis:
ñ incorrect surgery (wrong patient, procedure,
site or implant)
– Hospital completes a Comprehensive Event
Analysis;
ñ case that proceeds to incision with unresolved
discrepancy
– Hospital completes a minimum of a Concise
Event Analysis;
ñ case cancelled because of SOP-related
discrepancy
– Hospital completes a minimum of Concise
Event Analysis;
ñ case with discrepancy resolved at final Time Out
– Hospital completes a minimum of Concise
Event Analysis.
Hospitals can decide to complete a Comprehensive
Event Analysis of certain events at their discretion.
For these cases, they are also asked to consider
aggregate analysis of any group of related
individual event analyses. For no-harm cases of
the same type in these categories, which occur
at a frequency of three or more per month, cluster
analysis can be conducted.
Data collection and reporting
The ‘Event Analysis- Minimum Data Set’
(MDS) forms were developed to capture the key
findings of the analysis. Hospitals were asked
to complete all fields of the applicable forms,
and attach any additional information at their
discretion, before submission to their LTA.
The LTA would subsequently review the submission
and follow-up with the applicable hospital
to ensure that all information was properly
de-identified, understandable and complete.
Criteria for accuracy and completeness are defined
in Annex 5A and 5B. The LTA would then submit
this data to the Collaborating Centre, where
the information would be combined for analysis
and de-identified High 5s reporting. The
information would also be combined with
other evaluation findings to determine if any
changes should be made to the SOP.
3.4. Patient safety culture surveys
The ‘Hospital Survey on Patient Safety Culture’
was developed by Westat under contract with
the Agency for Healthcare Research and Quality
(AHRQ). The survey and accompanying toolkit
materials are available from the AHRQ website
www.ahrq.gov/qual/hospculture. In the context
of the High 5s Project the culture survey was
conducted as an additional voluntary evaluation
component to provide insight into the patient
safety culture of hospitals participating in the High
5s Project and to sensitize frontline staff and
hospital management about staff members’
perception of the hospital’s patient safety culture.
At the time the survey was administered,
participating Member States included Australia,
France, Germany, the Netherlands, Singapore
and the United Kingdom. The Project then included
the Medication Reconciliation, Correct Site Surgery
and Concentrated Injectables SOPs.
The survey, designed to assess hospital staff
opinions about patient safety issues, medical error,
and event reporting, included 42 items that
measure 12 areas or composites of patient safety
culture. Each of the 12 patient safety culture
composites is listed and defined in Table 3.
The survey also included two questions that
asked respondents to provide an overall grade
for patient safety for their work area/unit and
to indicate the number of events they had reported
over the past 12 months. In addition, respondents
40The High 5s Project Interim Report

Table 3: Patient safety culture composites and definitions
Patient safety culture Definition: The extent to which…composite
1. Communication openness Staff freely speak up if they see something that may negatively
affect a patient, and feel free to question those with more authority
2. Feedback and communication Staff are informed about errors that happen, given feedback about
about error changes implemented, and discuss ways to prevent errors
3. Frequency of events reported Mistakes of the following types are reported: (1) mistakes caught
and corrected before affecting the patient, (2) mistakes with no
potential to harm the patient, and (3) mistakes that could harm
the patient, but do not
4. Hand-offs and transitions Important patient care information is transferred across hospital units
and during shift changes
5. Management support for Hospital management provides a work climate that promotes patient
patient safety safety and shows that patient safety is a top priority
6. Non-punitive response Staff feel that their mistakes and event reports are not held against
to error them, and that mistakes are not kept in their personnel file
7. Organizational learning– Mistakes have led to positive changes and changes are evaluated
continuous improvement for effectiveness
8. Overall perceptions Procedures and systems are good at preventing errors and there
of patient safety is a lack of patient safety problems
9. Staffing There are enough staff to handle the workload and work hours are
appropriate to provide the best care for patients
10. Supervisor/manager Supervisors/managers consider staff suggestions for improving
expectations and actions patient safety, praise staff for following patient safety procedures,
promoting safety and do not overlook patient safety problems
11. Teamwork across units Hospital units cooperate and coordinate with one another to provide
the best care for patients
12. Teamwork within units Staff support each other, treat each other with respect, and work
together as a team
41 The design of the Project, its protocols and evaluation framework
Participating hospitals expressed interest in
comparing their results with those hospitals
in other participating Member States, as it provided
a new source of information to help them identify
and understand potential differences in patient
safety cultures across Member States. For this
reason AHRQ produced the High 5s ‘International
Comparative Report’ (see Annex 2).
The report presented survey administration and
respondent statistics across the Member States,
as well as percent-positive results on the patient
safety culture composites and survey items.
Comparative results from U.S.A. hospitals included
in the AHRQ Hospital Survey on Patient Safety
Culture 2011 Comparative Database Report were
also provided.
were asked to provide limited background
demographic information about themselves
(e.g., their work area/unit, staff position, whether
they had direct interaction with patients).
France, the Netherlands, and Germany translated
the survey for administration in their countries.
The United Kingdom, Singapore, and Australia
administered the survey in English, using an edited
version of the U.S. English version.

5Qualitative andquantitativeinterim findings

1. Summary of culture survey findings
Data from 6 Member States with a total of 59
hospitals was collected and analyzed for reporting
purposes (Table 4). The High 5s participating
hospitals administered the hospital survey to their
staff between November 2009 and November
2010 and voluntarily submitted their data for
inclusion in the database. The U.S.A. database
numbers are based on the AHRQ Hospital Survey
on Patient Safety Culture 2011 Comparative
Database Report.
44The High 5s Project Interim Report
Qualitative and quantitative interim findings
Table 4: Survey administration statistics
Member State Survey administration statistics High 5s SOP
No. of Total No. Total No. Overall
hospitals of completed of staff asked response
surveys to complete survey rate
United Kingdom 12 2 657 Not Available Not Available Concentrated Injectables
Singapore 7 18 204 23 792 77% Correct Site Surgery
France 7 621 1 000 62% Correct Site Surgery
Germany 5 1 083 3 881 28% Correct Site Surgery
Australia 24 3 485 8 410 41% Medication Reconciliation
The Netherlands 4 127 253 50% Medication Reconciliation
High 5s Total 59 23 520* 37 336* 63%*
* High 5s ‘Totals’ in these columns do not include United Kingdom due to missing data.
On average, hospitals across Member States scored
highest on teamwork within units (70% positive),
and scored lowest on handoffs and transitions
(34% positive). The hospitals in Singapore were
the most positive on seven of the 12 composites,
and were also the least positive on two of the
composites. The hospitals in the Netherlands were
the most positive on five of the 12 composites,
and were also the least positive on two of
the composites. The hospitals in Germany were
the least positive on four of the 12 composites.
The hospitals in Singapore had the smallest
variability on all 12 composites across participating
hospitals. Singaporean hospitals also had the
highest average composite score (58%) while
German hospitals had the lowest (46%) average
composite score. The U.S.A database hospitals
were more positive on four of the 12 composites
and more positive or equal on all 12 composites
in comparison to the High 5s average scores.
The hospitals in the United Kingdom had
the highest percentage of respondents giving
the work area/unit a patient safety grade of
an ‘A-Excellent’ or ‘B-Very Good’ (60%), while
hospitals in the Netherlands had the lowest
percentage (21%). Hospitals in the Netherlands
had the highest average percentage of respondents
reporting one or more events (78%), while
hospitals in Singapore had the lowest (37%).

Culture survey results by staff position were as
follows:
ñ the High 5s average composite score for all
physicians/consultants/medical officers was 51%,
with a low of 47% in Germany to a high of 54%
in Singapore;
ñ the High 5s average composite score for nursing
was 53%, ranging from 45% for the Netherlands
to 60% for Singapore;
ñ the High 5s average composite score for allied
health professionals was 55%, ranging from 49%
for Germany to 58% for France;
ñ the High 5s average composite score for
administration/ management was 57%, ranging
from 49% for France to 69% for Netherlands.
Survey and data limitations
The survey results represented a large compilation
of international patient safety culture survey data
and therefore provided a useful reference for
international comparisons. However, the following
limitations apply to these data and should be kept
in mind when considering the data:
1. The High 5s hospitals included for the report
were not a statistically selected sample of all
hospitals within each participating Member State
and therefore were not necessarily representative
of the status of the patient safety culture within
each Member State.
2. The number of hospitals and the number
of respondents varied greatly by Member State.
For instance, Singapore submitted data from
seven hospitals and 18 204 respondents, while
Australia submitted data from 24 hospitals
and 3 485 respondents. Given this wide range
of participation, the ability to generalize
the comparability of the results is limited.
3. Hospitals administered the survey in different
ways. Most hospitals used paper only, while
others used web only, and still others used
a combination of these two methods of data
collection. It is possible that these different
methods led to mode effects in the survey
scores. In addition, some hospitals surveyed all
hospital staff, while others administered the
survey to a sample of staff in selected work
units/areas. In cases in which a sample was used,
no information was available to determine
the method used to select the sample.
4. Differences in scores across Member States may
relate to a number of factors other than true
differences in patient safety culture, making
direct comparisons among Member States
complicated. For instance, there may be
significant cultural differences across Member
States in how respondents interpreted the survey
items and the ways in which they used the
response scales. In addition, there are differences
in the way health care is structured and provided
across Member States that could affect
responses. Furthermore, survey translations
were developed by individuals within the
Member States, but were not tested or externally
validated before administration.
5. The data was cleaned for out-of-range values
(e.g., invalid response values because of data
entry errors) and blank records (where responses
to all survey items were missing). Otherwise,
data was presented as submitted. No additional
attempts were made to verify or audit the
accuracy of the data submitted.
1.1. Culture surveys in participating Member
States
Australia
All participating hospitals were requested to
complete the AHRQ Patient Safety Culture Survey.
Seven hospitals chose to administer the survey
throughout the hospital, while the remainder
administered it in their emergency departments,
wards and services participating in the Project.
All hospitals administered the survey as hard copies
with one exception where a mix of paper and
online surveys was used. Twenty four hospitals
participated in the survey.
The survey was conducted between May 2010
and December 2010.
Australian hospitals reported high positive
responses to three patient safety culture
composites: teamwork within units (77%);
management support for patient safety (71%); and
organizational learning – continuous improvement
(69%). Conversely, only 34% reported a positive
response on handoffs and transitions; 39% of staff
surveyed believed that staffing levels were
sufficient for patient care; and only half (49%)
reported a positive response to teamwork across
units (Table 1 in Annex 6).
45 Qualitative and quantitative interim findings

Analysis of the data for the hand-offs and
transitions composite found a variation in patient
safety culture across work areas and among
the different categories of staff. Clinical handover,
staffing, teamwork across units, and engaging with
junior medical staff were identified as potential
areas for improvement. Hospitals were encouraged
to review their individual survey results and to:
ñ identify:
– lowest scoring safety culture composites
across items, unit areas, and staff areas and
look for linkages;
– areas for improvement;
– places where additional qualitative data
needed to be collected; and
– stakeholders who should be engaged in
improvement activities
ñ discuss possible improvement strategies; and
ñ develop and implement an action plan for
improvement and evaluate the plan impact.
France
The French LTA decided that only the ‘Correct Site
Surgery (CSS)’ participating hospitals would
complete the AHRQ culture survey, as the workload
of the ‘Medication Reconciliation’ participating
hospitals for the implementation and evaluation
of this SOP was considered too great to permit
their participation in the culture survey.
All of the CSS participating hospitals (nine in 2011)
were asked to complete the AHRQ culture survey,
but two of them did not participate: one because
of organizational issues (delay in the implementation
of the project) and the other because management
did not approve the administration of the survey.
In the seven participating hospitals, 1 000 surveys
were sent out and 620 completed responses were
received (42% to 95% in the various hospitals).
Questionnaires translated in French were distributed
either hospital-wide (three hospitals) or in the units
directly involved in SOP implementation in
the four other hospitals. The LTA trained all
the project coordinators and supplied to each
hospital a tool-kit with communication models.
The challenge encountered by the project hospital
coordinators was the lack of time to explain the
safety culture survey and to collect the surveys.
The areas with the three top scores were teamwork
within units (59%), organizational learning –
continuous improvement (58%) and openness of
communication (56%). Areas with the three lowest
scores were:
ñ handoffs and transitions (39%);
ñ non-punitive response to error (32%); and
ñ management support for patient safety (28%).
The overall level of patient safety was reported
to be between acceptable to excellent by 94% of
respondents. Feedback of the results was provided
to the front line staff and managers by the LTA via
conference call and site visit. Participating in the
High 5s Project was considered to reflect positively
on the safety culture.
Germany
Participation in the AHRQ culture survey was
voluntary, but was encouraged by the LTA. Only
the hospitals implementing the Correct Site Surgery
SOP were invited to take part in the survey, because
at the time the culture survey was administered
internationally, the ‘Medication Reconciliation’
hospitals had not yet been recruited in Germany.
Some of the participating hospitals were keen
to administer the survey a second time in order
to compare the results.
All hospitals had concerns regarding data
protection and had to obtain consent from
the works council and management approval.
Therefore the last section of the questionnaire
(Section H: Background Information) had to be
modified in a way that made identification of
an responder impossible.
Five of the 16 CSS hospitals participated in the
first survey and a total of 1 083 questionnaires
were completed (response rate of approximately
30%). In the second survey three of these five
hospitals participated and 252 questionnaires
were completed.
For the summary of culture survey findings from
Germany, see Annex 14.
The Netherlands
Dutch hospital participation in the culture survey
was not mandatory. Four hospitals completed
the culture survey in 2010 and after SOP
implementation in 2011. They adapted the culture
survey as an implementation intervention to create
awareness among healthcare professionals.
46The High 5s Project Interim Report

Table 5: Returned questionnaires and response rates
Before SOP implementation After SOP implementation
Distributed & returned Response rate Distributed & returned Response ratequestionnaires questionnaires
Hospital A 12/37 32% 22/50 44%
Hospital B 12/40 30% 20/42 48%
Hospital C 23/26 88% 13/25 52%
Hospital D 80/150 53% 91/160 57%
Total 207/403 51% 146/277 53%
In addition, Singapore tied with United Kingdom
for the lowest score of 36% for staffing.
Nonetheless, Singapore hospitals had the highest
average composite score of 58% with the lowest
score being 46% by German hospitals. In terms
of the average percentage respondents reporting
one or more events, Singapore had the lowest
reporting culture at 37%, while the Netherlands
had the highest at 78%.
It would seem that the drivers for Singapore’s
patient safety culture lie in its strong organizational
learning-continuous improvement culture with
a score of 81%, management support for patient
safety with a score of 75%, and teamwork across
units with a score of 62%.
The Singaporean LTA is currently working
to encourage a culture of reporting mishaps
by issuing patient safety alerts with each report
so that institutions see the value in reporting
as the reports are used to help other institutions
avoid the same errors. Every six months, a sharing
session is organized so institutions can learn from
each error report and treat reporting as a learning
opportunity rather than a punitive event.
Trinidad & Tobago
The aim of the AHRQ culture survey was to gain
an understanding of hospital priorities and
strategies regarding surgical safety. All five
hospitals were required to complete the survey,
and all five submitted completed survey forms
to the Directorate, Health Services Quality
Management, of the Ministry of Health. Only
one survey was conducted in May 2012 at each
of the five participating hospitals.
47 Qualitative and quantitative interim findings
No particular challenges were encountered in
evaluating the patient safety culture in participating
hospitals. After SOP implementation, hospitals
scored higher on most Patient Safety Culture
Composites. On the three composites of
communication openness, feedback and
communication about error, and frequency
of events reported, hospitals had low scores.
Before and after SOP implementation, management
support for patient safety was unchanged.
To define drivers for patient safety, positively
worded items, which about 75% of respondents
endorsed by answering “Agree/Strongly agree,”
or “Most of the time/Always”, were identified
as strengths. The Netherlands did not utilize
other mechanisms to evaluate the patient safety
culture in the 15 participating hospitals, but there
are many patient safety activities and projects
in Dutch hospitals.
Singapore
The Singaporean LTA facilitated the AHRQ
culture survey by asking all participating hospitals
to complete the questionnaire in March 2010.
Overall, there were not many challenges
encountered in requiring hospitals to complete
the survey. Singapore obtained a total of 18,204
respondents, a 77% overall response rate.
The overall survey results for Singapore hospitals
showed that they were the most positive on seven
of the 12 composites, though they were the least
positive on two of the composites, namely:
1. non-punitive response to error (27% as
compared to the highest score of 62% in the
Netherlands); and
2. communication openness (44% as compared
to the highest score of 77% in the Netherlands).
Table 5 shows the distributed and returned questionnaires and response rates.

2. Context survey of MedicationReconciliation
The context for implementation of the Med Rec
SOP in the participating Member States is very
different and its implementation varies greatly in
terms of numbers of hospitals, teams and support.
The context survey focused on identifying barriers
encountered by the participating Member States,
as well as the role of external drivers and supports
such as accreditation requirements and national
policies. Despite many differences in the context
of implementation, most Member States, reported
similar barriers and facilitators when implementing
the SOP.
The most significant barriers to Med Rec
implementation reported by all Member States
were a lack of staff and financial resources.
The most significant facilitators included
the presence of an accreditation system,
pharmaceutical reforms and state policies,
standards of practice for Med Rec, and internal
leadership/internal ambassadors for Med Rec
within a hospital. A variety of health-care
professionals have been involved in creating
the ‘Best Possible Medication History’ (BPMH) in
the different Member States.
Although the High 5s SOPs were expected to be
implemented in acute care settings, there were
efforts to extend Med Rec SOP implementation
across the system in several Member States.
Canada’s experience in this area suggests that there
48The High 5s Project Interim Report
Box 2: The context survey
At the September 2011 High 5s Steering Group
meeting, it was agreed that it would be useful
to examine the context of the implementation
of the Med Rec SOP in those Member States
implementing the SOP – Australia, France,
Germany and the Netherlands.
The objective of the context survey was to
identify:
ñ the current landscape of Med Rec in the
individual Member States;
ñ barriers and drivers affecting implementation
in the participating Member States;
ñ successful tools and resources which could be
shared globally.
Information was collected using an online survey.
is a real need for improved communication
and medication reconciliation from each health-
care setting through to home care. There are
many differences of health-care systems across
the participating Member States. For example,
in Germany, there are few, if any, pharmacists
in hospitals, which makes implementation of this
SOP challenging, while in the Netherlands a link
with community pharmacy dispensing databases
supports effective communication about
medications. In light of such differences it
is particularly commendable that four Member
States have chosen to implement this SOP.
Limitations
Participating Member States and hospitals across
and within Member States are in different stages
of implementation of the Med Rec SOP and operate
within very different health-care systems. Within
the context survey, it was difficult to differentiate
Med Rec activities implemented in health-care
settings outside the High 5s Project and those
within the High 5s Project. The survey results reflect
a point in time and not a continuous timeline.
Some general considerations
The primary objective of the context survey was
to provide information on the context in which
the High 5s Med Rec SOP was implemented to
understand what external factors were influencing
the uptake of Med Rec in the different Member States.
This information was collected in addition to
the quantitative performance data and hospital
implementation experience data collection.
The survey did not attempt to correlate hospital
results and accreditation performance, but rather
to determine whether sharing standards, resources,
and experiences learned from the context survey
could assist LTA’s to implement the SOP more
effectively.
Further, best practice tools and resources
obtained from the implementing teams of some
LTAs are available to be shared among the other
participating LTAs and hospitals. For example,
Canadian tools which are part of the High 5s
toolkit are uploaded onto the High 5s Wiki portal
as they are updated by ISMP Canada. Member
States with relevant Med Rec policies or
accreditation standards were able to share policy-
related information for the benefit of other
Member States.

reconciliation. The certification/accreditation
guidelines encourage hospitals to implement
several practices that should eventually evolve
towards a more generalized implementation
of medication reconciliation. For example,
the management system for pharmaceutical care
should take into account the need to ensure
continuity of medication reconciliation from
admission to discharge, including internal transfers.
Patients should be encouraged to pass on
information regarding their medications to
health-care professionals on admission and every
time they receive care. The latter depends on how
proactive a patient is.
The national guidelines for drug management
are consistent with the certification/accreditation
procedure of the National Authority for Health
The safety of drug therapy, in particular, regarding
the prevention of medication errors has become
a major focus of national policy. A February 2012
circular recommends understanding the therapeutic
management of the patient as a process and calls
on focusing on high risk patients and high risk
medication, as well as addressing the prevention
of ‘never-events’ related to drugs and organizations.
Germany
Medication reconciliation is a relatively new
activity in Germany which, prior to involvement
in the High 5s Project, has not been systematically
implemented and evaluated in German health-care
facilities. Medication safety is a key priority for
the Federal Ministry of Health, as evidenced by
its issuance of national “action plans for the
improvement of medication safety in Germany”
for the years 2008-2009 and 2010-2012. These
action plans list specific medication safety
measures, including Med Rec elements, to be
developed and tested in these time frames.
In addition, the German Society of Hospital
Pharmacists has published a statement in which
Med Rec is described as a practice of pharmacists
to support physicians and nurses.
In Germany, hospitals have a legal obligation to
introduce and use a quality management system.
Additionally hospitals can voluntarily be accredited
according to a large variety of programmes.
The degree to which medication safety standards
are included in the quality management systems
or certification criteria varies by programme.
49 Qualitative and quantitative interim findings
2.1. Medication Reconciliation context survey
findings in Member States
Australia
Major drivers for Australian hospitals to participate
in the High 5s Project included national and state
policy, public hospital pharmaceutical reforms,
and National Safety and Quality Health Service
Standards1. The existing Australian Pharmaceutical
Advisory Council Guiding principles to achieve
continuity of medication management, 2005
(Guiding principles)2 aligned with the High 5s Med
Rec SOP. Australian states and territories
implementing hospital pharmaceutical reforms
required participating hospitals to implement
the Guiding principles and report performance
measure data. In some states, there were incentives
for hospitals to perform Med Rec.
National Safety and Quality Health Service
Standards, 2011, contain two criteria relating
to medication reconciliation. In January 2013,
it became mandatory for all hospitals to be
assessed against these standards as part of the
new Australian Health Service Safety and Quality
Accreditation scheme.
Clinical pharmacy practice is well established in
Australia, and professional practice standards
for medication reconciliation have been available
since 20073. Medication reconciliation in hospitals
is almost exclusively performed by pharmacists.
The increasing number of pharmacists employed in
emergency departments has contributed to the spread
of medication reconciliation in Australian hospitals.
The Australian Commission:
ñ continues to develop resource materials to
support the spread of medication reconciliation;
ñ works with stakeholder organisations to gain
multi-disciplinary buy in; and
ñ advocates improved access to patient medication
information through information systems such as
the Personally Controlled Electronic Health
Record (PCEHR).
France
Medication reconciliation is not one of the
requirements of the certification/ accreditation
procedure of the National Authority for Health.
However, it is mandatory for all health-care
organizations to be fully involved in medication

