body of research has addressed several pertinent questions concerning this issue: Does substance abuse run in families? If so, is the risk inherited? If yes, just what is inherited—a vulnerability for abuse of a specific substance, or vulnerabil- ity factors underlying the risk for development of a number of substance use and addictive behavioral problems? Twin studies are particularly well suited for investigating these questions. The unique structure of twin data allows the relative effects of genetic, shared environmental, and unique environmental influences to be explicated. Monozy- gotic (MZ) twins share 100% of their genes, while dizygotic (DZ) twins share, on average, 50%. Both MZ and DZ twin pairs generally share 100% of their family environment; such influences are assumed to promote resemblance equally in MZ and DZ pairs. Thus, greater similarity among MZ twins compared with DZ twins suggests genetic influ- ences on the phenotype under investigation. By comparing MZ and DZ correlations, we can arrive at estimates for these three sets of influences. Over the past decade, we have stud- ied the genetic and environmental determinants of addic- REVIEW The Harvard Twin Study of Substance Abuse: What We Have Learned Ming T. Tsuang, MD, PhD, Jessica L. Bar, MA, Rebecca M. Harley, PhD, and Michael J. Lyons, PhD The Harvard Twin Study of Substance Abuse was carried out with the members of the Vietnam Era Twin (VET) Registry. The VET Registry comprises over 8000 male twins who served in the United States military between 1965 and 1975 and were subsequently inter- viewed regarding their use of licit and illicit substances, as well as various types of psychopathology. Our research has demonstrated significant influences by genetic, shared environmental, and unique environmental factors on the abuse of illicit substances. Multivariate analyses have indicated that the co-occurrence of abuse of various types of illicit drugs reflects a common vulnerability, influenced by both genetic and environmental factors, that cuts across all categories of illicit drugs. We have also demonstrated that some drugs have unique determinants, both genetic and environmental, that are not shared with other drugs. In part, the genetic influence on marijuana abuse is mediated by genetic influence on subjective effects in response to the drug. The determinants of transitions from one stage of drug use to another differ depending on which drug or which transition is examined. We determined significant genetic influences on several aspects of nicotine and alcohol use separately, as well as genetic influences shared by both substances. We found that the co-occurrence of illicit drug abuse and major depression is due to unique environmental influences. The phenotypic association between symptoms of conduct disorder and alcohol and marijuana dependence is due largely to shared environmental influences. Our results, thus far, indicate a complex pattern of genetic and environmental influences on substance use and abuse. (HARVARD REV PSYCHIATRY 2001;9:267– 279.) Substance abuse is widely recognized as one of the most com- plex and problematic issues facing today’s society. Agrowing From the Harvard Institute of Psychiatric Epidemiology and Genet- ics (Drs. Tsuang and Lyons), Massachusetts Mental Health Center (Dr. Tsuang), and the Department of Psychology, Boston University (Ms. Bar, Drs. Harley and Lyons), Boston, Mass. Supported by a grant (DA04604) from the National Institute on Drug Abuse (Dr. Tsuang), and the Department of Veterans Affairs Health Services Research and Development Service and Coopera- tive Studies Program (Study 992). Original manuscript received 20 March 2001; revised manuscript received 20 June 2001, accepted for publication 25 June 2001. Reprint requests: Ming T. Tsuang, MD, PhD, Massachusetts Mental Health Center, 74 Fenwood Rd., Boston, MA 02115 (e-mail: [email protected]). 2001 President and Fellows of Harvard College 267

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
body of research has addressed several pertinent questionsconcerning this issue: Does substance abuse run in families?If so, is the risk inherited? If yes, just what is inherited—avulnerability for abuse of a specific substance, or vulnerabil-ity factors underlying the risk for development of a numberof substance use and addictive behavioral problems?
Twin studies are particularly well suited for investigatingthese questions. The unique structure of twin data allowsthe relative effects of genetic, shared environmental, andunique environmental influences to be explicated. Monozy-gotic (MZ) twins share 100% of their genes, while dizygotic(DZ) twins share, on average, 50%. Both MZ and DZ twinpairs generally share 100% of their family environment;such influences are assumed to promote resemblanceequally in MZ and DZ pairs. Thus, greater similarity amongMZ twins compared with DZ twins suggests genetic influ-ences on the phenotype under investigation. By comparingMZ and DZ correlations, we can arrive at estimates for thesethree sets of influences. Over the past decade, we have stud-ied the genetic and environmental determinants of addic-
REVIEW
The Harvard Twin Study of Substance Abuse:What We Have Learned
Ming T. Tsuang, MD, PhD, Jessica L. Bar, MA, Rebecca M. Harley, PhD, and Michael J. Lyons, PhD
The Harvard Twin Study of Substance Abuse was carried out with the members of theVietnam Era Twin (VET) Registry. The VET Registry comprises over 8000 male twins whoserved in the United States military between 1965 and 1975 and were subsequently inter-viewed regarding their use of licit and illicit substances, as well as various typesof psychopathology. Our research has demonstrated significant influences by genetic,shared environmental, and unique environmental factors on the abuse of illicit substances.Multivariate analyses have indicated that the co-occurrence of abuse of various types ofillicit drugs reflects a common vulnerability, influenced by both genetic and environmentalfactors, that cuts across all categories of illicit drugs. We have also demonstrated thatsome drugs have unique determinants, both genetic and environmental, that are notshared with other drugs. In part, the genetic influence on marijuana abuse is mediatedby genetic influence on subjective effects in response to the drug. The determinants oftransitions from one stage of drug use to another differ depending on which drug or whichtransition is examined. We determined significant genetic influences on several aspectsof nicotine and alcohol use separately, as well as genetic influences shared by bothsubstances. We found that the co-occurrence of illicit drug abuse and major depressionis due to unique environmental influences. The phenotypic association between symptomsof conduct disorder and alcohol and marijuana dependence is due largely to sharedenvironmental influences. Our results, thus far, indicate a complex pattern of genetic andenvironmental influences on substance use and abuse. (HARVARD REV PSYCHIATRY 2001;9:267–279.)
Substance abuse is widely recognized as one of the most com-plex and problematic issues facing today’s society. A growing
From the Harvard Institute of Psychiatric Epidemiology and Genet-ics (Drs. Tsuang and Lyons), Massachusetts Mental Health Center(Dr. Tsuang), and the Department of Psychology, Boston University(Ms. Bar, Drs. Harley and Lyons), Boston, Mass.
Supported by a grant (DA04604) from the National Institute onDrug Abuse (Dr. Tsuang), and the Department of Veterans AffairsHealth Services Research and Development Service and Coopera-tive Studies Program (Study 992).
Original manuscript received 20 March 2001; revised manuscriptreceived 20 June 2001, accepted for publication 25 June 2001.
Reprint requests: Ming T. Tsuang, MD, PhD, Massachusetts MentalHealth Center, 74 Fenwood Rd., Boston, MA 02115 (e-mail:[email protected]).
� 2001 President and Fellows of Harvard College
267

tive behaviors using a large national cohort of twins whoare members of the Vietnam Era Twin (VET) Registry.This paper reviews our findings in an attempt to summarizewhat has been learned from the VET Registry thus farabout the phenomenology and etiology of substance use dis-orders.
THE VIETNAM ERA TWIN REGISTRY
The VET Registry consists of over 8000 male-male twinpairs born between 1939 and 1957 in which both siblingsserved on active military duty during the Vietnam era (May1965 to August 1975). Twins were originally identified in thelate 1980s through a search of the Department of Defensecomputer files of discharged servicemen.1,2 Individuals withthe same last name and date of birth but different firstnames were identified as potential twins. From a list ofapproximately 5.5 million veterans, 15,711 potential twinpairs were identified. Military records of possible pairs werethen examined to confirm twinship. Zygosity was evalu-ated by analyzing responses of twin siblings to a series ofquestions on twin similarity and limited blood group typingobtained from military records.3 This method achieved 95%accuracy.
In 1992, information about drug and alcohol use and life-time prevalence of comorbid psychiatric disorders was col-lected from VET Registry members by telephone interview.Of 10,300 individuals (5150 pairs) determined to be eligiblefor the study, 47 were deceased or incapacitated. Data weresuccessfully collected from 8169 of the remaining 10,253individuals (response rate, 79.7%). The 1874 MZ and 1498DZ pairs in which both members responded to the drugabuse items constituted the final sample. Sociodemographicbreakdown of the group revealed the following character-istics:
Age: Mean, 44.6 years (SD, 2.8; range,36–55 years)
Race: Non-Hispanic white: 90.4%African-American: 4.9%Hispanic: 2.7%Native American: 1.3%“Other”: 0.7%
Education: High school graduate: 33.3%Vocational school attendance: 15.8%College graduate: 38.6%Graduate training and/or a gradu-
ate degree: 10.6%Other/data not available: 1.7%
Employment: Employed full-time: 92.6%Employed part-time: 1.8%Unemployed: 5.6%
Marital status: Married: 75%Never married: 11%Currently unmarried/data not
available: 14%Residence: All 50 states of the U.S.
Registry members are representative of all twins who servedin the military during the Vietnam War on a variety of socio-demographic and other variables.4 A complete description ofVET Registry construction has been published elsewhere.1,2
Subjects were interviewed using the Diagnostic Inter-view Schedule Version III Revised (DIS-III-R),5 a structuredinterview employed in epidemiological research. Interviewswere performed over the telephone by the Institute forSurvey Research at Temple University. Interviewers weretrained by a member of our group (MJL) and their super-visor, who had attended a training course conducted by thedevelopers of the DIS-III-R. Telephone interviews wereused instead of on-location interviews because of the geo-graphic diversity of the sample. Several studies6–8 have sup-ported the comparability of telephone and face-to-face inter-views.
