THE GALLBLADDER AND THE BILIARY TREE BY MICHAEL BRILLANTES, MD, FPCS, FPSGS

THE GALLBLADDER AND THE BILIARY TREE BY MICHAEL BRILLANTES, MD, FPCS, FPSGS.
Dec 24, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

THE GALLBLADDER AND THE BILIARY TREE
BY
MICHAEL BRILLANTES, MD, FPCS, FPSGS
ANATOMY
• Gallbladder
• Bile ducts
• Blood Supply
• Anomalies
1.Gallbladder- most common is an intrahepatic gallbladder
2.Bile Ducts- most common is a CBD and cystic duct that runs parallel
3.Blood Supply- most common is a right hepatic from the superior mesentric artery


PHYSIOLOGY
• Concentrates bile by absorption of water and sodium
• Stimulus for gallbladder emptying is cholecystokinin (CCK-PZ) secondary to fat in the GIT
• Truncal vagotomy promotes stasis
• Composition of bile:
1.Cholesterol- 5%
2.Bile Salts – 80%
3.Lecithin – 15%
PATHOLOGY
GALLSTONES- approx. 10%of population
Pathogenesis:
1.Cholesterol Stones
Process:
a. Cholesterol saturation – crystallization
b. Nucleation- agglomeration of crystals

CLINICAL MANIFESTATIONS:
1.ASYMPTOMATIC- up to 50%, usually incidental findings
• No surgery needed for most• EXCEPTIONS:
1.High risk patients undergoing a laparotomy for another problem
2.Good risk patients
- Diagnosis: Ultrasound



2. Biliary Colic- self- limited, usually 2-3 hours bec. Of stones obstructing the cystic duct dislodges
•Recurrent biliray colic- the most common reason for cholecystectomy
3. Acute Cholecystitis
•Impacted stone in the cystic duct
•Murphy’s sign: inspiratory arrest on deep palpation of the RUQ
•WBC count >20,000, consider gangrenous cholecystitis
•Diagnosis: a. Scintigraphy/HIDA scan
b. Ultrasound

4. Gallstone pancreatitis
•Caused by transient obstruction of the ampulla of Vater causing reflux of the bile and pancreatic enzymes into the pancreatic duct causing obstruction of pancreatic parenchyma
•Wait for clinical improvement of pancreatitis to subside before cholecystectomy is done; cholecystectomy is usually done within the same hospital stay
•if patient deteriorates while being observed and supported, exploration or ERCP should be done
Diagnosis- ultrasoundTreatment
a. Open cholecystectomyc. Laparoscopic cholecystectomyd. Medical dissolution-inhibits HMG- COAe. Chenodeoxycholic acidf. Urosdeoxycholic acidg. Contact dissolution- methyl- terbutyl ether

View from laparoscopic View from laparoscopic cholecystectomycholecystectomy

View from open cholecystectomy View from open cholecystectomy


Complications
a. Hydrops- accumulation of mucoid material within the gallbladder with no inflammation and infection
b. Empyema- intramural abscess of the gallbladder
•Patient is toxic, w/ fever and leukocytosis
•Emergency cholecystectomy is needed
c. Emphysematous cholecystitis
•Gas within the gallbladder wall with ischemi necrosis
•Cl. Welchii, E. coli, Klebsiella
•Seen primarily in diabetics
•Emergency cholecystectomy is needed
d. Perforation with gallstone ileus
i. Free perforation
ii.Sub acute perforation with abscess formation
iii.Fistula formation
e. Acalculous cholecystits- seen in critically ill patients
•Urgent cholecystectomy needed
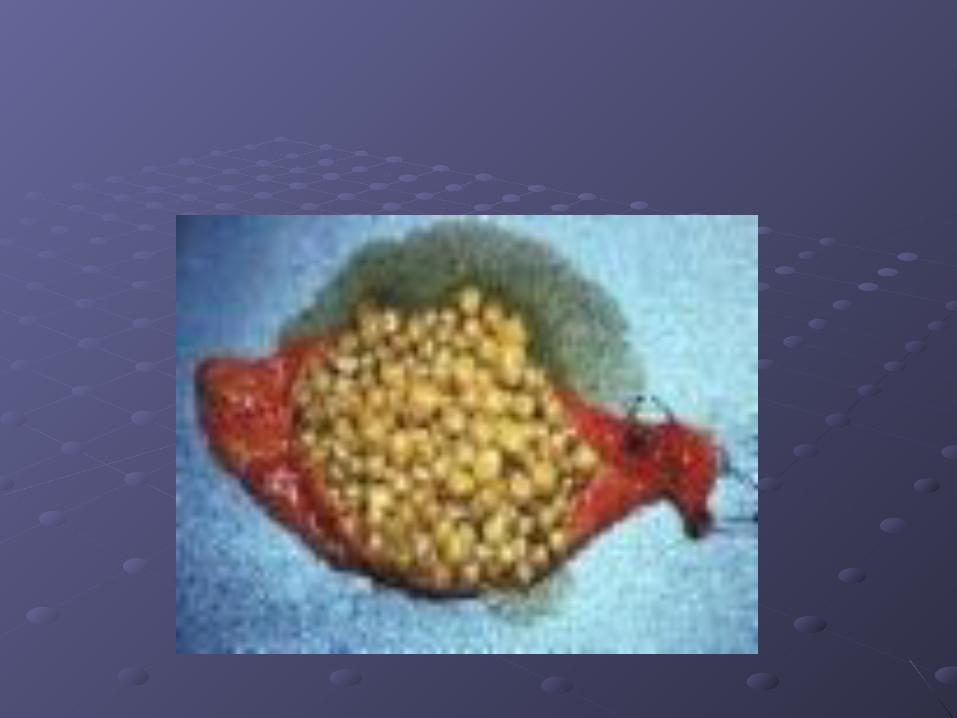
f. Hyperplastic Cholecystoses- symptomatic cholecystectomy
•Cholesterolosis- cholesterol deposits in the wall; “strawberry” gallbladder
•Adenomyosis- hyperplasia of the mucosa and the muscle layer