The Netherlands
The Dutch Government developed a National
Patient Safety Programme (2008-2012) to support
hospitals in obtaining a certified system by
December 2012. Hospitals are required to
implement ten improvement themes to reduce
preventable harm and reach the theme goals.
Prevention of medication errors through medication
reconciliation for elective patients and at discharge
was one of those themes. The Netherlands have
a national guideline for medication accuracy at
transitions in care which recommends a current
medication history within 24 hours for every patient
at every transition. The Med Rec SOP supports
the implementation of the national guideline for
medication accuracy at transitions in care (2008).
The application of the guideline of the Dutch
Inspectorate of Health has been mandatory since
January 2011. In addition, health insurance
companies are playing a greater role in negotiations
with hospitals about safe care for clients.
There is an accreditation and/or certification
initiative overseen by the national patient safety
programme (2008-2012). Another accreditation
body is the Netherlands Institute for Accreditation
in Healthcare (NIAZ); however, hospitals are not
required to be accredited. The first (non-High 5s)
hospital was accredited by Joint Commission
International (JCI) in 2012 and the second in 2013.
3. Context survey of Correct Site Surgery
The context survey on Correct Site Surgery
was conducted to better understand the existing
supporting structures for this SOP. Two Member
States returned completed CSS context surveys.
These were France and Germany.
Key questions on the CSS context survey addressed
reasons for selecting the CSS SOP, formal
expectations for CSS-related procedures which
existed prior to the introduction of the High 5s
Project, requirements for reporting events outside
of the hospital, and surgical safety requirements
of accreditation systems.
Germany and France selected CSS as one of
the SOPs to implement because of an increased
awareness of the topic of wrong site surgery
resulting from the WHO Safe Surgery campaign
and expert/media exposure. In Germany, more
and more hospitals started to implement surgical
safety checklists and the responsible quality
officers in the hospitals were looking to exchange
implementation experiences and advice. In line
with this, hospitals interested in joining the High 5s
Project were asked which SOPs they were interested
in, and CSS was the top topic chosen. In France,
health-care professions were putting an increased
emphasis on serious adverse events.
While there were no formal expectations of
having a surgical checklist in operating theatres
in Germany, a national surgical safety checklist,
inspired by the WHO Surgical Safety Checklist,
was implemented in France and mandated in 2010.
This checklist also became a requirement for
accreditation in France. In Germany,
implementation of surgical checklists was driven
by published recommendations by the Coalition
for Patient Safety and various scientific and medical
societies.
In Germany, while it is not mandatory to report
events outside of hospitals, hospitals can
voluntarily report ‘no harm’ events and
occasionally harm-events to inter-institutional
Critical Incident Reporting Systems databases.
It is mandatory in France to report any serious
adverse events and voluntary to report near misses.
France has a universal accreditation system.
Pre-operative verification and final time-out for
any surgery are required as part of the mandated
process. There were no financial incentives offered
50The High 5s Project Interim Report

in either Member State for quality improvement.
However, negative consequences such as
conditional accreditation, was associated with
poor performance in France. In Germany, various
certification programmes exist for hospitals,
and each one applies different criteria relating
to surgical safety.
4. Interim findings
4.1 Summary of qualitative findings
Implementation Status
The full scope of implementation of an SOP
is defined as follows:
1. all of the required steps in the process are
standardized;
2. all of the locations where those steps are to be
put into effect are involved;
3. the population of patients to which those steps
will apply (the eligible population) is involved.
A hospital is considered to be at ‘Full
implementation’ when it has put all required
components of the SOP into effect across all
eligible locations and patient populations
within the hospital. Once the SOP has been fully
implemented, the degree to which it has been
successfully implemented is determined primarily
through hospital’s self-reporting the experience
(i.e., the ‘Implementation Experience’
questionnaire) and through the High 5s
performance measure results.
For purposes of analyzing and reporting evaluation
data, the count of hospitals reporting their level
of implementation at ‘Full implementation’ is based
upon their self-reported status at the time each
quarterly report is generated (typically two weeks
prior to the release of the report).
To date, six Member States have been
implementing either the Correct Site Surgery SOP
or the Medication Reconciliation SOP or both.
One Member State initiated implementation
of the Concentrated Injectables SOP in 2013.
Implementation of this SOP was terminated
because the United Kingdom withdrew from
the High 5s Project. Table 6 shows the
implementation status of the SOPs.
51 Qualitative and quantitative interim findings
Table 6: Implementation status reported by LTAs
Standard No. of No. of No. of hospitals No. of hospitals No. of hospitals
Operating Member States hospitals indicating indicating with no indication
Protocol implementing implementing ‘Full ‘Not Full of Implementation
SOP SOP Implementation’ Implementation’ status
Correct Site Surgery 4 34 24 9 1
Medication Reconciliation 5 47 11 34 2
Concentrated Injectables 1 16
The primary reasons reported for not having
achieved full SOP implementation in all
participating hospitals and for both SOPs have
been:
ñ insufficient resources;
ñ lack of existing policies;
ñ competing priorities;
ñ inadequate support from leadership; and
ñ resistance to change.
Qualitative findings on Correct Site Surgery
Oversight of SOP implementation
The majority of hospitals assembled
a multidisciplinary group as a means to implement
the SOP. Membership of the oversight group
typically included nurses (operating theater nurses,
anesthesia nurses, nurses from various surgical
subspecialties, nursing directors), surgeons,
physicians (various specialties), patient safety
officers, quality directors, quality assurance
officers and other quality personnel, controllers,
risk managers, department chairs/chiefs of
services/directors of care, hospital administrators,

consultants, secretaries, and other administrative
personnel. Frequently, a principle leader in the
oversight group was identified as the individual
who guided the SOP implementation process.
In addition, more than half of hospitals indicated
that they had role models or “champions”
who assisted in the implementation process.
The most common challenge or barrier to
assembling the oversight group was the lack
of resources (funding and/or time). Resistance
to change and staff buy-in were also frequently
cited as significant barriers. Other barriers noted
by participating hospitals included poor
communication; lack of organizational leadership
buy-in/support, and lack of department leadership
buy-in/support. One participating hospital noted
that the data collection and validation processes
are labor intensive and required at least one
dedicated full-time employee. Another hospital
described difficulty in scheduling meetings,
especially when physicians and surgeons were
involved.
To overcome these barriers, hospitals employed
the following strategies:
ñ improving communication;
ñ obtaining leadership support;
ñ providing training/education on the SOP;
ñ developing strategies to manage change, involve
staff, improve the safety culture, increase
communication, and provide recognition; and
ñ requesting assistance from the LTA.
Risk assessment
Half of the participating hospitals reported that
they conducted a risk assessment as part of the SOP
implementation process. Of those that conducted
a risk assessment, the majority indicated that
they followed the process described in the SOP
materials. Most hospitals reported that the risk
assessment process helped them identify potential
areas for breakdown and allowed them to
implement controls, warnings or protections
to minimize identified problem areas. Through
the risk assessment process, one hospital identified
emergency cases and patients in non-surgical
departments as potential areas for breakdown/
failure. Controls were then put in place to include
a monthly check of operating room cases, use
of pre-operative checklists, and instructions that
only patients with a completed checklist can enter
the operating room theatre. Other hospitals
developed printed guides and posters to remind
staff to adhere to the SOP, and implemented new
processes for administrative staff (as well as
surgeons) to verify the operating room log.
Lack of staff involvement, resistance to change,
lack of experience in conducting risk assessments,
and lack of resources were the primary barriers to
conducting risk assessments in approximately half
of the hospitals. Others claimed that the process
was already implemented, hospitals were already
aware of their risks, the event was considered too
rare to make it necessary, or they did not think that
it was a requirement to conduct a risk assessment.
Pilot testing
Almost all of the hospitals reported that pilot
testing was conducted prior to full SOP
implementation. Pilot testing was conducted to
help hospitals determine the feasibility and impact
of SOP implementation on a small scale before
widespread implementation occurred. Pilot tests
were carried out in several units/wards including
the operating theatre/surgical ward and orthopedic
surgery, thoracic surgery, and gynecology services
as well as other general wards. The major
challenges and barriers to conducting pilot tests
were resistance to change, data collection burden,
and lack of resources. To address these barriers,
hospitals increased communication, enlisted staff
and leadership support, and provided education/
training. Despite challenges, the majority of
hospitals that conducted pilot testing reported
that it positively impacted related activities and
patient care.
Hospitals noted that the pilot tests increased
awareness of safety before the surgical operation,
assisted in encouraging pre-surgical operative
site-marking, and increased attention to verifying
patient identity.
Spread methodology
Approximately half of the responding hospitals
implemented the SOP sequentially in various
hospital locations. The other half implemented
the SOP concurrently in all sites. Three quarters
of responding hospitals integrated the SOP process
into or added it to existing systems processes.
Lack of staff buy-in, resistance to change, lack
of resources and data collection burden were
frequently cited barriers to spreading SOP
implementation. Increased communication, training
and education on the SOP, and leadership support
were the most commonly employed strategies
to address these barriers. One hospital reported
52The High 5s Project Interim Report

that the project was discussed in the medical
commission, and this led to additional resource
allocation for the project. Another hospital
provided continued training on the checklist
procedure, conducted audits, and utilized the
checklist training kit. Still some indicated that,
despite efforts, the barriers and challenges
continued to be a struggle.
High 5s Project information has been most
commonly shared during department and project-
specific meetings. Staff feedback has often been
solicited directly by High 5s project coordinators.
Most hospitals reported some formal
acknowledgement of staff members that actively
participated in the implementation of the SOP.
Recognition often occurred at project meetings,
grand rounds and in printed materials such as
newsletters.
Evaluation
Approximately three quarters of responding
hospitals indicated that they experienced challenges
and barriers in implementing the performance
measures. The primary barriers were lack of
resources (funding and time) to gather the data,
difficulty understanding the performance measure
definitions and/or methodology, and lack of staff
buy-in. For this reason, many hospitals reported
that they were not using the prescribed High 5s
data quality methodology.
Strategies to address barriers included improved
communication with staff that had access
to needed data, engaging staff, and enlisting
the help and guidance of those in leadership
positions. Additional steps taken to evaluate
SOP implementation included observation audits,
development of training programmes, computerized
checklists, and development of databases to assist
in the extraction of performance measure data.
One hospital noted, “With the High 5s SOP,
between 2010 and 2012, we were able to prevent
12 potential events in pre-operative patients.
We analyzed these events and found that nine
errors occurred during surgical consultation,
two errors occurred during site marking in
the surgical unit and one error from the primary
care physician (wrong side written on the letter
to the surgeon).”
Strategies for maintenance and improvement
Most of the hospitals reported that they had been
engaging in regular and ongoing monitoring
of key aspects and activities related to the SOP.
Hospitals were performing data quality monitoring,
conducting audits (chart and electronic),
soliciting information from staff, and engaging
in project oversight meetings. Many hospitals
identified opportunities for improvement that
included better involvement of staff, more training,
better definition of the site-marking procedure,
simplification of the checklist, IT system
enhancements, improved communication with
surgeons, and revision of the time-out process.
In many cases, opportunities for improvement
had been identified but not resolved. Many
hospitals reported ‘drifting’ from the intended
SOP as time went on. The drifting was identified
through data quality monitoring. To address
drifting, hospitals provided increased
educational/training opportunities and encouraged
participation in project-related meetings.
Qualitative findings on Medication
Reconciliation
Oversight of SOP implementation
Hospitals which responded to this issue reported
that they had assembled an oversight group to help
implement the SOP. Oversight groups usually
consisted of pharmacists, nurses, physicians,
quality managers, and a variety of other staff
working in the patient safety area. The majority
of respondents said that the principal leader of
their oversight group was a pharmacist or pharmacy
manager. Lack of resources (funding/time) was
the most common barrier to assembling the
oversight group. More effective communication,
training and education on the SOP, and securing
leadership “buy-in” were common strategies to
address the challenges associated with assembly
of an oversight group. Several hospitals noted
the importance of expanding participation of key
stakeholders beyond the pharmacy.
Risk assessment
Less than half of responding hospitals completed
a risk assessment. The primary reason for not
conducting a risk assessment was lack of resources
(time and funding). In addition, risk assessment
was considered a low priority activity for some
hospitals. These hospitals already had processes
in place for medication reconciliation, so found it
unnecessary. However, those who did conduct
53 Qualitative and quantitative interim findings

a risk assessment reported that it was beneficial in
helping to identify potential areas for breakdown.
In response to the risk assessment, a number
of hospitals implemented controls, warnings
or protections to minimize the potential for
breakdown or failure. Examples of controls and
protections that were implemented as a result of
a risk assessment include improved communication
through the hospital quality committee
and the medication management committee,
multi-disciplinary events analysis, and monthly
pharmacist meetings to implement actions
and monitor and review progress.
Pilot testing
Almost all of the hospitals completing the
questionnaire conducted a pilot test of the SOP.
For those that did not, lack of resources, data
collection burden, lack of organizational support
and resistance to change were cited as the most
common barriers. Pilot tests occurred in a variety
of units, including geriatrics, internal medicine,
rheumatology, emergency and cardiac care.
Routine auditing, use of independent observers,
development of specific forms and procedures,
and training and education on the SOP were
the most common methods hospitals used to
assure the consistency, timeliness and accuracy
of the implementation. Most hospitals reported
that implementation of the SOP had a positive
impact on related activities and on patient care.
Increased communication and more collaboration
among hospitals, physicians and community
health-care providers was a result of the pilot
test noted by many hospitals. Many pharmacists
indicated that they enjoyed being more directly
involved in patient care and that implementation
of the SOP improved the visibility, importance
and understanding of the role of the pharmacist in
the patient care process. Although some indicated
that implementation of the SOP increased staff
workload, most reported that it was a positive
experience that led to improved electronic
prescribing systems, new patient safety projects
related to medication reconciliation, and funding
for additional studies.
Spread methodology
Approximately half of the respondents implemented
the SOP sequentially in their hospitals. Many noted
that the SOP was just an extension of their existing
medication reconciliation process. Several
challenges to implementation were noted. These
included lack of resources, data collection burden,
insufficient communication, and resistance to
change. To overcome these barriers, hospitals
most frequently provided training and education,
increased communication, involved staff in the
process, and provided greater leadership support.
Despite these efforts, several hospitals noted
that many barriers still existed to successful SOP
implementation.
High 5s Project information has been most
commonly shared during department and
project-specific meetings. Staff feedback was
often solicited directly by High 5s Project
coordinators. Most hospitals reported some
formal acknowledgement of staff members
who actively participated in the implementation
of the SOP. Recognition often occurred at
project meetings and grand rounds and in printed
materials such as newsletters.
Evaluation
More than three quarters of responding hospitals
indicated that they experienced challenges or
barriers when implementing the SOP performance
measures. The primary barriers/challenges were
lack of resources dedicated to evaluation, lack of
staff to perform the required independent observer
role, lack of understanding/clarity regarding the
performance measure definitions and methodology,
and difficulty accessing medical records for
data collection purposes. Some hospitals also
experienced technical issues with sampling
and achievement of high inter-rater reliability.
In addition, some hospitals noted that nurses,
physicians and patients were dissatisfied with
the process because patients were asked twice
about current medications with no clear advantage.
One hospital noted that quality improvement,
alone, is insufficient to motivate behavioral change.
To address these barriers, most hospitals attempted
to better engage staff and provide training and
educational support on the evaluation component
of the project. Others provided additional
resources and staff such as a dedicated pharmacist
to work on the project and assist with timely
data collection. One hospital utilized students for
data collection and maintained a log of clinical
scenarios that are encountered and are outside
the realm of the SOP.
Many hospitals have taken additional steps to
evaluate the implementation of the SOP. These
include analysis of interventions by pharmacists
in response to unintentional medication
discrepancies, analysis of the number of errors
detected through timely medication reconciliation,
54The High 5s Project Interim Report

and attempts to build a business case for
an extended-hours model to present to hospital
executives and clinical staff. One hospital noted
that, in the future, they intend to measure patient
and physician satisfaction with the medication
reconciliation process.
Strategies for maintenance and improvement
Participating hospitals took many different
approaches to monitor the implementation
process, including data quality monitoring, project
oversight meetings, audits (direct observation
and chart review), soliciting information from staff,
and participation in LTA interviews. Several
hospitals indicated that they continue to struggle
with concurrent data collection and are several
months behind.
Hospitals provided examples of improvement
strategies that included development of data
collection forms, development of written
instructions/processes, training for data collection,
and increasing documentation required of pharmacy
staff. Through the auditing process, many hospitals
noted “drifting” from the intended SOP process.
To address drifting, additional project meetings
occurred and supplemental education/training
was made available to staff.
Summary of qualitative findings: successes
and lessons learned
At this stage of the High 5s Project, it is clear
that it is possible to implement specific patient
safety protocols with some degree of
standardization across multiple hospitals and
multiple Member States.
Participating hospitals were able to successfully
implement the key components of both the CSS
and Med Rec SOPs. However, the SOPs could not
be implemented as “one-size-fits-all” solutions.
Some local customization of each protocol
was necessary. This local customization (at both
the country-level and hospital-level) was essential
to secure initial buy-in. Customization was equally
important for sustaining post-implementation
changes.
Analysis of project data and the qualitative
experiences of project participants will be used
to produce a final set of SOPs that highlight
key components of the SOP, as well as offering
recommendations for local customization.
Interim lessons learned are summarized below.
A. General lessons learned
ñ Data collection is burdensome. Many
organizations have struggled to identify
adequate resources for data collection. Very
few organizations added resources for the
High 5s Project, thus providing little earmarked
staff time for SOP implementation, much less
the associated data collection activities.
ñ Data collection and measurement are absolutely
necessary for successful implementation
(i.e., they helped demonstrate the need for SOP
implementation, they provided the implementation
team with a tool for demonstrating the impact
of implementation efforts, and the act of data
collection and feedback of measure results helped
hospitals maintain attention on the patient safety
area).
ñ Resistance to change (staff and leadership)
is a challenge to implementation.
ñ Ongoing communication, education, and training
are important to achieve and sustain compliance
with the SOPs.
ñ Senior-level hospital leadership and support is
critical to the full and successful implementation
of the SOPs.
ñ On-site champions are critical to successful
implementation.
ñ The exchange of information among hospitals
(within Member States) and among LTAs (across
Member States) helped to build and maintain
enthusiasm for SOP implementation.
B. Med Rec SOP
ñ Implementation of this SOP was most successful
when a pharmacist (or pharmacy staff) was
available to perform the medication reconciliation.
ñ Pharmacists and pharmacy technicians tended
to produce timely and accurate BPMHs.
ñ Limited pharmacy resources were a major
limiting factor for implementation.
ñ Additional performance measures (or different
measures) were useful. In particular, measures
that identified the number of medication
discrepancies within 48 hours of admission,
and those discrepancies unresolved at 48 hours
from admission, were used to demonstrate
the importance of the SOP to clinicians and
decision makers.
55 Qualitative and quantitative interim findings

C. CSS SOP
ñ Surgeon resistance was a common challenge
to SOP implementation. Thus, placing a surgeon
in the role of SOP champion tended to facilitate
implementation.
ñ Concerns that patients may be resistant to site
marking were unfounded.
ñ In the absence of specific direction from
the Ministry of Health, the High 5s checklists
were not adopted “as-is.” Successful and
sustained implementation required customization
of the checklist so that it could be incorporated
into existing tools (i.e., once adopted, it is much
more difficult to terminate implementation if
the checklist is built into existing processes).
4.2. Member State implementation experiences
and qualitative findings
Australia
LTA role in implementation
Hospitals were recruited through an expression
of interest process, and 18 health services were
selected to participate. The project commenced
in January 2010 with the first teleconference
which was attended by over 60 participants from
the 18 sites. Teleconferences continued to be held
monthly throughout the first two years. In year
three, they were reduced to every second month.
A two-day train-the-trainer workshop was held
in Sydney on 19- 20 April 2010 and was attended
by 64 participants from the 18 health services.
A second two-day workshop was conducted in
October 2010 and two further one-day workshops
were conducted in 2011. Several webinars were
also held to provide further detail on the project
methodology. A table of the activities conducted
for the Australian sites is available in Annex 7.
Copies of all presentations and materials used
were placed on the Australian page of the High 5s
website. The sites were supported by a dedicated
project officer.
Resources
The Australian Commission developed a number of
resources to assist hospitals to implement the SOP.
These included:
ñ A national Medication Management Plan (MMP)
form to record the ‘Best Possible Medication
Histories’ (BPMH), and document the reconciliation
process, discrepancies and their resolution;
ñ Educational materials for health-care
professionals using the MATCH UP Medicines
theme;
ñ Information for consumers.
Examples of the resources are available in Annex 9.
Evaluation
Implementation experience was evaluated
through the use of the implementation experience
questionnaire, hospital interviews, and direct
feedback from sites (see Annex 8). All sites
were requested to complete the implementation
questionnaire as per the schedule set by
the Steering Group. Response rates were high.
Five hospitals were identified to participate in LTA
implementation interviews. A mix of hospitals
was selected from four states: a major teaching
hospital, a private hospital, two metropolitan
hospitals and a rural and regional health service
(nine hospitals). The first round of interviews
was conducted in 2011.
Challenges encountered
Ten out of 11 health services responding to
the implementation experience questionnaire
in June 2012 had implemented all the steps in the
medication reconciliation (Med Rec) process; five
health services had yet to spread the process to all
locations. Insufficient resources and competing
priorities were the most frequently identified reasons
for not implementing the SOP in all locations.
Eight sites identified lack of resources as a barrier
to implementing the SOP. Hospitals said they
underestimated the resources they would need,
especially for education and the evaluation process
(the independent observer role, collection of
performance measure data, and the event analysis).
The burden of the data collection for performance
measures MR 2-4 was an ongoing issue for all sites.
Lack of resources for data collection delayed the
start of data collection at several sites.
The five sites interviewed indicated that additional
resources were needed to implement and sustain
the SOP. This was particularly the case for hospitals
that introduced the process in pilot wards and then
moved to spread the process throughout the facility.
Hospitals opting to employ nursing and medical
56The High 5s Project Interim Report

staff to take the BPMH found they had to allocate
extensive time to initial and ongoing training.
Resistance of health-care professionals other
than pharmacists to engage in the process
was another challenge for Australian hospitals.
Prior to commencement of the High 5s Project,
several hospitals had an existing medication
reconciliation process in place that had been
provided by pharmacy staff. These hospitals had
a culture of medication reconciliation being
“pharmacy business”. The hospitals experienced
challenges on weekends and after hours when
pharmacists were unavailable and when
pharmacists were on leave.
In those hospitals where attempts were made
to involve nursing staff and training was provided,
there was resistance among the nursing
staff to take on increased activities as well as
a lack of confidence in their ability to participate
in the process – it was seen as ‘not their job’.
Two examples of barriers to Med Rec
implementation are presented in Box 3.
57 Qualitative and quantitative interim findings
Initially, independent observers had difficulty with
understanding the performance measures and
measuring consistently. Tightening the definitions
of the types of discrepancies, providing additional
training, and creation of a list of examples helped
overcome this problem.
Other challenges experienced in implementing
the SOP were those commonly experienced when
implementing quality improvement projects:
ñ competing priorities in the organization;
ñ lack of support from hospital leaders;
ñ loss or transfer of key personnel;
ñ initial lack of clinician buy-in; and
ñ the introduction of an electronic health record
that did not support the SOP.
‘Drivers’ of patient safety
Sites utilised a number of strategies to overcome
the barriers to implementing the SOP and effect
change in their organizations.
a) Engaging staff and obtaining ‘buy-in’.
Hospitals actively engaged staff in the project.
All sites assembled a project oversight group.
All groups included pharmacists and most included
nurses. Doctors, quality and safety personnel,
educators, and hospital leaders also participated.
Nine of the 11 health services designated at least
one role model or champion from each discipline
involved in SOP related activities. Most hospitals
developed a communication plan and used a variety
of methods to communicate with staff about
the project. These included regular feedback
on performance measures and periodic reports on
specific aspects of the project.
b) Training and education
Educating staff about the medication reconciliation
SOP and training staff on taking a BPMH and
reconciling medicines were key to the successful
implementation of the SOP. Hospitals devoted
considerable resources to training and employed
a number of different approaches to education.
Two examples of training and education on taking
a BPMH are presented in Box 4.
Box 3: Barriers to Med Rec SOP implementation in Australian hospitals
Hospital 1. Eight emergency department registered nurse “Pioneers” were trained to take a BPMH
and conduct medication reconciliation however one year later these ‘Pioneers’ were not performing
these processes, anecdotally because of time constraints.
Hospital 2. Nursing staff were not confident in conducting medication reconciliation on their own
despite the training provided. Barriers to successful implementation by nursing staff were cited as time
constraints, inadequate staff to perform the process, and lack of in-depth pharmaceutical knowledge.

c) Leadership support
Securing leadership support was cited by several
sites as one of the key strategies they employed for
overcoming the challenges and barriers experienced
in trying to spread the SOP throughout the
organisation.
d) Actions taken based on data
Data was used in a number of ways by the different
sites including:
ñ obtaining buy-in to the project and engaging
staff outside the pharmacy, including senior
clinicians and the hospital executive;
ñ building a business case to extend the hours
that medication reconciliation is performed;
ñ showcasing the quality of the process performed
by staff and addressing any training needs
identified;
ñ identifying gaps in processes and addressing
these gaps; and
ñ demonstrating the hospital’s compliance with
the National Safety and Quality Health Service
(NSQHS) Standards for accreditation purposes.
Two examples of positive outcomes based on data
are presented in Box 5.
58The High 5s Project Interim Report
Box 4: Training and education on taking a BPMH in Australian hospitals
Hospital 3 introduced medication history taking using BPMH principles as part of medical intern
orientation each year, followed by more focused case-based workshops on medication matching
for interns, residents and registrars.
Hospital 4 developed a simulation exercise to train clinicians (doctors, nurses and pharmacists) and
students to take a BPMH. The hospital had access to a simulation ward and experienced facilitators
who worked with the High 5s team at the hospital to develop the simulation exercise. A number
of different scenarios were developed, and the participants were able to access different sources
of information during the exercise, such as calling the patient’s community pharmacist – played by one
of the hospital pharmacists. The use of simulation has the advantage of providing a safe environment
for clinicians to practice their skills with no risk to patient care. It also allows participants to receive
immediate feedback and to learn from others, including the patients.
Box 5: Positive outcomes based on data in Australian hospitals
Hospital 3. The dissemination of Med Rec performance measure results from the top levels in the
hospital down through the Patient Safety Sub-Committee, including to hospital executives, has resulted
in executive engagement.
Hospital 5 used the performance measure data to restructure their clinical pharmacy duties by changing
to a team-based structure and increasing the number of BPMHs completed and medication
reconciliations documented.
e) Effect on patient care
About half the hospitals indicated that
implementation of the SOP had an impact on
related or interacting activities and on patient care.
Most were considered positive and included:
ñ having a standard and improved protocol for
medication reconciliation;
ñ improving processes through raising awareness
of the processes of obtaining a BPMH, reconciling
medicines and following up on discrepancies; and
ñ using data collected to plan interventions to
follow up on discrepancies.
Implementation Surprises
The first surprise was the realisation by the sites
that the SOP could not be implemented with
existing resources and additional resources would
be required to perform the medication reconciliation
process and spread the process to a greater number
of patients. Several hospitals were able to secure
funding to employ additional pharmacists to
introduce clinical pharmacy services to Emergency
Departments and extend clinical pharmacy hours.
Box 6 presents two examples of pharmacist services
that were extended over weekends.