Responses to the DIS-III-R were used to diagnose psy-chiatric disorders according to the revised third edition ofthe Diagnostic and Statistical Manual of Mental Disorders(DSM-III-R).9 Information was collected about VET Registrymembers’use and abuse of a number of substances, includingalcohol, nicotine, and five classes of illicit drugs (i.e., mari-juana, sedatives, stimulants, heroin/opiates, and psyche-delics). In our discussions of illicit drugs, we are referring tothe specific drugs in these five classes.
ILLICIT DRUGS
Approximately 10% of the VET Registry sample (totalsample size � 3372 twin pairs) had lifetime diagnoses ofabuse of or dependence on at least one illicit substance. Therate of drug dependence was 9.5%. This rate is similar tothat found for lifetime history of drug dependence amongmale participants in the National Comorbidity Survey(9.2%),10 supporting the generalizability of our findings tononveteran, nontwin males. Prevalences for abuse/depen-dence within individual drug classes ranged from 1.0%for heroin/opiates to 7.1% for marijuana (see Table 1). Forthe purposes of this series of studies on illicit drug use, anindividual was defined as having a drug use disorder ifhe met DSM-III-R criteria for abuse of or dependence onany of the five illicit drug categories assessed at any timeduring his life. We collapsed the categories of abuse and de-pendence because nearly all individuals who met the criteriafor abuse also exceeded the higher severity threshold for de-pendence.
Harvard Rev Psychiatry
November/December 2001268 Tsuang et al.

revealed that genetic factors contributed significantly tothe risk for lifetime drug abuse/dependence, accounting for34% of the variance. Significant shared environmental andunique environmental influences were also found, contribut-ing 28% and 38% of the variance, respectively. These esti-mates were similar to those from previous twin studies ofdrug abuse or dependence.12,13 Modeling of the risk for indi-vidual drug classes revealed significant genetic influencesfor marijuana (33%), heroin/opiates (43%), and stimulants(44%), and a significant shared environmental influence onmarijuana (29%). These results suggested that the probabil-ity of developing an illicit drug use disorder is substantiallyaffected by genes and by both shared and unique environ-mental factors. Although the relative influence of inheritedand environmental factors varied somewhat by drug type,the influence of genetic, shared environmental, and non-shared environmental factors on vulnerability to lifetime il-licit drug abuse/dependence (i.e., abuse of or dependence ondrugs in one or more categories) was approximately equal.
Does a Shared Vulnerability Underlie Risk for Abuse of/Dependence on Different Drug Classes?The findings described above led us to examine the extent towhich different classes of drugs are influenced by the samevulnerability factors. Are there specific vulnerabilities thatincrease the risk for abuse of one specific drug or class ofdrugs? Or, alternatively, is there a shared vulnerability fac-tor that cuts across drug classes, predisposing to abuse ofsubstances in general? Our examination of the co-occurrenceof abuse (i.e., DSM-III-R-defined abuse or dependence) of dif-ferent classes of drugs among VET Registry members14 sug-gested that both questions could be answered affirmatively.
Within-individual analyses (i.e., calculation of condi-tional probabilities, odds ratios, and tetrachoric correla-tions) clearly indicated that abuse of a drug in one class wasassociated with substantially increased risk for abusingdrugs from other classes. We therefore explored the mecha-nism(s) underlying this observed co-occurrence among thedrug classes by fitting a series of structural equation modelsto the data. Because the use of marijuana as a “gateway” tothe use of other illicit drugs appears to be increasingly im-portant (compared to nicotine and alcohol),15–17 we first ex-amined a model testing the theory that marijuana repre-sents an initial phase of illicit drug use that then facilitatesincreased involvement with “harder” drugs. The marijuanagateway model provided a poor fit to the data (�2 � 143.2;p � 0.000005). A single independent pathway model, whichassumes that co-occurrence across drug classes is explainedby the same genetic, shared environmental, and nonsharedenvironmental influences, but does not constrain these threefactors to influence each class in the same way, could not berejected (�2 � 79.4; p � 0.11). This model is less parsimoni-
Do Inherited and Environmental Factors Influence DrugAbuse and Dependence?Clinicians and researchers have long observed that abuse ofillegal drugs tends to run in families. In the first of a seriesof VET Registry studies on illegal substances, we11 aimed todistinguish between inherited and environmental factors asthe source of this observed family resemblance. One mea-sure of twin similarity is the pairwise concordance rate,which is the proportion of twin pairs with both members af-fected in a sample of pairs in which each pair has at least oneaffected member. Pairwise concordance rates for each of thefive drug classes were calculated separately for MZ (n �
1874) and DZ (n � 1498) pairs. MZ pairs were significantlymore likely to be concordant for DSM-III-R drug abuse/dependence diagnoses than were DZ pairs (26.2% versus16.5%, respectively; p � 0.01), suggesting a genetic influenceon drug use disorders. The tetrachoric correlation for each ofthe drug classes was also calculated. This statistic uses allavailable information about similarity within twin pairs,because pairs concordant for being unaffected are also in-cluded in its computation. The tetrachoric correlation forany drug use disorder was 0.63 in MZ twins and 0.44 in DZtwins.
Structural equation models can be fitted to correlationsto provide estimates of the proportions of phenotypic vari-ance due to additive genetic effects (heritability, or h2), com-mon or shared (“family”) environmental effects (c2), andunique or nonshared (“nonfamily”) environmental effects(e2). A �2 difference test is used to compare the fit of compet-ing models; if this difference is not significant, the modelwith the fewest parameters is selected on the basis of parsi-mony. As seen in Table 2, structural equation modeling
TABLE 1. Lifetime Prevalence of DSM-III-R Drug UseDisorders in the VET Registry*
Abuse† Dependence‡Illicit drug type (99% CI) (99% CI)
Any 0.6% (0.4–0.9) 9.5% (8.9–10.1)Marijuana 0.6% (0.4–0.9) 6.6% (6.0–7.2)Stimulants 0.2% (0.0–0.4) 4.2% (3.7–4.7)Sedatives 0.1% (0.0–0.2) 1.3% (1.0–1.6)Heroin/opiates 0.0% (0.0–0.1) 1.0% (0.7–1.3)PCP/psychedelics 0.1% (0.0–0.2) 1.0% (0.7–1.3)
CI, confidence interval; DSM-III-R, Diagnostic and StatisticalManual of Mental Disorders, 3rd edition (revised); PCP, phency-clidine.
*n � 3372 twin pairs.†Without dependence.‡Individuals who met criteria for dependence also met criteria
for abuse.
Harvard Rev Psychiatry
Volume 9, Number 6 Tsuang et al. 269
ous, however, than a common vulnerability model, which as-sumes that the co-occurrence across drug classes is deter-mined by a single common vulnerability (i.e., it constrainsgenetic, shared environmental, and unique environmentalinfluences to affect co-occurrence among the drug classes inthe same manner). The common vulnerability model alsoprovided a good fit to the data (�2 � 88.3; p � 0.11), so webased our remaining analyses on it because of its greaterparsimony. Parameter estimates were derived for the com-mon vulnerability itself (h2 � 0.31; c2 � 0.25; e2 � 0.44) andfor the individual drug classes, each of which can be influ-enced by specific genetic and environmental effects in addi-tion to the common vulnerability. Estimates derived there-fore included, for each drug class, total and specific geneticvariance, total and specific family environmental variance,and total and specific nonfamily environmental variance.