COMMON BILE DUCT STONES
Types
1.Primary Stones
•Arising from the bile ducts; usually caused by organisms that contain beta- glucoronidase such as E. coli
•Beta- glucoronidase deconjugates bilirubin diglucorinade into bilirubin and glucuronic acid
•Bilirubin binds with calcium to form calcium bilirubinate stones

Endoscopic Retrograde Endoscopic Retrograde CholangioPancreatographyCholangioPancreatography
Percutaneous Transhepatic Percutaneous Transhepatic CholangiographyCholangiography

Magnetic Resonance Imaginng Magnetic Resonance Imaginng CholangioPancreatographyCholangioPancreatography
2. For primary stones- cholecystectomy with:2. For primary stones- cholecystectomy with:
i.i. SphincteroplastySphincteroplasty
ii.ii. CholedochoduodenostomyCholedochoduodenostomy
iii.iii. CholedochojejunostomyCholedochojejunostomy
Inflammatory and Other Benign Diseases:
•Cholangitis
•Charcot’s triad
•RUQ Pain
•Fever
•Jaundice
•Reynold’s Pentad- Charcot’s Triad with signs of sepsis
•Neurologic change
•Hypotension
•Secondary to bacterobilia and obstruction with increased pressure within the CBD
•Bacteriology: E. Coli and Klebsiella

Treatment:Treatment:
IV and AntibioticsIV and Antibiotics
HydrationHydration
Biliary DecompressionBiliary Decompression
If patient is toxic (unstable and hypotensive), If patient is toxic (unstable and hypotensive), then just do CBD drainage with a T- tube the then just do CBD drainage with a T- tube the close; definitive operation can be done if patient close; definitive operation can be done if patient is stableis stable

Choledochal CystCholedochal Cyst
Clinical manifestation similar to obstruction of Clinical manifestation similar to obstruction of the CBD which are seen until adulthoodthe CBD which are seen until adulthood
Recurrent bouts of cholangitisRecurrent bouts of cholangitis
Types of cyst
Type I- fusiform dilatation of extrahepatic biliary tract
Type II- diverticulum of extrahepatic biliary duct
Type III- Choledochocoele
Type IV- Multiple intra and extrahepatic bile duct cysts
Type V- Single or multiple intrahepatic bile duct cysts

TreatmentTreatment
Resection depending on the type (due to Resection depending on the type (due to malignant potential)malignant potential)
ReconstructionReconstruction

Tumors:
A. Gallbladder
•Pathology- usually adenocarcinoma
•Chronic presence of stones
•Calcified or porcelain gallbladder

Clinical Manifestation
•Similar to GB disease
•Jaundice in advanced stage
•Weight loss, anorexia, nausea
Treatment
•Cholecystectomy with wedge resection of the liver and hyphadenectomy

B. Bile Ducts- Cholangiocarcinoma
•Pathology- adenocarcinomas
•Hilar or proximal- most common
•Mid-duct
•Distal Bile Duct
•Diffuse

Clinical Manifestation
•Acholic Stool
•Tea- colored urine
•Jaundice
•Pruritis

Diagnosis
•Ultrasound
•CT scan
•ERCP or PTC
Treatment
•Resection with Biliary reconstruction
•Whipple’s procedure
Related Documents