Private hospitals experienced difficulty implementing
the SOP, as their staffing and work practices
differ from public hospitals. Pharmacy services
are limited, and there are no junior medical staff.
Another surprise was the time commitment
required for education and training, particularly
at those sites implementing a multidisciplinary
approach to medication reconciliation. In addition,
junior medical staff regularly rotate through
a number of hospitals, requiring a new cohort
to be trained every three months.
All sites were surprised that collection
and management of the data for the performance
measures and the event analysis was so
burdensome. This resulted in delays in data
collection and reporting, particularly when
there were staff changes and departing staff
were not replaced.
Several sites were surprised by the number
of discrepancies identified by the independent
observer that remained unresolved 48 hours
after admission. Initially, up to as many as 53%
of patients at these sites had unresolved
discrepancies. Sometimes these discrepancies
were still unresolved at the time of discharge,
causing delays in discharge. Two additional
performance measures were developed to enable
hospitals to collect data on these discrepancies
(see section 5.4.5)
The introduction of an electronic health record
(EHR) in the ED in some hospitals that did not
support the medication reconciliation SOP
resulted in duplication of work and threatened
the continuation of the project in one site.
This was completely unexpected and highlighted
the importance of project teams being aware
of information technology initiatives and engaging
with IT services when introducing system changes.
Lessons learned
Successful implementation of the medication
reconciliation SOP hospital wide requires:
ñ recognition that medication reconciliation
is a patient safety priority;
ñ senior leadership support;
ñ resources;
ñ ongoing training; and
ñ integration of the process with hospital
information systems.
Further information technology systems on the
Australian medication reconciliation resources
is provided in Annex 9.
France
LTA role in implementation
Hospitals were recruited to implement the Correct
Site Surgery (CSS) and Medication Reconciliation
(Med Rec) SOPs through an expression of interest
resulting in commitments by 18 health-care
organizations – nine hospitals for each SOP–
to participate in and initiate the Project in 2010.
Subsequently, one hospital withdrew from the CSS
project following the retirement of the initial
surgical lead. Likewise, one hospital withdrew
from Med Rec SOP implementation because of
competing priorities, lack of leadership, and lack
of resources. Monthly communication with
the hospitals was done through teleconferences.
Currently, eight hospitals are participating in
the implementation and evaluation of each SOP.
A. Correct Site Surgery SOP
Evaluation
Monthly performance data were edited in an Excel file
created to generate numerators and denominators.
A sample of 20 anonymous checklists per hospital
was reviewed by the LTA every month. The LTA
59 Qualitative and quantitative interim findings
Box 6: Pharmacist services extended over weekends in Australian hospitals
Hospital 7: Pharmacy clinical services have increased over the past three years to include weekends
and pharmacist services to the emergency department have been extended to 21:00 hours.
Hospital 2: Initiation of a Saturday ward-based clinical pharmacist service responsible for medication
reconciliation on new, high-risk admissions at a metropolitan hospital significantly improved
performance measure MR-1 rates.

provided monthly feedback to the project hospital
coordinators through a conference call and
a report. This feedback aimed to promote the
correct use of the checklist and to help the hospital
teams to define the actions required to maintain
or improve reliable performance measurement.
Time Out observational audits were conducted in
addition to the monthly questionnaire, interviews
and event analyses required by the SOP.
Challenges encountered
During the first two years of the High 5s Project
(2010-2011) the challenges included:
ñ Difficulties in integrating the High 5s Checklist
into the WHO Surgical Safety Checklist.
Promoted by HAS, the WHO Checklist became
mandatory in the French accreditation/certification
process in 2010. This checklist does not include
an expectation of site-marking, while the High 5s
Checklist does. With the support of CEPPRAL,
each participating hospital team worked towards
integrating the checklists, and developed an
individualized checklist that included all mandatory
SOP items, while still retaining other items and
the format of their choice. Some health-care
organizations (HCOs) had worked on the patient
clinical pathway and had developed a booklet that
included similar procedures already implemented
before initiation of the High 5s Project.
ñ Surgical site marking as required by the CSS SOP
was new to all hospital teams. Its implementation
caused organizational challenges. The reluctance
of some surgeons to comply with this
requirement was one of the challenges.
ñ It took one year before CEPPRAL was able
to transmit data from participating hospitals
to the Collaborating Center. Only four HCOs
had valid data in 2011, but all eight HCOs had
valid data in 2012.
Disseminating information and lessons learned
remains a challenge, as half of the participating
hospitals are still at partial implementation.
With regard to the four hospitals at full
implementation, the lack of specific resources
dedicated to the project has been a persisting
challenge for evaluation – in terms of review
of performance measure data and analysis
of events – and communication. The duration
of the project and the turnover of staff (e.g., key
leaders, surgeons, risk managers) has also been
a challenge.
For most hospitals, the main barriers encountered
have been lack of time to form multidisciplinary
teams; develop leadership; achieve cultural
changes; and mobilize surgeons and anesthetists.
In addition, challenges encountered by a few
hospitals have included competing priorities and
lack of logistic support.
‘Drivers’ of patient safety
Across all hospitals the following stood out
as strong drivers for patient safety:
ñ performance measures (see example at Box 7);
ñ benchmarking; and
ñ generation of “success stories” (see example
at Box 8).
60The High 5s Project Interim Report
Box 7: Communicating results of performance measures by two French hospitals
Because of the resistance of some surgeons to implementing site-marking and Time Outs as required
in High 5s CSS SOP, and in an effort to motivate participation, two hospitals communicated on
a monthly basis the results of performance measures for a given surgeon. This was done by e-mail
(individual results) and also posted outside the operating theatre (anonymously).
Box 8: Success stories are about errors stopped during the pre-operative phase
Teams were requested to report errors not evaluated in the High 5s Project to the LTA which assessed
their frequency and time of occurrence and identified the steps where the errors had been intercepted.
Up to the present, about 20 success stories have been collected. Annex 13 presents the framework used
to collect such success stories.

Implementation surprises and lessons learned
ñ Commitment of paramedical staff (technicians
and administrative staff) to the High 5s Project.
ñ Rapid uptake of the High 5s checklist by
substitute nurses working during summer period
in ORs and on the wards (reported by one
HCO).
ñ Streamlining the Time Out (e.g., through
the use of key words) provided teams with
better communication and valuable Time Out
(1 HCO).
ñ About 70% of all errors were intercepted in
the pre-operative verification phase.
ñ Site-marking was well-accepted by the patients,
none refused the site-markings.
ñ A culture change was seen where members
of the non-medical staff felt empowered
to speak up when discrepancies arose.
ñ Great involvement of frontline staff; and
ñ Greater participation of patients in the
verification procedures.
B. Medication Reconciliation
Challenges encountered
ñ The appropriation of the Med Rec protocol
by various teams, as well as inadequate
understanding of the performance measures.
ñ Resistance to the BPMH completion deadline
of 24 hours after patient admission.
Reconciliation at 48 hours was considered
more realistic and reflected better the work
and progress made by the hospitals.
ñ The burden of data collection. The workload
associated with the implementation of this SOP
was a challenge and resulted in the application
of the process to a limited number of care units
in six out of the eight participating hospitals.
Implementation surprises or successes
ñ The increased understanding of the importance
of the problem achieved through demonstrating
the magnitude of the discrepancies between
the medications prescribed and those actually
taken and of the potential harm to patients
resulting from those discrepancies.
ñ The development of tools to measure the
potential significance of discrepancies.
ñ The ability of some participating hospitals to
streamline their medication management process
in order to perform on a regular basis a proactive
medication reconciliation in the emergency room.
ñ The development of information technology
tools to follow medication administration
and changes throughout the patient course
within the hospital and at discharge.
ñ The development of a clinical pharmacology
capacity integrated into the care units.
Germany
Summary how LTA evaluated implementation
The below description applies only to the
Correct Site Surgery SOP because no evaluation
of implementation experiences has yet been
conducted for the Med Rec SOP.
The evaluation component of interviews and
implementation questionnaires was conducted
as a part of a diploma thesis.
In addition to the High 5 Project requirements,
the German LTA analysed additional matters of
interest. This was because the implementation
questionnaire was felt to be rather general in scope.
Thus, the German LTA included SOP-specific
questions in the questionnaire which focused on
challenges encountered when implementing
the specific SOP process steps. The expanded
questionnaire was administered from December
2011 to February 2012 by the project coordinators
61 Qualitative and quantitative interim findings
Box 9: Examples of actions taken by LTAs based on data
1) Training of nurses to use the checklist correctly (one hospital).
2) Development of a national surgical site-marking guide in collaboration with the HCOs
and The Joint Commission (Annex 12-France).
3) Fostering leadership of directors: conference calls or meetings with leader of HCOs having
difficulties in the implementation process. A quarterly newsletter which includes results and
benchmarking data is being developed by the LTA.

in all 16 project hospitals; responses were received
from 11 hospitals.
Semi-structured interviews were conducted in
March 2012 with the project coordinators in three
hospitals to gain more detailed information about
barriers, drivers and the resources required for
implementation, as well as the potential for future
sustainability. The interview findings were analysed
using a systematic qualitative evaluation method
(method of Meuser & Nagel).
Challenges encountered
The main challenges for the hospitals’ implementation
processes were resistance to change, oncompliance
of staff/management, and a lack of resources
(funding/time). Hospitals described how individual
“sceptics” could torpedo progress in implementation
and that these sceptics needed to be addressed
individually.
In relation to the SOP process steps, the German
LTA identified the following main barriers:
resistance to change; frontline staff not sufficiently
acquainted with written standards on verification
process; difficulties in adapting to new process;
conflict about the preferred site mark; and team
Time Out not taken seriously and not exemplified
by role models.
Summary of findings
Key strategies for overcoming the challenges
encountered in the implementation process
were improved communication, involving staff/
management, and training/education on the SOP.
Essential strategies for overcoming barriers
related to the SOP process steps were the provision
of written instructions on the SOP, individual
‘pep talks’, retraining and further education, and
adjustment of the checklist.
Important drivers in implementing the CSS SOP
were the similar process design in different
departments; employees having previous experience
with standardization; interdisciplinary and cross-
hierarchical composition of the implementation
oversight group; regular meetings of the project
work group; and the fact that clinical leaders
used the checklist, thereby providing a role model
function.
Important factors identified in the interviews
included:
ñ intense support is necessary especially for the
implementation start and training phases;
ñ pilot site testing paves the way and unlocks
drivers for implementation; and
ñ substantial time and effort are needed for data
management because there is variable checklist
documentation quality.
There is no information available as to how the
hospitals used the data from the implementation
questionnaires.
On the LTA side, at the end of the project,
recommendations will be derived from these
results and published in order to produce guidance
for other health care organisations planning
on implementing similar processes.
Lessons learned
Some important lessons learned relating to
the implementation process:
ñ feedback of some hospitals: “It’s not just
a checklist, it has helped us to fundamentally
change the way we look at our process”. Thus
the systematic implementation of the SOP
radiates to other not yet standardised processes;
ñ the local tailoring of the instruments (i.e.,
the checklists) was relevant to the acceptance
by the participating hospitals;
ñ departments (and hospitals) ‘infect’ one another
with enthusiasm in relation to the SOP; and
ñ acceptance for the new process and completing
the checklists is generally higher in nursing staff
than among physicians.
For more information see Annex 15.
62The High 5s Project Interim Report

The Netherlands
Implementation surprises and lessons learned
The implementation questionnaires from 2010
to 2012 showed no differences in six hospitals
after successful implementation. One hospital
wrote that the SOP is continuously under review
and minor changes have been made. With no
changes in the SOP implementation status in 2012,
the SOP was implemented in two additional
departments. The increase in the number of patients
being verified within 24 hours was because extra
staff had been assigned to support medication
reconciliation.
In one hospital, a hospital-wide medication
multidisciplinary medication committee was
established at the end of 2012, and all
communication about Med Rec was processed
through this committee. Another hospital noted
that staff members did not always want to sign
for the medication reconciliation done by
the pharmacy. New doctors are now being trained
on the SOP implementation process and in using
the electronic prescribing system in this hospital.
Another hospital plans to expand the SOP
implementation to patients at discharge (i.e.
beyond the targeted High 5 population) in 2013,
provide feedback of data to the units, provide
a further educational programme, and continue
with the qualitative measurements according
to the High 5s SOP.
Box 11 presents some important lessons learned.
63 Qualitative and quantitative interim findings
Box 10: Two quotes about the High 5s Project
ñ ‘Yes, it is proven that it works. It was a positive experience, because of the interaction with other
participating hospitals and it really worked to go on with implementation activities and measurements.’
ñ ‘For our hospital it was clear that it would be easier to implement medication reconciliation when
being part of an international project, because of the status.’
Fifteen Dutch Med Rec hospitals are participating.
The first-group of 11 hospitals completed the
qualitative structured and web-based
implementation questionnaires starting six months
after SOP implementation in the summer of 2010
to March 2011. In measuring the follow-up to
these questionnaires, most hospitals showed no
significant changes, except for a few hospitals
which restarted performance measurement
or other activities when expanding the SOP
implementation hospital-wide. Hospitals where
the implementation progress was strong,
continued to spread their activities successfully
and experienced a sustained implementation of
the SOP to become part of daily practice.
Challenges encountered
All hospitals intend to expand the implementation
of the SOP to internal transfers and discharges,
and patients younger than 65. Full implementation
of the SOP has varied according to hospital size.
‘The best implementation and sustainability
strategy for our hospital is ‘to make it not
a hospital pharmacy thing.’
Dutch hospital leader
All hospitals assembled oversight groups and
created a work plan that was evaluated by the LTA.
The main challenges and barriers to spreading
results hospital-wide included limited resources
(funding and time); insufficient communication;
lack of access to medical records or incident
management systems; lack of leadership/staff
buy-in; and resistance to change. The principal
leader of the implementation process in all
participating hospitals was a hospital pharmacist.
Most hospitals chose to start the implementation
on a small scale first before spreading the SOP
hospital wide.

The six Dutch hospitals interviewed highly
recommend the Med Rec SOP developed by
the High 5s Project. Some of their quotes include:
ñ implementation for other hospitals is not
only recommended; it should be considered
a necessity;
ñ we surely recommend implementation of this
SOP to other hospitals. You can try to do this
on your own, but you might encounter pitfalls;
ñ the exchange of knowledge and experience is very
helpful; however, you still have to translate the
SOP to your own local setting;
ñ most of the hospitals advice was to let the
pharmacy technician interview patients: ‘…..it is
proven that interviews done by pharmacy
technicians are of better quality than when done
by doctors’;
ñ the hospitals have no doubt about continuing
to pursue the Med Rec SOP implementation
hospital-wide. One of the hospital staff said:
‘Oh yes! We want the SOP for all patients and
all departments for emergency patients, elective
admissions and discharged patients’;
ñ the strategy of one hospital has been never
to worry too much about resources and budgets.
As shared by one of its staff, ‘You always need
to be proactive. Just start and do instead
of believing something is impossible’;
ñ the key lessons learned from one hospital is
that it was important to keep most of the SOP
implementation in-house so there is no need
to depend on others or other systems nor to
compete with projects of other departments;
ñ another hospital mentioned that quality
improvement is not about implementing the SOP
only. Showing the benefits to all stakeholders
is needed to create support from others.
Generating awareness and communication are
the most important aspects of success, as many
people are involved in the SOP implementation.
Trinidad and Tobago
LTA role in implementation
The Correct Site Surgery SOP was selected for
implementation as a means of standardizing
patient safety solutions within surgical units
in selected hospitals. There were no formal
expectations for correct site surgery procedures
before introduction of the High 5s Project.
The LTA facilitated the piloting of this SOP
at four of the participating hospitals during the
latter half of 2012. The orthopaedic department
was the chosen area for the pilot of the SOP.
There was a total of 27 849 surgical cases
performed at all five participating hospitals
in-patient surgical facilities in the year 2011.
Of this number, there was an estimated one
to two wrong site surgeries. Reporting of wrong
site surgery is specified in the guidelines set out in
the Ministry of Health’s Adverse Events Policy.
This Policy was developed in collaboration with
the Pan American Health Organization (PAHO)
and issued by the Ministry of Health to both public
and private health-care facilities in December 2011.
Additionally, the WHO Surgical Safety Checklist
was adopted and implemented at all public
hospitals in 2010.
At each participating hospital, the project team
leader completed the ‘Hospital Implementation
Experience Questionnaire’ in collaboration
with team members. The completed questionnaires
were then forwarded to the Directorate Health
Services Quality Management, Ministry of Health.
Additionally, the team leader or representative
reported on the status of implementation at
the monthly High 5s team meeting. Meeting venues
were rotated among the participating hospitals.
64The High 5s Project Interim Report
Box 11: Lessons learned
ñ Integrate the SOP into routine care processes.
ñ Inform all involved about the process and
progress of implementation through regular
project meetings.
ñ Be enthusiastic.
ñ Be sensitive to the workload of the staff.
ñ Accept imperfection at the beginning
and work towards perfecting the operational
process. This is extremely important
to maintain buy-in and dedication.
ñ Be aware that the SOP requires input from
various sources to become practical. Work
toward integrating these sources.
ñ Implement step-by-step by creating internal
success stories to spread the SOP hospital-
wide and Keep It Stupidly Simple (KISS).
ñ Involve people: show results and apply.
www.high5s.org/Netherlands/2013.02.01

Challenges encountered
Major challenges common to all participating
hospitals included the frequent turnover of team
members, resistance to change by surgeons and
nurses, lack of staff buy-in, and real or perceived
implementation/data collection burden.
The support of the ‘Quality Improvement Unit’
staff at each hospital and regional health authority
proved to be instrumental in partially addressing
some of these challenges.
The United States of America
Challenges encountered
Even with automated data collection, a large
commitment of time by participating hospital
staff was needed to collect the data. The U.S.A.
LTA found there was initial interest in the SOP;
however, this was not enough once the burden
on resource commitments became apparent.
Another complicating factor was confusion
of purpose. Within the U.S.A., quality
improvement efforts were already underway
to work on this problem. The Joint Commission’s
Center for Transforming Healthcare ran one
in Rhode Island and produced materials and
tool kits to combat the problem of wrong site
surgery.
For the second round of recruitment of hospitals,
the LTA tried to alleviate some of these issues.
A modest hospital stipend is now being provided.
In addition, the LTA is emphasizing the international
aspects of the programme, as well as use the first
hospital as a “mentor” hospital for the new
hospitals interested in joining the Project.
4.3. Summary of event analysis findings
Overall interim findings
Five of the seven participating LTAs self-report
that some in-country hospitals are completing
event analyses. A number of participating hospitals
and LTAs have used de-identified analysis reports
and findings as the basis for case studies for
teaching purposes.
A total of nine EA reports were submitted
by LTAs to the Collaborating Centre in 2012
that related to 125 patients. Reports for three
Concise and one Cluster analyses related to the
Medication Reconciliation SOP (two of the patients
reportedly experienced temporary harm and the
other nine did not experience harm). Reports for
one Concise and four Cluster analyses related to
the Correct Site Surgery SOP (none of the 114
patients experienced harm).
Contributing factors identified by the hospitals
included the following:
a. lack of effective oral/written communication,
including inaccurate or incomplete
documentation;
b. lack of effective teamwork;
c. individual provider/patient factors;
d. insufficient education and training;
e. lack of clarity related to policies and procedures.
It is anticipated that the number of event analysis
reports submitted to the Collaborating Centre
for analysis and reporting will increase during
the last phase of the Project.
a) Medication Reconciliation
A high level summary of the four event analysis
(EA) reports (total of 11 patients involved)
received between January 1st to December 31st,
2012 is included in Graphic A. See Annex 5B
for a complete summary of the EA submissions.
65 Qualitative and quantitative interim findings

b) Correct Site Surgery
A high level summary of the five EA reports (total of 114 patients involved) received between January 1st and
December 31st, 2012 is included in Graphic B. See Annex 5A for a complete summary of the EA submissions.
66The High 5s Project Interim Report
Graphic A: Summary of Medication Reconciliation EA Reports Submitted to the CC in 2012
Graphic B: Summary of Correct Site Surgery EA Reports Submitted to the CC in 2012

a) Analysis
A small number of hospitals are reporting EA data
for both Medication Reconciliation (n = 3) and
Correct Site Surgery (n= 5) SOPs. Possible reasons
include limited capability and/or capacity for
identifying and analysing SOP-related events at
participating hospitals. The data collection burden
has been repeatedly identified as a challenge across
all participating Member States, so it is likely
that limited resources are being focused on
implementation rather than evaluation.
Nonetheless, it is clear from this limited number
of patients (n = 125) that process issues with SOP
implementation have occurred in all reporting
hospitals, with two patients experiencing temporary
harm (Medication Reconciliation SOP). Only one
hospital recommended making changes to the
applicable SOP (Correct Site Surgery) to ensure
the proper conduct of the Time Out, data
collection and data documentation. All hospitals
described local strategies to improve the
implementation of the SOPs through targeted
communication, policies and procedures, education,
and teamwork, among other factors.
EA data remains a potentially rich source
of information on the specific local challenges
involved in implementing a clinical SOP.
4.4. Summary of quantitative findings
Correct Site Surgery
Table 7 and Figure 1 present quantitative interim
data of CSS implementation. The line graphs
include two displays of High 5s Project data,
one by time period (i.e., monthly data points)
and the other by cohort (i.e., data points aligned
based upon the first instance of data submission
for each organization).
The line graphs with monthly data points in the
y-axis summarize hospital data submitted for each
individual month, independent of when the hospital
started the project. The country-level and
international comparison lines are calculated
as follows:
a) Country-level data (national comparison
groups)
Country-level data points for an individual measure
are calculated by aggregating all the hospital
numerator cases (from within a specific country)
and dividing this value by the sum of all of
the hospital denominator cases (from within
the country). The measure is calculated in the
aggregate for all hospitals in the country during
the specific time period. This calculation creates
a weighted mean (weighted by the number of cases
contributed by each hospital) rather than a grand
mean (simply taking the average of the calculated
hospital rates).
b) International-level data (international
comparison groups)
International-level data points are calculated
using a similar approach to the one employed
to calculate a country’s performance on a specific
measure. The major difference is that for rate
and ratio measures, all the hospital numerator
cases (from all countries) are summed and all of
the hospital denominator cases (from all countries)
are summed before calculating the measure rate
or ratio. The measure is then calculated in the
aggregate for all hospitals in contributing data
during the specific time period. This calculation
creates a weighted mean (weighted by the number
of cases contributed by each hospital) rather than
a grand mean (simply taking the average of
the calculated hospital rates or the average
of the national rates).
c) Confidence Intervals
The shaded areas around each line on the graph
represent a 95% confidence interval. The 95%
confidence interval indicates the estimated
probability (95%) that the population parameter
lies within the reported range of values (i.e.,
the degree of certainty that the true value lies
within a range of values). The confidence intervals
are calculated using a slightly different formula
for rate-based proportion measures and ratio
measures. The formula for each calculation is
provided below (p = the rate, r = the ratio, n =
the number of cases, SE = Standard Error).
67 Qualitative and quantitative interim findings
The cohort graphs use the same formula to
calculate measure rates/ratios, but they aggregate
data based upon each hospital’s first data point
(rather than the month) as its first measureable
experience with SOP implementation. Every
subsequent monthly data point is aligned
accordingly. For example, if Hospital A submitted
its first data point in January of 2011, and Hospital