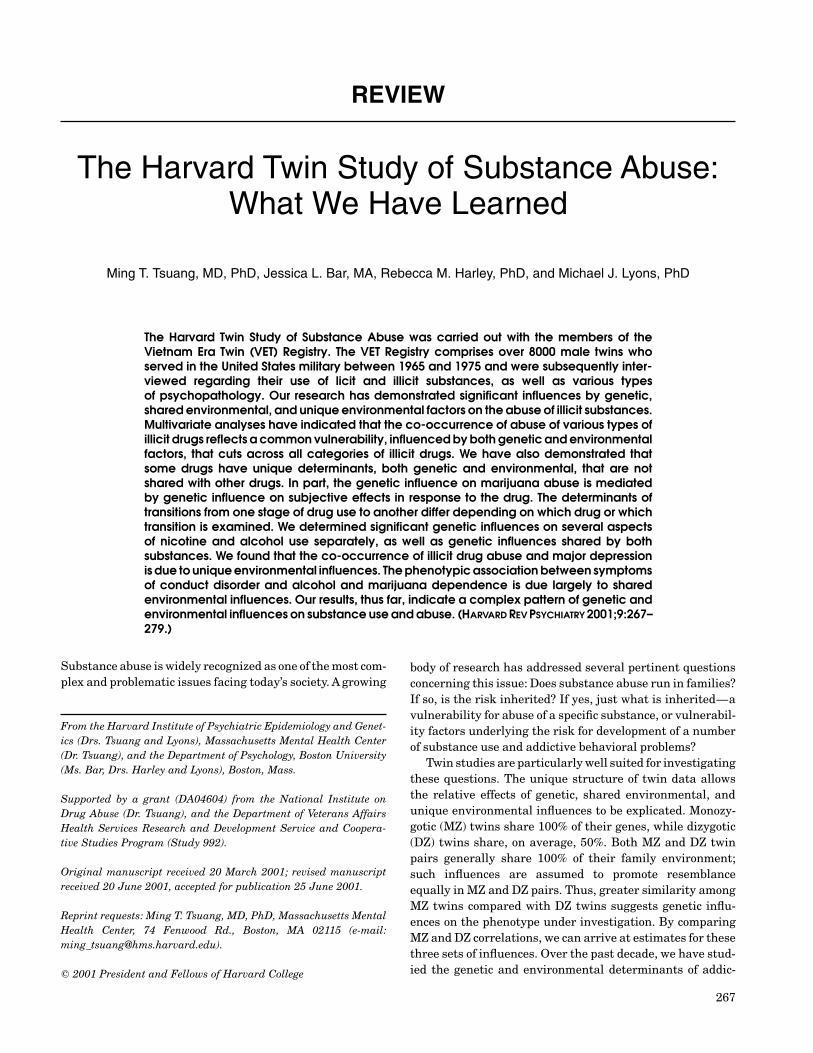
Figure 1 displays the relationship of the common vulner-ability to vulnerability for each illicit drug. The overlap ofthe circles representing the individual drugs with the ellipseindicates the amount of overall variance shared by each drugwith the common vulnerability. Overall shared variance wascalculated by subtracting the value for each specific varianceparameter from each total variance parameter and addingthe three values. For example, the figure indicates that 71%of the variance in the abuse of marijuana is shared with thecommon vulnerability (that is, shared genetic variance �
0.33–0.11; shared family environmental variance � 0.29–0.12; and shared nonfamily environmental variance � 0.38–0.06). In other words, 22% of the variance in marijuanaabuse is influenced by genes that also influence abuse ofother drugs, 11% of the variance is due to genetic factors thatonly influence marijuana abuse, 17% of the variance is dueto family environmental factors that also influence abuse ofother drugs, 12% of the variance is due to family environ-mental factors that only influence marijuana abuse, and so
on. The only drug that did not share at least 60% of its vari-ance with the common vulnerability was heroin (50%).
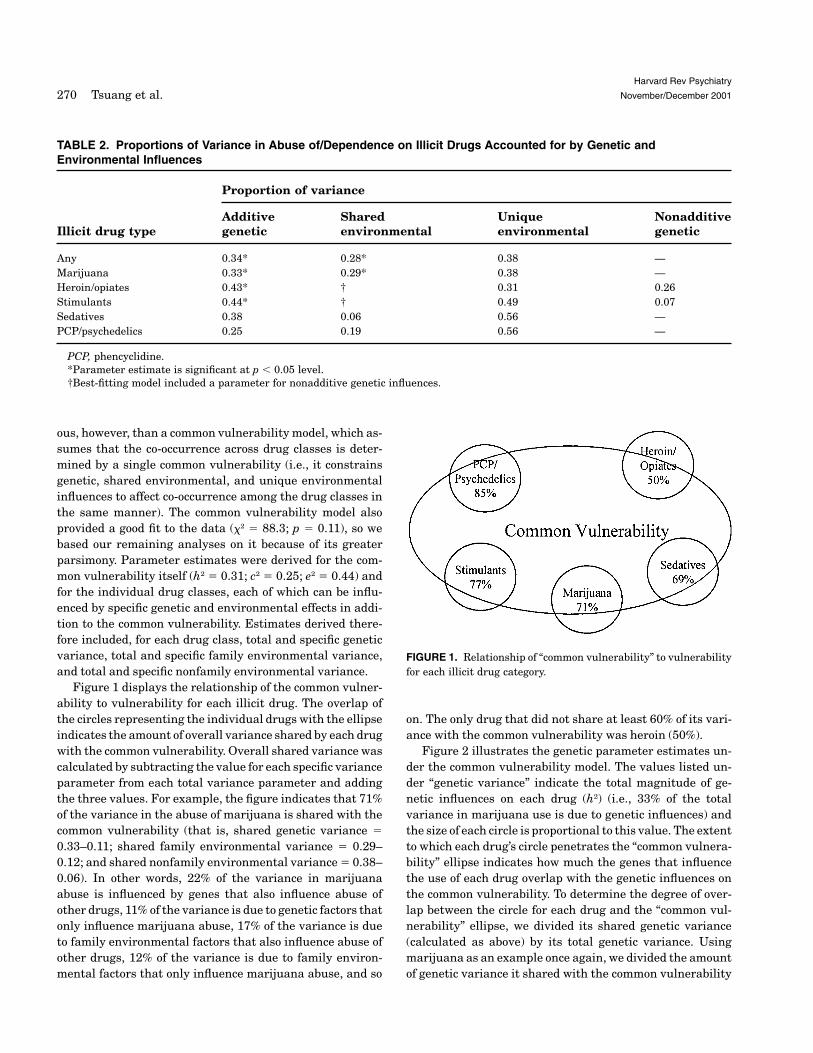
Figure 2 illustrates the genetic parameter estimates un-der the common vulnerability model. The values listed un-der “genetic variance” indicate the total magnitude of ge-netic influences on each drug (h2) (i.e., 33% of the totalvariance in marijuana use is due to genetic influences) andthe size of each circle is proportional to this value. The extentto which each drug’s circle penetrates the “common vulnera-bility” ellipse indicates how much the genes that influencethe use of each drug overlap with the genetic influences onthe common vulnerability. To determine the degree of over-lap between the circle for each drug and the “common vul-nerability” ellipse, we divided its shared genetic variance(calculated as above) by its total genetic variance. Usingmarijuana as an example once again, we divided the amountof genetic variance it shared with the common vulnerability
Harvard Rev Psychiatry
November/December 2001270 Tsuang et al.
TABLE 2. Proportions of Variance in Abuse of/Dependence on Illicit Drugs Accounted for by Genetic andEnvironmental Influences
Proportion of variance
Additive Shared Unique NonadditiveIllicit drug type genetic environmental environmental genetic
Any 0.34* 0.28* 0.38 —Marijuana 0.33* 0.29* 0.38 —Heroin/opiates 0.43* † 0.31 0.26Stimulants 0.44* † 0.49 0.07Sedatives 0.38 0.06 0.56 —PCP/psychedelics 0.25 0.19 0.56 —
PCP, phencyclidine.*Parameter estimate is significant at p � 0.05 level.†Best-fitting model included a parameter for nonadditive genetic influences.
FIGURE 1. Relationship of “common vulnerability” to vulnerabilityfor each illicit drug category.
aimed at risk reduction. However, a more complete aware-ness of the role(s) played by inherited factors may somedayallow implementation of more-aggressive interventions forthose with high genetic vulnerability.11 Toward this end, it isimportant to understand better how inherited factors influ-ence the use and abuse of substances. Demonstrating thatgenetic factors influence risk is only the first step—we thenneed to discover which genes impart risk and through whatmechanisms that risk operates.
One possible mechanism of action is that genetic influ-ences on personality may mediate risk-taking or sensation-seeking behaviors that bring a person into contact with illicitsubstances. Once an individual has been exposed to a drug-use situation, additional genetic influences on personalitydimensions such as openness to new experience, regulationof emotions, intolerance of boredom, or avoidance of harmmay play a role. Genetically influenced aspects of humanphysiology, such as metabolism and rates of absorption, alsomay affect vulnerability to drug use.A person’s physiologicalreactions to a substance determine, in part, the subjectiveeffect of that substance (i.e., whether ingestion of a drug isfollowed by pleasant or unpleasant physical sensations andfeelings). This subjective effect, in turn, is correlated withthe drug’s reinforcing effects, which presumably influencehow much the drug is used.18 Following this line of reason-ing, we hypothesized that positive subjective effects wouldbe associated with greater drug use in the VET Registrysample.19 If positive subjective effects are related to in-creased drug use, and if subjective effects are influenced by
(0.22) by its total genetic variance (0.33) and found that67% of its total genetic variance was shared with the com-mon vulnerability. Heroin abuse had the largest amount ofunique genetic variance (70%) and the smallest amount ofshared genetic variance (30%) of any of the categories. Incontrast, abuse of psychedelic drugs shared 100% of its ge-netic variance with the common vulnerability.