B submitted its first data point in July of 2012,
both points would aligned as the initial data
points for the hospitals.
Each subsequent monthly point was then aligned
based upon the time from initial SOP
implementation. This approach was used to track
time since implementation and account for gaps
in data collection. Continuing the example above,
if Hospital A submitted data for February,
March and June of 2011, the data points would be
assigned as month 2, month 3, and month 6
(as opposed to point 2, point 3 and point 4).
In this manner, the gap associated with the missing
data points (i.e., April and May) is addressed.
In order to aggregate hospital data within each
country (and across the project), each data point
was aggregated using the same approach,
beginning with the initial data point for each
hospital and calculating subsequent data points
(while correcting for gaps in data collection).
Note: For both graphs, it is important to consider
that the number of contributing hospitals could
change from month to month, based upon
the actual contributions of each hospital. The most
current three months represented in each graph
tend to contain fewer hospital contributions,
as many hospitals have a considerable lag time
in their data collection efforts. As a result,
the confidence intervals for later months tend
to be wider, and the rates more variable.
68The High 5s Project Interim Report
Table 7: General quantitative data on CSS
Member State Total No. Total No. of hospital submitted
hospitals data to High 5s IMS
implementing Average number of hospitals per month
SOP1,2 (07/2010-04/2013)
MUN8NS1Z 8 4
KEC43YH1 7 6
FDQ17XVY 1 1
RJ94137U 16 12
International Comparison 32 23
1 Implementing = Eligible to enter data in the High 5s Information Management System
2 Only data that has been approved by both the hospital and the LTA meets the criteria to be included in performance
measure calculations.
Figure 1: Interim quantitative data on CSS implementation
H5sCS-0 - Proportion of verification checklists for all eligible surgical cases
Pro
po
rtio
n o
f el
igib
le s
urg
ical
case
s
(All
case
s sc
hed
ule
d t
o b
e per
form
ed)
H5sCS-0 – By cohort
Time period
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%

69 Qualitative and quantitative interim findings
H5sCS-1 – Proportion of eligible surgical cases with a complete preoperative verification process
(exclusive of site marking and Time Out)
H5sCS-1 – By cohort
Time period
Time period
All Member States RJ94137U KEC43YH1 MUN8NS1Z
Pro
po
rtio
n o
f el
igib
le s
urg
ical
case
s
(All
case
s sc
hed
ule
d t
o b
e per
form
ed)
Pro
po
rtio
n o
f el
igib
le s
urg
ical
case
s
(All
case
s sc
hed
ule
d t
o b
e per
form
ed)
Jul 10 Oct 10 Ian 11 Apr 11 Jul 11 Oct 11 Jan 12 Apr 12 Jul 12 Oct 12 Jan 13 Apr 13
1
0.8
0.6
0.4
0.2
0
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%

70The High 5s Project Interim Report
H5sCS-2 – Proportion of cases with properly marked surgical site
Time period
Pro
po
rtio
n o
f el
igib
le s
urg
ical
case
s
(eli
gib
le f
or
site
mark
ing
)Pr
opo
rtio
n o
f el
igib
le s
urg
ical
case
s
(eli
gib
le f
or
site
mark
ing
)
H5sCS-2 – By cohort
Time period
All Member States RJ94137U KEC43YH1 MUN8NS1Z
Jul 10 Oct 10 Ian 11 Apr 11 Jul 11 Oct 11 Jan 12 Apr 12 Jul 12 Oct 12 Jan 13 Apr 13
1
0.8
0.6
0.4
0.2
0
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%

71 Qualitative and quantitative interim findings
H5sCS-3 – Proportion of cases with complete final ‘Time Out’
H5sCS-3 – By Cohort
Time period
Pro
po
rtio
n o
f el
igib
le s
urg
ical
case
s
(eli
gib
le f
or
a T
ime
Out)
Pro
po
rtio
n o
f el
igib
le s
urg
ical
case
s
(eli
gib
le f
or
a T
ime
Out)
Time period
All Member States RJ94137U KEC43YH1 MUN8NS1Z
Jul 10 Oct 10 Ian 11 Apr 11 Jul 11 Oct 11 Jan 12 Apr 12 Jul 12 Oct 12 Jan 13 Apr 13
1
0.8
0.6
0.4
0.2
0
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%

72The High 5s Project Interim Report
H5sCS-4 – Proportion of cases with discrepancy noted at final Time Out
Pro
po
rtio
n o
f el
igib
le s
urg
ical
case
s
(eli
gib
le f
or
a T
ime
Out)
Pro
po
rtio
n o
f el
igib
le s
urg
ical
case
s
(eli
gib
le f
or
a T
ime
Out)
Time period
All Member States RJ94137U KEC43YH1 MUN8NS1Z
Jul 10 Oct 10 Ian 11 Apr 11 Jul 11 Oct 11 Jan 12 Apr 12 Jul 12 Oct 12 Jan 13 Apr 13
1
0.8
0.6
0.4
0.2
0
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
H5sCS-4 – By cohort
Time period

73 Qualitative and quantitative interim findings
H5sCS-5 – Proportion of cases undergoing surgery with unresolved ‘Time Out’ discrepancies
Pro
po
rtio
n o
f el
igib
le s
urg
ical
case
s
(Wit
h D
iscr
epancy
at
Final
Tim
e O
ut)
Pro
po
rtio
n o
f el
igib
le s
urg
ical
case
s
(Wit
h D
iscr
epancy
at
Final
Tim
e O
ut)
Time period
All Member States RJ94137U KEC43YH1 MUN8NS1Z
Jul 10 Oct 10 Ian 11 Apr 11 Jul 11 Oct 11 Jan 12 Apr 12 Jul 12 Oct 12 Jan 13 Apr 13
1
0.8
0.6
0.4
0.2
0
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
H5sCS-5 – By cohort
Time period

74The High 5s Project Interim Report
H5sCS-6 – The proportion of surgical cases that are cancelled or postponed due
to discrepancies identified at any point in the conduct of the SOP
Pro
po
rtio
n o
f el
igib
le s
urg
ical
case
s
(eli
gib
le f
or
a T
ime
Out)
Time period
All Member States RJ94137U KEC43YH1 MUN8NS1Z
Jul 10 Oct 10 Ian 11 Apr 11 Jul 11 Oct 11 Jan 12 Apr 12 Jul 12 Oct 12 Jan 13 Apr 13
1
0.8
0.6
0.4
0.2
0
Pro
po
rtio
n o
f el
igib
le s
urg
ical
case
s
(All
case
s sc
hed
ule
d t
o b
e per
form
ed)
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
H5sCS-6 – By cohort
Time period

75 Qualitative and quantitative interim findings
H5sCS-7 – Proportion of cases with incorrect surgery (wrong site, procedure or person cases)
Time period
All Member States RJ94137U KEC43YH1 MUN8NS1Z
Jul 10 Oct 10 Ian 11 Apr 11 Jul 11 Oct 11 Jan 12 Apr 12 Jul 12 Oct 12 Jan 13 Apr 13
Pro
po
rtio
n o
f el
igib
le s
urg
ical
case
s
(All
case
s sc
hed
ule
d t
o b
e per
form
ed)
1
0.8
0.6
0.4
0.2
0
Pro
po
rtio
n o
f el
igib
le s
urg
ical
case
s
(All
case
s sc
hed
ule
d t
o b
e per
form
ed)
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
H5sCS-7 – By cohort
Time period

Medication Reconciliation
Figure 2 presents quantitative interim data of MR implementation. Please see the graph explanation in
section 5.4.1 under CSS to understand the differences between the line graphs and cohort displays.
Table 8: General quantitative data on Medication Reconciliation
Member State Total No. Total No. of hospital submitted
hospitals data to High 5s IMS
implementing Average number of hospitals per month
SOP1 (07/2010-04/2012)2
DVLR6PNK 14 6
OFI427W6 15 5
2K01AJF0 9 6
VES234TZ 7 0
BH4537QS 2 0
International Comparison 47 17
1 Implementing = Eligible to enter data in the High 5s Information Management System. One Member State has
recently started to implement the Med Rec SOP but is not yet depicted in this count.
2 Only data that has been approved by both the hospital and the LTA meets the criteria to be included in performance
measure calculations.
Figure 2: Interim quantitative data on Med Rec implementation
76The High 5s Project Interim Report
H5sMR-1 – Percent of patients with medications reconciled within 24 hours
of the decision to admit the patient
Perc
ent
of
Pati
ents
Time period
All Member States 2K01AJF0 OFI427W6 DVLR6PNK
Jul 10 Oct 10 Ian 11 Apr 11 Jul 11 Oct 11 Jan 12 Apr 12 Jul 12 Oct 12 Jan 13 Apr 13
100%
80%
60%
40%
20%
0%

77 Qualitative and quantitative interim findings
H5sMR-2 – The mean number of outstanding undocumented intentional medication discrepancies per patient
H5sMR-1 – By cohort
Perc
ent
of
Pati
ents
Num
ber
of
Dis
crep
anci
es p
er P
ati
ent
Time period
Jul 10 Oct 10 Ian 11 Apr 11 Jul 11 Oct 11 Jan 12 Apr 12 Jul 12 Oct 12 Jan 13 Apr 13
3.5
3
2.5
2
1.5
1
0.5
0
120%
100%
80%
60%
40%
20%
0%
Time period
All Member States 2K01AJF0 OFI427W6 DVLR6PNK

78The High 5s Project Interim Report
H5sMR-2 – By cohort
H5sMR-3 – The mean number of outstanding unintentional medication discrepancies per patient
Num
ber
of
Dis
crep
anci
es p
er P
ati
ent
Num
ber
of
Dis
crep
anci
es p
er P
ati
ent
Time period
2
1.8
1.6
1.4
1.2
1
0.8
0.6
0.4
0.2
0
Time period
All Member States 2K01AJF0 OFI427W6 DVLR6PNK
Jul 10 Oct 10 Ian 11 Apr 11 Jul 11 Oct 11 Jan 12 Apr 12 Jul 12 Oct 12 Jan 13 Apr 13
2
1.5
1
0.5
0

79 Qualitative and quantitative interim findings
H5sMR-3 – By cohort
H5sMR-4 – Percent of patients with at least one outstanding unintentional discrepancy
Num
ber
of
Dis
crep
anci
es p
er P
ati
ent
Perc
ent
of
Pati
ents
Time period
Time period
All Member States 2K01AJF0 OFI427W6 DVLR6PNK
Jul 10 Oct 10 Ian 11 Apr 11 Jul 11 Oct 11 Jan 12 Apr 12 Jul 12 Oct 12 Jan 13 Apr 13
80
60
40
20

4.5. Member State quantitative and event
analysis findings
Australia
Following the evaluation plan has been a challenge
for all hospitals because of the burden of data
collection for the performance measures, data
quality requirements, and requirements for the
event analysis. Ongoing collection of performance
measure data (MR 2-4) is seen as not sustainable
by some sites. The value of continuing to monitor
measures MR 2-4 once the process was stable and
the target had been reached was also questioned.
One site withdrew from the project in late 2012,
citing the need to prioritize their work because
of resource constraints and preferring to provide
direct patient care over data collection.
Performance measures
Performance measure data has been collected since
mid-2010. As of November 2012, nine Australian
hospitals were submitting data into the High 5s
IMS. In addition, two hospitals in the group
are conducting medication reconciliation but
are not collecting data because of resource
constraints. One health service with multiple
hospitals has stopped collecting performance
measure data for MR 2-4 because of lack of staff
to conduct the independent observer role and meet
data quality requirements.
Data submission into the High 5s IMS has been
staggered, with hospitals starting data collection
at different time points. A number of hospitals are
now collecting MR 2-4 data on a quarterly basis,
with three sites now moving to 6-monthly data
collection. Rates can vary substantially when
the comparative data is produced because of
the number of hospitals contributing data in
a particular month. Sample sizes across the period
from August 2010 to November 2012 ranged
from 2 to 10 hospitals. See figures in Annex 10.
Rates for measure MR-1 vary across hospitals
depending on the stage of implementation,
resources available, and the spread of the
intervention in the organization. Between August
2010 and November 2012, rates for the percentage
of eligible patients with medications reconciled
within 24 hours of admission ranged from 16%
to 96% across participating hospitals, with an
average of around 51%. The trend line for MR-1
has been stable over this period. As medication
reconciliation remains largely pharmacist-driven,
there is a close association between MR-1 rates and
available clinical pharmacist resources. Hospitals
report that without additional clinical pharmacist
resources, MR-1 rates are not likely to improve.
Rates for MR-2 are generally stable and low
(less than 0.3) with a trend towards zero over time
for the majority of hospitals. Australian hospitals
80The High 5s Project Interim Report
H5sMR-4 – By cohort
Perc
ent
of
Pati
ents
100%
90%
80%
70%
60%
50%
40%
30%
20%
0%
Time period

report they have used this measure to provide
feedback to medication prescribers around the
importance of clearly documenting intended
medication changes. Similarly, rates for MR-3
are generally less than the SOP absolute target
of 0.3 outstanding unintentional discrepancies
per patient with a trend towards zero over time
for several hospitals. The percentage of patients
with at least one outstanding discrepancy (MR-4),
also continues to decrease with time; however,
there is variation in MR-4 rates across hospitals
which is highlighted in the figures in Annex 10.
Event analysis
The collection of performance measure data has
overshadowed the event analysis (EA) component
of the evaluation with few sites reporting EAs.
Twelve event analysis reports have been received
from four hospitals, including 11 individual reports
and one cluster analysis. All individual reports were
concise analyses, with an assigned level of harm
ranging from temporary harm to no harm. There
have been no serious harm events reported.
In a sub-analysis of seven events, the most
common contributing factors were identified
as teamwork, education and training, and
communication. There were no requests for changes
to the SOP.
All events were the result of a failure to follow
the SOP medication reconciliation process. Most
events occurred during the BPMH stage (five) and
when reconciling the medicines (four); only one
report related to the resolution of a discrepancy.
Individual hospitals have used the event analysis
reports as the basis for case studies for teaching
purposes. Actions resulting from the reports have
resulted in changes to the medication reconciliation
form (one hospital), and regular orientation
sessions for junior medical staff on the medication
reconciliation form and process. Learning from
the events has been shared among the hospitals
participating in the High 5s Project.
81 Qualitative and quantitative interim findings
Other
Two additional performance measures were
developed to allow hospitals to collect data on
the discrepancies identified by the independent
observer that remained unresolved 48 hours after
admission. By late 2012, five hospitals were
collecting data on the number of these outstanding
unresolved discrepancies. In addition, three of these
hospitals measured the potential for harm from
the discrepancies using the National Coordinating
Council for Medication Error Reporting and
Prevention (NCC MERP) severity scale to classify
potential level of harm. The most common
discrepancies were classified as NCC MERP
Category D - an error occurred that reached
the patient and required monitoring to confirm
that it resulted in no harm to the patient and/or
required intervention to preclude harm. This data,
along with examples of actual discrepancies,
has been used by sites to provide feedback
to prescribers and encourage early resolution
of discrepancies. (See Figure 3.)
Box 12: Learning from error
Hospital 5: An event analysis was conducted on a patient prescribed the incorrect medicines on
admission to hospital. These medications were administered to the patient for a week until a pharmacist
completed a BPMH for the patient and the errors were noted. All of the health-care professionals
involved were informed of the errors, and this has been used as a teaching example to prevent this from
happening again. This case was also presented at facility quality and safety meetings.

France
Measures for Correct Site Surgery
Regarding the first months of evaluation, and
based on the CSS performance measures, it appears
that nearly all the hospitals made progress. The
most striking improvement involves site-marking.
Number of CL initiated / eligible cases
During 2012, the measure CS-0 national average
is 84% (Min = 55%, Max = 100%). Two hospitals
with low CS-0 rates are facing persisting difficulties
in making progress.
Pre-op verification CS-1
Significant variability has been observed among
the different health-care organizations (HCOs)
because of the reluctance of some professionals
(i.e., surgeons, anesthetists) to conform to
the process requirements. However, HCOs with
an electronic checklist integrated in the data
records have achieved good results, as traceability
is less time-consuming and the acceptability of
this preoperative component is better. In 2012,
the French national average for measure CS-1
was 29% (Min = 2%, Max = 69%).
Site-marking
All of the hospitals except one improved their
site-marking results. The mean value for measure
CS-2 was 62% in 2012 (Min=26%, Max=87%).
The hospital which did not show improvements
demonstrated poor Project leadership for the,
inappropriate site markings, such as marking
the site with a cross on the palm of the hand,
only partial implementation, and poor feedback
to frontline staff.
Time Outs
The mean value for measure CS-3 was 66%
(Min=32%, Max=89%). Discrepancies in the OR
were mainly because of a lack of traceability.
In addition evaluation of the Time Out by
observational audits started in June 2012.
Up to the present, the LTA has conducted four
observational audits in the operating rooms
of hospitals (audit grid designed by CEPPRAL).
Event analysis
Since the end of 2011, six hospitals have provided
analysis forms to the LTA. Only two were correctly
analyzed and therefore eligible for posting on the
High 5s Project website. Event analysis was difficult
because it was time consuming and there were
insufficient resources to support this activity.
82The High 5s Project Interim Report
Figure 3:
Mean number of unresolved medication discrepancies/patient > 48 hours after admission

Interviews with participating hospitals
Since January 2012, nine annual visits which
include interviews (individual and focus group)
have been performed by HAS and CEPPRAL.
About 45 interviews have been conducted thus
far and have involved 90 professionals (front-line
staff and managers, physicians, surgeons, war
nurses, secretaries, and anaesthetists). These
interviews have been invaluable in communicating
with the teams and HCOs as well as recognizing
the efforts they have achieved.
Measures for Medication Reconciliation
During the first months of evaluation of
medication reconciliation practice in France using
the High 5s performance measures, it appears
that all of the hospitals progressed as much
in the number of reconciled patients as in the
identification of discrepancies.
In France, the principal data used by the LTA was
measure MR-1 because it highlights the level of
medication reconciliation implementation for each
hospital. Indeed, from the beginning of the Project,
the other measure results were very low, especially
because the number of eligible patients reconciled
was not a priority. It was felt to be more relevant
to focus on measure MR-1 and on the number
of unintentional intercepted discrepancies as it
provides telling information for health-care
professionals, the CEOs and the nation as a whole.
For example, the medication reconciliation pilot
hospital in France has, over a period of 18 months,
succeeded in intercepting 1.664 unintentional
discrepancies thanks to the medication reconciliation
process. This result has a lot of teaching impact
and allows the promotion of this practice with
other professionals.
In France, the number of reconciled patients
initially varied from one hospital to another, as
shown by MR-1 rates which ranged between 2.5%
and 63.4%. This heterogeneity is explained by
the fact that two of the hospitals had a very low
number of eligible patients because of the hospital
size. However, over the first 13 months of
implementation, the number of patients who had
received formal medication reconciliation increased
for all of the hospitals. From August 2011 to May
2012, the aggregated MR-1 results increased
from 19.6% to 30.2%. In parallel, the number
of discrepancies decreased from 321 to 159
over the same period, which evidences better
understanding of the protocol by the teams as
well as an improvement in their daily practices.
Since the Med Rec teams do not encounter many
unintentional discrepancies, it is difficult to involve
them in event analysis. The Med Rec teams have
been more interested in focusing on the analysis
of the intercepted discrepancies and sharing
the experience gathered by stopping them.
Germany
Measures for Correct Site Surgery
German hospitals collect data for the performance
measures on carbon copies of the surgical checklist
and send one copy to the LTA. To date, over
115.000 checklists from 16 hospitals have been
scanned and imported into the national database.
In addition to the High 5s measures data,
key national data can also be analyzed (e.g.
documentation quality, completeness of checklists,
subgroup analysis of emergency cases) because
of the availability of the complete checklist data.
The German LTA has established a national feedback
system consisting of individual hospital quarterly
reports and bi-annual national benchmark reports
which is much appreciated by the participants.
The German LTA conducted an analysis of the High
5s measures results for those checklists which
were evaluated in the year 2012 (n=61.684).
Four hospitals consistently performed at a high
level for the measures CS-0 through CS-3. Two
of these four hospitals were also part of the top
25% for measure CS-4. These hospitals, however,
ranged completely differently for measures CS-5
and CS-6. The German LTA identified two hospitals
which continuously ranked in the lower 25% for
all of the first four performance measures. These
hospitals also ranked in the lower 33% for measure
CS-5. Both had presented a very low rate of case
cancellations because of discrepancies (for CS-6,
0.00% and 0.01%). Two years after starting SOP
CSS implementation, hospitals have reached
consistent levels of performance on the measures.
From review of checklists, it is evident that with
regard to the first four measures, Project hospitals
are divided into groups of high and low performers.
For the measures dealing with discrepancies (CS-4
through CS-6), high and low performers cannot
clearly be identified.
Measures for Medication Reconciliation
To date, the hospital which has officially started
with the Med Rec SOP has calculated its
performance measures for the months of March
83 Qualitative and quantitative interim findings

through October 2012. In this hospital, since
the beginning of implementation, Med Rec has been
conducted on an average of 36 patients per month.
The number of documentation errors has decreased
slightly. The number of medication errors
(unintentional discrepancies) has been reduced
by 78%. The proportion of patients with
at least one medication error has been reduced
by 69%.
Event analysis
CSS: The German LTA has learned that Event
Analyses have been conducted in some of
the hospitals, but the results have not yet been
shared with the LTA or the CC.
Other
By way of a baseline survey which the German
LTA conducted, it was found that hospitals
which had already established similar processes
experienced a much smoother transition compared
to those hospitals for which the SOP was a new
process. This is also reflected in the process
measure results.
The Netherlands
Process measures
All of the fifteen participating hospitals established
baseline performance levels before implementing
the SOP. Hospitals usually measured their
performance for at least three months after
implementation to show sustainability in the
reduction of medication discrepancies. Hospitals
would gather data for measures MR-1 through
MR-4 until achieving at least a 75% reduction of
discrepancies. Thereafter, most of the hospitals
only measured MR-1 monthly and measures MR-2
through MR-4 occasionally (e.g., every six months).
Two hospitals targeted almost 100% of their
patients for measure MR-1. Hospitals generally felt
no need to measure monthly only for the specific
High 5s target population (patients 65 years
and older admitted through ER) after the SOP
performance had demonstrated sustainability.
One hospital pharmacist said that, ‘As a hospital
pharmacy, we do see every adolescent clinical
patient within 24 hours. Probably now and then
a patient will slip through the process, but
we achieve 96-100% monthly. There’s no need
to keep on measuring MR-1 monthly, as the
outcome will remain the same.’
Hospitals spread the SOP implementation to all
age groups as this made implementation in daily
practice easier. Some hospitals started
implementation step-by-step, with a few categories
of patients first. For each hospital, the impact
of the SOP was all about the qualitative context
of SOP implementation underlying the quantitative
measures. An academic hospital highlighted that,
‘When we have no performance measurements
in our hospital it does not mean that our
reconciliation process is not of good quality.
Measurements to monitor the process are also
for the national patient safety programme. During
the upcoming months, we will have internal
sessions to provide feedback about how to create
an effective dashboard to monitor reconciliation
and to sustain the reconciliation process.’
Highlights of event analysis
The Dutch hospitals contributed to the development
of the event analysis methodology and
materials. Some hospitals piloted the draft event
analysis process in the spring of 2011, which
showed that the triggers identified in the medical
records did not appear frequently enough to be
used to support the event analysis process.
In 2011, the event analysis methodology was
modified and the new triggers and forms became
available in 2012. One hospital in the Netherlands
finished an event analysis and identified events
potentially related to the SOP. All required forms
were analyzed and reported to the LTA. This
hospital experienced resource-based challenges/
barriers, including the lack of staff to identify
events for analysis, difficulty defining an
independent observer role, and lack of staff and/or
staff time to perform event analysis after event
was identified. Action plans for improvement were
formulated after completing the event analysis,
and the hospital learned important information
about the SOP implementation processes on local
wards through carrying out the event analysis.
A second hospital completed an event analysis
at the end of 2012 and also identified events
potentially related to the SOP.
84The High 5s Project Interim Report