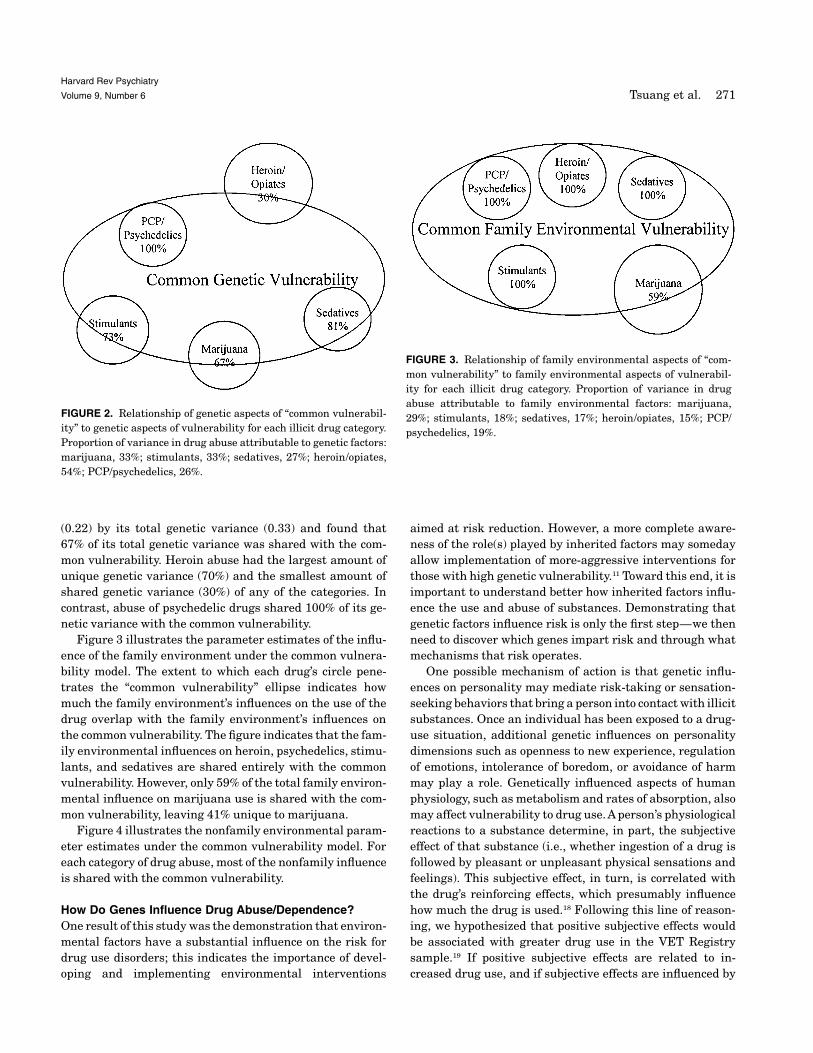
Figure 3 illustrates the parameter estimates of the influ-ence of the family environment under the common vulnera-bility model. The extent to which each drug’s circle pene-trates the “common vulnerability” ellipse indicates howmuch the family environment’s influences on the use of thedrug overlap with the family environment’s influences onthe common vulnerability. The figure indicates that the fam-ily environmental influences on heroin, psychedelics, stimu-lants, and sedatives are shared entirely with the commonvulnerability. However, only 59% of the total family environ-mental influence on marijuana use is shared with the com-mon vulnerability, leaving 41% unique to marijuana.
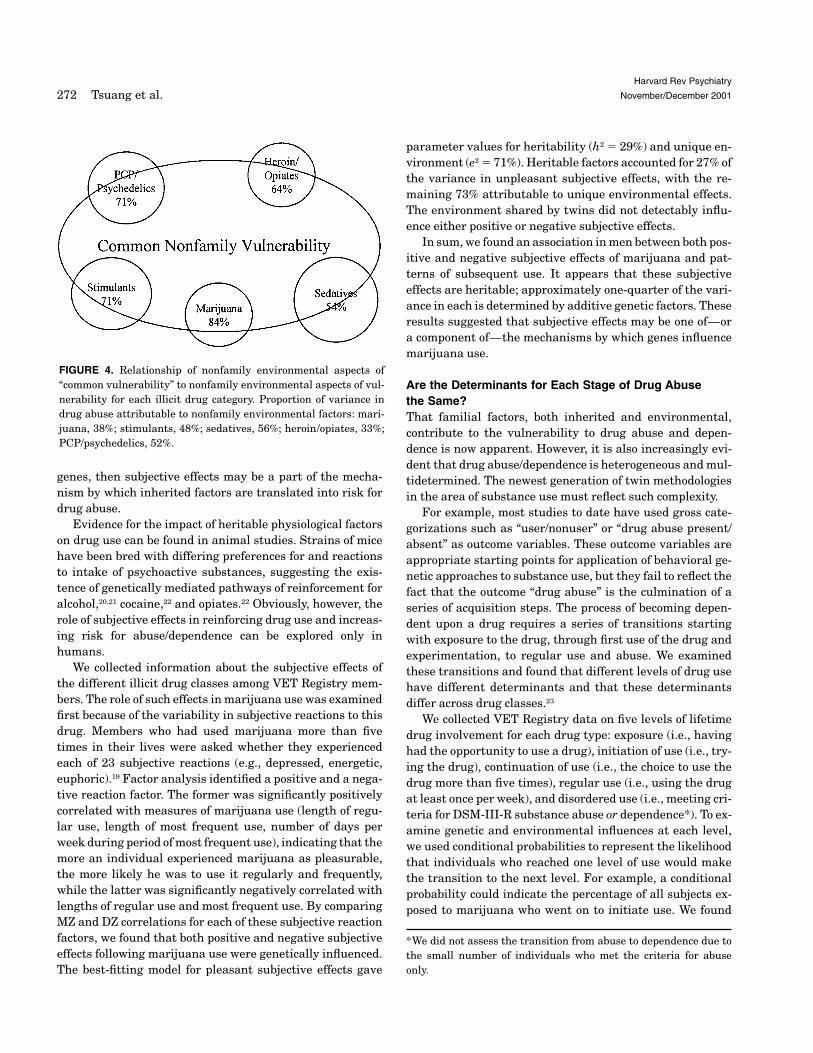
Figure 4 illustrates the nonfamily environmental param-eter estimates under the common vulnerability model. Foreach category of drug abuse, most of the nonfamily influenceis shared with the common vulnerability.
How Do Genes Influence Drug Abuse/Dependence?One result of this study was the demonstration that environ-mental factors have a substantial influence on the risk fordrug use disorders; this indicates the importance of devel-oping and implementing environmental interventions
Harvard Rev Psychiatry
Volume 9, Number 6 Tsuang et al. 271
FIGURE 2. Relationship of genetic aspects of “common vulnerabil-ity” to genetic aspects of vulnerability for each illicit drug category.Proportion of variance in drug abuse attributable to genetic factors:marijuana, 33%; stimulants, 33%; sedatives, 27%; heroin/opiates,54%; PCP/psychedelics, 26%.
FIGURE 3. Relationship of family environmental aspects of “com-mon vulnerability” to family environmental aspects of vulnerabil-ity for each illicit drug category. Proportion of variance in drugabuse attributable to family environmental factors: marijuana,29%; stimulants, 18%; sedatives, 17%; heroin/opiates, 15%; PCP/psychedelics, 19%.
genes, then subjective effects may be a part of the mecha-nism by which inherited factors are translated into risk fordrug abuse.
Evidence for the impact of heritable physiological factorson drug use can be found in animal studies. Strains of micehave been bred with differing preferences for and reactionsto intake of psychoactive substances, suggesting the exis-tence of genetically mediated pathways of reinforcement foralcohol,20,21 cocaine,22 and opiates.22 Obviously, however, therole of subjective effects in reinforcing drug use and increas-ing risk for abuse/dependence can be explored only inhumans.
We collected information about the subjective effects ofthe different illicit drug classes among VET Registry mem-bers. The role of such effects in marijuana use was examinedfirst because of the variability in subjective reactions to thisdrug. Members who had used marijuana more than fivetimes in their lives were asked whether they experiencedeach of 23 subjective reactions (e.g., depressed, energetic,euphoric).19 Factor analysis identified a positive and a nega-tive reaction factor. The former was significantly positivelycorrelated with measures of marijuana use (length of regu-lar use, length of most frequent use, number of days perweek during period of most frequent use), indicating that themore an individual experienced marijuana as pleasurable,the more likely he was to use it regularly and frequently,while the latter was significantly negatively correlated withlengths of regular use and most frequent use. By comparingMZ and DZ correlations for each of these subjective reactionfactors, we found that both positive and negative subjectiveeffects following marijuana use were genetically influenced.The best-fitting model for pleasant subjective effects gave
parameter values for heritability (h2 � 29%) and unique en-vironment (e2 � 71%). Heritable factors accounted for 27% ofthe variance in unpleasant subjective effects, with the re-maining 73% attributable to unique environmental effects.The environment shared by twins did not detectably influ-ence either positive or negative subjective effects.
In sum, we found an association in men between both pos-itive and negative subjective effects of marijuana and pat-terns of subsequent use. It appears that these subjectiveeffects are heritable; approximately one-quarter of the vari-ance in each is determined by additive genetic factors. Theseresults suggested that subjective effects may be one of—ora component of—the mechanisms by which genes influencemarijuana use.
Are the Determinants for Each Stage of Drug Abusethe Same?That familial factors, both inherited and environmental,contribute to the vulnerability to drug abuse and depen-dence is now apparent. However, it is also increasingly evi-dent that drug abuse/dependence is heterogeneous and mul-tidetermined. The newest generation of twin methodologiesin the area of substance use must reflect such complexity.
For example, most studies to date have used gross cate-gorizations such as “user/nonuser” or “drug abuse present/absent” as outcome variables. These outcome variables areappropriate starting points for application of behavioral ge-netic approaches to substance use, but they fail to reflect thefact that the outcome “drug abuse” is the culmination of aseries of acquisition steps. The process of becoming depen-dent upon a drug requires a series of transitions startingwith exposure to the drug, through first use of the drug andexperimentation, to regular use and abuse. We examinedthese transitions and found that different levels of drug usehave different determinants and that these determinantsdiffer across drug classes.23
We collected VET Registry data on five levels of lifetimedrug involvement for each drug type: exposure (i.e., havinghad the opportunity to use a drug), initiation of use (i.e., try-ing the drug), continuation of use (i.e., the choice to use thedrug more than five times), regular use (i.e., using the drugat least once per week), and disordered use (i.e., meeting cri-teria for DSM-III-R substance abuse or dependence*). To ex-amine genetic and environmental influences at each level,we used conditional probabilities to represent the likelihoodthat individuals who reached one level of use would makethe transition to the next level. For example, a conditionalprobability could indicate the percentage of all subjects ex-posed to marijuana who went on to initiate use. We found
*We did not assess the transition from abuse to dependence due tothe small number of individuals who met the criteria for abuseonly.
Harvard Rev Psychiatry
November/December 2001272 Tsuang et al.
FIGURE 4. Relationship of nonfamily environmental aspects of“common vulnerability” to nonfamily environmental aspects of vul-nerability for each illicit drug category. Proportion of variance indrug abuse attributable to nonfamily environmental factors: mari-juana, 38%; stimulants, 48%; sedatives, 56%; heroin/opiates, 33%;PCP/psychedelics, 52%.

ment. Investigations into the etiology of alcohol abuse/dependence are now focusing increasingly on exploring whatis inherited. Members of our group have approached this is-sue by examining genetic and environmental influences ondifferent facets of the disorders.
Do All Symptoms of Alcohol Abuse/Dependence Havethe Same Determinants?The extent to which there may be specific symptoms of al-cohol abuse/dependence that are more or less heritable isan important new area of inquiry. If a subset of symptomsstrongly influenced by genetic factors could be found, theywould represent a more heritable, homogeneous phenotype.Such a phenotype could then be studied via genetic linkageanalyses, and the likelihood of discovering the genes in-volved in imparting liability to alcohol abuse/dependencecould be increased. Unfortunately, attempts to examinethe role of genetic influences on individual symptoms of alco-hol abuse/dependence have generated inconsistent resultsto date.
Johnson and colleagues28 examined symptom concor-dances among MZ and DZ male twin pairs and identifiedseven alcohol symptoms that were more “genetic” and 14that were more “environmental “ (i.e., nongenetic) in theiretiology. We attempted to replicate these results using theVET Registry.29 Although our methodology was designed tobe comparable to that of Johnson and colleagues, we failedto replicate their findings. Our classification of symptom eti-ology as genetic or nongenetic was not significantly associ-ated with theirs, and this lack of correspondence did not ap-pear to be due to methodological differences or differencesin power between the two studies. Within our investigation,nine of the 23 symptoms included in DSM-III-R and DSM-IV criteria for alcohol dependence were consistently classi-fied as genetically influenced across random split-half sub-samples, and six of the 23 were classified as nongenetic intheir etiology. When model-fitting analyses were conductedto obtain heritability estimates for each alcohol symptom,considerable variation was seen in the genetic influences ondifferent symptoms, with estimates ranging from 0.03 to0.53 (mean � 0.34). However, confidence intervals aroundthese estimates were quite broad, ranging from 0.00 to 0.65and in most cases overlapping. Specific symptoms with highheritability that might represent a more heritable pheno-type could not be identified, given the limited evidence ofthese confidence intervals.
The failure to distinguish more from less heritable symp-toms of alcohol abuse/dependence may mean that it is notpossible to identify subtypes of alcohol use problems basedon symptoms that differ in their underlying genetic etiology.However, an alternative explanation might be that method-ological concerns prevented accurate identification of the
that marijuana had the highest conditional probability of allthe illicit drug classes for a number of transitions, indicatingthat most people who had the opportunity to try marijuanadid so (conditional probability of making transition from ex-posure to initiation of use � 0.57). Most who tried marijuanaonce continued to use it (0.64), and most of these became reg-ular users (0.70). However, only one-third of regular userswent on to meet criteria for abuse/dependence for mari-juana. In contrast, the majority of individuals who reachedthe transition for regular use of cocaine did make the finaltransition to abuse/dependence (0.56). Transition rates toregular use of heroin were also quite high (0.67), and thetransition from regular heroin use to abuse/dependence wasthe second highest after cocaine (0.42).
Comparison of tetrachoric correlations for MZ versus DZtwins and subsequent univariate biometric modeling re-vealed significant genetic effects on transitions from expo-sure to initiation of use (h2 � 0.44) and from initiating use tocontinuing use (h2 � 0.53) of marijuana. We also found sig-nificant heritabilities for transitions from exposure to initia-tion of use of amphetamine (h2 � 0.61) and cocaine (h2 �
0.54).These results suggest that the determinants of stages of
illicit drug use vary by stage and by drug type and that ge-netic factors are more influential at certain transition pointsin the use of each drug class than at other transition points.Just as the final outcome of DSM-diagnosed substanceabuse/dependence is clearly multidetermined, each transi-tion to greater drug involvement is likely multideterminedtoo. For example, whether an individual continues to use adrug after having tried it may be influenced by his or herpeer group, capacity to cope with stress, and expectationsconcerning the drug, by drug availability, and by the subjec-tive effects the particular drug has on that particular indi-vidual, to name just a few possible mechanisms. Each ofthese mechanisms may have a distinct combination of ge-netic and/or environmental determinants. As our under-standing of the complexity of drug use and abuse matures,we will need to identify the determinants of key transitionpoints. Detailed knowledge of these determinants can facili-tate interventions tailored to target influential factors ateach stage of involvement with illicit drugs.
ALCOHOL
Genetic contributions to alcohol abuse and dependence havebeen observed in a number of twin samples.24–26 Consistentwith estimates from other studies, our data27 suggested thatapproximately 55% of the variance in risk for alcohol depen-dence is genetically mediated and that the remainder of thevariance in liability is explained by unique environmentalfactors, with no detectable influence from family environ-
Harvard Rev Psychiatry
Volume 9, Number 6 Tsuang et al. 273

true heritability of each symptom. We chose to use Johnsonand colleagues’ method28 in an attempt to replicate their re-sults; this method has several disadvantages that may havelimited the findings of both studies. For example, the classi-fication of some symptoms as genetic and others as nonge-netic may be strongly influenced by differences in reliabilityand statistical power of different symptoms rather than bytrue differences in heritability. In the future, using clustersof conceptually related symptoms rather than individualitems as the unit of analysis may prove more successful. Ourresults suggest that important variations in the relativemagnitude of genetic influences on different symptoms ofalcohol abuse/dependence may exist, but that to demon-strate such variations, researchers must strive to maximizeprecision of heritability estimates, statistical power, andreplicability.
What Are the Determinants of Seeking Treatment forAlcohol Use Problems?We have also examined the question of what is inherited inthe context of health services research, targeting the likeli-hood of seeking treatment rather than familial risk for de-veloping an alcohol use problem. In a study that appears tobe the first to apply behavioral genetic analysis to this issue,we27 used the VET Registry to investigate whether seekingtreatment for alcohol dependence is influenced by geneticand/or environmental factors. Members who satisfied DSM-III-R lifetime criteria for alcohol dependence were askedwhether they had ever told a doctor about a problem theyhad with drinking, or whether they had ever had any treat-ment for drinking.
Genetic and environmental contributions to the decisionto seek treatment were assessed under competing multifac-torial threshold models. Such models assume multiple un-measured genetic and environmental risk factors that de-termine an underlying liability for development of a trait.Above a given threshold, the trait is expressed; below it, thetrait does not develop. A combined liability dimension (CLD)model offered the best fit to the data. This model includestwo independent dimensions that each influence liability;hence, some of the genetic variance for seeking treatmentwas associated with severity of alcohol symptoms (severitydimension), and some was unrelated to the determinantsof alcohol dependence (treatment utilization dimension).Forty-one percent of the variance in seeking treatment wasattributed to additive genetic effects, and 40% was attrib-uted to shared environment, leaving only 19% accounted forby unique environmental effects. These results indicate thatfamilial influences contribute substantially to decisions toseek treatment for alcohol use problems and that these in-fluences are not completely accounted for by severity of alco-hol symptoms.
Although our study demonstrated the potential of a ge-netic approach to seeking treatment, conclusions were lim-ited by the dearth of information on treatment utilizationavailable at the time. We have subsequently collected more-detailed data on alcohol-related health services use and de-terminants of treatment-seeking behavior in a subset ofVET Registry members in the hope that they will furtherilluminate treatment-seeking behavior for alcohol useproblems.
What Is the Relationship between Alcohol Use Problemsand Health-Related Quality of Life?Whether an individual with an alcohol use problem is suc-cessfully treated or continues to drink heavily, his or herhealth-related quality of life (HRQL), the perception ofhealth and its relation to daily functioning, is often nega-tively affected at some point. Alcohol-related medical ill-nesses,30 social impairment,31 and deficits in emotional func-tioning31 can have long-lasting effects on the quality of lifeof current and former problem drinkers. We32 examined therelationship between HRQL and alcohol dependence in theVET Registry using the Medical Outcomes Study 36 ItemShort Form (SF-36), a self-report scale measuring eighthealth dimensions, before and after adjustment for covari-ates. Covariates included zygosity, lifetime physical and psy-chiatric disorders, lifetime drug and nicotine dependence,current marital status, current income, and severity of alco-hol dependence. Prior to adjustment, six of eight SF-36scales were lower for alcohol-dependent twins in remission(defined as having no alcohol symptoms in the previous 5years) than for their never-alcohol-dependent co-twins.Scores on all eight SF-36 scales were lower for recentlyalcohol-dependent twins (defined as having at least onealcohol symptom in the previous 5 years) than for theirnever-alcohol-dependent co-twins. However, after we con-trolled for all covariates, neither current nor remitted alco-hol dependence had a direct impact on HRQL.