Singapore
Measurement of improvement
The effects of the planned changes were measured
by gathering compliance data collected according
the following High 5s measures:
ñ CS-1. Completed Preoperative Verification Check
List;
ñ CS-2. Properly Marked Surgical Site;
ñ CS-3. Complete Final ‘Time Out’;
ñ CS-4. Cases with Discrepancy Noted at Final
‘Time Out’;
ñ CS-5. Cases Undergoing Surgery with Unresolved
‘Time Out’ Discrepancies;
ñ CS-6. Case Cancellation Resulting From SOP
Implementation;
ñ CS-7. Incorrect Surgery (wrong site, procedure
or person cases).
The main points to highlight from the Singapore
hospitals’ performance versus other Member States
are that:
ñ Singapore’s national average consistently showed
higher compliance rates than the international
benchmark.
ñ Though hospitals have not all achieved 100%
compliance for measures CS-1 through CS-3, their
current rates have improved to a plateau at >90%.
ñ Measure CS-5 result suggested that Singapore
hospitals tend to let discrepancies pass
unresolved. However, on further investigation
the discrepancies were found to be mostly related
to documentation errors, such as ticking ‘No’
when it should be ‘NA’ and not because of
non-compliance with the SOP. The High 5s
Network is working within its own hospitals
to close the gaps for these discrepancies.
One of the ways they have chosen to do this
is through events analyses which they are just
starting to do now that the data collection
and submission processes have been stabilized.
ñ Measure results for CS-6 and CS-7 have
consistently been 0%.
Trinidad & Tobago
Implementation of the CSS SOP took place at four
participating hospitals. Despite the challenges
experienced, staff in the orthopaedic theatres were
still willing to advance the SOP to other theatres.
Figure 4 presents measure results in participating
hospitals in Trinidad and Tobago.
85 Qualitative and quantitative interim findings
CS-0 Eligible Surgical Cases
YES NO NA
TRHA 105 0 0
SWRHA 100 0 0
NCRHA 100 0 0
ERHA 62 38 0
Figure 4: Measures in participating hospitals
CS-0 Eligible Surgical Cases
TRHA
110
100
90
80
70
60
50
40
30
20
10
0
YES NO NA
Pati
ent
%
SWRHA
NCRHA
ERHA

86The High 5s Project Interim Report
CS-1 Completed Preoperative Verification Checklist
CS-1 Completed Preoperative
Verification Checklist
YES NO NA
TRHA 85 14 1
SWRHA 82 18 0
NCRHA 80 20 0
ERHA 90 10 0
TRHA
100
90
80
70
60
50
40
30
20
10
0
YES NO NA
CS-2 Properly Marked
Surgical Site
YES NO NA
TRHA 23 70 8
SWRHA 66 34 0
NCRHA 60 40 0
ERHA 100 0 0
CS-3 Complete Final Time Out
CS-3
Complete Final Time Out
YES NO NA
TRHA 61 38 1
SWRHA 67 33 0
NCRHA 60 40 0
ERHA 95 5 0
CS-2 Properly Marked Surgical Site
Pati
ent
%
100
90
80
70
60
50
40
30
20
10
0
Pati
ent
%
SWRHA
NCRHA
ERHA
TRHA
100
90
80
70
60
50
40
30
20
10
0
YES NO NA
Pati
ent
%
SWRHA
NCRHA
ERHA
TRHA
SWRHA
NCRHA
ERHA
YES NO NA

87 Qualitative and quantitative interim findings
CS-4 Cases with Discrepancies
noted at final time-out
YES NO NA
TRHA 0 100 0
SWRHA 21 79 0
NCRHA 2 98 0
ERHA 5 95 0
CS-5 Surgery with
Unresolved Discrepancies
YES NO NA
TRHA 0 100 0
SWRHA 5 95 0
NCRHA 0 100 0
ERHA 0 0 0
CS-6 Case cancellation resulting
from SOP Implementation
YES NO NA
TRHA 1 99 0
SWRHA 0 0 0
NCRHA 0 100 0
ERHA 0 0 0
TRHA
100
90
80
70
60
50
40
30
20
10
0
YES NO NA
CS-5 Surgery with Unresolved Discrepancies
Pati
ent
%
SWRHA
NCRHA
ERHA
CS-4 Cases with Discrepancies noted at final time-out
TRHA
100
90
80
70
60
50
40
30
20
10
0
YES NO NA
Pati
ent
%
SWRHA
NCRHA
ERHA
CS-6 Case cancellation resulting
from SOP Implementation
0
0100
90
80
70
60
50
40
30
20
10
0
Pati
ent
%
TRHA
SWRHA
NCRHA
ERHA
YES NO NA

88The High 5s Project Interim Report
CS-7 Incorrect Surgery
YES NO NA
TRHA 0 100 0
SWRHA 0 0 0
NCRHA 0 100 0
ERHA 0 0 0
CS-7 Incorrect Surgery
100
90
80
70
60
50
40
30
20
10
0
Pati
ent
%
TRHA
SWRHA
NCRHA
ERHA
YES NO NA
1 Australian Commission on Safety and Quality in Health Care. National Safety and Quality Health Service Standards.
Sydney: Australian Commission on Safety and Quality in Health Care, 2011.
2 Australian Pharmaceutical Advisory Council. Guiding principles to achieve continuity in medication management.
Canberra: Commonwealth of Australia, 2005.
3 Society of Hospital Pharmacists of Australia. SHPA Standards of practice for the provision of medication
reconciliation. Journal of Pharmacy Practice and Research 2007;37(3):231-3.

6Interimoutcomes

1. Feasibility
Feasibility refers to the degree to which an SOP
could be implemented as it was originally defined,
in a standardized way across hospitals within
a country or in multiple countries.
1.1. Overall issues
One of the primary objectives of the High 5s
Project has been to assess the feasibility of
implementing standardized approaches to specific
patient safety problems across multiple countries
and cultures. The rigorous, multidimensional High
5s evaluation strategy is providing a qualified “yes”
to the first of the key questions for the Project:
is process standardization across different hospitals
in different Member States feasible? Over the
course of the High 5s Project it became clear
that some aspects of the SOPs were more easily
implemented in some participating Member States
than in others. When participants encountered
issues with the implementation of a SOP, they
were invited to submit requests to adapt or modify
components of the SOPs that were problematic
or not working well. These requests were reviewed
by the Collaborating Centre and the High 5s Steering
Group and a decision was made to approve or
reject the modification request. To date, 15 SOP
modification requests have been submitted–two
for Medication Reconciliation, 11 for Correct Site
Surgery, and two for Concentrated Injectables.
Each participating Member State submitted at least
one request for modification. However, while there
have been several country-specific adaptations
to the SOP, the majority of participating hospitals
have achieved full implementation of the protocol.
That is, hospitals implemented all steps of the
protocol in all locations and for the entire eligible
population as specified in the SOP.
In some cases, modification requests led to
revisions of the SOP. These revisions included
changes to key definitions which helped to clarify
the intent of a process or a concept across the
varied languages and cultures of participating
Member States. In other cases, revision requests
identified opportunities for flexibility or local
customization of the SOP. Such requests required
the High 5s Steering Group to reconsider
which elements of the protocol needed to be
“standardized” and which aspects should be left
to the discretion of the hospital. For example, the
Correct Site Surgery protocol originally required
that site marking be performed directly by the
surgeon who was performing the procedure.
The SOP was revised to allow the responsibility
for site-marking to be delegated to another health
care professional, as long as that individual was
qualified, identified in the patient record, and
directly involved in the procedure. In other words,
the SOP continued to require a standardized
site-marking process, but the individual hospitals
could implement it in a way that fit best into
its existing processes.
Modifications to the SOPs are presented in
additional detail below:
Medication Reconciliation
Canada requested that the definition of ‘Best
Possible Medication History’ be revised to include
an expanded definition of ‘medication’ and
to define what is meant by ‘currently taking’
a medication. The requested revisions were
approved based on the assumption that they
provided clarity and a more uniform understanding
of the SOP across participating Member States.
The Netherlands requested to reduce the number
of times the patient/family is consulted to obtain
the patient’s current and past medication history.
The request was that the patient/family be consulted
only one time (instead of two) in order to more
effectively and efficiently utilize staff time.
90The High 5s Project Interim Report
Interim outcomes
The request was approved, and the SOP was revised
to allow for a more generalized model that allows
more freedom and flexibility for hospitals to define
their own process for obtaining the patient’s best
possible medication history. This change helped
to improve understanding of the SOP, reduce
redundancy, and create a more efficient work flow.
Concentrated Injectables (CIs)
The United Kingdom requested a proactive reduction of
authorized ward storage of concentrated injectables.
The requested language change focused on the
reduction of the number of clinical areas authorized
to store CIs and, where authorized, put limitations on
the types, amounts, concentrations and preparations
of CI drugs stored in those areas (outside of the
pharmacy). These language changes were approved,
and the SOP was modified accordingly.
The United Kingdom also requested that information
be added to the SOP that would help clarify the
intended population for the SOP. This request was
approved, and the wording was amended to read,
“This SOP applies to inpatient clinical areas only.”
Correct Site Surgery
Singapore, Germany and France all asked that
the procedure for site-marking be revised to allow
for a delegated health-care professional (other than
the operating surgeon) to mark the correct surgical
site. The request was approved, and the language
in the SOP was changed to reflect that:
1) another physician or registered nurse
participating in the procedure or directly
involved in patient surgical preparation can
mark the site;
2) hospital policy must include the minimum
qualifications and the role of the person
delegated to perform site-marking;
3) the individual performing the site-marking
is identified in the medical record or
pre-operative verification checklist.
Singapore also requested a waiver of the verification
of site and procedure during pre-operative testing
since surgical site and procedure are not usually
verified during this time. This request was approved,
and the pre-operative verification checklist was
revised accordingly.
In a few cases, requests for modifications to
the SOP did not lead to revision of the SOP,
but rather resulted in a country-wide adaptation
of the SOP. These requests generally involved
a conflict between an individual Member State’s
existing standard, and a critical component of
the SOP. In these cases, the Steering Group allowed
an individual Member State to adapt
the SOP to maintain consistency with the existing
standard. There were two such instances, both
involving the CSS SOP and standard practices
in Germany.
In order to avoid the possibility of misinterpretation,
the SOP prohibits the use of abbreviations in
surgical documentation. However, because there
are many established and commonly understood
abbreviations currently used in Germany, as well
as many long words in the German language that
look similar, Germany requested permission to use
abbreviations in the electronic operating room
(OR) log. In participating German hospitals,
these established abbreviations help distinguish
words and also require less space in the OR log.
A decision was made to make a country-specific
adaptation rather than a revision to the SOP that
would allow participating German hospitals to use
abbreviations in electronic (only) OR logs.
The SOP also specifies a number of approaches
to site-marking, including a prohibition on using “X”
to mark a site. In many cases, “X” can be variously
interpreted as a positive (i.e., “‘X’ marks the spot”)
or negative indication (i.e., “Do NOT…”), which
creates the potential for confusion and error.
In Germany, however, the “X” has been
recommended as a standard marking for the
correct/intended site for surgery by the German
Coalition for Patient Safety. This adaption was
approved for participating German hospitals
to use “X” for the intended surgical site marking.
Rejected requests
A number of additional requests were also
considered but rejected by the Steering Group.
These requests all related to the CSS SOP;
two related to site-marking and one related
to patient positioning.
Germany asked to use only the intraoperative
radiographic technique, not skin marking to mark
the surgical site for spinal procedures. Because both
skin marking and intraoperative marking are required
as part of the SOP, this request was rejected.
Singapore asked to exempt obstetric and
gynecological procedures from site marking
91 Interim outcomes

because of the fact that the many ob/gyn
procedures require exploratory surgery to determine
the correct site for the surgery. This request
was rejected based on the fact that the expected
or anticipated surgical site should be marked in
all surgical cases, regardless of specialty area.
Singapore also requested to waive the patient
position verification during the Time Out because
of the fact that the patient would be checked
during prepping and draping and it is unlikely
that the patient position would be inaccurate
by the time the time-out occurs. This request
was rejected because the verification of the
patient position is part of a minimum set of items
selected to be included in the final time-out.
This list was determined by expert consensus
to include the most measures for avoiding
wrong-site surgery.
1.2. Summary of in-country experiences
Australia
By December 2012, all 12 hospitals in the
collaborative had implemented the medication
reconciliation process. Nine of these hospitals
were submitting data into the High 5s IMS.
Only one hospital was able to perform medication
reconciliation on over 80% of its eligible patients
within 24 hours of admission. This hospital
had a seven-day-a-week pharmacy service with
extended hours in the emergency department (ED).
One hospital implemented a multidisciplinary
process with doctors and nurses trained in taking
a BPMH and reconciling medicines. In the other
hospitals, pharmacy staff, mainly pharmacists,
were responsible for taking the BPMH and
reconciling medicines for admissions through
the ED. Apart from the lack of engagement
by medical and nursing staff in performing
medication reconciliation the actual steps
of the medication reconciliation process were
implemented without change. Hospitals used
a mix of paper and electronic tools to document
the BPMH and record medicines reconciled.
However, not all hospitals followed all
components of the implementation strategy.
Hospitals with a medication reconciliation
process already in place did not run a pilot and
those hospitals that had medication reconciliation
already in place or that lacked expertise in
the failure modes and effects analysis (FMEA)
process did not complete the risk assessment.
Australia requested some modifications to the
performance measures. They affected all hospitals.
See table 9 for the modifications sought.
92The High 5s Project Interim Report
Table 9: Modifications to SOP sought by Australia
Performance Issues Requested change Outcomemeasure
MR-1 Hospitals could not Use sampling A sample of 50
collect data on all to collect MR-1 was approved*
admissions of eligible
patients
MR 2-4 Monthly data Collect 3 monthly 3 monthly data collection approved
collection or 6 monthly after after meeting target for 12 months,
unsustainable consistently meeting 2011* 6 monthly collection
target of < 0.3 outstanding approved after 12 months of quarterly
discrepancies/patient reports meeting target, 2012*
MR-1 Difficult to perform Extend timeframe Not approved.
Med Rec within for Med Rec Australia will collect own data
24 hours to < 48 hours on Med Rec completed within
48 hours in addition to MR 1-4.
MR 2- 4 Definitions of Definitions be more descriptive Table of discrepancy examples
discrepancies were and include inclusions/ created and added to Volume 4
unclear and there exclusions and provide examples, – ‘Getting Started’ kit. A local
was concern about particularly in relation to PRN “How to guide” was also developed.
inter-rater reliability and complementary, medicines
* Approved by High 5s Steering Group

In addition to the evaluation plan another
challenging aspect of the SOP implementation
was changing the organizational culture from one
where medication reconciliation was regarded as
being only “pharmacy business” to one involving
medical and nursing staff in the process (Box 13)
93 Interim outcomes
Despite the difficulties engaging disciplines other than pharmacy in the medication reconciliation process
sites reported that the initiative was accepted and valued by other staff (Box 14).
Sustainability
Sites with weekend pharmacy services reported
the SOP was sustainable.
The five sites interviewed suggested sustainability
of the SOP was dependent on a number of factors
including:
ñ reducing the requirement for hospital staff
to provide ongoing education and including
training within university curricula;
ñ availability of electronic tools to support
the medication reconciliation process that
are integrated with electronic-prescribing/
medication management systems;
ñ continued engagement and support from
stakeholders;
ñ extending pharmacy services to 7 days a week;
and
ñ provision of ongoing/additional funding to
continue collection of performance measure
data.
In summary
It was feasible to implement the medication
reconciliation SOP in Australian hospitals. It is
a complex process, and successful implementation
requires support from the hospital executive
and senior clinicians, adequate resources and
a commitment to on-going training.
Box 13: A quote on sharing ownership of medication reconciliation
Hospital 1. ‘…another challenge we have faced is in engaging staff to share ownership of medication
reconciliation. While we have tried to increase awareness of medication reconciliation with posters,
competitions, staff education, etc., pharmacists still have ownership of the process, and are the only
ones formally doing and documenting medication reconciliation’.
Box 14: A quote on the value of medication reconciliation
Hospital 2: The implementation of the High 5s Project in the Emergency Department has seen
increased cohesion among ED nursing staff, ward nursing staff and pharmacy staff with the initiative
being welcomed by the ED staff.
France
Experiences implementing the Correct Site
Surgery SOP
This SOP was fully implemented in four out of eight
participating hospitals, and among these four
hospitals at full implementation, three have a
computerized High 5s checklist which is extremely
useful.
ñ The most common strategy used to facilitate
implementation was initially to begin with one
or two surgical specialties for implementation.
Three of the four hospitals, having chosen this
option, encountered two kinds of difficulties:
existence of multiple verification tools and no
sense of urgency for change.
ñ All participating French hospitals except one
(having no out-patient surgery in the in-patient
area) adapted the SOP to permit the delegation
of site-marking to nurses, after training by the
surgeons. This adaptation was necessary because
of the high number of out-patients having surgery
in in-patient ORs (was allowed by the SOP) or
of in-patients who are admitted on the morning
of their surgical interventions.
ñ The most challenging aspects of the SOP were:
Data collection for all the hospitals except
for one who integrated the High 5s checklist

into its electronic record from the beginning.
The workload was heavy, and no resources were
dedicated to support this effort most of the time.
Currently, five of the eight hospitals are working
on integrating the High 5s checklist into their
electronic record projects.
Site-marking faced resistance from surgeons in
six out of the eight hospitals. Working together
with the LTA to create a High 5s site-marking
guide was helpful. Each hospital has developed
procedures for site-marking in accordance
with the requirements of the SOP. Site-marking,
as a new practice in France not included in
the WHO Surgical Safety Checklist promoted
by HAS and mandated in the accreditation
process since 2010, has raised many
organizational, cultural, and technical questions,
as well as debates on the legality of a surgeon
delegating the marking responsibility to a nurse.
Lack of involvement of anesthesiologists in
the pre-op verification process was a common
challenge.
94The High 5s Project Interim Report
Some lessons learned
ñ The importance of contextual conditions, such
as team instability and reduced cohesion, lack
of leadership, and physician resistance.
ñ The critical role of an organization approach
to safety and the emergence of credible opinion
leaders who are seen as influential in effecting
changes in clinical practices.
ñ The need to include surgeons who are willing
to be champions.
ñ The importance of achieving full implementation
within a reasonable timeline in order to impact
a sufficient number of health-care professionals.
Experiences implementing the Medication
Reconciliation SOP
At the beginning of the project and after having
solved the first difficulties related to understanding
the protocol, the teams involved in medication
reconciliation started the implementation
by following the protocol and respecting all
of the eligibility criteria. However, the teams
were quickly confronted with barriers linked
to the organization of care. The main difficulties
related to:
Box 15: Interview findings in two French hospitals
Nurses working in a surgical ward: ‘At the beginning of the project, site marking looked like
an additional task and responsibility. I was against the delegation of this task by surgeons, but then
I understood that we are one of the links in the chain.’
Project coordinator: ‘Marking was intended for all patients admitted to a surgical unit starting April
2012. However, the majority of patients are admitted on the same day or for ambulatory surgery;
very few are admitted the day before. The marking procedure was put in place. The task was delegated
to a resident and then a nurse, under the surgeon’s responsibility. In approximately 70% of cases,
the task was delegated to a nurse. The borderline between what can be delegated and what cannot
was not always clear to the teams.’
ñ The expectation of formal medication
reconciliation within 24 hours after patient
admission when most organizations strive
to meet a 48-hour timeline which itself
was felt to be challenging.
– Currently, three hospitals are monitoring
Med Rec with a measurement of reconciliation
at 48 hours and at 24 hours.
ñ Questions regarding the most convenient place
to reconcile the patients; should this be on
the medical ward or directly in the emergency
department:
– Regarding the place where medication
reconciliation has to be performed, the teams
had to define whether it was more convenient
in their own organization to reconcile directly
in the emergency department or on the medical
ward. Currently, all except one hospital are
conducting medication reconciliation on medical
wards. This hospital center was particularly
successful in reconciling all of its patients
within 24 hours.
ñ The difficulty in extracting the data to satisfy
the Project’s performance measures:
– Initially, the information systems did not allow
extraction of the data needed for the
performance measures. Currently, teams involved