These results suggested that alcohol dependence has nodirect impact on HRQL but exerts its effect through mediat-ing factors. The two factors with the strongest influence onHRQL in alcohol-dependent twins appeared to be zygosityand current marital status. Adjustment for zygosity reduceddifferences between alcohol-dependent twins and their non-alcohol-dependent co-twins on all SF-36 subscales (in mostcases to a nonsignificant level), suggesting that genes havesome influence on the relationship between alcohol depen-dence and perceived HRQL. (We did not attempt to quantifysuch influence in this study.) Particularly among recentlyalcohol-dependent twins, being married was associated withbetter SF-36 scores; none of the within-pair subscale differ-ences was significant following additional adjustment formarital status after adjustment for zygosity. Further re-
Harvard Rev Psychiatry
November/December 2001274 Tsuang et al.

netic and environmental contributions to both risk of initia-tion and risk of persistence of smoking. An individual whobegins to smoke may quit because of a low genetic liabilityat either of these two stages. Low liability at initiation, dueto a genetic predisposition to the unpleasant subjective ef-fects of nicotine, for example, might lead a person to quitsmoking after trying cigarettes a few times. In contrast,low liability on the persistence dimension might endow anindividual with low genetic vulnerability to nicotine depen-dence. This low level of dependence vulnerability might en-able a person to quit smoking successfully after years of reg-ular cigarette use.
Our model-fitting analysis demonstrated that both ge-netic and environmental factors influence initiation of regu-lar cigarette use. Approximately 50% of the variance in riskof becoming a regular smoker (“initiation”) was accountedfor by genetic liability, while 30% of the variance was attrib-uted to shared environmental influences. These estimatesare in agreement with previous twin studies of smoking ini-tiation.35,38,40 The heritability estimate of 70% for smokingpersistence was much higher than that for initiation. In fact,this genetic effect was more powerful than those we ob-served for vulnerability to alcohol or illicit substance abuse/dependence among members of the VET Registry. No evi-dence for a shared environmental influence on smoking per-sistence was found; the remaining 30% of the variance inrisk for persistent smoking was attributable to unique envi-ronmental factors.
These results suggest that once smoking has begun, itmay be maintained through predominantly genetic factors.The nature of these genetic factors remains unknown, al-though a genetically mediated susceptibility to nicotine de-pendence is probably involved. (We did not assess DSM-defined nicotine dependence in this study.) Animal modelssuggest a genetic influence on nicotine dependence,41 andmethods for studying individual differences in nicotine sen-sitivity are available.42,43 In light of the significant healthcosts of long-term smoking, our results emphasize the im-portance of continued research into the biological bases ofgenetic effects on smoking. If the mechanisms underlyingthe genetic contribution to the difficulty of quitting smokingcould be explicated, interventions could be developed to tar-get vulnerable individuals, and existing cessation aids couldbe improved.
Does a Shared Vulnerability Underlie Risk for Alcoholand Nicotine Dependence?Smoking is extremely common among alcohol-dependent in-dividuals seeking treatment44 and among alcohol-abusingindividuals identified in a general medical setting.45 Com-bined use of these substances can have a synergistic effect,increasing risk for certain health problems,46,47 thus making
search must confirm and extend these findings, but theypoint to contributions from both inherited factors and envi-ronmental factors such as social support in the relationshipamong alcohol use problems, perceived health, and qualityof life.
NICOTINE
With the genetic contribution to risk for alcohol and illicitdrug use disorders well established, studies of these sub-stances have gone on to explore mediators of genetic influ-ence.33 In contrast, our understanding of the etiology ofsmoking behavior and the genetic underpinnings of nicotineuse and dependence is less developed. After reviewing theliterature, we noted in 199733 that a number of twin stud-ies34,35 had reported family environmental and genetic in-fluences on initiation of cigarette smoking, but that findingsof familial influences on persistence (i.e., risk that those whoinitiate regular use will become long-term smokers) wereless consistent, perhaps due to cohort or cultural effects. Forexample, one study of twins in the United Kingdom36 hadfailed to find genetic influences on persistence, while othersusing twin samples from Australia, Sweden, and Finland37,38
had shown genetic influences on persistence that were inde-pendent of influences on smoking initiation.
Given the magnitude of the public health problemscaused by long-term smoking,39 it is important to continue toinvestigate the etiology of smoking behavior until the deter-minants of initiation and persistence are consistently repli-cated. Additional insight into why some regular smokers areable to quit while others fail to do so despite repeated at-tempts could lead to improvement in psychoeducation andcessation aids for persistent smokers. Toward this end, we33
examined the determinants of initiation and persistence ofsmoking behavior among VET Registry members.
Do Inherited and Environmental Factors InfluenceSmoking?For the purposes of our study, VET Registry members whoresponded positively to the questions “Have you smoked atleast 100 cigarettes in your life?” and “Do you smoke now?”were classified as current smokers. Individuals who re-sponded positively to the first question but negatively to thesecond were classified as ex-smokers. Individuals who re-ported never having smoked more than 100 cigarettes wereclassified as nonsmokers.
The percentage of VET Registry twins discordant forsmoking status was consistently higher among DZ thanamong MZ twin pairs, suggesting some genetic influence onsmoking behavior. When this influence was quantified usingmodel-fitting, a two-process CLD model provided the best fit(�2 � 21.2; p � 0.21). This model allows for estimation of ge-
Harvard Rev Psychiatry
Volume 9, Number 6 Tsuang et al. 275

heavy consumption of both nicotine and alcohol a crucialpublic health issue.48
Given the frequent co-occurrence of alcohol and tobaccouse and the genetic contributions that have been establishedthrough twin studies of alcohol and smoking independently,we wondered whether common genetic influences contributeto the mechanism underlying the close relationship betweenthe two substances. The two previous studies49,50 to investi-gate this question produced conflicting results. Prescott andKendler49 found very small genetic influences and modestfamily environmental influences common to alcohol and nic-otine dependence in female twins. In contrast, Swan and col-leagues50 found a genetic correlation of 0.47 between nico-tine and alcohol use among male twins. These disparatereports led us to investigate factors common to nicotine andalcohol dependence among VET Registry twins.48 Using bi-variate model-fitting, we found a substantial genetic correla-tion between DSM-III-R-defined alcohol and nicotine depen-dence (r � 0.68; 95% CI � 0.61–0.74), a modest uniqueenvironmental correlation (r � 0.23; 95% CI � 0.14–0.32),and no shared familial influences. From this model, we com-puted the amount of genetic variance that is common to riskfor both types of substance dependence. We found that 25.5%of the total variance in risk for alcohol dependence is sharedwith genetic influences on nicotine dependence and that2.4% of the risk for alcohol dependence overlaps with uniqueenvironmental influences on nicotine dependence.
These findings suggest that the phenotypic relationshipbetween alcohol and nicotine dependence in men is partiallydue to a common genetic liability shared by the two depen-dencies. Thus, for some nicotine- and alcohol-dependentmales, the co-occurrence of heavy smoking and drinking isnot coincidental but is instead the manifestation of a largerrisk for dual addiction.48 Future research is needed to iden-tify the biological mechanism(s) by which this shared riskbecomes manifest.
CO-OCCURRING PSYCHOPATHOLOGY
We observed that a portion of the underlying vulnerabilityfor abuse of illicit substances is common to all drug classes14
and that a portion of the vulnerability for alcohol and nico-tine dependence can be attributed to shared genetic influ-ences.48 Additional results from the VET Registry suggest,similarly, that substance abuse/dependence and other formsof psychopathology also share a common vulnerability.
Does a Shared Vulnerability Influence Risk for MajorDepression and Substance Abuse/Dependence?Major depression (MD) and substance use disorders occurtogether frequently.51 Studies have documented phenotypicassociations between MD and abuse of or dependence onalcohol,52,53 marijuana,54 cocaine,55 and other illicit sub-
stances.56,57 Using a co-twin control design, we set out to in-vestigate whether comorbidity between DSM-III-R-definedMD and substance abuse/dependence could be partially ex-plained by the same familial factors.51 In this design, onemember of each of the 1874 MZ twin pairs in our sample wasrandomly selected as the “index” twin. The co-twin of eachindex twin served to control for inherited and family envi-ronmental influences on MD and substance use disorders.
Examination of index twin data revealed that prevalenceof cannabis, amphetamine, cocaine, and sedative abuse ordependence was significantly higher among twins who hada lifetime diagnosis of MD than among those without MD.This discrepancy remained after adjustment for educationlevel, income, and Vietnam combat experience. Index twinswith a diagnosis of MD demonstrated a prevalence of canna-bis abuse/dependence 4.4 times as high, a prevalence of am-phetamine abuse/dependence 2.8 times as high, a preva-lence of cocaine abuse/dependence 1.8 times as high, and aprevalence of sedative abuse/dependence 4.5 times as highas was found among index twins without MD. We then con-trolled for the contribution of genetic factors and sharedenvironmental experiences by using conditional logistic re-gression on the subset of 234 MZ twin pairs discordant forMD. Lifetime diagnoses of abuse of/dependence on mari-juana, amphetamine, and sedatives remained significantlygreater among twins with MD than among their co-twinswithout MD (OR � 2.3, 5.8, and 10.9, respectively). Cocainewas not significantly associated with MD after we controlledfor genetic and shared environmental factors, but this wasprobably due to low statistical power (OR � 2.6; 95% CI �
0.9–7.6).That the prevalence of illicit drug abuse remained higher
in twins with MD than in their co-twins without MD, de-spite controlling for familial influences, suggests that theco-occurrence of MD and abuse of/dependence on illicit drugsis attributable to environmental influences unique to eachtwin. The negative legal, financial, and relational conse-quences associated with illicit substance use are significantlife stressors that may increase the risk of a major depres-sive episode in individuals with a genetic predisposition tothe disorder.51
Is There a Familial Relationship among ConductDisorder and Alcohol and Marijuana Dependence?Conduct disorder (CD) is another form of psychopathologythat often occurs together with substance use disorders.This is particularly true for alcohol and marijuana, two sub-stances that are often among the first to be abused by adoles-cents.58 We knew of no reports of familial factors common toall three phenotypes and therefore conducted a study to in-vestigate whether familial contributions to CD also increaserisk for abuse of alcohol and marijuana.59 If so, a better char-acterization of these familial associations could contribute
Harvard Rev Psychiatry
November/December 2001276 Tsuang et al.

fluences shared by members of a twin pair that are commonto all three sets of symptoms. Deviant parental behavior anda pathological home environment are the most widely stud-ied shared environmental influences on CD.63,64 These maycontribute to the development of CD, which may in turn fos-ter exposure to and abuse of alcohol and marijuana.58 If so,then family- and community-based efforts aimed at reducingexposure to environmental factors that increase risk for CDmay simultaneously reduce risk for the development of alco-hol and marijuana abuse/dependence.
CONCLUSIONS
The results that have emerged so far from the VET Registrydata indicate that genetic and environmental factors havepowerful and complicated effects on the use and abuse of il-licit drugs, alcohol, and nicotine and on related behaviors.We have demonstrated the substantial influence of environ-mental factors, aspects of the environment shared by themembers of a twin pair as well as aspects unique to eachmember, and the general importance of genetic influences onthe risk for substance abuse and dependence. With contin-ued progress in the refinement of molecular genetic technol-ogies, it may soon be possible to identify specific alleles thatconfer risk for or protection against various aspects of druguse. Following our multivariate analysis of illicit drugabuse, we concluded that heroin was the most promising in-dividual illicit drug for linkage research because it had themost-substantial heritability and the least overlap of its ge-netic vulnerability with “generic” genetic vulnerability forabuse of all illicit drugs. Therefore, we have recently beguna sib-pair design linkage study of heroin addiction in whatwe believe is the next step in the journey to understand howgenes influence substance abuse.
We wish to acknowledge numerous individuals for their helpwith this project. Department of Veterans Affairs: 1) Midwest Cen-ter for Health Services and Policy Research: VET Registry Director,William G. Henderson, PhD; Epidemiologist, Jack Goldberg, PhD;Registry Programmer, Kenneth Bukowski; Coordinator, Mary EllenVitek; Statistical Assistant, Rita Havlicek. 2) VET Registry Advi-sory Committee: Emil Coccaro, MD, PhD; Theodore Colton, ScD;Walter E. Nance, MD, PhD; Ralph S. Paffenbarger, Jr., MD, DrPH;and Roger R. Williams, MD (past). 3) VA Headquarters: Chief Re-search and Development Officer, John R. Feussner, MD; Staff Assis-tant, Ping Huang, PhD. The main collaborators on the research de-scribed in this paper were Drs. Seth Eisen, William True, JackGoldberg, Hong Xian, Lindon Eaves, and Joanne Meyer. We also ac-knowledge Drs. Irving Gottesman of University of Virginia and JagKhalsa of NIDA, whose contributions helped us to complete thisproject successfully. Most important, we wish to thank the membersof the Vietnam Era Twin Registry for their participation and cooper-ation. They willingly provided sensitive information and consider-able time in responding to the survey. Without their contribution,this research project would not have been possible.
to improved prevention and treatment for individuals at riskfor the co-occurrence of CD and substance abuse. We em-ployed broad definitions of these disorders because using fullDSM-III-R criteria would have yielded a prevalence of co-occurring CD and substance abuse too low to provide the sta-tistical power to resolve whether the familial contributionsto CD and substance abuse were genetic, environmental, orboth.
The prevalence of subjects reporting three or more life-time symptoms of CD, alcohol dependence, or marijuana de-pendence was 7.9%, 38.3%, and 6.7%, respectively. AmongVET Registry members with three or more lifetime symp-toms of CD, 64.8% also had three or more lifetime symptomsof alcohol dependence, and 17.8% had three or more lifetimesymptoms of marijuana dependence. Of VET Registry re-spondents without a history of CD symptoms, 34.8% hadthree or more alcohol dependence symptoms and 6.7% hadthree or more marijuana dependence symptoms. We used atrivariate Cholesky model60 to estimate the genetic and envi-ronmental correlations between CD and alcohol and mari-juana dependence symptoms. This method allowed us to es-timate genetic, shared, and unique environmental variancesfor each set of symptoms, as well as correlations between ge-netic and environmental effects for each pair of phenotypes.
The best-fitting, most parsimonious model (�2 � 13.51;p � 0.92) assumed no genetic contribution common to symp-toms of all three disorders. Instead, genetic influencesshared by alcohol dependence symptoms (accounting for44.7% of their total variance) and marijuana dependencesymptoms (7.6%), but not CD, were found. The model alsoincluded a specific genetic influence on marijuana depen-dence symptoms (36.3%). The model did allow for shared en-vironmental determinants common to all three phenotypes,explaining 46.7%, 11.9%, and 21.3% of the variance in riskfor symptoms of CD, alcohol dependence, and marijuana de-pendence, respectively. Unique environmental contributionswere common to risk for CD (53.3%) and alcohol dependencesymptoms (2.3%), and for alcohol (41.2%) and marijuana(5.4%) dependence symptoms, but no unique environmen-tal factors overlapped risk for all three sets of symptoms.A unique environmental influence specific to marijuana(30.4%) was also included in the model. Our best-fittingmodel did not allow for a genetic influence on comorbid CDsymptoms. This result fits with a previous examination ofjuvenile antisocial traits among VET Registry members61
that found them to be largely explained by environmentalfactors, with a small (7%) additive genetic contribution.However, results using VET Registry members are not con-sistent with all twin studies of CD,62 and the role of genes inthe risk for CD remains uncertain.
We concluded from these findings that the phenotypic as-sociation among symptoms of CD, alcohol dependence, andmarijuana dependence is largely due to environmental in-
Harvard Rev Psychiatry
Volume 9, Number 6 Tsuang et al. 277

REFERENCES
1. Eisen S, True W, Goldberg J, Henderson W, Robinette CD. TheVietnam Era Twin (VET) Registry: method of construction.Acta Genet Med Gemellol (Roma) 1987;36:61–6.
2. Henderson WG, Eisen S, Goldberg J, True WR, Barnes JE,Vitek ME. The Vietnam Era Twin Registry: a resource formedical research. Public Health Rep 1990;105:368–73.
3. Eisen S, Neuman R, Goldberg J, Rice J, True W. Determiningzygosity in the Vietnam Era Twin Registry: an approach usingquestionnaires. Clin Genet 1989;35:423–32.
4. Goldberg J, True W, Eisen S, Henderson W, Robinette CD. TheVietnam Era Twin (VET) Registry: ascertainment bias. ActaGenet Med Gemellol (Roma) 1987;36:67–78.
5. Robins L, Helzer J, Cottler L, Goldring E. NIMH DiagnosticInterview Schedule Version III Revised (DIS-III-R). St. Louis,Missouri: Department of Psychiatry, Washington UniversityMedical School, 1989.
6. Gfroerer JC, Hughes AL. The feasibility of collecting drugabuse data by telephone. Public Health Rep 1991;106:384–93.
7. Rohde P, Lewinsohn PM, Seeley JR. Comparability of tele-phone and face-to-face interviews in assessing Axis I and IIdisorders. Am J Psychiatry 1997;154:1593–8.
8. Sobin C, Weissman MM, Goldstein RB, Adams P, Wickrama-ratne P, Warner V, et al. Diagnostic interviewing for familystudies: comparing telephone and face-to-face methods for thediagnosis of lifetime psychiatric disorders. Psychiatr Genet1993;3:227–33.
9. American Psychiatric Association. Diagnostic and statisticalmanual of mental disorders. 3rd ed, revised. Washington, DC:American Psychiatric Association, 1987.
10. Warner LA, Kessler RC, Hughes M, Anthony JC, Nelson CB.Prevalence and correlates of drug use and dependence in theUnited States: results from the National Comorbidity Survey.Arch Gen Psychiatry 1995;52:219–29.
11. Tsuang MT, Lyons MJ, Eisen SA, Goldberg J, True W, Lin N,et al. Genetic influences on DSM-III-R drug abuse and depen-dence: a study of 3,372 twin pairs. Am J Med Genet 1996;67:473–7.
12. Grove WM, Eckert ED, Heston L, Bouchard TJ Jr, Segal N,Lykken DT. Heritability of substance abuse and antisocial be-havior: a study of monozygotic twins reared apart. Biol Psychi-atry 1990;27:1293–304.
13. Pickens RW, Svikis DS, McGue M, Lykken DT, Heston LL,Clayton PJ. Heterogeneity in the inheritance of alcoholism: astudy of male and female twins. Arch Gen Psychiatry 1991;48:19–28.
14. Tsuang MT, Lyons MJ, Meyer JM, Doyle T, Eisen SA, Gold-berg J, et al. Co-occurrence of abuse of different drugs in men:the role of drug-specific and shared vulnerabilities. Arch GenPsychiatry 1998;55:967–72.
15. Golub A, Johnson BD. The shifting importance of alcohol andmarijuana as gateway substances among serious drug abus-ers. J Stud Alcohol 1994;55:607–14.
16. Kandel DB, Yamaguchi K, Chen K. Stages of progressionin drug involvement from adolescence to adulthood: further
evidence for the gateway theory. J Stud Alcohol 1992;53:447–57.