with the Med Rec SOP are using an Excel file
which was elaborated by the LTA. In addition,
some hospitals are struggling to access the
measure data for the Project measures where
medication reconciliation is fully integrated
into pharmaceutical care and is not easily
identifiable as such in the care process. This
barrier explains why a hospital does not presently
send any data because the design of its process
does not allow it to extract exhaustive data
on the number of reconciled patients within
48 hours (see Box 16).
95 Interim outcomes
Box 16: Example on how to overcome the data collection burden in Med Rec
In order to facilitate the data collection that allows monitoring of the medication reconciliation
practice, a general hospital, in collaboration with the LTA, is currently working on integration of
the medication reconciliation sheet into the information systems. As the computerized physician order
entry (CPOE) system does not support the iterative steps in the Med Rec SOP, the hospital developed
a tailor-made application directly connected to the inpatient electronic medical record. This tool can be
accessed from a reconciliation tab on the medical record screen.
Med Rec data can then be displayed across multiple medical episodes. Physicians and pharmacists can
consult or change the data at any time, and a historical record of changes can be made available.
Data indicators support automated calculation through a supervisor tool. To increase visibility for
the clinician, a summary of discrepancies, warnings and additional information can be made available
when the software is opened. Patient data can be extended to see more specific data (patient ID,
compliance, sources, and author). Med Rec screens, available for admission or discharge, display only
the most useful information in order to increase visibility and allow quick checking. A warning check
box can be manually enabled to display warning logos (e.g., no compliance warning), and free text can
be entered to describe which drug is available. Additional information about drugs stopped before
hospitalization can also be entered in a free text box at the bottom of the screen.
Medication reconciliation performed outside
Med Rec criteria
Currently, French hospitals are performing
medication reconciliation beyond the eligibility
criteria of the Med Rec SOP. Therefore, those
patients not fulfilling Med Rec criteria who are
reconciled are not included in the High 5s Project
database.
For example, several hospitals have started
to spread Med Rec to other medical units.
In the different units, all patients are now eligible
for medication reconciliation- not simply patients
65 years and older entering through the Emergency
Department. From the point of view of the
hospitals teams, it has helped having a better
integration of the medication reconciliation process
into daily medical practices. The pharmaceutical
teams in three hospitals have also started
to implement medication reconciliation upon
discharge.
Germany
To what degree was the SOP implemented
in all hospitals as it was originally defined?
A total of 14 of the 16 hospitals implementing
the CSS SOP have reached full implementation.
Of the two hospitals that have not reached full
implementation status, one has implemented the
SOP in all but one department (Ophthalmology).
The other hospital is the only JCI-accredited
hospital of the 16 hospitals, and it has not
implemented the High 5s checklist evaluation
in all departments. In one hospital which started
with Med Rec implementation, the SOP has been
partially implemented, but it is unlikely that full
implementation will be achieved in the course of
the project because of a lack of human resources.
It is difficult to reach overall conclusions regarding
the feasibility of the SOPs in the German context
because of the likely selection bias which exists
among the German hospitals who decided to
implement the High 5s SOPs. These hospitals
participate in the High 5s Project on a voluntary
basis and thus represent a more dedicated and
experienced group of hospitals than their
counterparts.
How did in-country hospitals modify the SOP
to facilitate implementation?
a) Correct Site Surgery
The adaptation of the international patient safety
tools to the German hospital context involved a
close collaboration between hospitals and the LTA.
The surgical checklist is used in Germany for both
implementation of the SOP and collection of data
for evaluation purposes. After translation and
reduction of the complexity and text density (e.g.,
by creating an instruction leaflet) a national model
version of the checklist was created that contained
the minimum criteria needed to adhere to the High
5s standardization requirements. Therefore,
a process step that is not part of routine clinical
care in German hospitals was removed from
the checklist, and two adaptation requests from
German hospitals relating to the site-marking
process were accepted by the High 5s Steering
Group: (1) It is now permissible to mark the site
with an “X” (adaptation on a national level), and
(2) medical professionals other than surgeons
are allowed to mark the site as well.
As a further result of the joint hospital workshops
it also became clear that it was necessary to
incorporate the checklist into already existing
preoperative processes in the participating
hospitals. Furthermore, more than half of
the hospitals were using surgical checklists when
the project started and did not want to start using
a completely new checklist. Thus 11 different
hospital-individualized checklists were developed
that – depending on hospital needs – contain
additional elements while maintaining High 5s
standardization.
The hospital-individualized checklists differ from
each other with regard to:
ñ comprehensiveness of depicted processes (e.g.,
in some checklists additional items from the
WHO Surgical Safety Checklist are included);
ñ level of detail of the instructions;
ñ design/structure/grouping of the items.
Furthermore, in relation to the use of the High 5s
checklist as an evaluation tool, the hospital
coordinators required the German LTA to remove
the section “Outcomes” from the checklist because
of legal concerns (e.g., documentation whether
an incorrect or potentially incorrect surgery was
identified, information on the degree of harm).
This is the reason why the German LTA does not
gather data for measure CS-7.See also Annex 16.
b) For Medication Reconciliation
Because of the fact that Med Rec is a new process
in Germany, some hospitals did not wish to start
with the “more difficult” population of the older
(65+) emergency patients but rather wanted to
begin with patients who have a planned or elective
admission. The German LTA offered to conduct
data analysis and produce data feedback reports
on these additional cases to the hospital, while
submitting only the data for the internationally
targeted population to the Collaborating Centre.
On the other hand, German hospitals, especially
the large university medical centers, had great
interest in collecting more data than the required
High 5s performance measures. Therefore, a
comprehensive data set was developed which
included additional information on patients (e.g.,
gender, age, diagnosis), type of staff involved
in the SOP, and type of drug along with more
detailed classification information (e.g. change
of dose, discontinuation of medication) for each
discrepancy.
In general, implementing the evaluation
components for both SOPs is the most challenging
part of the High 5s Project for all German
hospitals.
Specific issues relating to the SOPs themselves
a) Correct Site Surgery
Site-marking by the person who is conducting
the procedure was not feasible for the majority
of the German hospitals. Because of workflow
considerations, especially in larger hospitals,
one person is responsible for all admission
processes and has responsibilities like obtaining
consent from the patient and site-marking, while
a separate team performs the procedure.
Further concerns that were identified by the
hospital project coordinators in relation to the
site-marking process were staff hygienic concerns
relating to the markers used as well as the fact
that the skin mark often washes off during skin
preparation.
96The High 5s Project Interim Report
Implementing the team Time Out was challenging
for those hospitals which had no experience
with this process. A process step for which many
hospitals reported problems was the verification
of special equipment and implants prior to
the procedure. This process step does not occur
in proximity to the patient and the hospitals
therefore found it difficult to integrate it into
the workflow of completing the checklist.
b) Medication Reconciliation
Performing Med Rec within 24 hours after
admission is a great challenge for all Med Rec
hospitals because of a lack of resources (staff,
time). In Germany, there are only 0.3 pharmacists
per 100 hospital beds, which is one of the lowest
ratios in Europe. Therefore, it is very challenging
to achieve 100% Med Rec in the target group.
In the majority of the hospitals only a small number
of the patients constitute the target population
being evaluated.
The Netherlands
Dutch hospitals implemented all SOP steps
of the flow chart, except for one process step
of the Med Rec SOP for the targeted population.
A modification was requested for the process step
of consulting the patient. The SOP required asking
patients for their current medication list directly
after entering the Emergency Department. After
receiving a current medication list from the patient,
other sources had to be consulted (community
pharmacist or primary care physician list). Based
on implementation experiences, Dutch hospitals
preferred consulting patients only once: after
obtaining all possible other medication sources.
The SOP was subsequently revised by the High 5s
Steering Group to provide for a more generalized
model for medication reconciliation that gives
clinicians and facilities the freedom to define their
own process to obtain the BPMH and incorporate
this into their existing processes and workflow.
The most challenging aspects in the SOP
implementation included:
ñ interview with the patient;
ñ a sufficient IT infrastructure;
ñ continuous CEO support;
ñ data collection for SOP evaluation and SOP
monitoring;
ñ hospitals expected additional time for pharmacy
technicians and more staff to be needed
to implement and sustain the SOP, but these
resources were not readily available.
97 Interim outcomes
Box 17: Staff quotes regarding implementation issues of the Med Rec SOP
ñ “We created this by pilot projects and business cases. The High 5s Project has played a role in this.
We discussed business cases with the CEO of the hospital, we lobbied a lot, we shared results about
the effect, and we created a sense of urgency about the implementation of the national guideline
for medication accuracy at transitions in care.”
ñ “You really need manpower to carry out the project. For the sustainability of results you need
the same budget in the end. The initial costs during implementation are based on enough time for
the project leader. After implementation, these costs are free.”
ñ “We have chosen to implement the SOP without extra manpower from the hospital pharmacy.
Departments address themselves to this.”
Issues relating to the SOP implementation
ñ Hospitals tried to create more time for current
staff and find other solutions than demanding
more capacity for reconciling medications within
24 hours after admission during nights and
weekends.
ñ IT modifications were necessary to obtain needed
information to create a BPMH. Hospitals faced
challenges in obtaining licenses, workspace (for
computers) and extensions for current software.
When IT requirements were not met, interventions
and processes had to be adjusted in order to meet
the Med Rec goals.
ñ Although hospitals received permission for High
5s participation from their CEOs, a few hospitals
could not spread the SOP hospital-wide because
of budget restrictions during the financial crisis.
However, most hospitals have managed to
successfully spread the SOP hospital-wide.

The spreading of the SOP takes time depending
on the size of the hospital, awareness of
medication reconciliation, and other competing
priorities.
ñ With increased national awareness of medication
safety, some project leaders were able to restart
SOP implementation and to spread the SOP
to other inpatient services.
ñ Hospitals experienced challenges in implementing
the labor-intensive data collection for the
performance measures mainly because of time
constraints, lack of access to medical records
and lack of resources (staff, funding) to carry out
the work. Performance measures have been useful
in creating a sense of urgency (baseline
measurement) and to show improvements
(measurements after implementation). A hospital
staff member said that, ‘the method of measuring
was very supportive and it was great to use
evidenced based tools and indicators in daily
practice.’
ñ Although project leaders were able to use
the performance results to boost implementation,
the trade-off always was interviewing more
patients for the SOP. Another hospital staff
shared that, “When we have no performance
measurements in our hospital it does not mean
that our reconciliation process is not of good
quality. Measurements to monitor the process
also support the national patient safety
programme. During the upcoming months,
we will have internal sessions to provide feedback
about how to create an effective dashboard
to monitor reconciliation and to sustain the
reconciliation process.”
The issues and challenges mentioned above were
experienced in all Dutch hospitals. Medication
interviews with patients are an ongoing challenge,
which has generated difficult discussions among
hospital leaders, pharmacy representatives,
and physicians in participating hospitals.
Annex 18 shows a summary of the implementation
questionnaires after SOP implementation with
participating hospitals in which issues related
to the SOP implementation are investigated.
Singapore
The Correct Site Surgery SOP was intended for
implementation from Jan 2011 onwards in all seven
participating hospitals. Local surgical checklists
were modified to conform to the SOP, and staff
education sessions were conducted to familiarize
hospitals with this SOP.
There were several challenges noted:
1. Difficulty in changing conventional surgical
practice: In the initial stage of the project,
the bulk of non-compliance related to resistance
by surgeons in complying with site-marking
requirements and Time Out drills, in part because
of refusal to change from conventional practice
and a lack of understanding of the rationale
and requirements of the SOP. Their compliance
eventually improved through hard driving
by OT nurses who refused patient entry into
the operating theatre without a site mark
and refused to pass the instruments and proceed
with the operation until the Time Out was
properly conducted. However, not all nurses
felt empowered to stand up to surgeons.
To maintain compliance, High5 leaders have
found it useful to let data drive performance
by providing monthly feedback on performance
data to surgical heads. In addition, regular staff
education helped new staff understand the SOP.
2. Unpredictable pre-operative scenarios not
covered in SOP: Nurses had difficulty following
pre-operative verification components when
complicated scenarios not covered in the SOP
arose, such as language barriers when asking
open-ended questions to check the correct site
of surgery. To overcome this, posters and videos
were used to offer alternative follow-up actions
and improve compliance with the expectations
of the SOP.
3. Varied adaptation of SOP: Almost all
participating hospitals reported that if they used
a surgical skin marker for site marking, the site
mark invariably got washed off by Chlorhexidine
solution after cleansing, making it impossible
to see the site mark right before the Time Out
which was to occur after draping and cleansing.
It was noted that if Chlorhexidine was not used,
the site mark would not be washed away;
however, Chlorhexidine is the recommended
choice of antiseptic for surgical cleansing
in Singapore’s hospitals. It was then agreed
98The High 5s Project Interim Report

collectively that for cases where the site mark
is not visible after draping because a) the window
to the operative site is too small to view the site
mark, and/or b) the site mark has been cleansed
off, an acceptable alternative would be to
verbally confirm the laterality of the operative
site with the surgeon.
One of the hospitals also chose, in the alternative,
to conduct the Time Out before draping so that
the whole team could visualize and confirm the site
mark right before draping, even though the SOP
requires this to be done just before skin incision.
The above adaptations of the SOP were shared
during the High 5s webinar held in Dec 2011.
It was then suggested that data be collected
to substantiate the evidence for or against
the practice variations.
There have been no reported cases of wrong-site
surgery in operating theatres since the
implementation of the SOP in Jan 2011.
Trinidad & Tobago
The CSS SOP was piloted and is being implemented
at four of the five participating hospitals in its
original format. No changes have been suggested.
However, Project Team Leaders have noted
the challenge staff are experiencing in coping with
the perceived data collection burden given the fact
that many other data collection forms were already
in use within the various surgical units. A review of
all of the data collection tools used in the surgical
units was recognised as being urgently required.
All project team leaders agreed that the CSS SOP
will have a positive impact when fully implemented.
The hospitals that piloted the SOP have already
identified positive impacts such as:
ñ increased compliance with site marking;
ñ increased staff awareness and vigilance for
surgical safety;
ñ provision of an opportunity for staff to double
check the information given before surgery;
ñ encouragement/reinforcement of the importance
of teamwork; and
ñ encouragement of communication among
members of the surgical team.
The United States of America
The US hospital successfully incorporated the
High 5s checklist into its pre-surgical process
and received Institutional Review Board approval
for participating in the High 5s Project. Further,
it incorporated the ‘Event Analysis’ documents
into its data collection processes. The IT
department at the hospital was able to build an
electronic bridge from the OR electronic medical
record (EMR) Centricity® to a database accessible
to the datacollector for both the pre-operative
records and operative records. However, the
hospital later switched its pre-operative EMR
to another system, and the data collector had
to then hand-filter the relevant records.
The only modification the hospital requested
was to start sampling its cases because of the large
volume of the surgeries that would need to be
reviewed in accordance with the SOP. It provided
the LTA with a request to the Steering Group
to sample (see Annex 21 for the request), and
the High 5s Steering Group approved the request.
Currently, the hospital samples at least 261 cases
per month.
2. Impact
2.1. Overall issues
The SOPs have had a significant impact in all
participating Member States. As a result
of implementation of the SOP, certain process
steps were implemented. Safety components
are now built into surgical and medication
management workflows, and a culture of shared
ideas and learning among hospitals is promoted.
Impact of the Medication Reconciliation SOP
Thirteen hospitals in the Netherlands that
implemented the Med Rec SOP have demonstrated
equally significant medication communication
safety improvements. Medication inaccuracies
were reduced by 90% within the first five months
of the SOP’s introduction in six hospitals.
The percentage of patients reconciled within
24 hours rose by 40% in nine hospitals after
the first year of implementation and has been
increasing to 60% and even 90% following
a few years of implementation. The role of the
pharmacist in the Netherlands gained more visibility
and importance. The care process was unified
through better communication. Electronic
99 Interim outcomes

prescribing systems were introduced in some Dutch
hospitals and others have been able to access
community dispensing records electronically, as
a result of SOP implementation in an effort to
reduce errors. Sites universally achieved a reduction
in unintentional discrepancies.
When all of the LTAs implementing the Med Rec
SOP met, the positive impacts of different models
of implementation, e.g., pharmacist vs. technicians
creating the BPMH, were apparent, as shown by
the process measure, percent reconciled. As a
result, the French LTA was encouraged to consider
the use of pharmacy technicians in the Med Rec
process, as had occurred in the Netherlands. Lastly,
the comparison of and learning from each Member
State’s data and implementation processes was felt
to be beneficial by all of the Member States.
Impact of the Correct Site Surgery SOP
After several years of designing and implementing
the High 5s CSS SOP, positive impacts can be seen
in organizational safety cultures, process
improvement, and outcomes. Clearly, among
the health-care leadership in participating LTAs
and in hospitals, the High 5s Project has achieved
a heightened awareness of the value of
standardization and the risks associated with use
of non-standardized processes; of the actual level
of performance of defined processes (often lower
than had been assumed prior to measurement);
and of the value of teamwork in achieving higher
levels of performance. Comparison of culture
survey results (average composite scores) with
performance measure results (CS-0 through CS-4)
suggests a positive influence of an organization’s
safety culture on the success of its implementation
and level of performance of the standardized
procedures. Yet to be demonstrated is the reverse
influence; that is, the impact of SOP
implementation on the organization’s culture.
Precisely defined, collected, transmitted and
analyzed performance data suggest an
improvement in the key patient care processes:
preoperative verification, surgical site-marking,
and the Time Out before surgery. For example,
in France, site-marking was not routinely done prior
to introduction of the High 5s Correct Site Surgery
SOP. Since then, performance of this step in the
participating hospitals has gained traction with
performance levels ranging between 52% and 89%
for all eligible cases. In Singapore, a Member State
recognized for its rules-based culture, site-marking
performance improved from 40% to 97%.
Meanwhile, compliance with complete preoperative
verification and the pre-operative Time Out has
been consistently in the high 90% range.
If implementation of standardized operating
protocols is successful, does it have an impact on
the patient safety problem that the SOP is designed
to address? Measuring outcomes in patient safety
initiatives is always challenging and especially
so when the outcomes to be measured, in this case,
incorrect surgeries, are relatively infrequent.
The small sample of hospitals, the limited
timeframe for the Project, and the uncertainty
of complete reporting of all wrong-site surgery
cases all add to the difficulty of demonstrating
an actual decrease in the number of incorrect
surgeries. By the end of the Project, there may be
sufficient data to answer this key question.
However, in the meantime, a surrogate measure
is available by considering the results of CSS
performance measure No. 4: Proportion of Cases
with Discrepancy Noted at Final Time Out and
performance measure No.5: Proportion of Cases
Undergoing Surgery with Unresolved Time Out
Discrepancies. Together, these measures indicate
cases at risk for incorrect surgery because of
identified discrepancies that remain unresolved
when the surgical procedure is begun. Certainly
not all of those cases would have resulted in wrong
site surgeries, but some of them may well have.
The relative proportion of the types of unresolved
discrepancies–factual, procedural, or documentary–
is, at this time, unclear but it is reasonable to assert
that a decrease in the number of unresolved
discrepancies is a proxy for a reduction in
the number of incorrect surgeries. However,
this approach is limited in that these measures
apply only to discrepancies identified during
pre-operative Time Out. Ideally, any discrepancies
that arise throughout the process of preparing
patients for surgery would be identified and
reconciled long before the patient gets to the
operating room.
Unfortunately, these “good catches” are not
routinely measured as part of the High 5s
evaluation strategy. Recently France has recognized
this deficiency and instituted a supplemental
measurement activity designed to identify cases
in which discrepancies have been identified and
reconciled at all stages of the preoperative process.
Data showing types of discrepancies, steps in the
100The High 5s Project Interim Report

process where they most frequently occur,
categories of health professionals who identify
them, and other useful data are emerging along
with compelling stories of individual cases that
were impacted by performance of the standardized
procedures of the SOP. Other participating
Member States have been encouraged to emulate
this measurement approach initiated by the French
LTA in hopes that the database for assessing impact
on surgical outcomes as a result of the High 5s
Project will be enhanced in time for the final
project report.
2.2. Summary of Member State experiences
Australia
Impact of SOP implementation or participation in
this Project
a) Leadership
At some sites, the performance measure data
has proven useful in obtaining executive and senior
clinician engagement with the SOP.
b) Hospital
Several sites have reported a change in the hospital
culture, with medication prescribers actively
looking for and responding to the pharmacist’s
BPMH and recommended actions in the medication
management plan (see Box 18).
101 Interim outcomes
c) Hospital processes
Eight sites integrated the medication reconciliation
SOP into their existing processes to some extent.
Box 18: Medication reconciliation culture change across the organization
“The successful implementation of medication reconciliation in an organization requires an entire
culture change across the organization involving all disciplines. Implementation is complex and difficult
and it’s hard not to get discouraged. However the positives have been a much greater awareness
of medication safety across the organization.”
Box 19: Raising awareness about best practice of medication reconciliation
Hospital 7: Raised awareness of the process of obtaining a BPMH, medication reconciliation and
follow up of discrepancies ultimately resulted in better processes.
Hospital 2: The High 5s Project has resulted in an increased awareness of best practice medication
reconciliation throughout the hospital.
The SOP enabled hospitals to have a standard,
defined and improved protocol for medication
reconciliation (see Box 19).
Several hospitals chose to use the national
Medication Management Plan (MMP) to
standardize the documentation of medication
reconciliation. This enabled pharmacists to record
outstanding discrepancies requiring resolution in
a standard place in the patient’s notes and readily
available when medicines were prescribed.
Since implementing the SOP the MMP has been
viewed as a multidisciplinary tool for
communication rather than a pharmacy document,
as had been the case prior to the High 5s Project
(see Box 20).
Box 20: MMP for reconciliation of medications
Hospital 5: The medical specialties within the hospital now look for the MMP for reconciliation of
the medications when reviewing the patient and completing the medication discharge summary. It has
enabled the doctors to provide complete medication summaries to the primary care providers, including
documenting the status of medications, e.g., continued, dose increased/decreased, ceased. This has led
to improved communication in the transitions of care and also with the patient.

One hospital reported implementation of
the SOP had effects beyond the medication
reconciliation process (see Box 21).
ñ improving patient safety.
Sites reported that the implementation of the
SOP has improved the quality of the medication
histories obtained and documented by pharmacy
staff. The low figures reported for the MR 2- 4
performance measures demonstrate the benefit
of having a standard process on the quality
of the medication reconciliation performed.
See section 5.4.5 for results.
Resolving discrepancies early in the admission
allowed for timely resolution of medication issues
on discharge, thus reducing delays in discharging
patients. It also freed up time for pharmacists to
educate patients about their medicines (see Box 22).
102The High 5s Project Interim Report
Box 21: SOP impact beyond the medication reconciliation process
Hospital 2: When reviewing existing processes, the hospital identified multiple problems with their
current medication management processes. As a result, there has been a greater focus on
standardization of medication management, prescribing and patient safety, including the introduction
of the National Inpatient Medication Chart in the Emergency Department.
Box 22: Comprehensive counseling to patients
Hospital 5: Having nursing staff aware that all discharge summaries must be reviewed by a pharmacist
prior to discharging a patient has enabled pharmacists to provide comprehensive counselling (written
and verbal) to patients with the opportunity for patients to ask questions.
d) Patient care/clinical impact
Around half of the hospitals indicated that
implementation of the SOP had an impact on
related or interacting activities and on patient care.
Most were considered positive and included:
ñ having a standard and improved protocol
for medication reconciliation;
ñ improving processes through raising awareness
of the processes of obtaining a BPMH, reconciling
medicines and following up on discrepancies;
ñ using data collected to plan interventions
to follow up on discrepancies;
ñ collection of data not previously accessible;
A downside of increasing the quantity and quality
of medication reconciliation performed when
resources are limited is that it is done at the
expense of other activities such as patients
receiving a regular review of their medicines. One
of the reasons given by hospitals for withdrawing
from the Project related to competing priorities.
e) Communication
Communication about the High 5s Project and
the organization’s commitment to the Project
was disseminated primarily through announcements
and progress reports made at department/project
specific meetings, newsletters, and information
posted in public areas. Staff updates on SOP
implementation are primarily provided through
regular reporting of performance measures,
quarterly reports, and periodic reports of specific
aspects of the Project. Lack of resources and
organizational support or guidance were
the primary challenges to communication.
f) Resolving discrepancies
By auditing the quality of the medication
reconciliation process hospitals were able
to identify that some discrepancies remained
unresolved for some days and sometimes until
the time of discharge. As a result, discharges were
often delayed while the discrepancy was resolved.
Initially identified as a problem by one hospital,
other hospitals soon reported similar problems.
This led to the development of two additional
performance measures to assist hospitals collect
data on outstanding discrepancies unresolved after

48 hours following admission. Hospitals used this
data to provide feedback to prescribers, thereby
reducing the number of unresolved discrepancies.
Impact of multi-pronged approach to SOP
evaluation
a) Patient care /clinical impact
Hospitals reported that implementation of the
SOP has resulted in a more standardized process
for obtaining a BPMH, training staff, reconciling
medicines and resolving discrepancies. The benefit
of using a standardized approach to medication
reconciliation is demonstrated in the results of
the audits undertaken by the independent observer.
Hospitals have found the performance measure
data useful for identifying gaps in practice and staff
training needs and for further improving their
processes. Overall the Australian performance
measures show patients that receive medication
reconciliation at admission are at low risk of having
an adverse medication event as the result of
a discrepancy between the medicines taken prior to
admission and those prescribed during the hospital
admission. This risk has continued to decrease over
the duration of the project. See figures in Annex 10.
A limited number of event analysis reports have
been submitted, none of them for a medication
reconciliation incident causing serious harm.
The four hospitals that have submitted event
analyses report that the process has provided
them with valuable information on their medication
reconciliation processes and failures (see Box 22).
This information has been used:
ñ to improve the medication reconciliation process;
ñ as case studies in education sessions to highlight
to other clinicians what can go wrong when the
medication reconciliation SOP is not followed.
See section 5.4.3 for further information on event
analysis.
b) Engagement of frontline providers and/or
senior leaders
Several sites reported that the performance
data has been useful in engaging executive staff
and senior leaders (see Box 23).
103 Interim outcomes
Box 23: Engagement of frontline providers
Hospital 1: Intermittent reporting of Med Rec rates increases knowledge and awareness, and
reinforces processes. All executive staff within the facility are now aware of the MMP and its use.
There is now heightened awareness of the benefits and value of obtaining a BPMH and performing
medication reconciliation.
Performance measure MR-1 allows hospitals to
measure the proportion of the eligible population
receiving medication reconciliation and has been
useful in some hospitals for making a successful
case for more resources (see Box 24).
Box 24: Improving services
Hospital 1: Significant and sustained improvement in MR-1 rates was realized with the initiation of
a Saturday ward-based clinical pharmacist service that provided medication reconciliation for new, high
risk admissions.
frontline clinicians about the project and
encouraging them to follow the SOP (see Box 25).
The performance measure data and event analysis
information has also been useful for informing
Box 25: Maintaining support
Hospital 1: Reporting of improving MR-1 rates maintains support and enthusiasm for the initiative.
104The High 5s Project Interim Report
c) In-country awareness and support for the
initiative
Inclusion of medication reconciliation within
Standard 4 (Medication Safety) of the National
Safety and Quality Health Service Standards
has raised the awareness of the process as
an important patient safety activity. The need
to demonstrate compliance with the Standards
for accreditation will drive the widespread uptake
of the process in Australian hospitals. In addition,
one of five medication safety priority activities in
the Australian Safety and Quality Goals for Health
Care requires everyone aged 65 and over to have
their medicines reconciled within 48 hours of
admission to hospital. The Commission continues
to support the initiative through working with
the hospitals implementing the High 5s Project
and leveraging off this work to advocate the
process with key stakeholders and develop
resources to assist hospitals with implementation.
France
Impact of the Correct Site Surgery SOP
This SOP has had significant impact on health-care
facilities in terms of improving communication
between health-care professionals and improving
the safety culture.
a) Patient care/clinical impact
All health-care professionals interviewed by the
LTA highlighted the impact of this SOP on patient
safety and improved communication between team
and patient.
b) Hospital processes
The High 5s Project has allowed health care
organizations (HCOs ) to optimize their surgical
care pathway and to better distribute tasks and
roles to each professional involved thus linking
all of the professionals involved in the patient’s
care ‘from scheduling to the intervention’.
c) Culture of safety
ñ Nurses feel more empowered, reflecting a real
cultural shift to be able to speak up in instances
of discordance which in turn can foster effective
communication among members of the
perioperative team.
ñ Standardized site-marking allows for shared
responsibilities among surgeons and nurses
when site-marking is delegated.
ñ The High 5s Project has had a positive impact
on teamwork for the hospitals at full
implementation.
d) Information
An ongoing process of information gathering
and verification along the patient’s preoperative
pathway has added value to the quality of patient
records. Most of the Project teams highlighted
that the use of the High 5s Checklist has led
to structured information and improved
communication among nurses, anesthetists,
physicians, secretaries and others involved in
the care pathway (Box 26).
A common and unique tool to collect information
during the surgical pathway, including procedures
already implemented before the High 5s Project
was in place has been developed in several
hospitals. It is known as the “Carnet de bloc”
or “livret de parcours interventionnel”.
Box 26: How best to implement the CSS SOP
The four HCOs at full implementation wish to continue using the CSS SOP. They believe that
implementing this SOP is sustainable in their hospitals provided that the pre-operative verification
component is less complex and time consuming and that an electronic checklist is linked to
the patient’s medical record.
Among the four HCOs at partial implementation, three are facing major barriers but are continuing
to carry out the SOP despite the fact that they have not succeeded in reaching full implementation.

105 Interim outcomes
Impact of the Medication Reconciliation SOP
This SOP has also had significant impact in
health-care facilities in the re-engineering of care,
improving communication between health
professionals, and improving the safety culture.
a) Process re-engineering of care to improve
efficiency
To improve the efficiency of medication
reconciliation and increase the number of patients
who received medication reconciliation within
24 hours, one Med Rec hospital has reorganized
its reconciliation process. To maintain the benefits
of medication reconciliation, pharmacists involved
in the process have designed a training programme
for physicians and residents. This programme
includes specific time to explain the flowchart
and makes physicians aware of how to stop
medication errors.
Physicians dedicated the same amount of time
to medication reconciliation before and after
the process re-engineering. However, there is no
shared information system between the hospital
and the community. The next challenge for this
hospital is full implementation of medication
reconciliation from patient admission to discharge.
b) Improvement of communication between
healthcare professionals for better patient care
In another hospital, it was noticed that after
18 months of implementation, this SOP had
actually contributed to increased cooperation
between physicians and pharmacists. Beyond
the improvement experienced in medical care,
the benefits of better communication and
coordination of health-care professionals can
contribute to saving physician time and
improvements to patient safety (Box 27).
Box 27: Improvements in the safety culture and quality of care
One Med Rec hospital used the experience of participating professionals to identify and highlight
potential significance of failures of the process, to assess the risks if these failures occur and to propose
preventive measures. The experience also helped to prioritize failures in terms of the potential severity
of their effects, frequency of occurrence, and the risks associated with their non-detection.
This study was conducted using FMEA (Failure Mode and Effects Analysis) to evaluate potential risks
emerging in the process of medication reconciliation.
The researchers used the Joint Commission worksheet adapted from the model used by Good
Samaritan Hospital (Dayton, Ohio) and a predefined scale index published by Williams. This work led
to a better understanding of the constraints of the process and sensitization of all stakeholders involved
in the process.
To improve practice, better performance must be defined as:
- setting a fixed time every day for reconciliation and immediate correction or documentation in
the computerized file;
- training for and assessing the quality of the patient interview; and
- recording the data collected by the pharmacist in the computerized medical file.
c) Measuring clinical impact of unintentional
discrepancies
One university hospital took the lead in studying
the clinical impact of unintentional discrepancies.
Based on their experiences in monitoring
practices, they developed an algorithm to assess
the potential clinical impact of unintentional
discrepancies. To evaluate the robustness of
the algorithm, the national Med Rec group initiated
a study in volunteer hospital participating in
the High 5s Project in order to see if there are
differences in how professional groups approach
unintentional discrepancies in different hospitals.
Germany
a) Hospital culture
In some hospitals the existing culture was
positively stimulated as a result of implementation
of the CSS SOP. Project coordinators reported
that there was heightened perception among
staff that there is an active commitment to patient
safety in the organization. Other hospitals
did not recognise a cultural change as a direct
result of the project because of its small
magnitude in relation to other initiatives.

b) Hospital processes
Feedback of some hospitals: “It’s not just
a checklist, it has helped us to fundamentally
change the way we look at our process.” Thus
the systematic implementation of the SOP radiates
to other not yet standardised processes, and other
projects were affected, for example in the
introduction of wristbands with identification tags
for patients. Hospitals experienced in the use
of surgical checklists prior to the High 5s Project
reported that the project provided a new impetus
in their implementation efforts and that the existing
processes were improved as a result.
c) Patient care/clinical impact
At this time, the overall change in patient safety
cannot be described with certainty. However,
the procedural steps can help to identify safety
gaps in the care of individual patients through
the documentation of the checklist. As a result,
the risk potential for patients at certain steps of
the process has been reduced. Project coordinators
reported that they feel that the awareness of
patient safety as a whole has improved in their
organizations.
d) Communication
By way of the CSS SOP, the pre-operative processes
have been defined more clearly, and a simplification
has subsequently been introduced. Because
of the implementation and individualisation of
the checklists, there is more transparency about
responsibilities (who does what and when) in
the already existing communication process.
It is difficult to draw conclusions about the impact
of the evaluation approach at this time.
Because of the fact that the checklist data
collected since mid-2012 is being fed back much
more rapidly to the hospitals, it will be interesting
to see whether an improvement in the process
measure results is noticeable after 2012. In
addition, national bi-annual benchmark reports
have been provided to the hospitals since
mid-2012, and their impact will be analysed later
through an updated implementation questionnaire.
The Netherlands
Impact was seen in several areas:
a) Leadership
The SOP implementation makes Med Rec
a multi-disciplinary process with clear steps for
each professional group, including the engagement
of patients. Hospital pharmacists contributed
more to the treatment of the patient, patients
were more involved in the process, doctors and
nurses were further aware of the hospital pharmacy
contribution during the Med Rec process, and
nurses experienced easier access to the hospital
pharmacy (Annex 19A and B).
b) Hospital culture
Implementing this SOP contributed to greater
awareness regarding the:
1. patient safety culture in hospitals; and
2. the existence of discrepancies in medication lists.
Some hospital staff have stated that, “because
of SOP implementation there’s more awareness
about the risks of medication errors. In combination
with the national patient safety programme there
are lots of positive changes made. It has led to
more awareness.” The SOP is part of patient safety
in our organization”.
c) Hospital processes
Through implementing the SOP, it has become
clear which professional group is responsible
for creating the BPMH. The steps are set to identify
and resolve discrepancies and assure interview
of patients about their medications within 24 hours
after admission in the Emergency Department.
The hospital pharmacy and through it the
medication reconciliation process, now becomes
part of the treatment of the patient.
d) Patient care/clinical impact
Hospitals have found it difficult to demonstrate
the impact of the SOP on patient safety. However,
with the help of the four performance measures,
it is possible to show the improvement in SOP
implementation (Annex 19A and B). One hospital
stated that SOP implementation had a huge impact
on the reduction of discrepancies in medication
accuracy during transfers, as well as an impact
on medication safety (Annex 19C). Although
the measured reduction in medication errors is
important, the clinical relevance of the reduction
measured is open to question. Broader studies
are needed, such as assessment of the duration
of hospitalization in order to demonstrate
its clinical impact on patient safety.
e) Communication
High 5s Project hospital teams were fully aware
that communication strategies were needed to
implement and sustain this SOP. They used internal
meetings, training sessions, newsletters, posters
and lots of discussion to introduce the SOP
106The High 5s Project Interim Report

interventions and to spread the new ways of
working together. The commitment to identifying
and resolving discrepancies within a multidisciplinary
processes has become a structured way of working
which, in turn, has improved Med Rec
communication among pharmacists, physicians,
nurses and other health-care professionals.
f) Resolving discrepancies
A greater awareness of medication discrepancies
was created in the Emergency Department
because of implementing this SOP. The SOP also
contributed to awareness raising regarding
this issue in other departments (Annex 19C).
In the Netherlands, a reduction of 75%-90%
in discrepancies within five months after SOP
implementation has been seen. A challenge faced
by most hospitals has been to increase the average
percentage of patients reconciled within 24 hours
because of insufficient pharmacy staff available
seven days a week. More resources are needed
to reconcile 100% of the patients within the
24 hour limit.
Singapore
a) Process for change
To enable effective implementation, the Ministry
of Health teamed up with patient safety champions
in each hospital to form a local High 5s Network.
In addition, the Ministry of Health funded an
additional Healthcare Performance Office (HPO)
High 5s executive in each hospital to assist in data
collection and gap closure. The Project was
a joint collaboration between the Ministry of
Health and all public hospitals, involving surgeons,
anaesthetists and nurses.
Gap closures initiated by institutions between July
2010 and March 2011 included:
ñ revising surgical checklists;
ñ educating staff on the SOP;
ñ developing data collection methods;
ñ developing SOP scripts and videos: KK Women’s
& Children’s Hospital, Jurong Health Services
and Tan Tock Seng Hospital (TTSH) wrote
a Time-Out script. These hospitals subsequently
experienced marked improvement in Time Out
compliance, as staff could follow the step-by-
step requirements in the Time Out drill. TTSH
prepared instructional video footage of actual
time-outs being performed. This received positive
feedback as staff learned the SOP steps better
by seeing them played out in real scenarios.
Gap closures initiatives by the Ministry
of Health included:
1. Regular platforms for sharing and learning:
The Ministry of Health hosted bi-annual
sharing platforms for the High 5s Network to
reach mutual consensus on changes to be
effected. In addition, between January and
March 2011 when data collection was first
launched, fortnightly informal meetings were
held to assist executives in overcoming
problems encountered.
2. Standardizing data collection: To standardize
data collection, an excel spreadsheet was
established for executives to enter data and
derive compliance rates. The Ministry of
Health also adapted the WHO Surgical Safety
Checklist to the local context, including
deriving a calculation sheet for institutions’
reference. This adaptation was a core catalyst
for institutions to adopt the High 5s checklist
and begin data collection.
3. Ensuring data validity: The institution’s
executive performed monthly observational
audits of documentation submissions to ensure
rigour of the data collected. In addition, SQI
co-ordinated additional quarterly Cross Review
Validation Exercises (CRVEs) that engaged
executives from participating institutions
to minimise bias. Discrepancies noted during
the observations enabled the institution’s
executives to identify differences in actual
practice versus paper audits and suggest
measures to address them.
b) Strategy for change
The High 5s champions are leaders in their professions
such as head surgeons and anaesthetists. As such,
initiatives were better disseminated to health-care
professional participants. The institution’s
executives were funded by the Ministry of Health
but reported directly to the hospital management.
From January 2011 onwards, monthly compliance
data were reported back to OR staff and senior
management. Based on the data, staff noted areas
that needed improvement and gradually showed
increased compliance with the SOP. Overall,
it took two years to implement the SOP and reach
a steady state in data collection.
107 Introduction

c) Impact of SOP implementation
The High 5s Network met to review and discuss
the data since the Ministry’s last update in May
2012, and observed that in addition to improved
hospital processes, there were other benefits of
the Time Out drill that were not measured through
the performance measures, such as improvement
in communication between surgical team members
and better coordination arising from the process
of identifying themselves to each other before
the procedure. These were noted to be important
intangible impacts of the SOP on the
communication culture in Singapore Hospitals.
The impact of the SOP on both leadership and
culture of the hospitals was positive. Many hospital
leaders gave positive feedback on how the
collaboration had led to:
ñ improved communication between the Ministry
and the hospitals;
ñ embedded a continuous learning culture in
the hospitals, showing that staff were willing
to change conventional practice given the right
resource support (i.e., with Ministry funding
support of the High 5s Executive); and
ñ demonstration that hospital processes can be
re-designed to provide better patient care.
The clinical impact was that there had been
zero wrong-site surgery cases reported from
major operating theatres since the SOP was
implemented.
Overall, there were four key achievements in the
implementation of the Correct Site Surgery SOP
project:
1) Incorporated permanent improvements in
the OR workflow of all hospitals, in particular:
ñ establishing that site-marking should be done
before the patient enters the OR;
ñ standardizing the site mark as an arrow, and
not a cross, circle or tick, or any other symbol;
ñ instituting a Time Out to ensure a last check
for site and side of the operation; and
ñ design of IT solutions to help hospital staff
follow the protocol. Initially, only one hospital
(National University Hospital) had an OR
dashboard. By the end of 2012, two other
hospitals (Khoo Teck Puat Hospital and Tan
Tock Seng Hospital) had similarly created
electronic systems to hard-wire the checklist
into their workflow.
2) Increased awareness of surgical safety issues:
ñ implementing the CSS SOP resulted in increased
awareness of safety components built into OR
workflows. Through monthly audits, OR staffs
in all hospitals were kept abreast of their
compliance data and the areas that needed
improvement. The High 5s Project then became
a buzzword for surgical safety.
3) Established a sharing platform:
ñ the setting up of the local High 5s Network
to implement the project provided an avenue
for staff in different hospitals to learn
from each other and continuously innovate
to support a patient safety culture.
4) Introduced data quality validation measures:
ñ the Ministry of Health successfully initiated
‘Cross Review Validation Exercises’ (CRVEs)
for hospitals to audit each other. While
external audits were not required as part of
the SOP, the executives found that it not only
helped to validate each other’s work, but
it also allowed them to reflect on each
institution’s workflow designs and take the
learning points back to their own institutions.
The journey for Singapore hospitals has been
a positive one, and the hospitals have requested
similar style collaborations with the Ministry
of Health to look at other patient safety matters
such as medication safety protocols, for example,
Medication Reconciliation.
The United States of America
The U.S.A. hospital has found that the High 5s SOP
strengthens processes and procedures. Using the
High 5s CSS SOP as a springboard, they evaluated
their pre-op process and are making improvements.
In particular, they evaluated the patient and
document flow in the pre-op holding area. Key
takeaways from this improvement process were
that nurses played a key role in the patient safety
process, and sufficient care in the pre-op holding
area is currently playing a key role in preventing
significant issues from arising in the OR.
108The High 5s Project Interim Report

7Developingnetworks andawarenessraising for the High 5sProject

1. Developing global networks andawareness raising
This global collaboration among international
organizations, agencies and WHO Member States
has been very fruitful. From the onset of
the Project, founding members from WHO and
The Joint Commission/Joint Commission
International– serving as the WHO Collaborating
Centre– sought to optimize the prospect of success
by reaching out to all participants and experts
to agree on the following characteristics:
ñ Collaboration and good will: The concepts of
standardization applied throughout the Project
have consistently been built and based on
consensus among the various networks of LTAs,
associates, and experts in the participating
Member States.
ñ Achievement of country ministerial commitments
to the Project through the existing WHO
networks of WHO with Ministries of Health
of the participating Member States.
ñ Shared global vision coupled with local
ownership among all those participating in
the High 5s Project.
ñ Provision of an evidence base for all steps in
the SOPs and the ‘Impact Evaluation Plan’
developed through global networks of experts.
ñ Project design that included engagement and
continuous improvement platforms as well as
the national networks of hospitals – the learning
communities– which permit necessary local
adaptations that do not change the given SOP,
but modify the way it is implemented in ways
acceptable to the hospitals and LTAs in the
Member States.
ñ Emphasis on the role and interrelationship
of the country-level networks of health care
professionals and teams rather than individuals
alone.
ñ Embodiment of the principles of patient-centered
care by actively involving the patients and
families in the SOP processes, particularly as
most participating Member States patients
are becoming more active participants in their
own care.
Building networks nationally and globally was
clearly one of the critical activities of this Project
that underlay its success. Project participants
had been actively building networks, and continue
to do so, since its inception in 2006.
Raising awareness of the Project was supported
by promoting its activities globally, engaging
interest on the importance of standardization as
a means to safety, attracting global experts and
expert institutions to the Project, securing funding,
and influencing public and political opinion about
the importance of patient safety.
International and national approaches to addressing
specific patient safety problems through extended,
multi-country networks can ensure that there
is true capacity-building in patient safety
worldwide. From a global perspective simply seeing
the implementation of standardized patient safety
protocols by a small number of resource-rich
countries is not sufficient. Over time, the networks
that participating Member States, WHO and
The Joint commission have with transitional and
resource-poor countries will help to support the
adaptation and implementation of these protocols
within the developing world. This is one important
way that the participating Member States, can share
their expertise and technical resources worldwide.
Despite the many other successes in building
global and national networks, implementation
of standardized operating protocols across the
boundaries of multiple countries was fraught with
sociopolitical challenges. The inherent differences
among national and international institutional
110The High 5s Project Interim Report
Developing networks and awareness raisingfor the High 5s Project
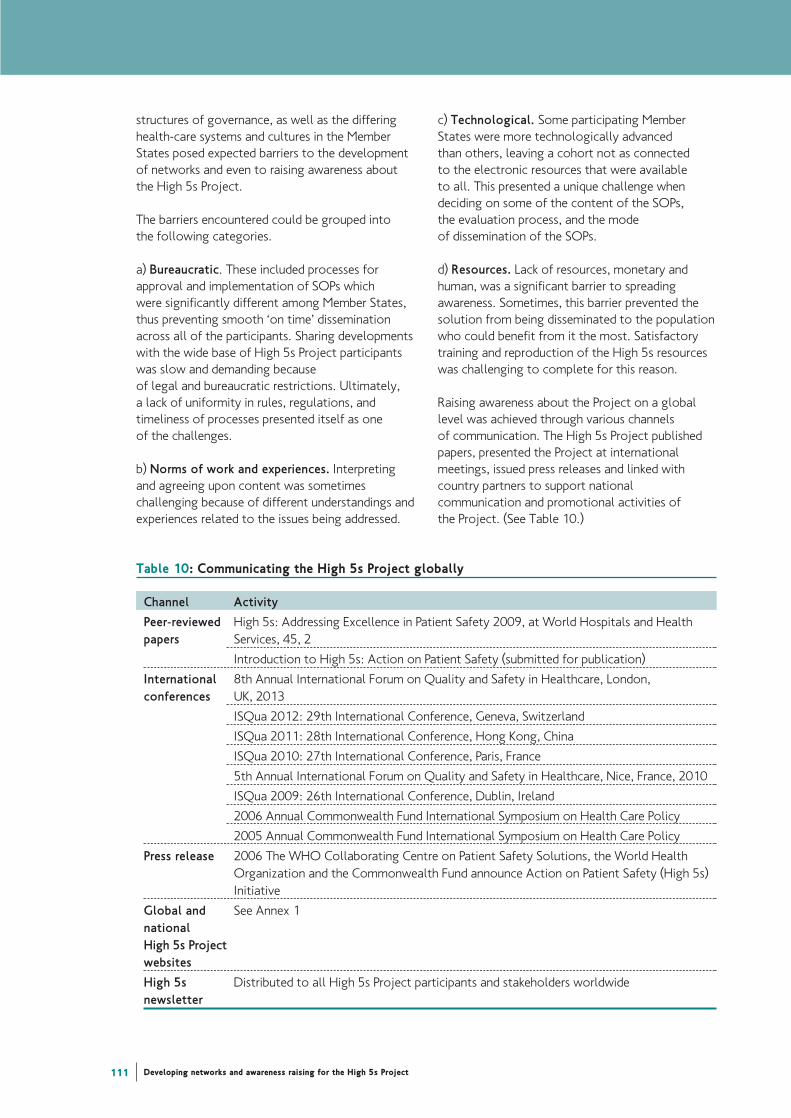
structures of governance, as well as the differing
health-care systems and cultures in the Member
States posed expected barriers to the development
of networks and even to raising awareness about
the High 5s Project.
The barriers encountered could be grouped into
the following categories.
a) Bureaucratic. These included processes for
approval and implementation of SOPs which
were significantly different among Member States,
thus preventing smooth ‘on time’ dissemination
across all of the participants. Sharing developments
with the wide base of High 5s Project participants
was slow and demanding because
of legal and bureaucratic restrictions. Ultimately,
a lack of uniformity in rules, regulations, and
timeliness of processes presented itself as one
of the challenges.
b) Norms of work and experiences. Interpreting
and agreeing upon content was sometimes
challenging because of different understandings and
experiences related to the issues being addressed.
c) Technological. Some participating Member
States were more technologically advanced
than others, leaving a cohort not as connected
to the electronic resources that were available
to all. This presented a unique challenge when
deciding on some of the content of the SOPs,
the evaluation process, and the mode
of dissemination of the SOPs.
d) Resources. Lack of resources, monetary and
human, was a significant barrier to spreading
awareness. Sometimes, this barrier prevented the
solution from being disseminated to the population
who could benefit from it the most. Satisfactory
training and reproduction of the High 5s resources
was challenging to complete for this reason.
Raising awareness about the Project on a global
level was achieved through various channels
of communication. The High 5s Project published
papers, presented the Project at international
meetings, issued press releases and linked with
country partners to support national
communication and promotional activities of
the Project. (See Table 10.)
111 Developing networks and awareness raising for the High 5s Project
Table 10: Communicating the High 5s Project globally
Channel Activity
Peer-reviewed High 5s: Addressing Excellence in Patient Safety 2009, at World Hospitals and Health
papers Services, 45, 2
Introduction to High 5s: Action on Patient Safety (submitted for publication)
International 8th Annual International Forum on Quality and Safety in Healthcare, London,
conferences UK, 2013
ISQua 2012: 29th International Conference, Geneva, Switzerland
ISQua 2011: 28th International Conference, Hong Kong, China
ISQua 2010: 27th International Conference, Paris, France
5th Annual International Forum on Quality and Safety in Healthcare, Nice, France, 2010
ISQua 2009: 26th International Conference, Dublin, Ireland
2006 Annual Commonwealth Fund International Symposium on Health Care Policy
2005 Annual Commonwealth Fund International Symposium on Health Care Policy
Press release 2006 The WHO Collaborating Centre on Patient Safety Solutions, the World Health
Organization and the Commonwealth Fund announce Action on Patient Safety (High 5s)
Initiative
Global and See Annex 1
national
High 5s Project
websites
High 5s Distributed to all High 5s Project participants and stakeholders worldwide
newsletter