17. Yamaguchi K, Kandel DB. Patterns of drug use from adoles-cence to young adulthood, III: Predictors of progression. Am JPublic Health 1984;74:673–81.
18. DeWit H, Johanson CD. A drug preference procedure for usewith human volunteers. In: Bozarth MA, ed. Methods of as-sessing the reinforcing properties of abused drugs. New York:Springer, 1987:559–72.
19. Lyons MJ, Toomey R, Meyer JM, Green AI, Eisen SA, Gold-berg J, et al. How do genes influence marijuana use? The roleof subjective effects. Addiction 1997;92:409–17.
20. Ball DM, Murray RM. Genetics of alcohol misuse. Br MedBull 1994;50:18–35.
21. McClearn GE, Anderson SM. Genetics and ethanol tolerance.Drug Alcohol Depend 1979;4:61–76.
22. George FR. Genetic models in the study of alcoholism and sub-stance abuse mechanisms. Prog Neuropsychopharmacol BiolPsychiatry 1993;17:345–61.
23. Tsuang MT, Lyons MJ, Harley RM, Xian H, Eisen S, GoldbergJ, et al. Genetic and environmental influences on transitionsin drug use. Behav Genet 1999;29:473–9.
24. Heath AC, Bucholz KK, Madden PAF, Dinwiddie SH, SlutskeWS, et al. Genetic and environmental contributions to alcoholdependence risk in a national twin sample: consistency offindings in women and men. Psychol Med 1997;27:1381–96.
25. McGue M. Genes, environment and the etiology of alcohol-ism. In: Zucker R, Boyd G, Howard J, eds. The developmentof alcohol problems: exploring the biopsychosocial matrix ofrisk. Rockville, Maryland: National Institutes of Health, 1994:1–40.
26. McGue M. Phenotyping alcoholism [Letter]. Alcohol Clin ExpRes 1999;23:757–8.
27. True WR, Heath AC, Bucholz K, Slutske W, Romeis JC, Scher-rer JF, et al. Models of treatment seeking for alcoholism: therole of genes and environment. Alcohol Clin Exp Res 1996;20:1577–81.
28. Johnson EO, Van den Bree MBM, Pickens RW. Indicators ofgenetic and environmental influence in alcohol-dependent in-dividuals. Alcohol Clin Exp Res 1996;20:67–74.
29. Slutske WS, True WR, Scherrer JF, Heath AC, Bucholz KK,Eisen SA, et al. The heritability of alcoholism symptoms: “in-dicators of genetic and environmental influence in alcohol-dependent individuals” revisited. Alcohol Clin Exp Res 1999;23:759–69.
30. Leevy CB, Leevy CM. Alcoholic liver disease. Compr Ther1994;20:6–9.
31. Moos RH, Moos BS. The process of recovery from alcoholism,III: Comparing functioning in families of alcoholics andmatched control families. J Stud Alcohol 1984;45:111–8.
32. Romeis JC, Waterman B, Scherrer JF, Goldberg J, Eisen SA,Heath AC, et al. The impact of sociodemographics, comorbidityand symptom recency on health-related quality of life in alco-holics. J Stud Alcohol 1999;60:653–62.
33. True WR, Heath AC, Scherrer JF, Waterman B, Goldberg J,Lin N, et al. Genetic and environmental contributions tosmoking. Addiction 1997;92:1277–87.
Harvard Rev Psychiatry
November/December 2001278 Tsuang et al.
bacco, alcohol, and coffee in Caucasian male twins: a multivar-iate analysis. J Subst Abuse 1996;8:19–31.
51. Lin N, Eisen SA, Scherrer JF, Goldberg J, True WR, LyonsMJ, et al. The influence of familial and non-familial factorson the association between major depression and substanceabuse/dependence in 1874 monozygotic male twin pairs. DrugAlcohol Depend 1996;43:49–55.
52. Kendler KS, Heath AC, Neale MC, Kessler RC, Eaves LJ. Al-coholism and major depression in women: a twin study of thecauses of comorbidity. Arch Gen Psychiatry 1993;50:690–8.
53. Maier W, Lichtermann D, Minges J. The relationship betweenalcoholism and unipolar depression—a controlled familystudy. J Psychiatr Res 1994;28:303–17.
54. Regier DA, Farmer ME, Rae DS, Locke BZ, Keith SJ, JuddLL, et al. Comorbidity of mental disorders with alcohol andother drug abuse: results from the Epidemiologic CatchmentArea (ECA) study. JAMA 1990;264:2511–8.
55. Kleinman PH, Miller AB, Millman RB, Woody GE, Todd T,Kemp J, et al. Psychopathology among cocaine abusers enter-ing treatment. J Nerv Ment Dis 1990;178:442–7.
56. Buckner JC, Mandell W. Risk factors for depressive symptom-atology in a drug using population. Am J Public Health 1990;80:580–5.
57. Rounsaville BJ, Kosten TR, Weissman MM, Prusoff B, PaulsD, Anton SF, et al. Psychiatric disorders in relatives of pro-bands with opiate addiction. Arch Gen Psychiatry 1991;48:33–42.
58. Young SE, Mikulich SK, Goodwin MB, Hardy J, Martin CL,Zoccolillo MS, et al. Treated delinquent boys’ substance use:onset, pattern, relationship to conduct and mood disorders.Drug Alcohol Depend 1995;37:149–62.
59. True WR, Heath AC, Scherrer JF, Xian H, Lin N, Eisen SA, etal. Interrelationship of genetic and environmental influenceson conduct disorder and alcohol and marijuana dependencesymptoms. Am J Med Genet 1999;88:391–7.
60. Neale MC, Cardon LR. Methodology for genetic studies oftwins and families. Norwell, Massachusetts: Kluwer, 1992.
61. Lyons MJ, True WR, Eisen SA, Goldberg J, Meyer JM, Far-aone SV, et al. Differential heritability of adult and juvenileantisocial traits. Arch Gen Psychiatry 1995;52:906–15.
62. Slutske WS, Heath AC, Dinwiddie SH, Madden PA, BucholzKK, Dunne MP, et al. Modeling genetic and environmental in-fluences in the etiology of conduct disorder: a study of 2,682adult twin pairs. J Abnorm Psychol 1997;106:266–79.
63. Lytton H. Child and parent effects in boys’ conduct disorder: areinterpretation. Dev Psychol 1990;26:683–97.
64. Rutter M. Family discord and conduct disorder: cause, conse-quence, or correlate? J Fam Psychol 1994;8:170–86.
34. Boomsma DI, Koopmans JR, Van Doornen LJP, Orlebeke JF.Genetic and social influences on starting to smoke: a study ofDutch adolescent twins and their parents. Addiction 1994;89:219–26.
35. Heath AC, Madden PAF. Genetic influences on smoking be-havior. In: Turner JR, Cardon LR, Hewitt JK, eds. Behaviorgenetic approaches in behavioral medicine: perspectives on in-dividual differences. New York: Plenum, 1995:45–66.
36. Heath AC. Persist or quit? Testing for a genetic contributionto smoking persistence. Acta Genet Med Gemellol (Roma)1990;39:447–58.
37. Heath AC, Madden PAF, Slutske WS, Martin NG. Personalityand the inheritance of smoking behavior: a genetic perspec-tive. Behav Genet 1995;25:103–17.
38. Heath AC, Martin NG. Genetic models for the natural historyof smoking: evidence for a genetic influence on smoking persis-tence. Addict Behav 1993;18:19–34.
39. Peto R, Lopez AD, Boreham J, Thun M, Heath C, Doll R. Mor-tality from smoking worldwide. Br Med Bull 1996;52:12–21.
40. Raaschou-Nielsen E. Smoking habits in twins. Dan Med Bull1960;7:82–8.
41. Marks MJ, Campbell SM, Romm E, Collins AC. Genotype in-fluences the development of tolerance to nicotine in the mouse.J Pharmacol Exp Ther 1991;259:392–402.
42. Pomerleau OF. Individual differences in sensitivity to nico-tine: implications for genetic research on nicotine dependence.Behav Genet 1995;25:161–77.
43. Pomerleau OF, Collins AC, Shiffman S, Pomerleau CS. Whysome people smoke and others do not: new perspectives. JConsult Clin Psychol 1993;61:723–31.
44. Maletzky BM, Klotter J. Smoking and alcoholism. Am J Psy-chiatry 1974;131:445–7.
45. Cyr MG, Wartman SA. The effectiveness of routine screeningquestions in the detection of alcoholism. JAMA 1998;259:51–4.
46. Johnson KA, Jennison KM. The drinking-smoking syndromeand social context. Int J Addict 1992;27:749–92.
47. Olsen J, Sabreo S, Fasting U. Interaction of alcohol and to-bacco as risk factors in cancer of the laryngeal region. J Epide-miol Community Health 1985;39:165–8.
48. True WR, Xian H, Scherrer JF, Madden PAF, Bucholz KK,Heath AC, et al. Common genetic vulnerability for nicotineand alcohol dependence in men. Arch Gen Psychiatry 1999;56:655–61.
49. Prescott CA, Kendler KS. Genetic and environmental influ-ences on alcohol and tobacco dependence among women. In:Fertig JB, Allen JP, eds. Alcohol and tobacco: from basic sci-ence to clinical practice. Bethesda, Maryland: National Insti-tutes of Health, 1995:59–87.
50. Swan, GE, Carmelli D, Cardon LR. The consumption of to-
Harvard Rev Psychiatry
Volume 9, Number 6 Tsuang et al. 279

Related Documents