2. National networks and awarenessraising
Australia
Participation of Australian hospitals in the High
5s Medication Reconciliation initiative has been
used to raise awareness and promote the concept
of multidisciplinary medication reconciliation
at a national level. The Australian Commission
published three articles on medication
reconciliation in professional journals and has
presented on the Australian experience with
the High 5s Project at a number of national and
international conferences over the period 2010
to 2012. These include the International Society
for Quality in Health Care (ISQua), The Society
of Hospital Pharmacists of Australia (SHPA)
Conference, the National Medicines Symposium,
and the Australian Association for Quality in
Health Care (AAQHC) conference. For a full listing
of titles of abstracts and peer-reviewed articles
see Annex 11.
The Commission has developed a medication
reconciliation webpage that houses a number
of resources to assist hospitals to implement
a formal process of medication reconciliation.
http://www.safetyandquality.gov.au/our-
work/medication-safety/medication-reconciliation/
Australian High 5s hospitals contributed to
the development of the resources. The national
Medication Management Plan (MMP) published
by the Commission in October 2010 provides
health service providers with a standardised form
that can be used by nursing, medical, and pharmacy
staff to record the BPMH and reconcile medicines
on admission. Other tools include an online
training presentation on how to use the MMP, and
a range of posters and brochures using the theme
MATCH UP Medicines for use in hospitals to
promote the process of medication reconciliation
(Annex 9).
The Commission also works closely with NPS
MedicineWise to have medication reconciliation
messages included in initiatives to improve the
quality use of medicines in the community. One
of the results of this work is a consumer wallet and
brochure that highlights the importance of being
knowledgeable about your medicines and having
an up-to-date medicines list. High 5s hospitals
provide the wallet to patients on discharge from
hospital with their discharge medication list,
and other medication information. It has been
distributed to a number of hospitals outside of
the High 5s group (see Annex 9 for an illustration
of the wallet insert).
The Commission has also raised awareness among
the ambulance authorities of the importance of
bringing the patient’s own medicines to the hospital
when patients are admitted by ambulance from
home.
France
On the CSS SOP
ñ Awareness was raised through presentations
and posters presented by the High 5s teams and
the LTA at national and international meetings
(e.g., International Conference on Quality
and Safety, French Annual National Patient Safety
Week, HAS Annual Meeting, French Society
for Orthopedic Surgery).
ñ A quarterly newsletter has been widely distributed
to hospitals and institutional partners as well as
within HAS.
ñ HAS has placed particular focus on site-marking
and will soon disseminate the site-marking guide.
ñ A national conference is planned for 2013-2014
will disseminate High 5s Project data and present
the outcomes of the Project to date, as well as
lessons learned.
On the Med Rec SOP
ñ The High 5s teams have realized several
opportunities to present to professional societies
and health care institutions during pharmaceutical
congresses to promote this practice.
ñ Presentations and posters presented by pharmacists
and the LTA, (e.g., French Pharmaceutical
Congress, French Society for Clinical Pharmacy,
French Regional Workshop on Quality and Safety).
ñ Presentations on the High 5s Project and the Med
Rec SOP at the national meetings of OMEDIT
Aquitaine, part of the national OMEDIT network
in collaboration with the Ministry of Health.
This meeting takes place every semester and
brings together stakeholders in medication safety.
This activity helped to provide visibility for all
of the hospitals that have been implementing
Med Rec but are not involved in the High 5s
Project. The LTA’s objective is to gather
information from these teams in order to
understand how they succeeded in setting up
the medication reconciliation process and
to develop a national network for sharing
experiences.
112The High 5s Project Interim Report

Germany
The participation of Germany in the High 5s Project
has fostered a strong German learning community
of hospitals. The LTA organizes workshops for
the hospitals with the aim of training the trainers
and sharing experiences. In addition to the High 5s
international news bulletins which are circulated
to the German hospitals, the German LTA has set
up a national mailing list. This mailing list is used
to distribute SOP-specific information to
the hospitals on an irregular basis. This information
encompasses recent SOP-specific literature, case
studies from CIRS, television programme tips
or newspaper articles regarding patient safety,
and conference presentations and posters, as well
as other patient safety resources.
The German LTA and the High 5s hospitals
regularly attend national and international patient
safety and quality conferences and give High 5s
presentations, thereby increasing the awareness
of the Project. In addition, SOP-specific
publications in several widely-read professional
journals have achieved much attention for
the Project in Germany. In this context, the LTA
and participating hospitals have received many
inquiries on SOP-specific issues.
The expert advisory committee convened by
the Ministry of Health ensures strong connections
between the High 5s Project and the German
Society of Surgery as well as the German
Association of Hospital Pharmacists. The Ministry
of Health and these experts have established links
between the High 5s Project and related projects
being conducted in Germany. Further, they support
Project implementation by making suggestions
for further Project development and for ensuring
its sustainability.
The Netherlands
The High 5s network started in the Netherlands
in 2009. Within this network, hospitals have
worked together to carry out the SOP. Hospitals
collaborated with CBO to disseminate results
at international/national conferences on patient
and medication safety through workshops/(master)
classes, (poster) presentations and site visits.
Twelve hospitals took part in an extra data-
collection effort on the effect of pharmacy-based
medication reconciliation in the Netherlands.
A list of dissemination activities from 2009 till
present can be found in Annex 20. Because of
a press release in February 2011 highlighting a 75%
reduction in medication discrepancies following
implementation of the Med Rec SOP, and because
the pilot hospitals were successful in their SOP
implementation and results, many more hospitals
became interested in joining the Project. Even
though it was difficult for them to find resources
to participate during the time of financial crisis,
four hospitals joined the network using their own
budgets. Mental health and long-term care were
enthusiastic about the Project, but unfortunately
were not able to allocate budgets and manpower
to become involved in the Project.
Singapore
The High 5s Correct Site Surgery project was
presented at the Ministry of Health Work Plan
Seminar 2012 held in August 2012 which was
attended by the Singapore Permanent Secretary
and Health Minister. The Work Plan Seminar is
an annual event that provides a platform for the
Ministry of Health to share Healthcare 2020 plans
and initiatives with all of the Public Hospitals,
and also serves as a forum for hospital clusters
to share initiatives that they have put in place
to support Healthcare 2020. The two part-time
Network co-chairs were invited to present the
journey and success in implementing the CSS SOP.
The messages highlighted (i) how cross-cluster
co-operation has brought about great success for
everyone and ultimately better care for patients,
and (ii) the innovations and different methods
adopted in the project. Feedback by the hospital
CEOs on the presentation was positive.
Internationally, Singapore efforts to implement
the High 5s Correct Site Surgery SOP have been
showcased via poster display at the 23rd Annual
National Forum on Quality Improvement in Health
Care in Florida in December 2011. An updated
poster was again displayed at the International
Forum on Quality and Safety in Healthcare in Paris
in April 2012, and another updated poster
was presented at ISQUA’s 29th International
Conference in Geneva in October 2012.
Trinidad & Tobago
The piloting of the CSS SOP on the orthopaedic
units has created a renewed awareness of the
importance of staff communication (verbal and
written) in achieving and maintaining patient safety.
Project team members have recognised the need
113 Developing networks and awareness raising for the High 5s Project

for ongoing monitoring, and evaluation of
the Project as well as continuing sensitization
of both executive and clinical staff. National
networks with other public and private hospitals
are yet to be established.
The United States of America
The Joint Commission alongside a number
of partners has made significant strides in raising
awareness of wrong-site surgery. Through
the Center for Transforming Healthcare, The Joint
Commission has engaged with the Lifespan
Hospital System in Rhode Island. A result of that
collaboration was the Targeted Solutions Tool
for Wrong Site Surgery, which allow organizations
to identify, measure, and reduce risks in key
processes that can contribute to a wrong-site
surgery.
114The High 5s Project Interim Report

8High 5smeetings

1. Steering Group meetings
The High 5s Steering Group includes participants
from all LTA, WHO and Collaborating Centre
leadership, experts from the fields of surgery and
pharmacy, and the US Agency of Healthcare
Research and Quality (AHRQ). Together, the
Steering Group has created and approved the SOP
content and the processes for evaluation and event
analysis. All collaboration takes place either via
electronic modes of communication such as emails,
conference calls, and webinars or through
the two face-to-face meetings every year.
Although the SOPs have been implemented
in different Member States and under different
conditions and cultures, it is both surprising and
comforting that similar problems are found in
all settings. When this happens, the Steering Group
is able to assist each other in identifying solutions
that work. Through collaboration, the High 5s
Project team has found supportive partners in
Ministries of Health and other groups who are
contributing to improving the feasibility and impact
of the standardized protocols.
2. International hospital meeting
A one-day ‘First International High 5s Hospitals
Meeting ‘took place at WHO Headquarters in
Geneva in October 2012. The meeting provided
a platform where High 5s hospital teams and LTAs
met to discuss experiences, share best practices,
compare evaluation data, and provide
recommendations and best ways forward for
the High 5s Project. The hospital meeting served
as a hub for an inter-country exchange of
knowledge and implementation experiences to
strengthen and motivate hospitals’ commitment.
The meeting brought together 80 participants
representing 31 High 5s hospitals from Australia,
France, Germany, the Netherlands, Singapore and
the United States of America. Participants included
hospital technical and management staff, and LTA,
Collaborating Centre and WHO Patient Safety
Programme staff. Three High 5s experts from
Canada and the United States of America joined
the meeting. Each participating Member State
had selected one hospital per SOP to share
implementation experiences and lessons learned.
In addition, High 5s hospitals from Australia,
France, Germany, the Netherlands and Singapore
presented 30 posters. Hospital data showed that
SOP implementation has had positive impacts on
hospital processes and patient care. The poster
jury consisting of the three High 5s experts
together selected one poster per SOP for the
“High 5s Achievement Award”. Singapore National
University Hospital won the “High 5s Achievement
Award” for the CSS SOP, and the “High 5s
Achievement Award” for the Med Rec SOP went
to The Netherlands Medical Center Alkmaar.
In the break-out session, meeting participants
formed five Working Groups to exchange
information on SOP implementation challenges,
qualitative and quantitative evaluation activities,
and the impact of the SOPs across diverse country
cultures and settings. Hospital participants were
able to discuss directly with High 5s Steering
Group members their experiences and challenges,
and to contribute ideas on the best ways forward.
For further information see Annex 22.
116The High 5s Project Interim Report
The High 5s Steering Group meetingsand international hospital meeting
9Next steps

1. Overview
Implementation of the SOPs is progressing
successfully in participating hospitals and Member
States. A collaborative effort by WHO, the
Collaborating Centre, all LTAs and experts is being
made to keep the SOPs updated and to amend
them as needed. Plans to disseminate the SOPs
and share the evaluation methodologies with
the rest of the world are also being developed.
It is expected that at the last Steering Group
meetings in 2014, discussions will focus on how
to promote and share SOPs, methodologies,
lessons learned and expertise worldwide, and on
how to build networks with the developing world.
The handover of the Information Management
System (IMS) and the primary location of project
data and analysis will be determined by the time
data collection comes to a close in September
2014. The Steering Group intends to make the
transfer smooth such that this utility can be used by
Member States and organizations after the official
close of the High 5s Project anticipated
in early 2015.
The SOPs have been developed with the intent
that hospitals and organizations worldwide can
readily adopt them and improve patient care and
safety. Cultural, bureaucratic and practical lessons
that were learned by the High 5s teams and LTA
staff will be shared with the world community.
Barriers faced by teams were similar despite
the differences in regions and cultural contexts,
for that reason, the documentation of some
solutions to these barriers should be useful.
Paramount to all efforts will be active engagement
with existing partnerships that the LTAs, WHO
and Joint Commission International already
have with transitional and developing countries
to support the promotion, adaptation and
implementation of the protocols within more
countries around the world.
Some of the successes of this international
collaborative have been largely the collaboration
itself. From the inception of the Project, the
leadership was composed of international public
health experts and those interested in patient
safety, along with organizations like WHO
and Joint Commission International. This special
relationship between organizations and individual
experts has led to the successful analysis of
the feasibility and impacts of the High 5s SOPs
at a ‘grassroots’-level.
2. The cross High 5s medicationreconciliation map
An interactive online map was developed by
the Institute for Safe Medication Practices (ISMP)
Canada, the Med Rec SOP lead, to profile High 5s
achievements in the participating Member States
which have implemented the Med Rec SOP.
The map includes Med Rec implementation site
information and highlights High 5’s Med Rec
implementation publications and national supports
such as accreditation standards. Links for all
are supplied where available. Participating Member
States were provided a country-specific map graphic
to use for marketing and communications and to
connect teams and sites. The map is available at
http://www.ismp-canada.org/medrec/map/world/
3. Next steps by LTAs
Australia
SOP implementation
The next step for Australia is to spread the SOP
to patient discharges. Quality improvement
measures are currently being developed and will be
available for hospitals (including High 5s hospitals)
to collect information on discharge medication
reconciliation and how to measure improvement.
118The High 5s Project Interim Report
Next steps

Adopting new SOPs
The Commission will not be adopting any new
High 5s SOP.
Expansion to additional hospitals
As of January 2013, all hospitals in Australia
are required to meet the NSQHS Standards as part
of the new national accreditation scheme.
This requires hospitals to be assessed against
two criteria in the Medication Safety Standard that
relate to medication reconciliation. The model
of medication reconciliation described in the
Standard 4 - Medication Safety Standard Safety
and Quality Improvement Guide – the resource
developed to assist hospitals implement
the NSQHS Standards - follows that of the High 5s
Medication Reconciliation SOP. The objective
is for the medication reconciliation SOP to be
implemented in all Australian hospitals.
The Commission will be working with the State
and Territories to achieve this objective and is
developing additional resources to assist hospitals
to implement Medication Reconciliation and
monitor their activities. These will include
a MATCH UP Medicines medication reconciliation
toolkit, a BPMH training tool, and performance
measures to measure medication reconciliation
performed on admission and at discharge.
France
Next steps are presented in Table 11.
119 Next steps

120The High 5s Project Interim Report
Table 11: Next steps for French LTA
CSS Med Rec
Full implementation of the CSS SOP in the four HCOs at partial To support and assist
implementation seven or eight hospitals to
develop full implementation
a)The LTA is reinforcing its support in order for the HCOs to overcome of medication reconciliation.
the barriers identified (visits, conference calls, and team training are Currently, they are not fully
going to be proposed by the CEPPRAL). The goal is to spread SOP operating within the framework
implementation throughout the entire hospital. The standardized of High 5s Med Rec criteria.
evaluation activities would be limited to a few units.
b) Advice is being developed on how to use these SOP results to help
organizations ensure safety when patients are admitted on the day of
the surgical intervention, as this situation will soon become prevalent.
Engage the hospitals CEOs
Targeted communications towards the CEOs of the participating hospitals will be conducted, e.g., for
the CSS SOP, a quarterly newsletter addressing issues of leadership, culture safety, and comparative results
A workshop is planned at the end of the year in order to share experiences and results.
Foster recognition of the contribution of the High 5s teams participating in the Project and reward
their efforts.
Dissemination of lessons learned and results of the High 5s Project
HAS is planning a conference with a large audience of interested stakeholders where outcomes and
lessons learned will be presented. This is essential for the successful integration of the High 5s experience
into the national strategy on patient safety. Publications and communications in French by the hospital
High 5s teams and the LTA will also support the dissemination effort.
Scale up the High 5s Project good practices to the national level
Site-marking and pre-operative verifications Medication Reconciliation
A committee including the Ministry of Health, HAS and
the CEPPRAL has recently been set up to develop a strategy
for spreading the learning about patient safety practices
derived from the High 5s Project to the national level.
Promoting site-marking at the national level
ñ The surgical checklist is a required practice in France but
does not include site markings. Spreading and adoption
of site-marking practices will have a major impact
on surgical safety. As a first step, HAS decided to promote
site-marking in the next HCO accreditation cycle. Feedback
from High 5s hospitals shows that a sense of “ownership”
of this practice has developed within the teams involved
in the Project. A community of “champions” has grown
and will have a major role in the uptake of this good practice
by other teams. Site-marking will also be extended to
outpatient surgery.
ñ Pre-operative verification: Additional analysis of the feedback
and High 5s data will be conducted on the pre-operative
verification process. Data and success stories derived from
this analysis will provide inputs on the HAS surgical safety
programmes.
Develop a strategy on the
spreading of High 5s Med Rec
outcomes and lessons learned
at national level, and also take
into account the experiences
of the health care facilities not
participating in the Med Rec
project which perform
medication reconciliation
ñ Integrate Med Rec as
a patient safety practice
in the medication safety
policy, working in
collaboration
with all the stakeholders
in the field;
ñ Provide Med Rec guideline
and toolkits adapted to the
different types of HCOs.

Adopting new SOPs
The adoption of new SOPs is not being considered
at present because of limited resources and funding
HAS, as well as ongoing policy requirements
concerning budget restrictions in the French public
sector.
To conclude, a large amount of work and sharing
of knowledge and experience has been undertaken
since France became engaged in the High 5s Project.
At present, integrating Project recommendations
and conclusions into the national strategy is one
of the main challenges. To this end, the French
experiences and exchanges within the global
learning community and the High 5s Steering
Group have been invaluable.
Germany
SOP implementation
CSS: The German LTA has encouraged the hospitals
to submit their data on a monthly basis for a period
of at least two years. Several hospitals are eager
to submit data for a longer period and to receive
feedback until the end of 2013. Because the
German data model is very resource-consuming
(i.e., scanning of the checklists, creation of
feedback reports for each hospital), the LTA will
stop accepting checklists at the end of 2013
and will focus on a detailed final analysis of the
checklist data during 2014. A majority of the
hospitals have signaled that they will maintain the
SOP processes (or modified versions of the SOP)
and checklists after the High 5s Project has ended.
Med Rec: Following the translation, adaption
of the implementation tools and the development
of a data collection tool, the hospitals officially
started implementation and evaluation of the SOP
in the spring of 2013. Data collection is to
continue until December 2014, with subsequent
final analysis of the data.
A public workshop will be organized in June 2015
to present the final Project results.
Expansion to additional hospitals
CSS: There is no expansion of the current project
planned. However, following the final analysis of
the multidimensional evaluation data on the
national and international levels, the German
LTA plans to draft a “best implementable surgical
checklist” and a clinically well-assessed SOP.
These High 5s findings will be published as
recommendations for German hospitals.
Med Rec: The German LTA is planning on recruiting
3 to 5 more hospitals for implementation.
The Netherlands
The Dutch Ministry of Health has been supporting
participation in the High 5s Project and the pilot
group since 2009. Follow up activities on the
SOPs are being discussed, and other parties will
be involved in planning about the spreading of
knowledge and outcomes to other hospitals and
facilities. The outcome of the national patient
safety hospital programme (2008-2012) shows
the importance of the theme of medication
reconciliation for elective and discharged patients,
which is still not effective enough. For the target
population (65 years and greater admitted
through the ED) of the High 5s SOP it is clear
that implementation of the SOP is still needed
after comparison of baseline and subsequent
performance measurements among three different
groups of hospitals between 2010 and2012.
Based on the results of the national patient safety
hospital programme and the experiences with
the High 5s SOP for Medication Accuracy
at Transitions in Care, the Dutch Inspectorate
of Health has highly recommended this SOP be
continued in the Netherlands (see Box 28).
121 Next steps

In June 2013, the High 5s SOPs were mentioned
by NIVEL in the evaluation research of the national
patient safety programme in Dutch hospitals
(NIVEL and EMGO). Dutch High 5s Med Rec
hospitals are also interested in adapting the SOP
for Concentrated Injectables SOP. These hospitals
have emphasized that, “the international
contribution is great because of the learning
community. We would also like to implement
another SOP, for example, the SOP for
Concentrated Injectable Medicines. This is also
a theme of the national patient safety programme.
If there’s any external budget available, we would
like to participate in this SOP”.
In the Netherlands the Concentrated Injectables
SOP could also be used to implement the national
guideline on this topic which was also part of
the national patient safety hospital programme
(high risk medication). In 2013, the LTA has started
a pilot on the Concentrated Injectables SOP in
16 hospitals in collaboration with national experts
and the support of the Ministry of Health.
Singapore
The High 5s Network has expressed interest in
implementing the High 5s SOP to other areas
where appropriate and feasible, such as the
Radiology Department and Day Surgery Operating
Theatres, and the Ministry of Health is strongly
supportive of this. They have also suggested
stepping up the frequency of CRVEs so that more
cross institutional observations can be conducted
to validate practices. The Ministry of Health will
continue to maintain a facilitative role for
institutions to do so.
Meanwhile, the Ministry of Health has gone ahead
to adopt the Medication Reconciliation SOP into
the National Standards for Healthcare document
for Public Hospitals in Singapore and to commence
implementation. The target date to begin to
collect data is currently set for April 2013.
The Ministry of Health will continue to support the
High 5s initiative through funding of the headcount
to support the data requirements of the Project
until the end of the Project in December 2015.
Trinidad & Tobago
The Ministry of Health plans for:
ñ full implementation of the CSS SOP at relevant
surgical units of all public hospitals by April 2014;
ñ expansion to the private hospitals within Trinidad
and Tobago during the latter half of 2014;
ñ development and issuance of a National Policy
on Site Marking to all health-care providers
(public and private); and
ñ review and revision of all supportive data
collection tools used by staff in the surgical units
to achieve standardization.
The United States of America
In the U.S.A., there are two potential avenues
for adoption of SOP components via process
of care measures. In general, the benefit of the
process of care measures is that they are designed
to provide prima facie evidence of linking process
to outcome. One avenue of leverage is through
accreditation, while the other avenue is through
re-imbursement.
122The High 5s Project Interim Report
Box 28: Committed to improve medication reconciliation in Dutch hospitals
The discussion in Dutch hospitals on the capacity of hospital pharmacy technicians to reconcile patients
and to complete the medication reconciliation process is all about costs for extra staff. However,
the Dutch Inspectorate of Health wrote in November 2012:
“WHO committed to improve medication accuracy at transitions in care. WHO integrated this topic
in the High 5s programme to improve patient safety. The implementation of this project which has been
supported by CBO in 15 Dutch hospitals showed us in the Netherlands a reduction of 75% of
inaccuracies in the actual medication overview of patients which can be realized by using the WHO
developed Standard Operating Procedure (SOP). Commitment to this topic is definitely worth it.
Because of the necessary deployment of extra staff, hospitals now appear quite able to actually carry
out medication reconciliation. Investment in this staff pays for itself quickly. Medication wrongly given
or not given while necessary, leads the patient and thereby the hospital to undesirable situations and
to greater costs [12:p.27, 28].

If the accreditation approach were to be pursued,
the obvious outlet would be through The Joint
Commission. The Joint Commission is the
accrediting body for over 20 000 healthcare
organizations and programmes in the U.S.A.
Accredited hospitals incur site visits every third
year and are evaluated by series of criteria.
The Joint Commission currently uses “Accountability
Measures” which are designed to incorporate
four constructs: research, proximity, accuracy, and
adverse events. According to The Joint Commission,
the measure needs to be proven by research that
the process being measured is closely connected
to the outcome it impacts. Further the measure
should accurately assess whether the care process
has actually been provided, and whether the
measure, as designed, minimizes or eliminates
unintended adverse effects. Most SOP measures
would fit within all four of these constructs.
The second avenue would be through hospital
re-imbursement from the US Centers for Medicare
& Medicaid Services (CMS). Starting in FY12,
hospitals are now scored on conducting certain
processes (compared to a benchmark) and
demonstrating their improvement. The scores are
used to calculate incentive payment amounts.
Hospitals risk losing 1% in Medicare inpatient
payments, eventually rising to 2% by 2017. It is
expected that the programme will expand in FY14,
with the addition of 20 more measures.
It should be noted that The Joint Commission
and CMS have worked together to develop
measures in the past. If this course is chosen, an
approach similar to the one taken in 2003 by CMS
and The Joint Commission when they co-wrote
the ‘Specifications Manual for National Hospital
Inpatient Quality Measures’ could be used.
123 Next steps
Related Documents











